A new diet plan that dictates that you eat only one food for several weeks to lose weight fast is drawing warnings from many experts who say it is dangerous and only successful in the short term.
The Mono Diet (sometimes called the Banana Island or Monotrophic Diet) was popularized by a YouTube star nicknamed “Freelee the Banana Girl” (real name: Leanne Ratcliffe) who claimed it helped her lose weight, the New York Post reports.
Ratcliffe claimed to have lost 40 pounds eating close to 30 bananas a day.
A new version, the Sweet Potato Diet, promises the spud can help you lose 12 pounds in just two weeks. The hashtag #monomeal on Instagram, which highlights pictures of people’s meals containing a single food, has more than 38,000 posts, and the diet was one of the most searched in 2016, according to Google.
Frances Largeman-Roth, a registered dietitian and author of “Eating in Color,” tells the Post you can lose weight by eating only one food, but it’s likely to result from eating less.
“Yes, this diet can produce weight loss,” she says “But, the weight loss is a result of caloric restriction — not because any particular food is magically producing weight loss. It’s an incredibly restrictive and unbalanced diet and I do not recommend that anyone follow it.”
Experts warn such diets can also cause symptoms like dizziness and lead to some serious health problems, including dangerous metabolic changes and muscle loss.
Here’s a scenario that’s probably easy for you to imagine: You’ve just endured a grueling flight to a far-off travel destination. After your arrival at the airport, you spot your luggage on the baggage carrousel. But as grab it, you feel that scary twinge in your back that feels like a pulled muscle or worse.
If this sounds like something you’ve experienced, you have plenty of company. Thousands of Americans suffer low back injuries when traveling each year. And, the truth is, the end of a long journey is the most dangerous moment for a traveler’s back, according to orthopedic specialists.
“When you rush to get your luggage and throw it on the cart to be the first to get customs and out, that’s when you can your hurt your back,” says Dr. Garth Russell, founding member of the Columbia Orthopedic Group in Missouri.
Travel can be a prescription for back pain and injury, experts agree. The long periods of forced immobility in airplanes, lifting the luggage packed with heavy documents or vacation gear, the fatigue, and the time pressure — not to mention the less-than-firm hotel beds — can add up to back spasms and sciatic nerve pain.
Since back pain is the most frequent cause of lost work days after the common cold, according to the American Academy of Orthopaedic Surgeons, it’s crucial take prudent precaution to protect your back when traveling.
“Summer vacation can spell disaster for your aching back if you don’t pay attention to how you move and how you prepare yourself for the journey,” says Dr. Richard Berger, a noted orthopedics surgeon and assistant professor of orthopedics at Rush University in Chicago. “People will be traveling in planes, trains and cars for hours and back pain can ruin even the best laid vacation plans.”
But Berger tells Newsmax Health a handful of back-saving tips can be the difference between a great vacation and a panful experience away from home. Here are his best suggestions:
Lift luggage in stages. “Move slowly and deliberately,” he says. “It’s the sudden jerking movements going full throttle that injure most patients.”
Never twist while lifting. This common error is the most frequent way people injure their back, says Berger, who explains that it takes much less force to cause injury when twisting than when lifting straight up and down.
Ask for help if you have back trouble. “Don’t hesitate to ask another passenger or flight attendant for help,” he says. “Explain your condition and most folks will be happy to assist.”
Ship bags instead. Mail your essentials to the designated destination and avoid luggage entirely. “With airline fees for checked luggage skyrocketing, this may also turn out to be an economical solution, too,” he says
Pack light. Moving a few light bags instead of one very heavy one, will likely avoid back injuries. “This is especially true if you are on an extended vacation with multiple stops so you have to transfer your bags in and out of your vehicles or into overhead bins and compartments,” he notes.
Plan for medication. If you are running low on your pain medication, get new prescriptions from your doctor and fill them so that you have enough. It may seem obvious but do not check medication with your luggage. “You may need them in flight or you may get delayed so that you may need more meds that you originally expected,” he says. Also: Bring backup over-the-counter medications such as Tylenol, Motrin or Aleve.
Ice, ice, baby. If you do suffer a back injury a pack of ice may be your first line of defense. Your flight attendant can fill a bag for you. Place it on your back for 20 minutes, then off for 20 minutes. Products like Icy Hot or Bengay Pain relief medicated patches may also provide relief.
Heat wraps work. There are disposable, portable hot packs that heat up after you open them and you can apply them as needed. Ask your pharmacist to suggest a few brands and check with your airline to make sure they allowed.
Muscle relaxants. These not only treat but may avoid back issues during a long flight. Ask your doctor if they are right for you.
Get the right seat. An aisle seat makes it easier to get in and out of your seat. Moreover, an aisle seat offers you the freedom to get up and move around more frequently.
Get up and move. This is crucial because sitting for an extend period of time stiffens the back muscles, putting stress on the spine and can cause pain. Get up to stretch often. Stretch the hamstrings muscles especially which will reduce stiffness and tension. If you are taking a road trip, stop for a stretch break every couple of hours.
Use a lumbar pillow. If you don’t own your own lumbar support, use a pillow, blanket or rolled up jacket to support the national curve of your back when traveling. Speaking of pillows, if you are staying in a hotel, your may sleep better if you bring your own pillow.
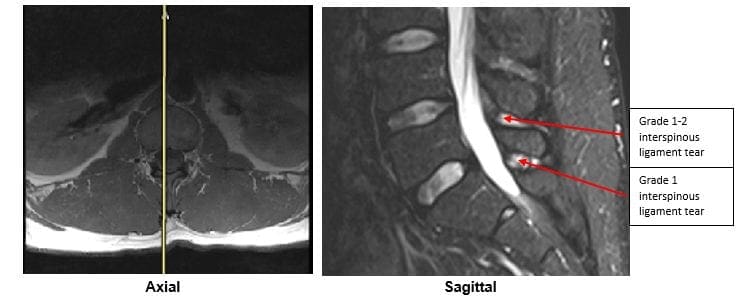
The importance of Magnetic Resonance Imaging to evaluate the integrity of the lumbar posterior ligament complex post trauma.
Abstract: Posterior ligamentous complex(PLC), consisting of the supraspinous ligament, interspinous ligament, ligamentum flavum, and the facet joint capsules is thought to contribute significantly to the stability of the lumbar spine. There has been much debate on whether Magnetic Resonance Imaging(MRI) is specific and sensitive in diagnosing pathology to the PLC. The objective is to determine the necessity of MRI imaging for evaluating the integrity of the lumbar posterior ligament complex post trauma.
Key Words: Magnetic Resonance Imaging(MRI), interspinous ligament, posterior ligament complex, low back pain, ligament laxity, electromyography, impairment rating
A 41-year-old male, presented to my office for an examination with complaints of low back pain with numbness, tingling and weakness into the left lower extremity after he was the restraint driver in a motor vehicle collision approximately three and a half months� post trauma.�He�rated the pain as a�3/10 on a visual analog scale with 10/10 being the worst and the pain and noted the pain as being�present most of the time.� He stated that he was on pain killers daily and this helped manage his daily activities. Without pain killers his pain levels are rated 8/10 being present most of the time. The pain killers stated by the patient are Oxycodone and Naproxen. He�reported that the pain would be aggravated by activities which required excessive standing, repetitive bending, and lifting. He further noted that in the morning the pain was increased and his left leg would be numb and weak for about the first hour.
The patient stated that his care to date had been managed by a pain management clinic and that he had minimal improvement with treatment which has included physical therapy and massage therapy. He reported the pain clinic next recommended steroid injections which he refused. He states there has been was no imaging ordered and that an Electromyography(EMG) had been performed. He was told the test was negative for pathology.
Prior History: No significant medical history was reported. Clinical Findings:�The patient is 6�0� and weighs 210 lbs.
Physical Exam Findings:
Cervical Spine:
Cervical spine range of motion is full and unrestricted. Maximum cervical compression is negative. Motor and other regional sensory exam are unremarkable at this time.
Thoracic Spine:
Palpation of the thoracic spine region reveals taught and tender fibers in the area of the bilateral upper and mid thoracic musculature. Thoracic spine range of motion is restricted in flexion, extension, bilateral lateral flexion, and bilateral rotation. Regional motor and sensory exam are unremarkable at this time.
Lumbar Spine:
Palpation of the lumbosacral spine region reveals taught and tender fibers in the area of the lumbar paraspinal musculature. Lumbar spine range of motion is limited in flexion, extension, bilateral lateral flexion and bilateral rotation. Extension restriction is due to pain and spasm. Straight leg raise causes pain at approximately 50 degrees when testing either side in the left low back. There is no radicular symptomatology down the leg. Kemp�s maneuver recreates pain in the L4 region on the left. No radicular symptoms are noted. The patient is able to heel and toe walk. Regional motor and sensory exam is unremarkable at this time other than L4, L5 and S1 dermatomes having decreased sensation with light touch.
Muscle testing of the upper and lower extremities was tested at a 5/5 with the exception of the left quadricep tested at a 4/5.� The patient�s deep tendon reflexes of the upper and lower extremities were tested including triceps, biceps, brachioradialis, patella, and Achilles and all were tested at 2+ bilaterally except the left patellar reflex was 1+.
RANGES OF MOTION EVALUATION
All range of motions are based on the�American Medical Association�s Guides to the Evaluation of Permanent Impairment, 5th�Edition1�and performed by a dual inclinometer for the lumbar spine.
�� Range of Motion������Normal�������� Examination�������� % Deficit
Flexion
60
48
20
Extension
25
12
52
Left Lateral Flexion
25
16
36
Right Lateral Flexion
25
18
28
An MRI was ordered to rule out gross pathology.
Imaging:
�
A lumbar MRI reveals;
1)��� Mild disc bulges at T11-T12, T12-L1, L1-L2 and L5-S1
2)��� Low disc signals indicative of disc desiccation at T11-T12, T12-L1, L1-L2, L2-L3, L3-L4 and L4-L5
3)��� Retrolisthesis of 2mm at L3-L4
4)��� Mild ligamentous hypertrophy at L1-L2, L2-L3, L3-L4, L4-L5 and L5-S1
5)��� L4-L5 has a Grade 1-2 tear of the interspinous ligament with mild inflammation
6)��� L5-S1 has a Grade 1 interspinous ligament tear with mild inflammation
After reviewing the MRI I ordered lumbar x-rays to rule out ligament laxity.
X-RAY STUDIES
Lumbar x-rays reveal the following:
1)��� Left lateral tilt
2)��� Retrolisthesis at L1 of 3mm
3)��� Retrolisthesis at L2 of 3mm
4)��� Combined excessive translation of 4mm of L1 during flexion-extension
5)��� Combined excessive translation of 4mm of L2 during flexion-extension
6)��� Excessive translation of L3 in extension posteriorly of 2.5mm
7)��� Decreased disc space at L5-S1
Chiropractic care was initiated. The patient was placed on an initial care plan of 2-3x/week for 3 months and then a recommended break in care for one month so the patient could be evaluated for permanency while he was not care dependent.
At maximum medical improvement, he had continued low back pain rated 4/10, continued numbness and tingling into his left leg and left quadricep weakness rated 4/5. He does not need pain killers for pain management anymore. He continues chiropractic care every two weeks to manage his symptoms.
Conclusion:
In this specific case, pathology to the posterior ligament complex diagnosed on MRI lead to the x-ray finding of excessive translation at L1-L2 and L2-L3. The patient was given a permanent impairment rating of 22% based on my interpretation of the American Medical Association�s Guides to the Evaluation of Permanent Impairment, 5th�Edition1. The interspinous ligament tears at the L4-L5 and L5-S1 level would not have been diagnosed without the MRI.
There has been much debate on whether MRI imaging has a role in evaluating lumbar PLC. MRI is a powerful diagnostic tool that can provide important clinical information regarding the condition of the PLC. Useful sequences for spinal MRI in trauma include sagittal and axial T1-weighted images, T2-weighted FSE, fat-saturated T2-weighted FSE, and STIR sequences to highlight bone edema.2�Ligamentous injuries are best identified on T2-weighted images with fat saturation because the ligaments are thin and bonded on either side by fat, which can appear as hyperintense on both T1 and T2 images.3�T1-weighted images are inadequate in isolation for identifying ligamentous injuries.4�
The diagnostic accuracy for MRI was reported for both supraspinous ligament and interspinous ligament injury with a sensitivity of 89.4% and 98.5%, respectively, and a specificity of 92.3% and 87.2% in 35 patients.5
For patients with persistent symptoms after trauma an MRI may be indicated to evaluate posterior ligamentous complex integrity.
Competing Interests:� There are no competing interests in the writing of this case report.
De-Identification: All of the patient�s data has been removed from this case.
References:
1. Cocchiarella L., Anderson G. Guides to the Evaluation of Permanent Impairment, 5th Edition, Chicago IL, 2001 AMA Press.
2. Cohen, W.A., Giauque, A.P., Hallam, D.K., Linnau, K.F. and Mann, F.A., 2003. Evidence-based approach to use of MR imaging in acute spinal trauma.�European journal of radiology,�48(1), pp.49-60.
3. Terk, M.R., Hume-Neal, M., Fraipont, M., Ahmadi, J. and Colletti, P.M., 1997. Injury of the posterior ligament complex in patients with acute spinal trauma: evaluation by MR imaging.�AJR. American journal of roentgenology,�168(6), pp.1481-1486.
4. Saifuddin, A., Green, R. and White, J., 2003. Magnetic resonance imaging of the cervical ligaments in the absence of trauma.�Spine,�28(15), pp.1686-1691.
5. Haba H, Taneichi H, Kotani Y, et al. Diagnostic accuracy of magnetic resonance imaging for detecting posterior ligamentous complex injury associated with thoracic and lumbar fractures.�J Neurosurg. 2003; 99(1 Suppl):20-26.
Whether your friend has hurt your feelings or you’re upset over a lovers tiff, swearing could help to ease your pain, according to new research published in the European Journal of Social Psychology.
Carried out by Dr Michael Philipp, a lecturer at Massey University’s School of Psychology, New Zealand, along with Laura Lombardo from the University of Queensland, Australia, the work looks at the effect of swearing on “short-term social distress,” which could be anything from an argument with your partner to being excluded from a social situation.
Although previous studies have looked at common methods for relieving both physical and social pain, fir example with paracetamol, none have so far looked at whether swearing aloud could also help relieve social distress in the same way that it has previously been shown to ease physical distress.
To test this idea, the study looked at Pain Overlap Theory, which suggests that physical and social/emotional pain share the same underlying processing system, and anything affecting physical pain will also have similar effects on social pain.
For the research 70 participants were split into two groups, and tested for feelings of social pain and sensitivity to physical pain.
During the study participants had to write either about an inclusive social situation, or a distressing one, to induce the corresponding emotions. They were then were randomly assigned to either swear aloud or say a non-swear word aloud.
The results showed that those participants who were socially distressed experienced less social pain and less sensitivity to physical pain than those who didn’t swear.
“Previous research suggests that social stressors, like rejection and ostracism, not only feel painful but also increase people’s sensitivity to physical pain,” explained Dr Phillip. He also added that swearing can help ease both social and physical pain by reducing its intensity, by distracting the person in pain.
However, Dr Phillip also pointed out that swearing may not have the same effect if used on an everyday basis or in a situation which is only mildly irritating or stressful, when the use of profanity may lose its impact.
He also added that swearing is not a quick answer for those experiencing serious emotional pain and stress such as grief or abuse, when clinical care may be needed.
Previous research on swearing has also found that cursing aloud can make you stronger. In a small-scale study published early last month, a team of researchers found that participants who completed a test of anaerobic power — a short, intense period on an exercise bike — and isometric handgrip test — produced more power and had a stronger grip if they swore while completing the exercises.
Be honest, you don’t know how your car works, do you? And despite spending most of the working day lashed to a QWERTY, if someone asked you how update their modem, you wouldn’t where to start (or what the modem even is).
And that’s fine. Other people do that stuff so you don’t have to. But the same can’t be said for your workout. You need to be okay with the specifics – do you honestly know what that dead lift is doing to your muscles? Or more importantly, the damage you could be doing to yourself if you’re getting it wrong.
Thankfully, experts are on hand. We’ve enlisted the help of Tim Walker, founder London’s Evolve Fitness to settle the form debate on five key exercises, once and for all.
First up, a pre-lift check list.
Breathing. Oxygen creates energy in the muscles, so don’t hold your breath.
Technical understanding. Understand which muscles you are about to engage, know the movement you’re about to make, and be deliberate with that movement.
Mental participation. Make sure you’re in the moment, and don’t think about what’s next. Connect your mind to your muscles, and aim for a full range of motion.
Load selection. Challenge yourself, but be realistic, your body will thank you in the long run. Go too heavy and you’ll fail to get a range of motion, too light and you won’t stimulate the muscle enough force growth.
1.Bicep Curls
The most common mistake: “Leaning back during the curl and bringing your elbows forward (rather than keeping them at your side).”
The damage it might be doing: You can incur bicep tendon injuries (tears, impingements and dislocations etc.) but the main reason you need to get your form right is so that the exercise actually has an effect. “Leaning too far backwards means that you’re not putting enough pressure on the bicep – you’re using your weight as momentum during the curl, rather than lifting only with the bicep muscles. And by lifting your elbows forwards, you’re shifting the focus of the exercise away from the bicep (you’ll be lifting with your shoulders and using the momentum from your body again), thus you won’t get the development you want.
Most Popular
How to fix it: “Focus on holding your posture more tightly; pull your shoulder blades back and down, and lift your chest up, lean forward slightly and keep your weight in your heels. Contract your abs at all times, too. To keep your elbow position, focus on keeping your elbows in line with your ears, and be forceful with that contraction in your abs when pulling the weight up.”
2. Bench Press
The most common mistake: “Elbow position. Most people have their elbows in line with their shoulders. It’s hampering your progress because it doesn’t target the chest. You’re looking for synergistic movement in the chest, shoulders and triceps.”
The damage it might be doing: The most common injuries are a Glenoid Labrum tear (front of upper arm), rotator cuff tears and shoulder impingement syndrome. Bench pressing is the kind of exercise that you want to keep increasing in weight, because the feeling of nailing that new three-rep max is unbeatable. But it only takes one lift with poor form for something to go wrong, so always think ‘form first, weight second’.
How you should be doing it: “I often ask my clients to lower their arms 20/25 degrees, so they are just above the nipple, and I always find it useful to keep my knuckles pointing to the ceiling, and my wrists straight.”
3. Deadlift
The most common mistake: “Rounding of the back, rather than keeping a natural arch.”
The damage it might be doing: “A slipped disc in the lower back is the main danger here.” You can also incur sprains and strains (different things), but if there’s any sharp pain at any point, you should stop.
How to fix it: “Try locking the upper body posture by keeping the chest high and arms long (aka fully extended, not bent). Keep your weight into your heels (make sure they don’t leave the ground, and you’re not feeling your full weight in your toes) concentrate on pressing through the legs and keep your core area strong by engaging your stomach muscles.”
4. Squat
The most common mistake: “For squats, there are several: bending forward too much, not squatting deep enough and allowing the knees to turn inwards.”
The damage it might be doing: “That mistake is damaging your body/hampering your progress because� Bending forward too much will put too much pressure on your back, and lead to the same kind of damage as an incorrect deadlift. If you’re not going deep enough you won’t be engaging the hamstrings and glutes as much as you could; if you’re aiming to build the muscles and boost metabolism you’ll be missing the mark. If you allow the knees to turn inwards you’re risking damage to the ligaments such as ACL.”
How to fix it: “For bending forward; this is commonly due to a general tightness in the chest and lats (latissimus dorsi muscles) and/or hip flexors, which is very common among office workers who spend a lot of time sitting. Fix it by stretching these muscles more regularly. For those not going deep enough, you need to man-up and understand the principles if fight-or-flight. Most people fear that when they go down deeper they won’t get back up, but you need to attack the movement with confidence and good technique. The worst that can happen is that the safety catches will stop the bar and you crawl out. For the knees, the best thing is to engage your brain. Think about what you are doing and what your knees are doing, you want your them to be in line with your second and third toes at all times.”
5. Single Arm Rows
The most common mistake: Rounding of the back, rotating too much as you pull the weight, and failing to achieve a full range of motion, i.e. not pulling the weight all the way into the body.
The damage it might be doing: “Rounding the back isn’t particularly dangerous, but it’ll prevent the most optimal development of your back. Over rotation when pulling the weight will mean you’re not working the back muscles as well as you could be, hampering your strength development. The same goes for not having a full range of motion; if you’re not pulling the weight all the way into your body, you’re not getting a full contraction of the muscles, which means you won’t be adequately stimulating them.”
How to fix it: “Stick your butt out and check your position in a mirror – your upper back should be flat, with a gentle/natural arch in your lower back. For over rotation, by more rigid in both your thinking and your positioning. When you hold the position more forcefully you will engage your abs and obliques better. This is one of my favourite back exercises – when done properly – it works and engages your core as well as the back.”
Tim Walker is the founder of Evolve Fitness,13-15 Bouverie Street, London, EC4Y 8DP
Bathing suit season is here, and for many of us that means no longer being able to hide those extra pounds beneath a chunky sweater. Fortunately, there are some small and easily implemented lifestyle adjustments that can quickly shrink your waistline.
Here are 10 ways to slim down for swimsuit season. The best part? None involve the gym.
Plan ahead: Making meals ahead of time can save you calories in the long run. Try cooking up large-batch dinners over the weekend and simply reheat throughout the week. Lisa Lillien, author of the “Hungry Girl” Website, featuring advice on guilt-free eating, suggests emphasizing lean proteins and veggies. Commit time on the weekend to meal prep and all you have to do is throw the ingredients in the pan during the week.
Drink more: Water, that is. Staying hydrated is important for your overall body function and can prevent you from feeling hungry. Sometimes the body confuses dehydration with the sensation of hunger. This problem comes with an easy solution — drink more water. Bring a travel water bottle with you when you’re on the go so you can remember to stay hydrated.
Limit or avoid alcohol: Cutting out alcohol is one of the quickest ways to lose weight. Alcohol triggers a process in the body similar to sugar. It can set off the same insulin resistance that can cause weight gain. For six days of the week, cut out alcohol.
Snack on healthy foods: Keep a variety of healthy snacks around to satisfy cravings. Protein bars and nuts are great snacks that will satisfy your hunger and prevent you from making poor food decisions at meal times. Fresh fruit and veggies are another great snack option.
Banish stress: Maintaining a healthy diet isn’t about never indulging. It’s about eating healthy foods the majority of the time and treating yourself on occasion. Don’t stress out if you veer off course. Instead, do what you can to get back on track. Stress can actually be a source of weight gain, so try to focus on the positive.
Careful with carbs: Processed white carbs are a no-no. They spike blood sugar levels and cause the pancreas to produce insulin, which causes the accumulation of fat. Instead, opt for refined carbs like brown rice and oats.
Start with soup: According to research from Penn State University, soup is a great diet food. The combination of liquids and solids helps make you feel full faster. Eat it before a meal and you may be able to decrease your overall calorie intake by up to 20 percent.
Consider your coffee: Black coffee isn’t a diet buster — it’s the milk and sugar that go in it. A latte from your favorite coffee shop can be a hidden source of fat and calories. Try swapping your usual espresso for a plain black or green tea.
Stop multitasking: A recent study in the American Journal of Clinical Nutrition found that multitasking while you eat will leave you feeling unsatisfied. Instead, slow down and enjoy your time savoring your meal without the distractions.
Spice it up: According to a recent study led by David Heber, a professor of medicine and director of the Center for Human Nutrition at the University of California-Los Angeles, capsaicin — the compound found in chili peppers — speeds metabolism and helps burn calories. Participants in the study were given a capsaicin supplement or a placebo for four weeks. The group who received capsaicin burned more fat for several hours after the meal for a total of 100 to 200 more calories a day. Spicy foods may also make you feel fuller more quickly than bland foods.
A compound in a plant found throughout Southeast Asia is a more powerful anti-HIV compound than the drug AZT that’s used to treat the condition, says a study published in the Journal of Natural Compounds.
Patentiflorin A, a chemical derived from the willow-leaved Justicia, stood out in a screening of more than 4,500 plant extracts by a team of scientists from the University of Illinois at Chicago, Hong Kong Baptist University, and the Vietnam Academy of Science and Technology to see if they had any effect against the HIV virus.
AZT is an anti-viral drug that doesn’t cure HIV, but reduces the amount of the virus in the body and reduces the risk of developing AIDS. It was the first drug approved by the FDA to treat HIV infection in 1987. Today, it is still the cornerstone of HIV treatment, although it is combined with other drugs to increase effectiveness and reduce side effects.
For the current study, Lijun Rong, professor of microbiology and immunology in the UIC College of Medicine, and his colleagues zeroed in on patentiflorin A because of its ability to inhibit an enzyme needed for HIV to incorporate its genetic code into a cell’s DNA.
AZT inhibits this enzyme, called reverse transcriptase. In studies of human cells infected with the HIV virus, patentiflorin A was significantly better at inhibiting the enzyme than AZT.
“Patentiflorin A was able to inhibit the action of reverse transcriptase much more effectively than AZT, and was able to do this both in the earliest stages of HIV infection when the virus enters macrophage cells, and alter infection when it is present in T cells of the immune system,” said Rong.
Patentiflorin A was also was effective against known drug-resistant strains of the HIV virus, making it a very promising candidate for further development into a new HIV drug.
“Patentiflorin A represents a novel anti-HIV agent that can be added to the current anti-HIV drug cocktail regimens to increase suppression of the virus and prevention of AIDS,” Rong said.
The researchers were also able to synthesize patentiflorin A. “If we can make the drug in the lab, we don’t need to establish farms to grow and harvest the plant, which requires significant financial investment, not to mention it has an environmental impact,” Rong said.
Other advances are being made in the battle against HIV. Last year, scientists at the Oregon National Primate Research Center found that giving infant monkeys human antibodies within 24 hours of being exposed to a virus similar to HIV totally cleared them of the virus within two weeks. Current HIV treatments keep the virus in check, but once a person stops taking anti-HIV drugs, the virus returns.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine