The human nervous system is made up of two parts: the central nervous system, which includes the brain and the spinal cord, and the peripheral nervous system, which includes the connection nerves running from the brain and the spinal cord to the rest of the human body, including the hands and the feet.
Many patients with neuropathy may experience a variety of painful symptoms due to nerve damage or injury. But, with the proper treatment approach, neuropathy can be effectively treated and even reversed. Diagnosis of neuropathy is fundamental towards proper treatment. Dr. Alex Jimenez, a chiropractor in El Paso, TX, can help patients with neuropathy.
Contents
Peripheral Neuropathy Causes & Symptoms | El Paso, TX (2019)
Neuropathy is a medical term used to describe a collection of general diseases or malfunctions which affect the nerves. The causes of neuropathy, or nerve damage, can vary greatly among each individual and these may be caused by a number of different diseases, injuries, infections, and even vitamin deficiency states. However, neuropathy can most commonly affect the nerves that control the motor and sensory nerves. Because the human body is composed of many different kinds of nerves which perform different functions, nerve damage is classified into several types.
Neuropathy can also be classified according to the location of the nerves being affected and according to the disease-causing it. For instance, neuropathy caused by diabetes is called diabetic neuropathy. Furthermore, depending on which nerves are affected will depend on the symptoms that will manifest as a result. Below we will discuss several specific types of neuropathies clinically treated by chiropractors, physical therapists and physical medicine doctors alike, as well as briefly describing their causes and their symptoms.
Peripheral neuropathy, which is often simply referred to as �neuropathy,� is a state that happens when your nerves become damaged or injured, oftentimes simply disrupted. It�s estimated that neuropathy affects roughly 2.4 percent of the general populace and approximately 8 percent of people older than age 55. However, this quote doesn�t include people affected by neuropathy caused by physical trauma to the nerves.
Types
Neuropathy can affect any of the three types of peripheral nerves:
Sensory nerves, which transmit messages from the sensory organs, eyes, nose to the brain
Motor nerves, which track the conscious movement of the muscles
Autonomic nerves, which regulate the involuntary functions of the body
Sometimes, neuropathy will only impact one nerve. This is medically referred to as mononeuropathy and instances of it include:
Ulnar neuropathy, which affects the elbow
Radial neuropathy, which affects the arms
Peroneal neuropathy, which affects the knees
Femoral neuropathy, which affects the thighs
Cervical neuropathy, which affects the neck
Sometimes, two or more isolated nerves in separate regions of the body can become damaged, injured or disrupted, resulting in mono neuritis multiplex neuropathy. Most often, however, multiple peripheral nerves malfunction at the same time, a condition called polyneuropathy. According to the National Institute for Neurological Disorders and Stroke, or the NINDS, there are over 100 kinds of peripheral neuropathies.
Causes
Neuropathies are often inherited from birth or they develop later in life. The most frequent inherited neuropathy is the neurological disease Charcot-Marie-Tooth disease, which affects 1 in 2,500 people in the USA. Although healthcare professionals are sometimes not able to pinpoint the exact reason for an acquired neuropathy, medically referred to as idiopathic neuropathy, there are many known causes for them, including systemic diseases, physical trauma, infectious diseases, and autoimmune disorders.
A systemic disease is one which affects the whole body. The most frequent systemic cause behind peripheral neuropathy is diabetes, which can lead to chronically high blood glucose levels that harm nerves.
Other systemic issues can cause neuropathy, including:
Kidney disorders, which permit high levels of nerve-damaging toxic chemicals to flow in the blood
Toxins from exposure to heavy metals, including arsenic, lead, mercury, and thallium
Certain drugs and/or medications, including anti-cancer medications, anticonvulsants, antivirals, and antibiotics
Chemical imbalances because of liver ailments
Hormonal diseases, including hyperthyroidism, which disturbs metabolic processes, potentially inducing cells and body parts to exert pressure on the nerves
Deficiencies in vitamins, such as E, B1 (thiamine), B6 (pyridoxine), B12, and niacin, that can be vital for healthy nerves
Alcohol abuse, which induces vitamin deficiencies and might also directly harm nerves
Cancers and tumors that exert damaging pressure on nerve fibers and pathways
Chronic inflammation, which can damage protective tissues around nerves, which makes them more vulnerable to compression or vulnerable to getting inflamed and swollen
Blood diseases and blood vessel damage, which may damage or injure nerve tissue by decreasing the available oxygen supply
Signs and Symptoms of Neuropathy
Depending on the reason and unique to each patient, signs, and symptoms of neuropathy can include:
Pain
Tingling
Burning/prickling sensations
Increased sensitivity to touch
Muscle weakness
Temporary or permanent numbness;
Paralysis
Dysfunction in glands or organs
Impairment in urination and
Sexual function
Such signs and symptoms are dependent on whether autonomic, sensory, or motor nerves, as well as a combination of them, are ultimately affected. Autonomic nerve damage can influence physiological functions like blood pressure or create gastrointestinal problems and issues. Damage or dysfunction in the sensory nerves may impact sensations and sense of equilibrium or balance, while harm to motor nerves may affect movement and reflexes. When both sensory and motor nerves are involved, the condition is known as sensorimotor polyneuropathy.
Complications
Peripheral�neuropathy�may result in several complications, as a result of disease or its symptoms. Numbness from the ailment can allow you to be less vulnerable to temperatures and pain, making you more likely to suffer from burns and serious wounds. The lack of sensations in the feet, for instance, can make you more prone to developing infections from minor traumatic accidents, particularly for diabetics, who heal more slowly than other people, including foot ulcers and gangrene.
Furthermore, muscle atrophy may cause you to develop particular physical disfigurements, such as pes cavus, a condition marked by an abnormally high foot arch, and claw-like deformities in the feet and palms.
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
Neuropathy can be caused by a variety of injuries and/or aggravated conditions, often manifesting into a plethora of associated signs and symptoms. While every type of neuropathy, such as diabetic neuropathy or autoimmune disease-associated neuropathy, develops its own unique group of signs and symptoms, many patients will often report common complaints. Individuals with neuropathy generally describe their pain as stabbing, burning or tingling in character.
If you experience unusual or abnormal tingling or burning sensations, weakness and/or pain in your hands and feet, it�s essential to seek immediate medical attention in order to receive a proper diagnosis of the cause of your specific signs and symptoms. Early diagnosis may help prevent further nerve injury. Visit http://www.neuropathycure.org�for more details.
Alzheimer�s disease (AD) is one of the most common types of dementia among older adults. Research studies have demonstrated that pathological changes in the human brain, whether directly or indirectly, can ultimately cause loss of synaptic function, mitochondrial damage, microglial cell activation, and neuronal cell death. However, the pathogenesis of AD is not yet fully understood and there is currently no definitive treatment for the neurological disease. Research studies have demonstrated that the activation and priming of microglial cells may contribute to the pathogenesis of AD. �
A proinflammatory status of the central nervous system (CNS) can also cause changes in the function of the microglial cells or microglia. Neuroinflammation is closely associated with the activation of microglia and astrocytes which are connected to a variety of neurological diseases by the synthesis and secretion of inflammatory mediators such as iNOS, ROS, and proinflammatory cytokines. According to research studies, microglial priming is also caused by the inflammation of the CNS. �
Therefore, whether microglial priming is the result or the cause of neuroinflammation is still controversial. Microglial cell activation commonly causes an increase of A? and tau proteins as well as a decrease of neurotrophic factors, ultimately leading to the loss of healthy brain cells or neurons and the development of neuritic plaques and neurofibrillary tangles which are closely associated with AD. With the progression of Alzheimer’s disease, changes from neuronal dysfunctions which may have no obvious symptoms to memory loss and cognitive impairment may become more noticeable. �
Contents
Microglial Priming, Neuroinflammation, and AD
Although the accurate and detailed, fundamental role of the microglial cells continues to be discovered and explained, there is a consensus among many researchers that primed microglia are associated with the inflammatory response of the CNS in AD. It has also been determined that neuroinflammation caused by microglial priming is mainly associated with aging, systemic inflammation, gene regulation, and blood-brain barrier impairment. The purpose of the article below is to discuss how microglial priming and neuroinflammation in Alzheimer’s disease can be caused due to a variety of risk factors. �
Aging
Aging is considered to be one of the main risk factors for AD and it is generally followed by chronic, systemic up-regulation of pro-inflammatory factors and a considerable decrease in an anti-inflammatory response. This change from homeostasis to an inflammatory state occurs through age-related elements which cause an imbalance between anti-inflammatory and pro-inflammatory systems. Microglia is primed into an activated state which can increase the consistent neuroinflammation and inflammatory reactivity in the aged human brain. Research studies have demonstrated that microglia in the brain of rodents developed an activated phenotype during aging characterized by the increased expression of CD11b, CD11c, and CD68. �
Systemic Inflammation
Recent research studies have determined that the neuroinflammation from primed microglial cells can also cause the pathogenesis of AD. Continuous activation of microglia can promote the synthesis and secretion of pro-inflammatory cytokines and trigger a pro-inflammatory response, ultimately causing neuronal damage. Neuroinflammation is an early symptom in the progression of AD. The microglia can have a tremendous effect on the inflammation of the human brain. �
The inflammation and health issues of the CNS can be associated with systemic inflammation through molecular pathways. One research study demonstrated that ROS development of primed microglia decreases the levels of intracellular glutathione and increases nitric oxide in NADPH oxidase subunit NOX2. Moreover, researchers demonstrated that these simultaneously occurring processes ultimately cause the development of more neurotoxic peroxynitrite. This is demonstrated in rodents with peripheral LPS or proinflammatory cytokines, such as TNF-?, IL-1?, and IL-6, IL-33. �
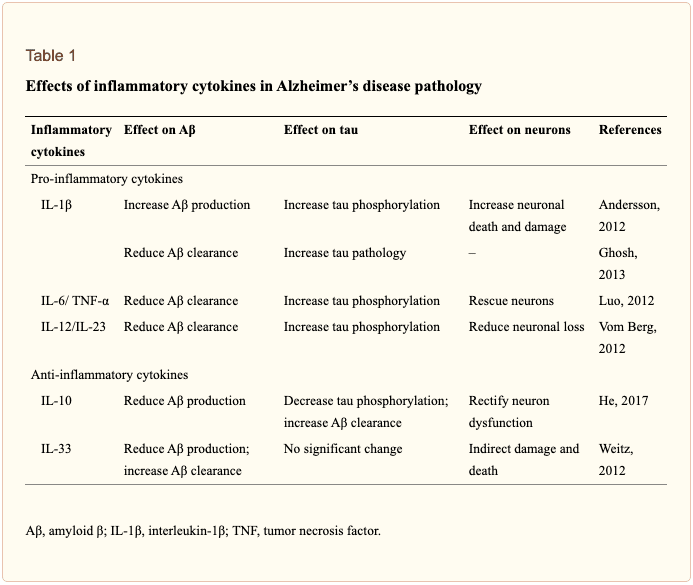
The outcome measures of numerous research studies have demonstrated that systemic inflammation can cause microglial activation. The results of the research studies emphasize the variability of the inflammatory response in the human brain associated with AD and the underlying health issues associated with systemic inflammation and neuroinflammation, as shown in Table 1. MAPK (mitogen-activated protein kinase) signaling pathways regulate mechanisms of the eukaryotic cell and microglial MAPK can also cause an inflammatory response to the aged brain with AD. Furthermore, chronic or continuous systemic inflammation causes neuroinflammation, resulting in the onset and accelerating the progression of AD. �
�
Genetic Regulation
In the aging human brain, gene regulation has ultimately been associated with an innate immune response. Recent preclinical, bioinformatics, and genetic data have demonstrated that the activation of the brain immune system is associated with the pathology of AD and causes the pathogenesis of this neurological disease. Genome-wide association studies (GWAS), functional genomics, and even proteomic evaluations of cerebrospinal fluid (CSF) and blood have demonstrated that dysfunctional immune pathways from genic mutation are risk factors in LOAD, which is the vast majority of AD. �
GWAS have become a fundamental tool in the screening of genes as well as demonstrating several new risk genes associated with AD. Apolipoprotein E (APOE) ?4allele is one of the most considerable and well-known risk genes for sporadic AD and this mutation ultimately increases the risk of neurological disease onset by 15 times in homozygous carriers and by three times in heterozygous carriers. Further research studies have demonstrated how microglial cell function can be affected through a variety of rare mutations which have demonstrated to have an increased risk factor of Alzheimer’s disease. �
An extracellular domain mutation of the TREM2 gene has also demonstrated an almost identical extent with APOE?4 in increasing the risk factor of AD. TREM2 is increasingly demonstrated on the surface of microglia and mediates phagocytosis as well as the removal of neuronal debris. Additionally, several other genes, such as PICALM, Bin1, CLU, CR1, MS4A, and CD33 have been demonstrated as risk genes for AD. Most of the risk mutation genes are expressed by microglial cells. �
Blood-Brain Barrier (BBB) Impairment
The blood-brain barrier (BBB) is a specialized barrier commonly developed between the blood and the brain by tight liner sheets consisting of specific endothelial cells and tight junctions or structures which connects a variety of cells together. The CNS is fundamental for the human body, and the BBB is fundamental for the CNS. The BBB and the blood-nerve barrier develop a defense system to control the communications of cells and soluble factors between blood and neural tissue where it plays a considerable role in maintaining and regulating the homeostasis of the CNS and peripheral nervous system. �
With development, continuous inflammation can also cause damage to the BBB. This damage can ultimately cause loss of hypersensitive neurons, neuroinflammatory regions, and focal white matter impairment following the damage. The compromised BBB also allows more leukocytes to enter into the CNS where an immune response can be aggravated by brain microglia under the condition of peripheral inflammation. These processes may ultimately be under the control of chemokine and cytokine signaling which can also have an effect on brain microglial cells as well as other health issues in AD. �
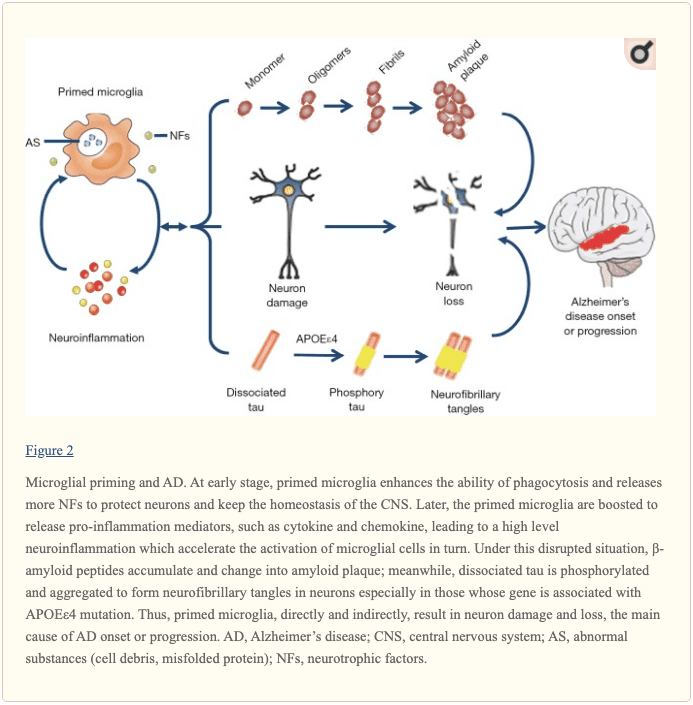
By way of instance, it has been determined that TNF-?, IL-17A, and IL-1? can reduce the tight junctions and eliminate the BBB. Loss of BBB integrity and abnormal expression of tight junctions are associated with neuroinflammation. Several research studies also demonstrated in an animal model of AD that the vulnerability of BBB to inflammation increases. Current evidence has also demonstrated that the BBB integrity is fundamental while further evidence of the BBB may demonstrate a new treatment approach for AD associated with microglial priming as shown in Figure 2 below. �
�
Conclusion
Microglia play a fundamental role in maintaining and regulating the homeostasis of the CNS’s micro-environment. If the balance of the homeostasis of the human brain is interrupted, the microglial cells can be activated to restore the balance in the CNS by defending against the stimulation and protecting the structure and function of the brain. However, chronic and continuous stimulation can trigger microglia into a state known as microglial priming, which is more sensitive to potentially minor stimulation, causing a variety of health issues, such as central sensitization, chronic pain, and fibromyalgia. �
Microglial priming mainly causes the boost of A?, tau protein as well as neuroinflammation and reduces neurotrophic factors which can cause the loss of healthy brain cells or neurons as well as the development of neuritic plaques and neurofibrillary tangles which are associated with Alzheimer’s disease. Although this �double-edged sword� plays a fundamental role, it can increase the progression of abnormal protein development and aggravate neuronal loss and dysfunction. However, research studies have ultimately demonstrated that aging can cause the progression of AD and there’s not much we can do about it. �
Microglial cells play a fundamental role as the protectors of the brain and they ultimately help maintain as well as regulate the homeostasis of the CNS microenvironment. However, continuous stimulation can cause the microglia to trigger and activate at a much stronger state which is known as microglial priming. Once the microglial cells go into protective mode, however, primed microglia can become much more sensitive to even minor stimulation and they have a much stronger possibility of reacting towards normal cells. Microglial priming has been associated with neuroinflammation and Alzheimer’s disease (AD) as well as central sensitization and fibromyalgia. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
AD is one of the most common types of dementia among older adults. However, the pathogenesis of AD is misunderstood and there is no definitive treatment for the neurological disease. Research studies have ultimately demonstrated that the activation and priming of microglial cells may contribute to the pathogenesis of AD. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Neural Zoomer Plus for Neurological Disease
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention. �
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force.
In the last article, we talked about how the microbiomes in our body worked and functioned. As well as learning what each microbe does in our bodies but mostly in our gut. When we are learning more and more about the microbiome, we discover many exciting things that our bodies are capable of as well as being the workers in our intricate immune system. In today�s article, we will be taking a look at what polyphenols does to our microbiomes as well as specific vitamins that are very helpful to our gut and going in-depth more with SCFAs (Short Chain Fatty Acids) and the Tight Junction.
Contents
The Role of Polyphenols in Microbiome Balance
Polyphenols, or phenolic compounds, are considered a type of micronutrients, and they are plentiful in plants. They have been well-studied for their role in the prevention of chronic diseases such as CVD, cancer, and neurodegenerative diseases. They also have antioxidant properties, and there are several hundreds of polyphenols that are found in edible plants that serve a giant purpose of defending our bodies against ultraviolet radiation or aggression by pathogens.
To figure this out, think of it like this: The bacteria in our large intestine releases polyphenols from the plants we eat in our diets. It is then transformed into a diet composition that alters the bacterial ecosystem (through the prebiotic effects and antimicrobial properties) to make our gut happy.
Here are some of the microbes that are in polyphenols:
Phenolic acids: These are derivatives of benzoic acid and derivatives of cinnamic acid.
Flavonoids: These microbes contain flavonols (e.g., quercetin), flavones, isoflavones (e.g., phytoestrogens), flavanones, anthocyanidins, and flavanols (e.g., catechins and proanthocyanidins)
Stilbenes: These microbes are resveratrol
Lignans: these are minor in the human diet and are linseed oil
Surprisingly some factors affect the polyphenol content of plants, and these include:
The ripeness at the time of harvest
The environmental factors (exposure to light, soil nutrients, pesticides)
processing and storage
When we eat organic fruits and vegetables, they have more polyphenol content that is usually, due to growing under slightly more stressed conditions. Which requires the plant to generate a stronger �defense and healing� response to the environment, and only 5�10% of the total polyphenol intake is absorbed in the small intestine. And 90-95% polyphenols that are linked to fibrous components must be liberated through hydrolysis by bacteria in the large intestine.
Surprisingly some polyphenols do not show up in plasma in humans after ingestion, and a large quantity is metabolized by intestinal bacteria or used to neutralize various pro-oxidizing agents in the intestinal lumen.
Clostridium and Eubacterium (which are both Firmicutes), are the primary metabolizers of polyphenols. Studies theorized that higher polyphenol intake may play a role in shaping the Bacteroidetes to Firmicutes ratio (e.g., inflammatory response potential, obesity, etc.) and can be harmful to our bodies.
However, more recent studies have shown effects of inhibition on Clostridium and Staphylococcus of polyphenols such as grape seed extract, in favor of Lactobacillus and other studies have demonstrated potent inhibition of phenolic compounds thymol (thyme) and carvacrol (oregano) on Escherichia, Clostridia and other pathogens, while simultaneously leaving Lactobacilli and Bifidobacteria have been unaffected.
Here are some other examples of some polyphenols:
Resveratrol increases Clostridia, Lactobacillus, and Bifidobacteria
Blueberry phenolics increase Bifidobacteria
Phenolic compounds in tea suppress C difficile and C perfringens
Catechins (found in high doses in teas and chocolate) act on different bacterial species (E. coli, Bordetella bronchiseptica, Serratia marcescens, Klebsiella pneumonia, Salmonella cholestasis, Pseudomonas aeruginosa, Staphylococcus aureus, and Bacillus subtilis) by generating hydrogen peroxide and by altering the permeability of the microbial membrane
Some studies have shown that polyphenols can interfere with bacterial cell signaling and quorum sensing (environmental sampling)
Polyphenols can also cause bacterial populations to stop expansion through signaling interference
Some research indicates certain polyphenols may be able to block the production of bacterial toxins (H. pylori and tea/wine polyphenols)
The Applications for A Diet
When it comes to eating a healthy diet, variety does matter. The colors, the types of fibers each organic food has, and whether you are going to do it daily or weekly. When you are trying to be in a healthy lifestyle, it always starts with the food. When you are looking for fresh produce, try to emphasize fresh, organic, and minimally processed versions of polyphenol-rich foods. However, don�t boil produce. Instead, try steaming then, and it is the best, but roasting or light frying is not only better, but it tastes so good.
Vitamins that help our Microbiome
When we are older, we tend to lose specific vitamins that actually helps us and our bodies to be healthier. Here are some of the vitamins that are really good for our gut and can help us prevent leaky gut.
Vitamin D
Vitamin D controls the development of gut-associated lymphoid tissue in our bodies. It is trafficking between gut dendritic cells, and they can differentiation of T-regs and T-reg function in our gut. But the expression of VDR, which influences IL (interleukin) production and tight junction integrity to help our gut.
When it comes to our gut, here are some of the effects of Vitamin D on the gut microbiome. The higher the Vitamin D levels are, they will allow commensal bacteria to secrete more AMPs (antimicrobial peptides). When patients take a high dose of Vitamin D, over 5 weeks can lead to a significant reduction in Pseudomonas spp and Shigella/Escherichia spp in upper gut intestines.
Another thing that Vitamin D does is that it can increase T cell differentiation in the colon. A lack of T-regs increased the incidence of asthma, allergies, autoimmune, and autism. But T-regs can prevent the development of aberrant immune responses such as autoimmune and food sensitivities. We here at Injury Medical Clinic, talk about functional medicine to our patients and try to help them recover from their ailments.
Because Vitamin D exposure fluctuates seasonally for many individuals, it has been observed that lower Vitamin D levels in the winter tend to lead to changes in the intestinal microbial balance. This will make our bodies have a decreased level of Bacteroidetes and an increased level of Firmicutes. This is the reason for �winter weight gain� in many individuals as F: B ratio changes.
Vitamin A
This is a retinoic acid that is required by dendritic cells (DCs) to induce T-cells (and B cells) which are the �tracking and regulation system� of the mucosal immune response. Because of this, T-cells must differentiate into T-regs to maintain a �calm and cool� system or immune tolerance to both our environment, symbiotic organisms, and food.
Omega-3 Fatty Acids
We talked about Omega-3s in a previous article as they are one of the many supplements that we can�t produce in our bodies. It can be mostly found in fish, and some plants can contain omega-3s. But it is a vital team player when we are trying to be healthy and can prevent a leaky gut. Not only that but omega-3s are crucial importance to more youthful skin.
SCFAs (Short Chained Fatty Acids)
SCFAs (Short Chained Fatty Acids)�are well-studied to demonstrate anti-inflammatory properties in the large intestine. They are the primary source of fuel for cells lining the intestinal epithelium of the large intestine. They contained: �Butyrate, Proprionate, Acetate. In a previous article, we discussed what SCFAs do when we eat fatty food. It can be both good or bad, depending on what kinds of food you consume. SCFAs act on G-protein coupled receptors to induce differentiation of T-cells, but also on those GPRs in DCs. They can both be direct and indirect influences on our gut.
SCFAs can produce bacteria and can directly impact T-reg production. And that SCFAs inhibit the mucosa and competitively inhibit opportunists. Some foods that provide higher resistant starch will typically yield the most short-chain fatty acids upon microbial fermentation
Tight Junction Modulations
The tight junctions are the gateways between the epithelial cells. In a previous article, we took a look at what the tight junction is. They control the flow of nutrients, macromolecules, and other substances that are usually allowed to pass through without cellular diffusion or absorption.
Conclusion
All in all, we covered a lot of information about what polyphenols does as well as specific vitamins and supplements that can help our bodies prevent a leaky gut. The microbiomes in our collection and the use of functional medicine can be beneficial in helping us not only to a better, healthier life but, a working, functional body for us when we are older. Tomorrow we will end this three-part series with foods and tips to have a healthy microbiome in our gut and our bodies.
These medications help return normal function to the osteoclasts and osteoblasts.
Bisphosphonates can manage the disease and reduce symptoms, but do not cure the disease.
Living with Paget�s
Advanced cases can cause spine problems, which includes spinal fractures.
Most with Paget�s disease have preferable outcomes.
When Paget’s disease is managed with medication, regular doctor visits, chiropractic care, and proper diet, then there shouldn�t be a problem in achieving a healthy quality of life.
El Paso, TX Lower Back Bain Pain Chiropractic Relief
David Garcia, maintenance Centre Employee and a proud Dad in El Paso, TX works at the Region 19 Education Services Center. However, Mr. Garcia’s daily life is frequently influenced by his chronic lower back pain. After undergoing worsening symptoms for a while, David Garcia was advocated to seek chiropractic care with Dr. Alex Jimenez by his sister, a former patient of Dr. Jimenez. Mr. Garcia has since experienced enormous relief out of his lower back pain, and he’s grateful to Dr. Alex Jimenez and his staff for supplying him with schooling regarding his health problems as well as adequately caring for him. David Garcia urges Dr. Alex Jimenez as the non-invasive surgical selection for lower back pain.
NCBI Resources
Several studies show that chiropractic care is a very effective treatment for back pain. The chiropractor will perform spinal manipulation to bring the spine (and body) into proper alignment. He may also offer advice on exercises, stretching, and ways to improve posture as well as recommending lifestyle changes and what to look for in supportive shoes. Chiropractic�s whole-body approach not only helps relieve back pain, but it also helps prevent it as well.
This allows the patient to gain whole body benefits from chiropractic.
To understand exactly how lipopolysaccharides and gram-negative bugs affect the immune system we must first investigate what lipopolysaccharides are and their role in gram-negative bacteria and the human body as a whole.
Contents
LPS (Lipopolysaccharides)
Lipopolysaccharides (LPS) are large molecules consisting of a lipid (fatty acid) and a polysaccharide composed of the O-antigen, outer core, and the inner core all joined by covalent bonds. �Lipid A in LPS is the hydrophobic component responsible for the major bioactivity of LPS. Hydrophilic polysaccharides consist of long chains of monosaccharides (simple sugars) linked together by glycosidic linkages. LPS play their role in the outer membrane of gram-negative bacteria by supporting the structure of the bacteria and shielding the membrane from chemical attack. Gram-negative bacteria are related to foodborne diseases, respiratory infections, plagues, and some sexually transmitted diseases. Some gram-negative bacteria have become so resistant to antibiotic drugs that they are often very difficult to treat and unfortunately vaccines are not available for these types of bacterial infections. Additional enzymes can sometimes alter the structure of the LPS, and though the structure is not required for the bacteria�s survival it is closely related to the virulence of bacteria. For example, the lipid A component of LPS can cause toxic reactions when lysed by immune cells. LPS in humans trigger the immune system to produce cytokines (hormone regulators). Production of cytokines is a common cause of inflammation.
Now that we are able to recognize the relationship between LPS, gram-negative bacteria, and inflammation/infections in the human body, we must understand how to prevent and treat infections related to gram-negative bacteria. Gram-negative bacterial infections are caused by contact between infected and non-infected peoples. They are very common in healthcare settings, but by taking simple measures such as hand washing and keeping a strong immune system will help prevent them. How do we keep a strong immune system? Choosing a healthy lifestyle is the first most basic step in this process. Because the immune system is a system, we must understand that there is no direct way to improve its strength. It is strengthened through what we put into our body and how we treat our body. However, it is important to distinguish between building a strong immune system and boosting the number of immune cells in our body. It is potentially harmful to boost the number of immune cells because there are so many different kinds of cells in the immune system that respond to so many different microbes in so many ways. Diet, exercise, reducing stress levels, and some herbs and supplements all contribute to building and supporting a strong immune system.
Conclusion
Throughout this article, we have learned about lipopolysaccharides and the role they play in gram-negative bacteria. Gram-negative bacteria are known to be harmful to the human body so we have found ways to prevent the harmful infections it causes. The immune system plays an obviously important role in fighting infections, but it needs to be strong to support our body and fight infections efficiently. This basic knowledge is provided to set the basis for further research on how to support the immune system.
The microbiomes in our bodies are fascinating. They help our various organs function correctly, helping out our immune systems battle terrible stuff. They can tell us what we are doing to our bodies when we consume food. However, the microbiomes in our gut tell us a different story as we are going to discuss what does microbiomes do as it functions in our body as well as our gut.
The relationship between the gut microbiota and its host plays a crucial role in:
immune system maturation
food digestion
drug metabolism
detoxification
vitamin production
prevention of pathogenic bacterial adhesion
Also, the composition of the microbiota is influenced by environmental factors such as diet, antibiotic therapy, and environmental exposure to microorganisms.
Contents
Why Don�t We All Have the Same Microbiome?
Whenever we are trying to live a healthy lifestyle, our bodies will go through so many changes. When we get rid of the bad stuff that is causing us problems and the beautiful thing start taking effect in what we put in our bodies. We, as humans, have different body structures and body types that are way different. Some people lose or gain weight differently. When other people exercises, they go at their own pace, and several factors influence the bacterial composition in taxa type and abundance. These factors include:
host phenotype, such as age, gender, body mass index (BMI)
lifestyle
immune function
geographical belonging and environmental factors
use of antibiotics, drugs, and probiotics
DIET
Moreover, long-term dietary habits have been shown to play a crucial role in creating an inter-individual variation in microbiota composition.
Manipulating the Microbiome: Key Terms
Here are some key terms to remember when we are talking about the microbiome.
Stability: resistance to change and the ability to maintain homeostasis.
Resilience: capacity to return to homeostasis after disturbance.
Diversity: DIVERSE microbiomes are more stable and more resilient (to antibiotics); more resistant to foreign invasion (pathogens).
Relative Abundance: Even �good� bacteria can be too abundant without balance from symbiotic species; the presence of �bad� bacteria is not necessarily always harmful if enough �good� are there to balance.
Colonization Resistance: The capacity of the microbiome communities to resist new colonization by pathogens and other transients.
This is a KEY factor for preventing GI infections; but also explains why probiotics are not always practical.
Our COMMENSAL microbiome is our first line and of defense
Restore balance/� reseeding�: (the term �reinoculate� is not really correct) Probiotics; Fermented foods; Prebiotics/Polyphenols.
Advantages to DNA Testing
For many practitioners, measuring microorganism DNA allows for:
Detection of a more diverse collection of microorganisms, (more genus and species, particularly anaerobic species)
They can measure at the species and subspecies level
They have a much better snapshot of dysbiosis and diversity
Have better accuracy of results
Much faster turnaround time and much less expensive
Concept of �epigenetics.�
However, DNA is DNA-dead or alive whenever practitioners are looking at a patient�s DNA structure. Culture Technology is still considered �gold standard� but has several limitations. They are trying to culture anaerobic bacteria, but some of the most important bacteria are anaerobic commensals. There is a limited detection of several microorganisms, but it�s usually genus level only. Microorganisms can grow and/or die in transit and what�s measured in the culture dish is not always 100% indicative of the sample at the time of collection; the environment can morph while in transit to the lab and changes in pH etc.
Important Groups
These are some of the microbiomes that are very functional to our bodies and what parts do they play.
Commensals
This microbiome provides the host with essential nutrients and contains Aerobic and Anaerobic microbiomes.
Aerobic (survives better in oxygenated environments; less prevalent in the colon, however, some are considered �obligate anaerobes�). They are:
Lactobacillus
Bifidobacterium
Bacillus
Anaerobic (more likely to be found colonizing the distal colon due to limited oxygen). They are:
Clostridia
Akkermansia
Lactobacillus and Bifidobacteria
These two are the most well-researched genus of bacteria. They are widely available in commercially available probiotic products.
Lactobacillus are:
lactic-acid forming bacteria
Form biofilms which allow surviving harsh/low pH conditions (stomach acid)
Helps maintain the integrity of the intestinal barrier
Abundant in probiotics/fermented foods
Bifidobacteria are:
One of the first bacteria to colonize the gut after birth
Aids in digestion, reducing inflammation, and stimulation of immune cells
Bacillus
These are spore-forming bacteria. They form spores in harsh environments which makes them more resilient, heat-stable, and have better viability in the gastric environment. But they may have better efficacy as probiotic therapy in SIBO population. These are in another category of commercially-produced probiotics beyond the standard Lactobacillus and Bifidobacterium.
In the health world, known as �Soil Based Probiotics.� They are very prominent in the environment and their primary role in immunomodulation; stimulation of the immune system. They are a production of GALT-Gut Associated Lymphoid Tissue and are known to be significant players in the production of B Vitamins and Vitamin K2 in the gut known as Bacillus subtilis
Clostridia
These are a major anaerobic group of commensals. They comprise 10% to >50% of the microbiome and are critical for the health of the gut barrier and intestinal lining, and barrier integrity. These are essential producers of butyrate (SCFA) and secondary bile acids. They also thrive on a high and diverse fiber diet, grape, and red wine polyphenols such as Blautia, Butyrivibrio, Eubacterium, Faecalibacterium prausnitizi, Roseburia, Ruminococcus, etc. However, there are usually no probiotic supplements to directly increase the abundance of clostridia.
Akkermansia
These microbiomes make up 1-3% of a healthy microbiome, and they help maintain the health and integrity of the mucosal barrier.
Akkermansia muciniphila = mucin lover
They also help with reducing inflammation and may impart protection of inflammatory bowel diseases. These microbiomes are keystone species that are highly correlated with higher microbiome diversity.
Proteobacteria
This is a PHYLUM category of bacteria. This microbiome contains gram-negative and all bacteria that carries an LPS. This group includes plenty of beneficial bacteria but also contains several pathogens that tend to thrive in pro-inflammatory condition.
Gram (+) vs Gram (-) Bacteria
These two types of bacteria are in our bodies as they have very different functions that can either protect or disrupt our gut.
Gram-Positive (+) contains:
Peptidoglycan
Lipoteichoic acid
Gram-Negative (-) contains:
LPS as a component of their cell wall
LPS is a very powerful ENDOTOXIN- a known contributor to induce significant inflammation and potent immune response
LPS antibodies are measured on Vibrant Wellness Wheat Zoomer/Intestinal Permeability Panel
However we can�t generalize Gram (-) as �bad� or Gram (+) as �good� or vice-versa, but we can control it with the Zoomers test.
LPS(Lipopolysaccharide)
In the last article, we mentioned them briefly, but here is a refresher on what theses microbes do. They are a fat/sugar molecule that lines the gram-negative bacteria inside the gut, and they protect those bacteria from bile salts. They are present inside the gut lumen under normal physiological conditions, and they usually should not enter the bloodstream. But if it does open in the blood then�
1) LPS antibodies are created-tagged as �non-self.�
4) Can help differentiate if leaky gut is happening between cells or through cells (or both), which are Transcellular vs. Paracellular pathways
Conclusion
These are the microbiomes that are in our body and how each of them plays a role to make our bodies healthy. We here at Injury Medical Clinic, do talk with our patients about what goes on in their bodies. We inform them on how to take care of themselves through the means of functional medicine. This is part one of a three-part series since tomorrow we will be discussing the roles of polyphenols in the Microbiome balance.
Before and after spine surgery the surgeon and medical staff prepare you for recovery. The recovery process can take a long time and be extremely challenging.
Pain after spine surgery is normal, but how to tell if it�s beyond the typical pain during recovery?
Contents
What indicates that the surgery failed?
Chiropractor Dr. Alex Jimenez has dealt with this issue throughout his career and discusses symptoms associated with failed back surgery syndrome (FBSS, also known as failed back surgery (FBS) or post-laminectomy syndrome).
Back Pain the most common symptom
Chronic back pain is the most common symptom from failed back surgery.
With FBSS, chronic pain in one patient can be very different from pain in another.
People with FBSS can experience a range of different types of pain based on:
Spinal disorder
Spinal procedure
The underlying cause of failed back surgery syndrome
Types of back and neck pain people with failed back surgery may experience. Some may have one or more types.
Chronic pain:
Sustained pain that lasts for more than 12 weeks.
Chronic pain is the opposite of acute pain, which is short-term�severe pain.
Acute pain is expected during spine surgery recovery but should fade during the healing.
Nociceptive pain:
Localized pain that can be dull or sharp.
This is the type of pain patients may experience immediately after surgery
Example: The pain felt around where the incision was made.
When most people think of pain, nociceptive pain is the type.
Neuropathic pain (neuropathy):
Nerve-related pain is caused by damage to the nerves or spinal cord.
Neuropathic pain shoots and moves around, thus affecting large areas of the body.
Examples of this type of pain include:
Numbness
Burning
Tingling
Weakness
Abnormal sensations (called paresthesia)
Radicular pain (radiculopathy):
A branch of nerve pain (neuropathy) is called radiculopathy, or radicular pain.
Radicular pain radiates from one area to another.
Examples include from the:
Low back
Down the buttocks
Legs
Feet
And then starts all over again, or goes in a different order.
Other symptoms:
The original symptoms return:
When the symptoms that put the patient in the surgery room return, then there is a definite possibility of failed back surgery.
New pain presents:
New pain, meaning pain in a different part of the spine or a different type merits a discussion with your doctor.
Mobility Reduced :
It does take time to recover and that process can affect:
Endurance
Flexibility
Movement
However, if mobility or limitation is different from what was talked about with the surgeon or develops after recovery, then it should be discussed with your doctor.
Example: A limited range of motion in the neck or low back.
Headaches begin to present:
If headaches were not an original part of your medical history, this may point to a nerve problem.
Nerve Symptoms & Quality of Life
Neuropathic pain/ neuropathy or nerve-related pain is the most complex, debilitating, and difficult-to-treat.
People who experience this type of pain find it lowers their quality of life.
An online survey of 1,000-2000 patients that underwent low back surgery responded and revealed the following:
94% of respondents reported post-surgery low back pain
A separate study noted that nerve-related pain suffered by people with FBSS is more life-altering than pain caused by joint and nerve disorders.
Patients with FBSS and neuropathic pain go through higher levels of pain and have less quality of life/physical function compared with people with osteoarthritis, rheumatoid arthritis, and fibromyalgia.
FBS Symptoms Emergency Treatment
After surgery, it can be difficult to tell whether the pain is within the bounds of normal recovery pain.
At follow-up appointments ask questions about the progress of your recovery and about any concerns.
Pain after surgery is normal, but there are some signs and symptoms that merit emergency attention.
If you experience any of the red flag symptoms, call your doctor immediately:
Symptoms of Failed Back Surgery Syndrome Are Different for Every Patient
Every patient goes through a unique surgical experience and if it fails, patients may experience unique symptoms.
Because failed back surgery has several possible causes, the symptoms are going to be different for each patient.
Before you are discharged and even before you go under, ask your surgeon questions about what to expect during the recovery process.
Educating yourself with possible expectations during recovery, you�ll be best positioned to know when things aren�t going as they should.
Low Back Pain Management El Paso, TX Chiropractor
Denise suffered an auto accident injury which resulted in back pain. When she realized she could not sit, walk or sleep for lengthy periods of time without having painful symptoms, Denise found chiropractic care with Dr. Alex Jimenez at El Paso, TX. Once she received therapy for her automobile accident injuries, Denise experienced relief from her symptoms and she was able to execute her regular tasks once again. Thanks to the education and maintenance Dr. Alex Jimenez supplied, Denise regained her initial health and health.
Back pain is more most common, with roughly nine out of ten adults undergoing it at some time in their lifetime, and five functioning adults developing it annually. Some quote around 95 percent of Americans will experience back pain at some time in their lifetime. It is undoubtedly the typical cause of chronic pain since it’s also a substantial contributor to missed work and handicap. In the United States alone, acute cases of lower back pain are the fifth most frequent reason for doctor visits and cause 40% of missed days off work. What’s more, it is the leading cause of disability worldwide.
NCBI Resources
Aside from the obvious invasiveness of the procedure as well as recovery time and probable physical therapy that would be required as part of your aftercare. Say you have neck or back pain. How will you treat it? Many people will go to a medical doctor who will look at the symptoms, such as pain, and treat it with a prescription or over the counter medications. In some cases, they may recommend surgery to manage the pain or correct the problem.
Microglial cells make up about 10 to 15 percent of all the glial cells in the human body, which can be found in the central nervous system (CNS) and play a fundamental role in the human brain. Microglial cells are responsible for maintaining and regulating changes in the physiological and pathological condition of the CNS by changing their morphology, phenotype and function. In an average physiological state, the microglial cells are continuously in charge of controlling their environment. �
However, when the homeostasis of the brain is interrupted, the microglia change into an amoeba-like shape and become a phagocyte where they can actively reveal a variety of antigens. If the homeostasis interruption in the CNS continues, the microglial cells will then trigger at a much stronger state, which is known as microglial priming. Microglia are the “Bruce Banner” of the CNS. However, once they go into protective “Hulk” mode, primed microglia become much more sensitive to stimulation and they have a much stronger possibility of reacting to stimulation, even reacting towards normal cells. �
�
Microglial priming can become a double-edged sword. As a matter of fact, primed microglia are created from different phenotypes of microglia and the phenotypes are context-dependent, which means they are associated to the sequence and duration of their exposure to different varieties of stimulation in a variety of pathologies. In the article below, we will demonstrate the effect of microglial priming on the central nervous system (CNS), especially in neurological diseases. �
Contents
Role of Microglial Cells in the CNS
Microglial cells are commonly found in the central nervous system (CNS), where they are considered to be one of the most flexible types of brain cells. Microglial cells are created from precursor cells found within mesoderm bone marrow, or more specifically found in the mesodermal yolk sac, and they are divided in different densities throughout several regions of the brain. As mentioned above, microglia will remain in a dormant state when the homeostasis of the brain remains stable. �
Microglia have a small cell body and morphological branches which extend towards all directions to help maintain and regulate the overall function of the CNS. Changes in their microenvironment can trigger microglia into an “activated� state. Research studies have demonstrated that microglia play a fundamental role in brain development and a variety of functions, including synaptic pruning and clearing out cell debris. Moreover, microglia create an immune surveillance system in the human brain and control fundamental processes associated with a variety of pathologies, including the clearance and uptake of A? and abnormal tau protein as well as the production of neurotrophic factors and neuroinflammatory factors. �
Microglial Priming Overview
Microglial priming activates when continuous interruptions in the brain’s microenvironment trigger a much stronger microglial response compared to an initial interruption which simply triggers microglial activation. Primed microglia in the CNS are also much more sensitive to possibly minor stimulation. This increased response involves microglial proliferation, morphology, physiology, and biochemical markers or phenotype. However, these changes will ultimately promote an increase in cytokines and inflammation mediator production which can have a tremendous impact on synaptic plasticity, neuronic survival, individual cognitive and behavioral function. Below is an overview of the effects of microglial priming in the CNS. �
Mechanisms of Microglial Priming in the CNS
The microenvironment of the central nervous system (CNS), by way of instance, is one of the main factors which can affect the microglial cells. Increased oxidative stress, lipid peroxidation and DNA damage associated with brain aging can all commonly trigger microglial priming. Another common factor for microglial priming includes traumatic brain injury. Research studies have shown that traumatic CNS injury activates microglia as well as the development of primed microglia. �
Many research studies have also shown that both focal and diffuse traumatic brain injury increase inflammation in the brain associated with microglia and astrocytes. CNS infections can also trigger microglial priming where viruses are the main cause of CNS infection. Both DNA and RNA viruses can trigger microglial priming including microglia and astrocytes. Recent research studies have shown that complement dysfunction can change the expression of complement receptors and trigger microglial priming after continuous activation following a variety of functions, including synapse maturation, immune product clearance, hematopoietic stem/progenitor cells (HSPC) mobilization, lipid metabolism, and tissue regeneration. �
Moreover, research studies have shown that there is increased priming of the microglia in a variety of neurological diseases. By way of instance, microglial cells with a morphological phenotype are found in large numbers in the human brain. In the last several years, research studies have suggested that neuroinflammation can continuously activate the microglia and trigger microglial priming. Furthermore, all of the previously mentioned situations are closely associated with neuroinflammation. Research studies have also demonstrated that neuroinflammation, as well as microbial debris and metabolic effects, are associated with central sensitization in neurological diseases, such as fibromyalgia, also referred to as the “brain on fire”. �
In the context of the previous situations mentioned above, microglia are primed though a series of pro-inflammatory stimulation, such as lipopolysaccharide (LPS), pathogenetic proteins (e.g., A?), ?synuclein, human immunodeficiency virus (HIV)-Tat, mutant huntingtin, mutant superoxide dismutase 1 and chromogranin A. There is also a variety of signaling pathways and it is common for different types of cells to express special pattern recognition receptors (PRRs) which can affect inflammatory signaling pathways. By way of instance, several signaling pathways, known as pathogen-associated molecular patterns (PAMPs), which can commonly increase in infected tissue, could also control microbial molecules. �
Additionally, peptides or mislocalized nucleic acids identified as misfolded proteins through a series of pathways, known as danger-associated molecular patterns (DAMPs), can also cause microglial priming. Toll-like receptors (TLRs) and carbohydrate-binding receptors commonly function in these pathways. There are also many different receptors found in microglia, including triggering receptors expressed on myeloid cells (TREM), Fc? receptors (Fc?Rs), CD200 receptor (CD200R), receptor for advanced glycation end products (RAGE), chemokine receptors (CX3CR1, CCR2, CXCR4, CCR5, and CXCR3), which can be recognized and mixed in with other signaling pathways, although some pathways are still not clear. �
Consequences of Microglial Priming in the CNS
Microglia show a low rate of mitosis in their normal state and a high rate of proliferation after microglial priming, showing that the microglia have the ability to affect cell turnover and pro-inflammation stimulation. With continued stimulation, microglia activate from their resting state, changing into amoeboid microglial cells in morphology. However, the changes in the shape of the microglia cannot differentiate the characteristics of microglial activation and the function of primed microglia depends on their phenotypes which are associated with receptors and molecules which they create and recognize. �
The different types of tissue macrophages, under microenvironmental impetus, are able to differentiate M1 and M2 phenotypes. First, M1 polarization, also known as classical activation, ultimately needs interferon-? (IFN-?) to be mixed with TLR4 signaling which then causes the production of inducible nitric oxide synthases (iNOS), reactive oxygen species (ROS), proinflammatory cytokines, and finally, ultimately reduces the release of neurotrophic factors, ultimately causing inflammation with increased markers of main histocompatibility complex II (MHC II), interleukin-1? (IL-1?) and CD68. �
Moreover, M2 polarization, also known as alternative activation, is ultimately believed to be associated with tissue-supportive in the situation of wound healing, reducing inflammation and improving tissue repair of collagen form. They trigger in response to IL-4 and IL-13 in vivo. M2 polarization is characterized by the increased expression of neurotrophic factors, proteases, enzymes arginase 1 (ARG1), IL-10 transforming growth factor-? (TGF-?), scavenger receptor CD206 and coagulation factors as well as improving phagocytic activity. As a matter of fact, there are currently no clear boundaries between the two polarizations and the M1 phenotype shares many similar characteristics with the M2 phenotype. �
Another phenotype of primed microglia, known as acquired deactivation, has been recently discovered. This new phenotype overlaps with M2 and has the ability to improve anti-inflammatory and functional recovery. Additionally, a research study conducted ultra-structural analyses and identified a brand-new phenotype, known as �dark microglia�, which is rarely seen in the microglial cell’s resting state. Systemic inflammation triggers microglia into an activated state to promote cell and tissue recovery and achieve homeostasis. Microglial priming is ultimately the second interruption in the CNS microenvironment. �
The primed microglia is a double-edged sword for brain health. Many research studies in vivo and in vitro have shown that neurological diseases are associated with microglial activation. The inflammatory phenotypes of the microglia create neurotoxic factors, mediators and ROS which can affect the CNS. Primed microglia play a fundamental and beneficial role in neuronal regeneration, repair, and neurogenesis. Primed microglia are also much more sensitive and respond much stronger to brain injury, inflammation, and aging as well as increase the activation of microglial cells by switching from an anti-inflammation, potentially protective phenotype to a pro-inflammation destructive phenotype, as shown in (Figure 1). �
�
In the early stages of microglial priming, the ability and function to phagocytize cell debris, misfolded proteins, and inflammatory medium are increased where more protective molecules, such as IL-4, IL-13, IL-1RA, and scavenging receptors, are created. The changes can affect wound healing and damage tissue repairment, neuron protection, and homeostasis recovery. Classically activated microglia (M1) make up a large proportion of all microglia and promote an increased creation of neurotoxic factors, such as IL-1?, TNF-?, NO and H2O2 (6), where more microglia are primed immediately afterward. �
This increased and extended neuroinflammation caused by primed microglia can ultimately be associated with the development and clustering of the protein tau and A?. Furthermore, it can lead to loss of neurons as well as the decrease of cognitive function and memory, such as in Alzheimer’s disease. Although the mechanisms are not clear enough, people have reached an agreement that primed microglia cause a chronic proinflammatory response and a self-perpetuating cycle of neurotoxicity. And this is believed to be the key factor in brain health issues resulting in neurological diseases. �
Microglia are known as the protectors of the brain and they play a fundamental role in maintaining as well as regulating the homeostasis of the CNS microenvironment. Constant stimulation causes the microglia to trigger at a much stronger state, which is known as microglial priming. Microglial cells are the “Bruce Banner” of the CNS. However, once they go into protective “Hulk” mode, primed microglia become much more sensitive to stimulation and they have a much stronger possibility of reacting to stimulation, even reacting towards normal cells. �- Dr. Alex Jimenez D.C., C.C.S.T. Insight
Microglial cells make up about 10 to 15 percent of all the glial cells in the human body, which can be found in the central nervous system (CNS) and play a fundamental role in the human brain. Microglial cells are responsible for maintaining and regulating changes in the physiological and pathological condition of the CNS. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Neural Zoomer Plus for Neurological Disease
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention. �
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download�
* All of the above XYMOGEN policies remain strictly in force.
In the last three articles, we introduced the wheat zoomer, went in-depth about the intestinal permeability, and the microbes in our gut. We also talked about the hidden problem with gluten as well. Today we will be discussing what to do after your patient comes in for a check-up after completing their gut healing process. For this to work, patients have to be gluten-free for the results to work. After the healing phase, local chiropractors, health coaches, and physicians can introduce gluten back slowly into the patient’s diet.
Contents
Checkups
When the patient comes in for a check-up, here are some of the things doctors look for:
If everything is green, re-introducing gluten may be possible for patients.
If anything is still yellow or red, patients must continue to avoid gluten and keep the gut healing process until the test results are all green.
After the appointment, patients can retest the wheat zoomer in about 3-9 months. However, there are about 50% of individuals with celiac disease that may also have antibodies to casein and may have to go dairy-free to heal their gut. Although some individuals are gluten sensitive may not be lactose intolerant but can go dairy free if they want to.
Lectins
Surprisingly all plants have lectin, but some of them are not problematic to humans thankfully. Legumes and grains play a role in increasing the diversity of microbes that may be beneficial or harmful to our bodies. Wheat Germ Agglutinin is the only specific lectin to the Wheat Zoomer, but it doesn�t reflect the overall lectin sensitivity but, consider the lectin zoomer to determine any particular lectins that your patient is sensitive to without eliminating unnecessary foods that are beneficial to the gut healing process.
Soy
Many studies show that soy may be a problem due to the saponin since it does have higher lectin count. Here at Injury Medical clinic, we suggest that running the Lectin Zoomer on our patients with intestinal permeability makes sense for them to heal correctly. But animal studies stated that soybean agglutinin has the effect of the increasing release of zonulin away from the TJ (tight junction). And a human study reported that if the soy saponin is poorly absorbed or utilized by the human intestinal epithelial cell will end up metabolizing the intestinal bacteria and cause more harm to human.
Surfactants
Known as sucrose monoester fatty acids is mostly used in cosmetics, food preservatives, food additives. Sucrose esters are used as a surface treatment on some fruits like peaches, pears, cherries, apples, and bananas. It keeps the moisture on the peel or rind controlled. Sucrose mono ester used in cosmetics as an emulsifier.
Bone broth/Collagen
Up to this date, there are minimal studies that have examined the role of bone broth or collagen that it repairs the intestinal barrier. It all depends on the animal and the bone it comes from and the contents that people have put in a bone broth soup.
However, there is a small body of evidence for the use of collagen peptides seem to support the usage in their autoimmune disease treatment protocol. But the results cant be extrapolated whether bone broth would have similar effects. So more studying about bone broth is needed.
Organic Produce
When people say that they are going organic, it is beneficial for people that are willing to change to a healthy lifestyle. Granted that organically produces are locally grown, but still, organic produce or non-organic produce will not have less or safer pesticides. They are different, but all of the crops like fruits and vegetables are grown with pesticides.
Just like all fruits and vegetables, still, wash them thoroughly to reduce the number of pesticides and surfactants exposure and enjoy them to your heart’s content.
Resistant Starches
Resistant starch foods are a form of carbohydrates that can be converted to short fatty acids by SCFA-producing bacteria. With higher SCFA levels, these starches aid immune tolerance, T-cell differentiation, and intestinal barrier homeostasis. Other types of fibers are high value, and variety is essential. Like for example, cooked/cooled rice and potatoes are excellent resistance starch foods.
“Eat like a vegetarian who eats meat.”- Dr. Alex Jimenez�D.C., C.C.S.T.
Polyphenol Foods
Polyphenols, flavonoids and other phenolic compounds will aid to maintained TJ stability through inhibiting phosphorylation of TJ complexes.
Fermented Foods
Fermented food or drinks that contain live probiotic cultures are excellent in promoting a healthy gut. However, it is challenging to study fermented food and beverages due to highly variable stains, composition, nutrient content. But studies found that participants who drink a fermented plant extract drink saw improvements in their body and increased total antioxidants and total phenolic in plasma as well as with reducing total C and LDL-C.
Beneficial bacteria like Bifido and Lactobacillus were increased while E Coli and C perfringens were decreased in the gut. So drinking or eating fermented food can help our gut and help our bile growth to be flushed out.
Granted, we all know that trying to be healthy is very hard. It is true that even though exercising is easy because we can do it over and over again until we are masters at it but, when we overdo the exercises it will cause harm to our bodies and hurting it in the process. �Eating healthy is hard as well because our bodies may have a food allergen or a food sensitivity that will make us disappointed that we can�t enjoy the foods we want to eat. Yes, eliminating diets are very hard and challenging to follow in the long term and have poor compliances when we don�t put in the work. So start by exploring other tests to tailor patients diets to meet their health needs and prolong their recovery period.
Supplements
Supplements are fantastic to aid the valuable nutrients and minerals our bodies can�t produce. Common supplements prescribed include:
L-glutamine
Vitamin D3
Collagen
Colostrum
Zinc carnosine
Ox bile
Omega-3s
Turmeric/Quercetin
Magnesium
Stress Management
Granted that stress is part of our lives and we can manage small amounts of it, and it is beneficial to us, but some people have chronic stress and have to go to a doctor to get it treated. But there is hope as there are ways to manage stress and doing it functionally and naturally.
Conclusion
So all in all, just to recap, if your patient is good to go and their test results are all green, you can introduce gluten back to their diets again in small increments and can be rested in about 3 to 9 months. But if your patient does have a gluten allergen then just let them know that they must continue to be gluten-free. We here at Injury Medical Clinic, always put our patient�s needs first for them to live their best lives with functional natural medicine.
What exercise/stretches help reduce sciatic nerve pain?
Here are 4 exercise/stretches that your chiropractor/physical therapist may recommend to help you reduce sciatic nerve pain:
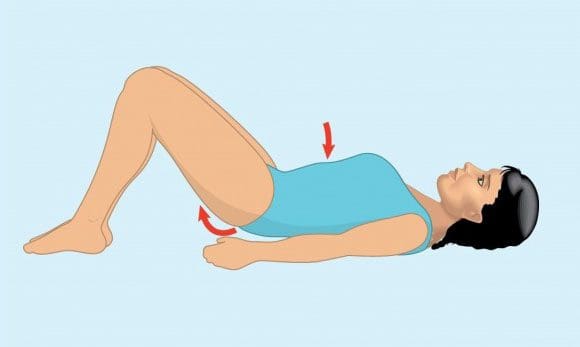
Pelvic tilt
Knee to chest
Lower trunk rotations
Arm and leg extensions
Pelvic Tilt
Its purpose is to strengthen the lower abdominal muscles and stretch the lower back.
How to do it:
Lie on back
Exhale and tighten abdominal muscles while pushing the belly button toward the floor and flatten the lower back
Hold the position for 5 seconds
Repeat 10 times holding the position for 5 seconds each
Am I doing it right?
Place the pinky finger on the hip bone and thumb on the lowest rib (same side).
When tightening the abdominal muscles, the amount of space between the pinky finger and thumb should get smaller.
Pelvic tilts help strengthen the lower abdominal muscles and stretch the low back.
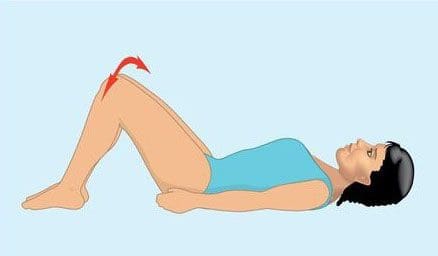
Knee to Chest
Its purpose is to help reduce nerve compression in the low back, that can help alleviate lower back pain.
Lie on back
Start with either� left or right knee and use hands to gently pull the bent knee toward chest
Hold for 10 seconds
Repeat movement on opposite knee
Perform 3 to 5 times holding position for 10 seconds each
Use hands to gently pull both knees toward chest
Hold for 10 seconds
Repeat movement with both knees 3 to 5 times holding position for 10 seconds each
Knee to chest exercise/stretches can help reduce nerve compression on the lumbar spine alleviating lower back pain.
Lower Trunk Rotation
Its purpose is to increase the spine�s mobility and flexibility.
Lie on back with both knees bent upright and both feet flat on the floor (aka the hook lying position).
Hold both knees together, rotate knees to one side
Hold for 3 to 5 seconds
There will be a gentle stretching sensation on the opposite side of lower back and hip area
Contract abdominal muscles and rotate both knees to opposite side
Hold for 3 to 5 seconds
Repeat 10 times on each side
Lower body rotations can help you strengthen your lower abdominal muscles and stretch your low back.�
All Fours Opposite Arm and Leg Extensions
Its purpose is to strengthen the abdominal muscles, low back and stabilize the areas.
Get in crawling position on all fours.
Contract abdominal muscles to keep back flat and straight
Raise one leg upward behind you and straighten outward
Hold for 3 to 5 seconds
Repeat the movement on the opposite side
Once this�exercise/stretch can be performed 10 times with functional pain, add arm movement with each leg extension:
Extend the arm (opposite side of leg) upward and outward in front of body
Hold for 3 to 5 seconds
Repeat on the opposite side
Perform 10 times
How do these exercise/stretches reduce sciatic pain
Abdominal and spinal muscles are essential components of the spine�s system.
These exercises/stretches can help:
Strengthen the spine
Increase flexibility
Increase range of motion
These exercises can help keep the spine�s structural components strong and healthy along with reducing pain and speeding up healing.
Regular exercise causes the body to release endorphins or hormones that interact with the pain receptors in the brain that reduce the perception of pain.
Will exercising with sciatica cause/exacerbate injury
Do not to perform any of these exercises without consulting your doctor,� spine specialist or chiropractor.
Whatever level of fitness, remember even trained professional athletes exercise with a doctor, physical therapist, or other healthcare expert’s approval and clearance.
Obtaining an accurate diagnosis for the exact cause of the sciatic pain
Is essential before considering any exercise program
Be gentle with your spine, don�t push too hard while doing exercises. This is to avoid exacerbating sciatic pain or creating a new injury.
If exercise increases pain or causes nerve-related symptoms like:
Weakness
Tingling sensation
Numbness
Stop and contact your doctor or chiropractor immediately!
El Paso, TX Best Sciatica Chiropractor Treatment
Sandra Rubio discusses Dr. Alex Jimenez and his team will help relieve your sciatica symptoms. Chiropractic care can improve pain and discomfort as well as reduce irritation and inflammation brought on by sciatica. Additionally, a chiropractor such as Dr. Jimenez can also offer nutritional and fitness tips for sciatic nerve pain. Other treatment procedures, such as deep-tissue massage, can help alleviate sciatica symptoms. Dr. Alex Jimenez is the homeopathic, noninvasive option for sciatic nerve disease and its related symptoms.
Sciatica is generally caused by the compression of lumbar or thoracic nerves or by compression of the sciatic nerve. When sciatica is caused by compression of a lower back nerve root, it’s called lumbar radiculopathy. This can happen due to a spinal disc bulge or spinal disk herniation (a herniated intervertebral disc), or by roughening, extending, or misalignment (spondylolisthesis) of the fascia, or as a result of degenerated discs that could reduce the diameter of the lateral foramen by which nerve roots exit the spine.
NCBI Resources
Sciatica is characterized by a shooting pain that originates in the lower back and travels down through the hip, buttock, and back of the leg. The pain can be so severe that it inhibits mobility and can prevent people from working, taking care of their home, or just enjoying their life. Doctors have treated the condition with medications and some invasive therapies, but chiropractic treatments have been found to be extremely effective in alleviating the pain and curing the condition.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine



 �
� �
�


 To figure this out, think of it like this: The bacteria in our large intestine releases polyphenols from the plants we eat in our diets. It is then transformed into a diet composition that alters the bacterial ecosystem (through the prebiotic effects and antimicrobial properties) to make our gut happy.
Here are some of the microbes that are in polyphenols:
To figure this out, think of it like this: The bacteria in our large intestine releases polyphenols from the plants we eat in our diets. It is then transformed into a diet composition that alters the bacterial ecosystem (through the prebiotic effects and antimicrobial properties) to make our gut happy.
Here are some of the microbes that are in polyphenols:
 When it comes to eating a healthy diet, variety does matter. The colors, the types of fibers each organic food has, and whether you are going to do it daily or weekly. When you are trying to be in a healthy lifestyle, it always starts with the food. When you are looking for fresh produce, try to emphasize fresh, organic, and minimally processed versions of polyphenol-rich foods. However, don�t boil produce. Instead, try steaming then, and it is the best, but roasting or light frying is not only better, but it tastes so good.
When it comes to eating a healthy diet, variety does matter. The colors, the types of fibers each organic food has, and whether you are going to do it daily or weekly. When you are trying to be in a healthy lifestyle, it always starts with the food. When you are looking for fresh produce, try to emphasize fresh, organic, and minimally processed versions of polyphenol-rich foods. However, don�t boil produce. Instead, try steaming then, and it is the best, but roasting or light frying is not only better, but it tastes so good.
 When it comes to our gut, here are some of the effects of Vitamin D on the gut microbiome. The higher the Vitamin D levels are, they will allow commensal bacteria to secrete more AMPs (antimicrobial peptides). When patients take a high dose of Vitamin D, over 5 weeks can lead to a significant reduction in Pseudomonas spp and Shigella/Escherichia spp in upper gut intestines.
Another thing that Vitamin D does is that it can increase T cell differentiation in the colon. A lack of T-regs increased the incidence of asthma, allergies, autoimmune, and autism. But T-regs can prevent the development of aberrant immune responses such as autoimmune and food sensitivities. We here at Injury Medical Clinic, talk about functional medicine to our patients and try to help them recover from their ailments.
Because Vitamin D exposure fluctuates seasonally for many individuals, it has been observed that lower Vitamin D levels in the winter tend to lead to changes in the intestinal microbial balance. This will make our bodies have a decreased level of Bacteroidetes and an increased level of Firmicutes. This is the reason for �winter weight gain� in many individuals as F: B ratio changes.
When it comes to our gut, here are some of the effects of Vitamin D on the gut microbiome. The higher the Vitamin D levels are, they will allow commensal bacteria to secrete more AMPs (antimicrobial peptides). When patients take a high dose of Vitamin D, over 5 weeks can lead to a significant reduction in Pseudomonas spp and Shigella/Escherichia spp in upper gut intestines.
Another thing that Vitamin D does is that it can increase T cell differentiation in the colon. A lack of T-regs increased the incidence of asthma, allergies, autoimmune, and autism. But T-regs can prevent the development of aberrant immune responses such as autoimmune and food sensitivities. We here at Injury Medical Clinic, talk about functional medicine to our patients and try to help them recover from their ailments.
Because Vitamin D exposure fluctuates seasonally for many individuals, it has been observed that lower Vitamin D levels in the winter tend to lead to changes in the intestinal microbial balance. This will make our bodies have a decreased level of Bacteroidetes and an increased level of Firmicutes. This is the reason for �winter weight gain� in many individuals as F: B ratio changes.
 This is a
This is a  We talked about Omega-3s in
We talked about Omega-3s in 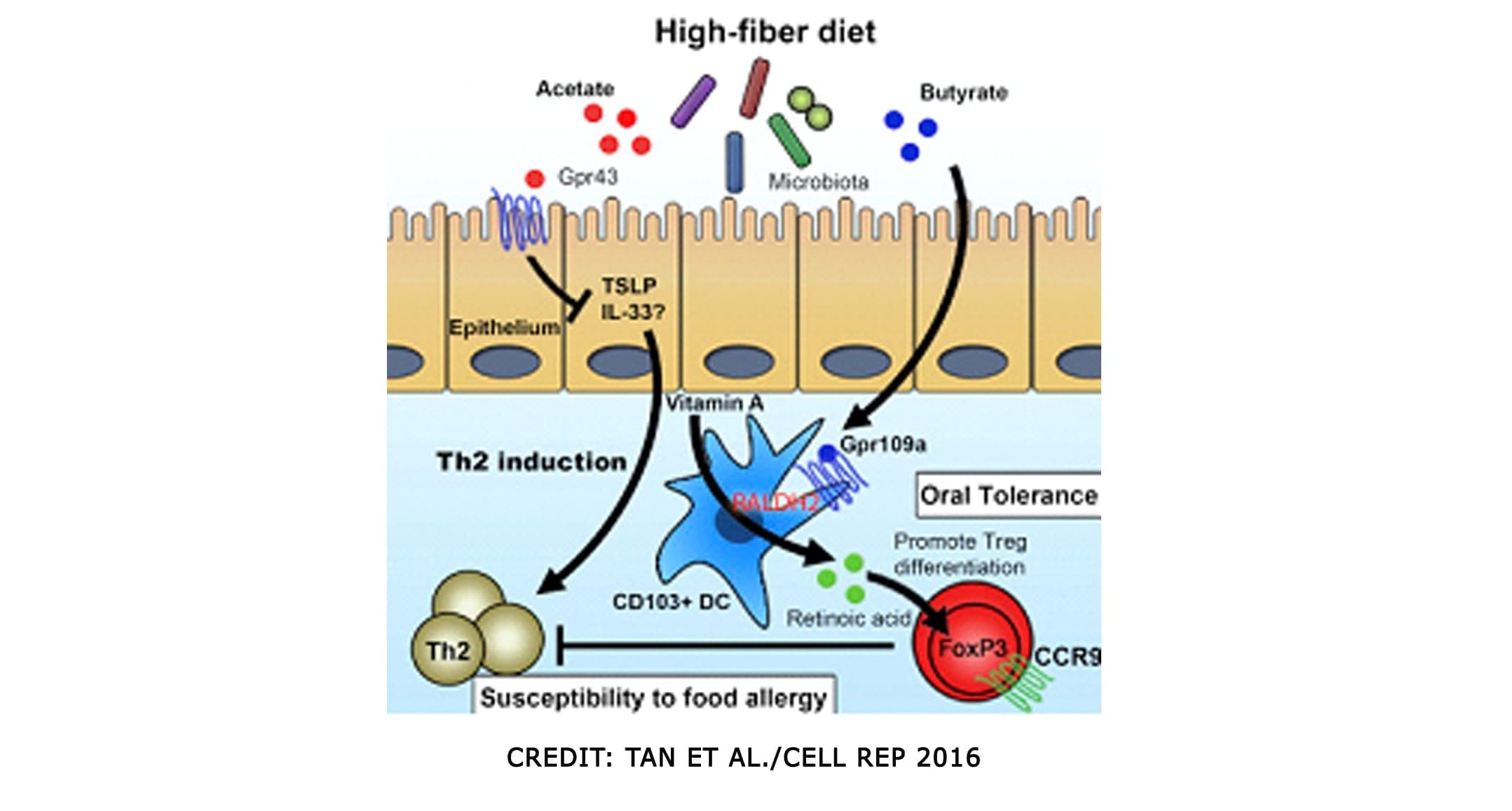
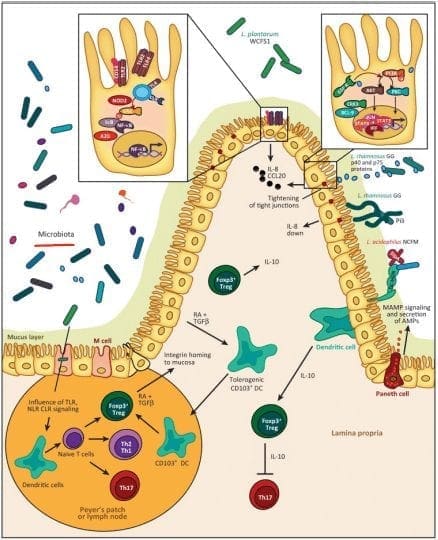 The
The 
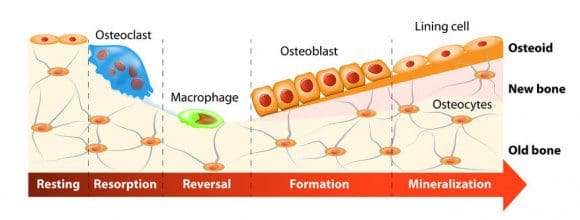

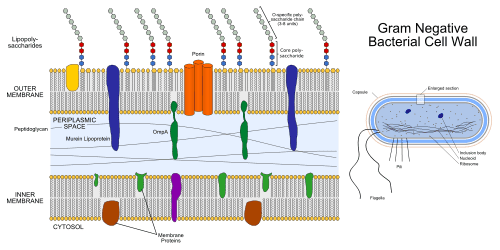






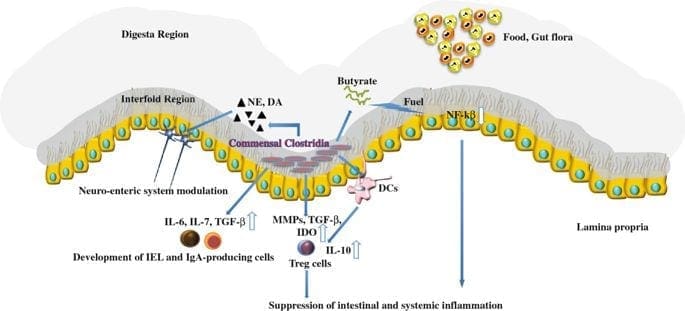


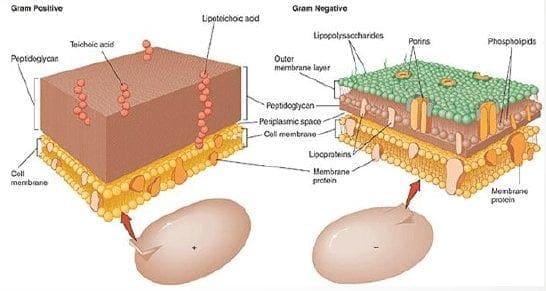
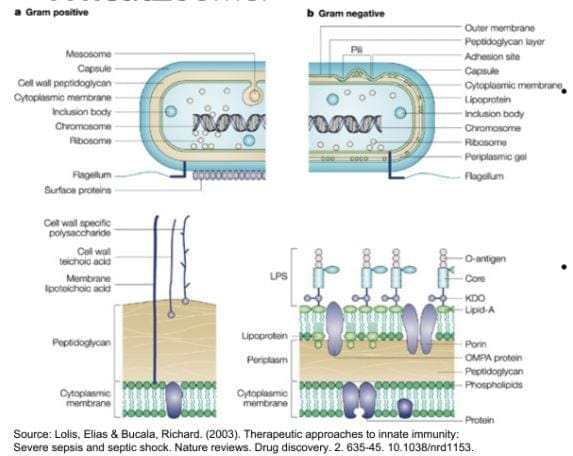


 �
�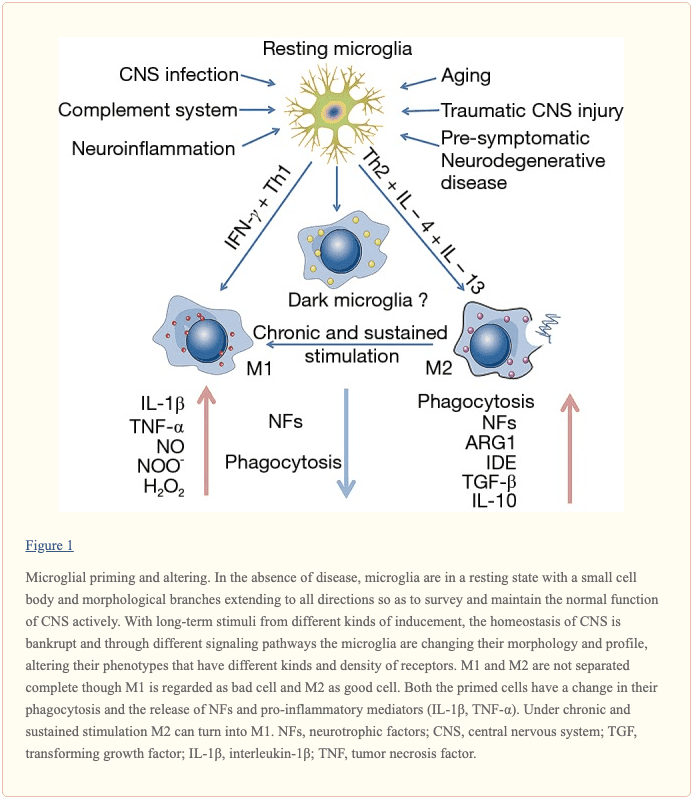 �
�

 Many studies show that soy may be a problem due to the saponin since it does have higher lectin count. Here at Injury Medical clinic, we suggest that running the Lectin Zoomer on our patients with intestinal permeability makes sense for them to heal correctly. But animal studies stated that soybean agglutinin has the effect of the increasing release of zonulin away from the TJ (tight junction). And a human study reported that if the soy saponin is poorly absorbed or utilized by the human intestinal epithelial cell will end up metabolizing the intestinal bacteria and cause more harm to human.
Many studies show that soy may be a problem due to the saponin since it does have higher lectin count. Here at Injury Medical clinic, we suggest that running the Lectin Zoomer on our patients with intestinal permeability makes sense for them to heal correctly. But animal studies stated that soybean agglutinin has the effect of the increasing release of zonulin away from the TJ (tight junction). And a human study reported that if the soy saponin is poorly absorbed or utilized by the human intestinal epithelial cell will end up metabolizing the intestinal bacteria and cause more harm to human.
 Known as sucrose monoester fatty acids is mostly used in cosmetics, food preservatives, food additives. Sucrose esters are used as a surface treatment on some fruits like peaches, pears, cherries, apples, and bananas. It keeps the moisture on the peel or rind controlled. Sucrose mono ester used in cosmetics as an emulsifier.
Known as sucrose monoester fatty acids is mostly used in cosmetics, food preservatives, food additives. Sucrose esters are used as a surface treatment on some fruits like peaches, pears, cherries, apples, and bananas. It keeps the moisture on the peel or rind controlled. Sucrose mono ester used in cosmetics as an emulsifier.
 Up to this date, there are minimal studies that have examined the role of bone broth or collagen that it repairs the intestinal barrier. It all depends on the animal and the bone it comes from and the contents that people have put in a bone broth soup.
Up to this date, there are minimal studies that have examined the role of bone broth or collagen that it repairs the intestinal barrier. It all depends on the animal and the bone it comes from and the contents that people have put in a bone broth soup.
 However, there is a small body of evidence for the use of collagen peptides seem to support the usage in their autoimmune disease treatment protocol. But the results cant be extrapolated whether bone broth would have similar effects. So more studying about bone broth is needed.
However, there is a small body of evidence for the use of collagen peptides seem to support the usage in their autoimmune disease treatment protocol. But the results cant be extrapolated whether bone broth would have similar effects. So more studying about bone broth is needed.
 When people say that they are going organic, it is beneficial for people that are willing to change to a healthy lifestyle. Granted that organically produces are locally grown, but still, organic produce or non-organic produce will not have less or safer pesticides. They are different, but all of the crops like fruits and vegetables are grown with pesticides.
Just like all fruits and vegetables, still, wash them thoroughly to reduce the number of pesticides and surfactants exposure and enjoy them to your heart’s content.
When people say that they are going organic, it is beneficial for people that are willing to change to a healthy lifestyle. Granted that organically produces are locally grown, but still, organic produce or non-organic produce will not have less or safer pesticides. They are different, but all of the crops like fruits and vegetables are grown with pesticides.
Just like all fruits and vegetables, still, wash them thoroughly to reduce the number of pesticides and surfactants exposure and enjoy them to your heart’s content.
 Resistant starch foods are a form of carbohydrates that can be converted to short fatty acids by SCFA-producing bacteria. With higher SCFA levels, these starches aid immune tolerance, T-cell differentiation, and intestinal barrier homeostasis. Other types of fibers are high value, and variety is essential. Like for example, cooked/cooled rice and potatoes are excellent resistance starch foods.
Resistant starch foods are a form of carbohydrates that can be converted to short fatty acids by SCFA-producing bacteria. With higher SCFA levels, these starches aid immune tolerance, T-cell differentiation, and intestinal barrier homeostasis. Other types of fibers are high value, and variety is essential. Like for example, cooked/cooled rice and potatoes are excellent resistance starch foods.

 Polyphenols, flavonoids and other phenolic compounds will aid to maintained TJ stability through inhibiting phosphorylation of TJ complexes.
Polyphenols, flavonoids and other phenolic compounds will aid to maintained TJ stability through inhibiting phosphorylation of TJ complexes.
 Fermented food or drinks that contain live probiotic cultures are excellent in promoting a healthy gut. However, it is challenging to study fermented food and beverages due to highly variable stains, composition, nutrient content. But studies found that participants who drink a fermented plant extract drink saw improvements in their body and increased total antioxidants and total phenolic in plasma as well as with reducing total C and LDL-C.
Beneficial bacteria like Bifido and Lactobacillus were increased while E Coli and C perfringens were decreased in the gut. So drinking or eating fermented food can help our gut and help our bile growth to be flushed out.
Granted, we all know that trying to be healthy is very hard. It is true that even though exercising is easy because we can do it over and over again until we are masters at it but, when we overdo the exercises it will cause harm to our bodies and hurting it in the process. �Eating healthy is hard as well because our bodies may have a food allergen or a food sensitivity that will make us disappointed that we can�t enjoy the foods we want to eat. Yes, eliminating diets are very hard and challenging to follow in the long term and have poor compliances when we don�t put in the work. So start by exploring other tests to tailor patients diets to meet their health needs and prolong their recovery period.
Fermented food or drinks that contain live probiotic cultures are excellent in promoting a healthy gut. However, it is challenging to study fermented food and beverages due to highly variable stains, composition, nutrient content. But studies found that participants who drink a fermented plant extract drink saw improvements in their body and increased total antioxidants and total phenolic in plasma as well as with reducing total C and LDL-C.
Beneficial bacteria like Bifido and Lactobacillus were increased while E Coli and C perfringens were decreased in the gut. So drinking or eating fermented food can help our gut and help our bile growth to be flushed out.
Granted, we all know that trying to be healthy is very hard. It is true that even though exercising is easy because we can do it over and over again until we are masters at it but, when we overdo the exercises it will cause harm to our bodies and hurting it in the process. �Eating healthy is hard as well because our bodies may have a food allergen or a food sensitivity that will make us disappointed that we can�t enjoy the foods we want to eat. Yes, eliminating diets are very hard and challenging to follow in the long term and have poor compliances when we don�t put in the work. So start by exploring other tests to tailor patients diets to meet their health needs and prolong their recovery period.
 Supplements are fantastic to aid the valuable nutrients and minerals our bodies can�t produce. Common supplements prescribed include:
Supplements are fantastic to aid the valuable nutrients and minerals our bodies can�t produce. Common supplements prescribed include:
 Granted that stress is part of our lives and we can manage small amounts of it, and it is beneficial to us, but some people have chronic stress and have to go to a doctor to get it treated. But there is hope as there are
Granted that stress is part of our lives and we can manage small amounts of it, and it is beneficial to us, but some people have chronic stress and have to go to a doctor to get it treated. But there is hope as there are