Sciatica is described as a series of intense and painful symptoms in one or both legs along the course of the sciatic nerve. The pain is generally felt at the back of the leg and runs from the buttocks down the back of the thigh into the calf and foot. The pain may begin suddenly or start gradually, and is typically distinguished by a sharp, shooting, or electric shock-like in quality. Movement of the lower extremities often worsens the symptoms. Pain may be uniformly spread along the leg, but there are certain areas where pain may be more intense. Also,� pain is frequently associated with numbness and/or tingling sensations along the sciatic nerve.
Sciatica can result from any health issue that causes pressure or irritation of the nerve roots that compromise the sciatic nerve. This pressure may result from a variety of injuries and/or aggravated conditions, such as a ruptured intervertebral disc, narrowing of the bony spinal canal, medically referred to as spinal stenosis, or infrequently from infection or tumor. The sciatic nerve is the longest and largest nerve in the body; it measures three-quarters of an inch in diameter and it originates from the sacral plexus; a network of nerves found in the low back, or the lumbosacral spine. The lumbosacral spine refers to the lumbar spine and the sacrum combined. The sciatic nerve and its associated nerves allow movement and enable feeling, known as motor and sensory functions, in the thigh, knee, calf, ankle, foot, and toes.
Contents
About the Sciatic Nerve
The sciatic nerve begins in your low back, which is known as the lumbar spine. The nerve roots are in the L4 and L5 vertebrae (the ‘L’ means lumbar, as well as the numbers indicate the degree of the vertebra found along the spine). The sciatic nerve also travels throughout your pelvic area, or the sacrum. In most individuals, the sciatic nerve runs beneath the piriformis muscle, which functions by moving your thigh from side to side. From there, the sciatic nerve descends through the buttocks and the back of your thighs. Behind your knee, smaller nerves branch out from the sciatic nerve and journey down to your toes.
Your sciatic nerve is a part of an intricate arrangement of the human body’s nervous system. The nervous system is responsible for transmitting pain and feelings, as well as other sensations, to other parts of the body. Therefore, when an injury and/or a condition presses on a nerve, you are going to feel it, and many of the times it won’t feel great. With sciatica, a health issue on your low back, such as a herniated disc, for instance, permeates the sciatic nerve, which then transmits pain down your legs.
The sciatic nerve exits the sacrum in the pelvic area of the body through a nerve passageway called the sciatic foramen. At the top part of the sciatic nerve, two branches form; the articular and muscular branches. The articular branch goes to the hip joint. The muscular branch serves the leg flexor muscles, which are the muscles that enable movement. Other complicated nerve structures are also involved, both the peroneal nerves and the tibial nerves. The peroneal nerves originate from the nerve roots in the fourth and fifth vertebrae of the lumbar spine (L4-L5) and first and second levels of the sacrum (S1-2). When the peroneal nerves leave the pelvis, they move down the front and side of the leg and along the outer side of the knee to the foot.
The tibial nerves originate from the nerve roots in L4-5 and S1-3. The tibial nerves move in the front of the knee and then back into the foot, through the heel, sole and toes. In case your sciatic nerve is compressed or irritated, it can cause pain along these pathways; this is how sciatic pain can “spread” or radiate to some of the other parts of the body.
Common Questions and Answers of Sciatica
What is causing my pain? Your sciatic nerve pain, or sciatica, may be commonly caused by but not limited to a bulging disc or a herniated disc, degenerative disc disease, piriformis syndrome, pregnancy, spinal stenosis, a spinal tumor or other spinal illness, spondylolisthesis, or due to trauma from a injury. Any one of those conditions, among others, can put pressure on the sciatic nerve or related nerve roots in your low back. That stress is what causes your pain and other symptoms.
Will I need surgery? Most patients with lumbar radiculopathy respond positively to non-surgical treatments, such as chiropractic care, therefore, spine surgery for sciatica symptoms is seldom needed to treat it. However, there are situations when you might want to check with your healthcare professional about considering spinal surgery, particularly if:
You have bowel or bladder dysfunction. This is rare, but it might happen with spinal cord compression.
You have spinal stenosis, and your doctor believes that surgery is your best way to take care of it.
You are having other neurologic dysfunctions, such as intense or severe leg weakness.
Your symptoms become severe and/or non-invasive treatments are no longer effective.
What types of surgery are used for lumbar radiculopathy? Two frequent spinal surgeries for sciatica are:
Discectomy or microdiscectomy: In both these procedures, the surgeon removes part or all of a herniated disc that is pushing in your sciatic nerve and causing the symptoms. The distinction between the processes is that a microdiscectomy is a minimally invasive operation. The surgeon uses microscopic magnification to operate through a really small incision with very tiny instruments. Because the surgery is minimally invasive, you should recover more quickly from a microdiscectomy.
Laminectomy or laminotomy: These processes both involve a part of the spine known as the lamina, a bony plate that protects the spinal canal and spinal cord. A laminectomy involves the removal of the whole lamina; a laminotomy removes only a section of the lamina. These processes can produce more space for the nerves, therefore reducing the likelihood of the nerves being compressed or pinched.
Can I utilize over-the-counter drugs and/or medications to deal with my pain? Over-the-counter non-steroidal anti-inflammatory drugs, or NSAIDs, can help reduce swelling and inflammation while relieving your pain. You and your doctor have plenty to choose from. You may use acetaminophen (eg, Tylenol), ibuprofen (eg, Advil), or naproxen (eg, Aleve). However, the use of drugs and/or medications only temporarily relieves the symptoms of sciatica without treating the source of the pain. Make sure to talk to a healthcare professional regarding the utilization of these and continue to seek the most appropriate treatment for your sciatic nerve pain, such as chiropractic care.
How Chiropractic Can Help Treat Sciatica
Sciatica is a frequent issue for a lot of people that is identified by pain that begins in the lower back or buttocks, then radiates into one or both legs. It may vary in terms of frequency and severity, but it may often be constant.
The pain from sciatica can often be severe, and in addition, it can be very sharp. It may be associated with tingling sensations, burning, or numbness and weakness. What people may not realize is that it’s a collection of symptoms, an indication that something isn’t right, rather than a single type of injury and/or condition itself. The problem which leads to pain is generally a misalignment, or subluxation, of the lumbar spine. The sciatic nerve begins in the lower back and extends to the lower leg. That is why the pain may often be felt everywhere along the sciatic nerve.
A chiropractor commonly treats patients with symptoms of sciatica. Spinal adjustments and manual manipulations will aim to realign the spine, taking the pressure from the sciatic nerve and often bringing immediate relief. When the stress is off, the body can begin to heal itself. While spinal adjustments and manual manipulations are probably most frequently used, other treatments may be provided, particularly if common chiropractic care may not be advisable. Other treatment modalities might include using ultrasound, a TENS, or transcutaneous electrical nerve stimulation, device, or ice therapy. Ultrasound warms the region and increases circulation, which can lessen the swelling and muscular tension. A TENS device brings relief using a minor electric current to relax muscle spasms and also to increase endorphins. Furthermore, physical therapy, massage and or a series of stretches and/or exercises, may also help improve sciatica.
Dr. Alex Jimenez’s Insight
Chiropractic care is a popular, alternative treatment option commonly utilized to help treat symptoms of sciatica. Sciatica is characterized as a collection of symptoms, rather than a single injury or condition. A chiropractor can help diagnose the source of a patient’s sciatic nerve pain, or sciatica, in order to properly determine the best treatment for their specific health issue. Spinal adjustments and manual manipulations can be utilized to help carefully correct the alignment of the spine, restoring the natural integrity of the spine and allowing the body to heal itself, without the need for drugs and medications or surgery.
In certain individuals, sciatica may fix itself, possibly happening just once or a few times throughout their lifetime. But, it’s important to remember that if an injury and/or aggravated condition is not treated effectively, symptoms may worsen. A chiropractor can help provide relief from your sciatic nerve pain. Physical activity will most likely be recommended to strengthen the muscles in the back to help prevent sciatica as well as to speed up the recovery process. The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Sciatica
Sciatica is medically referred to as a collection of symptoms, rather than a single injury and/or condition. Symptoms of sciatic nerve pain, or sciatica, can vary in frequency and intensity, however, it is most commonly described as a sudden, sharp (knife-like) or electrical pain that radiates from the low back down the buttocks, hips, thighs and legs into the foot. Other symptoms of sciatica may include, tingling or burning sensations, numbness and weakness along the length of the sciatic nerve. Sciatica most frequently affects individuals between the ages of 30 and 50 years. It may often develop as a result of the degeneration of the spine due to age, however, the compression and irritation of the sciatic nerve caused by a bulging or herniated disc, among other spinal health issues, may also cause sciatic nerve pain.
Sciatica is a condition characterized by painful symptoms, often originating from the lower back all the way down to the toes. Sciatica is brought on by the irritation of the sciatic nerve. The sciatic nerve begins around the lumbar spine and runs down to the feet. Sciatica can be caused by the irritation of the sciatic nerve anywhere along its length. But the most frequent cause of sciatica is irritation to the sciatic nerve either in the lower back or in the gluteal region caused by poor posture.
Sciatica generally presents itself as a very specific collection of symptoms. If you can’t pin-point exactly where your pain is (i.e. if the entire leg just aches or if your symptoms are quite vague), it’s unlikely that you have sciatica. Sciatica typically runs as a band of pain through the low back and the buttocks, and also down the hamstring, occasionally traveling as low as the calf muscle and even the feet and toes. If you experience a sensation similar to pins and needles and/or numbness, the severity of your sciatica is much worse than if you just have pain.
Contents
Poor Posture Reasons For Sciatica
Poor workplace ergonomics can be a significant contributing aspect to the development of sciatica. Further, if you already have sciatica, inadequate workstation ergonomics is very likely to make it worse. A leading ergonomic issue in regard to sciatica is increased back pain that’s brought on by poor posture while sitting and standing. It you embrace a slouched or slumped position, or you lean forward at your desk, you place a tremendous amount of strain on your lumbar spine. This can result in your lower back muscles going into spasm. The sciatic nerve has to operate through those muscles. If they are spasmodic, there is a heightened likelihood that the sciatic nerve will end up irritated and develop symptoms of sciatica.
Sitting for extended periods of time is just another issue, for two reasons:
First, in sitting, your bodyweight is transferred from your upper body to your pelvis, throughout the lumbar spine. This implies that there is a continuous, and dull, compressive force going through the lower spine. Over time, this may result in irritation to the nerves as they leave the spinal cord canal. This is much more of a problem for people who have sciatica. Sciatica will frequently cause inflammation around the nerve root where it exits the spinal canal. This means there’s less “wiggle” room for the nerve to move and continuous compression may impinge this nerve, causing symptoms.
Second, the sciatic nerve runs throughout the gluteal region. Especially, it runs through a muscle called the piriformis muscle, which happens to be in about the region of your sitting bone. When you sit, you really literally sit on the piriformis muscles along with the sciatic nerve. Therefore, when you sit you’re compressing the sciatic nerve. Compression that is constant could lead to the piriformis muscle moving into spasm. Similarly to above, in the event the piriformis muscle goes into spasm, the sciatic nerve is very likely to be compacted and irritated, leading to some kind of sciatic symptoms.
Furthermore, healthcare professionals say that poor posture may cause more than just back pain and sciatica. Poor posture may actually cause a variety of health issues, according to research studies.
Effects of Poor Posture
Posture is an important part of preventing issues which range from back pain to fatigue. When the spine is properly aligned, the spine is stabilized and supported, however as you slouch or practice other methods of poor posture, your spine no longer gets the support it needs to remain balanced, leading to many health issues. The following health issues may also present themselves as a result of poor posture.
Sore Muscles
The most common effect of poor posture includes sore muscles. As you slouch, the muscles have to work harder to keep the spine protected and stabilized. The extra work on these muscles may cause muscle stiffness and fatigue. This can lead to chronic health issues with sore and tight muscles from the neck all the way down to the lower spine. Two big muscle groups which bare the brunt of these problems are the flexors and extensors of the back, which allow you to bend forward and lift objects.
Spinal Curvature
Among the most serious health issues that could happen with bad posture is developing a severe spinal curvature. As stated by the Chiropractic Resource Organization, the human spine has four natural curves which form an “s” shape. When poor posture is practiced, the spine can experience pressure, gradually influencing the spine curves to modify their positions. The spine is particularly designed to help absorb shock and keep you balanced, but as the spinal column position changes, this capacity becomes compromised.
Subluxations
Once the spinal curve is altered, one major problem that may occur are subluxations, or spinal misalignments. Vertebral subluxations occurs when a vertebrae becomes misaligneds from the rest of the spine. This also affects the total integrity of the remaining spine. These misalignments can eventually lead to chronic health issues, such as stress and aggravation of neighboring spinal nerves.
Blood Vessel Constriction
As bad posture changes the alignment of the spine, the consequent movement and subluxations can cause problems with blood vessel constriction. The constriction of the arteries across the spine can cut off blood supply to the cells of their muscles, which may influence nutrient and oxygen supply. Blood vessel constriction can also raise your chances of clot formation and issues using deep vein thrombosis.
Nerve Compression
One of the most frequent side effects of bad posture is nerve compression. As the spine changes in shape, the resulting movements or subluxations can put stress on the surrounding spinal nerves. Since the nerves which connect to the spine come from all over the body, these pinched nerves can not only cause neck and back pain but might also cause pain in other unrelated regions of the body.
In a 2013 study conducted Japan done by Kamitani et al, posture was connected to a decrease in lifespan and in activities of daily living. The study concluded that posture had a significant impact on quality of life as well as life expectancy.
Dr. Alex Jimenez’s Insight
Whether you’re slouching over your laptop, looking down at your mobile phone, bending over to pick up a box or simply sitting behind a desk for an extended amount of time, all of these regular activities can negatively affect your posture. Poor posture can not only cause back pain and symptoms of sciatica, it can manifest into a wide array of health issues if not properly corrected in time. Various research studies have even demonstrated that poor posture can affect longevity and life expectancy. Chiropractic care can help carefully restore the alignment of the spine, to recover the human body from the effects of poor posture.
Correcting Poor Posture to Improve Sciatica
The first thing that needs to be done to correct poor posture is to find a diagnosis from a healthcare professional, such as a chiropractor or physical therapist. They will be able to aid you with a treatment program and with hands-on therapy to alleviate your symptoms. Chiropractic care is a well-known, alternative treatment option which focuses on the diagnosis, treatment and prevention of a variety of injuries and/or conditions associated to the musculoskeletal and nervous system. Also, an ergonomic evaluation is a good idea. It is best practice to allow an expert to perform an ergonomic assessment for you when you’re injured, as opposed to attempting to do it yourself. This is because of the probability of making things worse when it is not done properly.
But if an ergonomic appraisal isn’t a possibility for you, consider these hints:
?Try to integrate some standing into your daily work day, to decrease the constant pressure on the sciatic nerve.
Take regular walks during your working day and consider a stretch to your gluteal area.
Make sure your workstation is set up ergonomically to prevent additional exacerbation, paying special attention to the following:
Ensure you are not leaning forwards;
Make sure that your backrest is large enough so that the lumbar support is comfortably supporting the lower spine;
Ensure your seat cushion isn’t too tough;
Ensure that your feet are well supported;
Make sure your office chair is not too low, as this promotes slouching.
One last note, sciatica may be a difficult condition to take care of. So where possible, involving a healthcare professional, such as a chiropractor, or doctor of chiropractic, is in your best interests, towards correcting your poor posture and improving symptoms of sciatica, among others.�The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Back Pain
According to statistics, approximately 80% of people will experience symptoms of back pain at least once throughout their lifetimes. Back pain is a common complaint which can result due to a variety of injuries and/or conditions. Often times, the natural degeneration of the spine with age can cause back pain. Herniated discs occur when the soft, gel-like center of an intervertebral disc pushes through a tear in its surrounding, outer ring of cartilage, compressing and irritating the nerve roots. Disc herniations most commonly occur along the lower back, or lumbar spine, but they may also occur along the cervical spine, or neck. The impingement of the nerves found in the low back due to injury and/or an aggravated condition can lead to symptoms of sciatica.
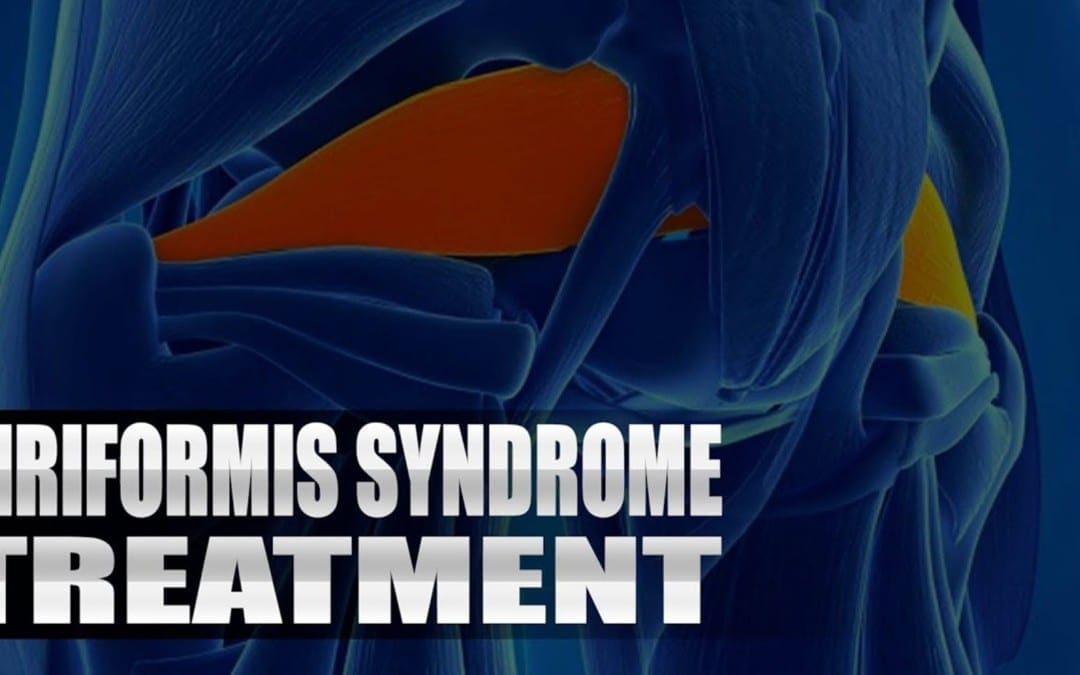
Piriformis Syndrome Treatment: Sandra Rubio defines sciatica, a collection of symptoms caused by the compression of the longest nerve in the body: the sciatic nerve. As further explained, symptoms of sciatica include, low back pain, followed by painful symptoms which radiate down the hips, buttocks, legs and feet. A lot of patients walk-in to Dr. Alex Jimenez’s office with sciatica caused by a variety of health issues. Dr. Alex Jimenez is the non-surgical choice for piriformis syndrome treatment with chiropractic care.
Piriformis Syndrome Treatment
Sciatica may feel like pain similar to an electrical sensation, or sharp. Until it goes off, the cramp can last for weeks. You might have pain, particularly when you move, sneeze, or cough. You might also have a tingling or burning sensation, numbness, pins and needles; weakness down your leg. You are likely to get sciatica between the ages of 50 and 30 years. It may happen as a consequence of the overall wear and tear of aging, and any sudden strain on the discs that cushion the bones (vertebrae) of your lower spine.
We focus on what works for you. We also strive to create fitness and better the body through researched methods and total wellness programs. These programs are natural, and use the body�s own ability to achieve goals of improvement, rather than introducing harmful chemicals, controversial hormone replacement, surgery, or addictive drugs.
We want you to live a life that is fulfilled with more energy, positive attitude, better sleep, less pain, proper body weight and educated on how to maintain this way of life. I have made a life of taking care of each and every one of my patients.
I assure you, I will only accept the best for you�
God Bless You & Your Health�?
If you have enjoyed this video and/or we have helped you in any way please feel free to subscribe and share us.
We all have learned about the importance of having good posture. From a young age, people are told time and time again that sitting tall, holding your head high and maintaining good posture is essential. Besides seeming poised and professional at all times, is having good posture significant towards our overall health and wellness?
When you keep good posture, you can reinforce the fundamental alignment of your neck and back, and you can keep your spine straight, healthy and aligned accordingly. Studies have shown that good posture can help you get more energy. If you would like to remain healthy, in reality, good posture is necessary. In summary, proper posture is a good sign of well-being. When you’ve got poor posture, it’s not just bad for your spine, it can also have catastrophic side effects as well as an impact on longevity.
Contents
Spinal Curvature Changes
One of the most prominent negative effects we have a tendency to see from poor posture is an alteration in the natural curve of the spine. Normal spinal curvature has a specific shape. Should you spend a year sitting or standing with improper posture, however, your spine is set under a lot of pressure. This is because you are placing your spine in a position that is unnatural. These changes in the spinal curve don’t just cause pain and discomfort, they might also prevent your spine from having the ability to absorb shock and maintain balance.
Poor Digestion
Studies have found that sitting all day with bad posture may affect your digestive system. Your organs are actually compressed by poor posture and leaves them incapable of functioning properly. This can slow down the digestive process and affect your metabolism, at the same time, lasting compression of the digestive organs can impair your body’s ability to consume and process food. You may wind up with life-changing metabolic issues.
Increased Risk of Cardiovascular Disease
Both an Australian research on poor posture and longevity as well as an English study on posture and sitting found that people that sit all day with bad posture have an increased likelihood of developing cardiovascular disease. You may not only experience a shorter life expectancy, but one assessment found that those who sit the majority of the day experienced a stunning 147 percent increase in cardiovascular disease.
Varicose Veins
If you sit all day with poor posture, you’re preventing your body from getting the essential circulation it needs. This can actually lead to the formation of varicose (spider) veins. This is particularly common in women.
Back Pain
If you spend enough time sitting with poor posture, you can begin to experience chronic back pain and disc degeneration, among other spinal health issues. People who maintain poor posture often experience painful symptoms without knowing the source of their health issues. These problems can often be traced back to the stress that’s been placed on the spine.
Overall, your poor posture may be doing more than simply impacting how you look. Take the opportunity to try and get up and move during the day, sit up with your shoulders back and your spine straight and visit a chiropractor for diagnosis and treatment of your back pain caused by poor posture. Taking the opportunity to correct your posture can not only help you look better, it can also keep you from experiencing a variety of serious health issues later on.
A recent study published in the Journal of the American Geriatrics Society has confirmed that poor posture is directly associated with longevity. The study followed 1,353 patients for a mean of 4.2 years. It confirmed, at least theoretically, what many chiropractors have been saying for many years: poor posture, including forward head posture, slumped shoulders, and excessive kyphosis from the upper or mid back, causes a significant effect on longevity.
In addition, bad posture can result in various spinal health issues, including hyperkyphosis or increased forward bend in the torso. This posture overtime will lead to the degeneration of one’s health by means of physiological processes like nerve wracking, organ compression, and arthritis, to name a few. The research study demonstrated that patients with hyperkyphosis had a greater rate of mortality compared to those without this postural problem. It was also found that the more severe the hyperkyphosis, the likelier the individual’s life expectancy would be affected.
Dr. Alex Jimenez’s Insight
Posture is the position in which a person holds their body while standing or sitting. While posture can say a lot about a person, whether they’re standing straight or hunching over, posture can actually define how healthy a person really is. Poor posture can cause a variety of side effects, according to research studies, and it may even impact an individual’s longevity. Chiropractic care is a safe and effective, alternative treatment option which can help promote proper posture to prevent spinal health issues.
Fundamentally, hyperkyphotic posture forecasts increased mortality because the problem increases the rate of aging. Chiropractic care is devoted to correcting as well as ensuring proper spinal alignment so that patients may live the longest, healthiest lives possible. Chiropractors emphasize the importance of correcting spinal misalignments, or subluxationx, by restoring the structure and function of the spine through the use of spinal adjustments and manual manipulations. The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Back Pain
According to statistics, approximately 80% of people will experience symptoms of back pain at least once throughout their lifetimes. Back pain is a common complaint which can result due to a variety of injuries and/or conditions. Often times, the natural degeneration of the spine with age can cause back pain. Herniated discs occur when the soft, gel-like center of an intervertebral disc pushes through a tear in its surrounding, outer ring of cartilage, compressing and irritating the nerve roots. Disc herniations most commonly occur along the lower back, or lumbar spine, but they may also occur along the cervical spine, or neck. The impingement of the nerves found in the low back due to injury and/or an aggravated condition can lead to symptoms of sciatica.
The spine is divided into three different parts: the neck or cervical spine, the upper back or thoracic spine, and the lower back or lumbar spine. Each region of the spine has its own function and abilities. The lower spine helps you lift heavy objects because it is elastic. The neck is also constructed for flexibility, but the upper spine is built for stability and is also essential in supporting the body.
All your ribs stretch out from the thoracic spine. While these ribs help to create a cage that protects most of your organs, if the thoracic spine is damaged, it can cause pain and discomfort in the shoulder and back area. To be able to acquire the best, most effective treatment for your upper back pain (also known as mid-back pain), you should first understand what may be causing it. A healthcare professional, such as chiropractor, can help you figure that out, but here are some of the most common causes of upper back pain.
Contents
Causes of Upper Back Pain
Poor posture: Sitting with a rounded back and the shoulders hunched forward can place too much stress on the muscles of the upper and mid back. Because many office employees spend their work days sitting in front of the computer, poor posture is considered one of the top causes of upper back pain. Especially when you’re at your desk for so many hours per day, it’s easy to fall into the bad habit of not sitting correctly.
Improper lifting: In order to protect your spine when choosing to lift something up, you should also use correct body mechanics. Not using the proper form for lifting can cause injury and lead to upper back pain.
Carrying a heavy back pack:�Anybody who uses a heavy back pack may be at risk for back injury. An over-loaded back pack can be harmful to the spine, but most importantly, not wearing a backpack correctly (eg, only using one strap) can cause more harm.
Trauma/injury: Traumatic events, such as automobile accidents, can cause upper back pain as a result of various factors. It is possible to suffer a fracture to the vertebrae of the spine or part of your vertebrae can press on a spinal nerve, which can lead to pain.
Infection:�Even a paraspinal abscess or a spinal epidural abscess can compress the spinal cord or spinal nerves, causing upper back pain, depending on the affected region of the spine.
Osteoporosis: This is a condition which affects the bones, also you might not understand you’ve got osteoporosis until you experience a spinal fracture (eg, spinal compression fracture). Osteoporosis can weaken your bones, making them more likely to fracture and less inclined to carry your weight. You may develop upper back pain if you have osteoporosis on your thoracic spine. Weakened vertebrae don’t support your body’s weight as well, so tendons, ligaments, and muscles need to work harder to make up for that vertebrae. This can result in sprain, strain, or muscle fatigue as well as upper back pain, among other symptoms. In case you have a fracture or fractures due to osteoporosis, you will probably develop a round back from poor posture.
Kyphosis: When looked at from the side, your spine is supposed to curve in your upper back (thoracic spine) area; that curve is called a kyphotic curve or kyphosis. However, it can begin to curve out too much which is referred to as problematic kyphosis. Various conditions, such as osteoporosis, can cause kyphosis in the thoracic spine, leading to upper back pain.
Scoliosis: Scoliosis causes an unusual lateral curvature of the spine. It can make your spine look like an “S”or a “C” when seen from behind. If your spine is curving to the left or to the right in the upper back (thoracic spine), then you might have pain due to how the curve affects spinal nerves, muscles, and other soft tissues.
Other conditions: Upper back pain may develop in conjunction with other medical conditions not related to the spine. For instance:
Acid reflux (GERD)
Ulcer
Cardiac conditions, such as angina
Anatomical Structure and Upper Back Pain
The upper back, or the thoracic spine, is significantly more stable compared to the neck, or the cervical spine, and the low back, or lumbar spine. It doesn’t move as far as the other regions of the spine since one of its most important functions is to protect the inner organs in the chest. It does this in conjunction with the ribs, which are attached to the vertebrae in the thoracic spine.
However, the thoracic spine is less prone to suffer from intervertebral disc issues as well as joint problems that commonly impact the neck and low back. It is much less common, although that does not imply that you can not have a herniated disc causing your upper back pain. It is less frequent to have spinal health issues in the thoracic spine. The neck and low back move much more compared to the upper back, therefore discs and joints may wear out earlier from overuse and misuse.
Chiropractic Care for Upper Back Pain
Although less common than lower back pain, for instance, many people will visit a chiropractor’s office seeking relief for upper back pain. Working with a highly qualified doctor of chiropractic, patients can find relief from their upper back pain. In a chiropractic office, the terms of a treatment are on the patient.
Since many thoracic spine issues also consist of cervical or lumbar spinal issues, a doctor of chiropractic can assess and treat all three regions successfully. Herniation of the upper and lower spine’s discs are common due to the versatility of these two regions. If pain is at the upper of mid back, however, most frequently the reason isn’t because of slippage, but rather an injury or poor posture.
When an individual has had bad posture for many years, their thoracic spine can get used to being pulled forward and the surrounding supporting muscles can become weak. Pain can often increase or worsen from the continuous pulling due to poor posture. A chiropractor can help develop a treatment program which involves carefully restoring the original alignment of the spine in order to improve posture.
Dr. Alex Jimenez’s Insight
Neck and back pain are some of the most common health issues treated in a chiropractic office. Although rare, however, upper back pain may also develop as a result of some of the prevalent causes behind cervical and lumbar spine problems. The thoracic spine is the most stable region of the spine. Because the rib cage is attached to the vertebrae of the thoracic spine, the upper back area of the human body must function efficiently to support the body’s weight. Chiropractic care can help carefully restore the original alignment of the thoracic spine, helping to decrease upper back pain and other symptoms.
If someone becomes injured during an automobile accident, the muscles of the upper back might not be strong enough to offer proper support for the body. Overstretching of significant muscles can lead to severe pain and can trigger the vertebrae of the upper back to slip out of place. If you’re suffering from upper back pain, then drop by a chiropractic office. Finding relief for your upper back pain is a walk-in away with no lengthy insurance forms to complete or odd appointment times to remember. The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Back Pain
According to statistics, approximately 80% of people will experience symptoms of back pain at least once throughout their lifetimes. Back pain is a common complaint which can result due to a variety of injuries and/or conditions. Often times, the natural degeneration of the spine with age can cause back pain. Herniated discs occur when the soft, gel-like center of an intervertebral disc pushes through a tear in its surrounding, outer ring of cartilage, compressing and irritating the nerve roots. Disc herniations most commonly occur along the lower back, or lumbar spine, but they may also occur along the cervical spine, or neck. The impingement of the nerves found in the low back due to injury and/or an aggravated condition can lead to symptoms of sciatica.
Daniel Alvarado, owner of PUSH Fitness, first met Dr. Alex Jimenez through the connection of a good friend and they became workout partners. Daniel Alvarado learned a lot regarding chiropractic alignment and physiology by training with Dr. Jimenez. After experiencing upper and mid back pain as well as shoulder pain, Daniel Alvarado began receiving regular chiropractic care with Dr. Alex Jimenez in order to restore the original alignment of his spine and improve the symptoms of his injury. Daniel Alvarado highly recommends Dr. Jimenez as the non surgical choice for sports injuries, as he discusses how Dr. Alex Jimenez’s relationship with his patients can ensure a positive environment for a better, more improved treatment. Together with Dr. Alex Jimenez’s chiropractic care and his own rehabilitation and sports therapy, Daniel Alvarado emphasizes the dynamic of their services.
Chiropractic Alignment
Sports injuries are injuries which occur in athletic activities or exercising. There are kids and approximately 30 million teens alone that participate in some form of sport. About 3 million sports athletes experience sports injuries annually, which causes some loss of time of participation in the sport. Prevention helps reduce sport injuries. It’s crucial to set up participation in warm-ups and exercises which focus on primary muscle groups utilized in the game of interest. Also, establishing an accident prevention program as a staff, including education on rehydration, nutrition, tracking staff members “in danger”, tracking behavior, skills, and techniques.
Our team has takes great�pride in bringing our families and injured patients only�clinically proven treatments protocols. �By teaching complete holistic wellness as a lifestyle,�we also change not only our patients lives but their families as well.� We do this so that we may reach as many El Pasoans who need us, no matter the affordability issues.
There is no reason we cannot help you.�?
Our uplifting southwest community surrounded by it limitless beauty is an amazing place to live and enjoy our families; it is therefore our mission to help each of our patients to�live,�to�love,�to�matter�and�to�thrive�pain free�in this wonderful special place.
If you have enjoyed this video and/or we have helped you in any way please feel free to subscribe and share us.
Pain in the upper or mid back is less frequent than neck or lower back pain. The upper back is the region below the cervical spine, or the neck, and above the lower back, or the lumbar spine. The upper spine is known as the thoracic spine, and it’s the most stable portion of the spine. The range of motion in the upper back is limited because of the spine’s attachments to the ribs, or the rib cage.
Contents
What is Upper Back Pain?
Also called the thoracic spine, the upper back is designed to support the ribs, sternum, vital organs and the vertebrae. Although uncommon, discomfort can be caused by upper back pain and is typically caused by joint irritation or improper posture. In fact, half of all working Americans admit to having back pain symptoms during the year caused by poor sitting posture while working in a desk.
What are the Symptoms of Upper Back Pain?
Upper back pain is generally caused by soft tissue injuries, such as sprains or strains, stress and tension caused by poor posture or from looking down for long time periods (eg, texting, cell phone usage). Symptoms might include:
Pain
Tightness
Stiffness
Muscle spasm
Tenderness to touch
Headache
Since the ribs are attached to the thoracic spine by the vertebral bodies of the spine, some patients experience pain when taking a deep breath, sneezing or coughing.
What Causes Upper Back Pain?
An episode of upper back pain can be triggered by various movements and actions, including:
Twisting
Excessive bending
Whiplash or other neck injury
Lifting improperly
Poor muscle tone
Overuse, repetitive movements
Contact sports
Carrying too heavy a load
Wearing an overloaded backpack
Smoking
Being overweight
Poor posture in general, without taking a break to walk around or working at the computer for a long time can contribute to upper back pain. Both muscle sprain or strain and muscle fatigue, which often results from poor posture, may cause the upper back pain.
Is Upper Back Pain Serious? What Can I Do About It?
In most cases, upper back pain is not a cause for stress although it can be painful, uncomfortable and inconvenient. Furthermore, if pain develops suddenly and is acute, such as in the case of an injury (eg, fall), also, if pain and symptoms (eg, weakness) progressively worsen, you may need to seek immediate medical attention. Generally, several home treatments may help alleviate upper back pain. These include:
Short-term rest
Gentle stretches
Over-the-counter drugs and/or medications, such as ibuprofen, (Motrin�), naproxen sodium (Aleve�), or acetaminophen (Tylenol�). Take with food, and do not take more than the recommended dosage.
Ice (to decrease pain and swelling). Use a cold pack that is commercially available or fill a plastic bag with ice and seal it then wrap it in a towel. Apply for 20 minutes every two to three hours for the first 2 to 3 days to the area.
Heat (following the first 72 hours). After applying moist heat, gently stretch the muscles to improve mobility and relieve stiffness.
Your doctor may prescribe certain drugs and/or medications, like a muscle relaxant or perform trigger point injections to help break up muscle spasms. They may also recommend physical therapy to relieve pain and further increase strength, mobility and flexibility.� Furthermore, a primary care physician may include other treatments, such as chiropractic care and acupuncture. Most cases of upper back pain resolve with no treatment in 1 to 2 weeks. Once you experience no symptoms, resume your normal activities gradually. Do not rush things, though. As always, however, acute or abrupt upper back pain ought to be addressed in order to determine the source of the symptoms.
How Can Chiropractic Care Help with Upper Back Pain?
Chiropractic care may be a great way to control and relieve pain and swelling caused by upper back pain. Routine chiropractic care supplies patients with upper back pain treatment that is a safe, non-invasive, non-addictive alternative to prescription drugs or over-the-counter pain medications (OTCs), that are generally prescribed to patients to help them manage their pain and discomfort.
Chiropractors deliver a gentle, non-invasive, non-addictive treatment, called a chiropractic adjustment. Spinal adjustments reduce misalignments or joint restrictions in the spine and joints and enhance functioning of the musculoskeletal and nervous system. By enhancing spinal health, your system function and decreasing joint stiffness, your body gets the ability to better handle symptoms as well as naturally heal itself. Below are some of the health advantages chiropractic care can provide for patients with upper back pain:
Reduced pain and discomfort
Decreased inflammation
Improved range of motion
Improved flexibility
Increased muscle tone and strength
Dr. Alex Jimenez’s Insight
Although pain and discomfort are most commonly reported along the neck, or the cervical spine, and the lower back, or the lumbar spine, the upper and mid back, or the thoracic spine, may occasionally manifest symptoms of pain and discomfort. The thoracic spine is the largest portion of the spine, consisting of 12 of the 14 vertebrae which make up the spine. Although it is also considered to be the most stable region of the spine, because the rib cage attaches to the thoracic spine, it’s not unknown for dysfunction to affect the upper and mid back regions of the spine, from time to time. Chiropractic care can help treat upper back pain utilizing spinal adjustments and manual manipulations to carefully realign the spine and restore the natural integrity of the spine.
To see if chiropractic care is ideal for your condition, chiropractors will execute a consultation and examination if necessary and they may refer you for diagnostic imaging, such as x-ray or MRI. Dependent on the findings of the chiropractic exam and appointment, your doctor of chiropractic may decide to co-treat your back pain with other healthcare professionals, including other primary care physicians, physical therapists or massage therapists. The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Back Pain
According to statistics, approximately 80% of people will experience symptoms of back pain at least once throughout their lifetimes. Back pain is a common complaint which can result due to a variety of injuries and/or conditions. Often times, the natural degeneration of the spine with age can cause back pain. Herniated discs occur when the soft, gel-like center of an intervertebral disc pushes through a tear in its surrounding, outer ring of cartilage, compressing and irritating the nerve roots. Disc herniations most commonly occur along the lower back, or lumbar spine, but they may also occur along the cervical spine, or neck. The impingement of the nerves found in the low back due to injury and/or an aggravated condition can lead to symptoms of sciatica.
Technology makes life more convenient, but it has also made our lifestyles more sedentary. Poor posture’s stress places unnecessary amounts of pressure and tension in the neck and back. We know neck pain and back pain can be debilitating, especially after years of improper posture and a sedentary lifestyle. Chiropractic care can help reduce pain and discomfort from the spine with spinal adjustments and manual manipulations, as well as several lifestyle modifications. Chiropractic can help treat a variety of injuries and conditions affecting spine health. Before further discussing what chiropractic care can do for you, we’ll first discuss the common causes of neck and back pain.
Contents
Back Pain
Back pain is common, but it doesn’t have to be permanent. Whether your pain has been brought on by years of heavy lifting or a single mishap or fall, a doctor of chiropractic, or chiropractor, will do their very best to discover which type of treatment method will guarantee you relief from your symptoms. Strengthening exercises help to train your heart to support your weight and spinal adjustments and manual manipulations are ways to relieve inflammation, reduce pressure and restore the proper alignment of the spine to decrease pain and discomfort. Pain relief methods will address your symptoms, but chiropractic care can promote recovery for long term spine pain relief.
Neck Pain
If you experience pain or discomfort in your neck, you may want to address the symptoms with safe and effective alternative treatment options. While the solutions that may assist with your pain are determined by the underlying cause of the distress, a chiropractor can properly diagnose the source of the symptoms, identifying the causes and giving a personalized treatment plan to assist with the situation. Chiropractic care can also provide treatment for a variety of issues causing symptoms of neck pain.
What Causes Pain?
Pain stems from a number of situations and problems. It may relate trauma from an injury or due to an aggravated condition along the length of the spine or it may even relate to posture and the way you sleep during the night. Depending on the origin of the pain and the regions affected by the discomfort, the specific treatments may vary.�Common reasons for your pain include:
A sedentary lifestyle or having a computer on your office, which causes long intervals of holding your head in the same place
Looking down in a tablet, computer, telephone or other device for extended periods
Whiplash or injuries to your neck and back in an automobile accident
A herniated disc in the neck or back
Injuries to the spine
Poor posture
Stress on several regions of the spine, or compression
Certain diseases or conditions, like degenerative disc disease or arthritis
5 Causes of Neck and Back Pain or Discomfort
If you have suffered from pain or discomfort in your neck or back, you may very well be aware of how debilitating the symptoms can become. We are able to complete all of our daily activities and tasks on a regular basis because the spine offers rigidity, stability, and endurance at the same exact time. Through the structure and function of the ligaments, tendons, intervertebral discs and facet joints, the mechanical connection that your body needs is provided by the spine. Just like any sort of apparatus, breakdowns can happen at any time, resulting in symptoms of neck and back pain or discomfort. Next, we will discuss the five common causes of neck and back pain.
Disc Herniation
Disc herniation is among the most frequent causes of neck and back pain. It goes by several names like a pinched nerve, and bulging or burning disc, but regardless of what you call it, it can be intense and long-lasting. Pain in the legs, also called sciatica, is often the first indication of a herniated disc in the lumbar spine, or low back. Since 90 percent of herniated discs occur within this region, leg pain is the most frequent symptom. Other signs may include severe pain, weakness and tingling sensations down one of both legs. Chiropractic care, physical therapy and gentle stretches and exercises are the most common kinds of treatment for a herniated disc. These conservative treatments can cut the need for more aggressive interventions and can be remarkably powerful. For surgical procedures, it might be considered in scenarios where non-operative remedies are ineffective.
Spinal Stenosis
Spinal stenosis is defined as an abnormal narrowing of the bony channel which contains the spinal cord or the spinal nerves. Unlike other spinal problems, spinal stenosis tends to come on slowly and gradually gets worse. Spinal stenosis is treated with a combination of gentle exercises and lifestyle modifications. You will see that some symptoms of spinal stenosis can be relieved by sitting or lying down, maintaining a proper posture, or preventing certain activities that cause the stenosis symptoms. In acute cases, spinal epidural shots may be used to deal with the pain and alleviate discomfort. Chiropractic care can also be used to treat spinal stenosis symptoms.
Sprains and Strains
When you have a sudden onset of pain or discomfort in your neck or back, the problem could be a sprain or strain. Moving the wrong way, overdoing an exercise regime, or decreasing physical activity frequency can lead to a sprain or strain. The good news is that if the time and appropriate treatment are performed, the pain and distress usually go away in a determined amount of time. It’s ideal to see a healthcare professional in case you’ve suffered a sprain or strain to your neck or back. Do not let what you believe is a small sprain or strain turn out to be a bigger issue. Healthcare professionals recommend rest and limited activity until you are feeling better if the issue is a sprain or strain. You may benefit from physical therapy and exercise like water aerobics and stretching exercises to help you heal and recover faster.
Spinal Osteoarthritis
Spinal osteoarthritis is� defined as the breakdown of cartilage in discs or the joints in the neck or back. In some cases, it can cause bone wane causing painful pressure on the nerves going into the spine. If diagnosed with spinal osteoarthritis, you may receive conservative or very aggressive treatment depending on the issue; for example, rest and hot or cold packs or specific medications. However, chiropractic care may be a safe and effective alternative treatment option for some people with spinal osteoarthritis. It’s essential to first talk to a qualified and experienced healthcare professional regarding the recommended treatment for you. If unsuccessful, surgery may be needed, which is usually recommended only as a last resort for patients with spinal osteoarthritis.
Vertebral Compression Fracture
A vertebral compression fracture can be a serious condition that creates pain in the neck or back, depending on where the fracture occurs. Vertebral compression fractures occur as a result of tiny cracks from the vertebrae; the bones of the spine. As time passes, hairline fractures may cause the vertebrae to collapse, which is what is known as a spinal or vertebral compression fracture. The symptoms of a compression fracture can be acute and sudden back pain during a change of posture or movement. Rather than standing tall, you might see that you have a stooped appearance. This sign should not be ignored by you; as with any medical illness, early intervention may often make it much easier to deal with.
There are several choices for treating your vertebral compression fracture, which can include some types of drugs and/or medications to temporarily relieve symptoms while ongoing with treatment. Other treatment choices are bracing of the neck, physical activity or exercise that is limited and bed rest. Understanding the causes of neck and back pain can offer you a head start on receiving the appropriate treatment option for your specific spine health issue. If you suffer from any type of pain or discomfort, please contact a healthcare professional who specializes in the diagnosis, treatment and prevention of spinal health issues, such as a chiropractor.
How Can a Chiropractor Help?
When you find chiropractic care for neck and back pain, they will first diagnose the source of your symptoms, utilizing the appropriate diagnostic tools to find out the underlying causes of the distress. Chiropractors supply treatments after determining the reasons to address the factors. A chiropractor helps with pain relief by correcting the compression or inadequate alignment on your own neck and back. When your spine is misaligned or subluxated, it can lead to a variety of spinal health issues, such as the ones mentioned above. Injuries and/or conditions which are left untreated for an extended period of time may worsen without proper treatment.
Chiropractic care utilizes spinal adjustments and manual manipulations to reduce the pressure in your spine and improve the alignment of the neck and back, in order to restore the original integrity of your spine. A doctor of chiropractic, or doctor will concentrate on helping your body heal and recuperate through natural solutions. They might also recommend nutritional advice and exercises, in addition to stretches to assist with the healing procedure. Chiropractors may additionally create a personalized treatment program based on the possible complications associated with the injuries on your own neck and back as well as the reason for your pain and discomfort.
Dr. Alex Jimenez’s Insight
Neck and back pain or discomfort are some of the most common types of issues frequently treated by a chiropractor. Although neck and back pain can be caused by a wide variety of spinal health problems, chiropractic care is a safe and effective, alternative treatment option that can help ease the symptoms associated with many injuries and/or conditions related to the musculoskeletal and nervous system. As an experienced chiropractor, spinal adjustment and manual manipulations can help reduce painful symptoms by allowing the body to naturally heal itself, restoring the quality of life of patients.
When to Seek Chiropractic Therapy
Seeking chiropractic treatment for pain and discomfort is a personal decision, nevertheless, you should consider treatment immediately after a car accident or some other type of injury or aggravated condition. We advise seeking treatment for persistent and chronic issues. You might want to consider chiropractic care if you notice symptoms due to using electronics throughout the day or sitting at your work, since it may worsen over time if left untreated, even if it is simply a slight soreness in your muscles.
Treating pain and discomfort in your body starts with improving the health and wellness of your spine. To learn more about addressing problems on your neck and spine or to set an appointment with a chiropractor, please make sure to talk to your primary care provider or healthcare professional. The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Back Pain
According to statistics, approximately 80% of people will experience symptoms of back pain at least once throughout their lifetimes. Back pain is a common complaint which can result due to a variety of injuries and/or conditions. Often times, the natural degeneration of the spine with age can cause back pain. Herniated discs occur when the soft, gel-like center of an intervertebral disc pushes through a tear in its surrounding, outer ring of cartilage, compressing and irritating the nerve roots. Disc herniations most commonly occur along the lower back, or lumbar spine, but they may also occur along the cervical spine, or neck. The impingement of the nerves found in the low back due to injury and/or an aggravated condition can lead to symptoms of sciatica.
Sciatica Pain: Sandra Rubio discusses sciatica, its causes and its symptoms. Sciatica is the collection of symptoms caused by the compression of the sciatic nerve, the longest nerve in the human body which extends from the lower back to the feet. Sandra Rubio describes how she’s witnessed many patients come into Dr. Alex Jimenez’s office feeling painful and often severe symptoms of sciatica caused by a variety of spinal health issues. Fortunately, Dr. Alex Jimenez is the non surgical choice for the safe and effective treatment of sciatica symptoms.
Sciatica Pain Explained
Based upon how it’s defined, approximately 2 percent to 40 percent of individuals will experience sciatica symptoms at some point in their lifetime. It is most frequent during people’s 40’s and 50’s, and men are more frequently affected than women. About 90 percent of the time, sciatica symptoms are because of a disc herniation. Other issues that may bring about sciatica comprise of spondylolisthesis, spinal stenosis, piriformis syndrome, pelvic tumors, and compression by a baby’s head during pregnancy, among other spinal health issues.
When your body is truly healthy, you will arrive at your optimal fitness level proper physiological fitness state. �We want to help you live a new and improved lifestyle. Over the last 2 decades while researching and testing methods with thousands of patients we have learned what works effectively at decreasing pain while increasing human vitality.
We focus on what works for you. We also strive to create fitness and better the body through researched methods and total wellness programs. These programs are natural, and use the body�s own ability to achieve goals of improvement, rather than introducing harmful chemicals, controversial hormone replacement, surgery, or addictive drugs.
We want you to live a life that is fulfilled with more energy, positive attitude, better sleep, less pain, proper body weight and educated on how to maintain this way of life. I have made a life of taking care of each and every one of my patients.
I assure you, I will only accept the best for you�
If you have enjoyed this video and/or we have helped you in any way please feel free to subscribe and share us.
Low back pain is a common complaint reported among the general population. Once it begins, however, what do you do? Here are 5 ways to help manage those sudden bouts of back pain. This guide is for people who are experiencing mild low back pain. For instance, in the event that you woke up with back pain or you overdid it at the gym and now have muscle strain pain, the following back pain management treatment strategies are right for you.
Rest (but just a bit). If your back hurts, take a rest. Lie down and avoid overusing your muscles for some time. This doesn’t mean remain in bed for a week. Actually, a lot of rest can make your back pain worse. After a brief break, get up, move around, and stretch. You will find it really helps reduce that nagging backache.
Try over-the-counter medications. There are several types of drugs and/or medications which can help ease back pain. Some medications relax muscle spasms, reduce inflammation, and relieve pain. Many can be found over-the-counter in the regional pharmacy. Prescription drugs, on the other hand, require your physician’s written consent. Some medications used for back pain include: acetaminophen (eg, Tylenol) or non-steriodal anti-inflammatory drugs (NSAIDs) (eg, aspirin, ibuprofen). Although these can help reduce symptoms of back pain, the effects are only meant to be temporary. If back pain persists, follow some of the other treatment strategies.
Attempt cold/heat therapy. Cold treatment can help decrease muscle soreness, inflammation, and pain. Cold therapy might be recommended following a strain or a sprain. Apply ice to your back, take a cool bath, or use iced towels/compresses, cold packs, ice cubes. Some healthcare professionals recommend utilizing heat therapy only on very select situations, as this can increase inflammation and symptoms.
Get a massage. Massage is a popular therapy that can help alleviate stiffness, spasms, inflammation, aches, muscle tension, and pain. It can also help improve circulation, flexibility, and range of movement. Massage can be managed by a professional, such as a massage therapist, or you can give yourself a mini-massage utilizing hand-held massagers which could help increase blood flow and alleviate pain.
Visit a doctor. The most crucial thing to remember about periodic bouts of back pain is that if they happen more frequently, increase in length (lasting more than a few days), or the pain begins to interfere with your usual activities, it’s time to see a healthcare professional. It might be more than just a sudden case of low back pain.
The good thing is that many lower spine issues can be treated with non-surgical treatments. Back pain that goes untreated can get worse, so it’s a good idea to manage your back pain now. You don’t need your bout of back pain to develop into a chronic pain health issue. Furthermore, some healthcare professionals are back pain specialists which can help treat a variety of injuries and/or conditions which may be the source of your symptoms. Chiropractic care is a recommended back pain management treatment strategy.
Contents
Chiropractic Care for Back Pain
Back pain management treatment strategies are chosen by people looking for back pain relief options. Chiropractors are visited by about 22 million Americans annually. Of them, 7.7 million, or 35 percent, are looking for relief from back pain due to various causes, including trauma or injury from accidents, sports injuries, and muscle strains. Other ailments include radiating pain in the arms, neck and legs as well as headaches.
What is Chiropractic Care?
Chiropractic care is a popular, alternative treatment option which focuses on the diagnosis, treatment and prevention of injuries and/or conditions associated with the musculoskeletal and nervous system. Chiropractors use spinal adjustments and manual manipulations, as well as other alternative treatment methods, to maintain the proper alignment of the musculoskeletal structure, especially the spine, in order to allow the human body to naturally heal itself. Chiropractic care can help restore mobility to joints limited by tissue injury caused by a traumatic event or stress, such as sitting without proper back support. It is occasionally used in conjunction with traditional therapy.
What Does Chiropractic for Back Pain Involve?
A chiropractor primarily takes a medical history, performs a physical exam, and may use diagnostic imaging or lab tests to determine if treatment is appropriate for your back pain. The treatment plan may involve one of more alterations where the doctor adjusts and manipulates the joints with a controlled force to improve high quality and range of motion. Many chiropractors also incorporate counseling and exercise/rehabilitation to the treatment program. The goals of chiropractic care include the restoration of function and prevention of future injury in addition to back pain relief.
What Are the Benefits and Risks of Chiropractic Care?
Chiropractic care is usually considered a safe and effective treatment for acute low back pain, the type of sudden injury that results from shifting furniture or getting handled. Acute pain, which can be much more common than chronic pain, lasts no more than six weeks and typically gets better by itself, however, it may worsen if left untreated for an extended period of time.
Research has also demonstrated chiropractic to be helpful in treating neck pain and headaches. Additionally, fibromyalgia and osteoarthritis may react to the treatment methods utilized both by chiropractors and professionals of deep tissue massage. Studies have not confirmed the potency of sclerotherapy or prolotherapy used by some chiropractors, osteopaths, and medical doctors, to treat chronic back pain, the sort of pain which may come on suddenly or slowly and continue for more than three months. The treatment involves injections, such as anesthetic or sugar water, in hopes of strengthening the ligaments in the back.
Individuals who have osteoporosis, spinal cord compression, arthritis, or those who take blood-thinning medications, should first talk to their healthcare professional about participating in chiropractic care treatment strategies. Patients with a history of cancer must obtain clearance from their doctor as well before undergoing chiropractic care.
Dr. Alex Jimenez’s Insight
Back pain is one of the most common reasons for chiropractor office visits. Back pain can be caused by a number of injuries and/or aggravated conditions and it can range from mild to severe. Whether you’re experiencing dull and achy pain or burning and spasming pain, finding the proper treatment strategies for the management of your back pain can determine whether your quality of life will be compromised or not. Chiropractic care is a safe and effective, alternative treatment option which can help restore the proper alignment of your spine, allowing your body to naturally heal itself without the need for drugs and/or medications or surgical interventions.
All treatment relies on an accurate diagnosis of your back pain. The chiropractor ought to be informed concerning your health history, including previous medical conditions, current medications, traumatic/surgical history, and lifestyle factors. There are cases where therapy was not effective towards the treatment of a herniated or slipped disc, although uncommon, and other complications may occur. To be safe, check to make sure that your condition will benefit from chiropractic care. The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Back Pain
According to statistics, approximately 80% of people will experience symptoms of back pain at least once throughout their lifetimes. Back pain is a common complaint which can result due to a variety of injuries and/or conditions. Often times, the natural degeneration of the spine with age can cause back pain. Herniated discs occur when the soft, gel-like center of an intervertebral disc pushes through a tear in its surrounding, outer ring of cartilage, compressing and irritating the nerve roots. Disc herniations most commonly occur along the lower back, or lumbar spine, but they may also occur along the cervical spine, or neck. The impingement of the nerves found in the low back due to injury and/or an aggravated condition can lead to symptoms of sciatica.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine





 We focus on what works for you. We also strive to create fitness and better the body through researched methods and total wellness programs. These programs are natural, and use the body�s own ability to achieve goals of improvement, rather than introducing harmful chemicals, controversial hormone replacement, surgery, or addictive drugs.
We focus on what works for you. We also strive to create fitness and better the body through researched methods and total wellness programs. These programs are natural, and use the body�s own ability to achieve goals of improvement, rather than introducing harmful chemicals, controversial hormone replacement, surgery, or addictive drugs.





 When your body is truly healthy, you will arrive at your optimal fitness level proper physiological fitness state. �We want to help you live a new and improved lifestyle. Over the last 2 decades while researching and testing methods with thousands of patients we have learned what works effectively at decreasing pain while increasing human vitality.
When your body is truly healthy, you will arrive at your optimal fitness level proper physiological fitness state. �We want to help you live a new and improved lifestyle. Over the last 2 decades while researching and testing methods with thousands of patients we have learned what works effectively at decreasing pain while increasing human vitality.






