Gender transitioning is the process of affirming and expressing an individual’s internal sense of gender rather than the one assigned at birth. How can learning the aspects of gender and gender transitioning help support the LGBTQ+ community?
Gender Transitioning
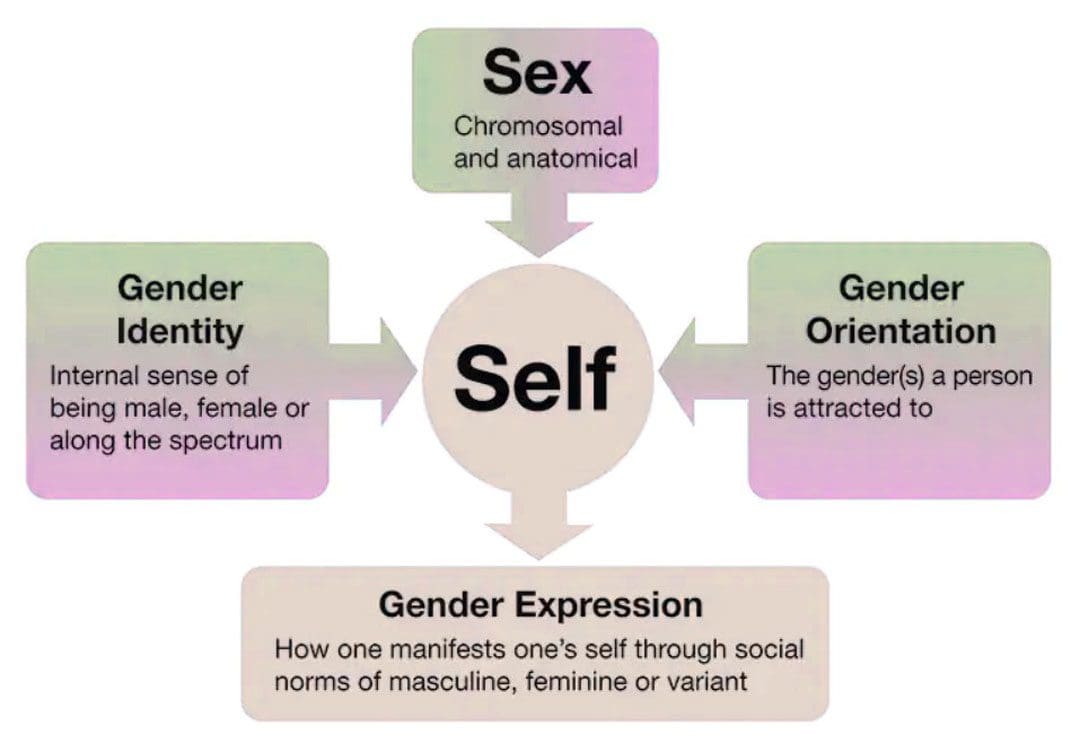
Gender transitioning or gender affirmation is a process through which transgender and gender-nonconforming individuals align their internal gender identity with their external gender expression. It can be described as a binary – male or female – but can also be non-binary, meaning an individual is neither exclusively male nor female.
The process can involve aesthetic appearances, changes in social roles, legal recognitions, and/or physical aspects of the body.
Social affirmation – dressing differently or coming out to friends and family.
Legal affirmation – changing name and gender on legal documents.
Medical affirmation – using hormones and/or surgery to change certain physical aspects of their body.
Transgender individuals can pursue some or all of these.
Barriers
Gender transitioning can be obstructed by various barriers that can include:
Cost
Lack of insurance
Lack of family, friends, or partner support.
Discrimination
Stigma
Addressing All Aspects
The process does not have a specific timeline and is not always linear.
Many transgender and gender-nonconforming individuals prefer gender affirmation to gender transitioning because transitioning is often taken to mean the process of medically transforming the body.
An individual does not have to undergo medical treatment to affirm their identity, and some transgender people avoid hormones or gender-affirming surgery.
Transitioning is a holistic process that addresses all aspects of who a person is inwardly and outwardly.
Certain aspects of transitioning may be more important than others, like changing one’s name and gender on their birth certificate.
Reevaluation and revision of gender identity can be continual rather than a step-by-step, one-way process.
Exploring Gender Identity
Gender transitioning often starts in response to gender dysphoria which describes the constant sense of uneasiness that occurs when the gender an individual was assigned at birth does not match how they experience or express their gender internally.
Some individuals have experienced symptoms of gender dysphoria as early as 3 or 4 years of age. (Selin Gülgöz, et al., 2019)
Gender dysphoria can be largely informed by the culture that surrounds the individual, specifically in cultures where strict codes determine what is masculine/male and feminine/female.
Unease Expressed in Different Ways
Dislike of one’s sexual anatomy.
A preference for clothes typically worn by the other gender.
Not wanting to wear clothes typically worn by their own gender.
A preference for cross-gender roles in fantasy play.
A strong preference for engaging in activities that are typically done by the other gender.
Dysphoria
Gender dysphoria can fully emerge during puberty when awareness about how an individual’s body defines them creates internal distress.
Feelings may be amplified when an individual is described as a tomboy, or a sissy, or is criticized and attacked for acting like a girl or acting like a boy.
During puberty, the physical changes can cause long-standing feelings of not fitting in and may evolve into feelings of not fitting in their own body.
This is when individuals can undergo a process referred to as internal transitioning and begin to change how they see themselves.
Gender transitioning/affirmation becomes the next step. Transitioning is not about changing or recreating oneself but about expressing their authentic self and asserting who they are socially, legally, and/or medically.
Social
Social transitioning involves how a person publicly expresses their gender. The transition can include:
Changing pronouns.
Using chosen name.
Coming out to friends, family, coworkers, etc.
Wearing new clothes.
Cutting or styling hair differently.
Changing mannerisms like moving, sitting, etc.
Changing voice.
Binding – strapping the chest to hide breasts.
Wearing breast and hip prosthetics to accentuate feminine curvature.
Packing – wearing a penile prosthesis to create a penile bulge.
Tucking – tucking the penis to conceal a bulge.
Playing certain sports
Pursuing different lines of work.
Participating in activities that might typically be seen as male or female.
Legal
Legal transitioning involves changing legal documents to reflect the individual’s chosen name, gender, and pronouns. This includes governmental and non-government documents that can include:
Birth certificates
Social Security ID
Driver’s license
Passport
Bank records
Medical and dental records
Voter registration
School ID
Provisions allowing for changes can vary by state.
Some states only allow changes if bottom surgery – genital reconstruction is performed.
Others will allow the changes without any form of gender-affirming surgery.
Medical transitioning typically involves hormone therapy to develop some of the male or female sex characteristics. It can also involve surgery to change certain physical aspects combined with hormone therapy.
Hormone therapy assists individuals to physically look more like the gender they identify as.
They can be used on their own and can also be used before gender-affirming surgery.
Hormone therapy takes two forms:
Transgender Men
Testosterone is taken to help deepen the voice, increase muscle mass, promote body and facial hair, and enlarge the clitoris. (M S Irwig, K Childs, A B Hancock. 2017)
Transgender Women
Estrogen is taken as well as testosterone blockers to redistribute body fat, increase breast size, reduce male-pattern baldness, and reduce testicle size. (Vin Tangpricha 1, Martin den Heijer. 2017)
Surgery
Gender affirmation surgery aligns an individual’s physical appearance to their gender identity. Many hospitals provide gender-affirming surgery through a transgender medicine department. Medical procedures include:
Facial surgery – Facial feminization surgery.
Breast augmentation – Increases breast size with implants.
Chest masculinization – Removes contours of breast tissues.
Tracheal shaving – Reduces the Adam’s apple.
Phalloplasty – Construction of a penis.
Orchiectomy – Removal of the testicles.
Scrotoplasty – Construction of a scrotum.
Vaginoplasty – Construction of a vaginal canal.
Vulvoplasty – Construction of the outer female genitalia.
Roadblocks
Transgender individuals are protected from public and private insurance discrimination under federal and state laws, including Medicare and Medicaid. (National Center for Transgender Equality. 2021)
Medicaid programs in nine states do not cover gender-affirming medical treatments, and only Illinois and Maine offer comprehensive standard care recommended by the World Professional Association for Transgender Health/WPATH. (Kaiser Family Foundation. 2022)
Medicare also has no consistent policy regarding the approval of gender-affirming surgery.
Others report family or partner disapproval as the main reason why they discontinue gender affirmation. (Jack L. Turban, et al., 2021)
If you know someone who is transgender or is considering transitioning, learning about gender and gender transitioning and how to be supportive is a great way to be an ally.
Enhancing Your Lifestyle
References
Gülgöz, S., Glazier, J. J., Enright, E. A., Alonso, D. J., Durwood, L. J., Fast, A. A., Lowe, R., Ji, C., Heer, J., Martin, C. L., & Olson, K. R. (2019). Similarity in transgender and cisgender children’s gender development. Proceedings of the National Academy of Sciences of the United States of America, 116(49), 24480–24485. https://doi.org/10.1073/pnas.1909367116
Irwig, M. S., Childs, K., & Hancock, A. B. (2017). Effects of testosterone on the transgender male voice. Andrology, 5(1), 107–112. https://doi.org/10.1111/andr.12278
Tangpricha, V., & den Heijer, M. (2017). Estrogen and anti-androgen therapy for transgender women. The Lancet. Diabetes & endocrinology, 5(4), 291–300. https://doi.org/10.1016/S2213-8587(16)30319-9
National Center for Transgender Equality. Know Your Rights in Health Care.
Kaiser Family Foundation. Update on Medicaid coverage of gender-affirming health services.
Center of Medicare and Medicaid Services. Gender dysphoria and gender reassignment surgery.
Transgender Legal Defense and Education Fund. Health insurance medical policies.
National Center for Transgender Equality and National Gay and Lesbian Task Force. Injustice at Every Turn: A Report of the National Transgender Discrimination Survey.
Turban, J. L., Loo, S. S., Almazan, A. N., & Keuroghlian, A. S. (2021). Factors Leading to “Detransition” Among Transgender and Gender Diverse People in the United States: A Mixed-Methods Analysis. LGBT health, 8(4), 273–280. https://doi.org/10.1089/lgbt.2020.0437
Ohio Attorney General Mike DeWine is suing five makers of opioid painkillers for their role in the state’s opioid epidemic.
The five companies named in the suit are Purdue Pharma, Johnson & Johnson, Teva Pharmaceuticals, Endo Health Solutions and Allergan.
This is the second suit of its kind brought by a state, after Mississippi.
Ohio attorney general sues 5 pharma companies over their role in the opioid epidemic��
Ohio Attorney General Mike DeWine is suing five makers of opioid painkillers for their role in the state’s opioid epidemic.
The suit, which DeWine said is the second by a U.S. state, after Mississippi, claims the drugmakers violated multiple state laws, including the Ohio Corrupt Practices Act, and committed Medicaid fraud.
Purdue Pharma, Johnson & Johnson and its Janssen Pharmaceuticals unit, Teva Pharmaceuticals and its Cephalon unit, Endo Health Solutions and Allergan are all named in the suit.
“In 2014 alone, pharmaceutical companies spent $168 million through sales reps peddling prescription opioids to win over doctors with smooth pitches and glossy brochures that downplayed the risks” of the medicines,” DeWine said at a press conference Wednesday. Last year, he said, 2.3 million people in Ohio, or about a fifth of the state’s population, were prescribed opioids.
In a statement, a spokesman for Purdue Pharma, which manufactures OxyContin, said the company shares the attorney general’s concerns about the opioid crisis and that it is “committed to working collaboratively to find solutions.”
“OxyContin accounts for less than 2% of the opioid analgesic prescription market nationally, but we are an industry leader in the development of abuse-deterrent technology, advocating for the use of prescription drug monitoring programs and supporting access to Naloxone � all important components for combating the opioid crisis,” he said.
Allergan declined to comment, as did a Teva spokeswoman, who said, “We have not completed review of the complaint.”
J&J’s Janssen unit said the company believed the allegations in the lawsuit were “both legally and factually unfounded.”
“Janssen has acted appropriately, responsibly and in the best interests of patients regarding our opioid pain medications, which are FDA-approved and carry FDA-mandated warnings about the known risks of the medications on every product label,” said Jessica Castles Smith, a Janssen spokeswoman.
Endo officials weren’t immediately available to comment.
The Ohio action follows suits from counties and cities seeking to hold accountable the industry that produces, markets and distributes opioid painkillers. DeWine said the Ohio suit, filed Wednesday morning in Ross County, “would compel these companies to clean up this mess through several remedies,” including an injunction to stop “continued deception and misrepresentation in marketing,” damages paid to the state for money spent on the crisis, and repayment to consumers.
Sales of prescribed opioids � including oxycodone, hydrocodone and methadone � almost quadrupled in the U.S. between 1999 and 2015, according to the Centers for Disease Control and Prevention, contributing to a more than quadrupling of deaths from prescription opioids in that same period. Almost 2 million Americans either abused or were dependent on prescription opioid painkillers in 2014, according to the CDC.
“We understand what we’re taking on: five huge drug companies,” DeWine told reporters Wednesday. “I don’t want to look back 10 years from now and say we should have had the guts to file. � It’s something we have to do.”
In February, an immigration enforcement case in El Paso earned the attention of domestic violence advocates across the country. As the El Paso Times reported, an undocumented woman was detained by immigration officers right after she went to the courthouse to get a restraining order against a violent and abusive partner. Domestic violence advocates were horrified, worried that it would potentially deter undocumented people from reporting abuse to law enforcement. “It sends a powerful message to victims and survivors that there is no safe place,” Ruth Glenn, executive director of the National Coalition Against Domestic Violence, told Bustle in February.
Now, a month later, the effect of fighting domestic violence is being felt. Sometime after the El Paso incident, Enrique Elizondo, a worker for a domestic violence hotline, received a call from an undocumented woman (I have not included any identifying details to protect her confidentiality), facing an abusive husband. According to Elizondo, she was at the point of fear that the abuse could become lethal. But, after selling all her belongings to come to the United States, she found herself feeling like she was out of options. According to Elizondo, her partner had specifically made threats about contacting Immigration and Customs Enforcement (ICE) and having her deported if she took action. The El Paso case made her fear he could. Elizondo tells Bustle he tried to help her contact legal help, but the woman asked him, Is this legal advocate going to deport me? Ultimately, Elizondo says he was able to get her legal help.
Supporting All Survivors on International Womens Day
As we celebrate International Women’s Day, it’s important to remember that ALL women deserve support and safety, regardless of race, religion, country of…
huffingtonpost.com
According to domestic violence advocates interviewed for this article, these situations are becoming the norm for dealing with undocumented survivors of domestic violence. The 2013 re-authorization of the Violence Against Women Act (VAWA) protects survivors of abuse from deportation for reporting the crime, but, as fear in undocumented communities has grown due to more expansive calls for immigration enforcement under Donald Trump’s administration, it’s hard for the people helping survivors to convince them they’re safe.
The February El Paso case may very well have been a fluke according to the El Paso Times, the woman detained had further criminal complaints against her beyond her immigration status. But the publicity generated by a women detained while seeking help from a court has nevertheless led to worry among violence survivors. Already, four cases in Denver of domestic violence were dropped due to fears of the survivors about immigration status, according to Denver City Attorney Kristin Bronsonm who spoke to NPR about the situation.
“That case [in El Paso] alone, I am actually sure had a chilling effect,” Ruth Glenn tells Bustle a month after we initially spoke. Her organization, the National Coalition Against Violence, is working “to ensure that advocates know how to support those victims by making sure that they know what the laws and the rules are,” she says. Specifically, it has been focusing on helping shelters figure out how to deal with these issues such as knowing that they are expected to maintain the confidentiality of their residents even if ICE officers shows up at the door.
Unfortunately, some are prioritizing continuing to live with abuse.
Under the Obama administration, a 2011 legal memorandum required ICE to exercise prosecutorial discretion when dealing with victims or witnesses to crimes like domestic violence.
According to a statement from Letitia Zamarippa, spokeswoman for ICE, that memo is still in effect. U.S. Immigration and Customs Enforcement (ICE) officers will take into consideration if an individual is the immediate victim or witness to a crime, in determining whether to take enforcement action. Particular attention is paid to victims of domestic violence, human trafficking or other serious crimes.”
But even with the law officially in place, the uncertainty caused by Trump administration actions stepping up deportations and limiting restrictions on ICE causes fear among survivors.
The Trump administration’s recent actions taking aim at sanctuary cities, hoping to push local police agencies to enforce immigration laws, worries advocates, as well.
If you think about victims of domestic violence who are already being controlled by a perpetrator, that is compounded and exacerbated when you rely on that person to interpret the laws for you, who is filtering all that information to control you.”
“When you have your local sheriff, whose job is to come to domestic violence scenes and to be in the community if they’re also enforcing immigration law the question is whether victims are going to come call when they’re being abused or sexually assaulted,” says Huang. “Entire communities are afraid of reaching out for help. ICE officers are not always the best at finding out if there’s victims.”
Overall, the growing sense of uncertainty, the anti-immigration rhetoric, and the threats to sanctuary city are leaving a strong impact on domestic violence victims who live in a legal gray area and may not be well versed in their legal rights. “If you think about victims of domestic violence who are already being controlled by a perpetrator, that is compounded and exacerbated when you rely on that person to interpret the laws for you, who is filtering all that information to control you,” Monica McLaughlin, Deputy Director of Public Policy at the National Network to End Domestic Violence, tells Bustle.
The underlying problem is that even if undocumented immigrants can technically get help, McLaughlin explains, “if what’s been communicated indicates that they can’t because they’re not safe, then survivors really aren’t going to reach out to law enforcement for help.”
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine