The term �ergogenic� stems from the Greek roots � �Ergon� and �genes,� meaning �work� and �born,� respectively. Any means of enhancing energy production or utilization may be described as an ergogenic aid.1 Ergogenic aids have classically been classified into five categories: mechanical, psychological, physiologic, pharmacologic, and nutritional.2 The present use of the term �ergogenic aid� usually revolves around the physiologic, pharmacologic, and nutritional categories.
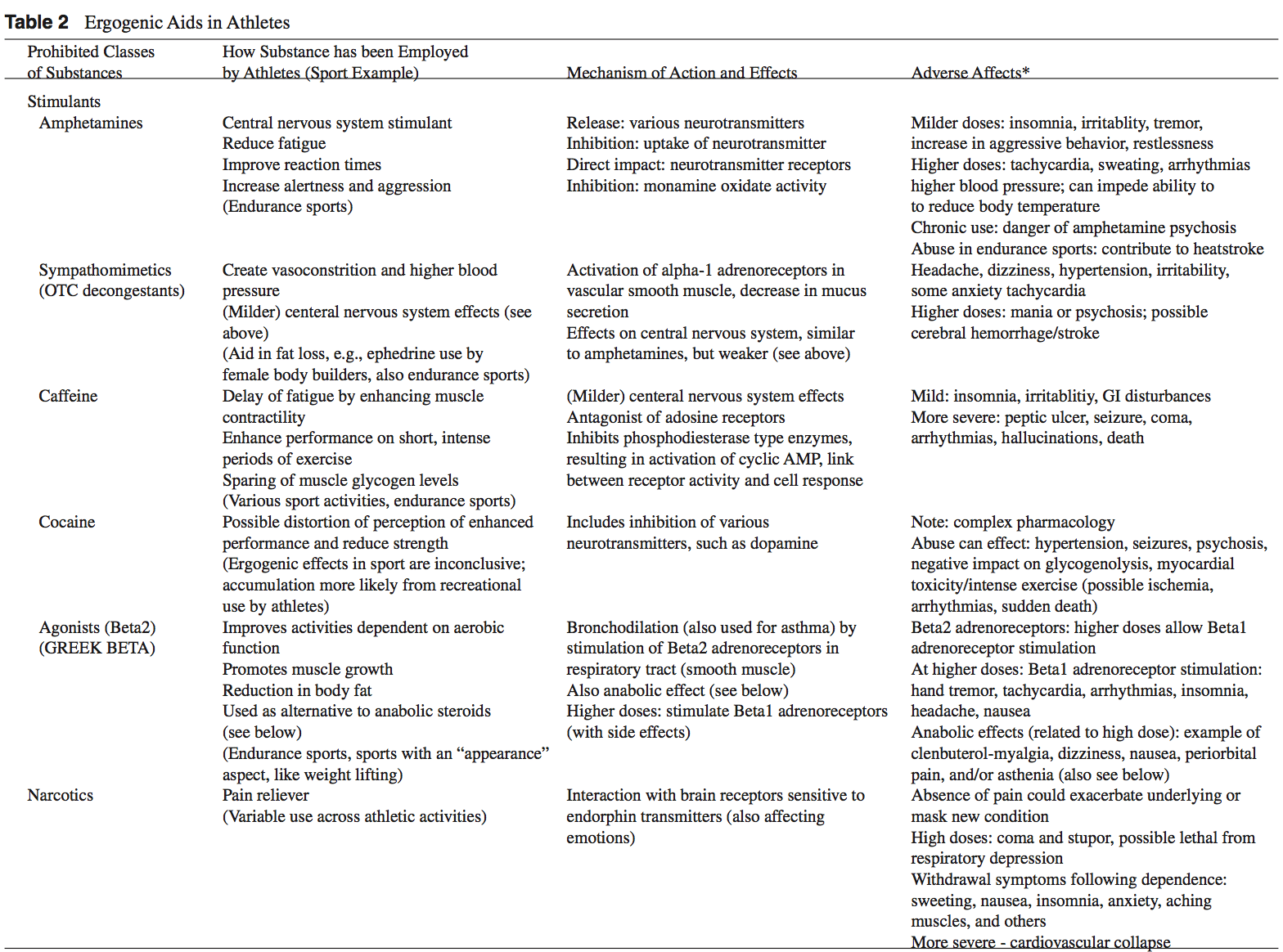
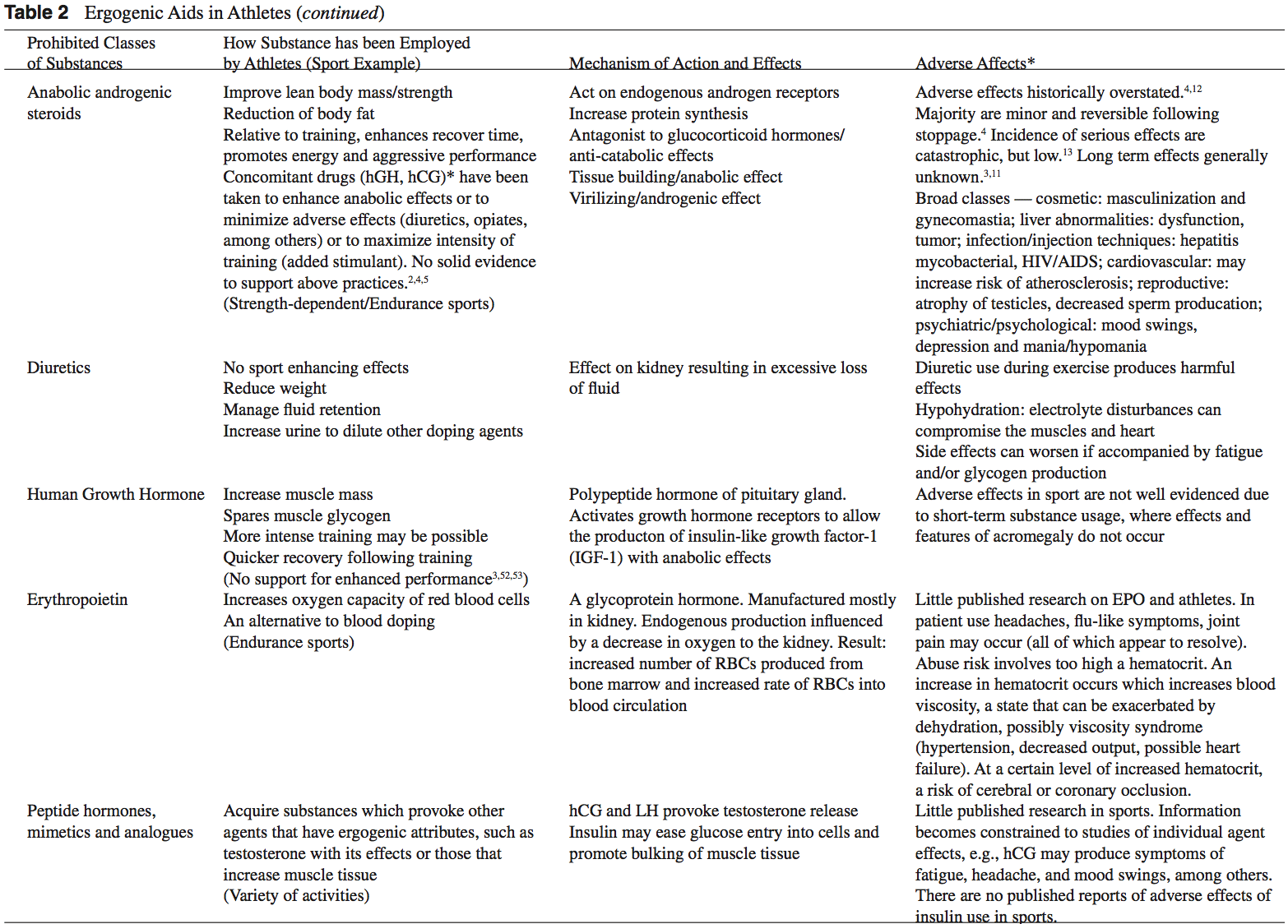
While ergogenic aids have been linked to athletic �doping,� the terms are not synonymous. Doping is a term used by the International Olympic Committee (IOC) to describe the administration or use of a substance by a competing athlete with the sole intention of increasing in an artificial and unfair manner his or her performance in competition.3 Not all ergogenic aids are banned by the IOC. A partial listing of substances banned by the United States Olympic Committee is found in Table 1.2,3 Table 2 provides a list of commonly used athletic ergogenic aids.
Ergogenic Aids:
Anabolic-Androgenic Steroids
Anabolic-androgenic steroids (AAS) are testosterone derivatives that exert anabolic (tissue building) and androgenic (masculinizing) influences on the body.3 Since the discovery of the chemical structure of testosterone in 1935, attempts to separate the anabolic and androgenic effects of AAS�have been unsuccessful.3 Athletes have been using AAS since the 1940s in efforts to improve their performance.2 Concerned with widespread abuse of AAS among athletes, the IOC banned AAS use in the early 1960s.2 The Anabolic Steroids Control Act was legalized in 1990, making it a felony to possess or distribute AAS for non-medical purposes in the United States.3,4 Oral, parenteral, transdermal, and intra-nasal forms of AAS are available. The vast majority of AAS used by athletes is thought to be obtained on the �black market,� as only an estimated 10% to 15% of AAS used by athletes for performance enhancement are obtained by prescription.3
AAS are believed to exert their main effect by increasing anabolic processes and inhibiting catabolic processes via specific receptor mediated responses within the target cells.5 Effects of AAS include: the anabolic build-up of muscle mass, the androgenic development of secondary male sexual characteristics, an anti-catabolic reversal of cortisol�s action, and a direct psychological effect thought to allow a more intense and sustained workout.2,5-8 Early studies of AAS and athletes produced mixed results.5,6 More recent reviews support the notions that AAS can provide significant increases in muscle mass and strength in athletes.2,5,6 In order to maximize the effects of AAS on strength and power athletes, an adequate diet and exercise regimen is needed.5 There seems to be little advantage gained while using AAS in the untrained individual.5,9 Benefits obtained from AAS are more established in strength-dependent sports. Data supporting increased aerobic capacity and improved endurance with AAS use is limited and inconclusive.4 AAS effect on endurance sports is currently an area of great interest given the large number of endurance athletes who still use AAS.4,10
An intricate terminology describing the dosing practices of athletes has evolved. Athletes will commonly use AAS over 6 to 12 week �cycles.�4 �Pyramiding� describes a�gradual escalation in the dose of AAS taken over a cycle.2,11 �Stacking� involves the use of more than one AAS, usually with staggered cycles of the individual drugs.2-4 An �array� describes the practice of using other drugs to counteract side effects or enhance the effects of AAS.3 The practices of cycling, pyramiding, and stacking are used by athletes in an attempt to minimize the negative effects of AAS while maximizing the desired enhancements.2,4 At the current time, no solid scientific support exists for these practices.2,4,5
The adverse effects attributed to AAS abuse have been historically overstated.4,12 The majority of AAS side effects are considered minor and reversible following the cessation of use.4 While the incidence of serious side effects from AAS use has been low, devastating consequences have been reported.13 Documented fatalities from myocardial infarc- tion, stroke, and hepatocarcinoma have been attributed to AAS use.2,3 The long-term effects of AAS use are generally unknown.3,11
Dehydroepiandrosterone (DHEA)
Dehydroepiandrosterone (DHEA) is a precursor to testos- terone produced primarily in the adrenal glands.4,14 Natural sources of DHEA include wild yams. The FDA banned sale of DHEA in 1996 due to insuf cient evidence of safety and value; however, DHEA remains a legal and popular item sold as a nutritional supplement.14,15
The mechanism of action of DHEA is poorly understood but most likely revolves around the conversion of DHEA to testosterone in peripheral tissues.4,14 Preliminary studies suggest that DHEA may have a broad range of clinical uses including anti-Alzheimer and anti-Parkinson capabilities, however randomized, double-blinded clinical studies are�lacking.5
DHEA is a pre-cursor to testosterone and theoretically may enhance athletic performance in a manner similar to AAS. Investigations of DHEA use and athletic performance are scarce.14 Existing studies do not support a significant increase in lean body mass, strength, or testosterone levels with the use of DHEA in athletes.14,16-18
Long-term side effects of DHEA use are currently un- known but are probably similar to those associated with AAS use.6,14
Androstenedione
Androstenedione is a testosterone pre-cursor produced in the adrenal glands and gonads. Several professional athletes have used this substance, bringing it to national attention.2 Androstenedione is found naturally in the pollen of Scottish pine trees.19
Similar to DHEA, the mechanism of action and side ef- fects attributed to androstenedione are poorly understood and thought to be related to the conversion of androstenedione to testosterone in the peripheral tissues.5
Despite manufacturers� claims to the contrary, there is little scientific evidence of the purported ergogenic aid effects of androstenedione.2,5,16,20 Recently concerns have grown over the unfavorable alterations in blood lipid and coronary heart disease profiles seen in men using androstenedione as an ergogenic aid.2,20,21
Dietary Supplements
The increased visibility of ergogenic aids in the last de- cade has occurred primarily because of the passage of the United States Dietary Supplement Health and Education Act (DSHEA) of 1994.22 Certain vitamins, minerals, amino acids, herbs, and other botanical preparations can be classified as a �dietary supplement� under the DSHEA guidelines. Dietary supplements, as a result of DSHEA, are no longer under the direct regulatory control of the FDA. In fact, substances sold as a dietary supplement do not require FDA evaluation for safety or efficacy, and do not have to meet quality control standards expected of approved drugs.5 The content and purity of dietary supplements are not regulated and can vary widely.5,23 Since androstenedione and DHEA have been found to occur naturally in plant sources, these testosterone precursors can be labeled as �dietary supplements� and sold legally over-the-counter.
Ephedra
Dietary supplements containing Chinese ephedra, also known as Mahaung, are marketed as performance enhancers and weight-loss aids.24 Ephedra species of herb have been used for over 5,000 years for respiratory ailments.25 Currently, ephedrine alkaloids are found in hundreds of prescriptions and over-the-counter products, such as antihistamines, decongestants, and appetite suppressants.24-26 Ephedra and related ephedrine alkaloids are sympathomimetic agents that�mimic epinephrine effects.
Multiple studies of isolated ephedrine alkaloids have shown no significant enhancement of power or endurance at dosages considered to be safe.24,27-31 In contrast, the combination of caffeine with ephedrine has been associated with improvements in performance and may promote metabolic effects that are conducive to body fat loss.26,32
The actual content of ephedra alkaloids in 20 ephedra- containing dietary supplements was studied using high- performance liquid chromatography.33 Ten of the twenty supplements exhibited marked discrepancies between the label claim for ephedra content and the actual alkaloid content. Between 1995 and 1997, 926 cases of possible Mahuang toxicity were reported to the Food and Drug Ad- ministration.34 A temporal relationship between Mahuang use and severe complications including stroke, myocardial infarction, and sudden death was established in 37 of the 926 cases. In 36 of these 37 cases, the Mahuang use was reported to be within the manufacturers� dosing guidelines.
Ephedra and related ephedrine alkaloids are currently banned by the U.S.O.C. and cannot be recommended for general use given their association with potentially life- threatening side effects.2,34
Creatine
Creatine use in athletes has grown as a result of a 1992 study that showed that creatine supplementation produced a 20% increase in skeletal muscle creatine concentration.2,35 In the phosphorylated form, creatine serves as an energy substrate that contributes to adenosine triphosphate (ATP) re-synthesis during high-intensity exercise.36 Creatine re- mains popular with power and resistance athletes as it is thought to produce increases in strength, muscle mass, and to delay fatigue.2,14,36
Creatine is synthesized from amino acids primarily in the liver, pancreas, and kidney and is excreted by the kidneys. Creatine is found in skeletal muscle, cardiac muscle, brain, retinal, and testicular tissues.2,37 The interest in creatine as an ergogenic aid revolves around its ability to participate as an energy substrate for muscle contraction.14 Creatine, which easily binds phosphorus, can act as a substrate to donate phosphorus for the formation of ATP. Furthermore, creatine-phosphate (PCr) can help buffer lactic acid because hydrogen ions are used when ATP is regenerated.14,36,38 This role of creatine in exercise is governed by the following reaction:
Normally PCr stores deplete within 10 seconds of short, high-intensity exercise.14,39 Increasing the level of PCr in skeletal muscle, in theory, should result in the ability to sustain high-power output longer and lead to a greater re-synthesis of PCr after exercise.14 The beneficial effects of creatine in response to resistance training are most likely mediated by the following sequence: increased muscle creatine concentration, increased training intensity, which lead to an enhanced physiologic adaptation to training with increased muscle mass and strength.36
Studies evaluating the effectiveness of creatine as an er- gogenic aid are mixed.2,36,40 Multiple reports do conclude that short-term creatine supplementation signi cantly enhances the ability to maintain muscular force and power output dur- ing high-intensity exercise.2,36,41,42 Data on results of creatine supplementation with highly trained athletes is inconclusive. While some papers report improvements with creatine use in highly trained individuals with regards to high-intensity exercise, many show no improvements.2,36,43
Most investigators agree that creatine supplementation does not seem to enhance aerobic-oriented activities.2,36,44
Human muscle is thought to have a maximum concen- tration of creatine that it can hold.14,45 There appears to be no additional bene ts of increasing creatine supplementa- tion above this storage capacity of muscle as the excess is simply excreted by the kidneys.2,46 Humans have differing baseline levels of muscle creatine.14 Accordingly, athletes with lower baseline levels of creatine may be more sensi- tive to creatine supplementation than those with a relatively higher baseline creatine level.14,36 The terms �responder� and �nonresponder� have been used to describe two groups of athletes: those with relatively low baseline creatine levels that may show signi cant performance enhancement with creatine supplementation, and those with high baseline creatine levels that do not show marked improvements with creatine supplementation.14,36,47 These differences in creatine concentrations are thought to play a signi cant role in the varied results on performance found in the literature examin- ing creatine supplementation.14
Reported side effects from creatine use have been scarce.2,14 The major reported side effect associated with creatine use is weight gain, which is thought to be primarily a result of water retention.2,14,48 Some reported longer-term side effects include dehydration, muscle cramping, nausea, and seizures.2,49 Given the relative lack of studies, caution still remains about the long-term effects of creatine usage.14 As creatine use among younger athletes continues to increase, concern is growing over the lack of studies that examine the possible side effects speci c to this age group.14,38
Human Growth Hormone
Human growth hormone (hGH) is a polypeptide produced in the anterior pituitary gland. After its release from the pituitary, hGH can exert its effect in all cells of the body via tissue specific receptors. Human growth hormone is shown to promote protein anabolism, carbohydrate tolerance, lipolysis, natriuresis, and bone and connective tissue turnover.4,50
Potential benefits of hGH abuse in athletes revolve around�its anabolic effect on the body.4 Human growth hormone is thought to increase muscle mass, and spare muscle glycogen by stimulating lipolysis during exercise.2,3 The popularity of hGH among athletes is furthered by the fact that hGH re- mains extremely difficult to detect by current drug screening processes.3,51 Human growth hormone may be particularly attractive to female athletes as the virilization side effects associated with AAS use are not thought to occur with hGH.4
There are no studies that demonstrate signi cant increases in athletic performance with the use of hGH.3,52,53 Neither human or animal studies show any signi cant strength gains with supplemental hGH use in non-de cient individuals.4 The abuse of hGH is thought to be increasing despite the lack of scienti c evidence linking hGH to improved athlete performance.3,52 A survey of high school males revealed that as many as 5% reported past or present use of hGH.54 The purity of hGH abused by athletes may be poor as Drug Enforcement Agency estimates project that up to 30% to 50% of the hGH products sold are phony.4,55
Adverse effects of exogenous hGH use are extrapolated from the ndings seen in patients with endogenous over- secretion of hGH.2 Adults with high levels of hGH are at risk for the clinical syndrome of acromegaly. Medical complications associated with acromegaly include: diabetes, hypertension, coronary heart disease, cardiomyopathy, men- strual irregularities, and osteoporosis.2,4 High levels of hGH in individuals with open physis may lead to gigantism.2
Erythropoietin (EPO)
Recombinant EPO (r-EPO) was approved by the FDA for manufacture in 1989 after the EPO gene was cloned in 1985.14 Since its approval, r-EPO has been abused for athletic personal gain as an alternative to blood doping.3,14 Recombinant EPO has largely replaced the practice of blood doping, as r-EPO produces a dose-dependent increase in hematocrit.2 In theory, r-EPO should provide all of the benefits of blood doping without the risks involved in blood transfusion.3
There are few studies evaluating the use of r-EPO in healthy athletes; however, numerous studies have shown a signi cant increase in work capacity due to r-EPO use in patients with renal disease.14 Berglund and Ekblom reported an increased maximal oxygen consumption and increased time to exhaustion in male athletes after a 6 week trial of r-EPO.56
The risks associated with r-EPO abuse involve the potential for dangerously high hematocrit levels.14 A resulting hyperviscosity syndrome may lead to a decreased cardiac output, hypertension, and potential heart failure.3 Further- more, thrombosis could be manifest as myocardial infarction, pulmonary embolism, or cerebrovascular accidents.2,3 Although the use of r-EPO has been banned by the IOC since 1990, its use is extremely difficult to detect with current drug screening measures.2,14
Antioxidants
The antioxidant capabilities of certain vitamins are believed by many to counter-act the production of free-radials that occurs during exercise.14 Most of the research to date involves vitamin E, vitamin C, and beta carotene.2 The existing literature does not support the notion that antioxidants have significant ergogenic capabilities.2,14,57 There are currently no recommendations for antioxidant use in athletes that exceeds the normal adult recommended daily allowance (RDA).
Beta-Hydroxy-Beta-Methylbutyrate
Beta-hydroxy-beta-methylbutyrate (HMB) is a metabolite of the branched-chain amino acid leucine. HMB is theorized to inhibit muscle breakdown during strenuous exercise but its exact mechanism of action remains unknown.14,58 Studies show that HMB supplementation may significantly lower serum lactate dehydrogenase (LDH), lower serum creatine phosphokinase (CPK) levels and delay blood lactate accumulation after endurance training compared to placebo.59,60 Furthermore, short-term HMB use has been shown to significantly increase strength gains with resistance-exercised training over placebo in one double-blinded study.61
HMB is a relatively new ergogenic aid and published results are considered preliminary.14,58 Although there is evidence for a potential ergogenic aid advantage with HMB use in resistance and endurance training, its use can not be recommended until more studies are performed and potential side effects are elicited.
Caffeine
Caffeine is a methylxanthine occurring naturally in many species of plants. Caffeine is thought to work through a variety of mechanisms. The central nervous system effect of caffeine is probably the result of adrenergic receptor antagonism.3 Its use by athletes stems from the theory that caffeine may delay fatigue by enhancing skeletal muscle contractility and spare muscle glycogen levels by enhancing fat metabolism.6 Multiple studies have reported an improved endurance time with caffeine use.6,62,63 There is evidence that caffeine use may enhance performance with more intense short-duration exercise as well.2 The caffeine dosages most associated with an ergogenic effect range in the literature from 3 to 9 mg per kilogram of body weight.2,6
Side effects associated with caffeine use include anxiety, diuresis, insomnia, irritability and gastrointestinal discom- fort.2,6 Higher doses of caffeine ingestion can lead to more serious consequences such as cardiac arrhythmia, hallucina- tions, and even death.2,3
The legal urine level of caffeine for athletes is 12 ?g/ml (IOC standards) and 15 ?g/ml (National Collegiate Athletics Association standards).6 An athlete would need to drink six to eight cups of coffee in one sitting and be tested within 2 to 3 hours to reach urine levels over the IOC legal limit.3 The amount of caffeine needed to produce ergogenic benefits is potentially far less than that required to exceed the athletic�legal limit.3
Ergogenic Aids: Summary
Claims championing exotic substances that produce healing or ergogenic powers have been around for centuries. The�competitive, peer-pressured environment enveloping today�s athletes and adolescences makes these groups particularly susceptible to the uproar surrounding the current ergogenic aid market. Presently, it seems that rumor and anecdotal information overwhelms the available scientific data. While there is evidence that some touted ergogenic aids do indeed enhance performance, there are many unanswered questions about product safety, efficacy, and long-term consequences. A working knowledge of specific ergogenic aids is essential for the treating physician in order to best advise patients and athletes as to the possible benefits and risks of any substance they may be using.
By Adam Bernstein, M.D., Jordan Safirstein, M.D., and Jeffrey E. Rosen, M.D.
Americans’ Perception Of Chiropractic
Blank
References
1. Williams MH: Ergogenic and ergolytic substances. Med Sci
Sports Exerc 24(9 Suppl):S344-S348, 1992.
2. Silver MD: Use of ergogenic aids by athletes. J Am Acad
Orthop Surg 9(1):61-70, 2001.
3. KnoppWD,WangTW,Bach JrBR: Ergogenic drugsin sports.
Clin Sports Med 16(3):375-392, 1997.
4. Sturmi JE, Diorio DJ: Anabolic agents. Clin Sports Med
17(2):261-282, 1998.
5. Blue JG, Lombardo JA: Steroids and steroid-like compounds.
Clin Sports Med 18(3):667-689, 1999.
6. Ahrendt DM: Ergogenic aids: counseling the athlete.Am Fam
Physician 63(5):913-922, 2001.
7. Adolescents and anabolic steroids:A subjectreview.American
Academy of Pediatrics. Committee on Sports Medicine and
Fitness. Pediatrics 99(6):904-908, 1997.
8. Haupt HA: Anabolic steroids and growth hormone. Am J
Sports Med 21(3):468-474, 1993.
9. Kuipers H, et al: Influence of anabolic steroids on body composition,
blood pressure, lipid profile and liver functions in
body builders. Int J Sports Med 12(4):413-418, 1991.
10. Lombardo JA: Medical and performance-enhancing effects
of anabolic steroids. Psychiatr Ann 22:19-23, 1992.
11. YesalisCE,Bahrke MS:Anabolic-androgenic steroids: current
issues. Sports Med 19(5):326-340, 1995.
12. Friedl KE: Effects of anabolic steroids on physical health.
In:Yesalis CE (ed): Anabolic Steroids in Sports and Exercise
(2nd ed). Champaign, IL: Human Kinetics Publishers, Inc.,
2000, pp. 35-48.
13. Bahrke MS, Yesalis CE, Brower KJ: Anabolic-androgenic
steroid abuse and performance-enhancing drugs among adolescents.
Child Adolesc Psychiatr Clin N Am 7(4):821-838,
1998.
14. Stricker PR: Other ergogenic agents. Clin Sports Med
17(2):283-297, 1998.
15. Dehydroepiandrosterone (DHEA). Med Lett Drugs Ther
38(985):91-92, 1996.
16. Wallace MB, et al: Effects of dehydroepiandrosterone vs
androstenedione supplementation in men. Med Sci Sports
Exerc 31(12):1788-1792, 1999.
17. Nestler JE, et al: Dehydroepiandrosterone reduces serum
low density lipoprotein levels and body fat but does not alter
insulin sensitivity in normal men. J Clin Endocrinol Metab
66(1):57-61, 1988.
18. Welle S,Jozefowicz R, Statt M: Failure of dehydroepiandrosterone
to influence energy and protein metabolism in humans.
J Clin Endocrinol Metab 71(5):1259-1264, 1990.
19. Saden-Krehula M, Tajic M, Kolbah D: Testosterone, epitestosterone
and androstenedione in the pollen of Scotch pine
P. silvestris L. Experientia 27(1):108-109, 1971.
20. King DS, et al: Effect of oral androstenedione on serum testosterone
and adaptationsto resistance training in young men:
a randomized controlled trial.JAm MedAssoc 281(21):2020-
2028, 1999.
21. Broeder CE, et al: The Andro Project: physiological and
hormonal influences of androstenedione supplementation in
men 35 to 65 years old participating in a high-intensity resistance
training program.Arch Intern Med 160(20):3093-3104,
2000.
22. Benning JR: Nutrition for exercise and sports performance. In:
Mahan LK (ed): Krause�s Food, Nutrition and Diet Therapy.
Philadephia: W.B. Saunders Co., 2000, pp. 534-557.
23. SkolnickAA: Scientific verdictstill out on DHEA.JAm Med
Assoc 276(17):1365-1367, 1996.
24. Bucci LR: Selected herbals and human exercise performance.
Am J Clin Nutr 72(2 Suppl):624S-636S, 2000.
25. Anonymous: The Ephedras. Lawrence Rev Nat Prod, 1989.
26. DiPasquale M: Stimulants and adaptogens: Part I. Drug Sports
1:2-6, 1992.
27. Sidney KH, Lefcoe NM: The effects of ephedrine on the
physiological and psychological responsesto submaximal and
maximal exercise in man. Med Sci Sports 9(2):95-99, 1977.
28. Bright TP, Sandage Jr BW, Fletcher HP: Selected cardiac and
metabolic responsesto pseudoephedrine with exercise.J Clin
Pharmacol 21(11-12):488-492, 1981.
29. DeMeersman R, Getty D, Schaefer DC: Sympathomimetics
and exercise enhancement: all in the mind? Pharmacol Biochem
Behav 28(3):361-365, 1987.
30. SwainRA, et al: Do pseudoephedrine or phenylpropanolamine
improve maximum oxygen uptake and time to exhaustion?
Clin J Sport Med 7(3):168-173, 1997.
31. Gillies H, et al: Pseudoephedrine is without ergogenic effects
during prolonged exercise. J Appl Physiol 81(6):2611-2617,
1996.
32. Bell DG, Jacobs I, Zamecnik J: Effects of caffeine, ephedrine
and their combination on time to exhaustion during
high-intensity exercise. Eur J Appl Physiol Occup Physiol
77(5):427-433, 1998.
33. Gurley BJ, Gardner SF, Hubbard MA: Content versus label
claims in ephedra-containing dietary supplements. Am J
Health Syst Pharm 57(10):963-969, 2000.
34. Samenuk D, et al: Adverse cardiovascular events temporally
associated with ma huang, an herbal source of ephedrine.
Mayo Clin Proc 77(1):12-16, 2002.
35. Juhn MS: Orla creatine supplementation: Separating fact from
hype. Phys Sportsmed 27:47-56, 1999.
36. Kraemer WJ, Volek JS: Creatine supplementation: Its role in
human performance. Clin Sports Med 18(3):651-666, 1999.
37. Williams MH: The use of nutritional ergogenic aidsin sports:
is it an ethical issue? Int J Sport Nutr 4(2):120-131, 1994.
38. MetzlJD, et al: Creatine use among young athletes. Pediatrics
108(2):421-425, 2001.
39. Spriet LL: Ergogenic aids: recent advances and retreats. In:
Lamb DR, Murray R (eds): Perspectives in Exercise Science
and Sports Medicine. Indianapolis, IN: Benchmark Press,
1998, pp. 185-238.
40. Johnson WA, Landry GL: Nutritional supplements: fact vs.
fiction. Adolesc Med 9(3):501-513, 1998.
41. Williams MH, Branch JD: Creatine supplementation and
exercise performance: an update. J Am Coll Nutr 17(3):216-
234, 1998.
42. Mujika I, Padilla S: Creatine supplementation as an ergogenic
aid forsports performance in highly trained athletes: a critical
review. Int J Sports Med 18(7):491-496, 1997.
43. Kreider RB, et al: Effects of creatine supplementation on body
composition,strength, and sprint performance. Med Sci Sports
Exerc 30(1):73-82, 1998.
44. Balsom PD, et al: Creatine supplementation per se does not
enhance endurance exercise performance.Acta Physiol Scand
149(4):521-523, 1993.
45. Harris RC, Soderlund K, Hultman E: Elevation of creatine in
resting and exercised muscle of normal subjects by creatine
supplementation. Clin Sci (Lond) 83(3):367-374, 1992.
46. Clark JF: Creatine: A review of its nutritional applications in
sport. Nutrition 14(3):322-324, 1998.
47. Casey A, et al: Creatine ingestion favorably affects performance
and muscle metabolism during maximal exercise in
humans. Am J Physiol 271(1):E31-E37, 1996.
48. Volek JS: Creatine supplementation: its effect on human
muscular performance and body composition.J Strength Cond
Res 10:200-210, 1996.
49. Feldman EB: Creatine: a dietary supplement and ergogenic
aid. Nutr Rev 57(2):45-50, 1999.
50. Yarasheski KE: Growth hormone effects on metabolism, body
composition, muscle mass, and strength. Exerc Sport Sci Rev
22:285-312. 1994.
51. Risser WL: Sports medicine. Pediatr Rev 14(11):424-431,
1993.
52. Bidlingmaier M, Wu Z, Strasburger CJ: Doping with growth
hormone. J Pediatr Endocrinol Metab 14(8):1077-1083,
2001.
53. Jenkins PJ: Growth hormone and exercise: physiology, use and
abuse. Growth Horm IGF Res 11(Suppl A):S71-S77, 2001.
54. Rickert VI, et al: Human growth hormone: a new substance
of abuse among adolescents? Clin Pediatr (Phila) 31(12):723-
726, 1992.
55. Council Report: Drug abuse in athletes, anabolic steroids and
human growth hormone. J Am Med Assoc 259:1703-1705,
1988.
56. Berglund B, Ekblom B: Effect of recombinant human erythropoietin
treatment on blood pressure and some haematological
parameters in healthy men. J Intern Med 229(2):125-130,
1991.
57. Williams MH: Nutritional supplements for strength trained
athletes. Sports Sci Exchange 6:1-6, 1993.
58. Williams MH: Facts and fallacies of purported ergogenic
amino acid supplements. Clin Sports Med 18(3):633-649,
1999.
59. Vukovich MD, Dreifort GD: Effect of beta-hydroxy betamethylbutyrate
on the onset of blood lactate accumulation
and VO2 peak in endurance-trained cyclists. J Strength Cond
Res 15(4):491-497, 2001.
60. Knitter AE, et al: Effects of beta-hydroxy-beta-methylbutyrate
on muscle damage after a prolonged run. J Appl Physiol
89(4):1340-1344, 2000.
61. Jowko E, et al: Creatine and beta-hydroxy-beta-methylbutyrate
(HMB) additively increase lean body mass and muscle
strength during a weight-training program. Nutrition 17(7-
8):558-566, 2001.
62. Graham TE, Spriet LL: Performance and metabolic responses
to a high caffeine dose during prolonged exercise. J Appl
Physiol 71(6):2292-2298, 1991.
63. KalmarJM, Cafarelli E: Effects of caffeine on neuromuscular
function. J Appl Physiol 87(2):801-808, 1999.
El Paso, TX. Chiropractor, Dr. Jimenez takes a look at top running shoes that are great for knee pain and Iliotibial (IT) Band Syndrome.
Running Shoes: Knee pain is one of the common problems with most active people. It could get worse for those who love running, especially the athletes. A majority of them suffer from knee pains each year. This pain hinders you from enjoying your daily sports activities and might even become worse with time if not treated correctly. There are causes and cures for such pains that this article is going to look at, but the main focus is on the best shoes for knee pain, also referred to as Iliotibial (IT) Band Syndrome.
This can happen due to various causes like overtraining, running many hills, and wrong running form, among others. These injuries are very frustrating as they can take up to months to go away. This is the reason different companies have designed shoes that will offer you support for any knee problem.
What Goes Wrong
The iliotibial band (ITB) is usually a structure whose job is to provide leg stability whenever you take a step. It works with the hip muscles in a thigh’s outward movement and also helps counter the movements within the knee joint. This band starts in the hip and ends just under the knee joint.
Repeated use of the ITB leads to stress, causing knee pain. You will also notice clicking sensations from the joint as ITB snaps across it. This pain is always experienced when the heel comes into contact with the ground; running slowly or downhill tends to make the symptoms worse.
ITBS will usually start as tightness while running but continues to a point where the pain is severe and unbearable. Although ITB continues to tighten when overstressed or injured from training, this is not the main problem. What causes the injury is how the ITB functions and the weakness around it.
The ITB is generally a weak structure and any weakness around it will lead to injury. Most runners have weak core muscles due to the fact that they don’t do strength training or have never been in any sports with side-to-side movement.
Signs Of IT Band Syndrome
If you are a runner, you will be able to distinguish ITBS by:
A swelling
A cracking feeling when stretching the knee
A feeling of burning, stinging and aching on the outer side of the knee that might migrate to the thigh. You will notice these discomforts especially, on your second half of the run.
Bending the knee at 45 degrees causes severe external knee pain
Criteria You Should Follow When Selecting The Best Running Shoes for ITBS
?There are various things that you should always consider when buying running shoes. Since most runners experience knee pain, it is wise to look for shoes that will help alleviate this pain without slowing them down. Below are some of the features to look out for in running shoes:
Stability/ Support
Since it is common to have knee pains due to lack of motion control and lack of stability, it is good to choose shoes that will offer you the support you need while running. If your running shoes don’t have any stability, you will end up stressing out your knee, which will result in pain and discomfort while running.
Fit
If you want to do away with pain, you might consider looking for a fit pair of shoes as they will reduce any pain, causing issues in the long run. Pay attention to small specifics like shoes that offer enough heel space, sufficient toe box room, and enough space for wide feet. Your toes should be able to move freely without being constricted.
If your foot cannot move freely and the toes are restricted from spreading, it could lead to painful issues in your feet, legs, and knees.
Motion control footwear is not the whole solution; you need to ensure your feet can still function naturally as they are supposed to.
Comfort
No one wants to wear uncomfortable shoes! Each of these selected best shoes come with upper and underfoot comforts to ensure you get to enjoy your run.
Most of these shoes are made with DNA technology, Gel cushioning, and REVlite midsole for ultimate comfort.
Durability
Your running shoes should run their course without falling apart as this will cause you pain in the long-run. If they promise to offer you support, they should do just that and not start peeling off and tearing when you are on the run.
The ??below 5 shoes have passed the durability test to ensure they give you maximum performance.
Breathability
Although this has nothing to do with knees, it is paramount that your running shoes have enough breathing space to avoid accumulating excess moisture, which might bring discomfort and other feet related problems.
There is no magical cure for knee pain and you should always know the root cause. This way, you will be able to come up with the best solution of minimizing or even eliminating the pain entirely. Although there are various causes of knee pain, this article is focusing on ITB syndrome which happens to be one of the causes.
Reviews Of The Top 5 Shoes
These shoes have been selected with the runner’s welfare in mind. They will help deal with the ITBS, which is a problem for most of them. Since one way of dealing with this condition is getting good running shoes, here is a review of such products.
Asics Gel Kayano 23
This upgraded version is lightweight to help with any knee problems. It offers you comfort through cushioning that help absorb shock as you run as well as other features like grip, fit, and durability. The shoe has an added outer sole to ensure it lasts you as long as possible.
PROS
?Gel cushioning will act as a shock absorber for more comfort
?Has superb breathability feature
?Is ideal for overpronation and knee pain
?The outsole’s traction will offer the intended support on various surfaces
CONS
?It is a bit pricey
New Balance 890v5
It tops the list of 5 best running shoes. Also, it has remained the first choice for most runners with knee pain issues. This pair offers all the above functionalities too, making it your best choice.
PROS
?It comes with one of a kind breathability and fit due to its great FantomFit design
?Its smooth upper construction will ensure no irritation occurs
?The REVlite midsole will give you much needed cushioning
CONS
?It has a narrow toe box and might not fit a person with a wide foot
?Puma Faas 600 V3
Puma models have never disappointed, and this one is no exception. Puma Faas 600 is the solution to your knee pain. It is also an affordable option for the short-handed.
PROS
?Great breathability
?Comes at a reasonable price
?It’s lacing system and fit offers you a secure and comfortable run
?It is designed to fit perfectly
CONS
?There have been reported concerns about the outsole’s durability
New Balance 1080v7
This is another great choice on the list. It is one of the New Balance Fresh Foam Series. Its midsole offers you the required support coupled with comfort to eliminate knee pains.
PROS
?Very durable
?Enough breathability for long runs
?Good amount of cushioning and support from the Fresh Foam midsole
?It fits like a sock giving you a confident use
CONS
?The upper design is not seamless
?Can be stiff
Saucony Hurricane 16
This is the 16th edition of the Saucony Hurricane, which offers a combination of steadiness and protection. Those with knee pain have agreed with the stability offered by this shoe. It is also cushioned to help you go for long runs without any pain or injury. It is perfect for heavy runners and those who are out of shape due to inactivity.
PROS
?Superb stability
?Lightweight rubber offers protection and cushioning
?Great ground contact
?Reflective parts allow you to have a safe run
?Comes with Sauc-Fit Technology that enhances its comfortability
CONS
?It is a bit narrow
?Limited colors to choose from
?Might be heavy for fast runners
If you are a long-distance runner, it is good to know that your shoes cushioning will wear out quite easily and you might be tempted to continue using them since they look good on the outside. This is a big mistake. The following will help you prevent any more ITBS recurrences:
Replace running shoes frequently to avoid wearing those with worn out inner cushioning
Always give your shoes time to rest so that the cushioning can get restored; it would be wise to have two pairs of running shoes.
Although shoes can offer you relief from ITBS, it is better to look out for other ways of helping you cope with or eliminate the pain entirely. Also, know what triggers the problem and avoid it at all costs.
These shoes have been tried and tested and found to offer support and help in managing the iliotibial band syndrome. Asics takes the lead on these best shoes. It comes with gel cushioning that will offer you the best shock absorption and maximum comfort as seen above. Its sole is also made to help you tackle any terrain and you can be assured that your knees will thank you later. The only drawback is the price, which is on the upper-side. However, always remember that cheap is expensive.
If you are an active person or an athlete suffering from ITBS, go ahead and get yourself a pair of these shoes as per your preference and choice.
Hey there, I’m Zoey, founder and the main editor of The Babble Out. I know nobody’s life is smooth as they wish, and it�s the same with mine. I had some terrible news a few years ago and running was the way I got through these issues. This has given me enough motivation to create this blog, so that I can give you a helping hand for as many daily problems as I can. If you are curious why “babble out” is the? name of the blog, then check the “About” page and find out more about me.
Yoga is a great way to improve flexibility and strength in your body. In this article we will go over some standing poses to use in your practice.
YOGA: MOUNTAIN POSE (TADASANA)
The mountain pose is the foundation of all standing poses. It might not look like much but the mountain pose is an important starting position, resting pose and tool to improve posture which leads to many other standing poses in yoga.
�
�
STANDING FORWARD BEND (UTTANASANA)
Standing forward bend is a smooth transition from mountain pose and you will find a deep stretch in the entire back body.
�
WARRIOR I POSE (VIRABHADRASANA I)
There are three variations of the warrior pose of which this is number I.
�
�
WARRIOR II (VIRABHADRASANA II)
Warrior II stretches and strengthens the body in the one movement, allowing you to feel like a strong warrior. This pose will build strength your ankles, legs, glutes, core, back and shoulders.
�
REVERSE WARRIOR (VIPARITA VIRABHADRASANA)
Reverse Warrior is a variation of the warrior II pose that provide a great stretch in the side body.
Occlusion training involves restricting the flow of blood to a muscle group while training. That is why it is also commonly called �blood flow restriction training.�
Basically you take a wrap or band and apply it to the top of your limb.
The aim of this�isn�t�to completely cut off circulation to the area as that is dangerous and painful.
This means that you aren�t restricting arterial flow to the area, but you are restricting the venous return from the muscles.
Arteries are what takes the blood from your heart to your muscles and it is then returned to your heart through a system of veins.
Restricting the blood flow back to your heart causes a pooling of the blood in the area that you are working.
This is what occlusion training uses to create an�anabolic effect�on your muscles.�
HOW DOES OCCLUSION TRAINING WORK?
The bloodstream is the network that connects the muscles in your body, providing oxygen and nutrients and carrying away waste products
Muscles require a steady flow of blood to operate.
That is why we aren�t cutting off the flow to the muscle, we are only slowing the rate at which the blood releases from it.
When performing any kind of resistance training your body directs more blood to your muscles performing the exercise.
The reason you get a �pump� when working out is that the speed at which your body is pumping blood into your muscles is faster than the amount of blood going out of them.
Your pump reduces when you rest between your sets as more blood is released from your muscle groups.
Blood flow restriction training prolongs and intensifies your pump.
This is done by placing wraps in one of two places during your working sets.
You wrap above your bicep for movements that involve your bicep�s, triceps, forearms, and even chest and back can benefit from this.
While wrapping in this position it makes sense that it would benefit your arms but how does it help your chest and back?
There is no possible way that you can restrict blood flow to your chest and back because of the positions they are located in.
However wrapping your arm allows you to pre-fatigue your arms and as a result chest and back exercises that you perform are going to require more involvement from those muscles rather than your biceps or triceps.
Wrap your upper thigh for movements that involve your quads, hamstrings, glutes and calves.
Building Muscle With Occlusion Training
During training you have two�types of muscle�that are responsible for all muscle growth in the gym.
Fast twitch fibers and slow twitch fibers.
Slow twitch muscle fibers are smaller muscle fibers and generate less power and strength than fast twitch fibers. However slow twitch fibers fatigue slower and can sustain activity for longer.
Fast twitch fibers are larger muscle fibers, generate more power and strength and have the most potential for growth.
Fast twitch fibers are recruited last during contractions and mostly don�t use oxygen. Slow twitch fibers on the other hand use oxygen and are recruited first in the movement.
This means that by restricting the blood flow to a muscle group you are pre-fatiguing the slow twitch fibers and forcing the fast twitch fibers to take control even when you�re using low weights.
Occlusion training seems to�trick your body�into thinking you are lifting heavy weights. This means you can get very�similar benefits�of heavy training by using 20-30% of your 1 rep max.
There are two main factors that lead to muscle growth during training. These are:
Metabolic Stress
Cellular Swelling
Metabolic Stress
When you�re working out your body is burning energy. As your body chews through its fuel stores, metabolic by-product accumulates in your muscles.
Metabolic by-products act as an anabolic signal, telling your body to increase size and strength.
Under normal training most of these by-products would be washed out by blood flow.
Occlusion training keeps them near the muscle helping to increase the anabolic effect that the by-products have on the muscles.�
Cellular Swelling
During resistance training your cells expand and fill with fluid and nutrients. This is known as cellular swelling and has also been shown to be an anabolic�signal for muscle growth.
Occlusion training isn�t a better option than heavy training, but that said it is a nice supplement.
Regularly pushing your muscles to the point of failure or at least close to it (1-2 reps) is an important factor of increasing your strength and muscle mass.
Occlusion training allows you to replicate this without putting anywhere near as much strain on your joints, ligaments and tendons as you would to get the same result from lifting heavy.
This means that you can do more volume without the risk of�overtraining.
Here are a couple of scenarios where this could be really beneficial for you:
If you suffer from joint issues
If you�re travelling and only have access to hotel weights
If you�re injured or have nagging aches and pains.
In short your body might not always feel up to another heavy training day. Occlusion training can be a great way to get a good workout in and help you maintain muscle mass.�
How To Do Blood Flow Restriction Training
As I mentioned earlier you only ever wrap yourself at the top of your biceps and the top of your thighs.
Elastic knee wraps, medical tourniquets and exercise band �are good options to use for your wraps.
Here�s two videos explaining how to wrap your arms and legs
Blood flow restriction training works best when with isolation exercises. If you are going to do compound movements do them at the start of your workout and save the blood flow restricted exercises for the end.
Layne Norton recommends performing lifts at 20%-30% of your 1rm for 20-30 reps of the first set and then the next three sets at 10-15 reps. Have a 30 second rest between sets before going again.
You want to keep the cuffs on your limbs for the entire 4 sets and then release them at the end.
If you�re in pain before the exercise starts that�s a good sign that your wraps are too tight.
Also if you can�t complete the prescribed sets either the wraps are too tight or the weight is too heavy.�
Conclusion
Blood flow restriction training has been getting a lot of hype lately.
While it isn�t better than regular strength training, it is a good supplement for it and can be beneficial when used in conjunction with your regular training.
This is more of an advanced training technique so if you are just starting out lifting it probably won�t give you any more benefits than your normal heavy training.
If you�re an advanced lifter, are injured, or don�t have access to heavier weights than this training technique could benefit you.
Deadlifts are one of the best strength and mass building exercises that you can perform.
When performing the deadlift you are working more muscles than any other exercise, including the squat.
Deadlifts have many different variations and forms. In this article we are going to focus on the difference between the Romanian Deadlift and standard deadlifts.
There are lots of valid arguments as to which exercise is better in a Romanian Deadlift vs regular deadlift battle.
Keep reading to learn the differences.
Romanian Deadlift Vs. Standard Deadlift
The Romanian Deadlift is one of the most�commonly used among the various deadlift techniques.
In fact a lot of people that think they are performing a deadlift are sometimes actually doing a Romanian Deadlift.
Both the conventional and Romanian Deadlifts are great strength and muscle building exercises.
Even though they are both deadlifts�variations the setup, execution and muscles activated are different.
Here�s a quick video that highlights the differences in form and setup between the two.
Regular Deadlift
As the name suggests the deadlift is a strength training exercise that involves�lifting dead weight.
The regular deadlift is one of the best total body exercises you can do as it works just about every fiber in your body.
The deadlift requires you to lift a weight off the ground�and lower it back down again. Although it may sound simple there is a lot going on in the movement and incorrect form can cause injuries.
One of the most common causes for injury while deadlifting is rounding the back. Your lower back must stay neutral during the whole movement. Rounding your lower back during heavy deadlifts puts uneven pressure on your spine. Always lift with a neutral lower back, allowing for the natural inward curve of your lower spine.
Don�t try and rush to lift heavier weights. the quickest way to improve your deadlift is through correct form. By pulling more efficiently you can use more muscles and deadlift heavier. So start out practicing correct form and build your way up.
The best way to approach the exercise is to think as if you were leg pressing the floor as opposed to�using your upper body to lift something. This will help you mentally focus on using your legs rather than your back (which can cause rounding) for the exercise.
The �dead� in deadlift stands for dead weight so each rep must start on the floor, from a dead stop. �Deadlifts are different to other exercises like the bench press or squat where the weight starts at the top. The deadlift movement�starts from the bottom and and you pull the weight up then return it to the floor�for one rep.
Here are�Stronglifts�5 steps to proper deadlift form:
Walk to the bar.�Stand with your mid-foot under the bar. Your shins shouldn�t touch it yet. Put your heels hip-width apart, narrower than on Squats. Point�your toes�out 15�.
Grab the bar.�Bend over without bending your legs. Grip the bar narrow, about shoulder-width apart like on the Overhead Press. Your arms must be vertical when looking from the front.
Bend your knees.�Drop into position by bending your knees until your shins touch the bar. Do NOT let the bar move away from your mid-foot. If it moves,�start from scratch with step one.
Lift your chest.�Straighten your back by raising you chest. Do not change your position � keep the bar over your mid-foot, your shins against the bar, and your hips where they are.
Pull.�Take a big breath, hold it and�stand up with the weight. Keep the bar in contact with your legs while you pull. Don�t shrug or lean back at the top.
Lower the bar by moving your hips back while keeping your legs almost straight. Once the bar is past your knees, bend your legs more. The bar will land over your mid-foot, ready for your next rep.
Rest a second between reps while staying in the setup position. Take a deep breath, get tight and pull again. Every rep must start from a dead stop on the floor. Don�t bounce the weight off the floor or you can end up lifting�with�bad form.
Ever felt pain in your hip, the center of the buttocks, or pain down the back of the leg, you’re likely suffering, at least partly, with piriformis syndrome. The piriformis is a muscle which runs from the sacrum (mid-line base of spine) into the outer hip bone (trochanter). This muscle works overtime on runners.
The muscles in and about the gluteal area help with three areas
� rotation of the hip and leg;
� balance while one foot is off the ground
� stability of the pelvic region.
Needless to say, every one of these attributes are highly needed by runners and everyone else.
Piriformis Injuries
RMI or repetitive motion injury occurs when a muscle has to perform beyond the level of its capability, not given time to recover and doing it again and again. The normal response from a muscle in this situation is to tighten, which is a defensive response of the muscle. This stimulation, however, manifests itself several ways.
First Symptom�indicating piriformis syndrome could be pain in and about the outer hip bone. The tightness of the muscle generates increased pressure between the bone and the tendon which produces pain and either discomfort or an increased tension in the joint which produces a bursitis. A bursitis is an inflammation of the fluid filled sac in a joint caused by tension and strain within that joint.
Second Symptom suggesting piriformis syndrome would be pain right at the middle of the buttocks. Although this is not as common as the other two symptoms, this pain can be brought on within the fatty part of the buttocks region with direct compression. A tight muscle becomes a sore muscle upon compression because of reduced blood flow to that muscle.
Third Symptom indicating piriformis syndrome would be a sciatic neuralgia, or pain from the buttocks down the back of the leg and at times into different parts of the lower leg.
The sciatic nerve runs directly through the belly of the piriformis muscle and in the event the piriformis muscle contracts from being overused, the sciatic nerve now becomes strangled, producing pain, numbness and tingling.
Physiology
Any muscle constantly used has to have an opportunity to recover. This recovery can be natural with time, or could be facilitated and sped up with treatment. Continuing use will make it even worse since the muscle is tightening due to overuse. This injured muscle needs to relax and have blood flow encouraged into it for a rapid recovery. The tightness� lessens the normal blood flow going to the muscle. To encourage new blood into the muscle is the way of getting the muscle to begin to unwind and operate normally. Massages daily to this area is greatly supported.
The next step in this “recovery” process is to use a tennis ball under the butt and hip area. Roll out from the side of engagement while sitting down on the ground and set a tennis ball inside the outer hip bone under the buttocks area. Note areas of pain and soreness, as you start to allow your weight onto the tennis ball. Trigger points will have a tendency to collect in a repetitively used muscle, and till these toxins are manually broken up and removed, the muscle will have an artificial well being concerning flexibility potential and recovery potential. Consequently, if it’s sore while your sitting on it, you’re doing a good job. Let the ball operate under every spot for 15-20 seconds before transferring it to a different place. After 4-5 minutes place cross legs with the ankle of the affected leg over the knee of the non-affected leg. Then place the tennis ball just inside the outer hip bone and work the tendon of the muscle. Although this pain requires some time to reduce and is excruciating, the advantages are enormous. Be patient and good things will happen.
Treatments
Due to how the sciatic neuralgia and the hip bursitis or tendonitis are both inflammatory in character, ice therapy, or cryotherapy, within the involved region 15-20 minutes at a time will be beneficial. This should be performed multiple times each day.
Once the acute pain is gone then start with gentle stretching, like a cross-legged stretch while pulling up on the knee. The muscle should have improved flexibility.
Finally the use of pharmaceutical anti-inflammatories are not encouraged. One the intestines are greatly aggravated by them, but they also suggest an artificial wellbeing that can lead to larger problems. Proteolytic enzymes, such as bromelain, extremely beneficial without any side effects and are organic.
Even though the effects of overweight and obesity on diabetes, cardiovascular disease, all-cause mortality, and other health outcomes are widely known, there is less awareness that overweight, obesity, and weight gain are associated with an increased risk of certain cancers. A recent review of more than 1000 studies concluded that sufficient evidence existed to link weight gain, overweight, and obesity with 13 cancers, including adenocarcinoma of the esophagus; cancers of the gastric cardia, colon and rectum, liver, gallbladder, pancreas, corpus uteri, ovary, kidney, and thyroid; postmenopausal female breast cancer; meningioma; and multiple myeloma.1�An 18-year follow-up of almost 93?000 women in the Nurses� Health Study revealed a dose-response association of weight gain and obesity with several cancers.2
Obesity Increase
The prevalence of obesity in the United States has been increasing for almost 50 years. Currently, more than two-thirds of adults and almost one-third of children and adolescents are overweight or obese. Youths who are obese are more likely to be obese as adults, compounding their risk for health consequences such as cardiovascular disease, diabetes, and cancer. Trends in many of the health consequences of overweight and obesity (such as type 2 diabetes and coronary heart disease) also are increasing, coinciding with prior trends in rates of obesity. Furthermore, the sequelae of these diseases are related to the severity of obesity in a dose-response fashion.2�It is therefore not surprising that obesity accounts for a significant portion of health care costs.
Cancers
A report released on October 3, 2017, by the US Centers for Disease Control and Prevention assessed the incidence of the 13 cancers associated with overweight and obesity in 2014 and the trends in these cancers over the 10-year period from 2005 to 2014.3�In 2014, more than 630?000 people were diagnosed as having a cancer associated with overweight and obesity, comprising more than 55% of all cancers diagnosed among women and 24% of cancers among men. Most notable was the finding that cancers related to overweight and obesity were increasingly diagnosed among younger people.
From 2005 to 2014, there was a 1.4% annual increase in cancers related to overweight and obesity among individuals aged 20 to 49 years and a 0.4% increase in these cancers among individuals aged 50 to 64 years. For example, if cancer rates had stayed the same in 2014 as they were in 2005, there would have been 43?000 fewer cases of colorectal cancer but 33?000 more cases of other cancers related to overweight and obesity. Nearly half of all cancers in people younger than 65 years were associated with overweight and obesity. Overweight and obesity among younger people may exact a toll on individuals� health earlier in their lifetimes.2�Given the time lag between exposure to cancer risk factors and cancer diagnosis, the high prevalence of overweight and obesity among adults, children, and adolescents may forecast additional increases in the incidence of cancers related to overweight and obesity.
Clinical Intervention
Since the release of the landmark 1964 surgeon general�s report on the health consequences of smoking, clinicians have counseled their patients to avoid tobacco and on methods to quit and provided referrals to effective programs to reduce their risk of chronic diseases including cancer. These efforts, coupled with comprehensive public health and policy approaches to reduce tobacco use, have been effective�cigarette smoking is at an all-time low. Similar efforts are warranted to prevent excessive weight gain and treat children, adolescents, and adults who are overweight or obese. Clinician referral to intense, multicomponent behavioral intervention programs to help patients with obesity lose weight can be an important starting point in improving a patient�s health and preventing diseases associatedwith obesity. The benefits of maintaining a healthy weight throughout life include improvements in a wide variety of health outcomes, including cancer. There is emerging but very preliminary data that some of these cancer benefits may be achieved following weight loss among people with overweight or obesity.4
The US Preventive Services Task Force (USPSTF)
The US Preventive Services Task Force (USPSTF) recommends screening for obesity and intensive behavioral interventions delivered over 12 to 16 visits for adults and 26 or more visits for children and adolescents with obesity.5,6�Measuring patients� weight, height, and body mass index (BMI), consistent with USPSTF recommendations, and counseling patients about maintaining a healthy weight can establish a foundation for preventive care in clinical care settings. Scientific data continue to emerge about the negative health effects of weight gain, including an increased risk of cancer.1�Tracking patients� weight over time can identify those who could benefit from counseling and referral early and help them avoid additional weight gain. Yet less than half of primary care physicians regularly assess the BMI of their adult, child, and adolescent patients. Encouraging discussions about weight management in multiple health care settings, including physicians� offices, clinics, emergency departments, and hospitals, can provide multiple opportunities for patients and reinforce messages across contexts and care environments.
Weight Loss Programs
Implementation of clinical interventions, including screening, counseling, and referral, has major challenges. Since 2011, Medicare has covered behavioral counseling sessions for weight loss in primary care settings. However, the benefit has not been widely utilized.7�Whether the lack of utilization is a consequence of lack of clinician or patient knowledge or for other reasons remains uncertain. Few medical schools and residency programs provide adequate training in prevention and management of obesity or in understanding how to make referrals to such services. Obesity is a highly stigmatized condition; many clinicians find it difficult to initiate a conversation about obesity with patients, and some may inadvertently use alienating language when they do. Studies indicate that patients with obesity prefer the use of terms such as�unhealthy weight�or�increased BMI�rather than�overweight�or�obesity�and�improved nutrition and physical activity�rather than�diet and exercise.8�However, it is unknown if switching to these terms will lead to more effective behavioral counseling. Effective clinical decision support tools to measure BMI and guide physicians through referral and counseling interventions can provide clinicians needed support within the patient-clinician encounter. Inclusion of recently developed competencies for prevention and management of obesity into the curricula of health care professionals may improve their ability to deliver effective care. Because few primary care clinicians are trained in behavior change strategies like cognitive behavioral therapy or motivational interviewing, other trained health care professionals, such as nurses, pharmacists, psychologists, and dietitians could assist by providing counseling and appropriate referrals and help people manage their own health.
Achieving sustainable weight loss requires comprehensive strategies that support patients� efforts to make significant lifestyle changes. The availability of clinical and community programs and services to which to refer patients is critically important. Although such programs are available in some communities, there are gaps in availability. Furthermore, even when these programs are available, enhancing linkages between clinical and community care could improve patients� access. Linking community obesity prevention, weight management, and physical activity programs with clinical services can connect people to valuable prevention and intervention resources in the communities where they live, work, and play. Such linkages can give individuals the encouragement they need for the lifestyle changes that maintain or improve their health.
The high prevalence of overweight and obesity in the United States will continue to contribute to increases in health consequences related to obesity, including cancer. Nonetheless, cancer is not inevitable; it is possible that many cancers related to overweight and obesity could be prevented, and physicians have an important responsibility in educating patients and supporting patients� efforts to lead healthy lifestyles. It is important for all health care professionals to emphasize that along with quitting or avoiding tobacco, achieving and maintaining a healthy weight are also important for reducing the risk of cancer.
Corresponding Author:�Greta M. Massetti, PhD, Centers for Disease Control and Prevention, 4770 Buford Hwy NE, Atlanta, GA 30341 ([email protected]).
Conflict of Interest Disclosures:�All authors have completed and submitted the ICMJE Form for Disclosure of Potential Conflict of Interest. Dr Dietz reports receipt of scientific advisory board fees from Weight Watchers and consulting fees from RTI. No other disclosures were reported.
Disclaimer:�The findings and conclusions in this report are those of the authors and not necessarily the official position of the Centers for Disease Control and Prevention.
References
1. Lauby-Secretan B, Scoccianti C, Loomis D, Grosse Y, Bianchini F, Straif K; International Agency for Research on Cancer Handbook Working Group. Body fatness and cancer�viewpoint of the IARC Working Group. N Engl J Med. 2016;375(8):794-798. PubMedArticle
2. Zheng Y, Manson JE, Yuan C, et al. Associations of weight gain from early to middle adulthood with major health outcomes later in life. JAMA. 2017;318(3):255-269. PubMedArticle
4. Byers T, Sedjo RL. Does intentional weight loss reduce cancer risk? Diabetes Obes Metab. 2011;13(12):1063-1072. PubMedArticle
5. Grossman DC, Bibbins-Domingo K, Curry SJ, et al; US Preventive Services Task Force. Screening for obesity in children and adolescents: US Preventive Services Task Force recommendation statement. JAMA. 2017;317(23):2417-2426. PubMedArticle
7. Batsis JA, Bynum JPW. Uptake of the centers for Medicare and Medicaid obesity benefit: 2012-2013. Obesity (Silver Spring). 2016;24(9):1983-1988. PubMedArticle
8. Puhl R, Peterson JL, Luedicke J. Motivating or stigmatizing? public perceptions of weight-related language used by health providers. Int J Obes (Lond). 2013;37(4):612-619. PubMedArticle
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine


 Anabolic-Androgenic Steroids
Anabolic-Androgenic Steroids Anabolic-androgenic steroids (AAS) are testosterone derivatives that exert anabolic (tissue building) and androgenic (masculinizing) influences on the body.3 Since the discovery of the chemical structure of testosterone in 1935, attempts to separate the anabolic and androgenic effects of AAS�have been unsuccessful.3 Athletes have been using AAS since the 1940s in efforts to improve their performance.2 Concerned with widespread abuse of AAS among athletes, the IOC banned AAS use in the early 1960s.2 The Anabolic Steroids Control Act was legalized in 1990, making it a felony to possess or distribute AAS for non-medical purposes in the United States.3,4 Oral, parenteral, transdermal, and intra-nasal forms of AAS are available. The vast majority of AAS used by athletes is thought to be obtained on the �black market,� as only an estimated 10% to 15% of AAS used by athletes for performance enhancement are obtained by prescription.3
Anabolic-androgenic steroids (AAS) are testosterone derivatives that exert anabolic (tissue building) and androgenic (masculinizing) influences on the body.3 Since the discovery of the chemical structure of testosterone in 1935, attempts to separate the anabolic and androgenic effects of AAS�have been unsuccessful.3 Athletes have been using AAS since the 1940s in efforts to improve their performance.2 Concerned with widespread abuse of AAS among athletes, the IOC banned AAS use in the early 1960s.2 The Anabolic Steroids Control Act was legalized in 1990, making it a felony to possess or distribute AAS for non-medical purposes in the United States.3,4 Oral, parenteral, transdermal, and intra-nasal forms of AAS are available. The vast majority of AAS used by athletes is thought to be obtained on the �black market,� as only an estimated 10% to 15% of AAS used by athletes for performance enhancement are obtained by prescription.3 Dehydroepiandrosterone (DHEA) is a precursor to testos- terone produced primarily in the adrenal glands.4,14 Natural sources of DHEA include wild yams. The FDA banned sale of DHEA in 1996 due to insuf cient evidence of safety and value; however, DHEA remains a legal and popular item sold as a nutritional supplement.14,15
Dehydroepiandrosterone (DHEA) is a precursor to testos- terone produced primarily in the adrenal glands.4,14 Natural sources of DHEA include wild yams. The FDA banned sale of DHEA in 1996 due to insuf cient evidence of safety and value; however, DHEA remains a legal and popular item sold as a nutritional supplement.14,15 Androstenedione is a testosterone pre-cursor produced in the adrenal glands and gonads. Several professional athletes have used this substance, bringing it to national attention.2 Androstenedione is found naturally in the pollen of Scottish pine trees.19
Androstenedione is a testosterone pre-cursor produced in the adrenal glands and gonads. Several professional athletes have used this substance, bringing it to national attention.2 Androstenedione is found naturally in the pollen of Scottish pine trees.19 The increased visibility of ergogenic aids in the last de- cade has occurred primarily because of the passage of the United States Dietary Supplement Health and Education Act (DSHEA) of 1994.22 Certain vitamins, minerals, amino acids, herbs, and other botanical preparations can be classified as a �dietary supplement� under the DSHEA guidelines. Dietary supplements, as a result of DSHEA, are no longer under the direct regulatory control of the FDA. In fact, substances sold as a dietary supplement do not require FDA evaluation for safety or efficacy, and do not have to meet quality control standards expected of approved drugs.5 The content and purity of dietary supplements are not regulated and can vary widely.5,23 Since androstenedione and DHEA have been found to occur naturally in plant sources, these testosterone precursors can be labeled as �dietary supplements� and sold legally over-the-counter.
The increased visibility of ergogenic aids in the last de- cade has occurred primarily because of the passage of the United States Dietary Supplement Health and Education Act (DSHEA) of 1994.22 Certain vitamins, minerals, amino acids, herbs, and other botanical preparations can be classified as a �dietary supplement� under the DSHEA guidelines. Dietary supplements, as a result of DSHEA, are no longer under the direct regulatory control of the FDA. In fact, substances sold as a dietary supplement do not require FDA evaluation for safety or efficacy, and do not have to meet quality control standards expected of approved drugs.5 The content and purity of dietary supplements are not regulated and can vary widely.5,23 Since androstenedione and DHEA have been found to occur naturally in plant sources, these testosterone precursors can be labeled as �dietary supplements� and sold legally over-the-counter. Dietary supplements containing Chinese ephedra, also known as Mahaung, are marketed as performance enhancers and weight-loss aids.24 Ephedra species of herb have been used for over 5,000 years for respiratory ailments.25 Currently, ephedrine alkaloids are found in hundreds of prescriptions and over-the-counter products, such as antihistamines, decongestants, and appetite suppressants.24-26 Ephedra and related ephedrine alkaloids are sympathomimetic agents that�mimic epinephrine effects.
Dietary supplements containing Chinese ephedra, also known as Mahaung, are marketed as performance enhancers and weight-loss aids.24 Ephedra species of herb have been used for over 5,000 years for respiratory ailments.25 Currently, ephedrine alkaloids are found in hundreds of prescriptions and over-the-counter products, such as antihistamines, decongestants, and appetite suppressants.24-26 Ephedra and related ephedrine alkaloids are sympathomimetic agents that�mimic epinephrine effects. Creatine use in athletes has grown as a result of a 1992 study that showed that creatine supplementation produced a 20% increase in skeletal muscle creatine concentration.2,35 In the phosphorylated form, creatine serves as an energy substrate that contributes to adenosine triphosphate (ATP) re-synthesis during high-intensity exercise.36 Creatine re- mains popular with power and resistance athletes as it is thought to produce increases in strength, muscle mass, and to delay fatigue.2,14,36
Creatine use in athletes has grown as a result of a 1992 study that showed that creatine supplementation produced a 20% increase in skeletal muscle creatine concentration.2,35 In the phosphorylated form, creatine serves as an energy substrate that contributes to adenosine triphosphate (ATP) re-synthesis during high-intensity exercise.36 Creatine re- mains popular with power and resistance athletes as it is thought to produce increases in strength, muscle mass, and to delay fatigue.2,14,36 Human growth hormone (hGH) is a polypeptide produced in the anterior pituitary gland. After its release from the pituitary, hGH can exert its effect in all cells of the body via tissue specific receptors. Human growth hormone is shown to promote protein anabolism, carbohydrate tolerance, lipolysis, natriuresis, and bone and connective tissue turnover.4,50
Human growth hormone (hGH) is a polypeptide produced in the anterior pituitary gland. After its release from the pituitary, hGH can exert its effect in all cells of the body via tissue specific receptors. Human growth hormone is shown to promote protein anabolism, carbohydrate tolerance, lipolysis, natriuresis, and bone and connective tissue turnover.4,50 Recombinant EPO (r-EPO) was approved by the FDA for manufacture in 1989 after the EPO gene was cloned in 1985.14 Since its approval, r-EPO has been abused for athletic personal gain as an alternative to blood doping.3,14 Recombinant EPO has largely replaced the practice of blood doping, as r-EPO produces a dose-dependent increase in hematocrit.2 In theory, r-EPO should provide all of the benefits of blood doping without the risks involved in blood transfusion.3
Recombinant EPO (r-EPO) was approved by the FDA for manufacture in 1989 after the EPO gene was cloned in 1985.14 Since its approval, r-EPO has been abused for athletic personal gain as an alternative to blood doping.3,14 Recombinant EPO has largely replaced the practice of blood doping, as r-EPO produces a dose-dependent increase in hematocrit.2 In theory, r-EPO should provide all of the benefits of blood doping without the risks involved in blood transfusion.3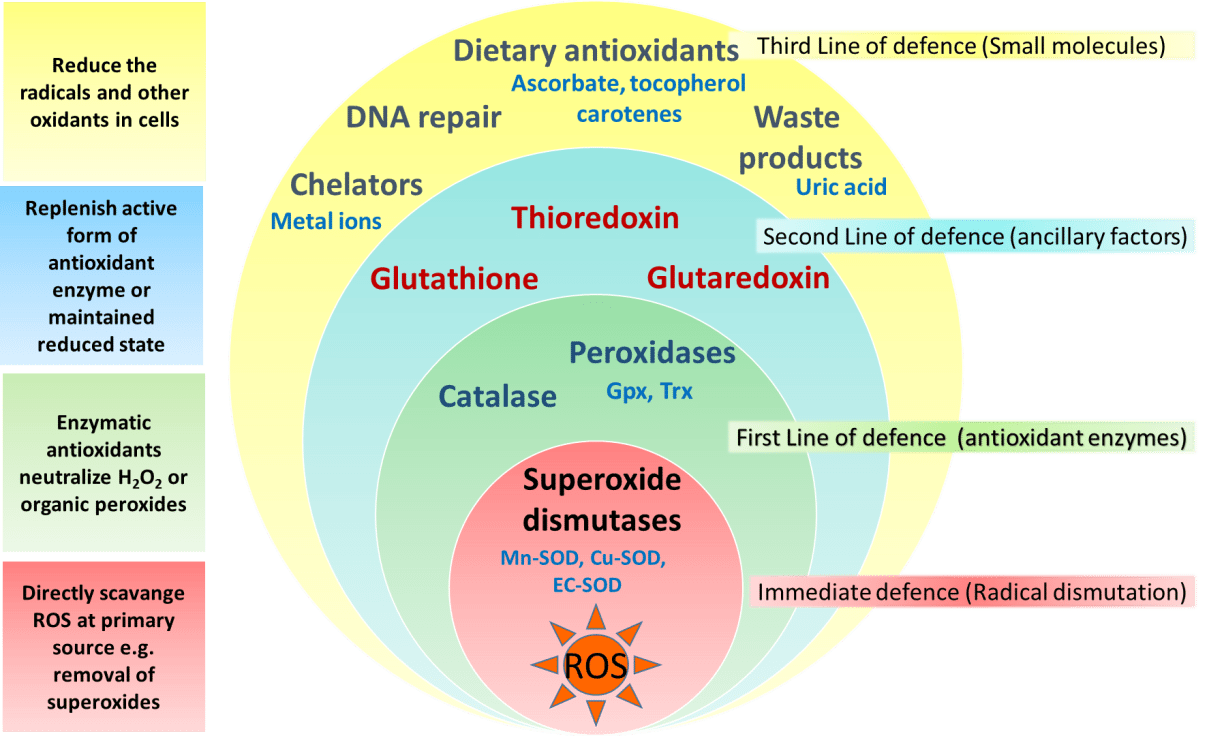 The antioxidant capabilities of certain vitamins are believed by many to counter-act the production of free-radials that occurs during exercise.14 Most of the research to date involves vitamin E, vitamin C, and beta carotene.2 The existing literature does not support the notion that antioxidants have significant ergogenic capabilities.2,14,57 There are currently no recommendations for antioxidant use in athletes that exceeds the normal adult recommended daily allowance (RDA).
The antioxidant capabilities of certain vitamins are believed by many to counter-act the production of free-radials that occurs during exercise.14 Most of the research to date involves vitamin E, vitamin C, and beta carotene.2 The existing literature does not support the notion that antioxidants have significant ergogenic capabilities.2,14,57 There are currently no recommendations for antioxidant use in athletes that exceeds the normal adult recommended daily allowance (RDA). Beta-hydroxy-beta-methylbutyrate (HMB) is a metabolite of the branched-chain amino acid leucine. HMB is theorized to inhibit muscle breakdown during strenuous exercise but its exact mechanism of action remains unknown.14,58 Studies show that HMB supplementation may significantly lower serum lactate dehydrogenase (LDH), lower serum creatine phosphokinase (CPK) levels and delay blood lactate accumulation after endurance training compared to placebo.59,60 Furthermore, short-term HMB use has been shown to significantly increase strength gains with resistance-exercised training over placebo in one double-blinded study.61
Beta-hydroxy-beta-methylbutyrate (HMB) is a metabolite of the branched-chain amino acid leucine. HMB is theorized to inhibit muscle breakdown during strenuous exercise but its exact mechanism of action remains unknown.14,58 Studies show that HMB supplementation may significantly lower serum lactate dehydrogenase (LDH), lower serum creatine phosphokinase (CPK) levels and delay blood lactate accumulation after endurance training compared to placebo.59,60 Furthermore, short-term HMB use has been shown to significantly increase strength gains with resistance-exercised training over placebo in one double-blinded study.61 Caffeine is a methylxanthine occurring naturally in many species of plants. Caffeine is thought to work through a variety of mechanisms. The central nervous system effect of caffeine is probably the result of adrenergic receptor antagonism.3 Its use by athletes stems from the theory that caffeine may delay fatigue by enhancing skeletal muscle contractility and spare muscle glycogen levels by enhancing fat metabolism.6 Multiple studies have reported an improved endurance time with caffeine use.6,62,63 There is evidence that caffeine use may enhance performance with more intense short-duration exercise as well.2 The caffeine dosages most associated with an ergogenic effect range in the literature from 3 to 9 mg per kilogram of body weight.2,6
Caffeine is a methylxanthine occurring naturally in many species of plants. Caffeine is thought to work through a variety of mechanisms. The central nervous system effect of caffeine is probably the result of adrenergic receptor antagonism.3 Its use by athletes stems from the theory that caffeine may delay fatigue by enhancing skeletal muscle contractility and spare muscle glycogen levels by enhancing fat metabolism.6 Multiple studies have reported an improved endurance time with caffeine use.6,62,63 There is evidence that caffeine use may enhance performance with more intense short-duration exercise as well.2 The caffeine dosages most associated with an ergogenic effect range in the literature from 3 to 9 mg per kilogram of body weight.2,6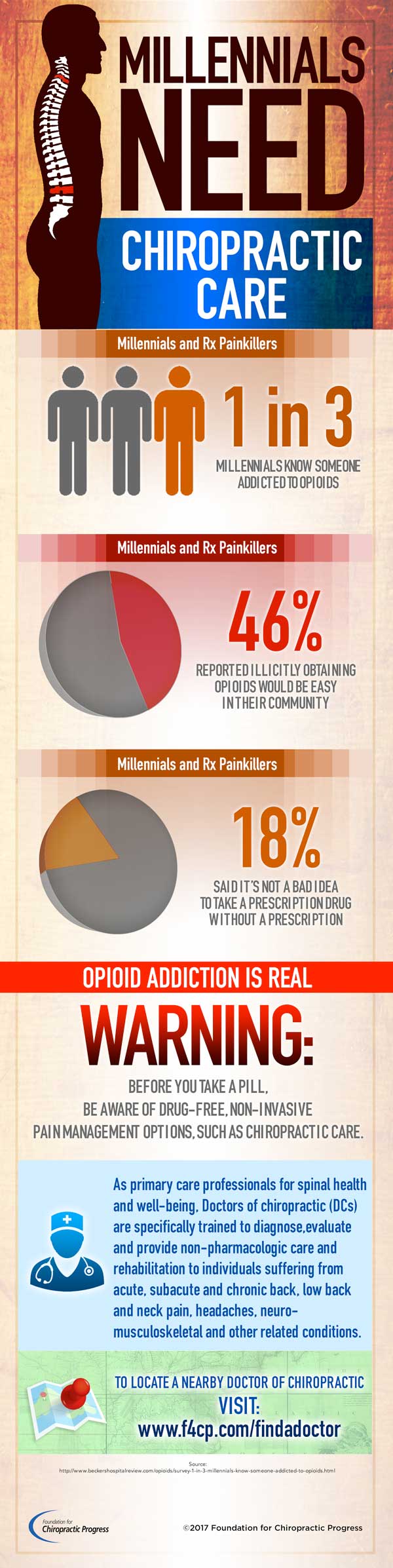

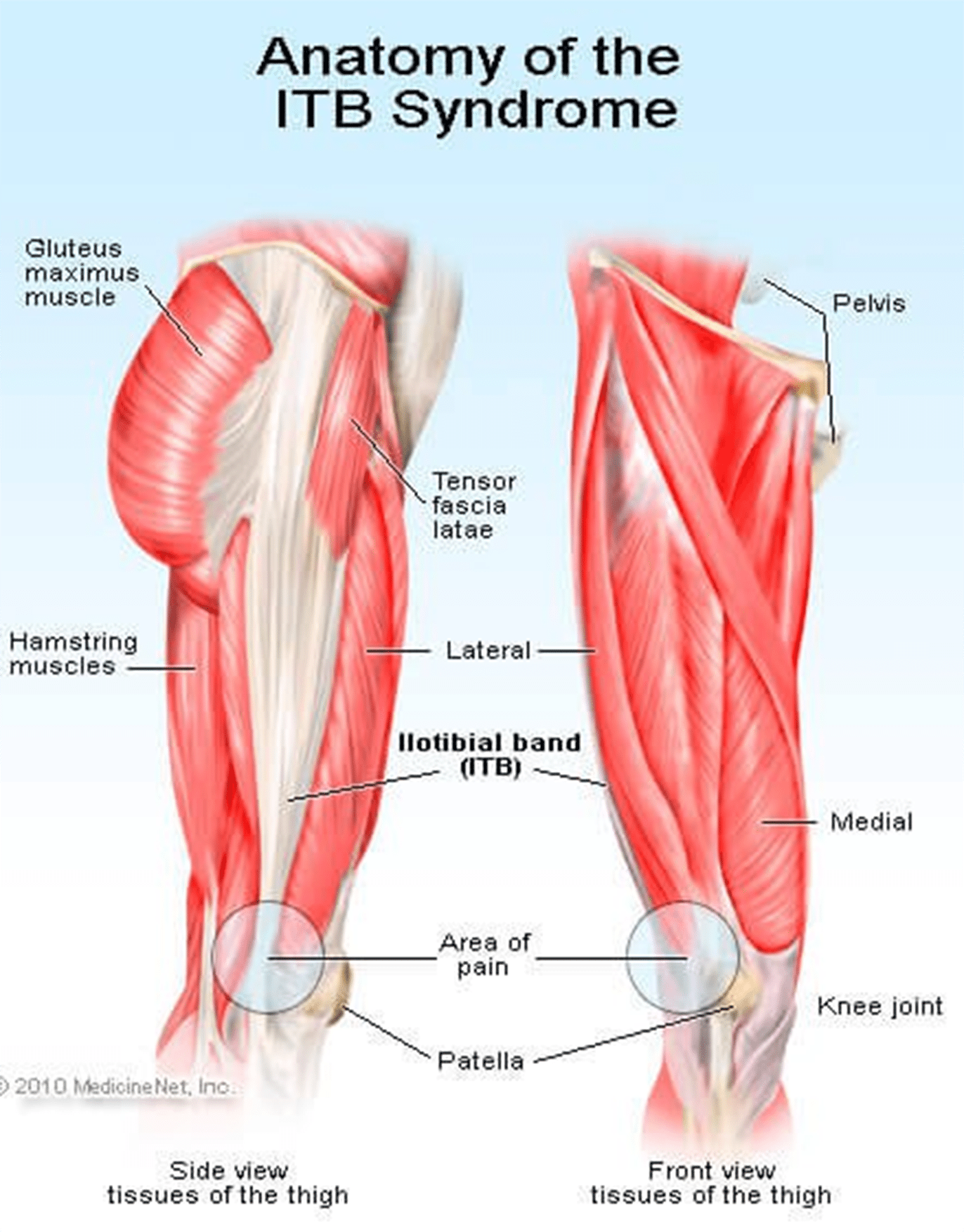 Signs Of IT Band Syndrome
Signs Of IT Band Syndrome If you are a runner, you will be able to distinguish ITBS by:
If you are a runner, you will be able to distinguish ITBS by: If you want to do away with pain, you might consider looking for a fit pair of shoes as they will reduce any pain, causing issues in the long run. Pay attention to small specifics like shoes that offer enough heel space, sufficient toe box room, and enough space for wide feet. Your toes should be able to move freely without being constricted.
If you want to do away with pain, you might consider looking for a fit pair of shoes as they will reduce any pain, causing issues in the long run. Pay attention to small specifics like shoes that offer enough heel space, sufficient toe box room, and enough space for wide feet. Your toes should be able to move freely without being constricted. This upgraded version is lightweight to help with any knee problems. It offers you comfort through cushioning that help absorb shock as you run as well as other features like grip, fit, and durability. The shoe has an added outer sole to ensure it lasts you as long as possible.
This upgraded version is lightweight to help with any knee problems. It offers you comfort through cushioning that help absorb shock as you run as well as other features like grip, fit, and durability. The shoe has an added outer sole to ensure it lasts you as long as possible. It tops the list of 5 best running shoes. Also, it has remained the first choice for most runners with knee pain issues. This pair offers all the above functionalities too, making it your best choice.
It tops the list of 5 best running shoes. Also, it has remained the first choice for most runners with knee pain issues. This pair offers all the above functionalities too, making it your best choice. Puma models have never disappointed, and this one is no exception. Puma Faas 600 is the solution to your knee pain. It is also an affordable option for the short-handed.
Puma models have never disappointed, and this one is no exception. Puma Faas 600 is the solution to your knee pain. It is also an affordable option for the short-handed. This is another great choice on the list. It is one of the New Balance Fresh Foam Series. Its midsole offers you the required support coupled with comfort to eliminate knee pains.
This is another great choice on the list. It is one of the New Balance Fresh Foam Series. Its midsole offers you the required support coupled with comfort to eliminate knee pains. This is the 16th edition of the Saucony Hurricane, which offers a combination of steadiness and protection. Those with knee pain have agreed with the stability offered by this shoe. It is also cushioned to help you go for long runs without any pain or injury. It is perfect for heavy runners and those who are out of shape due to inactivity.
This is the 16th edition of the Saucony Hurricane, which offers a combination of steadiness and protection. Those with knee pain have agreed with the stability offered by this shoe. It is also cushioned to help you go for long runs without any pain or injury. It is perfect for heavy runners and those who are out of shape due to inactivity.








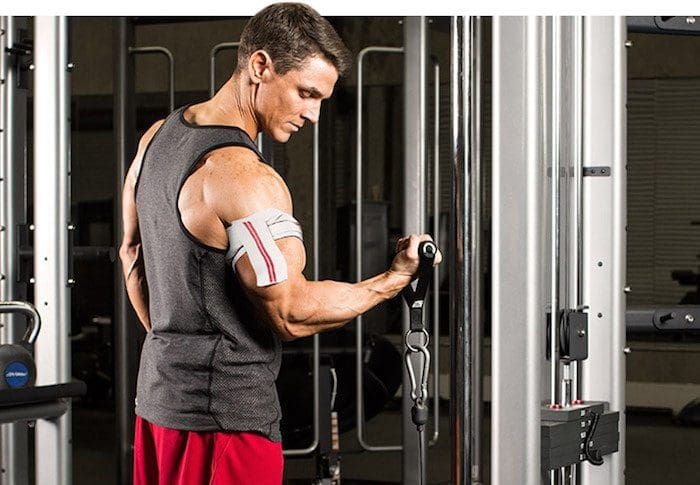


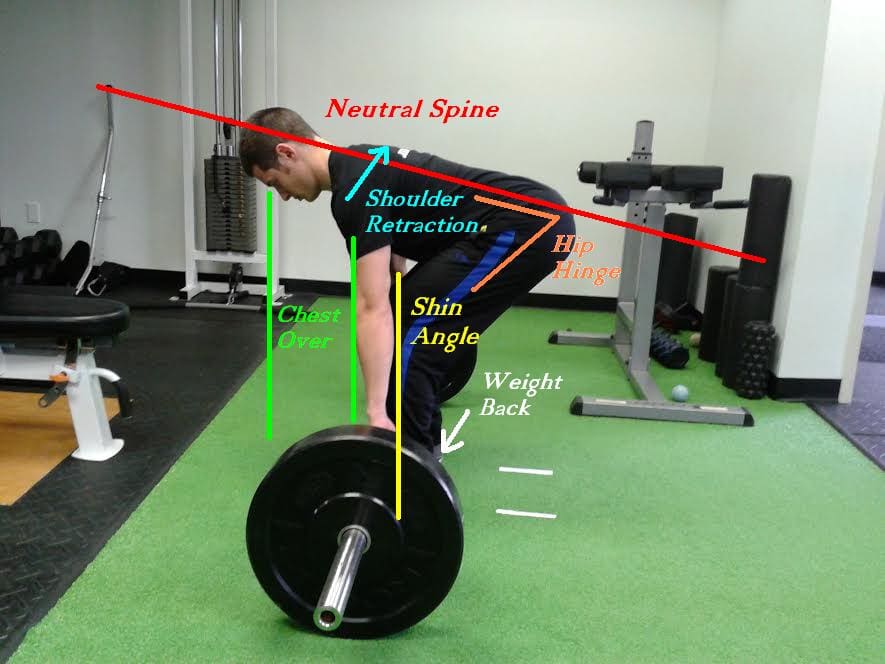

 Any muscle constantly used has to have an opportunity to recover. This recovery can be natural with time, or could be facilitated and sped up with treatment. Continuing use will make it even worse since the muscle is tightening due to overuse. This injured muscle needs to relax and have blood flow encouraged into it for a rapid recovery. The tightness� lessens the normal blood flow going to the muscle. To encourage new blood into the muscle is the way of getting the muscle to begin to unwind and operate normally. Massages daily to this area is greatly supported.
Any muscle constantly used has to have an opportunity to recover. This recovery can be natural with time, or could be facilitated and sped up with treatment. Continuing use will make it even worse since the muscle is tightening due to overuse. This injured muscle needs to relax and have blood flow encouraged into it for a rapid recovery. The tightness� lessens the normal blood flow going to the muscle. To encourage new blood into the muscle is the way of getting the muscle to begin to unwind and operate normally. Massages daily to this area is greatly supported.
 The prevalence of obesity in the United States has been increasing for almost 50 years. Currently, more than two-thirds of adults and almost one-third of children and adolescents are
The prevalence of obesity in the United States has been increasing for almost 50 years. Currently, more than two-thirds of adults and almost one-third of children and adolescents are 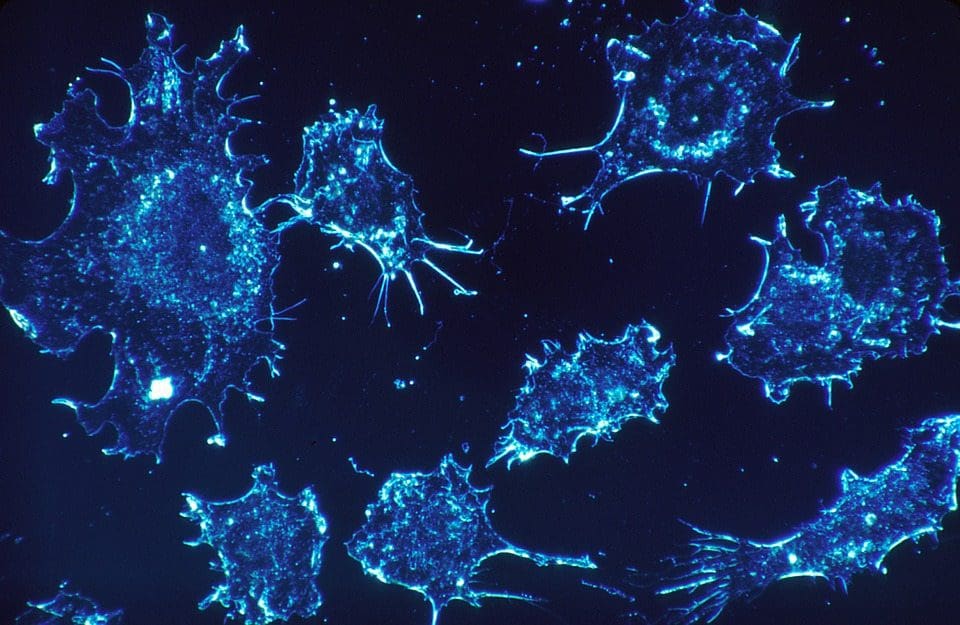
 From 2005 to 2014, there was a 1.4% annual increase in cancers related to overweight and obesity among individuals aged 20 to 49 years and a 0.4% increase in these cancers among individuals aged 50 to 64 years. For example, if cancer rates had stayed the same in 2014 as they were in 2005, there would have been 43?000 fewer cases of colorectal cancer but 33?000 more cases of other cancers related to overweight and obesity. Nearly half of all cancers in people younger than 65 years were associated with overweight and obesity. Overweight and obesity among younger people may exact a toll on individuals� health earlier in their lifetimes.
From 2005 to 2014, there was a 1.4% annual increase in cancers related to overweight and obesity among individuals aged 20 to 49 years and a 0.4% increase in these cancers among individuals aged 50 to 64 years. For example, if cancer rates had stayed the same in 2014 as they were in 2005, there would have been 43?000 fewer cases of colorectal cancer but 33?000 more cases of other cancers related to overweight and obesity. Nearly half of all cancers in people younger than 65 years were associated with overweight and obesity. Overweight and obesity among younger people may exact a toll on individuals� health earlier in their lifetimes.
 The
The  Implementation of clinical interventions, including screening, counseling, and referral, has major challenges. Since 2011, Medicare has covered behavioral counseling sessions for weight loss in primary care settings. However, the benefit has not been widely utilized.
Implementation of clinical interventions, including screening, counseling, and referral, has major challenges. Since 2011, Medicare has covered behavioral counseling sessions for weight loss in primary care settings. However, the benefit has not been widely utilized. Achieving sustainable weight loss requires comprehensive strategies that support patients� efforts to make significant lifestyle changes. The availability of clinical and community programs and services to which to refer patients is critically important. Although such programs are available in some communities, there are gaps in availability. Furthermore, even when these programs are available, enhancing linkages between clinical and community care could improve patients� access. Linking community obesity prevention, weight management, and physical activity programs with clinical services can connect people to valuable prevention and intervention resources in the communities where they live, work, and play. Such linkages can give individuals the encouragement they need for the lifestyle changes that maintain or improve their health.
Achieving sustainable weight loss requires comprehensive strategies that support patients� efforts to make significant lifestyle changes. The availability of clinical and community programs and services to which to refer patients is critically important. Although such programs are available in some communities, there are gaps in availability. Furthermore, even when these programs are available, enhancing linkages between clinical and community care could improve patients� access. Linking community obesity prevention, weight management, and physical activity programs with clinical services can connect people to valuable prevention and intervention resources in the communities where they live, work, and play. Such linkages can give individuals the encouragement they need for the lifestyle changes that maintain or improve their health. The high prevalence of overweight and obesity in the United States will continue to contribute to increases in health consequences related to obesity, including cancer. Nonetheless, cancer is not inevitable; it is possible that many cancers related to overweight and obesity could be prevented, and physicians have an important responsibility in educating patients and supporting patients� efforts to lead healthy lifestyles. It is important for all health care professionals to emphasize that along with quitting or avoiding tobacco, achieving and maintaining a healthy weight are also important for reducing the risk of cancer.
The high prevalence of overweight and obesity in the United States will continue to contribute to increases in health consequences related to obesity, including cancer. Nonetheless, cancer is not inevitable; it is possible that many cancers related to overweight and obesity could be prevented, and physicians have an important responsibility in educating patients and supporting patients� efforts to lead healthy lifestyles. It is important for all health care professionals to emphasize that along with quitting or avoiding tobacco, achieving and maintaining a healthy weight are also important for reducing the risk of cancer.





