If you are an active amateur or a competitive runner, using the services of a chiropractor can make a vast change in your overall health, reduce your pain from injuries and improve your alignment for a more effective run.
Chiropractors are excellent when it comes to rehabilitation, and they can help you keep your body in top condition as an athlete. All sports is an area that chiropractors can specialize in, focusing their training and experience on targeted treatments for runners.
Recovering from Sports Injury/s
Most athletes get injured at one point or another in their career, whether it is while participating in their sport or an accident in their daily lives. Recovery from an injury can be difficult at times, and even after hours of physical therapy, you may feel that you aren’t ready to start training again.
Physical therapy is a great help in recovering strength in soft tissue and muscle after an injury or surgery. However, sports-medicine trained chiropractors can improve the mobility of your joints after an injury. Sports chiropractors work with the soft tissue in conjunction with the joints in a coordinated fashion. An examination will take a look at:
After the examination, the sports chiropractor will assess the runner to recommend treatment.
People running fast in a city marathon on street
Sports Chiropractic
According to U.S. News and World Report, there are four primary chiropractic treatments for running injuries.
Active Release Technique (ART) – combines massage and stretching by applying deep tension while moving a joint through its range of motion. This treatment is used primarily for adhesions in the muscle.
Graston Technique – used to break down surface-level scar tissue with hand-held stainless steel tools.
Functional Dry Needling – releases tension in trigger points through deep muscle stimulation with needles. This treatment can help the psoas muscle, a hip flexor muscle.
Electrical Muscle Stimulation (EMS) – releases tension through the stimulation of surface muscles.
General Adjustments
Chiropractors are trained to look at the whole body and align it for optimum balance. Many runners find it beneficial to have regular periodic adjustments to regain their body’s balance from daily stress and the impact of running. Aligning the body can relieve tension or pain that is caused by misalignment before it becomes more than a minor impediment.
Runners may not even realize that the tension they feel is the beginning of pain caused by being out of balance until it is adjusted. Chiropractic adjustments are often part and parcel of a runner’s training program to strengthen and improve performance. They can also help recover from pregnancy and postpartum bodily changes.
Prevents Injury and Promotes Optimal Performance
With regular care of a sports-trained chiropractor, runners can actually prevent injury and promote optimal performance by keeping their bodies fine-tuned, working at maximum capacity. A trained chiropractor can find imbalances that may lead to injury and correct them before they become a problem. With your body in perfect balance, muscles and joints work more efficiently, powering up your performance as a runner and making the most of your body’s resources.
Misalignment can be caused by many common runners� experiences including running on the same type of surface every day, running on a slanted surface such as a beach or replacing running shoes too infrequently. As a runner, you can work to vary your running surfaces and keep a better watch on your shoes, but your chiropractor will let you know if your body is in need of more balance.
To learn more or to schedule an appointment, please give us a call at the number provided at the top of this website. We’re here to help!
Red Flags of foot *PRONATION* | El Paso, Tx
Feet: A foundation for pain
99% of feet are normal at birth. But after the first year, 8% develop foot problems, 41% by age 5 and 80% by age 20. By age 40, almost everyone has a foot condition of some sort. Many foot conditions eventually contribute to health concerns, especially the generalized condition of �back pain� or runner�s knee. Spotting a potential problem originating in the feet can prevent other injuries from affecting your health and lifestyle.
Runners who are able to avoid injury are those who land the lightest on their feet, which sustains the lowest levels of impact. Researchers suggest that runners think about landing more softly and adjust their stride so that they land closer to the midfoot.
But that is easier said than done, as most runners tend to be heel-strikers.
Runners with excessive pronation that try to transition to a forefoot strike pattern could be more susceptible to inner foot and ankle injuries.
Runners with high arches who attempt to transition to a forefoot strike pattern are prone to suffer sprained ankles and metatarsal stress fractures.
Running can lead to a number of different injuries
Sudden trauma
Developed over time from microtrauma
Biomechanical errors
Structural asymmetries
Tissue weaknesses
Excessive external loads
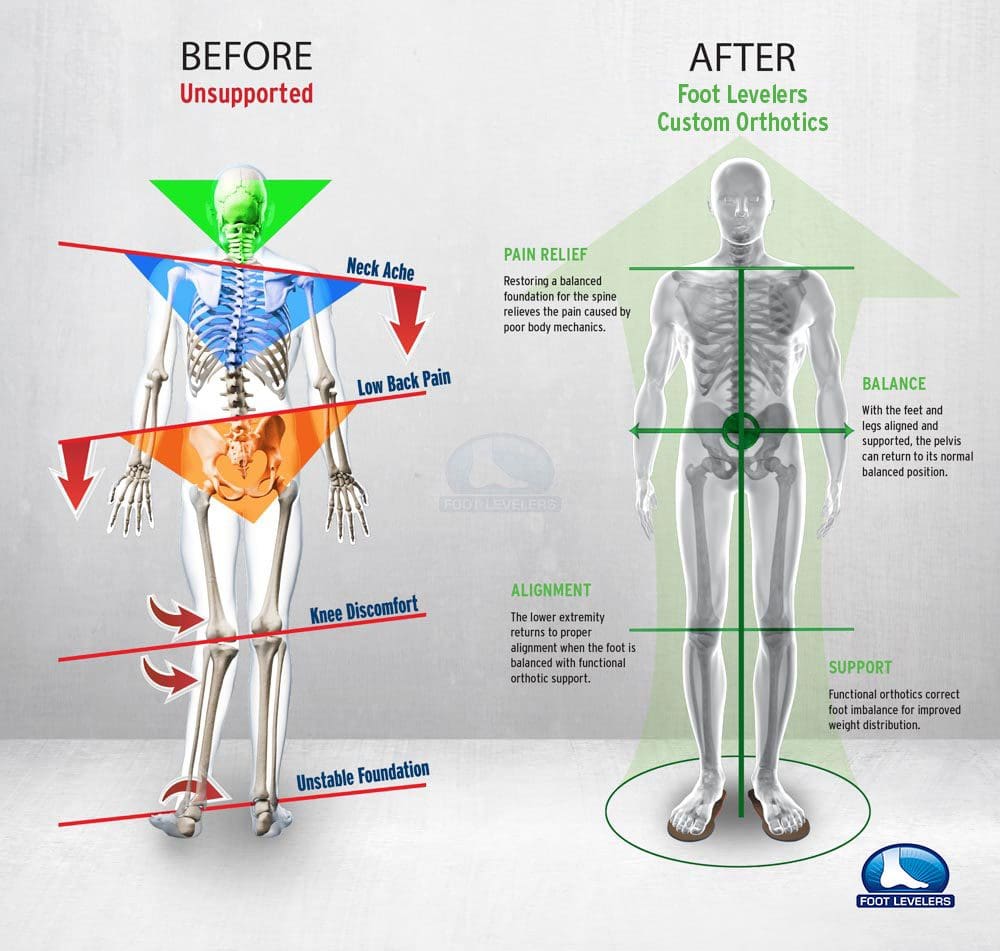
Runners do their best to treat pain through stretching or exercises that target the area that hurts, but sometimes the source of the pain might actually be elsewhere. That source is foot imbalance.
Custom orthotics improve biomechanics
Custom orthotics are used to align and support the foot/ankle complex in a more near-normal physiologic position for a weight-bearing foot to prevent dysfunction and/or improve the function of movable body parts.[3] They are indicated to:
Creates a symmetrical foundation by blocking pronation or support supination
Provides heel strike shock absorption
Inhibits serial biomechanical stress
Enhances neuromuscular re-education
Custom-made orthotics that use viscoelastic materials can help to reduce the musculoskeletal impact from heel strikes when running.
This shock absorption can be of help particularly when there is instability, chronic degeneration, or inflammatory arthritis in the joints.
Orthotics are designed specifically to cushion foot impact and reduce pain triggers.
Everyone is misaligned
Patellofemoral pain care
Understanding the exact mechanical contributions of the knee is critical for the therapist to effectively manage injuries or conditions.
NCBI Resources
These injuries and conditions affect runners, cross fitters, group exercise enthusiasts (PUMP classes) and simple recreational walkers who spend a lot of time on hills and stairs.
You need to understand your feet! Flat feet, foot pronation, and foot imbalances can lead to all kinds of pain:
Knee pain
Hip pain
Back pain
Yes even Shoulder pain
If you are considering custom orthotics, a health care professional such as Doctor Jimenez and Injury Medical Chiropractic Clinic can perform a foot scan to show you what imbalances in the feet can lead to. The foot scan will show how the orthotics can help. Following the foot scan, a report will provide the caregiver a Pronation/Stability Index, Foot Assessment, and Body Assessment.
Pronation & Stability
The Pronation/Stability Index� score appears on the clinical report that is produced when your feet are scanned by our 3D machine.
The Pronation/Stability Index� is an algorithm based on 16 different measurements. Taken from a laser scan of the feet, the index indicates the amount of arch collapse. The higher the number, the more collapse.
The index reveals the severity of pronation/stability of your feet, which can be anywhere from optimal to severe. An index of 102, for example, is a moderate pronation/instability. Untreated imbalances at any level can lead to chronic problems.
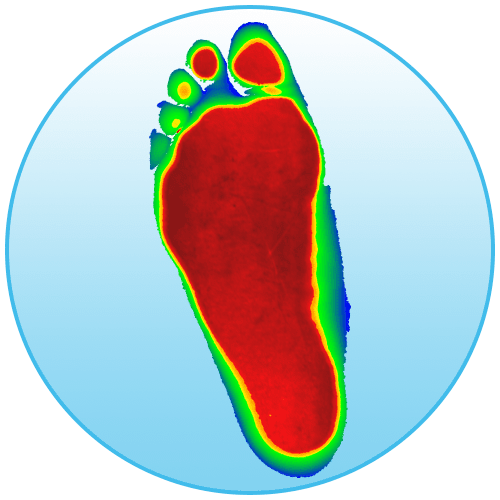
Optimal Feet
This image shows what the optimal foot looks like.
The red areas represent where pressure on your foot should be:
The toes
The balls of the foot
The heel
Unfortunately, 99% of feet do not look like this.
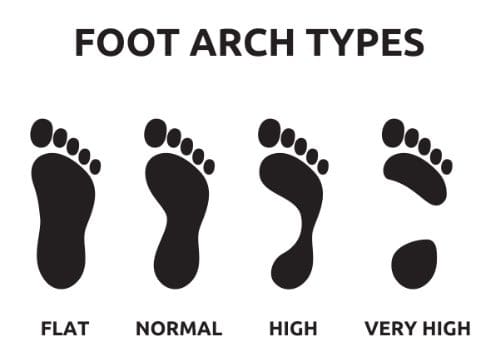
Flat Feet
This image shows what flat feet look like. Here, all three arches of the foot have collapsed. Once the arches collapse it throws the rest of the body off. So when you move there is a higher risk for pain. This includes pain in the feet, knees, hips, back, and neck.
The Body
The body image shows imbalances in the feet and how they can lead to knee rotation, pelvic tilt and shoulder drop.
Throughout our lives, we need some type of support for our feet. After all, they take all of our weight, so let’s treat them right and understand your feet.
El Paso Back Clinic
NCBI Resources
Effective footwear can make a huge difference. Especially when it comes to being able to stand and walk in a comfortable manner.
The human body is an intricate machine; everything is connected in one way or another. This means that when one part is not functioning as it should, it can throw everything out of balance. The relationship between the feet, back, and hips is significant, so when there is a problem with feet, it can cause pain in those areas. Fallen arches are�a foot problem that is a prevalent cause of lower back pain. However, many people who have fallen arches don�t even realize that they have an issue.
What are Fallen Arches?
There are more than 100 ligaments and muscles in the foot that stabilize the bones and keep everything in the proper position. Ligaments prevent joints from extending beyond their intended limits. They contain elastin which allows them to act much like a rubber band, stretching with movement or flexion then returning to their regular length when the joint returns to its resting position.
There are a�variety of things that can happen that cause those ligaments to stretch, causing them to lose their ability to support the foot as they should. This can lead to pes planus (flat feet), also known as fallen arches.
Most people don�t realize that there are three arches in the foot, not just one: lateral, medial, and anterior. They act as shock absorbers for the body. When they don�t function as they should, don�t absorb the shock of movement and activity, it puts added wear and tear on the body. While foot, knee, hip, and back pain is common with fallen arches, it also is a major cause of impaired functioning of the lower extremities. It can also lead to balance problems.
Causes of Fallen Arches
The primary cause of fallen arches is improper footwear. Shoes that do not adequately support your foot and arch can lead to structural problems.
Other causes of fallen arches include:
Tendons in the foot that are torn or stretched
Certain health conditions including
Rheumatoid arthritis
Pregnancy
Diabetes
Obesity
Aging
Structural abnormalities that are present from birth
Inflammation, deformity, or damage of the posterior tibial tendon that runs from the middle of the arch to the lower leg, running along the ankle
Nerve issues
Bones that are dislocated or broken
Recognizing the symptoms of fallen arches and knowing that you have a problem can help to prevent the pain but can also arrest further damage to the foot.
Do you have Fallen Arches?
While many people with fallen arches experience no symptoms or problems, others do. If you experience any of these symptoms of flat feet, it should prompt a visit to your doctor.
Pain in the foot, knee, leg, hip, or lower back
Feet that easily get tired
Difficulty with balance
Swelling on the bottom of the foot
Pain or achiness in the foot, particularly in the heel or arch
Certain movements. such as standing on tiptoe, are difficult
There is a quick, simple test that you can do at home to see if you have fallen arches:
Wet your feet
Stand on a flat, hard surface, such as a floor or concrete pad (you need to be able to see your footprint) or walk in soft soil or sand
Look at your footprints. If you see a print that shows the heel and ball of your foot with a thin, curved imprint running along the outside, then your foot structure is normal. If you can see the print of your entire foot, then you probably have fallen arches.
The problem with fallen arches is that the damage cannot be reversed once it begins. However, the progression can be stopped with proper treatment.
What are the Treatments for Fallen Arches?
The treatment for fallen arches depends on the cause and severity of the condition. If it isn�t causing pain or other problems, the doctor may elect to do nothing.
However, if there are pain or mobility issues present, treatments may include bracing, prescribing NSAIDs for pain and inflammation, and even surgery in some cases of torn tendons or broken bones. An increasingly popular treatment for fallen arches is chiropractic care. This natural, non-invasive therapy treats the whole body so that it addresses the cause of the condition as well as associated risk factors and helps patients manage the pain, significantly improving their quality of life.
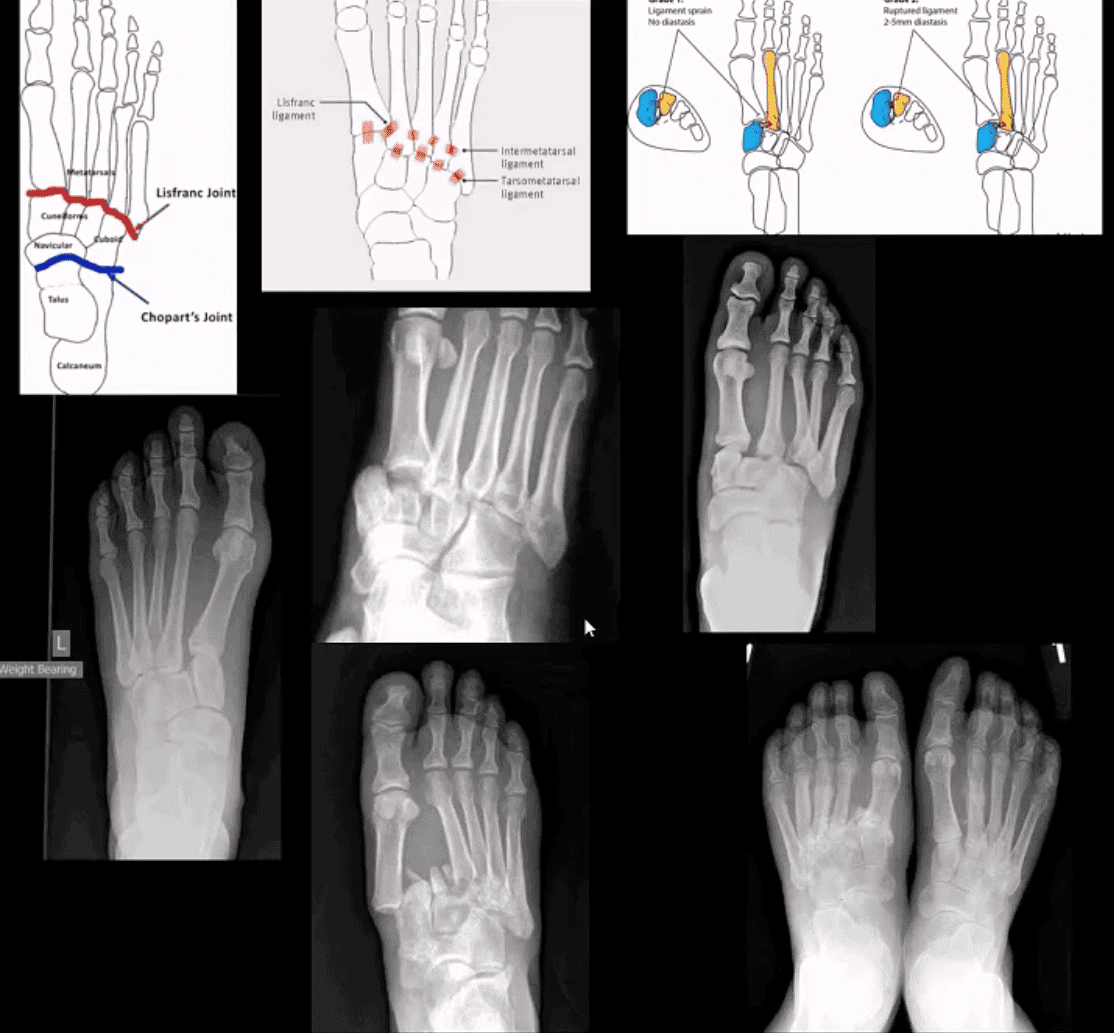
M/C dislocation of the foot at tarsal-metatarsal articulation (Lisfranc joint). Direct impact or landing and plantar or dorsal flexing the foot. Lisfranc ligament holding 2nd MT base and 1st Cu is torn. Manifests with or w/o fracture-avulsion.
Imaging: 1st step: foot radiography in most cases sufficient to Dx. MSK US may help: show disrupted Cu1-Cu2. Ligament and widened space > 2.5mm. MRI may help but not essential. Weight-bearing view aids Dx.
2-types: homolateral (1st MTP joint in contact) and divergent (2-5 MT displaced laterally and 1st MT medially)
Management: operative fixation is crucial
N.B. Atraumatic Lisfranc dislocation is a frequent complication of a diabetic Charcot foot
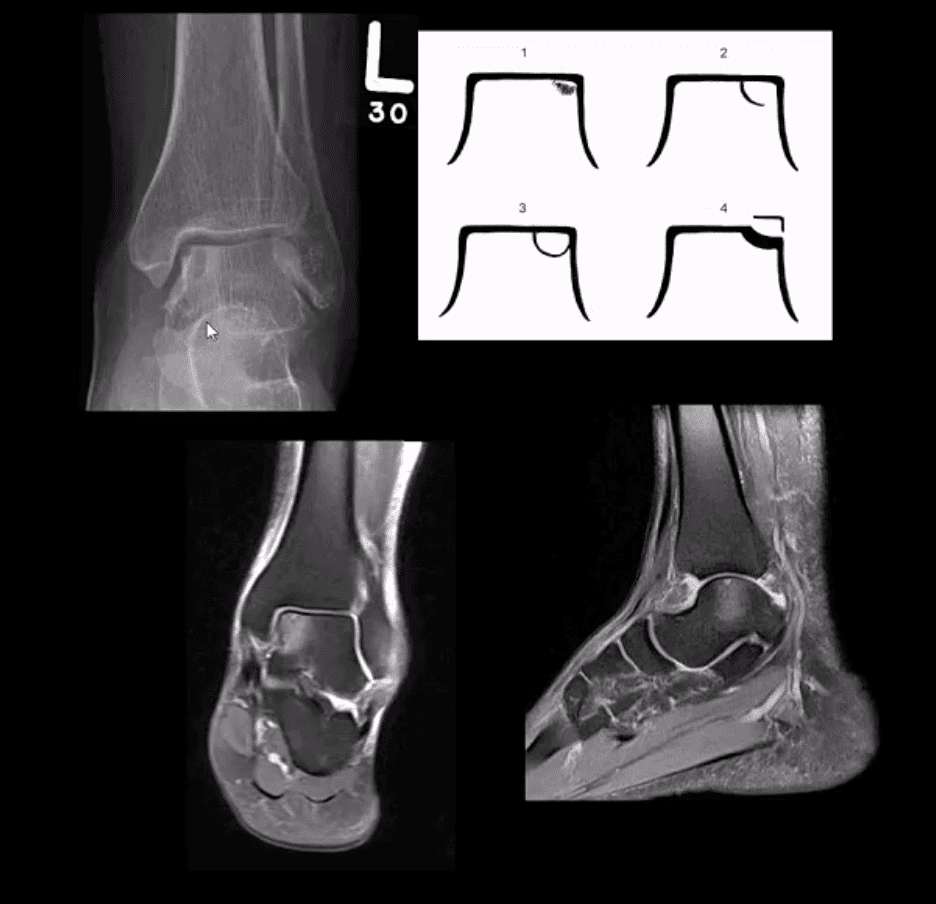
Osteochondral Injury of the Talus (OCD)
Common. Non-traumatic found in superior-medial talar dome. Traumatic may affect supero-lateral dome.
Clinically: pain/effusion/locking. Imaging is crucial.
1st step: radiography may reveal focal radiolucent concavity/halo, fragment.
MRI helpful esp. if OCD is cartilaginous and to demonstrate bone edema.
Jones Fx: extra-articular Fx of proximal metaphysis of the 5th MT. Prone to non-union. Often fixed operatively.
Pseudo-Jones: intra-articular avulsion of 5th MT styloid/base by eccentric contraction of Peroneus Brevis M. Managed conservatively: boot-cast immobilization. Both Jones & Pseudo-Jones Dx by foot series radiography.
Stress Fx. Calcaneus, 2nd, 3rd, 5th MTs. Repeated loading (running) or “March foot” 2nd/3rd MT. Clinically: pain on activity, reduced by rest. Dx: x-rays often unrewarding earlier. MRI or MSK US may help. Managed: Conservatively. Complications; progress into complete Fx
Turf toe: common athletic hyperextension of 1st MTP-sesamoid/plantar plate complex is tearing. 1st MTP unstable/loose. Managed operatively.
Arthritis of the Foot & Ankle
DJD of the ankle: uncommon a primary OA. Typically develops as 2nd to trauma/AVN, RA, CPPD, Hemophilic arthropathy, Juvenile Idiopathic Arthritis, etc. manifests as DJD: osteophytes, JSL, subchondral cysts all seen on x-rays
Inflammatory Arthritis: RA may develop in the ankle or any synovial joint. Will typically presents with symmetrical Hands/feet RA initially (2nd, 3rd MCP, wrists, MTPs in feet) usually with erosion, uniform JSL, juxta-articular osteopenia, and delayed subluxations.
HLA-B27 spondyloarthropathies: commonly affect lower extremity: heel, ankle esp in Reactive (Reiter). Erosive-productive bone proliferation is a crucial Dx.
Gouty Arthritis: common in the lower extremity. Ankle, mid-foot foot esp 1st MTPs. Initial onset: acute gouty arthritis with ST effusion and no erosions/tophi. Chronic tophaceous gout: peri-articular, intra-osseous punched-out erosions with over-hanging edges, no initial JSL/osteopenia, ST. Tophi may be seen.
Miscellaneous arthropathy: PVNS. Not common. Affects 3-4th decades of life. The result of synovial proliferation with Macrophages and multi-nucleated Giant Cells filled with hemosiderin and fatty accumulation may lead to inflammation, cartilage damage, extrinsic bone erosions. Dx: x-rays are insensity, MRI modality of choice. Synovial biopsy. Management: operative, can be difficult.
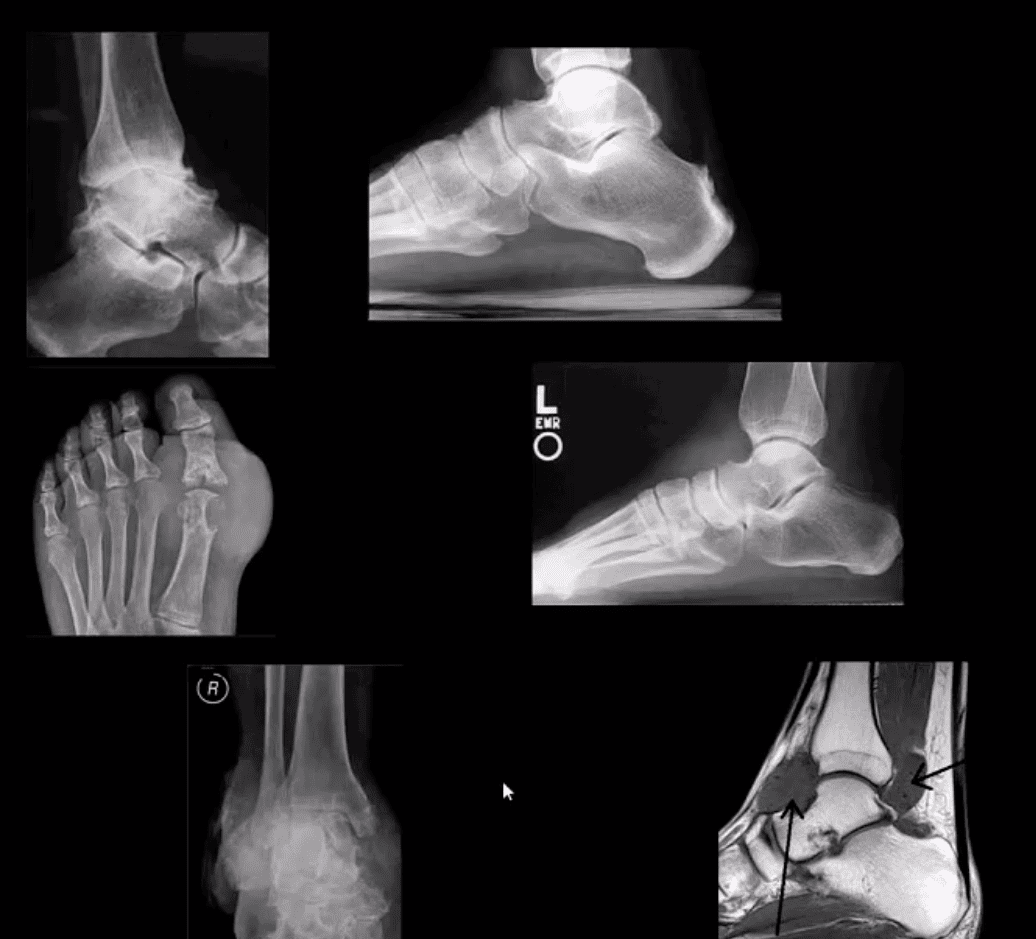
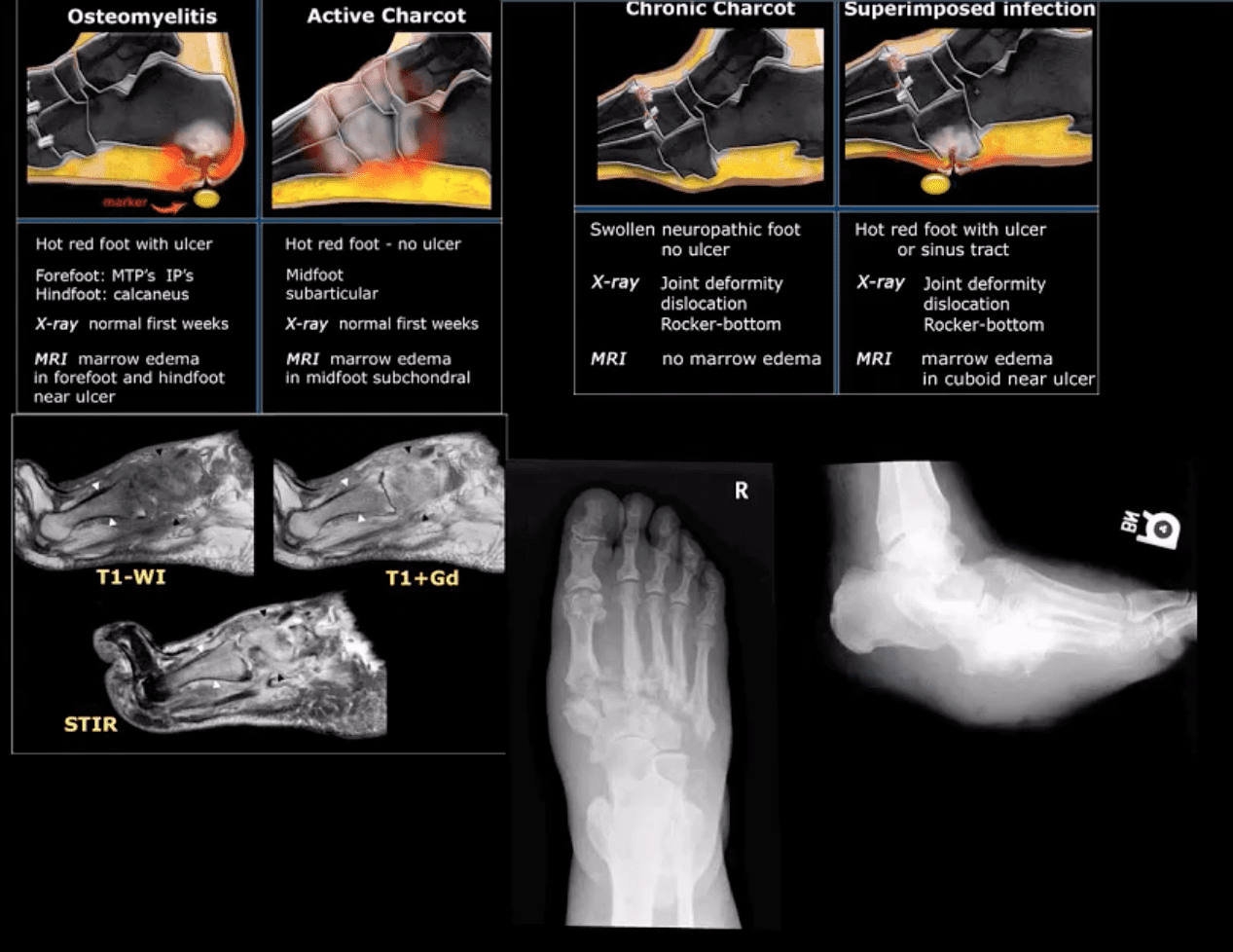
Neuropathic Osteoarthropathy
(Charcot’s joint) Common and on the rise d/t epidemic in type 2 DM. May present with pain initially (50% of cases) and painless destructive arthropathy as a late manifestation. Early Dx: delayed. Imaging is crucial: x-rays: initially unrewarding, some SF effusion is seen. MRI helps with early Dx and extremity off-loading. Late Dx: irreversible dislocations, collapse, disability. Note: Lisfrance dislocation in Charcot joint
M/C mid-foot (TM joint) in 40% of cases, ankle 15%. Progression: Rocker-bottom foot, ulcerations, infections, increased morbidity, and mortality.
Early Dx: by MRI is crucial. Suspect it in patients with type 2 DM especially if early non-traumatic foot/ankle pain reported.
10% of all fractures. 2nd m/c following femoral neck Fx. Demographics: active young males and older osteoporotic females
Stable Fx: overall prognosis is good
Unstable Fx: require ORIF. 15%-20% chances of 2nd OA.
Role of imaging is to determine the complexity, stability and care planning (i.e., operative vs. conservative)
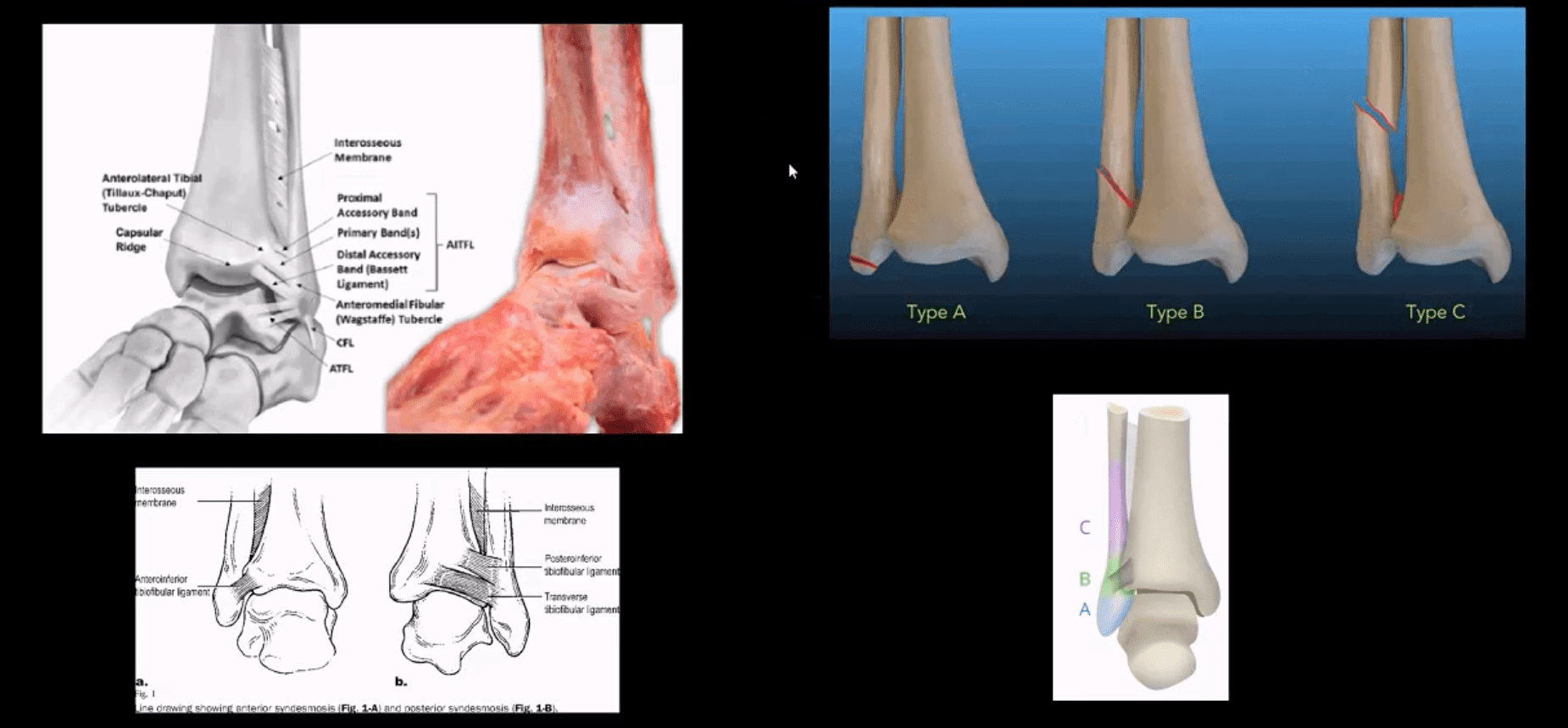
Weber classification considers tearing of distal tibial-fibular syndesmosis and potential instability
Weber A – below syndesmosis. Stable, typically avulsion of the distal fibular malleolus
Weber B – at the level of syndesmosis: may be outside syndesmosis and stable or tearing syndesmosis and unstable
Weber C – above syndesmosis. Always unstable d/t tearing of syndesmosis
Variations of fractures may involve the position/role of the talus bone during Fx (e.g., abduction, adduction, rotation, etc.) this is known as Lauge-Hanson classification
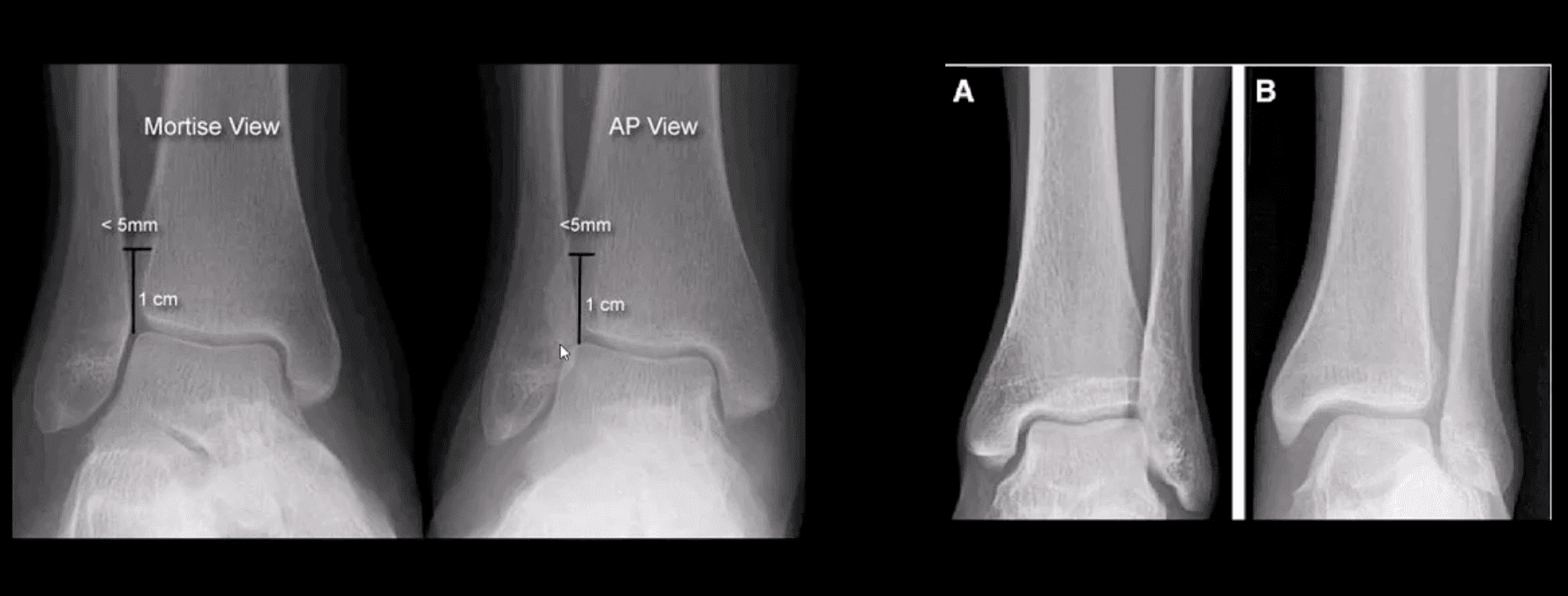
Reveal infrasyndesmotic Fx of fibular malleolus (Weber A)
Stable Injury
Conservative care in the form of short-leg walking cast/boot can be used. Good recovery. If no evidence of osteochondral injury, relatively low chances of post-traumatic OA
No further imaging required. MRI may help to reveal bone contusion and osteochondral injury
Weber B at Level of Syndesmosis
Can be stable or unstable. On occasions, the decision is made during operative exploration.
CT scanning may help with further evaluation
Management: depends on stability. Additional stabilization required if syndesmosis is ruptured
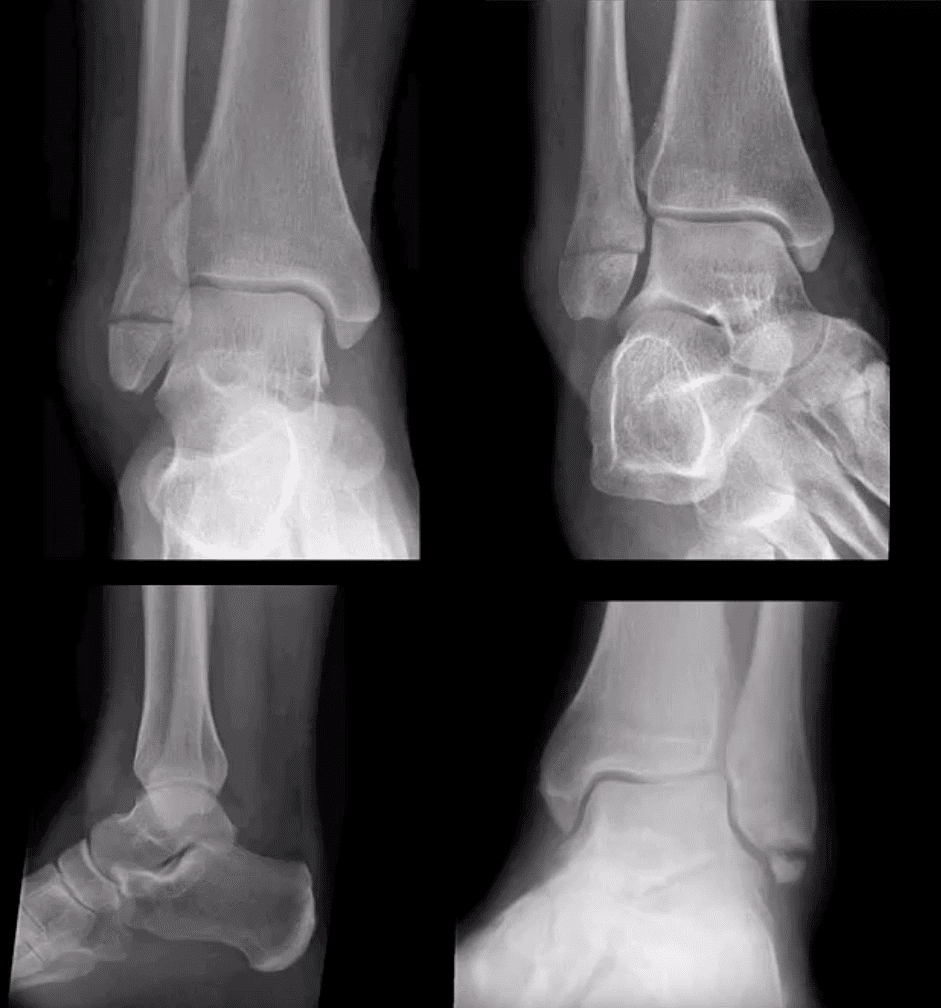
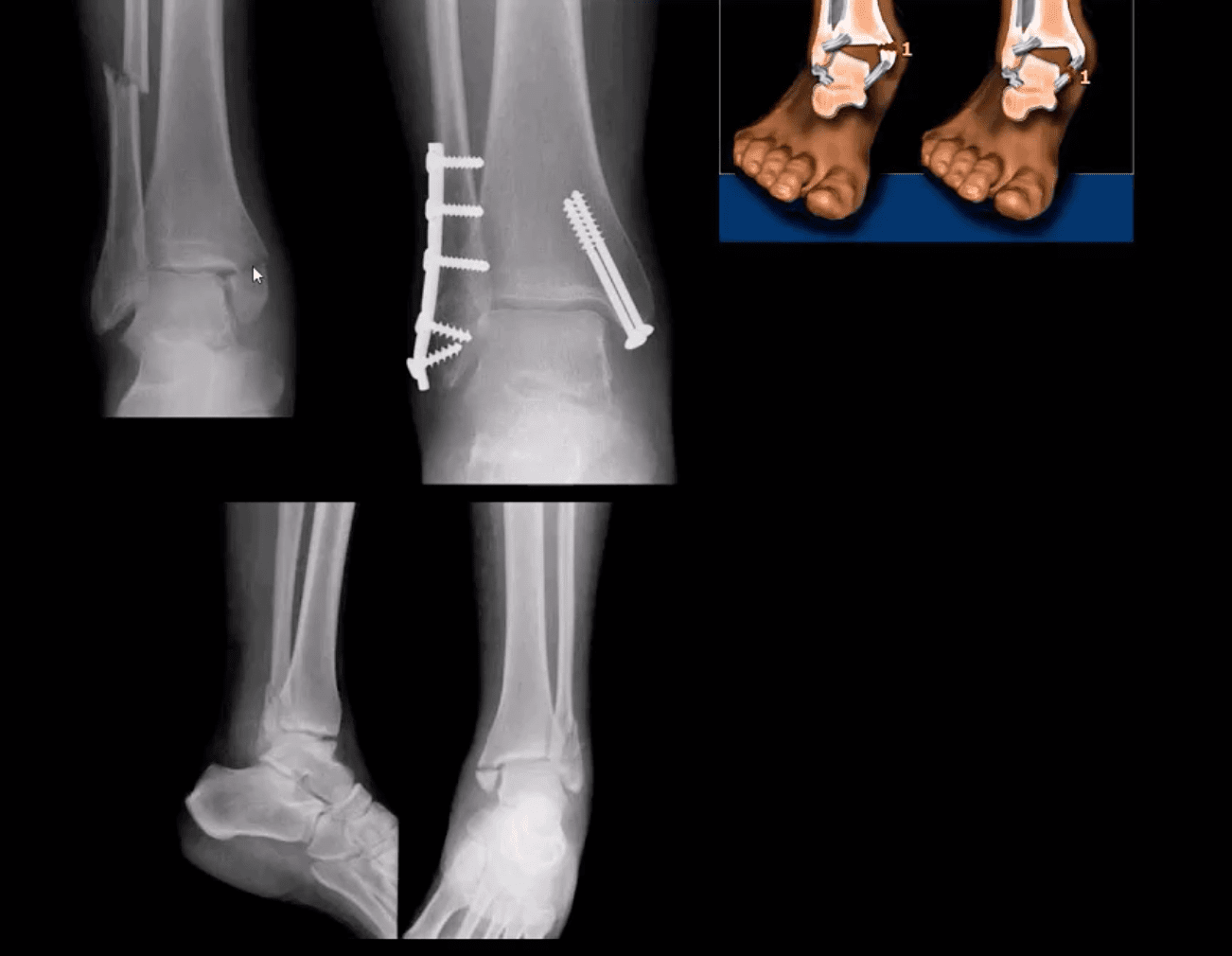
Weber C
AP, medial oblique and lateral views reveal Weber C – suprasyndesmotic injury with abnormal joint widening d/t disruption of the tib-fib syndesmosis. Very unstable injury.
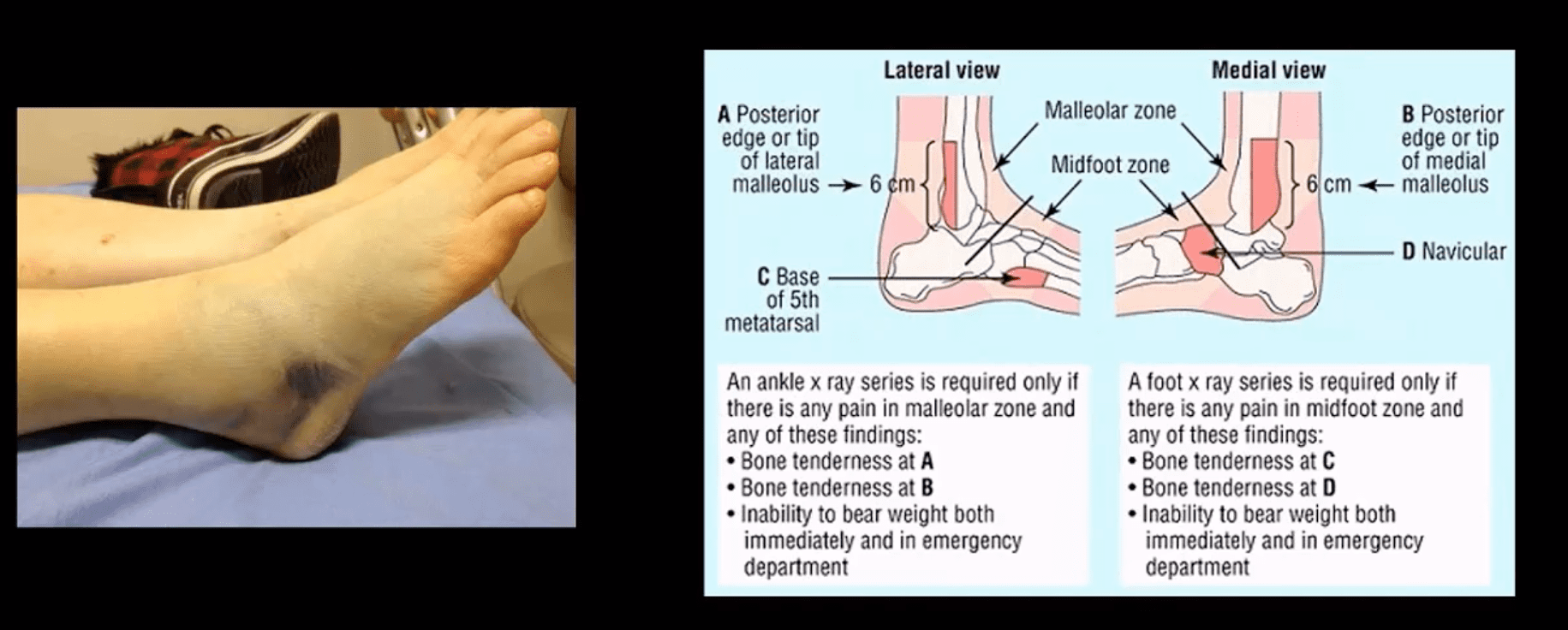
Occasionally, when Weber C Fx positioned 6-cm from the tip of the lateral malleolus, it may be termed as Pott’s ankle Fx (name after Percival Pott’s who has proposed the original classification of ankle fractures based on their stability and degree of rotation). The term is somewhat outdated.
Management: operative with additional stabilization of the syndesmosis
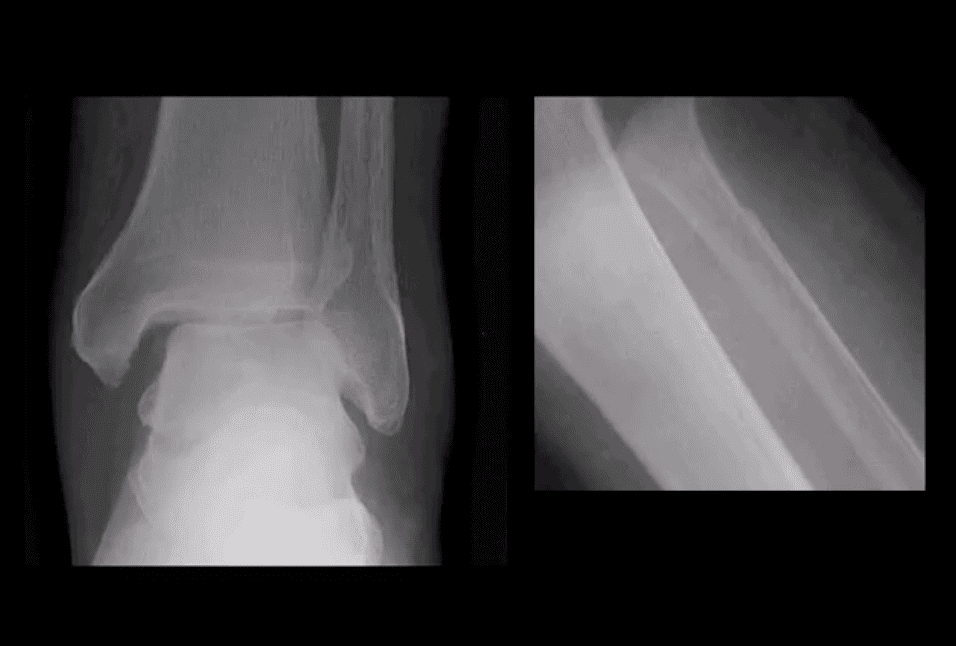
Maisonneuve Fracture
Often spiral fracture of the proximal fibula combined with an unstable ankle injury
No immediate ankle fracture is noted radiographically, thus can be missed on ankle views and require tibia and fibula views
Rad features: widening of the ankle d/t syndesmosis tear and sometimes deltoid ligament disruption. Interosseous membrane is torn with proximal fibular Fx caused by pronation with external-rotation force
Management: operative
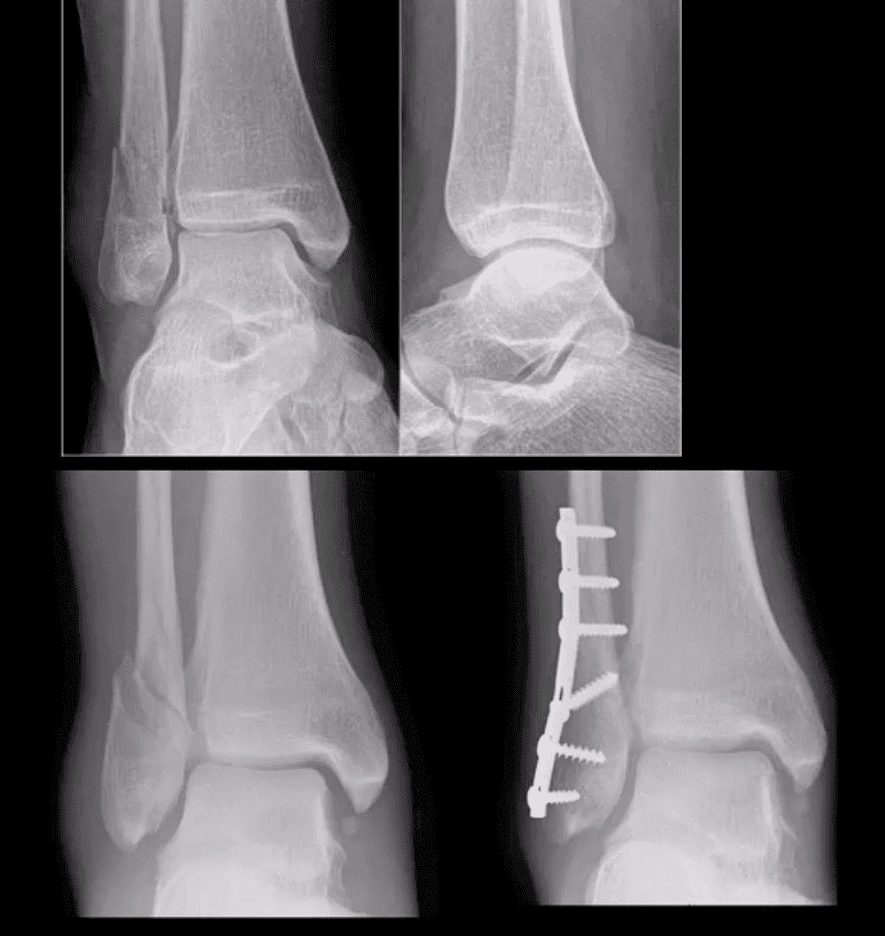
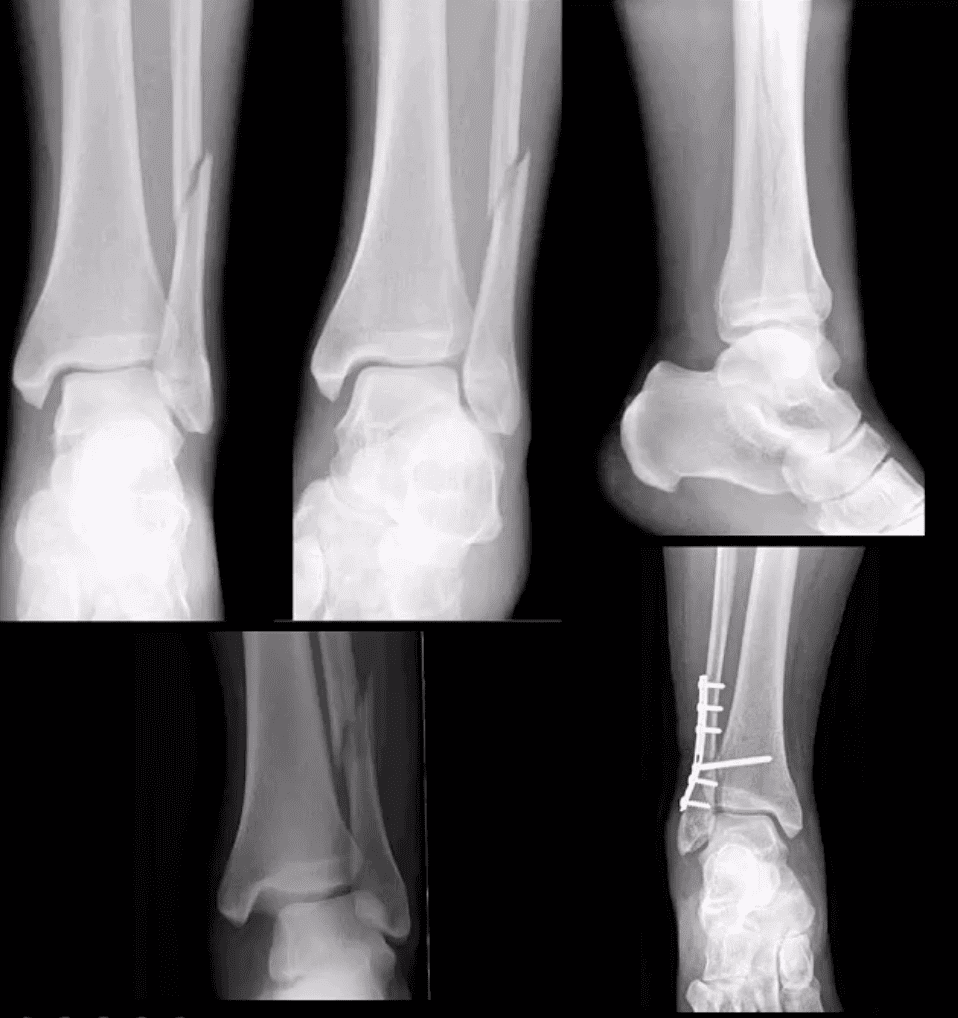
Bimalleolar & Trimalleolar Fx
Above top images Bimalleolar Fx v. unstable, the result of pronation and abduction/external rotation. Rx: ORIF.
Trimalleolar Fx: 3-parts ankle Fx. Medial and lateral malleolus and avulsion of the posterior aspect of tibial plafond. More unstable. Rx: operative
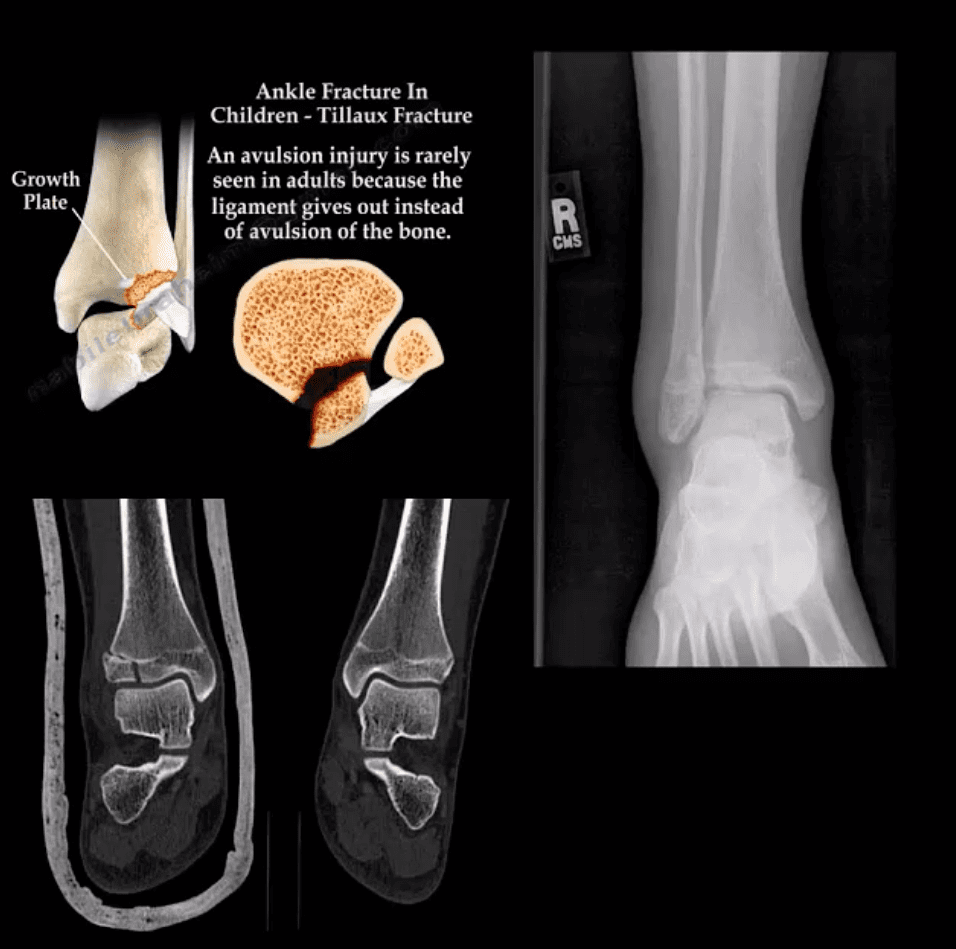
Tillaux Fx
Pediatric Fx affecting older child when the medial side of the physis is closed or about to close with lateral side till open. Avulsion by the anterior tibi-fibular ligament. Complications: 2nd dry/premature OA. Rx: can be conservative if stable by boot cast immobilization.
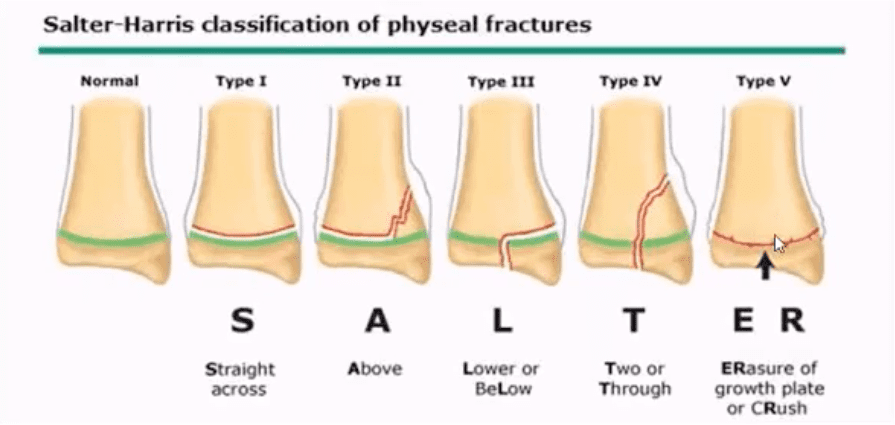
Pediatric Growth Plate Injuries
Salter-Harris classification helps to diagnose and prognosticate physeal injuries.
Helpful mnemonic: SALTR
S: type 1-slip through the growth plate
A: type 2-above, Fx extends into the metaphysis
L: type 3-lower, intra-articular Fx extends through the epiphysis
T: type4, “through” Fx extends through all: physis, metaphysis, and epiphysis.
R: type 5, “ruined.” Crush injury to physis leading to complete death of the growth plate
Type 1 and 5: present with no fracture
Type 2: has the best prognosis and considered the most common.
Management: referral to a pediatric orthopedic surgeon
Complications: early physis closure, limb shortening, premature OA and others.
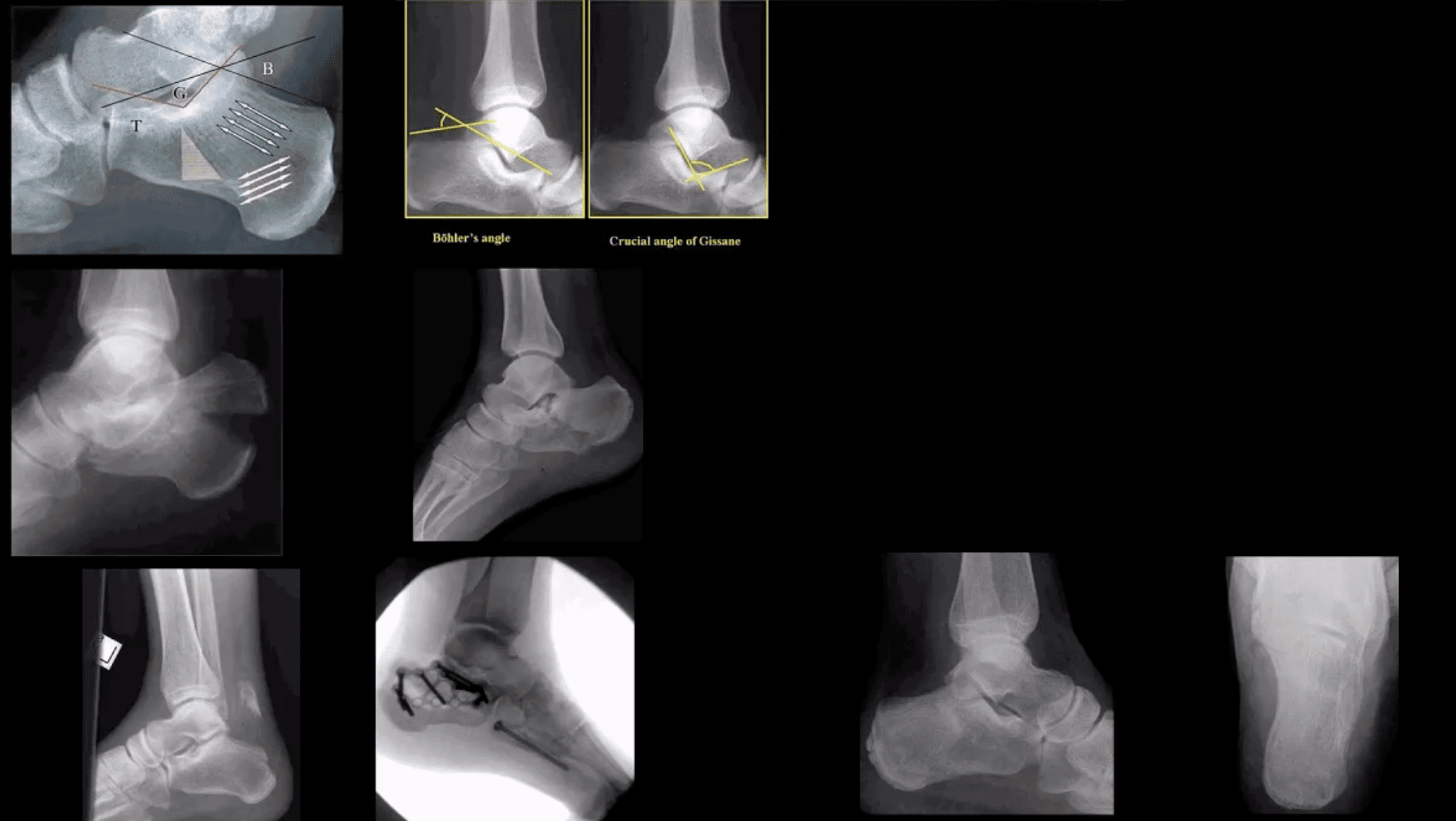
Calcaneal Fracture
Most frequent tarsal Fx. 17% open Fx
Mechanisms: axial loading (intra-articular Fx into sub-talar and calcaneal-cuboid joints in 75% cases). Avulsion by Achilles tendon (m/c in osteoporotic bone). Stress (fatigue) Fx.
Intra-articular Fx carries a poor prognosis. Typically comminuted. Rx: operative.
B/I calcaneal intra-articular fx with associated vertebra compression Fx with associated vertebral compression Fx (T10-L2) often termed Casanova aka Don Juan (Lover’s) fx.
Imaging: x-radiography with added “heel view” 1st step. CT scanning is best for Dx and pre-op planning.
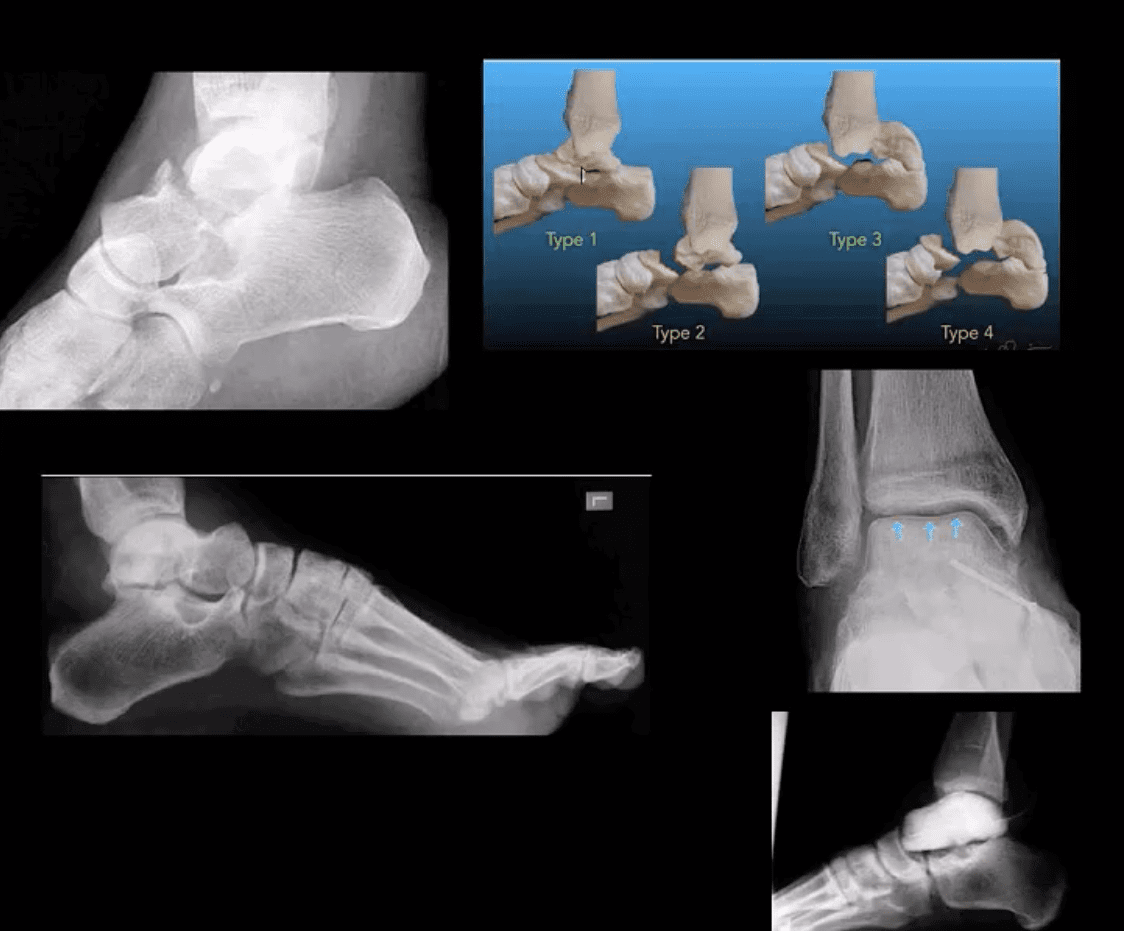
M/C fractured tarsal bone is the Talus. M/C region: talar neck (30-50%). Mechanism: Axial loading in dorsiflexion. Complications: Ischemic osteonecrosis (AVN) of the talus. Premature (2nd OA). Imaging: 1st step: radiographs, CT can be helpful with further delineation
Hawkins classification helps with Dx, prognosis & treatment. “Hawkins sign’ on plain film/CT scan may help with AVN Dx. (above blue arrows indicate good prognosis d/t radiolucent line indicating no AVN because the bone is vascularized and hence resorbed)
Rx: Type 1: conservative with short leg cast or boot (risk of AVN-0-15%), Type 2-4-ORIF (risk of AVN 50%-100%)
Blanca suffered from heel spurs as a result of her occupation as a registered nurse. Her painful symptoms made it challenging for her to accomplish her daily tasks, both in the workplace and in her everyday life. Due to her unbearable heel spurs, Blanca considered finding a new job until she found Dr. Alex Jimenez, doctor of chiropractic. Blanca highly recommends Dr. Alex Jimenez as the non-surgical choice for heel spurs, among other sports injuries and health issues.
Heel Spurs Treatment
A heel spur is a health issue which occurs when a bony-like expansion, known as a calcium deposit, develops between the heel arch and bone of the foot. Heel spurs frequently start in front of the heels and finally affect different elements of the foot. Indicators of heel spurs can include pain, soreness, swelling, and inflammation in the front of the foot. The affected area may also feel hot to the touch. The indicators can also spread to the back of the foot. Finally, a tiny bony protrusion could be observable if left untreated.
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused on treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
If you have enjoyed this video and we have helped you in any way, please feel free to subscribe and recommend�us.
The human body is an intricate machine, and everything is connected so when something goes wrong in one area, it can cause problems in other areas. The back carries a lot of the stress in the body so when there is a problem with the hips, knees, or a foot dysfunction, the spine can bear at least some of the brunt of the pain and other effects.
Pronation describes the way that the foot rolls inward during its normal motion. The foot turns inward, flattening out, as the heel�s outer edge strikes the ground.
For the foot to function correctly, there must be a significant degree of pronation. However, excessive pronation, or overpronation, can cause injury and damage to the foot and ankle. It creates the arch in the foot to flatten, and the ligaments, tendons, and muscles under the foot overstretch.
What is Supination and Oversupination
Supination describes the way the foot rolls outward during its normal motion. It occurs during the push off part of the gait, mainly when running when the heel lifts. The heel leaves the ground, and the movement carries through as weight transfers to the forefront and toes. It moves the body in a forward direction.
When there is excessive supination or oversupination, it strains the tendons and muscles that provide stabilization for the ankle. Causing the ankle to roll, causing injury to the ankle including overpronation sprain, a torn tendon, or ligament rupture.
Conditions and Injuries Caused by Overpronation and Oversupination
Overpronation and oversupination can cause a variety of injuries and conditions that affect not only the feet and ankles, but also the knees, hips, and back as well. Some of the more common injuries and conditions include:
Flat feet or posterior tibial tendon dysfunction
Ankle Sprains
Achilles tendinitis
Arch pain
Plantar fasciitis
Corns
Shin splints
Heel pain
Tight calves
Calluses
Knee pain
Patellar tendonitis
Hip pain
Tight hip flexors
Back pain
Sciatica
Herniated disks
How Foot Problems can Cause Back Pain
Foot Dysfunction can very easily cause a domino effect that extends all the way to the back. The feet are the foundation of the body and when there is a problem with the way they function it can cause the entire body to shift out of alignment.
For instance, overpronation of the foot causes a series of internal changes that extend up through the leg. The femur may rotate causing hip pain and inflammation of the sacroiliac joint which leads to back pain. Other misalignments in the body that are caused by foot problems can also lead to chronic lower back pain as well.
Chiropractic to Treat Foot Problems
Chiropractic seeks to find the cause of the conditions it is used to treat, including pain, instead of just treating symptoms. Because of this, the chiropractor will work to find the cause of the pain, in this case, overpronation and overpronation, and correct it � or the effects of the condition � in addition to treating the back pain.
Typically, overpronation and oversupination, are caused by muscle imbalances in the foot, ankle, and lower leg. Improper shoes, misalignment in the body, and other issues can cause these muscle imbalances. The chiropractor will work with the patient to find the cause of the foot problem so that can be corrected, then work to the damage or injury done.
Foot Dysfunction & Back Pain Chiropractic Treatment
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine