Glutamate is the main excitatory neurotransmitter in the central nervous system, or CNS, of mammals and it primarily interacts with both metabotropic and ionotropic receptors to activate and regulate postsynaptic responses. Both AMPA and NMDA receptors are fundamental mediators of synaptic plasticity, the ability of synapses to strengthen or weaken, where dysregulation of those receptors leads to neurodegeneration in a variety of disorders, including Alzheimer’s disease. �
The main difference between AMPA and NMDA receptors is that sodium and potassium increases in AMPA receptors where calcium increases along with sodium and potassium influx in NMDA receptors. Moreover, AMPA receptors do not have a magnesium ion block while NMDA receptors do have a calcium ion block. AMPA and NMDA are two types of ionotropic, glutamate receptors. They are non-selective, ligand-gated ion channels, which mainly enable the passage of sodium and potassium ions. Furthermore, glutamate is a neurotransmitter which creates excitatory postsynaptic signals in the CNS. �
�
What are AMPA Receptors?
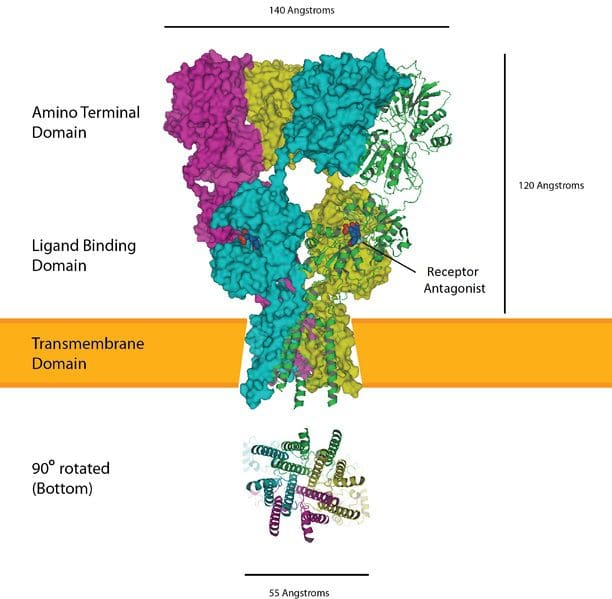
AMPA, also known as ?-amino-3-hydroxy-5-methyl-4-isoxazole-propionate, receptors are glutamate receptors which are in charge of maintaining the rapid, synaptic transmission in the central nervous system. AMPA receptors have four subunits, GluA1-4. Moreover, the GluA2 subunit is not permeable to calcium ions because it contains arginine from the TMII region. �
Furthermore, AMPA receptors are involved in the transmission of the majority of the rapid, excitatory synaptic signals. The increase of the post-synaptic response depends on the amount of receptors in the post-synaptic surface. The type of agonist which activates the AMPA receptors is ?-amino-3-hydroxy-5-methyl-4-isoxazole propionic acid. The activation of the AMPA receptors leads to the non-selective transportation of cations, such as sodium and potassium ions, into the cell. This generates an action potential in the postsynaptic membrane. Figure 1 below demonstrates a diagram of AMPA receptors. �
What are NMDA Receptors?
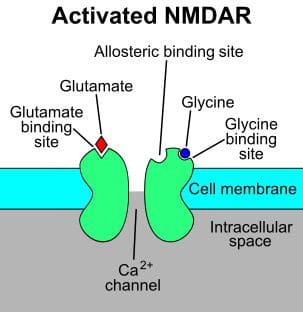
NMDA, also known as N-methyl-d-aspartate, receptors are glutamate receptors which are found in the postsynaptic membrane. The NMDA receptors are made up of two varieties of subunits: GluN1 and GluN2. The GluN1 subunit is fundamental for the role of the receptor. This subunit can associate with one of the four types of GluN2 subunits, GluN2A-D. �
Furthermore, the main utilization of the NMDA receptors is to maintain the synaptic response. In the resting membrane potential, these receptors are inactive due to the creation of a magnesium block. The agonist of the NMDA receptor is N-methyl-d-aspartic acid. L-glutamate, including glycine, can connect to the receptor to activate it. Upon stimulation, NMDA receptors activate the calcium influx along with the potassium and sodium influx. Figure 2 demonstrates NMDA receptors. �
Similarities Between AMPA and NMDA Receptors
AMPA, NMDA, and kainate receptors are the three main types of glutamate receptors.
These are ligand-gated ion channels which activate and regulate sodium and potassium ions.
These are known due to the type of agonist which activates the receptor.
Moreover, the activation of these receptors produces excitatory postsynaptic responses or ESPSs.
Furthermore, several protein subunits connect together to form these receptors.
Difference Between AMPA and NMDA Receptors
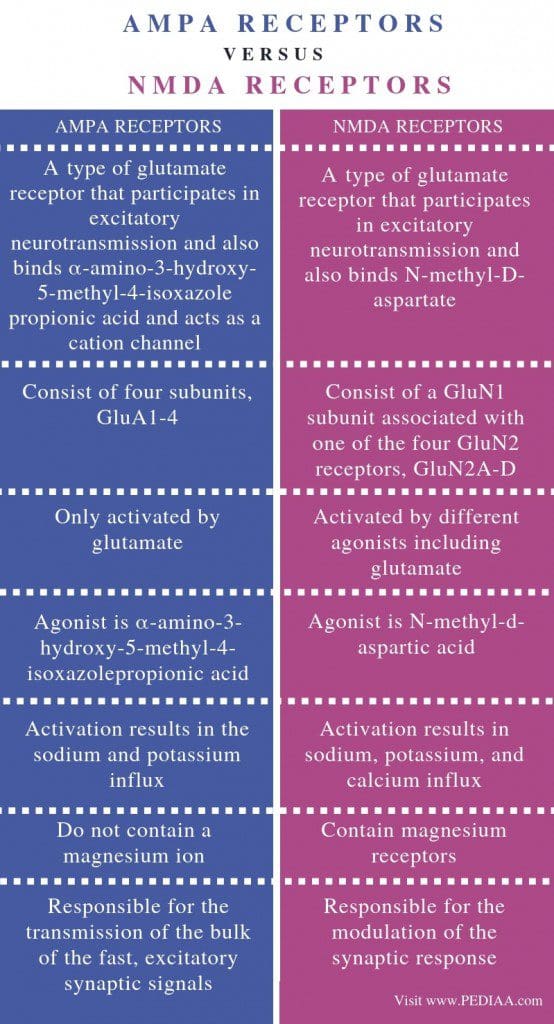
AMPA receptors are best known as a type of glutamate receptor which activates in excitatory neurotransmission and connects ?-amino-3-hydroxy-5-methyl-4-isoxazole propionic acid which additionally works as a cation channel. Where the NMDA receptors are best known as a type of glutamate receptor which helps in excitatory neurotransmission and also connects N-methyl-D-aspartate. This is the most fundamental difference between AMPA and NMDA receptors. �
AMPA receptors have four subunits, GluA1-4 while NMDA receptors have a GluN1 subunit associated with one of the four GluN2 receptors, GluN2A-D. Activation can also be a difference between AMPA and NMDA receptors. AMPA receptors are only activated by glutamate while NMDA receptors are activated by different agonists. The agonist for AMPA receptors is ?-amino-3-hydroxy-5-methyl-4-isoxazole propionic acid where the agonist for NMDA receptors is N-methyl-d-aspartic acid. �
Ion influx is a fundamental difference between AMPA and NMDA receptors. Activation of AMPA receptors results in the sodium and potassium influx while the activation of NMDA receptors leads to an increase in potassium, sodium, and calcium. Another distinction between AMPA and NMDA receptors is that AMPA receptors do not contain a calcium ion where NMDA receptors contain magnesium receptors. Also, AMPA receptors are responsible for the transmission of the majority of the rapid, excitatory synaptic signals while NMDA receptors are responsible for the modulation of the synaptic response. �
AMPA receptors are glutamate receptors which lead to the influx of sodium and potassium ions. NMDA receptors are another type of glutamate receptors which result in the influx of calcium ions with potassium and sodium ions. The main difference between AMPA and NMDA receptors is the type of ion influx associated with their activation and regulation. �
Several varieties of ionotropic glutamate receptors have been demonstrated in the following article. Three of these main excitatory neurotransmitter in the central nervous system, or CNS, are ligand-gated ion channels best known as AMPA receptors, NMDA receptors, and kainate receptors. These ionotropic glutamate receptors are best referred to after the agonists which activate and regulate them: AMPA or ?-amino-3-hydroxy-5-methyl-4-isoxazole-propionate, NMDA or N-methyl-d-aspartate, and kainic acid. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
The purpose of the article above is to demonstrate the difference between AMPA and NMDA receptors for brain health. Neurological diseases are associated with the brain, the spine, and the nerves. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force. �
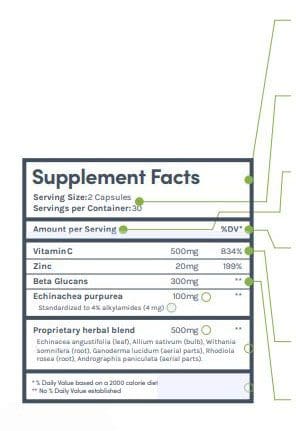
Supplemental Facts title indicates that the product is marketed for sale in the USA and is FDA standard.
Serving size, and the number of servings per container will be included to help you compare between products.
Make sure the serving sizes match when comparing supplements to get an accurate comparison.
Vitaminsand minerals always show the dose in weight and % percentage daily value to help you understand your dietary requirements.
Supplements often will have doses that exceed the recommended daily value.
Dietary supplement ingredients that are not vitamins or minerals will not have the % percentage daily value because they are not essential ingredients in the diet.
Dietary supplements are regulated by the FDA, and all labels must follow a consistent format to make it easier for consumers to understand. Understanding dietary supplement labels well require some attention to the following points when you�re evaluating supplements.
Herbs sometimes have additional information listed in the supplement panel. You might see ratio numbers (example 4:1) that show how much raw material of the herb (fresh or dried herb) is in the supplement version.
Herbs might have a standardization amount that shows how much of an active ingredient is present. The dose of the active ingredient is often listed, but sometimes it is not.
Proprietary blends are common. Only the total amount of the blend in a serving needs to be listed, which means that you don�t get all of the information about every ingredient.
Proprietary blend ingredients are listed in order from most to least. Similar to how food ingredients are listed on prepared foods nutrition facts panels.�
The daily value percent is established against a 2000 calorie diet. This is the standard calorie amount, however, it�s always important to determine your calorie requirements that you need for your health goals.
How To Identify Organic Foods
In the United States, a food or product that is labeled as organic is required to be certified by the�U.S. Department of Agriculture (USDA). The USDA has a certification program for natural growers and it has a set of very stringent standards that the product or food must meet.
There are some exemptions. For instance, a producer who does not sell more than $5,000 annually just in organic foods is not required to get the certification although they do have to adhere to the USDA�s stringent requirements for organic foods.
When a food carries the USDA Organic label, it means that it meets the requirements. While natural producers are not required to put the label on their products, many do.
The labeling varies, depending on the type of food. Single-ingredient foods like eggs, vegetables, and fruits�are considered to be 100 percent natural and are allowed to carry the USDA seal.
Foods that contain two or more ingredients, like breakfast cereal, are still allowed to use the USDA seal, but also must include the following information:
Organic � The product must be 95 percent organic or greater in order to be able to use this term
100 percent organic � The product must be completely organic or all of its ingredients must be natural
Made with organic ingredients � The product contains no less than 70 percent natural ingredients
If the product has less than 70 percent natural ingredients, they are not allowed to use the word �organic� anywhere on their product labels.
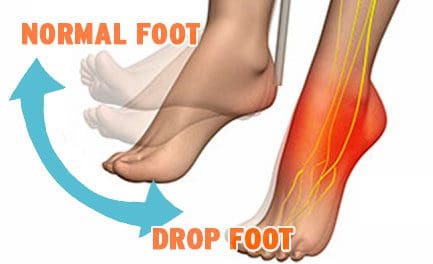
Drop Foot
Drop Foot is a symptom associated with an underlying neurological, muscular or anatomical problem that is often treated with a combination of non-invasive techniques and procedures.
Overview
Drop foot/foot drop is a general term that means lifting the forefoot (front part of the foot) is difficult to do.
Drop foot is not a diagnosis but a symptom associated with an underlying condition such as:
Neurological
Muscular
Anatomical problem
Nerve or muscle injury
Brain/spinal cord disorder, including
Herniated disc
Spinal Stenosis
Spondylolisthesis
Vertebral Fractures
Walking can be difficult, so the foot tends to drag on the floor.
Those suffering from drop foot sometimes raise the thigh up in an exaggerated fashion, such as when climbing stairs.
Stepping high is the most common symptom.
Symptoms of Drop Foot
High steppage gait
Foot drop may be experienced in one or both feet.
It is typically experienced in one foot if the drop foot is caused by:
Braces can provide additional support, stability, and shock absorption
Specific exercises to help the affected muscles
Physical therapy
Prevention
Prevention includes keeping your bones and tissues strong and healthy through diet and�exercise.
Avoid tobacco and excessive alcohol use creates weak bones and problems with the blood supply
Reduce the risk of injury by following safety measures on the job and beyond (i.e. wear a seatbelt).
Custom orthotics can provide additional support, stability, and shock absorption.
Kneeling for extended periods, such as on the job (certain construction functions laying tile, yard work).
Recovery
Some cases of drop foot are temporary; however, others can become permanent.
The recovery time and process depend on the cause.
Reduce *PLANTAR FASCIITIS PAIN* with Custom Foot Orthotics | El Paso, TX (2019)
Foot problems can affect the overall well-being of the human body. Many health issues which affect the foot can result in poor posture, low back pain, and sciatica. These imbalances can ultimately result in a variety of other health issues. Custom-made foot orthotics can help promote and support overall well-being by relieving foot problems.
Dr. Alex Jimenez is the non-surgical choice for foot problems and other health issues. Dr. Alex Jimenez can help promote and support overall well-being with the use of custom-made foot orthotics and other treatments approaches.
What’s Afoot
Foot Dysfunction can very easily cause a domino effect that extends all the way to the back. The feet are the foundation of the body and when there is a problem with the way they function it can cause the entire body to shift out of alignment. Overpronation and oversupination, for example, can cause a variety of injuries and conditions that affect not only the feet and ankles, but also the knees, hips, and back as well.
NCBI Resources
If you have further questions or concerns about your particular�diet, please ask us! Our Doctor of Chiropractic can help guide you toward a more healthy life, including the foods you consume. It comes down to two major areas: safety and�nutrition. That is what consumers need to understand when they are trying to make a decision on whether to purchase foods that have been conventionally farmed or foods that are natural.
Until only several decades ago, neuroscientists believed that the brain stopped creating new neural connections, meaning that your memory starts to become irreversibly worse when the human body stopped developing, which is generally in your early 20s.� Neuroscientists also understood that neurons weaken and die as we age. The loss of brain function due to neural breakdown was believed to be a normal part of aging until recent research studies demonstrated the opposite of this belief. �
Over the last several years, it has become evident to neuroscientists that you can, as a matter of fact, create new neurons and develop new neural connections starting in your early 20s and continuing well into your old age. As the older regions of the brain start to wear out, you can ultimately rewire your brain and improve your overall brain health. But, how can you improve brain health? In the following article, we will discuss 5 ways you can improve your brain health and promote your well-being. �
Eat Healthy Foods
You are what you eat, or at least, your brain can be affected by the types of foods you eat. Eating junk food can have a tremendous impact on your brain health because trans fats and saturated fats, frequently found in processed foods, can negatively alter the brain’s synapses. Synapses connect the brains neurons and are fundamental for memory and learning. But, a balanced diet rich in omega-3 fatty acids, which are found in salmon, walnuts, and kiwi, can provide the synapses with a boost which can ultimately help fight against neurological diseases, including depression, dementia, and Alzheimer’s disease. �
Participate in Exercise
Participating in exercise and physical activity can also help boost your memory and help you think more clearly, reducing the risk of developing neurological diseases. Because exercise and some physical activity is a moderate stressor to the body, which uses energy needed by the brain, it triggers the release of substances, known as growth factors, which make the brain’s neurons fitter and stronger. Participating in 30 minutes of exercise or physical activity every other day can help improve brain health, and don’t forget to stretch. Stretching can help reduce anxiety, which can affect overall brain health. �
Mental Stimulation
Make sure to also give your brain a workout with brainteasers, crossword puzzles, and memory games. Research studies have demonstrated that using these tools to remain mentally active can help reduce the risks of developing dementia and other neurological diseases by building and maintaining a reserve of stimulation on your brain. Mental stimulation can help boost the regions of your brain which control and regulate learning and attention, which are hard-wired into the brain. �
Memory Training
Maintaining information stored in your memory banks and retaining that memory with age may also be a simple matter of mind control. By way of instance, confidence in your cognitive abilities might actually influence how well your memory works, especially for the elderly. Because many older adults tend to blame memory lapses on age, regardless of whether or not that is the reason, they may often be keeping themselves out of even trying to remember. Prediction can also enhance memory. If you have an idea of the information you have to remember afterward, you’re more likely to remember it. �
Get Enough Sleep
Getting enough sleep can help improve your overall well-being, especially your brain health. Sleep gives your brain an opportunity to match the memories of the day and combine them for long-term storage. One research study demonstrated that the brain can perform its reviewing much quicker when you are asleep than when you’re wide awake. A 90-minute mid-afternoon nap can help store long-term memories, such as events or skills you are attempting to master. Research studies have demonstrated that developing Alzheimer’s disease and other types of dementia are generally due to genetics. �
One research study, presented in July at the Alzheimer’s Association’s International Conference on Alzheimer’s Disease, demonstrated a connection between moms who develop Alzheimer’s disease and the chances that their children will develop the health issue in older age. Another research study suggests that a pattern of proteins is a risk factor for neurological disease. But, no one can predict who will develop dementia. While neuroscientists discover better treatments for these health issues, following ways to improve brain health is probably the best you can do to promote your overall well-being. �
Many neuroscientists once believed that the brain stopped developing new neurons and new neural connections as soon as you reached adulthood. However, recent research studies have demonstrated that we can create new neurons and new neural connection which can continue well into your old age.�In the following article, we discuss 5 ways you can improve your brain health and promote your well-being. From eating healthy foods to getting enough sleep, maintaining your overall well-being can help improve your brain health. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
The purpose of the article above is to demonstrate 5 ways which can ultimately help improve your overall brain health. Neurological diseases are associated with the brain, the spine, and the nerves. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force. �
Supplements can become overwhelming with everything that’s out there. This will touch on key categories of supplements and the best way on how to use them.
Supplements are divided into categories:
Nutrients
(Nutraceuticals or Orthomolecular Medicine)
Botanicals
(Herbal Medicine or Phytotherapy)
Hormones
Hormone Replacement Therapy or Restorative Medicine
Each category is meant to support underlying excesses or deficiencies, with the ultimate goal of bringing the body back into balance.
Where it becomes complicated is understanding the different uses and dosing of specific:
Extracts
Chelates (a chemical compound that dissolves more easily and is easily absorbed compared to other types of molecules and compounds)
Prepared Compounds
Hormones
Integrative medicine and hormone therapy usually involve synthetic versions of plant extracts, that mimick the chemical structure of endogenous hormones.
What are Hormones?
Hormones are chemical messengers that are produced by the endocrine glands.
These messengers have an effect on most tissues and major bodily functions.
Establishing and resolving the causes of hormonal imbalance is one of the core therapeutic systems not only in integrative medicine but in conventional medicine.
How do Hormones Work?
Hormones flow through the body�s circulation in abundance. In order for hormones to perform a function, the cells being used require specific receptors.
When hormones bind to these receptors, it causes a biological response inside the cell, which is why a single hormone can have such an effect.
The entire endocrine system is based on positive and negative feedback loops. This informs the endocrine glands to produce more or fewer hormones.
Balance of endogenous hormone production is maintained through diet and lifestyle. However,�when this unique balance is disrupted is when disease can occur.
Despite their broad and potent effect on the body’s systems, hormones therapy must be done with caution and skill.
There can be long-term negative side effects with hormone therapy and should be limited to highly-trained practitioners.
Examples of Hormone Ingredients
Exogenous hormones are available in different forms.
Examples include:
Pregnenolone – this is the mother of steroidogenic hormones
Dehydroepiandrosterone (DHEA) – elevates estrogen and testosterone
Vitamin D – regulates bone density, and balances parathyroid hormone secretion
There is evidence that shows beneficial therapeutic uses for exogenous hormones.
Similar to botanical medicine, hormone therapy should be used exclusively and with caution by certified clinicians.
Fasting Mimicking Diet Basics
Some people today might eat a slightly higher amount of calories the first day as they ease into the fasting-mimicking diet. They might then decrease their total caloric intake. You also want to make sure you eat smaller amounts of foods which are easy to digest.
ProLon��offers a pre-packaged box which contains all five days� worth of meals for you to do the diet. The meals are all plant-based. One day, by way of instance, offers tea and a nut bar for breakfast, a small portion of vegetable soup and a few kale crackers for lunch, several olives in the afternoon, and finally another small portion of vegetable soup for dinner.
You can also do the fasting-mimicking diet without the need for a pre-packaged box-like ProLon�. Simply follow the right proportions and plan out how you will space them out every day. Macros for the fast mimicking diet are 34 percent carbohydrates, 10 percent protein, and 56 percent fat for the very first day and 47 percent carbohydrates, 9 percent protein, and 44 percent fat to the rest days.
A cup of black tea and coffee every day are generally allowed. Just make sure they don�t contain any added sugars or oils. Remember that people with health issues should consult a healthcare professional prior to doing the fast mimicking diet in your own home.
Foods
Dr. Anthony Gusting followed a four-day ketogenic fasting-mimicking diet. Every day, he consumed different amounts of bone broth, coconut milk, coconut oil, BCAAs, and exogenous ketones. Avocados and grass-fed butter can also be included in the fast mimicking diet. This is a great way to combine the ketogenic diet with the fasting-mimicking diet to benefit from the two regimens.
Supplements
Taking nutritional supplements can also make the fasting-mimicking diet easier by providing enough nutrition. These may include:
Electrolytes like magnesium and salt to replenish any lost during water loss
Grass-fed liver tablets to provide micronutrient support
Branch chain amino acids, or BCAAs, to help prevent loss of lean tissue
Greens powder to provide micronutrients
Algal oil or cod liver oil for omega-3s
You may also take exogenous ketones to achieve ketosis through the keto diet. The fast mimicking diet can also help you achieve ketosis before following a ketogenic diet. Below, we will discuss how the fast mimicking diet promotes ketosis.
Ketosis And The Fast Mimicking Diet
The fast mimicking diet is an excellent way to prepare you for the ketogenic diet. This is because it allows you to get into ketosis. Additionally, eating keto foods makes it possible to remain in ketosis throughout the regimen. To follow a ketogenic fasting-mimicking diet you must maintain your macros over the suitable range of 5 to 10 percent of carbohydrates, 20 to 25percent of proteins, and 70 to 80 percent of fats. If you�re unsure about whether you�re properly maintaining your macros, always choose something with more fat.
If you or a loved one need additional dietary guidance, give us a call. Our Doctor of Chiropractic is here to help!
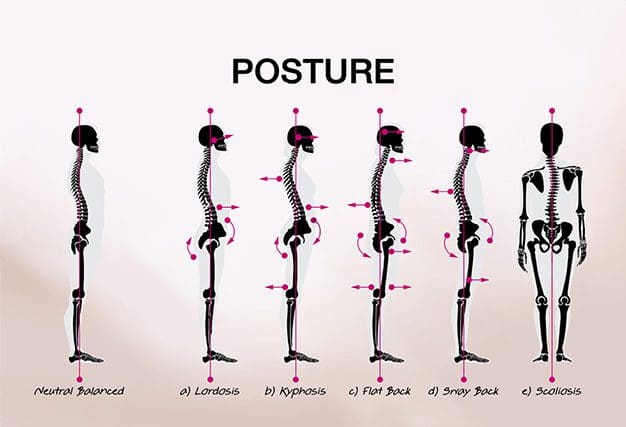
*CORRECT BAD POSTURE* with Custom Foot Orthotics | El Paso, TX (2019)
Posture is the way in which we hold our bodies while standing, sitting, or performing tasks such as lifting, bending, pulling, or reaching. However, when a person practices bad posture, it can cause a variety of health issues. According to research studies, signs and symptoms associated with a bad posture are the 3rd most common reason for doctor office visits in the United States.
The spine helps support the weight of the head and stabilizes the human body when standing upright. However, bad posture can strain the spine, causing a variety of health issues. Custom orthotics can help support good posture and promote pain relief. Dr. Alex Jimenez can help patients improve their overall health and wellness through custom orthotics. Patients recommend Dr. Alex Jimenez as the non-surgical choice for posture.
Posture
Poor posture takes a serious toll on health. Here are a few negative results:
Muscle soreness
Subluxations
Blood vessel constriction
Nerve constriction
As time passes, body/health problems also arise, which result in pain, restricted motion, and make the body more susceptible to injury and disease. Posture can even affect your emotional well-being, including self-confidence!
Treatment
Chiropractic can help you maintain proper posture with alignment adjustments, and custom orthotics can benefit the treatment making it last longer.
The American Chiropractic Association maintains proper posture involves sitting, standing, and lying down properly. Here’s an excerpt:
Sitting properly
Keep your feet on the floor or footrest, for feet to be stabilized.
Ankles should be in front of your knees.
Keep a small space between the back of the knees and the front of the seat.
Your knees should be at or below the level of your hips.
Standing properly
Keep your weight on the balls of your feet.
Keep your knees slightly bent.
Keep your feet in line with your shoulders.
Arms hang naturally down the sides of the body.
Sleeping properly
Find the mattress that is right for you.
A firm mattress is generally recommended but sometimes people do better with a
Softer mattresses to reduce back pain.
Remember comfort is important.
Sleep with a pillow.
Special pillows are available to help with posture problems that come from a poor sleeping position.
The feet are complex structures which function to provide protection and support to the body in relation to the spine and head posture. The feet are essential towards balancing the body�s entire weight, allowing it to walk, run, stand, and, jump. Foot complications may cause severe issues throughout the spine, hips, knees, and ankles if left untreated. Chiropractic care can be effective for treating injuries or conditions such as plantar fasciitis, Achilles tendonitis, and ankle sprains. Foot health is essential towards establishing the body�s proper support and balance, together with a proper spinal posture. In the presence of foot complications, chiropractic treatment can be used to achieve long-lasting health.
NCBI Resources
It seems our moms were right; we are what we eat. Unfortunately, in today�s marketplace, there are many valid worries about the foods we consume. Antibiotics, pesticides, and foods tainted with dangerous diseases are a top concern for many Americans. In addition, processed and genetically modified foods�and artificial ingredients contribute to a number of health issues from�obesity�to�cancer.
For many years, most neuroscientists believed we were born with all the neurons we were ever going to carry in our brains. As children, we may develop new neurons to help create the pathways, known as neural circuits, which function as information highways between different regions of the brain. However, scientists believed that after a neural circuit was created, developing any new neurons could interrupt the flow of information and disable the brain’s communication system. �
Introduction to Brain Basics
In 1962, scientist Joseph Altman questioned this belief when he saw evidence of neurogenesis, or the birth of neurons, in a region of an adult rat’s brain known as the hippocampus. He then reported that newborn neurons migrated from their birthplace in the hippocampus to other regions of the brain. In 1979, another scientist, Michael Kaplan, proved Altman’s findings in the rat brain and in 1983, Kaplan found neural precursor cells in the forebrain of an adult monkey. �
In the early 1980s, a scientist attempting to explain how birds learn how to sing suggested that neuroscientists should once again analyze neurogenesis in the adult brain and start to determine how it can make sense. In several experiments, Fernando Nottebohm and his team revealed that the numbers of neurons in the forebrains of male canaries tremendously increased during the mating season. This was the same time in which the birds had to learn new songs to attract females. �
However, why did these bird’s brains create new neurons during such a vital time in learning? Nottebohm believed it was because new neurons helped keep new song patterns inside the neural tissues of the forebrain, or the region of the brain which regulates complex behaviors. These new neurons made learning possible. If birds developed new neurons to help them remember and learn new song patterns, Nottebohm believed that the brains of mammals may also be able to do the same. �
Elizabeth Gould discovered evidence of newborn neurons in a different region of the brain in monkeys. Fred Gage and Peter Eriksson also demonstrated that the adult human brain developed new neurons in a similar region. For several neuroscientists, neurogenesis in the adult brain is still an unproven theory. However, other neuroscientists believe that the evidence provides interesting possibilities associated with the role of adult-generated neurons in memory and learning. �
Architecture of the Neuron
The central nervous system, which includes the brain and the spinal cord, consists of two primary types of cells: the neurons and the glia. Glia outnumber neurons in several regions of the brain, however, neurons are the key structures in the brain. Neurons are information messengers. They utilize electrical impulses and chemical signals to transfer information between different regions of the brain and between the brain and the rest of the nervous system. Everything we think, feel, and do would be impossible without the utilization of neurons and the glial cells, known as astrocytes and oligodendrocytes. �
Neurons have three primary parts including a cell body and two extensions known as an axon and a dendrite. Within the cell body is a nucleus, which regulates the cell’s activities and holds the cell’s genetic material. The axon is characterized by a very long tail and it transfers messages from the cell. Dendrites are characterized similar to that of the branches of a tree and they receive messages from the cell. Neurons communicate with one another by sending chemicals, known as neurotransmitters, across a very small region, known as a synapse, found between the axons and the dendrites of adjacent neurons. � There are three types of neurons: �
Sensory neurons: Transfer information from the sense organs, such as the eyes and ears, to the brain.
Motor neurons: Manage voluntary muscle activity and transfer messages from nerve cells in the brain to muscles.
All other neurons are known as interneurons.
Scientists believe that neurons are the most varied type of cell in the human body. Within these three types of neurons are hundreds of different types of neurons, each with specific message-carrying abilities. The way these neurons communicate with one another by establishing connections is ultimately what makes people unique in how we think, feel, and act. �
Birth of the Neuron
The range to which new neurons are created in the brain has been a controversial topic among neuroscientists for many years. Meanwhile, although nearly all neurons are currently present in our brains by the time we’re born, there’s recent evidence to support that neurogenesis, or the scientific word utilized to describe the birth of neurons, is a lifelong procedure. Neurons are born in regions of the brain which are full of neural precursor cells, known as neural stem cells. These cells have the potential to develop all, if not all, of the different types of neurons and glia found in the brain. Neuroscientists have discovered how neural precursor cells function in the laboratory. Although this may not be exactly how these cells behave when they are in the brain, it gives us data about how they may function when they are in the brain’s environment. �
The science of stem cells is still very recent and could ultimately change with further discoveries, however, researchers have discovered enough evidence to support as well as to be able to demonstrate how neural stem cells create the other cells of the brain. Neuroscientists refer to this as a stem cell’s lineage and it is similar in principle to the concept of a family tree. �
Neural stem cells increase by dividing into two and creating two new stem cells, two early progenitor cells, or one of each. When a stem cell divides to create another stem cell, it is believed to self-renew. This new cell has the potential to make more stem cells. When a stem cell divides to create an early progenitor cell, it is said to differentiate. Differentiation is when a new cell is more technical in structure and function. An early progenitor cell doesn’t have the potential of a stem cell to create several different types of cells. It can only make cells within their distinct lineage. Early progenitor cells may self-renew or go in either of two ways. One type will develop astrocytes. The other type will develop neurons or oligodendrocytes. �
Migration of the Neuron
Once a neuron is born, it must go to the region of the brain where it will function. But, how does a neuron understand where to go? And, what helps it get there? Neuroscientists have determined that neurons utilize two different methods to travel: �
Several neurons migrate by following the long fibers of cells known as radial glia. These fibers extend from the inner layers to the outer layers of the brain. Neurons glide along the fibers until they reach their destination.
Neurons also travel by using chemical signals. Scientists have found special molecules on the surface of neurons, known as adhesion molecules, which bind with similar molecules on nearby glial cells or nerve axons. These chemical signals will also ultimately help guide the neuron to its final destination in the brain.
Not all neurons are successful in their journey. Scientists believe that only one-third of these neurons will reach their destination. Some cells die during the process of neuronal growth. Some neurons may also survive, but end up where they don’t belong. Mutations in the genes which regulate migration create regions of misplaced or abnormal neurons which can cause disorders, such as epilepsy. Scientists believe that schizophrenia is partially caused by misguided neurons. �
Differentiation of the Neuron
When a neuron reaches its destination, then it must begin to perform its initial function. This final measure of differentiation is one of the most misunderstood sections of neurogenesis. Neurons are in charge of the transfer and uptake of neurotransmitters, or chemicals which deliver information between cells. Depending on its location, a neuron may perform the role of a sensory neuron, a motor neuron, or an interneuron, sending and receiving specific neurotransmitters. �
In the developing brain, a neuron depends on molecular signals from other cells, including astrocytes, to determine its form and location, the type of transmitter it creates, and to which other neurons it can connect. These newborn cells establish neural circuits, or data pathways that connect from neuron to neuron, which is determined during adulthood. However, in the mature brain, neural circuits are already developed and neurons must find a way to fit in. As a new neuron settles in, it starts to look like enclosing cells. It then develops an axon and dendrites and begins to communicate with its neighbors. �
Death of the Neuron
Although neurons are the longest living cells within the human body, large numbers of them often die during migration and differentiation. The lives of some neurons can sometimes take unexpected turns. Several health issues associated with the brain, the spinal cord, and the nerves are the consequence of the unnatural deaths of neurons and supporting cells. �
In Parkinson’s disease, neurons which create the neurotransmitter dopamine die off at the basal ganglia, a region of the brain which controls body movements. This causes difficulty initiating movement.
In Huntington’s disease, a genetic mutation causes the over-production of a neurotransmitter known as glutamate, which kills neurons in the basal ganglia. As a result, individuals twist and writhe uncontrollably.
In Alzheimer’s disease, unusual proteins build up in and around neurons in the neocortex and hippocampus, sections of the brain which manage memory. When these neurons die, people lose their ability to remember and perform regular tasks. Physical damage to the brain and other regions of the central nervous system can also kill nerves.
Injury to the brain, or damage caused by a stroke, can kill nerves completely or gradually starve them of the oxygen and nutrients they need to survive. Spinal cord injury may disrupt communications between the brain and nerves when these lose their link to axons located under the site of injury. These neurons survive but they may lose their ability to communicate. �
Conclusion to Brain Basics
Scientists hope that by understanding more about the life and death of neurons, they could develop treatment options and perhaps even cures for brain diseases and disorders which ultimately affect the lives of many people in the United States. �
The most current research studies suggest that neural stem cells can generate many, if not all, of the several types of neurons located in the brain and the nervous system. Determining how to control these stem cells from the laboratory into specific types of neurons can develop a new supply of brain cells to replace the ones which have been damaged or died. �
Treatment approaches may also be created to take advantage of growth factors and other signaling mechanisms within the brain which tells precursor cells to make new neurons. This will make it easy to fix, reshape, and renew the brain from within. �
A neuron is characterized as a nerve cell which is considered to be the basic building block of the central nervous system. Neurons are similar to other cells in the human body, however, neurons are responsible for transferring and transmitting information throughout the human body. As previously mentioned above, there are also several different types of neurons which are in charge of a variety of functions. Understanding the life and death of neurons is essential to help understand the mechanisms of neurological diseases and hopefully their treatment and cure.� – Dr. Alex Jimenez D.C., C.C.S.T. Insight
The purpose of the article is to understand the life and death of neurons and how these relate with neurological diseases. Neurological diseases are associated with the brain, the spine, and the nerves. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force. �
Supplements can become overwhelming with everything that’s out there. This will touch on key categories of supplements and the best way on how to use them.
Supplements are divided into categories:
Nutrients
(Nutraceuticals or Orthomolecular Medicine)
Botanicals
(Herbal Medicine or Phytotherapy)
Hormones
Hormone Replacement Therapy or Restorative Medicine
Each category is meant to support underlying excesses or deficiencies, with the ultimate goal of bringing the body back into balance.
Where it becomes complicated is understanding the different uses and dosing of specific:
Extracts
Chelates (a chemical compound that dissolves more easily and is easily absorbed compared to other types of molecules and compounds)
Prepared Compounds
Botanicals
(Herbal Medicine or Phytotherapy)
Botanicals?
Records of humanity using botanical extracts therapeutically date back to the beginning of first recorded history.
Today, botanical medicine serves as an inspiration for pharmaceutical inventions and continues�via modern research.
Botanical medicine is essential in integrative medicine and normally elicits fewer and less significant adverse side effects than pharmaceutical interventions.
Growing research shows that when used correctly, botanical extracts are more effective than pharmaceutical equivalents, and more cost-effective as well.
Botanical Work?
Given their capacity to interact with virtually every system and tissue in the body, there are thousands of therapeutic uses.
There is a great deal of literature on traditional botanical medicine, however, there is a very little amount of modern research relative to modern medicine.
As a result, it becomes somewhat challenging to compare botanicals with pharmaceuticals regarding
clinical outcomes.
Botanical Ingredients
Botanical medicine provides very helpful effective therapeutics and allows everyone, from professional practitioners to common laypeople apply these treatments.
Common examples:
Garlic (Allium sativum) – immune function, cardiovascular function
Bottom line, diets are temporary. There are some serious consequences that can come from dieting, especially fad or crash diets. The effects of these types of diets can also seriously impact your chiropractic care, hindering your progress.
Also, because diets are temporary, once you return to your regular eating habits the weight usually comes back.
A lifestyle change is a far better choice. It involves making smart, healthy eating choices � choices that you maintain for the rest of your life. This also impacts your chiropractic care by strengthening your body and keeping it healthy so that it is in an optimal state for healing and responds well to treatment.
Diet Type
There are all sorts of diets out there. Some are blatantly unhealthy but others are sneaky. They come with claims of being healthy, of being created or endorsed by doctors, or include tons of vitamin supplements but very limited food intake. It is important to be able to spot these destructive fad diets so you don�t get suckered into their hype.
Some of the most common�types of fad diets include high protein, low or no-carb, liquid, cabbage, grapefruit, broth or juice, and food combining. Some of these can cause serious health problems including vital organ damage. Others can cause vitamin deficiencies and dehydration. None of them can (or should) be maintained over a long period of time, much less the rest of your life.
Healthy Eating/Lifestyle
When you make the life-changing commitment to adopt a healthy eating lifestyle you open yourself up to a world of better health, more energy, and better focus. Your body will heal faster and you will feel better.
A diet of fresh�fruits and vegetables, lean meats, fresh fish, and whole grains, along with lots of water should become a way of life. It is far healthier than the temporary diets that are out there and more effective too.
If you or a loved one need additional dietary guidance, give us a call. Our Doctor of Chiropractic is here to help!
Get Rid of *FOOT PRONATION PAIN* with Custom Foot Orthotics | El Paso, TX (2019)
Foot pronation is the natural movement which occurs during foot landing while walking or running. Foot pronation also occurs while standing, and in this instance, it is the amount in which the foot rolls inward toward the arch. Foot pronation is normal, however, excessive foot pronation can cause a variety of health issues, including bad posture. The following video describes the 5 red flags of excessive foot pronation, which can ultimately affect a person’s overall health and wellness. Dr. Alex Jimenez can help diagnose and treat excessive foot pronation. Patients recommend Dr. Alex Jimenez and his staff as the non-surgical choice for excessive foot pronation health issues.
What’s Afoot
The feet are complex structures which function to provide protection and support to the body in relation to the spine and head posture. The feet are essential towards balancing the body�s entire weight, allowing it to walk, run, stand, and, jump. Consequently, foot complications may cause severe issues throughout the spine, hips, knees, and ankles if left untreated. Chiropractic care can be effective for treating injuries or conditions such as plantar fasciitis, Achilles tendonitis, and ankle sprains, among others. Foot health is essential towards establishing the body�s proper support and balance, together with a proper spinal posture. In the presence of foot complications, chiropractic treatment can be used to achieve long-lasting health.
NCBI Resources
While most of us know that proper nutrition is vital in assisting us to reach our optimum health and feel our best; finding time to eat a balanced diet on a daily basis seems a formidable job in this fast-paced, affluent society. Though your life may be frantic, there are still many good tasting, healthful alternatives which can assist you to lose weight and enhance your health.
Neurological diseases are characterized as health issues associated with the brain, the spine, and the nerves which connect them. Neurological disease is considered to be one of the most prevalent health issues with a high burden to the patients, their families, and society. However, there are now estimates of the burden of neurological diseases in the United States. �
Neurological Disease Prevalence and Costs
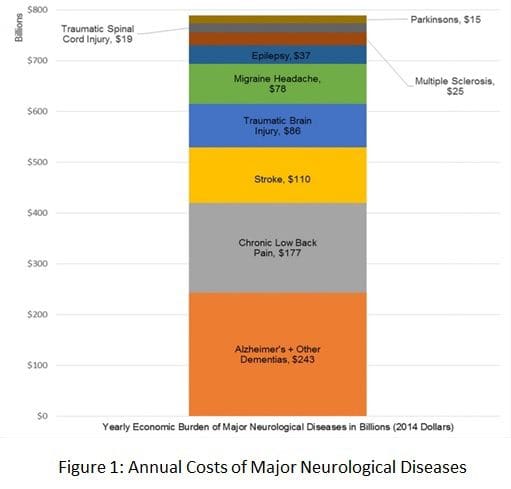
The most prevalent and costly neurological diseases, according to several recent research studies, include Alzheimer disease and other dementias, chronic low back pain, stroke, traumatic brain injury, migraine headaches, epilepsy, multiple sclerosis, spinal cord injury, and Parkinson’s disease. Many other neurological diseases were excluded due to their mixed etiologies. �
The most common neurological disorders described above cost the United States approximately $789 billion in 2014, which may increase as the elderly population increases between 2011 and 2050, according to a research study published in the Annals of Neurology. The research study demonstrates the price of the serious annual financial burden in the US and has been demonstrated as healthcare professionals have suggested budget reductions for federally-funded research studies. �
According to these demographic statistics, the American Neurological Association, or the ANA, commissioned a research study by former ANA marketing committee and public advocacy committee chair Clifton L. Gooch, MD, currently professor and chair of the Department of Neurology in the University of South Florida’s Morsani College of Medicine in Tampa. �
The research study, the Burden of Neurological Disease in the United States: A Summary Report and Call to Action, demonstrated the annual cost of the most prevalent neurological diseases, including Alzheimer’s disease and other dementias, chronic low back pain, stroke, traumatic brain injury, migraine headaches, epilepsy, multiple sclerosis, spinal cord injury, and Parkinson’s disease. Neurological disease ultimately affects an estimated 100 million people in the United States every year and, together with the costs of stroke and dementia alone, these are estimated to total over $600 billion by 2030. �
Funding for Neurology in the United States
The tremendous and sustained capital investments made in cardiovascular and cancer research studies beginning in the 1970s have considerably increased lifespan. Ironically, however, the number of older adults who have a higher chance of developing neurological diseases have increased, which has developed a growing outbreak among healthcare professionals. �
“Preliminary research studies, including those of cancer, focus considerable research study investment to the neurological diseases which are impacting the quality of life and mortality of more and more people in the United States every year,” stated Gooch, referring to the $1.8 billion in funding for cancer and neurology research approved by Congress in 2016. �
“We hope the findings of the report will serve as a wake-up call to Congress to improve much needed clinical and basic research funding necessary to discover treatments which can mitigate, and finally cure, the considerable amount of neurological diseases which have developed profound consequences in our patients as well as for the national economy.” �
“The future of funding for neurological research studies was an issue in 2012 when the ANA voted to support this particular research study,” stated ANA President Barbara G. Vickrey, MD, MPH. “With the reductions now being suggested to the NIH funding from the President of the United States, this has become of even greater concern today. As representatives of the scholars working to eradicate these health issues, we feel we must raise our collective perceptions, armed with the facts.” �
Annual Cost of Neurological Disease Overview
Researchers gathered the information from the research study through a complete review of the world literature among the most prevalent and costly neurological diseases in the United States. To be conservative, researchers focused on the prevalence and cost estimates they considered to be the most comprehensive and accurate, excluding neurological diseases, such as depression and chronic pain, which frequently have mixed etiologies beyond primary nervous system injury. �
“A complete accounting of all neurological diseases would considerably increase price tag estimates,” wrote the authors of the research study. Indirect and direct costs for the most common neurological diseases previously mentioned above, have been demonstrated in the research study and were estimated according to maintenance standards for each health issue. �
Alzheimer’s disease and other dementias accounted for $243 billion of their $789 billion total, while chronic lower back pain represented $177 billion, and stroke represented $110 billion.�As well as documenting the fiscal costs of neurological disease, Gooch and his USF colleagues ultimately recommend an action plan for reducing the burden of these health issues through infrastructure investment in neurological research and enhanced clinical management of neurological disorders. �
Many research studies have demonstrated how several of the most common neurological diseases pose a serious annual financial burden in the United States. The most prevalent and costly neurological health issues, such as Alzheimer’s disease and other dementias, chronic low back pain or sciatica, as well as stroke, among other common neurological diseases mentioned above, have been estimated to have an annual cost totalling $789 billion in 2014, according to research studies. These annual costs have also been demonstrated to considerable increase further over time.� – Dr. Alex Jimenez D.C., C.C.S.T. Insight
The purpose of the article is to demonstrate the annual cost of several of the most prevalent neurological diseases. Neurological diseases are associated with the brain, the spine, and the nerves. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force. �
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine
 �
�



 Herbs sometimes have additional information listed in the supplement panel. You might see ratio numbers (example 4:1) that show how much raw material of the herb (fresh or dried herb) is in the supplement version.
Herbs sometimes have additional information listed in the supplement panel. You might see ratio numbers (example 4:1) that show how much raw material of the herb (fresh or dried herb) is in the supplement version.