Your health is easily one of the most important things in your life. When your health is good, you feel better, are more productive and generally happier. When your health is not good, it becomes difficult to accomplish even the smallest tasks�and your mood and ability to enjoy life suffer. Fortunately, there are some simple steps you can take to lead a healthier life. Read on to learn some of the most important tips for healthy living!
3 Tips for Healthy Living
Magnified Healthy Living word illustration on white background.
1. Keep the body’s alignment with regular chiropractic.
Many times people are unaware of how to move in the best way for their bodies. Poor movement patterns can lead to injuries, which make it impossible to stay as active as you like. If you start to notice any pain caused when you move�like when adopting a new exercise routine�stop doing what you are doing and consult with your chiropractor. Chiropractors are trained to identify movement problems and help correct them. Your chiropractor should be able to help you find a way to exercise that does not cause pain or lead to injury.
2. Keep track of your health.
It is important to get an accurate assessment of your current health on a regular basis. The goals you set for the future will be much more easily achieved if you know where you are starting from. Some of the ways you can keep track of your health include:
Maintain a relationship with your doctor, dentist, and chiropractor. Preventative healthcare is more effective and less expensive than waiting for something to go wrong. By keeping regular appointments with your doctor, dentist, and chiropractor, you can get valuable feedback on your current state of health. They can also help you catch potential problems early on.
Keep a diary of your exercise, diet, and mood. The diary does not have to be complicated or overly detailed. You just need a clear picture of how much you are exercising, what kinds of exercises you are doing, what food you are eating and how you are feeling.
3. Basics�a healthy diet and regular exercise.
Good health is built on a foundation of diet and exercise. The goal is to improve and maintain a regimen where you eat healthily and exercise regularly over the long-term. You do not have to do anything drastic, either. You will have an easier time making changes if you start small and gradually shift towards a lifestyle that you think is best for you.
Some points to remember:
The perfect diet for one person may not be perfect for another, but there are some basics that work well for the vast majority of people. A diet focused on whole foods, including plenty of vegetables, fruits, and whole grains, is ideal. Repeated studies have shown that a Mediterranean style diet is healthy and easy to maintain, making it a good place to start if you are new to healthy eating.
Take baby steps. Extreme shifts in diet can be mentally exhausting and difficult to maintain. Drastic changes in exercise habits risk injury and are also hard to maintain. Focus on taking small, incremental steps to reach your goals.
Contact Us Today to Set up an Appointment
If you would like a personalized plan for improving your health, please contact us. One of our chiropractic team members is ready to assist you!
Reduce *PLANTAR FASCIITIS PAIN* with Custom Foot Orthotics | El Paso, TX (2019)
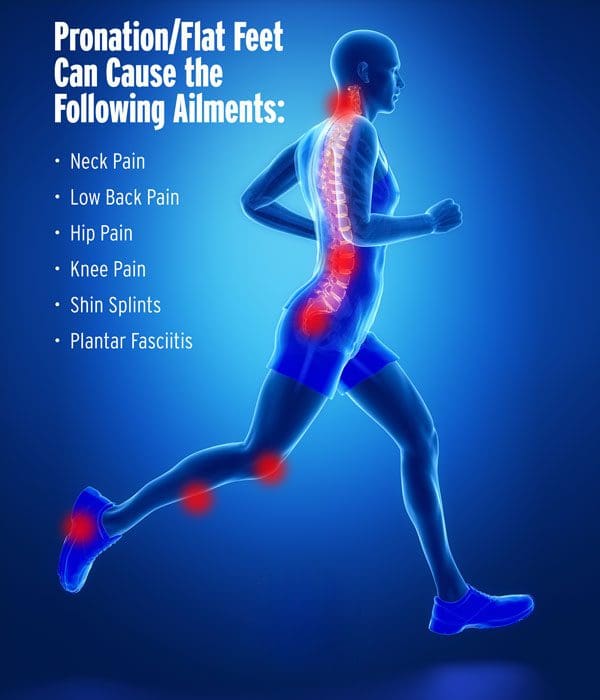
Foot pronation is the natural movement which occurs during foot landing while walking or running. Foot pronation also occurs while standing, and in this instance, it is the amount in which the foot rolls inward toward the arch. Foot pronation is normal, however, excessive foot pronation can cause a variety of health issues, including bad posture.
Plantar fasciitis: A Perspective In Functionality
Plantar fasciitis is the inflammation of the plantar fascia or aponeurosis. Which can be caused by trauma, e.g. jumping/running activity, or more from longstanding stretching of pronated feet.
The pain of plantar fasciitis is commonly at its worst when getting out of bed in the morning.
The initial steps cause a painful stretching of the tissue after hours of being in a shortened position.
As a person sleeps, the feet naturally go into a position of plantarflexion and shorten down in a relaxed.
Mild relief is common after moving about for a while.
Treatment options
Treatment options for plantar fasciitis include:
Reduced activity
Cryotherapy
Ultrasound
Taping
Massage
Chiropractic
Orthotics
If the patient is capable of walking without an antalgic gait, look to see how much foot flare occurs during the gait cycle.
Rule of thumb for foot flare:
Both feet should be pointing in the general direction you are walking toward.
Any deviation from a line directly in front involving one foot more than the other is a red flag for dysfunction in the kinetic (moving) chain and may be a contributing factor in the syndrome.
Foot flare is a compensation mechanism to help balance a wobbly pelvis.
If this is detected, remove shoes and socks and look at the medial arch.
Gentle care
Direct palpation of the plantar fascia may reveal painful thickened muscle, especially along the medial longitudinal arch.
This thickened muscle is the result of repetitive tear and repair process.
With the foot relaxed, grasp the toes and gently pull them up into passive dorsiflexion.
Gentleness is essential; as this motion stretches the irritated plantar area.
It often presents with fixations or subluxations of the bones of the feet.
The collapse of any of the three arches of the foot sets the stage for joint fixation.
Mobility & function
Mobility is life to a joint, so don�t overlook the benefit of adjusting the subluxations or fixations of the lower extremity.
Once the acute phase of plantar fasciitis is under control, you can address the factors that contributed to the condition.
Most of the time patients need arch structure to be supported in an optimal functioning position.
Custom-made orthotics support all three arches of the foot provide the necessary support to reduce the tension on the plantar fascia by blocking the excessive pronation stretches.
Improvement through non-invasive treatment
Improvement of muscle function of the kinetic chain through massage or other forms of muscle management can improve muscle compliance, or the ability of the muscle to contract and relax.
Chronic muscle tension creates joint dysfunction and can lead to inflammation in the plantar fascia.
A massaging or mechanical chiropractic compression down the length of the plantar fascia can restore flexibility to that tissue.
Roll the foot over a golf ball or similar device for the purpose of restoring fascia flexibility can have profound effects on foot pain and function.
Patient tolerance is the key to any technique used, so try to understand that the chiropractor/physical/massage therapists are trying their best to bring relief, increasing the pressure and the length of any intervention.
Plantar or Neural
Feet are important. When you consider what your feet go through, taking 8,000 steps over the course of a day, according to the�Illinois Podiatric Medical Association�(IPMA), it�s easy to see how 75 percent of all Americans will have some type of�foot pain�at some point in their lives.�Plantar fasciitis is a common and very painful foot condition that can become chronic if not treated. It is also a condition that responds very well to chiropractic care. As it Reduces Stress in the Plantar Fascia�� When a ligament is inflamed or stressed the tissue can develop very small tears that cause the pain of plantar fasciitis. Chiropractic adjustments made to the heel and foot take the pressure off of the plantar fascia, allowing it to relax.
NCBI Resources
The SMART approach is a guide for setting realistic goals and attaining them. It is an acronym that outlines a success-focused�strategy for goal setting:
Specific
Measurable
Accountable
Realistic
Timeframe
Each step will bring you closer to achieving your goals and improve your health.
Runner’s knee is a term commonly utilized to characterize a variety of health issues which can ultimately cause pain, discomfort, and other symptoms around the kneecap also referred to as the patella. These health issues include anterior knee pain syndrome, patellofemoral malalignment, chondromalacia patella, and iliotibial band syndrome. �
Runner’s knee commonly occurs in athletes, especially runners, however, any type of exercise or physical activity which repeatedly stresses the knee joint could cause the health issue. This may include walking, skiing, biking, jumping, cycling, and playing soccer. According to the Harvard Medical School, runner’s knee is more prevalent in women than in men. �
What are the Symptoms of Runner’s Knee?
The most common symptoms associated with runner’s knee includes is a dull, aching pain around or behind the kneecap, also referred to as the patella, especially where it meets the lower region of the thighbone or femur. You may feel pain when: �
Walking
Climbing (or descending) stairs
Squatting
Kneeling
Running
Sitting down or standing up
Sitting for extended periods of time with the knee bent
Other symptoms include swelling and popping or grinding in the knee.
In the case of iliotibial band syndrome, the pain is most intense on the exterior region of the knee. This is where the iliotibial band, which runs from the hip to the lower leg, connects to the tibia, or the thicker, inner bone of the lower leg. � Moreover, the symptoms commonly associated with runner’s knee can also ultimately affect an individual’s gait, or manner of walking, and even their posture while standing or walking. These changes can cause the structures of the human body to compensate for the altered functions, resulting in a variety of health issues, such as low back pain and sciatica. �
What are the Causes of Runner’s Knee?
The pain and discomfort of runner’s knee may be brought on by the irritation of the complex soft tissues or lining of the knee, and worn or torn cartilage, as well as strained tendons. Any of the following causes can cause runner’s knee, including: �
Overuse
Trauma or injury to the kneecap
Misalignment of the kneecap
Complete or partial dislocation of the kneecap
Flat feet
Weak or tight thigh muscles
Insufficient stretching before exercise or physical activity
Arthritis
A fractured or broken kneecap
Plica syndrome or synovial plica syndrome, where the lining of the joint becomes thickened and inflamed
Occasionally, the painful symptoms can originate in the lower back and hip into the knee. This is known as “referred pain.” �
How is Runner’s Knee Diagnosed?
To determine a diagnosis of runner’s knee, the healthcare professional requires a complete medical history and a thorough physical evaluation which may often include blood tests, X-rays, MRI scans, or CT scans for an accurate diagnosis. �
What is the Treatment for Runner’s Knee?
The healthcare professional will determine the best treatment approach depending on the cause of runner’s knee, however in most instances, runner’s knee can be treated without surgery. Most often, the initial step in treatment is to utilize RICE: �
Rest: Avoid repetitive pressure on the knee.
Ice: Decrease pain and swelling by applying an ice pack and prevent heat to the knee.
Compression: Wrap the knee utilizing an elastic bandage or sleeve to restrict swelling.
Elevation: Place a pillow under the knee when sitting or bending down to prevent further swelling. If there is considerable swelling, maintain the foot raised above the knee and the knee above the level of the heart.
Over-the-counter nonsteroidal anti-inflammatory drugs or NSAIDs, such as aspirin, ibuprofen, and naproxen can also help further reduce pain, discomfort, and swelling. Acetaminophen can also help reduce symptoms. You may want to speak with your doctor before taking these medications, especially if you have other health issues or take other prescription drugs. � The healthcare professional may also recommend stretches and exercises to improve strength and range of motion. They may tape your knee or provide you with a brace to offer additional pain relief. You may also utilize custom foot orthotics to support your knee. Surgery may be recommended if your cartilage is damaged or if your kneecap has to be realigned. �
How Can Runner’s Knee be Prevented?
The American Academy of Orthopaedic Surgeons recommends these methods and techniques to prevent runner’s knee: �
Stay in form. Ensure that your overall health and wellness is good. If you are overweight, speak with your healthcare professional about developing a customized weight loss program.
Stretch. Do a five-minute warmup followed by stretching exercises before you run or perform any physical activity which adds pressure to the knee. Your doctor can show you how to improve your knee’s flexibility.
Gradually increase training. Never suddenly increase the intensity of your workout. Instead, make gradual changes.
Use proper footwear. Purchase quality shoes with good shock absorption, and be sure they fit properly and comfortably. Don’t run in shoes which are too worn out. Wear custom foot orthotics if you’ve got flat feet.
Use the proper running form. Keep a tight core to prevent yourself from leaning too far forward or backward and keep your knees flexed. Attempt to run on a soft, smooth surface. Prevent running on concrete. Walk or run in a zigzag pattern when moving down a steep incline to avoid adding unnecessary pressure on your knees and feet.
Runner’s knee is a well-known term utilized to describe a variety of health issues associated with a similar collection of painful symptoms. Runner’s knee generally includes patellofemoral pain syndrome, or PFPS, and/or iliotibial band syndrome, or ITBS, both of which are considered repetitive stress injuries. It’s essential to seek immediate medical attention to determine an accurate diagnosis of runner’s knee and continue with the proper treatment approach.� – Dr. Alex Jimenez D.C., C.C.S.T. Insight
Low Back Pain
�
The purpose of the article is to understand how runner’s knee can be associated with sciatica and other symptoms. Sciatica is a collection of symptoms characterized by pain, tingling sensation, and numbness. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Foot Orthotics
Low back pain and sciatica are common health issues which affect many individuals worldwide. However, did you know that chronic pain may be due to foot problems? Health issues originating in the foot may ultimately cause imbalances in the spine, such as poor posture, which can cause the well-known symptoms of low back pain and sciatica. Custom foot orthotics, individually designed with 3-arch support can help promote overall health and wellness by supporting and promoting good posture and correcting foot problems. Custom foot orthotics can ultimately help improve low back pain and sciatica. �
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force. �
Kyphosis is a condition that is most typically identified by a humped mid to upper back. It can be frustrating to find yourself diagnosed with kyphosis, both due to the unusual appearance it causes and the physical discomfort that can come with the condition. Fortunately, chiropractic offers a variety of treatment options for kyphosis that are non-invasive, drug-free and quite effective. With the right approach, it should be possible to get significant relief for your symptoms through chiropractic care.
Causes
Many times kyphosis is caused by poor posture. Years of hunching your back can cause the body to change the way the vertebrae sit atop one another�leading to stretching of soft tissues and a resting position that is hunched instead of upright.
Not all cases of kyphosis are the result of poor posture, however. There are some people who are born with kyphosis. There are also those that develop kyphosis following trauma or due to disease. One of the most common diseases that result in kyphosis is Scheuermann’s disease.
Chiropractic can often help resolve kyphosis that is caused by poor posture. If your kyphosis is due to trauma or other issues, chiropractic can still provide a much-needed relief from many of your symptoms�including pain and stiffness.
How Chiropractic Helps With Kyphosis
HEALTHCARE AND MEDICAL CONCEPT: KYPHOSIS
Diagnosing the Cause
Your first visit to the chiropractor will begin with a comprehensive examination to determine the cause of your condition. An accurate diagnosis is key to developing an effective treatment plan. The examination will most likely include imaging tests like an x-ray or MRI. It may also include a physical examination to figure out how your body currently moves, where you are tender and/or in pain, etc.
Treatment Plan
Your chiropractor will never move forward with treatment until he or she has explained your options and gotten your permission to begin. The treatment plan you are offered may include:
The joint in the human body, particularly the spinal joints, have an ideal alignment where everything fits together best. The more you can achieve and maintain this alignment, the less pain, stiffness and other disruptions you can expect to experience. Chiropractic adjustments aim to bring your body back into alignment.
Regular adjustments should help to improve your spinal alignment and straighten your back. In the case of poor posture, adjustments can aid you in learning how to improve your posture and keep those improvements over the long term.
Mobility Increased
The curving of the back typical of kyphosis can lead to a lot of stiffness in the spine and surrounding soft tissues. Lack of mobility makes everything you do more difficult, so it makes sense to try and increase your mobility when possible.
Chiropractic adjustments and complementary therapies are ideal for relaxing the soft tissues that may have become stiff as the kyphosis developed. One of the great things about improving the mobility of the spine is that it allows you to improve your posture. Over time, it should become easier to keep your back in a more healthy alignment.
Pain Lessened
Pain is common with kyphosis. The spine is not meant to hump as it does with kyphosis, which explains why pain is so typical with the condition. Chiropractic is very useful for decreasing pain related to spinal issues. Many patients get relief immediately following their first adjustment.
Schedule an Appointment With Us Today
If you are suffering from kyphosis, please contact us to schedule an appointment. Our chiropractic team is standing by to answer your questions and help you get treatment for your condition.
What is a Pronated Foot & What Can Custom Orthotics Do?
When a foot is pronated, it means its arches have fallen and the foot is flat. Flat feet do not absorb shock as well and make for a less stable base for�the bones, muscles, ligaments, and tendons. They can also:
Shift the body’s alignment out of order
Cause aches and pains in the feet, knees, hips, neck and/or spine
Lead to injury and problems like shin splints, Achilles tendinitis, and plantar fasciitis
Up to a third of people suffer from flat feet
Causes
The connective tissue, called the plantar fascia, on the underside of the foot is what maintains the foot�s healthy arch shape. Injury and health conditions can cause the fascia to stretch out and flatten. But so can everyday walking and standing. Once the fascia stretches out, it is unable to spring back. When the foot structure becomes flattened, the body�s foundation is prone to injury and health conditions.
Treatment
Chiropractic adjusting to ensure proper positioning of bones and joints
Custom orthotics in every pair of shoes for pronation control, support, and comfort
Get Rid of *Foot Pronation* with *FOOT ORTHOTICS* | El Paso, Tx (2019)
Pronation
Pronation describes the way that the foot rolls inward during its normal motion. The foot turns inward, flattening out, as the heel�s outer edge strikes the ground. For the foot to function correctly, there must be a significant degree of pronation. However, excessive pronation, or overpronation, can cause injury and damage to the foot and ankle. It creates the arch in the foot to flatten, and the ligaments, tendons, and muscles under the foot overstretch. For instance, overpronation of the foot causes a series of internal changes that extend up through the leg. The femur may rotate causing hip pain and inflammation of the sacroiliac joint which leads to back pain. Other misalignments in the body that are caused by foot problems can also lead to chronic lower back pain as well.
NCBI Resources
Sometimes there are abnormalities of the spine and it causes a misalignment of the natural curvatures or some curvatures may be exaggerated. These unnatural curvatures of the spine are characterized by three health conditions called�lordosis, kyphosis, and scoliosis. They gently curve, sloping slightly inward at the small of the back, and again slightly at the neck. The pull of gravity, combined with body movement, can put a great deal of stress on the spine and these slight curves help absorb some of the impact. Spinal manipulations for spinal curvature disorders�have been shown to be very effective. Chiropractic helps restore the spine�s natural balance even if the patient has one of these types of conditions.
Foot drop is a health issue which identifies a weakening of the muscles which allow for flexing of the ankle and toes. This health issue causes the patient to drag the front part of the foot when walking. To compensate for this dragging, the patient will often flex the knee to raise the foot higher than in a standard stride, frequently referred to as high steppage gait. �
Foot drop generally affects the muscles in charge of moving the ankle and foot upward, especially the anterior tibialis, the extensor halluces longus, and the extensor digitorum longus. Although foot drop is a neuromuscular disorder which affects the muscles and the nerves, it’s not a disease. It is a symptom of an underlying health issue, perhaps a spinal health issue. �
What are the Symptoms of Foot Drop?
The most well-known symptom of foot drop, high steppage gait, is commonly characterized by raising the thigh up in an exaggerated manner while walking, similar to climbing the stairs. High steppage gait is associated with one of the following: �
Dragging of the foot and toes
Scraping of the toes throughout the floor
Uncontrolled slapping of the toes against the floor
The affected muscles are often utilized to maintain the foot off the ground during the swing-through phase of walking. If these are weak, they can’t maintain the foot up and the foot will scrape throughout the floor if the foot is not raised high. Aside from the common symptoms above, additional problems typically associated with foot drop can ultimately include: �
The inability to raise the foot at the ankle
The inability to point the toes upward in the human body, frequently referred to as dorsiflexion
Struggling to walk normally in a heel-to-toe manner
Other well-known symptoms also associated with foot drop may ultimately include one or a combination of the following: �
Excessive, swinging hip motion. With foot drop, the hip may swing out to prevent the toes from hitting the floor.
Limp foot. The affected foot may flop away from the individual.
Pain, tingling sensations, and numbness in the foot. The intensity of the symptoms can vary from person to person. Symptoms can make regular tasks, such as walking or driving, difficult. The foot pain may be associated with sciatica.
Difficulty engaging in exercise and/or physical activities requiring the utilization of the front of the foot. By way of instance, climbing stairs may become challenging for patients with foot drop.
Muscle atrophy in the lower extremities. Muscle atrophy refers to a muscle decreasing in mass and weakening. Because the anterior tibialis, the extensor halluces longus, and the extensor digitorum longus muscles are affected by foot drop, muscle atrophy may occur and make it more challenging to exert force in the lower extremities.
Foot drop may be experienced in one or both feet. Foot drop is generally experienced in a single foot.
What are the Causes of Foot Drop?
Foot drop is a symptom of an underlying health issue. Foot drop causes fall into one or a combination of three categories: �
Muscle damage or injury
Skeletal or anatomical abnormalities affecting the foot
Nerve damage
Specific conditions or diseases and other health issues which may cause foot drop may also include: �
A lumbar spine health issue
A stroke or tumor
Parkinson’s disease
Diabetes
Motor neuron disease
Multiple sclerosis
Adverse reactions to drugs and/or medications as well as alcohol
An injury to the leg or foot
There’s a variety of lumbar spine health issues which can ultimately affect the nerve roots, including the peroneal nerve and the sciatic nerve. Any compression or impingement of the nerve roots in the lower back may cause foot drop. Common lower back or lumbar spine health issues which can cause foot drop and a variety of other symptoms, such as sciatica, may include: �
Lumbar herniated disc
Lumbar spinal stenosis
Spondylolisthesis
Bone fractures or lacerations
It should be known that determining the underlying cause of foot drop is often necessary to be able to effectively treat it. �
How is Foot Drop Diagnosed?
Foot drop is generally diagnosed through a physical evaluation. The healthcare professional will watch the patient walk and check their leg muscles for weakness. The doctor should also check for pain, tingling sensation, and numbness on the foot. �
Imaging Tests
Foot drop is sometimes caused by an overgrowth of bone in the spinal canal or by a tumor or cyst pressing on the nerve roots in the lumbar spine. Imaging tests will help pinpoint these kinds of health issues. These imaging tests can include: �
X-rays. Plain X-rays utilize a minimal amount of radiation to show a soft tissue mass or even a bone lesion.
Ultrasound. This technology, which utilizes sound waves to create images of internal structures, may check for tumors or cysts on the nerves or demonstrate swelling on the nerves due to compression or impingement.
CT scan. This combines X-ray images from distinct angles to form cross-sectional perspectives of structures.
Magnetic resonance imaging or MRI. This test utilizes radio waves and a strong magnetic field to produce detailed images. MRI is very useful in showing soft tissue lesions which may be irritating a nerve.
Nerve Tests
Electromyography, or EMG, and nerve conduction studies measure electrical activity in the muscles and nerves. These tests can be uncomfortable, but they’re helpful in determining the region of the damage or injury along the affected nerve. �
What is the Treatment for Foot Drop?
Treatment for foot drop depends on the cause of the health issue. If the cause is successfully treated, foot drop may improve or even disappear. If the cause can’t be treated, foot drop may be irreversible. Treatment for foot drop may include:
Braces or splints. A brace or splint on your ankle and foot which fits a shoe can maintain the foot in a normal position.
Chiropractic care or physical therapy. Alternative treatment options including stretches and exercises can help strengthen the lower extremities and their range of motion which may improve gait problems associated with foot drop. Stretching stretches and exercises are especially important to protect against stiffness in the heel. The healthcare professional may also provide custom foot orthotics to provide additional support, stability, and shock absorption.
Nerve stimulation. Occasionally stimulating the nerve which lifts the foot can help improve foot drop.
Surgery. Depending on the cause and if the patient’s foot drop is comparatively new, surgical interventions may be useful. If the patient’s foot drop is long-standing, the healthcare professional may suggest surgery which fuses the ankle and foot bones or a process which transfers an attached muscle and tendon to another region of the foot.
Foot drop is a health issue in which the raising of the front part of the foot is difficult. Foot drop is not a condition or disease but rather, a symptoms of an underlying health issue. Muscle and/or nerve damage caused by injury and/or an aggravated health issue, such as a lumbar herniated disc, spinal stenosis, spondylolisthesis, and/or fractures can ultimately cause foot drop. These health issues can also cause low back pain and sciatica as well as other painful symptoms.� – Dr. Alex Jimenez D.C., C.C.S.T. Insight
Low Back Pain
The purpose of the article is to understand how foot drop can be associated with sciatica and other symptoms. Sciatica is a collection of symptoms characterized by pain, tingling sensation, and numbness. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Foot Orthotics
Low back pain and sciatica are common health issues which affect many individuals worldwide. However, did you know that chronic pain may be due to foot problems? Health issues originating in the foot may ultimately cause imbalances in the spine, such as poor posture, which can cause the well-known symptoms of low back pain and sciatica. Custom foot orthotics, individually designed with 3-arch support can help promote overall health and wellness by supporting and promoting good posture and correcting foot problems. Custom foot orthotics can ultimately help improve low back pain and sciatica. �
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force. �
Chiropractic can help with a wide variety of health conditions, particularly those involving the spine. Your chiropractor�s ability to adjust your spine makes it possible to correct many issues with the back and neck. Chiropractic also offers the advantage of being drug-free and non-invasive, so the side effects you need to worry about are minimal.
6 Spine Disorders that Chiropractic Helps
1. Degenerative Disc Disease
Most often, degenerative disc disease is a condition that strikes people as they get older. The discs that sit between your vertebrae are supposed to be relatively soft to provide cushion and flexibility to the spine. Unfortunately, years of use and various injuries can cause the discs to wear down. When they wear down it can lead to pressure on nerves and bone on bone contact.
2. Herniated Disc
Sometimes a disc can rupture, allowing the interior matter to protrude from the outer shell and press against nerves in the spine. The most common areas of the body to have a herniated disc are the lower back and the neck.
3. Sciatica
The sciatic nerve travels from the lower back and down the legs. The nerve can become irritated if there are issues with the lower back, such as degenerative disc disease, herniated disc or misalignment. Pressure on the nerve can cause symptoms like shooting pains, numbness, tingling, dull aching, and other discomforts.
4. Whiplash
Whiplash is most common in rear-end car accidents, where a car hits you from behind and causes your head to whip forward and backward. The force generated by the whipping motion can cause significant damage to your neck. Stiffness and pain are common symptoms. Whiplash should be treated as soon as possible following an accident.
5. Myofascial Pain
The fascia is the sheath-like material that surrounds your muscles. Adhesions can occur in the fascia due to overuse or injury. Sometimes the painful points can feel like hard knots under the skin. Myofascial pain often causes discomfort in other areas of the body that you would not assume are related to the problem area.
6. Back Sprains and Strains
There are many ways that the back can become sprained or strained. A sprain involves the ligaments that are attached to your bones, while a strain involves your muscles and/or tendons. Either condition can cause significant pain and a loss of mobility.
Chiropractic Can Help By
Your chiropractor will offer you different options for healing your spinal condition. These may include:
Adjustments
Many times the problems with your spine can be improved by realigning the vertebrae. Injuries and spinal conditions are often associated with misalignment�where the vertebrae are not sitting on top of one another as they should be. A chiropractic adjustment gently returns your vertebrae to alignment.
Massage Therapy
Massage is a great complementary therapy to chiropractic adjustments. It can help to relax muscles, eliminate adhesions and improve mobility. It can also help your spinal adjustments to stay in place as you go about your day to day life.
Ultrasound
Ultrasound treatments are an effective way to encourage your body�s own healing mechanisms without causing any unwanted side effects. The sound waves penetrate deep into the tissues to create heat energy, which encourages circulation and aids in healing.
Get Help with Your Spinal Disorder
If you are struggling with a spinal disorder like those mentioned above, we would love the opportunity to help. Our chiropractic team understands how to administer safe, effective treatments that are non-invasive and work together to improve healing outcomes.
Please contact us today to discuss your spinal condition and schedule an appointment.
Heel Spurs
Do you have a sharp pain in your heel? When you take a step, does it feel like a knife is stabbing your heel? If the answer is yes, then you might have a heel spur.
A heel spur is a degenerative outgrowth of bone on the calcaneus. While the heel spur itself is sometimes painless, the condition is commonly associated with Plantar Fasciitis.
Though adjustments may help reduce symptoms, they do not restore plantar aponeurosis laxity or the resultant excessive pronation.
Custom orthotics support all 3 arches, which help control pronation and protect against heel shock.
Your healthcare provider and custom orthotic’s center can offer a special cut out�at the site of the insertion of the plantar fascia to reduce pressure.
Conclusion
Heel spur pain can be reduced by seeing your movement patterns of the foot and ankle. While there is no cure for heel spurs, chiropractic foot adjustments, orthotics and home stretching can help.
El Paso, TX Chiropractic Heel Spur Treatment
Blanca, born and raised in El Paso, TX, has been suffering from heel spurs for approximately two years. As a registered nurse, her symptoms appreciably affected her ability to work and her general quality of life. Determined to improve her health, Blanca believed care. Once she began treatment with Dr. Alex Jimenez, however, Blanca experienced enormous relief from her heel spurs, nearly immediately. Blanca highly recommends chiropractic care with Dr. Alex Jimenez as the nonsurgical selection for the treatment of heel spurs. A heel spur is a calcium residue resulting in a bony protrusion on the bottom of the heel bone.
Although heel spurs are often painless, they can lead to heel pain. They are often associated with plantar fasciitis, a painful inflammation of the fibrous band of connective tissue (plantar fascia) which runs across the bottom of the foot and connects the heel bone to the ball of the foot. Heel spurs are usually caused by strains on foot ligaments and tendons, stretching of the plantar fascia, and repeated tearing of the membrane that covers the heel bone. Heel spurs are especially common among athletes.
Orthotics
Foot Dysfunction can very easily cause a domino effect that extends all the way to the back. The feet are the foundation of the body and when there is a problem with the way they function it can cause the entire body to shift out of alignment. Overpronation and oversupination can cause a variety of injuries and conditions that affect not only the feet and ankles, but also the knees,�hips, and back as well.
Functional Hallux Limitus
Functional hallux limitus is unfortunately still considered to be a rare health issue which often goes unaddressed. Outcomes for many different foot disorders will be jeopardized if treatment doesn�t address functional hallux limitus. Foot and postural abnormalities have a basis in poor function of stabilization and the windlass mechanism of the foot structure through the plantar fascia.
NCBI Resources
Although many people try to treat their low back pain on their own first, one of the fastest and best ways to treat it is through custom orthotics, which actually optimize the performance of your entire body, not just your feet and lower back. For instance, overpronation of the foot causes a series of internal changes that extend up through the leg. The femur may rotate causing hip pain and inflammation of the sacroiliac joint which leads to back pain. Other misalignments in the body that are caused by foot problems can also lead to chronic lower back pain as well.
Heel spurs are a health issue which causes the development of a bony-like expansion, known as a calcium deposit, which develops between the heel bone and arch. Heel spurs generally begin in the front of the heel and may affect other regions of the foot. They’re generally about a quarter of an inch in length and they may not necessarily be visible to the naked eye. �
Diagnosing heel spurs can be challenging for healthcare professionals because these don’t necessarily trigger painful symptoms and not all heel pain is associated with heel spurs. The purpose of the following article is to discuss the symptoms, causes, treatment, and prevention of heel spurs as well as their association with radiating pain and sciatica symptoms. �
What are the Symptoms of Heel Spurs?
Common symptoms of heel spurs may include pain, discomfort, swelling, and inflammation in the front of the heel. Alongside the painful symptoms previously described, the affected region may also feel warm to the touch. The painful symptoms can also radiate or spread to the back of the foot. Over time, a small bony protrusion may become observable to the naked eye. �
Some heel spurs may also cause no painful symptoms. However, approximately 50 percent of people with heel spurs will experience heel pain.� Some heel spurs may also not result in any changes to the bones or soft tissues surrounding the heel. Moreover, the painful symptoms may affect an individual’s gait and posture, causing compensation which can ultimately result in a variety of other health issues. A spinal misalignment, or subluxation, may cause low back pain and sciatica. �
Heel spurs are frequently diagnosed utilizing X-rays and other clinical evaluations for foot health issues. Heel spurs are difficult to diagnose because the symptoms are similar to other types of heel pain. It’s fundamental to visit a healthcare professional to receive a proper diagnosis. The healthcare professional can then diagnose a heel spur utilizing X-rays. �
What are the Causes of Heel Spurs?
Heel spurs are caused by long-term muscle and ligament strain. The excess strain can affect the soft tissues of the heel and wear them out. Heel spurs generally develop over an extended period of time and often after the individual ignores early signs, such as heel pain.�Repetitive pressure from walking, running, or jumping on hard surfaces is a common cause of heel spurs. These may also develop from wearing shoes which don’t properly support the foot. Heel spurs may also be caused by: �
Arthritis
Bruising of the heel
Excess body weight
Poorly fitted shoes
Walking gait problems
Using flip-flops too often
Worn-out shoes
What is the Treatment for Heel Spurs?
Fortunately, there are a variety of treatment approaches for heel spurs. Treatment choices for heel spurs can include: �
Cold compresses. Applying ice packs after exercise and/or physical activity may be especially beneficial.
Anti-inflammatory injections. This helps alleviate pain and inflammation in the heel of the foot and arch.
Over-the-counter pain drugs and/or medications. These could include acetaminophen, aspirin, or ibuprofen.
Chiropractic care and physical therapy. These, alongside stretches and exercise, can help improve symptoms.
Rest. It is essential to rest the feet after standing or engaging in physical activities for an extended period of time.
Orthotic shoe inserts. These may help provide you arch support.
Healthcare professionals may recommend surgery as a last resort if other alternative treatment options don’t help improve heel spurs. This surgical intervention involves the removal of the heel spur. Sometimes it also involves releasing the plantar fascia muscle. Heel spur surgery can reduce painful symptoms and help boost mobility in the foot. Due to the safety and effectiveness of other alternative treatment options, surgery is generally not recommended for the treatment of heel spurs. �
Heel spurs are characterized as a degenerative outgrowth of bone on the calcaneus, or the heel bone. Although heel spurs may be commonly associated with heel pain and discomfort, not all cases of heel spurs cause painful symptoms. Long-term stress and/or pressure can cause heel spurs. Heel spurs can also cause low back pain and sciatica. Because of the altered gait during heel strike and foot-off due to the painful symptoms, heel spurs can cause hip imbalances and compensation health issues. Spinal misalingments, or subluxations, due to altered posture can ultimately cause low back pain and sciatica.� – Dr. Alex Jimenez D.C., C.C.S.T. Insight
Low Back Pain
The purpose of the article is to understand how heel spurs can be associated with sciatica and other symptoms. Sciatica is a collection of symptoms characterized by pain, tingling sensation, and numbness. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Foot Orthotics
Low back pain and sciatica are common health issues which affect many individuals worldwide. However, did you know that chronic pain may be due to foot problems? Health issues originating in the foot may ultimately cause imbalances in the spine, such as poor posture, which can cause the well-known symptoms of low back pain and sciatica. Custom foot orthotics, individually designed with 3-arch support can help promote overall health and wellness by supporting and promoting good posture and correcting foot problems. Custom foot orthotics can ultimately help improve low back pain and sciatica. �
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force. �
At least 80% of the U.S. population will experience back pain at some point in their life, which accounts for more than 3 million reported cases of lower back pain each year. Lower back pain is also one of the biggest reasons why people miss work.
There is a solution that doesn�t include trips to the doctor, insurance agency, or prescription medication.
Understand Low Back Pain
The symptoms of low back pain can be different for everyone, ranging from dull aches to sharp /stabbing pain.
Low back pain can inhibit our ability to stand up straight, move around, lift everyday items, and do our household chores e.g. laundry and garbage.
When the pain comes quick such as, after lifting something heavy or from an injury, it is considered acute.
If the pain lasts for more than three months, it is considered chronic.
Common Causes
Heavy lifting, exercise or sudden jerking movements and injury can cause acute pain.
Injury can also lead to more chronic issues like sciatica
Those of us with desk jobs are at risk for chronic low back pain.
When carrying a bag, be careful
Purses, backpacks, and briefcases carried over the shoulder put a greater risk of developing chronic back pain because it is the lower back that takes all the weight.
Instead, get a rolling bag/case or a backpack that distributes the weight evenly over the body, across both shoulders.
Other causes of lower back pain can be hormones, weight, lifestyle, and environmental factors.
The Solution to Low Back Pain
Many chiropractors encourage the use of custom orthotics to help treat a variety of problems, ranging from joint pain, foot discomfort, and posture issues.
Custom orthotics are insoles that are slipped into shoes and made especially for your body.
Wearing custom orthotics provides nearly immediate relief from lower back pain, and also helps prevent it from returning.
Custom orthotics are created by scanning and assessing your feet in less than five minutes.
By simply standing barefoot on a kiosk inside your chiropractor�s office, a one-of-a-kind solution is created.
No X-rays, MRI�s, or further testing is required.
The foot scan assesses the three arches in both of your feet, as well as how you distribute your weight on the foundation of your body.
Although many people try to treat their low back pain on their own first, one of the fastest and best ways to treat it is through custom orthotics, which actually optimize the performance of your entire body, not just your feet and lower back.
Over-the-counter orthotics do not provide proper support and can even cause more damage to the body.
Chronic lower back pain is not a normal thing that has to do with age or lifestyle.
If you are experiencing lower back pain, call a chiropractor and ask about how custom orthotics can help you.
Low Back Pain? Fix it with *FOOT ORTHOTICS* | El Paso, Tx
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
After a quick scan, your feet will be assessed and your custom orthotics will be designed and made especially for you.
El Paso Back Clinic Foot Orthotic Kiosk
The Kiosk helps guide patients in selecting the best custom-made orthotics for their condition and lifestyle. It’s�
Fast:�Push the Start button and the scanner begins.
Easy to use:�User-friendly easy touch screen.
Engaging:�Videos explain the importance of healthy feet and the benefits of custom-made orthotics.
Cloud-based:�Results can be securely accessed from anywhere.
Comprehensive:�Easily retrieve previous scans to compare them to new scans and see the difference.
The Foot Levelers Kiosk saves time so you can spend more time living your life.
Orthotics
When there are problems with the feet, it can cause problems through the legs and all the way to the spine. This can cause the ankle to pronate, meaning it rolls inward. This alters the way the�bones of the foot line up which extends through the tibia, or shin bone. Ankle pain�and injury are not issues reserved solely for athletes. In the United States, more than 25,000 people deal with�ankle sprains�or pain every day. Studies show that somewhere around 40 percent of ankle sprains are not treated correctly or are misdiagnosed, which leads to disability or chronic ankle pain.
Ankle Manipulation
The typical treatment for pain, such as with a sprain, is R.I.C.E., which is rest, ice, compression and elevation. A somewhat newer treatment approach replaces the R with an M, meaning that instead of rest, movement is required instead. However, it is important that the movement is done safely and carefully. Certain types of�ankle injuries can be exacerbated by movement so it should be approached with care. Chiropractic can help reduce pain without prescription medication and the associated side effects. This alone is often a great draw for many patients. However, there are other benefits that chiropractic can provide for ankle pain.
31 million Americans experience low back pain at any given time. This condition affects many, but finding the exact cause can be a challenge. Chiropractors are spinal specialists that are trained to not only alleviate pain but also find and help correct the cause of the problem. A�chiropractor�is the ideal�medical professional to consult with for any unexplained pain in the musculoskeletal system. They are highly qualified professionals that their specialty is treating conditions like lower back pain and they are very affordable.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine