After a slip-and-fall accident,�Aracely Norte was limited�in her ability to work, that affected her quality of life. Due to chronic pain, Aracely had difficulty engaging in regular, everyday responsibilities. After hearing about El Paso, TX. Chiropractor, Dr. Alex Jimenez, from her lawyer, Aracely found relief from her chronic pain. Aracely describes how Dr. Jimenez cared for her injuries while he educated her about her health issues and the treatment he provided her with. Aracely highly recommends Dr. Jimenez as the non-surgical choice for chronic pain. Chronic pain is a common issue which can occur due to a variety of reasons, including injuries and underlying conditions, however, chiropractic care can help eliminate chronic pain symptoms.�
Chiropractic Rehab
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused on treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
We want you to live a life that is fulfilled with more energy, positive attitude, better sleep, less pain, proper body weight and educated on how to maintain this way of life. I have made a life of taking care of every one of my patients.
I assure you, I will only accept the best for you�
If you have enjoyed this video and we have helped you in any way, please feel free to subscribe and recommend�us.
Asthma is a chronic lung disease that is marked by narrowing and inflammation in the airways. The condition causes recurring periods of symptoms that include shortness of breath, wheezing, coughing, and tightness in the chest. It often starts in childhood, but it affects people of all ages and adults can suddenly experience an asthma attack. According to the American Academy of Allergy, Asthma, and Immunology (AAAI), approximately one in 12 people in the United States have asthma � and that number is growing each year.
Causes of Asthma
Doctors do not know why some people have asthma while others do not. Research suggests that genetics, environmental factors, or a combination of the two likely play some part in it.
Certain substances and irritants can trigger asthma attacks. These are often the same triggers for allergies since asthma and allergies often go hand in hand. Asthma triggers usually vary from person to person, but some of the more common ones include:
Cold air
Stress and strong emotions.
Airborne substances � Particles of cockroach waste, pollen, mold spores, dust mites, and pet dander.
Certain medications � Naproxen, beta-blockers, ibuprofen, and aspirin.
Physical activity � Exercise or physical labor.
Gastroesophageal reflux disease (GERD)
Respiratory infections � Allergies, cold, and bronchitis.
Air pollutants and irritants -Perfume, smoke, and air fresheners.
Additives in some foods � Preservatives, sulfites, additives added to processed potatoes, shrimp, beer, dried fruit, and wine.
Treatments for Asthma
Prevention of asthma attacks has proven to be the most effective method for managing asthma. It is essential for patients to learn to recognize their triggers so they can avoid them. If known to them they can take steps to minimize the attack. This involves tracking your breathing to ensure that your medication is adequately keeping symptoms at bay. However, most asthmatics carry a quick-relief inhaler for emergencies because sometimes prevention is not enough.
There are two types of asthma control medications: long-term and quick relief. The most common asthma medications for each type include:
Long-term
Combination inhalers
Inhaled corticosteroids
Long-acting beta agonists
Theophylline
Leukotriene modifiers
Quick-relief
Ipratropium
Short-acting beta agonists
Oral and intravenous corticosteroids
Allergy medications are an effective asthma treatment. Immunotherapy, or allergy shots, can lead to a decreased immune response to allergens. It can take a while for this to build up so the patient could be waiting for a long time. Omalizuman, or Xolair, is also an injection that is specifically for people with severe allergies or asthma
Chiropractic for Asthma
Regular chiropractic care can be very effective in treating asthma. Some studies have shown that it is effective in adult asthma as well as children with asthma.
One primary reason is that poor spinal health can contribute to an asthmatic condition. When the body is out of alignment, and it puts pressure on the sensitive nerves along the spinal column it can cause serious health problems throughout the body.
Chiropractic�s approach to whole body wellness, coupled with good spinal health and you have an asthma treatment that works.
The chiropractor may also make recommendations to the patient regarding certain lifestyle changes like advising them to stop smoking. He or she may also recommend certain foods that lower the amount of inflammation in the body and to reduce their contact with things in their environment that may be asthma triggers.
They will work with the patient to create a plan that will strengthen the immune system, minimize allergic responses, and decrease the instances of asthma attacks so that the patient can live a full, quality life.
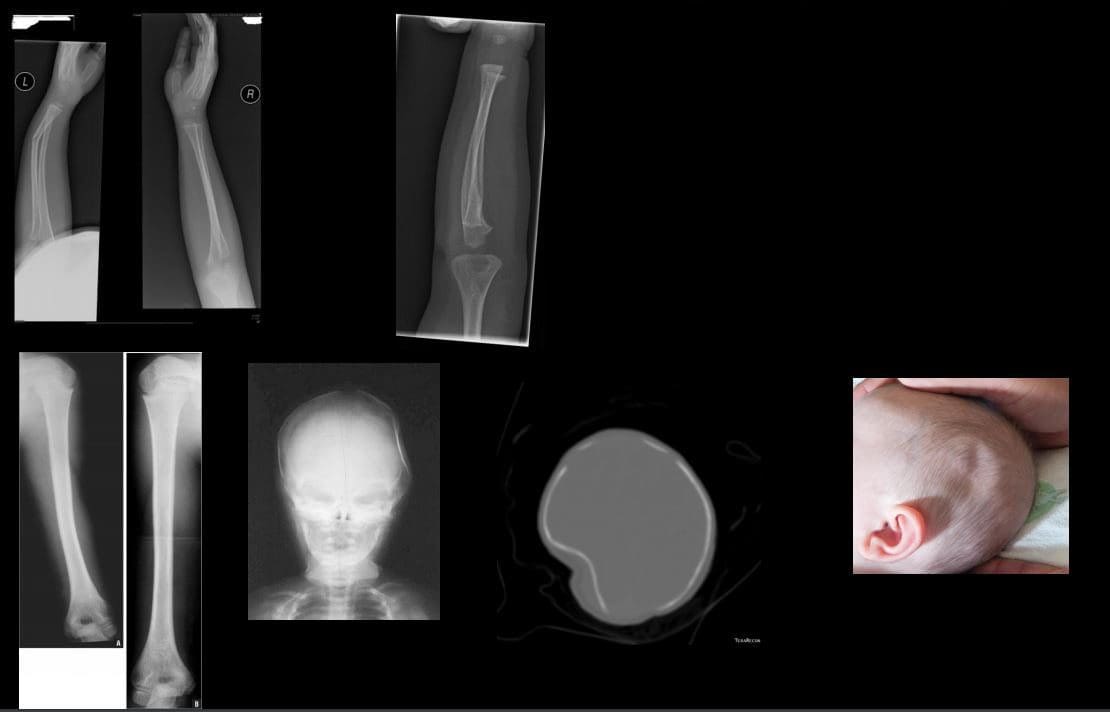
Gartland classification grades minimally displaced subtle injuries treated with simple immobilization vs. posterior elbow dislocation treated operatively
A potential risk of ischemic compromise if care is delayed (Volkmann contracture)
The Radiological exam is crucial: sail sign & posterior fat pad sign with anterior humeral line failed to intersect mid/2/3 of Capitellum.
Incomplete pediatric Fx:
Most in <10 y.o. Greenstick, Torus, Plastic aka Bowing deformity
Typically heal well, treated conservatively with immobilization
Plastic deformity if >20-degrees requires closed reduction
Ping pong skull fracture may develop following trauma, forceps delivery and complications of birth trauma. May need to be assessed by the pediatric neurosurgeo.n
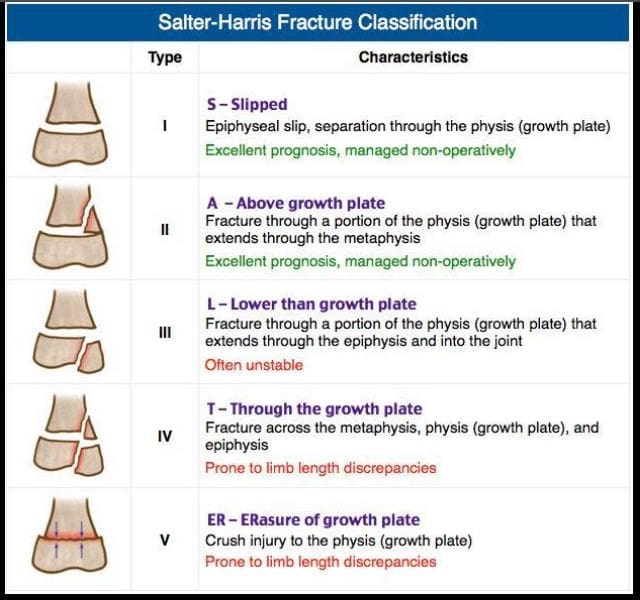
Salter-Harris types of physeal growth plate injuries
Type 1-slip. e.g., Slipped Capital Femoral Epiphysis. Typically no bone fracture noted
Type 2-M/C with good prognosis
Type 3- intra-articular, thus carries the risk of premature osteoarthritis and may require operative care d/t being unstable
Type 4- Fx through all regions about the physis. Unfavorable prognosis and limb shortening
Type 5- often no evidence of actual bone fracture. Poor prognosis d/t crush injury and vascular damage with limb shortening
Imaging evaluation is crucial
Non-Accidental Injury (NAI)in Children
There different forms of child abuse. Physical abuse may range from skin injuries to different MSK/systemic injuries affecting bones and soft tissues. Imaging is crucial and may identify definite signs alerting medical providers and informing child protection services and law enforcement agencies about physical abuse.
In an infant: �shaken baby syndrome� may present with CNS signs d/t tearing of immature bridging vein and subdural hematoma which can be fatal. Retinal hemorrhaging often a clue. Head CT is crucial.
MSK Radiological Red Flags:
1) major bone Fx in an un-ambulatory very young child (0-12 m.o.)
2) Posterior ribs Fx: naturally never occur d/t accidents. Most likely mechanisms: grabbing and squeezing a child or direct hit.
3) Multiple Fractures with different chronological healing rates, i.e., bone calluses indicating repeated physical trauma
4) Metaphyseal corner Fx aka Bucket handle Fx, often pathognomonic for NAI in children. Occurs when the affected extremity is held and violently twisted.
5) Spiral fracture of long bones in a young child is another example of NAI.
Other important clues of NAI. Inconsistent history provided by guardians/caregivers. No evidence of congenital/metabolic bone abnormalities like Osteogenesis Imperfecta or Rickets/osteomalacia etc.
N.B. When child�s guardians state a history that reports fall and accidents in the house, It is important to know that apparently most accidents/falls in the house are very rarely or unlikely result in major bone fractures.
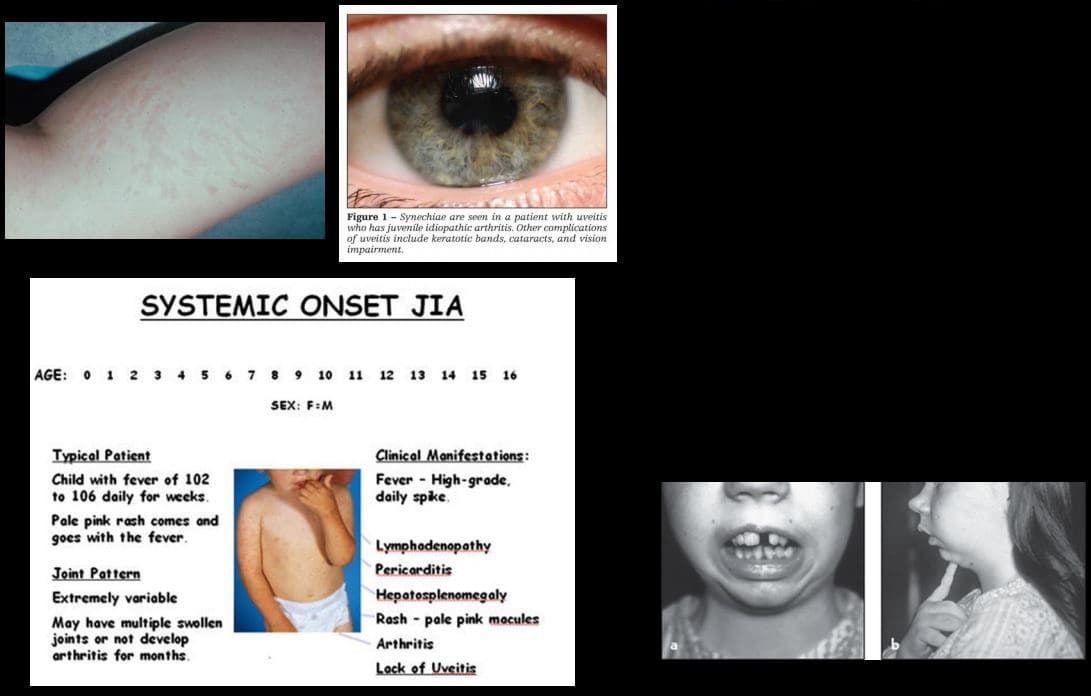
Juvenile Idiopathic Arthritis (JIA)-considered M/C chronic disease of childhood. Clinical Dx: joint pain/swelling for 6-weeks or longer in a child <16-y.o. Different forms exist: Early Dx is crucial to prevent delayed complications
Most familiar forms of JIA:
1) Pauciarticular disease (40%)- m/c form of JIA. Girls are at greater risk. Presents as arthritis in <4 joints: knees, ankles, wrist. Elbow. This type shows high association with ocular involvement as iridocyclitis (25%) that may potentially lead to blindness. Labs: RF-ve, ANA positive.
2) Polyarticular disease (25%): RF-ve. Girls are at greater risk. Affects small and large joints often affect Cervical spine
3) Systemic form of JIA (20%): often presents with acute systemic manifestation as spiking fevers, arthralgias, myalgias, lymphadeno[pathy, hepatosplenomegaly, polyserositis (pericardial/pleural effusion). Important Dx features characteristic evanescent salmon pink rash on the extremities and trunk. The Systemic form has a distinct lack of ocular involvement. Joints typically shoe no erosions compared to other types. Thus joint destruction is not typically seen
Imaging in JIA
Joint effusion bone overgrowth squaring of patella cartilage/bone erosion superimposed DJD
Fingers and long bones early physeal closure/limb shortening
Rad DDx knee/ankle: Hemophilic arthropathy Rx: DMARD.
Osteosarcoma (OSA) & Ewing�s sarcoma (ES) are 1 st and 2nd M/C primary malignant bone neoplasms of childhood (peak at 10-20 y.o.) Clinically: bone pain, change in activity, early metastasis especially pulmonary mets may occur. Poor prognosis
Ewing�s may present with bone pain, fever and elevated ESR/CRP mimicking infection. Early Dx with imaging and staging are crucial.
Imaging of OSA & ES: x-ray, followed by MRI, chest CT, PET/CT. On x-rays: OSA may affect any bone but most present as aggressive bone forming neoplasms about the knee (50% cases) especially as osteoid forming an aggressive lesion in the metaphysis with speculated/sunburst periostitis & Codman triangle. Marked soft tissue invasion.
ES may present in the shaft and show very early soft tissue spread. MRI is crucial to reveal the extent of bone and ST invasion, MRI required for surgical planning
OSA & ES Rx: A combination of surgery, radiation, chemo. Limb salvage techniques are performed in some cases. Poor prognosis if detected late.
Imaging of Ewing�s sarcoma
Permeating bone distraction
Early and extensive soft tissue invasion
Aggressive periosteal reaction with laminated (onion skin) response
Saucerisation of cortical bone (orange arrow)
A Lesion is typically diaphyseal with some metaphyseal extension
Known as Round cell tumor along with Multiple Myeloma and Lymphoma
Common Childhood Malignancies
Neuroblastoma (NBL) M/C malignancy of infancy. Derives from neural crest cells aka PNET tumors (e.g., sympathetic ganglia). Most occur in children <24-months. Some show good prognosis but >50% cases present with advanced disease. 70-80% at age 18-months or older present with advanced metastasis. NBL may develop in the adrenal medulla, sympathetic ganglia and other location. Presents as an abdominal mass, vomiting. >50% presents with bone pain d/t metastasis. Clinically: physical exam, labs, imaging: chest and abd x-rays, CT abdomen and chest is crucial to Dx. MRI may help. NBL may metastasize to the skull and infiltrate sutures with a characteristic presentation as pathological sutural diastasis.
Acute Lymphoblastic Leukemia is the m/c malignancy of childhood. Pathology: leukemic cell infiltration of bone marrow leading to bone pain and replacement of other normal marrow cells with anemia, thrombocytopenia, neutropenia and associated complications. Leukemic cells may infiltrate other sites including CNS, spleen, bone and other regions. Dx: CBC, serum lactate dehydrogenase levels, Bone marrow aspiration biopsy is the key. Imaging may help but not essential to diagnosis. On radiography, leukemic infiltration of the bone may typically appear as radiolucent bands along the physeal growth plate. Rx: chemotherapy and treating complications
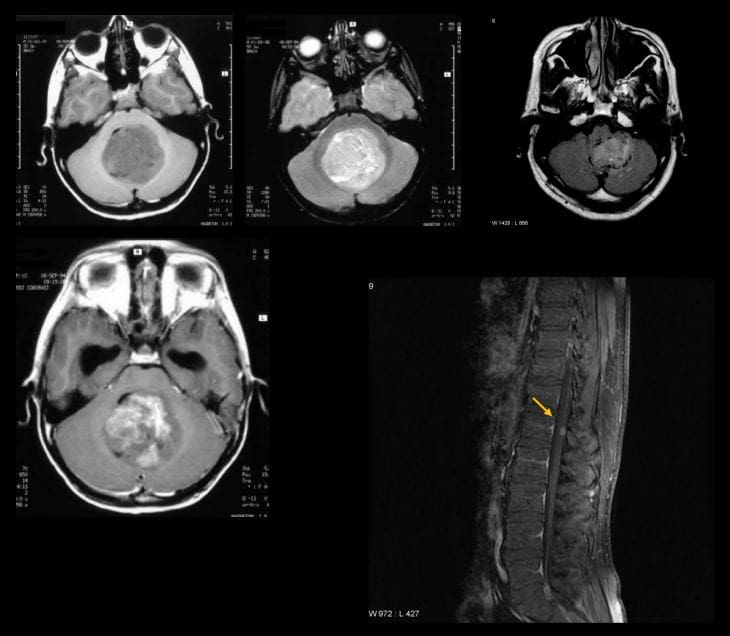
Medulloblastoma: M/C malignant CNS neoplasm in children
Majority develop before 10-y.o.
M/C location: cerebellum and posterior fossa
Histologically represents a PNET type tumor not a glioma as was originally thought
MBL, as well as Ependymoma and CNS lymphoma, may lead to drop metastasis via CSF and additionally represent a unique that unlike other CNS tumors demonstrate metastatic spread outside CNS, m/c to the bone
50% of MBL may be fully resectable
If Dx and treatment begin before metastasis, 5- year survival is 80%
Imaging is crucial: CT scanning may be used but the imaging modality of choice is MRI that will additionally provide a more superior evaluation of the entire neuraxis for metastasis.
MBL typically appears as heterogenous hypo, iso and hyperintense lesion on T1, T2 and FLAIR scans (top images) if compare to surrounding brain tissue. Often compressing 4th ventricle with obstructive hydrocephalus. The tumor typically shows contrast enhancement on T1+C gad (bottom left image). Drop metastasis from MBL with T1+C enhancing lesion in the cord
Important Pediatric Infections
In the neonate/infant <1month: fever >100.4 (38C) may indicate bacterial and some viral infection. Strep B, Listeria, E. Coli may lead to sepsis, meningitis. Approach: chest x-ray, lumbar puncture with culture, blood culture, CBC, urinalysis.
In young children, Hemophilus influenza type B (HIB) may lead to Epiglottitis a rare but serious complication. The current vaccine helps to reduce the number of cases of Epiglottitis and other HIB related illnesses.
Parainfluenza or RSV virus may lead to Croup or acute Laryngotracheobronchitis.
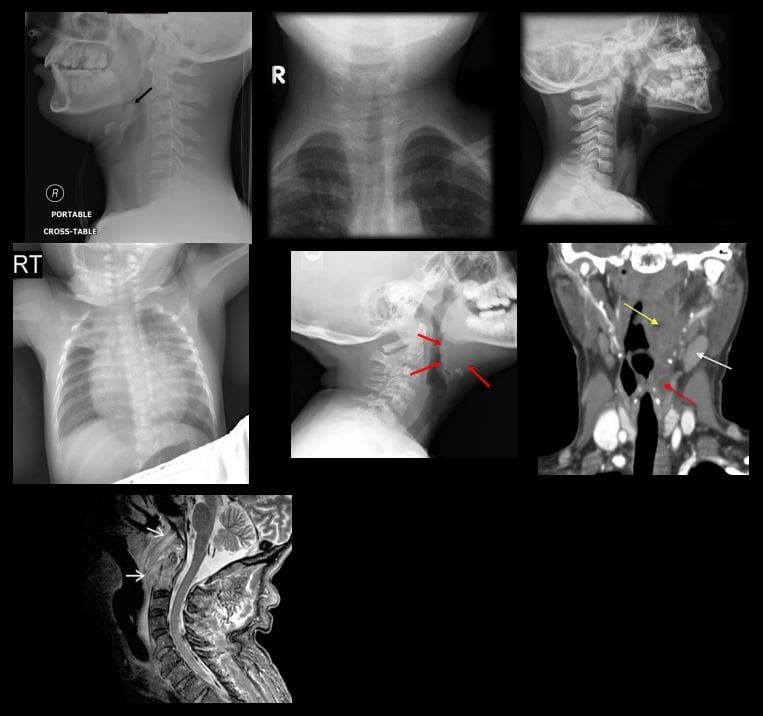
Epiglottitis and Croup are Dx clinically but AP and lateral soft tissue neck x-rays are very helpful
Epiglottitis presents with a characteristic �thumb sign� that is consistent with thickened epiglottis d/t epiglottic edema. This can be a life-threatening emergency compromising airways (top left)
Croup may show a �steeple sign� or �wine bottle sign� with distended hypopharynx as acute narrowing of subglottic airway on AP and lateral neck soft tissue x-ray (top right)
Respiratory Syncytia Virus (RSV) and influenza may lead to viral pneumonia potentially with life-threatening complications in the immunocompromised, very young and children with comorbidities. CXR is crucial (middle left)
Streptococcal pharyngitis with GABHS infection may lead to some acute or delayed complications (e.g., Rheumatic fever)
Peritonsillar abscess (above middle right) may develop in some cases and be complicated by spreading along soft tissue planes in the neck potentially leading to spread into sublingual/submandibular spaces (Ludwig Angina) when airways need to be controlled d/t base of tongue edema
Development of a retropharyngeal abscess may potentially lead to spread of the infection through freely communicating neck fascia resulting in necrotizing mediastinitis, Lemmier syndrome and invasion of carotid spaces (all are potentially life-threatening complications)
Griesel syndrome- (above bottom left) rare complication of regional tonsillar/pharyngeal oral infections that can spread to prevertebral space leading to C1-2 ligaments laxity and instability
Other important infections in children are typical bacterial (Pneumococcal) pneumonia, Urinary tract infection and Acute Pyelonephritis (especially in girls) and Meningococcal Meningitis
Pediatric Metabolic Disease
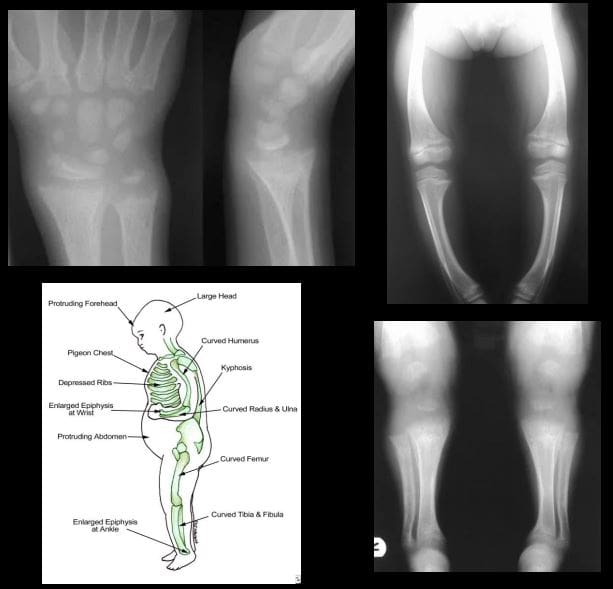
Rickets: considered osteomalacia in skeletally immature. Zone of provisional calcification of the epiphyseal growth plate is particularly affected
Clinically presents with growth retardation, extremity bowing, rachitic rosary, pigeon chest, depressed ribs, enlarged and swollen wrists, and ankles, skull deformity
Pathology: Vit D and calcium abnormality is the m/c cause. Lack of sun exposure esp. dark-skinned individual, restrictive clothing to light exposure, prolonged exclusive breastfeeding, veganism, malabsorption syndromes of the gut, renal damage and others
Imaging: frayed metaphysis aka paint brush metaphysis with flaring, widening of the growth plate, bulbous costochondral junction as a rachitic rosary, extremity bowing
Rx: treat underlying causes, correct nutritional deficit, etc.
Chronic pain is one of the most prevalent conditions in the United States, affecting an estimated 100 million Americans each year. To put that into perspective, that�s more than the number of people suffering from cancer, heart disease, and diabetes, combined.
Many of these chronic pain sufferers are looking for relief beyond pharmaceuticals which can have unpleasant and even harmful side effects. This has brought them to natural pain management methods like chiropractic care as well as natural substances like curcumin. For many people, these treatment options have brought them relief from the pain and help them return to a more normal lifestyle.
How does it work though? And, more importantly, can it work for you?
What is Curcumin?
Natural herbal turmeric capsules with fresh herb leaves and dry curcumin in paper
Curcumin is a spice that is a relative of ginger and is a component of turmeric. Often in the U.S., the terms curcumin and turmeric are used interchangeably. However, curcumin is what gives turmeric its bright yellow color.
While it is often found in curries and other traditional Indian food, it has also long been used to treat a variety of health issues including inflammation that causes pain in the body. These claims have been backed up by several studies that show the tasty spice has tremendous health benefits to offer.
These studies have shown that curcumin has strong anti-inflammatory properties although why it works is not yet completely understood. This information has prompted further studies to determine the efficacy of curcumin in treating a wide range of conditions including chronic pain.
One study examined the spice�s effects on people suffering from arthritis or joint pain. The results determined that turmeric extract (curcumin) supplements were just as effective as ibuprofen in relieving the pain in patients with knee osteoarthritis. It helped to reduce the inflammation that was causing the pain, bringing the patients much-needed relief.
Taking Curcumin for Better Health
You can get curcumin or turmeric supplements, but there is no standard dosage information available. Your chiropractor can advise you on how much to take and which supplement brands are the best.
You can also use the spice in the foods you eat and gain a good bit of the health properties that way. However, it may be more efficient and more comfortable to take curcumin or turmeric supplements, especially when you are treating inflammation and pain.
Curcumin is generally safe with very few side effects. As with any medication or supplement, some people are sensitive to the spice and may experience diarrhea and nausea.
However, that usually occurs at higher doses or after the patient has been using it for a long time. High doses could also pose a risk if the person has ulcers. It can also irritate the skin is applied topically.
If you are considering incorporating curcumin into your daily diet as a health supplement, you should first talk to your doctor or chiropractor to make sure it is safe for you. Women who are pregnant or nursing should not take the supplements.
People with conditions like diabetes, gallbladder issues, bleeding disorders, kidney disease, or immunity problems should take special care when using the supplement. Also, it can interact with medications like NSAIDs, aspirin, diabetes drugs, statins, blood thinners, and blood pressure medications so talk to your health professional, such as your chiropractor, before taking. They may adjust your dosage or recommend certain nutritional therapies to better support the supplement.
Your chiropractor can help you live a more natural, pain-free life and supplements like curcumin may be a part of that plan. They can help put you on the path to a life well lived.
Why is it that the ketogenic diet and intermittent fasting always seem to fall within the same topic of conversation? This is simply because intermittent fasting may be utilized as an instrument to achieve ketosis, the metabolic state associated with the keto diet. During intermittent fasting, the human body is depleted of glycogen stores. Once these glycogen stores are eliminated, fat stores are then released into the bloodstream in order to be converted into energy molecules, known as ketones, from the liver.
What is Ketosis?
Ketosis is a metabolic state which uses ketone bodies, or ketones, as fuel for energy. On a normal carbohydrate-based diet, the human body burns glucose as its main fuel source, where excess glucose is subsequently stored as glycogen. If the human body cannot utilize sugar as fuel for energy, it will utilize glycogen as fuel for energy. Once glycogen is depleted, you begin to burn fat. The ketogenic diet generates a metabolic state which enables you to break down fat into ketones, or ketone bodies, in the liver for energy.
There are 3 major types ketone bodies found in the blood, urine, and breath, including:
Acetoacetate: The type of ketone which is created first. It may be converted to beta-hydroxybutyrate or flipped into acetone.
Acetone: Made spontaneously in the breakdown of acetoacetate. It is a very volatile ketone and it is frequently detectable on the breath once an individual first enters ketosis.
Beta-hydroxybutyrate (BHB): The type of ketone which is utilized for energy and is most abundant on the bloodstream as soon as you’re completely into ketosis. It is the kind that is located in exogenous ketones and what blood tests quantify.
Intermittent Fasting in the Keto Diet
Intermittent fasting is composed of eating within a specific feeding window rather than eating throughout the day. Each individual, whether they are conscious of it or not, fasts intermittently from dinner to breakfast. There are lots of methods to intermittent fasting. A few individuals fast for 16-20 hours intervals on alternate days while others follow a 24-hour day fast. The most common intermittent fasting variety is the 16/8 method, in which you eat in an 8-hour window followed by a 16-hour fasting window.
Other fasting programs incorporate the 20/4 or even 14/10 methods. Other people follow 24-hour fasts one or two times each week. Intermittent fasting can get you in ketosis quicker because your cells will immediately absorb your glycogen stores and begin burning fat. However, what about once you get into ketosis? Is intermittent fasting worth following consistently? Following the ketogenic diet and intermittent fasting can be a great addition towards an individual’s overall health and wellness, providing various health benefits.
The keto diet and intermittent fasting can provide the following health benefits, including:
Healthy weight-loss
Fat reduction, not muscle reduction
Balancing cholesterol levels
Enhancing insulin sensitivity
Maintaining blood glucose levels steady
Health Benefits of the Ketogenic Diet
The ketogenic diet dramatically reduces your caloric intake, forcing your body to burn fat instead of sugar, which makes it a powerful tool for weight reduction. While individual results vary, the keto diet has always resulted in a decrease in body fat in a selection of situations. Within a 2017 study, subjects who followed a very low carbohydrate keto meal program significantly decreased body fat percentage and body fat mass, losing an average of 7.6 lbs and 2.6 percent body fat while preserving lean muscle mass.
Likewise, a 2004 research detecting the long-term consequences of a ketogenic diet in overweight patients discovered that the weight and body mass of those patients diminished dramatically over the span of two decades. Individuals who radically reduced their carb intake saw a substantial decline in LDL (bad) cholesterol, triglycerides, and enhanced insulin sensitivity. In 2012, researchers compared a ketogenic diet to eating fewer calories for overweight kids and adults. The results showed kids after the keto diet lost significantly more body fat. They also revealed a dramatic decline in insulin levels, a biomarker of Type 2 diabetes.
Health Benefits of Intermittent Fasting
Studies have shown that intermittent fasting may be an effective weight loss tool, more powerful than just cutting calories. In one analysis, intermittent fasting has been proven to be as successful as constant calorie restriction in combating obesity. In studies done by the NIH, there was reported weight reduction with over 84 percent of participants, regardless of which fasting program they picked.
Much like ketosis, intermittent fasting increases fat loss while preserving lean muscle mass. In one study, researchers reasoned that fasting led to greater weight loss compared to a low-carb diet, though the overall caloric consumption was exactly the same. If you are attempting to lose weight, then a keto diet or intermittent fasting can be a massive help. But that is not where the rewards stop.
Intermittent Fasting and the Keto Diet for Mental Health
Both intermittent fasting and the ketogenic diet can provide various mental health advantages. Both have been clinically shown to boost memory, improve mental clarity and focus, as well as prevent the development of neurological disorders like Alzheimer’s and epilepsy. On a carb-based diet, changes in glucose can cause changes in energy levels. During ketosis, your brain employs a more consistent supply of fuel: ketones from the fat stores, leading to better productivity and psychological performance.
Whenever you’ve got a consistent and clean energy source from ketones, the brain works better. In addition to this, ketones are better at protecting your brain. Studies reveal that ketone bodies might have antioxidant properties which protect your brain cells from free radicals and oxidative stress. In one study conducted on adults with diminished memory, the growth of BHB ketones in their own blood helped enhance cognition. Also, when you’ve got difficulty staying focused, your hormones can be to blame.
Your brain has two chief neurotransmitters: glutamate and GABA. Glutamate will help you form new memories, and get your brain cells to communicate with one another. GABA is what helps restrain glutamate. If there is too much glutamate, it can cause brain cells to quit working and finally perish. GABA is there to control and slow down glutamate. If GABA levels are reduced, glutamate reigns free and you experience mental fog. Ketones stop damage to cells by processing surplus glutamate into GABA. Considering that ketones raise GABA and lessen glutamate, they assist in preventing cell damage, preventing cell death and enhancing mental focus.
Researchers believe that intermittent fasting enhances memory, decreases oxidative stress, and conserves learning abilities. Since your cells are under moderate strain whilst fasting, the top cells adapt to the stress by improving their particular ability to deal with these circumstances while the weakest tissues die. This is much like the strain that your body gets when you reach the gym.
Exercise is a kind of stress that your body adjusts to improve and get more powerful. This also applies for intermittent fasting: so long as you are still alternate between routine eating habits and fasting, it is going to continue to benefit you. Implying equally that ketosis and intermittent fasting will help improve your cognitive functioning because of the synergistic and protective effects of ketones.
The ketogenic diet and intermittent fasting are two different nutritional strategies which provide many common health benefits. According to various research studies, both the keto diet and intermittent fasting can help boost ketones, helping the body burn fat more efficiently than any other nutritional strategy. And when these are utilized together, they definitely form a powerful dietary program. The article above discusses the differences between the ketogenic diet and intermittent fasting as well as demonstrates the health benefits of both of these dietary programs and how they can help improve overall health and wellness. Dr. Alex Jimenez D.C., C.C.S.T. Insight
The Perks of Intermittent Fasting and the Keto Diet
The ketogenic diet and intermittent fasting possess similar health benefits because both approaches involve ketosis. Ketosis has lots of physical and mental advantages, from weight loss to enhanced brain function. People following a ketogenic diet may use intermittent fasting as a tool to achieve ketosis and enhance their general well-being. The scope of our information is limited to chiropractic and spinal health issues. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topic Discussion:�Acute Back Pain
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief. �
Say you have neck or back pain. How will you treat it? Many people will go to a medical doctor who will look at the symptoms, such as pain, and treat it with prescription or over the counter medications. In some cases, they may recommend surgery to manage the pain or correct the problem. But there is a safe and less expensive alternative. Chiropractic is the better choice over drugs and surgery!
An increasing number of people are foregoing the medical doctor and opting for chiropractic care for pain management � and often with excellent results. So, what is it about chiropractic that people feel makes it a better choice than drugs or surgery for their pain or mobility issues? There is more to the answer than you may realize.
Drug Therapy
When it comes to certain types of pain, particularly neck pain, medication is not the best way to manage it. Studies show that patients who opted to undergo chiropractic treatments and exercise regularly were more than twice as likely to significantly reduce their pain or even eliminate it entirely, compared to those who choose to take medication.
Aside from efficacy though, many medications have unpleasant and even dangerous side effects. Even over the counter medications can cause problems.
For instance, acetaminophen has been linked to serious health issues like pancreatitis and impaired liver function. NSAIDs like ibuprofen can upset the stomach and can cause rebound headaches in migraine patients (studies show that chiropractic is extremely effective in preventing migraines).
Prescription drugs can be highly addictive and lead to overdose. The Centers for Disease Control (CDC) has declared opioid addiction and overdose in the United States to be an epidemic. They have set forth guidelines for doctors who prescribe opioids for chronic pain, but the epidemic continues.
Surgery
Any treatment that can help a patient avoid invasive surgery is an optimal alternative, and chiropractic care provides that. One study shows that patients who saw a medical doctor as their first treatment option when dealing with back pain were more likely to have surgery than patients who say a chiropractor first.
Almost 43% of the medical patients eventually underwent surgery while only 1.5% of chiropractic patients had surgery. This means that if you are a medical patient trying to resolve your back pain you are 28 times more likely to eventually have surgery for it than you would if you went to a chiropractor.
Aside from the obvious invasiveness of the procedure as well as recovery time and probable physical therapy that would be required as part of your aftercare, there are many other downsides. The time and money necessary for the surgery, pre-surgery appointments, post-surgery appoints, recovery, and therapy can be significant.
However, a significant concern in hospital settings is the risk of C-diff (Clostridium difficile). C-diff is bacteria that can cause C. diff colitis, an inflammation of the colon or large intestine that can make you very sick. It can be passed from person to person but can also occur in people who take antibiotics � which are often given when a person undergoes surgery.
Chiropractic Care
Chiropractic care gets to the cause of the problem instead of treating the symptoms like most medical doctors. The whole-body approach also empowers patients to make lifestyle adjustments that aid in their care and healing. It allows them to take ownership of their health and pain management so that they feel more in control.
Chiropractors take a natural, holistic approach to pain management by bringing the body back into alignment if necessary and recommending exercises and other activities to help patients regain their normal range of motion and flexibility while relieving not only the pain symptoms but often correcting the problem that is causing the pain.
Diagnosis of the diseases of the abdomen can be classified into:
Abnormalities of the gastrointestinal tract (esophagus, stomach, small & large bowel, and the appendix)
Abnormalities of the accessory digestive organs (Hepatobiliary & pancreatic disorders)
Abnormalities of the genitourinary & reproductive organs
Abnormalities of the abdominal wall and major vessels
This presentation aims to provide the most basic understanding of general diagnostic imaging approach and appropriate clinical management of patients with the most common diseases of the abdomen
Imaging modalities used during an investigation of the abdominal complaints:
AP abdomen (KUB) and upright CXR
Abdominal CT scanning (with oral and I.V. contrast and w/o contrast)
Upper and Lower GI Barium studies
Ultrasonography
MRI (most used as Liver MRI)
MRI enterography & enteroclysis
MRI rectum
Endoscopic Retrograde Cholangiopancreatography (ERCP)- mostly hepatobiliary and pancreatic ductal pathology
Nuclear imaging
Why Order An Abdominal X-ray?
Include a preliminary evaluation of bowel gas in an emergent setting. For example, a negative study in a low probability patient may obviate the need for a CT or other invasive procedures
Evaluation of radiopaque tubes, lines, and radiopaque foreign bodies
Post-procedural evaluation intraperitoneal/retroperitoneal free gas
Monitoring the amount of bowel gas and resolution of postoperative (adynamic) ileus
Monitoring the passage of contrast through the bowel
Colonic transit studies
Monitoring renal calculi
What to Note on AP Abdomen: Supine vs. Upright vs. Decubitus
Free Air (pneumoperitoneum)
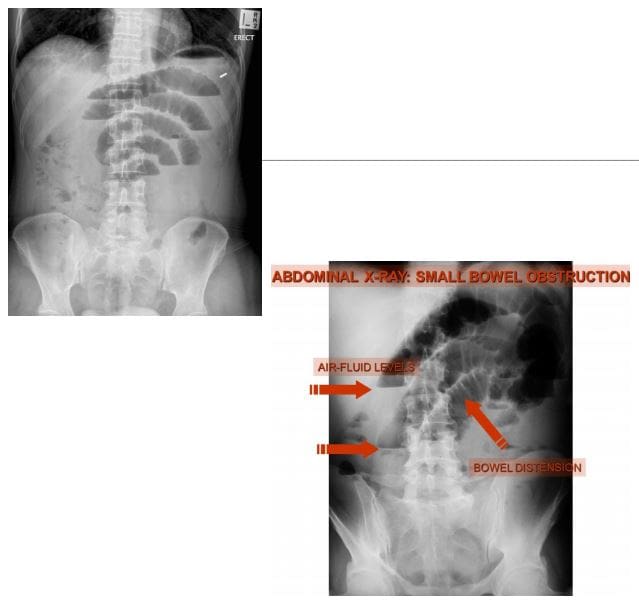
Bowel obstruction: Dilated loops: SBO vs LBO (3-6-9 rule) SB-upper limit-3-cm, LB-upper limit-6-cm, Caecum-upper limit-9-cm. Note loss of haustra, note dilation (presence) of valvule conivente (plica semilunaris) in SBO
SBO: note different heights air-fluid levels on upright film step ladder� appearance, typical of SBO
Note paucity of rectal/colonic gas (evacuated) in SBO
Abdominal CT scanning -modality of choice during the investigation of acute and chronic abdominal complaints especially in adults. For example, abdominal malignancy can be successfully diagnosed and staged providing clinical information for care planning
Abdominal, renal and pelvic ultrasound can be performed to help the diagnosis of appendicitis (esp. in children), acute & chronic vascular pathology, hepatobiliary abnormalities, obstetric and gynecological pathology
Use of ionizing radiation (x-rays & CT) should be minimized in children and other vulnerable groups.
Diagnostic Imaging of Major Diseases of the Gastrointestinal System
1) Esophageal disorders
2) Gastric carcinoma
3) Gluten Sensitive Enteropathy
4) Inflammatory Bowel Disease
5) Pancreatic ductal adenocarcinoma
6) Colorectal carcinoma
7) Acute Appendicitis
8) Small bowel obstruction
9) Volvulus
Esophageal disorders
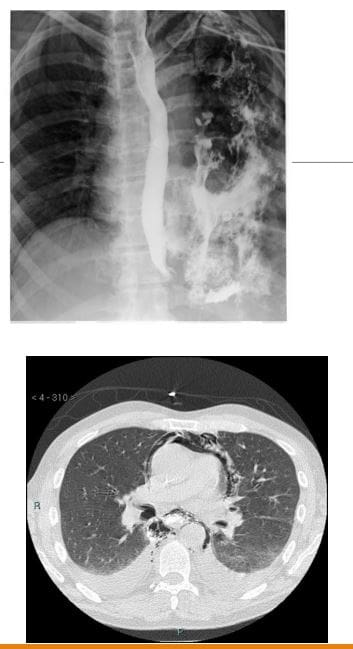
Achalasia (primary achalasia): failure of organized esophageal peristalsis d/t impaired relaxation of the lower esophageal sphincter (LOS) with marked dilatation of the esophagus and food stasis. Obstruction of the distal esophagus (often due to tumor) has been termed “secondary achalasia” or “pseudoachalasia.� Peristalsis in the distal smooth muscle segment of the esophagus may be lost due to an abnormality of Auerbach plexus (responsible for smooth muscle relaxation). Vagus neurons can also be affected
Primary: 30 -70s, M: F equal
Chagas disease (Trypanosoma Cruzi infection) with the destruction of the Myenteric plexus neurons of the GI system (megacolon & esophagus)
However, the heart is the M/C affected organ
Clinically: Dysphagia for both solids and liquids, in comparison to dysphagia for solids only in cases of esophageal carcinoma. Chest pain and regurgitation. M/C mid esophageal squamous cell carcinoma in approximately 5% due to chronic irritation of the mucosa by stasis of food and secretions. Aspiration pneumonia may develop. Candida esophagitis
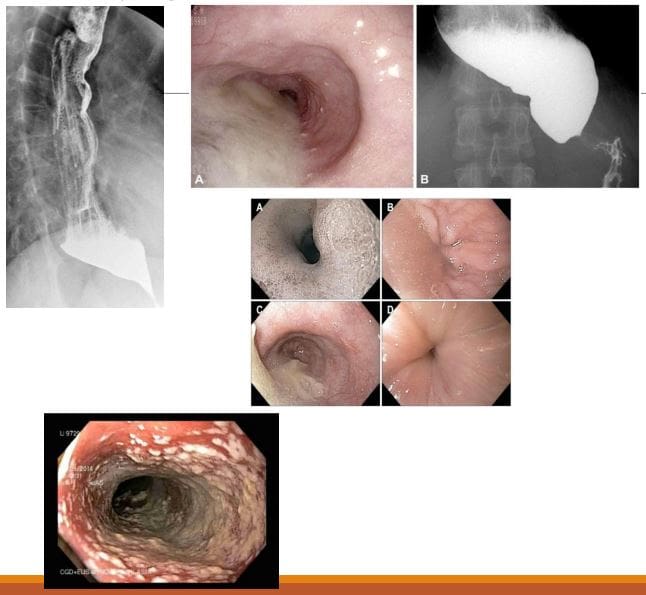
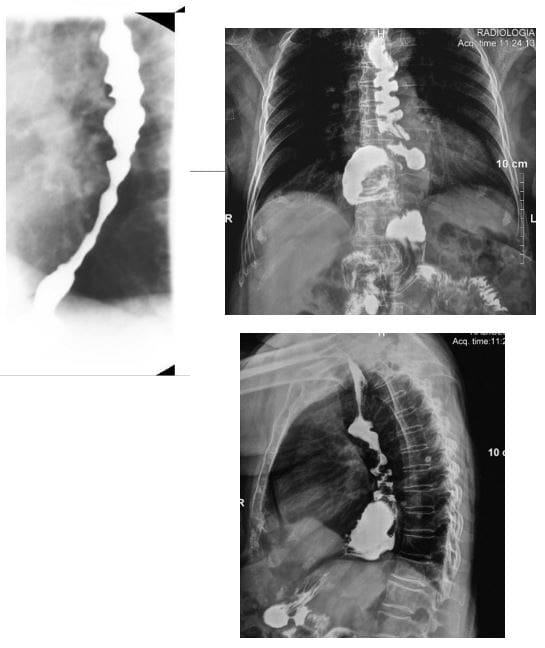
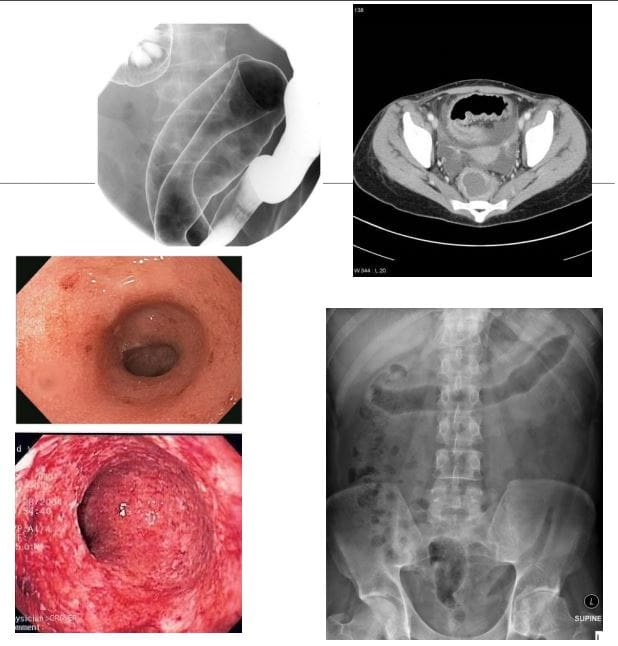
Imaging: �Bird -beak� on upper GI barium swallow, dilated esophagus, loss of peristalsis. An endoscopic exam is crucial.
Rx: difficult. Calcium channel blockers (short -term).Pneumatic dilatation, effective in 85% of patients with 3 -5% risk of bleeding/perforation. Botulinum toxin injection lasts only approx. 12 months per treatment. May scar the submucosa leading to increased risk of perforation during subsequent myotomy. Surgical myotomy (Heller myotomy)
10 -30% of patients develop gastroesophageal reflux (GERD)
Presbyesophagus: used to describe the manifestations of degenerating motor function in the aging esophagus >80-y.o. Due to interruption of the reflex arc with decreased sensitivity to distension and alteration in peristalsis.
Patients may complain of dysphagia or chest pain, but most are asymptomatic
Diffuse/distal esophageal spasm (DES) is a motility disorder of the esophagus that may appear as a corkscrew or rosary bead esophagus on barium swallow.
2% of non-cardiac chest pain
Manometry is the gold-standard diagnostic test.
Zenker diverticulum (ZD) aka pharyngeal pouch
An outpouching at the level of the hypopharynx, just proximal to the upper esophageal sphincter, known as the Killian dehiscence or Killian triangle
Patients are 60-80 y.o and present with dysphagia, regurgitation, halitosis, globus sensation
May complicate with aspiration and pulmonary abnormalities
Patients may accumulate medications
ZD- is a pseudodiverticulum or pulsion diverticulum resulting from herniation of the submucosa through the Killian dehiscence, forming a sac where food and other contents may accumulate.
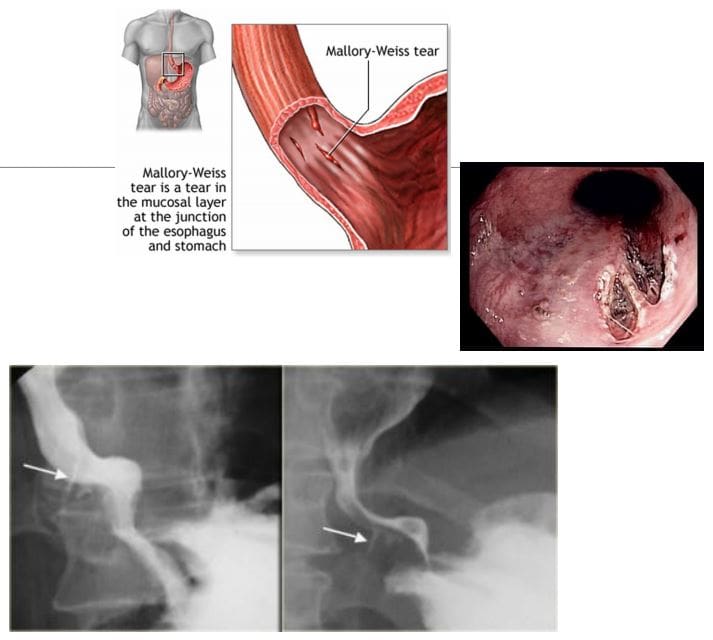
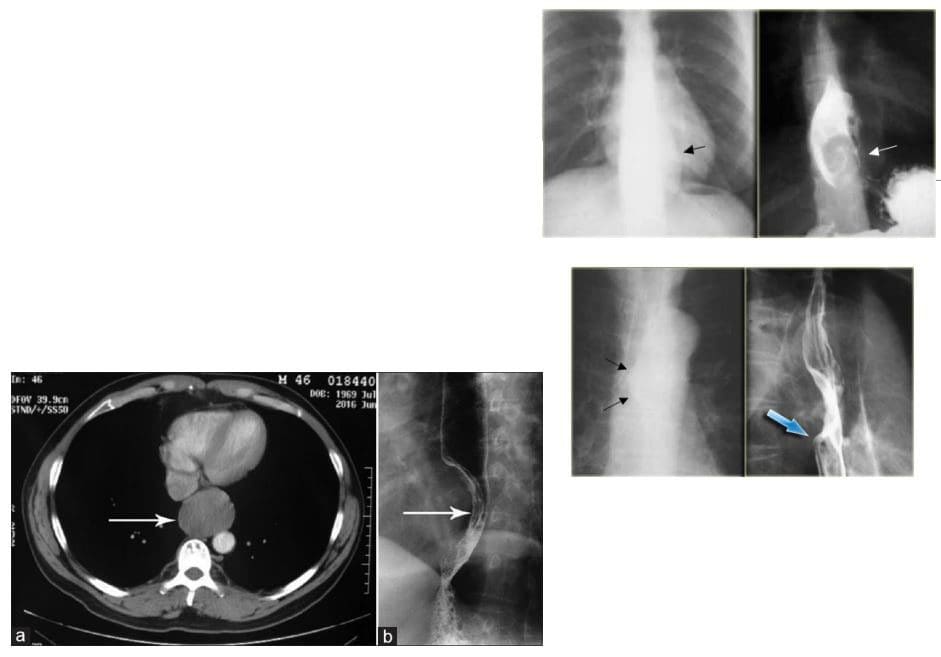
Mallory-Weiss syndrome refers to mucosal and submucosal tears of the distal oesophageal venous plexus associated with violent retching/vomiting and projection of gastric contents against the lower esophagus. Alcoholics are at particular risk. Cases present with painless hematemesis. Treatment is typically supportive.
Dx: imaging plays little role, but contrast esophagram may demonstrate some mucosal tears filled by contrast (bottom right image). CT scanning may help to exclude other causes of upper GI bleeding
Boerhaave syndrome: esophageal rupture secondary to forceful vomiting
Mechanisms involve forceful expulsion of gastric contents especially with large undigested foods when esophagus forcefully contracts against closed glottis with 90% occurring along left posterolateral wall
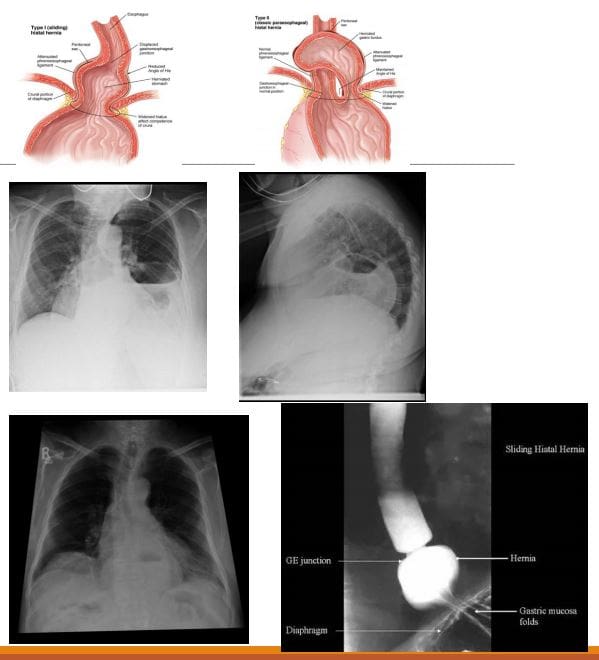
Hiatus hernias (HH): herniation of abdominal contents through the esophageal hiatus of the diaphragm into the thoracic cavity.
Many patients with HH are asymptomatic, and it is an incidental finding. However, symptoms may include epigastric/chest pain, postprandial fullness, nausea and vomiting
Sometimes HH is considered synonymous with gastro-oesophageal reflux disease (GORD), but there is a poor correlation between the two conditions!
2-types: sliding hiatus hernia 90% & rolling (paraoesophageal) hernia 10%. The latter may strangulate leading to ischemia and complications.
Esophageal Leiomyoma is the M/C benign esophageal neoplasm. It is often large but yet non-obstructive. Gastrointestinal stromal tumors (GIST) are the least common in the esophagus. Should be differentiated from Esophageal carcinomas.
Imaging: contrast esophagram, upper GI barium swallow, CT scanning. Gastroesophagoscopy is the Dx method of choice.
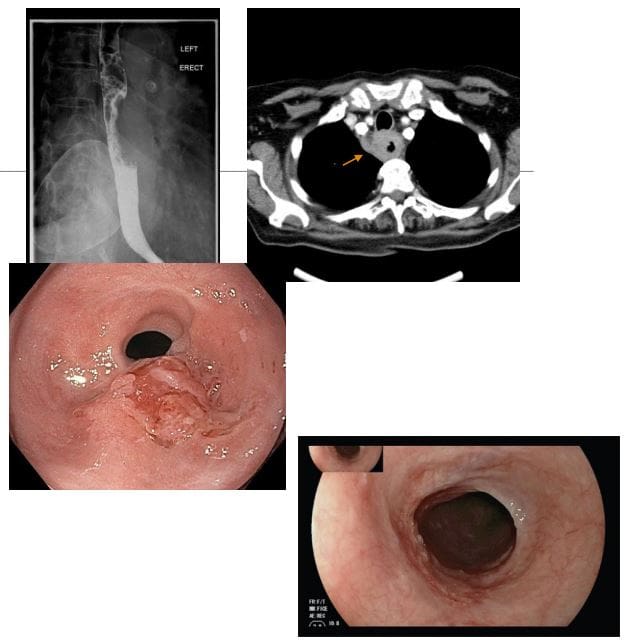
Esophageal carcinoma: presented with increasing dysphagia, initially to solids and progressing to liquids with obstruction in more advanced cases
<1% of all cancers and 4-10% of all GI malignancies. There is recognized male preponderance with the squamous cell subtype due to smoking and alcohol. Barrett esophagus and adenocarcinoma
M: F 4:1. Black individuals are more susceptible than White individuals 2:1. Poor prognosis!
A barium swallow can be sensitive in identifying esophageal mass. Gastroesophagoscopy (endoscopy) confirms the diagnosis with tissue biopsy
Overall the most common malignancy is 2ndary gastric fundal carcinoma invading distal esophagus
Squamous cell is typically found in the mid esophagus, Adenocarcinoma in the distal region
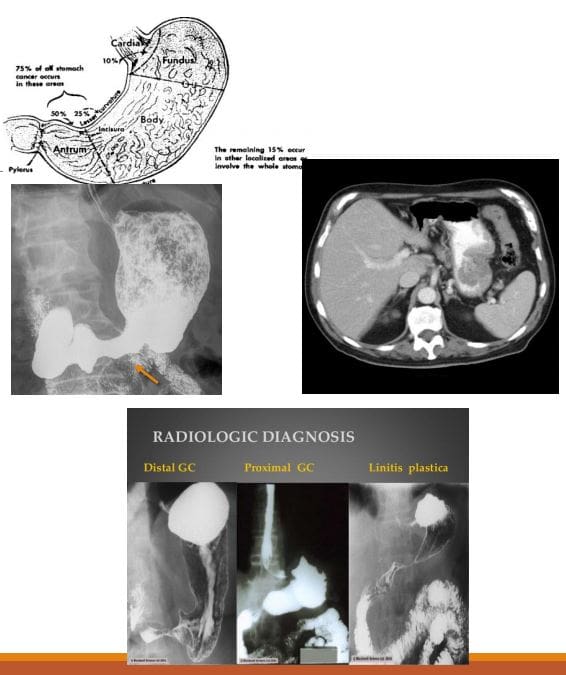
Gastric carcinoma: primary malignancy of gastric epithelium. Rare before the age of 40. The median age at diagnosis in the United States is 70 years for males and 74 years for females. Japan, South Korea, Chile, and Eastern European countries have one of the highest rates of stomach cancer in the world. Stomach cancer rates are declining worldwide. Gastric cancer is the 5th causes of cancer-related death. Association with Helicobacter pylori infection 60- 80%, but only 2% population with H. Pyloris develop Stomach cancer. 8-10% have an inherited familial component.
Gastric Lymphoma is also linked to H. Pyloris infection. Gastrointestinal Stromal Cell Tumour or GIST is another neoplasm affecting the stomach
Clinically: No symptoms when it is superficial and potentially curable. Up to 50% of patients may have non-specific GI complaints. Patients may present with anorexia and weight loss (95%) as well as vague abdominal pain. Nausea, vomiting, and early satiety d/t obstruction may occur with bulky tumors or infiltrative lesions that impair stomach distension.
Prognosis: Most gastric cancers diagnosed late and may reveal local invasion with regional adenopathy, liver, and mesenteric spread. A 5-year survival rate of 20% or less. In Japan and S. Korea, early screening programmes increased survival to 60%
Imaging: Barium upper GI study, CT scanning. Endoscopic examination is the method of choice for the diagnosis. On imaging, Gastric cancer may appear as an exophytic (polypoid) mass or Fungative type, Ulcerative or Infiltrative/diffuse type (Linitis Plastica). CT scanning is important to evaluate local invasion (nodes, mesentery, liver, etc.)
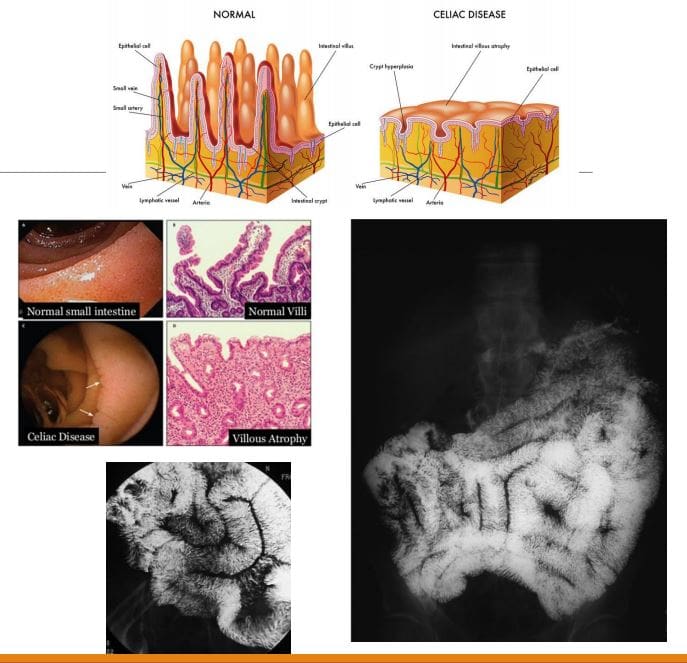
Celiac disease aka non-tropical sprue aka Gluten-sensitive enteropathy: A T-cell mediated autoimmune chronic gluten-induced mucosal damage resulting in loss of villi in the proximal small bowel and gastrointestinal malabsorption (i.e., sprue). Considered in some cases of iron deficiency anemia of undetermined cause. Common in Caucasians (1 in 200) but rare in Asian and black individuals. Two peaks: a small cluster in early childhood. Typically in 3rd and 4th decades of life.
Clinically: Abdominal pain is the m/c symptom, malabsorption of nutrients/vitamins: IDA and guaiac-positive stools, diarrhea, constipation, steatorrhea, weight loss, osteoporosis/osteomalacia, dermatitis herpetiformis. Increased association with T-cell lymphoma, Increased association with esophageal squamous cell carcinoma, SBO
Dx: Upper GI endoscopy with multiple duodenal biopsies is considered a diagnostic standard for celiac disease. Histology reveals T-cell infiltration and lymphoplasmacytosis, Villi atrophy, Crypts hyperplasia, Submucosa, and Serosa are spared. Rx: elimination of gluten-containing products
Imaging: Not required for Dx but on Barium swallow fluoroscopy: mucosal atrophy and obliteration of mucosal folds (advanced cases only). SB dilation is the most typical finding. Nodularity of the duodenum (bubbly duodenum). Reversal of jejunal and ileal mucosal folds:
�The jejunum looks like ileum, the ileum looks like the jejunum, and the duodenum looks like hell.�
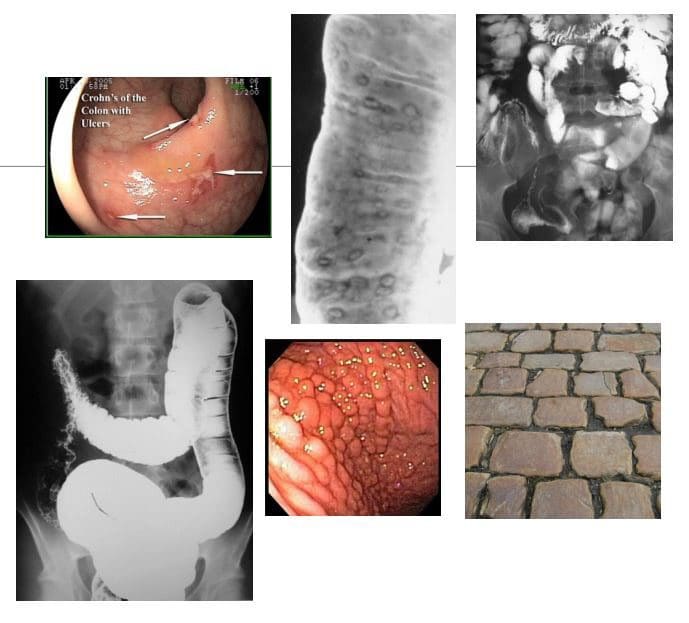
CD: chronic relapsing-remitting autoimmune inflammation that affects any part of the GI tract from the mouth to the anus but at onset most typically involves the terminal ileum. M/C presentation: abdominal pain/cramping and diarrhea. Path: granulomata formation that unlike UC is transmural, potentially leading to strictures. Areas affected by the inflammation are typically patchy
Complications are numerous: malabsorption of nutrients/vitamins (anemia, osteoporosis, developmental delay in children, susceptibility to GI malignancy, bowel obstruction, fistula formation, extra-abdominal manifestations: uveitis, arthritis, AS, erythema nodosum and others. 10- 20% may require abdominal surgery after 10-years of CD usually for strictures, fistiluzation, BO.
Dx: clinical, CBC, CMP, CRP, ESR, serological tests: DDx of IBD: anti-Saccharomyces cerevisiae antibodies (ASCA), perinuclear antineutrophil cytoplasmic antibody (p-ANCA) histologically or in serum. Fecal Calprotectin test helps to DDx IBS and evaluate response to treatment, disease activity/relapses.
Dx of choice: endoscopy, ileoscopy, and multiple biopsies may reveal endoscopic and histological changes. Video capsule endoscopy (VCE), Imaging may help with Dx of complications. Rx: immunomodulatory drugs, complementary medicine, diet, probiotics, operative. No cure but the aim is to induce remission, control symptoms and prevent/treat complications
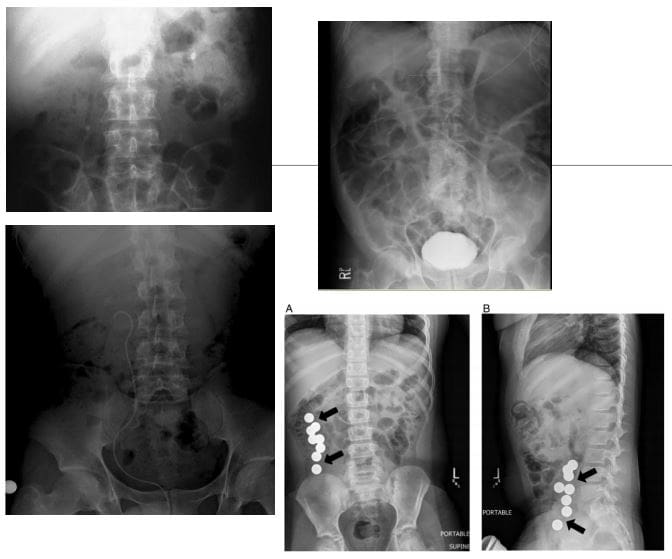
Imaging Dx: KUB to DDx SBO, Barium enema (single and double contrast), small bowel follow through. Findings: skip lesions, aphthous/deep ulcerations, fistula/sinus tracts, String sign, creeping fat pushed loops of LB, cobblestone appearance d/t fissures/ulcers pushing mucosa, CT scanning with oral and IV contrast.
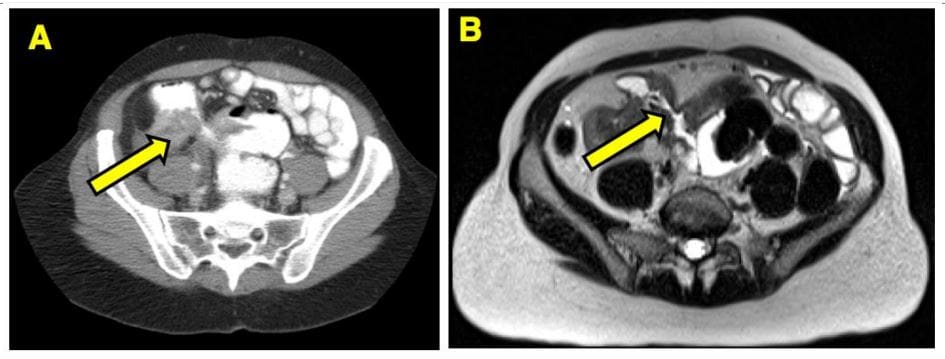
Imaging from a Crohn’s patient who had a small bowel resection for obstruction.
(B) MRE of the same area shows a fibrostenotic stricture
UC: characteristically involves only the colon but backwash ileitis may develop. Onset is typically at 15-40s and is more prevalent in males, but the onset after the age of 50 is also common. More common in North America and Europe (hygiene hypothesis). Etiology: A combination of environmental, genetic and gut microbiome changes are involved. Smoking and early appendectomy tend to show a negative association with UC, unlike in CD considered some of the risk factors.
Clinical Features: Rectal bleeding (common), diarrhea, rectal mucous discharge, tenesmus (occasionally), lower abdominal pain and severe dehydration from purulent rectal discharge (in severe cases, especially in the elderly), fulminant colitis and toxic megacolon can be fetal but are rare complications. Pathology: No granulomata. Ulcerations affect mucosa and submucosa. Pseudopolyps present as elevated spared mucosa.
An initial process always affects the rectum and remain a local disease (proctitis) in (25%). 30% Proximal disease extension may occur. UC may present as left-sided (55%) and pancolitis (10%). Majority of cases are mild to moderate
Imaging: not required for Dx but barium enema may reveal ulcerations, thumbprinting, in advanced cases loss of haustra and narrowing of the colon producing �lead-pipe colon.� CT scanning may help with Dx seen as mucosal thickening detected only in moderate and severe cases. CT may help with of Dx of complications. Plain film image reveals �lead-pipe colon� and sacroiliitis as Enteropathic arthritis (AS)
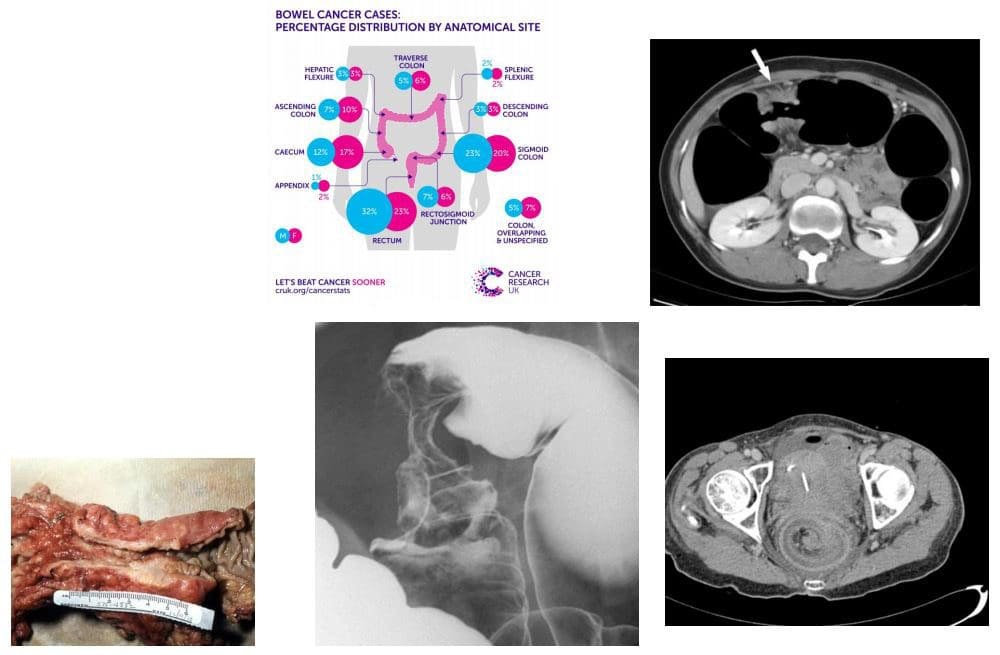
Colorectal carcinoma (CRC) m/c cancer of the GI tract and the 2nd most frequent malignancy in adults. Dx: endoscopy and biopsy. CT is the modalities most frequently used for staging. Surgical resection may be curative although the five-year survival rate is 40- 50% depending on staging. Risk factors: low fiber and high fat and animal protein diet, obesity (especially in men), chronic ulcerative colitis. Colonic adenomas (polyps). Familial adenomatous polyposis syndromes (Gardener syndrome) and Lynch syndrome as non-familial polyposis.
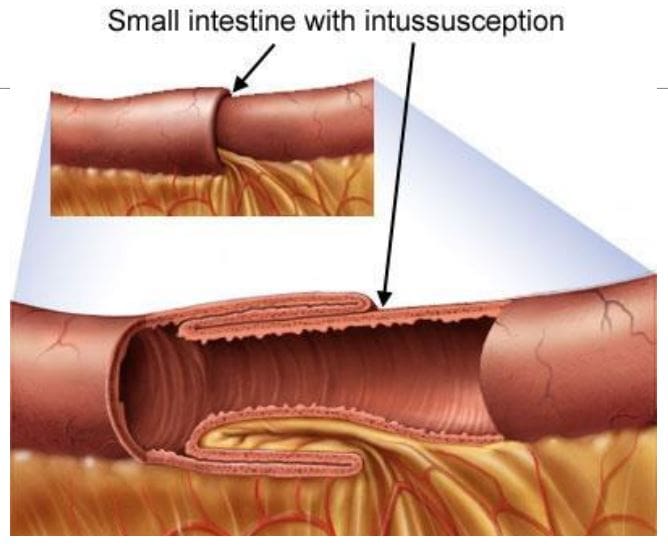
Clinically: insidious onset with altered bowel habits, fresh blood or melena, iron deficiency anemia from chronic occult blood loss especially in the right-sided tumors. Bowel obstruction, intussusception, heavy bleeding and metastatic disease especially to the Liver may be initial presentation. Path: 98% are adenocarcinomas, arise from pre-existing colonic adenomas (neoplastic polyps) with malignant transformation. The five-year survival rate is 40-50%, with stage at operation the single most important factor affecting prognosis. M/C rectosigmoid tumors (55%),
N.B. Some adenocarcinomas esp. mucinous types typically presented late and usually carry poor prognosis due to late presentation and mucin secretion and local/distant spread
Imaging: Barium enema is sensitivities for polyps >1 cm, single contrast: 77-94%, double contrast: 82-98%. Colonoscopy is a modality of choice for prevention, detection, and identification of colorectal carcinoma. Contrast-enhanced CT scanning is used for staging and prognosis evaluation of mets.
Screening: colonoscopy: men 50 y.o.-10-years if normal, 5-years if polypectomy, FOB, 1st degree relative with CA begin surveillance at 40 y.o
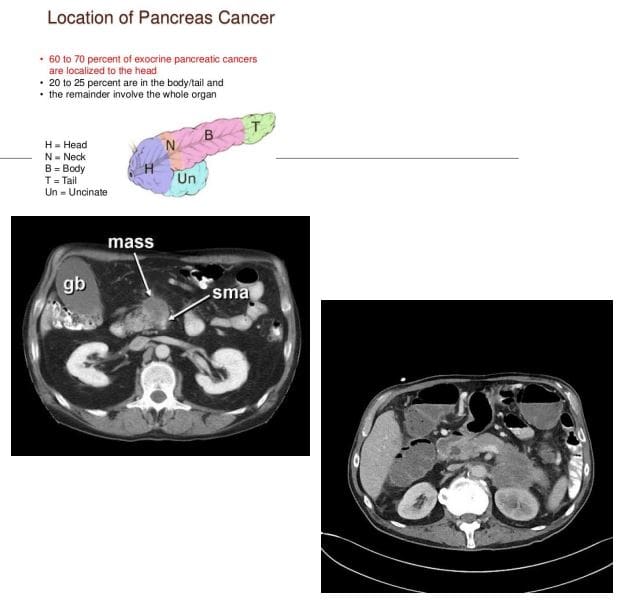
Pancreatic Cancer: ductal epithelial adenocarcinoma (90%), very poor prognosis with high mortality. 3rd M/C abdominal cancer. Colon is #1, stomach #2. Pancreatic cancer accounts for 22% of all deaths due to gastrointestinal malignancy, and 5% of all cancer deaths. 80% of cases in 60+. Cigarette smoking is the strongest environmental risk factor, a diet rich in animal fats and protein. Obesity. Family history. M/C detected in the head and uncinate process.
Dx: CT scanning is crucial. Invasion of Superior Mesenteric Artery (SMA) indicates unresectable disease. 90% of pancreatic adenocarcinomas are unresectable at Dx. Most patients die within 1-year of Dx. Clinically: painless jaundice, abd. Pain, Courvoisier�s gallbladder: painless jaundice and enlarged gallbladder, Trousseau�s syndrome: migratory thrombophlebitis, new onset diabetes mellitus, regional and distant metastasis.
CT Dx: pancreatic mass with strong desmoplastic reaction, poor enhancement, and slightly lower attenuation compared to the adjacent normal gland, SMA invasion.
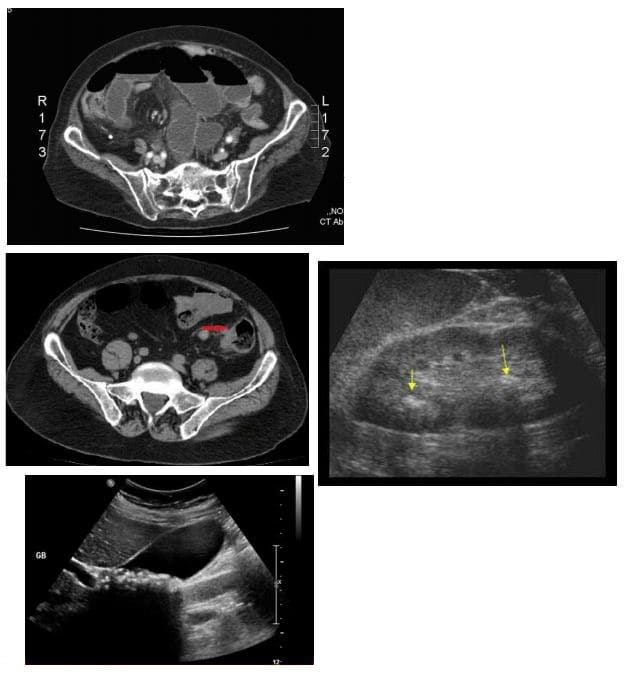
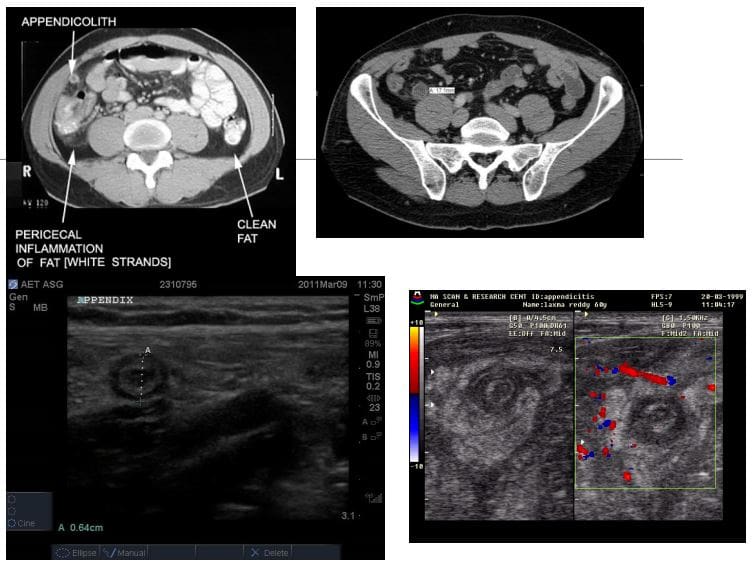
Appendicitis: very common condition in general radiology practice and is a major cause of abdominal surgery in young patients
CT is the most sensitive modality to detect appendicitis
Ultrasound should be employed in younger patients and children
KUB Radiographs should play no role in the diagnosis of appendicitis
On imaging, appendicitis reveals inflamed appendix with wall thickening, enlargement, and periappendiceal fat stranding. Similar findings of wall thickening and enlargement are noted on US. Typical �target sign� is noted on short axis US probe position.
If the appendix is retro-caecal than US may fail to provide accurate Dx and CT scanning may be required
Rx: operative to avoid complications
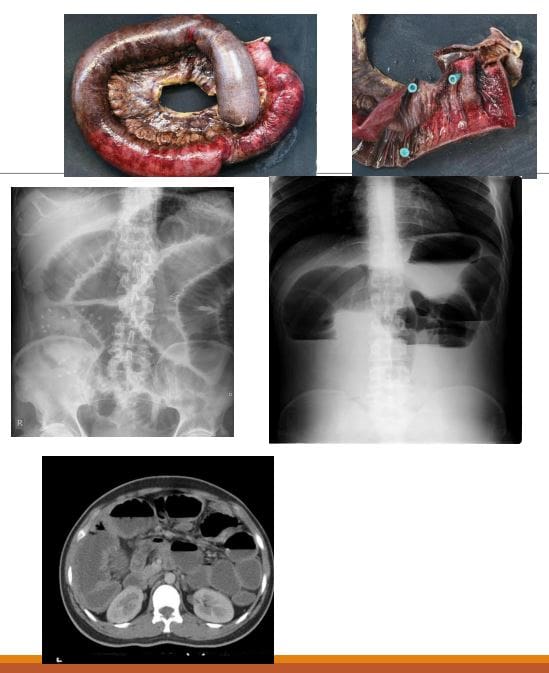
Small bowel obstruction (SBO)-80% of all mechanical intestinal obstruction; the remaining 20% result from large bowel obstruction. It has a mortality rate of 5.5%
M/C cause: any Hx of previous abdominal surgery and adhesions
Classical presentation is constipation, increasing abdominal distension with nausea and vomiting
Radiographs are only 50% sensitive for SBO
CT will demonstrate the cause of SBO in 80% of cases
There are variable criteria for maximal small bowel obstruction, but 3.5 cm is a conservative estimate of dilated bowel
On Abd x-ray: supine vs. upright. Dilated bowel, stretched valvulae conivente (mucosal folds), alternative air-fluid levels �step ladder.� Absent gas in the rectum/colon
Rx: operative as �acute abdomen.�
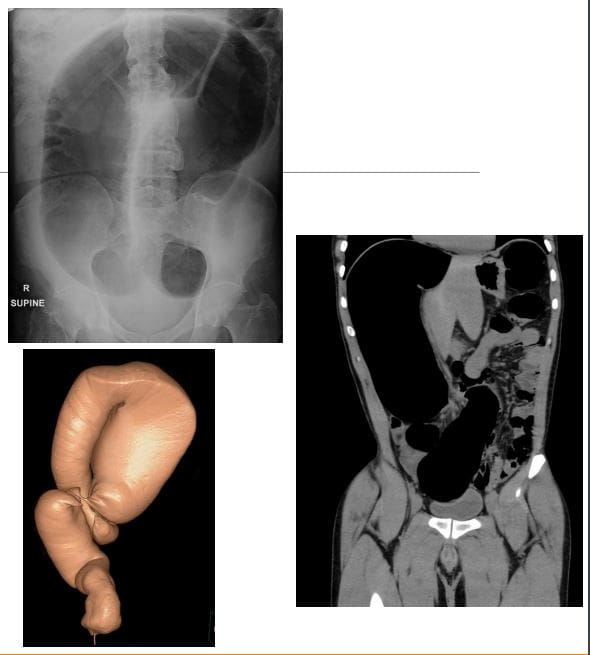
Volvulus-m/c in the Sigmoid colon esp. in elderly. The main reason: chronic constipation with redundant sigmoid twisting on sigmoid mesocolon. Leads to Large bowel obstruction (LBO). Other common causes: a colon tumor. Sigmoid vs. Caecum volvulus
Clinically: signs of LBO with constipation, abdominal bloating, pain, nausea, and vomiting. Onset may be acute or chronic
Radiographically: loss of haustra in the LB, LB distension (>6-cm), �coffee bean sign� next slide, the lower end of volvulus points to the pelvis
N.B: Rule of thumb for dilated bowel should be 3-6-9 where 3-cm SB, 6-cm LB & 9-cm Coecum
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine