Can postural assessments help identify problems with how a person stands or sits, which can lead to various musculoskeletal issues?
Postural Assessment
Proper posture is an exercise in which the muscles support the skeleton in a comfortable, stable, and efficient alignment. Healthy posture is present when the body is still and when moving. However, numerous factors can affect and hinder posture. These include daily wear and tear, injury, illness, or a condition. A posture assessment is a process that identifies posture issues and their root causes, often using visual and palpation techniques, and can help determine appropriate treatment or exercises. (Science Direct, 2007)
Visual Assessment
Observing the body’s alignment and symmetry from different angles (anterior, posterior, and lateral views).
Consider their daily activities, work environment, and any previous injuries. (Du, S. H. et al., 2023)
Wall Test
The patient stands against a wall with their feet shoulder-width apart and heels about 6 inches from the baseboard.
If they have good posture, their ears will be vertically aligned with their shoulders, and their head will be no more than three finger widths from the wall. (Physiopedia, 2025)
Professionals Who Can Perform a Posture Assessment
Physiotherapists
Professionals trained in assessing and treating musculoskeletal problems.
Chiropractors
Professionals who focus on the spine and nervous system.
Fitness Professionals
Personal trainers or other fitness professionals can use posture assessments to help clients improve their posture and movement.
Ergonomists
Professionals who specialize in designing workspaces and environments to promote good posture and reduce strain.
Injury Medical Chiropractic & Functional Medicine Clinic
Talk to a healthcare provider to learn what interventions would help the most. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, and prevent injury. Regarding musculoskeletal pain, specialists like chiropractors, acupuncturists, and massage therapists can help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal issues.
Singla, D., & Veqar, Z. (2014). Methods of postural assessment used for sports persons. Journal of clinical and diagnostic research: JCDR, 8(4), LE01–LE4. https://doi.org/10.7860/JCDR/2014/6836.4266
Du, S. H., Zhang, Y. H., Yang, Q. H., Wang, Y. C., Fang, Y., & Wang, X. Q. (2023). Spinal posture assessment and low back pain. EFORT open reviews, 8(9), 708–718. https://doi.org/10.1530/EOR-23-0025
Learn about the clinical approach of identity formation and its role in facilitating personal insight and emotional well-being.
Introduction
Many individuals deal with musculoskeletal, autoimmune, gut, or body issues that can affect their daily routine and how they perceive themselves when getting checked out by their doctors. Many healthcare professionals can help assess individuals with these pain-like symptoms causing overlapping risk profiles by creating a safe and positive experience with a clinical approach. By creating a secure environment, many individuals can have good experiences when pain-like issues are affecting their bodies. By delving into today’s article, we are going to look into identity formation, the four identity statuses, and the various areas of identity development.
Theories & Types of Identity Formation
A lot of individuals have an identity, but have they always had one? Everyone’s identity is a conglomeration of the characteristics, values, and attributes they consider significant and use to define themselves. People’s identities are developed as they mature and gain knowledge about the world; they are not forced upon them. Adolescence is the first period when individuals notice a significant change toward identity creation and self-exploration.
A major concern in theories of teenage development is identity building. Identity formation, for instance, was emphasized as the main sign of effective development throughout adolescence in Erikson’s 1968 classic theory of developmental phases. Teenagers who struggle to define their identities may have role confusion, which suggests that they need to do more self-discovery and are unclear of their place in the world.
The Four Identity Statuses
Many healthcare providers will hear their patients describe identity formation during adolescence as it involves decision points and commitments regarding belief systems (e.g., religion, politics) and occupations. The four modes of reacting to late identity crises during the adolescent phase were described, measured, and validated so that individuals could figure out their identity status. (Marcia, 1966) The four described identity statuses are:
Foreclosure: An individual commits to an identity without exploring options.
Identity diffusion: When individuals neither explore nor commit to any identities.
Moratorium: A state in which individuals actively explore options but have not made commitments.
Identity achievement: When individuals have explored different options and made identity commitments.
For example, teens may commit to an identity without exploring if they are content with the values, culture, and religion they were raised in. Teens in foreclosure status may adopt large parts of their parents’ identities or the identity parents have put them on. However, when teens achieve identity, they can explore the world for themselves and decide how they identify due to those experiences. This causes them to relinquish their claims of infantile sources of gratification, thus renouncing lingering fantasies of competence. (Marcia, 1967) At the same time, many people have experienced things that led to a crisis. The thing is that a crisis doesn’t necessarily mean a negative event; it’s simply branching out from what’s comfortable to discover who they are.
Understanding The Effects Of Personal Injury- Video
Various Areas of Identity Development
As a stage in the adolescent life cycle, identity development happens to many people. For many, the search for identity begins in the teenage years. During these years, adolescents are more open to taking on different behaviors and appearances to discover who they are. In an attempt to find their own identity and discover who they are, adolescents tend to cycle through several identities to find one that suits them best. Multiple factors like family life, environment, and social status can make it difficult to develop and maintain an identity. Some studies suggest that this process might be more accurate to identity development rather than formation but confirm this is a typical change process in people’s thoughts about themselves.
Several different areas of identity development are described:
Religious identity: Teens’ religious views are similar to those of their families. Many may question specific customs, practices, or ideas in their parents’ faith, but a few may completely reject their families’ religion. This is due to the dynamic of the parent-adolescent relationship with religion, which exerts positive effects on adolescent adjustments. (Kim-Spoon et al., 2012)
Political identity: Adolescents’ political identity is influenced by their parents’ political beliefs. In the 21st century, a new trend shows decreased political affiliation among young adults. However, many adolescents tend to be more liberal than their elders on social issues. This is because many adolescents encounter events that trigger their civic interest and challenge their beliefs and moralities. (Stattin et al., 2017) Like in other aspects of identity formation, adolescent individuals are predicted by their parents’ involvement and current events when there is an interest in politics.
Vocational identity: Adolescents in earlier generations envisioned themselves working in a particular job and often worked as apprentices or part-time in such occupations. This is a rare case for many people in today’s world. Vocational identity is also related to ego identity by correlating with a successful transition from school to work, allowing individuals to be more confident in their decision-making ability, especially in environmental ambiguities. (Koo & Kim, 2016) Still, vocational identity takes a bit longer to develop since many workplaces require specific skills and knowledge that require additional education or are acquired on the job. Additionally, many job opportunities held by teens are not in occupations many will seek as adults.
Ethnic identity: Ethnic identity refers to how many individuals come to terms with who they are based on ethnicity or racial ancestry. According to the U.S. Census 2012, Americans under 18 are from historically marginalized ethnic groups. Many people who identify under BIPOC (Black, Indigenous, people of color) have discovered their ethnoracial identity as an important part of their identity formation as teens.
Gender identity: Gender identity involves an individual’s sense of gender and can be similar to or different from their biological sex regardless of age group. Gender identity greatly influences many adolescents during these years of self-discovery and can impact other areas of identity, like religion and politics.
Self-Concept
Self-concept and self-esteem are the two primary facets of identity formation. The capacity of an individual to have views and beliefs established with confidence, consistency, and stability throughout the course of their life is the central premise of self-concept. Cognitive growth in early adolescence leads to increased self-consciousness, awareness of others and their opinions, the ability to think about abstract future possibilities, and the ability to weigh many alternatives at once. As a consequence, many teenagers will stop using straightforward, global, and concrete self-descriptions when they are younger. As kids, they use physical characteristics like gender, hair color, or whether they’re quick to identify themselves.
Many teenagers have the ability to imagine many “possible selves” that they may become, and the decisions they make may have long-term effects or possibilities. Exploring these options may cause individuals to make sudden changes in how they show themselves when the teenager selects or rejects traits and actions. In addition, when combining their combinational operation with their degree of identification, both men and females exhibit strong positive connections. (Wagner, 1987) This in turn means directing the real self in the direction of the ideal self. The ideal self differs from person to person; many individuals aspire to be the person they want to be, while many others dread becoming the person they do not want to be. Many may find this unsettling, but it may also serve as motivation by demonstrating consistent conduct that aligns with the ideals and distinguishes the feared potential selves.
Our ideal and frightened selves may be simultaneously explored and discovered. In an effort to create their own identities, many young people may observe characteristics in their family members, friends, or other community members and begin to consider what they like and dislike at the same time. Teenagers learn to identify the factors that impact their conduct and how others see them, which leads to a further distinction in their self-concept known as differentiation. Differentiation seems to be completely established by mid-adolescence and peaks when students enter the seventh or ninth grade. Nowadays, identifying contradictory material in one’s self-concept is a frequent cause of anxiety. Nonetheless, by promoting their exploration and growth, it might help a lot of teenagers.
Self-Esteem
Self-esteem is the other component of identity building. By definition, one’s ideas and emotions about one’s identity and self-concept constitute one’s self-esteem. Many views contend that a strong desire to preserve, defend, and improve oneself is a component of self-esteem. Contrary to common opinion, little evidence supports these views, suggesting that teenage self-esteem has significantly declined. The two sexes have distinct levels of self-esteem; women have higher levels of self-esteem when they have supportive friendships. However, women have poor self-esteem when they are unable to meet someone with similar interests and hobbies or when they are unable to get the acceptance of their friends.
Males have varied levels of self-esteem. Males are more focused on defining authority and establishing and claiming their independence regarding self-esteem. This, in turn, enables men to effectively have high self-esteem via the influence of their peers and friends. However, a male’s poor self-esteem may be further exacerbated by a lack of romantic abilities or the inability to sustain another person’s attachment.
Conclusion
Numerous medical experts may use a clinical approach to identity development to provide a secure environment and a satisfying experience for people when evaluating the pain-like sensations impacting their bodies. Additionally, by offering a variety of alternatives in their individualized treatment plans to improve their health and well-being, a thorough awareness of the significance of identity development helps foster positive relationships with patients.
Injury Medical & Functional Medicine Clinic
We associate with certified medical providers who understand the importance of identity formation when assessing individuals dealing with various pain-like symptoms within their bodies. When asking important questions to our associated medical providers, we advise patients to implement small changes to their daily routine to reduce the pain-like symptoms associated with body pains. Dr. Alex Jimenez, D.C., utilizes this information as an academic service. Disclaimer.
References
Kim-Spoon, J., Longo, G. S., & McCullough, M. E. (2012). Parent-adolescent relationship quality as a moderator for the influences of parents’ religiousness on adolescents’ religiousness and adjustment. J Youth Adolesc, 41(12), 1576-1587. https://doi.org/10.1007/s10964-012-9796-1
Koo, H.-Y., & Kim, E.-J. (2016). Vocational Identity and Ego Identity Status in Korean Nursing Students. Asian Nursing Research, 10(1), 68-74. https://doi.org/10.1016/j.anr.2015.11.001
Marcia, J. E. (1966). Development and validation of ego-identity status. J Pers Soc Psychol, 3(5), 551-558. https://doi.org/10.1037/h0023281
Marcia, J. E. (1967). Ego identity status: relationship to change in self-esteem, “general maladjustment,” and authoritarianism. J Pers, 35(1), 118-133. https://doi.org/10.1111/j.1467-6494.1967.tb01419.x
Stattin, H., Hussein, O., Ozdemir, M., & Russo, S. (2017). Why do some adolescents encounter everyday events that increase their civic interest whereas others do not? Dev Psychol, 53(2), 306-318. https://doi.org/10.1037/dev0000192
The Cobb angle is a mathematical measurement tool for assessing the curvature of the spine. Along with physical exams and other tests, how is it used to evaluate scoliosis and kyphosis of the spine?
Cobb Angle
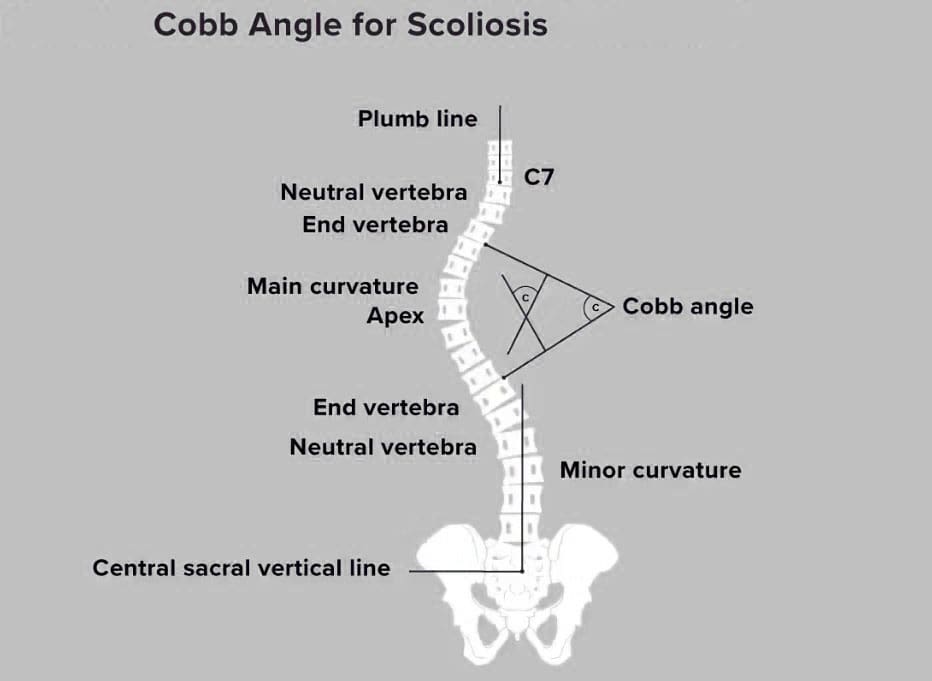
The Cobb angle is used to quantify the curvature of the spine, particularly in conditions like scoliosis. It measures the degree of side-to-side spinal curvature, a deformity called scoliosis. The angle’s size helps determine what kind of treatment is needed. Monitoring may be all that’s necessary for mild curvature. With severe scoliosis, treatment may require spinal fusion surgery. Named for orthopedic surgery pioneer John Robert Cobb, it describes the distance a scoliotic curve may deviate from being straight. (Botterbush K. S. et al., 2023) Generally, it takes at least 10 degrees of deviation from straight before scoliosis is confirmed.
X-Ray and Interpretation
An X-ray is taken to measure the Cobb angle. Side and back views are taken. The healthcare provider or examiner then views the X-rays and locates the most affected vertebra in the curve, the apical vertebra. In a scoliotic curve, the apical vertebra is the spinal bone with the greatest degree of rotation that takes the biggest curve away from the center of a normal spine column.
Visualizing the Angle
The apical vertebra is where two lines drawn from the X-rays meet. Two lines are drawn along the edge of the top and bottom bones of the curve. The lines extend out as follows:
On the top bone, the line starts on the high side, continues along the top edge, and then slopes down according to the angle of the vertebra. (Jin, C. et al., 2022)
On the bottom vertebra, the line starts on the low side, continues along the bottom edge, and slopes upward.
The Cobb angle is found by measuring the angle of the two intersecting lines where they meet.
Then, the top and bottom vertebrae of the side-to-side curve are identified to create a number for the Cobb angle. These bones have the most tilt but the least rotation and displacement and are located above and below the apical vertebra. Computer software is commonly used to calculate the Cobb angle. (Jin, C. et al., 2022) Treatment is based on the:
Angle size
Gender: Scoliosis is more common and likely to progress in females
Scoliosis is diagnosed when the Cobb angle reaches 10 degrees or more. However, this is not generally considered a significant curvature (American Association of Neurological Surgeons, 2024). In around 80% of cases, the scoliosis is considered idiopathic or without congenital or other underlying causes.
Less Than 25 Degrees Cobb Angle
If a scoliotic curve is less than 25 degrees, individuals may only need to visit their healthcare provider periodically so long as the scoliosis is monitored. These are mild cases, often without symptoms, but there is a chance that the curvature can progress. This usually means reassessing the Cobb angle every four to six months in a growing child or adolescent. (National Scoliosis Foundation, 2015) A 5-degree or more progression can change the diagnosis and treatment. (Jin, C. et al., 2022)
Between 25 and 40 Degrees Cobb Angle
A Cobb angle of 25 to 40 degrees usually requires wearing a back brace and intensive physical therapy. The goal of these treatments is to help halt the curve’s progression. Braces are generally worn 16 to 23 hours every day. (National Scoliosis Foundation, 2015) The healthcare provider will provide a referral for physical therapy. Many report excellent results with the Schroth or other scoliosis-specific exercise methods. A study found that core stabilization exercise programs can decrease Cobb angles in adolescents with idiopathic scoliosis. (Ko K. J. & Kang S. J. 2017)
Scoliosis in Adults
Scoliosis is diagnosed in adults, usually in those who have had the condition, treated or not, that was identified in their youth. A study that followed various cases for 20 years found disease progression occurred in 40% of adults but was usually less than one degree per year. However, degenerative scoliosis can also occur in individuals aged 65 and older. (American Association of Neurological Surgeons, 2024)
40 Degrees or More Cobb Angle
Surgery may be recommended once the Cobb angle reaches 40 to 50 degrees. A spinal fusion is often used to force the curve to stop developing. In adults, surgery may be needed if the angle reaches 50 degrees and they experience complications, such as nerve damage or bowel/bladder dysfunction. Risk factors in adults include older age, a history of smoking, and a diagnosis of other conditions, including being overweight. (American Association of Neurological Surgeons, 2024)
Variations
Variations occur in measuring scoliosis, and it is important to understand the difference between a change in scoliosis and a change in the tools or measurement. Equipment errors, imaging errors, and the subjective reading of the healthcare provider can change the values. (Jin, C. et al., 2022) Scoliosis measurement software and intelligent medical devices continue to improve how scoliosis is evaluated and treated. Physical exams, symptoms, and careful monitoring of changes in posture or function are still critical to an accurate diagnosis. The healthcare provider will explain the Cobb angle and other test results.
Injury Medical Chiropractic & Functional Medicine Clinic
Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, and prevent injury. Regarding musculoskeletal pain, specialists like chiropractors, acupuncturists, and massage therapists can help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal issues.
Academic Low Back Pain: Impact and Chiropractic Solutions
References
Botterbush, K. S., Zhang, J. K., Chimakurty, P. S., Mercier, P., & Mattei, T. A. (2023). The life and legacy of John Robert Cobb: the man behind the angle. Journal of neurosurgery. Spine, 39(6), 839–846. https://doi.org/10.3171/2023.7.SPINE23146
Jin, C., Wang, S., Yang, G., Li, E., & Liang, Z. (2022). A Review of the Methods on Cobb Angle Measurements for Spinal Curvature. Sensors (Basel, Switzerland), 22(9), 3258. https://doi.org/10.3390/s22093258
National Scoliosis Foundation. (2015). Scoliosis Media & Community Guide. https://www.scoliosis.org/nsf2/wp-content/uploads/2015/06/ScoliMediaGuide_9June3.pdf
American Association of Neurological Surgeons. (2024). Scoliosis. https://www.aans.org/patients/conditions-treatments/scoliosis/
Ko, K. J., & Kang, S. J. (2017). Effects of 12-week core stabilization exercise on the Cobb angle and lumbar muscle strength of adolescents with idiopathic scoliosis. Journal of Exercise Rehabilitation, 13(2), 244–249. https://doi.org/10.12965/jer.1734952.476
Can the straight leg test help find the cause of back or hamstring pain in individuals experiencing it?
Straight Leg Test
The straight leg raise test is often used to diagnose sciatica/radiculopathy, herniated discs, and other spinal problems. The healthcare provider giving the test performs most of the movement as they assess what’s causing the leg and/or back pain. The patient lies on their back with the legs straight. The provider will have the patient perform specific movements and inform them of how it feels. Then, they’ll raise the leg to see if and at what point symptoms begin to show. Providers often use this test alongside imaging studies.
Some studies suggest the straight leg test helps diagnose sciatica and other causes. (Pesonen J. et al., 2021)
Purpose
The straight leg raise is one of the most common manual tests done during physical exams. The straight leg raise test seeks to reproduce the pain or other symptoms in a controlled fashion to provide clues to what’s happening. It is a manual exam, and the healthcare provider will:
Position the patient
Moves the patient
Create pressure to see how well the patient can resist it
This is often used alongside imaging tests, such as an X-ray or CT scan. (Allegri M. et al., 2016) Its goal is to check for nerve movement and sensitivity of nerve tissue to compression. The straight leg lift test is neurodynamic because it uses movement to diagnose nerve problems. (Baselgia L.T. et al., 2017)
During the Test
Expect to feel some pain during the test, as the whole point is to see what aggravates the symptoms. They may be caused by:
Most of the tests are passive, with the provider doing the lifting. The patient can help achieve the most accurate result by staying as relaxed as possible and being clear about what is felt. (Pande K. 2015) The procedure:
The patient lies on their back with their legs straight.
The provider will ask the patient to turn one of the legs in.
This tells them what hip position affects the lower back symptoms.
They’ll then ask you to bring the leg toward the body’s center.
Then, they’ll lift the straight leg until the patient experiences symptoms.
Pain suggests a herniated disc.
If there is no pain, this also provides valuable information.
The procedure is repeated with the other leg.
Modifications
It’s important to let the examiner know about any limitations. The straight leg raise test has modifications if the patient cannot lift their leg while it’s straight or if they have difficulty lying on their back, which can also help avoid an injury during the test.
Variations
The healthcare provider may repeat the test with the ankle in a dorsiflexed position/raising the foot. Then, they’ll have the patient do it with their chin tucked into their chest. (Young R. et al., 2013) These variations can help check for nerve involvement in specific locations, such as the spinal cord or the dura mater, the membrane covering the brain and spinal cord. (Venne G. et al., 2017) The spinal cord nerves are likely involved and affected if the usual pain is in the back or leg but not the chin, neck, or foot. (Camino Willhuber GO, Piuzzi NS. 2023)
Injury Medical Chiropractic and Functional Medicine Clinic
Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to build optimal health and wellness solutions. We focus on what works for you to relieve pain, restore function, prevent injury, and mitigate issues through adjustments that help the body realign itself. The clinic can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal problems.
From Injury to Recovery with Chiropractic Care
References
Casiano, V. E., Sarwan, G., Dydyk, A. M., & Varacallo, M. A. (2025). Back Pain. In StatPearls. https://www.ncbi.nlm.nih.gov/pubmed/30844200
Pesonen, J., Shacklock, M., Suomalainen, J. S., Karttunen, L., Mäki, J., Airaksinen, O., & Rade, M. (2021). Extending the straight leg raise test for improved clinical evaluation of sciatica: validity and diagnostic performance with reference to the magnetic resonance imaging. BMC musculoskeletal disorders, 22(1), 808. https://doi.org/10.1186/s12891-021-04649-z
Allegri, M., Montella, S., Salici, F., Valente, A., Marchesini, M., Compagnone, C., Baciarello, M., Manferdini, M. E., & Fanelli, G. (2016). Mechanisms of low back pain: a guide for diagnosis and therapy. F1000Research, 5, F1000 Faculty Rev-1530. https://doi.org/10.12688/f1000research.8105.2
Baselgia, L. T., Bennett, D. L., Silbiger, R. M., & Schmid, A. B. (2017). Negative Neurodynamic Tests Do Not Exclude Neural Dysfunction in Patients With Entrapment Neuropathies. Archives of physical medicine and rehabilitation, 98(3), 480–486. https://doi.org/10.1016/j.apmr.2016.06.019
Pande K. (2015). The Use of Passive Straight Leg Raising Test: A Survey of Clinicians. Malaysian Orthopaedic Journal, 9(3), 44–48. https://doi.org/10.5704/MOJ.1511.012
Young, R., Nix, S., Wholohan, A., Bradhurst, R., & Reed, L. (2013). Interventions for increasing ankle joint dorsiflexion: a systematic review and meta-analysis. Journal of foot and ankle research, 6(1), 46. https://doi.org/10.1186/1757-1146-6-46
Venne, G., Rasquinha, B. J., Kunz, M., & Ellis, R. E. (2017). Rectus Capitis Posterior Minor: Histological and Biomechanical Links to the Spinal Dura Mater. Spine, 42(8), E466–E473. https://doi.org/10.1097/BRS.0000000000001867
Camino Willhuber, G. O., & Piuzzi, N. S. (2025). Straight Leg Raise Test. In StatPearls. https://www.ncbi.nlm.nih.gov/pubmed/30969539
For individuals who have to be in one position for long periods, have poor postural alignment, and perform repetitive motions, what are myofascial pain syndrome spasm cycles?
Myofascial Pain Syndrome Spasm Cycles
Myofascial pain syndrome is a common condition that causes pain symptoms in a particular body area (Jafri M. S. 2014). A myofascial pain syndrome spasm cycle is a recurring pattern in which muscle tension and spasms in affected regions, caused by myofascial pain syndrome, lead to pain, triggering more muscle spasms. This creates a vicious cycle of discomfort and tightness that can be difficult to break without treatment; the pain perpetuates muscle spasms and vice versa.
Spasm Pain Cycle
Left untreated, myofascial pain is often experienced as a recurring cycle of spasm, pain, and spasm. (Kojidi M. M. et al., O2016) The exact cause of the spasm is not known. It may be related to excessive accumulation and release of acetylcholine, which causes sustained muscle contraction. (Nicol A, Crooks M, Hsu E, Ferrante M. 2018) Another theory is that repetitive small muscle trauma helps create a trigger point or knot in the muscle. (Thorne. 2021)
Active trigger points in muscles characterize myofascial pain syndrome. (Shah J. P. et al., 2015) These trigger points cause pain in the area where they are located and sometimes in other places, known as referred pain. Each muscle has a particular referral pattern of pain that goes from a trigger point in that muscle to another place in the body. (Shah J. P. et al., 2015) Medical providers and massage therapists trained in this area can identify trigger points by their pain patterns. With myofascial pain syndrome, muscles tense, and joint range of motion may decrease. (Jafri M. S. 2014)
Trigger Points
Myofascial pain syndrome is characterized by trigger points and sensitive knots within muscles that can cause referred pain when pressed, contributing to the spasm cycle.
Muscle Tension
A repeatedly tense or injured muscle can develop trigger points, which can lead tocle tightness and potential spasms.
Pain-Spasm-Pain Cycle
The pain from a trigger point can cause the muscle to further contract and spasm, leading to even more pain and perpetuating the cycle.
How Spasms and Pain Present
Myofascial pain is often caused by long periods of poor postural alignment, muscle injury, and repetitive motions. (Cleveland Clinic, 2023) For example, the upper body slumps forward when sitting at a desk workstation all day. The upper section of the trapezius muscle is located on the back of the neck and the top of the shoulder. The upper trapezius muscle works to raise the head. (Yoo W. G. 2015) The trapezius muscle now has to work more than it is used to. This overuse may cause microscopic muscle injury, leading to muscle spasms and pain. (Bron C., & Dommerholt J. D. 2012) (Nicol A, Crooks M, Hsu E, Ferrante M. 2018) Without treatment, the muscle spasms, pain, and microscopic muscle injury may persist or worsen, leading to trigger points and chronic pain. (Jafri M. S. 2014)
Causes
Repetitive Motions
Repeating the same movement, like typing on a computer, can trigger muscle tension and points.
Poor Posture
Maintaining incorrect posture for extended periods can strain muscles and contribute to trigger point development.
Muscle Injury
Past injuries can leave muscles susceptible to developing trigger points and pain cycles.
Stress
Psychological stress can lead to muscle tension and exacerbate existing trigger points.
Break the Cycle
Physical Therapy
A physical therapist can use stretching, massage, and trigger point therapy to release muscle tension and address trigger points.
Exercise
Regular exercise, including gentle stretching, can help improve muscle flexibility and reduce tension.
Heat Therapy
Applying heat to affected areas can help relax muscles and alleviate pain.
Ergonomics
Modifying work habits and posture to reduce strain on muscles.
Stress Management
Techniques like deep breathing and meditation can help reduce stress-related muscle tension.
Injury Medical Chiropractic and Functional Medicine Clinic
Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to build optimal health and wellness solutions. We focus on what works for you to relieve pain, restore function, prevent injury, and help mitigate issues through adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal problems.
Personal Injury Rehabilitation
References
Jafri M. S. (2014). Mechanisms of Myofascial Pain. International scholarly research notices, 2014, 523924. https://doi.org/10.1155/2014/523924
Kojidi, M. M., Okhovatian, F., Rahimi, A., Baghban, A. A., & Azimi, H. (2016). Comparison Between the Effects of Passive and Active Soft Tissue Therapies on Latent Trigger Points of Upper Trapezius Muscle in Women: Single-Blind, Randomized Clinical Trial. Journal of Chiropractic Medicine, 15(4), 235–242. https://doi.org/10.1016/j.jcm.2016.08.010
Nicol A, C. M., Hsu E, Ferrante M. (2018). Myofascial Pain Syndrome. Science Direct, 207-212. https://doi.org/https://doi.org/10.1016/B978-0-323-40196-8.00025-5
THORNE. (2021). Understanding Muscle Pain, Fascia, and Myofascial Release. https://www.thorne.com/take-5-daily/article/understand-muscle-pain-fascia-and-myofascial-release?srsltid=AfmBOop3Pp0wWEeiQEqpfPgAaTOpLvU7lOAGUv5VRYQdoH8OBcW4D_wk
Shah, J. P., Thaker, N., Heimur, J., Aredo, J. V., Sikdar, S., & Gerber, L. (2015). Myofascial Trigger Points Then and Now: A Historical and Scientific Perspective. PM & R: the journal of injury, function, and rehabilitation, 7(7), 746–761. https://doi.org/10.1016/j.pmrj.2015.01.024
Yoo W. G. (2015). Comparison of activation and change in the upper trapezius muscle during painful and non-painful computer work. Journal of Physical Therapy Science, 27(10), 3283–3284. https://doi.org/10.1589/jpts.27.3283
Bron, C., & Dommerholt, J. D. (2012). Etiology of myofascial trigger points. Current pain and headache reports, 16(5), 439–444. https://doi.org/10.1007/s11916-012-0289-4
Can understanding the planes of motion help individuals adjust fitness training to maximize fitness for physical and sports performance and reduce the risk of injury?
Planes of Motion
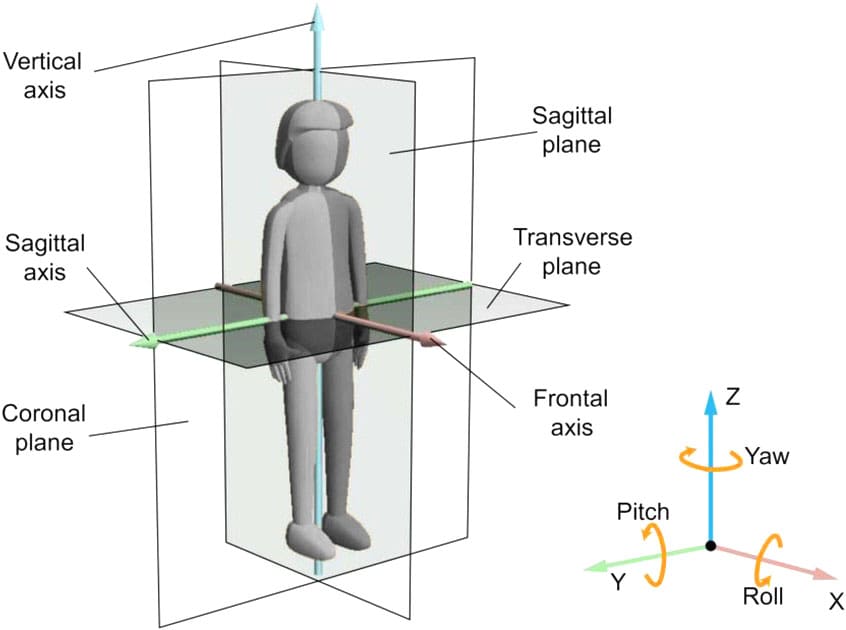
The body’s planes of motion are the sagittal, frontal, and transverse planes, which divide it into left and right, front and back, and top and bottom halves. The body moves in different dimensions during daily work, house chores, and physical activity/exercises. The movements in each plane correspond to forward/backward, side-to-side, and rotational motions. Think of each plane as an imaginary line or a pane of glass that divides the body into opposing segments when standing in the anatomical position. (National Academy of Sports Medicine, 2024)
Sagittal plane -Divides the body into right and left sides.
Frontal plane – Divides the body into front and back.
Transverse plane – Divides the body into top and bottom sections.
To determine the plane of motion of a particular movement, consider how the movement would interact with the imaginary lines or plates. When a movement runs parallel to the imaginary line, the movement is occurring in that plane of motion. For example, when going upstairs, the forward and upward movement at the hip, knee, and ankle occurs primarily in the sagittal plane because that movement runs parallel to the imaginary line that divides the body into right and left sides. Frontal plane movements occur while you walk up the stairs and reach for the handrail. The movement is in the frontal plane because the lateral hand reach runs parallel to the line, dissecting the body into front and back sections. If you turn around to look behind, the rotational movement occurs in the transverse plane because your upper torso runs parallel to the line, dissecting the body into an upper and lower section. Individual movements at any joint in the body can occur in a single plane or multiple planes. Complex movements usually happen in several planes of motion concurrently.
Sagittal Plane
Movement in the sagittal plane generally happens in front or behind. This is the most familiar plane of motion because many typical day-to-day activities happen within arm’s reach in front. Walking, texting, or computer work involves movement primarily in the sagittal plane. Several eating mechanics occur in the sagittal plane. Movements include:
Flexion – A bending movement that decreases the angle at a joint.
Extension – An extending movement that increases the angle at a joint.
Hyperextension – Extending the angle at a joint beyond neutral.
Dorsiflexion – Bending at the ankle so the top of the foot moves toward the shin.
Plantarflexion – Pushing the foot down and away from the body.
Many strength-training exercises in the sagittal plane include biceps curls, forward or reverse lunges, squats, vertical jumping, running, downward dog, and yoga chair poses.
Frontal Plane
The frontal plane divides the body into front/anterior and back/posterior sections. Frontal plane movements are lateral or side-to-side and include:
Abduction – Moving the body or a limb laterally and away from the body’s midline.
Adduction – Moving the body or a limb towards the body’s midline.
Elevation – Moving the shoulder blades up.
Depression – Moving the shoulder blades down.
Eversion – Rolling the foot towards the inside/medial side.
Inversion – Rolling the foot towards the outside/lateral side.
Frontal plane movements are less common than sagittal movements. For example, individuals walk forward more than side to side or reach for something in front rather than directly to the side. Frontal plane movements in fitness include side lunges, lateral shoulder raises, and side shuffles, and in yoga poses, standing side bends and the triangle.
Transverse Plane
The transverse plane divides the body into upper/superior and lower/inferior sections. Transverse plane movements generally involve rotation. Movement in this plane is less common. Exercise injuries most often occur during transverse/rotational movements. (National Academy of Sports Medicine, 2024) Movements include:
Rotation – Moving the torso or a limb around its vertical axis.
Pronation – Rotating the forearm or foot to a palm-side or foot-side down position.
Supination – Rotating the forearm or foot to a palm-side or foot-side-up position.
Horizontal Abduction – Moving the upper arm away from the body’s midline when elevated to 90 degrees.
Horizontal Adduction – Moving the upper arm towards the body’s midline when elevated to 90 degrees.
Typical everyday activities in the frontal plane include turning the head to look behind or turning a doorknob. Exercises in the transverse plane include hitting a golf ball, swinging a baseball bat, or performing a seated twist.
Training Within the Planes of Motion Benefits
Training in all three planes can help with movement in several ways, providing greater ease in life and sports.
Prepares Body for Daily Tasks
Many traditional strength-training programs focus on training one muscle at a time, often in a single plane of motion. For example, weight lifters might do bicep curls to primarily work the biceps in the sagittal plane, a chest fly exercise to primarily work the pectoral muscles in the transverse plane, or lateral raises to work the shoulders in the frontal plane. However, compound exercises have recently become much more common. Compound movements allow individuals to train several muscle groups simultaneously and in different planes of motion.
In this way, training activities mimic daily living activities. For example, individuals often lift several heavy bags of groceries and turn to open the car or trunk, involving both sagittal and transverse movement. Preparing the body for complex activities with compound exercises allows individuals to perform them more easily throughout the day.
Prepares Body for Sports and Physical Activities
Complex multi-planar movements help prepare for safe and effective physical activity and sports performance (National Academy of Sports Medicine, 2024). Researchers and experts understand that many physical and athletic activities require the body to move in different directions, often quickly and under high stress. Several studies have found that anterior cruciate ligament/ACL injuries are more likely to occur during multi-planar rather than single-planar movements. (Quatman C. E., Quatman-Yates C. C., & Hewett T. E. 2010) Training the body to perform multi-planar movements safely and effectively through exercise can help reduce the risk of injury during daily activities or stressful athletic competitions.
Encourages Variation For Full Body Strengthening
Individuals tend to fall into certain movement patterns, such as repeatedly performing the same fitness activity or exercises. This can cause them to have a favorite plane of motion. One way to break away from the same routine is to include movement from all planes of motion. For example, many abdominal workout machines help train in multiple planes of motion, challenging your body to move in different ways. Dumbbells, kettlebells, TRX straps, and bands allow individuals to move joints freely in various planes of motion and work several muscles.
Runners train primarily in the sagittal plane, even if they cross-train by swimming, cycling, or using cardio machines. For this reason, trainers and coaches often recommend doing some form of yoga or weight training that allows them to move their joints in different ways, including lateral movements or rotation. Even flexibility training should incorporate all three planes of motion. For example, walkers might choose to do a simple calf or hamstring stretch at the end of their workout but may also benefit from a seated spine rotation or a lying hip stretch.
Injury Medical Chiropractic and Functional Medicine Clinic
Understanding the concept and importance of training in the three planes of motion can help improve sports and physical performance and prevent musculoskeletal injuries. Chiropractic care aims to help individuals enhance movement with less pain due to condition, after injury, or surgery. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to build optimal health and wellness solutions. We focus on what works for you to relieve pain, restore function, prevent injury, and help mitigate issues through adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal problems.
The Difference of Using Custom Foot Orthotics
References
National Academy of Sports Medicine. (2024). Sagittal, Frontal and Transverse Body Planes: Exercises & Movements. NASM. https://blog.nasm.org/exercise-programming/sagittal-frontal-traverse-planes-explained-with-exercises?utm_source=blog&utm_medium=referral&utm_campaign=organic&utm_content=ReasonsToBecomeCES
Quatman, C. E., Quatman-Yates, C. C., & Hewett, T. E. (2010). A ‘plane’ explanation of anterior cruciate ligament injury mechanisms: a systematic review. Sports medicine (Auckland, N.Z.), 40(9), 729–746. https://doi.org/10.2165/11534950-000000000-00000
While some disc herniations don’t cause symptoms, individuals who are overweight with a herniated disc may experience obesity pressure symptoms such as pain, weakness, numbness, or tingling. Can implementing a physical therapy and weight loss treatment program help individuals find relief?
Obesity Pressure
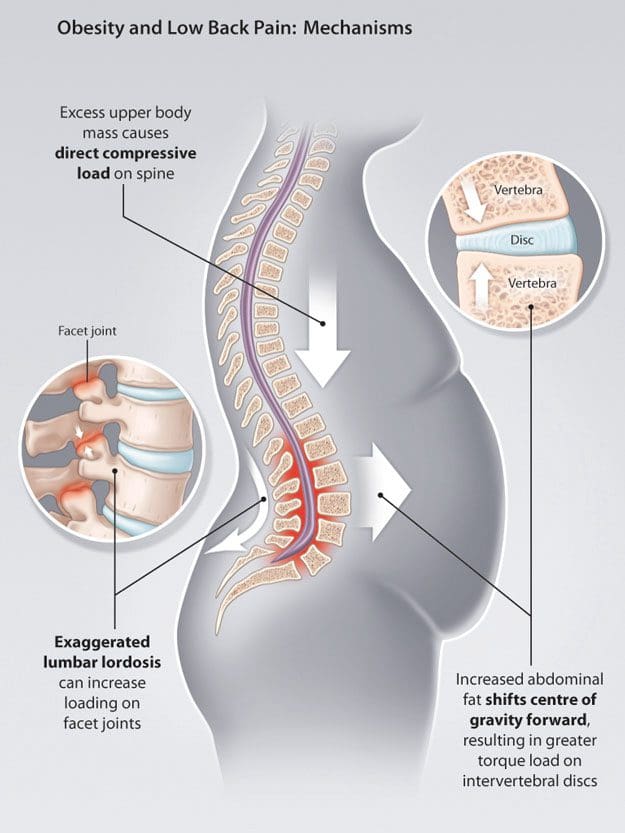
Obesity is one major factor that can contribute to a herniated disc and chronic back pain. When the body has to carry added weight, it can lead to obesity pressure on the intervertebral discs and affect posture and spine position. Researchers have found that other factors, such as inflammation or metabolic changes associated with obesity, can also be involved. (Sheng B. et al., 2017) For individuals who are overweight, weight loss can help resolve a herniated disc combined with physical therapy and can significantly increase herniated disc prevention. (Tokmak M. et al., 2015)
Spine Problems
According to Dr. Alexander Jimenez, owner and head chiropractor at Injury Medical Chiropractic and Functional Medicine Clinic, “When the position of the pelvis and lumbar spine shift out of alignment and become altered, it can profoundly contribute to advanced wearing away of outer fibers in the back region of the discs. These outer fibers house and protect the soft material that cushions and absorbs shock in the spine. Over time, the obesity pressure wear and tear on the fibers can cause chronic pain and microscopic radial tears, leading to a complete rupture.” A rupture causes the soft material to leak, irritate, and inflame surrounding nerve roots. Most herniated discs occur between the sides and back of the vertebra.
Movement Problems
Obesity makes movement difficult, often causing symptoms like shortness of breath and/or early fatigue and exhaustion even with minimal physical activity.
Physical therapy and exercise help relieve obesity and disc herniation.
However, the obesity pressure and herniation pain can make it hard to participate in cardiovascular exercises on a regular basis.
Diagnosis Complications
Obesity can interfere with the diagnosis and treatment of spinal diseases.
This is because weight restrictions and certain imaging tests, like a spinal MRI, can be difficult or impossible to obtain.
A physical examination might not be able to identify signs of nerve compression if an individual is obese. These factors can delay diagnosis.
Disc Position and Posture
Obesity is not the only thing that places pressure on the discs. An individual’s body position significantly influences the health of the shock-absorbing cushions. Sitting generates the most pressure, followed by standing, while lying on your back places the least strain on the discs and, depending on the injury, may help relieve symptoms.
Symptoms depend on the location of the herniation.
The two most common locations are the cervical spine/neck area and the lumbar spine/lower back.
Disc herniations in the neck can affect the arms.
Disc herniations in the lower back affect the buttocks and legs.
Injury Medical Chiropractic and Functional Medicine Clinic
See a healthcare provider if you’re experiencing any of these symptoms. If it is a herniated disc causing symptoms, you might be started on 6 weeks of conservative treatment. This can include physical therapy, rest, health coaching, medication, and surgery, which may be recommended in certain cases. Overcoming these limitations is possible. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, prevent injury, and help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal issues.
Weight Loss Techniques
References
Sheng, B., Feng, C., Zhang, D., Spitler, H., & Shi, L. (2017). Associations between Obesity and Spinal Diseases: A Medical Expenditure Panel Study Analysis. International journal of environmental research and public health, 14(2), 183. https://doi.org/10.3390/ijerph14020183
Tokmak, M., Altiok, I. B., Guven, M., Aras, A. B., & Cosar, M. (2015). Spontaneous Regression of Lumbar Disc Herniation After Weight Loss: Case Report. Turkish neurosurgery, 25(4), 657–661. https://doi.org/10.5137/1019-5149.JTN.9183-13.1
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine