Fibromyalgia is a chronic pain disorder affecting millions and mostly women. It is physically and emotionally distressing. Those with the condition experience widespread chronic muscle pain. Research has shown that individuals with fibromyalgia could have a lower threshold for pain. This can come from injury, emotional distress, or abnormal levels of substances/chemicals in the brain and spine linked to pain sensitivity. One of the most common treatments is chiropractic medicine.
Common symptoms/conditions individuals report:
Chronic fatigue syndrome
Irritable bladder
Irritable bowel syndrome
Migraines
Sleep disorders
Restless legs syndrome
TMJ or Temporomandibular joint disorder
Raynaud’s Syndrome�-�a�rare blood vessel disorder causing the toes and hands to feel cold or numb.
Doctors are still trying to figure out the relationship between these conditions and fibromyalgia.
Causes
Doctors have yet to determine the exact cause, however, research is ongoing and beginning to shed light on the condition. Some possible causes include:
Abnormalities in the endocrine system
Abnormalities in the autonomic nervous system
Genetics
Muscle tissue abnormalities
Abnormal blood flow
As research has discovered many conditions/disorders do not have one cause but rather, several factors that impact the probability of developing the condition.
Questions
It has become one of the most common chronic pain conditions. 1 in 50 Americans are dealing with fibromyalgia. The condition can be difficult to diagnose, and, because of its chronic nature, it can linger for months and even years. Typically it causes pain throughout the body and creates areas that become tender to the slightest touch. There are both traditional and alternative treatments available.
Traditional approaches to manage the pain:
Anti-inflammatory’s
Over-the-counter pain relievers
Sleep medications
Muscle relaxants
Fibromyalgia medications include:
Lyrica – pregabalin, which is a nerve pain medication
Cymbalta – duloxetine hydrochloride, which is an antidepressant that can also help manage pain
Savella – milnacipran HCI, which is an antidepressant and nerve pain medicine
The type of treatment depends on the symptoms. For example, a doctor could prescribe an antidepressant to reduce pain and depression. If stress, anxiety, and trouble sleeping are presenting,�a therapeutic exercise program could be the answer. Individuals prefer natural remedies/therapies instead of more medications like vitamin therapy, acupuncture, and meditation.
Other treatment options include alternative treatments like:
The most common issue is constant and consistent pain, which can affect the entire body for weeks and even months. Individuals realize that chiropractic helps restore overall health and aids the body to heal itself. Adjustments to the spine bring alignment and balance back to the body. Also incorporated is soft tissue work that can relieve and reduce painful pressure/trigger points and decrease pain in tender spots.
Range of motion is increased
Chiropractic medicine also adjusts the body’s joints and helps loosen them up. This increases the range of motion and allows the individual to move more freely and easily. Depending on how long the individual has been dealing with the condition, it can take a few treatments to achieve optimal results, so it does take a commitment from the individual patient. However, in the long run, it is well worth the time.
Sleep is improved
The pain associated with fibromyalgia often affects an individual’s ability to sleep well. Being unable to sleep normally will leave you exhausted, foggy, unable to accomplish things and irritable to downright angry. A chiropractor’s ability to loosen the body’s joints, massage tender points, and kickstart the body’s self-healing mechanisms means individuals with this condition can enjoy deep sleep, and stay asleep.
Complements other therapies
Medicines/treatments/therapies can counteract with each other, or get mixed up and cause side effects. Chiropractic medicine can be utilized in combination with medications/treatments, either traditional or natural. Individuals diagnosed with this condition should speak to their chiropractor about the different treatments available. Customized treatment programs are created case-by-case and are tailored to the specific needs of that individual. Remember there is not a one-stop solution.
Empowers the individual
Individuals that have to deal with painful, chronic conditions can exhaust themselves with the varying treatment options and can feel as if they have no control over the situation. This causes stress, anxiety, and depression, which works against achieving overall wellness. With chiropractic, individuals are more in charge of their treatment plan, which leads to an optimistic outlook in their recovery.�
Chiropractic medicine treats not only the symptoms of fibromyalgia but attempts to get to the root cause to alleviate the condition or to activate the body’s self-healing response. Patients that commit will see the benefits along with reduced pain, better mobility, and sound sleep.
The best benefit is being able to take control of the circumstances and playing a vital role in the managing of an individual’s well-being. Understand that there are options available for fibromyalgia pain management. If you or a loved one has been diagnosed with fibromyalgia, don�t go it alone. Dr. Alex Jimenez is passionate about helping those who are injured or struggling with a condition get relief. Contact us today to schedule an appointment.
If you are experiencing any of these situations, then you might be experiencing fibromyalgia.
Fibromyalgia is a common and chronic syndrome that causes pain and mental distress in the body. It causes widespread musculoskeletal pain, and it is accompanied by fatigue, sleep memory, and mood issues to the body.�The symptoms may be similar to arthritis; however, fibromyalgia is a rheumatic condition and causes soft tissue pain or myofascial pain.
There are three symptoms that fibromyalgia causes a person to have discomfort in their daily lives. They are:
Widespread pain: This pain is associated with fibromyalgia, and it is described as a constant dull ache that can last for at least three months. For it to be considered as widespread pain, it must occur both sides of the body, as well as above and below the waist.
Fatigue:Individuals with fibromyalgia often awaken tired, even though they have been sleeping for long periods. The pain that fibromyalgia causes can disrupt the person’s sleep patterns, causing them to have sleep disorders such as restless legs syndrome and sleep apnea.
Cognitive difficulties: This symptom is commonly known as �fibro fog.� It impairs the person�s ability to focus, pay attention, and concentrate on mental tasks.
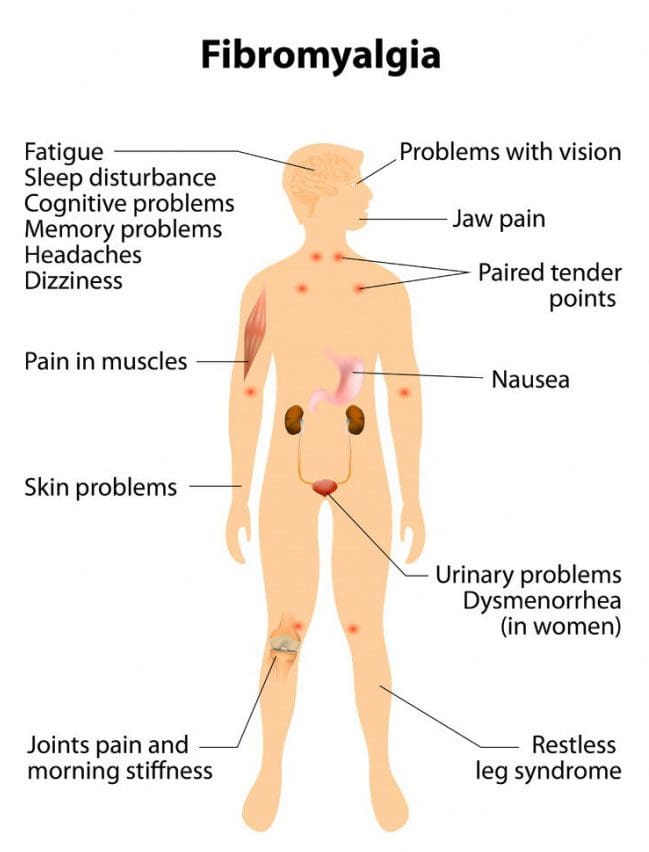
Other symptoms can include:
IBS (irritable bowel syndrome)
Stiff joints and muscles in the morning
Headaches
Problems with vision
Nausea
Pelvic and urinary problems
Depression and anxiety
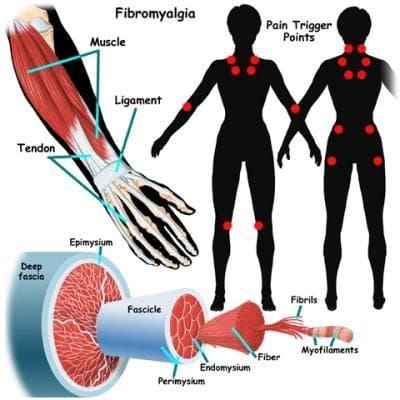
In the past, studies have shown that patients diagnosed with fibromyalgia had 11 out of 18 specific trigger points all around their bodies. Healthcare providers would check their patients and document how many of these points were painful to their patients by firmly, but gently, pressing their bodies to get a diagnosis.
The typical trigger points include:
The back of the head
The tops of the shoulders
The upper chest
The hips
The knees
The outer elbows
Nowadays, in a 2016 revised diagnostic criteria, healthcare providers can diagnose patients with fibromyalgia if the patient has pain in 4 out of 5 areas of the body that is causing them pain. The protocol when diagnosing patients is referred to as �multisite pain.�
Fibromyalgia Affecting the Endocrine System
When it comes to fibromyalgia, the symptoms are associated with the endocrine system. Research shows that fibromyalgia-like symptoms such as muscle pain and tenderness, exhaustion, reduced exercise capacity, and cold intolerance can resemble symptoms that are associated with the endocrine dysfunction like hypothyroidism and adrenal or growth hormone insufficiency.
More research has stated that fibromyalgia causes a person to develop chronic fatigue syndrome. Chronic fatigue syndrome causes the body to have a deficiency of serotonergic activity and the hypofunction of sympathetic nervous system function that could contribute to the abnormalities of the central components of the HPA axis. It can distort the body’s hormonal pattern that is being attributed to the hyperactivity of the CRH neurons. The hyperactivity caused by the CRH neurons can be driven and sustained by stress being exerted by chronic pain that has originated in the musculoskeletal system or the alternation of the central nervous system mechanism of nociception.
Researchers believe that repeated nerve stimulation causes the brains of patients with fibromyalgia to change. The change causes an abnormal increase level of certain chemicals (neurotransmitters) in the brain that signals pain. In addition, the brain�s pain receptors will develop a sort of memory of the pain that is causing problems to the patient�s body and causing them to be more sensitive since the signals are overreacting.
Treating Fibromyalgia
Even though fibromyalgia pain can be uncomfortable and consistent enough to interfere with a person�s daily routine. There are ways to relieve the pain and inflammation that fibromyalgia causes the body. Pain medication can bring down the inflammation and help a person sleep a little better. Other safe treatments that can help manage fibromyalgia pain are:
Acupuncture: Acupuncture is a Chinese medical system that uses needles to cause changes in the blood flow and the levels of neurotransmitters in the brain and spinal cord.
Therapy: A variety of different therapies can help a person reduce the effects that fibromyalgia has caused.
Yoga and tai chi: These practices combine meditation, slow movements, deep breathing, and relaxation � both help control fibromyalgia symptoms.
Reducing stress: Developing a plan to avoid or limit overexertion and emotional stress is useful when dealing with fibromyalgia. Learning to meditate and trying stress management techniques can help a person feel calm and recharged for the rest of the day.
Getting enough sleep: Since fatigue is one of the main characteristics of fibromyalgia, getting enough sleep is essential. Practicing good sleep habits and going to bed and getting up at the same time each day can lessen the effects of fatigue.
Exercising regularly: At first, exercising may increase the pain, but doing it gradually and regularly over time can decrease the symptoms. This can be walking, swimming, biking, and water aerobics can be beneficial to the body.
Pacing yourself: Keeping track of activities is beneficial for people with fibromyalgia. Moderation of daily activities on the good days can help a person overcome the symptoms when they flare-up.
Maintaining a healthy lifestyle: Eating healthy food that has anti-inflammatory properties can be useful for the body, and finding enjoyable hobbies can be beneficial as well.
Conclusion
Fibromyalgia is a chronic illness that causes pain and inflammation that affects the soft tissue in the body. The symptoms can resemble joint inflammation and causes people to have fatigue and discomfort all over their body. When these symptoms flare up, it can cause body damage. Treatments can help a person reduce the effects of fibromyalgia and be beneficial. Some products are formulated to counter the effects of temporary stress and offer support in the gastrointestinal system and the body�s metabolism.
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues as well as functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or chronic disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at�915-850-0900�.
References:
Felman, Adam. �Fibromyalgia: Symptoms, Causes, and Treatment.� Medical News Today, MediLexicon International, 5 Jan. 2018, www.medicalnewstoday.com/articles/147083.php.
Geenen, Rinie, et al. �Evaluation and Management of Endocrine Dysfunction in Fibromyalgia.� Rheumatic Diseases Clinics of North America, U.S. National Library of Medicine, May 2002, www.ncbi.nlm.nih.gov/pubmed/12122926.
Neeck, G, and L J Crofford. �Neuroendocrine Perturbations in Fibromyalgia and Chronic Fatigue Syndrome.� Rheumatic Diseases Clinics of North America, U.S. National Library of Medicine, Nov. 2000, www.ncbi.nlm.nih.gov/pubmed/11084955.
Staff, Mayo Clinic. �Fibromyalgia.� Mayo Clinic, Mayo Foundation for Medical Education and Research, 11 Aug. 2017, www.mayoclinic.org/diseases-conditions/fibromyalgia/symptoms-causes/syc-20354780.
Staff, Mayo Clinic. �Fibromyalgia.� Mayo Clinic, Mayo Foundation for Medical Education and Research, 11 Aug. 2017, www.mayoclinic.org/diseases-conditions/fibromyalgia/diagnosis-treatment/drc-20354785.
Unknown, Unknown. �Fibromyalgia.� National Institute of Arthritis and Musculoskeletal and Skin Diseases, U.S. Department of Health and Human Services, 30 Sept. 2019, www.niams.nih.gov/health-topics/fibromyalgia.
Wolfe, Frederick, et al. �2016 Revisions to the 2010/2011 Fibromyalgia Diagnostic Criteria.� Seminars in Arthritis and Rheumatism, W.B. Saunders, 30 Aug. 2016, www.sciencedirect.com/science/article/abs/pii/S0049017216302086?via%3Dihub.
Gluteus Tendinopathy and Sciatica Symptoms in Fibromyalgia
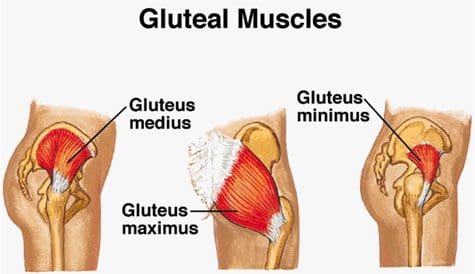
Gluteus medius tendinopathy (GMT), also known as dead butt syndrome (DBS), is a painful health issue caused by the inflammation of the tendons in the gluteus medius muscle. The gluteus medius (GM) is one of the smallest, less-known muscles of the buttocks which ultimately functions by providing stability and support to the structures of the hip and pelvis, especially throughout weight-bearing physical activities. Although GMT most commonly affects athletes, it can also affect people starting a new exercise program, during an intense workout routine or due to an underlying health issue. �
Healthcare professionals have reported an increased number of GMT cases over the past several years. While many doctors and functional medicine practitioners believe that this may perhaps be due to how many people participate and engage in exercise or physical activities after sitting down for extended periods of time, many GMT cases may actually be due to a well-known health issue called fibromyalgia. In the following article, we will discuss gluteus medius tendinopathy (GMT), or dead butt syndrome (DBS), fibromyalgia and how these two conditions can also be associated with sciatica symptoms. �
�
Sciatica and Gluteus Medius Tendinopathy Causes in Fibromyalgia
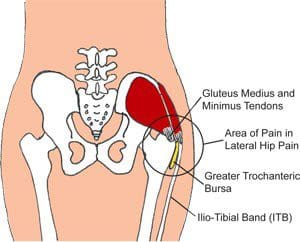
The common symptoms associated with gluteus medius tendinopathy, or GMT, include pain and discomfort, stiffness, and weakness in the hip or buttocks region. The painful symptoms can generally worsen throughout weight-bearing exercises, such as walking, running, and/or climbing. For many people, the pain and discomfort associated with dead butt syndrome, or DBS, can radiate down the hips, buttocks, and legs or thighs, similar to sciatica and hamstring tendinopathy. Sciatica is a collection of symptoms characterized by pain and discomfort, tingling sensations, and numbness along the sciatic nerve. �
Many patients diagnosed with GMT also report experiencing painful symptoms when lying in bed on the affected hip or buttocks region as well as pain, discomfort, stiffness, and weakness throughout the night and upon rising in the morning. Moreover, if DBS progresses past the initial stage, the hip bursa may become inflamed, another health issue known as trochanteric bursitis, which may also cause swelling, tenderness, redness or warmth in the hip. In people with fibromyalgia, the widespread pain and discomfort caused by the inflammation of the condition may also ultimately cause GMT symptoms. �
The role of the gluteus medius muscle is to contract the weight-bearing hip throughout walking and running. When this small, lesser-known muscle triggers, the hip flexors release and vice versa. However, when the tendon becomes inflamed due to an injury or an aggravated underlying condition, such as fibromyalgia, the gluteus medius can fail to trigger appropriately, hence why the “dead butt” term is utilized as an alternate name for this health issue. People sitting down for extended periods of time may cause their hip flexors to become tight and failure to stretch before physical activities can cause DBS. �
Furthermore, poor gluteal or buttocks and hip muscle control cause excess stress on the gluteal medius tendon and/or muscle. Several athletes, especially runners, generally avoid utilizing cross-training and weight-lifting in order to help strengthen the larger muscles which support the pelvis when running, however, the hip’s and buttock’s smaller tendons and muscles may take on the excess pressure. If left untreated, gluteus medius tendinopathy (GMT), or dead butt syndrome (DBS) may lead to complications,�including trochanteric bursitis, IT band syndrome, and plantar fasciitis, among other health issues.
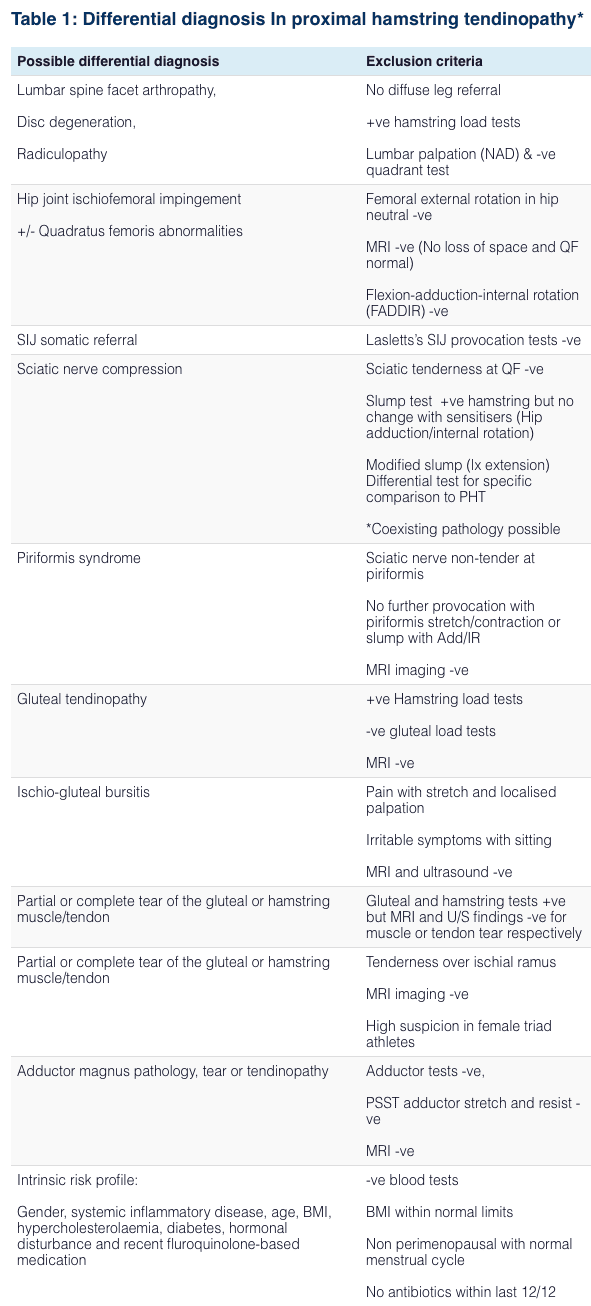
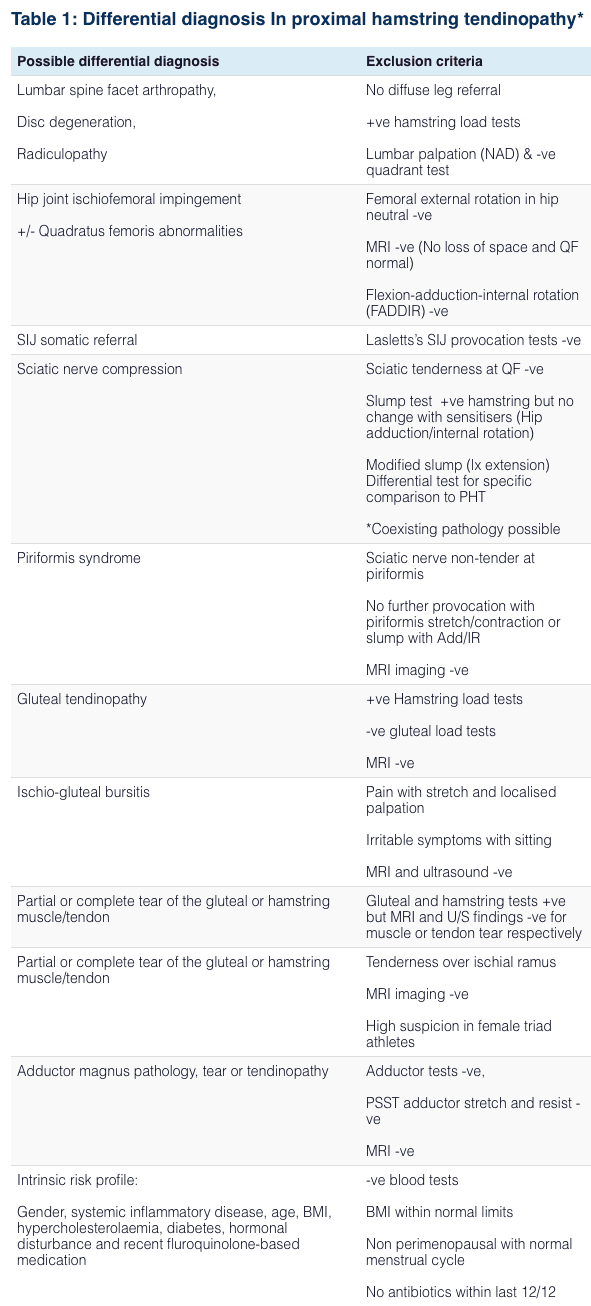
Differential Diagnosis of Hip Pain and Discomfort
� �
Fibromyalgia is widespread pain and discomfort throughout the human body. People with this painful condition can experience a variety of symptoms, including sciatica or sciatic nerve pain. Doctors and functional medicine practitioners believe that fibromyalgia can aggravate how the human body feels painful sensations by affecting how the human brain processes pain signals. Fibromyalgia and sciatica are two well-known conditions which can commonly coexist together. However, many fibromyalgia sufferers have also reported experiencing gluteal medius tendinopathy (GMT), or dead butt syndrome (DBS), a painful health issue caused by the inflammation of the tendons in the gluteus medius muscle. Because fibromyalgia is often associated with increased inflammation and painful symptoms, GMT or DBS and sciatica can commonly develop together. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
�
Fibromyalgia Magazine
People with fibromyalgia experience widespread pain and discomfort as a result of their medical condition, however, healthcare professionals have demonstrated that fibromyalgia may also cause other symptoms and health issues to manifest, such as sciatica, or sciatic nerve pain, and gluteal tendinopathy. The purpose of the article above was to demonstrate and compare fibromyalgia, sciatica and gluteal tendinopathy symptoms. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900�. �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Severe Sciatica
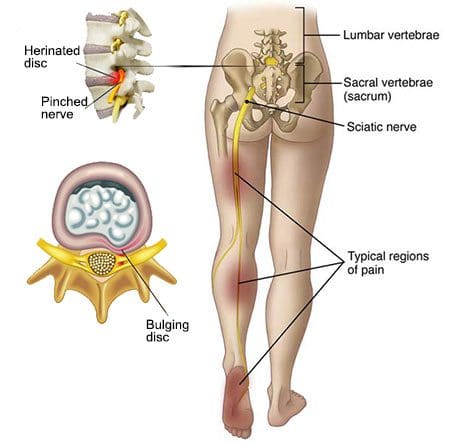
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. Your spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of sciatica, or sciatic nerve pain. Sports injuries or automobile accident injuries are often the most frequent cause of painful symptoms, however, sometimes the simplest of movements can have these results. Fortunately, alternative treatment options, such as chiropractic care, can help ease sciatic nerve pain, or sciatica, through the utilization of spinal adjustments and manual manipulations, ultimately improving pain relief. �
�
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force. �
Fibromyalgia and sciatica are two well-known health issues which can commonly occur at seemingly the same time in people, however, these may also frequently require different treatment approaches to help manage their painful symptoms. Fibromyalgia is characterized by widespread pain throughout numerous regions of the human body. As complex as the diagnosis and treatment for fibromyalgia might be, it’s ultimately fundamental for patients to be aware of any other conditions which may subsequently develop due to the painful symptoms of these well-known health issues. �
Sciatica, also known as sciatic nerve pain, is a collection of symptoms rather than a single condition and it is one of the most common health issues to coexist together with fibromyalgia. In this instance, one condition doesn’t necessarily cause the other, however, they can basically be present together. Fibromyalgia�patients should understand how sciatica and its characteristic symptoms can affect their overall health and wellness. Many people with fibromyalgia may subsequently develop other health issues when these painful symptoms overlap with other conditions, such as piriformis syndrome. �
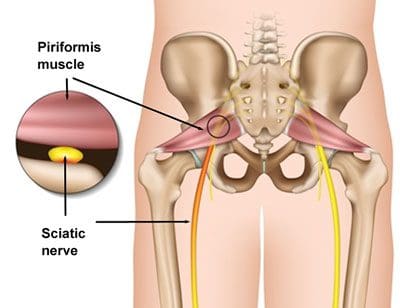
Piriformis Syndrome vs Sciatica and Fibromyalgia
People with sciatic nerve pain, or sciatica, will often report experiencing pain and discomfort, tingling sensations, and numbness anywhere along the length of the sciatic nerve. The sciatic nerve is the longest and largest nerve in the human body, which travels from the lower back into the hip and buttocks, down into the thighs, knees, legs, and feet. Healthcare professionals may perform a variety of evaluations and tests to determine the source of a patient’s symptoms. People with fibromyalgia and sciatica may also experience another common health issue known as piriformis syndrome. �
Sciatica is caused by the compression or impingement of the sciatic nerve, frequently due to a herniated disc. Piriformis syndrome can cause sciatica when a piriformis muscle spasm irritates the sciatic nerve. The piriformis is a muscle which extends from the front of the sacrum, or the triangle-shaped bone between the two hipbones in the pelvis, across the sciatic nerve and into the top of the femur, or the large bone in the upper leg.� The piriformis muscle is fundamental because it allows the thighs to move from side to side. When an injury or underlying condition causes the piriformis muscle to compress or impinge the sciatic nerve due to irritation and/or inflammation, the end result is typically piriformis syndrome. �
�
Sciatica is the most common symptom associated with piriformis syndrome. Other common symptoms associated with piriformis syndrome include tingling sensations and numbness, muscle tenderness, pain and discomfort while sitting or engaging in physical activities, and difficulty sitting comfortably. Because fibromyalgia causes widespread pain and inflammation, it’s also fundamental for people with fibromyalgia to seek immediate medical attention to diagnose all of their symptoms and rule out the possibility of their sciatica symptoms being due to piriformis syndrome or any other health issue. �
As previously mentioned above, sciatica, or sciatic nerve pain, is a medical condition or rather a collection of symptoms which causes pain and discomfort anywhere along the entire length of the sciatic nerve. For both fibromyalgia sufferers and people with the health issue alone, the pain and discomfort will generally manifest on one or both sides of the hips, buttocks, and thighs, where it will then radiate down the back of the leg, knees, and feet. In some instances, other common symptoms may manifest along the lower extremities, including tingling sensations, burning sensations, numbness, and weakness.
Sciatic nerve pain is most frequently caused by a slipped disc, a bulging disc, a herniated disc, or any other health issue which ultimately causes nerve pain and discomfort, such as fibromyalgia. When sciatica due to piriformis syndrome and/or another medical condition is experienced by fibromyalgia sufferers, it may be difficult for healthcare professionals to find the true source of their painful symptoms. Also, the symptoms associated with sciatic nerve pain and piriformis syndrome are generally the same for fibromyalgia sufferers, however, the most common causes may not be responsible for the symptoms.
Differential Diagnosis in Hip Pain
�
Fibromyalgia is characterized as widespread pain and discomfort throughout the human body. People with this painful health issue can experience a variety of symptoms, including sciatic nerve pain, or sciatica. Healthcare professionals believe that fibromyalgia can increase the way the human body experiences painful sensations by affecting the way the brain processes pain signals. Fibromyalgia and sciatica are two well-known conditions which can commonly coexist together. However, many fibromyalgia sufferers have reported piriformis syndrome, a condition caused when the piriformis muscle irritates the sciatic nerve. Because fibromyalgia can often be associated with increased pain and inflammation, these painful symptoms and health issues can ultimately occur. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
�
Fibromyalgia Magazine
�
�
People with fibromyalgia experience widespread pain and discomfort as a result of their medical condition, however, healthcare professionals have demonstrated that fibromyalgia may also cause other symptoms and health issues to manifest, such as sciatica, or sciatic nerve pain, and piriformis syndrome. The purpose of the article above was to demonstrate and compare fibromyalgia and sciatica symptoms versus piriformis syndrome. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900�. �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Severe Sciatica
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. Your spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of sciatica, or sciatic nerve pain. Sports injuries or automobile accident injuries are often the most frequent cause of painful symptoms, however, sometimes the simplest of movements can have these results. Fortunately, alternative treatment options, such as chiropractic care, can help ease sciatic nerve pain, or sciatica, through the utilization of spinal adjustments and manual manipulations, ultimately improving pain relief. �
�
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
*All of the above XYMOGEN policies remain strictly in force. �
Fibromyalgia is a disorder characterized by widespread musculoskeletal pain which is also generally accompanied by fatigue, sleep, memory, and mood health issues. The most common symptoms associated with fibromyalgia include muscle pain and tenderness, however, many people with this painful condition also experience sciatica, a collection of symptoms characterized by pain, discomfort, tingling sensations, and numbness along the length of the sciatic nerve in the lower back. �
Because fibromyalgia can cause painful symptoms throughout several regions of the human body, many people with fibromyalgia may also be diagnosed with other health issues which may overlap with their present symptoms, such as sciatica. It’s essential for patients to seek immediate medical attention from a healthcare professional to receive a proper diagnosis of all of their symptoms as these other health issues may generally require different treatment approaches. �
Sciatica is one of the most common health issues to coexist with fibromyalgia. Fibromyalgia doesn’t necessarily cause sciatica or sciatic nerve pain, however, these can ultimately exist together. It’s also essential for people with fibromyalgia to understand what sciatica is and how these painful symptoms can affect their health and wellness. Healthcare professionals believe that fibromyalgia amplifies painful sensations by affecting the way the human brain processes pain signals. Moreover, fibromyalgia can affect a variety of other structures and functions in the human body, such as the gastrointestinal tract. �
Fibromyalgia and Digestion Problems
Along with muscle pain and tenderness, patients with this painful disorder also experience digestive health issues. About 70 percent of people with fibromyalgia suffer from irritable bowel syndrome symptoms, including gas, bloating, constipation, and diarrhea. Although the causes of digestion health issues and fibromyalgia are unknown, healthcare professionals have demonstrated that there is an undeniable connection between fibromyalgia and digestive health issues. �
The gastrointestinal, or GI, system consists of several fundamental parts including, the esophagus, the stomach, the small intestine, and the bowel. When digestion slows down or a food intolerance, described in further detail below, disrupts the natural process of digestion, a chain of events can cause pain and discomfort, among other symptoms, throughout the entire gastrointestinal, or GI, tract. Patients with fibromyalgia commonly report frustrating digestive problems, such as: �
Acid reflux. When the gastric juices are not being utilized in the stomach, they can often travel back up through the esophagus, causing heartburn or a painful sensation in the chest, known as acid reflux.
Cramping and constipation. When the process of peristalsis, or the smooth muscle contractions which move food through the gastrointestinal tract, becomes affected due to the irritation of the intestines, it can begin to cramp and prevent the movement of waste through the bowel, causing cramping and constipation.
Diarrhea. When the digestive process slows down or stops, undigested food can move from the stomach and into the intestine, where it can irritate the lining of the colon and produce IBS symptoms, such as diarrhea.
Gas. The longer food stays in your stomach and intestines, the longer the natural GI bacteria has to break down the compounds and the more methane gas is produced from bacteria metabolism, resulting in gas.
Research studies have utilized brain scans to demonstrate the physiological responses of patients with irritable bowel syndrome, or IBS, and patients with fibromyalgia. According to the research studies, both groups of patients demonstrated higher neurological responses to pain. Patients with IBS and fibromyalgia also demonstrated higher pain awareness. Due to the similar brain activity to pain stimulus, researchers suspect that the two health issues may share underlying causes. �
Many people with fibromyalgia frequently report that certain types of foods irritate their stomach or exacerbate their fibromyalgia symptoms. Dairy and gluten, among other foods, can worsen fibromyalgia. Many people have food intolerances which can be challenging to diagnose. Another common explanation for the digestion problems of patients with fibromyalgia involves the autonomic nervous system, which is in charge of regulating the structure and function of internal organs. �
This autonomic nervous system is made up of two subsystems: the sympathetic nervous system and the parasympathetic nervous system, which rarely work together simultaneously. In patients with fibromyalgia, the sympathetic nervous system, which is largely responsible for increasing blood pressure, heart rate and adrenaline, is almost always active, causes the parasympathetic system, which is largely responsible for relaxation and digestion, to become inactive. Fortunately, patients with fibromyalgia and its associated symptoms like sciatica and digestive problems, can find relief through treatment.
�
Patients with fibromyalgia commonly experience widespread pain and discomfort, however, research studies have demonstrated a connection between other symptoms and health issues, such as sciatica and digestive problems. The purpose of the following article is to educate as well as discuss how fibromyalgia may be connected to other symptoms like sciatica and irritable bowel syndrome, among other digestive problems. By understanding how these symptoms and health issues are associated with fibromyalgia, patients and doctors can safely and effectively treat this painful condition and its symptoms. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
Non-Invasive Treatments for Chronic Low Back Pain
�
Fibromyalgia is a disorder characterized by widespread musculoskeletal pain accompanied by a variety of symptoms. Many people with this painful condition also experience sciatica and digestive problems. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900�. �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Severe Sciatica
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. Your spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of sciatica, or sciatic nerve pain. Sports injuries or automobile accident injuries are often the most frequent cause of painful symptoms, however, sometimes the simplest of movements can have these results. Fortunately, alternative treatment options, such as chiropractic care, can help ease sciatic nerve pain, or sciatica, through the utilization of spinal adjustments and manual manipulations, ultimately improving pain relief. �
�
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
� For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force. �
Although oral devices, such as splints and bite guards, are the most prevalent treatments for facial pain associated with temporomandibular disorders, or TMD, patients have found that these remedies are frequently less effective than self-care techniques, such as jaw exercises or warm compresses, according to a new research study published by researchers at the New York University (NYU) College of Dentistry in New York City.
The research study, published in the journal Clinical Oral Investigations, demonstrates that self-care techniques should primarily be utilized to help treat muscle-related temporomandibular disorders or TMD.
TMD, occasionally known as TMJ after the temporomandibular joint, is a collection of prevalent painful conditions which develop in the jaw joint and its surrounding muscles. Myofascial temporomandibular disorder, or mTMD, is a muscular condition which affects over 10 percent of women. Individuals with TMD often suffer from other chronic pain conditions. Research studies found that 7 to 18 percent of people with TMD also experience fibromyalgia, a condition characterized by widespread pain.
Treatments for TMD and Fibromyalgia
Dentists and patients utilize an assortment of treatments to help manage facial pain, such as oral devices like splints and bite guards, pain medicines, including nonsteroidal anti-inflammatory drugs, and self-care methods like jaw exercises and hot compresses.
Oral devices are a prevalent first-line treatment for TMD, regardless of research study outcome measures regarding their advantages, stated Vivian Santiago, Ph.D., MPH, research study scientist at the Department of Oral and Maxillofacial Pathology, Radiology, and Medicine at NYU College of Dentistry, and the research study’s leading author.
“While oral splints have been discovered to have some benefits, they have yet to be found to be as successful for patients who have widespread pain when treating mTMD,” she explained.
In this research study, the researchers evaluated what non-medication remedies women with mTMD utilized to handle their pain as well as how successful patients perceived these remedies. The researchers interviewed a total of 125 women including 26 women who had fibromyalgia and mTMD, so as to find out whether treatment differed for patients.
The most frequent treatments reported were oral devices (utilized by 59 percent of participants), physical therapy (utilized by 54 percent of participants), and at-home jaw exercises (utilized by 34 percent of participants). The least frequent treatments reported were acupuncture (utilized by 20 percent), chiropractic care (utilized by 18 percent), trigger point injections (utilized by 14 percent), yoga (utilized by 7 percent), and meditation (utilized by 6 percent). Participants frequently used more than one treatment.
Participants reported the most improvement in their pain from well-known self-care techniques, such as jaw exercises, yoga, meditation, massage, and warm compresses, with over 84 percent reporting that these techniques helped reduce painful symptoms. Only 64 percent of participants who used the oral devices reported that they helped improve their pain. About 11 percent of women who used oral devices stated that these made their pain worse, an area which warrants further research studies.
Oral devices failed to outperform self-care techniques in improving facial pain, according to Karen Raphael, Ph.D., professor at the Department of Oral and Maxillofacial Pathology, Radiology, and Medicine at NYU College of Dentistry, and the research study’s co-author.
“Our outcome measures encourage utilizing self-care techniques as the first line of treatment for mTMD before contemplating more costly interventions,” stated Raphael.
The researchers didn’t find substantial differences between the amount of remedies reported by women with and without fibromyalgia. While the use of alternative treatment options for mTMD was reported among women with fibromyalgia, further research studies are still required. Pain relief tended to be greater through the use of self-care techniques in women with and without fibromyalgia.
“While fibromyalgia is diagnosed by a healthcare professional, such as a rheumatologist, TMD is typically diagnosed and treated by a dentist,” said Santiago. “Our research study demonstrates that dentists must ask patients with facial pain if they also have widespread chronic pain because this might provide more information to help plan their treatment.”
Fibromyalgia is a health issue characterized by widespread chronic pain accompanied by fatigue, sleep, memory and mood problems. Fibromyalgia has been associated with a variety of other health issues, such as TMD and/or TMJ. Individuals with this painful disorder may often struggle to engage in their everyday physical activities. As a qualified and experienced chiropractor, I’ve helped treat numerous patients with fibromyalgia. It’s important for patients to know that they are not alone when it comes to treating their painful symptoms. Chiropractic care is an alternative treatment option which can help treat a variety of health issues, including fibromyalgia.
Dr. Alex Jimenez D.C., C.C.S.T. Insight
The scope of our information is limited to chiropractic, spinal health issues, and functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topic Discussion: Acute Back Pain
Back pain is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. Your spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly, Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download
* All the above XYMOGEN policies remain strictly in force.
I actually feel pretty good right away, just because I know what I need and he knows how to take care of my particular injury. So, I’m usually good to go, next day, after I get re-aligned. Without a shadow of a doubt. I like the way he treats his patients, I like the way he treats me and he gets it done for me. I would recommend Dr. Jimenez to anyone. He is incredible. He is awesome. And I think he can pretty much pinpoint a lot of the issues that you may have. – Carlos Hermosillo
The vast majority of people are capable of dealing with a little bit of pain. Some people may often experience the occasional aggravation from overdoing their workout at the gym or perhaps some people have experienced that sudden twinge out of hitting their shins on the mattress, however, most of the time, these symptoms can be easily dismissed through the use of an over-the-counter anti-inflammatory drug and/or medication and they can go about their everyday life again as usual. But when pain is much more widespread throughout the whole body and it starts to be accompanied with fatigue, changes in mood and sleep patterns, these people may be dealing with a more serious health issue: fibromyalgia.
What is Fibromyalgia?
Fibromyalgia is a medical term utilized to describe a group of symptoms, rather than a single condition. Ordinarily, someone who is experiencing debilitating fatigue, tender areas around their the body, changes in mood or muscular pain, it may be characterized as common symptoms associated with this particular illness. Even though many healthcare professionals are still not sure about what causes fibromyalgia, most believe the pain is due to an overactive sympathetic nervous system, the part of the human body which activates the fight or flight response. A great deal of individuals experience symptoms after a physically or emotionally traumatic event. Other individuals begin having pain after spells of chronic depression or anxiety although others have symptoms that grow gradually over time. Fibromyalgia has been demonstrated to impact more women than men and in the event that they’ve got a relative with the disease, they are more likely to develop it also.
How is Fibromyalgia Treated?
Because fibromyalgia is not considered to be a single illness but rather a collection of symptoms and since it’s cause is unknown, there is currently no known cure for fibromyalgia. Instead, healthcare professionals generally focus on improving as well as managing the symptoms, typically by prescribing pain drugs and/or medications. Frequently, in case the sympathetic nervous system does respond to drugs/medications, the pain will subside. Healthcare professionals usually prescribe a combination of pain drugs and/or medications, antidepressants or anti-seizure medication to achieve this sort of regulation and alleviate symptoms. However, this treatment approach only temporarily relieves the symptoms associated with fibromyalgia instead of treating the health issue at its source. Chiropractic care is a safe and effective, alternative treatment option which focuses on the diagnosis, treatment and prevention of a variety of injuries and conditions associated with the musculoskeletal and nervous system.
Dr. Alex Jimenez’s Insight
Many patients with fibromyalgia seek chiropractic care to help ease neck pain, back pain and leg cramps which are often common symptoms associated with this syndrome. Research studies have also demonstrated that spinal adjustments and manual manipulations can help relieve chronic pain. One research study evaluated the effectiveness of chiropractic care on relieving symptoms related to fibromyalgia. The outcome measures demonstrated a decrease in pain and fatigue as well as an increase in the quality of sleep of the patients. A chiropractor who specializes in patients with fibromyalgia can carefully correct the alignment of the spine, alleviating the chronic pain associated with fibromyalgia.
Chiropractic Care for Fibromyalgia
Although fibromyalgia cannot be cured, one of the most well-known ways of managing and improving your symptoms is with chiropractic care. Chiropractic care can help relieve fibromyalgia pain by�carefully correct any spinal misalignments, or subluxations, through the use of spinal adjustments and manual manipulations. A variety of research studies have also demonstrated that other treatment techniques, such as aerobic exercise together with postural strengthening activities, which not only alleviate widespread pain, but also increase energy levels, improve sleep and elevate mood. Through an appropriate treatment plan, a chiropractor can help balance your own body’s capability to control nerve impulses, thus relieving your fibromyalgia symptoms. Normally, chiropractic care can include the following treatment techniques, besides spinal adjustments and manual manipulations.
Cardiovascular Exercise
One of the best methods to alleviate widespread pain would be by means of low-impact movement. This may include exercises and physical activities, such as walking on a treadmill, water aerobics or other exercises aimed towards improving blood flow, reducing strain and increasing cardiovascular fitness. A doctor of chiropractic, or chiropractic, can prescribe an exercise and physical activities program designed to your abilities, in order to help relieve fibromyalgia pain and symptoms.
Muscle Strengthening and Range of Motion
If you are in pain, the human body’s natural tendency is to protect the area, or limit its motion from fear of causing aggravation. This limited mobility can weaken substantial muscle structures and functions which further limit your range of motion and lift your stress� levels. This vicious cycle can only be improved by working to strengthen weakened muscles and reunite range of motion to the area you have been guarding. But how can you do this if you are in pain? A chiropractor will combine special exercises and physical activities together with other treatment approaches in order to help promote a faster recovery as well as decrease the symptoms of pain. A chiropractor will also closely assess the patient to make sure they are performing the right treatments.
Pain Relieving Modalities
A doctor of chiropractic, or chiropractor, comprises a large number of tools aimed toward relieving pain without the need for drugs and/or medications. These may consist�of ice, heat, trigger point therapy, stretching, massage, electrical stimulation, or other therapeutic tools that can help limit your pain and retrain your body. With concentrated exercise together with a cardiovascular exercise program, it is very likely to retrain your body without triggering widespread pain. Whether you have a disease which cannot be cured, such as fibromyalgia, it is very likely to get relief in the worst indications throughout alternative treatment options. Contact a healthcare professional to schedule your evaluation and find out how we can get you on the road to recovery. The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Acute Back Pain
Back pain is one of the most prevalent causes for disability and missed days at work worldwide. As a matter of fact, back pain has been attributed as the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience some type of back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine








 �
� 
 �
�

 �
�
 �
�