Sinding-Larsen-Johansson, or SLJ, syndrome is a debilitating knee condition that most commonly affects teens during periods of rapid growth. The kneecap, or patella, is attached to the shinbone, or tibia, from the patellar tendon. The tendon connects to an expansion plate at the bottom of the kneecap throughout growth.
Repetitive stress on the patellar tendon can make the growth plate within the knee become inflamed and irritated. SLJ mainly develops in children and adolescents between the ages of 10 and 15 because that is when most people experience growth spurts. SLJ is most common in young athletes due to excess or repetitive strain in the knee.
Causes of SLJ Syndrome
The large muscle group at the front of the upper leg is known as the quadriceps. When straightening the leg, the quadriceps pull to deliver the leg forward. This puts pressure on the growth plate at the bottom of the kneecap. During rapid growth, the bones and muscles don’t always grow at precisely the same rate.
Since the bones grow, tendons and muscles can get tight and stretched. This increases the strain around the patellar tendon and also on the growth plate it’s attached to. Repetitive or extra stress and pressure in this area can cause the growth plate to become irritated and painful. Matters that can contribute to growing SLJ syndrome are comprised of:
Sports that involve a lot of running and jumping, such as field and track or other sports such as football, gymnastics, basketball, lacrosse, and field hockey, can place stress on the knees.
Increased or incorrect physical activity can add strain on the knees. Improper form while training, shoes that don’t support the toes or an unusual way of jogging can increase chances of SLJ syndrome.
Tight or stiff quadriceps muscles can also lead to SLJ syndrome. Muscles that are more powerful and more elastic will work better, reducing the strain on the patellar and kneecap tendon.
Activities that place more pressure on the knees or demanding tasks for the knees, such as lifting heavy items, walking up and down stairs, and squatting can cause SLJ syndrome. If there’s already pain on the knee, then these movements may make it worse.
Symptoms of SLJ Syndrome
Symptoms demonstrating the presence of�Sinding-Larsen-Johansson, or SLJ, syndrome include: pain at the front of the knee or near the bottom of the kneecap, as this is the main symptom of SLJ; swelling and tenderness around the kneecap; pain that increases with physical activities like jogging, climbing stairs, or leaping; pain that becomes more acute when kneeling or squatting; and a swollen or bony bump at the bottom of the kneecap.
Sinding-Larsen-Johansson, or SLJ, syndrome is medically referred to as a juvenile osteochondrosis which affects the patella tendon in the kneecap which attaches to the inferior pole of the patella in the shinbone. Commonly characterized by knee pain and inflammation, SLJ is considered an overuse knee injury rather than a traumatic injury. Sinding-Larsen-Johansson syndrome is similar to Osgood-Schlatter syndrome.
Dr. Alex Jimenez D.C., C.C.S.T. Insight
Diagnosis of SLJ
Should you see a healthcare professional for knee problems, they will generally ask questions about how much pain the patient is experiencing and if they do any sports or other physical activities and exercises. Whether or not the patient has also had a recent growth spurt, the doctor will examine the patient’s knee for swelling and tenderness.
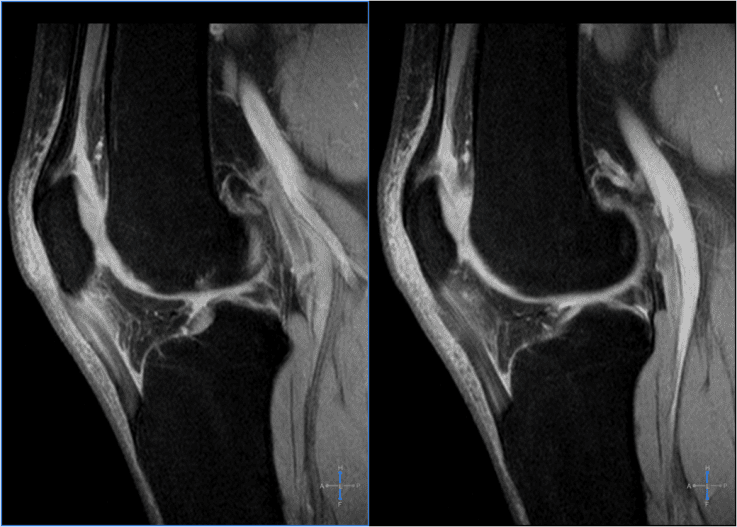
In very rare instances, the healthcare professional may also ask patients to acquire an X-ray or other imaging diagnostics, such as magnetic resonance imaging, or MRI, to rule out other health issues like fracture or disease.
Prevention of SLJ
The most significant way that patients can prevent getting SLJ is to stop doing physical activities which cause pain in the knee. The patient should limit themselves before the pain goes off.
It is crucial to warm up well and stretch before exercising, playing sports or engaging in any other physical activities. A jog around the track for a couple of minutes and some dynamic stretching is enough to warm up the body.
If the quadriceps muscles are tight, then you might want to do some specialized exercise and physical activity routines. Talk to your healthcare professional, such as a chiropractor or physical therapist, to discuss what’s best for you. Doing a few stretches and warm up exercises after sports or physical activities can help prevent SLJ syndrome from developing.
Treatment of SLJ
The first and most important way to treat SLJ is to stop any action that causes irritation in the knee. It’s essential for a patient to not resume any physical activities without first being cleared by a healthcare professional.
SLJ can be challenging to treat since it may not completely resolve before the bones have completely matured and the growth plates are completely shut. During physical activities, knee pain may come and go in the meantime. Other treatments to help ease SLJ syndrome include:
Use the RICE formula.
Rest. Limit physical activities as much as possible and keep weight off the knee. Walking must be kept to a minimum.
Ice. Apply ice or a cold compress to the affected area for 15 to 20 minutes every few hours. Repeat this for 2 to 3 days or until the painful symptoms have decreased.
Compress. Give the knee additional support with a strap, a band, or a ribbon. This will also�help manage symptoms.
Elevate. Keep the knee higher than the heart to reduce swelling.
Take anti-inflammatory or painkilling drugs. Painkillers like acetaminophen and ibuprofen can help relieve pain and decrease swelling.
Begin a stretching and strengthening program. After the pain and tenderness on your knee have been gone, speak with your physician or sports injury professional about a physical rehabilitation program to strengthen the muscles of your leg and increase their flexibility and range of movement.
It’s easy to become impatient when sidelined by an injury, but the proper treatment can help build the strength needed for future physical activities.�The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topic Discussion: Relieving Knee Pain without Surgery
Knee pain is a well-known symptom which can occur due to a variety of knee injuries and/or conditions, including sports injuries. The knee is one of the most complex joints in the human body as it is made-up of the intersection of four bones, four ligaments, various tendons, two menisci, and cartilage. According to the American Academy of Family Physicians, the most common causes of knee pain include patellar subluxation, patellar tendinitis or jumper’s knee, and Osgood-Schlatter disease. Although knee pain is most likely to occur in people over 60 years old, knee pain can also occur in children and adolescents. Knee pain can be treated at home following the RICE methods, however, severe knee injuries may require immediate medical attention, including chiropractic care.
Patellar tendinitis is a common health issue characterized by the inflammation of the tendon which joins the kneecap, or patella, to the shinbone, or tibia. The knee pain associated with this problem may range from mild to severe depending on the circumstances of the knee injury.
Patellar tendinitis, or jumper’s knee, is a well-known sports injury among athletes who play in basketball and volleyball. Among recreational volleyball players, an estimated 14.4 percent of them have jumper’s knee, where the incidence is even higher for professional athletes. An estimated 40 to 50 percent of elite volleyball players have patellar tendinitis.
Causes of Patellar Tendinitis
Patellar tendinitis is caused by repetitive strain on the knee, most often from overuse in physical activities. Stress can create tears along the tendons which can cause inflammation in the complex structures of the knee.
Other contributing factors of patellar tendinitis include:
Tight or stiff leg muscles
Uneven leg muscle strength
Misaligned toes, ankles, and legs
Obesity
Sneakers without enough padding
Tough playing surfaces
Chronic health issues that weaken the tendon
Athletes have a higher chance of developing patellar tendinitis because running, jumping, and squatting put more force over the tendon. Running can place a force of as many as five times the body weight on the knees.
Intense physical activity for an extended amount of time has been previously associated with jumper’s knee. A 2014 research study noted that jump frequency was also a significant risk factor for amateur players.
Symptoms of Patellar Tendinitis
The initial symptoms of patellar tendinitis include pain,�discomfort, and tenderness at the base of the kneecap or patella. Other symptoms of patellar tendinitis may include a burning sensation. For many patients, getting up from a squat or kneeling down can also be particularly debilitating.
The pain associated with patellar tendinitis may be irregular at first, manifesting immediately after participating in physical activities. Damage or injury to the tendon can also make the pain worse. Jumper’s knee can affect regular daily activities, such as climbing stairs or sitting in a vehicle.
�
Patellar tendinitis, also known as “jumper’s knee”, is a particularly common cause of pain and discomfort in the patellar region of many athletes. While it frequently occurs as a result of repetitive or continuous jumping, research studies have demonstrated that patellar tendinitis may be associated with stiff ankle movements and ankle sprains, among other sports injuries.
Dr. Alex Jimenez D.C., C.C.S.T. Insight
Patellar Tendinitis Diagnosis
At the start of a�consultation, the healthcare professional will first ask the patient about their specific health issue. The doctor will then physically evaluate the patient’s knee, probe for where they are feeling pain, and test the assortment of knee motion by bending and extending the patient’s leg.
Furthermore, the healthcare professional may additionally order imaging diagnostics to find out if there’s any damage or injury to the tendon or even the bone. These tests can help rule out a broken bone, or fracture. The doctor may use an X-ray to look for a displaced or fractured kneecap, and an MRI or an ultrasound to reveal any harm to the soft tissue.
Patellar Tendinitis Treatment
Treatment for patellar tendinitis depends on the damage or injury to the knee. Conservative steps to reduce pain, such as rest or exercises are generally the first line of treatment. The healthcare professional will usually recommend a span of controlled rest, where they will prevent the patient from engaging in physical activities that put�pressure on the knee.
Drugs and/or Medications
The healthcare professional may prescribe over-the-counter drugs and/or medications for short-term pain relief and inflammation reduction.
These can consist of:
Ibuprofen (Advil)
Naproxen sodium (Aleve)
cetaminophen (Tylenol)
If the patient’s symptoms are severe, the healthcare professional may recommend the use of corticosteroid injection in the area around the patellar tendon. This treatment is effective in reducing acute pain.
Another method of utilizing corticosteroid for patellar tendinitis is by spreading the medication over the affected knee and use a low electrical charge to push it through the skin, in a process known as iontophoresis.
Chiropractic Care and Physical Therapy
The goal of chiropractic care and physical therapy for patellar tendinitis is to reduce pain and inflammation, among other symptoms, as well as to strengthen the leg and thigh muscles with stretches and exercises.
If the patient’s symptoms are severe, even while resting, the doctor may recommend that you wear a brace and then use crutches to avoid additional damage or injury to the tendon. If the patient has no painful symptoms, then they can start participating in a physical therapy activities.
A rehabilitation program generally consists of:
A warm-up interval
Massage, heat or ice to the�knee
Stretching exercises
Strengthening exercises
A doctor of chiropractic, or chiropractor, may use ultrasound and electrical stimulation to relieve the patient’s knee pain. A�knee brace or taping of the knee might also help reduce pain by supporting the kneecap when engaging in physical activities. The healthcare professional may develop a workout program that may include a series of stretches and exercises.
Surgery
When other treatments are not effective in relieving painful symptoms associated with patellar tendinitis, the doctor may advise surgery to repair the patellar tendon. Traditional surgery involves opening the knee to scrape on the kneecap and tendon. More recently,�arthroscopic surgery is used for this particular process. This surgical intervention involves making four small incisions in the knee and it has a shorter recovery time.
The recovery period for surgery varies per procedure. Some surgical intervention advise for immobilization with a cast. Others suggest�an immediate rehabilitation program. Regardless of the level of damage and/or injury, it’s essential for patients to seek medical attention for their patellar tendinitis. The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topic Discussion: Relieving Knee Pain without Surgery
Knee pain is a well-known symptom which can occur due to a variety of knee injuries and/or conditions, including sports injuries. The knee is one of the most complex joints in the human body as it is made-up of the intersection of four bones, four ligaments, various tendons, two menisci, and cartilage. According to the American Academy of Family Physicians, the most common causes of knee pain include patellar subluxation, patellar tendinitis or jumper’s knee, and Osgood-Schlatter disease. Although knee pain is most likely to occur in people over 60 years old, knee pain can also occur in children and adolescents. Knee pain can be treated at home following the RICE methods, however, severe knee injuries may require immediate medical attention, including chiropractic care.
I went through the physical therapy, and then I used chiropractic care, as well as crossfit, to kinda get me to that 100% mark. And I haven’t had a problem since, I continue to do crossfit and I use chiropractic care to make sure my body is aligned. It gives me that extra sense of feeling that I’m not gonna injure myself again, that my body is feeling good and 100%. I never have that feeling in the back of my mind, that, you know, I’m gonna injure myself. Sometimes I forget I even had a surgery and I think I can attribute that to a combination of chiropractic care and to the overall training aspect of crossfit. – Andrew Hutchison
There are a variety of causes for both hip pain and knee pain. While the hip joint can withstand a tremendous amount of wear-and-tear, it’s not indestructible. With age and usage, the hip cartilage can begin to degenerate, resulting in hip pain. Tendons and ligaments at the hip may also get excessive overused and can start to demonstrate signs of wear-and-tear over time. The anatomy of the knee, however, is more complex. The knee is collectively made up of bones, pads of cartilage and a joint capsule. Trauma or damage from an injury or degeneration associated with aging may cause knee pain.
Causes of Hip Pain
Hip pain is the general term used to define pain felt in or around the hip joint. Certain injuries and/or conditions may commonly cause hip pain. Arthritis, especially rheumatoid arthritis, are the primary culprits of hip pain in older individuals. Both may result in the breakdown of cartilage in the hip joint and can cause inflammation in the area. Combined with pain and discomfort, there’s generally also reduced range of motion in the hip as well as stiffness. Bursitis may also result in hip pain. The bursae are sacs of fluid which function by helping to reduce friction between the joints. If these become inflamed, however, they can lead to pain. Typically, it’s only repetitive movements that irritate the hip joint and result in pain.
Similar to bursitis, tendinitis can also lead to inflammation and is usually caused by repetitive stress from movements. Muscle or tendon strain can be a result of overuse. Repeated physical activities can additionally place unnecessary amounts of pressure on the ligaments, tendons and joints of the hip, especially in those which support the buttocks. If some of these are inflamed, the hip won’t be able to function normally and there will be painful symptoms as a result. Below, we will describe the various causes of hip pain as well as discuss their effects on the structure of the hip in detail.�Hip pain isn’t always felt in the hip itself as it may also be felt in the groin or thigh.
Tendonitis
The most frequent cause of severe hip pain is inflamed tendons, or tendonitis. This can generally be due to excessive exercise or physical activities. This health issue can be quite debilitating but it usually heals within a couple of days with proper care.
Arthritis
As mentioned above, one of the most common causes of chronic hip pain is arthritis. Arthritis can cause painful, stiff and tender joints, and it can cause walking problems. Various types of arthritis can cause hip pain, including:
Osteoarthritis might be the final result of age-related degeneration in the cartilage that surrounds the joints.
Trauma, damage or injury to a joint, like a fracture, may cause traumatic arthritis similar to atherosclerosis.
Infectious arthritis is a result of an infection in the joint caused by the degeneration of cartilage.
Rheumatoid arthritis is a result of the human body’s immune system attacking its own joints. This type of arthritis can ultimately destroy joint bones and cartilage.
Osteoarthritis is a a lot more commonly diagnosed than rheumatoid arthritis.It’s fundamental to understand the different types of arthritis as these can be powerful diagnostic tools to help effectively treat hip pain.
Trochanteric Bursitis
Another possible cause of hip pain involves a health issue medically referred to as trochanteric bursitis, as previously mentioned. This condition occurs when the bursa, which are liquid-filled sacs near the hip joint, become inflamed. Any number of variables can lead to trochanteric bursitis, such as hip injury, overuse of the joints, underlying health issues, or even the presence of other conditions like rheumatoid arthritis. This condition is reportedly much more common in females than in males.
Hip Fractures
Hip fractures are common causes of hip pain which most frequently occur in older adults and in people who have osteoporosis, which is a weakening of the bones associated with age and various other factors. Hip fractures cause very sudden and extreme hip pain, where they will require immediate medical attention. There are complications that can happen due a fractured hip, like a blood clot in the leg. A hip fracture usually requires surgical interventions to be corrected. Additionally, you may be required to seek further care from a qualified healthcare professional in order to engage in a rehabilitation program.
Less Common Causes of Hip Pain
There are additional, less common conditions that can result in hip pain. These include snapping hip syndrome and osteonecrosis, or avascular necrosis. Below, we will discuss these two health issues in detail.
Snapping Hip Syndrome
Snapping hip syndrome, which most commonly occurs in athletes, especially dancers, is characterized by a snapping noise or feeling from the hip. By way of instance, this snapping may happen when you’re walking or getting up from a chair. The problem is usually painless, but it can cause pain in several cases. Snapping hip with pain is generally an indication of a tear in the hip cartilage or other structure surrounding the hip joint.
Osteonecrosis
Osteonecrosis, also known as avascular necrosis, occurs when blood isn’t able to reach the bones, either permanently or temporarily. This can cause the reduction of bone. The cartilage of individuals with this condition is normal initially, however, it will eventually collapse as the disease evolves. Finally, bones may crack or crumble. It’s not always clear what triggers osteonecrosis. Joint harm, heavy usage of steroid drugs or alcohol, and cancer treatments could put you at greater risk of developing this condition, however, the cause is never determined in many osteonecrosis cases.
Causes of Knee Pain
Similar to hip pain, arthritis, especially rheumatoid arthritis and osteoarthritis, may commonly cause knee pain. With the breakdown of cartilage associated with osteoarthritis in the knee, the bones can begin to rub against one another, causing pain and discomfort which could eventually lead to other painful symptoms. Rheumatoid arthritis is a chronic inflammatory disorder of the joints and it can affect the soft tissue which lines the knee joints. The final result is inflammation, joint damage and joint pain at the knee. The knee joint is very prone to accidents. Typical knee injuries include: meniscal injuries, anterior cruciate ligament injuries and tendon injuries.
The meniscus might be damaged when the knee is bent and twisted in an unnatural way, where ligaments and tendons could also be overstretched and ultimately torn as a result. If it is not repaired, the probability of developing osteoarthritis increases. Any abrupt change in movement can additionally injure the anterior cruciate ligament. Nearly all causes of knee injury and knee pain are the result of a blow to the surface of the knee. Exercises or physical activities which could harm the complex structures of the knee include jogging and jumping. A dislocated kneecap is still another frequent source of knee pain. This occurs when the patella is moved from place and it can be very debilitating.
Temporary knee pain differs from chronic knee pain. Persistent knee pain is not always attributable to one incident. It the result of many causes or conditions.Persistent knee pain is characterized as long-term pain, swelling, or sensitivity in a single or both knees. The reason behind your knee pain can determine the symptoms you develop. Many conditions may cause or lead to chronic knee pain, and lots of treatments exist. Every person’s experience with chronic knee pain will most likely be different. Understanding the causes of knee pain can be a powerful diagnostic tool which can help healthcare professionals properly determine the proper treatment option for your specific health issue.�Common causes of knee pain include:
osteoarthritis: pain, inflammation and joint destruction brought on by degeneration of a joint.
tendinitis: pain in the knee which worsens when climbing, taking stairs, or walking up an incline.
bursitis: inflammation caused by repeated overuse or trauma of the knee.
chondromalacia patella: damaged cartilage under the kneecap.
gout: arthritis brought on by the buildup of uric acid.
Baker’s cyst: a buildup of synovial fluid, fluid which lubricates the joint, supporting the knee.
rheumatoid arthritis, or RA: a chronic autoimmune inflammatory disease that causes painful swelling, joint deformity and bone erosion.
dislocation: dislocation of the kneecap most commonly caused by trauma, damage or injury.
meniscus tear: a rupture in one or more of the soft tissues in the knee.
torn ligament: tear at one of the four ligaments in the knee, the most commonly injured ligament is the anterior cruciate ligament, or the ACL.
bone tumors: osteosarcoma, is the second most common bone cancer, which most commonly occurs in the knee.
Dr. Alex Jimenez’s Insight
While the hip and knee joints are capable of sustaining various degrees of stress when performing physical activities, trauma, damage or injury as well as the degeneration of these complex structures, can ultimately lead to knee and hip pain. The balance of the human body as a whole is fundamental towards overall health and wellness. Therefore, if an individual experiences hip or knee pain, the entire structure and function of their body can be tremendously affected. It’s important for a person with knee or hip pain to seek immediate medical attention from a qualified and experienced healthcare professional, such as a chiropractor or physical therapist, in order to restore the balance of their entire body.
Treatment for Knee and Hip Pain
The treatment of hip pain is based upon the cause. For many instances of trauma, damage or injury, rest is generally enough to enable the hip to heal. By way of instance, exercise-associated hip pain is normally eliminated within a couple of days. When you have arthritis, a healthcare professional may sometimes prescribe drugs and/or medications to help relieve stiffness and pain. Furthermore, your physician will refer you to a doctor who can provide additional information regarding the cause of your hip pain along with recommending an alternative treatment option, such as chiropractic care and physical therapeutics, that will explain to you how you can perform rehabilitation exercises to help maintain joint strength, mobility and flexibility.
For injuries, therapy typically involves bed rest and the use of drugs and/or medications, such as naproxen, to alleviate pain, swelling and stiffness. Hip fractures, malformation of the hip and some injuries may require surgical intervention to repair or replace the hip. In hip replacement surgery, a surgeon will replace a broken hip joint with an artificial one. Although hip replacement surgery will need rehabilitation to become accustomed to the new joint, this type of treatment option is often considered.
Alternative Treatment Options
Some holistic remedies can offer relief from hip pain. Make certain you discuss treatment options with your doctor before considering any treatment option. Potential alternative treatment options include visiting a chiropractor for a spinal adjustment or manual manipulation. Chiropractic care is a well-known treatment approach which focuses on the diagnosis, treatment and prevention of a variety of injuries and/or conditions associated with the musculoskeletal and nervous system. Chiropractic care can help carefully re-align the spine as well as help reduce pain and discomfort, improve swelling and inflammation and even increase strength, flexibility and mobility on other structures of the human body. Physical therapeutics can also help treat both hip and knee pain.
There are many benefits of physical therapeutics, including increased range of motion, reduction of pain, less inflammation and swelling, as well as an overall improvement of quality of life. The first steps a chiropractor or physical therapist will perform if you have hip pain will consist of tests, such as a gait evaluation, range of motion measurement and intensity measurements. Afterwards, the healthcare professional will create a personalized treatment program. Treatment techniques may also include ultrasound and ice. There will also be specific exercises and stretches to help boost hip strength, mobility and flexibility to decrease pain. For knee pain, tests are also done along with active and passive treatments. Chiropractic care and physical therapeutics can help promote healing without the need for drugs and/or medications, and surgical interventions.
Bursitis, a frequent cause of knee pain, can be treated in the following ways:
Ice the knee for 15 minutes once an hour for three of four hours. Do not apply the ice directly to the knee, instead, cover your knee with a cotton towel. Put ice in a plastic zip-close bag, then place the bag on the towel.
Wear cushioned, flat shoes that support your toes and do not worsen your pain.
Avoid sleeping on your side. Use cushions positioned on both sides of your body to keep you from rolling on your side. When lying on the side, keep a pillow between your knees.
Stay seated when possible. Should you need to stand, prevent hard surfaces and maintain your weight evenly distributed on both legs.
Participate or engage in weight loss programs and strategies to lose weight if you are overweight or obese, to reduce the amount of stress that is placed on the knees.
If you are experiencing hip pain, knee pain or some other type of joint pain, make sure to contact a qualified healthcare professional, in order to receive a proper diagnosis to begin the best treatment approach for your specific health issue. Trained and skilled doctors will take you on the path to better healing. Make sure you prepare a one-on-one consultation to acquire a comprehensive examination and say good-bye to your pain. Healthcare professionals are devoted to providing you with a healthy and wholesome lifestyle.�The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Back Pain
Back pain is one of the most prevalent causes for disability and missed days at work worldwide. As a matter of fact, back pain has been attributed as the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience some type of back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
Patellofemoral pain is an extremely common and disabling condition that affects both men and women of all ages. Functionally it limits everyday movements and activities such as squats, lunging, walking up stairs and hills. It has been suggested and research concludes that dysfunction between the Vastus Medialis Oblique (VMO) and the Vastus Lateralis is one of the common predisposing factors that precedes patellofemoral pain.
The anatomical structure of the patella and the groove in the femur (trochlear groove) dictate that if the patella does not sit within the groove perfectly, then the hard edge of the lateral femoral condyle will contact the undersurface of the patella and create a pressure area that begins to wear down the cartilage structure of the patella and femur. Dysfunction of the VMO creates the situation whereby the patella is not able to be centralised in the groove and thus rides up on the lateral femoral condyle.
Physiotherapists, Chiropractors and exercise professionals have for decades been utilising VMO exercises in the treatment of patellofemoral pain.
Some of these exercises have been validated as effective VMO exercises and others have not.This month the focus of this research review is on VMO activity in rehabilitation exercises and also the validation that VMO dysfunction is associated with patellofemoral pain. The first study from Stanford University in California (Pal et al 2011) studied the relationship between VM activation delay and patellar tracking measures in different groups of knee pain patients. They hoped to find that measures of patellar tracking, patellar tilt and bisect offset correlate with VM activation delay in patellofemoral pain patients labelled as lateral maltrackers.
They selected 40 subjects who had suffered for more than 3 months with patellofemoral pain.
They had to have had pain on at least 2 of the following provoking movements � stairs, kneeling, squatting, prolonged sitting and isometric quadriceps contraction. They also selected 15 active, painfree control subjects. The subjects were initially studied in a motion analysis laboratory whilst walking and jogging. From this they collected data on ground reaction force and also the EMG data of the quadriceps was measured during leg swing phase before heel strike. Heel strike was the start of the measurement period and they continued to collect EMG data between the VM and VL during stance phase.
The researchers then measured the EMG signals from the VM and VL in all 55 subjects whilst performing isometric quadriceps contractions to generate �normal� data on each individuals maximum VM and VL activation. The isometric contraction was performed with the subject seated and the knee flexed to 80 degrees and they contracted against the resistance of the examiner. Magnetic resonance images of the subject�s knee in standing with the knee flexed to 5 degrees was also undertaken. From this they could evaluate the relative position of the patella in relation to the femur. They looked at the patella
The research papers
1. Pal et al (2011) Patellar maltracking correlates with vastus medialis
activation delay in patellofemoral pain patients. American Journal of Sports
Medicine. 39(3). 590-598.
2. Sousa A and Macedo R (2010) Effect of the contraction of medial rotators of the
tibia on the electromyographic activity of vastus medialis and vastus lateralis.
Journal of Electromyography and Kinesiology. 20: 967-972.
3. Irish et al (2010) The effect of closed kinetic chain exercises and open kinetic
chain exercise on the muscle activity of vastus medialis oblique and vastus
lateralis. Journal of Strength and Conditoning Research. 24(5): 1256-1262.
bisect offset value (which is how far lateral the patella sits relative to the midline of the femur) as well as patella tilt angle which is a measure of the lateral rotation of the patella in relation to the femur. From this data they statistically compared the VL/VM activation during walking and running between 5 groups; pain free controls, all patellofemoral pain patients, patellofemoral pain patients classified as normal trackers, patellofemoral pain patients who were maltrackers either with the patella tilt or the patella bisect offset and those with both tilt and offset. What they discovered was that subjects with both patella tilt and bisect offset as shown on MRI had the greatest and significant differences in VM activation delay. Interestingly, from the 40 subjects with patellofemoral pain, 7 were maltrackers with either a tilt or bisect abnormality whereas 8 had both. The other 25 pain subjects did not show tilt or bisect abnormalities. But when the painfree normal subjects were compared as a group to the pain group, there existed no significant correlation between the groups in VM activation delay in both walking and running. The second study from Portugal (Sousa and Macedo 2010)
approached VM/VL activation in a novel way. They compared maximum quadriceps contraction and the VM/VL ratio between normal quadriceps contraction and quadriceps contraction with resisted tibial medial rotation. The hypothesis was that activation of the medial tibia rotators would increase the VM/VL ratio favourably to recruit the VM over the VL. They selected 24 normal healthy females to participate in the study, all of whom had no injury to the knee, were not athletes and had a Q angle of 14-17 degrees. They had the subjects perform 4 series of contractions with 3 repetitions of each � a total of 12 maximum contractions held for 5 seconds with a 2 min rest. They randomised the sequence of contractions to avoid the fatigue effect. The 4 series were, isometric quadriceps contraction, isometric with forced medial tibial rotation with the tibia internally rotated, neutral rotation and externally rotated.
They found that significant differences existed between VM/VL ration with no tibial rotation and with forced activation of tibial rotators. It did not matter if the leg was medially rotated, neutral or externally rotated, contraction of the medial tibial rotators preferentially recruited VM over VL during isometric quadriceps contraction. The final study from Plymouth in the United Kingdom assessed the VM/VL activation in 3 commonly used rehabilitation exercises – leg extension, squat with resisted adduction and lunge. They selected 22 healthy asymptomatic subjects (11 men and 11 women) to perform the series of exercises. They initially collected normalised data for maximum EMG activity by
performing repeat maximal isometric quadriceps contractions at 45 degrees of knee flexion. This was done over three trials. They then had the subjects perform 3 trials of the following exercises; 1. Knee extension � seated and contracting the thigh with the knee from 90 degrees to full extension. 2. Double leg squat with isometric hip adduction. With the back flat against a wall and a pillow between the knees, the subject squatted to 45 degrees with constant pressure against the pillow. 3. Lunge exercise. Standing in a stride stance position the knee was flexed to 45 degrees followed by a return to full extension.
What they found was that the squat with the pillow and the lunge produced a greater VM/VL ratio than knee extension. There was no difference between the squat and the lunge with VM/ VL ratio, but the squat showed greater VM activation than the lunge. Furthermore, the leg extension showed greater VL than VM activation. The lunge
exercise showed the best idealised ratio of 1.1 with the VM/VL. Swimmers who covered more than 35 km in training were 4 times more likely to have tendinopathy than those who swam less.
Need to know Is any of it really new?
The first study from Stanford University is the first study to look at standing MRI images of patella position and have this correlated with EMG data for VM activation
delay during walking and running. Previous studies had looked at supine MRI of the patella with the leg relaxed. The patella engages the trochlear groove at 30 degrees knee bend so patients suffering from patellofemoral pain tend to notice their pain once the patella engages into the groove.
By investigating the patella position in standing, it would more approximate what the patella does in weightbearing activities such as walking.
The UK study is one of the first to have studied the VM/VL ratio in a lunge position. Considering that this is a commonly used rehabilitation exercise, it adds to the evidence of the effectiveness of this exercise as a useful rehabilitation exercise for patellofemoral pain.
Does it challenge the consensus? The Australian EMG study does challenge previous research that If anything, the Standford University study demonstrates that evidence for patella maltracking and patellofemoral pain is in fact quite unrelated. Many of the subjects who suffered patellofemoral pain had normal patella tracking on MRI imaging.
Any clinical implications? Absolutely. If patellofemoral pain and patella maltracking and VM onset is only loosely correlated, then perhaps many of the causes of patellofemoral pain are unrelated to poorly functioning VM and patella maltracking. Perhaps reasons as simple as tight overall quadriceps which may increase the compression force between the patella and femur in knee flexion may be a simpler explanation. The study from Portugal adds another dimension to VMO rehabilitation. By actively internally rotating the tibia (even isometrically) the VM increases its activity. The suggestion is that the VMO also acts as a tibial internal rotator due to its position on the medial patella. However, they measured the activity at 90 degrees knee flexion, a position not suitable for painful knees and post-operative knees. The UK study adds further credibility to the understanding that closed kinetic chain exercises are more favourable for knee rehabilitation than open kinetic chain exercises. Possibly the lunge is a better exercise for gaining preferential 1.1 ratio of activation but the squat with the isometric hip adduction may be better if the goal is to selectively activate the VM.
Any loose ends? Unfortunately for the Stanford University study, the MRI images of the patella were only taken at 5 degrees knee flexion and not 30 degrees. It would be interesting to view the patella position at greater angles of knee bend whilst standing. Furthermore, it cannot be concluded that what a patella to femur relationship looks like in standing is the same as what happens in walking/running. Due the impact of gait on the limb, perhaps the patella maltracking may be more pronounced due to the influence of the supporting soft tissues such as VL, ITB and also hip joint position. Furthermore, the Stanford University study did not differentiate from the EMG data if the activity was from the Vastus Medialis Obliquus (VMO) or the entire VM. Perhaps with more defined EMG analysis of the VMO � which has been shown to be a significant patella stabilizer � the correlation between VM delay and knee pain may have been more pronounced. It would be interesting if the Portuguese study also looked at their study with the knee flexed to 60 and 30 degrees knee flexion.
Perhaps the knee angle plays a large part on selective activation of the VM when the tibial rotators are activated. Furthermore, they did not specify how much force was placed on the tibia to be resisted for the medial rotation. This may also have a bearing in the clinical setting. Similar to the Portuguese study, the UK study only looked at the effect of the exercises on normal subjects. Would the results have been different in patients with patellofemoral pain?
Individuals with a previous knee injury often describe feeling continuous symptoms for an extended period of time after the original trauma. Fortunately, the majority of knee injuries usually involve minor damage and injury to the ligaments of the knee. Most knee complications that chiropractic doctors and other medical specialists diagnose are often caused by stiffness and soreness that, when�
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine