Many people in the workplace suffer from back pain, which can limit and affect their ability to function and lead to a lifetime of discomfort and disability. Back pain can range from a dull, slow ache to a sharp, radiating pain and can cause the body to be misaligned. Fortunately, non-surgical treatments such as spinal decompression can help to relieve pain and discomfort. In this article, we will witness the impact of back pain in the workplace, how different occupations are associated with back pain, and how spinal decompression can help to alleviate these symptoms. We work with certified medical providers who use our patients’ valuable information to provide non-surgical treatments, including spinal decompression, to relieve pain-like symptoms associated with back pain in the workplace. We encourage patients to ask essential questions and seek education about their condition. Dr. Jimenez, D.C., provides this information as an educational service. Disclaimer
The Impact Of Back Pain In The Workplace
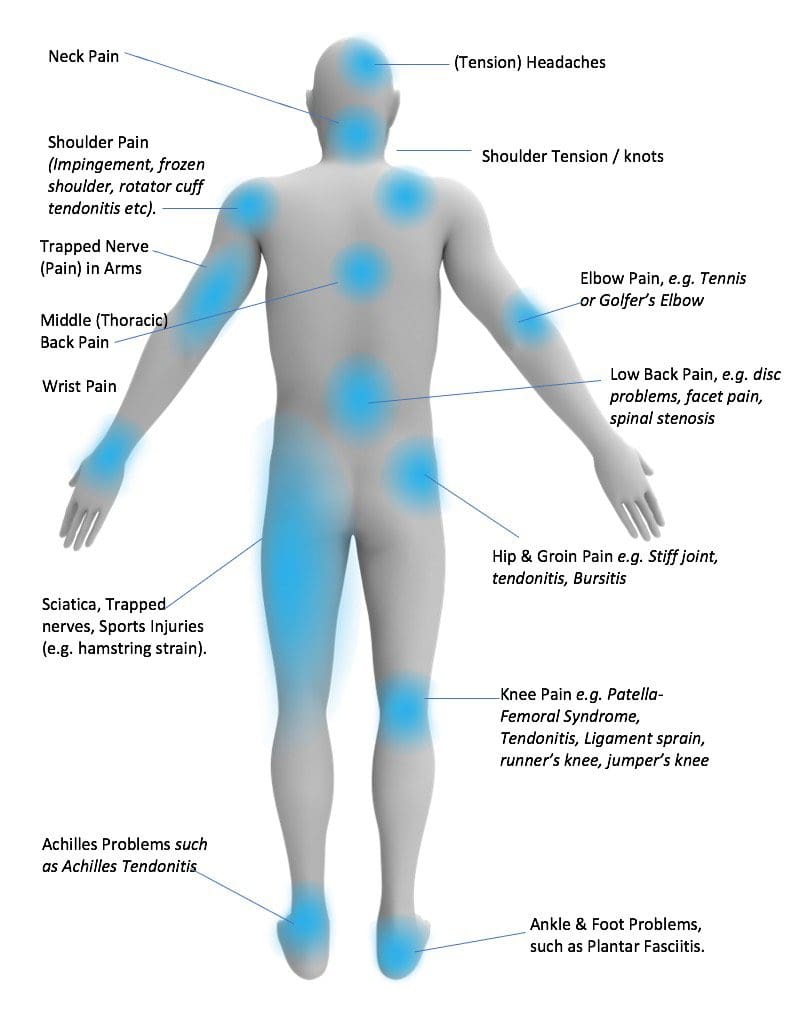
Are you experiencing headaches or neck tension? Do you feel pain radiating down your leg from sitting for extended periods? Or do you feel aches in your lower back after sitting at a computer for a long time? These symptoms could be due to the development of back pain. Research studies revealed that back pain is a common cause of missed work and reduced productivity. Depending on the severity, back pain has various mechanical or non-specific reasons. Some of the categories that many individuals in the workplace have back pain include:
Acute back pain: Last for a few days to a few weeks.
Subacute back pain: Last between 4 to 12 weeks.
Chronic back pain: Last longer than 12 weeks.
Occupations Associated With Back Pain
Back pain is a problem that many working individuals have experienced. This can lead to constant pain and compensating for the pain by using other muscle groups. Research studies revealed that both men and women in the workforce are affected by back pain, which can be influenced by psychological factors and can significantly impact their ability to perform occupational activities. Jobs like truck drivers, office workers, healthcare providers, and manual laborers are associated with back pain due to the physical demands of these occupations, increasing the risk of developing back pain. Some of the common causes associated with back pain at work include the back and surrounding muscles being under constant strain include:
Force: Exerting excessive force on the back muscles can cause injuries
Repetition: Repeating movements can lead to muscle strain on the surrounding muscles and affect the spine.
Inactivity: Sitting down for an extended period can lead to poor posture and cause the back muscles to be shortened.
Examples Of Workplace Conditions Associated With Back Pain
In many jobs, employees have to exert themselves physically, which can increase the risk of developing back pain. Some common workplace conditions that contribute to this risk include:
Using hands or body as a clamp to hold heavy objects while performing tasks.
Maintaining the same posture while performing tasks.
Performing motions constantly without small breaks in between.
Performing tasks that involve long reach, both vertical and horizontal.
Cold temperatures
Vibrating working surfaces, machinery, or vehicles.
The floor surface is uneven, slippery, or sloped.
Fortunately, there is hope for those experiencing back pain. Research studies have shown that available treatments can aid in modifying activities and improving workplace conditions, providing relief and preventing pain from returning.
Non-Surgical Treatments For Pain Relief-Video
If you’re experiencing back pain due to work-related strain, there are treatments available that can help alleviate the pain and reduce its effects from returning. Many people who work for a living suffer from this issue because of the physical demands of their job, which can lead to various risk factors. Fortunately, several non-surgical treatments are available to help reduce the symptoms of low back pain. Spinal decompression and chiropractic care are two examples of such therapies. These methods use traction, manual manipulation, and other techniques to restore the spine to its proper alignment and relieve back pain. Both treatments are gentle and non-invasive, as they work with the body’s natural healing process to stretch tight muscles and prevent future pain. The video above explains how these treatments can help enhance your body’s healing process and avoid recurring back pain.
Spinal Decompression Relieving Back Pain
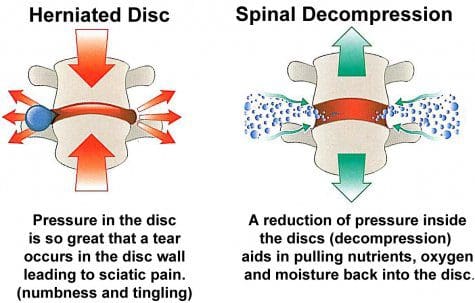
It’s important to know that putting too much pressure on your back can lead to back pain. If you’re experiencing back pain, spinal decompression can help. This technique involves gently stretching out tight muscles in your back and reducing pain and other symptoms. According to Dr. Eric Kaplan, D.C., FIAMA, and Dr. Perry Bard, D.C., authors of “The Ultimate Spinal Decompression,” spinal decompression uses gentle traction to slowly pull the spine and alleviate painful spinal pressure that causes back pain. Adding spinal decompression to your daily routine can help reduce muscle weakness and pain and increase awareness of your body to prevent future injuries.
Conclusion
Missing work due to back pain is common among many working individuals. Certain job occupations require physical exertion, which can push the body beyond its limits. When individuals try to compensate for the pain in their back muscles, it puts more strain on other muscle groups. Fortunately, treatments such as spinal decompression can provide relief by realigning the body and reducing subluxation associated with back pain. This non-surgical treatment helps the body naturally heal, enabling individuals to experience a pain-free journey toward health and wellness.
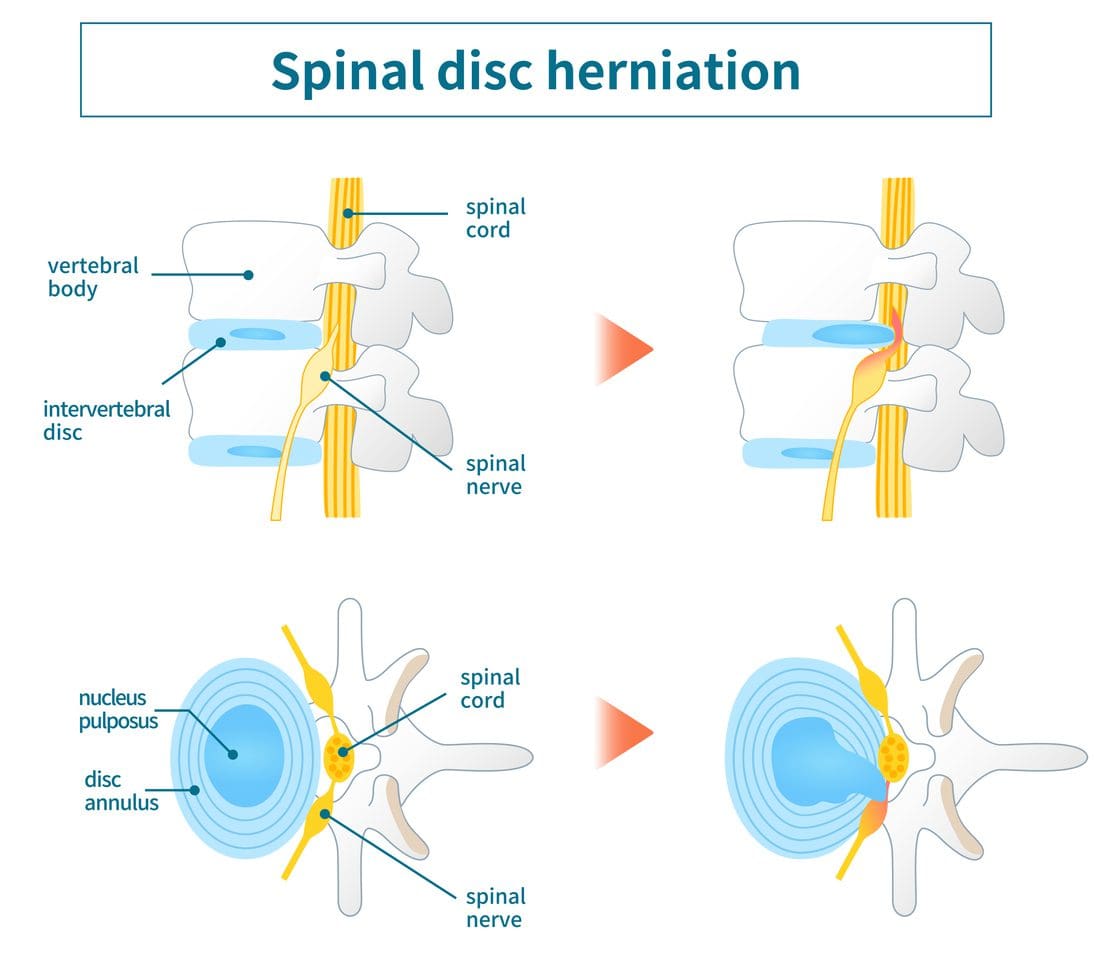
The spine consists of soft tissues, ligaments, the spinal cord, nerve roots, and cartilage, forming an S-shaped curve with three regions: cervical, thoracic, and lumbar. Its primary functions are to keep the body upright, provide mobility, and support the upper body’s weight. Injuries or other factors can cause mild to severe pain-like symptoms that affect the spine’s three regions, leading to misalignment and disc herniation, which can cause further complications. Fortunately, non-surgical treatments like spinal decompression can restore the spine’s functionality by realigning the body and restoring the spinal discs. This article will discuss how disc herniation affects the spine and body and how decompression therapy can treat it. We work with certified medical providers who use our patients’ valuable information to provide non-surgical treatments, including spinal decompression, to relieve pain-like symptoms associated with disc herniation and prevent chronic musculoskeletal issues. We encourage patients to ask essential questions and seek education about their condition. Dr. Jimenez, D.C., provides this information as an educational service. Disclaimer
How Does Disc Herniation Affect The Spine?
Do you experience stiffness or tingling in your neck, shoulders, or low back? Do you have radiating pain that is similar to other musculoskeletal conditions? Or do you feel aches and pains during stretching? These symptoms are often associated with spinal disc herniation, as research studies revealed, where the nucleus pulposus within the spine displaces and compresses the spinal nerve or cord. This can be caused by poor posture, incorrect lifting of heavy objects, or excessive twisting and turning, leading to wear and tear on the spinal disc. Left untreated, this can cause neurologic compromise or activity limitation to the rest of the body, as additional research shows. The three spinal regions can all be affected by this condition, causing a range of issues such as:
Numbness and tingling in the arms, hands, and fingers
Muscle weakness and stiffness in the neck and shoulders
Gait disturbances
Paralysis
Cardiovascular abnormalities
Back pain
Muscle weakness in hips, legs, buttocks, and feet
Sciatic nerve mimicry
An Overview Of Disc Herniation-Video
Have you been experiencing numbness, tingling sensations, or instability when walking? These issues could be caused by disc herniation, which occurs when the spinal cord and nerves are compressed or aggravated by the nucleus pulposus. This can cause pain in the cervical, thoracic, and lumbar areas and affect the functioning of your extremities. Research studies have revealed the severity of the herniation depends on the section affected, the size of the spinal canal, and pressure on the nerves. However, non-surgical, safe, and gentle treatments, such as chiropractic care and decompression therapy, can alleviate the effects of disc herniation. Watch the video above to learn more about the causes of disc herniation and the available treatments.
Decompression Therapy Treating Disc Herniation
If you are experiencing disc herniation, some treatments can help restore functionality to your spine. According to research studies, decompression therapy is one such treatment that works by using negative pressure within the spinal disc to increase hydration. This process pulls nutrients and oxygenated blood back into the disc, reducing pressure on the entrapped surrounding nerve root. Additionally, decompression therapy relieves the associated symptoms caused by disc herniation. In “The Ultimate Spinal Decompression,” written by Dr. Perry Bard, D.C., and Dr. Eric Kaplan, D.C., FIAMA, they explain that individuals with a herniated disc who use decompression therapy will feel negative or non-gravitational pressure within their spinal canal, which reduces the pressure from inside the disc. Decompression therapy helps restore the spine’s functionality and facilitates natural healing.
Other Treatments For Disc Herniation
Combining decompression therapy with chiropractic care can be effective in treating disc herniation. Chiropractic care involves spinal adjustments and manual manipulation to restore the natural alignment of the spine, which can relieve pressure on nerves caused by disc herniation. Gradual realignment of the vertebrae can help alleviate symptoms and reduce pain and discomfort while restoring the spine’s strength, flexibility, and mobility.
Conclusion
If the spinal cord is affected by environmental factors or injuries, it can cause pain and discomfort to the person. This is known as disc herniation, where the nucleus pulposus in the spine protrudes out of the spinal socket and presses on the spinal nerve. This can lead to neurological problems and affect the three spinal regions, causing mild to severe issues depending on the pressure on the spinal cord. However, non-surgical treatments like chiropractic care and decompression therapy can safely and gently manipulate the spine, realigning and hydrating the disc so the body can heal naturally. This can relieve pain and discomfort in the spine and restore mobility to the body.
The spine is essential for maintaining our upright posture and allowing us to move without pain. The cervical, thoracic, and lumbar sections support different body areas. However, environmental factors and pathogens can cause musculoskeletal pain, leading to spine misalignment and stress on the surrounding muscles and nerve roots. Non-surgical treatments like IDD therapy can help realign the spine and relieve pain. We utilize and incorporate valuable information about our patients to certified medical providers using non-surgical treatments like IDD therapy to alleviate pain associated with musculoskeletal pain along the spine. We encourage and refer patients to associated medical providers based on their findings while supporting that education is a remarkable and fantastic way to ask our providers the essential questions at the patient’s acknowledgment. Dr. Alex Jimenez, D.C., comprises this information as an educational service. Disclaimer
The Pathological Effects Of Musculoskeletal Pain On The Spine
Are you experiencing muscle pain in various parts of your body? Do you feel stiffness in your back, neck, hips, or shoulders? Or are you experiencing localized pain in a specific area? These are common symptoms of musculoskeletal pain, which affects the spine. Unfortunately, research studies reveal that musculoskeletal pain is a leading cause of long-term suffering, disability, and decreased productivity. This type of pain can strain the surrounding muscles in the upper and lower body, affect joints, and cause overlapping risk factors that make diagnosis challenging. Research studies also suggest that musculoskeletal pain can arise from different structures, leading to local or central sensitization and correlating pain intensity and duration.
Did you know that musculoskeletal pain can have pathological effects on the spine? Research studies revealed that the musculoskeletal system significantly impacts the central nervous system regarding pain. This means that when pain occurs in a certain area, neuron signals are sent to the brain, increasing sensitivity markers to that location. In the case of a traumatic spinal cord injury, these signals can become chaotic, leading to additional risk factors for the muscles surrounding the spine. This can result in musculoskeletal pain, which may cause referred pain in other body parts. Additionally, research has indicated that severe pathologies associated with the central nervous system can also lead to musculoskeletal pain. This is because the brain’s neuron signals alert the immune system that something is wrong and needs immediate attention.
The Science Of Motion-Video
Have you been experiencing stiffness or pain in different parts of your body? Do you feel discomfort lifting heavy objects or feel a pinched nerve in your lower back or legs? These daily issues could be caused by musculoskeletal pain affecting your spinal cord. Traumatic or non-specific issues can lead to overlapping risk profiles and the development of musculoskeletal pain associated with the spine. If the spinal column is affected, it can cause neuron signals to become hypersensitive, resulting in a misalignment of the body. Fortunately, non-surgical treatments can help realign and heal the body naturally, reducing the effects on affected muscles while allowing necessary nutrients and blood to flow back to the spine. The video above explains how non-surgical treatments like chiropractic care can harness the body’s ability to heal and restore stability through manual manipulation. Chiropractic care can also be combined with decompression therapy to stretch and alleviate pressure off the spine gently.
What Is IDD Therapy?
The musculoskeletal system depends on nerves, bones, and muscles for body structure and function. When affected by unwanted pathogens, it can cause pain in various areas and make a person feel miserable. Fortunately, non-surgical treatments like IDD therapy or intervertebral differential dynamic therapy can help reduce musculoskeletal pain affecting the spine. IDD therapy is decompression therapy that can help reduce pain by mobilizing and lengthening compressed spinal discs with special treatment forces. In “The Ultimate Spinal Decompression,” Dr. Eric Kaplan, D.C., FIAMA, and Dr. Perry Bard, D.C., states IDD therapy effectively alleviates spinal pain associated with the musculoskeletal system. The book also mentions that this therapy helps free the spinal discs and nerve roots as the compressed pressure is dropped. To that point, it allows the oxygen-riched blood and nutrients back to the spinal discs to begin the healing process, as research studies revealed.
Conclusion
When the spine experiences traumatic forces or injuries, it can result in musculoskeletal pain that can be constant and miserable for the individual. However, no one should have to endure such pain. The spine supports the upper and lower sections of the body and needs to be mobile to perform this task. Non-surgical treatments, such as IDD therapy, can help alleviate unwanted pressure off the spinal discs and nerve roots that have become hyper-sensitive due to trauma or injury. This decompression therapy can help restore mobility to the spine and rehydrate the spinal discs to begin the healing process. With IDD therapy, individuals can relieve pain and experience freedom of movement.
References
Arendt-Nielsen, L., Fernández-de-Las-Peñas, C., & Graven-Nielsen, T. (2011). Basic aspects of musculoskeletal pain: from acute to chronic pain. The Journal of manual & manipulative therapy, 19(4), 186–193. https://doi.org/10.1179/106698111X13129729551903
Bang, A. A., Bhojraj, S. Y., & Bang, A. T. (2021). Back pain and musculoskeletal pain as public health problems: Rural communities await solution. Journal of global health, 11, 01007. https://doi.org/10.7189/jogh.11.01007
George, S. Z., & Bishop, M. D. (2018). Chronic Musculoskeletal Pain is a Nervous System Disorder… Now What?. Physical therapy, 98(4), 209–213. https://doi.org/10.1093/ptj/pzy002
Kaplan, E. & Bard, P. (2023). The Ultimate Spinal Decompression. JETLAUNCH.
Puntillo, F., Giglio, M., Paladini, A., Perchiazzi, G., Viswanath, O., Urits, I., Sabbà, C., Varrassi, G., & Brienza, N. (2021). Pathophysiology of musculoskeletal pain: a narrative review. Therapeutic advances in musculoskeletal disease, 13, 1759720X21995067. https://doi.org/10.1177/1759720X21995067
Schimmel, J. J., de Kleuver, M., Horsting, P. P., Spruit, M., Jacobs, W. C., & van Limbeek, J. (2009). No effect of traction in patients with low back pain: a single centre, single blind, randomized controlled trial of Intervertebral Differential Dynamics Therapy. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society, 18(12), 1843–1850. https://doi.org/10.1007/s00586-009-1044-3
Dealing with pain in muscles can cause multiple risks, leading to disability and unhappy life. Environmental factors play a role in shaping a person’s health and wellness journey. Eating habits, sleeping patterns, and physical activity levels affect the muscles, tissues, joints, and vital organs, all essential for a healthy body. However, pathogens and environmental factors can cause chronic conditions, challenging the body’s functioning. Fortunately, various treatments can reduce musculoskeletal pain and help revitalize the body. This article will discuss traction therapy and spinal decompression and how they can help alleviate musculoskeletal pain. We utilize and incorporate valuable information about our patients to certified medical providers using non-surgical treatments like traction therapy and spinal decompression to relieve musculoskeletal pain. We encourage and refer patients to associated medical providers based on their findings while supporting that education is a remarkable and fantastic way to ask our providers the essential questions at the patient’s acknowledgment. Dr. Alex Jimenez, D.C., comprises this information as an educational service. Disclaimer
What Is Traction Therapy?
Are you experiencing referred pain in different parts of your body that seem connected? Are your muscles feeling tight or strained? Or have you noticed that you’re hunching over more than usual? If you’re dealing with musculoskeletal pain related to these issues, consider incorporating non-surgical treatments like spinal decompression and traction therapy to alleviate the pain. Research studies have revealed that traction therapy is a commonly used conservative treatment for reducing musculoskeletal pain along the spine. This therapy also reduces pain and relieves pressure on the spinal disc and nerves while restoring joint function. Physical therapists, massage therapists, and chiropractors frequently use traction therapy by applying gentle force to stretch and elongate soft tissues while restoring spine mobility. Traction therapy is known to be effective in treating musculoskeletal disorders such as herniated discs, sciatica, and referred musculoskeletal pain.
How Does It Help Musculoskeletal Pain?
When environmental factors cause pain issues in the body, they can cause damage to the spine, leading to muscles, spinal discs, and nerves compensating for the pain. This can result in referred pain in various body parts. Pain specialists use traction therapy to reduce the effects of musculoskeletal pain. Research indicates that technological changes and living standards can cause musculoskeletal pain and weaken muscle groups. Combined with non-invasive techniques, traction therapy can improve the body’s kinetic function by correcting spinal subluxation, rehydrating, and restoring the spinal disc. It can also help treat chronic musculoskeletal conditions related to spinal subluxation caused by musculoskeletal pain.
Revitalize and Rebuild with Chiropractic Care-Video
Do you suffer from muscle or joint pain, especially in your back? You may have noticed limited mobility or stiffness in your muscles. If so, you may be experiencing musculoskeletal pain associated with your spine. Fortunately, non-surgical treatments, such as spinal decompression and traction therapies, are available, which can help alleviate pressure on your spine and rehydrate your discs. These therapies stretch your muscles gently, reducing referred pain and restoring mobility to the affected joints. The video above demonstrates how these treatments can revitalize your body, reduce pain, and accelerate the healing process naturally. Additionally, physical therapy and chiropractic care can be combined with these treatments to promote optimal health and wellness.
What Is Spinal Decompression?
Have you ever experienced pain in different parts of your body due to issues with your spine? Spinal decompression therapy can help. It can alleviate musculoskeletal disorders associated with the spine and restore your body to normal. Spinal decompression reduces pressure on the spinal disc by gently stretching the spine and increasing hydration, which can decrease stress on the trapped nerve root. Studies have shown that it is a non-surgical option for individuals suffering from musculoskeletal pain.
How Do These Two Therapies Work Together?
“The Ultimate Spinal Decompression,” written by Dr. Eric Kaplan, D.C., FIAMA, and Dr. Perry Bard, D.C., explains that spinal decompression and traction therapy both address musculoskeletal pain related to the spine but in different ways. Traction therapy reduces pressure on the outer part of the spinal disc, while spinal decompression creates negative pressure inside the disc to hydrate it. Both treatments work together to restore blood flow and nutrients to the affected area and promote natural healing. These safe and non-invasive therapies have been reported to reduce pain after just a few sessions.
Conclusion
Regarding musculoskeletal pain, non-surgical treatments like traction therapy and spinal decompression allow the body to naturally heal itself by reducing pain through gentle stretching and remobilizing the joints. These non-invasive treatments help realign the body out of subluxation. Pain specialists can combine traction therapy and spinal decompression with associated therapies to help the individual be more mindful of their bodies while getting them back to their daily routine without worrying about constant pain.
References
Choi, Jioun, et al. “Influences of Spinal Decompression Therapy and General Traction Therapy on the Pain, Disability, and Straight Leg Raising of Patients with Intervertebral Disc Herniation.” Journal of Physical Therapy Science, Feb. 2015, www.ncbi.nlm.nih.gov/pmc/articles/PMC4339166/.
Kaplan, Eric, and Perry Bard. The Ultimate Spinal Decompression. JETLAUNCH, 2023.
Oh, Hyunju, et al. “The Impact of Manual Spinal Traction Therapy on the Pain and Oswestry Disability Index of Patients with Chronic Back Pain.” Journal of Physical Therapy Science, Dec. 2018, ncbi.nlm.nih.gov/pmc/articles/PMC6279706/.
Öten, Erol, et al. “Traction Therapy in Lumbar Disc Hernias: A Finite Element Analysis Study.” Joint Diseases and Related Surgery, 2022, www.ncbi.nlm.nih.gov/pmc/articles/PMC9057540/.
Back pain is a common issue experienced by people all over the world. The human body’s main structure is the back, divided into three sections: cervical, thoracic, and lumbar. These sections help in body movement, including twisting and turning, moving the extremities, and have a relationship with the gut and central nervous system. The surrounding muscles in the back also provide support and protect the spine. However, normal activities like bending down to pick up a heavy object, sitting down for an extended period, or falling can cause changes that lead to back pain, misalignment, and risk profiles in the upper and lower extremities. Today’s article focuses on the causes of back pain and the treatments available to relieve its effects. We utilize and incorporate valuable information about our patients to certified medical providers using non-surgical treatments to reduce the impact of back pain. We encourage and refer patients to associated medical providers based on their findings while supporting that education is a remarkable and fantastic way to ask our providers the essential questions at the patient’s acknowledgment. Dr. Alex Jimenez, D.C., comprises this information as an educational service. Disclaimer
An Overview Of Back Pain
Do you have pain in your upper, middle, or lower back? Do you experience aches and pains in the morning? Did lifting something heavy cause you pain? These symptoms could be signs of back pain, a common and costly reason for emergency room visits. Research studies reveal that back pain can have various causes and affect the entire body, either mechanically or non-specifically. The three sections of the back – cervical, thoracic, and lumbar – can all be impacted, causing referred pain in different parts of the body. For instance, cervical (upper) back pain can cause stiffness in the neck, while thoracic (middle) back pain can lead to shoulder and posture issues. Lumbar (low) back pain, the most common type, can cause hip and sciatic problems. Additional research studies reveal that back pain is a complex issue that can severely affect body function, and environmental factors can also influence it.
Causes Of Back Pain
Various factors can be the cause of back pain, thus resulting in spine misalignment. In their book, “The Ultimate Spinal Decompression,” Dr. Eric Kaplan, D.C., FIAMA, and Dr. Perry Bard, D.C., explain that the back muscles play a significant role in protecting the spine. Environmental factors can also impact the spine, leading to potential back pain. The book further notes that wear and tear and disc protrusion on the spine can result in disc herniation and degeneration, also associated with back pain. Some common causes of back pain include:
Visceral-somatic/Somato-visceral pain (Affected organ or muscle causes referred pain to different body parts)
Pregnancy
Further research indicates that various environmental factors, such as physical activity, lifestyle, stress, and work conditions, are associated with back pain and can overlap as risk factors. If left untreated, these environmental factors can lead to chronic conditions and significantly impact a person’s quality of life.
Chiropractic Secrets Exposed- Video
Have you been feeling numbness or tingling in your arms or legs? Do you experience back muscle pain when you stretch? Or do you feel pain in your low back or other parts of your body? These issues are often associated with back pain and, if left untreated, can lead to disability and loss of function. Fortunately, there are many ways to reduce back pain and its associated symptoms and promote natural healing. The video above explains how non-surgical treatments like chiropractic care can help alleviate back pain through manual manipulation. This treatment can realign the spine, stretch out tight muscles, and restore the body’s range of motion.
Treatments For Back Pain
If you are experiencing back pain, various treatments can help ease your symptoms and improve your mobility. You have two options for treating back pain: surgical and non-surgical. Surgical treatment may be necessary if you are experiencing nerve compression or have sustained an injury that requires spinal fusion. Non-surgical treatments can help relieve pressure on your spine, reduce back pain, and even alleviate pain in other areas of your body. Some non-surgical treatments for back pain include:
Physical therapy
Exercise
Chiropractic care
Acupuncture
Spinal Decompression
According to research, non-surgical treatments can alleviate pressure on spinal discs, loosen tight muscles, improve joint mobility, and promote natural healing. Many people supplement these treatments with healthy lifestyle choices, making small adjustments to their routine and paying closer attention to their physical well-being.
Conclusion
Since back pain is a widespread problem affecting people globally, it can be caused by various environmental factors that impact the cervical, thoracic, and lumbar back sections, leading to overlapping risk profiles and affecting different body parts. Tight and strained muscles and a compressed spine are common symptoms of this issue. However, treatments available can effectively reduce pain, stretch tight muscles, and relieve pressure off the spinal disc. By incorporating these treatments, individuals can alleviate back pain and allow their bodies to heal naturally.
References
Allegri, Massimo, et al. “Mechanisms of Low Back Pain: A Guide for Diagnosis and Therapy.” F1000Research, 28 June 2016, www.ncbi.nlm.nih.gov/pmc/articles/PMC4926733/.
Casiano, Vincent E, et al. “Back Pain.” In: StatPearls [Internet]. Treasure Island (FL), 20 Feb. 2023, www.ncbi.nlm.nih.gov/books/NBK538173/.
Choi, Jioun, et al. “Influences of Spinal Decompression Therapy and General Traction Therapy on the Pain, Disability, and Straight Leg Raising of Patients with Intervertebral Disc Herniation.” Journal of Physical Therapy Science, Feb. 2015, www.ncbi.nlm.nih.gov/pmc/articles/PMC4339166/.
Kaplan, Eric, and Perry Bard. The Ultimate Spinal Decompression. JETLAUNCH, 2023.
See, Qin Yong, et al. “Acute Low Back Pain: Diagnosis and Management.” Singapore Medical Journal, June 2021, www.ncbi.nlm.nih.gov/pmc/articles/PMC8801838/.
Back problems can affect everyone. The most healthy individuals can experience back issues from time to time because of unhealthy postures, standing or sitting for extended periods at a job or school, athletes, and individuals with previous injuries. Back soreness and pain symptoms are common in today’s active and inactive world. The pain can range from dull and constant aches to sharp and sudden piercing sensations. This causes pressure to build up against different regions of the spine. Individuals trying to reposition the body can cause an imbalance in the spine that often leads to more pain and problems. It is impossible to adjust one’s spine effectively and should be evaluated and treated by a professional chiropractor and therapy team.
Professional Chiropractor
Problems With DIY adjustments
Self-cracking or having a friend/family/spouse walk on their back or squeeze the body to achieve the crack or pop forces an increase in mobility that can lead to overexerting the spine.
Can loosen all of the joints instead of just the tight joints.
This can overly loosen already flexible joints that must compensate for the stiff joints.
The muscles have to work overtime to maintain stability, adding stress which increases muscle tension.
This can cause the health of compressed segments to continue to decline and worsen and/or cause further injury.
It can cause abnormal vertebral degeneration.
It can be dangerous if the individual has weak bones.
Injuries can include herniated and dislocated discs.
In the worst-case scenario, fractures and broken vertebrae.
Although rare, there is the possible risk of rib fracture or subluxation.
This can cause pain and symptoms to turn into a serious health or chronic condition.
Chiropractic Training
Chiropractors are trained medical specialists on the body’s structure and function. Chiropractors know the correct positioning and function of every area of the spine, from the neck to the tailbone. The most common injuries that chiropractic treats include:
Muscle Strains
Sciatica
Overuse/Repetitive Strains
Neck Sprains
Whiplash
Headaches
Herniated Discs
Dislocations
Fractures
Proper Realignment
Individuals think the popping sound is the goal; however, it’s not what relieves the pain or symptoms. The relief comes from the improved movement of the joints. The term for the popping sound is cavitation. Chiropractic manipulation is a specific force applied in a specific direction to a particular joint. During a professional realignment session, the pressure inside the joint decreases, releasing gasses within the synovial fluid into the joint space. That’s the popping sound. When a professional chiropractor performs adjustments/cavitations, they:
ImproveJoint function.
Relax the muscles.
Relieve nerve irritation.
There’s also the possibility of an unknown underlying cause for the pain symptoms. Therefore, friends and family should not attempt back adjustments unless they are professional chiropractors. When symptoms persist, treatment from a professional licensed chiropractic clinic is safer and more effective, and early treatment can prevent permanent damage caused by chronic inflammation. Professional chiropractor treatments include:
Adjustments
To gently realign joints to decrease pain and increase range of motion.
Soft-Tissue Therapy
Relaxes tight muscles, relieves spasms, and releases tension in the tissues that surround the muscle fascia.
Exercises and Stretches
Restore and maintain joint stability and mobility.
Joint Bracing and Kinesio Taping
Supports sprained joints or muscles during recovery.
Referrals to Medical Experts
For guidance on diet and nutrition to reduce inflammation and promote healthy weight.
The Path To Healing
References
Dunning, James, et al. “CAVITATION SOUNDS DURING CERVICOTHORACIC SPINAL MANIPULATION.” International Journal of sports physical therapy vol. 12,4 (2017): 642-654.
Evans, David W, and Nicholas Lucas. “What is manipulation? A new definition.” BMC musculoskeletal disorders vol. 24,1 194. 15 March 2023, doi:10.1186/s12891-023-06298-w
Hardy, Katie, and Henry Pollard. “The organization of the stress response, and its relevance to chiropractors: a commentary.” Chiropractic & osteopathy vol. 14 25. 18 October 2006, doi:10.1186/1746-1340-14-25
LaPelusa, Andrew. and Bruno Bordoni. “High-Velocity Low Amplitude Manipulation Techniques.” StatPearls, StatPearls Publishing, 6 February 2023.
Navid, Muhammad Samran, et al. “The effects of chiropractic spinal manipulation on central processing of tonic pain – a pilot study using standardized low-resolution brain electromagnetic tomography (sLORETA).” Scientific Reports vol. 9,1 6925. 6 May. 2019, doi:10.1038/s41598-019-42984-3
The immune system is crucial in protecting the body from foreign pathogens that cause inflammation in the affected area. Cytokines produce inflammation in the body to fight off infections or bacteria. However, inflammation can be beneficial or harmful, depending on the severity of the affected area. Acute inflammation is a natural healing process that causes redness, swelling, and heat in the affected area, and it usually resolves within a few days. In contrast, chronic inflammation causes pain and damages healthy tissues, mistaking them for foreign invaders. Environmental factors can trigger chronic inflammation, leading to muscle and joint pain and other chronic conditions. Fortunately, an anti-inflammatory diet combined with soft tissue therapy can help reduce the effects of chronic inflammation. Our article today discusses how these diets work and how they can be combined with MET therapy to restore the body. We utilize and incorporate valuable information about our patients to certified medical providers using MET therapy to relieve chronic inflammation associated with the musculoskeletal system through dieting. We encourage and refer patients to associated medical providers based on their findings while supporting that education is a remarkable and fantastic way to ask our providers the essential questions at the patient’s acknowledgment. Dr. Alex Jimenez, D.C., comprises this information as an educational service. Disclaimer
What Are Anti-Inflammatory Diets?
Are you experiencing inflammation in your muscles, joints, or vital organs? Do you feel musculoskeletal pain or have uncertain symptoms after eating certain foods? Chronic stress, obesity, autoimmune disorders, and abdominal pain can cause chronic inflammation. These conditions may be caused by environmental factors leading to chronic inflammation. Research shows that certain dietary components can contribute to inflammation, which can be beneficial and harmful. While additional research studies reveal that incorporating lean meats, omega-3s, antioxidants, fruits, and vegetables can help minimize inflammasome activation and its negative effects on the muscles, joints, and vital organs to reduce chronic inflammation.
How Anti-Inflammatory Diets Help The Body?
Did you know that adopting an anti-inflammatory diet can help reduce the effects of chronic inflammation in the body? Research studies reveal that lowering the intake of pro-inflammatory foods and increasing the consumption of unsaturated fats, fruits, and vegetables can effectively combat inflammation. While inflammation is a natural defense mechanism, excessive production of inflammatory cytokines can lead to chronic conditions. However, combining an anti-inflammatory diet with exercise or physical therapy can help reduce these cytokines and identify the underlying causes of inflammation. By consuming specific foods and vitamins, an individual can effectively reduce the progression of inflammation and prevent further damage to the body.
Understanding Inflammation- Video
Are you experiencing muscle or joint pain, tenderness, or redness in certain body areas? Do you notice that certain foods cause issues with your organs? These symptoms may be caused by inflammation affecting your body. Inflammation is a natural immune system response that releases cytokines to affected areas. When cytokines are released onto healthy tissue can lead to aggravating issues such as autoimmune disorders and chronic pain. However, there is hope. You can understand the root cause of inflammation and reduce its effects on your body. The video above provides an excellent overview of how environmental factors can cause inflammatory impacts on the body and how whole-nutritional foods and vitamins with antioxidants can help reduce pain associated with inflammation.
Anti-Inflammatory Diets & MET Therapy
According to “Clinical Application of Neuromuscular Techniques” by Judith Walker DeLany, L.M.T. and Leon Chaitow, N.D., D.O., inflammation can be a normal part of healing. Still, if left untreated, it can cause soft tissue injuries. Muscle energy techniques (MET) can help reduce inflammation by stretching soft tissues, improving joint mobility, and draining the lymphatic system. Combining MET with an anti-inflammatory diet can help reduce inflammation and heal the body naturally. Here are some diets to consider merging with MET.
The Exclusion Diet
The exclusion diet is a way to identify which foods are causing negative symptoms in the body. By listing foods that cause allergic or inflammatory reactions, the doctor can create a personalized dietary plan for the patient, excluding these problem foods. After at least 3-4 weeks of avoiding these foods, reintroduce them to see if symptoms return. If they do, remove the food from the diet. This anti-inflammatory diet can help reduce muscle and joint pain associated with inflammation and is effective for many people with food sensitivities/allergies.
The Oligoantigenic Diet
The oligoantigenic diet is an anti-inflammatory diet involving whole foods rich in vitamins and minerals to reduce inflammation in individuals with severe food allergies. This diet allows the person to identify which foods are causing inflammation by removing them from their diet for a few weeks and then reintroducing them one at a time. If the symptoms return, the food can be eliminated from the diet.
Conclusion
Inflammation is a double-edged sword as it can have beneficial and harmful effects on the body depending on environmental factors and can result in musculoskeletal pain. Nevertheless, one can aid the body’s natural recovery process by consuming whole foods rich in anti-inflammatory properties and undergoing therapies that can alleviate the effects of inflammation in the musculoskeletal system. By adopting these approaches, individuals can eliminate foods and other environmental factors that may trigger chronic inflammation, enhancing their quality of life.
References
Chaitow, Leon, and Judith Walker DeLany. Clinical Applications of Neuromuscular Techniques. Churchill Livingstone, 2003.
Dragan, Simona, et al. “Dietary Patterns and Interventions to Alleviate Chronic Pain.” Nutrients, 19 Aug. 2020, www.ncbi.nlm.nih.gov/pmc/articles/PMC7551034/.
Kiecolt-Glaser, Janice K. “Stress, Food, and Inflammation: Psychoneuroimmunology and Nutrition at The Cutting Edge.” Psychosomatic Medicine, May 2010, www.ncbi.nlm.nih.gov/pmc/articles/PMC2868080/.
Sears, Barry, and Asish K Saha. “Dietary Control of Inflammation and Resolution.” Frontiers in Nutrition, 10 Aug. 2021, www.ncbi.nlm.nih.gov/pmc/articles/PMC8382877/.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine