How often do you feel you have something that must be done? How often do you have difficulty concentrating before eating? Do you suffer from headaches and/or migraines? Head pain is commonly characterized by a variety of symptoms, including pain and discomfort, photophobia or light sensitivity, dizziness, lethargy, and mood changes. However, one of the most common symptoms of head pain is brain fog, which also causes its own variety of symptoms. In the following article, we will discuss brain fog associated with head pain and pressure as well as the common cause of brain fog and headache/migraine. �
�
�
Many patients will commonly visit healthcare professionals reporting mild or moderate head pain and pressure as well as a variety of other symptoms, such as brain fog, fatigue, and even vision problems, among others.� The patients frequently experience a “constant cloud” over their brain and they generally never have a clear head or mental clarity. Many patients will commonly report numerous other symptoms, including poor short-term memory, detachment from reality, sharp pain and discomfort in the head, and ringing in the ears. Many others report anxiety, caused or worsened by the symptoms. �
�
�
Brain Fog and Head Pain
The first approach towards characterizing brain fog associated with head pain is to make sure it’s not caused by a secondary headache or a headache with an identifiable cause. Several types of head pain are more severe than others, such as giant cell arteritis or inflammation of the arteries that run along the temples, raised blood pressure or hypertension,�brain hemorrhage, brain infections like encephalitis, increased pressure in the fluid of the brain or raised intracranial pressure, and brain tumors. Less severe types of head pain include�carbon monoxide poisoning, taking too many painkillers or medication-overuse headache, disorders of the joints of the jaw or temporomandibular joint disorders, dental problems, and sinus infections or sinusitis. Below, we will discuss several of the most common causes of brain fog associated with head pain.
�
Causes of Brain Fog and Head Pain
Researchers and healthcare professionals have offered their own hypotheses for why brain fog occurs with head pain, based on their own knowledge and experiences. They believe that brain fog and head pain occur due to epilepsy, overactive parathyroid glands or hyperparathyroidism, overactive thyroid gland or thyrotoxicosis, and brain circulation problems. Researchers and healthcare professionals also suggest it could be due to a vitamin B12 deficiency. Fortunately, the utilization of CT and MRI brain scans, heart tracing, EEG and blood tests, can be utilized to rule out many of these health issues.
Moreover, several health issues require specific tests and evaluations. These include tests for lupus or an inflammatory disorder, magnesium deficiency, zinc deficiency,�Lyme disease or an infection resulting from a tick bite, and postural tachycardia syndrome or an increase in heart rate on standing. Many researchers and healthcare professionals also recommend a detailed examination and investigation of a misalignment or subluxation of the neck or cervical spine. �
If all these tests and evaluations return as normal, then the next approach towards characterizing brain fog associated with head pain is to make sure it’s not caused by a primary headache or a headache without an underlying secondary cause. Primary headaches are diagnosed in 9 out of 10 cases of head pain and pressure. The most common types of primary headaches include tension-type headache,�migraine, and daily persistent headache. Diagnosis depends on the pattern of symptoms as well as examinations and investigations to rule out underlying causes. Although there are specific treatment options for several primary headaches like migraines, in many instances, treatment is frequently a matter of trial and error. �
Furthermore, despite the best efforts of researchers and healthcare professionals as well as comprehensive examinations and investigations, many people who suffer from brain fog associated with head pain and pressure are still left without any explanation for their symptoms. Researchers and healthcare professionals have a name even for this type of brain fog-related head pain known as medically unexplained symptoms or MUS. This ultimately means exactly what reads as: no one is denying that the person has the symptoms, but doctors have been unable to find a medical condition to explain them. �
Several people with MUS undoubtedly do have stress, anxiety, and even depression whether as a result of the symptoms or as a cause of the symptoms. Researchers and healthcare professionals recommend continuing to pursue psychological support if you have brain fog and head pain, as this may help to relieve a potential cause as well as helping to cope with the symptoms. Cognitive-behavioral therapy�would be ideal for this purpose, as would�mindful awareness, a technique that would arm people with a way of deflecting their mind away from their troubling symptoms, improving overall well-being. �
Brain fog can make people feel as if they’re not able to focus or concentrate accordingly and it’s commonly accompanied by head pain, fatigue and even vision problems. While brain fog is a symptom rather than a single health issue, it can be a cause or be caused by other underlying health issues. Head pain and pressure can have a variety of symptoms on its own but head pain-related brain fog has a whole different variety of symptoms. Understanding brain fog associated with head pain and pressure as well as what you can do about the symptoms can help manage brain fog symptoms and promote overall brain health and wellness. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
Neurotransmitter Assessment Form
The following Neurotransmitter Assessment Form can be filled out and presented to Dr. Alex Jimenez. Symptoms listed on this form are not intended to be utilized as a diagnosis of any type of disease, condition, or any other type of health issue. �
In honor of Governor Abbott’s proclamation, October is Chiropractic Health Month. Learn more about the proposal. �
How often do you feel you have something that must be done? How often do you have difficulty concentrating before eating? Do you suffer from headaches and/or migraines? Head pain is commonly characterized by a variety of symptoms, including pain and discomfort, photophobia or light sensitivity, dizziness, lethargy, and mood changes. However, one of the most common symptoms of head pain is brain fog, which also causes its own variety of symptoms. In the following article, we will discuss brain fog associated with head pain and pressure as well as the common cause of brain fog and headache/migraine. �
The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Neural Zoomer Plus for Neurological Disease
�
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention. �
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link. *XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force.
How often do you feel you have something that must be done? How often do you have difficulty concentrating before eating? Do you suffer from migraines and/or headaches?�A migraine headache is commonly characterized by a variety of symptoms, including pain and discomfort, photophobia or light sensitivity, dizziness, lethargy, and mood changes. However, one of the most common symptoms of migraine headaches is brain fog, which also causes its own variety of symptoms. In the following article, we will discuss brain fog associated with migraines and offer several simple tips to help manage migraine brain fog. �
What is Migraine Brain Fog?
Several people experience migraine-associated brain fog before the severe headaches occur, although it most commonly occurs after the migraines have passed. As a matter of fact, a research study demonstrated that almost 70 percent of people with migraines experience brain fog, which can last from a few hours to several days or more. This percentage may be even higher as symptoms of confusion and difficulty focusing or concentrating are also frequently reported, all of which can suggest the presence of post-migraine brain fog. According to researchers, migraine brain fog can include symptoms such as: �
forgetfulness or short-term memory loss
loss of sense of direction
inability to complete everyday tasks and activities
a brain that feels as if it “doesn’t function properly”
feeling as though you’re having to think through a fog
Migraine headache brain fog can make it difficult to participate and engage in daily tasks and activities. Cooking, which requires focus and concentration as well as multiple steps, may feel nearly impossible to do with this health issue. People who suffer from migraines may also feel that driving is downright dangerous, especially if their brain fog is accompanied by a lack of sense of direction. To others, people experiencing migraine brain fog may ultimately appear to be half-asleep. �
What Does Brain Fog Really Feel Like?
Many people have experienced moments where they walk into a room only to find out that they can no longer remember why they even walked into the room. Migraine patients, however, experience these symptoms much more frequently and much more severely. They may often find themselves forgetting what they are doing or where they are going, they become easily distracted, or completely lose track of their purpose. Migraine patients have described migraine-associated brain fog as a feeling of disconnection, trouble making complete sentences or thoughts, or simply as a heaviness or numbing of the mind. � Several people have characterized it as �feeling dumb.� However, the simple fact is that even the most intelligent individual can feel as though their brain has been reduced to little more than mush with migraine brain fog. This can ultimately also cause feelings of guilt over the lack of productivity and it is often aggravated due to challenges accurately explaining the symptoms of the post-migraine brain fog. It is fundamental for both healthcare professionals and patients to be able to recognize that these symptoms are still associated with migraine headaches, even though the pain may have subsided. �
Tips for Managing Migraine Brain Fog
Following a migraine headache, it may be necessary to return to everyday tasks and activities, in spite of the brain fog, including going to school or back to work, taking care of one�s family. The tips below will help ease migraine brain fog. �
Write Things Down
Keep a planner, utilize a smartphone, or stick post-its in relevant areas so that you’ll be able to see them later. Lists to track tasks or activities will help give you the confidence you need to know that you are not missing any important to-do items. �
Be as Organized as Possible
When your environment is organized, it becomes easier for you to find the things that you are looking for to keep moving forward with regular tasks and activities. Several specific organization strategies can include the following, such as: �
Utilizing clearly labeled basket organizers on your desk
Utilizing a filing system that is easy for both you and others to understand
Writing checklists of what you need to accomplish, including grabbing your keys, phone, and wallet, if necessary
Placing medicines into boxes with times and dates so that you will know whether or not you have taken them
Ask for Help if Needed
This is one of the most vital parts of managing migraine brain fog. You can’t always do everything yourself. If you need help, don’t be afraid to seek help from a healthcare professional. Be honest about your needs to achieve migraine brain fog relief. �
Brain fog can make people feel as if they’re not able to focus or concentrate accordingly and it’s commonly accompanied by fatigue and even migraine headaches. While brain fog is a symptoms rather than a single health issue, it can also have a variety of causes. Migraine headaches can have a variety of symptoms on their own but migraine-associated brain have has a whole different variety of symptoms. Understanding migraine brain fog and what you can do about the symptoms can help manage migraine brain fog symptoms and promote overall brain health and wellness. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
Neurotransmitter Assessment Form
The following Neurotransmitter Assessment Form can be filled out and presented to Dr. Alex Jimenez. Symptoms listed on this form are not intended to be utilized as a diagnosis of any type of disease, condition, or any other type of health issue. �
In honor of Governor Abbott’s proclamation, October is Chiropractic Health Month. Learn more about the proposal. �
How often do you feel you have something that must be done? How often do you have difficulty concentrating before eating? Do you suffer from migraines and/or headaches? A migraine headache is commonly characterized by a variety of symptoms, including pain and discomfort, photophobia or light sensitivity, dizziness, lethargy, and mood changes. However, one of the most common symptoms of migraine headaches is brain fog, which also causes its own variety of symptoms. In the article above, we discussed brain fog associated with migraines and offered several simple tips to help manage migraine brain fog. � The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Neural Zoomer Plus for Neurological Disease
�
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention. �
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
� For your convenience and review of the XYMOGEN products please review the following link. *XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force.
If you are suffering from any of these symptoms, then you might be experiencing an allergy attack in your body.
The Rise of Allergies
The rise of allergies has not gone unnoticed amongst the young and the old. The allergy disease has affected over 30% of individuals in many communities, particularly young children, have underscored the need for effective prevention strategies in their early lives. Some individuals will blame the increase in toxin exposure while others blame the food, but mostly everyone will admit that the answers to how the allergy disease comes from are still unclear. Whether it be food, environmental factors, or skin allergies, the common denominator that causes the allergies to develop is in the immune system, especially in its inflammatory department.
The body�s immune system is linked to the entire body microbiome, and it also resides in the gastrointestinal tract. It has been said that the health and function of the immune system are directly associated with the diversity as well as the health of the microbiome. So it is reasonable to consider the microbiome when healthcare professionals are seeking to solve the allergy enigma.
Types of Allergic Reactions
With most allergy reactions, they are manifested in either the gastrointestinal tract, respiratory tract, or the skin. It is not a surprise that these organ systems are also where the body’s microbiome is the most heavily concentrated. A variety of bacterial species make their homes in these organ systems since these three organ systems represent the primary portals of entry for these pathogens.
It is logically that the microbiome of the body is so heavily concentrated as it functions as the first line of defense against invading pathogens and antigens. When there is a weak microbiome, or it lacks biodiversity, it will become a weak defense system, and the immune system is required to “pick up the slack” by identifying and protecting the body against these foreign invaders, which includes the common allergens that a person can get.
Skin Allergies
Skin allergies are where the skin becomes red, bumpy, and itchy rashes to become irritating, painful, and embarrassing for some people. Rashes can be caused by many factors, including exposure to certain plants, an allergic reaction to specific medication or food, or by illnesses like measles or chickenpox. Eczema, hives, and contact dermatitis are the three types of skin rashes. Eczema and hives are the two most common types of skin rashes and are related to allergies.
Eczema: Also known as atopic dermatitis, can affect between 10 to 20 percent of children and 1 to 3 percent of adults. People with eczema will experience dry, red, irritated, and itchy skin. When it is infected, the skin may have small fluid-filled bumps that can ooze clear or yellowish liquid. Anyone with eczema can often have a family history of allergies.
Hives: Also known as urticaria, this skin rash is raised, red bumps or welts that appear on the body. Hives can cause two conditions, and they are acute urticaria and chronic urticaria. Acute urticaria is most commonly caused by exposure to an allergen or by an infection, while the causes of chronic urticaria are still mostly unknown.
Contact dermatitis: This skin rash is a reaction that appears when the skin comes in contact with an irritant or an allergen. Soaps, laundry products, shampoos, Excessive exposure to water, or the sun are some of the factors that can cause contact dermatitis. The symptoms can include rashes, blisters, itching, and burning.
Food Allergies
Anyone with a food allergy has an immune system that reacts to specific proteins found in food. Their immune system starts attacking these compounds as if they were harmful pathogens like a bacterium or a virus. Food allergies can affect 250 million to 550 million people in developed and developing countries.
The symptoms can range from mild to severe and can affect individuals differently. The most common signs and symptoms of an individual’s experience include:
The skin may become itchy or blotchy
Lips and face might swell
Tingling in the mouth
Burning sensation on the lips and mouth
Wheezing
Runny nose
Studies have found out that many people who think they have a food allergy may have a food intolerance. These two are entirely different because food intolerances do not involve the IgE antibodies, and the symptoms may be immediate, delayed, or similar to food allergies. Food intolerances occur due to proteins, chemicals, and other factors that can compromise the intestinal permeability. While food allergies mean that even a small amount of food is going to trigger the immune system, causing an allergic reaction.
Seasonal Allergies
Seasonal allergies are one of the most common allergic reactions that people get. About 8 percent of Americans experience it, according to the American Academy of Allergy, Asthma, and Immunology, and it is commonly known as hay fever. Hay fever occurs when the immune system overreacts to outdoor allergens like pollen, weeds, cut grasses, and wind-pollinated plants.� Seasonal allergies are less common in the winter; however, it is possible to experience allergic rhinitis year-round, depending on where the individual lives and on the allergy triggers they may have.
Symptoms of seasonal allergies can range from mild to severe, including:
Sneezing
Runny or stuffy nose
Water and itchy eyes
Itchy throat
Ear congestion
Postnasal drainage
Conclusion
Allergies are a disease that attacks the immune system and can be triggered by many factors, whether it be from food, environmental factors, or the toxins that a person is exposed to. There are ways to lower the allergy symptoms through medicine or foods that have prebiotics and probiotic nutrients that can reduce the reactions. Some products can help support the immune system and can offer nutrients to the gastrointestinal tract and metabolic support.
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues as well as functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or chronic disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
References:
Brosseau, Carole, et al. �Prebiotics: Mechanisms and Preventive Effects in Allergy.� Nutrients, MDPI, 8 Aug. 2019, www.ncbi.nlm.nih.gov/pubmed/31398959.
Kerr, Michael. �Seasonal Allergies: Symptoms, Causes, and Treatment.� Healthline, 7 May, 2018, www.healthline.com/health/allergies/seasonal-allergies.
Molinari, Giuliano, et al. �Respiratory Allergies: a General Overview of Remedies, Delivery Systems, and the Need to Progress.� ISRN Allergy, Hindawi Publishing Corporation, 12 Mar. 2014, www.ncbi.nlm.nih.gov/pmc/articles/PMC3972928/.
Newman, Tim. �Food Allergies: Symptoms, Treatments, and Causes.� Medical News Today, MediLexicon International, 17 July 2017, www.medicalnewstoday.com/articles/14384.php.
Team, DFH. �Attack Allergies with Prebiotics.� Designs for health, 24 Oct. 2019, blog.designsforhealth.com/node/1133.
Let’s be honest, making a change to your lifestyle is hard. Whether that is due to lack of time, motivation, or not knowing where to begin, there is one thing that makes it easier: accountability. This is where health coaching comes into play. Going through the process with someone and having another individual to talk about it with,� makes the change seem more achievable. The bottom line is that people need support. When it comes to changing one’s lifestyle and adapting new healthy behaviors, individuals who have support are more successful.
What Is A Health Coach?�
A health coach can be defined by The Institute for Integrative Nutrition as, ” a wellness authority and supportive mentor who motivates individuals to cultivate positive health choices. Health coaches educate and support clients to achieve their health goals through lifestyle and behavior adjustments.�
Health coaches are becoming more and more essential as modern medicine continues to improve. Now more than ever, the medical field is advancing at high rate speeds and practitioners do not always have the available time some patients need. Here is where health coaches come into play. Essentially, the position of a health coach was created to fill the void in many doctor offices.� Many doctors contribute but do not have the time or resources to help each patient build healthy habits on a day to day basis. However, health coaches are available to be a supportive mentor who help and guide patients in making healthy lifestyle changes.
What Does A Health Coach Do?�
Health coaches play a vital role in modern medicine. Health coaches can work in multiple settings including for a doctor, a spa, a gym, wellness centers, or even have their own private practice. Health coaches help individuals make lasting changes and keep patients on track to feel their best. In addition to this, health coaches motivate, push, encourage, and create plans with patients to optimize energy and decrease stress and fatigue.
Health coaches are not just for diet and exercise help, but for other aspects of life as well. Health coaches are able to help with stress, sleep, relationships, habits, and even one’s career.
Health coaches work with individuals to go through the problem areas in their life and give them tools to improve their lifestyles. By working with a health coach, the individual begins to learn and create habits that will affect and improve their lives while also giving them the essential life skills they can use for a lifetime.� One of the main things that coaches do is aid patients in setting goals. For many, goals are set but are not attainable, healthy, nor realistic. Health coaches work to break down these goals with patients into smaller, more reachable goals. This helps patients push themselves and not get discouraged because they are hitting these smaller marks along the way.
Aside from setting goals, health coaches also prepare the patient for the emotional fallout that can occur. As mentioned earlier, lifestyle changes are not easy and do not occur overnight. This being said, it is normal to have negative emotions regarding the subject along the way. Health coaches are prepared for this and will help you to not only work through them but learn to adapt to these situations and how to overcome the barriers.
How Can You Benefit?�
In the United States, over half of the adult population is affected by at least one chronic disease, many having to do with joint inflammation (Pecoraro, 2019).� Integrative health coaching allows patients to visualize their goals and work with their health coach to properly identify their values and create action steps to achieve optimal health and wellbeing.
People can utilize health coaches at any moment in time. However, many people choose to have a health coach help them after they receive a diagnosis or are overall unhappy in their health and lifestyle choices.
Health coaches are respectful of the personal knowledge one has of their own life and body. Thus, letting the patient have a say in their plan and protocol. This is beneficial because if a patient is included in the creation of their health plan, they are more likely to comply and make it attainable. Not only does this build trust in the professional relationship, but it allows a health coach to consider all areas in the patient’s life.
Individuals can benefit by learning to lessen health issues, problem solve, and gain a new perspective on their life.
A health coach can do a lot more than just aid in diet and exercise. As one can see, health coaches are helpful in many different aspects of one’s life. The qualifications for a health coach can vary. Personally, I have a bachelors degree in Exercise Science with an emphasis in Health Education from Grand Canyon University. In addition to this, I gained my Exercise Physiologist Certification through the American College of Sports Medicine (ACSM). With this background, I am knowledgeable in the pillars of health and how to successfully guide an individual. Almost every person can benefit from a health coach in at least one way. – Kenna Vaughn, Senior Health Coach
The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or chronic disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
If you are experiencing any of these situations, then you might be experiencing chronic kidney disease.
About over 10% of the adult population suffers from CKD (chronic kidney disease), and the two leading underlying causes of the end-stage of chronic kidney disease are type 2 diabetes and hypertension. Other chronic ailments like dysbiosis of the gut microbiome, inflammation, oxidative stress, as well as environmental toxins and PPI (proton pump inhibitor). All these chronic ailments have been linked to chronic kidney disease in the body.
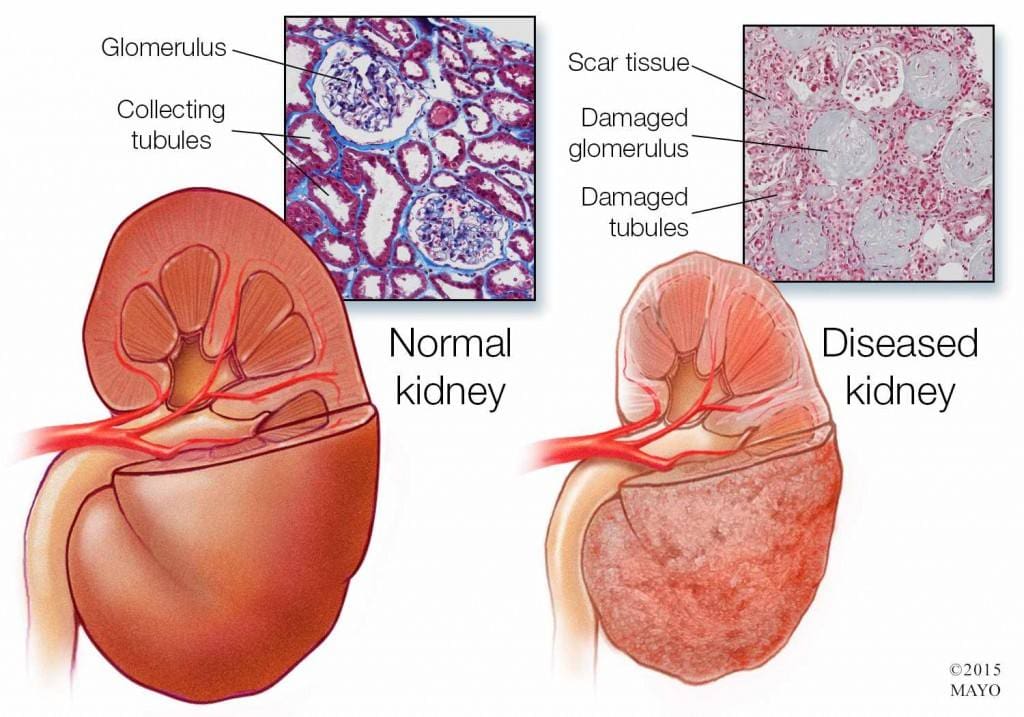
Chronic Kidney Disease
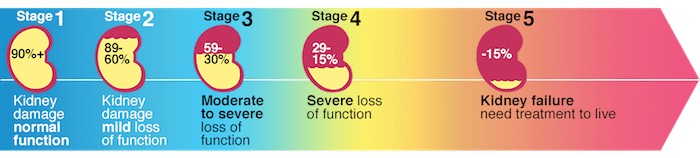
Chronic kidney disease is a slow and progressive loss of kidney function over several years. Also known as chronic renal failure, it much more widespread, and it often goes undetected and undiagnosed until the disease is well advanced. It is not unusual for anyone to realize they have chronic kidney failure when their kidneys are functioning only at 25% than average. As it advances and the kidney’s function is severely impaired, dangerous levels of waste and fluid can rapidly build up in the body.
Chronic kidney failure is different from acute kidney failure due to being a slow and gradually progressive disease. When the disease is fairly well advanced, the conditions are more severe than the signs and symptoms are noticeable, making most of the damage irreversible. Here are some of the most common signs and symptoms of chronic kidney disease include:
Anemia
Blood in urine
Dark urine
Edema- swollen feet, hands, ankles, and face
Fatigue
Hypertension
More frequent urination, especially at night
Muscle cramps and twitches
Pain on the side or mid to lower back
Dietary Fibers for CKD
Researchers have investigated that the role of dietary fibers and the gut microbiome is in renal diets. When there is a dysbiosis in the gut microbiome, it can be a risk factor for the development of chronic kidney disease, thus reducing the renal function. That function will significantly contribute to dysbiosis. The current renal dietary recommendations include a reduction of protein intake with an increase in complex carbohydrates and fiber.
A systemic review did a test that included 14 controlled trials and 143 participants that had chronic kidney disease. The test demonstrated that all 143 participants had a reduction in serum creatinine and urea that is associated with dietary fiber intake, which occurs in a dose-dependent matter. These participants had an average intake of 27 grams of fiber per day in their diet. It is also an essential note that creatinine is metabolized in the intestinal bacteria in the body.
A high fiber diet can lead to the production of SCFAs (short-chain fatty acids) in the gastrointestinal tract. They play an essential role in T regulatory cell activation, which regulates the intestinal immune system. When there is dysregulation in the immune system, it can cause an increase of inflammation that may occur in chronic kidney disease. With a high fiber diet, the intake is associated with lowering the risk of inflammation and the mortality in kidney disease.
Increasing fiber intake is relatively easy with some of these high fiber foods that are both healthy and nutritious and can help individual’s that have kidney disease. These include:
Pears
Strawberries
Avocados
Apples
Carrots
Beets
Broccoli
Lentils
Research has previously demonstrated that a high fiber diet for CDK patients is characterized by the control increase of plant-origin protein and animal-origin foods. This is useful for individuals to limit the consumption of processed food products because of modern conservation processes, which has the purpose of eliminating pathogenic bacteria. People who have chronic kidney disease that go on a high fiber diet have been linked to better kidney function and lowering the risk of inflammation and mortality.
Some individuals may experience some gastrointestinal side effects when they are trying to increase their fiber intake.�Research has been stated that patients should consider resistant starches since it has shown no side effects with the recommended doses.
Conclusion
Chronic kidney disease is a slow and progressive loss of kidney function. The signs and symptoms are noticeable as the disease progress in the later stages. With a high fiber diet, individuals can lower the risk of inflammation and mortality of CDK. When this disease causes inflammation and chronic illness in the kidneys, complications can travel through the entire body. The high fiber diet can also be beneficial for the gut microbiome to function correctly, and some products can help lower the stress hormones and make sure that the body’s hypothalamic-pituitary-adrenal axis is functioning correctly.
October is Chiropractic Health Month. To learn more about it, check out Governor Abbott�s bill on our website to get full details on this historic moment.
The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or chronic disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
References:
D�Alessandro, Claudia. �Dietary Fiber and Gut Microbiota in Renal Diets.� MDPI, Multidisciplinary Digital Publishing Institute, 9 Sept. 2019, www.mdpi.com/2072-6643/11/9/2149/htm.
Gunnars, Kris. �22 High-Fiber Foods You Should Eat.� Healthline, 10 Aug. 2018, www.healthline.com/nutrition/22-high-fiber-foods.
Jurgelewicz, Michael. �New Article Investigates the Role of Dietary Fiber and the Gut Microbiome in Chronic Kidney Disease.� Designs for Health, 13 Sept. 2019, blog.designsforhealth.com/node/1105.
Khosroshahi, H T, et al. �Effects of Fermentable High Fiber Diet Supplementation on Gut Derived and Conventional Nitrogenous Product in Patients on Maintenance Hemodialysis: a Randomized Controlled Trial.� Nutrition & Metabolism., U.S. National Library of Medicine, 12 Mar. 2019, www.ncbi.nlm.nih.gov/pubmed/?term=30911321.
Krishnamurthy, Vidya M Raj, et al. �High Dietary Fiber Intake Is Associated with Decreased Inflammation and All-Cause Mortality in Patients with Chronic Kidney Disease.� Kidney International, U.S. National Library of Medicine, Feb. 2012, www.ncbi.nlm.nih.gov/pmc/articles/PMC4704855/.
Newman, Tim. �Chronic Kidney Disease: Symptoms, Causes, and Treatment.� Medical News Today, MediLexicon International, 13 Dec. 2017, www.medicalnewstoday.com/articles/172179.php.
Staff, Mayo Clinic. �Chronic Kidney Disease.� Mayo Clinic, Mayo Foundation for Medical Education and Research, 15 Aug. 2019, www.mayoclinic.org/diseases-conditions/chronic-kidney-disease/symptoms-causes/syc-20354521.
Do you have difficulty concentrating before eating a meal? Do you experience fatigue after meals? Do you feel as if you’re not getting enough rest or sleep? Do you have noticeable variations in mental speed? If so, you may have brain fog. �
What is Brain Fog?
Brain fog is a health issue that can occur due to a variety of factors. You may struggle to focus on everyday tasks, conversations, or even on the words you�re currently reading. You may also have difficulty making choices where minimal decisions can be overwhelming, you may need coffee to concentrate or snacks to stay awake and even alcohol at night to temporarily relieve the brain fog. In severe instances, you may also have headaches, vision problems, and nausea. �
What Causes Brain Fog?
Brain fog is a symptom rather than a single health issue. It can occur due to nutrient deficiency, bacterial overgrowth from consuming too much sugar, sleep disorder, depression, or even due to thyroid problems. Other common causes of brain fog can ultimately include eating too much and too often, lack of exercise or physical activity, not getting enough rest or sleep, chronic stress, and a poor diet. Below, we will discuss several of the most common causes of brain fog and brain health issues. �
Hormonal Changes
Hormonal changes, frequently caused when our body is producing too much or too little of a specific hormone, is a well-known cause of brain fog. Hormone imbalances due to thyroid health issues are associated with brain fog. This is especially true with Hashimoto�s thyroiditis, an autoimmune disease where the immune system attacks the thyroid as well as causes inflammation and affects the production of enough thyroid hormones. Low thyroid hormone production or hypothyroidism can cause decreased cognitive function and low blood sugar or glucose levels that can ultimately lead to brain fog. �
Lack of Rest or Sleep
Poor sleeping hygiene, such as an irregular sleep and wake time, getting less than seven to eight hours of sleep a night, or blue light exposure before bed, can interrupt our natural circadian rhythm or our internal body clock. This can cause brain fog in a variety of ways. In the instance of blue light exposure close to bedtime, the blue wavelengths can decrease the production of the hormone melatonin, which is essential for deep REM sleep. Both REM and non-REM sleep is necessary for optimal brain function. From 10 pm to 2 am, our body and brain detoxify the most, therefore, staying in an active state throughout this time period can ultimately interrupt our body and brain’s natural detoxification process, which can also cause brain fog. �
Nutritional Deficiencies and Food Sensitivities
Vitamin B12 contributes to the production of red blood cells as well as the maintenance of the central nervous system. A vitamin B12 deficiency can affect your energy levels and cause an overall feeling of fatigue. A vitamin D deficiency can also cause brain fog as decreased vitamin D levels are associated with impaired cognitive function. An unidentified food sensitivity can also contribute to brain fog. By way of instance, gluten sensitivities can ultimately lead to cognitive dysfunction through inflammatory pathways. Advanced blood work that analyzes nutrient levels, as well as an elimination diet or a food allergy/sensitivity test, can help determine if any of these could be contributing to your brain fog. �
How to Naturally Improve Brain Fog
Do Intermittent Fasting
Intermittent fasting can help improve brain fog. Not only can it help you lose weight, calorie restriction and going long periods of time between meals can also help promote brain health and reduce the risk of neurological diseases. Start by trying to extend the time between the last meal of the day and the first meal of the next day. Ideally, intermittent fasting requires you go 12 hours between eating the last meal of the day and the first meal of the next day. This promotes a process called ketogenesis, which can stimulate brain regeneration.� Intermittent fasting should ultimately be practiced after following the guidance of a healthcare professional, such as a health coach, who understands intermittent fasting. �
Participate in Exercise or Physical Activity
Neurological diseases, such as Alzheimer�s disease, dementia, and even moderate cognitive dysfunction, are more common in sedentary populations. Increased activity levels have been associated with sharper mental acuity, better memory, and positive mood changes. Exercise and physical activity cause the release of substances known as cytokines as well as chemicals known as endorphins. These substances and chemicals ultimately improve brain health and function. Try to engage in exercise or physical activity every day. Walking, running, or even dancing can help improve brain fog and boost your mood. �
Rest More and Sleep Better
The most common mistake people make, whether it involves dealing with school, work, or whatever looming project deadline, is that they try to maximize their time by staying up late and/or getting up early. However, this generally backfires because cognitive abilities decrease with sleep deprivation. Rest and sleep at least seven hours a night, preferably eight or even nine if possible. Your efficiency will increase while the time it takes to create quality work will likely decrease. �
Reduce Stress
Stress can cause a variety of symptoms, including brain fog. To reduce stress, you also need to learn how to flex your parasympathetic nervous system, which is engaged during rest and relaxation as well as helps to calm your body and your mind. You can help reduce stress by incorporating more meditation and yoga into your daily workout routine. �
Feed your Brain
The human brain is made up of a lot of fat and protein. Too much sugar and frozen as well as fried or processed foods are not ideally nourishing for our brain. You can follow a plant-based Paleo diet, consisting mostly of vegetables, protein, and good fats. Also, make sure to get plenty of omega-3 fatty acids, for their anti-inflammatory powers, lots of antioxidants and coenzyme Q10, essential for energy, and boost your body�s energy and regeneration with essential vitamins and minerals. �
Brain fog can make people feel as if they’re not able to focus or concentrate accordingly and it’s often accompanied by fatigue and other well-known symptoms. While brain fog is a symptoms rather than a single health issue, it can have a variety of causes, from hormonal changes to lack of rest and sleep to nutritional deficiencies or food sensitivities. Fortunately, there are several steps to help naturally improve brain fog symptoms and promote overall brain health and wellness. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
Neurotransmitter Assessment Form
The following Neurotransmitter Assessment Form can be filled out and presented to Dr. Alex Jimenez. Symptoms listed on this form are not intended to be utilized as a diagnosis of any type of disease, condition, or any other type of health issue. �
In honor of Governor Abbott’s proclamation, October is Chiropractic Health Month. Learn more about the proposal. �
Do you have difficulty concentrating? Do you experience fatigue after meals? Do you feel as if you’re not getting enough rest or sleep? Do you have noticeable variations in mental speed? As previously mentioned above, you may have brain fog. � The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Neural Zoomer Plus for Neurological Disease
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention. �
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link. *XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force.
Back pain can affect every part of the body, including the:
Head
Neck
Legs
Feet
Dental complications are common for people using medications for acute and chronic back pain. Therefore, regular dental care is necessary to spot these problems before they become serious.
Pain medications can at times be the root cause of some dental decay issues.
Myofascial pain syndrome (MPS) requires the highest level of specialized dental care because of the highly sensitive nature of the condition.
I asked a local dentist that specializes in treating patients with chronic pain conditions why dental care is important?
Dental
Regular dental visits are as important as general check-ups with a primary doctor.
Any issues will have time to grow and become more complicated to treat once diagnosed.
Locate a dentist who treats patients with chronic pain issues, specifically in the upper body, and understands the special needs.
Ask about specific tools to help minimize and control pain:
Before
During
After treatment
Call your primary or pain management physician to ask if there are any specific treatment that the dentist needs to know about.
Dry Mouth
People with chronic pain usually have to use various medications.
These medications can cause dry mouth that can lead to tooth decay and gum disease.
Dry mouth condition is called xerostomia and can cause major issues like:
Normal swallowing
Taste problems
Speech problems
Oral tissue integrity
Chronic mouth irritation
Inflammation
Dental decay
Erosion
Stay hydrated by keeping water around throughout the day, and chew sugarless gum or keep sugarless hard candy around to keep saliva flow.
There is also moisturizing mouth spray, that a dentist can provide.
Periodontal Disease
Periodontal disease is when over time, gums pull away from the teeth and form pockets that can get infected.
The body�s immune system fights the bacteria as the plaque�grows and begins to spread out.
Bacterial toxins and the body�s natural fight response to the infection begin to break down bone and the connective tissue that holds the teeth in place.
If left untreated the:
Bones
Gums
Tissue
That support the teeth are destroyed,� which means that the infected tooth has to be pulled.
Tooth Extraction
People with chronic pain try there best to avoid potential pain triggers, which include dental exams.
Tooth or gum pain/sensitivity usually presents in the later stages of decay when the tooth cannot be saved.
Unfortunately, the result is tooth removal.
There are medications that are known to contribute or cause tooth decay:
Antidepressants
Anti-inflammatories
Aspirin
Methadone
Best Defense Strong Offense
So brush your teeth at least twice a day and floss. Although we’ve all heard this throughout our lives, it is true. Just remember brushing and flossing can go a long way in dealing and managing chronic pain issues.
Give the tongue a good brushing to remove bacteria that can lead to plaque and chronic bad breath.
Tooth cleanings and exams are necessary to prevent any issues before they become serious and require major surgery.
Talk with your primary caregiver before visiting the dentist to figure out any special protocol or medication requirements needed.
After dental treatment, allow plenty of time to rest and recover.
Eat soft food during recovery and avoid:
Meats
Popcorn
Hard candy
These can become lodged in the teeth.
Prevention of dental disease will definitely pay off in the end and allow your immune system to perform at its optimal level.
It is worth the effort, I want all my patients to be in top health and proper oral hygiene can prevent so many diseases and is an essential part of a healthy lifestyle.
*CHRONIC* pain Chiropractic Relief | El Paso, Tx
Living with chronic pain symptoms can tremendously affect an individual’s quality of life. Neck and back pain caused by a variety of health issues, such as herniated discs and/or automobile accident injuries, can cause persistent symptoms which may last weeks, months, even years if left untreated.
Dr. Alex Jimenez is a chiropractor in El Paso, TX, who has helped his patients with chronic neck and back pain find the treatment they deserve. Patients describe how Dr. Alex Jimenez has helped them find pain relief and achieve overall health and wellness.
NCBI Resources
Dental visits help you maintain healthy teeth and gums. Gum disease and poor dental health have been linked to a variety of health issues, including heart disease. Researchers have drawn a direct line between tooth loss and heart disease. What�s more, regular oral exams and teeth cleaning can lead to the detection of early-stage medical conditions, some of which can be life-threatening which include:
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine


 �
�