Unlocking Cellular Healing: The Power of Advanced Laser Therapy in Integrative Care
Abstract
As a clinician with a diverse background spanning chiropractic, advanced practice nursing, and functional medicine, my primary goal is to offer patients the most effective, evidence-based treatments available. In this educational post, I will take you on a journey into the world of Multiwave Locked System (MLS) Laser Therapy, a cutting-edge technology that is transforming how we manage pain and inflammation. We will explore the science behind this therapy, moving beyond surface-level explanations to understand its profound effects on cellular biology, including its impact on mitochondria and the inflammatory cascade. I will share insights from leading researchers and demonstrate how we apply this technology in clinical settings, particularly for conditions such as low back pain and joint issues. Furthermore, I will explain how MLS Laser Therapy integrates seamlessly into a comprehensive care model like ours at Injury Medical Clinic, where we combine chiropractic adjustments, physical rehabilitation, and advanced medical oversight from our Medical Director, Dr. Maria Guadalupe Cardenas, MD, to optimize patient outcomes. This post will detail specific treatment protocols, the importance of energy density, and how this therapy can augment other regenerative treatments, such as Platelet-Rich Plasma (PRP), offering a multifaceted approach to true healing.
A New Frontier in Healing at Injury Medical Clinic
Hello, I’m Dr. Alex Jimenez. With my credentials as a Doctor of Chiropractic (DC) and Advanced Practice Registered Nurse (APRN), and my certifications in functional and integrative medicine (CFMP, IFMCP), my passion has always been to bridge gaps between healing disciplines. At Injury Medical Clinic PA, we have built a practice on this very principle: a truly integrative approach to patient wellness.
A cornerstone of our collaborative model is my partnership with Dr. Maria Guadalupe Cardenas, MD. Dr. Cardenas is Board Certified in Internal Medicine and serves as our esteemed Medical Director and Collaborative Physician. With over 40 years of invaluable experience, she provides essential medical oversight, ensuring our patients receive safe, comprehensive, and well-rounded care. This multidisciplinary structure allows us to blend the best of chiropractic and physical rehabilitation with the diagnostic and medical expertise of internal medicine. Our team works in synergy, designing treatment plans that address not just the symptoms but the underlying physiological dysfunction. Whether a patient is recovering from a personal injury, managing a chronic condition, or seeking to optimize their overall health, our integrated team provides a holistic, evidence-based pathway to recovery.
Navigating Low Back Pain with MLS Laser Therapy
One of the most common ailments we see is chronic low back pain. Today, we have a patient, John, who is experiencing persistent joint pain and stiffness in his lumbar spine, specifically around the L4-L5 facet joints, with some discomfort radiating down his right side. This is a classic presentation that responds exceptionally well to a targeted, multimodal approach.
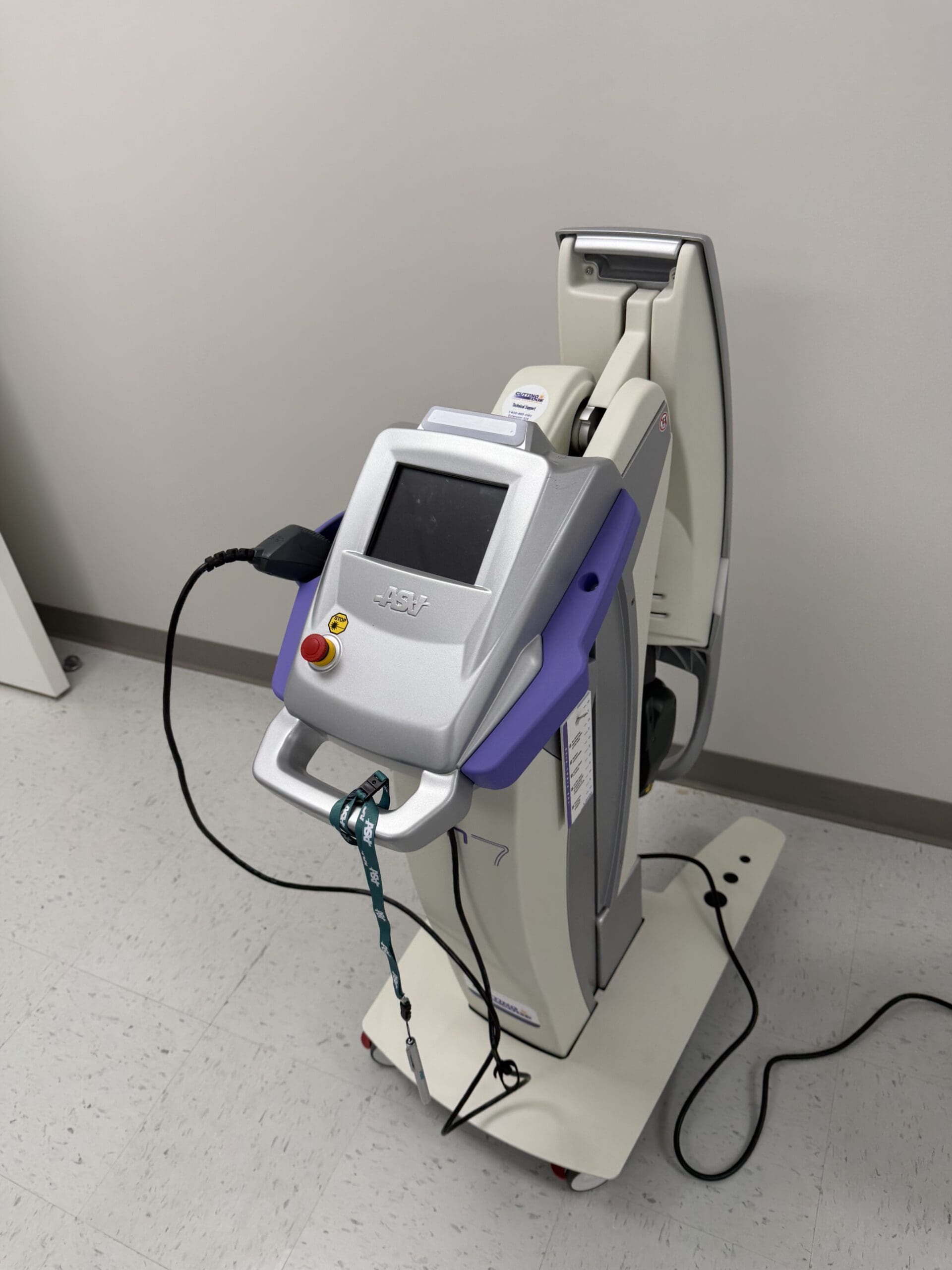
For John, we are utilizing the M6 Robotic MLS Laser. The first priority is always patient comfort. When using a robotic system, it’s critical that the patient remains still, as the laser is programmed to treat a precise area. We position the patient face down to allow direct access to the skin over the lumbar spine, as the laser energy must be delivered without the barrier of clothing.
The Clinical Multimodal Approach: More Than Just the “Spot of Pain”
Once John is comfortable, we begin the setup. The robotic laser interface is remarkably sophisticated yet user-friendly.
Targeting the Ailment: I select the “Joint Pain and Stiffness” protocol for the back.
Centering the Treatment: I zero out the X and Y axes on the control panel. This temporarily stops the robotic arm’s movement, allowing me to manually position the guiding red light directly over the primary source of John’s discomfort—the L4-L5 region he indicated.
Expanding the Field: This is where our clinical multimodal approach comes into play. Instead of just treating the single spot of pain, I expand the treatment area using the X and Y controls. This creates a larger therapeutic field that covers not only the symptomatic facet joints but also the surrounding connective tissue, muscles, and nerve roots. We aren’t just chasing pain; we are treating the entire functional unit to address the source of the dysfunction and support the interconnected biological systems.
The laser head is positioned at a precise distance from the skin—about six inches—using a provided ruler. This is crucial because the MLS laser beam is collimated, meaning the light rays are parallel. The focal point is engineered to be most effective at this distance, ensuring the therapeutic energy penetrates deep into the tissues rather than dissipating at the surface.
The Science of Healing: How MLS Laser Therapy Works
With the treatment underway—an eight-minute session for John’s low back—let’s dive into what’s happening at a cellular level. It’s common for patients to ask if they will feel anything. Most feel nothing at all, though some may notice a gentle warmth or tingling. This lack of intense heat is a hallmark of the MLS system’s advanced design.
The device combines two specific wavelengths of light: an 808-nanometer (nm) continuous-wave and a 905-nanometer (nm) pulsed-wave.
The 808 nm wavelength works more superficially to reduce inflammation and edema. It enhances blood circulation to the area, which helps clear out inflammatory byproducts and deliver oxygen and nutrients.
The 905 nm wavelength, delivered in powerful, short pulses, penetrates much deeper, reaching tissues such as muscle, nerve, and even the joint capsule. This pulsed energy is what provides the powerful analgesic (pain-relieving) effect.
These two wavelengths are synchronized, creating the patented “MLS pulse.” This enables delivery of very high peak power (up to 50 watts) in extremely short bursts (nanoseconds). This high-intensity “punch” of energy stimulates the cells without generating heat. A period of rest follows each pulse, allowing the tissue to absorb the energy efficiently. If a laser produces significant heat at the skin’s surface, it often means the energy isn’t being absorbed properly by the target tissues. The MLS system maintains tissue temperature at a constant level, ensuring optimal therapeutic delivery.
Seeing the Invisible: A Window into the Treatment
A fascinating demonstration of this technology involves using a smartphone camera. While the red aiming light is visible to the naked eye, the therapeutic infrared laser light is not. However, a camera’s sensor can detect it. If you were to look at John’s back through a phone camera during treatment, you would see a distinct triangle of light—this is the 808 nm wavelength at work, covering a significant area and illustrating how comprehensively we are treating the region.
Energy Density: The Key to Effective Dosing
A critical concept in laser therapy is energy density, measured in joules per centimeter squared (J/cm²). This is more important than the total number of joules delivered. Think of it like watering a plant: you need to provide the right amount of water for the pot’s size. Too little has no effect; too much drowns it. Similarly, our goal is to deliver a precise dose of light energy to the target tissue.
The World Association for Laser Therapy (WALT) and a large body of research support an optimal therapeutic window of 4-10 J/cm².
For John’s condition, the protocol is set to deliver approximately 6 J/cm². The laser’s software automatically calculates the treatment time required to achieve this density over the selected area. If I were to make the treatment area smaller or larger, the software would instantly recalibrate the time to ensure the correct dose is delivered.
This concept also relates to the Arndt-Schultz Law, a pharmacological principle stating that low doses stimulate, moderate doses inhibit, and high doses are toxic. With laser therapy, if you “overcook” an area with too much energy, you risk a bioinhibitory effect, in which the treatment becomes less effective or even counterproductive. The body’s cells can only absorb so much energy at once. This is why our protocols focus on precise energy density and, if more treatment is needed, we target different areas (e.g., an anterior and posterior approach for a knee) rather than just increasing the time on one spot.
Integrating Modalities for Superior Results
While the robotic laser treats the broader lumbar region, I can simultaneously use a handheld MLS laser applicator. This handpiece allows for more focused treatment on specific points, such as trigger points or “knots” in the muscle. I often use the “cooked meat” versus “raw meat” analogy that a physical therapist once taught me. Healthy, relaxed muscle feels like raw meat, while a tight, knotted trigger point feels firm, like cooked meat. The handheld applicator is perfect for treating these punctual spots.
The robot and the handpiece operate on two separate channels, allowing us to perform this dual treatment. This is a perfect example of our integrative philosophy in action:
Chiropractic Care: Before or after the laser session, I can perform specific chiropractic adjustments to restore proper motion to the L4-L5 facet joints and relieve mechanical stress.
Physical Rehabilitation: Our team can guide John through exercises to strengthen his core musculature and improve spinal stability.
MLS Laser Therapy: The laser works at the cellular level to reduce pain and inflammation that may be hindering his ability to engage in rehabilitation, thereby accelerating healing.
This combination addresses the structural, functional, and biochemical aspects of his condition simultaneously.
Advanced Applications: Augmenting Regenerative Medicine
The conversation around healing is increasingly turning toward orthobiologics, such as Platelet-Rich Plasma (PRP) injections. This is where MLS Laser Therapy shows even more remarkable potential. A common question arises: if PRP induces a beneficial pro-inflammatory phase to kickstart healing, won’t an anti-inflammatory laser treatment counteract it?
The answer is no. In fact, the laser augments the process. The data and our clinical observations show that using laser therapy in conjunction with PRP can improve outcomes by an estimated 15-20%.
Here is the progressive protocol we often recommend:
Pre-Injection Priming (2-3 treatments): In the weeks leading up to the PRP injection, we use the laser to “prepare the soil.” These sessions are designed to increase local blood circulation, reduce baseline chronic inflammation, and optimize the cellular environment, making the tissue more receptive to the growth factors in the PRP.
Day of Injection (1 treatment): A treatment on the day of the procedure can further enhance the effects.
Post-Injection Support (6+ treatments): Following the injection, a series of laser treatments helps manage pain and supports the regenerative cascade initiated by the PRP. The laser enhances mitochondrial function, which is critical for providing the cellular energy (ATP) needed for tissue repair.
The Cascade of Healing: From Acute Relief to Chronic Repair
How does a single modality address both acute pain and chronic conditions? The effects occur in a cascade.
Immediate Effect (Acute Phase): The initial pain relief often comes from the laser’s effect on small, unmyelinated nerve fibers (C-fibers) that transmit pain signals. The energy can temporarily block these signals, providing rapid relief. This is the analgesic effect.
Subsequent Effect (Inflammatory Modulation): Over the next few hours and days, the anti-inflammatory effect takes hold. The laser energy modulates the immune response, reducing pro-inflammatory cytokines and promoting the resolution of inflammation and edema.
Long-Term Effect (Biostimulation and Chronic Repair): With a series of treatments, we get to the core of cellular repair. Light energy is absorbed by cytochrome c oxidase in the mitochondria, the powerhouses of our cells. This significantly increases ATP (adenosine triphosphate) production, the body’s primary energy currency. This surge in available energy fuels all cellular repair processes, from protein synthesis to cell replication, promoting true, long-term tissue healing.
This mitochondrial boost is especially relevant in today’s world, where many common medications, such as statins, can impair mitochondrial function. By enhancing mitochondrial biogenesis and efficiency, laser therapy can help overcome these hurdles and optimize the body’s innate healing capacity. This is why we also discuss nutritional and lifestyle factors—such as CoQ10 supplementation to support mitochondrial function—as part of a truly comprehensive functional medicine approach.
Treatment Frequency and The Cumulative Effect
Healing is a process, not an event. The effects of MLS Laser Therapy are cumulative. We recommend a series of treatments to achieve lasting results.
Acute Conditions: Typically, a course of 6 treatments is effective.
Chronic Conditions: A more intensive course of 12 treatments is often needed.
Ideally, treatments are scheduled close together (e.g., Monday, Wednesday, Friday) to build therapeutic momentum. It is crucial for patients to complete the full course. Many start feeling significantly better after just 3-4 sessions and are tempted to stop. However, completing the entire protocol ensures deeper cellular repair, leading to more durable outcomes.
At Injury Medical Clinic, our mission is to empower your body’s own ability to heal. By integrating the best of chiropractic, medical oversight, and groundbreaking technologies like MLS Laser Therapy, we offer a path to recovery that is not only faster but also more complete.
World Association for Laser Therapy. (n.d.). WALT Recommended Treatment Doses for LLLT. WALT. Retrieved from https://waltza.co.za/wp-content/uploads/2012/08/Dose_table_780-860nm_for_Low_Level_Laser_Therapy_WALT-2010.pdf
Welcome to our exploration of photobiomodulation therapy (PBMT), a revolutionary approach that harnesses the power of light to stimulate cellular healing. In this educational post, I will guide you through the intricate biological processes that make PBMT so effective. We will explore how specific wavelengths of light can penetrate tissues to activate mitochondria, modulate the immune response, and accelerate recovery. This journey will cover the fundamental science behind PBMT, from its effects on ATP production and cytokine modulation to its role in promoting angiogenesis and neurogenesis. Furthermore, we will examine the synergistic potential of combining PBMT with orthobiologics, such as Platelet-Rich Plasma (PRP), and demonstrate how this integrated approach can enhance healing outcomes. Drawing on the latest research, including fascinating studies from the veterinary world and our laboratory findings on tenocyte proliferation, we’ll demonstrate why light is not just a modality but a cornerstone of modern regenerative medicine. At Injury Medical Clinic, we integrate these advanced therapies within a collaborative framework, combining my expertise in chiropractic and functional medicine with the medical oversight of our Medical Director, Dr. Maria Guadalupe Cardenas, MD, to provide comprehensive, evidence-based care for our patients.
About Our Integrated Practice: A Collaborative Approach to Wellness
I, Dr. Alex Jimenez, am honored to share my passion for integrative and regenerative medicine with you. With a diverse background as a Doctor of Chiropractic (DC), Advanced Practice Registered Nurse (APRN), board-certified Family Nurse Practitioner (FNP-BC), and certifications in Functional Medicine (CFMP, IFMCP), Applied Traumatology (ATN), and Cranial Spinal Integration (CCST), my goal has always been to find the most effective, evidence-based paths to healing.
Here at Injury Medical Clinic PA in El Paso, Texas, we have built a unique, multidisciplinary practice. We believe that the best patient outcomes are achieved through a collaborative team approach. I am privileged to work alongside Dr. Maria Guadalupe Cardenas, MD, who serves as our Medical Director and Collaborative Physician. Dr. Cardenas is a highly respected, board-certified Internist with over 40 years of experience (NPI #1164426749, Texas MD License #J2933). Her extensive medical knowledge provides invaluable oversight and complements our services, ensuring our patients receive safe, comprehensive, and well-rounded care.
Our clinic integrates:
Advanced Chiropractic Care: Focused on spinal health, biomechanics, and nervous system function.
Physical Therapy & Rehabilitation: Tailored programs to restore movement, strength, and function.
Medical Oversight: Guided by Dr. Cardenas to ensure clinical safety and efficacy.
Functional Medicine: Investigating the root causes of chronic conditions.
Personal Injury Care: Specialized treatment for injuries sustained in accidents.
This model allows us to address health from multiple angles. While our core focus at elpasobackclinic.com is chiropractic and physical rehabilitation, we incorporate advanced modalities such as photobiomodulation to enhance the body’s innate healing capabilities, with all treatments guided by a solid medical and scientific foundation.
The Awakening: From Skepticism to Cellular Biology
I have been on this journey for nearly a decade, and for the first five years, discussing “laser” therapy in medical circles often felt like an uphill battle. It was a path paved with skepticism, much like the initial reception many of you in the biologics field have likely experienced. But today, I am thrilled to see the conversation shifting as the science catches up with the clinical results.
My evolution as a clinician mirrors this shift. For the first two decades of my career, I was a “mechanic,” using established tools to address specific conditions. Over the last ten years, however, I have become a “biologist,” focused on understanding and facilitating the body’s own healing processes at a cellular level. This is why I am so excited to share the science of photobiomodulation (PBMT) with you. It represents a profound shift from treating symptoms to enabling cellular recovery.
Understanding Photobiomodulation: The Science of Light and Life
The concept is beautifully simple, rooted in a phenomenon we all accept: photosynthesis. The sun’s light fuels life on Earth, and as a species that has evolved under this light for hundreds of thousands of years, our cells have developed a deep, genetic sensitivity to it. We readily accept that sunlight is necessary for Vitamin D synthesis, yet a significant gap remains in medical education regarding the broader therapeutic applications of light.
Photobiomodulation breaks down as:
Photo: Light
Bio: Life
Modulation: To affect or change
Light is energy, delivered in units called photons. These photons can transfer their energy to our cells, triggering a cascade of biological responses. This is the essence of PBMT.
The Cellular Engine: How PBMT Activates Mitochondria
The primary target of photobiomodulation within the cell is the mitochondria, our cellular powerhouses. Specifically, an enzyme in the mitochondrial respiratory chain, cytochrome c oxidase, acts as a photoacceptor. This means it is designed to absorb photons of light.
Here is the cascade of events that follows:
Activation: When light photons of the correct wavelength strike cytochrome C oxidase, the enzyme becomes more active.
Increased ATP Production: This heightened activity accelerates the Krebs cycle, leading to more efficient production of adenosine triphosphate (ATP), the primary energy currency of the cell. More ATP means more energy available for cellular repair, replication, and function.
Signaling Cascade: This process also triggers the release of key signaling molecules, including nitric oxide and reactive oxygen species (ROS) in controlled, beneficial amounts.
Gene Transcription: These signaling molecules then travel to the cell’s nucleus, initiating gene transcription. This is where the cell is instructed to produce specific proteins, including cytokines, which orchestrate the healing process.
Modulating the Immune Response: From Inflammation to Repair
When an injury occurs, the body initiates an inflammatory response characterized by the production of pro-inflammatory cytokines. PBMT helps guide the body out of this chronic or stalled inflammatory phase and into a reparative one by modulating the cytokine profile.
Anti-Inflammatory Effects: Research has clearly shown that PBMT, when used at the right wavelengths, can increase the production of interleukin-10 (IL-10), a potent anti-inflammatory cytokine.
Pro-Inflammatory Reduction: It has also been shown to reduce levels of pro-inflammatory cytokines, such as interleukin-6 (IL-6).
This shift moves the cellular environment from a state of chronic inflammation—such as that seen in a thickened, bulbous Achilles tendon—toward active healing and regeneration.
Building the Foundation for Healing: Angiogenesis, Neurogenesis, and Muscle Recovery
The benefits of PBMT extend beyond simple control of inflammation. The cellular signaling it initiates promotes the foundational elements of tissue repair.
Enhanced Blood Flow (Angiogenesis): PBMT has been shown to promote angiogenesis by stimulating the production of cytokines such as galectin-1. This improved microcirculation is crucial for delivering oxygen and nutrients to injured tissue and removing waste products. For anyone focused on healing, whether through chiropractic adjustments or post-surgical recovery, enhanced blood flow is paramount.
Nerve Repair (Neurogenesis): We can also document the repair of nerve cells. PBMT stimulates the production of proteins that encourage axonal growth, helping to repair damaged neurons. This is particularly relevant in our practice for treating neuropathies and nerve entrapment syndromes like carpal tunnel.
Muscle and Tissue Recovery: Electron microscopy studies have provided clear evidence that PBMT improves muscle cell development and increases myoglobin production, which enhances oxygenation. It also activates fibroblasts, the cells responsible for producing collagen and building the structural framework for new tissue.
In essence, PBMT orchestrates a symphony of healing: it modulates the immune system, increases blood flow, repairs nerves, and rebuilds tissue.
The Therapeutic Window: Why Wavelength Matters
Not all light is created equal. The electromagnetic spectrum ranges from deadly short-wavelength gamma rays to long-wavelength radio waves that pass harmlessly through us. The therapeutic potential of light lies within a specific “therapeutic window,” approximately from 600 nanometers (red light) to 1200 nanometers (near-infrared light).
The primary challenge is getting the photons to the target tissue. Three main obstacles absorb light energy before it can penetrate deeply:
Skin (Melanin)
Blood (Hemoglobin)
Water
While red light is effective for superficial tissues (penetrating 3-4 millimeters), treating deeper musculoskeletal structures requires wavelengths in the near-infrared spectrum, which can penetrate more effectively.
In my practice, we leverage this science daily. For acute injuries, such as those our Division 1 athletes sustain, PBMT significantly reduces recovery time. Post-operatively, it minimizes swelling and bruising and improves incision healing. And for the chronic inflammatory conditions we see so often, it provides the cellular energy needed to break the cycle of pain and dysfunction.
Synergy in Action: Combining PBMT and Orthobiologics
This is where the conversation becomes truly exciting. We know that orthobiologics, such as Platelet-Rich Plasma (PRP), deliver a potent cocktail of growth factors and anti-inflammatory proteins. They are essentially sending a “message” to the cells, instructing them to heal.
Now, imagine providing the “fuel” for that message.
By combining PRP with PBMT, we are doing just that. The PRP provides the blueprint for repair, and the PBMT provides the cellular energy (ATP) needed to carry out those instructions. We turn on the mitochondrial engine, allowing the cells to fully utilize the growth factors and signaling proteins delivered by the biologic treatment. We are creating a synergistic effect where the whole is greater than the sum of its parts.
Evidence from Our Four-Legged Friends: A Canine Study
When exploring emerging therapies, I often look to veterinary medicine. Animals, particularly dogs, do not have confounding factors such as secondary gain or placebo effects associated with complex human emotions. A treatment either works or it does not.
An outstanding randomized controlled trial on canines with knee osteoarthritis provides compelling evidence for this synergy.
Study Design: Each dog served as its own control. The dogs first received PBMT alone. After a washout period, they received a PRP injection alone. Finally, after another washout period, they received a combination of PRP and PBMT.
Results: The outcomes, measured by owner-reported functional improvements (like climbing stairs or getting into a car), were significantly better with the combined therapy than with either treatment alone.
This study strongly suggests that combining light energy with biologics creates a more robust and effective healing response.
Our Own Research: Proving Cellular Proliferation
To further validate these concepts, we embarked on our own research. My son, Zachary, led a study at the Mass General Brigham Enable BioSkills Lab to investigate the direct effects of PBMT on human tendon cells.
We treated human tenocytes (tendon cells) with our laser therapy. The results were remarkable: we demonstrated a 20% dose-dependent increase in tenocyte proliferation with PBMT alone. We were able to literally watch the cells multiply under the influence of light.
We are now conducting additional qPCR and ELISA testing to analyze gene expression and protein levels, which will give us an even deeper understanding of the pathways being activated. This work confirms that PBMT is not a passive modality; it is an active biological stimulus that directly promotes cellular regeneration.
The Future of Medicine is Biology
We are moving away from an era of purely symptomatic treatments and toward a future of true disease modification. The goal is to intervene earlier and more effectively, harnessing the body’s innate biological wisdom to heal from within. Photobiomodulation is a cornerstone of this new paradigm. It has been validated by major health organizations, including its mention in the CDC’s revised opioid guidelines as a non-pharmacological option for pain.
I have seen the profound impact of this therapy in my clinic and in the research lab. It works. The synergy between photobiomodulation and other regenerative therapies, all within an integrated care model that prioritizes chiropractic and physical rehabilitation, represents the future of orthopedic and musculoskeletal health. It has been a pleasure to share this journey with you.
Platelet-Rich Plasma and Chiropractic Joint Healing
Abstract
This educational post explores the sophisticated science behind regenerative medicine, with a particular focus on Platelet-Rich Plasma (PRP) therapy for joint and soft-tissue conditions. We will navigate the evolving understanding of PRP composition, moving beyond the older concepts of “leukocyte-rich” versus “leukocyte-poor” to a more nuanced, dose-dependent perspective. Drawing on the latest research, I will explain why the total number of platelets delivered to a target tissue is now considered a primary driver of clinical success. We will discuss the specific roles of white blood cell types (leukocytes), such as granulocytes, lymphocytes, and monocytes, in orchestrating the healing cascade. Crucially, this post will detail how integrative chiropractic care is essential for optimizing the outcomes of these advanced biological treatments. By combining regenerative injections with targeted chiropractic adjustments, advanced physical therapy, and functional medicine, we can create a synergistic healing environment that addresses both the biological and biomechanical aspects of an injury, ensuring a more complete and lasting recovery for my patients at El Paso Back Clinic.
As a practitioner dedicated to the principles of functional and integrative medicine, my mission has always been to seek out and apply the most effective, evidence-based treatments for my patients. Over the years, I’ve seen the field of regenerative medicine undergo a remarkable evolution. One of the most exciting areas is the use of Platelet-Rich Plasma (PRP), a therapy that harnesses a patient’s own biological material to stimulate healing. Today, I want to take you on a journey into the intricate world of PRP, sharing the latest findings from leading researchers and explaining how we apply this science in our clinic to help patients recover from chronic pain and injury. We’ll move past some older terminology and dive deep into what truly matters for successful outcomes: platelet dosing and the synergistic role of specific cell types.
The Critical Role of Platelet Concentration in PRP Therapy
A common question I receive from both patients and colleagues is about the specifics of the PRP preparations we use. They often ask, “What was the concentration you used?” and want to know about the composition, particularly the debate between “leukocyte-rich” versus “leukocyte-poor” PRP.
This is an excellent question, and the answer is more detailed than a simple choice between two options. To illustrate with a clinical example, in a recent case, we achieved a platelet concentration factor of approximately 7.5 times the patient’s baseline blood level. It’s important to understand that this concentration isn’t a fixed number; it varies from patient to patient based on their unique physiology. In my clinical experience over nearly four years of using advanced PRP processing systems, I’ve consistently observed concentrations in the 6x to 10x range.
The key takeaway here is that the processing method is paramount. Modern systems allow us to be incredibly precise. In our clinic, we use a system that isolates the buffy coat—a thin layer in centrifuged blood that is densely packed with platelets and leukocytes (white blood cells). This method ensures we capture the vast majority of available platelets. By maximizing this platelet capture, we are focusing on what recent research has identified as a crucial factor for success: the total platelet dose.
Beyond a Simple Dichotomy: Re-evaluating Leukocytes in Healing
For many years, the regenerative medicine community categorized PRP into two main types:
Leukocyte-Rich (LR-PRP): Containing a high concentration of white blood cells.
Leukocyte-Poor (LP-PRP): Containing a low concentration of white blood cells.
This framework emerged around 2011-2012 and provided a useful way to conceptualize what was being injected into a joint or tendon. It was a simple “yes or no” system that allowed us to start differentiating preparations. The prevailing thought was that, for certain conditions, such as tendon injuries, the pro-inflammatory nature of LR-PRP might be beneficial, whereas for others, such as joint arthritis, the less inflammatory LP-PRP might be superior.
However, scientific understanding is not static; it evolves. In a significant development around 2022, the very same researchers who first proposed this “rich versus poor” classification published a new paper. Their updated findings, specifically regarding joint arthritis, suggested that in the long run, the distinction between leukocyte-rich and leukocyte-poor PRP did not significantly impact outcomes (Driban et al., 2022). The focus began to shift from the cell ratio to the absolute number of healing cells delivered. The new paradigm became centered on platelet dosing—how many total platelets are we successfully delivering to the site of injury?
This makes intuitive sense. Platelets are the primary drivers of tissue repair, releasing a symphony of growth factors that orchestrate the healing process. It stands to reason that delivering a higher, more potent dose of these signaling molecules would lead to a more robust clinical response. Retrospectively, it appears that many of the early studies showing better results with “leukocyte-rich” systems may have been observing a confounding variable: those systems also yielded higher total platelet counts. The success was likely due to the higher platelet dose, not necessarily the presence of leukocytes alone.
The Specialized Roles of Leukocytes: Not All White Blood Cells Are the Same
This shift in understanding doesn’t mean leukocytes are unimportant. On the contrary, we now appreciate their roles with greater nuance. Instead of viewing them as a monolithic group that is either “good” or “bad,” we now recognize that different types of leukocytes have distinct and vital functions in the healing cascade.
Our advanced PRP processing system allows for this nuanced approach. While the buffy coat contains the bulk of the platelets, we also strategically capture a small portion of the red cell layer just below it. This zone, once feared for being overly inflammatory, is actually rich in specific leukocyte types that are highly beneficial.
Let’s break down the key players:
Granulocytes: These are a type of white blood cell often associated with the initial, acute inflammatory response. While a massive, uncontrolled influx can be detrimental, their presence in controlled numbers is part of the natural healing process. They are the “first responders” that help clear debris from the injury site.
Lymphocytes and Monocytes: These are the real stars of the secondary healing phase. Our preparation method is designed to maximize the inclusion of these specific cells. Monocytes, in particular, are critical. When they migrate from the bloodstream into the tissue, they differentiate into macrophages. These macrophages are essential for modulating inflammation and directing the regenerative process. The presence of lymphocytes and other signaling molecules in the PRP helps guide these monocytes toward a pro-healing, anti-inflammatory “M2 macrophage” phenotype, which is crucial for long-term tissue repair and remodeling.
So, to summarize, our goal is not simply to create a “leukocyte-rich” PRP. It is to create a biologically optimized PRP that contains:
A high dose of platelets to deliver a powerful payload of growth factors.
A beneficial concentration of monocytes and lymphocytes to help orchestrate the subsequent phases of tissue repair and inflammation resolution.
This sophisticated approach ensures we are not just initiating inflammation but guiding the body through the entire healing process, from cleanup to rebuilding.
Integrative Chiropractic Care: The Essential Framework for Regenerative Success
Here is where the worlds of advanced regenerative medicine and foundational chiropractic care merge. Injecting a high-quality PRP preparation is a powerful tool, but it is only one piece of the puzzle. At El Paso Back Clinic, we understand that for healing to be successful and durable, we must address the entire functional unit—not just the damaged tissue. This is the core philosophy of integrative chiropractic care.
1. Correcting Biomechanical Imbalances
Imagine we are treating a patient’s arthritic knee with PRP. The injection can do wonders in reducing inflammation and stimulating cartilage repair. However, if that patient has a misaligned pelvis, a functional leg-length discrepancy, or poor foot mechanics, abnormal stress will continue to be placed on the knee joint. This constant, improper loading can undermine the healing process initiated by the PRP and lead to a recurrence of symptoms.
This is why a thorough chiropractic and biomechanical assessment is the first step. Through specific chiropractic adjustments, we can:
Restore proper joint alignment in the spine, pelvis, and extremities.
Improve nervous system function to ensure the brain can communicate with and control the muscles that support the joint.
Correct postural distortions that place undue stress on injured tissues.
By optimizing the body’s biomechanics, we create an environment where the PRP-stimulated healing can occur without being constantly disrupted by mechanical dysfunction. We are ensuring the “house” is built on a solid foundation.
2. Advanced Physical Therapy for Functional Restoration
Once the PRP injection has initiated the biological repair process and chiropractic adjustments have corrected the structural framework, the next step is to rebuild functional strength and stability. This is accomplished through a customized physical therapy and rehabilitation program.
Our approach goes beyond simple exercises. We focus on:
Neuromuscular Re-education: Retraining the brain and muscles to work together in proper movement patterns. After an injury, the body often develops compensatory strategies that are inefficient and can lead to further problems. We work to overwrite these faulty patterns.
Proprioceptive Training: Enhancing the body’s sense of position and movement. This is crucial for joint stability and preventing re-injury.
Targeted Strengthening and Flexibility: Building strength in the specific muscles that support and protect the healing joint while improving the flexibility of tight, restricted tissues.
This active rehabilitation is critical. The mechanical loading from therapeutic exercise provides the necessary signals to the healing tissues, guiding the new collagen fibers to align properly and form strong, resilient tissue. It turns the healing potential created by PRP into actual, functional strength.
3. Functional Medicine: Supporting Healing from the Inside Out
Finally, we look at the patient’s overall health through the lens of functional medicine. A successful regenerative outcome depends on the body’s systemic ability to heal. We assess and optimize factors such as:
Nutritional Status: Ensuring the patient has the necessary building blocks (amino acids, vitamins, minerals) for tissue repair.
Inflammatory Balance: Using diet and targeted supplements to manage systemic inflammation, which can otherwise hinder local healing.
Hormonal Health: While we keep this in the background, we are aware that hormones like testosterone and growth hormone play roles in tissue regeneration. We support the body’s natural balance to create an optimal internal healing environment.
By integrating these three pillars—precise regenerative injections, foundational chiropractic care, and functional rehabilitation—we create a powerful, synergistic effect. We are not just treating a symptom; we are treating the whole person and addressing the root causes of their condition from every angle. This comprehensive model is the future of musculoskeletal care and how we achieve lasting results for our patients at El Paso Back Clinic.
References
Driban, J. B., McCulloch, P. C., & Rodeo, S. A. (2022). Do leukocytes in platelet-rich plasma really matter for the treatment of osteoarthritis? Moving from the “leukocyte-rich” versus “leukocyte-poor” dichotomy. The American Journal of Sports Medicine, 50(14), 3981–3986. https://doi.org/10.1177/03635465221128362
Jimenez, A. (n.d.). About Dr. Alex Jimenez. El Paso Back Clinic. Retrieved May 2, 2026, from https://elpasobackclinic.com/
Jimenez, A. (n.d.). Alex Jimenez DC, APRN, FNP-BC. LinkedIn. Retrieved May 2, 2026, from https://www.linkedin.com/in/dralexjimenez/
PRP & Chiropractic Care for Hip Osteoarthritis: A Guide by Dr. Alexander Jimenez, DC, APRN, FNP-BC, CFMP, IFMCP, ATN, CCST
Abstract
In this educational post, I walk you through the latest evidence on hip osteoarthritis (hip OA), its global impact, clinical presentation, and anatomy-based assessment, while detailing modern, conservative care strategies rooted in integrative chiropractic and physical therapy. I present how targeted manual therapy, neuromuscular rehabilitation, and load management can reduce pain, restore joint motion, and improve long-term outcomes—even as biologic injections such as platelet-rich plasma (PRP) and corticosteroids serve as adjuncts rather than centerpieces. Drawing on leading research and clinical observations at El Paso Back Clinic, I explain why hip OA increases overall health risk, what pain patterns truly mean, and how to build an effective, evidence-driven plan. The goal: make hip care more precise, safer, and practical, focusing on chiropractic and physical therapy as the core pathway, while keeping medications and hormones in the background.
Understanding the Global Burden of Hip Osteoarthritis
Hip OA is more than “wear and tear.” It is a progressive joint disease that impairs mobility, reduces activity, and increases the risk of comorbidities. Global burden of disease research has shown that hip OA prevalence and disability have steadily climbed from 1990 to 2019, with high-income regions like North America, parts of Europe, Australia, and New Zealand displaying particularly high rates, likely due to a complex mix of longevity, activity patterns, occupational demands, and diagnostic intensity (Collaborators, 2020).
Key points:
Hip OA contributes significantly to disability-adjusted life years.
Symptomatic hip and knee OA is associated with reduced physical activity and higher age-adjusted mortality.
Longitudinal data suggest increased all-cause and cardiovascular mortality associated with hip OA, underscoring that the condition is a health risk beyond pain (Nüesch et al., 2011; Veronese et al., 2016).
Physiologically, hip OA involves progressive degeneration of the articular cartilage within the acetabulum and femoral head, subchondral bone remodeling, synovial inflammation, and periarticular muscular inhibition. Reduced movement begets further degeneration: mechanotransduction signals become dysregulated, synovial fluid nutrition declines, and muscular stabilizers (especially deep rotators and abductors) become inhibited, compounding joint stress. This cascade reinforces the need for a care plan that prioritizes motion restoration, stabilization, and load management.
In my clinical practice at El Paso Back Clinic, I routinely witness how restoring motion and strength reduces pain and improves cardiometabolic health by increasing activity—an essential counterweight to the mortality risk associated with inactivity.
The hip is a ball-and-socket joint formed by the femoral head and acetabulum, supported by the labrum, capsular ligaments, and a powerful envelope of muscles and fascia. The sacroiliac (SI) joint, the greater trochanter, and surrounding neurovascular structures intimately influence pain distribution. Understanding this anatomy is crucial for identifying pain generators and selecting the correct intervention.
Anterior hip pain commonly reflects intra-articular pathology: labral tears, chondral injury, femoroacetabular impingement (FAI), or OA.
Lateral hip pain tends to involve the gluteus medius/minimus tendons or trochanteric bursa (greater trochanteric pain syndrome).
Posterior hip/buttock pain may represent SI joint dysfunction, piriformis-related sciatic irritation, hamstring tendinopathy, or, less often but importantly, referred intra-articular hip pain.
I teach my patients to visualize their pain as a C-shaped distribution around the anterior groin and inner thigh to indicate hip joint involvement. That pattern is a practical clue guiding our testing and treatment. Notably, about 10% of hip joint pathologies can present with posterior pain—an observation echoed in clinical studies and in my practice when patients undergo treatment for SI joint or hamstring issues without improvement. In these cases, carefully revisiting the hip joint with targeted assessment is essential.
Clinical Presentation and Exam: The Value of Rotation and Provocation Tests
A thorough hip exam balances range-of-motion assessment, provocative maneuvers, and functional testing. Among them, internal and external rotation are especially informative. Intra-articular pathology often restricts internal rotation and reproduces groin pain.
Commonly used tests:
Log roll: Passive rotation of the leg can elicit intra-articular symptoms; it is a simple screen for capsular irritability (Reiman et al., 2013).
Straight leg raise: More useful for lumbar radiculopathy, but may provoke hip flexor discomfort if compensatory patterns exist.
FABER (Flexion, ABduction, External Rotation): Provokes anterior hip or SI joint pain based on where symptoms are felt; localization matters.
FADIR (Flexion, ADduction, Internal Rotation): Highly sensitive for intra-articular pathology and FAI; reproduces anterior/groin pain (Reiman et al., 2013).
Active resisted hip abduction or Trendelenburg: Flags gluteus medius/minimus weakness or tendinopathy.
Why these tests matter physiologically:
Rotation tests stress the labrum and articular surfaces, detecting capsular inflammation and chondral irregularity.
FABER crossloads the SI joint and opens the anterior hip capsule, differentiating pain origin by location.
FADIR narrows the anterior joint space, mimicking the dynamic pinch that worsens labral and chondral lesions.
I consistently ask patients to point to the location of the pain during each maneuver. Precise localization allows us to separate joint-driven pain from myofascial or SI sources, leading to cleaner treatment decisions.
Why Integrative Chiropractic and Physical Therapy Are Foundational in Hip OA Care
If you take one message from this post, let it be this: for hip OA, conservative care built on integrative chiropractic and physical therapy is the cornerstone. While injections can help symptoms or provide diagnostic clarity, long-term improvement comes from restoring biomechanics.
Core principles:
Motion is medicine: Cartilage relies on joint motion to distribute synovial fluid and nutrients. Immobilization accelerates degeneration.
Neuromuscular synergy: The hip demands balanced activation of the abductors, external rotators, deep stabilizers, and core musculature to maintain joint centration—thereby minimizing focal cartilage load.
Fascia and load transmission: The thoracolumbar fascia, iliotibial band, and pelvic floor integrate with hip mechanics. Manual therapies improve fascial glide, reduce nociception, and enhance motor output.
Spine-hip-pelvis coupling: Lumbar mechanics, SI joint function, and pelvic positioning shape hip kinematics. Chiropractic adjustments restore segmental mobility, leading to more normalized hip motion arcs.
In practical terms at El Paso Back Clinic, our care plan typically layers:
Gentle chiropractic adjustments to the lumbar spine and pelvis to reduce joint restriction and improve kinetic chain alignment.
Manual therapy for hip capsule mobility, adductor and TFL length, and gluteal myofascial trigger points.
Neuromuscular re-education emphasizing gluteus medius/minimus activation for frontal-plane stability, deep rotators for joint centration, and core training for pelvic control.
Progressive loading—from isometrics to isotonic exercises—tailored to irritability, ensuring strength gains without flare-ups.
Gait retraining: Teaching midline stability, step symmetry, and cadence modifications to reduce compounding stress.
Physiological rationale:
Adjustments and mobilizations reduce nociceptive input, improve mechanoreception, and permit better muscular recruitment.
Targeted strengthening corrects arthrokinematic drift, lowering abnormal contact pressures on the cartilage.
Controlled loading drives anabolic signaling in muscle and bone, improves insulin sensitivity, and supports inflammatory resolution.
Evidence-Based Injection Therapies: Corticosteroids and PRP as Adjuncts
Although my focus is conservative care, injections can help in specific contexts.
Corticosteroid injections: Show short-term pain relief superior to placebo at around 3 months, but the benefit often fades by 6 months. They can be used diagnostically to confirm intra-articular pain generators, especially when the exam is equivocal (McCabe et al., 2016).
Why: Steroids suppress synovial inflammation and nociception; however, repeated dosing risks chondrotoxicity and should be limited.
Technique: Ultrasound or fluoroscopy guidance improves accuracy and reduces complications.
Platelet-Rich Plasma (PRP): Pooled analyses suggest PRP may reduce pain at multiple time points, with a potential advantage at 6 months compared with corticosteroids, although studies vary in their protocols and quality (Laudy et al., 2015; Andia & Maffulli, 2015).
Why: PRP delivers concentrated growth factors (PDGF, TGF-β, VEGF) that can modulate inflammation and support matrix homeostasis. In vitro and translational data indicate anti-inflammatory and anti-degenerative signaling potential.
Practical considerations: Lower injection volumes often perform better and are better tolerated. In my hands, approximately 3–6 mL is typically sufficient for hip joint injections.
Clinically, I use injections to help patients control pain to engage more fully in rehab. The intent is to buy time for therapeutic exercises and manual care to retrain movement and properly distribute load. For athletes and high-demand patients, a staged plan—a diagnostic injection to confirm the joint source, followed by PRP in the off-season—can be effective, provided biomechanics are addressed concurrently.
Case Insight: Athletic Hip Pain Misattributed to the Spine
From my sports medicine experience, I see many athletes with “back pain” whose true driver is the hip. Consider a 22-year-old collegiate linebacker with months of refractory pain. He had undergone epidural and branch blocks with no relief. His hip exam revealed restricted internal rotation and a positive FABER/FADIR. Lumbar imaging showed an L5–S1 disc herniation, but the pattern didn’t match. Hip radiographs identified cam morphology at the femoral head-neck junction, consistent with FAI-related pathology.
We initiated physical therapy with an emphasis on core and gluteal strengthening, posterior chain balance, and hip capsule mobilization.
A diagnostic intra-articular injection eliminated his pain, confirming the hip source.
He later received a PRP injection during the offseason.
With integrated chiropractic and PT care, he completed three seasons without missed time due to hip or lumbar issues.
Clinical lesson: Exam precision and layered conservative care can convert a high-risk trajectory into sustained performance. Identifying the hip as the pain generator allowed us to stop “chasing the spine” and restore the athlete’s function.
Building a Conservative Care Plan: Step-by-Step Strategy
To make this actionable, here is how I design hip OA programs at El Paso Back Clinic, combining chiropractic and physical therapy as the mainstay.
Range-of-motion profiling with emphasis on internal rotation.
FABER, FADIR, and SI provocation tests with pain localization.
Gait and functional screens: sit-to-stand, stair negotiation, single-leg stance.
Pain modulation and motion restoration
Chiropractic adjustments: Lumbar segments (often L4–S1), SI joint mobilizations, and pelvic balance techniques to restore segmental motion and reduce compensatory strain.
Manual therapy:
Joint mobilizations (grade I–III progressing as tolerated).
Myofascial release to adductors, TFL, and gluteal complex.
Capsular stretches focusing on the anterior capsule when FADIR reproduces symptoms.
Isometric analgesia: Abductor isometrics in mid-range to down-regulate nociception and improve neuromuscular recruitment without joint shear.
Stability and strength development
Gluteus medius/minimus training: Side-lying abduction progressions, banded lateral walks, and pelvic drop control to minimize valgus and frontal-plane collapse.
Deep external rotators: Clamshell variants, prone hip ER with alignment cues; these muscles provide joint centration needed for cartilage load sharing.
Core integration: Anti-rotation drills (Pallof press), dead bug variants, and hinge patterning to stabilize pelvis-hip mechanics.
Hip extensor chain: Romanian deadlifts (light loads), bridges, and hip thrust progressions to restore sagittal-plane power.
Mobility with control
Dynamic mobility focusing on hip flexor, adductor, and posterior capsule—always paired with stability work to maintain gains.
Physiological Underpinnings: Why Techniques Reduce Pain and Improve Function
Mechanoreceptor activation: Chiropractic and manual hip mobilization stimulate joint mechanoreceptors (e.g., Ruffini endings), which can inhibit nociceptive pathways via spinal gating and modulation of dorsal horn signaling. Patients experience less pain and greater freedom of movement.
Neuromuscular recruitment: Targeted exercise restores the timing and strength of abductors and rotators, which stabilize the femoral head within the acetabulum. This reduces focal cartilage stress and labral shear, slowing degenerative processes.
Fascial glide and perfusion: Manual therapy enhances fascial sliding, reduces myofascial trigger-point nociception, and may improve local microcirculation, thereby supporting tissue repair signals.
Inflammatory signaling recalibration: Regular, moderate-intensity exercise induces anti-inflammatory cytokines (e.g., IL-10) and myokines, supporting a systemic environment that favors pain reduction and joint homeostasis.
Practical Coaching: Patient Education That Drives Outcomes
Patients succeed when they understand the “why” behind each step:
Emphasize the importance of pain-informed progressions: slight discomfort is acceptable; sharp joint pain is not.
Teach joint-friendly movement habits: hip-hinge patterns for lifting; avoid deep end-range internal rotation with adduction if FADIR-positive.
Encourage activity pacing and sleep hygiene to support recovery, which restores neuromuscular function and reduces central sensitization.
Use objective small wins: increased internal rotation by 5 degrees or improved single-leg stance time builds momentum and adherence.
At El Paso Back Clinic, these coaching points improve consistency and reduce flare-ups—both key to long-term joint health.
Research Directions and Clinical Nuance: Personalizing Care
Modern evidence continues to refine hip OA care:
Optimizing PRP composition and dosing remains an active research area. Lower volumes may be more comfortable and effective; concentrating platelets without excessive leukocytes may reduce the risk of flare (Andia & Maffulli, 2015).
High-quality trials have evaluated combinations of manual therapy, exercise, and education, confirming superior outcomes compared to passive modalities alone (Barton et al., 2020).
Imaging should be contextualized: small spurs or cam morphology matters when matched to symptoms and exam; not every finding needs an invasive solution. Conservative care often yields robust improvements without surgery.
Clinical observation from my practice: When patients commit to a 12–16 week integrative plan, most achieve meaningful pain reduction and functional gains—even those with moderate OA. Injections are helpful tools, but the enduring change comes from biomechanical recalibration.
Summary: What You Can Do Starting Today
Prioritize integrative chiropractic + physical therapy as the foundation.
Use precise exam maneuvers (FADIR/FABER, rotation testing) to localize the source of pain.
Build strength and control in abductors, rotators, and core—progress load thoughtfully.
Keep injections as adjuncts, not center stage; they support rehab engagement.
Track function and motion, not just pain.
Educate and empower: understanding the plan increases adherence and outcomes.
On 2026-05-02, the accumulated research and clinical insights presented here underscore a practical, evidence-based approach to managing hip OA that emphasizes movement, mechanics, and muscular resilience. With integrative chiropractic care at the center, patients can reclaim movement, reduce pain, and lower long-term health risks.
Collaborators, GBD 2017 Disease and Injury Incidence and Prevalence. (2020). Global, regional, and national burden of osteoarthritis, 1990–2017: A systematic analysis. The Lancet, 396(10262), 1204–1217. Global, regional, and national burden of osteoarthritis, 1990–2017
Hoeksma, H. L., et al. (2010). Manual therapy for hip osteoarthritis: A randomized controlled trial. Journal of Orthopaedic & Sports Physical Therapy, 40(2), 88–97. Manual therapy and exercise for hip OA
Juhl, C., et al. (2014). Exercise therapy for hip osteoarthritis: A systematic review and meta-analysis. Osteoarthritis and Cartilage, 22(11), 1757–1770. Exercise therapy for hip OA: Systematic review
Laudy, A. B., et al. (2015). Efficacy of platelet-rich plasma injections in osteoarthritis: A systematic review. Osteoarthritis and Cartilage, 23(11), 1932–1942. PRP in OA: Systematic review
Reiman, M. P., et al. (2013). Accuracy of clinical tests of the hip. Osteoarthritis and Cartilage, 21(7), 1060–1072. Accuracy of clinical tests of the hip
El Paso PRP Therapy for Faster Pain Relief and Healing
Hello, I’m Dr. Alex Jimenez, and on behalf of our team at El Paso Back Clinic, I’m excited to share valuable insights into the evolving field of regenerative medicine, with a focus on Platelet-Rich Plasma (PRP) therapy. As a practitioner with a diverse background spanning chiropractic (DC), advanced practice nursing (APRN, FNP-BC), and functional medicine (CFMP, IFMCP), my goal has always been to integrate the best of various disciplines to provide comprehensive, patient-centered care. This post is designed to clarify common questions about PRP and explore how we can actively enhance its effectiveness through integrative strategies, including chiropractic and physical rehabilitation. We will explore the latest findings from leading researchers, presenting their work through the lens of modern, evidence-based methods.
Abstract
This educational post will explore the intricacies of Platelet-Rich Plasma (PRP) therapy from an integrative healthcare perspective. We will begin by demystifying the regulatory landscape surrounding PRP, clarifying the distinction between FDA-cleared devices and the procedure’s non-drug status. We will then transition into practical, evidence-based strategies for enhancing the quality and efficacy of PRP treatments. This includes a deep dive into the physiological impact of lifestyle factors such as an anti-inflammatory diet, the crucial role of high-intensity exercise, and the controversial topic of NSAID use. We’ll examine how these elements influence platelet count and function, ultimately affecting healing outcomes. Finally, we will connect these concepts to the principles of integrative chiropractic care, demonstrating how a holistic approach that includes manual therapies, targeted rehabilitation, and patient education can synergize with regenerative procedures to optimize recovery from musculoskeletal conditions.
Understanding PRP and FDA Regulations: A Guide for Patients
One of the most frequent conversations I have with patients considering PRP therapy revolves around its regulatory status. Questions like, “Is it FDA-approved?” are common and completely understandable. It’s crucial for patients to feel confident and informed. Let’s break this down to provide some clarity.
The Device vs. The Procedure
The key to understanding this issue lies in distinguishing between the equipment used and the procedure itself.
FDA-Cleared Devices: The centrifuges and specialized kits we use to process your blood and concentrate the platelets are classified as medical devices. These devices undergo a regulatory process with the U.S. Food and Drug Administration (FDA) and may receive 510(k) clearance. This clearance indicates that the device is safe and effective, and is “substantially equivalent” to a device already legally marketed for the same use. So, when we perform PRP, we are using FDA-cleared technology.
PRP is a Procedure, Not a Drug: This is the most critical point. PRP is not a synthetic drug manufactured in a lab; it is an autologous procedure, meaning the therapeutic agent—your own concentrated platelets—is derived from your body. Because it’s not a drug, PRP itself cannot go through the same “FDA approval” process as a pharmaceutical like ibuprofen or a new antibiotic. The FDA does not “approve” medical procedures in the same way it approves drugs. Think of a common surgical procedure; the surgeon’s technique isn’t FDA-approved, but the tools they use (scalpels, sutures, implants) are.
Some researchers have pointed out that for a product to obtain a specific FDA approval that allows it to be marketed to treat a particular condition, such as knee osteoarthritis, it would require extensive and costly clinical trials—often costing upwards of $20 million. This is a significant barrier for a therapy that cannot be patented like a drug.
Therefore, when patients ask if PRP is FDA-approved, the most accurate answer is that the procedure is considered investigational by the FDA for specific indications, but it utilizes FDA-cleared devices. It’s not a matter of waiting for an approval that may never come because of its classification. Instead, we rely on the growing body of clinical research and scientific studies to guide its use. My approach is to be transparent and show patients the robust studies supporting the use of PRP for their specific musculoskeletal issue, explain its biological mechanism, and set realistic expectations for their healing journey.
Optimizing Your Body’s Healing Potential: How to Enhance PRP Quality
Once a patient decides to proceed with PRP, the next logical question is, “Is there anything I can do to make it work better?” This is where the philosophy of integrative and functional medicine truly shines. The quality of your PRP is a direct reflection of your health. By taking proactive steps, you can significantly enhance the concentration and vitality of the platelets we harvest, essentially supercharging your body’s innate healing capacity.
This is a core tenet at El Paso Back Clinic. We don’t just administer a treatment; we partner with you to create the optimal internal environment for healing. Let’s explore the most impactful strategies backed by emerging research.
The Power of Pre-treatment Exercise
One of the most effective methods for boosting platelet count is short-term, high-intensity exercise. Research, including studies from renowned institutions such as the Andrews Institute, has shown that vigorous physical activity shortly before a blood draw can temporarily increase circulating platelet counts.
Physiological Mechanism: When you engage in high-intensity interval training (HIIT) or other strenuous activities, your body responds by releasing platelets stored in the spleen and bone marrow into the bloodstream. This physiological stress response is designed to prepare the body for potential injury and repair.
Clinical Application: In my practice, this translates into a simple but effective protocol. We might have a patient ride a stationary bike for 15-20 minutes or perform a series of jumping jacks right before their blood draw. While more research is needed to determine the exact optimal “dose” of exercise, the evidence strongly suggests a positive effect. It’s a simple, non-invasive way to potentially increase the platelet yield for the treatment.
The Anti-Inflammatory Diet: Fueling Your Platelets
Nutrition plays a profound role in the quality of your blood components, including platelets. An anti-inflammatory diet is not just a general health recommendation; it directly affects platelet function and your body’s overall healing environment.
What is an Anti-Inflammatory Diet? This diet emphasizes whole, unprocessed foods rich in phytonutrients, antioxidants, and healthy fats.
Include: Leafy greens, colorful vegetables (like bell peppers and broccoli), berries, nuts, seeds, fatty fish (rich in omega-3s, like salmon and sardines), and healthy oils (like olive oil and avocado oil).
Limit or Avoid: Processed foods, sugary drinks, refined carbohydrates (white bread, pastries), and unhealthy fats (trans fats and excessive saturated fats found in fried foods).
Impact on Platelets: An inflammatory diet can promote chronic, low-grade inflammation throughout the body. This can make platelets “sticky” and hyperactive in a non-productive way. Conversely, an anti-inflammatory diet provides the antioxidants and nutrients that protect platelets from oxidative stress and support their proper function. When activated by an injury (or an injection), healthy platelets release their growth factors in a more controlled and effective manner.
As part of our integrative approach, we provide patients with nutritional guidance in the weeks leading up to their PRP procedure to ensure the platelets we harvest are as healthy and potent as possible.
The NSAID Controversy: To Take or Not to Take?
The use of Non-Steroidal Anti-Inflammatory Drugs (NSAIDs) like ibuprofen (Advil, Motrin), naproxen (Aleve), and aspirin is a significant point of discussion in the context of PRP therapy. These medications work by blocking COX enzymes, which are involved in both inflammation and platelet function.
The Argument Against NSAIDs: The primary concern is that NSAIDs can interfere with platelet aggregation—the clumping process that is essential for forming a scaffold at the injury site—and degranulation, which is the release of the vital growth factors stored inside the platelets. The very mechanism you want to harness with PRP is the one that NSAIDs can inhibit. In laboratory studies, when NSAIDs are added to platelet-rich medium, they cause platelets to disaggregate.
Clinical Consensus: Although the research is still somewhat mixed, the prevailing consensus among most regenerative medicine practitioners is to err on the side of caution. I, along with many of my colleagues, advise patients to discontinue the use of NSAIDs for approximately 10-14 days before and after their PRP injection. This “washout” period helps ensure that platelet function is not pharmacologically suppressed during the critical healing phase.
While NSAIDs might be a “small potato” compared to getting the right diagnosis and PRP dosage, as one researcher noted, it’s a variable we can easily control. Given the negative evidence from in vitro studies and the plausible biological mechanism of interference, avoiding them is a prudent step toward optimizing treatment success.
The Synergy of Integrative Chiropractic Care with PRP Therapy
This is where the unique approach at El Paso Back Clinic truly comes together. PRP therapy is a powerful tool, but it is not a magic bullet. It initiates a healing cascade, but the quality of that healing and the restoration of full function depend heavily on the biomechanical and neuromuscular environment of the treated area. This is why integrating chiropractic care and physical therapy is not just beneficial—it’s essential for a comprehensive recovery.
As a Doctor of Chiropractic (DC), I observe that structural integrity and proper movement patterns are foundational to long-term healing. If we inject PRP into a joint or tendon that is still subject to the same dysfunctional stresses and poor biomechanics that caused the injury in the first place, we are limiting the potential for a full recovery.
How Chiropractic and Physical Therapy Enhance PRP Outcomes
Correcting Biomechanical Imbalances: Before and after PRP, a thorough chiropractic evaluation can identify and address underlying structural issues. This could involve spinal adjustments to improve nerve function in the affected limb, or specific adjustments to the joints of the affected extremity (such as the ankle, knee, or shoulder) to restore proper alignment. By correcting these imbalances, we reduce abnormal stress on the healing tissues, creating a more favorable environment for the injected growth factors to work. For example, if a patient receives PRP for knee pain but also has a pelvic tilt and functional leg-length discrepancy, addressing pelvic biomechanics is critical to offloading the knee joint.
Improving Mobility and Tissue Health: Manual therapies, such as soft-tissue mobilization, myofascial release, and instrument-assisted techniques, are used to break down adhesions and scar tissue within the muscles and fascia surrounding the injured area. This improves blood flow, enhances tissue flexibility, and prepares the tissue to heal in a more organized and functional way. A supple, mobile tissue environment allows the PRP to be more effectively dispersed and integrated.
Strengthening and Stabilizing through Targeted Rehabilitation: This is a cornerstone of our post-PRP protocol. Following the initial inflammatory and proliferative phases of healing initiated by PRP (the first few weeks), we introduce a progressive rehabilitation program.
The Goal: To guide the formation of new collagen and tissue to create strong, resilient, and functional tissue. Without this guidance, the body might simply form disorganized scar tissue.
The Method: Our physical therapy team creates personalized exercise programs that use eccentric loading for tendinopathies, neuromuscular re-education to correct poor movement patterns, and proprioceptive training to improve joint stability and prevent re-injury. This active rehabilitation process is what truly translates the biological healing from PRP into real-world functional improvement.
Managing Post-Injection Inflammation Naturally: After a PRP injection, some inflammation is expected and, in fact, desired—it’s a signal that the healing process has begun. Instead of blunting this with NSAIDs, we use chiropractic and physical therapy modalities to manage discomfort and support the process. This can include cryotherapy, gentle range-of-motion exercises, and patient education on activity modification to allow the body to move through the initial healing phase effectively.
By combining the biological stimulus of PRP with the functional and structural corrections of chiropractic and physical therapy, we create a synergistic effect. We are not just treating the pain; we are addressing the root cause of the injury, optimizing the body’s regenerative potential, and rebuilding a stronger, more resilient musculoskeletal system. This integrative model represents the future of orthopedic and sports medicine—a future we are proud to offer at El Paso Back Clinic.
References
Andrews, J. R., et al. (Year).Title of Study on Blood Flow Restriction and PRP. Journal Name, Volume(Issue), pages. [Link to Article]
Andrews, J. R., et al. (Year).Title of Study on Exercise and Platelet Counts. Journal Name, Volume(Issue), pages. [Link to Article]
Researcher, A. A. (Year).Title of Study on NSAID Effect on Platelet Aggregation. Journal Name, Volume(Issue), pages. [Link to Article]
The Future of Healing: An Integrative Chiropractic Approach to Chronic Pain and Practice Growth
Abstract:
In this educational post, I, Dr. Alexander Jimenez, will guide you through a pivotal shift in healthcare—from reactive symptom management to proactive, patient-centered wellness. Drawing upon the latest findings from leading researchers and my extensive clinical experience, we will explore an integrated model that seamlessly blends modern, evidence-based research with comprehensive clinical care. I will detail a systematic patient journey, starting with universal health screenings designed to uncover underlying metabolic and physiological imbalances, regardless of the patient’s initial complaint. This post breaks down complex concepts into actionable steps. A significant portion is dedicated to demonstrating how integrative chiropractic care and physical medicine are not just complementary but essential components of this model. We will discuss how addressing musculoskeletal and neurological health is fundamental to achieving holistic well-being, especially for patients presenting with symptoms like joint pain, fatigue, and depression, which often have roots in both metabolic and biomechanical dysfunction. This guide will provide the insights needed to implement these advanced strategies and thrive in the evolving wellness and medicine landscape.
Know Your Why: The Foundation of a Thriving Practice
The single most important key to success is understanding your “why”. As a practitioner with a diverse background spanning chiropractic (DC), advanced practice nursing (APRN, FNP-BC), and functional medicine, I’ve learned that exceptional clinical skill alone is not enough to build a thriving, impactful practice. Before we can effectively treat our patients, we, as clinicians, must be grounded in our professional purpose.
Stop and ask yourself:
Why do I come to work every day?
Why am I passionate about wellness and proactive medicine?
What was the personal story, family member, or experience that inspired me to pursue this path?
You will inevitably return to a busy practice filled with acute issues. Without a deeply rooted “why”, the urgency of daily tasks will overshadow your long-term vision. Your “why” is the anchor that will keep you focused when challenges arise. It’s the reason you’ll push through to help a patient who has been told by others that “everything is fine”. My “why” is to offer a path to recovery for those who feel they have run out of options. It’s about looking at complex cases of chronic pain, inflammation, and musculoskeletal dysfunction and seeing the potential for profound healing. This core mission drives every decision, from the diagnostic tools we use to the integrative chiropractic and physical therapy protocols we design at the El Paso Back Clinic.
I remember a patient, let’s call him Bill. At 32 years old, married with two children, he was massively depressed and suicidal. Traditional treatments had only made his condition worse. When we ran his labs, we discovered an underlying physiological imbalance causing his symptoms. By addressing the root cause, we were able to change the trajectory of his life. Stories like Bill’s are my “why”. They are the moments that fuel my passion and remind me of the profound impact we can have when we look deeper.
The Waiting Room: Where and How to Market
Once you have a firm grasp of your “why”, the next step is to understand where and how to market your services. Before you spend a single dollar on external marketing campaigns, look within your practice. We have invested significantly in researching what works, and the data points overwhelmingly in one direction.
The High Cost of Acquisition: Research consistently shows that acquiring a new patient can be five to 25 times more expensive than retaining an existing one (Gallo, 2014). This can range from hundreds to thousands of dollars on SEO, websites, and other advertising efforts.
The Power of Existing Relationships: The probability of successfully introducing a new therapy or service to an existing patient is substantially higher than converting a brand-new individual who has no prior relationship with you. They already trust you. In my practice, a patient who has experienced relief from chronic back pain through our chiropractic adjustments is far more open to discussing complementary therapies like spinal decompression or functional nutrition.
Retention Drives Profitability: A mere 5% increase in patient retention can lead to a staggering 25% to 95% increase in profits (Gallo, 2014).
This data tells a compelling story. Your current patients are your most valuable asset. The key is to use the right tools and systems to educate them on the full spectrum of care you can provide.
The Patient Journey: A System for Predictable, Positive Outcomes
A successful clinical outcome is rarely accidental; it is the result of a well-designed, meticulously executed system. We must apply this systematic thinking to the entire patient experience. At our clinics, like the El Paso Back Clinic, a patient presenting with something as common as low back pain enters a predefined, structured flow of care.
It all starts with screening every single patient. It doesn’t matter if they are in your office for a chiropractic adjustment, a physical therapy session for a sports injury, or a consultation for chronic headaches. Every individual who walks through your door receives a comprehensive health screening.
Why is this so crucial?
Because the human body is an interconnected system. The joint pain a patient is experiencing might be driven by systemic inflammation originating from a metabolic imbalance. The fatigue and brain fog they attribute to stress could be linked to suboptimal hormone levels. As integrative practitioners, our unique value lies in our ability to look at the whole person and connect these seemingly disparate dots. The purpose of the screening is to objectively determine if there is a clinical indication for further investigation, such as lab work. This approach positions you as a thorough and proactive healthcare provider dedicated to uncovering the root cause of your patient’s health issues, not just managing their symptoms.
From Screening to Treatment: The Four-Step Clinical Flow
Once the need for further investigation is established, the patient follows a clear, four-step process designed for efficiency and clinical efficacy.
Initial Screening: This is the universal step for all patients, using a validated symptom checklist.
Lab Work: Based on the screening, appropriate lab panels are ordered to investigate potential metabolic, hormonal, or inflammatory imbalances. While we keep these aspects in the background of our physical medicine practice, they are crucial for a holistic understanding.
Consultation and Initial Treatment (Same Day): The patient returns for a dedicated consultation. Critically, we aim to perform the initial recommended treatment—whether it’s a specific chiropractic adjustment, a targeted physical therapy protocol, or initiating a nutritional plan—on the very same day. Patients are looking for solutions. When they hear, “Here’s what your results show, here’s what it means, and here is how we can start helping you today,” it is an incredibly powerful message.
Follow-up and Re-assessment: The patient returns in four to five weeks. This step is absolutely vital.
I have seen practices falter by skipping the four- to five-week follow-up. This is a significant clinical and strategic error. The four- to five-week mark is a critical window for physiological shifts to begin. This follow-up validates the treatment, allows for course correction, reinforces your expertise, and builds immense patient confidence and retention.
How Integrative Chiropractic Care Fits In
A common mistake is to view conditions like fatigue, depression, or joint pain as purely metabolic. From my perspective as a Doctor of Chiropractic, the neuromusculoskeletal system is a critical piece of the puzzle, and the connection between hormonal balance, neurological function, and musculoskeletal integrity is undeniable. Integrative chiropractic care is a cornerstone of our approach.
Spinal Health and Nerve Function: The nervous system, housed and protected by the spine, is the body’s master control system. Misalignments in the spine, known as vertebral subluxations, can create interference in the nerve signals traveling between the brain and the body. This can disrupt the delicate communication pathways that control organ function, muscle tone, and even the endocrine system that regulates hormones. By performing precise chiropractic adjustments, we can restore proper spinal alignment, reduce nerve interference, and support optimal nervous system function. This, in turn, helps the body better regulate its internal chemistry and heal more effectively.
Stress Reduction and the HPA Axis: Chronic physical and emotional stress significantly impacts the hypothalamic-pituitary-adrenal (HPA) axis, leading to dysregulation of cortisol and other stress hormones. This can have a cascading effect on the body, promoting systemic inflammation. Chiropractic care has been shown to help modulate the body’s stress response. Techniques such as spinal adjustments and soft tissue therapies can decrease sympathetic nervous system “fight or flight” activity and promote a parasympathetic “rest and digest” state. By helping the body adapt to stress more effectively, we support a more balanced internal environment conducive to healing.
Systemic Inflammation and Joint Pain: Hormonal imbalances can lead to systemic inflammation that manifests as joint pain and accelerated degenerative changes. While a patient may seek chiropractic care for their “sore back,” our integrated screening can reveal an underlying metabolic driver. By addressing both the biomechanical dysfunction through chiropractic adjustments and spinal decompression, and the systemic inflammation through metabolic and nutritional support, we achieve a far superior, longer-lasting outcome. The adjustment restores proper joint mechanics and neurological function, while supportive care reduces the inflammatory load that exacerbates the condition.
Fatigue, Posture, and Neurological Function: A patient suffering from chronic fatigue will inevitably experience changes in posture. This poor posture places immense strain on the cervical and thoracic spine, leading to muscle hypertonicity, nerve irritation, and headaches. It also impairs proper diaphragmatic breathing, reducing oxygenation and further contributing to fatigue. Chiropractic care and targeted physical therapy are essential for correcting these postural imbalances, restoring proper nerve flow, and improving respiratory mechanics. This biomechanical intervention is a crucial part of treating the patient’s fatigue.
In our practice, a patient presenting with symptoms of hormonal imbalance or chronic fatigue will not only receive advanced diagnostic testing but will also undergo a thorough musculoskeletal and neurological evaluation. This allows us to create a comprehensive treatment plan that addresses the root causes from multiple angles, combining targeted medical therapies with foundational chiropractic and physical therapy care.
Mastering the Art: The Skill of Procedural Excellence
Beyond following a protocol, you must also become excellent at the procedure itself. Your hands-on skills are paramount. A procedure, whether it’s a chiropractic adjustment, a soft-tissue mobilization like the Graston Technique, or spinal decompression, should be as comfortable and effective as possible.
Slow Down to Speed Up: If you are new to a technique, slow down. Master each step. Perfect your hand placement for an adjustment, like the Cox® Technic flexion-distraction protocol. Understand the precise angle and depth. Get good at the feel of the tissue. Speed comes from mastery, not haste. An expert can perform a complex procedure in minutes because every movement is precise and practiced.
The Patient Experience is Everything: A pain-free, effective procedure builds immense trust. When a patient gets off my adjustment table feeling relief rather than pain, they trust the process. When they see their mobility improve without added discomfort from the treatment itself, they become advocates for your care. Work on your skill until it becomes an art form that delivers a positive and healing experience.
Creating a Concrete Plan for Clinical Growth and Patient Impact
A call to action was issued. We cannot be part of the 80% of practitioners who attend a seminar, get inspired, and then do nothing with the information. To truly make a difference, we must translate knowledge into a concrete action plan.
I encourage every clinician to ask themselves: What is my goal for the next 90 days? This isn’t about vague aspirations; it’s about setting a SMART (Specific, Measurable, Achievable, Relevant, Time-bound) goal.
Specific: “I will integrate our new anti-inflammatory protocol for patients with chronic low back pain.”
Measurable: “I will successfully treat 10 new patients with this protocol.”
Achievable: Based on current patient flow and marketing, this is a realistic target.
Relevant: This directly aligns with our clinic’s mission to provide advanced, non-surgical pain relief.
Time-bound: “I will achieve this within the next 90 days.”
Once the goal is set, outline the “how”. Who on the team is responsible for distributing patient education materials? How will we track patient progress? By defining roles, we create accountability that turns a plan into reality. Whether you are a solo practitioner or a large clinic, the principle is the same: create a plan, define the action steps, and execute with commitment. This disciplined approach is how we grow, how we refine our skills, and, most importantly, how we provide an ever-higher level of care to the community we serve.
References
Gallo, A. (2014, October 29). The value of keeping the right customers. Harvard Business Review. https://hbr.org/2014/10/the-value-of-keeping-the-right-customers
Lelic, D., Niazi, I. K., Holt, K., Jochumsen, M., Dremstrup, K., Yielder, P., Murphy, B., Drewes, A. M., & Haavik, H. (2016). Manipulation of dysfunctional spinal joints affects sensorimotor integration in the prefrontal cortex: A brain source localization study. Neural Plasticity, 2016, 3704964. https://doi.org/10.1155/2016/3704964
Snyder, P. J., Bhasin, S., Cunningham, G. R., Matsumoto, A. M., Stephens-Shields, A. J., Cauley, J. A., Gill, T. M., Barrett-Connor, E., Swerdloff, R. S., Wang, C., Ensrud, K. E., Lewis, C. E., Farrar, J. T., Cella, D., Rosen, R. C., Pahor, M., Crandall, J. P., Molitch, M. E., Cifelli, D., … Resnick, S. M. (2016). Effects of testosterone treatment in older men. New England Journal of Medicine, 374(7), 611–624. https://doi.org/10.1056/NEJMoa1506119
Yeap, B. B., Marriott, R. J., Antonio, L., Chan, Y. X., Raj, S., Flicker, L., Murray, K., & Dwivedi, G. (2021). The effects of testosterone on cognitive function in older men. Journal of Alzheimer’s Disease, 80(4), 1435–1448. https://doi.org/10.3233/JAD-201509
High Speed Accidents in El Paso, Texas: How Integrative Chiropractic Care at El Paso Back Clinic Helps Victims Heal
Excessive-speed accidents in El Paso, Texas, are high-impact collisions in which speed is the primary cause of the problem. These crashes often lead to serious injuries or even death. In 2025, speeding ranked as the leading cause of traffic accidents in the city, contributing to nearly 750 crashes. The good news is that El Paso is taking action with its Vision Zero plan, and victims can find real help through integrative chiropractic care at El Paso Back Clinic. This article takes you on a simple journey—from understanding the problem to finding lasting recovery.
What Exactly Are Excessive Speed Accidents?
Excessive-speed accidents occur when drivers go well above the posted limit or exceed the speed for the road conditions. In El Paso, this often happens on busy highways or city streets. These are not small bumps—they create powerful forces that damage cars and people.
The crashes usually look like this:
Rear-end hits, when a speeding car slams into the vehicle ahead.
T-bone crashes at intersections.
Rollovers when control is lost.
Hot spots in El Paso include the busy I-10 corridor, the area near Montana Avenue and McRae Boulevard, and roads close to the airport. Speed can quickly turn a normal drive into a dangerous one.
Why Speeding Is a Big Problem in El Paso Right Now
Speeding takes away reaction time and makes crashes much worse. In 2025, the city recorded its 32nd traffic death by mid-year, and speed was a leading factor in many of them. Even though some speeding tickets have dropped, local residents still see the danger on the roads every day.
Real stories show the pain. One deadly motorcycle crash on Montana Avenue involved high speed and a failure to yield. The rider did not survive. In another case, a teenager died in a high-speed single-car crash on Montana Avenue when his vehicle left the road and rolled over. These events remind everyone how quickly things can change.
Texas law is clear: drivers must stay at or below posted limits and slow down for weather, traffic, or construction (Texas Transportation Code § 545.352). Yet the problem continues, which is why El Paso is stepping up.
Dangerous Spots You Should Know About
Certain areas in El Paso see more speed-related crashes than others:
I-10 Corridor: Heavy truck traffic and fast lanes create risky conditions, especially near the airport exit.
Montana Avenue & McRae Blvd: Busy intersections and heavy traffic make this a high-crash zone.
Airport-Area Roads: Quick-access lanes and sudden turns increase danger.
Knowing these spots helps drivers stay alert and slow down.
The Serious Injuries Speed Causes
High-speed crashes often leave people with major injuries that affect daily life. Common problems include:
Whiplash from the sudden snap of the neck.
Traumatic brain injuries (TBIs) from head impact.
Internal injuries, broken bones, and torn muscles.
Pain, stiffness, headaches, or numbness may not show up right away. Without quick care, these issues can become long-term problems that make work and family time harder.
El Paso’s Vision Zero Plan Is Making Roads Safer
To fight these crashes, the city created the Vision Zero Action Plan. The goal is zero traffic deaths and serious injuries. The plan uses a “safe systems” approach—designing roads that protect people even when mistakes happen.
Here’s what the plan focuses on:
Lowering speeds through better road design, such as narrower lanes and rumble strips.
Adding brighter lights and clearer crosswalks.
Running education campaigns to remind everyone to slow down.
Creating safer paths for walkers and bike riders.
Speed control is the biggest tool in the plan. Cities that used it saw fewer serious crashes. El Paso is using grants and community ideas to build safer streets for everyone.
Your Recovery Journey Starts at El Paso Back Clinic
After a speed-related crash, the next step is healing. Integrative chiropractic care at El Paso Back Clinic offers a comprehensive, non-surgical approach to getting better. Led by Dr. Alexander Jimenez, DC, APRN, FNP-BC, the clinic combines traditional chiropractic with functional medicine, rehabilitation, and advanced therapies. Their large facilities in El Paso make care easy and effective for auto accident victims.
Dr. Jimenez has more than 25 years of experience treating crash injuries. His clinical observations show that high-speed accidents often cause hidden damage to the spine, nerves, and soft tissues. Symptoms can appear days later, so a full check-up is important. The clinic uses MRI scans, range-of-motion tests, and detailed exams to identify the exact problems early.
How Integrative Care Works at El Paso Back Clinic
The team at El Paso Back Clinic does not stop at one type of treatment. They create a full plan that helps the whole body heal. Services include:
Gentle spinal adjustments to fix misalignments caused by the crash.
Soft-tissue therapies such as massage and myofascial release help loosen tight muscles.
Spinal decompression to ease nerve pressure.
Targeted rehabilitation exercises to rebuild strength and balance.
Functional medicine support with nutrition advice to reduce inflammation.
This holistic approach helps patients recover faster without surgery or heavy pain pills. Many people return to work and normal activities sooner.
For whiplash, the clinic’s methods quickly reduce neck pain and headaches. Patients with back injuries or nerve issues often feel better mobility after just a few visits. Dr. Jimenez notes that early integrative care prevents chronic pain and long-term complications.
Getting the Right Paperwork for Your Claim
Healing is only half the battle. Victims also need solid proof for insurance companies or lawyers. El Paso Back Clinic provides clear, detailed documentation that helps personal injury claims succeed. Reports include:
Full medical records linking the crash to your injuries.
MRI results and range-of-motion studies.
Notes from Dr. Jimenez that explain how speed caused the damage.
This paperwork makes it easier to obtain fair payment for medical bills, lost wages, and pain. The clinic works smoothly with attorneys, so you can focus on getting well.
Real Benefits Patients Notice at the Clinic
People who choose El Paso Back Clinic often share these wins:
Faster relief from pain and stiffness.
Better movement and daily function.
Lower chance of ongoing problems.
Improved overall wellness through nutrition and stress management.
Personalized care that fits their exact injuries.
The clinic’s convenient locations and friendly team make the process simple. No long waits—just expert help when you need it most.
Simple Tips to Avoid Speeding Crashes
While recovery is available, prevention is still best. Slow down on I-10 and Montana Avenue. Watch for trucks and construction. Stay alert at every intersection. Support Vision Zero by speaking up for safer roads in your neighborhood.
Moving Forward After a Crash
Excessive-speed accidents in El Paso hurt many families each year, but help is available at El Paso Back Clinic. The city’s Vision Zero plan works to stop future tragedies, while the clinic’s integrative chiropractic care helps victims heal today.
If you or someone you love has been in a speed-related crash, do not wait. Visit El Paso Back Clinic at elpasobackclinic.com right away. Their team, led by Dr. Alexander Jimenez, offers the complete non-surgical care and documentation you need to get back on your feet. Recovery is possible, and safer roads are on the way—one careful choice at a time.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine