Chiropractic care is a safe, natural treatment for people of all ages, and senior citizens can benefit from it. It is far more preferable than many other options, including pharmaceuticals with unpleasant and even harmful side effects and surgery. Several studies have also shown that regular chiropractic treatment benefits geriatric patients and can help keep them out of long-term care facilities and nursing homes. In short, seniors who get chiropractic regularly are healthier and enjoy these great benefits.
Contents
Reduced Risk of Degeneration of the Joints (Including the Spine)
When the spine is not aligned, it can cause wear and friction on the joints, resulting in damage. Regular spinal alignment keeps the spine in the correct position so that the body is balanced. It reduces the risk of spinal degeneration and certain types of arthritis by decreasing the amount of stress on the spine and bringing it into a more normal, natural alignment.
Improved Range of Motion
As a person gets older, their range of motion decreases. This is especially true of sedentary people or those who have sustained an injury that kept them confined to a bed or wheelchair for a long time.
Helping improve a person’s range of motion is one of the best benefits of chiropractic. While there are certain levels and each person has a goal for how much range of motion they want, a chiropractor can help them get as close to those goals as possible.
Better Coordination and Balance
Most of the coordination and balance problems seniors experience come from degenerative changes or injuries that affect the cervical spine. The backside of the cervical spine joints houses mechanoreceptors responsible for providing the brain with vital information that regulates coordination and balance. When that area is compromised, their function is hindered. By stimulating the mechanoreceptors, a chiropractor can help restore or improve the condition.
Decreased Risk of Falls
According to the Centers for Disease Control (CDC), in the United States, some older adult falls every second of every day. Among Americans aged 65 and older, there are 850,000 bone fractures each year, and falls are the cause of 90% of them. A chiropractor can stimulate the mechanoreceptors which reside in the cervical spine, normalizing them and helping to restore the patient’s balance and coordination.
Stronger Immune System and Better Health
When the spine is properly aligned, the body is better able to function as it should. This includes the digestive system, respiratory system, and even the heart. Neural impulses can be transmitted and received more efficiently and effectively.
This strengthens the immune system making the patient less susceptible to illness and disease. Regular care can provide better health and wellness while improving the patient’s quality of life.
More Effective Pain Management
Chiropractic has been proven time and again to be one of the safest, most effective methods for treating pain, particularly those that involve the spine. Chiropractic helps correct the problem that is causing the pain and helps heal the soft tissue structures around the area. Where pain medicine, muscle relaxants, and anti-inflammatory medication are little more than band-aids that treat the symptoms while ignoring the cause, chiropractic gets to the root of the problem and begins treatment there.
In addition to spinal adjustments, the chiropractor will typically recommend stretching and special exercises, lifestyle changes, and diet modifications. Elderly patients benefit from the whole body, holistic approach to health care at the heart of chiropractic. The result is better health and a better quality of life.
Functional Medicine Doctor Explains Men’s Hormones
Hello there, it�s Dr. Alex Jimenez again and welcome to part four of �Taking Control of your Healthcare�. Today, we�re going to discuss hormones. Hormones regulate most of the human body�s systems as they are recognized as the messenger molecules of the endocrine system. Hormone imbalances can cause subtle changes, however, their effects can tremendously impact an individual�s overall health and wellness. And what�s worse, most healthcare professionals don�t treat hormonal imbalances unless they�ve already been considered extreme.
The sex hormones, the thyroid hormones, and the adrenal hormones are the most important hormones we have to keep in balance. There�s a variety of other hormones, of course, but health issues associated with those are often more rare. Many doctors generally won�t test a person for hormone imbalances unless they�ve been trying to conceive a baby or they have sexual dysfunction or any other health issue of this type. And frequently, many doctors miss other problems by performing a screening test rather than a complete test.
Contents
What are Hormones?
Hormones are essential towards mental health, gut health, and reproductive health. In functional medicine, we even believe that hormones are vital towards maintaining a healthy immune system. Even if you�re not trying to conceive a baby or if you don�t have sexual dysfunction, it�s important for both men and women to known what their hormone levels look like.
Now, let�s discuss hormonal imbalances in sex hormones. First of all, How does a hormone imbalance manifest itself? Do you experience mood swings and fluctuations in your energy levels? Or if you�re a female, do you experience symptoms of PMS? Or perhaps you need coffee to wake up in the morning and wine to sleep at night? Has your sex drive, or libido, decreased? Do you have brain fog? Or is it difficult for you to focus on tasks?
If you�ve experienced any of these symptoms, you might have a hormonal imbalance in your sex hormones. Hormones are small molecules in charge of transmitting signals from one body system to another. But, if these molecules aren�t functioning accordingly, our energy levels and our mood can be tremendously affected. If you feel that something is off within your own body, talk to your doctor and seek proper testing. Don�t simply guess.
Let�s begin by discussing how you test your hormones. In functional medicine, we can test through saliva, blood, urine, and even stool. But, which is best for testing hormones? The truth is, knowing how and when to test your hormones is important because testing can depend on the marker that you want to look at. By way of instance, blood testing is one of the best and most affordable if you�re simply looking for a preliminary screening. A functional medicine doctor can also determine when a urine test will be more helpful than a blood test or a saliva test.
Taking Control of Men’s Hormones
So, now that you know how to test your hormones, we�ll discuss the different health issues caused by hormonal imbalances in the sex hormones of both men and women. First, let�s talk about men. As for the women, this is still an essential topic for you to learn about because the men in your lives are much less likely to schedule a doctor�s appointment for themselves.
Approximately 39 percent of men over the age of 45 have low levels of testosterone, or what�s known as low T. Elevated insulin levels associated with diabetes and obesity can lower your testosterone levels, which in turn, can increase estrogen levels. When testosterone goes down, your sex drive, or libido, and other functions can be tremendously affected. Excess consumption of sugar and starch can have different impacts for both men and women. Additionally, the utilization of certain drugs and/or medications, lack of exercise and physical activity, as well as inflammation, can also contribute to lower testosterone levels. While the majority of doctors won�t test testosterone levels in a man unless they have sexual dysfunction, I always want to make sure to test the sex hormones if a man has belly fat.
I would also like to discuss the serious side effects of a drug/medication which is commonly prescribed for sexual dysfunction. Statins can help lower cholesterol, however, did you know that your testosterone is made from cholesterol? That�s right. And when you start taking a drug/medication which was designed to decrease your cholesterol, you may also potentially be decreasing your sex hormones. It�s well-known that statins can decrease testosterone, leading to sexual dysfunction and even sometimes causing men to grow breasts, a condition known as gynecomastia. Side effects like these occur when we don�t treat the source of a health issue.
What you eat, including mainly sugar and starch, can be associated with your low testosterone levels and your abnormal cholesterol levels. Treatments like these where you take a drug for one thing but then end up taking another medication for the side effects of the fist medicine is unfortunately something that happens a lot in the medical field, and it can be a real nightmare.
Male testosterone levels are decreasing so much with each generation that normal reference ranges for testosterone levels in males are changing. But, that�s not something we want to happen. We don�t want these abnormal changes to become normal. Therefore, shouldn�t we be trying to find out why the overall health and wellness of our population is decreasing at such an alarming rate rather than lowering our normal standards of well-being?
Before we do that, however, we first have to understand why this problem is happening. From our increased exposure to toxins and our elevated levels of stress to our higher consumption of processed foods, these are only several of the more obvious reasons why our hormones are being affected.
In conventional medicine, the reference ranges for testosterone are between 264 and 916.
When you think about it, however, this is a tremendous range. Does a man with a testosterone level of 265 have the same sexual function as a man with a testosterone level of 916? Most definitely not. Yet these two people are classified under the same category. And with that in mind, what are the optimal reference ranges for testosterone? Men under the age of 30 should have a testosterone level of over 700, and men over the age of 30 should have a testosterone level of at least 500.
Evaluating men�s total testosterone levels is essential but we also need to evaluate their active hormone levels, or their free testosterone levels. Testosterone is carried around on what is known as a sex hormone binding globulin, which then releases it as the human body needs it. This carrier protein is found in the blood and when there�s too much of it, it becomes difficult for the human body to release testosterone when it�s needed.
In men, free testosterone levels should be of at least 10 but, they should optimally be closer to 15 or 20. Additionally, your doctor should check the sex hormone binding globulin or SHBG. As we discussed before, this carrier protein for testosterone and other hormones, can decrease your free testosterone levels. If you don�t check your SHBG, your total testosterone levels might be normal but your free testosterone levels might be too low.
By way of instance, SHBG is similar to a bus filled with many workers. In this case, the workers are testosterone. When we have too many buses, the majority of the workers will stay on the bus while only a few will be out doing their job. A man can have a total testosterone level of 700, however, if they have a free testosterone level of only 5, they�re bound to still feel like they have a total testosterone level of 300.
In summary, we want to make sure that our total testosterone level is over 500 or better, over 600 and we also want to make sure that our free testosterone level is between 15 and 20.
Another hormone you might want to make sure you get tested for is known as dehydroepiandrosterone, or DHEA. DHEA is a precursor hormone for testosterone. It�s also an adrenal hormone, however, we will discuss this later in another article. If an individual�s DHEA is too low, it can indicate that the adrenal glands, which are in charge of the human body�s stress response, may not be functioning appropriately. DHEA levels should be between two to 400.
DHEA, or dehydroepiandrosterone, can be supplemented directly. Many doctors and functional medicine practitioners may also implement stress-relieving methods and techniques into your life, such as mindfulness meditation and yoga, to treat the source of the health issue. Herbal supplements can also help regulate DHEA as well as testosterone levels.
Now, we will discuss a fundamental hormone that is generally only considered to be important in female health, however, this hormone also plays an essential role in men; estrogen. Estrogen helps maintain a healthy sex function as it promotes your libido. It is also protective for the brain. In men�s health, estrogen is often demonized because it can cause health issues like breast development if estrogen levels are too high in men. But, normal estrogen levels are fundamental towards maintaining hormone balance as well as mental health.
Estrogen can increase in men with diabetes and obesity. Elevated insulin exchanges more testosterone into estrogen which may cause additional symptoms like fatigue. This can also create more problems alongside sexual dysfunction, including hair loss. So, if you have less than optimal testosterone levels, you should seek help from a doctor or functional medicine practitioner to find out why. And looking at your estrogen levels is a great place to start.
There are two types of estrogen tests which can help demonstrate your estradiol and estrone levels. These are important markers to look at because one can be elevated while the other can be in the normal range. The brain is the other place you can look at to determine your estrogen levels. Your brain produces hormones which can stimulate sex hormones, such as the follicle stimulating hormone, or FSH, and the luteinizing hormone, or LH, which helps produce testosterone and sperm within the testicles. If your LH is low, then your low testosterone levels may be caused by a brain health issue. However, it�s much more likely that sugar and starch consumption may be causing hormonal imbalances in your sex hormones.
Approximately 70 percent of the testosterone deficiencies in the United States are associated with insulin resistance due to diabetes and obesity. So, if your diet is filled with sugar and starch or if you have belly fat, you may already have decreased testosterone levels.
Hormones are secreted directly into the blood stream in order to control a variety of bodily functions. These can affect growth and development, mood, sexual function, reproduction, and metabolism. As a fundamental part of the endocrine system, hormone imbalances can have a tremendous effect on our overall health and wellness. Men’s hormones, by way of instance, can significantly impact a man’s quality of life. Research studies have demonstrated that decreased testosterone in men can cause a variety of health issues. Evaluating sex hormones in both men and women is essential towards overall health and wellness. Dr. Alex Jimenez D.C., C.C.S.T. Insight
Understanding Men’s Hormones
While we keep discussing the importance of lab tests, we also need to keep asking ourselves why these health issues are happening in the first place. The answers trace back to the basics of health and wellness. What are you eating? Do you participate in exercise or physical activities? Do you sleep properly? Do you have stress? What are your nutrient levels? Of course, several of these answers require more evaluations. That�s why I highly recommend you find a functional medicine doctor who can help get you on the right path towards optimal health and wellness. Most of the time, basic lifestyle modifications including diet, exercise, stress management, sleep and supplements can help. Other times you may need hormone replacement therapy.
The scope of our information is limited to chiropractic and spinal health issues as well as functional medicine topics and discussions. To further discuss the subject matter, please feel free to ask Dr. Alex Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topic Discussion:�Acute Back Pain
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download
* All the above XYMOGEN policies remain strictly in force.
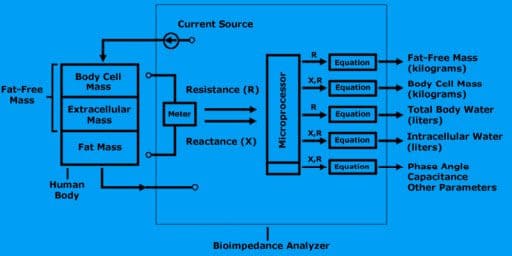
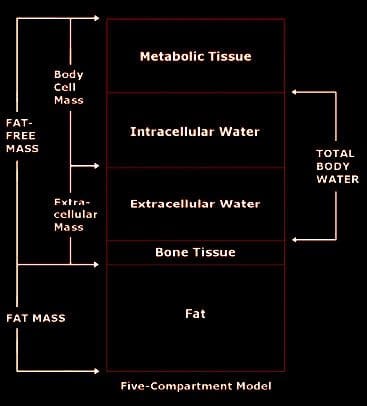
Bioimpedance Analysis (BIA) is defined as the analysis of resistance and reactance in the human body.
Energy dissipation is called resistance (R).
Energy storage is called reactance (X).
Units of resistance and reactance are called ohms.
Resistance and reactance taken together create impedance (Z).
Fat-free mass in the human body is proportional to its resistance.
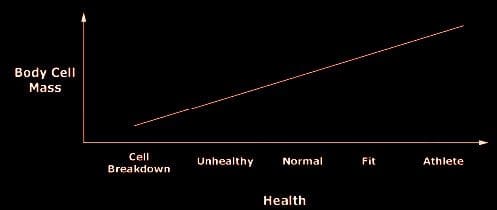
Body cell mass is proportional to its reactance.
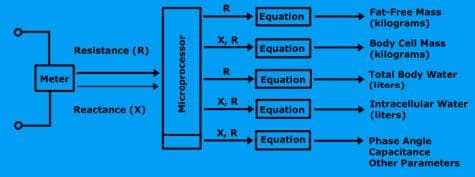
A bioimpedance analyzer is a device that contains a highly precise frequency meter, a processor, and a printer. The meter is called an impedance meter. It measures resistance and reactance.
The microprocessor computes the size of the fat-free mass and body cell mass along with all subsequent calculations.
A bioimpedance analyzer measures resistance and reactance, computes fat-free mass, body cell mass, total body water, and intracellular water.
To measure resistance and reactance, the bioimpedance analyzer generates a small electrical current to the body.
Contents
Measurements
Bioimpedance analysis is an assessment of change in electrical tissue conductivity, which indicates altered body composition.
The following electrical characteristics are measured and used to evaluate body composition.
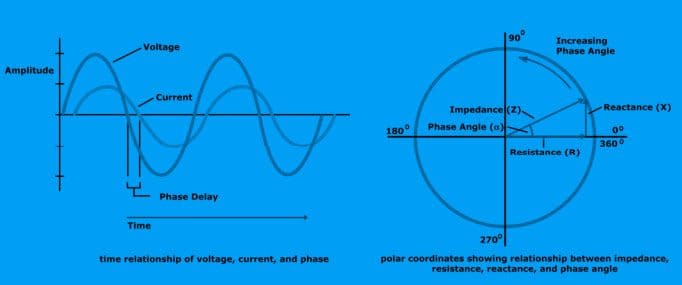
Impedance (Z)
Impedance is a measurement of a medium to conduct current. It is a ratio of voltage injected current in a conductive medium and has two components: resistance and reactance.
Resistance (R)
Resistance is the component of impedance related to the dissipation of energy.
Reactance (X)
Reactance is the component of impedance related to the storage of energy.
Phase angle is a time delay between stimulating current and the voltage generated by an alternating current. The phase angle is expressed in degrees.
Electrical characteristics and their relation to each other?
The time relationship of voltage, current, and phase is shown below.
The Circuit
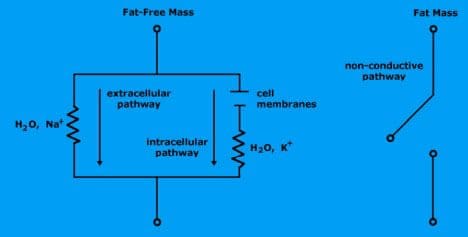
Water is the body’s conductor and determines the resistance.
Electrolytic fluid in fat-free mass consists of water and charged ions that conduct electrical current.
Extracellular fluid (water and ionized sodium Na+) provides a low-resistance pathway.
Intracellular fluid (water and ionized potassium K+) provides a low-resistance pathway.
Fat mass is non-conductive because there is no water.
Cell membranes within intracellular mass determine reactance.
The cell membranes consist of a layer of nonconductive, lipophilic material interposed between two layers of conductive molecules. They are tiny capacitors that store electrical charge.
Extracellular pathway (which is sodium ionized water) is represented by single resistance.
Intracellular pathway (potassium ionized water and cell membranes) is represented by resistance and reactance.
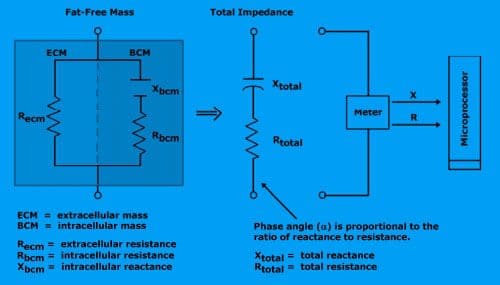
Total resistance is proportional to the amount of fat-free mass.
Reactance is proportional to body cell mass (intracellular mass).
The meter reports total resistance and total reactance to the microprocessor.
Equation for Regression
Bioimpedance analyzers use algorithms to compute amounts of fat-free mass, body cell mass, body water, and intracellular water.
What is the regression equation?
This equation is a mathematical formula that predicts the relationship between two or more variables based on the analysis of data.
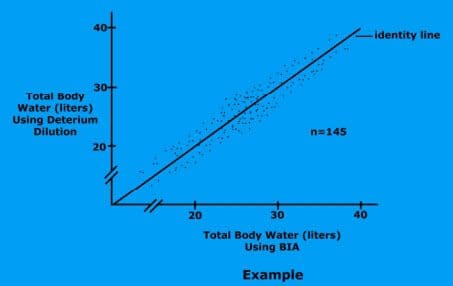
For example, total body water�regression�equation
(TBW) = form:
TBW = a * Ht2 / R + b * Weight + c * Age + d
The terms are Ht2 / R, Weight, and Age.
The weighting constants are a, b, c, and d.
Resistance, height, weight, gender, and age are supplied for each subject. A computer then generates an algorithm which best describes the relationship between TBW, resistance, height, weight, gender, and age.
This is called Regression Analysis.
How do you use regression equations?
Once the bioimpedance analyzer measures the resistance and reactance, the results are sent to the microprocessor to perform the calculations. All the equations, (FFM, BCM, TBW, and ICW) are encoded into the analyzer’s software.
Diagram
Fat-Free Mass
Fat-free mass is derived by applying a small alternating current to the body.
The resistance of the body is measured using the measured resistance (R), the analyzer estimates the fat-free mass.
Body Cell Mass
Body cell mass is derived by measuring both the resistance (R) and reactance (X) of the body. With this measurement, the analyzer estimates body cell mass.
Total Body Water
Using the measured resistance, the analyzer estimates total body water.
Intracellular Water
Using the measured resistance and reactance, the analyzer estimates intracellular water.
If you�ve been experiencing lower back pain and can�t seem to pinpoint the cause, try looking down � at your feet. What kind of shoes are you wearing? Your shoes can have a tremendous effect on your spine, causing back pain. While this is traditionally considered to be a �female issue,� some men�s shoe styles are unsafe as well. Take a look at the most common culprits and find out how you can be safely shod.
Contents
The Truth About High Heels
Wearing high heels puts your body in a position that is very similar to walking on a ramp. It causes your calf muscles to stay in a constantly flexed position and increases fatigue throughout the lower body. What�s worse, though, is that high heels cause your entire posture to change, they:
Thrust your chest forward
Push your lower back forward
Tilt your pelvis up so the spine and hips are out of alignment
Put excessive pressure on the knees
Tendons get thicker and calf muscles get shorter
Shift your weight to the balls of your feet with increased downward force pressure
Extended regular wear can actually cause your anatomy to change
Wearing high heels for even a few hours can cause lower back pain. Wearing them regularly can have a detrimental effect on your body. This does not take into account the increased risk of falls and twisted ankles.
Why Flip Flops are a Flop
Flip flops are a popular summer shoe. They are easy to slip on and take off, they�re cool and fairly comfortable. Most even stand up to getting wet without damage. However, you may be sacrificing your safety and spine health for choosing these easy to wear shoes.
The biggest problem is, they do not offer any ankle or foot support � none at all. The cushioning is minimal at best and they aren�t really secure on your foot. All of this leaves you vulnerable to trips and falls � a leading cause of injury and death in the United States. It also leaves you vulnerable to back pain and spinal injury.
There are several problems with wearing flip-flops, especially on a regular basis:
You have to unnaturally shorten your stride
You have to curl or pinch your toes to keep your shoes on while you walk
Your foot contacts the ground in an unnatural way that causes your leg to rotate slightly
All of these things put pressure on your spine, causing unusual strain on your hips, knees, feet, and lower back. It can cause muscular pain and strain, but it can also cause misalignment of your spine.
So, are Flat Shoes Better?
When compared to high heels, flat shoes are much better, especially when it comes to posture. Flats keep your spine pretty straight and your calf muscles are relaxed. They also help to distribute your body weight more evenly through your whole foot as opposed to pushing it to the balls of the feet. However, not all flat shoes are created equal. For instance, flip flops are flat, but we know that they are bad for your body, so be careful when choosing your flat footwear.
Throughout the course of the day, your foot naturally expands. Go shoe shopping in the afternoon to get a more accurate fit.
Get your feet measured every time you buy shoes.
Always try on new shoes, walk around in them and stand.
When determining length and width, do it while standing.
Look for shoes that provide foot support and have arch support.
Don�t get shoes that are too wide or too narrow � or too long or short.
Look at both size and width. Going up a half a size may not necessarily mean a shoe is wide enough if the shoes you are trying on pinch.
Speaking of size, let it be a guide, not a rule. Gauge your shoe size by your comfort, not a number.
Feel the insides of the shoes, along the heel and down to the toe to make sure that there are no seams, tags, or anything else that will affect your comfort or rub your foot.
Check the shoe for sturdiness and soundness. Is the sole thick? Does the sole adhere well to the shoe (no gaps or loose spots)? Is the shoe made from durable, quality material?
Shoes are not accessories, they are tools that help protect much more than just your feet. Wear them well.
Sports Injury Rehabilitation Chiropractor | El Paso, Tx (Best)
El Doctor de Medicina Funcional Explica la Nutrici�n
Cada reacci�n qu�mica que ocurre en el cuerpo humano requiere de enzimas y cada uno de estos procesos necesita una coenzima. Pero �qu� son las coenzimas? Son vitaminas y minerales. Aproximadamente 37 billones, billones de reacciones qu�micas ocurren en el cuerpo humano cada segundo.
Es por eso que una nutrici�n adecuada y una dieta balanceada rica en alimentos integrales con vitaminas y minerales es fundamental para la salud y el bienestar general. La mayor�a de las personas en los Estados Unidos son deficientes en vitaminas y / o minerales. Pero, �c�mo sabes si eres parte del 90 por ciento de las personas con suficientes deficiencias para desarrollar una enfermedad? Discutiremos las pruebas que puede realizar para averiguar si tiene deficiencia de vitaminas y / o minerales y qu� puede hacer al respecto.
Contents
�Que es la Nutrici�n?
Hola, bienvenidos a la tercera parte de “C�mo Tomar el Control de su Salud”. Hoy, discutiremos uno de los temas mas divertidos de la medicina funcional: la nutrici�n. Desafortunadamente, la nutrici�n es una de las conversaciones m�s importantes que muchos doctores no est�n dispuestos a tener con sus pacientes. El doctor promedio aprende sobre las enfermedades y la desnutrici�n en lugar de aprender c�mo usar la nutrici�n como tratamiento o incluso c�mo usar terapias nutricionales para lograr salud y bienestar �ptimos.
Personalmente creo que la comida puede ser utilizada como una forma de medicina. Que deber�a ser la base de la pr�ctica m�dica, no una idea tard�a en la medicina. No hay mejor tratamiento que la nutrici�n adecuada. Aproximadamente el 90 por ciento de las personas en los Estados Unidos no obtienen los nutrientes esenciales que necesitan para las funciones corporales saludables. Y m�s que eso probablemente no est� obteniendo suficientes nutrientes para prevenir enfermedades asociadas con deficiencias nutricionales. Sin embargo, �qu� se necesita para lograr un bienestar �ptimo? M�s del 98 por ciento de los estadounidenses son deficientes en omega-3, 80 por ciento en vitamina D, 50 por ciento en magnesio y 10 por ciento en vitamina C. Las deficiencias de nutrientes tambi�n pueden seguir causando problemas de salud durante a�os.
Las enfermedades agudas, como el raquitismo, el escorbuto, el beriberi o la anemia por deficiencia de hierro, suelen ser los problemas de salud m�s comentados asociados con las deficiencias de nutrientes. Sin embargo, tambi�n se conocen como enfermedades de deficiencia de latencia prolongada. Entonces, �cu�nta vitamina D necesitamos para no tener raquitismo? No mucho, solo 30 unidades realmente. �Y cu�nto necesitamos para no tener osteoporosis? Tal vez unas 3,000 a 4,000 unidades por d�a. Ahora, �cu�nto folato necesitamos para no tener anemia? Tambi�n no mucho. Pero, �cu�nto necesitamos para prevenir las enfermedades card�acas, el c�ncer y la demencia? Definitivamente se necesitan muchas m�s unidades por d�a.
Cada reacci�n qu�mica que ocurre en el cuerpo humano requiere enzimas y cada uno de estos procesos necesita una coenzima. Pero �qu� son las coenzimas? Son vitaminas y minerales. Aproximadamente 37 billones, billones de reacciones qu�micas ocurren en el cuerpo humano cada segundo.
Es por eso que una nutrici�n adecuada y una dieta balanceada rica en alimentos integrales con vitaminas y minerales es fundamental para la salud y el bienestar general. La mayor�a de las personas en los Estados Unidos son deficientes en vitaminas y / o minerales. Pero, �c�mo sabes si eres parte del 90 por ciento de las personas con suficientes deficiencias para desarrollar una enfermedad? S�lo hay varios nutrientes que generalmente se analizan. Y para la mayor�a de estos, los doctores no son conscientes de cu�les deber�an ser los valores �ptimos, lo que puede dificultar mucho la correcci�n de la deficiencia de nutrientes.
Tomando el Control de su Nutrici�n
Uno de los nutrientes m�s fundamentales que se necesita medir es la vitamina D. Aunque se le conoce como una vitamina, en realidad es m�s como una hormona y se produce por parte del colesterol. Esta es otra raz�n por la cual el colesterol es esencial. Aproximadamente el 80 por ciento de la poblaci�n tiene una deficiencia de vitamina D. A menos que est� al sol 20 minutos todos los d�as entre las 10:00 am y las 2:00 pm, es posible que deba tomar suplementos de vitamina D. Para complementar adecuadamente, necesitamos saber desde qu� nivel est� comenzando desde un principio. A modo de ejemplo, los niveles �ptimos de vitamina D deben de ser entre 50 y 80 nanogramos por mililitro de sangre. La cantidad recomendada de vitamina D que podemos complementar es de aproximadamente 2,000 a 4,000 unidades.
Si tiene niveles m�s bajos de vitamina D o si tiene problemas gen�ticos, es posible que necesite un suplemento con hasta 10,000 unidades de vitamina D. Por eso es fundamental trabajar con un doctor o especialista de medicina funcional que pueda medir y evaluar sus niveles de nutrients, as� como ayudarles a optimizarlos. La mayor�a de los suplementos contienen aproximadamente 400 unidades, que es 10 veces menos que la cantidad que la mayor�a de nosotros necesitamos. Los niveles comunes son generalmente un poco m�s de 20. Esto es demasiado bajo. En un estudio de investigaci�n, las mujeres con niveles de vitamina D entre 45 y 60 experimentaron una reducci�n en los partos prematuros hasta de un 60 por ciento. La vitamina D tambi�n es esencial para ayudar a desarrollar huesos y m�sculos fuertes, mejorar la funci�n del sistema inmunol�gico, prevenir el c�ncer asi como para ayudarlo a vivir m�s tiempo. Es incre�ble.
Otra medida o prueba realizada por la mayor�a de los doctores, pero que no siempre se interpreta correctamente, se conoce como MCV o volumen corpuscular medio. La medida de MCV eval�a el tama�o de sus gl�bulos rojos en una prueba llamada CBC, o hemograma completo, que es uno de los paneles de sangre m�s comunes solicitados por profesionales de la salud. Por lo tanto, si usted es deficiente en nutrientes, sus c�lulas pueden hacerse m�s peque�as o m�s grandes. A modo de ejemplo, si sus c�lulas son demasiado grandes, podr�an ser signos de una deficiencia de folato o vitamina B12.
Las vitaminas B son esenciales en numerosas reacciones qu�micas en el cuerpo humano. Nos ayudan a producir energ�a y nos ayudan a regular la expresi�n gen�tica para crear prote�nas que aseguran nuestra salud y bienestar en general. Si nuestras vitaminas B estan demasiado bajas, eventualmente podr�amos desarrollar una deficiencia de hierro, anemia o incluso podr�a causar un trastorno gen�tico.
Los niveles �ptimos de vitaminas B deben estar entre 80 y 90. Los suplementos vitam�nicos del complejo B pueden ayudar a optimizar f�cilmente los niveles de vitaminas B. Pero, �por qu� alguien ser�a deficiente en vitaminas B? �Acaso su dieta no les proporciona suficientes nutrientes? �Son veganos? �Est�n tomando medicamentos que evitan la absorci�n de la vitamina B12? Adem�s, las vitaminas B se agotan en momentos de gran estr�s que, como quiropr�ctico, puedo decir que le sucede con frecuencia a la mayor�a de la poblaci�n en los Estados Unidos.
El MCV no es la �nica medida o prueba que eval�a los niveles de vitaminas B de un paciente. La homociste�na es un marcador alternativo que analizaremos en futuros art�culos que demuestran los niveles de B6, folato y B12. Sin embargo, tanto el MCV como la medida o prueba de homociste�na solo demuestran que uno o m�s de estos nutrientes pueden ser deficientes. No necesariamente nos dice cu�l. Por lo tanto, se pueden requerir algunas evaluaciones adicionales de seguimiento.
La medida o prueba del MMA, o �cido metilmal�nico, tambi�n muestra los niveles de vitamina B12. La vitamina B12 es esencial para muchos procesos en el cuerpo humano, incluida la producci�n de energ�a, la expresi�n de genes, la metilaci�n, la funci�n nerviosa y el estado de �nimo, entre muchos otros procesos. Los veganos tienen una mayor probabilidad de desarrollar una deficiencia de B12 porque este solo se encuentra en los productos animales. El folato es otra vitamina B fundamental. Se puede determinar directamente en la sangre, pero la homociste�na es un marcador m�s preciso para los niveles de folato.
En esta secci�n, tambi�n hablaremos sobre gen�tica porque existe una medida o prueba que puede demostrar mucho m�s con respecto al estado de sus vitaminas B y su capacidad para utilizarlas. Nuestros genes son capaces de producir prote�nas. Tenemos aproximadamente 20,000 genes que est�n dise�ados para crear prote�nas. Y un tercio de todas las prote�nas que producen son para nuestras enzimas. Las enzimas convierten los nutrientes en otros nutrientes. Estas enzimas tambi�n dependen en gran cantidad de ciertos nutrientes espec�ficos. Uno de los genes m�s fundamentales que pueden verse afectados es conocido como MTHFR o metilentetrahidrofolato reductasa. Pero puedes llamarlo MTHFR.
El MTHFR es esencial porque ayuda a regular la metilaci�n, la homociste�na y el folato, que son vitales para nuestra salud y bienestar general. Cuando se tienen niveles elevados de homociste�na, se debe verificar su estado de metilaci�n buscando el gen MTHFR a trav�s de un simple an�lisis de sangre.
La metilaci�n es un proceso bioqu�mico clave que es fundamental para la funci�n adecuada de la mayor�a de los sistemas del cuerpo humano. Se dispara miles de millones de veces cada segundo. Y ayuda a controlar la homociste�na, una sustancia que puede da�ar los vasos sangu�neos y se ha asociado con la demencia, asi como enfermedades card�acas y c�ncer, entre otros problemas de salud. La metilaci�n tambi�n ayuda a reparar su ADN de manera regular, ya que ayuda a reciclar las mol�culas necesarias para la desintoxicaci�n o para eliminar las toxinas. Tambi�n ayuda a controlar su estado de �nimo y ayuda a controlar la inflamaci�n. La metilaci�n es vital.
Pero, para asegurarse de que su metilaci�n est� activa, el cuerpo humano necesita niveles �ptimos de vitaminas B. Sin suficientes vitaminas B, el proceso de metilaci�n se puede descomponer y los efectos pueden ser destructivos. Aqu� es donde comenzamos a ver un aumento en los defectos cong�nitos, como la espina b�fida, el s�ndrome de down y m�s abortos involuntarios.
MTHFR es frecuentemente anormal en aproximadamente el 35 por ciento de la poblaci�n. La descomposici�n de la metilaci�n tambi�n puede aumentar el riesgo de desarrollar problemas de salud como la osteoporosis y la diabetes, la displasia cervical o el c�ncer, incluido el c�ncer de colon y el c�ncer de pulm�n, e incluso la depresi�n, la disfunci�n cognitiva pedi�trica, as� como los trastornos del humor y del comportamiento, la demencia y los problemas cerebrovasculares. La metilaci�n es verdaderamente un proceso bioqu�mico clave.
Cuando hablamos de la gen�tica, debemos entender que nuestro entorno puede alterar nuestros genes. Entonces, �qu� pasa si tienes una variaci�n MTHFR en tus genes? En primer lugar, no todas las mutaciones causan problemas de salud. Una mutaci�n, por modo de ejemplo, conocida como C677T, es una versi�n del gen que es m�s significativa que otra versi�n del gen, conocida como A1298C. Ahora no hay que preocuparse por estas variaciones gen�ticas. Sirven como ejemplos para demostrarle la calidad de estas mutaciones y c�mo funcionan. Las personas con estas variaciones del gen, por ejemplo, solo pueden necesitar m�s folato o pueden necesitar un tipo particular de folato conocido como metilfolato. Aqu� es donde un practicante de medicina funcional puede ayudarle a sus pacientes.
Una prueba gen�tica puede hacerle saber si tiene una de estas variaciones gen�ticas. Pero, no te estreses. Hay mucho que puede hacer para optimizar su salud y bienestar en general. Muchos pacientes han visitado mi consultorio despu�s de descubrir que tienen estas variaciones en sus genes. Y aprenden r�pidamente que tienen la opci�n de tomar el control de su bienestar. Sin embargo, lo que controlas no son tus genes, controlas tu expresi�n gen�tica.
Si alteras tus h�bitos alimenticios, alteras tus nutrientes. Si altera su entorno, altera qu� genes se activan y cu�les se vuelven inactivos. Y con estas mutaciones, puedes hacer casi lo mismo simplemente siguiendo una nutrici�n adecuada. Cuando encuentre un m�dico o practicante de medicina funcional que est� dispuesto a trabajar con usted, le dir�n qu� modificaciones de estilo de vida debe seguir para prevenir problemas de salud.
Por lo tanto, acabamos de discutir las vitaminas B. A continuaci�n, discutiremos otro nutriente fundamental en el cuerpo humano: el magnesio. El magnesio es un mineral s�per esencial. Aproximadamente el 48 por ciento de las personas en los Estados Unidos consumen menos de la cantidad requerida de magnesio en los alimentos. El magnesio es necesario en m�s de 300 reacciones qu�micas en el cuerpo humano. Tambi�n es fundamental en la producci�n de ATP, o la energ�a que el cuerpo humano utiliza como combustible.
Una prueba o medida del nivel de magnesio en la sangre puede ayudar a determinar si usted tiene una deficiencia. El magnesio tambi�n puede ayudar a reducir la ansiedad, calmar el sistema nervioso y mejorar el sue�o. Tambi�n es un nutriente esencial en el manejo de los niveles de az�car en la sangre. Si un profesional de la salud le ha dicho que tiene un nivel promedio de az�car en la sangre de m�s de cinco y medio, algo conocido como A1c, entonces el magnesio puede ayudar.
Adem�s, es muy f�cil saber si tiene una deficiencia de magnesio al observar su dieta y s�ntomas actuales. �Come suficientes alimentos ricos en magnesio como verduras de hojas verdes, frijoles, nueces y semillas? �O come muchos alimentos procesados? Quiz�s tambi�n tenga s�ntomas como ansiedad, insomnio, estre�imiento, contracciones musculares, calambres musculares, s�ndrome premenstrual y palpitaciones. Si tiene uno o m�s de los s�ntomas que acabo de mencionar, es posible que tenga una deficiencia de magnesio.
A continuaci�n, hablaremos sobre el zinc, el mineral que estimula la inmunidad y la testosterona en el cuerpo humano. Este importante nutriente se encarga de mantener el volumen de su cabello, as� como de reparar su tracto gastrointestinal. Tambi�n es responsable de asegurarse de que su tiroides funcione correctamente. El zinc puede medirse o analizarse f�cilmente en la sangre y, desafortunadamente, es otro nutriente de el que tenemos una gran deficiencia en los Estados Unidos. Adem�s, tambi�n se pueden observar sus niveles de fosfatasa alcalina, que pueden calcularse a trav�s de una evaluaci�n de la funci�n hep�tica en un panel de sangre regular. Los niveles altos de fosfatasa alcalina pueden indicar la presencia de c�ncer o problemas �seos, entre otros problemas de salud; sin embargo, los niveles bajos de fosfatasa alcalina pueden indicar una deficiencia de zinc, ya que es una enzima dependiente de zinc.
Finalmente, el �ltimo nutriente fundamental de el que vamos a discutir es el hierro. El hierro es frecuentemente deficiente en veganos y vegetarianos, o en mujeres en general debido a la menstruaci�n. El hierro es necesario para transportar ox�geno a trav�s del cuerpo humano y es esencial para la salud y el bienestar del cerebro. El hierro tambi�n es importante para el cabello y las u�as, el sue�o y muchas otras cosas.
La ferritina es un tipo de hierro almacenado y es este nutriente el que ayuda a ver tus niveles de hierro. Los niveles �ptimos de ferritina deben estar entre 50 y 150 en las mujeres y entre 100 y 300 en los hombres. Muchas veces he visto a mujeres visitar mi oficina con niveles de ferritina de menos de 50, o peor, de un solo d�gito. Esto se debe a que las mujeres premenop�usicas pierden sangre cada mes debido a sus ciclos menstruales y se les hace mucho m�s dif�cil mantener los niveles adecuados de ferritina. Muchas mujeres tambi�n comen mucho menos de lo que se supone que deben comer todos los d�as. Los altos niveles de ferritina, por otro lado, podr�an ser un signo de inflamaci�n, generalmente causada por la resistencia de la insulina al az�car, o podr�a ser un signo de hemocromatosis o enfermedad por almacenamiento de hierro, un trastorno gen�tico que puede ser muy peligroso.
Tener niveles reducidos de ferritina tambi�n puede hacer que se sienta cansado, y puede causar p�rdida de cabello, al igual que puede causar insomnio. Entonces, incluso si su recuento sangu�neo es normal, si sus niveles de ferritina son bajos o sus niveles de hierro son bajos, tambi�n puede causar estos s�ntomas. Por eso, si experimenta s�ntomas de fatiga, es esencial medir o probar sus niveles de ferritina. Y se puede complementar f�cilmente.
Aparte de la ferritina, un MCV bajo tambi�n puede determinar si usted tiene una deficiencia de hierro. Las deficiencias de hierro pueden hacer que los gl�bulos rojos se vuelvan muy peque�os y eso se puede demostrar en los niveles bajos de MCV, que eval�an el tama�o de sus gl�bulos rojos. Adem�s, la saturaci�n de transferencia, el hierro s�rico, la TIBC o la capacidad de uni�n al hierro total, y la hemoglobina, pueden brindarnos un an�lisis m�s profundo del estado de su hierro para distinguir las diferentes causas de la anemia. Estos se incluyen en un panel de sangre de hierro regular en una prueba de laboratorio.
Hemos discutido varios nutrientes que pueden ser solicitados por la mayor�a de los profesionales de la salud con acceso a pruebas de laboratorio convencionales. Adem�s, hay otra prueba que nos puede dar m�s informaci�n sobre qu� tipo de nutrientes necesitamos en funci�n de nuestros genes. Se llama la prueba de salud de ADN y es proporcionada por una compa��a llamada DNAlife. Esta prueba eval�a una variedad de marcadores gen�ticos asociados con la desintoxicaci�n, el metabolismo de los l�pidos y la inflamaci�n, incluido el gen MTHFR y otros marcadores de vitamina B. Ahora, DNA Health demuestra los diferentes genes que evaluamos. Y la mayor�a de estos son genes comunes, son aquellos sobre los que podemos hacer algo. Analizamos los genes que podemos cambiar seg�n su nutrici�n y otros factores del estilo de vida.
El gen MTHFR nos muestra otros marcadores de vitamina B, genes que controlan B6, folato y B12, adem�s de demostrar c�mo funcionan y si usted tiene deficiencias de nutrientes. Luego, nos indica qu� nutrientes necesitar� complementar y cu�nto le daremos. Es tremendamente �til.
Hubo un individuo que ten�a dos variables del gen MTHFR. Esta mujer tuvo un aborto involuntario tras otro aborto involuntario tras otro aborto involuntario. Visit� a su m�dico para una evaluaci�n y result� que ten�a una mutaci�n reguladora del folato. Entonces, su m�dico comenz� a darle la cantidad adecuada de folato que necesitaba y ella comenz� a tener beb�s sanos. A veces, la nutrici�n puede ser asi de poderosa para mejorar la salud y el bienestar general del paciente.
La prueba de salud del ADN puede ayudar a personalizar su enfoque al optimizar su bienestar basado en su gen�tica. Lo que medimos utilizando la prueba de salud del ADN proporciona informaci�n bien establecida acerca de sus genes y lo que puede hacer al respecto.
Una prueba de micronutrientes conocida como el perfil de nutrici�n optimizado individualizado o el panel ION, son opciones de prueba alternativas que tambi�n pueden proporcionar informaci�n sobre su estado nutricional actual. Esta prueba es de Genova. Esta es una prueba s�lida que mide todas las vitaminas y minerales esenciales, �cidos grasos, �cidos org�nicos y antioxidantes que tiene actualmente. Esta prueba busca desequilibrios, insuficiencias o deficiencias, en lugar de buscar una enfermedad espec�fica. Busca cosas que la mayor�a de los m�dicos nunca buscan.
Los profesionales de la medicina funcional o los m�dicos observan los niveles de amino�cidos, niveles de minerales e incluso los niveles de toxinas de los metales pesados ??como mercurio, plomo, ars�nico y muchos m�s. Tambi�n analizamos sus niveles de antioxidantes, niveles de vitamina A y vitamina E, as� como su antioxidante CoQ10 y el estado de betacaroteno. Podemos determinar si una persona come verduras o no si, a modo de ejemplo, tienen niveles bajos de betacaroteno. Tambi�n analizamos los niveles de vitamina D, �cidos grasos esenciales, incluidas las grasas omega-3 y las grasas omega-6. Podemos determinar si una persona come comida chatarra. Podemos determinar si una persona est� comiendo pescado. Y podemos determinar si una persona est� comiendo demasiado aceite de oliva o grasas saturadas. Todo est� demostrado en estas medidas y pruebas.
Una prueba OAT, o prueba de �cidos org�nicos, tambi�n analiza lo que se conoce como �cidos org�nicos. Esta prueba demuestra una amplia gama de par�metros asociados con sus mitocondrias, que analizaremos en el siguiente art�culo, sus vitaminas B, sus neurotransmisores, su flora intestinal y su desintoxicaci�n. En �ltima instancia, es un examen completo que me muestra si un paciente est� bien o enfermo. Me muestra d�nde est�n los desequilibrios y d�nde debo recomendar modificaciones en su estilo de vida. Tambi�n ayuda a proporcionar pistas sobre otros problemas de salud.
A modo de ejemplo, si sus mitocondrias no funcionan correctamente porque tiene niveles reducidos de amino�cidos esenciales o si tiene un mayor estr�s oxidativo o si simplemente tiene niveles bajos de selenio y zinc, existe la posibilidad de que tenga alg�n tipo de sobrecarga t�xica por metales pesados. Y eso es precisamente lo que ir�a buscando. Los signos como estos proporcionan mucha informaci�n sobre lo que podemos hacer para tratar a un paciente. Y un m�dico o practicante de medicina funcional con experiencia puede determinar qu� est� pasando realmente con un paciente o puede ayudar a los pacientes a descubrir c�mo optimizar su salud y bienestar en general.
La nutrici�n es el estudio de los nutrientes en los alimentos y c�mo el cuerpo humano utiliza los nutrientes, as� como la relaci�n entre la dieta, las enfermedades, la salud y el bienestar en general. Los nutrientes son una fuente de nutrici�n, incluidos los carbohidratos, prote�nas, grasas, vitaminas, minerales, fibra y agua. La medicina funcional se enfoca en el uso de alimentos como una forma de medicina. Una nutrici�n equilibrada puede ayudar a prevenir y tratar una variedad de problemas de salud. De manera similar, la nutrici�n en la medicina funcional implica c�mo ciertas enfermedades y condiciones pueden estar asociadas con factores diet�ticos, como una mala alimentaci�n o malnutrici�n, alergias a los alimentos e intolerancias a los alimentos. Dr. Alex Jimenez D.C, C.C.S.T.
Entendiendo su Nutrici�n
Como buenos doctores de medicina funcional, a menudo nos preguntamos, �por qu� es que tantas personas en los Estados Unidos est�n sobrealimentadas pero desnutridas? O, �por qu� es que los estadounidenses comen demasiadas calor�as y muy pocos nutrientes? Las principales causas de las deficiencias nutricionales generalizadas son las siguientes: Primero, los humanos evolucionaron de comer alimentos silvestres que conten�an niveles tremendamente m�s altos de nutrientes. Segundo, el suelo que utilizamos actualmente para cultivar nuestros cultivos se ha agotado en gran medida de nutrientes. Las t�cnicas de hibridaci�n de la agricultura industrial est�n produciendo animales y vegetales para tener niveles reducidos de nutrientes. Tercero, los alimentos procesados ??no tienen absolutamente ning�n nutriente, por lo que con frecuencia tienen que ser fortificados. Y por �ltimo, pero no menos importante, la exposici�n a las toxinas ambientales, la falta de luz solar, el estr�s cr�nico y la mala alimentaci�n, incluido el aumento del consumo de alcohol, cafe�na y az�car, pueden aumentar nuestras necesidades nutricionales, muchas de las cuales ya no estamos obteniendo lo suficiente de nuestra dieta.
Bueno, es posible que no necesite ninguna vitamina, sin embargo, si puede cumplir con ciertas condiciones. Tal vez si solo cazara y recolectara alimentos silvestres y no estuviera expuesto a toxinas ambientales. O tal vez si se acostaba con el sol y se despertara con el sol, durmiendo nueve horas por noche. Y si no experimenta absolutamente ninguna cantidad de estr�s cr�nico. En �ltima instancia, si solo bebe agua pura y limpia y respira aire puro y limpio. Entonces, probablemente no necesitar�a vitaminas. Pero el resto de nosotros que no seguimos estas condiciones, si las necesitamos.
Y con ese pensamiento, terminamos este art�culo. En el pr�ximo art�culo, hablaremos de hormonas. Las hormonas pueden afectar casi todos los aspectos de nuestro bienestar, y muchos profesionales de la salud no entienden cu�les deben ser nuestros niveles hormonales �ptimos o incluso cu�ndo probarlos y qu� hacer al respecto una vez que lo hacen. La medida y prueba de los niveles hormonales debe ser una pr�ctica est�ndar, y muchos pacientes nunca han tenido un panel de sangre para observar sus hormonas. Es fundamental saber y comprender lo que sucede dentro de su propio cuerpo. Y es por eso es que este pr�ximo art�culo es tan importante. No querr� perderse de nuestra pr�xima actualizaci�n. Los veo pronto. El alcance de nuestra informaci�n se limita a problemas quiropr�cticos y de salud de la columna, as� como a temas y discusiones de medicina funcional. Para seguir discutiendo el tema, no dude en preguntarle al Dr. Alex Jimenez o comun�quese con nosotros al�915-850-0900�.
Curado por el Dr. Alex Jim�nez
Discusi�n del Tema Adicional: Dolor de Espalda Agudo
El dolor de espalda es una de las causas m�s frecuentes de discapacidad y d�as perdidos en el trabajo en todo el mundo. El dolor de espalda se atribuye a la segunda raz�n m�s com�n para las visitas al consultorio del m�dico, superada �nicamente por infecciones respiratorias superiores. Aproximadamente el 80 por ciento de la poblaci�n experimentar� dolor de espalda al menos una vez a lo largo de su vida. La columna vertebral es una estructura compleja formada por huesos, articulaciones, ligamentos y m�sculos, entre otros tejidos blandos. Las lesiones y / o afecciones agravadas, como las hernias de disco, pueden provocar s�ntomas de dolor de espalda. Las lesiones deportivas o las lesiones por accidentes automovil�sticos suelen ser la causa m�s frecuente de dolor de espalda; sin embargo, a veces los movimientos m�s simples pueden tener resultados dolorosos. Afortunadamente, las opciones de tratamiento alternativo, como la atenci�n quiropr�ctica, pueden ayudar a aliviar el dolor de espalda mediante el uso de ajustes de la columna vertebral y manipulaciones manuales, lo que finalmente mejora el alivio del dolor. �
De XYMOGEN�Las f�rmulas profesionales exclusivas est�n disponibles a trav�s de profesionales de atenci�n m�dica con licencia seleccionados. La venta por internet y el descuento de f�rmulas XYMOGEN est�n estrictamente prohibidos.
Con orgullo�El Dr. Alexander Jimenez�hace que las f�rmulas de XYMOGEN est�n disponibles solo para los pacientes bajo nuestro cuidado.
Llame a nuestro consultorio para que podamos asignar una consulta m�dica para acceso inmediato.
Si eres paciente de�Injury Medical & Chiropractic�Clinic, puedes preguntar por XYMOGEN llamando�915-850-0900.
Para su conveniencia y revisi�n de la�XYMOGEN�productos por favor revise el siguiente enlace. *XYMOGEN-Descargar-Catalogo
* Todas las pol�ticas de XYMOGEN anteriores se mantienen estrictamente.
Can being grateful make you healthier? Several studies say yes. There is a great deal of evidence that shows being thankful benefits your health both physically and mentally. Researchers have found that an attitude of gratitude helps you have a stronger immune system, a healthier heart, more energy, and a happier outlook on life.
Contents
The Science of Being Thankful
When you are grateful, just like any other emotion, it affects your outlook. Gratitude is particularly powerful when used as a way of viewing the word, of interpreting and perceiving your life. Other positive emotions come attached to appreciation and these work in the body to provide powerful physical health benefits.
According to research, the simple act of thinking about the things you are grateful for, causes the parasympathetic nervous system, the part that promotes calm and peaceful feelings, to be triggered. This can cause chemical reactions such as increasing oxytocin (the hormone that helps with bonding in relationships and increases good feelings) while decreasing cortisol (the stress hormone that can cause a variety of health issues).
Studies on Gratefulness
Several studies have been done over the past few years exploring the connection between gratitude and health. One study published in the European Scientific Journal in June 2017, drew a direct line between appreciation and coping with PTSD. It found that the more gratitude increases in a person the less psychological distress decreases. A research report published in June 2017, found that gratitude could be a viable means for helping ease fibromyalgia symptoms. In
November 2016, the American Heart Association published information on a study that was conducted on heart patients who had asymptomatic heart failure. The researchers measured evaluated their levels of gratitude and found that the patients who were more grateful slept better, experienced less anxiety, and had decreased depression. These people also had healthier hearts and lower levels of inflammation. The lower levels of inflammation, as well as a more positive outlook, also help patients better manage pain.
7 Tips for Being more Grateful
Even if gratitude does not come naturally to you, it is possible to learn it. It can become a habit that can be cultivated and incorporated into everyday life. Try these tips for developing gratefulness in your life.
1. Think about being grateful. The more you think about it, the more you will find that you are thankful.
2. Avoid comparing up. There will always be someone who has more than you do or is more advantaged. Seeking them out and ruminating on what you don�t have or don�t have enough of is a recipe for discontent, anger, and frustration.
3. Keep a gratitude journal and write down the things you are thankful for. This will not only serve as a reminder, but it will also help to develop the habit of being grateful.
4. If you don�t think you have anything to be thankful for, find just one thing and focus on that. Gradually add items you are grateful for, and you will find them.
5. Change your perspective. When something doesn�t go your way, look for the positives in it. This can be internal or external. How did you grow? What did you gain?
6. Change your thinking. Choose positive language and banish negative language from your vocabulary. Don�t allow negativity to color your life experiences. Choose to be happy and maintain a positive outlook.
7. Say it out loud. Use your voice and tell people that you are grateful. Tell them you appreciate them, that you are thankful for things. Let yourself hear your positive words of gratitude so that it can take hold in you and become a part of who you are.
Being thankful makes you a healthier, happier person, so take some time to find several things that you�re grateful for (or a lot!). You�ll love the benefits.
Doctor de Medicina Funcional Explica los Signos Vitales
Hoy comenzaremos a analizar c�mo el espectro que la medicina actualmente considera “normal” puede no ser realmente �ptimo para su salud y bienestar general. Estos rangos de referencia pueden cambiar seg�n la edad, el sexo, la actividad f�sica y m�s. De hecho, si evalu�ramos el peso de una persona en los Estados Unidos, se considerar�a “normal” tener sobrepeso, simplemente porque el 70 por ciento de la poblaci�n tiene sobrepeso. Los rangos de referencia para las pruebas de laboratorio de hoy se basan en una poblaci�n enferma cuando debemos aspirar a un bienestar �ptimo.
Luego, les demostrar� c�mo este conocimiento puede aplicarse a las medidas m�dicas m�s b�sicas: sus signos vitales. Todo el mundo sabe que cuando se visita a un m�dico por primera vez, toman sus signos vitales, incluyendo su peso, su presi�n arterial, su frecuencia card�aca y su temperatura. Sin embargo, �su m�dico le dice lo que significan sus resultados? �C�mo puede saber si est� sano?
Contents
�Cuales�son�los�Signos�Vitales?
Hola a todos, soy el Dr. Alex Jim�nez. Bienvenidos a la parte 2 de “C�mo Tomar el Control de su Salud”. Hoy, discutiremos los rangos de referencia de laboratorio asociados con sus signos vitales. Puede que no parezca un tema interesante, pero es realmente importante para su bienestar.
La mayor�a de los m�dicos generalmente definen los resultados de las pruebas de un paciente como “normales” o “anormales”. Pero, �qu� significa exactamente “normal” y “anormal”? Normal es cuando el 95 por ciento de la poblaci�n cae dentro de un rango com�n, mientras que anormal es cuando el porcentaje restante de la poblaci�n cae fuera de ese rango com�n. Ya sea que est� sano o enfermo, joven o viejo, aunque puede haber algunas variaciones para los ni�os, normal y anormal son simplemente n�meros estad�sticos que caen dentro de dos desviaciones est�ndar.
Sin embargo, estas desviaciones est�ndar no necesariamente significan que sea �ptimo o no. Es s�lo un n�mero estad�stico, despu�s de todo. De hecho, la enfermedad puede ocurrir en personas sanas. Estos rangos de referencia de laboratorio deben definirse de acuerdo con lo que es mejor para un ser humano.
A modo de ejemplo, los niveles de vitamina D se clasifican como normales si son m�s de 20, sin embargo, los niveles ideales son m�s de 50. �Entonces por qu� se considera que 20 es “normal”? Esto se debe a que aproximadamente el 80 por ciento de la poblaci�n es deficiente en vitamina D, por lo tanto, se encuentran dentro de lo que se considera el rango “normal”. Sin embargo, esto no significa que estos niveles sean los mejores para su salud y bienestar en general. Adem�s, los niveles “normales” de az�car en la sangre se han clasificado en menos de 100, aunque sabemos que los niveles “�ptimos” de az�car en la sangre se han clasificado entre 70 y 80. Los niveles de az�car en la sangre mayores de 80 pueden tener un mayor riesgo de enfermedad. Y desafortunadamente, nuestros rangos de referencia de laboratorio “normales” no son �ptimos porque nos hemos convertido en una poblaci�n enferma. En los Estados Unidos puede considerarse “normal” tener sobrepeso porque el 70 por ciento de nuestra poblaci�n tiene sobrepeso. Pero, aunque el sobrepeso u obesidad se considera normal en los Estados Unidos, no es algo a lo que quisi�ramos aspirar. Queremos aspirar a alcanzar la salud y el bienestar general.
Ahora continuemos discutiendo el significado de lo que es normal. Muchos pacientes a menudo visitan al m�dico solo para que se les diga que sus an�lisis de laboratorio han regresado normales, sin embargo, pueden sentirse enfermos. Qu� significa eso? �Significa que est� enfermo? �Significa que est� sano? Como mencion� anteriormente, o a su m�dico le falta algo o usted est� loco, pero estoy bastante seguro de que a su m�dico le falta algo. Esta es una de las principales diferencias entre la medicina convencional y la medicina funcional. A trav�s de la medicina funcional, muchos m�dicos se enfocan en el cuidado de la salud en lugar del cuidado de la enfermedad. Estamos buscando desviaciones m�s sutiles de las �ptimas.
Hasta que su funci�n se considere anormal seg�n el est�ndar actual, es posible que sus c�lulas ya est�n muriendo. Un m�dico de medicina funcional puede revisar sus pruebas de laboratorio de manera diferente a un m�dico convencional. Esto se debe principalmente a que los rangos de referencia en los que nos enfocamos apuntan hacia una salud �ptima, no a la enfermedad. Muchos m�dicos convencionales eval�an las pruebas de laboratorio de manera diferente a los m�dicos de medicina funcional, y luego siguen un “enfoque de espera”, o lo etiquetan como “no enfermo” despu�s de la cantidad m�nima de pruebas de laboratorio. De hecho, un paciente que me visit� ten�a niveles de az�car en la sangre de 120, donde un nivel de az�car en la sangre de 126 ya se considera diabetes tipo 2. Y le dije: “�Visito a su m�dico con respecto a esto?” Y �l dijo: “S�”. Le pregunt� sobre qu� le dec�a el doctor. Y finalmente dijo: “Bueno, �l dijo que esperara hasta que yo realmente tuviera diabetes y luego volviera por medicamentos”. Y eso es lo �ltimo que queremos hacer como profesionales de la salud.
Los rangos de referencia nos dan un n�mero promedio de valores que se han registrado entre la poblaci�n general. Pero no olvidemos que los rangos de referencia “normales” son relativos. Cambian seg�n la edad, el g�nero, la actividad f�sica y m�s. Si tuviera que evaluar el peso de una persona en los Estados Unidos hoy, ser�a normal tener sobrepeso, como lo mencion�, solo porque el 70 por ciento de las personas tienen sobrepeso. Y desafortunadamente, seguimos cambiando nuestros rangos de referencia en funci�n de nuestra poblaci�n enferma. Esto no es lo que deber�amos aspirar a hacer como m�dicos. Es por esto que la medicina funcional trata al individuo, no solo a los n�meros.
Adem�s, los rangos de referencia que alguna vez se consideraron normales tambi�n pueden cambiar con el tiempo. Un ejemplo de c�mo cambian los rangos de referencia fue demostrado por una compa��a de laboratorio global conocida como LabCorp, donde recientemente cambiaron sus rangos de referencia para los niveles de testosterona masculina. Anteriormente, LabCorp consideraba que los niveles normales de testosterona para un hombre adulto estaban entre 348 y 1.197. Este valor se bas� en una poblaci�n de machos adultos saludables. Sin embargo, en 2017, bajaron los niveles normales de testosterona para un hombre adulto entre 264 y 916. Adem�s, los hombres con sobrepeso, excluyendo a los hombres obesos, probablemente se incluyeron en el estudio, lo que finalmente cambi� los rangos de referencia para los niveles de testosterona masculina. Los estudios de investigaci�n han encontrado que el exceso de grasa abdominal puede causar niveles m�s bajos de testosterona. Sin embargo, al cambiar los rangos de referencia, esto demuestra que la medicina convencional considera que los individuos con sobrepeso son parte de la norma. Pero esto no es lo que queremos. Queremos luchar por el bienestar general.
Es por esto que necesita comenzar a tomar control de su propia salud. Como una de cada dos personas tiene alg�n tipo de enfermedad cr�nica, tenemos que evaluar c�mo interpretamos las pruebas de laboratorio y c�mo �normal� puede no significar necesariamente salud y bienestar, sino simplemente un promedio para una poblaci�n enferma en crecimiento en los Estados Unidos.
Tomando el Control de sus Signos Vitales
El objetivo principal de esta serie de videos es alentarlo a que se convierta en el l�der de su propio bienestar al comprender lo que significan sus ex�menes de laboratorio, a comprender c�mo se ve el aspecto �ptimo y al comprender qu� ex�menes de laboratorio est�n dise�ados para ayudarlo a lograr una salud general y bienestar en lugar de centrarse en la enfermedad. Tambi�n me gustar�a educarlo para que pueda tomar una decisi�n informada sobre a qui�n elige para ser su m�dico o compa�ero en su viaje hacia el bienestar. Ahora veamos las medidas m�dicas m�s comunes: sus signos vitales.
Sus signos vitales son tomados inicialmente por la enfermera cuando visita al m�dico. Estos signos vitales generalmente incluyen presi�n arterial, peso, frecuencia card�aca, temperatura e incluso saturaci�n de ox�geno. Sin embargo, �esta consciente de lo que significan estos n�meros? �Ha discutido su m�dico estos n�meros con usted? �Por qu� tomar�an sus signos vitales si solo los van a apuntar y nunca los discutir�n con usted? �Los n�meros realmente demuestran su salud y bienestar? Si tiene presi�n arterial alta o un problema de ritmo card�aco, lo m�s probable es que su profesional de la salud le avise, pero de lo contrario, es posible que no descubra cu�l es el valor de sus signos vitales.
Su frecuencia card�aca es probablemente uno de los signos vitales m�s importantes que se toman durante una visita al m�dico. El pulso es una medida de qu� tan r�pido est� latiendo su coraz�n. El coraz�n humano late m�s de 115,000 veces por d�a. Entonces, si su frecuencia card�aca est� por encima de 100, entonces definimos eso como tener una frecuencia card�aca alta. Pero, si tiene una frecuencia card�aca superior a 80, eso puede aumentar su riesgo de desarrollar una enfermedad card�aca. �Qu� causa este aumento? Aunque muchos factores pueden conducir a una enfermedad cardiovascular, el estr�s es una de las causas m�s comunes porque aumenta la adrenalina y causa un aumento del ritmo card�aco y la presi�n arterial. Tomar demasiado caf�, medicamentos estimulantes como Adderall o un problema de salud de la tiroides, y el coraz�n o los pulmones hiperactivos, tambi�n pueden aumentar el riesgo de enfermedades del coraz�n.
La respuesta de lucha o escape, una reacci�n fisiol�gica que se activa en momentos de estr�s, tambi�n puede causar un aumento en la frecuencia card�aca. Cuando el ritmo card�aco de un individuo con frecuencia es superior a 80, puede ser el momento de comenzar a incorporar algunas t�cnicas de manejo del estr�s en su vida, por ejemplo, la meditaci�n consciente y otras formas de meditaci�n. El estr�s no es la �nica causa de un aumento de la frecuencia card�aca. La ansiedad, las deficiencias de magnesio, la falta de condicion y la deshidrataci�n, tambi�n pueden causar un aumento de la frecuencia card�aca. Idealmente, queremos lograr una frecuencia card�aca m�s baja, �ptimamente por debajo de 70.
En el otro lado del espectro, una disminuci�n de la frecuencia card�aca por debajo de 60 tambi�n podr�a demostrar la presencia de disfunci�n de la tiroides o una funci�n tiroidea baja. Los atletas y los corredores de distancia en realidad tienen una frecuencia card�aca baja porque est�n muy bien acondicionados. Su frecuencia card�aca puede ser tan baja, como 50 o incluso 45. Pero, si tiene una frecuencia card�aca baja y no es un atleta o un corredor de distancia, puede que sea el momento de hablar con su m�dico.
Aunque la frecuencia card�aca es uno de los signos vitales m�s importantes que se toman durante una visita al m�dico, existe otro signo vital que puede ser igual de importante: la variabilidad de la frecuencia card�aca. Esto refleja la salud de su sistema nervioso autom�tico o aut�nomo, que se encarga de controlar todos los elementos inconscientes de su sistema nervioso, como la digesti�n y la respiraci�n. La variabilidad de la frecuencia card�aca se ha asociado frecuentemente con la longevidad e incluso la muerte. Cuanto menos variable sea la frecuencia card�aca, mayor ser� la tasa de mortalidad. Muchos m�dicos no miden la variabilidad del ritmo card�aco de un paciente, pero afortunadamente, usted puede controlarlo por si mismo. Las terapias de fr�o y calor, los saunas, el ejercicio, el yoga y la meditaci�n pueden ayudar a mejorar la variabilidad del ritmo card�aco del paciente.
Ahora pasemos a la siguiente, la m�s importante de los signos vitales tomados durante una visita al m�dico, la presi�n arterial. Si tuviera que alinear todos los vasos sangu�neos de su cuerpo, se extender�an aproximadamente 59,000 millas. Eso es casi siete veces alrededor de la tierra. Estos mismos vasos sangu�neos transportan m�s de 7,500 litros de sangre por todo el cuerpo de manera regular. Con cada latido del coraz�n, la sangre se empuja contra las paredes de las arterias, lo que provoca un aumento de la presi�n.
Las medidas m�dicas para la presi�n arterial tienen dos n�meros. El n�mero superior se conoce como sist�lica, o la presi�n cuando el coraz�n se est� contrayendo, y el n�mero inferior se conoce como diast�lica, o la presi�n cuando el coraz�n est� relajado o en reposo. Los rangos de referencia normales para la presi�n arterial contin�an cambiando porque seguimos descubriendo que los rangos de referencia que sol�amos considerar normales, que fueron primero 140/90, luego 130/80, todav�a estaban asociados con un mayor riesgo de ataque cerebral y apoplej�a . Hoy en d�a, muchos m�dicos pueden mencionar un problema con su presi�n arterial solo si tiene m�s de 130/80.
La raz�n por la que la presi�n arterial es tan importante es porque cuando est� elevada, puede ejercer una presi�n adicional sobre el coraz�n y las arterias, lo que podr�a provocar una enfermedad card�aca, un accidente cerebrovascular, una insuficiencia card�aca o incluso una insuficiencia renal. Y no solo el coraz�n y las arterias se ven afectados por la presi�n arterial: el cerebro, los ri�ones e incluso los ojos pueden verse tremendamente afectados, lo que provoca accidentes cerebrovasculares, demencia, insuficiencia renal y ceguera, entre otros problemas de salud. Mantener su presi�n arterial a un nivel �ptimo es fundamental para su salud y bienestar general. De hecho, actualmente se cree que la presi�n arterial normal es inferior a 120/80, sin embargo, puede llegar a ser incluso m�s baja.
Mientras que la presi�n arterial alta es mala, la presi�n arterial baja tambi�n puede ser mala. Un buen m�dico de medicina funcional discutir� con usted los riesgos tanto de la presi�n arterial alta como de la presi�n arterial baja. La presi�n arterial por debajo de 100/60 puede causar problemas, pero no necesariamente. Los vasos sangu�neos en el cuerpo humano funcionan como los pistones en un autom�vil. Si no se acumula suficiente presi�n, puede ser realmente dif�cil que la sangre fluya contra la gravedad. Y debido a que el cerebro humano est� en una posici�n m�s alta que el coraz�n, dependemos de nuestra presi�n arterial para suministrar a nuestro cerebro la cantidad necesaria de ox�geno y nutrientes necesarios para funcionar en consecuencia.
Si tiene presi�n arterial baja, puede experimentar otros s�ntomas, como fatiga. Otros s�ntomas asociados con la presi�n arterial baja incluyen mareos al estar de pie, debilidad e incluso niebla cerebral. Adem�s, tanto la presi�n arterial alta cr�nica como la presi�n arterial baja cr�nica pueden contribuir a un mayor riesgo de demencia.
Ahora hemos discutido la importancia de la frecuencia card�aca y la presi�n arterial. Pero, �Qu� tal si hablamos de otro signo vital importante: la temperatura de su cuerpo? Una fiebre o una temperatura corporal elevada a menudo pueden ser un signo de infecci�n. La temperatura tambi�n puede proporcionar una visi�n de la funci�n de nuestro metabolismo. Cuanto m�s bajo es el metabolismo de un individuo, menos calor produce, que puede manifestarse como una temperatura corporal ligeramente m�s baja de lo normal. La tiroides juega un papel importante en el metabolismo y en la regulaci�n de la temperatura. Por lo tanto, si con frecuencia se siente fr�o, es posible que desee hablar con su m�dico sobre c�mo solicitar el panel de tiroides correcto. Pero, �qu� pruebas debe pedirle a su m�dico para determinar esto? No se preocupe, analizaremos qu� pruebas de tiroides debe realizar en el video sobre las hormonas. La temperatura corporal �ptima debe ser de aproximadamente 98.6 grados Fahrenheit. Sin embargo, si es inferior a 97.7 grados Fahrenheit, puede indicar que tiene un problema de tiroides.
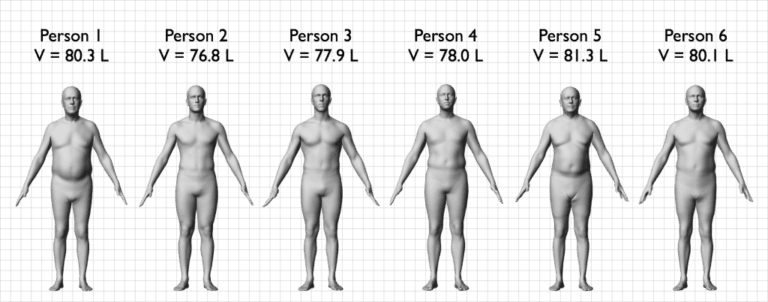
Las medidas m�dicas finales que vamos a discutir son su estatura y su peso. Los m�dicos utilizan su altura y peso para calcular su �ndice de masa corporal o IMC. En nuestra cl�nica, a modo de ejemplo, utilizamos el InBody 770, un analizador de composici�n corporal y agua corporal, para ayudar a determinar f�cilmente su �ndice de masa corporal y m�s. Sin embargo, el �ndice de masa corporal no siempre tiene en cuenta la composici�n corporal o el porcentaje de grasa contra m�sculo en el cuerpo humano. A modo de ejemplo, un jugador de f�tbol profesional de 6’6 “y 265 libras tiene un �ndice de masa corporal de m�s de 30, lo que los coloca en la categor�a de obesos.
Pero si viera el cuerpo de este individuo, nunca se clasificar�an como obesos. Esto demuestra que el IMC no es una medida precisa, especialmente para los atletas. Adem�s, una mujer de 65 a�os puede tener m�s grasa que m�sculo en su cuerpo, mientras que sus medidas de IMC pueden parecer “�ptimas”. En cambio, muchos m�dicos de medicina funcional usan medidas m�dicas de cintura a cadera. Esta es una medida simple que puede hacer en casa para determinar la distribuci�n de la grasa corporal, que tambi�n puede ayudar a demostrar el riesgo de disfunci�n metab�lica. La obesidad, la diabetes tipo 2 y las enfermedades del coraz�n son causadas por el exceso de grasa abdominal o grasa acumulada alrededor de los �rganos. El exceso de grasa alrededor de la secci�n media puede, en �ltima instancia, aumentar el riesgo de enfermedades card�acas y problemas metab�licos, como diabetes, demencia, c�ncer y muchos otros problemas de salud.
Pero primero, hablemos de c�mo puede calcular su relaci�n cintura-cadera. Para medir su cintura, simplemente tome las medidas del �rea m�s ancha alrededor de su cintura, que generalmente es la parte m�s grande alrededor de su ombligo. Para medir su cadera, luego tome las medidas del �rea m�s ancha alrededor de su cadera, que es generalmente donde sus huesos de cadera est�n de los lados. Entonces, toma estas medidas y luego divide las medidas de su cintura por las medidas de su cadera. Y este es el n�mero m�s fundamental que tiene que mirar.
En los hombres, una relaci�n cintura-cadera inferior a 0,9 se considera �ptima. Si la proporci�n es mayor que uno, lo que significa que su vientre es m�s grande que su cadera, puede poner a los hombres en mayor riesgo de desarrollar s�ndrome metab�lico, enfermedad card�aca, diabetes, accidente cerebrovascular, c�ncer y demencia. En las mujeres, una proporci�n de cintura-cadera de menos de 0,8 se considera �ptima. Si la proporci�n es mayor que 0,85, puede poner a las mujeres en mayor riesgo de desarrollar s�ndrome metab�lico, as� como a los otros problemas de salud mencionados anteriormente.
Las medidas m�dicas, incluyendo la frecuencia card�aca, la temperatura, la frecuencia respiratoria y la presi�n arterial, son varios signos vitales que ayudan a indicar a los m�dicos el estado de las funciones corporales fundamentales de un paciente. Los rangos de referencia de hoy en d�a se utilizan para determinar los espectros “normales” de salud y bienestar, sin embargo, los estudios de investigaci�n han demostrado que estos rangos de referencia pueden no ser espectros �ptimos. Comprender las medidas m�dicas m�s b�sicas, o los signos vitales, es importante para el bienestar del paciente, ya que puede ayudar a las personas a reconocer si se sienten saludables o enfermos, independientemente de lo que es normal. Dr. Alex Jimenez D.C., C.C.S.T.
Entendiendo sus Signos Vitales
Y estos fueron sus signos vitales, sus medidas m�dicas m�s b�sicas. Estos n�meros son muy importantes ya que son fundamentales para su salud y bienestar en general. Comprender c�mo funciona su cuerpo como un todo es importante para optimizar su bienestar. Por lo tanto, la pr�xima vez que visite a su m�dico, pregunte sobre sus signos vitales y discuta estos rangos de referencia con ellos. Realmente creo que una combinaci�n de su propia investigaci�n y tener una buena relaci�n con un profesional de la salud calificado puede llevarlo por el camino correcto hacia la salud y el bienestar en general.
Encontrar un m�dico que trabaje con usted es esencial para lograr los resultados que merece. Si su m�dico no est� dispuesto a conversar con usted sobre su bienestar o las pruebas de laboratorio que se necesitan para realizar un seguimiento de sus resultados, es posible que desee considerar la posibilidad de buscar otro m�dico.
Si aprendi� acerca de las medidas m�dicas m�s simples, definitivamente disfrutar� el pr�ximo articulo, donde analizaremos los an�lisis de sangre utilizados para determinar las deficiencias nutricionales. M�s del 90 por ciento de las personas en los Estados Unidos son deficientes en nutrientes a nivel de la RDA. Esa es la cantidad m�nima necesaria para prevenir enfermedades causadas por deficiencias nutricionales.
Vamos a discutir c�mo un m�dico que se especializa en medicina funcional eval�a los resultados y qu� otras pruebas que su m�dico desconoce pueden decirnos mucho sobre su estado nutricional. Gracias de nuevo por acompa�arme hasta ahora y los ver� m�s tarde. El alcance de nuestra informaci�n se limita a problemas quiropr�cticos y de salud de la columna, as� como a temas y discusiones de medicina funcional. Para seguir discutiendo el tema, no dude en preguntarle al Dr. Alex Jimenez o comun�quese con nosotros al�915-850-0900�.
Curado por el Dr. Alex Jim�nez
Discusi�n del Tema Adicional: Dolor de Espalda Agudo
El dolor de espalda es una de las causas m�s frecuentes de discapacidad y d�as perdidos en el trabajo en todo el mundo. El dolor de espalda se atribuye a la segunda raz�n m�s com�n para las visitas al consultorio del m�dico, superada �nicamente por infecciones respiratorias superiores. Aproximadamente el 80 por ciento de la poblaci�n experimentar� dolor de espalda al menos una vez a lo largo de su vida. La columna vertebral es una estructura compleja formada por huesos, articulaciones, ligamentos y m�sculos, entre otros tejidos blandos. Las lesiones y / o afecciones agravadas, como las hernias de disco, pueden provocar s�ntomas de dolor de espalda. Las lesiones deportivas o las lesiones por accidentes automovil�sticos suelen ser la causa m�s frecuente de dolor de espalda; sin embargo, a veces los movimientos m�s simples pueden tener resultados dolorosos. Afortunadamente, las opciones de tratamiento alternativo, como la atenci�n quiropr�ctica, pueden ayudar a aliviar el dolor de espalda mediante el uso de ajustes de la columna vertebral y manipulaciones manuales, lo que finalmente mejora el alivio del dolor. �
De XYMOGEN�Las f�rmulas profesionales exclusivas est�n disponibles a trav�s de profesionales de atenci�n m�dica con licencia seleccionados. La venta por internet y el descuento de f�rmulas XYMOGEN est�n estrictamente prohibidos.
Con orgullo�El Dr. Alexander Jimenez�hace que las f�rmulas de XYMOGEN est�n disponibles solo para los pacientes bajo nuestro cuidado.
Llame a nuestro consultorio para que podamos asignar una consulta m�dica para acceso inmediato.
Si eres paciente de�Injury Medical & Chiropractic�Clinic, puedes preguntar por XYMOGEN llamando�915-850-0900.
Para su conveniencia y revisi�n de la�XYMOGEN�productos por favor revise el siguiente enlace. *XYMOGEN-Descargar-Catalogo
* Todas las pol�ticas de XYMOGEN anteriores se mantienen estrictamente.
Gardening is a favorite warm-weather activity for many people. Unfortunately, it can often send them straight to the chiropractor with back pain and stiffness. If you enjoy your garden but your back doesn�t take heart. An estimated�80% of the population has experienced back pain�or will experience it at some point in their lifetime.
It is common, but it doesn�t have to keep you from doing the things you enjoy. There are some fairly simple things you can do to make it easier and less painful.
Stretching is a good way to prevent back pain for nearly any activity. The more limber you are and the more warmed up your muscles are, the more comfortable you will be while you are gardening and afterward.
Stretches for gardeners�aren�t all that different from stretches for other activities. You need to address your hamstrings, triceps, and of course your back. Then you will be ready to get in the dirt and do what you love.
Contents
Use Back Friendly Tools and Gardening Methods
It may feel wonderful to get close to the dirt as you dig, breathing in its earthiness, feeling at one with nature, but your back likely does not hold the same appreciation. You can mix it up a little, but allow at least part of your gardening time to the use of tools that are �back friendly.�
Long handled and telescopic tools allow you to do your garden work without overworking your back. This is also great for people who don�t have full range of motion in their backs or who have trouble getting up and down.
Another back saver is a raised container garden. This will put your garden within easy reach, saving you from trying to get on the ground or, worse, feeling like you have to forego a garden because you can�t get around like you once did.
You can set the containers at whatever height you choose and include benches and seats for more comfortable gardening. If you do get on the ground, knee pads or a mat can help reduce some of the stress and prevent some pain.
Change Your Position Frequently
It�s easy to get in the zone and lose track of time, only for your body to remind you when you try to move and are met with painful stiffness. Carry a small timer with you and set it so that you are reminded every 30 minutes to stop, walk around, and stretch a little. This not only prevents pain and stiffness, but it also helps with your circulation and blood flow, even digestion.
You can also vary your garden tasks so that you don�t over-tax a single muscle group. You may weed for a while, then move to your potting bench for a while or pruning trees or shrubs. It isn�t good to stay in one position for too long no matter what you are doing. A physical activity like gardening, though, requires more movement.
Take Care when Bending, Reaching, and Lifting
Gardening involves a lot of reaching, bending, and lifting. When you don�t do it correctly you would wind up with a�sore back�� or worse.
To lift:�Don�t bend at your waist. Squat, grasp the object with both hands while pulling it close to your body. Straighten your legs slowly, letting those muscles to the work of lifting. You may also use a dolly, wheelbarrow, or wagon to move heavy items around and minimize the need to lift them.
Push:�Pushing doesn�t strain the back as much as pulling does. Push your seeder, wheelbarrow, and lawnmower and try to avoid pulling as much as possible.
Reaching:�Be careful when you reach, especially if you are reaching to lift. Even something that doesn�t weigh much can throw off your balance or cause you to twist your back. Try to minimize lifting while reaching as much as possible.
Bending:�Keep your knees soft when you bend and try bending from the waist. If you are doing a task that requires bending, take frequent breaks where you can stand upright. If you bend to lift, make sure you use proper lifting techniques.
Gardening can be wonderful for the mind, body, and spirit. It can also be painful if you don�t take the necessary precautions. When you go out to tend your plants, remember these back-saving gardening tips. Your back will thank you.
El Doctor de Medicina Funcional Explica el Cuidado de Enfermos y el Cuidado de Salud
Hoy analizaremos los fundamentos de la medicina funcional y c�mo puede construir una relaci�n saludable entre m�dico y paciente.
Si visita al m�dico porque ha experimentado migra�as, eczema, s�ndrome del intestino irritable y depresi�n, lo m�s probable es que lo refieran a cuatro especialistas diferentes e incluso se le receten un m�nimo de cuatro medicamentos diferentes. Un enfoque de la medicina funcional comprende que puede haber problemas comunes de salud que pueden estar causando los s�ntomas de un paciente. Una vez que llegue al origen del problema, se puede solucionar los problemas de salud que crean los s�ntomas.
La medicina funcional pregunta: “�Por qu� tiene esos s�ntomas y c�mo podemos tratar la fuente del problema y mejorar su salud y bienestar general?”, en lugar de “�Qu� enfermedad tiene y qu� medicamento usa para tratarla?”
Contents
�Que es el Cuidado de Enfermos y el Cuidado de Salud?
Hola a todos, mi nombre es Dr. Alex Jim�nez. Soy quiropr�ctico y practicante de medicina functional en El Paso, Texas. Estoy muy contento/a de poder presentarles la primera parte de “C�mo Tomar el Control de su Salud”, donde analizaremos las diferencias entre �el Cuidado de Enfermos y el Cuidado de la Salud”. Por lo tanto, con frecuencia escucho a las personas hablar sobre lo dif�cil que es encontrar al m�dico adecuado, a alguien que est� dispuesto a trabajar con ellos, que los escuche y que est� abierto a satisfacer sus demandas mientras les ense�a todo lo que necesitan saber sobre sus problemas. Un m�dico que acepta avances innovadores en la ciencia y los enfoques de sistemas para determinar la fuente del problema. Esto se conoce como medicina funcional, y discutiremos m�s de eso en un minuto.
Mi objetivo en este momento es mostrarle c�mo puede encontrar al m�dico adecuado y establecer la mejor relaci�n con ellos para obtener la atenci�n que merece. Es importante hacerle varias preguntas a su m�dico para determinar si son adecuados para usted, si est�n dispuestos a trabajar con usted, a escucharlo y si est�n abiertos a sus solicitudes, as� como a aprender sobre los problemas que se les presentan. En lugar de no est�r familiarizado con ellos o que no sigan nuevos enfoques de tratamiento si se les presenta. A modo de ejemplo, si el m�dico que elige dice que la nutrici�n no tiene nada que ver con una enfermedad, entonces probablemente deber�a buscar otro m�dico. Ahora hablemos sobre las preguntas que debe hacerle a su m�dico sobre su salud y bienestar general para estar informado sobre lo que est� sucediendo en su propio cuerpo.
He hablado con pacientes que han visitado a numerosos m�dicos con la esperanza de encontrar una respuesta sobre por qu� no se sienten bien o tienen alg�n tipo de enfermedad. Muchos son referidos frecuentemente a uno o m�s especialistas y, en algunos casos, reciben Prozac, o se les dice que todos sus s�ntomas est�n en su cabeza o a veces incluso se les dice que no hay nada de malo despu�s de que todos los resultados de su laboratorio son normales. Y es frecuente que estos mismos pacientes sean enviados a varios m�dicos por cada parte de su cuerpo en lugar de ser enviados a un m�dico que pueda diagnosticar y tratar su cuerpo por completo. Si acude al m�dico y tiene migra�as, eczema, s�ndrome del intestino irritable y depresi�n, en la mayor�a de los casos, se le enviar� a cuatro especialistas diferentes y se le administrar�n, al menos, cuatro medicamentos diferentes, en lugar de visitar a un especialista que pueda comprender la fuente subyacente del problema y tratar la ra�z de los s�ntomas.
�Alguna vez ha visitado a un m�dico que, despu�s de explicarles sus s�ntomas, dice: “Oh, hice un panel de sangre completo y todo regreso normal”. Esto podr�a significar una de dos cosas, ya sea que est� loco o que les esta faltando algo. Y estoy seguro de que a menudo falta algo porque no buscan las respuestas en los lugares correctos. Es como una persona que deja caer sus llaves en la calle y cuando su amigo lo ve buscando debajo de una farola, dice: “Oye, �qu� est�s haciendo?”, Dice: “Estoy buscando mis llaves”. Entonces dice, �Pues d�nde las perdiste “. Y el dice:” Bueno, las perd� por la calle “.”� Entonces por qu� est�s buscando aqu�? “” Bueno, la luz est� mejor aqu� “. Y desafortunadamente, eso pasa mucho en la medicina. Los m�dicos buscar�n respuestas donde los problemas son f�ciles de encontrar. Y ese es el prop�sito de este video. Para ayudarlo a comprender c�mo puede encontrar la fuente de los problemas de salud subyacentes que lo hacen sentir mal.
Esto me recuerda a un caso de una mujer que vi en mi consultorio que ten�a artritis psori�sica, una afecci�n autoinmune que le caus� erupciones en todo el cuerpo junto con dolor e inflamaci�n en las articulaciones. Como resultado, ella consum�a grandes cantidades de drogas y / o medicamentos que sumaban alrededor de $60,000 d�lares al a�o o m�s. Tambi�n ten�a otros problemas de salud, ten�a reflujo �cido, s�ndrome del intestino irritable, pre-diabetes, migra�as, insomnio y depresi�n. Esta mujer visit� a muchos especialistas diferentes y estaba tomando recetas para tratar cada uno de sus s�ntomas. Cuando lleg� el momento de verla, todo lo que hice fue llegar a la fuente del problema.
Entonces, durante el diagn�stico, me dije a m� mismo: “Bueno, esta paciente tiene inflamaci�n, pero �cu�l es la causa de su inflamaci�n?” Y en lugar de recomendarla a muchos otros especialistas para que pudiera recibir medicamentos para sus migra�as, reflujo �cido, depresi�n, etc., me dije a m� mismo: “Oh, todos estos s�ntomas son inflamatorios, entonces, �cu�l es la ra�z de la inflamaci�n?” Bueno, resulta que la paciente tuvo problemas con su intestino todo el tiempo. Luego la ayud� a eliminar los “bichos malos” en su intestine, recomend�ndole una dieta anti-inflamatoria, inclu� algunos suplementos, aceite de pescado, vitamina D, probi�ticos. Sinceramente, remedios naturales realmente b�sicos. Cuando regres� seis semanas despu�s, todos sus s�ntomas hab�an desaparecido. Se hab�a retirado todos sus medicamentos recetados y hab�a perdido 20 libras. No le dije que dejara de tomar sus medicamentos, simplemente lo hizo por su propia cuenta. Fue absolutamente extraordinario y eso es lo que sucede cuando se trata la fuente de los problemas de salud subyacentes de un paciente. Y no tiene que hacer mucho para llegar a la ra�z del problema.
Entiendo que es posible que no siempre se pueda trabajar con un m�dico que est� capacitado en medicina funcional, de lo que hablaremos en un minuto. Sin embargo, es posible encontrar un m�dico que est� dispuesto a trabajar con usted, qui�n va a escuchar, qui�n tendr� la mente abierta y qui�n ser� su compa�ero durante su viaje hacia la salud y el bienestar en general. A lo largo de este video, analizar� las pruebas de laboratorio convencionales y las pruebas de laboratorio de medicina funcional innovadora, demostrando todo con el prop�sito de crear bienestar en lugar de verlo todo desde la perspectiva de la enfermedad para encontrar la fuente de los problemas de salud de un paciente y corregir los desequilibrios a trav�s de un enfoque de medicina funcional.
Tomando el Control de el Cuidado de Enfermos y el Cuidado de Salud
La medicina funcional a menudo se conoce como el futuro de la medicina, pero muchos m�dicos la ofrecen actualmente si visita el lugar correcto. El prop�sito de la medicina funcional es diagnosticar y tratar la causa de una variedad de enfermedades mediante la evaluaci�n del cuerpo por completo, en lugar de analizar cada colecci�n de �rganos de forma independiente a trav�s de especialistas independientes. La medicina funcional trata todo el sistema, no solo los s�ntomas. Los m�dicos que practican la medicina funcional con frecuencia se preguntan: “�Por qu� tiene el paciente estos s�ntomas y c�mo puedo corregir las causas y mejorar su salud y bienestar general?”, En lugar de “�Qu� enfermedad tiene el paciente y qu� medicamento utilizan para tratarlo?�
He sido un quiropr�ctico practicante por m�s de 25 a�os. Y he presenciado innumerables milagros todos los d�as. Mis pacientes no solo encuentran alivio de sus s�ntomas, realmente logran alcanzar el bienestar general. Desafortunadamente, nuestro sistema de salud actual est� roto. Muchos m�dicos se ven tremendamente afectados debido a las limitaciones de tiempo establecidas por las compa��as de seguros para pagar las facturas, lo que hace que se apresuren a acudir a sus citas. A la vez, este ciclo continuo con frecuencia puede terminar dejando a los pacientes con preguntas sin respuesta y frustraci�n. Nuestro sistema de atenci�n m�dica actual hace que las personas se sientan impotentes, a menudo manteni�ndolas atrapadas con sus enfermedades.
Como parte de este sistema de salud, es importante que entendamos que algunas enfermedades no son tan f�ciles de tratar como un resfriado. Varias enfermedades tampoco se desarrollan de forma aleatoria. La mayor�a de las enfermedades que existen en la actualidad est�n relacionadas con su entorno y como estos factores externos e internos interact�an con sus genes y estilo de vida para influir en su salud y bienestar.
Lo que hoy conocemos como el enfoque de la �medicina convencional� se conoce generalmente como el juego de �nombrarlo, culparlo y domesticarlo�. Primero, el m�dico diagnosticar� al paciente y le proporcionar� una etiqueta, por ejemplo, dicen que un paciente tiene depresi�n. Ahora tienen el nombre de la enfermedad. Y finalmente, el m�dico tratar� la enfermedad con medicamentos recetados. Al final, el paciente se queda tomando un antidepresivo. Sin embargo, la depresi�n puede ser causada por una amplia gama de factores y la soluci�n no es necesariamente un antidepresivo. Este tipo de pr�ctica no solo est� desactualizada, sino que en realidad se considera bastante inseguro a largo plazo. Y a menudo no proporciona a los pacientes los resultados que necesitan. Las personas son diagnosticadas err�neamente y con frecuencia quedan enfermas sin recibir realmente la atenci�n adecuada que merecen.
La medicina convencional tambi�n puede ser �til en las etapas finales de algunas enfermedades, as� como para enfermedades agudas. Si tiene una emergencia o se siente muy enfermo, si se rompe un hueso, o si tiene una infecci�n, la medicina convencional, los cuidados intensivos, los medicamentos pueden ser la soluci�n adecuada y deber�amos estar sumamente agradecidos por ellos. Pero este no es el enfoque que necesitamos para prevenir y curar enfermedades cr�nicas. Si realmente entendi�ramos c�mo cuidar nuestros cuerpos como deber�amos, la mayor�a de nosotros no nos sentir�amos tan enfermos. Y muchas personas seguiran sinti�ndose enfermas, pero no tiene que hacerlo, no es normal. Muchos m�dicos ahora entienden que se requiere un cambio para convertir todo nuestro sistema de atenci�n de enfermos en uno que realmente respalde la atenci�n m�dica.
Me gustar�a capacitarlo para ayudar a transformar el futuro del campo de la medicina al tomar su bienestar en sus propias manos. A lo largo de los pr�ximos videos, compartir� con usted c�mo puede encontrar un m�dico que tenga en cuenta sus valores y creencias personales para que pueda lograr los resultados que est� buscando mientras se encuentra en un entorno seguro y c�modo. Puede aprender a ser su propio defensor de la salud y convertirse en un verdadero socio con su m�dico. Y hay muchos otros m�dicos y practicantes de medicina funcional como yo que est�n esperando para ayudar.
Adem�s, compartir� con usted c�mo puede encontrar al mejor m�dico y tambi�n le proporcionar� muchas otras herramientas para ayudarlo a ser el l�der de su salud y bienestar en general. Ademas de c�mo puede tomar el control de su propio bienestar. Incluyendo el trabajo de laboratorio que debe solicitar a su m�dico y c�mo entender qu� significa la informaci�n y qu� debe hacer con ella. Una de las formas m�s comunes en que los m�dicos utilizan los laboratorios es evaluar qu� es lo que no funciona cuando el paciente no se siente bien y analizar el final de un continuo de la enfermedad. Si su funci�n cambia, sus c�lulas hep�ticas pueden estar muriendo. Sin embargo, si son normales, muchos m�dicos dicen: “Oh, usted es normal”. Pero en realidad puede no ser normal. La buena noticia es que puede encontrar desequilibrios antes para tratarlos a tiempo.
Aunque est� cambiando lentamente, muchos m�dicos tienen la costumbre de no darles a los pacientes sus an�lisis de laboratorio reales. Y si este no es el caso, varios m�dicos no brindan explicaciones detalladas de las pruebas de laboratorio del paciente que no sean “Sus pruebas de laboratorio regresaron normales” o “Su colesterol esta un poco alto” o “Su nivel de az�car en la sangre esta alto”. Como quiropr�ctico, creo que todos deber�an tener acceso a sus an�lisis de laboratorio y que estos deben explicarsele al paciente. Tenemos que empezar a democratizar la medicina. Y esto se ha vuelto m�s fundamental que nunca.
Ahora, �por qu� es esto tan importante? Aproximadamente 133 millones de estadounidenses se ven afectados por enfermedades cr�nicas y ese n�mero es a�n mayor dependiendo de c�mo se define la enfermedad cr�nica. Aproximadamente uno de cada dos individuos en los Estados Unidos tiene pre-diabetes o diabetes tipo 2. La tasa de una variedad de enfermedades, incluyendo problemas digestivos, enfermedades al�rgicas, enfermedades del coraz�n, enfermedades autoinmunes, c�ncer, obesidad, diabetes tipo 2 y demencia, ha aumentado. Donde aproximadamente uno de cada tres ni�os nacidos hoy tendr�n diabetes tipo 2 durante su vida y una de cada dos personas mayores de 85 a�os y una de cada cuatro personas mayores de 75 a�os tendr� demencia.
Problemas de salud como estos se est�n manifestando en toda nuestra poblaci�n a un ritmo tremendo y pueden afectar a todos, ya sea personalmente o a trav�s del sufrimiento de un ser querido. Adem�s, las enfermedades cr�nicas han causado una carga econ�mica dram�tica en nuestro pa�s.
Sin embargo, la raz�n por la que estoy tan feliz de compartir este video con ustedes es porque hay mucho que podemos hacer para cambiar el futuro de nuestro sistema de atenci�n m�dica. Muchos m�dicos y yo tenemos el conocimiento que necesitamos para disminuir o incluso eliminar el sufrimiento de tantas personas y para salvar la econom�a. Todos los d�as en mi consultorio, veo que los pacientes recuperan su calidad de vida despu�s de que esperaban sufrir toda su vida debido a enfermedades cr�nicas como el reflujo �cido, el s�ndrome del intestino irritable, los dolores de cabeza, la fatiga y la artritis, entre otros problemas de salud. Problemas como alergias, problemas hormonales, obesidad, diabetes, enfermedades del coraz�n, enfermedades autoinmunes y depresi�n. Y los pacientes realmente pueden mejorar y prosperar, no solo enfrentar o controlar su enfermedad. En unos pocos meses, incluso semanas, de visitarnos a m� y a mi personal, las vidas de los pacientes pueden cambiar enormemente.
La medicina funcional analiza c�mo funciona el cuerpo humano por completo, y su enfoque m�s b�sico es comprender primero los factores, los genes y los desencadenantes de la enfermedad, y c�mo el estilo de vida y las aportaciones ambientales, incluyendo la dieta, el estr�s, las toxinas, los al�rgenos y los microbios , interact�an con el cuerpo humano para crear desequilibrios que com�nmente pueden conducir a problemas cr�nicos de salud.
Entonces, d�jenme tomar un momento para discutir algo. El cuerpo humano es un sistema. Y todo este sistema est� formado por “sistemas peque�os” que interact�an din�micamente. Pero, cuando uno o m�s de estos sistemas se desequilibran, puedes enfermarte. Y cuando estos sistemas se equilibran de nuevo, te vuelves sano. Y eso es lo que es la medicina funcional. La medicina funcional es simplemente comprender las causas de los desequilibrios en el cuerpo humano y el tratamiento para restablecer el equilibrio y proporcionar necesidades esenciales a todos los sistemas del cuerpo humano. Creando salud y bienestar en general es una ciencia. Y los m�dicos logran esto utilizando el historial m�dico detallado de un paciente, combinado con pruebas de laboratorio espec�ficas. Los m�dicos que siguen un enfoque de medicina funcional, como yo, a modo de ejemplo, generalmente eval�an su intestino y su microbioma, que no son muchos los m�dicos que analizan esto. Tambi�n queremos analizar su sistema inmunol�gico y si la inflamaci�n lo est� afectando, algo que llamamos defensa y reparaci�n. Y queremos saber c�mo sus mitocondrias producen energ�a con los alimentos y el ox�geno. Los profesionales de la medicina funcional desean saber si tiene alguna disfunci�n en la producci�n de energ�a, que suele ser la fuente de numerosas enfermedades, como la enfermedad de Alzheimer y el autismo, la diabetes tipo 2 y la fatiga, entre muchas otras. Tambi�n determinamos su carga t�xica y su capacidad de desintoxicaci�n, involucrando la funci�n de otros sistemas de comunicaci�n en su cuerpo, como sus hormonas. Finalmente, evaluamos su sistema estructural, desde sus c�lulas hasta sus estructuras biomec�nicas y c�mo �stas interact�an con sus creencias, emociones y m�s.
He usado estos procedimientos, una y otra vez, para ayudar a revertir las enfermedades cr�nicas en mis pacientes y educarlos sobre c�mo lograr la salud y el bienestar a largo plazo, al mismo tiempo que aprended como convertirse en las mejores versiones de s� mismos. Todos tenemos la oportunidad de curar o mejorar enormemente los problemas de salud o problemas que a menudo se diagnostican con la medicina convencional. La medicina funcional ofrece la oportunidad de descubrir el bienestar general a cualquier edad.
De hecho, trat� a un hombre llamado George, que ten�a 63 a�os, pesaba 300 libras y ten�a una variedad de problemas de salud. Ten�a reflujo �cido, problemas de sinusitis, diabetes, problemas card�acos, angina, problemas de pr�stata, disfunci�n sexual y edema en las piernas. Y como resultado, estaba bajo una amplia gama de medicamentos. Un d�a vino a mi oficina y me dijo: “�Me puede ayudar?”. Le dije: “S�, pero tendr� que hacer todo lo que yo le diga”.
Entonces, le recomend� una dieta anti-inflamatoria, que consist�a de alimentos integrales y una cantidad baja de az�car, y le aconsej� que tomara una variedad de suplementos para optimizar su nutrici�n, mientras lo guiaba a participar en ejercicios y actividades f�sicas. Dentro de un a�o, fue como un milagro, el paciente hab�a perdido 155 libras, revirti� todos sus problemas de salud y dej� de usar sus medicamentos. Ahora, �l est� planeando el resto de su vida, cuando antes de venir a visitarme, estaba planeando el final de su vida. Otra paciente que trat�, llamada Isabel, luch� contra una enfermedad autoinmune. Ten�a solo 10 a�os y ya estaba bajo un mont�n de drogas, esteroides, inmunosupresores e incluso quimio. Resulta que su dieta y la exposici�n a metales pesados ??estaban afectando sus intestinos y causando inflamaci�n. Ahora, simplemente trat� la fuente de sus problemas y su enfermedad autoinmune desapareci�. Dej� de usar sus medicamentos recetados y, en conjunto, su calidad de vida mejor� y prosper�.
La medicina funcional es un enfoque de tratamiento alternativo que se centra en las interacciones entre factores externos o ambientales, as� como factores internos asociados con los sistemas gastrointestinal, endocrino e inmunol�gico del cuerpo humano. Encontrar el m�dico adecuado puede hacer una gran diferencia cuando se trata de obtener atenci�n m�dica en vez de atenci�n por enfermedad. La medicina funcional trata la fuente del problema en lugar de tratar solo los s�ntomas. Como quiropr�ctico y practicante de medicina funcional, mi objetivo principal es brindar a los pacientes la atenci�n que merecen por sus problemas de salud, as� como educarlos sobre los fundamentos de la medicina funcional. El prop�sito de este art�culo es ayudar a los pacientes a encontrar al m�dico adecuado y establecer una relaci�n sana entre m�dico y paciente. Dr. Alex Jimenez D.C., C.C.S.T.
Informacion General Sobre el el Cuidado de Enfermos y el Cuidado de Salud
Durante las pr�ximas semanas, repasaremos algunos de los principios y conceptos fundamentales que me ayudaron a encontrar la causa subyacente de la enfermedad a trav�s del uso de la medicina funcional. Y eso los ayudar� a alcanzar la salud y el bienestar general.
En nuestro pr�ximo video, le ense�ar� c�mo puede tomar sus propias medidas para comprender su propio bienestar y qu� puede hacer para mejorar sus signos vitales. Este procedimiento ayudar� a proporcionarle datos e informaci�n de referencia importantes para ayudarlo a comprender mejor sus riesgos de salud. Tambi�n le permitir� evaluar y analizar su propio progreso a medida que trabaja para alcanzar sus objetivos de bienestar finales.
En el tercer video, voy a tratar de cubrir todo sobre nutrici�n. Le explicar� c�mo podemos evaluar su estado nutricional y c�mo puede utilizar los alimentos como tratamiento para comenzar a cambiar su salud y bienestar general lo mas antes posible. Su dieta es una de las partes m�s eficientes que puede controlar para crear un estilo de vida m�s saludable. Estar� compartiendo consejos y trucos para una mejor nutrici�n.
Debido a que las hormonas pueden afectar casi todos los aspectos de nuestra salud, tambi�n los vamos a destacar en el cuarto video. Desafortunadamente, la mayor�a de los m�dicos no entienden los niveles �ptimos de hormonas ni son conscientes de los m�todos adecuados para evaluar las hormonas. Lo preparar� para tener una conversaci�n efectiva con su m�dico sobre qu� tipo de prueba hormonal realmente importa, qu� significan y qu� puede hacer al respecto.
En el video cinco, me centrar� en la salud del coraz�n, discutiendo la presi�n arterial alta, colesterol alto y enfermedades cardiovasculares. Estas condiciones son extremadamente comunes, y desafortunadamente, la medicina convencional frecuentemente trata de tratarlas simplemente controlando los s�ntomas. Reducir el colesterol, disminuir la presi�n arterial, eso no resuelve la ra�z de los problemas. La mayor�a de las veces, el aumento de los niveles de az�car en la sangre, la obesidad y la diabetes son la causa de las enfermedades cardiovasculares. Voy a demostrar c�mo podemos prevenir y revertir estas enfermedades utilizando modificaciones en su estilo de vida, incluyendo la nutrici�n, para mejorar la salud del coraz�n.
En el sexto video, hablar� sobre la obesidad y la diabetes, trastornos metab�licos que van desde la grasa m�nima y la resistencia moderada a la insulina hasta la prediabetes y la diabetes tipo 2. Lo bueno de estos trastornos metab�licos, sin embargo, es que son completamente reversibles. Pero la mayor�a de los m�dicos convencionales no saben que es reversible. Voy a ense�arles c�mo pueden recuperar un metabolismo saludable y c�mo revertir la gama de problemas relacionados con la diabetes, que, como aprender�, son muchas enfermedades diferentes.
En el video siete, hablar� sobre el sistema inmunol�gico, en particular sobre la inflamaci�n oculta y la enfermedad. Como se describe que la inflamaci�n es la causa subyacente de la mayor�a de las enfermedades cr�nicas, continuamos observando tasas crecientes de enfermedades autoinmunes y alergias, que son se�ales de que nuestro sistema inmunol�gico no funciona correctamente. Sin embargo, la inflamaci�n tambi�n est� asociada con la obesidad, la diabetes tipo 2, las enfermedades del coraz�n, el c�ncer, la demencia e incluso la depresi�n. Le explicar� c�mo puede hablar con su m�dico sobre las pruebas de inflamaci�n, qu� significan los marcadores y c�mo puede cuidar su sistema inmunol�gico a un nivel m�s profundo.
En el video ocho, vamos a pasar al tema del metabolismo y las mitocondrias. Ahora, cada una de nuestras c�lulas contiene cientos o miles de mitocondrias, los generadores de energ�a de nuestras c�lulas. Cuando estos se da�an, podemos sufrir una variedad de problemas, como dolor, p�rdida de memoria, fatiga y muchos otros s�ntomas. Voy a explicar c�mo podemos cuidar sus mitocondrias a nivel celular y por qu� esta es una pieza vital de salud y bienestar �ptimos.
Luego, en el video nueve, vamos a explorar el significado de la desintoxicaci�n o el sistema de desintoxicaci�n del cuerpo humano y por qu� esto es una parte esencial del proceso de curaci�n. Desde el moho hasta los metales pesados ??y otras toxinas, explicar� lo que debe saber para evitar las toxinas y c�mo puede eliminar las que ya tiene para optimizar su capacidad de desintoxicaci�n. Con la cantidad de toxinas a las que estamos expuestos de manera regular, es importante identificar las causas que pueden estar afect�ndote y c�mo puedes comenzar a eliminarlas de inmediato. Afortunadamente, esto es algo que puede hacer f�cilmente para crear un estilo de vida m�s limpio para usted y sus seres queridos.
Finalmente, en el video diez estaremos hablando sobre la digesti�n. La salud digestiva es uno de los temas m�s discutidos en la medicina funcional. Debido a que nuestro sistema digestivo es el centro de nuestra salud, al diagnosticar problemas en este sistema, podemos mejorar todo, desde la salud mental, la absorci�n de nutrientes y el riesgo cardiovascular hasta la funci�n del sistema inmunol�gico. En el d�cimo video, los guiar� a trav�s de las pruebas disponibles para controlar su salud intestinal, as� como lo que puede hacer para mejorar su propia salud digestiva, lo antes posible.
Estoy muy contento de que me acompa�en en esta serie de videos porque el futuro de la medicina depende de ello. Cuando se aprende c�mo puede impactar su bienestar al ser proactivo y al asociarse con su m�dico, todo cambia. A trav�s de la medicina funcional, tambi�n puede ayudar a transformar nuestro sistema de atenci�n m�dica en un sistema de atenci�n m�dica real.
Entonces, terminemos este video con las preguntas que desea hacerle a su m�dico cuando los entreviste para ver si pueden ser un socio para usted y su salud y bienestar en general. Estas son solo algunas preguntas de alto nivel para comenzar con su discusi�n. �Est� dispuesto a trabajar conmigo como socio para mi bienestar?, �Cu�l es su punto de vista sobre nutrici�n y salud? �Cree que la comida es medicina? �Est� dispuesto a darme copias de los resultados de mis pruebas y explicarme qu� significan? La raz�n por la que nos hacemos estas preguntas es para asegurarnos de que su m�dico est� dispuesto a trabajar con usted y comprender el papel de la medicina funcional.
�
Estoy muy feliz de ser parte de su camino hacia una mejor salud y bienestar. Muchas gracias por acompa�arme el dia de hoy. El alcance de nuestra informaci�n se limita a problemas quiropr�cticos y de salud de la columna, as� como a temas y discusiones de medicina funcional. Para seguir discutiendo el tema, no dude en preguntarle al Dr. Alex Jimenez o comun�quese con nosotros al�915-850-0900�.
Curado por el Dr. Alex Jim�nez
Discusi�n del Tema Adicional: Dolor de Espalda Agudo
El dolor de espalda es una de las causas m�s frecuentes de discapacidad y d�as perdidos en el trabajo en todo el mundo. El dolor de espalda se atribuye a la segunda raz�n m�s com�n para las visitas al consultorio del m�dico, superada �nicamente por infecciones respiratorias superiores. Aproximadamente el 80 por ciento de la poblaci�n experimentar� dolor de espalda al menos una vez a lo largo de su vida. La columna vertebral es una estructura compleja formada por huesos, articulaciones, ligamentos y m�sculos, entre otros tejidos blandos. Las lesiones y / o afecciones agravadas, como las hernias de disco, pueden provocar s�ntomas de dolor de espalda. Las lesiones deportivas o las lesiones por accidentes automovil�sticos suelen ser la causa m�s frecuente de dolor de espalda; sin embargo, a veces los movimientos m�s simples pueden tener resultados dolorosos. Afortunadamente, las opciones de tratamiento alternativo, como la atenci�n quiropr�ctica, pueden ayudar a aliviar el dolor de espalda mediante el uso de ajustes de la columna vertebral y manipulaciones manuales, lo que finalmente mejora el alivio del dolor. �
De XYMOGEN�Las f�rmulas profesionales exclusivas est�n disponibles a trav�s de profesionales de atenci�n m�dica con licencia seleccionados. La venta por internet y el descuento de f�rmulas XYMOGEN est�n estrictamente prohibidos.
Con orgullo�El Dr. Alexander Jimenez�hace que las f�rmulas de XYMOGEN est�n disponibles solo para los pacientes bajo nuestro cuidado.
Llame a nuestro consultorio para que podamos asignar una consulta m�dica para acceso inmediato.
Si eres paciente de�Injury Medical & Chiropractic�Clinic, puedes preguntar por XYMOGEN llamando�915-850-0900.
Para su conveniencia y revisi�n de la�XYMOGEN�productos por favor revise el siguiente enlace. *XYMOGEN-Descargar-Catalogo
* Todas las pol�ticas de XYMOGEN anteriores se mantienen estrictamente.
Body composition analysis is becoming a standard tool that is being used by fitness experts, coaches, and healthcare professionals.
In 2019 we can�discard reliance on body mass index (BMI)�as a means to measure health.
Other than our appearance, there is a list of diseases associated with obesity. This is what’s at the top of our minds. The list is long and includes heart disease, hypertension, cancer, joint problems, dementia, and diabetes.
Body composition analysis is defined as the clinical assessment of tissue and fluid in the human body.
Fat Mass
Fat-Free Mass
Body Cell Mass
Extracellular Mass
Total Body H2O
Intracellular H2O
Extracellular H2O
Normal distribution of tissue and fluid is associated with immunity, high function, and longevity.
However, not being able to have detailed insight�into your personal body composition can�lead to critical errors�in understanding what’s going on, along with recommendations. This can hinder the�ability to reach a specific fitness goal.
Body composition analysis is utilized in preventative, therapeutic, and research applications.
Nutrition
Anti-Aging
Physical Performance Assessment
Weight Management
Geriatrics
Lifestyles Assessment
Athletic Performance
To perform body composition analysis, mass and fluid are modeled, measurements taken, and results analyzed.
Bioimpedance (BIA) body composition analyzers measure body composition electronically. However, they do not, diagnose disease, or calculate treatment options. Only qualified health care professionals can diagnose and recommend treatment options.
There are concerns that affect everyone, which is why knowledge of body composition is important for your health in 2019 onward.
Contents
Model Body
Look at the images below of six males, all of whom are 5′ 9″ and 170 pounds. There could be some envy from their 25.4 BMI, as the results are come up on the computer screen. However, looking at the actual patient or their scans using today’s technology, the results are pretty revealing.
Notice the difference in the midsection, where there is an abnormal accumulation of visceral fat.
This occurs in metabolic syndrome and what is known as Adiposity disease.
Fat Mass (FM): Total amount of stored lipids in the body and consists of the following types:
Subcutaneous Fat is located right under the skin. Subcutaneous fat functions as an energy reserve and as insulation from the cold.
Visceral Fat is located deeper in the body. This fat serves as an energy reserve and as a cushion between the organs.
Fat-Free Mass (FFM), aka Lean Body Mass (LBM): Total amount of nonfat (lean) parts of the body.
Consists of approximately 73% water, 20% protein, 6% mineral, and 1% ash.
Fat-free mass divides further into body cell mass and extracellular mass:
Body Cell Mass (BCM): All the metabolically active tissues (cells) of the body, which include muscle, organ, blood, and immune cells.
BCM includes the “living” portion of fat cells, but not fat lipids.
BCM also includes H2O inside living cells. This water is called Intracellular Water (ICW). The main electrolyte is potassium.
Extracellular Mass (ECM): All the metabolically inactive (non-living) parts of the body, such as bone minerals and blood plasma. ECM includes water contained outside living cells. This water is called Extracellular Water (ECW). The main electrolyte is sodium.
Composition & Body Health
Body composition correlates directly to maintained proper health, that range from mortality/morbidity to immunity, longevity, high function, and athletic performance.
Body composition analysis’ purpose is to monitor and improve function.
Healthy patients analysis of fat-free mass and body cell mass helped maintain function, productivity, immunity, physical performance, and longevity.
Every case is different but through body composition analysis, people can have a better understanding of their body, what options are available to them, and most importantly do not have to be on medication/s for the rest of their lives.
References:
Kyle UG, et al. Physical activity and fat-free and fat mass by bioelectrical impedance in 3853 adults. Medicine and Science in Sports and Exercise, 2001;33:576-584.
Mattar JA, et al. Application of total body bioimpedance to the critically ill patient. New Horizons, 1995, Vol 4., No. 4; 493-503.
Ott M, et al. Bioelectrical impedance analysis as a predictor of survival in patients with human immunodeficiency virus infection. Journal of Acquired Immune Deficiency Syndromes and Human Retrovirology, 1995; 9:20-25.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine