These assessment and treatment recommendations represent a synthesis of information derived from personal clinical experience and from the numerous sources which are cited, or are based on the work of researchers, clinicians and therapists who are named (Basmajian 1974, Cailliet 1962, Dvorak & Dvorak 1984, Fryette 1954, Greenman 1989, 1996, Janda 1983, Lewit 1992, 1999, Mennell 1964, Rolf 1977, Williams 1965).
Clinical Application of Neuromuscular Techniques: the Subscapularis Muscle
The subscapularis is a large triangular muscle which fills the subscapular fossa and inserts into the lesser tubercle of the humerus and the front of the capsule of the shoulder-joint.
The subscapularis rotates the head of the humerus medially (internal rotation) and adducts it; when the arm is raised, it draws the humerus forward and downward. It is a powerful defense to the front of the shoulder-joint, preventing displacement of the head of the humerus.
Damage or trauma from an injury or an aggravated condition can cause shortness in the subscapularis muscle. The following assessments and treatments can help improve structure and function.
Assessment of Shortness in the Subscapularis Muscle
Subscapularis shortness test (a) Direct palpation of subscapularis is required to define problems in it, since pain patterns in the shoulder, arm, scapula and chest may all derive from subscapularis or from other sources.
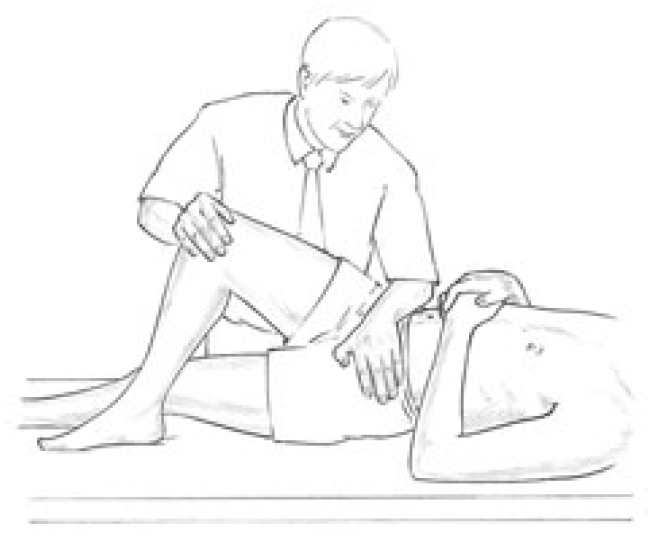
The patient is supine and the practitioner grasps the affected side hand and applies traction while the fingers of the other hand palpate over the edge of latissimus dorsi in order to make contact with the ventral surface of the scapula, where subscapularis can be palpated. There may be a marked reaction from the patient when this is touched, indicating acute sensitivity.
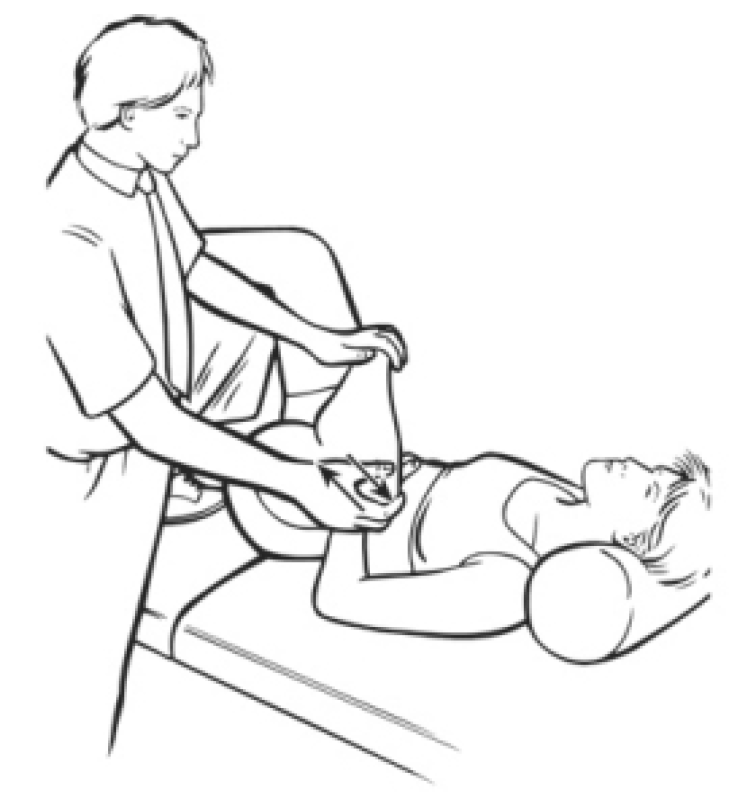
Subscapularis shortness test (b) (as seen on Fig. 4.39 below) The patient is supine with the arm abducted to 90�, the elbow flexed to 90�, and the forearm in external rotation, palm upwards. The whole arm is resting at the restriction barrier, with gravity as its counterweight.
If subscapularis is short the forearm will be unable to rest easily parallel with the floor but will be somewhat elevated.
Figure 4.39A, B Assessment and MET self-treatment position for subscapularis. If the upper arm cannot rest parallel to the floor, possible shortness of subscapularis is indicated.
Care is needed to prevent the anterior shoulder becoming elevated in this position (moving towards the ceiling) and so giving a false normal picture.
Assessment of Weakness in the Subscapularis Muscle
The patient is prone with humerus abducted to 90� and elbow flexed to 90�. The humerus should be in internal rotation so that the forearm is parallel with the trunk, palm towards ceiling. The practitioner stabilises the scapula with one hand and with the other applies pressure to the patient�s wrist and forearm as though taking the humerus towards external rotation, while the patient resists.
The relative strength is judged and the method discussed by Norris (1999) should used to increase strength (isotonic eccentric contraction performed slowly).
MET Treatment of the Subscapularis Muscle
The patient is supine with the arm abducted to 90�, the elbow flexed to 90�, and the forearm in external rotation, palm upwards. The whole arm is resting at the restriction barrier, with gravity as its counterweight. (Care is needed to prevent the anterior shoulder becoming elevated in this position (moving towards the ceiling) and so giving a false normal picture.)
The patient raises the forearm slightly, against minimal resistance from the practitioner, for 7�10 seconds and, following relaxation, gravity or slight assistance from the operator takes the arm into greater external rotation, through the barrier, where it is held for not less than 20 seconds.
Dr. Alex Jimenez offers an additional assessment and treatment of the hip flexors as a part of a referenced clinical application of neuromuscular techniques by Leon Chaitow and Judith Walker DeLany. The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
By Dr. Alex Jimenez
Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.
Several types of headaches can affect the average individual and each may result due to a variety of injuries and/or conditions, however, migraine headaches can often have a much more complex reason behind them. Many healthcare professionals and numerous evidence-based research studies have concluded that a subluxation in the neck, or a misalignment of the vertebrae in the cervical spine, is the most common reason for migraine headaches. Migraine is characterized by severe head pain typically�affecting one side of the head, accompanied by nausea and disturbed vision. Migraine headaches can be debilitating. The information below describes a case study regarding the effect of atlas vertebrae realignment on patients with migraine.
Effect of Atlas Vertebrae Realignment in Subjects with Migraine: An Observational Pilot Study
Abstract
Introduction. In a migraine case study, headache symptoms significantly decreased with an accompanying increase in intracranial compliance index following atlas vertebrae realignment. This observational pilot study followed eleven neurologist diagnosed migraine subjects to determine if the case findings were repeatable at baseline, week four, and week eight, following a National Upper Cervical Chiropractic Association intervention. Secondary outcomes consisted of migraine-specific quality of life measures. Methods. After examination by a neurologist, volunteers signed consent forms and completed baseline migraine-specific outcomes. Presence of atlas misalignment allowed study inclusion, permitting baseline MRI data collection. Chiropractic care continued for eight weeks. Postintervention reimaging occurred at week four and week eight concomitant with migraine-specific outcomes measurement. Results. Five of eleven subjects exhibited an increase in the primary outcome, intracranial compliance; however, mean overall change showed no statistical significance. End of study mean changes in migraine-specific outcome assessments, the secondary outcome, revealed clinically significant improvement in symptoms with a decrease in headache days. Discussion. The lack of robust increase in compliance may be understood by the logarithmic and dynamic nature of intracranial hemodynamic and hydrodynamic flow, allowing individual components comprising compliance to change while overall it did not. Study results suggest that the atlas realignment intervention may be associated with a reduction in migraine frequency and marked improvement in quality of life yielding significant reduction in headache-related disability as observed in this cohort. Future study with controls is necessary, however, to confirm these findings. Clinicaltrials.gov registration number is NCT01980927.
Introduction
It has been proposed that a misaligned atlas vertebra creates spinal cord distortion disrupting neural traffic of brain stem nuclei in the medulla oblongata encumbering normal physiology [1�4].
The objective of the National Upper Cervical Chiropractic Association (NUCCA) developed atlas correction procedure is restoration of misaligned spinal structures to the vertical axis or gravity line. Described as the �restoration principle,� realignment aims to reestablish a patient’s normal biomechanical relationship of the upper cervical spine to the vertical axis (gravity line). Restoration is characterized as being architecturally balanced, being capable of unrestricted range of motion, and allowing a significant decrease in gravitational stress [3]. The correction theoretically removes the cord distortion, created by an atlas misalignment or atlas subluxation complex (ASC), as specifically defined by NUCCA. Neurologic function is restored, specifically thought to be in the brain stem autonomic nuclei, which affect the cranial vascular system that includes Cerebrospinal Fluid (CSF) [3, 4].
The intracranial compliance index (ICCI) appears to be a more sensitive assessment of changes made in craniospinal biomechanical properties in symptomatic patients than the local hydrodynamic parameters of CSF flow velocities and cord displacement measurements [5]. Based on that information, previously observed relationships of increased intracranial compliance to marked reduction in migraine symptoms following atlas realignment provided incentive for using the ICCI as the study objective primary outcome.
ICCI affects the ability of the Central Nervous System (CNS) to accommodate physiologic volume fluctuations that occur, thereby avoiding ischemia of underlying neurologic structures [5, 6]. A state of high intracranial compliance enables any volume increase to occur in the intrathecal CNS space without causing an intracranial pressure increase that occurs primarily with arterial inflow during systole [5, 6]. Outflow occurs in the supine position via the internal jugular veins or when upright, via paraspinal or secondary venous drainage. This extensive venous plexus is valveless and anastomotic, allowing blood to flow in a retrograde direction, into the CNS through postural changes [7, 8]. Venous drainage plays an important role in regulating the intracranial fluid system [9]. Compliance appears to be functional and dependent on the free egress of blood via these extracranial venous drainage pathways [10].
Head and neck injury could create abnormal function of the spinal venous plexus that may impair spinal venous drainage, possibly because of autonomic dysfunction secondary to spinal cord ischemia [11]. This decreases accommodation of volume fluctuations within the cranium creating a state of decreased intracranial compliance.
Damadian and Chu describe return of a normal CSF outflow measured at mid-C-2, exhibiting a 28.6% reduction of the measured CSF pressure gradient in the patient where the atlas had been optimally realigned [12]. The patient reported freedom from symptoms (vertigo and vomiting when recumbent) consistent with the atlas remaining in alignment.
A hypertension study using the NUCCA intervention suggests a possible mechanism underlying the blood pressure decrease could be resultant from changes in cerebral circulation in relation to atlas vertebrae position [13]. Kumada et al. investigated a trigeminal-vascular mechanism in brain stem blood pressure control [14, 15]. Goadsby et al. have presented compelling evidence that migraine originates via a trigeminal-vascular system mediated through the brain stem and upper cervical spine [16�19]. Empirical observation reveals significant reduction of migraine patients’ headache disability after application of the atlas correction. Using migraine-diagnosed subjects seemed ideal for investigating proposed cerebral circulation changes following atlas realignment as originally theorized in the hypertension study conclusions and seemingly supported by a possible brain stem trigeminal-vascular connection. This would further advance a developing working pathophysiologic hypothesis of atlas misalignment.
Results from an initial case study demonstrated substantial increase in ICCI with decrease in migraine headache symptoms following the NUCCA atlas correction. A 62-year-old male with neurologist diagnosed chronic migraine volunteered for a before-after intervention case study. Using Phase Contrast-MRI (PC-MRI), changes in cerebral hemodynamic and hydrodynamic flow parameters were measured at baseline, 72 hours, and then four weeks after the atlas intervention. The same atlas correction procedure used in the hypertension study was followed [13]. 72 hours after study revealed a noteworthy change in the intracranial compliance index (ICCI), from 9.4 to 11.5, to 17.5 by week four, after intervention. Observed changes in venous outflow pulsatility and predominant secondary venous drainage in the supine position warranted additional investigation further inspiring a study of migraine subjects in this case series.
The possible effects of the atlas misalignment or ASC on venous drainage are unknown. Careful examination of intracranial compliance in relation to effects of an atlas misalignment intervention may provide insight into how the correction might influence migraine headache.
Using PC-MRI, this current study’s primary objective, and primary outcome, measured ICCI change from baseline to four and eight weeks following a NUCCA intervention in a cohort of neurologist selected migraine subjects. As observed in the case study, the hypothesis supposed that a subject’s ICCI would increase following the NUCCA intervention with a corresponding decrease in migraine symptoms. If present, any observed changes in venous pulsatility and drainage route were to be documented for further comparison. To monitor migraine symptoms response, the secondary outcomes included patient reported outcomes to measure any related change in Health Related Quality of Life (HRQoL), similarly used in migraine research. Throughout the study, subjects maintained headache diaries documenting the decrease (or increase) in the number of headache days, intensity, and medication used.
Conducting this observational case series, pilot study, allowed for additional investigation into aforementioned physiologic effects in further development of a working hypothesis into the pathophysiology of an atlas misalignment. Data required for estimation of statistically significant subject sample sizes and resolving procedural challenges will provide needed information for developing a refined protocol to conduct a blinded, placebo controlled migraine trial using the NUCCA correction intervention.
Methods
This research maintained compliance with the Helsinki Declaration for research on human subjects. The University of Calgary and Alberta Health Services Conjoint Health Research Ethics Board approved the study protocol and subject informed consent form, Ethics ID: E-24116. ClinicalTrials.gov assigned the number NCT01980927 after registration of this study (https://clinicaltrials.gov/ct2/show/NCT01980927).
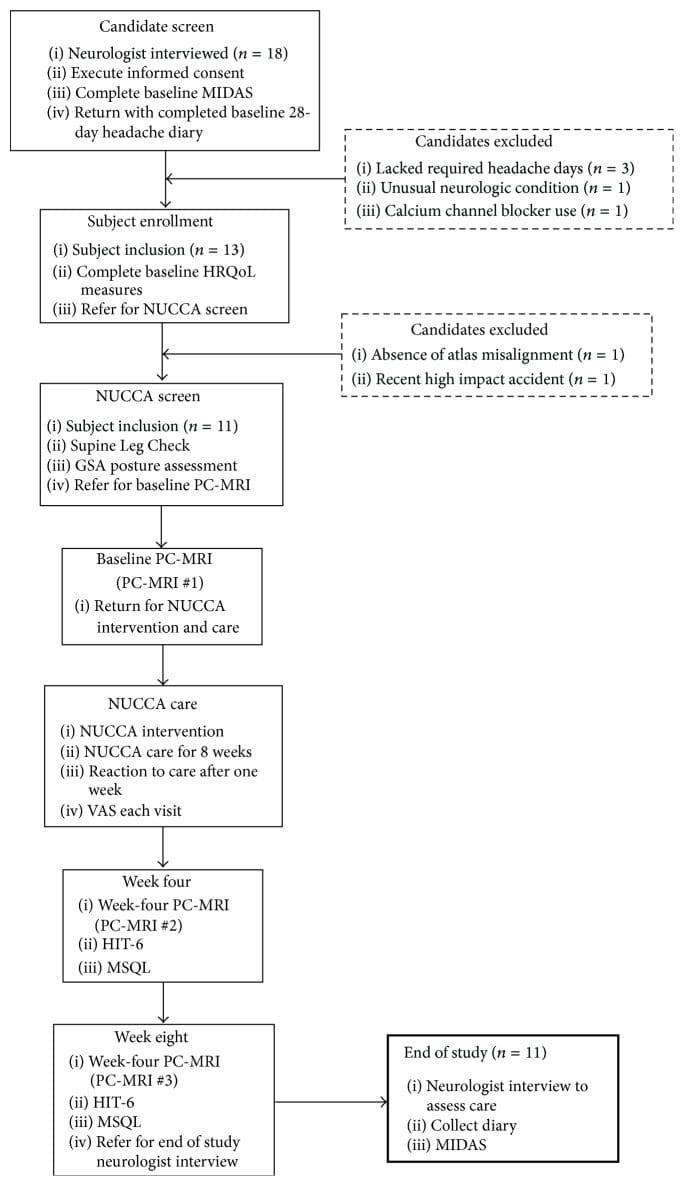
Subject recruitment and screening occurred at the Calgary Headache Assessment and Management Program (CHAMP), a neurology-based specialist referral clinic (see Figure 1, Table 1). CHAMP evaluates patients resistant to standard pharmacotherapy and medical treatment for migraine headache that no longer provides migraine symptom relief. Family and primary care physicians referred potential study subjects to CHAMP making advertising unnecessary.
Figure 1: Subject disposition and study flow (n = 11). GSA: Gravity Stress Analyzer. HIT-6: Headache Impact Test-6. HRQoL: Health Related Quality of Life. MIDAS: Migraine Disability Assessment Scale. MSQL: Migraine-Specific Quality of Life Measure. NUCCA: National Upper Cervical Chiropractic Association. PC-MRI: Phase Contrast Magnetic Resonance Imaging. VAS: Visual Analog Scale.
Table 1: Subject inclusion/exclusion criteria. Potential subjects, na�ve to upper cervical chiropractic care, demonstrated between ten and twenty-six headache days per month self-reported over the previous four months. Requisite was at least eight headache days per month, where intensity reached at least four, on a zero to ten Visual Analog Scale (VAS) pain scale.
Study inclusion required volunteers, between the ages of 21 and 65 years, that satisfy specific diagnostic criteria for migraine headache. A neurologist with several decades of migraine experience screened applicants utilizing the International Classification of Headache Disorders (ICHD-2) for study inclusion [20]. Potential subjects, na�ve to upper cervical chiropractic care, must have demonstrated through self-report between ten and twenty-six headache days per month over the previous four months. At least eight headache days per month had to reach an intensity of at least four on a zero to ten VAS pain scale, unless treated successfully with a migraine-specific medication. At least four separate headache episodes per month separated by at least a 24-hour pain-free interval were required.
Significant head or neck trauma occurring within one year prior to study entry excluded candidates. Further exclusion criteria included acute medication overuse, a history of claustrophobia, cardiovascular or cerebrovascular disease, or any CNS disorder other than migraine. Table 1 describes the complete inclusion and exclusion criteria considered. Using an experienced board certified neurologist to screen potential subjects while adhering to the ICHD-2 and guided by the inclusion/exclusion criteria, the exclusion of subjects with other sources of headache such as muscular tension and medication overuse rebound headache would increase the likelihood of successful subject recruitment.
Those meeting initial criteria signed informed consent and then completed a baseline Migraine Disability Assessment Scale (MIDAS). The MIDAS requires twelve weeks to demonstrate clinically significant change [21]. This allowed adequate time to pass to discern any possible changes. Over the next 28 days, candidates recorded a headache diary providing baseline data while confirming the number of headache days and intensity required for inclusion. After the four weeks, the diary check diagnostic substantiation permitted administration of remaining baseline HRQoL measures:
Migraine-Specific Quality of Life Measure (MSQL) [22],
Headache Impact Test-6 (HIT-6) [23],
Subject current global assessment of headache pain (VAS).
Referral to the NUCCA practitioner, to determine presence of atlas misalignment, confirmed need for intervention finalizing a subject’s study inclusion?exclusion. Absence of atlas misalignment indicators excluded candidates. After scheduling appointments for NUCCA intervention and care, qualified subjects obtained baseline PC-MRI measures. Figure 1 summarizes subject disposition throughout the study.
The initial NUCCA intervention required three consecutive visits: (1) Day One, atlas misalignment assessment, before-correction radiographs; (2) Day Two, NUCCA correction with after-correction assessment with radiographs; and (3) Day Three, after-correction reassessment. Follow-up care occurred weekly for four weeks, then every two weeks for the remainder of the study period. At each NUCCA visit, subjects completed a current assessment of headache pain (please rate your headache pain on average over the past week) using a straight edge and pencil in marking a 100?mm line (VAS). One week after the initial intervention, subjects completed a �Possible Reaction to Care� questionnaire. This assessment has past been used for successfully monitoring adverse events related to various upper cervical correction procedures [24].
At week four, PC-MRI data were obtained and subjects completed an MSQL and HIT-6. End of study PC-MRI data were collected at week eight followed by a neurologist exit interview. Here, subjects completed final MSQOL, HIT-6, MIDAS, and VAS outcomes and headache diaries were collected.
At the week-8 neurologist visit, two willing subjects were offered a long-term follow-up opportunity for a total study period of 24 weeks. This involved further NUCCA reassessment monthly for 16 weeks after completion of the initial 8-week study. The purpose of this follow-up was to help determine if headache improvement continued contingent upon maintenance of atlas alignment while observing for any long-term effect of NUCCA care on ICCI. Subjects desiring to participate signed a second informed consent for this phase of study and continued monthly NUCCA care. At the end of 24 weeks from the original atlas intervention, the fourth PC-MRI imaging study occurred. At the neurologist exit interview, final MSQOL, HIT-6, MIDAS, and VAS outcomes and headache diaries were collected.
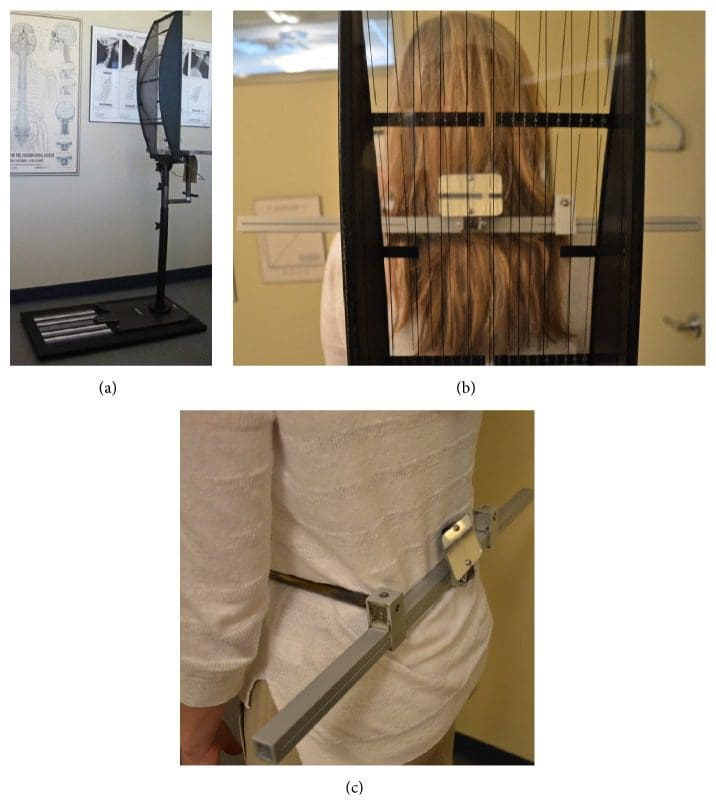
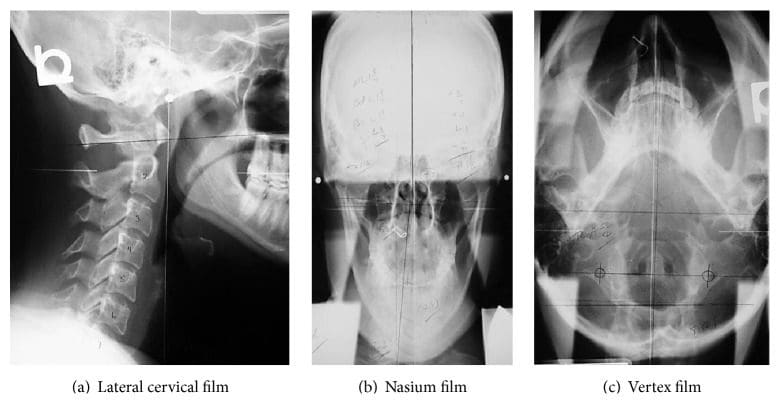
The same NUCCA procedure as previously reported was followed using the established protocol and standards of care developed through NUCCA Certification for assessment and atlas realignment or correction of the ASC (see Figures ?Figures22�5) [2, 13, 25]. Assessment for the ASC includes screening for functional leg-length inequality with the Supine Leg Check (SLC) and examination of postural symmetry using the Gravity Stress Analyzer (Upper Cervical Store, Inc., 1641 17 Avenue, Campbell River, BC, Canada V9W 4L5) (see Figures ?Figures22 and 3(a)�3(c)) [26�28]. If SLC and postural imbalances are detected, a three-view radiographic exam is indicated to determine the multidimensional orientation and degree of craniocervical misalignment [29, 30]. A thorough radiographic analysis provides information to determine a subject specific, optimal atlas correction strategy. The clinician locates anatomic landmarks from the three-view series, measuring structural and functional angles that have deviated from established orthogonal standards. The degree of misalignment and atlas orientation are then revealed in three dimensions (see Figures 4(a)�4(c)) [2, 29, 30]. Radiographic equipment alignment, reduction of collimator port size, high-speed film-screen combinations, special filters, specialized grids, and lead shielding minimize subject radiation exposure. For this study, average total measured Entrance Skin Exposure to subjects from the before-after-correction radiographic series was 352 millirads (3.52 millisieverts).
Figure 2: Supine Leg Check Screening Test (SLC). Observation of an apparent �short leg� indicates possible atlas misalignment. These appear even.
Figure 3: Gravity Stress Analyzer (GSA). (a) Device determines postural asymmetry as a further indicator of atlas misalignment. Positive findings in the SLC and GSA indicate need for NUCCA radiographic series. (b) Balanced patient with no postural asymmetry. (c) Hip calipers used to measure pelvis asymmetry.
Figure 4: NUCCA radiograph series. These films are used to determine atlas misalignment and developing a correction strategy. After-correction radiographs or postfilms ensure the best correction has been made for that subject.
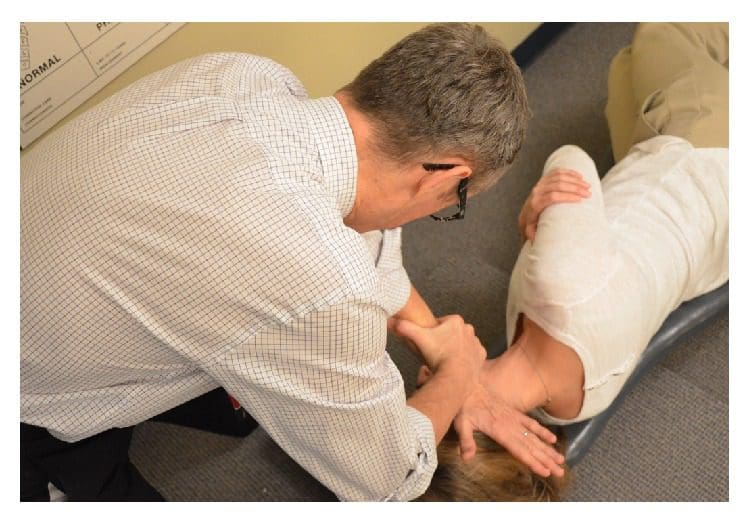
Figure 5: Making a NUCCA correction. The NUCCA practitioner delivers a triceps pull adjustment. The practitioner’s body and hands are aligned to deliver an atlas correction along an optimal force vector using information obtained from radiographs.
The NUCCA intervention involves a manual correction of the radiographically measured misalignment in the anatomical structure between the skull, atlas vertebra, and cervical spine. Utilizing biomechanical principles based on a lever system, the doctor develops a strategy for proper
subject positioning,
practitioner stance,
force vector to correct the atlas misalignment.
Subjects are placed on a side-posture table with the head specifically braced using a mastoid support system. Application of the predetermined controlled force vector for the correction realigns the skull to the atlas and neck to the vertical axis or center of gravity of the spine. These corrective forces are controlled in depth, direction, velocity, and amplitude, producing an accurate and precise reduction of the ASC.
Using the pisiform bone of the contact hand, the NUCCA practitioner contacts the atlas transverse process. The other hand encircles the wrist of the contact hand, to control the vector while maintaining the depth of force generated in application of the �triceps pull� procedure (see Figure 5) [3]. By understanding spinal biomechanics, the practitioner’s body and hands are aligned to produce an atlas correction along the optimal force vector. The controlled, nonthrusting force is applied along the predetermined reduction pathway. It is specific in its direction and depth to optimize the ASC reduction assuring no activation in the reactive forces of the neck muscles in response to the biomechanical change. It is understood that an optimal reduction of the misalignment promotes long-term maintenance and stability of spinal alignment.
Following a short rest period, an after-assessment procedure, identical to the initial evaluation, is performed. A postcorrection radiograph examination uses two views to verify return of the head and cervical spine into optimum orthogonal balance. Subjects are educated in ways to preserve their correction, thus preventing another misalignment.
Subsequent NUCCA visits were comprised of headache diary checks and a current assessment of headache pain (VAS). Leg length inequality and excessive postural asymmetry were used in determining the need for another atlas intervention. The objective for optimal improvement is for the subject to maintain the realignment for as long as possible, with the fewest number of atlas interventions.
In a PC-MRI sequence, contrast media are not used. PC-MRI methods collected two data sets with different amounts of flow sensitivity acquired by relating gradient pairs, which sequentially dephase and rephase spins during the sequence. The raw data from the two sets are subtracted to calculate a flow rate.
An on-site visit by the MRI Physicist provided training for the MRI Technologist and a data transfer procedure was established. Several practice scans and data transfers were performed to ensure data collection succeeded without challenges. A 1.5-tesla GE 360 Optima MR scanner (Milwaukee, WI) at the study imaging center (EFW Radiology, Calgary, Alberta, Canada) was used in imaging and data collection. A 12-element phased array head coil, 3D magnetization-prepared rapid-acquisition gradient echo (MP-RAGE) sequence was used in anatomy scans. Flow sensitive data were acquired using a parallel acquisition technique (iPAT), acceleration factor 2.
To measure blood flow to and from the skull base, two retrospectively gated, velocity-encoded cine-phase-contrast scans were performed as determined by individual heart rate, collecting thirty-two images over a cardiac cycle. A high-velocity encoding (70?cm/s) quantified high-velocity blood flow perpendicular to the vessels at the C-2 vertebra level includes the internal carotid arteries (ICA), vertebral arteries (VA), and internal jugular veins (IJV). Secondary venous flow data of vertebral veins (VV), epidural veins (EV), and deep cervical veins (DCV) were acquired at the same height using a low-velocity encoding (7�9?cm/s) sequence.
Subject data were identified by Subject Study ID and imaging study date. The study neuroradiologist reviewed MR-RAGE sequences to rule out exclusionary pathologic conditions. Subject identifiers were then removed and assigned a coded ID permitting transfer via a secured tunnel IP protocol to the physicist for analysis. Using proprietary software volumetric blood, Cerebrospinal Fluid (CSF) flow rate waveforms and derived parameters were determined (MRICP version 1.4.35 Alperin Noninvasive Diagnostics, Miami, FL).
Using the pulsatility-based segmentation of lumens, time-dependent volumetric flow rates were calculated by integrating the flow velocities inside the luminal cross-sectional areas over all thirty-two images. Mean flow rates were obtained for the cervical arteries, primary venous drainage, and secondary venous drainage pathways. Total cerebral blood flow was obtained by summation of these mean flow rates.
A simple definition of compliance is a ratio of volume and pressure changes. Intracranial compliance is calculated from the ratio of the maximal (systolic) intracranial volume change (ICVC) and pressure fluctuations during the cardiac cycle (PTP-PG). Change in ICVC is obtained from momentary differences between volumes of blood and CSF entering and exiting the cranium [5, 31]. Pressure change during the cardiac cycle is derived from the change in the CSF pressure gradient, which is calculated from the velocity-encoded MR images of the CSF flow, using the Navier-Stokes relationship between derivatives of velocities and the pressure gradient [5, 32]. An intracranial compliance index (ICCI) is calculated from the ratio of ICVC and pressure changes [5, 31�33].
Statistical analysis considered several elements. ICCI data analysis involved a one-sample Kolmogorov-Smirnov test revealing a lack of normal distribution in the ICCI data, which were therefore described using the median and interquartile range (IQR). Differences between baseline and follow-up were to be examined using a paired t-test.
NUCCA assessments data were described using mean, median, and interquartile range (IQR). Differences between baseline and follow-up were examined using a paired t-test.
Depending on the outcome measure, baseline, week four, week eight, and week twelve (MIDAS only) follow-up values were described using the mean and standard deviation. MIDAS data collected at initial neurologist screening had one follow-up score at the end of twelve weeks.
Differences from baseline to each follow-up visit were tested using a paired t-test. This resulted in numerous p values from two follow-up visits for each outcome except the MIDAS. Since one purpose of this pilot is to provide estimates for future research, it was important to describe where differences occurred, rather than to use a one-way ANOVA to arrive at a single p value for each measure. The concern with such multiple comparisons is the increase in Type I error rate.
To analyze the VAS data, each subject scores were examined individually and then with a linear regression line that adequately fits the data. Use of a multilevel regression model with both random intercepts and random slope provided an individual regression line fitted for each patient. This was tested against a random intercept-only model, which fits a linear regression line with a common slope for all subjects, while intercept terms are allowed to vary. The random coefficient model was adopted, as there was no evidence that random slopes significantly improved the fit to the data (using a likelihood ratio statistic). To illustrate the variation in the intercepts but not in the slope, the individual regression lines were graphed for each patient with an imposed average regression line on top.
Results
From initial neurologist screening, eighteen volunteers were eligible for inclusion. After completion of baseline headache diaries, five candidates did not meet inclusion criteria. Three lacked the required headache days on baseline diaries to be included, one had unusual neurological symptoms with persistent unilateral numbness, and another was taking a calcium channel blocker. The NUCCA practitioner found two candidates ineligible: one lacking an atlas misalignment and the second with a Wolff-Parkinson-White condition and severe postural distortion (39�) with recent involvement in a severe high impact motor vehicle accident with whiplash (see Figure 1).
Eleven subjects, eight females and three males, average age forty-one years (range 21�61 years), qualified for inclusion. Six subjects presented chronic migraine, reporting fifteen or more headache days a month, with a total eleven-subject mean of 14.5 headache days a month. Migraine symptom duration ranged from two to thirty-five years (mean twenty-three years). All medications were maintained unchanged for the study duration to include their migraine prophylaxis regimens as prescribed.
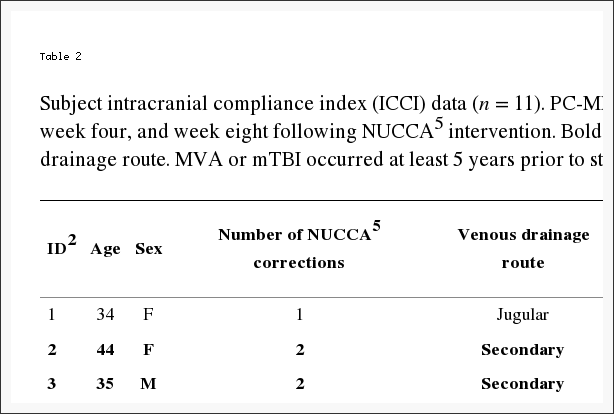
Per exclusion criteria, no subjects included received a diagnosis of headache attributed to traumatic injury to the head and neck, concussion, or persistent headache attributed to whiplash. Nine subjects reported a very remote past history, greater than five years or more (average of nine years) prior to neurologist screen. This included sports-related head injuries, concussion, and/or whiplash. Two subjects indicated no prior head or neck injury (see Table 2).
Table 2: Subject intracranial compliance index (ICCI) data (n = 11). PC-MRI6 acquired ICCI1 data reported at baseline, week four, and week eight following NUCCA5 intervention. Bolded rows signify subject with secondary venous drainage route. MVA or mTBI occurred at least 5 years prior to study inclusion, average 10 years.
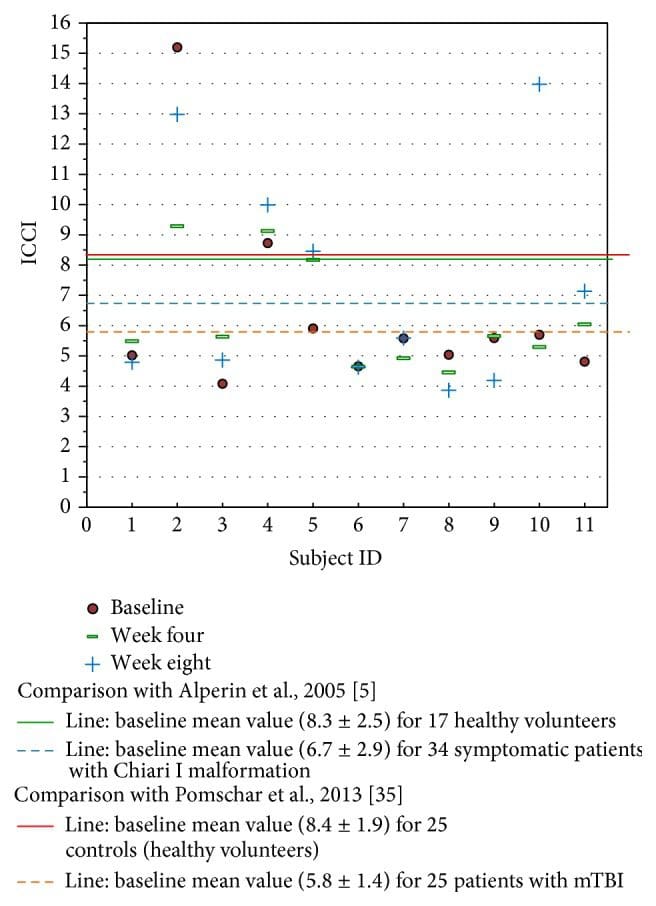
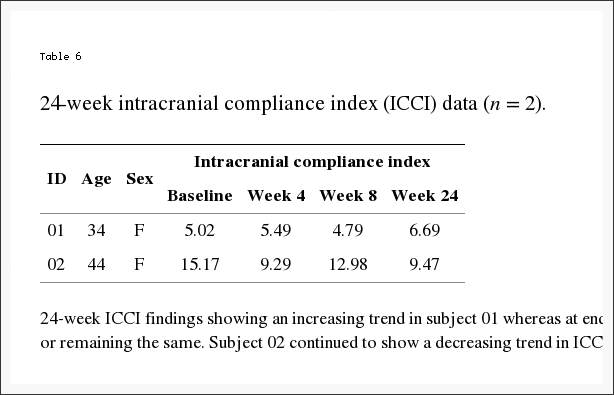
Individually, five subjects demonstrated an increase in ICCI, three subject’s values remained essentially the same, and three showed a decrease from baseline to end of study measurements. Overall changes in intracranial compliance are seen in Table 2 and Figure 8. The median (IQR) values of ICCI were 5.6 (4.8, 5.9) at baseline, 5.6 (4.9, 8.2) at week four, and 5.6 (4.6, 10.0) at week eight. Differences were not statistically different. The mean difference between baseline and week four was ?0.14 (95% CI ?1.56, 1.28), p = 0.834, and between baseline and week eight was 0.93 (95% CI ?0.99, 2.84), p = 0.307. These two subject’s 24-week ICCI study results are seen in Table 6. Subject 01 displayed an increasing trend in ICCI from 5.02 at baseline to 6.69 at week 24, whereas at week 8, results were interpreted as consistent or remaining the same. Subject 02 demonstrated a decreasing trend in ICCI from baseline of 15.17 to 9.47 at week 24.
Figure 8: Study ICCI data compared to previously reported data in the literature. The MRI time values are fixed at baseline, week 4, and week 8 after intervention. This study’s baseline values fall similar to the data reported by Pomschar on subjects presenting only with mTBI.
Table 6: 24-week ICCI findings showing an increasing trend in subject 01 whereas at end of study (week 8), results were interpreted as consistent or remaining the same. Subject 02 continued to show a decreasing trend in ICCI.
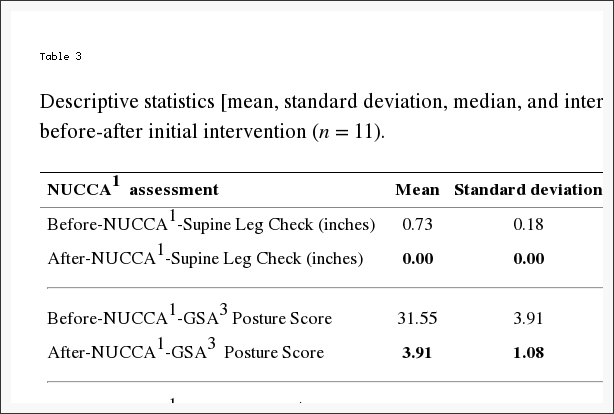
Table 3 reports changes in NUCCA assessments. The mean difference from before to after the intervention is as follows: (1) SLC: 0.73 inches, 95% CI (0.61, 0.84) (p < 0.001); (2) GSA: 28.36 scale points, 95% CI (26.01, 30.72) (p < 0.001); (3) Atlas Laterality: 2.36 degrees, 95% CI (1.68, 3.05) (p < 0.001); and (4) Atlas Rotation: 2.00 degrees, 95% CI (1.12, 2.88) (p < 0.001). This would indicate that a probable change occurred following the atlas intervention as based on subject assessment.
Table 3: Descriptive statistics [mean, standard deviation, median, and interquartile range (IQR2)] of NUCCA1 assessments before-after initial intervention (n = 11).
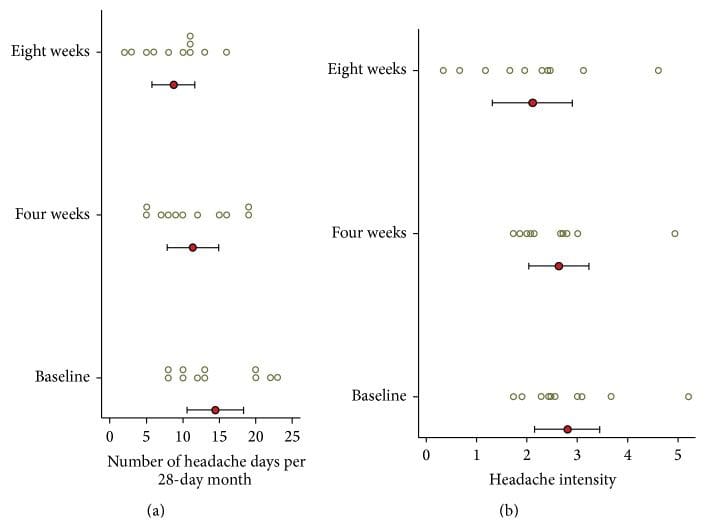
Headache diary results are reported in Table 4 and Figure 6. At baseline subjects had mean 14.5 (SD = 5.7) headache days per 28-day month. During the first month following NUCCA correction, mean headache days per month decreased by 3.1 days from baseline, 95% CI (0.19, 6.0), p = 0.039, to 11.4. During the second month headache days decreased by 5.7 days from baseline, 95% CI (2.0, 9.4), p = 0.006, to 8.7 days. At week eight, six of the eleven subjects had a reduction of >30% in headache days per month. Over 24 weeks, subject 01 reported essentially no change in headache days while subject 02 had a reduction of one headache day a month from study baseline of seven to end of study reports of six days.
Figure 6: Headache days and headache pain intensity from diary (n = 11). (a) Number of headache days per month. (b) Average headache intensity (on headache days). Circle indicates the mean and the bar indicates the 95% CI. Circles are individual subject scores. A significant decrease in headache days per month was noticed at four weeks, almost doubling at eight weeks. Four subjects (#4, 5, 7, and 8) exhibited a greater than 20% decrease in headache intensity. Concurrent medication use may explain the small decrease in headache intensity.
At baseline, mean headache intensity on days with headache, on a scale of zero to ten, was 2.8 (SD = 0.96). Mean headache intensity showed no statistically significant change at four (p = 0.604) and eight (p = 0.158) weeks. Four subjects (#4, 5, 7, and 8) exhibited a greater than 20% decrease in headache intensity.
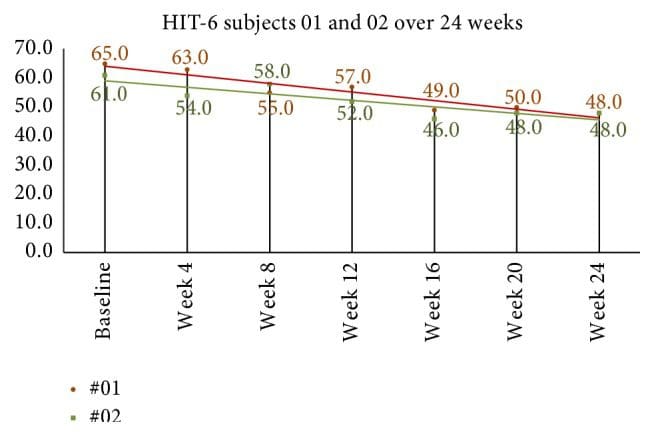
Quality of life and headache disability measures are seen in Table 4. The mean HIT-6 score at baseline was 64.2 (SD = 3.8). At week four after NUCCA correction, mean decrease in scores was 8.9, 95% CI (4.7, 13.1), p = 0.001. Week-eight scores, compared to baseline, revealed mean decrease by 10.4, 95% CI (6.8, 13.9), p = 0.001. In the 24-week group, subject 01 showed a decrease of 10 points from 58 at week 8 to 48 at week 24 while subject 02 decreased 7 points from 55 at week 8 to 48 at week 24 (see Figure 9).
Figure 9: 24-week HIT-6 scores in long-term follow-up subjects. Monthly scores continued to decrease after week 8, end of first study. Based on Smelt et al. criteria, it can be interpreted that a within-person minimally important change occurred between week 8 and week 24. HIT-6: Headache Impact Test-6.
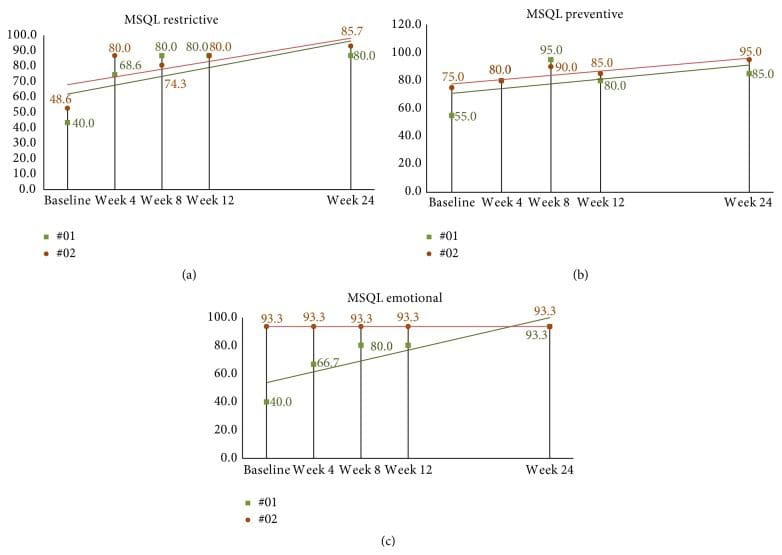
MSQL mean baseline score was 38.4 (SD = 17.4). At week four after correction, mean scores for all eleven subjects increased (improved) by 30.7, 95% CI (22.1, 39.2), p < 0.001. By week eight, end of study, mean MSQL scores had increased from baseline by 35.1, 95% CI (23.1, 50.0), p < 0.001, to 73.5. The follow-up subjects continued to show some improvement with increasing scores; however, many scores plateaued remaining the same since week 8 (see Figures 10(a)�10(c)).
Figure 10: ((a)�(c)) 24-week MSQL scores in long-term follow-up subjects. (a) Subject 01 has essentially plateaued after week 8 throughout to end of the second study. Subject 02 shows scores increasing over time demonstrating minimally important differences based on Cole et al. criteria by week 24. (b) Subject scores seem to peak by week 8 with both subjects showing similar scores reported at week 24. (c) Subject 2 scores remain consistent throughout the study while subject 01 shows steady improvement from baseline to the end of week 24. MSQL: Migraine-Specific Quality of Life Measure.
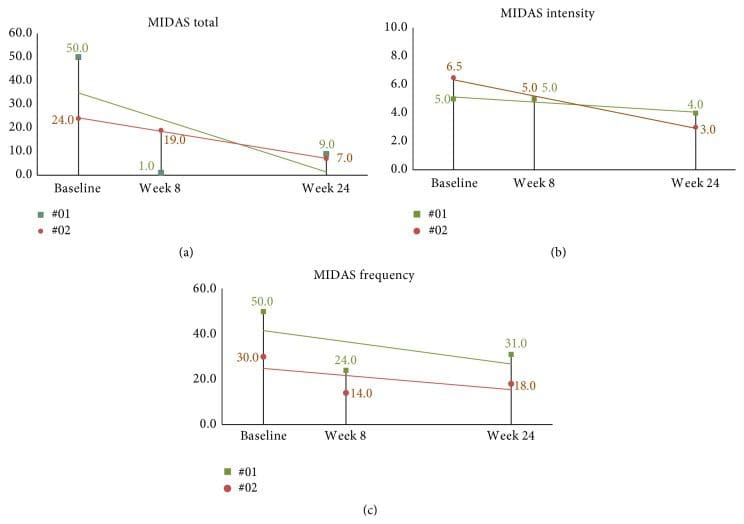
Mean MIDAS score at baseline was 46.7 (SD = 27.7). At two months after NUCCA correction (three months following baseline), the mean decrease in subject’s MIDAS scores was 32.1, 95% CI (13.2, 51.0), p = 0.004. The follow-up subjects continued to show improvement with decreasing scores with intensity showing minimal improvement (see Figures 11(a)�11(c)).
Figure 11: 24-week MIDAS scores in long-term follow-up subjects. (a) Total MIDAS scores continued a decreasing trend over the 24-week study period. (b) Intensity scores continued improvement. (c) While 24-week frequency was higher than at week 8, improvement is observed when compared to baseline. MIDAS: Migraine Disability Assessment Scale.
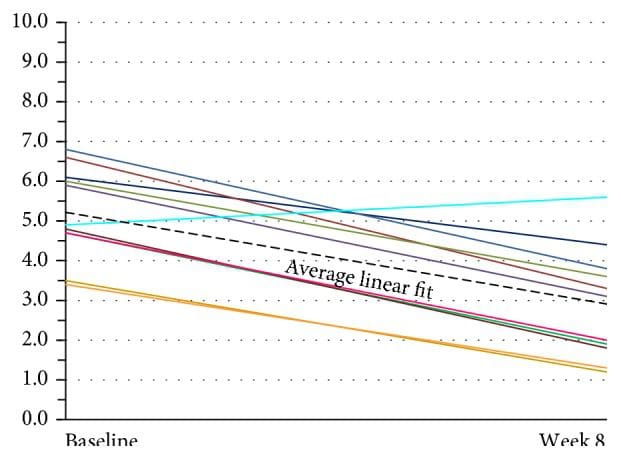
Assessment of current headache pain from VAS scale data is seen in Figure 7. The multilevel linear regression model showed evidence of a random effect for the intercept (p < 0.001) but not for the slope (p = 0.916). Thus, the adopted random intercept model estimated a different intercept for each patient but a common slope. The estimated slope of this line was ?0.044, 95% CI (?0.055, ?0.0326), p < 0.001, indicating that there was a significant decrease in the VAS score of 0.44 per 10 days after baseline (p < 0.001). The mean baseline score was 5.34, 95% CI (4.47, 6.22). The random effects analysis showed substantial variation in the baseline score (SD = 1.09). As the random intercepts are normally distributed, this indicates that 95% of such intercepts lie between 3.16 and 7.52 providing evidence of substantial variation in the baseline values across patients. VAS scores continued showing improvement in the 24-week two-subject follow-up group (see Figure 12).
Figure 7: Subject global assessment of headache (VAS) (n = 11). There was substantial variation in baseline scores across these patients. The lines show individual linear fit for each of eleven patients. The thick dotted black line represents the average linear fit across all eleven patients. VAS: Visual Analog Scale.
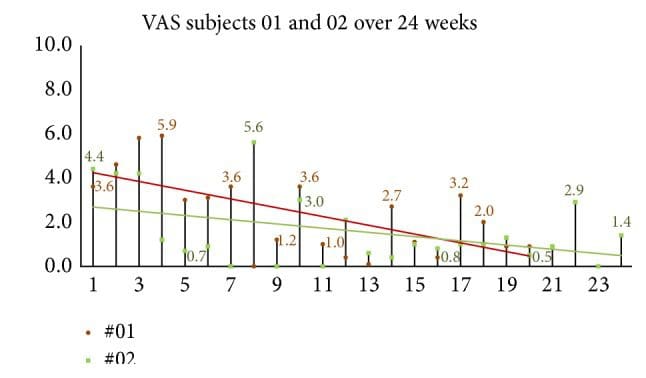
Figure 12: 24-week follow-up group global assessment of headache (VAS). When subjects were queried, �please rate your headache pain on average over the past week� VAS scores continued showing improvement in the 24-week two-subject follow-up group.
The most obvious reaction to the NUCCA intervention and care reported by ten subjects was mild neck discomfort, rated an average of three out of ten on pain assessment. In six subjects, pain began more than twenty-four hours after the atlas correction, lasting more than twenty-four hours. No subject reported any significant effect on their daily activities. All subjects reported satisfaction with NUCCA care after one week, median score, ten, on a zero to ten rating scale.
Dr. Alex Jimenez’s Insight
“I’ve been experiencing migraine headaches for several years now. Is there a reason for my head pain? What can I do to decrease or get rid of my symptoms?”�Migraine headaches are believed to be a complex form of head pain, however, the reason for them is much the same as any other type of headache. A traumatic injury to the cervical spine, such as that of whiplash from an automobile accident or a sports injury, can cause a misalignment in the neck and upper back, which may lead to migraine. An improper posture can also cause neck issues which could lead to head and neck pain. A healthcare professional who specializes in spinal health issues can diagnose the source of your migraine headaches. Furthermore, a qualified and experienced specialist can perform spinal adjustments as well as manual manipulations to help correct any misalignments of the spine which could be causing the symptoms. The following article summarizes a case study based on the improvement of symptoms after atlas vertebrae realignment in participants with migraine.
Discussion
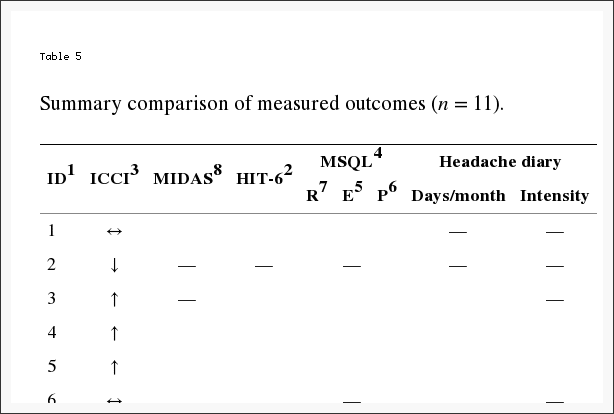
In this limited cohort of eleven migraine subjects, there was no statistically significant change in ICCI (primary outcome) after the NUCCA intervention. However, a significant change in HRQoL secondary outcomes did occur as summarized in Table 5. The consistency in the magnitude and direction of improvement across these HRQoL measures indicates confidence in enhancement of headache health over the two-month study following the 28-day baseline period.
Table 5: Summary Comparison of Measured Outcomes
Based on the case study results, this investigation hypothesized a significant increase in ICCI after the atlas intervention which was not observed. Use of PC-MRI allows quantification of the dynamic relationship between arterial inflow, venous outflow, and CSF flow between the cranium and the spinal canal [33]. Intracranial compliance index (ICCI) measures the brain’s ability to respond to incoming arterial blood during systole. Interpretation of this dynamic flow is represented by a monoexponential relationship existing between CSF volume and CSF pressure. With increased or higher intracranial compliance, also defined as good compensatory reserve, the incoming arterial blood can be accommodated by the intracranial contents with a smaller change in intracranial pressure. While a change in intracranial volume or pressure could occur, based on the exponential nature of the volume-pressure relationship, a change in after-intervention ICCI may not be realized. An advanced analysis of the MRI data and further study are required for pinpointing practical quantifiable parameters to use as an objective outcome sensitive for documenting a physiologic change following atlas correction.
Koerte et al. reports of chronic migraine patients demonstrate a significantly higher relative secondary venous drainage (paraspinal plexus) in the supine position when compared to age- and gender-matched controls [34]. Four study subjects exhibited a secondary venous drainage with three of those subjects demonstrating notable increase in compliance after intervention. The significance is unknown without further study. Similarly, Pomschar et al. reported that subjects with mild traumatic brain injury (mTBI) demonstrate an increased drainage through the secondary venous paraspinal route [35]. The mean intracranial compliance index appears significantly lower in the mTBI cohort when compared to controls.
Some perspective may be gained in comparison of this study’s ICCI data to previously reported normal subjects and those with mTBI seen in Figure 8 [5, 35]. Limited by the small number of subjects studied, the significance these study’s findings may have in relation to Pomschar et al. remains unknown, offering only speculation of possibilities for future exploration. This is further complicated by the inconsistent ICCI change observed in the two subjects followed for 24 weeks. Subject two with a secondary drainage pattern exhibited a decrease in ICCI following intervention. A larger placebo controlled trial with a statistically significant subject sample size could possibly demonstrate a definitive objectively measured physiologic change after application of the NUCCA correction procedure.
HRQoL measures are used clinically to assess the effectiveness of a treatment strategy to decrease pain and disability related to migraine headache. It is expected that an effective treatment improves patient perceived pain and disability measured by these instruments. All HRQoL measures in this study demonstrated significant and substantial improvement by week four following the NUCCA intervention. From week four to week eight only small improvements were noted. Again, only small improvements were noted in the two subjects followed for 24 weeks. While this study was not intended to demonstrate causation from the NUCCA intervention, the HRQoL results create compelling interest for further study.
From the headache diary, a significant decrease in headache days per month was noticed at four weeks, almost doubling at eight weeks. However, significant differences in headache intensity over time were not discernable from this diary data (see Figure 5). While the number of headaches decreased, subjects still used medication to maintain headache intensity at tolerable levels; hence, it is supposed that a statistically significant difference in headache intensity could not be determined. Consistency in the headache day numbers occurring in week 8 in the follow-up subjects could guide future study focus in determining when maximum improvement occurs to help in establishing a NUCCA standard of migraine care.
Clinically relevant change in the HIT-6 is important for completely understanding observed outcomes. A clinically meaningful change for an individual patient has been defined by the HIT-6 user guide as ?5 [36]. Coeytaux et al., using four different analysis methods, suggest that a between-group difference in HIT-6 scores of 2.3 units over time may be considered clinically significant [37]. Smelt et al. studied primary care migraine patient populations in developing suggested recommendations using HIT-6 score changes for clinical care and research [38]. Dependent on consequences resulting from false positives or negatives, within-person minimally important change (MIC) using a �mean change approach� was estimated to be 2.5 points. When using the �receiver operating characteristic (ROC) curve analysis� a 6-point change is needed. Recommended between-group minimally important difference (MID) is 1.5 [38].
Using the �mean change approach,� all subjects but one reported a change (decrease) greater than ?2.5. The �ROC analyses� also demonstrated improvement by all subjects but one. This �one subject� was a different person in each comparison analysis. Based on Smelt et al. criteria, the follow-up subjects continued to demonstrate within-person minimally important improvement as seen in Figure 10.
All subjects but two showed improvement on the MIDAS score between baseline and three-month results. The magnitude of the change was proportional to the baseline MIDAS score, with all subjects but three reporting an overall fifty percent or greater change. The follow-up subjects continued to show improvement as seen in continued decrease in scores by week 24; see Figures 11(a)�11(c).
Use of the HIT-6 and MIDAS together as a clinical outcome may provide a more complete assessment of headache-related disability factors [39]. The differences between the two scales can predict disability from headache pain intensity and headache frequency, by providing more information on factors related to the reported changes than either outcome used alone. While the MIDAS appears to change more by headache frequency, headache intensity seems to affect HIT-6 score more than the MIDAS [39].
How migraine headache affects and limits patient perceived daily functioning is reported by the MSQL v. 2.1, across three 3 domains: role restrictive (MSQL-R), role preventive (MSQL-P), and emotional functioning (MSQL-E). An increase in scores indicates improvement in these areas with values ranging from 0 (poor) to 100 (best).
MSQL scales reliability evaluation by Bagley et al. report results to be moderately to highly correlated with HIT-6 (r = ?0.60 to ?0.71) [40]. Study by Cole et al. reports minimally important differences (MID) clinical change for each domain: MSQL-R = 3.2, MSQL-P = 4.6, and MSQL-E = 7.5 [41]. Results from the topiramate study report individual minimally important clinical (MIC) change: MSQL-R = 10.9, MSQL-P = 8.3, and MSQL-E = 12.2 [42].
All subjects except one experienced an individual minimally important clinical change for MSQL-R of greater than 10.9 by the week-eight follow-up in MSQL-R. All but two subjects reported changes of more than 12.2 points in MSQL-E. Improvement in MSQL-P scores increased by ten points or more in all subjects.
Regression analysis of VAS ratings over time showed a significant linear improvement over the 3-month period. There was substantial variation in baseline scores across these patients. Little to no variation was observed in the rate of improvement. This trend appears to be the same in the subjects studied for 24 weeks as seen in Figure 12.
Many studies using pharmaceutical intervention have shown a substantial placebo effect in patients from migrainous populations [43]. Determining possible migraine improvement over six months, using another intervention as well as no intervention, is important for any comparison of results. The investigation into placebo effects generally accepts that placebo interventions do provide symptomatic relief but do not modify pathophysiologic processes underlying the condition [44]. Objective MRI measures may help in revealing such a placebo effect by demonstrating a change in physiologic measurements of flow parameters occurring after a placebo intervention.
Use of a three-tesla magnet for MRI data collection would increase the reliability of the measurements by increasing the amount of data used to make the flow and ICCI calculations. This is one of the first investigations using change in ICCI as an outcome in evaluating an intervention. This creates challenges in interpretation of MRI acquired data to base conclusions or further hypothesis development. Variability in relationships between blood flow to and from the brain, CSF flow, and heart rate of these subject-specific parameters has been reported [45]. Variations observed in a small three-subject repeated measures study have led to conclusions that information gathered from individual cases be interpreted with caution [46].
The literature further reports in larger studies significant reliability in collecting these MRI acquired volumetric flow data. Wentland et al. reported that measurements of CSF velocities in human volunteers and of sinusoidally fluctuating phantom velocities did not differ significantly between two MRI techniques used [47]. Koerte et al. studied two cohorts of subjects imaged in two separate facilities with different equipment. They reported that intraclass correlation coefficients (ICC) demonstrated a high intra- and interrater reliability of PC-MRI volumetric flow rate measurements remaining independent of equipment used and skill-level of the operator [48]. While anatomic variation exists between subjects, it has not prevented studies of larger patient populations in describing possible �normal� outflow parameters [49, 50].
Being based solely on patient subjective perceptions, there are limitations in using patient reported outcomes [51]. Any aspect affecting a subject’s perception in their quality of life is likely to influence the outcome of any assessment used. Lack of outcome specificity in reporting symptoms, emotions, and disability also limits interpretation of results [51].
Imaging and MRI data analysis costs precluded use of a control group, limiting any generalizability of these results. A larger sample size would allow for conclusions based on statistical power and reduced Type I error. Interpretation of any significance in these results, while revealing possible trends, remains speculation at best. The big unknown persists in the likelihood that these changes are related to the intervention or to some other effect unknown to the investigators. These results do add to the body of knowledge of previously unreported possible hemodynamic and hydrodynamic changes after a NUCCA intervention, as well as changes in migraine HRQoL patient reported outcomes as observed in this cohort.
The values of collected data and analyses are providing information required for estimation of statistically significant subject sample sizes in further study. Resolved procedural challenges from conducting the pilot allow for a highly refined protocol to successfully accomplish this task.
In this study, the lack of robust increase in compliance may be understood by the logarithmic and dynamic nature of intracranial hemodynamic and hydrodynamic flow, allowing individual components comprising compliance to change while overall it did not. An effective intervention should improve subject perceived pain and disability related to migraine headache as measured by these HRQoL instruments used. These study results suggest that the atlas realignment intervention may be associated with reduction in migraine frequency, marked improvement in quality of life yielding significant reduction in headache-related disability as observed in this cohort. The improvement in HRQoL outcomes creates compelling interest for further study, to confirm these findings, especially with a larger subject pool and a placebo group.
Acknowledgments
The authors acknowledge Dr. Noam Alperin, Alperin Diagnostics, Inc., Miami, FL; Kathy Waters, Study Coordinator, and Dr. Jordan Ausmus, Radiography Coordinator, Britannia Clinic, Calgary, AB; Sue Curtis, MRI Technologist, Elliot Fong Wallace Radiology, Calgary, AB; and Brenda Kelly-Besler, RN, Research Coordinator, Calgary Headache Assessment and Management Program (CHAMP), Calgary, AB. Financial support is provided by (1) Hecht Foundation, Vancouver, BC; (2) Tao Foundation, Calgary, AB; (3) Ralph R. Gregory Memorial Foundation (Canada), Calgary, AB; and (4) Upper Cervical Research Foundation (UCRF), Minneapolis, MN.
Abbreviations
ASC: Atlas subluxation complex
CHAMP: Calgary Headache Assessment and Management Program
CSF: Cerebrospinal Fluid
GSA: Gravity Stress Analyzer
HIT-6: Headache Impact Test-6
HRQoL: Health Related Quality of Life
ICCI: Intracranial compliance index
ICVC: Intracranial volume change
IQR: Interquartile range
MIDAS: Migraine Disability Assessment Scale
MSQL: Migraine-Specific Quality of Life Measure
MSQL-E: Migraine-Specific Quality of Life Measure-Emotional
MSQL-P: Migraine-Specific Quality of Life Measure-Physical
MSQL-R: Migraine-Specific Quality of Life Measure-Restrictive
NUCCA: National Upper Cervical Chiropractic Association
PC-MRI: Phase Contrast Magnetic Resonance Imaging
SLC: Supine Leg Check
VAS: Visual Analog Scale.
Conflict of Interests
The authors declare that there are no financial or any other competing interests regarding the publication of this paper.
Authors’ Contribution
H. Charles Woodfield III conceived the study, was instrumental in its design, helped in coordination, and helped to draft the paper: introduction, study methods, results, discussion, and conclusion. D. Gordon Hasick screened subjects for study inclusion/exclusion, provided NUCCA interventions, and monitored all subjects on follow-up. He participated in study design and subject coordination, helping to draft the Introduction, NUCCA Methods, and Discussion of the paper. Werner J. Becker screened subjects for study inclusion/exclusion, participated in study design and coordination, and helped to draft the paper: study methods, results and discussion, and conclusion. Marianne S. Rose performed statistical analysis on study data and helped to draft the paper: statistical methods, results, and discussion. James N. Scott participated in study design, served as the imaging consultant reviewing scans for pathology, and helped to draft the paper: PC-MRI methods, results, and discussion. All authors read and approved the final paper.
In conclusion, the case study regarding the improvement of migraine headache symptoms following atlas vertebrae realignment demonstrated an increase in the primary outcome, however, the average results of the research study also demonstrated no statistical significance. Altogether, the case study concluded that patients who received atlas vertebrae realignment treatment experienced considerable improvement in symptoms with decreased headache days. Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Neck Pain
Neck pain is a common complaint which can result due to a variety of injuries and/or conditions. According to statistics, automobile accident injuries and whiplash injuries are some of the most prevalent causes for neck pain among the general population. During an auto accident, the sudden impact from the incident can cause the head and neck to jolt abruptly back-and-forth in any direction, damaging the complex structures surrounding the cervical spine. Trauma to the tendons and ligaments, as well as that of other tissues in the neck, can cause neck pain and radiating symptoms throughout the human body.
1. Magoun H. W. Caudal and cephalic influences of the brain stem reticular formation. Physiological Reviews. 1950;30(4):459�474. [PubMed]
2. Gregory R. Manual of Upper Cervical Analysis. Monroe, Mich, USA: National Upper Cervical Chiropractic Association; 1971.
3. Thomas M., editor. NUCCA Protocols and Perspectives. 1st. Monroe, Mich, USA: National Upper Cervical Chiropractic Association; 2002.
4. Grostic J. D. Dentate ligament-cord distortion hypothesis. Chiropractic Research Journal. 1988;1(1):47�55.
5. Alperin N., Sivaramakrishnan A., Lichtor T. Magnetic resonance imaging-based measurements of cerebrospinal fluid and blood flow as indicators of intracranial compliance in patients with Chiari malformation. Journal of Neurosurgery. 2005;103(1):46�52. doi: 10.3171/jns.2005.103.1.0046. [PubMed][Cross Ref]
6. Czosnyka M., Pickard J. D. Monitoring and interpretation of intracranial pressure. Journal of Neurology, Neurosurgery and Psychiatry. 2004;75(6):813�821. doi: 10.1136/jnnp.2003.033126. [PMC free article][PubMed][Cross Ref]
7. Tobinick E., Vega C. P. The cerebrospinal venous system: anatomy, physiology, and clinical implications. MedGenMed: Medscape General Medicine. 2006;8(1, article 153) [PubMed]
8. Eckenhoff J. E. The physiologic significance of the vertebral venous plexus. Surgery Gynecology and Obstetrics. 1970;131(1):72�78. [PubMed]
9. Beggs C. B. Venous hemodynamics in neurological disorders: an analytical review with hydrodynamic analysis. BMC Medicine. 2013;11, article 142 doi: 10.1186/1741-7015-11-142. [PMC free article][PubMed][Cross Ref]
10. Beggs C. B. Cerebral venous outflow and cerebrospinal fluid dynamics. Veins and Lymphatics. 2014;3(3):81�88. doi: 10.4081/vl.2014.1867. [Cross Ref]
11. Cassar-Pullicino V. N., Colhoun E., McLelland M., McCall I. W., El Masry W. Hemodynamic alterations in the paravertebral venous plexus after spinal injury. Radiology. 1995;197(3):659�663. doi: 10.1148/radiology.197.3.7480735. [PubMed][Cross Ref]
12. Damadian R. V., Chu D. The possible role of cranio-cervical trauma and abnormal CSF hydrodynamics in the genesis of multiple sclerosis. Physiological Chemistry and Physics and Medical NMR. 2011;41(1):1�17. [PubMed]
13. Bakris G., Dickholtz M., Meyer P. M., et al. Atlas vertebra realignment and achievement of arterial pressure goal in hypertensive patients: a pilot study. Journal of Human Hypertension. 2007;21(5):347�352. doi: 10.1038/sj.jhh.1002133. [PubMed][Cross Ref]
14. Kumada M., Dampney R. A. L., Reis D. J. The trigeminal depressor response: a cardiovascular reflex originating from the trigeminal system. Brain Research. 1975;92(3):485�489. doi: 10.1016/0006-8993(75)90335-2. [PubMed][Cross Ref]
15. Kumada M., Dampney R. A. L., Whitnall M. H., Reis D. J. Hemodynamic similarities between the trigeminal and aortic vasodepressor responses. The American Journal of Physiology�Heart and Circulatory Physiology. 1978;234(1):H67�H73. [PubMed]
16. Goadsby P. J., Edvinsson L. The trigeminovascular system and migraine: studies characterizing cerebrovascular and neuropeptide changes seen in humans and cats. Annals of Neurology. 1993;33(1):48�56. doi: 10.1002/ana.410330109. [PubMed][Cross Ref]
17. Goadsby P. J., Fields H. L. On the functional anatomy of migraine. Annals of Neurology. 1998;43(2, article 272) doi: 10.1002/ana.410430221. [PubMed][Cross Ref]
18. May A., Goadsby P. J. The trigeminovascular system in humans: pathophysiologic implications for primary headache syndromes of the neural influences on the cerebral circulation. Journal of Cerebral Blood Flow and Metabolism. 1999;19(2):115�127. [PubMed]
19. Goadsby P. J., Hargreaves R. Refractory migraine and chronic migraine: pathophysiological mechanisms. Headache. 2008;48(6):799�804. doi: 10.1111/j.1526-4610.2008.01157.x. [PubMed][Cross Ref]
20. Olesen J., Bousser M.-G., Diener H.-C., et al. The international classification of headache disorders, 2nd edition (ICHD-II)�revision of criteria for 8.2 medication-overuse headache. Cephalalgia. 2005;25(6):460�465. doi: 10.1111/j.1468-2982.2005.00878.x. [PubMed][Cross Ref]
21. Stewart W. F., Lipton R. B., Whyte J., et al. An international study to assess reliability of the Migraine Disability Assessment (MIDAS) score. Neurology. 1999;53(5):988�994. doi: 10.1212/wnl.53.5.988. [PubMed][Cross Ref]
22. Wagner T. H., Patrick D. L., Galer B. S., Berzon R. A. A new instrument to assess the long-term quality of life effects from migraine: development and psychometric testing of the MSQOL. Headache. 1996;36(8):484�492. doi: 10.1046/j.1526-4610.1996.3608484.x. [PubMed][Cross Ref]
23. Kosinski M., Bayliss M. S., Bjorner J. B., et al. A six-item short-form survey for measuring headache impact: the HIT-6. Quality of Life Research. 2003;12(8):963�974. doi: 10.1023/a:1026119331193. [PubMed][Cross Ref]
24. Eriksen K., Rochester R. P., Hurwitz E. L. Symptomatic reactions, clinical outcomes and patient satisfaction associated with upper cervical chiropractic care: a prospective, multicenter, cohort study. BMC Musculoskeletal Disorders. 2011;12, article 219 doi: 10.1186/1471-2474-12-219. [PMC free article][PubMed][Cross Ref]
25. National Upper Cervical Chiropractic Association. NUCCA Standards of Practice and Patient Care. 1st. Monroe, Mich, USA: National Upper Cervical Chiropractic Association; 1994.
26. Gregory R. A model for the supine leg check. Upper Cervical Monograph. 1979;2(6):1�5.
27. Woodfield H. C., Gerstman B. B., Olaisen R. H., Johnson D. F. Interexaminer reliability of supine leg checks for discriminating leg-length inequality. Journal of Manipulative and Physiological Therapeutics. 2011;34(4):239�246. doi: 10.1016/j.jmpt.2011.04.009. [PubMed][Cross Ref]
28. Andersen R. T., Winkler M. The gravity stress analyzer for measuring spinal posture. Journal of the Canadian Chiropractic Association. 1983;2(27):55�58.
29. Eriksen K. Subluxation X-ray analysis. In: Eriksen K., editor. Upper Cervical Subluxation Complex�A Review of the Chiropractic and Medical Literature. 1st. Philadelphia, Pa, USA: Lippincott Williams & Wilkins; 2004. pp. 163�203.
30. Zabelin M. X-ray analysis. In: Thomas M., editor. NUCCA: Protocols and Perspectives. 1st. Monroe: National Upper Cervical Chiropractic Association; 2002. p. p. 10-1-48.
31. Miyati T., Mase M., Kasai H., et al. Noninvasive MRI assessment of intracranial compliance in idiopathic normal pressure hydrocephalus. Journal of Magnetic Resonance Imaging. 2007;26(2):274�278. doi: 10.1002/jmri.20999. [PubMed][Cross Ref]
32. Alperin N., Lee S. H., Loth F., Raksin P. B., Lichtor T. MR-intracranial pressure (ICP). A method to measure intracranial elastance and pressure noninvasively by means of MR imaging: baboon and human study. Radiology. 2000;217(3):877�885. doi: 10.1148/radiology.217.3.r00dc42877. [PubMed][Cross Ref]
33. Raksin P. B., Alperin N., Sivaramakrishnan A., Surapaneni S., Lichtor T. Noninvasive intracranial compliance and pressure based on dynamic magnetic resonance imaging of blood flow and cerebrospinal fluid flow: review of principles, implementation, and other noninvasive approaches. Neurosurgical Focus. 2003;14(4, article E4) [PubMed]
34. Koerte I. K., Schankin C. J., Immler S., et al. Altered cerebrovenous drainage in patients with migraine as assessed by phase-contrast magnetic resonance imaging. Investigative Radiology. 2011;46(7):434�440. doi: 10.1097/rli.0b013e318210ecf5. [PubMed][Cross Ref]
35. Pomschar A., Koerte I., Lee S., et al. MRI evidence for altered venous drainage and intracranial compliance in mild traumatic brain injury. PLoS ONE. 2013;8(2) doi: 10.1371/journal.pone.0055447.e55447 [PMC free article][PubMed][Cross Ref]
36. Bayliss M. S., Batenhorst A. S. The HIT-6 A User’s guide. Lincoln, RI, USA: QualityMetric Incorporated; 2002.
37. Coeytaux R. R., Kaufman J. S., Chao R., Mann J. D., DeVellis R. F. Four methods of estimating the minimal important difference scores were compared to establish a clinically significant change in Headache Impact Test. Journal of Clinical Epidemiology. 2006;59(4):374�380. doi: 10.1016/j.jclinepi.2005.05.010. [PubMed][Cross Ref]
38. Smelt A. F. H., Assendelft W. J. J., Terwee C. B., Ferrari M. D., Blom J. W. What is a clinically relevant change on the HIT-6 questionnaire? An estimation in a primary-care population of migraine patients. Cephalalgia. 2014;34(1):29�36. doi: 10.1177/0333102413497599. [PubMed][Cross Ref]
39. Sauro K. M., Rose M. S., Becker W. J., et al. HIT-6 and MIDAS as measures of headache disability in a headache referral population. Headache. 2010;50(3):383�395. doi: 10.1111/j.1526-4610.2009.01544.x. [PubMed][Cross Ref]
40. Bagley C. L., Rendas-Baum R., Maglinte G. A., et al. Validating migraine-specific quality of life questionnaire v2.1 in episodic and chronic migraine. Headache. 2012;52(3):409�421. doi: 10.1111/j.1526-4610.2011.01997.x. [PubMed][Cross Ref]
41. Cole J. C., Lin P., Rupnow M. F. T. Minimal important differences in the Migraine-Specific Quality of Life Questionnaire (MSQ) version 2.1. Cephalalgia. 2009;29(11):1180�1187. doi: 10.1111/j.1468-2982.2009.01852.x. [PubMed][Cross Ref]
42. Dodick D. W., Silberstein S., Saper J., et al. The impact of topiramate on health-related quality of life indicators in chronic migraine. Headache. 2007;47(10):1398�1408. doi: 10.1111/j.1526-4610.2007.00950.x. [PubMed][Cross Ref]
43. Hr�bjartsson A., G�tzsche P. C. Placebo interventions for all clinical conditions. Cochrane Database of Systematic Reviews. 2010;(1)CD003974 [PubMed]
44. Meissner K. The placebo effect and the autonomic nervous system: evidence for an intimate relationship. Philosophical Transactions of the Royal Society B: Biological Sciences. 2011;366(1572):1808�1817. doi: 10.1098/rstb.2010.0403. [PMC free article][PubMed][Cross Ref]
45. Marshall I., MacCormick I., Sellar R., Whittle I. Assessment of factors affecting MRI measurement of intracranial volume changes and elastance index. British Journal of Neurosurgery. 2008;22(3):389�397. doi: 10.1080/02688690801911598. [PubMed][Cross Ref]
46. Raboel P. H., Bartek J., Andresen M., Bellander B. M., Romner B. Intracranial pressure monitoring: invasive versus non-invasive methods-A review. Critical Care Research and Practice. 2012;2012:14. doi: 10.1155/2012/950393.950393 [PMC free article][PubMed][Cross Ref]
47. Wentland A. L., Wieben O., Korosec F. R., Haughton V. M. Accuracy and reproducibility of phase-contrast MR imaging measurements for CSF flow. American Journal of Neuroradiology. 2010;31(7):1331�1336. doi: 10.3174/ajnr.A2039. [PMC free article][PubMed][Cross Ref]
48. Koerte I., Haberl C., Schmidt M., et al. Inter- and intra-rater reliability of blood and cerebrospinal fluid flow quantification by phase-contrast MRI. Journal of Magnetic Resonance Imaging. 2013;38(3):655�662. doi: 10.1002/jmri.24013. [PMC free article][PubMed][Cross Ref]
49. Stoquart-Elsankari S., Lehmann P., Villette A., et al. A phase-contrast MRI study of physiologic cerebral venous flow. Journal of Cerebral Blood Flow and Metabolism. 2009;29(6):1208�1215. doi: 10.1038/jcbfm.2009.29. [PubMed][Cross Ref]
50. Atsumi H., Matsumae M., Hirayama A., Kuroda K. Measurements of intracranial pressure and compliance index using 1.5-T clinical MRI machine. Tokai Journal of Experimental and Clinical Medicine. 2014;39(1):34�43. [PubMed]
51. Becker W. J. Assessing health-related quality of life in patients with migraine. Canadian Journal of Neurological Sciences. 2002;29(supplement 2):S16�S22. doi: 10.1017/s031716710000189x. [PubMed][Cross Ref]
Being involved in an automobile accident can cause damage or injury to the complex structures of the cervical spine which can go unnoticed for months if left untreated. Medically referred to as whiplash-associated disorders, or whiplash, symptoms resulting after an auto accident can often take days to even weeks or months to manifest. Persistent neck pain that lasts for more than 3 months then becomes chronic neck pain, an issue which can be difficult to manage if not treated accordingly. Chronic neck pain may also result due to other underlying issues. The following article demonstrates which types of treatment methods can help relieve chronic neck pain symptoms and its associated complications, including capsular ligament laxity and cervical instability.
Chronic Neck Pain: Making the Connection Between Capsular Ligament Laxity and Cervical Instability
Abstract
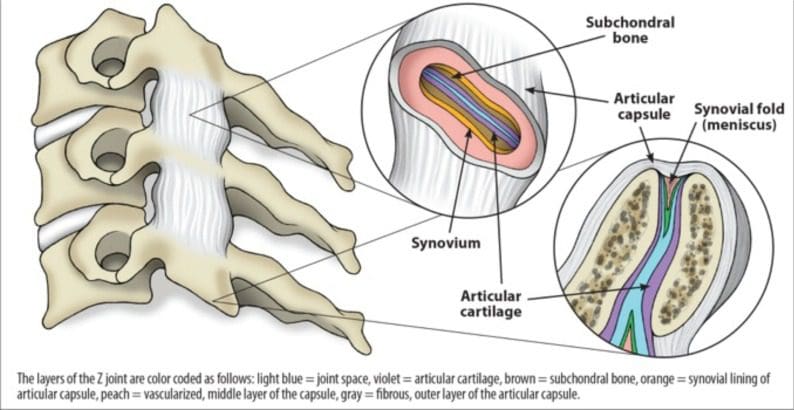
The use of conventional modalities for chronic neck pain remains debatable, primarily because most treatments have had limited success. We conducted a review of the literature published up to December 2013 on the diagnostic and treatment modalities of disorders related to chronic neck pain and concluded that, despite providing temporary relief of symptoms, these treatments do not address the specific problems of healing and are not likely to offer long-term cures. The objectives of this narrative review are to provide an overview of chronic neck pain as it relates to cervical instability, to describe the anatomical features of the cervical spine and the impact of capsular ligament laxity, to discuss the disorders causing chronic neck pain and their current treatments, and lastly, to present prolotherapy as a viable treatment option that heals injured ligaments, restores stability to the spine, and resolves chronic neck pain.
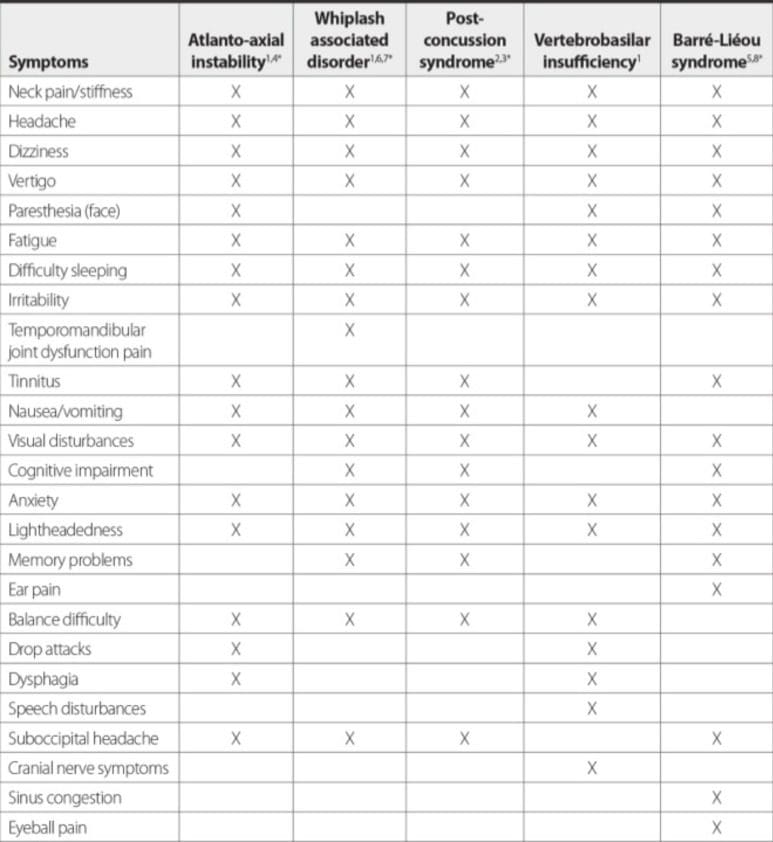
The capsular ligaments are the main stabilizing structures of the facet joints in the cervical spine and have been implicated as a major source of chronic neck pain. Chronic neck pain often reflects a state of instability in the cervical spine and is a symptom common to a number of conditions described herein, including disc herniation, cervical spondylosis, whiplash injury and whiplash associated disorder, postconcussion syndrome, vertebrobasilar insufficiency, and Barr�-Li�ou syndrome.
When the capsular ligaments are injured, they become elongated and exhibit laxity, which causes excessive movement of the cervical vertebrae. In the upper cervical spine (C0-C2), this can cause a number of other symptoms including, but not limited to, nerve irritation and vertebrobasilar insufficiency with associated vertigo, tinnitus, dizziness, facial pain, arm pain, and migraine headaches. In the lower cervical spine (C3-C7), this can cause muscle spasms, crepitation, and/or paresthesia in addition to chronic neck pain. In either case, the presence of excessive motion between two adjacent cervical vertebrae and these associated symptoms is described as cervical instability.
Therefore, we propose that in many cases of chronic neck pain, the cause may be underlying joint instability due to capsular ligament laxity. Currently, curative treatment options for this type of cervical instability are inconclusive and inadequate. Based on clinical studies and experience with patients who have visited our chronic pain clinic with complaints of chronic neck pain, we contend that prolotherapy offers a potentially curative treatment option for chronic neck pain related to capsular ligament laxity and underlying cervical instability.
In the realm of pain management, an ever-growing number of treatment-resistant patients are being left with relatively few conventional treatment options that effectively and permanently relieve their chronic pain symptoms. Chronic cervical spine pain is particularly challenging to treat, and data regarding the long-term efficacy of traditional therapies has been extremely discouraging [1]. The prevalence of neck pain in the general population has been reported to range between 30% and 50%, with women over 50 making up the larger portion [1-3]. Although many of these cases resolve with time and require minimal intervention, the recurrence rate of neck pain is high, and about one-third of people will suffer from chronic neck pain (defined as pain that persists longer than 6 months), and 5% will develop significant disability and reduction in quality of life [2, 4]. For this group of chronic pain patients, modern medicine offers few options for long-term recovery.
Treatment protocols for acute and sub-acute neck pain are standard and widely agreed upon [1, 2]. However, conventional treatments for chronic neck pain remain debatable and include interventions such as use of nonsteroidal anti-inflammatory drugs (NSAIDs) and narcotics for pain management, cervical collars, rest, physiotherapy, manual therapy, strengthening exercises, and nerve blocks. Furthermore, the literature on long-term treatment outcomes has been inconclusive at best [5-9]. Chronic neck pain due to whiplash injury or whiplash associated disorder (WAD) is particularly resistant to long-term treatment; conventional treatment for these conditions may give temporary relief but long-term outcomes have been disappointing [10].
In light of the poor treatment options and outcomes for chronic neck pain, we propose that in many of these cases, the underlying condition may be related to capsular ligament laxity and subsequent joint instability of the cervical spine. Should this be the case and joint instability is the fundamental problem causing chronic neck pain, a new treatment approach may be warranted.
The diagnosis of chronic neck pain due to cervical instability is particularly challenging. In most cases, diagnostic tools for detecting cervical instability have been inconsistent and lack specificity [11-15], and are therefore inadequate. A better understanding of the pathogenesis of cervical instability may better enable practitioners to recognize and treat the condition more effectively. For instance, when cervical instability is related to injury of soft tissue (eg, ligaments) alone and not fracture, the treatment modality should be one that stimulates the involved soft tissue to regenerate and repair itself.
In that context, comprehensive dextrose prolotherapy offers a promising treatment option for resolving cervical instability and the subsequent pain and disability it causes. The distinct anatomy of the cervical spine and the pathology of cervical instability described herein underlie the rationale for treating the condition with prolotherapy.
Anatomy
The cervical spine consists of the first seven vertebrae in the spinal column and is divided into two segments, the upper cervical (C0-C2) and lower cervical (C3-C7) regions. Despite having the smallest vertebral bodies, the cervical spine is the most mobile segment of the entire spine and must support a high degree of movement. Consequently, it is highly reliant on ligamentous tissue for stabilizing the neck and spinal column, as well as for controlling normal joint motion; as a result, the cervical spine is highly susceptible to injury.
The upper cervical spine consists of C0, called the occiput, and the first two cervical vertebrae, C1 and C2, or atlas and axis, respectively. C1 and C2 are more specialized than the rest of the cervical vertebrae. C1 is ring-shaped and lacks a vertebral body. C2 has a prominent vertebral body called the odontoid process or dens which acts as a pivot point for the C1 ring [16]. This pivoting motion (Fig. ?1), coupled with the lack of intervertebral discs in the upper cervical spine, allows for more movement and rotation of the joint, thus facilitating mobility rather than stability [17]. Collectively, the upper cervical spine is responsible for 50% of total neck flexion and extension at the atlanto-occipital (C0-C1) joint, as well as 50% of total neck rotation that occurs at the atlanto-axial joint (C1-C2) [16]. This motion is possible because the atlas (C1) rotates around the axis (C2) via the dens and the anterior arch of the atlas.
Figure 1: Atlanto-axial rotational instability. The atlas is shown in the rotated position on the axis. The pivot is the eccentrically placed odontoid process. In rotation, the wall of the vertebral foramen of Cl decreases the opening of the spinal canal between Cl and C2. This can potentially cause migraine headaches, C2 nerve root impingement, dizziness, vertebrobasilar insufficiency, ‘drop attacks; neck-tongue syndrome, Barr�-Li�ou syndrome, severe neck pain, and tinnitus.
The intrinsic, passive stability of the spine is provided by the intervertebral discs and surrounding ligamentous structures. The upper cervical spine is stabilized solely by ligaments, including the transverse, alar, and capsular ligaments. The transverse ligament runs behind the dens, originating on a small tubercle on the medial side of a lateral mass of the atlas and inserting onto the identical tubercle on the other side. Thus, the transverse ligament restricts flexion of the head and anterior displacement of the atlas. The left and right alar ligaments originate from the posterior dens and attach to the medial occipital condyles on the ipsilateral sides. They work to limit axial rotation and are under the greatest tension in rotation and flexion. By holding C1 and C2 in proper position, the transverse and alar ligaments help to protect the spinal cord, brain stem, and nervous system from excess movement in the upper cervical spine [18].
The lower cervical spine, while less specialized, allows for the remaining 50% of neck flexion, extension, and rotation. Each vertebra in this region (C3-C7) has a vertebral body, in between which lies an intervertebral disc, the largest avascular structure of the body. This disc is a piece of fibrocartilage that helps cushion the joints and allows for more stability and is comprised of an inner gelatinous nucleus pulposus, which is surrounded by an outer, fibrous annulus fibrosus. The nucleus pulposus is designed to sustain compression loads and the annulus fibrosus, to resist tension, shear and torsion [19]. The annulus fibrosus is thought to determine the proper functioning of the entire intervertebral disc [20] and has been described as a lamellar structure consisting of 15-26 distinct concentric fibrocartilage layers that constitute a criss-crossing fiber matrix [19]. However, the form of this structure has been disputed. A microdissection study using cadavers reported that the cervical annulus fibrosus does not consist of concentric laminae of collagen fibers as it does in lumbar discs. Instead, the authors contend that the three-dimensional architecture of the cervical annulus fibrosus is more like that of a crescentic anterior interosseous ligament surrounding the nucleus pulposus [21].
In addition to the discs, multiple ligaments and the two synovial joints on each pair of adjacent vertebrae (facet joints) allow for controlled, fully three dimensional motions. Capsular ligaments wrap around each facet joint, which help to maintain stability during neck rotation. Each vertebra in the lower cervical spine (in addition to C2) contains a spinous process that serves as an attachment site for the interspinal ligaments. These tissues connect adjacent spinous processes and limit flexion of the cervical spine. Anteriorly, they meet with the ligamentum flavum.
Three other ligaments, the ligamentum flavum, anterior longitudinal ligament (ALL), and posterior longitudinal ligament (PLL), help to stabilize the cervical spine during motion and protect against excess flexion and extension of the cervical vertebrae. From C1-C2 to the sacrum, the ligamentum flava run down the posterior aspect of the spinal canal and join the laminae of adjacent vertebrae while helping to maintain proper neck posture. The ALL and PLL both run alongside the vertebral bodies. The ALL begins at the occiput and runs anteriorly to the anterior sacrum, helping to stabilize the vertebrae and intervertebral discs and limit spinal extension. The PLL also helps to stabilize the vertebrae and intervertebral discs, as well as limit spinal flexion. It extends from the body of the axis to the posterior sacrum and runs within the anterior aspect of the spinal canal across from the ligamentum flava.
A spinous process and two transverse processes emanate off the neural arch (or vertebral arch) which lies at the posterior aspect of the cervical vertebral column. The transverse processes are bony prominences that protrude postero-laterally and serve as attachment sites for various muscles and ligaments. With the exception of C7, each of these processes has a foramen which allows for passage of the vertebral artery towards the brain; the C7 transverse process has foramina which allow for passage of the vertebral vein and sympathetic nerves [22]. The transverse processes of the cervical vertebrae are connected via the intertransverse ligaments; each attaches a transverse process to the one below and helps to limit lateral flexion of the cervical spine.
Facet Joints
The inferior articular process of the superior cervical vertebra, except for C0-C1, and the superior articular process of the inferior cervical vertebra join to form the facet joints of the cervical spine; in the case of C0-C1, the inferior articular process of C1 joins the occipital condyles. Also referred to as zygapophyseal joints (Fig. ?2), the facet joints are diarrthrodial, meaning they function similar to the knee joint in that they contain synovial cells and joint fluid and are surrounded by a capsule. They also contain a meniscus which helps to further cushion the joint, and like the knee, are lined by articular cartilage and surrounded by capsular ligaments, which stabilize the joint. These capsular ligaments hold adjacent vertebrae to one another, and the articular cartilage therein is aligned such that its opposing tissue surfaces provide for a low-friction environment [23].
Figure 2: Typical Z (zygapophyseal/ facet) joint. Each facet joint has articular cartilage, the synovium where synovial fluid is produced, and a meniscus.
There is some dissimilarity in facet joint anatomy between the upper and lower cervical spine. Even in the upper cervical region, C0-C1 and C1-C2 facet joints differ anatomically. At C0-C1, the convex shape of the occipital condyles enables them to fit into the concave surface of the inferior articular process. The C1-C2 facet joints are oriented cranio-caudally, meaning they run more parallel to their transverse processes. As such, their capsular ligaments are normally relatively lax, and thus, are inherently less stable and meant to facilitate mobility (i.e., rotation) [23, 24].
In contrast, the facet joints of the lower cervical spine are positioned at more of an angle. In the transverse plane, the angles of the right and left C2-C3 facet joints are estimated to be 32� to 65� and 32� to 60�, respectively, while those of the C6-C7 facet joints are typically steeper at 45� to 75� and 50� to 78� [25]. As the cervical spine extends downward, the angle of the facet joint becomes bigger such that the joint slopes backwards and downwards. Thus, the facet joints of the lower cervical spine have progressively less rotation than those of the upper cervical spine. Furthermore, the presence of intervertebral discs helps give the lower cervical spine more stability.
Nevertheless, injury to any of the facet joints can cause instability to the cervical spine. Researchers have found there is a continuum between the amount of trauma and degree of instability to the cervical facets, with greater trauma causing a higher degree of facet instability [26-28].
Cervical Capsular Ligaments
The capsular ligaments are extremely strong and serve as the main stabilizing tissue in the spinal column. They lie close to the intervertebral centers of rotation and provide significant stability in the neck, especially during axial rotation [29]; consequently, they serve as essential components for ensuring neck stability with movement. The capsular ligaments have a high peak force and elongation potential, meaning they can withstand large forces before rupturing. This was demonstrated in a dynamic mechanical study in which the capsular ligaments and ligamentum flavum were shown to have the highest average peak force, up to 220 N and 244 N, respectively [30]. This was reported as considerably greater than the force shown in the anterior longitudinal ligament and middle third disc.
While much has been reported about the strength of the capsular ligaments as related to cervical stability, when damaged, these ligaments lose their strength and are unable to support the cervical spine properly. For instance, in an animal study, it was shown that sequential removal of sheep capsular ligaments and cervical facets caused an undue increase in range of motion, especially in axial rotation, flexion and extension with caudal progression [31]. Human cadaver studies have also indicated that transection or injury of joint capsular ligaments significantly increases axial rotation and lateral flexion [32, 33]. Specifically, the largest increase in axial rotation with damage to a unilateral facet joint was 294% [33].
Capsular ligament laxity can occur instantaneously as a single macrotrauma, such as a whiplash injury, or can develop slowly as cumulative microtraumas, such as those from repetitive forward or bent head postures. In either case, the cause of injury occurs through similar mechanisms, leading to capsular ligament laxity and excess motion of the facet joints, which often results in cervical instability. When ligament laxity develops over time, it is defined as �creep� (Fig. ?3) and refers to the elongation of a ligament under a constant or repetitive stress [34]. While this constitutes low-level subfailure ligament injuries, it may represent the vast majority of cervical instability cases and can potentially incapacitate people due to disabling pain, vertigo, tinnitus or other concomitant symptoms of cervical instability. Such symptoms can be caused by elongation-induced strains of the capsular ligaments; these strains can progress to subsequent subfailure tears in the ligament fibers or to laxity in the capsular ligaments, leading to instability at the level of the cervical facet joints [35]. This is most evident when the neck is rotated (ie, looking to the left or right) and that movement�causes a �cracking� or �popping� sound. Clinical instability indicates that the spine is unable to maintain normal motion and function between vertebrae under normal physiological loads, inducing irritation to nerves, possible structural deformation, and/or incapacitating pain.
Figure 3: Ligament laxity and creep. When ligaments are under a constant stress, they display creep behavior. Creep refers to a time-dependent increase in strain and causes ligaments to “stretch out” over time.
Furthermore, the capsular ligaments surrounding the facet joints are highly innervated by mechanoreceptive and nociceptive free nerve endings. Hence, the facet joint has long been considered the primary source of chronic spinal pain [36-38]. Additionally, injury to these nerves has been shown to affect the overall joint function of the facet joints [39]. Therefore, injury to the capsular ligaments and subsequent nerve endings could explain the prevalence of chronic pain and joint instability in the facet joints of the cervical spine.
Cervical Instability
Clinical instability is not to be confused with hypermobility. In general, instability implies a pathological condition with resultant symptoms, whereas joint hypermobility alone does not (Fig. ?4). Clinical instability refers to a loss of motion stiffness in a particular spinal segment when the application of force to it produces greater displacement(s) than would otherwise be seen in a normal structure. In clinical instability, symptoms such as pain and muscle spasms can thus be experienced within a person�s range of motion, not just at its furthest extension point. These muscle spasms can cause intense pain and are the body�s response to cervical instability in that the ligaments act as sensory organs involved in ligamento-muscular reflexes. The ligamento-muscular reflex is a protective reflex emanating from mechanoreceptors (ie, pacinian corpuscles, golgi tendon organs, and ruffini endings) in the ligaments and transmitted to the muscles. Subsequent activation of these muscles helps to preserve joint stability, either directly by muscles crossing the joint or indirectly by muscles that do not cross the joint but limit joint motion [40].
Figure 4: Cervical spinal motion continuum and role of prolotherapy. When minor or moderate spinal instability occurs, treatment with prolotherapy may be of benefit in alleviating symptoms and restoring normal cervical joint function.
In a clinically unstable joint where neurologic insult is present, it is presumed that the joint has undergone more severe damage in its stabilizing structures, which may include the vertebrae themselves. In contrast, joints that are hypermobile demonstrate increased segmental mobility but are able to maintain their stability and function normally under physiological loads [41].
Clinical instability can be classified as mild, moderate or severe, with the later being associated with catastrophic injury. Minor injuries of the cervical spine are those involving soft tissues alone without evidence of fracture and are the most common causes of cervical instability. Mild or moderate clinical instability is that which is without neurologic (somatic) injury and is typically due to cumulative micro-traumas.
Diagnosis of Cervical Instability
Cervical instability is a diagnosis based primarily on a patient�s history (ie, symptoms) and physical examination because there is yet to be standardized functional X-rays or imaging able to diagnose cervical instability or detect ruptured ligamentous tissue without the presence of bony lesions [24]. For example, in one autopsy study of cryosection samples of the cervical spine, [42] only one out of ten gross ligamentous disruptions was evident on x-ray. Furthermore, there is often little correlation between the degree of instability or hypermobility shown on radiographic studies and clinical symptoms [43-45]. Even after severe whiplash injuries, plain radiographs are usually normal despite clinical findings indicating the presence of soft tissue damage.
However, functional computerized tomography (fCT) and magnetic resonance imaging (fMRI) scans and digital motion x-ray (DMX) are able to adequately depict cervical instability pathology [46, 47]. Studies using fCT for diagnosing soft tissue ligament or post-whiplash injuries have demonstrated the ability of this technique to show excess atlanto-occipital or atlanto-axial movement during axial rotation [48, 49]. This is especially pertinent when patients have signs and symptoms of cervical instability, yet have normal MRIs in a neutral position.
Functional imaging technology, as opposed to static standard films, is necessary for adequate radiologic depiction of instability in the cervical spine because they provide dynamic imaging of the neck during movement and are helpful for evaluating the presence and degree of cervical instability (Fig. ?5). There are also specialized physical examination tests specific for upper cervical instability, such as the Sharp-Purser test, upper cervical flexion test, and cervical flexion-rotation test.
Figure 5: 3D CT scan of upper cervical spine. C1-C2 instability can easily be seen in the patient, as 70% of C1 articular facet is subluxed posteriorly (arrow) on C2 facet when the patient rotates his head (turns head to the left then the right).
Upper Cervical Pathology and Instability
Although not usually apparent radiographically, injury to the ligaments and soft tissues of C0-C2 from head or neck trauma is more likely than are cervical fractures or subluxation of bones [50, 51]. Ligament laxity across the C0-C1-C2 complex is primarily caused by rotational movements, especially those involving lateral bending and axial rotation [52-54]. With severe neck traumas, especially those with rotation, up to 25% of total lesions can be attributed to ligament injuries of C0-C2 alone. Although some ligament injuries in the C0-C2 region can cause severe neurological impairment, the majority involve sub-failure loads to the facet joints and capsular ligaments, which are the primary source of most chronic pain in post-neck trauma [26, 55].
Due to its lack of osseous stability, the upper cervical spine is also vulnerable to injury by high velocity manipulation. The capsular ligaments of the atlanto-axial joint are especially susceptible to injury from rotational thrusts, and thus, may be at risk during mechanically mediated manipulation. The capsular ligaments in the occipto-atlantal joint function as joint stabilizers and can also become injured due to excessive or abnormal forces [46].
Excessive tension on the capsular ligaments can cause upper cervical instability and related neck pain [56]. Capsular ligament tension is increased during abnormal postures, causing elongation of the capsular ligaments, with magnitudes increased by up to 70% of normal [57]. Such excessive ligament elongation induces laxity to the facet joints, which puts the cervical spine more at risk for further degenerative changes and instability. Therefore, capsular ligament injury appears to cause upper cervical instability because of laxity in the stabilizing structure of the facet joints [58].
Cervical Pain Versus Cervical Radiculopathy
According to the International Association for the Study of Pain (IASP), cervical spinal pain is pain perceived as anywhere in the posterior region of the cervical spine, defining it further as pain that is �perceived as arising from anywhere within the region bounded superiorly by the superior nuchal line, inferiorly by an imaginary transverse line through the tip of the first thoracic spinous process, and laterally by sagittal planes tangential to the lateral borders of the neck� [59]. Similarly, cervical pain is divided equally by an imaginary transverse plane into upper cervical pain and lower cervical pain. Suboccipital pain is that pain located between superior nuchal line and an imaginary transverse line through the tip of the second cervical spinous process. Likewise, cervico-occipital pain is perceived as arising in the cervical region and extending over the occipital region of the skull. These sources of pain could be a result of underlying cervical instability.
The IASP defines radicular pain as that arising in a limb or the trunk wall, caused either by ectopic activation of nociceptive afferent fibers in a spinal nerve or its roots or by other neuropathic mechanisms, and may be episodic, recurrent, or sudden [59]. Clinically, there is a 30% rate of radicular symptoms during axial rotation in those with rotator instabilities [60]. Thus, radicular pain may also be a result of underlying cervical instability.
With capsular ligament laxity, hypertrophic facet joint changes occur (including osteophytosis) as cervical degeneration progresses, causing encroachment on cervical nerve roots as they exit the spine through the neural foramina. This condition is called cervical radiculopathy and manifests as stabbing pain, numbness, and/or tingling down the upper extremity in the area of the affected nerve root.
The neural foramina lie between the intervertebral disc and the joints of Luschka (uncovertebral joints) anteriorly and the facet joint posteriorly. Their superior and inferior borders are the pedicles of adjacent vertebral bodies. Cervical nerve roots there are vulnerable to compression or injury by the facet joints posteriorly or by the joints of Luschka and the intervertebral disc anteriorly.
Cadaver studies have demonstrated that cervical nerve roots take up as much as 72% of the space in the neural foramina [61]. Normally, this provides ample room for the nerves to function optimally. However, if the cervical spine and capsular ligaments are injured, facet joint hypertrophy and degeneration of the cervical discs can occur. Over time, this causes narrowing of the neural foramina (Fig. ?6) and a decrease in space for the nerve root. In the event of another ligament injury, instability of the hypertrophied bones can occur and further reduce the patency of the neural foramen.
Figure 6: Digital motion X-ray demonstrating multi-level cervical instability. Neural foraminal narrowing is shown at two levels during lateral extension versus lateral flexion.
Cervical radiculopathy from a capsular ligament injury typically produces intermittent radicular symptoms which become more noticeable when the neck is moved in a certain direction, such as during rotation, flexion or extension. These movements can cause encroachment on cervical nerve roots and subsequent paresthesia along the pathway therein of the affected nerve and may be why evidence of cervical radiculopathy does not show up on standard MRI or CT scans.
When disc herniation is the cause of cervical radiculopathy, it typically presents with acute onset of severe neck and arm pain unrelieved by any position and often results in encroachment on a cervical nerve root. While disc herniation can easily be seen on routine (non-functional) MRI or CT scans, evidence of radiculopathy from cervical instability cannot. Most cases of acute radiculopathy due to disc herniation resolve with non-surgical active or passive therapies, but some patients continue to have clinically significant symptoms, in which case surgical treatments such as anterior cervical decompression with fusion or posterior cervical laminoforaminotomy can be performed [62]. Cervical radiculopathy is also strongly associated with spondylosis, a disease generally attributed to aging that involves an overall degeneration of the cervical spine. The disorder is characterized by degenerative changes in the intervertebral disc, osteophytosis of the vertebral bodies, and hypertrophy of the facet joints and laminar arches. Since more than one cervical spine segment is usually affected in spondylosis, the symptoms of radiculopathy are more diffuse than those typical of unilateral soft disc herniation and present as neck, mid-upper back, and arm pain with paresthesia.
Dr. Alex Jimenez’s Insight
“I was involved in an automobile accident that left me with chronic neck pain. What could be causing my painful and persistent neck pain symptoms?”�Being involved in an automobile accident can be a traumatic experience, resulting in both mental and physical harm. Whiplash-associated injuries are some of the most common diagnosis behind reported cases of chronic neck pain after an auto accident. During a car crash, the force of the impact can abruptly jerk the head back-and-forth, stretching the complex structures around the cervical spine beyond their natural range, causing damage or injury.The following article provides an overview of chronic neck pain, its mechanism of injury and effective treatment methods for neck pain.
Cervical Spondylosis: the Instability Connection
Spondylosis has previously been described as occurring in three stages: the dysfunctional stage, the unstable stage, and the stabilization stage (Fig. ?7) [63]. Spondylosis begins with repetitive trauma, such as rotational strains or compressive forces to the spine. This causes injury to the facet joints which can compromise the capsular ligaments. The dysfunctional phase is characterized by capsular ligament injuries and subsequent cartilage degeneration and synovitis, ultimately leading to abnormal motion in the cervical spine. Over time, facet joint dysfunction intensifies as capsular laxity occurs. This stretching response can cause cervical instability, marking the unstable stage. During this progression, ongoing degeneration is occurring in the intervertebral discs, along with other parts of the cervical spine. Ankylosis (stiffening of the joints) can also occur at the unstable cervical spine segment, and rarely, causes entrapment of nearby spinal nerves. The stabilization phase occurs with the formation of marginal osteophytes as the body tries to heal the spine. These bridging bony deposits can lead to a natural fusion of the affected vertebrae [64].
Figure 7: Cervical OA: The 3 phases of the degenerative cascade. Used with permission from: Kramer WC, et al. Pathogenetic mechanisms of posttraumatic osteoarthritis: opportunities for early intervention. Int J Clin Exp Me d. 2011; 4(4): 285-298.
The degenerative cascade, however, begins long before symptoms become evident. Initially, spondylosis develops silently and is asymptomatic [65]. When symptoms of cervical spondylosis do develop, they are generally nonspecific and include neck pain and stiffness [66]. Only rarely do neurologic symptoms develop (ie, radiculopathy or myelopathy), and most often they occur in people with congenitally narrowed spinal canals [67]. Physical exam findings are often limited to restricted range of neck motion and poorly localized tenderness. Clinical symptoms commonly manifest when a new cervical ligament injury is superimposed on the underlying degeneration. In patients with spondylosis and underlying capsular ligament laxity, cervical radiculopathy is more likely to occur because the neural foramina may already be narrowed from facet joint hypertrophy and disc degeneration, enabling any new injury to more readily pinch on an exiting nerve root.
Thus, there are compelling reasons to believe that facet joint/capsular ligament injuries in the cervical spine may be an etiological basis for the degenerative cascade in cervical spondylosis and may be responsible for the attendant cervical instability. Animal models used for initiating disc degeneration in research studies have shown the induction of spinal instability through injury of the facet joints [68, 69]. In similar models, capsular ligament injuries of the facet joints caused multidirectional instability of the cervical spine, greatly increasing axial rotation motion correlating with cervical disc injuries [31, 28, 70, 71]. Using human specimens, surgical procedures such as discectomy have been shown to cause an immediate increase in motion of the segments involved [72]. Stabilization procedures such as neck fusion have been known to create increased pressure on the adjacent cervical spinal segments; this is referred to as adjacent segment disease. This can develop when the loss of motion from cervical fusion causes greater shearing and increased rotation and traction stress on adjacent vertebrae at the facet joints [73-75]. Thus, instability can �travel� up or down from the fused segment, furthering disc degeneration. These findings support the theory that iatrogenic-introduced stress and instability at adjacent spinal segments contribute to the pathogenesis of cervical spondylosis [74].
Whiplash Trauma
Damage to cervical ligaments from whiplash trauma has been well studied, yet these injuries are still often difficult to diagnose and treat. Standard x-rays often do not reveal present injury to the cervical spine and as a consequence, these injuries go unreported and patients are left without proper treatment for their condition [76]. Part of the difficulty lies in the fact that major injury to the cervical spine may only produce minor symptoms in some patients, whereas minor injury may produce more severe symptoms in others [77]. These symptoms include acute and/or chronic neck pain, headache, dizziness, vertigo and paresthesia in the upper extremities [78, 79].
MRI and autopsy studies have both shown an association between chronic symptoms in whiplash patients and injuries to the cervical discs, ligaments and facet joints [42, 80]. Success in relieving neck pain in whiplash patients has been documented by numerous clinical studies using nerve block and radiofrequency ablation of facet joint afferents, including capsular ligament nerves, such that increased interest has developed regarding the relationships between injury to the facet joints and capsular ligaments and post-whiplash dysfunction and related symptoms [36, 81].
Multiple studies have implicated the cervical facet joint and its capsule as a primary anatomical site of injury during whiplash exposure to the neck [55, 57, 82, 83]. Others have shown that injury to the cervical facet joints and capsular ligaments are the most common cause of pain in post-whiplash patients [84-86]. Cinephotographic and cineradiographic studies of both cadavers and human subjects show that under the conditions of whiplash, a resultant high impact force occurs in the cervical facet joints, leading to their injury and the possibility of cervical spine instability [84].
In whiplash trauma, up to 10 times more force is absorbed in the capsular ligaments versus the intervertebral disc [30]. Unlike the disc, the facet joint has a much smaller area in which to disperse this force. Ultimately, the capsular ligaments become elongated, resulting in abnormal motions in the spinal segments affected [30, 87]. This sequence has been documented with both in vitro and in vivo studies of segmental motion characteristics after torsional loads and resultant disc degeneration [88-90].
Injury to the facet joints and capsular ligaments has been further confirmed during simulated whiplash traumas [91]. Maximum capsular ligament strains occur during shear forces, such as when a force is applied while the head is rotated (axial rotation). While capsular ligament injury in the upper cervical spinal region can occur from compressive forces alone, exertion from a combination of shear, compression and bending forces is more likely and usually involves much lower loads to cause injury [92]. However, if the head is turned during whiplash trauma, the peak strain on the cervical facet joints and capsular ligaments can increase by 34% [93]. In one study reporting on an automobile rear-impact simulation, the magnitude of the joint capsule strain was 47% to 196% higher in instances when the head was rotated 60� during impact, compared with those when the head was forward facing [94]. The impact was greatest in the ipsilateral facet joints, such that head rotation to the left caused higher ligament strain at the left facet joint capsule.
In other simulations, whiplash trauma has been shown to reduce cervical ligament strength (ie, failure force and average energy absorption capacity) compared with controls or computational models [30, 87]; this is especially true in the case of capsular ligaments, since such trauma causes capsular ligament laxity. One study conclusively demonstrated that whiplash injury to the capsular ligaments resulted in an 85% to 275% increase in ligament elongation (ie, laxity) compared to that of controls [30]. The study also reported evidence that tension of the capsular ligaments is requisite for producing pain from the facet joint.
Post-Concussion Syndrome
Each year in the United States, approximately 1.7 million people are diagnosed with traumatic brain injury (TBI), although many more go undiagnosed because they do not seek out medical care [95]. Of these, approximately 75% – 90% are diagnosed as having a concussion. A concussion is considered a mild TBI and is defined as any transient neurologic dysfunction resulting from a biomechanical force, usually a sudden or forceful blow to the head which may or may not cause a loss of consciousness. Concussion induces a barrage of ionic, metabolic, and physiologic events [96] and manifests in a composite of symptoms affecting a patient�s physical, cognitive, and emotional states, and his or her sleep cycle, any one of which can be fleeting or long-term in duration [97]. The diagnosis of concussion is made by the presence of any one of the following: (1) any loss of consciousness; (2) any loss of memory for events immediately before or after the injury; (3) any alteration in mental status at the time of the accident; (4) focal neurological deficits that may or may not be transient [98].
While most individuals recover from a single concussion, up to one-third of those will continue to suffer from residual effects such as headache, neck pain, dizziness and memory problems one year after injury [99]. Such symptoms characterize a disorder known as post-concussion syndrome (PCS) and are much like those of WAD; both disorders are likely due to cervical instability. According to the International Classification of Diseases, 10th Revision (ICD-10), the diagnosis of PCS is made when a person has had a head injury sufficient enough to result in loss of consciousness and develops at least three of eight of the following symptoms within four weeks: headache, dizziness, fatigue, irritability, sleep problems, concentration difficulties, memory issues, and problems tolerating stress [100, 101]. Of those treated for PCS who had mild head injury, 80% report having chronic daily headaches; surprisingly, of those with moderate to severe head injury, only 27% reported having chronic daily headaches [102]. The impact of the brain on the skull is believed to be the cause of the symptoms of both concussion and PCS, although the specific mechanisms underlying neural tissue damage are still being investigated.
PCS-associated symptoms also overlap with many symptoms common to WAD. This overlap in symptomology may be due to a common etiology of underlying cervical instability that affects the cervical spine near the neck. Data has revealed that over half of patients with damage to the upper cervical spine from whiplash injury had evidence of concurrent head trauma [103]. It was shown that whiplash can cause minor brain injuries similar to that of concussion if it occurs with such rapid neck movement that there is a collision between the brain and skull. Thus, one may conjecture that concussion involves a whiplash-type injury to the neck.
Despite unique differences in the biomechanics of concussion and whiplash, both types of trauma involve an acceleration-deceleration of the head and neck. This impact to the head can not only cause injury to the brain and skull, but can also damage surrounding ligaments of the neck since these tissues undergo the same accelerating-decelerating force. The acceleration-deceleration forces which occur during whiplash injury are staggering. Direct head trauma has been shown to produce forces between 10,000 and 15,000 N on the head and between 1,000 and 1,500 N on the neck, depending on the angle at which the object hits the head [104, 105]. Cervical capsular ligaments can become lax with as little as 5 N of force, although most studies report cervical ligament failure at around 100 N [30, 55, 91, 106]. Even low speed rear impact collisions at as little as 7 mph to 8 mph can cause the head to move roughly 18 inches at a force as great as 7 G in less than a quarter of a second [107]. Numerous experimental studies have suggested that certain features of injury mechanisms including direction and degree of acceleration and deceleration, translation and rotation forces, position and posture of head and neck, and even seat construction may be linked to the extent of cervical spine damage and to the actual structures damaged [23, 27, 35, 50, 61].
Debate over the veracity of PCS or WAD symptomology has persisted; however, there is no single explanation for the etiology of these disorders, especially since the onset and duration of symptoms can vary greatly among individuals. Many of the symptoms of PCS and WAD tend to increase over time, especially when those affected are engaged in physical or cognitive activity. Chronic neck pain is often described as a long-term result of both concussion and whiplash, indicating that the most likely structures to become injured during these traumas are the capsular ligaments of the cervical facet joints. In light of this, we propose that the best scientific anatomical explanation is cervical instability in the upper cervical spine, resulting from ligament injury (laxity).
Vertebrobasilar Insufficiency
The occipito-atlanto-axial complex has a unique anatomical relationship with the vertebral arteries. In the lower cervical spine, the vertebral arteries lie in a relatively straight-forward course as they travel through the transverse foramina from C3-C6. However, in the upper cervical spine the arteries assume a more serpentine-like course. The vertebral artery emerges from the transverse process of C2 and sweeps laterally to pass through the transverse foramen of C1 (atlas). From there it passes around the posterior border of the lateral mass of C1, at which point it is farthest from the midline plane at the level of C1 [108, 109]. This pathway creates extra space which allows for normal head rotation without compromising vertebral artery blood flow.
Considering the position of the vertebral arteries in the canals of the transverse processes in the cervical vertebrae, it is possible to see how head positioning can alter vertebral arterial flow. Even normal physiological neck movements (ie, neck rotation) have been shown to cause partial occlusion of up to 20% or 30% in at least one vertebral artery [110]. Studies have shown that contralateral neck rotation is associated with vertebral artery blood flow changes, primarily between the atlas and axis; such changes can also occur when osteophytes are present in the cervical spine [111, 112].
Proper blood flow in the vertebral arteries is crucial because these arteries travel up to form the basilar artery at the brainstem and provide circulation to the posterior half of the brain. When this blood supply is insufficient, vertebrobasilar insufficiency (VBI) can develop and cause symptoms, such as neck pain, headaches/migraines, dizziness, drop attacks, vertigo, difficulty swallowing and/or speaking, and auditory and visual disturbances. VBI usually occurs in the presence of atherosclerosis or cervical spondylosis, but symptoms can also arise when there is intermittent vertebral artery occlusion induced by extreme rotation or extension of the head [113, 114]. This mechanical compression of the vertebral arteries can occur along with other anomalies, including cervical osteophytes, fibrous bands, and osseous prominences [115, 116] These anomalies were seen in about half of the cases of vertebral artery injury after cervical manipulation, as reported in a recent review [117].
Whiplash injury itself has been shown to reduce vertebral artery blood flow and elicit symptoms of VBI [118, 119]. In one study, the authors concluded that patients with persistent vertigo or dizziness after whiplash injury are likely to have VBI if the injury was traumatic enough to cause a circulation disorder in the vertebrobasilar arterial system [118]. Other researchers have surmised that excessive cervical instability, especially of the upper cervical spine, can cause obstruction of the vertebral artery during neck rotation, thus compromising blood flow and triggering symptoms [120-122].
Barr�-Li�ou Syndrome
A lesser known, yet relatively common, cause of neck pain is Barr�-Li�ou syndrome. In 1925, Jean Alexandre Barr�, and in 1928, Yong Choen Li�ou, each independently described a syndrome presenting with headache, orbital pressure/pain, vertigo, and vasomotor disturbances and proposed that these symptoms were related to alterations in the posterior cervical sympathetic chain and vertebral artery blood flow in patients who had cervical spine arthritis or other arthritic disorders [123, 124]. Barr�-Li�ou syndrome is also referred to as posterior cervical syndrome or posterior cervical sympathetic syndrome because the condition is now presumed to develop more from disruption of the posterior cervical sympathetic nervous system, which consists of the vertebral nerve and the sympathetic nerve network surrounding it. Symptoms include neck pain, headaches, dizziness, vertigo, visual and auditory disturbances, memory and cognitive impairment, and migraines. It has been surmised that cervical arthritis or injury provokes an irritation of both the vertebral and sympathetic nerves. As a result, current treatment now centers on resolution of cervical instability and its effects on the posterior sympathetic nerves [124]. Other research has found an association between the sympathetic symptoms of Barr�-Li�ou and cervical instability and has documented successful outcomes in case reports when the instability was addressed by various means including prolotherapy [125].
Symptoms of Barr�-Li�ou syndrome also appear to develop after trauma. In one study, 87% of patients with a diagnosis of Barr�-Li�ou syndrome reported that they began experiencing symptoms after suffering a cervical injury, primarily in the mid-cervical region [126]; in a related study, this same region was found to exhibit more instability than other spinal segments [127] The various symptoms that characterize Barr�-Li�ou syndrome can also mimic symptoms of PCS or WAD, [128] which can pose a challenge for practitioners in making a definitive diagnosis (Fig. ?8). The diagnosis of Barr�-Li�ou syndrome is made on clinical grounds, as there is yet to be a definitive test to document irritation of the sympathetic nervous system.
Figure 8: Overlap in chronic symptomology between atlanto-axial instability, whiplash associated disorder, post-concussion syndrome, vertebrobasilar insufficiency, and Barr�-Li�ou syndrome. There is considerable overlap in symptoms amongst these conditions, possibly because they all appear to be due to cervical instability.
Other Sources of Cervical Pain
Various tensile forces place strains with differing deformations on a variety of viscoelastic spinal structures, including the ligaments, the annulus and nucleus of the intervertebral disc, and the spinal cord. Further to this, cadaver experiments have shown that the spinal cord and the intervertebral disc components carry considerably lower tensile forces than the spinal ligament column [129, 130]. Encapsulated mechanoreceptors and free nerve endings have been identified in the periarticular tissues of all major joints of the body including those in the spine, and in every articular tissue except cartilage [131]. Any innervated structure that has been injured by trauma is a potential chronic pain generator; this includes the intervertebral discs, facet joints, spinal muscles, tendons and ligaments [132-134].
The posterior ligamentous structures of the human spine are innervated by four types of nerve endings: pacinian corpuscles, golgi tendon organs, and ruffini and free nerve endings [40]. These receptors monitor joint excursion and capsular tension, and may initiate protective muscular reflexes that prevent joint degeneration and instability, especially when ligaments, such as the anterior and posterior longitudinal, ligamentum flavum, capsular, interspinous and supraspinous, are under too much tension [131, 135]. Collectively, the cervical region of the spinal column is at risk to sustain deformations at all levels and in all components, and when the threshold crosses a particular level at a particular component, injury is imminent owing to the relative increased flexibility or joint laxity.
Other Sources of Trauma
As described earlier, the nucleus pulposus is designed to sustain compression loads and the annulus fibrosus that surrounds it, to resist tension, shear and torsion. The stress in the annulus fibers is approximately 4-5 times the applied stress in the nucleus [136, 137]. In addition, annulus fibers elongate by up to 9% during torsional loading, but this is still well below the ultimate elongation at failure of over 25% [138]. Pressure within the nucleus is approximately 1.5 times the externally applied load per unit of disc area. As such, the nucleus is relatively incompressible, which causes the intervertebral disc to be susceptible to injury in that it bulges under loads – approximately 1 mm per physiological load [139]. As the disc degenerates on bulging (herniates), it looses elasticity, further compromising its ability to compress. Shock absorption is no longer spread or absorbed evenly by the surrounding annulus, leading to greater shearing, rotation, and traction stress on the disc and adjacent vertebrae. The severity of disc herniation can range from protrusion and bulging of the disc without rupture of the annulus fibrosus to disc extrusion, in which case, the annulus is perforated, leading to tearing of the structure.
Dr. Alex Jimenez’s Insight
“What type of treatment methods can provide effective relief from my chronic neck pain symptoms?”�The symptoms of chronic neck pain can be debilitating and can ultimately affect any individual’s ability to carry on with their everyday activities. While neck pain is a common symptom in a variety of injuries and/or conditions affecting the cervical spine, there are also a number of treatment methods available to help improve neck pain. However, some treatments also address stabilizing the cervical spine as well as healing damaged or injured tissues. Chiropractic care is a well-known alternative treatment option which has been demonstrated to help cure symptoms of neck pain at the source, according to several research studies.
Treatment Options
There are a number of treatment modalities for the management of chronic neck pain and cervical instability, including injection therapy, nerve blocks, mobilization, manipulation, alternative medicine, behavioral therapy, fusion, and pharmacologic agents such as NSAIDS and opiates. However, these treatments do not address stabilizing the cervical spine or healing ligament injuries, and thus, do not offer long-term curative options. In fact, cortisone injections are known to inhibit, rather than promote healing. As mentioned earlier in this paper, most treatments have shown limited evidence in their efficacy or are inconsistent in their results. In a systematic review of the literature from January 2000 to July 2012 on physical modalities for acute to chronic neck pain, acupuncture, laser therapy, and intermittent traction were found to provide moderate benefits [5].
The literature contains many reports on injection therapy for the treatment of chronic neck pain. Cervical interlaminar epidural injections with or without steroids may provide significant improvement in pain and function for patients with cervical disc herniation and radiculitis [140]. As a follow-up to its one-year results, a randomized, double-blind controlled trial found that the clinical effectiveness of therapeutic cervical medial branch blocks with or without steroids in managing chronic neck pain of facet joint origin provided significant improvement over a period of 2 years [141].
However, many other studies have had more nebulous results. In a systematic review of therapeutic cervical facet joint interventions, the evidence for both cervical radiofrequency neurotomy and cervical medial branch blocks is fair, and for cervical intra-articular injections with local anesthetic and steroids, the evidence is limited [142]. In a later corresponding systematic review, the same group of authors concluded that the strength of evidence for diagnostic facet joint nerve blocks is good (?75% pain relief), but stated the evidence is limited for dual blocks (50% to 74% pain relief), as well as for single blocks (50% to 74% pain relief) and (?75% pain relief.) [6]. In another systematic review evaluating cervical interlaminar epidural injections, the evidence indicated that the injection therapy showed significant effects in relieving chronic intractable pain of cervical origin; specific to long-term relief the indicated level of evidence was Level II-1 [143].
In the case of manipulative therapy, the results of a randomized trial disputed the hypothesis that supervised home exercises, combined or not with manual therapy, can be of benefit in treating non-specific chronic neck pain, as compared to no treatment [7]. The study found that there were no differences in primary or secondary outcomes among the three groups and that no significant change in health-related quality of life was associated with the preventive phase. Participants in the combined intervention group did not have less pain or disability and fared no better functionally than participants from the two other groups during the preventive phase of the trial. Another randomized clinical trial comparing the effects of applying joint mobilization at symptomatic and asymptomatic cervical levels in patients with chronic nonspecific neck pain was inconclusive in that there was no significant difference in pain intensity immediately after treatment between groups during resting position, painful active movement, or vertebral palpation [8]. Massage therapy had similar inconclusive results. Evidence was reported as �not strong� [144] in one randomized trial comparing groups receiving massage treatment for neck pain versus those reading a self-care book, while another found that cupping massage was no more effective than progressive muscle relaxation in reducing chronic non-specific neck pain [9]. Acupuncture appears to have better results in relieving neck pain but leaves questions as to the effects on the autonomic nervous system, suggesting that acupuncture points per se have different physical effects according to location [145].
Cervical disc herniation is a major source of chronic neck and spinal pain and is generally treated by either surgery or epidural injections, but their effectiveness continues to be debatable. In a randomized, double-blind, controlled clinical trial assigning patients to treatment with epidural injections with lidocaine or lidocaine mixed with betamethasone, 72% of patients in the local anesthetic group and 68% of patients in the local anesthetic with steroid group had at least a 50% improvement in pain and disability at 2 years, indicating that either protocol may be beneficial in alleviating chronic pain from cervical disc herniation [146].
In a systematic review of pharmacological interventions for neck pain, Peloso, et al. [147] reported that, aside from evidence in one study of a small immediate benefit for the psychotropic agent eperison hydrochloride (a muscle relaxant), most studies had low to very low quality methodologic evidence. Furthermore, they found evidence against a long-term benefit for medial branch block of facet joints with steroids and against a short-term benefit for botulinum toxin-A compared to saline, concluding that there is a lack of evidence for most pharmacological interventions.
Collectively, these interventions for the treatment of chronic neck pain may each offer temporary relief, but many fall short of a cure. Aside from these conventional treatment options, there are pain medications and pain patches, but their use is controversial because they offer little restorative value and often lead to dependence. If joint instability is the fundamental problem causing chronic neck pain and its associated autonomic symptoms, prolotherapy may be a treatment approach that meets this challenge.
Prolotherapy for Cervical Instability
To date, there is no consensus on the diagnosis of cervical spine instability or on traditional treatments that relieve chronic neck pain. In such cases, patients often seek out alternative treatments for pain and symptom relief. Prolotherapy is one such treatment which is intended for acute and chronic musculoskeletal injuries, including those causing chronic neck pain related to underlying joint instability and ligament laxity (Fig. ?9).
Figure 9: Stress-strain curve for ligaments and tendons. Ligaments can withstand forces and revert back to their original position up to Point C. At this point, prolotherapy treatment may succeed in tightening the tissue. Once the force continues past Point C. the ligament becomes permanently elongated or stressed.
Chronic neck pain and cervical instability are particularly difficult to treat when capsular ligament laxity is the cause because ligament cartilage is notoriously slow in healing due to a lack of blood supply. Most treatment options do not address this specific problem, and therefore, have limited success in providing a long-term cure.
Whiplash is a prime example because it often results in ligament laxity. In a five-part series evaluating the strength of evidence supporting WAD therapies, Teasell, et al. [10, 148-151] report that there is insufficient evidence to support any treatment for subacute WAD, stating that radiofrequency neurotomy may be the most effective treatment for chronic WAD. Furthermore, they state that immobilization with a soft collar is ineffective to the point of impeding recovery, saying that activation-based therapy is recommended instead, a conclusion similar to that of Hauser et al. [40] For chronic WAD, exercise programs were the most effective noninvasive treatment and radiofrequency neurotomy, the most effective of surgical or injection-based interventions, although evidence was not strong enough to establish the efficacy of any one treatment [10].
Prolotherapy is referred to as a regenerative injection technique (RIT) because it is based on the premise that the regenerative/reparative healing process consists of three overlapping phases: inflammatory, proliferative with granulation, and remodeling with contraction (Fig. ?10) [152]. The prolotherapy technique involves injecting an irritating solution (usually a dextrose/sugar solution) at painful ligament and tendon attachment sites to produce a mild inflammatory response. Such a response initiates a healing cascade that duplicates the natural healing process of poorly vascularized tissue (ligaments, tendons, and cartilage) [40, 153]. In doing so, tensile strength, elasticity, mass and load-bearing capacity of collagenous connective tissues become increased [152]. This occurs because the increased glucose concentration causes increases in cell protein synthesis, DNA synthesis, cell volume, and proliferation, all of which stimulate ligament size and mass and ligament-bone junction strength, as well as the production of growth factors, which are essential for ligament repair and growth [154].
Figure 10: The biology of prolotherapy.
While the most studied type of prolotherapy is the Hackett-Hemwall procedure which uses dextrose as the proliferant, there are multiple other choices that are suitable, such as polidocanol, manganese, human growth hormone, and zinc. In addition to the Hackett-Hemwall procedure, there is another procedure called cellular prolotherapy, which involves the use of a patient�s own cells from blood, bone marrow, or adipose tissue as the proliferant to generate healing.
It is important to note that prolotherapy not only involves the treatment of joints, but also the associated tendon and ligament attachments surrounding them; hence, it is a comprehensive and highly effective means of wound healing and pain resolution. The Hackett-Hemwall prolotherapy technique was developed in the 1950s and is being transitioned into mainstream medicine due to an increasing number of studies reporting positive outcomes [155-158].
Prolotherapy has a long history of being used for whiplash-type soft tissue injuries of the neck. In separate studies, Hackett and his colleagues early on had remarkably successful outcomes in treating ligament injuries; more than 85% of patients with cervical ligament injury-related symptoms, including those with headache or WAD, reported they had minor to no residual pain or related symptoms after prolotherapy [125, 159, 160]. Similar favorable outcomes for resolving neck pain were reported recently by Hauser, et al. [161]. Hooper, et al. also reported on a case series [162] in which patients with whiplash received intra-articular injections (prolotherapy) into each zygapophysial (facet)
joint and attained consistently improved scores in the Neck Disability Index (NDI) at 2, 6 and 12 months post treatment; average change in Neck Disability Index (NDI) was significant (13.77; p < 0.001) at baseline versus 12 months. Specific to cervical instability, Centeno, et al. [163] performed fluoro-scopically guided prolotherapy and reported that stabilization of the cervical spine with prolotherapy correlated with symptom relief, as depicted in blinded pre and post radiographic readings. Prolotherapy has also been found effective for other ligament injuries, including the lower back, [164-166] knee, [167-169] and other peripheral joints, [170-172] as well as congenital systemic ligament laxity conditions [173].
Evidence that prolotherapy induces the repair of ligaments and other soft tissue structures has been reported in both animal and human studies. Animal research conducted by Hackett [174] demonstrated that proliferation and strengthening of tendons occurred, while Liu and associates [175] found that prolotherapy injections to rabbit ligaments increased ligamentous mass (44%), thickness (27%), as well as ligament-bone junction strength (28%) over a six-week period. In a study on human subjects, Klein et al. [176] used electron microscopy and found an average increase in ligament diameter from 0.055 �m to 0.087 �m after prolotherapy, as shown in biopsies of posterior sacroi-liac ligaments. They also found a linear ligament orientation similar to what is found in normal ligaments. In a case study, Auburn, et al. [177] documented a 27% increase in iliolum-bar ligament size after prolotherapy, via ultrasound.
Studies have also been published on the use of prolotherapy for resolving chronic pain, [152, 178, 179] as well as for conditions specifically related to joint instability in the cervical spine [163, 180] In our own pain clinic, we have used prolotherapy successfully on patients who had chronic pain in the shoulder, elbow, low back, hip, and knee [181-186].
Conclusion
The capsular ligaments are the main stabilizing structures of the facet joints in the cervical spine and have been implicated as a major source of chronic neck pain. Such pain often reflects a state of instability in the cervical spine and is a symptom common to a number of conditions such as disc herniation, cervical spondylosis, whiplash injury and whiplash associated disorder, postconcussion syndrome, vertebrobasilar insufficiency, and Barr�-Li�ou syndrome.
When the capsular ligaments are injured, they become elongated and exhibit laxity, which causes excessive movement of the cervical vertebrae. In the upper cervical spine (C0-C2), this can cause symptoms such as nerve irritation and vertebrobasilar insufficiency with associated vertigo, tinnitus, dizziness, facial pain, arm pain, and migraine headaches. In the lower cervical spine (C3-C7), this can cause muscle spasms, crepitation, and/or paresthesia in addition to chronic neck pain. In either case, the presence of excessive motion between two adjacent cervical vertebrae and these associated symptoms is described as cervical instability.
Therefore, we propose that in many cases of chronic neck pain, the cause may be underlying joint instability due to capsular ligament laxity. Furthermore, we contend that the use of comprehensive Hackett-Hemwall prolotherapy appears to be an effective treatment for chronic neck pain and cervical instability, especially when due to ligament laxity. The technique is safe and relatively non-invasive as well as efficacious in relieving chronic neck pain and its associated symptoms. Additional randomized clinical trials and more research into its use will be needed to verify its potential to reverse ligament laxity and correct the attendant cervical instability.
Acknowledgements
Declared none.
Conflict of Interest
Ms. Woldin and Ms. Sawyer have nothing to declare. Dr. Hauser and Ms. Steilen declare that they perform prolotherapy at Caring Medical Rehabilitation Services.
Dr. Alex Jimenez’s Insight
“I was diagnosed with a whiplash-associated disorder after reporting chronic neck pain symptoms following an automobile accident. What form of care can help me manage the persistent symptoms?”�In order to manage chronic neck pain symptoms, not only is it essential for you to seek immediate medical attention from the proper healthcare professional, its also important to understand the mechanism of injury behind your persistent symptoms. Tendons, ligaments and other structures surrounding the cervical spine, such as the facet joints, can become damaged or injured during an auto accident and their care must be consistent to achieve overall recovery. Many healthcare professionals can provide patients with individualized guidelines on the management of their whiplash-associated disorders and chronic neck pain.
Facet Joint Kinematics and Injury Mechanisms During Simulated Whiplash
Abstract
Study Design: Facet joint kinematics and capsular ligament strains were evaluated during simulated whiplash of whole cervical spine specimens with muscle force replication.
Objectives: To describe facet joint kinematics, including facet joint compression and facet joint sliding, and quantify peak capsular ligament strain during simulated whiplash.
Summary of Background Data: Clinical studies have implicated the facet joint as a source of chronic neck pain in whiplash patients. Prior in vivo and in vitro biomechanical studies have evaluated facet joint compression and excessive capsular ligament strain as potential injury mechanisms. No study has comprehensively evaluated facet joint compression, facet joint sliding, and capsular ligament strain at all cervical levels during multiple whiplash simulation accelerations.
Methods: The whole cervical spine specimens with muscle force replication model and a bench-top trauma sled were used in an incremental trauma protocol to simulate whiplash of increasing severity. Peak facet joint compression (displacement of the upper facet surface towards the lower facet surface), facet joint sliding (displacement of the upper facet surface along the lower facet surface), and capsular ligament strains were calculated and compared to the physiologic limits determined during intact flexibility testing.
Results: Peak facet joint compression was greatest at C4-C5, reaching a maximum of 2.6 mm during the 5 g simulation. Increases over physiologic limits (P < 0.05) were initially observed during the 3.5 g simulation. In general, peak facet joint sliding and capsular ligament strains were largest in the lower cervical spine and increased with impact acceleration. Capsular ligament strain reached a maximum of 39.9% at C6-C7 during the 8 g simulation.
Conclusions: Facet joint components may be at risk for injury due to facet joint compression during rear-impact accelerations of 3.5 g and above. Capsular ligaments are at risk for injury at higher accelerations.
The Treatment of Neck Pain-Associated Disorders and Whiplash-Associated Disorders: A Clinical Practice Guideline
Abstract
Objective: The objective was to develop a clinical practice guideline on the management of neck pain-associated disorders (NADs) and whiplash-associated disorders (WADs). This guideline replaces 2 prior chiropractic guidelines on NADs and WADs.
Methods: Pertinent systematic reviews on 6 topic areas (education, multimodal care, exercise, work disability, manual therapy, passive modalities) were assessed using A Measurement Tool to Assess Systematic Reviews (AMSTAR) and data extracted from admissible randomized controlled trials. We incorporated risk of bias scores in the Grading of Recommendations Assessment, Development, and Evaluation. Evidence profiles were used to summarize judgments of the evidence quality, detail relative and absolute effects, and link recommendations to the supporting evidence. The guideline panel considered the balance of desirable and undesirable consequences. Consensus was achieved using a modified Delphi. The guideline was peer reviewed by a 10-member multidisciplinary (medical and chiropractic) external committee.
Results: For recent-onset (0-3 months) neck pain, we suggest offering multimodal care; manipulation or mobilization; range-of-motion home exercise, or multimodal manual therapy (for grades I-II NAD); supervised graded strengthening exercise (grade III NAD); and multimodal care (grade III WAD). For persistent (>3 months) neck pain, we suggest offering multimodal care or stress self-management; manipulation with soft tissue therapy; high-dose massage; supervised group exercise; supervised yoga; supervised strengthening exercises or home exercises (grades I-II NAD); multimodal care or practitioner’s advice (grades I-III NAD); and supervised exercise with advice or advice alone (grades I-II WAD). For workers with persistent neck and shoulder pain, evidence supports mixed supervised and unsupervised high-intensity strength training or advice alone (grades I-III NAD).
Conclusions:�A multimodal approach including manual therapy, self-management advice, and exercise is an effective treatment strategy for both recent-onset and persistent neck pain.
In conclusion, chronic neck pain, particularly that resulting from whiplash-associated disorders, can be treated using treatment methods which focus on the rehabilitation of the complex structures surrounding the cervical spine. Furthermore, by understanding chronic neck pain as it relates to cervical instability as well as its impact on capsular ligament laxity, patients can seek the proper treatment for their type of chronic neck pain, including whiplash. Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Neck Pain
Neck pain is a common complaint which can result due to a variety of injuries and/or conditions. According to statistics, automobile accident injuries and whiplash injuries are some of the most prevalent causes for neck pain among the general population. During an auto accident, the sudden impact from the incident can cause the head and neck to jolt abruptly back-and-forth in any direction, damaging the complex structures surrounding the cervical spine. Trauma to the tendons and ligaments, as well as that of other tissues in the neck, can cause neck pain and radiating symptoms throughout the human body.
1. Childs J, Cleland J, Elliott J , et al. Neck pain clinical practice guidelines linked to the international classification of functioning, disability, and health from the orthopaedic section of the American Physical Therapy Association. J Orthop Sports Phys Ther. 2008;38(9): A1�34. [PubMed]
2. C�t� P, Cassidy JD, Carroll LJ, Kristman V. The annual incidence and course of neck pain in the general population a population based cohort study. Pain. 2004;112(3): 267�73. [PubMed]
3. Hogg-Johnson S, van der Velde G, Carroll LJ , et al. The burden and determinants of neck pain in the general population. Eur Spine J. 2008;17(Suppl 1 ): 39�51.
4. Childs JD, Fritz JM, Flynn TW , et al. A clinical prediction rule to identify patients with low back pain most likely to benefit from spinal manipulation a validation study. Ann Intern Med. 2004;141(12): 920�8. [PubMed]
5. Graham N, Gross AR, Carlesso LC , et al. ICON. An ICON overview on physical modalities for neck pain and associated disorders. Open Orthop J. 2013;7(Suppl 4 ): 440�60. [PMC free article][PubMed]
6. Onyewu O, Manchikanti L, Falco FJE , et al. An update of the appraisal of the accuracy and utility of cervical discography in chronic neck pain. Pain Physician. 2012;15: E777�806. [PubMed]
7. Martel J, Dugas C, Dubois JD, Descarreaux M. A randomised controlled trial of preventive spinal manipulation with and without a home exercise program for patients with chronic neck pain. BMC Musculoskelet Disord. 2011;12: 41. [PMC free article][PubMed]
8. Aquino RL, Caires PM, Furtado FC, Loureiro AV, Ferreira PH, Ferreira ML. Applying joint mobilization at different cervical vertebral levels does not influence immediate pain reduction in patients with chronic neck pain a randomized clinical trial. J Manual Manipulative Ther. 2009;17(2): 95�100. [PMC free article][PubMed]
9. Lauche R, Materdey S, Cramer H , et al. Effectiveness of home-based cupping massage compared to progressive muscle relaxation in patients with chronic neck pain-a randomized controlled trial. PLoS ONE. 2013;8(6): e65378. [PMC free article][PubMed]
10. Teasell RW, McClure JA, Walton D , et al. A research synthesis of therapeutic interventions for whiplash-associated disorder (WAD): part 1 – overview and summary. Pain Res Manage. 2010;15(5): 287�94. [PMC free article][PubMed]
11. Murphy DR, Hurwitz EL. Application of a diagnosis-based clinical decision guide in patients with neck pain. Chiropr Manual Ther. 2011;19: 19. [PMC free article][PubMed]
12. Suzuki F, Fukami T, Tsuji A, Takagi K, Matsuda M. Discrepancies of MRI findings between recumbent and upright positions in atlantoaxial lesion. Report of two cases. Eur Spine J. 2008;17(Suppl 2 ): S304�7. [PMC free article][PubMed]
13. R�ijezon U, Djupsj�backa M, Bj�rklund M, H�ger-Ross C, Grip H, Liebermann DG. Kinematics of fast cervical rotations in persons with chronic neck pain a cross-sectional and reliability study. BMC Musculoskelet Disord. 2010;11: 22. [PMC free article][PubMed]
14. Gelalis ID, Christoforou G, Arnaoutoglou CM, Politis AN, Manoudis G, Xenakis TA. Misdiagnosed bilateral C5-C6 dislocation causing cervical spine instability a case report. Cases J. 2009;2: 6149. [PMC free article][PubMed]
15. Taylor M, Hipp JA, Gertzbein SD, Gopinath S, Reitman CA. Observer agreement in assessing flexion-extension X-rays of the cervical spine, with and without the use of quantitative measurements of intervertebral motion. Spine J. 2007;7(6): 654�8. [PMC free article][PubMed]
17. Driscoll DR. Anatomical and biomechanical characteristics of upper cervical ligamentous structures a review. J Manipulative and Physiol Ther. 1987;10(3): 107�10. [PubMed]
18. Cusick JF, Yoganandan N. Biomechanics of the cervical spine part 4: major injuries. Clin Biomech. 2002;17(1): 1�20. [PubMed]
19. Nachemson A. The influence of spinal movements of the lumbar intradiscal pressure on the tensile stresses in the annulus fibrosus. Acta Orthop Scan. 1963;33: 183�207. [PubMed]
20. Zak M, Pezowicz C. Spinal sections and regional variations in the mechanical properties of the annulus fibrosus subjected to tensile loading. Acta Bioeng Biomech. 2013;15(1): 51�9. [PubMed]
21. Mercer S, Bogduk N. The ligaments and annulus fibrosus of human adult cervical intervertebral discs. Spine (Phila Pa 1976). 1999;24(7): 619�28. [PubMed]
22. Kuri J, Stapleton E. The spine at trial practical medicolegal concepts about the spine. http: //books.google.com/books?id=Gi6w jdftC7cC&pg=PA12&lpg=PA12&dq=cervical+spine+transverse+processes&source=bl&ots=tboGEQAnuB&sig=Vi4bIDA24bLxGWWEivgAmmlETFo&hl=en&sa=X&ei=YETZUteXHMTAyAGNkICIBQ&ved=0CDYQ6AEwAjgK#v=onepage&q=cervical%20spine%20transverse%20processes&f=false [Accessed April 14. 2014.
23. Jaumard N, Welch WC, Winkelstein BA. Spinal facet joint biomechanics and mechanotransduction in normal, injury, and degenerative conditions. J Biomech Eng. 2011;133(7): 071010. [PMC free article][PubMed]
24. Volle E. Functional magnetic resonance imaging video diagnosis of soft-tissue trauma to the craniocervical joints and ligaments. Int Tinnitus J. 2000;6(2): 134�9. [PubMed]
25. Pal GP, Routal RV, Saggu KG. The orientation of the articular facets of the zygapophyseal joints at the cervical and upper thoracic region. J Anat. 2001;198(Pt 4): 431�41. [PMC free article][PubMed]
26. Quinn KP, Lee KE, Ahaghotu CC, Winkelstein BA. Structural changes in the cervical facet capsular ligament potential contributions to pain following subfailure loading. Stapp Car Crash J. 2007;51: 169�87. [PubMed]
27. Panjabi MM, Bibu K, Cholewicki J. Whiplash injuries and the potential for mechanical instability. Eur Spine J. 1998;7: 484�92. [PMC free article][PubMed]
28. Zdeblick TA, Abitbol JJ, Kunz DN, McCabe RP, Garfin S. Cervical stability after sequential capsule resection. Spine (Phila Pa 1976). 1993;18: 2005�8. [PubMed]
29. Rasoulinejad P, McLachlin SD, Bailey SI, Gurr KR, Bailey CS, Dunning CE. The importance of the posterior osteoligamentous complex to subaxial cervical spine stability in relation to a unilateral facet injury. Spine J. 2012;12(7): 590�5. [PubMed]
30. Ivancic PC, Coe MP, Ndu AB , et al. Dynamic mechanical properties of intact human cervical spine ligaments. Spine J. 2007;7(6): 659�65. [PMC free article][PubMed]
31. DeVries NA, Gandhi AA, Fredericks DC, Grosland NM, Smucker JD. Biomechanical analysis of the intact and destabilized sheep cervical spine. Spine (Phila Pa 1976). 2012;37(16): E957�63. [PubMed]
32. Crisco JJ, 3rd, Oda T, Panjabi MM, Bueff HU, Dvor�k J, Grob D. Transections of the C1-C2 joint capsular ligaments in the cadaveric spine. Spine (Phila Pa 1976). 1991;16: S474�9. [PubMed]
33. Nadeau M, McLachlin SD, Bailey SI, Gurr KR, Dunning CE, Bailey CS. A biomechanical assessment of soft-tissue damage in the cervical spine following a unilateral facet injury. J Bone Joint Surg. 2012;94(21): e156. [PubMed]
34. Frank CB. Ligament structure, physiology, and function. J Musculoskelet Neuronal Interact. 2004;4(2): 199�201. [PubMed]
35. Chen HB, Yang KH, Wang ZG. Biomechanics of whiplash injury. Chin J Traumatol. 2009;12(5): 305�14. [PubMed]
36. Boswell MV, Colson JD, Sehgal N, Dunbar EE, Epter R. A systematic review of therapeutic facet joint interventions in chronic spinal pain. Pain Physician. 2007;10(1): 229�53. [PubMed]
37. Aprill C, Bogduk N. The prevalence of cervical zygapophyseal joint pain a first approximation. Spine (Phila Pa 1976). 1992;17: 744�7. [PubMed]
38. Barnsley L, Lord SM, Wallis BJ, Bogduk N. The prevalence of cervical zygapophaseal joint pain after whiplash. Spine (Phila Pa 1976). 1995;20: 20�5. [PubMed]
39. McLain RF. Mechanoreceptor endings in human cervical facet joints. Iowa Orthop J. 1993;13: 149�54. [PMC free article][PubMed]
40. Hauser RA, Dolan EE, Phillips HJ, Newlin AC, Moore RE Woldin BA. Ligament injury and healing a review of current clinical diagnostics and therapeutics. Open Rehabil J. 2013;6: 1�20.
41. Bergmann TF, Peterson DH. Chiropractic technique principles and procedures, 3rd ed. New York Mobby Inc. 1993
42. J�nsson H , Jr, Bring G, Rauschning W, Sahlstedt B. Hidden cervical spine injuries in traffic accident victims with skull fractures. J Spinal Disord. 1991;4(3): 251�63. [PubMed]
43. van Mameren H, Drukker J, Sanches H, Beursgens J. Cervical spine motion in the sagittal plane (I) range of motion of actually performed movements, an x-ray cinematographic study. Eur J Morphol. 1990;28(1): 47�68. [PubMed]
44. van Mameren H, Sanches H, Beursgens J, Drukker J. Cervical spine motion in the sagittal plane II positions of segmental averaged instantaneous centers of rotation-a cineradiographic study. Spine (Phila Pa 1976). 1992;17(5): 467�74. [PubMed]
45. Bogduk N, Mercer S. Biomechanics of the cervical spine 1: normal kinematics. Clin Biomech. 2000;15(9): 633�48. [PubMed]
46. Radcliff K, Kepler C, Reitman C, Harrop J, Vaccaro A. CT and MRI-based diagnosis of craniocervical dislocations the role of the occipitoatlantal ligament. Clin Orthop Rel Res. 2012;70(6): 1602�13. [PMC free article][PubMed]
47. Hino H, Abumi K, Kanayama M, Kaneda K. Dynamic motion analysis of normal and unstable cervical spines using cineradiography.an in vivo study. Spine (Phila Pa 1976). 1999;24(2): 163�8. [PubMed]
48. Dvorak J, Penning L, Hayek J, Panjabi MM, Grob D, Zehnder R. Functional diagnostics of the cervical spine using computer tomography. Neuroradiology. 1988;30: 132�7. [PubMed]
49. Antinnes J, Dvorak J, Hayek J, Panjabi MM, Grob D. The value of functional computed tomography in the evaluation of soft-tissue injury in the upper cervical spine. Eur Spine J. 1994;3: 98�101. [PubMed]
51. Levine A, Edwards CC. Traumatic lesions of the occipitoatlantoaxial complex. Clin Orthop Rel Res. 1989;239: 53�68. [PubMed]
52. Chang H, Gilbertson LG, Goel VK, Winterbottom JM, Clark CR, Patwardhan A. Dynamic response of the occipito-atlanto-axial (C0-C1-C2):complex in right axial rotation. J Orthop Res. 1992;10(3): 446�53. [PubMed]
53. Goel VK, Winterbottom JM, Schulte KR, Chang H , et al. Ligamentous laxity across C0-C1-C2 complex.Axial torque-rotation characteristics until failure. Spine (Phila Pa 1976). 1990;5(10): 990�6. [PubMed]
54. Goel VK, Clark CR, Gallaes K, Liu YK. Moment-rotation relationships of the ligamentous occipito-atlanto-axial complex. J Biomech. 1988;21(8): 673�80. [PubMed]
55. Quinn KP, Winkelstein BA. Cervical facet capsular ligament yield defines the threshold for injury and persistent joint-mediated neck pain. J Biomech. 2007;40(10): 2299�306. [PubMed]
56. Winkelstein BA, Santos DG. An intact facet capsular ligament modulates behavioral sensitivity and spinal glial activation produced by cervical facet joint tension. Spine (Phila Pa 1976). 2008;33(8): 856�62. [PubMed]
57. Stemper BD, Yoganandan N, Pintar FA. Effects of abnormal posture on capsular ligament elongations in a computational model subjected to whiplash loading. J Biomech Eng. 2005;38(6): 1313�23. [PubMed]
58. Ivancic PC, Ito S, Tominaga Y , et al. Whiplash causes increased laxity of cervical capsular ligament. Clin Biomech. 2008;23(2): 159�65. [PMC free article][PubMed]
59. IASP Spinal pain, section 1: spinal and radicular pain syndromes. http: //www.iasp-pain.org/AM/Template.cfm?Section=Classification _of_Chronic_Pain&Template=/CM/ContentDisplay.cfm&ContentID=16268. Accessed Nov 25. 2013.
60. Argenson C, Lovet J, Sanouiller JL, de Peretti F. Traumatic rotatory displacement of the lower cervical spine. Spine (Phila Pa 1976). 1988;3(7): 767�73. [PubMed]
61. Tominaga Y, Maak TG, Ivancic PC, Panjabi MM, Cunningham BW. Head-turned rear impact causing dynamic cervical intervertebral foraminal narrowing implications for ganglion and nerve root injury. J Neurosurg Spine. 2006;4: 380�7. [PubMed]
62. Caridi JM, Pumberger M, Hughes AP. Cervical radiculopathy a review. HSS J. 2011;7(3): 265�72. [PMC free article][PubMed]
63. Kirkaldy-Willis HF, Farfan HF. Instability of the lumbar spine. Clin Orthop Rel Res. 1982;(165): 110�23. [PubMed]
64. Voorhies RM. Cervical spondylosis recognition, differential diagnosis, and management. Ochsner J. 2001;3(2): 78�84. [PMC free article][PubMed]
66. Aker PD, Gross AR, Goldsmith CH, Peloso P. Conservative management of mechanical neck pain systematic overview and meta-analysis. BMJ. 1996;313: 1291�6. [PMC free article][PubMed]
67. McCormack BM, Weinstein PR. Cervical spondylosis an update. West J Med. 1996;165: 43�51. [PMC free article][PubMed]
68. Peng BG, Hou SX, Shi Q, Jia LS. The relationship between cartilage end-plate calcification and disc degeneration an experimental study. Chin Med J. 2001;114: 308�12. [PubMed]
69. Mauro A, Eisenstein SM, Little C , et al. Are animal models useful for studying human disc disorders/degeneration?. Eur Spine J. 2008;17: 2�19. [PMC free article][PubMed]
70. Oxland TR, Panjabi MM, Southern EP, Duranceau JS. An anatomic basis for spinal instability a porcine trauma model. J Orthop Res. 1991;9(3): 452�62. [PubMed]
71. Wang JY, Shi Q, Lu WW , et al. Cervical intervertebral disc degeneration induced by unbalanced dynamic and static forces a novel in vivo rat model. Spine (Phila Pa 1976) 2006;Jun 15; 31: 1532�38. [PubMed]
72. Schulte K, Clark CR, Goel VK. Kinematics of the cervical spine following discectomy and stabilization. Spine (Phila Pa 1976). 1989;(10): 1116�21. [PubMed]
73. Kelly MP, Mok JM, Frisch RF, Tay BK. Adjacent segment motion after anterior cervical discectomy and fusion versus prodisc-c cervical total disk arthroplasty analysis from a randomized, controlled trial. Spine (Phila Pa 1976) 2011; 36(15): 1171�9. [PubMed]
74. Bydon M, Xu R, Macki M , et al. Adjacent segment disease after anterior cervical discectomy and fusion in a large series. Neurosurgery. 2014;74: 139�46. [PubMed]
75. Song JS, Choi BW, Song KJ. Risk factors for the development of adjacent segment disease following anterior cervical arthrodesis for degenerative cervical disease comparison between fusion methods. J Clin Neurosci. 2014;21(5): 794�8. [PubMed]
76. Johansson BH. Whiplash injuries can be visible by functional magnetic resonance imaging. Pain Res Manage. 2006;11(3): 197�9. [PMC free article][PubMed]
78. Barnsley L, Lord S, Bogduk N. Whiplash injury. Pain. 1994;58: 283�307. [PubMed]
79. Spitzer WO, Skovron ML, Salmi LR , et al. Scientific monograph of the Quebec task force on whiplash-associated disorders redefining “whiplash” and its management. Spine (Phila Pa 1976). 1995;20(8) Suppl : 1S�73. [PubMed]
80. Kaale BR, Krakenes J, Albrektsen G, Wester K. Head position and impact direction in whiplash injuries associations with MRI-verified lesions of ligaments and membranes in the upper cervical spine. J Neurotrauma. 2005;22(11): 1294�302. [PubMed]
81. Falco FJ, Erhart S, Wargo BW , et al. Systematic review of diagnostic utility and therapeutic effectiveness of cervical facet joint interventions. Pain Physician. 2009;12(2): 323�44. [PubMed]
82. Winkelstein BA, Nightingale RW, Richardson WJ, Myers BS, editors. Proceedings of the 43rd Stapp Car Crash Conference. Saniego CA.: 1999. Cervical facet joint mechanics its application to whiplash injury.
83. Lee DJ, Winkelstein BA. The failure response of the human cervical facet capsular ligament during facet joint retraction. J Biomech. 2012;45(14): 2325�9. [PubMed]
84. Bogduk N, Yoganandan N. Biomechanics of the cervical spine part 3: minor injuries. Clin Biomech. 2001;16(4): 267�75. [PubMed]
85. Lord SM, Barnsley L, Wallis BJ, Bogduk N. The prevalence of chronic cervical zygapophysial joint pain after whiplash. Spine (Phila Pa 1976). 1995;20(1): 20�5. [PubMed]
86. Lee KE, Davis MB, Mejilla RM, Winkelstein BA. In vivo cervical facet capsule distraction mechanical implications for whiplash and neck pain. Stapp Car Crash J. 2004;48: 373�95. [PubMed]
87. Tominaga Y, Ndu AB, Coe MP , et al. Neck ligament strength is decreased following whiplash trauma. BMC Musculoskelet Disord. 2006;7: 103. [PMC free article][PubMed]
88. Stokes IA, Frymoyer JW. Segmental motion and instability. Spine (Phila Pa 1976). 1987;7: 688�91. [PubMed]
89. Stokes IA, Iatridis JC. Mechanical conditions that accelerate intervertebral disc degeneration overload versus immobilization. Spine (Phila Pa 1976). 2004;29: 2724�32. [PubMed]
90. Veres SP, Robertson PA, Broom ND. The influence of torsion on disc herniation when combined with flexion. Eur Spine J. 2010;19: 1468�78. [PMC free article][PubMed]
91. Winkelstein BA, Nightingale RW, Richardson WJ, Myers BS. The cervical facet capsule and its role in whiplash injury a biomechanical investigation. Spine (Phila Pa 1976). 2000;25(10): 1238�46. [PubMed]
92. Siegmund GP, Myers BS, Davis MB, Bohnet HF, Winkelstein BA. Mechanical evidence of cervical facet capsule injury during whiplash a cadaveric study using combined shear, compression, and extension loading. Spine (Phila Pa 1976). 2001;26(19): 2095�101. [PubMed]
93. Siegmund GP, Davis MB, Quinn KP , et al. Head-turned postures increase the risk of cervical facet capsule injury during whiplash. Spine (Phila PA 1976). 2008;33(15): 1643�9. [PubMed]
94. Storvik SG, Stemper BD. Axial head rotation increases facet joint capsular ligament strains in automotive rear impact. Med Bio Eng Comput. 2011;49(2): 153�61. [PubMed]
95. Centers for Disease Control Injury prevention & control traumatic brain injury. http: //www.cdc.gov/TraumaticBrainInjury/statistics. html [Accessed March 4. 2014.
96. Centers for Disease Control Concussion.facts for physicians booklet. http: //www.cdc.gov/concussion/HeadsUp/physicians_too l_kit.html [Accessed March 4. 2014.
97. Giza C, Hovda D. The neurometabolic cascade of concussion. J Athl Train. 2001;36: 228�35. [PMC free article][PubMed]
98. Cuccurullo S, Elovic E, Baerga E, Cuccurullo S, editors. Demos Medical Publishing: New York; 2004. Mild traumatic brain injury and postconcussive syndrome Physical medicine and rehabilitation board review.
99. Leddy J, Sandhu H, Sodhi V, Baker J, Willer B. Rehabilitation of concussion and post-concussion syndrome. Sports Health. 2012;4(2): 147�54. [PMC free article][PubMed]
100. ICD-10, International statistical classification of diseases and related health problems 10th revision. World Health Organization. [PubMed]
101. Boake C, McCauley SR, Levin HS , et al. Diagnostic criteria for postconcussional syndrome after mild to moderate traumatic brain injury. J Neuropsych Clin Neurosci. 2005;17: 350�6. [PubMed]
102. Couch Jr, Bears C. Chronic daily headache in the posttrauma syndrome relation to extent of head injury. Headache. 2001;41: 559�64. [PubMed]
103. Barkhoudarian G, Hovda DA, Giza CC. The molecular pathophysiology of concussive brain injury. Clin Sports Med. 2011;30: 33�48. [PubMed]
104. Saari A, Dennison CR, Zhu Q , et al. Compressive follower load influences cervical spine kinematics and kinetics during simulated head-first impact in an in vitro model. J Biomech Eng. 2013;135(11): 111003. [PubMed]
105. Zhou S-W, Guo L-X, Zhang S-Q, Tang C-Y. Study on cervical spine injuries in vehicle side impact. Open Mech Eng J. 2010;4: 29�35.
106. Yoganandan N, Kumaresan S, Pintar FA. Geometric and mechanical properties of human cervical spine ligaments. J Biomech Invest. 2000;122: 623�9. [PubMed]
107. Radanov BP, Sturzenegger M, Distefano G, Schnidrig A, Aljinovic M. Factors influencing recovery from headache after common whiplash. BMJ. 1993;307: 652�5. [PMC free article][PubMed]
108. Martins J, Pratesi R, Bezerra A. Anatomical relationship between vertebral arteries and cervical vertebrae a computerized tomography study. Int J Morph. 2003;21: 123�9.
109. Cacciola F, Phalke U, Goel A. Vertebral artery in relationship to C1-C2 vertebrae an anatomical study. Neurology India. 2004;52: 178�84. [PubMed]
110. Mitchell JA. Changes in vertebral artery blood flow following normal rotation of the cervical spine. J Manip Physiol Ther. 2003;26: 347�51. [PubMed]
111. Mitchell J. Vertebral artery blood flow velocity changes associated with cervical spine rotation a meta-analysis of the evidence with implications for professional practice. J Man Manip Ther. 2009;17: 46�57. [PMC free article][PubMed]
112. Haynes M, Hart R, McGeachie J. Vertebral arteries and neck rotation doppler velocimeter interexaminer reliability. Ultrasound Med Biol. 2000;26: 57�62. [PubMed]
113. Kuether TA, Nesbit GM, Clark VM, Barnwell SL. Rotational vertebral artery occlusion a mechanism of vertebrobasilar insufficiency. Neurosurgery. 1997;41: 427�32. [PubMed]
114. Yang PJ, Latack JT, Gabrielsen TO, Knake JE, Gebarski SS, Chandler WF. Rotational vertebral artery occlusion at C1-C2. Am J Neuroradiol. 1985;6: 96�100. [PubMed]
115. Cape RT, Hogan DB. Vertebral-basilar insufficiency. Can Family Physician. 1983;29: 305�8. [PMC free article][PubMed]
116. Go G, Soon-Hyun H, Park IS, Park H. Rotational vertebral artery compression bow hunter’s syndrome. J Korean Neurosurg Soc. 2013;54: 243�5. [PMC free article][PubMed]
117. Gordin K, Hauser R. The case for utilizing prolotherapy as a promising stand-alone or adjunctive treatment for over-manipulation syndrome. J Applied Res. 2013;13: 1�28.
118. Endo K, Ichimaru K, Komagata M, Yamamoto K. Cervical vertigo and dizziness after whiplash injury. Eur Spine J. 2006;15: 886�90. [PMC free article][PubMed]
119. Creighton D, Kondratek M, Krauss J, Huijbregts P, Qu H. Ultrasound analysis of the vertebral artery during non-thrust cervical translatoric spinal manipulation. J Man Manip Ther. 2011;19: 84�90. [PMC free article][PubMed]
120. Inamasu J, Nakatsukasa M. Rotational vertebral artery occlusion associated with occipitoatlantal assimilation, atlantoaxial subluxation and basilar impression. Clin Neurol Neurosurg. 2013;115: 1520�3. [PubMed]
121. Kim HA, Yi HA, Lee CY, Lee H. Origin of isolated vertigo in rotational vertebral artery syndrome. Neuro Sci. 2011;32: 1203�7. [PubMed]
122. Yacovino DA1, Hain TC. Clinical characteristics of cervicogenic related dizziness and vertigo. Sem Neurol. 2013;33: 244�55. [PubMed]
123. Limousin CA. Foramen arcuale and syndrome of Barr�-Li�ou. Int Orthop. 1980;4(1): 19�23. [PubMed]
125. Hackett GS, Huang TC, Raferty A. Prolotherapy for headache; pain in the head and neck, and neuritis. Headache. 1962:3�11. [PubMed]
126. Tamura T. Cranial symptoms after cervical injury.Aetiology and treatment of the Barr -Li ou syndrome. J Bone Joint Surg Br. 1989;71B:282�7. [PubMed]
127. Qian J, Tian Y, Qiu GX, Hu JH. Dynamic radiographic analysis of sympathetic cervical spondylosis instability. Chin Med Sci J. 2009;24: 46�9. [PubMed]
128. Humphreys BK, Peterson C. Comparison of outcomes in neck pain patients with and without dizziness undergoing chiropractic treatment a prospective cohort study with 6 month follow-up. Chiropr Man Ther. 2013;21(1): 3. [PMC free article][PubMed]
129. Pintar FA, Yoganandan N, Myers T, Elhagediab A, Sances A ., Jr Biomechanical properties of human lumbar spine ligaments. J Biomech. 1992;25: 1351�6. [PubMed]
130. Yoganandan N, Pintar D, Maiman J, Cusick JF, Sances A , Jr, Walsh PR. Human head-neck biomechanics under axial tension. Med Eng Phys. 1996;18: 289�94. [PubMed]
131. Mc Lain R. Mechanoreceptors endings in human cervical facet joints. Iowa Orthop J. 1993;13: 149�54. [PMC free article][PubMed]
132. Steindler A, Luck J. Differential diagnosis of pain low in the back allocation of the source of pain by the procaine hydrochloride method. JAMA. 1938;110: 106�13.
133. Donelson R, Aprill C, Medcalf R, Grant W. A prospective study of centralization of lumbar and referred pain a predictor of symptomatic discs and anular competence. Diagn Ther. 1997;22: 1115�22. [PubMed]
134. Meleger AL, Krivickas LS. Neck and back pain musculoskeletal disorders. Neurol Clin. 2007;25: 419�38. [PubMed]
135. Silver P. Direct observation of changes in tension in the supraspinous and interspinous ligaments during flexion and extension of the vertebral column in man. J Anat. 1954:550�1.
136. Nachemson A. Lumbar intradiscal pressure.Experimental studies on post-mortem material. Acta Orthop Scand. 1960;43S:1�104. [PubMed]
137. Galante J. Tensile properties of the human lumbar annulus fibrosus. Acta Orthop Scand. 1967;100S:1�91. [PubMed]
138. Stokes IA. Surface strain on human intervertebral discs. J Orthop Res. 1987;5: 348�55. [PubMed]
139. Stokes IA. Bulging of the lumbar intervertebral discs non-contacting measurements of anatomical specimens. J Spinal Disord. 1988;1: 189�93. [PubMed]
140. Manchikanti L, Malla Y, Cash KA, McManus CD, Pampati V. Fluoroscopic cervical interlaminar epidural injections in managing chronic pain of cervical postsurgery syndrome preliminary results of a randomized, double-blind, active control trial. Pain Physician. 2012;15: 13�26. [PubMed]
141. Manchikanti L, Singh V, Falco FJE, Cash KA, Fellows B. Comparative outcomes of a 2-year follow-up of cervical medial branch blocks in management of chronic neck pain a randomized, double-blind controlled trial. Pain Physician. 2010;13: 437�50. [PubMed]
142. Falco FJE, Manchikanti L, Datta S , et al. Systematic review of the therapeutic effectiveness of cervical facet joint interventions an update. Pain Physician. 2012;15: E839�68. [PubMed]
143. Benyamin R, Singh V, Parr AT, Conn A, Diwan S, Abdi S. Systematic review of the effectiveness of cervical epidurals in the management of chronic neck pain. Pain Physician. 2009;12: 137�57. [PubMed]
145. Matsubara T, Arai Y-CP, Shiro Y , et al. Comparative effects of acupressure at local and distal acupuncture points on pain conditions and autonomic function in females with chronic neck pain. Evidence-Based Complementary Alternative Med. 2011; 2011: 543921. [PMC free article][PubMed]
146. Manchikanti L, Cash KA, Pampati V, Wargo BW, Malla Y. A randomized, double-blind, active control trial of fluoroscopic cervical interlaminar epidural injections in chronic pain of cervical disc herniation results of a 2-year follow-up. Pain Physician. 2013;16: 465�78. [PubMed]
147. Peloso PM, Khan M, Gross AR , et al. Pharmacological interventions including medical injections for neck pain an overview as part of the ICON project. Open Orthop J. 2013;7(Suppl 4 M8 ): 473�93. [PMC free article][PubMed]
148. Teasell RW, McClure JA, Walton D, Pretty J , et al. A research synthesis of therapeutic interventions for whiplash-associated disorder (WAD): part 2 – interventions for acute WAD. Pain Res Manage. 2010;15(5): 295�304. [PMC free article][PubMed]
149. Teasell RW, McClure JA, Walton D , et al. A research synthesis of therapeutic interventions for whiplash-associated disorder (WAD): part 3 – interventions for subacute WAD. Pain Res Manag. 2010;15(5): 305�12. [PMC free article][PubMed]
150. Teasell RW, McClure JA, Walton D , et al. A research synthesis of therapeutic interventions for whiplash-associated disorder (WAD): part 4 -noninvasive interventions for chronic WAD. Pain Res Manag. 2010;15(5): 313�22. [PMC free article][PubMed]
151. Teasell RW, McClure JA, Walton D , et al. A research synthesis of therapeutic interventions for whiplash-associated disorder (WAD): part 5 – surgical and injection-based interventions for chronic WAD. Pain Res Manag. 2010;15(5): 323�34. [PMC free article][PubMed]
152. Linetsky FS, Manchikanti L. Regenerative injection therapy for axial pain. Tech Reg Anaesh Pain Manag. 2005;9: 40�9.
153. Hackett G, editor. Oak Park IL. 5th ed. 1993. Ligament and tendon relaxation treated by prolotherapy ; pp. 94�6.
154. Goswami A. Prolotherapy. J Pain Palliative Care Pharmacother. 2012;26: 376�8. [PubMed]
155. Hauser RA, Maddela HS, Alderman D , et al. Journal of Prolotherapy international medical editorial board consensus statement on the use of prolotherapy for musculoskeletal pain. J Prolotherapy. 2011;3: 744�6.
156. Kim J. The effect of prolotherapy for osteoarthritis of the knee. J Korean Ac Rehab Med. 2002;26: 445�8.
157. Rabago D, Slattengren A, Zgierska A. Prolotherapy in primary care practice. Primary Care. 2010;37: 65�80. [PMC free article][PubMed]
158. Distel LM, Best TM. Prolotherapy a clinical review of its role in treating chronic musculoskeletal pain. PMR. 2011;3(6) Suppl1 : S78�81. [PubMed]
159. Hackett G. Prolotherapy in whiplash and low back pain. Postgrad Med. 1960:214�9. [PubMed]
160. Kafetz D. Whiplash injury and other ligamentous headache – its management with prolotherapy. Headache. 1963;3: 21�8. [PubMed]
161. Hauser RA, Hauser MA. Dextrose prolotherapy for unresolved neck pain an observational study of patients with unresolved neck pain who were treated with dextrose prolotherapy at an outpatient charity clinic in rural Illinois. Pract Pain Manage. 2007;10: 56�69.
162. Hooper RA, Frizzell JB, Faris P. Case series on chronic whiplash related neck pain treated with intraarticular zygapophysial joint regeneration injection therapy. Pain Physician. 2007;10: 313�8. [PubMed]
163. Centeno CJ, Elliott J, Elkins WL, Freeman M. Fluoroscopically guided cervical prolotherapy for instability with blinded pre and post radiographic reading. Pain Physician. 2005;8(1): 67�72. [PubMed]
164. Lee J, Lee HG, Jeong CW, Kim CM, Yoon MH. Effects of intraarticular prolotherapy on sacroiliac joint pain. Korean J Pain. 2009:229�33.
165. Cusi M, Saunders J, Hungerford B, Wisbey-Roth T, Lucas P, Wilson S. The use of prolotherapy in the sacroiliac joint. Brit J Sports Med. 2010;44: 100�4. [PubMed]
166. Naeim F, Froetscher L, Hirschberg GG. Treatment of chronic iliolumbar syndrome by infiltration of the iliolumbar ligament. West J Med. 1982;136: 372�4. [PMC free article][PubMed]
167. Kim J. Effects of prolotherapy on knee joint pain due to ligament laxity. J Korean Pain Soc. 2004;17: 47�5.
168. Reeves K, Hassanein KM. Long-term effects of dextrose prolotherapy for anterior cruciate laxity. Alternative Ther. 2003;9: 58�62. [PubMed]
169. Jo D. Effects of prolotherapy on knee joint pain due to ligament laxity. J Korean Pain Soc. 2004;17: 47�50.
170. Kim S. Effects of prolotherapy on chronic musculoskeletal disease. Korean J Pain. 2002;15: 121�5.
171. Wheaton MT, Jensen N. The ligament injury-osteoarthritis connection the role of prolotherapy in ligament repair and the prevention of osteoarthritis. J Prolotherapy. 2011;3: 790�812.
172. Refai H, Altahhan O, Elsharkawy R. The efficacy of dextrose prolotherapy for temporomandibular joint hypermobility a preliminary prospective, randomized double-blind, placebo-controlled clinical trial. J Oral Maxillofac Surg. 2011;69(12): 2962�70. [PubMed]
173. Hauser R, Phillips HJ. Treatment of joint hypermobility syndrome, including Ehlers-Danlos syndrome, with Hackett-Hemwall prolotherapy. J Prolotherapy. 2011;3: 612�29.
174. Hackett G. Joint stabilization an experimental, histologic study with comments on the clinical application in ligament proliferation. Am J Surg. 1955;89: 967�73. [PubMed]
175. Liu Y, Tipton C, Matthes R, Bedford TG, Maynard JA, Walmer HC. An in situ study of the influence of a sclerosing solution in rabbit medial collateral ligaments and its junction strength. Connect Tissue Res. 1983;11: 95�102. [PubMed]
176. Klein R, Dorman T, Johnson C. Proliferant injections for low back pain histologic changes of injected ligaments and objective measurements of lumbar spine mobility before and after treatment. J Neuro Ortho Med Surg. 1989;10: 123�6.
177. Auburn A, Benjamin S, Bechtel R, Matthews S. Increase in cross sectional area of the iliolumbar ligament using prolotherapy agents an ultrasonic case study. J Prolotherapy. 1999;1: 156�62.
178. Linetsky FS, Miguel R, Torres F. Treatment of cervicothoracic pain and cervicogenic headaches with regenerative injection therapy. Curr Pain Headache Rep. 2004;8(1): 41�8. [PubMed]
179. Alderman D. Prolotherapy for knee pain. Pract Pain Manage. 2007;7(6): 70�9.
180. Hooper RA, Yelland M, Fonstad P, Southern D. Prospective case series of litigants and non-litigants with chronic spinal pain treated with dextrose prolotherapy. Int Musculoskelet Med. 2011;33: 15�20.
181. Hauser RA. A retrospective study on Hackett-Hemwall dextrose prolotherapy for chronic shoulder pain at an outpatient charity clinic in rural Illinois. J Prolotherapy. 2009;4: 205�16.
182. Hauser RA, Hauser MA, Holian P. Hackett-Hemwall dextrose prolotherapy for unresolved elbow pain. Pract Pain Manage. 2009:14�26.
183. Hauser RA. Dextrose prolotherapy for unresolved low back pain a retrospective case series study. J Prolotherapy. 2009;3: 145�55.
184. Hauser RA. A retrospective study on Hackett-Hemwall dextrose prolotherapy for chronic hip pain at an outpatient charity clinic in rural Illinois. J Prolotherapy. 2009;(2): 76�88.
185. Hauser RA. A retrospective study on dextrose prolotherapy for unresolved knee pain at an outpatient charity clinic in rural Illinois. J Prolotherapy. 2009;(1): 11�21.
186. Hauser R, Woldin B. Treating osteoarthritic joints using dextrose prolotherapy and direct bone marrow aspirate injection therapy. Open Arthritis J. 2014;7: 1�9.
Back pain is one of the most common causes people visit their healthcare professional every year. A primary care physician is often the first doctor who can provide treatment for a variety of injuries and/or conditions, however, among those individuals seeking complementary and alternative treatment options for back pain, most people choose chiropractic care. Chiropractic care focuses on the diagnosis, treatment and prevention of trauma and disease of the musculoskeletal and nervous systems, by correcting misalignments of the spine through the use of spinal adjustments and manual manipulations.
Approximately 35% of individuals seek chiropractic treatment for back pain caused by automobile accidents, sports injuries, and a variety of muscle strains. When people suffer an trauma or injury as a result of an accident, however, they may first receive treatment for their symptoms of back pain in a hospital. Hospital outpatient care describes treatment which does not require an overnight stay at a medical facility. A research study conducted an analysis comparing the effects of chiropractic care and hospital outpatient management for back pain. The results are described in detail below.
Abstract
Objective: To compare the effectiveness over three years of chiropractic and hospital outpatient management for low back pain.
Design: Randomised allocation of patients to chiropractic or hospital outpatient management.
Setting: Chiropractic clinics and hospital outpatient departments within reasonable travelling distance of each other in I I centres.
Subjects: 741 men and women aged 18-64 years with low back pain in whom manipulation was not contraindicated.
Outcome measures: Change in total 0swestry questionnaire score and in score for pain and patient satisfaction with allocated treatment.
Results: According to total 0swestry scores improvement in all patients at three years was about 291/6 more in those treated by chiropractors than in those treated by the hospitals. The beneficial effect of chiropractic on pain was particularly clear. Those treated by chiropractors had more further treatments for back pain after the completion of trial treatment. Among both those initially referred from chiropractors and from hospitals more rated chiropractic helpful at three years than hospital management.
Conclusions: At three years the results confirm the findings of an earlier report that when chiropractic or hospital therapists treat patients with low back pain as they would in day to day practice those treated by chiropractic derive more benefit and long term satisfaction than those treated by hospitals.
Introduction
In 1990 we reported greater improvement in patients with low back pain treated by chiropractic compared with those receiving hospital outpatient management. The trial was “pragmatic” in allowing the therapists to treat patients as they would in day to day practice. At the time of our first report not all patients had been in the trial for more than six months. This paper presents the full results up to three years for all patients for whom follow up information from Oswestry questionnaires and for other outcomes was available for analysis. We also present data on pain from the questionnaire, which is by definition the main complaint prompting referral or self referral.
Methods
Methods were fully described in our first report. Patients initially referred or presenting either to a chiropractic clinic or in hospital were randomly allocated to be treated either by chiropractic or in hospital. A total of 741 patients started treatment. Progress was measured with the Oswestry questionnaire on back pain, which gives scores for I 0 sections for example, intensity of pain and difficulty with lifting, walking, and travelling. The result is expressed on a scale ranging from 0 (no pain or difficulties) to 100 (highest score for pain and greatest difficulty on all items). For an individual item, such as pain, scores range from 0 to 10. The main outcome measures are the changes in Oswestry score from before treatment to each follow up. At one, two, and three years patients were also asked about further treatment since the completion of their trial treatment or since the previous annual questionnaire. At the three year follow up patients were asked whether they thought their allocated trial treatment had helped their back pain.
In the random allocation of treatment minimisation was used within each centre to establish groups for the analysis of results according to initial referral clinic, length of current episode (more or less than ‘a month), presence or absence of a history of back pain, and an Oswestry score at entry of > 40 or <=40%.
Results were analysed on an intention to treat basis (subject to the availability of data at follow up as well as at entry for individual patients). Differences between mean changes were tested by unpaired t tests, and X2 tests were used to test for differences in proportions between the two treatment groups.
Dr. Alex Jimenez’s Insight
Chiropractic is a natural form of health care which purpose is to restore and maintain the function of the musculoskeletal and nervous systems, promoting spinal health and allowing the body to heal itself naturally. Our philosophy emphasizes on the treatment of the human body as a whole, rather than on the treatment of a single injury and/or condition. As an experienced chiropractor, my goal is to properly assess patients in order to determine which type of treatment will most effectively heal their individual type of health issue. From spinal adjustments and manual manipulations to physical activity, chiropractic care can help correct spinal misalignments that cause back pain.
Results
Follow up Oswestry questionnaires were returned by a consistently higher proportion of patients allocated to chiropractic than to hospital treatment. At six weeks, for example, they were returned by 95% and 89% of chiropractic and hospital patients, respectively and at three years by 77% and 70%.
Mean (SD) scores before treatment were 29-8 (14-2) and 28-5 (14-1) in the chiropractic and hospital treatment groups, respectively. Table I shows the differences between the mean changes in total Oswestry scores according to randomly allocated treatment group. The difference at each follow up is the mean change for the chiropractic group minus the mean change for the hospital group.
Positive differences therefore reflect more improvement (due to a greater change in score) in those treated by chiropractic than in hospital (negative differences the reverse). The 3-18 percentage point difference at three years in table I represents a 29% greater improvement in patients treated with chiropractic compared with hospital treatment, the absolute improvement in the two groups at this time being 14-1 and 10-9 percentage points, respectively. As in the first report those with short current episodes, a history of back pain, and initially high Oswestry scores tended to derive most benefit from chiropractic. Those referred by chiropractors consistently derived more benefit from chiropractic than those referred by hospitals.
Table II shows changes between the scores on pain intensity before treatment and the corresponding scores at the various follow up intervals. All these changes were positive that is, indicated improvement but were all significantly greater in those treated by chiropractic, including the changes early on that is, at six weeks and six months, when the proportions returning questionnaires were high. As with the results based on the full Oswestry score the improvement due to chiropractic was greatest in those initially referred by chiropractors, although there was also a non-significant improvement (ranging from 9% at six months to 34% at three years) due to chiropractic at each follow up interval in those referred by hospitals.
Other scores for individual items on the Oswestry index to show significant improvement attributable to chiropractic were ability to sit for more than a short time and sleeping (P=0’004 and 0 03, respectively, at three years), though the differences were not as consistent as for pain. Other scores (personal care, lifting, walking, standing, sex life, social life, and travelling) also nearly all improved more in the patients treated with chiropractic, though most of the differences were small compared with the differences for pain.
Higher proportions of patients allocated to chiropractic sought further treatment (of any kind) for back pain after completion of trial treatment than those managed in hospital. For example, between one and two years after trial entry 122/292 (42%) patients treated with chiropractic compared with 80/258 (3 1%) of hospital treated patients did so (Xl=6 8, P=0 0 1).
Table III shows the proportions of patients at three years who thought their allocated trial treatment had helped their back pain. Among those initially referred by hospitals as well as among those initially referred by chiropractors higher proportions treated by chiropractic considered that treatment had helped compared with those treated in hospital.
Key Messages
Back pain often remits spontaneously
Effective treatments for non-remitting episodes need to be more clearly identified
Chiropractic seems to be more effective than hospital management, possibly because more treatments are spread over longer time periods
A growing number of NHS purchasers are making complementary treatments, including chiropractic, available
Further trials to identify the effective components of chiropractic are needed
Discussion
The results at six weeks and six months shown in table I are identical with those in our first report, as all patients had then been followed up for six months. The findings at one year are similar as many patients had also been followed up then. The considerably larger numbers of patients with data now available at two and three years show smaller benefits at these intervals than previously, though these still significantly favour chiropractic. The substantial benefit of chiropractic on intensity of pain is evident early on and then persists. The consistently larger proportions lost to follow up throughout the trial in those treated in hospital than in those treated by chiropractic suggests greater satisfaction with chiropractic. This conclusion is supported (table III) by the higher proportions in each referral group considering chiropractic helpful by comparison with hospital treatment.
The main criticism of the trial after our first report centred on its “pragmatic” nature, particularly the larger number of chiropractic than hospital treatments and the longer period over which the chiropractic treatments were spread and which were deliberately allowed. These considerations and any consequences of the higher proportions of patients allocated to chiropractic who received further treatment in the later stages of follow up, however, do not apply to the results at six weeks and only apply to a limited extent at six months, when the proportions followed up were high and extra treatment had either not occurred at all or was not yet extensive. Benefits atributable to chiropractic were already evident (especially on pain, table II) at these shorter intervals.
We believe there is now more support for the need for “fastidious” trials focusing on specific components of management and on their feasibility. Meanwhile, the results of our trial show that chiropractic has a valuable part to play in the management of low back pain.
We thank Dr Iain Chalmers for commenting on an earlier draft of the paper. We thank the nurse coordinators, medical staff, physiotherapists, and chiropractors in the 11 centres for their work, and Dr Alan Breen of the British Chiropractic Association for his help. The centres were in Harrow Taunton, Plymouth, Bournemouth and Poole, Oswestry, Chertsey, Liverpool, Chelmsford, Birmingham, Exeter, and Leeds. Without the assistance of many staff members in each the trial could not have been completed.
Funding: Medical Research Council, the National Back Pain Association, the European Chiropractors Union, and the King Edward’s Hospital Fund for London.
Conflict of interest: None.
In conclusion,�after three years, the results of the research study comparing chiropractic care and hospital outpatient management for low back pain determined that people treated by chiropractic experienced more benefits as well as long-term satisfaction than those treated by hospitals. Because back pain is one of the most common�causes people visit their healthcare professional every year, its essential to seek the most effective type of health care. Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
References
Meade TW, Dyer S, Browne W, Townsend J, Frank AO. Low back pain of mechanical origin: randomised comparison of chiropractic and hospital outpatient treatment.�BMJ.�1990 Jun 2;300(6737):1431�1437.�[PMC free article]�[PubMed]
Fairbank JC, Couper J, Davies JB, O’Brien JP. The Oswestry low back pain disability questionnaire.�Physiotherapy.�1980 Aug;66(8):271�273.�[PubMed]
Pocock SJ, Simon R. Sequential treatment assignment with balancing for prognostic factors in the controlled clinical trial.�Biometrics.�1975 Mar;31(1):103�115.�[PubMed]
Additional Topics: Sciatica
Sciatica is referred to as a collection of symptoms rather than a single type of injury or condition. The symptoms are characterized as radiating pain, numbness and tingling sensations from the sciatic nerve in the lower back, down the buttocks and thighs and through one or both legs and into the feet. Sciatica is commonly the result of irritation, inflammation or compression of the largest nerve in the human body, generally due to a herniated disc or bone spur.
Understanding clinical and experimental evidence,�manual therapies, or manipulative therapies, are physical treatments that utilize skilled, hands-on techniques, such as manipulation and/or mobilization, used by a physical therapist, among other healthcare professionals, to diagnose and treat a variety of musculoskeletal and non-musculoskeletal injuries and conditions. Spinal manipulation/mobilization has been determined to be effective for back pain, neck pain, headache and migraine, as well as for several types of joint pain, including various other disorders in adults.
For additional notice, the following research study is a comprehensive summary of the scientific evidence regarding the effectiveness of manual therapies for the management of a variety of musculoskeletal and non-musculoskeletal injuries and conditions. The conclusions are based on the results of randomized clinical trials, widely accepted and primarily UK and United States evidence-based guidelines and the results of other randomized clinical trials not yet included.
Background
The impetus for this report stems from the media debate in the United Kingdom (UK) surrounding the scope of chiropractic care and claims regarding its effectiveness particularly for non-musculoskeletal conditions.
The domain of evidence synthesis is always embedded within the structure of societal values. What constitutes evidence for specific claims is framed by the experience, knowledge, and standards of communities. This varies substantially depending on jurisdictional restrictions by country and region. However, over the last several decades a strong international effort has been made to facilitate the systematic incorporation of standardized synthesized clinical research evidence into health care decision making.
Evidence-Based Healthcare (EBH)
EBH is about doing the right things for the right people at the right time. It does so by promoting the examination of best available clinical research evidence as the preferred process of decision making where higher quality evidence is available. This reduces the emphasis on unsystematic clinical experience and pathophysiological rationale alone while increasing the likelihood of improving clinical outcomes. The fact that randomized clinical trial (RCT) derived evidence of potentially effective interventions in population studies may not be translated in a straight forward manner to the management of individual cases is widely recognized. However, RCTs comprise the body of information best able to meet existing standards for claims of benefit from care delivery. The evidence provided by RCTs constitutes the first line of recommended action for patients and contributes, along with informed patient preference, in guiding care. Practice, as opposed to claims, is inherently interpretative within the context of patient values and ethical defensibility of recommendations. Indeed, the need to communicate research evidence, or its absence, to patients for truly informed decision-making has become an important area of health care research and clinical practice.
While some may argue that EBH is more science than art, the skill required of clinicians to integrate research evidence, clinical observations, and patient circumstances and preferences is indeed artful. It requires creative, yet informed improvisation and expertise to balance the different types of information and evidence, with each of the pieces playing a greater or lesser role depending on the individual patient and situation.
It has become generally accepted that providing evidence-based healthcare will result in better patient outcomes than non-evidence-based healthcare. The debate of whether or not clinicians should embrace an evidence-based approach has become muted. Put simply by one author: “…anyone in medicine today who does not believe in it (EBH) is in the wrong business.” Many of the criticisms of EBH were rooted in confusion over what should be done when good evidence is available versus when evidence is weak or nonexistent. From this, misunderstandings and misperceptions arose, including concerns that EBH ignores patient values and preferences and promotes a cookbook approach. When appropriately applied, EBH seeks to empower clinicians so they can develop fact-based independent views regarding healthcare claims and controversies. Importantly, it acknowledges the limitations of using scientific evidence alone to make decisions and emphasizes the importance of patients’ values and preferences in clinical decision making.
The question is no longer “should” we embrace EBH but “how”? With EBH comes the need for new skills including: efficient literature search strategies and the application of formal rules of evidence in evaluating the clinical literature. It is important to discern the role of the health care provider as an advisor who empowers informed patient decisions. This requires a healthy respect for which scientific literature to use and how to use it. “Cherry-picking” only those studies which support one’s views or relying on study designs not appropriate for the question being asked does not promote doing the right thing for the right people at the right time.
Perhaps most critical is the clinician’s willingness to change the way they practice when high quality scientific evidence becomes available. It requires flexibility born of intellectual honesty that recognizes one’s current clinical practices may not�really�be in the best interests of the patient. In some cases this will require the abandonment of treatment and diagnostic approaches once believed to be helpful. In other cases it will require the acceptance and training in new methods. The ever-evolving scientific knowledge base demands that clinicians be accepting of the possibility that what is “right” today might not be “right” tomorrow. EBH requires that clinicians’ actions are influenced by the evidence. Importantly a willingness to change must accompany the ability to keep up to date with the constant barrage of emerging scientific evidence.
Purpose
The purpose of this report is to provide a brief and succinct summary of the scientific evidence regarding the effectiveness of manual treatment as a therapeutic option for the management of a variety of musculoskeletal and non-musculoskeletal conditions based on the volume and quality of the evidence. Guidance in translating this evidence to application within clinical practice settings is presented.
Methods
For the purpose of this report, manual treatment includes spinal and extremity joint manipulation or mobilization, massage and various soft tissue techniques. Manipulation/mobilization under anaesthesia was not included in the report due to the procedure’s invasive nature. The conclusions of the report are based on the results of the most recent and most updated (spans the last five to ten years) systematic reviews of RCTs, widely accepted evidence-based clinical guidelines and/or technology assessment reports (primarily from the UK and US if available), and all RCTs not yet included in the first three categories. While critical appraisal of the included reviews and guidelines would be ideal, it is beyond the scope of the present report. The presence of discordance between the conclusions of systematic reviews is explored and described. The conclusions regarding effectiveness are based on comparisons with placebo controls (efficacy) or commonly used treatments which may or may not have been shown to be effective (relative effectiveness), as well as comparison to no treatment. The strength/quality of the evidence relating to the efficacy/effectiveness of manual treatment is graded according to an adapted version of the latest grading system developed by the US Preventive Services Task Force (see�http://www.ahrq.gov/clinic/uspstf/grades.htm). The evidence grading system used for this report is a slight modification of the system used in the 2007 Joint Clinical Practice Guideline on low back pain from the American College of Physicians and the American Pain Society.
Through a search strategy using the databases MEDLINE (PubMed), Ovid, Mantis, Index to Chiropractic Literature, CINAHL, the specialized databases Cochrane Airways Group trial registry, Cochrane Complementary Medicine Field, and Cochrane Rehabilitation Field, systematic reviews and RCTs as well as evidence-based clinical guidelines were identified. Search restrictions were human subjects, English language, peer-reviewed and indexed journals, and publications before October 2009. In addition, we screened and hand searched reference citations located in the reviewed publications. The description of the search strategy is provided in Additional file�1�(Medline search strategy).
Although findings from studies using a nonrandomized design (for example observational studies, cohort studies, prospective clinical series and case reports) can yield important preliminary evidence, the primary purpose of this report is to summarize the results of studies designed to address efficacy, relative efficacy or relative effectiveness and therefore the evidence base was restricted to RCTs. Pilot RCTs not designed or powered to assess effectiveness, and RCTs designed to test the immediate effect of individual treatment sessions were not part of the evidence base in this report.
The quality of RCTs, which have not been formally quality-assessed within the context of systematic reviews or evidence based guidelines, was assessed by two reviewers with a scale assessing the risk of bias recommended for use in Cochrane systematic reviews of RCTs. Although the Cochrane Collaboration handbook�http://www.cochrane.org/resources/handbook/�discourages that scoring be applied to the risk of bias tool, it does provide suggestion for how trials can be summarized. We have been guided by that suggestion and the adapted evidence grading system used in this report requires that we assess the validity and impact of the latest trial evidence. These additional trials are categorized as higher, moderate, or lower-quality as determined by their attributed risk of bias. For details, see Additional file�2�(The Cochrane Collaboration tool for assessing risk of bias and the rating of the bias for the purpose of this report).
The overall evidence grading system allows the strength of the evidence to be categorized into one of three categories:�high quality evidence, moderate quality evidence, and inconclusive (low quality) evidence. The operational definitions of these three categories follow below:
High quality evidence
The available evidence usually includes consistent results from well-designed, well conducted studies in representative populations which assess the effects on health outcomes.
The evidence is based on at least two consistent higher-quality (low risk of bias) randomized trials. This conclusion is therefore unlikely to be strongly affected by the results of future studies.
Moderate quality evidence
The available evidence is�sufficient�to determine the effectiveness relative to health outcomes, but confidence in the estimate is constrained by such factors as:
� The number, size, or quality of individual studies.
� Inconsistency of findings across individual studies.
� Limited generalizability of findings to routine practice.
� Lack of coherence in the chain of evidence.
The evidence is based on at least one higher-quality randomized trial (low risk of bias) with sufficient statistical power, two or more higher-quality (low risk of bias) randomized trials with some inconsistency; at least two consistent, lower-quality randomized trials (moderate risk of bias). As more information becomes available, the magnitude or direction of the observed effect could change, and this change may be large enough to alter the conclusion.
Inconclusive (low quality) evidence
The available evidence is�insufficient�to determine effectiveness relative to health outcomes. Evidence is insufficient because of:
� The limited number or power of studies.
� Important flaws in study design or methods (only high risk of bias studies available).
� Unexplained inconsistency between higher-quality trials.
� Gaps in the chain of evidence.
� Findings not generalizable to routine practice.
� Lack of information on important health outcomes
For the purpose of this report a determination was made whether the inconclusive evidence appears favorable or non-favorable or if a direction could even be established (unclear evidence).
Additionally, brief evidence statements are made regarding other non-pharmacological, non-invasive physical treatments (for example exercise) and patient educational interventions, shown to be effective and which can be incorporated into evidence-based therapeutic management or co-management strategies in chiropractic practices. These statements are based on conclusions of the most recent and most updated (within last five to ten years) systematic reviews of randomized clinical trials and widely accepted evidence-based clinical guidelines (primarily from the UK and US if available) identified through our search strategy.
Translating Evidence to Action
Translating evidence requires the communication of salient take-home messages in context of the user’s applications. There are two message applications for information derived from this work. First, the criteria for sufficiency of evidence differ depending on the context of the considered actions. Sufficient evidence to proffer claims of effectiveness is defined within the socio-political context�of ethics and regulation. Separate is the second application of evidence to inform decision making for individual patients. Where there is strength of evidence and the risk of bias is small, the preferred choices require little clinical judgment. Alternatively, when evidence is uncertain and/or there is higher risk of bias, then greater emphasis is placed on the patient as an active participant. This requires the clinician to effectively communicate research evidence to patients while assisting their informed decision-making.
In summary, the information derived within this report are directed to two applications 1) the determination of supportable public claims of treatment effectiveness for chiropractic care within the context of social values; and 2) the use of evidence information as a basis for individualized health care recommendations using the hierarchy of evidence (Figure 1).
Figure 1 Translating evidence to action.
Dr. Alex Jimenez’s Insight
The purpose of the research study was to provide substantial clinical and experimental evidence on the effectiveness of manual therapies, or manipulative therapies. Systematic reviews of randomized clinical trials, or RCTS, helped demonstrate the strength and quality of the evidence regarding the effectiveness of these, such as manipulation and/or mobilization. The results of the research study provide two additional purposes: to determine supportable public claims of treatment effectiveness for chiropractic care within the context of social values; and to utilize the information from the evidence as a basis for individualized healthcare recommendations using the hierarch of evidence. Detailed results of each research study method and conclusive outcome is recorded below regarding the effectiveness of manual therapies, including spinal manipulation and/or mobilization, among others.
Results
By September 2009, 26 categories of conditions were located containing RCT evidence for the use of manual therapy: 13 musculoskeletal conditions, four types of chronic headache and nine non-musculoskeletal conditions (Figure 2). We identified 49 recent relevant systematic reviews and 16 evidence-based clinical guidelines plus an additional 46 RCTs not yet included within the identified systematic reviews and guidelines. A number of other non-invasive physical treatments and patient education with evidence of effectiveness were identified including exercise, yoga, orthoses, braces, acupuncture, heat, electromagnetic field therapy, TENS, laser therapy, cognitive behavioral therapy and relaxation. The report presents the evidence of effectiveness or ineffectiveness of manual therapy as evidence summary statements at the end of the section for each condition and in briefer summary form in Figures 3, 4, 5, 6, and 7. Additionally, definitions and brief diagnostic criteria for the conditions reviewed are provided. Diagnostic imaging for many conditions is indicated by the presence of “red flags” suggestive of serious pathology. Red flags may vary depending on the condition under consideration, but typically include fractures, trauma, metabolic disorders, infection, metastatic disease, and other pathological disease processes contraindicative to manual therapy.
Figure 2 Categories of conditions included in this report.
Figure 3 Evidence summary of spinal conditions in adults.
Figure 4 Evidence summary of extremity conditions in adults.
Figure 5 Evidence summary of headache and other conditions in adults.
Figure 6 Evidence summary of non musculoskeletal conditions in adults.
Figure 7 Evidence summary of non musculoskeletal conditions in pediatrics.
Non-specific Low Back Pain (LBP)
Definition
Non-specific LBP is defined as soreness, tension, and/or stiffness in the lower back region for which it is not possible to identify a specific cause of pain.
Diagnosis
Diagnosis of non-specific LBP is derived from the patient’s history with an unremarkable neurological exam and no indicators of potentially serious pathology. Imaging is only indicated in patients with a positive neurological exam or presence of a “red flag”.
Evidence base for manual treatment
Systematic reviews (most recent)
Since 2004, five systematic reviews made a comprehensive evaluation of the benefit of spinal manipulation for non-specific LBP. Approximately 70 RCTs were summarized. The reviews found that spinal manipulation was superior to sham intervention and similar in effect to other commonly used efficacious therapies such as usual care, exercise, or back school. For sciatica/radiating leg pain, three reviews�found manipulation to have limited evidence. Furlan et al�concluded massage is beneficial for patients with subacute and chronic non-specific low-back pain based on a review of 13 RCTs.
Evidence-based clinical guidelines
Since 2006, four guidelines make recommendations regarding the benefits of manual therapies for the care of LBP: NICE, The American College of Physicians/American Pain Society , European guidelines for chronic LBP, and European guidelines for acute LBP. The number of RCTs included within the various guidelines varied considerably based on their scope, with the NICE guidelines including eight trials and The American College of Physicians/American Pain Society guidelines including approximately 70 trials. These guidelines in aggregate recommend spinal manipulation/mobilization as an effective treatment for acute, subacute, and chronic LBP. Massage is also recommended for the treatment of subacute and chronic LBP.
Recent randomized clinical trials not included in above
Hallegraeff et al�compared a regimen of spinal manipulation plus standard physical therapy to standard physical therapy for acute LBP. Overall there were no differences between groups for pain and disability post treatment. Prediction rules may have affected outcomes. This study had a high risk of bias.
Rasmussen et al found patients receiving extension exercise or receiving extension exercise plus spinal manipulation experienced a decrease in chronic LBP, but no differences were noted between groups. This study had a high risk of bias.
Little et al�found Alexander technique, exercise, and massage were all superior to control (normal care) at three months for chronic LBP and disability. This study had a moderate risk of bias.
Wilkey et al found chiropractic management was superior to NHS pain clinic management for chronic LBP at eight weeks for pain and disability outcomes. This study had a high risk of bias.
Bogefeldt et al found manual therapy plus advice to stay active was more effective than advice to stay active alone for reducing sick leave and improving return to work at 10 weeks for acute LBP. No differences between the groups were noted at two years. This study had a low risk of bias.
Hancock et al found spinal mobilization in addition to medical care was no more effective than medical care alone at reducing the number of days until full recovery for acute LBP. This study had a low risk of bias.
Ferreira et al found spinal manipulation was superior to general exercise for function and perceived effect at eight weeks in chronic LBP patients, but no differences were noted between groups at six and 12 months. This study had a moderate risk of bias.
Eisenberg et al found that choice of complementary therapies (including chiropractic care) in addition to usual care was no different from usual care in bothersomeness and disability for care of acute LBP. The trial did not report findings for any individual manual therapy. This study had a low risk of bias.
Hondras et al found lumbar flexion-distraction was superior to minimal medical care at 3,6,9,12, and 24 weeks for disability related to subacute or chronic LBP, but spinal manipulation was superior to minimal medical care only at three weeks. No differences between spinal manipulation and flexion-distraction were noted for any reported outcomes. Global perceived improvement was superior at 12 and 24 weeks for both manual therapies compared to minimal medical care. This study had a low risk of bias.
Mohseni-Bandpei et al showed that patients receiving manipulation/exercise for chronic LBP reported greater improvement compared with those receiving ultrasound/exercise at both the end of the treatment period and at 6-month follow-up. The study had a high risk of bias.
Beyerman et al evaluated the efficacy of chiropractic spinal manipulation, manual flexion/distraction, and hot pack application for the treatment of LBP of mixed duration from osteoarthritis (OA) compared with moist heat alone. The spinal manipulation group reported more and faster short term improvement in pain and range of motion. The study had a high risk of bias.
Poole et al showed that adding either foot reflexology or relaxation training to usual medical care in patients with chronic LBP is no more effective than usual medical care alone in either the short or long term. The study had a moderate risk of bias.
Zaproudina et al found no differences between groups (bonesetting versus exercise plus massage) at one month or one year for pain or disability. The global assessment score of improvement was superior for the bonesetting group at one month. This study had a high risk of bias.
Evidence Summary (See Figure 3)
? High quality evidence that spinal manipulation/mobilization is an effective treatment option for subacute and chronic LBP in adults.
? Moderate quality evidence that spinal manipulation/mobilization is an effective treatment option for subacute and chronic LBP in older adults.
? Moderate quality evidence that spinal manipulation/mobilization is an effective treatment option for acute LBP in adults.
? Moderate evidence that adding spinal mobilization to medical care does not improve outcomes for acute LBP in adults.
? Moderate quality evidence that massage is an effective treatment for subacute and chronic LBP in adults.
? Inconclusive evidence in a favorable direction regarding the use of manipulation for sciatica/radiating leg pain.
? Inconclusive evidence in a non-favorable direction regarding the addition of foot reflexology to usual medical care for chronic LBP.
Other effective non-invasive physical treatments or patient education
Advice to stay active, interdisciplinary rehabilitation, exercise therapy, acupuncture, yoga, cognitive-behavioral therapy, or progressive relaxation for chronic LBP and superficial heat for acute LBP.
Non-specific mid back pain
Definition
Non-specific thoracic spine pain is defined as soreness, tension, and/or stiffness in the thoracic spine region for which it is not possible to identify a specific cause of pain.
Diagnosis
Diagnosis of non-specific thoracic spine pain is derived from the patient’s history with an unremarkable neurological exam and no indicators of potentially serious pathology. Imaging is only indicated in patients with a positive neurological exam or presence of a “red flag”.
Evidence base for manual treatment
Systematic reviews (most recent)
No systematic reviews addressing the role of manual therapy in thoracic spine pain that included randomized clinical trials were located.
Evidence-based clinical guidelines
The Australian acute musculoskeletal pain guidelines group concludes there is evidence from one small pilot study that spinal manipulation is effective compared to placebo for thoracic spine pain.
Recent randomized clinical trials not included in above
Multiple randomized clinical trials investigating the use of thoracic spinal manipulation were located; however, most of the trials assessed the effectiveness of thoracic manipulation for neck or shoulder pain.
Evidence Summary (See Figure 3)
? Inconclusive evidence in a favorable direction regarding the use of spinal manipulation for mid back pain.
Other effective non-invasive physical treatments or patient education
None
Mechanical neck pain
Definition
Mechanical neck pain is defined as pain in the anatomic region of the neck for which it is not possible to identify a specific pathological cause of pain. It generally includes neck pain, with or without pain in the upper limbs which may or may not interfere with activities of daily living (Grades I and II). Signs and symptoms indicating significant neurologic compromise (Grade III) or major structural pathology (Grade IV including fracture, vertebral dislocation, neoplasm, etc.) are NOT included.
Diagnosis
Diagnosis of mechanical neck pain is derived from the patient’s history. Imaging is only indicated in patients with a positive neurological exam or presence of a “red flag”.
Evidence base for manual treatment
Systematic reviews (most recent)
The recently published best evidence synthesis by the Bone and Joint Decade 2000-2010 Task Force on Neck Pain and Its Associated Disorders represents the most recent and comprehensive systematic review of the literature for non-invasive interventions, including manual treatment, for neck pain. For whiplash associated disorders, they concluded that mobilization and exercises appear more beneficial than usual care or physical modalities. For Grades I and II neck pain, they concluded that the evidence suggests that manual treatment (including manipulation and mobilization) and exercise interventions, low-level laser therapy and perhaps acupuncture are more effective than no treatment, sham or alternative interventions. No one type of treatment was found to be clearly superior to any other. They also note that manipulation and mobilization yield comparable results. Conclusions regarding massage could not be made due to lack of evidence.
Since 2003, there were five other systematic reviews. One found that spinal manipulation was effective for non-specific neck pain alone and in combination with exercise, while two found effectiveness only for the combination of spinal manipulation and exercise. Differences between review conclusions are expected. It is likely they can be attributed to additional primary studies and diversity in review strategies, including inclusion criteria, methodological quality scoring, and evidence determination.
Evidence-based clinical guidelines
The American Physical Therapy Association’s guidelines on neck pain recommends utilizing cervical manipulation and mobilization procedures to reduce neck pain based on strong evidence.�They found cervical manipulation and mobilization with exercise to be more effective for reducing neck pain and disability than manipulation and mobilization alone. Thoracic spine manipulation is also recommended for reducing pain and disability in patients with neck and neck-related arm pain based on weak evidence.
Recent randomized clinical trials not included in above
H�kkinen et al used a cross-over design to compare manual therapy and stretching for chronic neck pain. Manual therapy was more effective than stretching at four weeks, but no difference between the two therapies was noted at 12 weeks. This study had a high risk of bias.
Gonz�lez-Iglesias et al examined the effectiveness of adding general thoracic spine manipulation to electrotherapy/thermal therapy for acute neck pain. In two separate trials they found an advantage for the manipulation group in terms of pain and disability. The trials had moderate to low risk of bias.
Walker et al compared manual therapy with exercise to advice to stay active and placebo ultrasound. The manual therapy group reported less pain (in the short term) and more improvement and less disability (in the long term) than the placebo group. This study had a low risk of bias.
Cleland et al�showed that thoracic spine thrust mobilization/manipulation results in a significantly greater short-term reduction in pain and disability than does thoracic non-thrust mobilization/manipulation in people with mostly subacute neck pain. The study had a low risk of bias.
Fernandez et al�found that adding thoracic manipulation to a physical therapy program was effective in treating neck pain due to whiplash injury. The study had a high risk of bias.
Savolainen et al�compared the effectiveness of thoracic manipulations with instructions for physiotherapeutic exercises for the treatment of neck pain in occupational health care. The effect of the manipulations was more favorable than the personal exercise program in treating the more intense phase of pain. The study had a moderate risk of bias.
Zaproudina et al�assessed the effectiveness of traditional bone setting (mobilization) of joints of extremities and the spine for chronic neck pain compared with conventional physiotherapy or massage. The traditional bone setting was superior to the other two treatments in both in the short and long term. The study had a moderate risk of bias.
Sherman et al compared massage therapy to self-care for chronic neck pain. Massage was superior to self-care at 4 weeks for both neck disability and pain. A greater proportion of massage patients reported a clinically significant improvement in disability than self-care patients at four weeks, and more massage patients reported a clinically significant improvement in pain at four and 10 weeks. No statistically significant differences between groups were noted at 26 weeks. This study had a low risk of bias.
Evidence Summary (See Figure 3)
? Moderate quality evidence that mobilization combined with exercise is effective for acute whiplash-associated disorders.
? Moderate quality evidence that spinal manipulation/mobilization combined with exercise is effective for chronic non-specific neck pain.
? Moderate quality evidence that thoracic spinal manipulation/mobilization is effective for acute/subacute non-specific neck pain.
? Moderate quality evidence that spinal manipulation is similar to mobilization for chronic non-specific neck pain.
? Moderate quality evidence that massage therapy is effective for non-specific chronic neck pain.
? Inconclusive evidence in a favorable direction for cervical spinal manipulation/mobilization alone for neck pain of any duration.
Other effective non-invasive physical treatments or patient education
Exercise, low-level laser therapy, acupuncture
Coccydynia
Definition
Coccydynia is defined as symptoms of pain in the region of the coccyx.
Diagnosis
Diagnosis of coccydynia is derived from the patient’s history and exam with no indicators of potentially serious pathology. Imaging is only indicated in patients with a presence of a “red flag”.
Evidence base for manual treatment
Systematic reviews (most recent)
None located
Evidence-based clinical guidelines
None located
Recent randomized clinical trials not included in above
Maigne et al found manipulation was more effective than placebo for pain relief and disability in the treatment of coccydynia at one month. This study had a moderate risk of bias.
Evidence Summary (See Figure 3)
? Inconclusive evidence in a favorable direction for the use of spinal manipulation in the treatment of coccydynia.
Other effective non-invasive physical treatments or patient education
None
Shoulder pain
Definition
Shoulder pain is defined as soreness, tension, and/or stiffness in the anatomical region of the shoulder and can be secondary to multiple conditions including, but not limited to rotator cuff disease and adhesive capsulitis.
Diagnosis
Diagnosis of shoulder pain is derived mainly from the patient’s history and physical exam with no indicators of potentially serious pathology. Imaging studies are confirmatory for diagnoses of rotator cuff disorders, osteoarthritis, glenohumeral instability, and other pathologic causes of shoulder pain.
Evidence base for manual treatment
Systematic reviews (most recent)
Two systematic reviews evaluated the benefit of manual therapy for shoulder pain. Six RCTs evaluating the effectiveness of manual therapy for the treatment of shoulder pain were included. Five of the trials evaluated mobilization�while one trial evaluated the use of manipulation and mobilization�for shoulder pain. The review concluded there is weak evidence that mobilization added benefit to exercise for rotator cuff disease.
Evidence-based clinical guidelines
The Philadelphia Panel’s evidence based clinical practice guidelines on selected rehabilitation interventions for shoulder pain concluded there is insufficient evidence regarding the use of therapeutic massage for shoulder pain.
Recent randomized clinical trials not included in above
Vermeulen et al�found that high-grade mobilization techniques were more effective than low-grade mobilization techniques for active range of motion (ROM), passive ROM, and shoulder disability for adhesive capsulitis at three to 12 months. No differences were noted for pain or mental and physical general health. Both groups showed improvement in all outcome measures. This study had low risk of bias.
van den Dolder and Roberts�found massage was more effective than no treatment for pain, function, and ROM over a two week period in patients with shoulder pain. This study had moderate risk of bias.
Bergman et al�found no differences between groups during the treatment period (6 wks). More patients reported being “recovered” in the usual care plus manipulative/mobilization group at 12 and 52 weeks compared to usual care alone. This study had low risk of bias.
Johnson et al�found no differences in pain or disability between anterior and posterior mobilization for the care of adhesive capsulitis. This study had a high risk of bias.
Guler-Uysal et al�concluded that deep friction massage and mobilization exercises was superior in the short term to physical therapy including diathermy for adhesive capsulitis. The study had a high risk of bias.
? Moderate quality evidence that high-grade mobilization is superior to low-grade mobilization for reduction of disability, but not for pain, in adhesive capsulitis.
? Inconclusive evidence in an unclear direction for a comparison of anterior and posterior mobilization for adhesive capsulitis.
? Moderate evidence favors the addition of manipulative/mobilization to medical care for shoulder girdle pain and dysfunction.
? Inconclusive evidence in a favorable direction for massage in the treatment of shoulder pain.
? Inconclusive evidence in a favorable direction for mobilization/manipulation in the treatment of rotator cuff pain.
Other effective non-invasive physical treatments or patient education
Exercise therapy
Lateral epicondylitis
Definition
Lateral epicondylitis is defined as pain in the region of the lateral epicondyle which is exacerbated by active and resistive movements of the extensor muscles of the forearm.
Diagnosis
Diagnosis is made solely from the patient’s history and clinical examination.
Evidence base for manual treatment
Systematic reviews (most recent)
Three systematic reviews evaluating the benefit of manual therapy for lateral epicondylitis have been identified. Eight RCTs were included�in the systematic reviews examining the effect of various manual therapies including elbow�and wrist manipulation, cervical spine�and elbow mobilization, and cross-friction massage. Bisset et al�concluded there is some evidence of positive initial effects of manual techniques (massage/mobilization) for lateral epicondylitis, but no long term evidence. Smidt et al�concluded there is insufficient evidence to draw conclusions on the effectiveness of mobilization techniques for lateral epicondylitis.
Evidence-based clinical guidelines
None located
Recent randomized clinical trials not included in above
Verhaar et al showed that corticosteroid injection was superior to Cyriax physiotherapy for the number of pain free subjects at six weeks. No differences between groups were noted at one year. This study had a high risk of bias.
Bisset et al�found corticosteroid injections were superior to elbow mobilization with exercise which was superior to wait and see approaches for pain-free grip strength, pain intensity, function, and global improvement at six weeks. However, both elbow mobilization with exercise and the wait and see approach were superior to corticosteroid injections at six months and one year for all of the previously reported outcomes. This study had a low risk of bias.
Nourbakhsh and Fearon�found oscillating energy manual therapy (tender point massage) was superior to placebo manual therapy for pain intensity and function. This study had a high risk of bias due to sample size (low risk of bias otherwise).
Evidence Summary (See Figure 4)
? Moderate quality evidence that elbow mobilization with exercise is inferior to corticosteroid injections in the short term and superior in the long term for lateral epicondylitis.
? Inconclusive evidence in a favorable direction regarding the use of manual oscillating tender point therapy of the elbow for lateral epicondylitis.
Other effective non-invasive physical treatments or patient education
Laser therapy, acupuncture
Carpal tunnel syndrome
Definition
Carpal tunnel syndrome is defined as compression of the median nerve as it passes through the carpal tunnel in the wrist.
Diagnosis
Diagnosis of carpal tunnel syndrome is made from the patient’s history, physical exam, and confirmatory electrodiagnostic tests.
Evidence base for manual treatment
Systematic reviews (most recent)
Since 2003, four systematic reviews evaluated the benefit of manual therapy for carpal tunnel syndrome. Two RCTs evaluating the effectiveness of manual therapy were included. One of the trials examined the use of spinal and upper extremity manipulation, while the other trial examined the use of wrist manipulation for carpal tunnel syndrome. The reviews concluded uncertain or limited evidence for manipulation/mobilization.
Evidence-based clinical guidelines
The American Academy of Orthopaedic Surgeons clinical practice guideline on the treatment of carpal tunnel syndrome�made no recommendations for or against the use of manipulation or massage therapy due to insufficient evidence.
Recent randomized clinical trials not included in above
None
Evidence Summary (See Figure 4)
? Inconclusive evidence in a favorable direction for manipulation/mobilization in the treatment of carpal tunnel syndrome.
Other effective non-invasive physical treatments or patient education
Splinting
Hip pain
Definition
Hip pain is defined as soreness, tension, and/or stiffness in the anatomical region of the hip and can be secondary to multiple conditions including hip osteoarthritis.
Diagnosis
Diagnosis of hip pain is derived from the patient’s history and physical exam with an unremarkable neurological exam and no indicators of potentially serious pathology. Imaging studies are confirmatory for diagnoses of moderate or severe osteoarthritis.
Evidence base for manual treatment
Systematic reviews (most recent)
One systematic review evaluating manual therapy for hip pain has been published. One RCT evaluating the effectiveness of hip manipulation for the treatment of hip osteoarthritis was included in the published systematic review. The review concluded there is limited evidence for manipulative therapy combined with multimodal or exercise therapy for hip osteoarthritis.
Evidence-based clinical guidelines
The NICE national clinical guidelines for care and management of adults with osteoarthritis�recommends manipulation and stretching should be considered as an adjunct to core treatment, particularly for osteoarthritis of the hip. This recommendation is based on the results of one RCT.
The orthopaedic section of the American Physical Therapy Association’s guidelines on hip pain and mobility deficits�recommends clinicians should consider the use of manual therapy procedures to provide short-term pain relief and improve hip mobility and function in patients with mild hip osteoarthritis based on moderate evidence.
Recent randomized clinical trials not included in above
Licciardone et al found decreased rehabilitation efficiency with osteopathic manipulative therapy (OMT) compared to sham OMT following hip arthroplasty. No other significant differences were found between the two groups. This study had a high risk of bias.
Evidence Summary (See Figure 4)
? Moderate quality evidence that hip manipulation is superior to exercise for the treatment of the symptoms of hip osteoarthritis.
? Inconclusive evidence in a non-favorable direction regarding osteopathic manipulative therapy for rehabilitation following total hip arthroplasty.
Other effective non-invasive physical treatments or patient education
Exercise therapy, advice about weight loss, and appropriate footwear
Knee pain
Definition
Knee pain is defined as soreness, tension, and/or stiffness in the anatomical region of the knee and can be secondary to multiple conditions including knee osteoarthritis or patellofemoral pain syndrome.
Diagnosis
Diagnosis of knee pain is derived from the patient’s history and physical exam with an unremarkable neurological exam and no indicators of potentially serious pathology. Imaging studies are confirmatory for diagnoses of moderate or severe osteoarthritis.
Evidence base for manual treatment
Systematic reviews (most recent)
As of September 2009, one systematic review evaluating the benefit of manual therapy for knee pain has been identified . Ten RCT’s evaluating the effectiveness of manual therapy for the treatment of knee pain were included in the published systematic review. Both osteoarthritis knee pain and patellofemoral pain syndrome were included in the conditions reviewed. Various manual therapy techniques including spinal mobilization,�spinal manipulation, knee mobilization, and knee manipulation were examined within the review. The review concludes there is fair evidence for manipulative therapy of the knee and/or full kinetic chain (Sacro-iliac to foot), combined with multimodal or exercise therapy for knee osteoarthritis and patellofemoral pain syndrome.
Evidence-based clinical guidelines
The NICE national clinical guidelines for care and management of adults with osteoarthritis�recommends manipulation and stretching should be considered as an adjunct to core treatment.
Recent randomized clinical trials not included in above
Pollard et al�assessed a manual therapy protocol compared to non-forceful manual contact (control). They concluded that a short term of manual therapy significantly reduced pain compared to the control group. This study had a high risk of bias.
Perlman et al�found massage therapy was more effective than wait list control for osteoarthritis related knee pain, stiffness, and function. This study had a high risk of bias.
Licciardone et al�assessed osteopathic manipulative treatment following knee arthroplasty. This study found decreased rehabilitation efficiency with OMT compared to sham OMT; otherwise, no significant differences were found between the two groups. This study had a high risk of bias.
? Moderate quality evidence that manual therapy of the knee and/or full kinetic chain (SI to foot) combined with multimodal or exercise therapy is effective for the symptoms of knee osteoarthritis.
? Moderate quality evidence that manual therapy of the knee and/or full kinetic chain (SI to foot) combined with multimodal or exercise therapy is effective for patellofemoral pain syndrome.
? Inconclusive evidence in a favorable direction that massage therapy is effective for the symptoms of knee osteoarthritis.
? Inconclusive evidence in a non-favorable direction for the effectiveness of osteopathic manipulative therapy for rehabilitation following total hip or knee arthroplasty.
Other effective non-invasive physical treatments or patient education
Exercise therapy, advice about weight loss, appropriate footwear, pulsed electromagnetic field therapy, acupuncture, and TENS
Ankle and foot conditions
Definition
A variety of conditions are included under ankle and foot conditions including ankle sprains, plantar fasciitis, morton’s neuroma, hallux limitus/rigidus, and hallux abducto valgus.
Diagnosis
The diagnosis of ankle/foot conditions relies mainly on the patient’s history and physical examination. Imaging studies are indicated for morton’s neuroma or in the presence of potential pathology.
Evidence base for manual treatment
Systematic reviews (most recent)
As of September 2009, two systematic reviews evaluating the benefit of manual therapy for ankle and foot conditions have been published. The ankle and foot conditions reviewed included ankle sprain, plantar fasciitis, morton’s neuroma, hallux limitus, and hallux abducto valgus. Thirteen RCTs evaluating the effectiveness of manual therapy for the treatment of various ankle and foot conditions were included in the published systematic reviews. Of the thirteen trials, six examined the use of ankle/foot manipulation, six examined the use of ankle/foot mobilization, and one trial examined the combined use of manipulation and mobilization.
The review by Brantingham et al concluded there is fair evidence for manipulative therapy of the ankle and/or foot combined with multimodal or exercise therapy for ankle inversion sprain. The same authors found limited evidence for manipulative therapy combined with multimodal or exercise therapy for plantar fasciitis, metatarsalgia, and hallux limitus and insufficient evidence for the use of manual therapy for hallux abducto valgus.
The review by van der Wees et al concluded it is likely that manual mobilization has an initial effect on dorsiflexion range of motion after ankle sprains.
Evidence-based clinical guidelines
None making recommendations based on RCTs were located
Recent randomized clinical trials not included in above
Wynne et al found an osteopathic manipulative therapy group had greater improvement in plantar fasciitis symptoms versus placebo control. This study had a high risk of bias.
Cleland et al compared manual therapy with exercise to electrotherapy with exercise for patients with plantar heel pain. They found manual therapy plus exercise was superior. This study had a low risk of bias.
Lin et al found the addition of manual therapy (mobilization) to a standard physiotherapy program provided no additional benefit compared to the standard physiotherapy program alone for rehabilitation following ankle fracture. This study had a low risk of bias.
Evidence Summary (See Figure 4)
? Moderate quality evidence that mobilization is of no additional benefit to exercise in the rehabilitation following ankle fractures.
? Moderate quality evidence that manual therapy of the foot and/or full kinetic chain (SI to foot) combined with exercise therapy is effective for plantar fasciitis.
? Inconclusive evidence in a favorable direction for the effectiveness of manual therapy with multimodal or exercise therapy for ankle sprains.
? Inconclusive evidence in a favorable direction regarding the effectiveness of manual therapy for morton’s neuroma, hallux limitus, and hallux abducto valgus.
Other effective non-invasive physical treatments or patient education
Stretching and foot orthoses for plantar fasciitis, ankle supports for ankle sprains
Temporomandibular disorders
Definition
Temporomandibular disorders consist of a group of pathologies affecting the masticatory muscles, temporomandibular joint, and related structures.
Diagnosis
Diagnosis of temporomandibular disorders is derived from the patient’s history and physical exam with no indicators of potentially serious pathology.
Evidence base for manual treatment
Systematic reviews (most recent)
As of September 2009, two systematic reviews evaluating the benefit of manual therapy for temporomandibular dysfunction have been published. Three RCTs evaluating the effectiveness of manual therapy were included in the published systematic reviews. Two of the trials examined the effectiveness of mobilization�and one trial assessed massage. The reviews conclude there is limited evidence for the use of manual therapy in the treatment of temporomandibular dysfunction.
Evidence-based clinical guidelines
None located
Recent randomized clinical trials not included in above
Monaco et al�examined the effects of osteopathic manipulative treatment on mandibular kinetics compared to a no treatment control group; however, no between group analysis was performed. This study had a high risk of bias.
Ismail et al�found physical therapy including mobilization in addition to splint therapy was superior to splint therapy alone after three months of treatment for active mouth opening. No differences were found between groups for pain. This study had a moderate risk of bias.
? Inconclusive evidence in a favorable direction regarding mobilization and massage for temporomandibular dysfunction.
Other effective non-invasive physical treatments or patient education
None
Fibromyalgia
Definition
Fibromyalgia syndrome (FMS) is a common rheumatological condition characterized by chronic widespread pain and reduced pain threshold, with hyperalgesia and allodynia.
Diagnosis
Diagnosis of fibromyalgia is made primarily from the patient’s history and physical exam. The American College of Rheumatology have produced classification criteria for fibromyalgia including widespread pain involving both sides of the body, above and below the waist for at least three months and the presence of 11 out of 18 possible pre-specified tender points.
Evidence base for manual treatment
Systematic reviews (most recent)
Since 2004, three systematic reviews evaluating the benefit of manual therapy for fibromyalgia have been published. Six RCTs evaluating the effectiveness of manual therapy for the treatment of fibromyalgia were included in the published systematic reviews. Five of the studies assessed the effectiveness of spinal manipulation for fibromyalgia, while one assessed the effectiveness of massage.
Schneider et al�conclude there is moderate level evidence from several RCTs and a systematic review�that massage is helpful in improving sleep and reducing anxiety in chronic pain; however, few of the studies included in the systematic review�specifically investigated fibromyalgia.
Ernst�states that the current trial evidence is insufficient to conclude that chiropractic is an effective treatment of fibromyalgia.
Goldenberg et al�conclude there is weak evidence of efficacy for chiropractic, manual, and massage therapy in the treatment of fibromyalgia.
Evidence-based clinical guidelines
The 2007 a multidisciplinary task force with members from 11 European countries published evidence based recommendation for FMS. The task force notes the clinical trial evidence for manual therapy is lacking.
Randomized clinical trials not included in above
Ekici et al found improvement was higher in the manual lymph drainage group compared to connective tissue massage on the fibromyalgia impact questionnaire, but no differences were noted between groups for pain, pain pressure threshold, or health related quality of life. This study had a moderate risk of bias.
Evidence Summary (See Figure 5)
? Inconclusive evidence in a favorable direction regarding the effectiveness of massage and manual lymph drainage for the treatment of fibromyalgia.
? Inconclusive evidence in an unclear direction regarding the effectiveness of spinal manipulation for the treatment of fibromyalgia.
Other effective non-invasive physical treatments or patient education
Heated pool treatment with or without exercise, supervised aerobic exercise
Myofascial Pain Syndrome
Definition
Myofascial pain syndrome is a poorly defined condition that requires the presence of myofascial trigger points.
Diagnosis
Diagnosis of myofascial pain syndrome is made exclusively from the patient’s history and physical exam.
Evidence base for manual treatment
Systematic reviews (most recent)
As of September 2009, one systematic review evaluating the benefit of manual therapy for myofascial pain syndrome was identified, which concludes there is limited evidence to support the use of some manual therapies for providing long-term relief of pain at myofascial trigger points. Fifteen RCTs evaluating the effectiveness of manual therapy for the treatment of myofascial pain syndrome were included in the published systematic review. Only two of the truly randomized trials assessed the effectiveness of manual therapy beyond the immediate post-treatment period. One trial assessed the effectiveness of massage combined with other therapies, while the other trial assessed the effectiveness of self-treatment with ischemic compression.
Evidence-based clinical guidelines
None
Recent randomized clinical trials not included in above
None
Evidence Summary (See Figure 5)
? Inconclusive evidence in a favorable direction regarding the effectiveness of massage for the treatment of myofascial pain syndrome.
Other effective non-invasive physical treatments or patient education
Laser, acupuncture
Migraine Headache
Definition
Migraine headache is defined as recurrent/episodic moderate or severe headaches which are usually unilateral, pulsating, aggravated by routine physical activity, and are associated with either nausea, vomiting, photophobia, or phonophobia.
Diagnosis
Diagnosis of migraine headaches is made primarily from the patient’s history and a negative neurological exam. Neuroimaging is only indicated in patients with a positive neurological exam or presence of a “red flag”.
Evidence base for manual treatment
Systematic reviews (most recent)
Since 2004, two systematic reviews evaluated the benefit of manual therapy for migraine headache. The reviews evaluated three RCTs on spinal manipulation. Astin and Ernst�concluded that due to methodological limitations of the RCTs, it is unclear whether or not spinal manipulation is an effective treatment for headache disorders. In contrast, the conclusion from a Cochrane review�was that spinal manipulation is an effective option for the care of migraine headache. The conclusions of the two reviews differed in methodology for determining RCT quality and the strength of evidence. Astin and Ernst�evaluated study quality using a scale that is no longer recommended by the Cochrane Collaboration and did not apply evidence rules for their conclusions. The Cochrane review used a pre-specified, detailed protocol for synthesizing the evidence from the quality, quantity, and results of RCTs.
Evidence-based clinical guidelines
The SIGN guidelines�for the diagnosis and management of headache in adults concludes the evidence of effectiveness for manual therapy is too limited to lead to a recommendation.
Recent randomized clinical trials not included in above
Lawler and Cameron�found that massage therapy significantly reduced migraine frequency in the short term compared to filling out a diary with no other treatment. This study had a high risk of bias.
? Moderate quality evidence that spinal manipulation has an effectiveness similar to a first-line prophylactic prescription medication (amitriptyline) for the prophylactic treatment of migraine.
? Inconclusive evidence in a favorable direction comparing spinal manipulation to sham interferential.
? Inconclusive evidence in a favorable direction regarding the use of massage therapy alone.
Other effective non-invasive physical treatments or patient education
Tension-type headache is defined as a headache that is pressing/tightening in quality, mild/moderate in intensity, bilateral in location, and does not worsen with routine physical activity.
Diagnosis
Diagnosis of tension-type headaches is made primarily from the patient’s history and a negative neurological exam. Neuroimaging is only indicated in patients with a positive neurological exam or presence of a “red flag”.
Evidence base for manual treatment
Systematic reviews (most recent)
Since 2002, five systematic reviews evaluated the benefit of manual therapy for tension-type headache. Eleven RCTs were included in the published systematic reviews. Three of the RCTs assessed the effectiveness of spinal manipulation, six of the trials evaluated the use of combined therapies including a form of manual therapy, one trial evaluated a craniosacral technique, and the remaining trial compared connective tissue manipulation to mobilization. The reviews generally conclude there is insufficient evidence to draw inference on the effectiveness of manual therapy in the treatment of tension-type headache. An exception is the Cochrane review�which found that some inference regarding spinal manipulation could be made from two trials with low risk of bias. One trial�showed that for the prophylactic treatment of chronic tension-type headache, amitriptyline (an effective drug) is more effective than spinal manipulation during treatment. However, spinal manipulation is superior in the short term after cessation of both treatments, but this could be due to a rebound effect of the medication withdrawal. The other trial�showed that spinal manipulation in addition to massage is no more effective than massage alone for the treatment of episodic tension-type headache.
Evidence-based clinical guidelines
The SIGN guideline�for the diagnosis and management of headache in adults draws no conclusions.
Recent randomized clinical trials not included in above
Anderson and Seniscal�found that participants receiving osteopathic manipulation in addition to relaxation therapy had significant improvement in headache frequency compared to relaxation therapy alone. This study had a moderate risk of bias.
Evidence Summary (See Figure 5)
? Moderate quality evidence that spinal manipulation in addition to massage is no more effective than massage alone for the treatment of episodic tension-type headache.
? Inconclusive evidence in an unclear direction regarding the use of spinal manipulation alone or in combination with therapies other than massage for most forms of tension-type headache.
Other effective non-invasive physical treatments or patient education
Acupuncture, biofeedback
Cervicogenic Headache
Definition
Cervicogenic headache is defined as unilateral or bilateral pain localized to the neck and occipital region which may project to regions on the head and/or face. Head pain is precipitated by neck movement, sustained awkward head positioning, or external pressure over the upper cervical or occipital region on the symptomatic side.
Diagnosis
Diagnosis of cervicogenic headaches is made primarily from the patient’s history and a negative neurological exam. Neuroimaging is only indicated in patients with a positive neurological exam or presence of a “red flag”.
Evidence base for manual treatment
Systematic reviews (most recent)
Since 2002, four systematic reviews have been published on manual therapy for cervicogenic headache. The reviews made inference based on six RCTs that evaluated a range of manual therapy treatments including spinal manipulation, mobilization, and friction massage. Astin and Ernst�concluded that due to methodological limitations of the RCTs, it is unclear whether or not spinal manipulation is an effective treatment for headache disorders. In contrast, a Cochrane review concluded that spinal manipulation is an effective option for the care of cervicogenic headache. The conclusions of the two reviews differed in methodology for determining RCT quality and the strength of evidence. Ernst evaluated study quality using a scale that is no longer recommended by the Cochrane Collaboration and did not apply evidence rules for their conclusions. The Cochrane review�used a pre-specified, detailed protocol for synthesizing the evidence from the quality, quantity, and results of RCTs.
Evidence-based clinical guidelines
The SIGN guidelines�for the diagnosis and management of headache in adults concluded spinal manipulation should be considered in patients with cervicogenic headache.
Recent randomized clinical trials not included in above
Hall et al�evaluated the efficacy of apophyseal glide of the upper cervical region in comparison to a sham control. They found a large clinically important and statistically significant advantage of the intervention over sham for pain intensity. The study had a low risk of bias.
? Moderate quality evidence that spinal manipulation is more effective than placebo manipulation, friction massage, and no treatment.
? Moderate quality evidence that spinal manipulation is similar in effectiveness to exercise.
? Moderate quality evidence that self-mobilizing natural apophyseal glides are more effective than placebo.
? Inclusive evidence that deep friction massage with trigger point therapy is inferior to spinal manipulation.
? Inconclusive evidence in an unclear direction for the use of mobilization.
Other effective non-invasive physical treatments or patient education
Neck exercises
Miscellaneous Headache
Definition
Headaches not classified as tension-type, migraine, or cervicogenic in nature according to the International Headache Society’s 2004 diagnostic criteria.
Evidence base for manual treatment
Systematic reviews (most recent)
One systematic review (2004) evaluated the benefit of manual therapy for other types of chronic headache. One RCT evaluating the use of mobilization for post-traumatic (post-concussive) headache was included. The review found the evidence to be inconclusive.
Evidence-based clinical guidelines
None
Recent randomized clinical trials not included in above
? Inconclusive evidence in a favorable direction regarding mobilization for post-traumatic headache.
Other effective non-invasive physical treatments or patient education
None
Asthma
Definition
Asthma is a common, complex chronic disorder of the airways that is characterized by variable and recurring symptoms, airflow obstruction, bronchial hyperresponsiveness, and an underlying inflammation.
Diagnosis
The diagnosis is made through the combination of the patient’s history, upper respiratory physical exam, and pulmonary function testing (spirometry). Patient administered peak flow measurement is often used to monitor effects of treatment.
Evidence base for manual treatment
Systematic reviews
Since 2002, four systematic reviews, one a Cochrane review, on manual therapy for asthma have been published. Of the total of five RCTs on the effectiveness of manual therapy�available from the searched literature, two investigated chiropractic spinal manipulation for chronic asthma, one in adults�and the other in children. Two trials assessed the effectiveness on chronic asthma in children, one examined osteopathic manipulative/manual therapy, and the other massage. The fifth trial evaluated the effect of foot manual reflexology for change in asthma symptoms and lung function in adults. The four systematic reviews collectively concluded that the evidence indicates that none of the manual therapy approaches have been shown to be superior to a suitable sham manual control on reducing severity and improving lung function but that clinically important improvements occur over time during both active and sham treatment.
Evidence-based clinical guidelines
The asthma guidelines by The US National Heart, Lung, and Blood Institutes�and by The British Thoracic Society�both conclude that there is insufficient evidence to recommend the use of chiropractic or related manual techniques in the treatment of asthma.
Recent randomized clinical trials not included in above
None
Evidence Summary (See Figures 6 & 7)
? There is moderate quality evidence that spinal manipulation is not effective (similar to sham manipulation) for the treatment of asthma in children and adults on lung function and symptom severity.
? There is inconclusive evidence in a non-favorable direction regarding the effectiveness of foot manual reflexology for change in asthma symptoms and lung function in adults.
? There is inconclusive evidence in a favorable direction regarding the effectiveness of osteopathic manipulative treatment for change in asthma symptoms and lung function in children.
? There is inconclusive evidence in an unclear direction regarding the effectiveness of massage for change in asthma symptoms and lung function in children.
Other effective non-invasive physical treatments or patient education
Education and advice on self-management, maintaining normal activity levels, control of environmental factors and smoking cessation
Pneumonia
Definition
Pneumonia is defined as an acute inflammation of the lungs caused by infection.
Diagnosis
Diagnosis of pneumonia relies primarily on chest radiography in conjunction with the patient’s history, examination, and laboratory findings.
Evidence base for manual treatment
Systematic reviews (most recent)
Since 2007, one systematic review evaluating the benefit of manual therapy for pneumonia has been published. One RCT evaluating the effectiveness of manual therapy for the treatment of pneumonia was included in the published systematic review. The included trial assessed the effectiveness of osteopathic spinal manipulation for acute pneumonia in hospitalized elderly adults. The review concluded there is promising evidence for the potential benefit of manual procedures for hospitalized elderly patients with pneumonia. Our risk of bias assessment places this trial in the moderate risk of bias category.
? There is inconclusive evidence in a favorable direction regarding the effectiveness of osteopathic manual treatment for the treatment of acute pneumonia in elderly hospitalized patients.
Other effective non-invasive physical treatments or patient education
Cases of pneumonia that are of public health concern should be reported immediately to the local health department. Respiratory hygiene measures, including the use of hand hygiene and masks or tissues for patients with cough, should be used in outpatient settings as a means to reduce the spread of respiratory infections.
Vertigo
Definition
Vertigo is defined as a false sensation of movement of the self or the environment. Vertigo is a sensation and not necessarily a diagnosis as there are multiple underlying pathologies responsible for vertigo.
Diagnosis
Diagnosis of vertigo relies primarily on the patient’s history and clinical examination. Potential causes of vertigo include both pathological disorders such as vertebrobasilar insufficiency or central nervous system lesions as well as more benign causes such as cervicogenic vertigo or benign paroxysmal positional vertigo.
Evidence base for manual treatment
Systematic reviews (most recent)
Since 2004, two systematic reviews evaluating the benefit of manual therapy for vertigo have been published.�One RCT evaluating the effectiveness of mobilization and soft-tissue massage for the treatment of cervicogenic vertigo was included in both published systematic reviews. One review concluded limited evidence of effectiveness. The other concluded effectiveness, but the inference was on the inclusion of other types of evidence.
Evidence-based clinical guidelines
None addressing the use of manual therapy
Recent randomized clinical trials not included in above
Reid et al�compared sustained natural apophyseal glides (SNAGs), delivered manually by a therapist, to detuned laser treatment for the treatment of cervicogenic dizziness. Patients receiving SNAGs reported less dizziness, disability and cervical pain after six weeks, but not at 12 weeks. This study had a low risk of bias.
? Moderate quality evidence that manual treatment (specifically sustained natural apophyseal glides) is an effective treatment for cervicogenic dizziness, at least in the short term.
Other effective non-invasive physical treatments or patient education
Particle repositioning maneuvers for benign paroxysmal positional vertigo, vestibular rehabilitation
Infantile Colic
Definition
Colic is a poorly defined condition characterized by excessive, uncontrollable crying in infants.
Diagnosis
The diagnosis of colic is based solely on the patient’s history and the absence of other explanations for the excessive crying. The “rule of threes” is the most common criteria used in making a diagnosis of colic. The rule of three’s is defined as an otherwise healthy and well fed infant with paroxysms of crying and fussing lasting for a total of three hours a day and occurring more than three days a week for at least three weeks.
Evidence base for manual treatment
Systematic reviews (most recent)
Since 2003, six systematic reviews evaluating the benefit of manual therapy for infantile colic have been published. Two of the systematic reviews evaluated the effectiveness of manual therapy for non-musculoskeletal�and pediatric�conditions as a whole but fail to draw specific conclusions regarding the use of manual therapy for infantile colic. Of the eight RCTs evaluating the effectiveness of manual therapy for the treatment of colic, five were included in the published systematic reviews. All five of the trials assessed the effectiveness of chiropractic spinal manipulation for infantile colic. All four systematic reviews concluded there is no evidence manual therapy is more effective than sham therapy for the treatment of colic.
Evidence-based clinical guidelines
No clinical guidelines located
Randomized clinical trials not included in above
Hayden et al�found cranial osteopathy was more effective than no treatment for crying duration. This study had a high risk of bias
Huhtala et al�found no difference between groups treated with massage therapy or given a crib vibrator for crying duration. This study had a high risk of bias.
Arikan et al�found all four interventions (massage, sucrose solution, herbal tea, hydrolysed formula) showed improvement compared to a no treatment control group. This study had a moderate risk of bias.
Evidence Summary (See Figure 7)
? Moderate quality evidence that spinal manipulation is no more effective than sham spinal manipulation for the treatment of infantile colic.
? Inconclusive evidence in a favorable direction regarding the effectiveness of cranial osteopathic manual treatment and massage for the treatment of infantile colic.
Other effective non-invasive physical treatments or patient education
Reduce stimulation, herbal tea, and trial of hypoallergenic formula milk
Nocturnal Enuresis
Definition
Nocturnal enuresis is defined as the involuntary loss of urine at night, in the absence of organic disease, at an age when a child could reasonably be expected to be dry (typically at the age of five).
Diagnosis
The diagnosis of nocturnal enuresis is derived mainly from the patient’s history given the absence of other organic causes including congenital or acquired defects of the central nervous system. Psychological factors can be contributory in some children requiring proper assessment and treatment.
Evidence base for manual treatment
Systematic reviews (most recent)
Since 2005, two systematic reviews, one a Cochrane review, evaluating the benefit of manual therapy for nocturnal enuresis were published. The systematic reviews included a total of two randomized clinical trials. Both of the included trials examined the use of spinal manipulation for nocturnal enuresis. Both reviews concluded there is insufficient evidence to make conclusions about the effectiveness of spinal manipulation for the treatment of enuresis.
Evidence-based clinical guidelines
None addressing manual therapy as a treatment option
? Inconclusive evidence in a favorable direction regarding the effectiveness of chiropractic care for the treatment of enuresis.
Other effective non-invasive physical treatments or patient education
Education, simple behavioral interventions, and alarm treatment
Otitis Media
Definition
Otitis media is characterized by middle ear inflammation which can exist in an acute or chronic state and can occur with or without symptoms.
Diagnosis
Diagnosis of otitis media relies on otoscopic signs and symptoms consistent with a purulent middle ear effusion in association with systemic signs of illness.
Evidence base for manual treatment
Systematic reviews (most recent)
Hawk et al�found promising evidence for the potential benefit of spinal manipulation/mobilization procedures for children with otitis media. This was based on one trial. Two other reviews specifically addressed spinal manipulation by chiropractors for non-musculoskeletal�and pediatric�conditions. Both found insufficient evidence to comment on manual treatment effectiveness or ineffectiveness for otitis media.
Evidence-based clinical guidelines
The American Academy of Pediatrics 2004 guidelines on the diagnosis and management of acute otitis media�concluded no recommendation for complementary and alternative medicine for the treatment of acute otitis media can be made due to limited data.
Recent randomized clinical trials not included in above
Wahl et al investigated the efficacy of osteopathic manipulative treatment with and without Echinacea compared to sham and placebo for the treatment of otitis media. The study found that a regimen of up to five osteopathic manipulative treatments does not significantly decrease the risk of acute otitis media episodes. This study had a high risk of bias.
? Inconclusive evidence in an unclear direction regarding the effectiveness of osteopathic manipulative therapy for otitis media.
Other effective non-invasive physical treatments or patient education
Patient education and “watch and wait” approach for 72 hours for acute otitis media
Hypertension
Definition
Hypertension is defined as the sustained elevation of systolic blood pressure over 140 mmHg, diastolic blood pressure over 90 mm Hg, or both.
Diagnosis
Diagnosis of hypertension is made by the physical exam, specifically sphygmomanometry. The patient’s history, clinical exam and laboratory tests help identify potential etiologies.
Evidence base for manual treatment
Systematic reviews (most recent)
Since 2007, one systematic review evaluating the benefit of manual therapy for hypertension has been published (Hawk et al). Two RCTs evaluating the effectiveness of manual therapy for the treatment of stage I hypertension were included in this systematic review. One of the included trials evaluated the use of spinal manipulation and the other evaluated the use of instrument assisted spinal manipulation. The review found no evidence of effectiveness for spinal manipulation.
Evidence-based clinical guidelines
None addressing the use of manual therapy
Recent randomized clinical trials not included in above
A study by Bakris et al found NUCCA upper cervical manipulation to be more effective than sham manipulation in lowering blood pressure in patients with Stage I hypertension. This study had a high risk of bias.
Evidence Summary (See Figure 6)
? Moderate quality evidence that diversified spinal manipulation is not effective when added to a diet in the treatment of stage I hypertension.
? Inconclusive evidence in a favorable direction regarding upper cervical NUCCA manipulation for stage I hypertension .
? Inconclusive evidence in an unclear direction regarding instrument assisted spinal manipulation for hypertension.
Other effective non-invasive physical treatments or patient education
Advice on lifestyle interventions including diet, exercise, moderate alcohol consumption and smoking cessation
Relaxation therapies including biofeedback, meditation, or muscle relaxation
Dysmenorrhea
Definition
Dysmenorrhea is defined as painful menstrual cramps of uterine origin. Dysmenorrhea is grouped into two categories, primary and secondary dysmenorrhea. Secondary dysmenorrhea is painful menstruation associated with a pelvic pathology like endometriosis, while primary dysmenorrhea is painful menstruation in the absence of pelvic disease.
Diagnosis
Diagnosis of primary dysmenorrhea is made from the patient’s history. Diagnosis of secondary dysmenorrhea requires further investigation including a pelvic exam and potential ultrasound or laparoscopy.
Evidence base for manual treatment
Systematic reviews (most recent)
We identified two systematic reviews evaluating the benefit of manual therapy for dysmenorrhea. Five studies evaluating the effectiveness of manual therapy for the treatment of dysmenorrhea were included in the systematic reviews. Four of the included trials examined the use of spinal manipulation�and one examined the use of osteopathic manipulative techniques. Based on these trials, the Cochrane review by Proctor et al concluded there is no evidence to suggest that spinal manipulation is effective in the treatment of primary and secondary dysmenorrhea. The review by Hawk et al concluded the evidence was equivocal regarding chiropractic care for dysmenorrhea.
Evidence-based clinical guidelines
We identified consensus guidelines from the Society of Obstetricians and Gynecologists of Canada (SOGC) published in 2005 which included an assessment of manual treatment for primary dysmenorrhea. The authors concluded there is no evidence to support spinal manipulation as an effective treatment for primary dysmenorrhea.
Recent randomized clinical trials not included in above
None
Evidence Summary (See Figure 7)
? Moderate quality evidence that spinal manipulation is no more effective than sham manipulation in the treatment of primary dysmenorrhea.
Other effective non-invasive physical treatments or patient education
High frequency TENS
Premenstrual Syndrome
Definition
Premenstrual syndrome is defined as distressing physical, behavioral, and psychological symptoms, in the absence of organic or underlying psychiatric disease, which regularly recurs during the luteal phase of the menstrual cycle and disappears or significantly regresses by the end of menstruation and is associated with impairment in daily functioning and/or relationships.
Diagnosis
Diagnosis of premenstrual syndrome is made through patient history and the use of a patient diary over two menstrual cycles.
Evidence base for manual treatment
Systematic reviews (most recent)
Since 2007, three systematic reviews evaluating the benefit of manual therapy for premenstrual syndrome have been published. Three RCTs evaluating the effectiveness of manual therapy for the treatment of premenstrual syndrome were included in the reviews. The included trials examined different forms of manual therapy including spinal manipulation, massage therapy, and reflexology. Overall, the reviews concluded that the evidence is “not promising”, “equivocal”, and that high quality studies are needed to draw firm conclusions.
Evidence-based clinical guidelines
None discussing manual therapy
Recent randomized clinical trials not included in above
None
Evidence Summary (See Figure 7)
? Inconclusive evidence in a favorable direction regarding the effectiveness of reflexology and massage therapy for the treatment of premenstrual syndrome.
? Inconclusive evidence in an unclear direction regarding the effectiveness of spinal manipulation for the treatment of premenstrual syndrome.
Other effective non-invasive physical treatments or patient education
Cognitive behavioral therapy
Discussion
Making claims
There are two important questions underlying the medical and media debate surrounding the scope of chiropractic care and claims regarding its effectiveness particularly for non-musculoskeletal conditions: 1) should health professionals be permitted to use generally safe but as yet unproven methods? 2) What claims, if any, can and should be made with respect to the potential value of unproven treatments?
In response to the first question, a reasonable answer is “yes” given that professionals operate within the context of EBH, where it is acknowledged what is known today, might change tomorrow. It requires flexibility born of intellectual honesty that recognizes one’s current clinical practices may not�really�be in the best interests of the patient and as better evidence emerges, clinicians are obligated to change. Further, where evidence is absent, they are open to promoting the development of new knowledge that expands understanding of appropriate health care delivery.
In response to the second question, no claims of efficacy/effectiveness should be made for which there isn’t sufficient evidence. Unsubstantiated claims can be dangerous to patient health. We maintain the best evidence for efficacy/effectiveness that meets society’s standards comes from well-designed RCTs. While other study designs and clinical observations do offer insight into the plausibility and potential value of treatments, the concepts of plausibility and evidence of efficacy/effectiveness should not be confused when making claims.
Clinical Experience versus Clinical effectiveness
Why is it that the results of RCTs often do not confirm the results observed in clinical practice? There are several reasons. One of the problems is that both the provider and the patient are likely to interpret any improvement as being solely a result of the intervention being provided. However this is seldom the case. First, the natural history of the disorder (for example. acute LBP) is expected to partially or completely resolve by itself regardless of treatment. Second, the phenomenon of regression to the mean often accounts for some of the observed improvement in the condition. Regression to the mean is a statistical phenomenon associated with the fact that patients often present to the clinic or in clinical trials at a time where they have relatively high scores on severity outcome measures. If measured repeatedly before the commencement of treatment the severity scores usually regress towards lower more normal average values.
Additionally, there is substantial evidence to show that the ritual of the patient practitioner interaction has a therapeutic effect in itself separate from any specific effects of the treatment applied. This phenomenon is termed contextual effects. The contextual or, as it is often called, non-specific effect of the therapeutic encounter can be quite different depending on the type of provider, the explanation or diagnosis given, the provider’s enthusiasm, and the patient’s expectations. Some researchers have suggested that relying on evidence from RCTs and systematic reviews of RCTs is not adequate to determine whether a treatment is effective or not. The main issue, they contend, is that the intervention when studied in RCTs is too highly protocolized and does not reflect what is going on in clinical practice. They advocate a whole systems research approach that more accurately represents the entire clinical encounter. When using this perspective and systematically synthesizing the literature regarding chiropractic treatment of non-musculoskeletal conditions, also reviewed in this report, they conclude, for example that chiropractic is beneficial to patients with asthma and to children with infantile colic. This conclusion is at odds with the evidence summaries found in this report. We submit that whole systems research approach in this instance is clouding the interpretation of the literature regarding effectiveness as it relates to making claims, and incorrectly giving the consumer the impression that chiropractic care shows effectiveness over and above the contextual effects as it relates to the two examples above.
In a placebo-controlled RCT the question is: does the treatment provided have a specific effect over and above the contextual or non-specific effects. The result of such a trial may show that there is no important difference between the active intervention and the sham intervention. However, the patients may exhibit clinically important changes from baseline in both groups and thus the outcome would be consistent with what clinicians observe in their practice. An example of this is the results of the pragmatic placebo controlled RCT on chiropractic co-management of chronic asthma in adults (care delivered by experienced chiropractors consistent with normal clinical practice), which showed that patients improved equally during both the active and the sham intervention phases of the trial.
The Pieces of The Evidence-Based Healthcare Puzzle
It is essential to recognize what each piece of the EBH puzzle offers. Patient values and preferences do not provide sound evidence of a treatment’s effectiveness and may be misleading. A patient can be satisfied with a treatment, but it still may not be effective. The clinician’s observations, if well documented, can attest to patient improvement while under care and encourage perception of a treatment’s clinical plausibility. However, the narrow focus of attention under non-systematic observations common to practice experience tends to obscure other factors influencing case outcome. Similarly, EBH can be flawed, not because it fails to be scientific, but because-like all sciences-it imports the biases of researchers and clinicians. Well-performed clinical research however, does provide evidence for claims that a treatment is effective when the results are consistently applied to relevant patients. This is because of its reliance on methods for systematic observation and efforts to minimize bias.
Other authors’ work has been used to argue that a range of study types should be included when evaluating a treatment’s efficacy/effectiveness (case series, etc.). We maintain the best evidence that rises to societal standards to support claims of efficacy/effectiveness comes from well-designed RCTs. This is largely due to the powerful effect of successful randomization and design factors intended to minimize bias (all which help ensure that the results are due to the intervention and not some other known or unknown factor). Other evidence may be useful to inform treatment options when conditions for individual patients are not consistent with the best evidence or when better evidence is unavailable. Other types of research are more appropriate for answering related questions including, but not limited to, safety or mechanistic plausibility. This can lead to the refinement of interventions, inform the design of clinical trials, and aid in the interpretation of clinical observations. Similarly, clinical data from epidemiological studies, case reports, and case series can suggest that a treatment is�clinically plausible. That is, clinical observations demonstrate that�it is possible�that an intervention is effective. However, a gain in plausibility, biological or clinical, does NOT constitute proof of a treatment’s efficacy in human populations. Conversely lack of proof (as demonstrated through well performed randomized clinical trials) does not exclude plausibility.
Research on systematic reviews have taught us that individual studies can often lead to a conclusion very different from that of a systematic analysis of all available studies. Moreover, the scientific process is a systematic means of self-correcting investigations that classically begin with observations and hypotheses that support plausibility and/or mechanisms. Ideally, these precede and inform the conduct of RCTs under conditions most likely to yield clear results, often referred to as efficacy studies. Separately, studies that emulate general practice conditions may be used to develop an understanding of effectiveness. Historically, the modern investigation of manual treatment methods represents an aberration in this process. With the advent of social support and funding for research at the end of the 20th�Century, there was an underlying presumption that the long-term practice of these methods provided a sound clinical wisdom on which to ground RCTs, bypassing mechanistic studies. The early emphasis on clinical trials has illuminated the gaps in understanding of appropriate indications for treatment, dosage and duration of care, consistency of treatment application, and the appropriate outcome measures to monitor results. In response, funding agencies in North America have renewed research emphasis on the potential mechanisms of effect. Data from this work is expected to inform future clinical research questions, and subsequently lead to well-grounded studies that are likely to yield more complete evidence regarding appropriate and effective care.
Safety of Manual Treatment
Choosing an intervention should always be tempered by the risk of adverse events or harm. Adverse events associated with manual treatment can be classified into two categories: 1) benign, minor or non-serious and 2) serious. Generally those that are benign are transient, mild to moderate in intensity, have little effect on activities, and are short lasting. Most commonly, these involve pain or discomfort to the musculoskeletal system. Less commonly, nausea, dizziness or tiredness are reported. Serious adverse events are disabling, require hospitalization and may be life-threatening. The most documented and discussed serious adverse event associated with spinal manipulation (specifically to the cervical spine) is vertebrobasilar artery (VBA) stroke. Less commonly reported are serious adverse events associated with lumbar spine manipulation, including lumbar disc herniation and cauda equina syndrome.
Estimates of serious adverse events as a result of spinal manipulation have been uncertain and varied. Much of the available evidence has been relatively poor due to challenges in establishing accurate risk estimates for rare events. Such estimates are best derived from sound population based studies, preferably those that are prospective in nature.
Estimates of VBA stroke subsequent to cervical spine manipulation range from one event in 200,000 treatments to one in several million. In a subsequent landmark population-based study, Cassidy et al revisited the issue using case-control and case-crossover designs to evaluate over 100 million person-years of data. The authors confirmed that VBA stroke is a very rare event in general. They stated, “We found no evidence of excess risk of VBA stroke associated with chiropractic care compared to primary care.” They further concluded, “The increased risk of VBA stroke associated with chiropractic and PCP (primary care physician) visits is likely due to patients with headache and neck pain from VBA dissection seeking care before their stroke.” In regards to benign adverse reactions, cervical spine manipulation has been shown to be associated with an increased risk when compared to mobilization.
Appropriately, the risk-benefit of cervical spine manipulation has been debated. As anticipated, new research can change what is known about the benefit of manual treatment for neck pain. Currently, the evidence suggests that it has some benefit. It has been suggested that the choice between mobilization and manipulation should be informed by patient preference.
Estimates of cervical or lumbar disc herniation are also uncertain, and are based on case studies and case series. It has been estimated that the risk of a serious adverse event, including lumbar disc herniation is approximately 1 per million patient visits. Cauda equina syndrome is estimated to occur much less frequently, at 1 per several million visits.
Safety of Manual Treatment in Children
The true incidence of serious adverse events in children as a result of spinal manipulation remains unknown. A systematic review published in 2007 identified 14 cases of direct adverse events involving neurologic or musculoskeletal events, nine of which were considered serious (eg. subarachnoid hemorrhage, paraplegia, etc.). Another 20 cases of indirect adverse events were identified (delayed diagnosis, inappropriate application of spinal manipulation for serious medical conditions). The review authors note that case reports and case series are a type of “passive” surveillance, and as such don’t provide information regarding incidence. Further, this type of reporting of adverse events is recognized to underestimate true risk.
Importantly, the authors postulate that a possible reason for incorrect diagnosis (for example. delayed diagnosis, inappropriate treatment with spinal manipulation) is due to lack of sufficient pediatric training. They cite their own survey�which found that in a survey of 287 chiropractors and osteopaths, 78% reported one semester or less of formal pediatric education and 72% received no pediatric clinical training. We find this particularly noteworthy.
Limitations of the Report Conclusions
The conclusions in this report regarding the strength of evidence of presence or absence of effectiveness are predicated on the rules chosen for which there are no absolute standards. Different evidence grading systems and rules regarding impact of study quality may lead to different conclusions. However, we have applied a synthesis methodology consistent with the latest recommendations from authoritative organizations involved in setting standards for evidence synthesis. Although we used a comprehensive literature search strategy we may not have identified all relevant RCTs, guidelines, and technology reports. Conditions for which this report concludes the evidence currently shows manual treatment to be effective or even ineffective, sometimes rests on a single RCT with adequate statistical power and low risk of bias. Additional high quality RCTs on the same topics have a substantial likelihood of changing the conclusions. Including only English language reviews and trials may be considered another limitation of this report leading to language bias; however, the impact of excluding non-English trials from meta-analyses and systematic reviews is conflicting, and the incidence of randomized trials published in non-English journals is declining. Another potential limitation of this report is the lack of critical appraisal of the systematic reviews and clinical guidelines included in the report. Systematic reviews and clinical guidelines can differ widely in methodologic quality and risk of bias. While critical appraisal of the included reviews and guidelines would be ideal, it was beyond the scope of the present report. When drawing conclusions about relative effectiveness of different forms of manual treatments it is acknowledged that it has usually not been possible to isolate or quantify the specific effects of the interventions from the non-specific (contextual) effect of patient-provider interaction. It was beyond the scope of this report to assess the magnitude of the effectiveness of the different manual therapies relative to the therapies to which comparisons were made. However, if moderate or high quality evidence of effectiveness was established the therapy was interpreted as a viable treatment option, but not necessarily the most effective treatment available. We recognize that findings from studies using a nonrandomized design (for example. observational studies, cohort studies, prospective clinical series and case reports) can yield important preliminary evidence on potential mechanisms and plausibility of treatment effects. However, the primary purpose of this report is to summarize the results of studies designed to specifically address treatment efficacy and effectiveness from which claims of clinical utility, consistent with that literature, may be considered defensible. Therefore, the evidence base on the effects of care was restricted to RCTs.
Conclusions
Spinal manipulation/mobilization is effective in adults for acute, subacute, and chronic low back pain; for migraine and cervicogenic headache; cervicogenic dizziness; and a number of upper and lower extremity joint conditions. Thoracic spinal manipulation/mobilization is effective for acute/subacute neck pain, and, when combined with exercise, cervical spinal/manipulation is effective for acute whiplash-associated disorders and for chronic neck pain. The evidence is inconclusive for cervical manipulation/mobilization alone for neck pain of any duration, and for any type of manipulation/mobilization for mid back pain, sciatica, tension-type headache, coccydynia, temporomandibular joint disorders, fibromyalgia, premenstrual syndrome, and pneumonia in older adults. Spinal manipulation is not effective for asthma and dysmenorrhea when compared to sham manipulation, or for Stage 1 hypertension when added to an antihypertensive diet. For children, the evidence is inconclusive regarding the effectiveness of spinal manipulation/mobilization for otitis media and enuresis, but shows it is not effective for infantile colic and for improving lung function in asthma when compared to sham manipulation.
The evidence regarding massage shows that for adults it is an effective treatment option for chronic LBP and chronic neck pain. The evidence is inconclusive for knee osteoarthritis, fibromyalgia, myofascial pain syndrome, migraine headache, and premenstrual syndrome. For children, the evidence is inconclusive for asthma and infantile colic.
Competing interests
All authors are trained as doctors of chiropractic but are now full time professional researchers.
Authors’ contributions
GB was responsible for the methodology used to select and summarize the evidence, for organizing and participating in the analysis of the evidence and formulating conclusions and drafting and finalizing the report.
MH participated in analyzing the evidence and formulating conclusions for the majority of the musculoskeletal conditions and the different types of headache.
RE participated in analyzing the evidence and formulating conclusion for part of the musculoskeletal and non-musculoskeletal conditions and providing substantial input to the background and discussion sections.
BL was responsible for retrieving the research articles and providing draft summary statements for all conditions as well as participating in drafting and proof reading the manuscript.
JT was responsible for conceiving and drafting the section on translation of research into action and providing substantial input to the background and discussion sections. All authors have read and approved the final manuscript.
Includes the criteria used for evaluating risk of bias from randomized controlled trials not included within systematic reviews, evidence based guidelines, or health technology assessments.
The UK General Chiropractic Council provided the funding for this scientific evidence report.
Della Shupe, librarian at NWHSU, is acknowledged for helping design and perform the detailed search strategy used for the report.
In conclusion, the results of the above research study determined that manual therapies, such as manipulation and/or mobilization are effective in adults for acute, subacute and chronic low back pain, migraine and cervicogenic headache, cervicogenic dizziness, as well as for several extremity joint conditions and acute/subacute neck pain. The clinical and experimental evidence was inconclusive alone for some cases of neck and back pain, sciatica, tension-type headache coccydynia, temporomandibular joint disorders, fibromyalgia, premenstrual syndrome and pneumonia in older adults.� Manual therapies, such as manipulation and/or mobilization were not effective for asthma and dysmenorrhea and well as for otitis media and enuresis or infantile colic and asthma.
Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Sciatica
Sciatica is referred to as a collection of symptoms rather than a single type of injury or condition. The symptoms are characterized as radiating pain, numbness and tingling sensations from the sciatic nerve in the lower back, down the buttocks and thighs and through one or both legs and into the feet. Sciatica is commonly the result of irritation, inflammation or compression of the largest nerve in the human body, generally due to a herniated disc or bone spur.
Goldberg M. On evidence and evidence-based medicine: lessons from the philosophy of science.�Soc Sci Med.�2006;62:2621�2632. doi: 10.1016/j.socscimed.2005.11.031.�[PubMed]�[Cross Ref]
Nelson LH. In:�In Feminist epistemologies.�Alcoff, Potter E, editor. 1993. Epistemological communities; pp. 121�160.
Lavis JN, Robertson D, Woodside JM, McLeod CB, Abelson J. How can research organizations more effectively transfer research knowledge to decision makers?�Milbank Q.�2003;81:221�222. doi: 10.1111/1468-0009.t01-1-00052.�[PMC free article]�[PubMed]�[Cross Ref]
Straus SE, Tetroe J, Graham I. Defining knowledge translation.�CMAJ.�2009;181:165�168.[PMC free article]�[PubMed]
Muir Gray JA.�Evidence Based Healthcare How to make Health Policy and Management Decisions.2. Harcourt Publishers Limited; 2001.
Guyatt G, Cook D, Haynes B. Evidence based medicine has come a long way.�BMJ.�2004;329:990�991. doi: 10.1136/bmj.329.7473.990.�[PMC free article]�[PubMed]�[Cross Ref]
Lambert H. Accounting for EBM: notions of evidence in medicine.�Soc Sci Med.�2006;62:2633�2645. doi: 10.1016/j.socscimed.2005.11.023.�[PubMed]�[Cross Ref]
Davey Smith G, Egger M. Incommunicable knowledge? Interpreting and applying the results of clinical trials and meta-analyses.�J Clin Epidemiol.�1998;51:289�295. doi: 10.1016/S0895-4356(97)00293-X.�[PubMed]�[Cross Ref]
Schatter A, Fletcher RH. Research evidence and the individual patient.�Quarterly Journal of Medicine.�2003;96:1�5.�[PubMed]
Triano JJ. What constitutes evidence for best practice?�J Manipulative Physiol Ther.�2008;31:637�643. doi: 10.1016/j.jmpt.2008.10.009.�[PubMed]�[Cross Ref]
Greenhalgh T, Hurwitz B. Narrative based medicine; Why study narrative?�BMJ.�1999;318:48�50.[PMC free article]�[PubMed]
Hope T. Evidence-based patient choice and psychiatry.�Evid Based Ment Health.�2002;5:100�101. doi: 10.1136/ebmh.5.4.100.�[PubMed]�[Cross Ref]
Evidence-based patient choice: Inevitable or impossible?�Oxford University Press; 2001.
Shaughnessy AF, Slawson DC, Becker L. Clinical jazz: harmonizing clinical experience and evidence-based medicine.�J Fam Pract.�1998;47:425�428.�[PubMed]
Straus SE. What’s the E for EBM?�BMJ.�2004;328:535�536. doi: 10.1136/bmj.328.7439.535.[PMC free article]�[PubMed]�[Cross Ref]
Marmot MG. Evidence based policy or policy based evidence?�BMJ.�2004;328:906�907. doi: 10.1136/bmj.328.7445.906.�[PMC free article]�[PubMed]�[Cross Ref]
Chou R, Huffman LH. Nonpharmacologic therapies for acute and chronic low back pain: a review of the evidence for an American Pain Society/American College of Physicians clinical practice guideline.�Ann Intern Med.�2007;147:492�504.�[PubMed]
Haynes RB, Devereaux PJ, Guyatt GH. Physicians’ and patients’ choices in evidence based practice.�BMJ.�2002;324:1350. doi: 10.1136/bmj.324.7350.1350.�[PMC free article]�[PubMed]�[Cross Ref]
Gordon EJ. The political contexts of evidence-based medicine: policymaking for daily hemodialysis.�Soc Sci Med.�2006;62:2707�2719. doi: 10.1016/j.socscimed.2005.11.024.�[PubMed]�[Cross Ref]
Savigny P, Watson P, Underwood M. Early management of persistent non-specific low back pain: summary of NICE guidance.�BMJ.�2009;338:b1805. doi: 10.1136/bmj.b1805.�[PubMed]�[Cross Ref]
Chou R, Qaseem A, Snow V, Casey D, Cross JT Jr, Shekelle P. Diagnosis and treatment of low back pain: a joint clinical practice guideline from the American College of Physicians and the American Pain Society.�Ann Intern Med.�2007;147:478�491.�[PubMed]
Airaksinen O, Brox JI, Cedraschi C, Hildebrandt J, Klaber-Moffett J, Kovacs F. Chapter 4. European guidelines for the management of chronic nonspecific low back pain.�Eur Spine J.�2006;15(Suppl 2):S192�S300. doi: 10.1007/s00586-006-1072-1.�[PMC free article]�[PubMed]�[Cross Ref]
van Tulder M, Becker A, Bekkering T, Breen A, Del Real MT, Hutchinson A. Chapter 3. European guidelines for the management of acute nonspecific low back pain in primary care.�Eur Spine J.�2006;15(Suppl 2):S169�S191. doi: 10.1007/s00586-006-1071-2.�[PMC free article]�[PubMed][Cross Ref]
Assendelft WJ, Morton SC, Yu EI, Suttorp MJ, Shekelle PG. Spinal manipulative therapy for low back pain.�Cochrane Database Syst Rev.�2004. p. CD000447.�[PubMed]
van Tulder MW, Koes B, Malmivaara A. Outcome of non-invasive treatment modalities on back pain: an evidence-based review.�Eur Spine J.�2006;15(Suppl 1):S64�S81. doi: 10.1007/s00586-005-1048-6.�[PMC free article]�[PubMed]�[Cross Ref]
Lawrence DJ, Meeker W, Branson R, Bronfort G, Cates JR, Haas M. Chiropractic management of low back pain and low back-related leg complaints: a literature synthesis.�J Manipulative Physiol Ther.�2008;31:659�674. doi: 10.1016/j.jmpt.2008.10.007.�[PubMed]�[Cross Ref]
Bronfort G, Haas M, Evans R, Kawchuk G, Dagenais S. Evidence-informed management of chronic low back pain with spinal manipulation and mobilization.�Spine J.�2008;8:213�225. doi: 10.1016/j.spinee.2007.10.023.�[PubMed]�[Cross Ref]
Bronfort G, Haas M, Evans RL, Bouter LM. Efficacy of spinal manipulation and mobilization for low back pain and neck pain: a systematic review and best evidence synthesis.�Spine J.�2004;4:335�356. doi: 10.1016/j.spinee.2003.06.002.�[PubMed]�[Cross Ref]
Furlan AD, Imamura M, Dryden T, Irvin E. Massage for Low Back Pain: An Updated Systematic Review Within the Framework of the Cochrane Back Review Group.�Spine.�2009;34:1669�1684. doi: 10.1097/BRS.0b013e3181ad7bd6.�[PubMed]�[Cross Ref]
National Institute for Health and Clinical Excellence. Low back pain: Early management of persistent non-specific low back pain.�Clinical guideline.�2009;88
Hallegraeff JM, de Greef M, Winters JC, Lucas C. Manipulative therapy and clinical prediction criteria in treatment of acute nonspecific low back pain.�Percept Mot Skills.�2009;108:196�208. doi: 10.2466/PMS.108.1.196-208.�[PubMed]�[Cross Ref]
Rasmussen J, Laetgaard J, Lindecrona AL, Qvistgaard E, Bliddal H. Manipulation does not add to the effect of extension exercises in chronic low-back pain (LBP). A randomized, controlled, double blind study.�Joint Bone Spine.�2008;75:708�713.�[PubMed]
Little P, Lewith G, Webley F, Evans M, Beattie A, Middleton K. Randomised controlled trial of Alexander technique lessons, exercise, and massage (ATEAM) for chronic and recurrent back pain.�Br J Sports Med.�2008;42:965�968. doi: 10.1136/bjsm.2007.039560.�[PubMed]�[Cross Ref]
Wilkey A, Gregory M, Byfield D, McCarthy PW. A comparison between chiropractic management and pain clinic management for chronic low-back pain in a national health service outpatient clinic.�J Altern Complement Med.�2008;14:465�473. doi: 10.1089/acm.2007.0796.�[PubMed]�[Cross Ref]
Bogefeldt J, Grunnesjo MI, Svardsudd K, Blomberg S. Sick leave reductions from a comprehensive manual therapy programme for low back pain: the Gotland Low Back Pain Study.�Clin Rehabil.�2008;22:529�541. doi: 10.1177/0269215507087294.�[PubMed]�[Cross Ref]
Hancock MJ, Maher CG, Latimer J, McLachlan AJ, Cooper CW, Day RO. Assessment of diclofenac or spinal manipulative therapy, or both, in addition to recommended first-line treatment for acute low back pain: a randomised controlled trial.�Lancet.�2007;370:1638�1643. doi: 10.1016/S0140-6736(07)61686-9.�[PubMed]�[Cross Ref]
Ferreira ML, Ferreira PH, Latimer J, Herbert RD, Hodges PW, Jennings MD. Comparison of general exercise, motor control exercise and spinal manipulative therapy for chronic low back pain: A randomized trial.�Pain.�2007;131:31�37. doi: 10.1016/j.pain.2006.12.008.�[PubMed]�[Cross Ref]
Eisenberg DM, Post DE, Davis RB, Connelly MT, Legedza AT, Hrbek AL. Addition of choice of complementary therapies to usual care for acute low back pain: a randomized controlled trial.�Spine.�2007;32:151�158. doi: 10.1097/01.brs.0000252697.07214.65.�[PubMed]�[Cross Ref]
Hondras MA, Long CR, Cao Y, Rowell RM, Meeker WC. A randomized controlled trial comparing 2 types of spinal manipulation and minimal conservative medical care for adults 55 years and older with subacute or chronic low back pain.�J Manipulative Physiol Ther.�2009;32:330�343. doi: 10.1016/j.jmpt.2009.04.012.�[PubMed]�[Cross Ref]
Mohseni-Bandpei MA, Critchley J, Staunton T. A prospective randomised controlled trial of spinal manipulation and ultrasound in the treatment of chronic low back pain.�Physiotherapy.�2006;92:34�42. doi: 10.1016/j.physio.2005.05.005.�[Cross Ref]
Beyerman KL, Palmerino MB, Zohn LE, Kane GM, Foster KA. Efficacy of treating low back pain and dysfunction secondary to osteoarthritis: chiropractic care compared with moist heat alone.�J Manipulative Physiol Ther.�2006;29:107�114. doi: 10.1016/j.jmpt.2005.10.005.�[PubMed][Cross Ref]
Poole H, Glenn S, Murphy P. A randomised controlled study of reflexology for the management of chronic low back pain.�Eur J Pain.�2007;11:878�887. doi: 10.1016/j.ejpain.2007.01.006.�[PubMed][Cross Ref]
Zaproudina N, Hietikko T, Hanninen OO, Airaksinen O. Effectiveness of traditional bone setting in treating chronic low back pain: a randomised pilot trial.�Complement Ther Med.�2009;17:23�28. doi: 10.1016/j.ctim.2008.08.005.�[PubMed]�[Cross Ref]
Australian Acute Musculoskeletal Pain Guidelines Group.�Evidence-Based Management of Acute Musculoskeletal Pain.�Bowen Hills QLD, Australian Academic Press Pty. Ltd; 2003.
Bussieres AE, Taylor JA, Peterson C. Diagnostic imaging practice guidelines for musculoskeletal complaints in adults-an evidence-based approach-part 3: spinal disorders.�J Manipulative Physiol Ther.�2008;31:33�88. doi: 10.1016/j.jmpt.2007.11.003.�[PubMed]�[Cross Ref]
Schiller L. Effectiveness of spinal manipulative therapy in the treatment of mechanical thoracic spine pain: a pilot randomized clinical trial.�J Manipulative Physiol Ther.�2001;24:394�401. doi: 10.1067/mmt.2001.116420.�[PubMed]�[Cross Ref]
Cleland JA, Childs JD, McRae M, Palmer JA, Stowell T. Immediate effects of thoracic manipulation in patients with neck pain: a randomized clinical trial.�Man Ther.�2005;10:127�135. doi: 10.1016/j.math.2004.08.005.�[PubMed]�[Cross Ref]
Savolainen A, Ahlberg J, Nummila H, Nissinen M. Active or passive treatment for neck-shoulder pain in occupational health care? A randomized controlled trial.�Occup Med (Lond)�2004;54:422�424. doi: 10.1093/occmed/kqh070.�[PubMed]�[Cross Ref]
Allison GT, Nagy BM, Hall T. A randomized clinical trial of manual therapy for cervico-brachial pain syndrome — a pilot study.�Man Ther.�2002;7:95�102. doi: 10.1054/math.2002.0453.�[PubMed][Cross Ref]
Bergman GJ, Winters JC, Groenier KH, Pool JJ, Meyboom-de Jong B, Postema K. Manipulative therapy in addition to usual medical care for patients with shoulder dysfunction and pain: a randomized, controlled trial.�Ann Intern Med.�2004;141:432�439.�[PubMed]
Winters JC, Sobel JS, Groenier KH, Arendzen HJ, Meyboom-de Jong B. Comparison of physiotherapy, manipulation, and corticosteroid injection for treating shoulder complaints in general practice: randomised, single blind study.�BMJ.�1997;314:1320�1325.�[PMC free article]�[PubMed]
Winters JC, Jorritsma W, Groenier KH, Sobel JS, Meyboom-de Jong B, Arendzen HJ. Treatment of shoulder complaints in general practice: long term results of a randomised, single blind study comparing physiotherapy, manipulation, and corticosteroid injection.�BMJ.�1999;318:1395�1396.[PMC free article]�[PubMed]
Haldeman S, Carroll L, Cassidy D, Schubert J, Nygren A. The Bone and Joint Decade 2000-2010 Task Force on Neck Pain and Its Associated Disorders: executive summary.�Spine.�2008;33:S5�S7. doi: 10.1097/BRS.0b013e3181643f40.�[PubMed]�[Cross Ref]
Hurwitz EL, Carragee EJ, Velde G van der, Carroll LJ, Nordin M, Guzman J. Treatment of neck pain: noninvasive interventions: results of the Bone and Joint Decade 2000-2010 Task Force on Neck Pain and Its Associated Disorders.�J Manipulative Physiol Ther.�2009;32:S141�S175. doi: 10.1016/j.jmpt.2008.11.017.�[PubMed]�[Cross Ref]
Childs JD, Cleland JA, Elliott JM, Teyhen DS, Wainner RS, Whitman JM. Neck pain: Clinical practice guidelines linked to the International Classification of Functioning, Disability, and Health from the Orthopedic Section of the American Physical Therapy Association.�J Orthop Sports Phys Ther.�2008;38:A1�A34.�[PubMed]
Ernst E. Chiropractic spinal manipulation for neck pain: a systematic review.�J Pain.�2003;4:417�421. doi: 10.1067/S1526-5900(03)00735-1.�[PubMed]�[Cross Ref]
Gross AR, Hoving JL, Haines TA, Goldsmith CH, Kay T, Aker P. Manipulation and mobilisation for mechanical neck disorders.�Cochrane Database Syst Rev.�2004. p. CD004249.�[PubMed]
Vernon HT, Humphreys BK, Hagino CA. A systematic review of conservative treatments for acute neck pain not due to whiplash.�J Manipulative Physiol Ther.�2005;28:443�448. doi: 10.1016/j.jmpt.2005.06.011.�[PubMed]�[Cross Ref]
Ezzo J, Haraldsson BG, Gross AR, Myers CD, Morien A, Goldsmith CH. Massage for mechanical neck disorders: a systematic review.�Spine (Phila Pa 1976)�2007;32:353�362.�[PubMed]
Hakkinen A, Salo P, Tarvainen U, Wiren K, Ylinen J. Effect of manual therapy and stretching on neck muscle strength and mobility in chronic neck pain.�J Rehabil Med.�2007;39:575�579. doi: 10.2340/16501977-0094.�[PubMed]�[Cross Ref]
Gonzalez-Iglesias J, Fernandez-de-las-Penas C, Cleland JA, Gutierrez-Vega MR. Thoracic spine manipulation for the management of patients with neck pain: a randomized clinical trial.�J Orthop Sports Phys Ther.�2009;39:20�27.�[PubMed]
Gonzalez-Iglesias J, Fernandez-de-las-Penas C, Cleland JA, Alburquerque-Sendin F, Palomeque-del-Cerro L, Mendez-Sanchez R. Inclusion of thoracic spine thrust manipulation into an electro-therapy/thermal program for the management of patients with acute mechanical neck pain: a randomized clinical trial.�Man Ther.�2009;14:306�313. doi: 10.1016/j.math.2008.04.006.�[PubMed][Cross Ref]
Walker MJ, Boyles RE, Young BA, Strunce JB, Garber MB, Whitman JM. The effectiveness of manual physical therapy and exercise for mechanical neck pain: a randomized clinical trial.�Spine (Phila Pa 1976)�2008;33:2371�2378.�[PubMed]
Cleland JA, Glynn P, Whitman JM, Eberhart SL, MacDonald C, Childs JD. Short-term effects of thrust versus nonthrust mobilization/manipulation directed at the thoracic spine in patients with neck pain: a randomized clinical trial.�Phys Ther.�2007;87:431�440. doi: 10.2522/ptj.20060155.�[PubMed][Cross Ref]
Fernandez-de-las-Penas C, Fernandez-Carnero J, Fernandez A, Lomas-Vega R, Miangolarra-Page JC. Dorsal Manipulation in Whiplash Injury Treatment: A Randomized Controlled Trial.�Journal of Whiplash & Related Disorders.�2004;3:55�72. doi: 10.1300/J180v03n02_05.�[Cross Ref]
Zaproudina N, Hanninen OO, Airaksinen O. Effectiveness of traditional bone setting in chronic neck pain: randomized clinical trial.�J Manipulative Physiol Ther.�2007;30:432�437. doi: 10.1016/j.jmpt.2007.05.004.�[PubMed]�[Cross Ref]
Maigne JY, Chatellier G, Faou ML, Archambeau M. The treatment of chronic coccydynia with intrarectal manipulation: a randomized controlled study.�Spine (Phila Pa 1976)�2006;31:E621�E627.[PubMed]
Bussieres AE, Peterson C, Taylor JA. Diagnostic imaging guideline for musculoskeletal complaints in adults-an evidence-based approach-part 2: upper extremity disorders.�J Manipulative Physiol Ther.�2008;31:2�32. doi: 10.1016/j.jmpt.2007.11.002.�[PubMed]�[Cross Ref]
Green S, Buchbinder R, Hetrick S. Physiotherapy interventions for shoulder pain.�Cochrane Database Syst Rev.�2003. p. CD004258.�[PubMed]
Desmeules F, Cote CH, Fremont P. Therapeutic exercise and orthopedic manual therapy for impingement syndrome: a systematic review.�Clin J Sport.�2003;13:176�182. doi: 10.1097/00042752-200305000-00009.�[PubMed]�[Cross Ref]
Bang MD, Deyle GD. Comparison of supervised exercise with and without manual physical therapy for patients with shoulder impingement syndrome.�J Orthop Sports Phys Ther.�2000;30:126�137.[PubMed]
Bulgen DY, Binder AI, Hazleman BL, Dutton J, Roberts S. Frozen shoulder: prospective clinical study with an evaluation of three treatment regimens.�Ann Rheum Dis.�1984;43:353�360. doi: 10.1136/ard.43.3.353.�[PMC free article]�[PubMed]�[Cross Ref]
Conroy DE, Hayes KW. The effect of joint mobilization as a component of comprehensive treatment for primary shoulder impingement syndrome.�J Orthop Sports Phys Ther.�1998;28:3�14.�[PubMed]
Nicholson GG. The effects of passive joint mobilization on pain and hypomobility associated with adhesive capsulitis of the shoulder.�J Orthop Sports Phys Ther.�1985;6:238�246.�[PubMed]
Winters JC, Jorritsma W, Groenier KH, Sobel JS, Meyboom-de Jong B, Arendzen HJ. Treatment of shoulder complaints in general practice: long term results of a randomised, single blind study comparing physiotherapy, manipulation, and corticosteroid injection.�BMJ.�1999;318:1395�1396.[PMC free article]�[PubMed]
Windt DA van der, Koes BW, Deville W, Boeke AJP, de Jong BA, Bouter LM. Effectiveness of corticosteroid injections versus physiotherapy for treatment of painful stiff shoulder in primary care: randomised trial.�BMJ.�1998;317:1292�1296.�[PMC free article]�[PubMed]
Philadelphia Panel evidence-based clinical practice guidelines on selected rehabilitation interventions for shoulder pain.�Phys Ther.�2001;81:1719�1730.�[PubMed]
Vermeulen HM, Rozing PM, Obermann WR, le Cessie S, Vliet Vlieland TP. Comparison of high-grade and low-grade mobilization techniques in the management of adhesive capsulitis of the shoulder: randomized controlled trial.�Phys Ther.�2006;86:355�368.�[PubMed]
Dolder PA van den, Roberts DL. A trial into the effectiveness of soft tissue massage in the treatment of shoulder pain.�Aust J Physiother.�2003;49:183�188.�[PubMed]
Johnson AJ, Godges JJ, Zimmerman GJ, Ounanian LL. The effect of anterior versus posterior glide joint mobilization on external rotation range of motion in patients with shoulder adhesive capsulitis.�J Orthop Sports Phys Ther.�2007;37:88�99.�[PubMed]
Guler-Uysal F, Kozanoglu E. Comparison of the early response to two methods of rehabilitation in adhesive capsulitis.�Swiss Med Wkly.�2004;134:353�358.�[PubMed]
Piligian G, Herbert R, Hearns M, Dropkin J, Landsbergis P, Cherniack M. Evaluation and management of chronic work-related musculoskeletal disorders of the distal upper extremity.�Am J Ind Med.�2000;37:75�93. doi: 10.1002/(SICI)1097-0274(200001)37:1<75::AID-AJIM7>3.0.CO;2-4.[PubMed]�[Cross Ref]
Bisset L, Paungmali A, Vicenzino B, Beller E. A systematic review and meta-analysis of clinical trials on physical interventions for lateral epicondylalgia.�Br J Sports Med.�2005;39:411�422. doi: 10.1136/bjsm.2004.016170.�[PMC free article]�[PubMed]�[Cross Ref]
McHardy A, Hoskins W, Pollard H, Onley R, Windsham R. Chiropractic treatment of upper extremity conditions: a systematic review.�J Manipulative Physiol Ther.�2008;31:146�159. doi: 10.1016/j.jmpt.2007.12.004.�[PubMed]�[Cross Ref]
Smidt N, Assendelft WJ, Arola H, Malmivaara A, Greens S, Buchbinder R. Effectiveness of physiotherapy for lateral epicondylitis: a systematic review.�Ann Med.�2003;35:51�62. doi: 10.1080/07853890310004138.�[PubMed]�[Cross Ref]
Langen-Pieters P, Weston P, Brantingham JW. A randomized, prospective pilot study comparing chiropractic care and ultrasound for the treatment of lateral epicondylitis.�Eur J Chiro.�2003;50:211�8.
Vicenzino B, Collins D, Wright A. The initial effects of a cervical spine manipulative physiotherapy treatment on the pain and dysfunction of lateral epicondylalgia.�Pain.�1996;68:69�74. doi: 10.1016/S0304-3959(96)03221-6.�[PubMed]�[Cross Ref]
Paungmali A, O’Leary S, Souvlis T, Vicenzino B. Hypoalgesic and sympathoexcitatory effects of mobilization with movement for lateral epicondylalgia.�Phys Ther.�2003;83:374�383.�[PubMed]
Struijs PA, Damen PJ, Bakker EW, Blankevoort L, Assendelft WJ, van Dijk CN. Manipulation of the wrist for management of lateral epicondylitis: a randomized pilot study.�Phys Ther.�2003;83:608�616.�[PubMed]
Vicenzino B, Paungmali A, Buratowski S, Wright A. Specific manipulative therapy treatment for chronic lateral epicondylalgia produces uniquely characteristic hypoalgesia.�Man Ther.�2001;6:205�212. doi: 10.1054/math.2001.0411.�[PubMed]�[Cross Ref]
Smidt N, Windt DA van der, Assendelft WJ, Deville WL, Korthals-de Bos IB, Bouter LM. Corticosteroid injections, physiotherapy, or a wait-and-see policy for lateral epicondylitis: a randomised controlled trial.�Lancet.�2002;359:657�662. doi: 10.1016/S0140-6736(02)07811-X.[PubMed]�[Cross Ref]
Drechsler WI, Knarr JF, Snyder-Mackler L. A comparison of two treatment regimens for lateral epicondylitis: a randomized trial of clinical interventions.�J Sport Rehabil.�1997;6:226�234.
Dwars BJ, Feiter Pde, Patka P, Haarman H. Functional treatment of tennis elbow.�Sports Medicine and Health.�1990. pp. 237�241.
Verhaar JA, Walenkamp GH, van Mameren H, Kester AD, Linden AJ van der. Local corticosteroid injection versus Cyriax-type physiotherapy for tennis elbow.�J Bone Joint Surg Br.�1996;78:128�132.[PubMed]
Bisset L, Beller E, Jull G, Brooks P, Darnell R, Vicenzino B. Mobilisation with movement and exercise, corticosteroid injection, or wait and see for tennis elbow: randomised trial.�BMJ.�2006;333:939. doi: 10.1136/bmj.38961.584653.AE.�[PMC free article]�[PubMed]�[Cross Ref]
Nourbakhsh MR, Fearon FJ. The effect of oscillating-energy manual therapy on lateral epicondylitis: a randomized, placebo-control, double-blinded study.�J Hand Ther.�2008;21:4�13. doi: 10.1197/j.jht.2007.09.005.�[PubMed]�[Cross Ref]
Bjordal JM, Lopes-Martins RA, Joensen J, Couppe C, Ljunggren AE, Stergioulas A. A systematic review with procedural assessments and meta-analysis of low level laser therapy in lateral elbow tendinopathy (tennis elbow)�BMC Musculoskelet Disord.�2008;9:75. doi: 10.1186/1471-2474-9-75.[PMC free article]�[PubMed]�[Cross Ref]
Trinh KV, Phillips SD, Ho E, Damsma K. Acupuncture for the alleviation of lateral epicondyle pain: a systematic review.�Rheumatology (Oxford)�2004;43:1085�1090. doi: 10.1093/rheumatology/keh247.�[PubMed]�[Cross Ref]
American Academy of Orthopaedic Surgeons. Clinical practic guidelines on the diagnosis of carpal tunnel syndrome. 2008.
O’Connor D, Marshall S, Massy-Westropp N. Non-surgical treatment (other than steroid injection) for carpal tunnel syndrome.�Cochrane Database Syst Rev.�2003. p. CD003219.�[PubMed]
Goodyear-Smith F, Arroll B. What can family physicians offer patients with carpal tunnel syndrome other than surgery? A systematic review of nonsurgical management.�Ann Fam Med.�2004;2:267�273. doi: 10.1370/afm.21.�[PMC free article]�[PubMed]�[Cross Ref]
Piazzini DB, Aprile I, Ferrara PE, Bertolini C, Tonali P, Maggi L. A systematic review of conservative treatment of carpal tunnel syndrome.�Clin Rehabil.�2007;21:299�314. doi: 10.1177/0269215507077294.�[PubMed]�[Cross Ref]
Davis PT, Hulbert JR, Kassak KM, Meyer JJ. Comparative efficacy of conservative medical and chiropractic treatments for carpal tunnel syndrome: a randomized clinical trial.�J Manipulative Physiol Ther.�1998;21:317�326.�[PubMed]
Tal-Akabi A, Rushton A. An investigation to compare the effectiveness of carpal bone mobilisation and neurodynamic mobilisation as methods of treatment for carpal tunnel syndrome.�Man Ther.�2000;5:214�222. doi: 10.1054/math.2000.0355.�[PubMed]�[Cross Ref]
Cibulka MT, White DM, Woehrle J, Harris-Hayes M, Enseki K, Fagerson TL. Hip pain and mobility deficits–hip osteoarthritis: clinical practice guidelines linked to the international classification of functioning, disability, and health from the orthopaedic section of the American Physical Therapy Association.�J Orthop Sports Phys Ther.�2009;39:A1�25.�[PMC free article]�[PubMed]
Bussieres AE, Taylor JA, Peterson C. Diagnostic imaging practice guidelines for musculoskeletal complaints in adults–an evidence-based approach. Part 1. Lower extremity disorders.�J Manipulative Physiol Ther.�2007;30:684�717. doi: 10.1016/j.jmpt.2007.10.004.�[PubMed]�[Cross Ref]
Brantingham JW, Globe G, Pollard H, Hicks M, Korporaal C, Hoskins W. Manipulative therapy for lower extremity conditions: expansion of literature review.�J Manipulative Physiol Ther.�2009;32:53�71. doi: 10.1016/j.jmpt.2008.09.013.�[PubMed]�[Cross Ref]
Hoeksma HL, Dekker J, Ronday HK, Heering A, van der LN, Vel C. Comparison of manual therapy and exercise therapy in osteoarthritis of the hip: a randomized clinical trial.�Arthritis Rheum.�2004;51:722�729. doi: 10.1002/art.20685.�[PubMed]�[Cross Ref]
National Institute for Health and Clinical Excellence. Osteoarthritis: National clinical guideline for care and management in adults.�Clinical guideline 59.�2008.
Licciardone JC, Stoll ST, Cardarelli KM, Gamber RG, Swift JN Jr, Winn WB. A randomized controlled trial of osteopathic manipulative treatment following knee or hip arthroplasty.�J Am Osteopath Assoc.�2004;104:193�202.�[PubMed]
Hernandez-Molina G, Reichenbach S, Zhang B, Lavalley M, Felson DT. Effect of therapeutic exercise for hip osteoarthritis pain: results of a meta-analysis.�Arthritis Rheum.�2008;59:1221�1228. doi: 10.1002/art.24010.�[PMC free article]�[PubMed]�[Cross Ref]
Deyle GD, Henderson NE, Matekel RL, Ryder MG, Garber MB, Allison SC. Effectiveness of manual physical therapy and exercise in osteoarthritis of the knee. A randomized, controlled trial.�Ann Intern Med.�2000;132:173�181.�[PubMed]
Deyle GD, Allison SC, Matekel RL, Ryder MG, Stang JM, Gohdes DD. Physical therapy treatment effectiveness for osteoarthritis of the knee: a randomized comparison of supervised clinical exercise and manual therapy procedures versus a home exercise program.�Phys Ther.�2005;85:1301�1317.[PubMed]
Crossley K, Bennell K, Green S, Cowan S, McConnell J. Physical therapy for patellofemoral pain: a randomized, double-blinded, placebo-controlled trial.�Am J Sports Med.�2002;30:857�865.[PubMed]
Suter E, McMorland G, Herzog W, Bray R. Conservative lower back treatment reduces inhibition in knee-extensor muscles: a randomized controlled trial.�J Manipulative Physiol Ther.�2000;23:76�80. doi: 10.1016/S0161-4754(00)90071-X.�[PubMed]�[Cross Ref]
Bennell KL, Hinman RS, Metcalf BR, Buchbinder R, McConnell J, McColl G. Efficacy of physiotherapy management of knee joint osteoarthritis: a randomised, double blind, placebo controlled trial.�Ann Rheum Dis.�2005;64:906�912. doi: 10.1136/ard.2004.026526.[PMC free article]�[PubMed]�[Cross Ref]
Moss P, Sluka K, Wright A. The initial effects of knee joint mobilization on osteoarthritic hyperalgesia.�Man Ther.�2007;12:109�118. doi: 10.1016/j.math.2006.02.009.�[PubMed]�[Cross Ref]
Tucker M, Brantingham JW, Myburg C. The relative effectiveness of a non-sterodial anti-inflammatory medicaion (meloxicam) versus manipulation in the treatment of osteoarthritis of the knee.�Eur J Chiro.�2003;50:163�84.
Rowlands B, Brantingham JW. The efficacy of patella mobilisation in patients suffering from patellofemoral pain syndrome.�J Neuromusculoskel System.�1999;7:9.
Stakes N, Myburgh C, Brantingham JW, Moyer R, Jensen M, Globe G. A prospective randomized clinical trial to determine efficacy of combined spinal manipulation and patella mobilization compared to patella mobilization alone in the conservative management of patellofemoral pain syndrome.�J Am Chiro Assoc.�2006;43:11�8.
Taylor K, Brantingham JW. An investigation into the effect of exercise combined with patella mobilisation/manipulation in the treatment of patellofemoral pain syndrome.�Eur J Chiro.�2003;51:17.
Pollard H, Ward G, Hoskins W, Hardy K. The effect of a manual therapy knee protocol on osteoarthritic knee pain: a randomised controlled trial.�JCCA J Can Chiropr Assoc.�2008;52:229�242.�[PMC free article]�[PubMed]
Perlman AI, Sabina A, Williams AL, Njike VY, Katz DL. Massage therapy for osteoarthritis of the knee: a randomized controlled trial.�Arch Intern Med.�2006;166:2533�2538. doi: 10.1001/archinte.166.22.2533.�[PubMed]�[Cross Ref]
Vavken P, Arrich F, Schuhfried O, Dorotka R. Effectiveness of pulsed electromagnetic field therapy in the management of osteoarthritis of the knee: a meta-analysis of randomized controlled trials.�J Rehabil Med.�2009;41:406�411. doi: 10.2340/16501977-0374.�[PubMed]�[Cross Ref]
Hulme J, Robinson V, DeBie R, Wells G, Judd M, Tugwell P. Electromagnetic fields for the treatment of osteoarthritis.�Cochrane Database Syst Rev.�2002. p. CD003523.�[PubMed]
White A, Foster NE’, Cummings M, Barlas P. Acupuncture treatment for chronic knee pain: a systematic review.�Rheumatology (Oxford)�2007;46:384�390. doi: 10.1093/rheumatology/kel413.[PubMed]�[Cross Ref]
Fransen M, McConnell S. Exercise for osteoarthritis of the knee.�Cochrane Database Syst Rev.�2008. p. CD004376.�[PubMed]
Bjordal JM, Johnson MI, Lopes-Martins RA, Bogen B, Chow R, Ljunggren AE. Short-term efficacy of physical interventions in osteoarthritic knee pain. A systematic review and meta-analysis of randomised placebo-controlled trials.�BMC Musculoskelet Disord.�2007;8:51. doi: 10.1186/1471-2474-8-51.�[PMC free article]�[PubMed]�[Cross Ref]
Wees PJ van der, Lenssen AF, Hendriks EJ, Stomp DJ, Dekker J, de Bie RA. Effectiveness of exercise therapy and manual mobilisation in ankle sprain and functional instability: a systematic review.�Aust J Physiother.�2006;52:27�37.�[PubMed]
Vicenzino B, Branjerdporn M, Teys P, Jordan K. Initial changes in posterior talar glide and dorsiflexion of the ankle after mobilization with movement in individuals with recurrent ankle sprain.�J Orthop Sports Phys Ther.�2006;36:464�471. doi: 10.2519/jospt.2006.2265.�[PubMed][Cross Ref]
Eisenhart AW, Gaeta TJ, Yens DP. Osteopathic manipulative treatment in the emergency department for patients with acute ankle injuries.�J Am Osteopath Assoc.�2003;103:417�421.�[PubMed]
Green T, Refshauge K, Crosbie J, Adams R. A randomized controlled trial of a passive accessory joint mobilization on acute ankle inversion sprains.�Phys Ther.�2001;81:984�994.�[PubMed]
Pellow JE, Brantingham JW. The efficacy of adjusting the ankle in the treatment of subacute and chronic grade I and grade II ankle inversion sprains.�J Manipulative Physiol Ther.�2001;24:17�24. doi: 10.1067/mmt.2001.112015.�[PubMed]�[Cross Ref]
Coetzer D, Brantingham JW, Nook B. The relative effectiveness of piroxicam compared to manipulation in the treatment of acute grades 1 and 2 inversion ankle sprains.�J Neuromusculoskel System.�2001;9:9�12.
Collins N. P. Vicenzino B. The initial effects of a Mulligan’s mobilization with movement technique on dorsiflexion and pain in subacute ankle sprains.�Man Ther.�2004;9:77�82. doi: 10.1016/S1356-689X(03)00101-2.�[PubMed]�[Cross Ref]
Lopez-Rodriguez S, Fernandez de-Las-Penas C, Alburquerque-Sendin F, Rodriguez-Blanco C, Palomeque-del-Cerro L. Immediate effects of manipulation of the talocrural joint on stabilometry and baropodometry in patients with ankle sprain.�J Manipulative Physiol Ther.�2007;30:186�192. doi: 10.1016/j.jmpt.2007.01.011.�[PubMed]�[Cross Ref]
Kohne E, Jones A, Korporaal C, Price JL, Brantingham JW, Globe G. A prospective, single-blinded, randomized, controlled clinical trial of the effects of manipulation on proprioception and ankle dorsiflexion in chronic recurrect ankle sprain.�J Am Chiro Assoc.�2007;44:7�17.
Dimou E, Brantingham JW, Wood T. A randomized, controlled trial (with blinded observer) of chiropractic manipulation and Achilles stretching vs orthotics for the treatment of plantar fasciitis.�J Am Chiro Assoc.�2004;41:32�42.
Govender N, Kretzmann H, Price J, Brantingham JW, Globe G. A single-blinded randomized placebo-controlled clinical trial of manipulation and mobilization in the treatment of Morton’s neuroma.�J Am Chiro Assoc.�2007;44:9�18.
Shamus J, Shamus E, Gugel RN, Brucker BS, Skaruppa C. The effect of sesamoid mobilization, flexor hallucis strengthening, and gait training on reducing pain and restoring function in individuals with hallux limitus: a clinical trial.�J Orthop Sports Phys Ther.�2004;34:368�376. doi: 10.1016/S8756-3282(04)00007-9.�[PubMed]�[Cross Ref]
Brantingham JW, Guiry S, Kretzmann H, Globe G, Kite V. A pilot study of the efficacy of a conservative chiropractic protocol using graded mobilization and ice in the treatment of sympomatic hallux abductogalvus bunions.�Clin Chiro.�2005;8:117�33. doi: 10.1016/j.clch.2005.06.001.[Cross Ref]
Brooks SC, Potter BT, Rainey JB. Treatment for partial tears of the lateral ligament of the ankle: a prospective trial.�Br Med J (Clin Res Ed)�1981;282:606�607. doi: 10.1136/bmj.282.6264.606.[PMC free article]�[PubMed]�[Cross Ref]
Wynne MM, Burns JM, Eland DC, Conatser RR, Howell JN. Effect of counterstrain on stretch reflexes, hoffmann reflexes, and clinical outcomes in subjects with plantar fasciitis.�J Am Osteopath Assoc.�2006;106:547�556.�[PubMed]
Cleland JA, Abbott JH, Kidd MO, Stockwell S, Cheney S, Gerrard DF. Manual physical therapy and exercise versus electrophysical agents and exercise in the management of plantar heel pain: a multicenter randomized clinical trial.�J Orthop Sports Phys Ther.�2009;39:573�585.�[PubMed]
Lin CW, Moseley AM, Haas M, Refshauge KM, Herbert RD. Manual therapy in addition to physiotherapy does not improve clinical or economic outcomes after ankle fracture.�J Rehabil Med.�2008;40:433�439. doi: 10.2340/16501977-0187.�[PubMed]�[Cross Ref]
McPoil TG, Martin RL, Cornwall MW, Wukich DK, Irrgang JJ, Godges JJ. Heel pain–plantar fasciitis: clinical practice guildelines linked to the international classification of function, disability, and health from the orthopaedic section of the American Physical Therapy Association.�J Orthop Sports Phys Ther.�2008;38:A1�A18.�[PubMed]
Handoll HH, Rowe BH, Quinn KM, de Bie R. Interventions for preventing ankle ligament injuries.�Cochrane Database Syst Rev.�2001. p. CD000018.�[PubMed]
McNeill C.�Temporomandibular Disorders: Guidelines For Classification, Assessment, and Management.�Quintessence Publishing Co, Inc; 1993. Epidemiology; pp. 19�22.
Dworkin SF, Huggins KH, Wilson L, Mancl L, Turner J, Massoth D. A randomized clinical trial using research diagnostic criteria for temporomandibular disorders-axis II to target clinic cases for a tailored self-care TMD treatment program.�J Orofac Pain.�2002;16:48�63.�[PubMed]
McNeely ML, Armijo OS, Magee DJ. A systematic review of the effectiveness of physical therapy interventions for temporomandibular disorders.�Phys Ther.�2006;86:710�725.�[PubMed]
Medlicott MS, Harris SR. A systematic review of the effectiveness of exercise, manual therapy, electrotherapy, relaxation training, and biofeedback in the management of temporomandibular disorder.�Phys Ther.�2006;86:955�973.�[PubMed]
Taylor M, Suvinen T, Reade P. The effect of grade IV distraction mobilization on patients with temporomandibular pain-dysfunction disorder.�Physiotherapy Theory and Practice.�1994;10:129�136. doi: 10.3109/09593989409036389.�[Cross Ref]
Carmeli E, Sheklow SL, Blommenfeld I. Comparitive study of repositioning splint therapy and passive manual range of motion techniques for anterior displaced temporomandibular discs with unstable excursive reduction.�Physiotherapy.�2001;87:26�36. doi: 10.1016/S0031-9406(05)61189-3.[Cross Ref]
De Laat A, Stappaerts K, Papy S. Counseling and physical therapy as treatment for myofascial pain of the masticatory system.�J Orofac Pain.�2003;17:42�49.�[PubMed]
Monaco A, Cozzolino V, Cattaneo R, Cutilli T, Spadaro A. Osteopathic manipulative treatment (OMT) effects on mandibular kinetics: kinesiographic study.�Eur J Paediatr Dent.�2008;9:37�42.[PubMed]
Ismail F, Demling A, Hessling K, Fink M, Stiesch-Scholz M. Short-term efficacy of physical therapy compared to splint therapy in treatment of arthrogenous TMD.�J Oral Rehabil.�2007;34:807�813. doi: 10.1111/j.1365-2842.2007.01748.x.�[PubMed]�[Cross Ref]
Carville SF, Arendt-Nielsen S, Bliddal H, Blotman F, Branco JC, Buskila D. EULAR evidence-based recommendations for the management of fibromyalgia syndrome.�Ann Rheum Dis.�2008;67:536�541. doi: 10.1136/ard.2007.071522.�[PubMed]�[Cross Ref]
Wolfe F, Smythe HA, Yunus MB, Bennett RM, Bombardier C, Goldenberg DL. The American College of Rheumatology 1990 Criteria for the Classification of Fibromyalgia. Report of the Multicenter Criteria Committee.�Arthritis Rheum.�1990;33:160�172. doi: 10.1002/art.1780330203.[PubMed]�[Cross Ref]
Schneider M, Vernon H, Ko G, Lawson G, Perera J. Chiropractic management of fibromyalgia syndrome: a systematic review of the literature.�J Manipulative Physiol Ther.�2009;32:25�40. doi: 10.1016/j.jmpt.2008.08.012.�[PubMed]�[Cross Ref]
Ernst E. Chiropractic treatment for fibromyalgia: a systematic review.�Clin Rheumatol.�2009;28:1175�1178. doi: 10.1007/s10067-009-1217-9.�[PubMed]�[Cross Ref]
Goldenberg DL, Burckhardt C, Crofford L. Management of fibromyalgia syndrome.�JAMA.�2004;292:2388�2395. doi: 10.1001/jama.292.19.2388.�[PubMed]�[Cross Ref]
Blunt KL, Rajwani MH, Guerriero RC. The effectiveness of chiropractic management of fibromyalgia patients: a pilot study.�J Manipulative Physiol Ther.�1997;20:389�399.�[PubMed]
Tyers S, Smith RB. A comparison of cranial electrotherapy stimulation alone or with chiropractic therapies in the treatment of fibromyalgia.�Am Chiropractor.�2001;23:39�41.
Wise P, Walsh M, Littlejohn G. Efficacy of chiropractic treatment on fibromyalgia syndrome; a randomized controlled trial.�Eur J Chiro.�2002;102:321�5.
Panton LB, Figueroa A, Kingsley JD, Hornbuckle L, Wilson J, St John N. Effects of resistance training and chiropractic treatment in women with fibromyalgia.�J Altern Complement Med.�2009;15:321�328. doi: 10.1089/acm.2008.0132.�[PubMed]�[Cross Ref]
Gamber RG, Shores JH, Russo DP, Jimenez C, Rubin BR. Osteopathic manipulative treatment in conjunction with medication relieves pain associated with fibromyalgia syndrome: results of a randomized clinical pilot project.�J Am Osteopath Assoc.�2002;102:321�325.�[PubMed]
Brattberg G. Connective tissue massage in the treatment of fibromyalgia.�Eur J Pain.�1999;3:235�244. doi: 10.1016/S1090-3801(99)90050-2.�[PubMed]�[Cross Ref]
Richards KC, Gibson R, Overton-McCoy AL. Effects of massage in acute and critical care.�AACN Clin Issues.�2000;11:77�96. doi: 10.1097/00044067-200002000-00010.�[PubMed]�[Cross Ref]
Ekici G, Bakar Y, Akbayrak T, Yuksel I. Comparison of manual lymph drainage therapy and connective tissue massage in women with fibromyalgia: a randomized controlled trial.�J Manipulative Physiol Ther.�2009;32:127�133. doi: 10.1016/j.jmpt.2008.12.001.�[PubMed][Cross Ref]
Busch AJ, Barber KA, Overend TJ, Peloso PM, Schachter CL. Exercise for treating fibromyalgia syndrome.�Cochrane Database Syst Rev.�2007. p. CD003786.�[PubMed]
Vernon H, Schneider M. Chiropractic management of myofascial trigger points and myofascial pain syndrome: a systematic review of the literature.�J Manipulative Physiol Ther.�2009;32:14�24. doi: 10.1016/j.jmpt.2008.06.012.�[PubMed]�[Cross Ref]
Gam AN, Warming S, Larsen LH, Jensen B, Hoydalsmo O, Allon I. Treatment of myofascial trigger-points with ultrasound combined with massage and exercise–a randomised controlled trial.�Pain.�1998;77:73�79. doi: 10.1016/S0304-3959(98)00084-0.�[PubMed]�[Cross Ref]
Dardzinski JA, Ostrov BE, Hamann LS. Myofascial pain unresponsive to standard treatment: successful use of a strain and counterstrain technique with physical therapy.�J Clin Rheumatol.�2000;6:169�174. doi: 10.1097/00124743-200008000-00001.�[PubMed]�[Cross Ref]
Greene C, Debias D, Helig D, Nicholas A, England K, Ehrenfeuchter W. The effect of helium-neon laser and osteopathic manipulation on soft-tissue trigger points.�J Am Osteopath Assoc.�1990;90:638�639.
Hanten WP, Olson SL, Butts NL, Nowicki AL. Effectiveness of a home program of ischemic pressure followed by sustained stretch for treatment of myofascial trigger points.�Phys Ther.�2000;80:997�1003.�[PubMed]
Jaeger B, Reeves JL. Quantification of changes in myofascial trigger point sensitivity with the pressure algometer following passive stretch.�Pain.�1986;27:203�210. doi: 10.1016/0304-3959(86)90211-3.�[PubMed]�[Cross Ref]
Hong CZ, Chen YC, Pon CH, Yu J. Immediate effects of various physical medicine modalities on pain threshold of an active myofascial trigger point.�j musculoskel pain.�1993;1:37�53. doi: 10.1300/J094v01n02_04.�[Cross Ref]
Hou CR, Tsai LC, Cheng KF, Chung KC, Hong CZ. Immediate effects of various physical therapeutic modalities on cervical myofascial pain and trigger-point sensitivity.�Arch Phys Med Rehabil.�2002;83:1406�1414. doi: 10.1053/apmr.2002.34834.�[PubMed]�[Cross Ref]
Hanten WP, Barret M, Gillespie-Plesko M, Jump KA, Olson SL. Effects of active head retraction with retraction/extension and occipital release on the pressure pain threshold of cervical and scapular trigger points.�Physiother Theory Pract.�1997;13:285�291. doi: 10.3109/09593989709036475.[Cross Ref]
Fernandez-de-las-Penas C, Alonso-Blanco C, Fernandez-Carnero J, Miangolarra-Page JC. The immediate effects of ischemic compression technique and transverse friction massage on tenderness of active and latent myofascial trigger points: a pilot study.�J Bodywork Mov Ther.�2009;10:3�9. doi: 10.1016/j.jbmt.2005.05.003.�[Cross Ref]
Terrett AC, Vernon H. Manipulation and pain tolerance. A controlled study of the effect of spinal manipulation on paraspinal cutaneous pain tolerance levels.�Am J Phys Med.�1984;63:217�225.[PubMed]
Vernon HT, Aker P, Burns S, Viljakaanen S, Short L. Pressure pain threshold evaluation of the effect of spinal manipulation in the treatment of chronic neck pain: a pilot study.�J Manipulative Physiol Ther.�1990;13:13�16.�[PubMed]
Cote P, Mior SA, Vernon H. The short-term effect of a spinal manipulation on pain/pressure threshold in patients with chronic mechanical low back pain.�J Manipulative Physiol Ther.�1994;17:364�368.�[PubMed]
Atienza-Meseguer A, Fernandez-de-las-Penas C, Navarro-Poza JL, Rodriguez-Blanco C, Bosca-Gandia JJ. Immediate effects of the strain/counterstrain technique in local pain evoked by tender points in the upper trapezius muscle.�Clin Chiro.�2006;9:112�118. doi: 10.1016/j.clch.2006.06.003.[Cross Ref]
Fryer G, Hodgson L. The effect of manual pressure release on myofascial trigger points in the upper trapezius muscle.�J Bodywork Mov Ther.�2005;9:248�255. doi: 10.1016/j.jbmt.2005.02.002.[Cross Ref]
Cephalalgia.�2. Suppl 1. Vol. 24. 2004. The International Classification of Headache Disorders; pp. 9�160.�[PubMed]
Scotish Intercollegiate Guideline Network. Diagnosis and management of headache in adults. 2008.
Astin JA, Ernst E. The effectiveness of spinal manipulation for the treatment of headache disorders: a systematic review of randomized clinical trials.�Cephalalgia.�2002;22:617�623. doi: 10.1046/j.1468-2982.2002.00423.x.�[PubMed]�[Cross Ref]
Bronfort G, Nilsson N, Haas M, Evans R, Goldsmith CH, Assendelft WJ. Non-invasive physical treatments for chronic/recurrent headache.�Cochrane Database Syst Rev.�2004. p. CD001878.[PubMed]
Parker GB, Pryor DS, Tupling H. Why does migraine improve during a clinical trial? Further results from a trial of cervical manipulation for migraine.�Aust N Z J Med.�1980;10:192�198.�[PubMed]
Tuchin PJ, Pollard H, Bonello R. A randomized controlled trial of chiropractic spinal manipulative therapy for migraine.�J Manipulative Physiol Ther.�2000;23:91�95. doi: 10.1016/S0161-4754(00)90073-3.�[PubMed]�[Cross Ref]
Nelson CF, Bronfort G, Evans R, Boline P, Goldsmith C, Anderson AV. The efficacy of spinal manipulation, amitriptyline and the combination of both therapies for the prophylaxis of migraine headaches.�J Manipulative Physiol Ther.�1998;21:511�519.�[PubMed]
Lawler SP, Cameron LD. A randomized, controlled trial of massage therapy as a treatment for migraine.�Ann Behav Med.�2006;32:50�59. doi: 10.1207/s15324796abm3201_6.�[PubMed][Cross Ref]
Linde K, Allais G, Brinkhaus B, Manheimer E, Vickers A, White AR. Acupuncture for migraine prophylaxis.�Cochrane Database Syst Rev.�2009. p. CD001218.�[PMC free article]�[PubMed]
Nestoriuc Y, Martin A, Rief W, Andrasik F. Biofeedback treatment for headache disorders: a comprehensive efficacy review.�Appl Psychophysiol Biofeedback.�2008;33:125�140. doi: 10.1007/s10484-008-9060-3.�[PubMed]�[Cross Ref]
McCrory DC, Penzien DB, Hasselblad V, Gray RN. Evidence Report: Behavioral and Physical Treatments for Tension-type and Cervicogenic Headache.�FCER Research.�2001.
Lenssinck ML, Damen L, Verhagen AP, Berger MY, Passchier J, Koes BW. The effectiveness of physiotherapy and manipulation in patients with tension-type headache: a systematic review.�Pain.�2004;112:381�388. doi: 10.1016/j.pain.2004.09.026.�[PubMed]�[Cross Ref]
Fernandez-de-las-Penas C, Alonso-Blanco C, Cuadrado ML, Miangolarra JC, Barriga FJ, Pareja JA. Are manual therapies effective in reducing pain from tension-type headache?: a systematic review.�Clin J Pain.�2006;22:278�285. doi: 10.1097/01.ajp.0000173017.64741.86.�[PubMed]�[Cross Ref]
Boline PD, Kassak K, Bronfort G, Nelson C, Anderson AV. Spinal manipulation vs. amitriptyline for the treatment of chronic tension-type headaches: a randomized clinical trial.�J Manipulative Physiol Ther.�1995;18:148�154.�[PubMed]
Bove G, Nilsson N. Spinal manipulation in the treatment of episodic tension-type headache: a randomized controlled trial.�JAMA.�1998;280:1576�1579. doi: 10.1001/jama.280.18.1576.[PubMed]�[Cross Ref]
Hanten WP, Olson SL, hodson JL, imler VL, knab VM, Magee JL. The Effectiveness of CV-4 and Resting Position Techniques on Subjects with Tension-Type Headaches.�The Journal of Manual & Manipulative Therapy.�1999;7:64�70.
Demirturk F, Akarcali I, Akbayrak R, Citak I, Inan L. Results of two different manual therapy techniques in chronic tension-type headache.�The Pain Clinic.�2002;14:121�128. doi: 10.1163/156856902760196333.�[Cross Ref]
Donkin RD, Parkin-Smith GF, Gomes AN. Possible effect of chiropractic manipulation and combined manual traction and manipulation on tension-type headache: a pilot study.�Journal of the Neuromusculoskeletal System.�2002;10:89�97.
Ahonen E, Hakumaki M, Mahlamaki S, Partanen J, Riekkinen P, Sivenius J. Effectiveness of acupuncture and physiotherapy on myogenic headache: a comparative study.�Acupunct Electrother Res.�1984;9:141�150.�[PubMed]
Carlsson J, Fahlcrantz A, Augustinsson LE. Muscle tenderness in tension headache treated with acupuncture or physiotherapy.�Cephalalgia.�1990;10:131�141. doi: 10.1046/j.1468-2982.1990.1003131.x.�[PubMed]�[Cross Ref]
Wylie KR, Jackson C, Crawford PM. Does psychological testing help to predict the response to acupuncture or massage/relaxation therapy in patients presenting to a general neurology clinic with headache?�J Tradit Chin Med.�1997;17:130�139.�[PubMed]
Hoyt WH, Shaffer F, Bard DA, Benesler JS, Blankenhorn GD, Gray JH. Osteopathic manipulation in the treatment of muscle-contraction headache.�JAOA.�1979;78:322�325.�[PubMed]
Jay GW, Brunson J, Branson SJ. The effectiveness of physical therapy in the treatment of chronic daily headaches.�Headache.�1989;29:156�162. doi: 10.1111/j.1526-4610.1989.hed2903156.x.[PubMed]�[Cross Ref]
Marcus DA, Scharff L, Turk DC. Nonpharmacological management of headaches during pregnancy.�Psychosom Med.�1995;57:527�535.�[PubMed]
Anderson RE, Seniscal C. A comparison of selected osteopathic treatment and relaxation for tension-type headaches.�Headache.�2006;46:1273�1280. doi: 10.1111/j.1526-4610.2006.00535.x.�[PubMed][Cross Ref]
Linde K, Allais G, Brinkhaus B, Manheimer E, Vickers A, White AR. Acupuncture for tension-type headache.�Cochrane Database Syst Rev.�2009. p. CD007587.�[PMC free article]�[PubMed]
Sjaastad O, Fredriksen TA, Pfaffenrath V. Cervicogenic headache: diagnostic criteria.�Headache.�1998;38:442�445. doi: 10.1046/j.1526-4610.1998.3806442.x.�[PubMed]�[Cross Ref]
Fernandez-de-las-Penas C, Alonso-Blanco C, Cuadrado ML, Pareja JA. Spinal manipulative therapy in the management of cervicogenic headache.�Headache.�2005;45:1260�1263. doi: 10.1111/j.1526-4610.2005.00253_1.x.�[PubMed]�[Cross Ref]
Bitterli J, Graf R, Robert F, Adler R, Mumenthaler M. Zur Objektivierung der manualtherapeutischen BeeinfluBbarkeit des spondylogenen Kopfschmerzes [Objective criteria for the evaluation of chiropractic treatment of spondylotic headache]�Nervenarzt.�1977;48:259�262.[PubMed]
Howe DH, Newcombe RG, Wade MT. Manipulation of the cervical spine — a pilot study.�J R Coll Gen Pract.�1983;33:574�579.�[PMC free article]�[PubMed]
Ammer K, Hein L, Rathkolb O. [Physical therapy in occipital headaches]�Manuelle Med.�1990;28:65�68.
Jull G, Trott P, Potter H, Zito G, Niere K, Shirley D. A randomized controlled trial of exercise and manipulative therapy for cervicogenic headache.�Spine.�2002;27:1835�1843. doi: 10.1097/00007632-200209010-00004.�[PubMed]�[Cross Ref]
Nilsson N, Christensen HW, Hartvigsen J. The effect of spinal manipulation in the treatment of cervicogenic headache.�J Manipulative Physiol Ther.�1997;20:326�330.�[PubMed]
Whittingham W.�The efficacy of cervical adjustments (Toggle recoil) for chronic cervicogenic headaches [thesis]�Melbourne, Australia: Royal Melbourne Institute of Technology;; 1999.
Hall T, Chan HT, Christensen L, Odenthal B, Wells C, Robinson K. Efficacy of a C1-C2 self-sustained natural apophyseal glide (SNAG) in the management of cervicogenic headache.�J Orthop Sports Phys Ther.�2007;37:100�107.�[PubMed]
Jensen OK, Nielsen FF, Vosmar L. An open study comparing manual therapy with the use of cold packs in the treatment of post-traumatic headache.�Cephalalgia.�1990;10:241�250. doi: 10.1046/j.1468-2982.1990.1005241.x.�[PubMed]�[Cross Ref]
National Heart LaBI. US Guidelines on the Management of Asthma.�Expert Panel Report 3.�2007;3
Scottish Intercollegiate Guidelines Network. British Guideline on the Management of Asthma.�The British Thoracic Society.�2009. pp. 1�132.
Ernst E. Spinal manipulation for asthma: A systematic review of randomised clinical trials.�Respir Med.�2009;103:1791�1795. doi: 10.1016/j.rmed.2009.06.017.�[PubMed]�[Cross Ref]
Hondras MA, Linde K, Jones AP. Manual therapy for asthma.�Cochrane Database Syst Rev.�2001. p. CD001002.�[PubMed]
Balon JW, Mior SA. Chiropractic care in asthma and allergy.�Ann Allergy Asthma Immunol.�2004;93:S55�S60. doi: 10.1016/S1081-1206(10)61487-1.�[PubMed]�[Cross Ref]
Hawk C, Khorsan R, Lisi AJ, Ferrance RJ, Evans MW. Chiropractic care for nonmusculoskeletal conditions: a systematic review with implications for whole systems research.�J Altern Complement Med.�2007;13:491�512. doi: 10.1089/acm.2007.7088.�[PubMed]�[Cross Ref]
Nielsen NH, Bronfort G, Bendix T, Madsen F, Weeke B. Chronic asthma and chiropractic spinal manipulation: a randomized clinical trial.�Clin Exp Allergy.�1995;25:80�88. doi: 10.1111/j.1365-2222.1995.tb01006.x.�[PubMed]�[Cross Ref]
Balon J, Aker PD, Crowther ER, Danielson C, Cox PG, O’Shaughnessy D. A comparison of active and simulated chiropractic manipulation as adjunctive treatment for childhood asthma.�N Engl J Med.�1998;339:1013�1020. doi: 10.1056/NEJM199810083391501.�[PubMed]�[Cross Ref]
Guiney PA, Chou R, Vianna A, Lovenheim J. Effects of osteopathic manipulative treatment on pediatric patients with asthma: a randomized controlled trial.�J Am Osteopath Assoc.�2005;105:7�12.[PubMed]
Field T, Henteleff T, Hernandez-Reif M, Martinez E, Mavunda K, Kuhn C. Children with asthma have improved pulmonary functions after massage therapy.�J Pediatr.�1998;132:854�858. doi: 10.1016/S0022-3476(98)70317-8.�[PubMed]�[Cross Ref]
Brygge T, Heinig JH, Collins P, Ronborg S, Gehrchen PM, Hilden J. Reflexology and bronchial asthma.�Respir Med.�2001;95:173�179. doi: 10.1053/rmed.2000.0975.�[PubMed]�[Cross Ref]
BTS Guidelines for the Management of Community Acquired Pneumonia in Adults.�Thorax.�2001;56(Suppl 4):IV1�64.�[PMC free article]�[PubMed]
Mandell LA, Wunderink RG, Anzueto A, Bartlett JG, Campbell GD, Dean NC. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults.�Clin Infect Dis.�2007;44(Suppl 2):S27�S72. doi: 10.1086/511159.�[PubMed]�[Cross Ref]
Noll DR, Shores JH, Gamber RG, Herron KM, Swift J Jr. Benefits of osteopathic manipulative treatment for hospitalized elderly patients with pneumonia.�J Am Osteopath Assoc.�2000;100:776�782.�[PubMed]
Bhattacharyya N, Baugh RF, Orvidas L, Barrs D, Bronston LJ, Cass S. Clinical practice guideline: benign paroxysmal positional vertigo.�Otolaryngol Head Neck Surg.�2008;139:S47�S81. doi: 10.1016/j.otohns.2008.08.022.�[PubMed]�[Cross Ref]
Reid SA, Rivett DA. Manual therapy treatment of cervicogenic dizziness: a systematic review.�Man Ther.�2005;10:4�13. doi: 10.1016/j.math.2004.03.006.�[PubMed]�[Cross Ref]
Karlberg M, Magnusson M, Malmstrom EM, Melander A, Moritz U. Postural and symptomatic improvement after physiotherapy in patients with dizziness of suspected cervical origin.�Arch Phys Med Rehabil.�1996;77:874�882. doi: 10.1016/S0003-9993(96)90273-7.�[PubMed]�[Cross Ref]
Reid SA, Rivett DA, Katekar MG, Callister R. Sustained natural apophyseal glides (SNAGs) are an effective treatment for cervicogenic dizziness.�Man Ther.�2008;13:357�366. doi: 10.1016/j.math.2007.03.006.�[PubMed]�[Cross Ref]
Hillier SL, Hollohan V. Vestibular rehabilitation for unilateral peripheral vestibular dysfunction.�Cochrane Database Syst Rev.�2007. p. CD005397.�[PubMed]
Wessel MA, Cobb JC, Jackson EB, Harris GS, Detwiler AC. Paroxysmal fussing in infancy, sometimes called “colic”.�Pediatrics.�1954;14:421�434.�[PubMed]
Husereau D, Clifford T, Aker P.�Spinal manipulation for infantile colic.�Vol. 42. Canadian Coordinating office for Health Technology Assessment. Ottawa; 2003.
Brand P, Engelbert R, Helders P. Systematic review of effects of manual therapy in infants with kinetic imbalance due to suboccipital strain (KISS) syndrome.�J Man & Manip Ther.�2005;13:209�214.
Ernst E. Chiropractic manipulation for non-spinal pain–a systematic review.�N Z Med J.�2003;116:U539.�[PubMed]
Gotlib A, Rupert R. Chiropractic manipulation in pediatric health conditions – an updated systematic review.�Chiropr Osteopat.�2008;16:11. doi: 10.1186/1746-1340-16-11.�[PMC free article]�[PubMed][Cross Ref]
Ernst E. Chiropractic spinal manipulation for infant colic: a systematic review of randomised clinical trials.�Int J Clin Pract.�2009;63:1351�1353. doi: 10.1111/j.1742-1241.2009.02133.x.�[PubMed][Cross Ref]
Koonin S, Karpelowsky AS, Yelverton CJ. A comparative study to determine the efficacy of chiropractic spinal manipulative therapy and allopathic medication inthe treatment of infantile colic.�WFC 7th Biennial Congress Proceedings; Orlando. May 1-3, 2003.�pp. 330�1.
Mercer C, Nook B. In:�World Federation of Chiropractic. 5th Biennial Congress, 17-22 May 1999.Haldman S, Murphy B, editor. The efficacy of chiropractic spinal adjustments as a treatment protocol in the management of infant colic; pp. 170�1.
Wiberg JM, Nordsteen J, Nilsson N. The short-term effect of spinal manipulation in the treatment of infantile colic: a randomized controlled clinical trial with a blinded observer.�J Manipulative Physiol Ther.�1999;22:517�522. doi: 10.1016/S0161-4754(99)70003-5.�[PubMed]�[Cross Ref]
Browning M. Comparison of the short-term effects of chiropractic spinal manipulation and occipito-sacral decompression in the treatment of infant colic: a single-blinded, randomised, comparison trial.�Clinical Chiropractic.�2009;11:122�129. doi: 10.1016/j.clch.2008.10.003.�[Cross Ref]
Olafsdottir E, Forshei S, Fluge G, Markestad T. Randomised controlled trial of infantile colic treated with chiropractic spinal manipulation.�Arch Dis Child.�2001;84:138�141. doi: 10.1136/adc.84.2.138.[PMC free article]�[PubMed]�[Cross Ref]
Hayden C, Mullinger B. A preliminary assessment of the impact of cranial osteopathy for the relief of infantile colic.�Complement Ther Clin Pract.�2006;12:83�90. doi: 10.1016/j.ctcp.2005.12.005.[PubMed]�[Cross Ref]
Huhtala V, Lehtonen L, Heinonen R, Korvenranta H. Infant massage compared with crib vibrator in the treatment of colicky infants.�Pediatrics.�2000;105:E84. doi: 10.1542/peds.105.6.e84.�[PubMed][Cross Ref]
Arikan D, Alp H, Gozum S, Orbak Z, Cifci EK. Effectiveness of massage, sucrose solution, herbal tea or hydrolysed formula in the treatment of infantile colic.�J Clin Nurs.�2008;17:1754�1761. doi: 10.1111/j.1365-2702.2008.02504.x.�[PubMed]�[Cross Ref]
Lucassen PL, Assendelft WJ, Gubbels JW, van Eijk JT, van Geldrop WJ, Neven AK. Effectiveness of treatments for infantile colic: systematic review.�BMJ.�1998;316:1563�1569.�[PMC free article][PubMed]
Garrison MM, Christakis DA. A systematic review of treatments for infant colic.�Pediatrics.�2000;106:184�190.�[PubMed]
World Health Organization. The ICD-10 classification of mental and behavioural disorders: Clinical descriptions and diagnostic guidelines. 1992.
Fritz G, Rockney R, Bernet W, Arnold V, Beitchman J, Benson RS. Practice parameter for the assessment and treatment of children and adolescents with enuresis.�J Am Acad Child Adolesc Psychiatry.�2004;43:1540�1550. doi: 10.1097/01.chi.0000142196.41215.cc.�[PubMed]�[Cross Ref]
Glazener CM, Evans JH, Cheuk DK. Complementary and miscellaneous interventions for nocturnal enuresis in children.�Cochrane Database Syst Rev.�2005. p. CD005230.�[PubMed]
Reed WR, Beavers S, Reddy SK, Kern G. Chiropractic management of primary nocturnal enuresis.�J Manipulative Physiol Ther.�1994;17:596�600.�[PubMed]
Leboeuf C, Brown P, Herman A, Leembruggen K, Walton D, Crisp TC. Chiropractic care of children with nocturnal enuresis: a prospective outcome study.�J Manipulative Physiol Ther.�1991;14:110�115.�[PubMed]
Pediatric Society of New Zealand. Best practice evidence based guideline: Nocturnal enuresis. 2005.
Scottish Intercollegiate Guidelines Network. Diagnosis and management of childhood otitis media in primary care. 2003.
Mills MV, Henley CE, Barnes LL, Carreiro JE, Degenhardt BF. The use of osteopathic manipulative treatment as adjuvant therapy in children with recurrent acute otitis media.�Arch Pediatr Adolesc Med.�2003;157:861�866. doi: 10.1001/archpedi.157.9.861.�[PubMed]�[Cross Ref]
Subcommittee on Management of Acute Otitis Media. Diagnosis and management of acute otitis media.�Pediatics.�2004;113:1451�1465. doi: 10.1542/peds.113.5.1451.�[PubMed]�[Cross Ref]
Wahl RA, Aldous MB, Worden KA, Grant KL. Echinacea purpurea and osteopathic manipulative treatment in children with recurrent otitis media: a randomized controlled trial.�BMC Complement Altern Med.�2008;8:56. doi: 10.1186/1472-6882-8-56.�[PMC free article]�[PubMed]�[Cross Ref]
Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL Jr. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report.�JAMA.�2003;289:2560�2572. doi: 10.1001/jama.289.19.2560.�[PubMed][Cross Ref]
National Institute for Health and Clinical Excellence. Hypertension: management of hypertension in adults in primary care.�Clinical Care Guideline.�2006;34
Goertz CH, Grimm RH, Svendsen K, Grandits G. Treatment of Hypertension with Alternative Therapies (THAT) Study: a randomized clinical trial.�J Hypertens.�2002;20:2063�2068. doi: 10.1097/00004872-200210000-00027.�[PubMed]�[Cross Ref]
Yates RG, Lamping DL, Abram NL, Wright C. Effects of chiropractic treatment on blood pressure and anxiety: a randomized, controlled trial.�J Manipulative Physiol Ther.�1988;11:484�488.[PubMed]
Bakris G, Dickholtz M Sr, Meyer PM, Kravitz G, Avery E, Miller M. Atlas vertebra realignment and achievement of arterial pressure goal in hypertensive patients: a pilot study.�J Hum Hypertens.�2007;21:347�352.�[PubMed]
Lefebvre G, Pinsonneault O, Antao V, Black A, Burnett M, Feldman K. Primary dysmenorrhea consensus guideline.�J Obstet Gynaecol Can.�2005;27:1117�1146.�[PubMed]
Proctor ML, Hing W, Johnson TC, Murphy PA. Spinal manipulation for primary and secondary dysmenorrhoea.�Cochrane Database Syst Rev.�2006;3:CD002119.�[PubMed]
Boesler D, Warner M, Alpers A, Finnerty EP, Kilmore MA. Efficacy of high-velocity low-amplitude manipulative technique in subjects with low-back pain during menstrual cramping.�J Am Osteopath Assoc.�1993;93:203�204.�[PubMed]
Snyder BJ, Sanders GE. Evaluation of the Toftness system of chiropractic adjusting for subjects with chronic back pain, chronic tension headaches, or primary dysmenorrhea.�Chiro Tech.�1996;8:3�9.
Kokjohn K, Schmid DM, Triano JJ, Brennan PC. The effect of spinal manipulation on pain and prostaglandin levels in women with primary dysmenorrhea.�J Manipulative Physiol Ther.�1992;15:279�285.�[PubMed]
Tomason PR, Fisher BL, Carpenter PA. Effectiveness of spinal manipulative therapy in treatment of primary dysmenorrhea: A pilot study.�J of Man and Phys Therapeutics.�1979;2:140�145.
Hondras MA, Long CR, Brennan PC. Spinal manipulative therapy versus a low force mimic maneuver for women with primary dysmenorrhea: a randomized, observer-blinded, clinical trial.�Pain.�1999;81:105�114. doi: 10.1016/S0304-3959(99)00004-4.�[PubMed]�[Cross Ref]
Royal College of Obstetricians and Gynaecologists. Management of premenstual syndrome.�Green-top Guideline.�2007;48
Halbreich U, Backstrom T, Eriksson E, O’brien S, Calil H, Ceskova E. Clinical diagnostic criteria for premenstrual syndrome and guidelines for their quantification for research studies.�Gynecol Endocrinol.�2007;23:123�130. doi: 10.1080/09513590601167969.�[PubMed]�[Cross Ref]
Stevinson C, Ernst E. Complementary/alternative therapies for premenstrual syndrome: a systematic review of randomized controlled trials.�Am J Obstet Gynecol.�2001;185:227�235. doi: 10.1067/mob.2001.113643.�[PubMed]�[Cross Ref]
Fugh-Berman A, Kronenberg F. Complementary and alternative medicine (CAM) in reproductive-age women: a review of randomized controlled trials.�Reprod Toxicol.�2003;17:137�152. doi: 10.1016/S0890-6238(02)00128-4.�[PubMed]�[Cross Ref]
Walsh MJ, Polus BI. A randomized, placebo-controlled clinical trial on the efficacy of chiropractic therapy on premenstrual syndrome.�J Manipulative Physiol Ther.�1999;22:582�585. doi: 10.1016/S0161-4754(99)70018-7.�[PubMed]�[Cross Ref]
Hernandez-Reif M, Martinez A, Field T, Quintero O, Hart S, Burman I. Premenstrual symptoms are relieved by massage therapy.�J Psychosom Obstet Gynaecol.�2000;21:9�15. doi: 10.3109/01674820009075603.�[PubMed]�[Cross Ref]
Oleson T, Flocco W. Randomized controlled study of premenstrual symptoms treated with ear, hand, and foot reflexology.�Obstet Gynecol.�1993;82:906�911.�[PubMed]
Reventlow SD, Hvas L, Malterud K. Making the invisible body visible. Bone scans, osteoporosis and women’s bodily experiences.�Soc Sci Med.�2006;62:2720�2731. doi: 10.1016/j.socscimed.2005.11.009.�[PubMed]�[Cross Ref]
Barnett AG, Pols JC van der, Dobson AJ. Regression to the mean: what it is and how to deal with it.�Int J Epidemiol.�2005;34:215�220. doi: 10.1093/ije/dyh299.�[PubMed]�[Cross Ref]
Kaptchuk TJ. The placebo effect in alternative medicine: can the performance of a healing ritual have clinical significance?�Ann Intern Med.�2002;136:817�825.�[PubMed]
Sox HC Jr, Margulies I, Sox CH. Psychologically mediated effects of diagnostic tests.�Ann Intern Med.�1981;95:680�685.�[PubMed]
Kaptchuk TJ. Powerful placebo: the dark side of the randomised controlled trial.�The Lancet.�1998;351:1722�1725. doi: 10.1016/S0140-6736(97)10111-8.�[PubMed]�[Cross Ref]
Kelley JM, Lembo AJ, Ablon JS, Villanueva JJ, Conboy LA, Levy R. Patient and Practitioner Influences on the Placebo Effect in Irritable Bowel Syndrome.�Psychosom Med.�2009;71:789�797. doi: 10.1097/PSY.0b013e3181acee12.�[PMC free article]�[PubMed]�[Cross Ref]
Kaptchuk TJ, Stason WB, Davis RB, Legedza AR, Schnyer RN, Kerr CE. Sham device v inert pill: randomised controlled trial of two placebo treatments.�BMJ.�2006;332:391�397. doi: 10.1136/bmj.38726.603310.55.�[PMC free article]�[PubMed]�[Cross Ref]
Oths K. Communication in a chiropractic clinic: how a D.C. treats his patients.�Cult Med Psychiatry.�1994;18:83�113. doi: 10.1007/BF01384878.�[PubMed]�[Cross Ref]
Adler HM, Hammett VB. The doctor-patient relationship revisited. An analysis of the placebo effect.�Ann Intern Med.�1973;78:595�598.�[PubMed]
Novack DH. Therapeutic aspects of the clinical encounter.�J Gen Intern Med.�1987;2:346�355. doi: 10.1007/BF02596174.�[PubMed]�[Cross Ref]
De Vries R, Lemmens T. The social and cultural shaping of medical evidence: case studies from pharmaceutical research and obstetric science.�Soc Sci Med.�2006;62:2694�2706. doi: 10.1016/j.socscimed.2005.11.026.�[PubMed]�[Cross Ref]
Verhoef MJ, Lewith G, Ritenbaugh C, Boon H, Fleishman S, Leis A. Complementary and alternative medicine whole systems research: beyond identification of inadequacies of the RCT.�Complement Ther Med.�2005;13:206�212. doi: 10.1016/j.ctim.2005.05.001.�[PubMed]�[Cross Ref]
Antman K, Lagakos S, Drazen J. Designing and funding clinical trials of novel therapies.�N Engl J Med.�2001;344:762�763. doi: 10.1056/NEJM200103083441010.�[PubMed]�[Cross Ref]
Hoffer LJ. Proof versus plausibility: rules of engagement for the struggle to evaluate alternative cancer therapies.�CMAJ.�2001;164:351�353.�[PMC free article]�[PubMed]
Khalsa PS, Eberhart A, Cotler A, Nahin R. The 2005 conference on the biology of manual therapies.�J Manipulative Physiol Ther.�2006;29:341�346. doi: 10.1016/j.jmpt.2006.04.002.�[PubMed][Cross Ref]
Rubinstein SM. Adverse events following chiropractic care for subjects with neck or low-back pain: do the benefits outweigh the risks?�J Manipulative Physiol Ther.�2008;31:461�464. doi: 10.1016/j.jmpt.2008.06.001.�[PubMed]�[Cross Ref]
Ernst E. Adverse effects of spinal manipulation: a systematic review.�J R Soc Med.�2007;100:330�338. doi: 10.1258/jrsm.100.7.330.�[PMC free article]�[PubMed]�[Cross Ref]
Rubinstein SM, Peerdeman SM, van Tulder MW, Riphagen I, Haldeman S. A systematic review of the risk factors for cervical artery dissection.�Stroke.�2005;36:1575�1580. doi: 10.1161/01.STR.0000169919.73219.30.�[PubMed]�[Cross Ref]
Michaeli A. A reported occurrence and nature of complications following manipulative physiotherapy in South Afrika.�Aust Physiother.�1993;39:309�315.�[PubMed]
Haldeman S, Carey P, Townsend M, Papadopoulos C. Arterial dissections following cervical manipulation: the chiropractic experience.�CMAJ.�2001;165:905�906.�[PMC free article]�[PubMed]
Cassidy JD, Boyle E, Cote P, He Y, Hogg-Johnson S, Silver F. Risk of vertebrobasilar stroke and chiropractic care: results of a population-based case-control and case-crossover study.�Spine.�2008;33:S176�S183. doi: 10.1097/BRS.0b013e3181644600.�[PubMed]�[Cross Ref]
Hurwitz EL, Morgenstern H, Vassilaki M, Chiang LM. Adverse reactions to chiropractic treatment and their effects on satisfaction and clinical outcomes among patients enrolled in the UCLA Neck Pain Study.�J Manipulative Physiol Ther.�2004;27:16�25. doi: 10.1016/j.jmpt.2003.11.002.[PubMed]�[Cross Ref]
Hurwitz EL, Morgenstern H, Vassilaki M, Chiang LM. Frequency and clinical predictors of adverse reactions to chiropractic care in the UCLA neck pain study.�Spine.�2005;30:1477�1484. doi: 10.1097/01.brs.0000167821.39373.c1.�[PubMed]�[Cross Ref]
Assendelft WJ, Bouter LM, Knipschild PG. Complications of spinal manipulation: a comprehensive review of the literature.�J Fam Pract.�1996;42:475�480.�[PubMed]
Institute for Clinical Systems Improvement.�ICSI Health Care Guidelines: Assessment and management of chronic pain.�Institute for Clinical Systems Improvement; 2005. pp. 1�77.
Haldeman S, Rubinstein SM. Cauda equina syndrome in patients undergoing manipulation of the lumbar spine.�Spine.�1992;17:1469�1473. doi: 10.1097/00007632-199212000-00005.�[PubMed][Cross Ref]
Vohra S, Johnston BC, Cramer K, Humphreys K. Adverse events associated with pediatric spinal manipulation: a systematic review.�Pediatrics.�2007;119:e275�e283. doi: 10.1542/peds.2006-1392.[PubMed]�[Cross Ref]
Stevinson C, Honan W, Cooke B, Ernst E. Neurological complications of cervical spine manipulation.�J R Soc Med.�2001;94:107�110.�[PMC free article]�[PubMed]
Adams D, Amernic H, Humphreys K.�A survey of complementary and alternative medicine practitioners’ knowledge, attitudes, and behavior regarding children in their practice.�San Francisco, CA; p. 206.
Moher D, Pham B, Lawson ML, Klassen TP. The inclusion of reports of randomised trials published in languages other than English in systematic reviews.�Health Technol Assess.�2003;7:1�90.[PubMed]
Juni P, Holenstein F, Sterne J, Bartlett C, Egger M. Direction and impact of language bias in meta-analyses of controlled trials: empirical study.�Int J Epidemiol.�2002;31:115�123. doi: 10.1093/ije/31.1.115.�[PubMed]�[Cross Ref]
Galandi D, Schwarzer G, Antes G. The demise of the randomised controlled trial: bibliometric study of the German-language health care literature, 1948 to 2004.�BMC Med Res Methodol.�2006;6:30. doi: 10.1186/1471-2288-6-30.�[PMC free article]�[PubMed]�[Cross Ref]
Moher D, Tetzlaff J, Tricco AC, Sampson M, Altman DG. Epidemiology and reporting characteristics of systematic reviews.�PLoS Med.�2007;4:e78. doi: 10.1371/journal.pmed.0040078.[PMC free article]�[PubMed]�[Cross Ref]
Consider the following, sciatica is a medical term used to describe a collective group of symptoms resulting from the irritation or compression of the sciatic nerve, generally due to an injury or aggravated condition. Sciatica is commonly characterized by radiating pain along the sciatic nerve, which runs down one or both legs from the lower back. The following case vignette discusses Mr. Winston’s medical condition, a 50-year-old bus driver who reported experiencing chronic, lower back and leg pain associated with sciatica during a 4-week time period. Ramya Ramaswami, M.B., B.S., M.P.H., Zoher Ghogawala, M.D., and James N. Weinstein, D.O., provide a comprehensive analysis of the various treatment options available to treat sciatica, including undergoing lumbar disk surgery and receiving nonsurgical therapy.
On a personal note, as a practicing doctor of chiropractic, choosing the correct treatment care for any type of injury or condition can be a personal and difficult decision. If the circumstances are favorable, the patient may determine what is the best form of treatment for their type of medical issue. While nonsurgical therapies, such as chiropractic care, can often be utilized to improve symptoms of sciatica, more severe cases of sciatica may require surgical interventions to treat the source of the issue. In most cases, nonsurgical therapies should be considered first, before turning to surgical therapies for sciatica.
Case Vignette
A Man with Sciatica Who is Considering Lumbar Disk Surgery
Ramya Ramaswami, M.B., B.S., M.P.H.
Mr. Winston, a 50-year-old bus driver, presented to your office with a 4-week history of pain in his left leg and lower back. He described a combination of severe sharp and dull pain that originated in his left buttock and radiated to the dorsolateral aspect of his left thigh, as well as vague aching over the lower lumbar spine. On examination, passive raising of his left leg off the table to 45 degrees caused severe pain that simulated his main symptom, and the pain was so severe that you could not lift his leg further. There was no leg or foot weakness. His body-mass index (the weight in kilograms divided by the square of the height in meters) was 35, and he had mild chronic obstructive pulmonary disease as a result of smoking one pack of cigarettes every day for 22 years. Mr. Winston had taken a leave of absence from his work because of his symptoms. You prescribed 150 mg of pregabalin per day, which was gradually increased to 600 mg daily because the symptoms had not abated.
Now, 10 weeks after the initial onset of his symptoms, he returns for an evaluation. The medication has provided minimal alleviation of his sciatic pain. He has to return to work and is concerned about his ability to complete his duties at his job. He undergoes magnetic resonance imaging, which shows a herniated disk on the left side at the L4�L5 root. You discuss options for the next steps in managing his sciatica. He is uncertain about invasive procedures such as lumbar disk surgery but feels limited by his symptoms of pain.
Treatment Options
Which of the following would you recommend for Mr. Winston?
Undergo lumbar disk surgery.
Receive nonsurgical therapy.
To aid in your decision making, each of these approaches is defended in a short essay by an expert in the field. Given your knowledge of the patient and the points made by the experts, which option would you choose?
Option 1: Undergo Lumbar Disk Surgery Option 2: Receive Nonsurgical Therapy
1. Undergo Lumbar Disk Surgery
Zoher Ghogawala, M.D.
Mr. Winston�s case represents a common scenario in the management of symptomatic lumbar disk herniation. In this particular case, the patient�s symptoms and the physical examination are consistent with nerve-root compression and inflammation directly from an L4�L5 herniated disk on his left side. The patient does not have weakness but has ongoing pain and has been unable to work for the past 10 weeks despite receiving pregabalin. Two questions emerge: first, does lumbar disk surgery (microdiskectomy) provide outcomes that are superior to those with continued nonoperative therapy in patients with more than 6 weeks of symptoms; and second, does lumbar microdiskectomy improve the likelihood of return to work in patients with these symptoms?
The highest quality data on the topic come from the Spine Patient Outcomes Research Trial (SPORT). The results of the randomized, controlled trial are difficult to interpret because adherence to the assigned treatment strategy was suboptimal. Only half the patients who were randomly assigned to the surgery group actually underwent surgery within 3 months after enrollment, and 30% of the patients assigned to nonoperative treatment chose to cross over to the surgical group. In this study, the patients who underwent surgery had greater improvements in validated patient-reported outcomes. The treatment effect of microdiskectomy was superior to that of nonoperative treatment at 3 months, 1 year, and 2 years. Moreover, in an as-treated analysis, the outcomes among patients who underwent surgery were superior to those among patients who received nonoperative therapy. Overall, the results of SPORT support the use of microdiskectomy in this case.
Results of clinical trials are based on a comparison of treatment options in study populations and may or may not apply to individual patients. SPORT did not specify what type of nonoperative therapy was to be used. Physical therapy was used in 73% of the patients, epidural injections in 50%, and medical therapies (e.g., nonsteroidal antiinflammatory drugs) in more than 50%. In the case of Mr. Winston, pregabalin has been tried, but physical therapy and epidural glucocorticoid injections have not been attempted. Despite widespread use of physical therapy for the treatment of lumbar disk herniation, the evidence supporting its effectiveness is inconclusive, according to published guidelines of the North American Spine Society. On the other hand, there is evidence that transforaminal epidural glucocorticoid injection provides short-term relief (30 days) in patients with nerve-root symptoms directly related to a herniated disk. Overall, there is evidence, from SPORT and from a randomized trial from the Netherlands published in the Journal, that early surgery between 6 and 12 weeks after the onset of symptoms provides greater alleviation of leg pain and better overall pain relief than prolonged conservative therapy.
The ability to return to work has not been formally studied in comparisons of operative with nonoperative treatments for lumbar disk herniation. Registry data from the NeuroPoint-SD study showed that more than 80% of the patients who were working before disk herniation returned to work after surgery. The ability to return to work may be dependent on the type of vocation, since patients who are manual laborers may need more time to recover to reduce the risk of reherniation.
It is well recognized that many patients who have a symptomatic lumbar disk herniation will have improvement spontaneously over several months. Surgery can alleviate symptoms more quickly by immediately removing the offending disk herniation from the affected nerve root. The risk�benefit equation will vary among individual patients. In the case of Mr. Winston, obesity and mild pulmonary disease might increase the risk of complications from surgery, although in SPORT, 95% of surgical patients did not have any operative or postoperative complication. For Mr. Winston, a patient with pain that has persisted for more than 6 weeks, microdiskectomy is a rational option that is supported by high-quality evidence.
2. Receive Nonsurgical Therapy
James N. Weinstein, D.O.
This case involves a common presentation of low back pain radiating to the buttock and posterolateral thigh that might represent either referred mechanical pain or radiculopathy. Classic radiculopathy resulting from compression of a lower lumbar nerve root (L4, L5, or S1) results in pain that radiates distal to the knee and is often accompanied by weakness or numbness in the respective myotome or dermatome. In this case, the pain is proximal to the knee and is not associated with weakness or numbness. In SPORT, surgery resulted in faster recovery and a greater degree of improvement than nonoperative treatment in patients with pain that radiated distal to the knee and was accompanied by neurologic signs or symptoms. However, since Mr. Winston would not have met the inclusion criteria for SPORT, the results of diskectomy in this case would be somewhat unpredictable. He does not have radiculopathy that radiates below the knee, and he does not have weakness or numbness; nonoperative treatment should be exhausted before any consideration of a surgical procedure that in most cases has not been shown to be effective in patients with this type of presentation. In this issue of the Journal, Mathieson and colleagues report the results of a randomized, controlled trial that showed that pregabalin did not significantly alleviate pain related to sciatica. Mr. Winston has been treated only with pregabalin; therefore, other conservative options should be explored.
Saal and Saal reported that more than 80% of patients with radiculopathy associated with a lumbar disk herniation had improvement in a matter of months with exercise-based physical therapy. In the nonoperative SPORT cohort, patients had significant improvement from baseline, and approximately 60% of those with classic radiculopathy who initially received nonoperative treatment avoided surgery. Mr. Winston has had minimal treatment and has had symptoms for only 10 weeks. He should undergo a course of exercise-based physical therapy and a trial of a nonsteroidal antiinflammatory medication and may consider a lumbar epidural glucocorticoid injection. Although there is little evidence of the effectiveness of these nonoperative options alone, the combination of these treatments and the benign natural history of the patient�s condition could result in alleviation or resolution of symptoms. If these interventions � and time � do not resolve his symptoms, surgery could be considered as a final option, but it may not have long-term effectiveness and could in and of itself cause the possibility of more harm than good. Mr. Winston has risk factors, such as obesity and a history of smoking, that have been shown to contribute to poor surgical outcomes of certain spinal procedures.
Mr. Winston has symptoms of back pain that interfere with his quality of life. He would need to understand, through shared decision making, that a nonsurgical approach is likely to be more effective than surgery over time.
Information referenced from the National Center for Biotechnology Information (NCBI) and the New England Journal of Medicine (NEJM). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Cited by Dr. Alex Jimenez
Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.
1. Weinstein JN, Tosteson TD, Lurie JD, et al. Surgical vs nonoperative treatment for lumbar disk herniation: the Spine Patient Outcomes Research Trial (SPORT): a randomized trial. JAMA2006;296:2441–2450
2. Weinstein JN, Lurie JD, Tosteson TD, et al. Surgical vs nonoperative treatment for lumbar disk herniation: the Spine Patient Outcomes Research Trial (SPORT) observational cohort. JAMA2006;296:2451–2459
3. Kreiner DS, Hwang SW, Easa JE, et al. An evidence-based clinical guideline for the diagnosis and treatment of lumbar disc herniation with radiculopathy. Spine J2014;14:180–191
4. Ghahreman A, Ferch R, Bogduk N. The efficacy of transforaminal injection of steroids for the treatment of lumbar radicular pain. Pain Med2010;11:1149–1168
6. Ghogawala Z, Shaffrey CI, Asher AL, et al. The efficacy of lumbar discectomy and single-level fusion for spondylolisthesis: results from the NeuroPoint-SD registry: clinical article. J Neurosurg Spine2013;19:555–563
8. Lurie JD, Tosteson TD, Tosteson AN, et al. Surgical versus nonoperative treatment for lumbar disc herniation: eight-year results for the spine patient outcomes research trial. Spine (Phila Pa 1976)2014;39:3–16
11. Pinto RZ, Maher CG, Ferreira ML, et al. Drugs for relief of pain in patients with sciatica: systematic review and meta-analysis. BMJ2012;344:e497–e497
12. Pearson A, Lurie J, Tosteson T, et al. Who should have surgery for an intervertebral disc herniation? Comparative effectiveness evidence from the Spine Patient Outcomes Research Trial. Spine2012;37:140–149
These assessment and treatment recommendations represent a synthesis of information derived from personal clinical experience and from the numerous sources which are cited, or are based on the work of researchers, clinicians and therapists who are named (Basmajian 1974, Cailliet 1962, Dvorak & Dvorak 1984, Fryette 1954, Greenman 1989, 1996, Janda 1983, Lewit 1992, 1999, Mennell 1964, Rolf 1977, Williams 1965).
Clinical Application of Neuromuscular Techniques: Piriformis
Assessment of Shortened Piriformis
Test (a) Stretch test. When short, piriformis will cause the affected side leg of the supine patient to appear to be short and externally rotated. With the patient supine, the tested leg is placed into flexion at the hip and knee so that the foot rests on the table lateral to the contralateral knee (the tested leg is crossed over the straight non-tested leg, in other words as shown in Fig. 4.17). The angle of hip flexion should not exceed 60� (see notes on piriformis in Box 4.6).
Figure 4.17 MET treatment of piriformis muscle with patient supine. The pelvis must be maintained in a stable position as the knee (right in this example) is adducted to stretch piriformis following an isometric contraction.
The non-tested side ASIS is stabilised to prevent pelvic motion during the test and the knee of the tested side is pushed into adduction to place a stretch on piriformis. If there is a short piriformis the degree of adduction will be limited and the patient will report discomfort behind the trochanter.
Test (b) Palpation test (Fig. 4.18) The patient is side-lying, tested side uppermost. The practitioner stands at the level of the pelvis in front of and facing the patient, and, in order to contact the insertion of piriformis, draws imaginary lines between:
ASIS and ischial tuberosity, and
PSIS and the most prominent point of trochanter.
Where these reference lines cross, just posterior to the trochanter, is the insertion of the muscle, and pressure here will produce marked discomfort if the structure is short or irritated.
Figure 4.18 Using bony landmarks as coordinates the commonest tender areas are located in piriformis, in the belly and at the attachment of the muscle.
If the most common trigger point site in the belly of the muscle is sought, then the line from the ASIS should be taken to the tip of the coccyx rather than to the ischial tuberosity. Pressure where this line crosses the other will access the mid-point of the belly of piriformis where triggers are common. Light compression here which produces a painful response is indicative of a stressed muscle and possibly an active myofascial trigger point.
Piriformis Strength Test
The patient lies prone, both knees flexed to 90�, with practitioner at foot of table grasping lower legs at the limit of their separation (which internally rotates the hip and therefore allows comparison of range of movement permitted by shortened external rotators such as the piriformis).
The patient attempts to bring the ankles together as the practitioner assesses the relative strength of the two legs. Mitchell et al (1979) suggest that if there is relative shortness (as evidenced by the lower leg not being able to travel as far from the mid-line as its pair in this position), and if that same side also tests strong, then MET is called for. If there is shortness but also weakness then the reasons for the weakness need to be dealt with prior to stretching using MET.
Box 4.6 Notes on Piriformis
Piriformis paradox. The performance of external rotation of the hip by piriformis occurs when the angle of hip flexion is 60� or less. Once the angle of hip flexion is greater than 60� piriformis function changes, so that it becomes an internal rotator of the hip (Gluck & Liebenson 1997, Lehmkuhl & Smith 1983). The implications of this are illustrated in Figures 4.17 and 4.19.
This postural muscle, like all others which have a predominence of type l fibres, will shorten if stressed. In the case of piriformis, the effect of shortening is to increase its diameter and because of its location this allows for direct pressure to be exerted on the sciatic nerve, which passes under it in 80% of people. In the other 20% the nerve passes through the muscle so that contraction will produce veritable strangulation of the sciatic nerve.
In addition, the pudendal nerve and the blood vessels of the internal iliac artery, as well as common perineal nerves, posterior femoral cutaneous nerve and nerves of the hip rotators, can all be affected.
If there is sciatic pain associated with piriformis shortness, then on straight leg raising, which reproduces the pain, external rotation of the hip should relieve it, since this slackens piriformis. (This clue may, however, only apply to any degree if the individual is one of those in whom the nerve actually passes through the muscle.)
The effects can be circulatory, neurological and functional, inducing pain and paraesthesia of the affected limb as well as alterations to pelvic and lumbar function. Diagnosis usually hinges on the absence of spinal causative factors and the distributions of symptoms from the sacrum to the hip joint, over the gluteal region and down to the popliteal space. Palpation of the affected piriformis tendon, near the head of the trochanter, will elicit pain and the affected leg will probably be externally rotated.
The piriformis muscle syndrome is frequently characterised by such bizarre symptoms that they may seem unrelated. One characteristic complaint is a persistent, severe, radiating low back pain extending from the sacrum to the hip joint, over the gluteal region and the posterior portion of the upper leg, to the popliteal space. In the most severe cases the patient will be unable to lie or stand comfortably, and changes in position will not relieve the pain. Intense pain will occur when the patient sits or squats since this type of movement requires external rotation of the upper leg and flexion at the knee.
Compression of the pudendal nerve and blood vessels which pass through the greater sciatic foramen and re-enter the pelvis via the lesser sciatic foramen is possible because of piriformis contracture. Any compression would result in impaired circulation to the genitalia in both sexes. Since external rotation of the hips is required for coitus by women, pain noted during this act could relate to impaired circulation induced by piriformis dysfunction. This could also be a basis for impotency in men. (See also Box 4.7.)
Piriformis involvement often relates to a pattern of pain which includes: pain near the trochanter; pain in the inguinal area; local tenderness over the insertion behind trochanter; SI joint pain on the opposite side; externally rotated foot on the same side; pain unrelieved by most positions with standing and walking being the easiest; limitation of internal rotation of the leg which produces pain near the hip; and a short leg on the affected side.
The pain itself will be persistent and radiating, covering anywhere from the sacrum to the buttock, hip and leg including inguinal and perineal areas.
Bourdillon (1982) suggests that piriformis syndrome and SI joint dysfunction are intimately connected and that recurrent SI problems will not stabilise until hypertonic piriformis is corrected.
Janda (1996) points to the vast amount of pelvic organ dysfunction to which piriformis can contribute due to its relationship with circulation to the area.
Mitchell et al (1979) suggest that (as in psoas example above) piriformis shortness should only be treated if it is tested to be short and stronger than its pair. If it is short and weak (see p. 110 for strength test), then whatever is hypertonic and influencing it should be released and stretched first (Mitchell et al 1979). When it tests strong and short, piriformis should receive MET treatment.
Since piriformis is an external rotator of the hip it can be inhibited (made to test weak) if an internal rotator such as TFL is hypertonic or if its pair is hypertonic, since one piriformis will inhibit the other.
Box 4.7 Notes on Working and Resting Muscles
Richard (1978) reminds us that a working muscle will mobilise up to 10 times the quantity of blood mobilised by a resting muscle. He points out the link between pelvic circulation and lumbar, ischiatic and gluteal arteries and the chance this allows to engineer the involvement of 2400 square metres of capillaries by using repetitive pumping of these muscles (including piriformis).
The therapeutic use of this knowledge involves the patient being asked to repetitively contract both piriformis muscles against resistance. The patient is supine, knees bent, feet on the table; the practitioner resists their effort to abduct their flexed knees, using pulsed muscle energy approach (Ruddy�s method) in which two isometrically resisted pulsation/contractions per second are introduced for as long as possible (a minute seems a long time doing this).
Figure 4.19 MET treatment of piriformis with hip fully flexed and externally rotated (see Box 4.6, first bullet point).
Figure 4.20 A combined ischaemic compression (elbow pressure) and MET side-lying treatment of piriformis. The pressure is alternated with isometric contractions/stretching of the muscle until no further gain is achieved.
MET Treatment of Piriformis
Piriformis method (a) Side-lying The patient is side-lying, close to the edge of the table, affected side uppermost, both legs flexed at hip and knee. The practitioner stands facing the patient at hip level.
The practitioner places his cephalad elbow tip gently over the point behind trochanter, where piriformis inserts. The patient should be close enough to the edge of the table for the practitioner to stabilise the pelvis against his trunk (Fig. 4.20). At the same time, the practitioner�s caudad hand grasps the ankle and uses this to bring the upper leg/hip into internal rotation, taking out all the slack in piriformis.
A degree of inhibitory pressure (sufficient to cause discomfort but not pain) is applied via the elbow for 5�7 seconds while the muscle is kept at a reasonable but not excessive degree of stretch. The practitioner maintains contact on the point, but eases pressure, and asks the patient to introduce an isometric contraction (25% of strength for 5�7 seconds) to piriformis by bringing the lower leg towards the table against resistance. (The same acute and chronic rules as discussed previously are employed, together with cooperative breathing if appropriate, see Box 4.2.)
After the contraction ceases and the patient relaxes, the lower limb is taken to its new resistance barrier and elbow pressure is reapplied. This process is repeated until no further gain is achieved.
Piriformis method (b)1 This method is a variation on the method advocated by TePoorten (1960) which calls for longer and heavier compression, and no intermediate isometric contractions.
In the first stage of TePoorten�s method the patient lies on the non-affected side with knees flexed and hip joints flexed to 90�.The practitioner places his elbow on the piriformis musculotendinous junction and a steady pressure of 20�30 lb (9�13 kg) is applied. With his other hand he abducts the foot so that it will force an internal rotation of the upper leg.
The leg is held in this rotated position for periods of up to 2 minutes. This procedure is repeated two or three times. The patient is then placed in the supine position and the affected leg is tested for freedom of both external and internal rotation.
Piriformis method (b)2 The second stage of TePoorten�s treatment is performed with the patient supine with both legs extended. The foot of the affected leg is grasped and the leg is flexed at both the knee and the hip. As knee and hip flexion is performed the practitioner turns the foot inward, so inducing an external rotation of the upper leg. The practitioner then extends the knee, and simultaneously turns the foot outward, resulting in an internal rotation of the upper leg.
During these procedures the patient is instructed to partially resist the movements introduced by the practitioner (i.e. the procedure becomes an isokinetic activity). This treatment method, repeated two or three times, serves to relieve the contracture of the muscles of external and internal hip rotation.
Piriformis method (c) A series of MET isometric contractions and stretches can be applied with the patient prone and the affected side knee flexed. The hip is rotated internally by the practitioner using the foot as a lever to ease it laterally, so putting piriformis at stretch. Acute and chronic guidelines described earlier are used to determine the appropriate starting point for the contraction (at the barrier for acute and short of it for chronic).
The patient attempts to lightly bring the heel back towards the midline against resistance (avoiding strong contractions to avoid knee strain in this position) and this is held for 7�10 seconds. After release of the contraction the hip is rotated further to move piriformis to or through the barrier, as appropriate. Application of inhibitory pressure to the attachment or belly of piriformis is possible via thumb, if deemed necessary.
Piriformis method (d) A general approach which balances muscles of the region, as well as the pelvic diaphragm, is achieved by having the patient squat while the practitioner stands and stabilises both shoulders, preventing the patient from rising as this is attempted, while the breath is held. After 7�10 seconds the effort is released; a deeper squat is performed, and the procedure is repeated several times.
Piriformis method (e) This method is based on the test position (see Fig. 4.17) and is described by Lewit (1992). With the patient supine, the treated leg is placed into flexion at the hip and knee, so that the foot rests on the table lateral to the contralateral knee (the leg on the side to be treated is crossed over the other, straight, leg). The angle of hip flexion should not exceed 60� (see notes on piriformis, Box 4.6, for explanation).
The practitioner places one hand on the contralateral ASIS to prevent pelvic motion, while the other hand is placed against the lateral flexed knee as this is pushed into resisted abduction to contract piriformis for 7�10 seconds. Following the contraction the practitioner eases the treated side leg into adduction until a sense of resistance is noted; this is held for 10�30 seconds.
Piriformis method (f) Since contraction of one piriformis inhibits its pair, it is possible to self-treat an affected short piriformis by having the patient lie up against a wall with the non-affected side touching it, both knees flexed (modified from Retzlaff 1974). The patient monitors the affected side by palpating behind the trochanter, ensuring that no contraction takes place on that side.
After a contraction lasting 10 seconds or so of the non-affected side (the patient presses the knee against the wall), the patient moves away from the wall and the position described for piriformis test (see Fig. 4.17) above is adopted, and the patient pushes the affected side knee into adduction, stretching piriformis on that side. This is repeated several times.
Dr. Alex Jimenez offers an additional assessment and treatment of the hip flexors as a part of a referenced clinical application of neuromuscular techniques by Leon Chaitow and Judith Walker DeLany. The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
By Dr. Alex Jimenez
Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine