Living with sciatica can be debilitating and exhausting. Find out how different individuals reduced their pain from this condition. Sciatica has different treatment options. It is often a matter of trial and error to find a treatment/therapy that works for the individual. These include:
Different individuals with sciatica share what works for them. Here are their stories.
Rudy Found Relief With Self Care
A bad fall left Rudy, a graphic designer, with a broken pelvis and broken foot. I was in the hospital for a few days, and when I came home, I noticed I was hobbling. I had developed sciatica. I was in a lot of pain but decided to try the treatment that had helped me manage chronic migraines. This was yoga. Specifically, it was hot yoga sessions that, despite the pain, worked. However, for others, he recommends not staying still. The body can’t stay stagnant with no movement.
Rudy follows a plant-based diet. Eating right has helped significantly. He starts the day with a green smoothie and sips one throughout the day. This reduces inflammation and pain. His stress would also contribute to the pain. Anything felt from a pain perspective becomes amplified when in a sad, frustrated, confused mood. Rudy’s advice is to get the body moving. And follow a plant-based anti-inflammation diet.
Medication and a Topical Pain Balm Work For Jose
Jose, 66, figured how his sciatica developed was when he decided to insulate the garage. I was bending, twisting, turning, and contouring my body every which way. A week after the job, I developed excruciating pain that got worse over the following weeks. I would jolt out of bed at 2-3 in the morning with severe pain. My doctor gave me steroids that didn’t do anything. I could barely sit down and had to go through a careful method of getting into a chair. I was prescribed Vicodin – hydrocodone/acetaminophen. I took them for a week and a half.
The pain went away, but it came right back as soon as I stopped taking the meds. The meds were only masking the pain. I decided only to use it when the pain was excruciating. This was because I was worried about addiction. I tried chiropractic, massage, acupuncture, cupping, and physical therapy. Unfortunately, I was not feeling any real relief. Then I went to a pain management doctor, who ordered an X-ray and an MRI.
The doctor informed me that my spine was in great shape. The pain management doctor gave me a piriformis injection and, later, an epidural steroid injection. There were still no positive results. My primary care doctor prescribed gabapentin. This is an anti-epilepsy medication that has been shown to help some cases of back pain. Most of the major pain is gone, and I’m pretty sure it’s from the gabapentin along with weekly deep massage sessions. I also use CBD cream with arnica. Movement is important; during the day, I make sure to stand up and walk around.
Epidural Injections Work For Isabel
Isabel has chronic pain. This comes from arthritis, migraines, and fibromyalgia. Sciatica developed as a result of these conditions. Soon she couldn’t get into the car or even empty the dishwasher without going through excruciating pain. Nerve ablation or physical therapy was ineffective at relieving the pain. Then my doctor suggested getting an epidural injection. This is not the same type of injection as when having a baby. It is not the same at all. The injection includes a steroid medication called a corticosteroid that is an anti-inflammatory, along with an anesthetic. I tried it and got some relief, but the pain came back. However, after a month and a half, I began to feel more relief. The pain is not completely gone. I do feel better, but there is still some pain. My doctor told me that patients are all different and require different amounts of medication and time to work.
Surgery Gave Pablo His Life Back
Pablo, 50, is no stranger to back pain or back surgery. After living with chronic back pain from a roll-over auto accident, Pablo underwent a laminectomy. A doctor removed a portion of the vertebra in 1998 and spinal fusion in 2004 that fused the discs from L5 to S1. Life was going well until I was laid off from my desk job. I started working at a warehouse doing light work, but I would still help lift moderate/heavy bags, boxes, etc. I just pushed through the pain, thinking it was a strain that would go away.
However, during the last six months, the pain was so bad I had to stop working. I needed a cane to get out of a chair. Friends and family told me I was walking like a 90-year-old. I also lost feeling in a couple of my toes. In 2021 I had another fusion and had a broken screw from my earlier fusion repaired. The surgery went well, and they said as long as I don’t do any heavy lifting, I should be alright. Although there is still pain, it is much less than it was before the surgery. My doctor recommended a new desk job and a physical therapy rehabilitation, stretching, and strengthening program.
Body Composition
Calories burned from 10,000 steps
Estimations of how many calories are burned from exercises like walking or running depends on how heavy an individual is. Heavier people use more energy to move than lighter people. Estimates revolve around 100 calories burned per mile for a 180-pound person. 10,000 steps comes to around roughly 5 miles. Assuming an individual weighs 180 pounds means 100 calories x 5 miles equals 500 calories. Over a week, it becomes 3,500 calories. However, lighter or heavier individuals will burn less or more calories while walking the same number of steps or distance.
Diagnosis of the diseases of the abdomen can be classified into:
Abnormalities of the gastrointestinal tract (esophagus, stomach, small & large bowel, and the appendix)
Abnormalities of the accessory digestive organs (Hepatobiliary & pancreatic disorders)
Abnormalities of the genitourinary & reproductive organs
Abnormalities of the abdominal wall and major vessels
This presentation aims to provide the most basic understanding of general diagnostic imaging approach and appropriate clinical management of patients with the most common diseases of the abdomen
Imaging modalities used during an investigation of the abdominal complaints:
AP abdomen (KUB) and upright CXR
Abdominal CT scanning (with oral and I.V. contrast and w/o contrast)
Upper and Lower GI Barium studies
Ultrasonography
MRI (most used as Liver MRI)
MRI enterography & enteroclysis
MRI rectum
Endoscopic Retrograde Cholangiopancreatography (ERCP)- mostly hepatobiliary and pancreatic ductal pathology
Nuclear imaging
Why Order An Abdominal X-ray?
Include a preliminary evaluation of bowel gas in an emergent setting. For example, a negative study in a low probability patient may obviate the need for a CT or other invasive procedures
Evaluation of radiopaque tubes, lines, and radiopaque foreign bodies
Post-procedural evaluation intraperitoneal/retroperitoneal free gas
Monitoring the amount of bowel gas and resolution of postoperative (adynamic) ileus
Monitoring the passage of contrast through the bowel
Colonic transit studies
Monitoring renal calculi
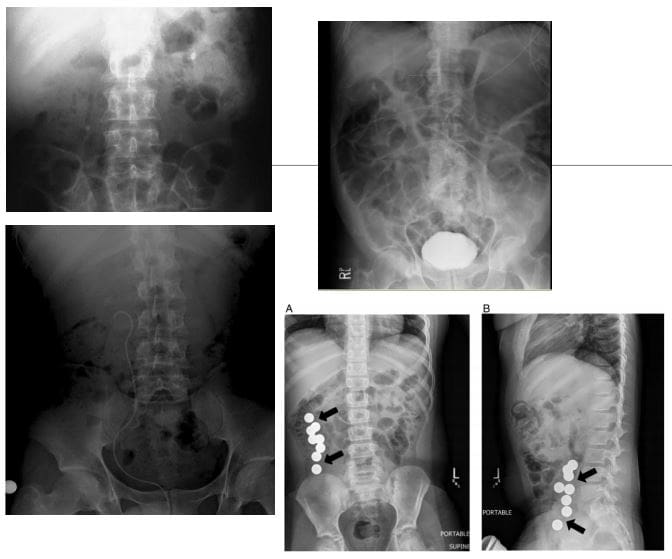
What to Note on AP Abdomen: Supine vs. Upright vs. Decubitus
Free Air (pneumoperitoneum)
Bowel obstruction: Dilated loops: SBO vs LBO (3-6-9 rule) SB-upper limit-3-cm, LB-upper limit-6-cm, Caecum-upper limit-9-cm. Note loss of haustra, note dilation (presence) of valvule conivente (plica semilunaris) in SBO
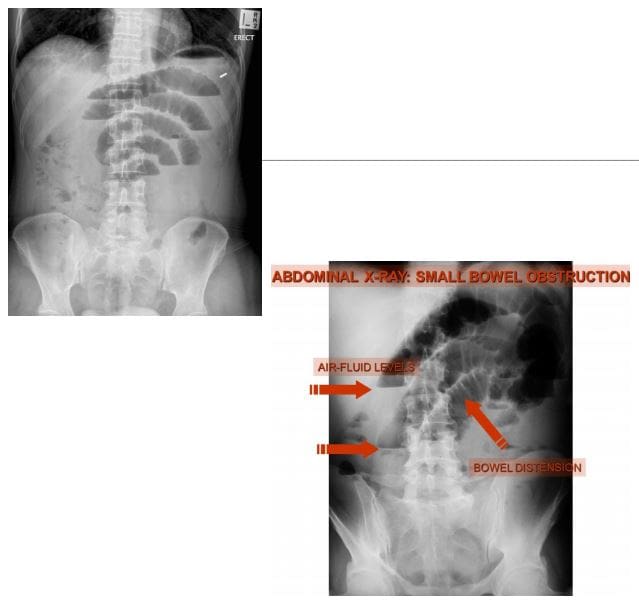
SBO: note different heights air-fluid levels on upright film step ladder� appearance, typical of SBO
Note paucity of rectal/colonic gas (evacuated) in SBO
Abdominal CT scanning -modality of choice during the investigation of acute and chronic abdominal complaints especially in adults. For example, abdominal malignancy can be successfully diagnosed and staged providing clinical information for care planning
Abdominal, renal and pelvic ultrasound can be performed to help the diagnosis of appendicitis (esp. in children), acute & chronic vascular pathology, hepatobiliary abnormalities, obstetric and gynecological pathology
Use of ionizing radiation (x-rays & CT) should be minimized in children and other vulnerable groups.
Diagnostic Imaging of Major Diseases of the Gastrointestinal System
1) Esophageal disorders
2) Gastric carcinoma
3) Gluten Sensitive Enteropathy
4) Inflammatory Bowel Disease
5) Pancreatic ductal adenocarcinoma
6) Colorectal carcinoma
7) Acute Appendicitis
8) Small bowel obstruction
9) Volvulus
Esophageal disorders
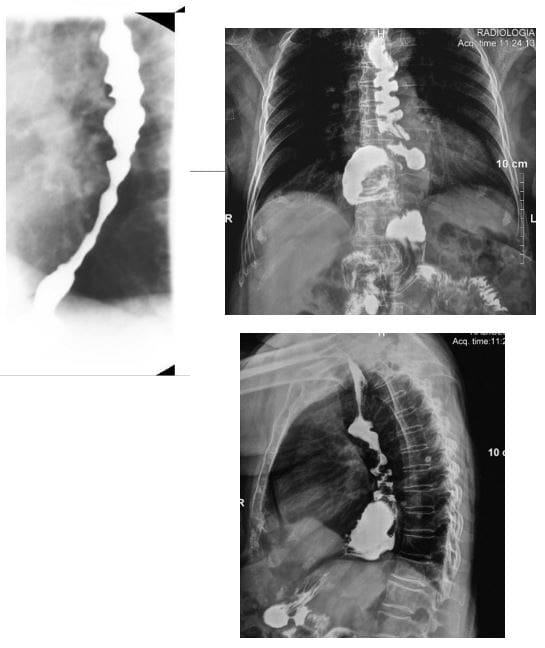
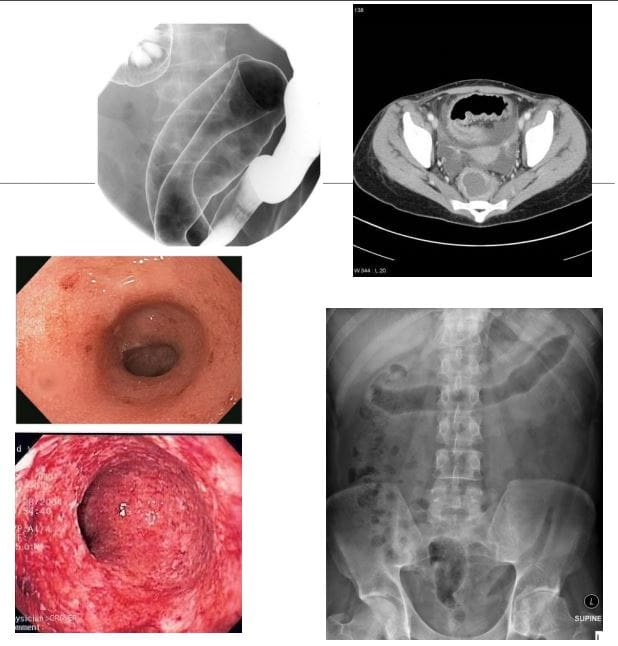
Achalasia (primary achalasia): failure of organized esophageal peristalsis d/t impaired relaxation of the lower esophageal sphincter (LOS) with marked dilatation of the esophagus and food stasis. Obstruction of the distal esophagus (often due to tumor) has been termed “secondary achalasia” or “pseudoachalasia.� Peristalsis in the distal smooth muscle segment of the esophagus may be lost due to an abnormality of Auerbach plexus (responsible for smooth muscle relaxation). Vagus neurons can also be affected
Primary: 30 -70s, M: F equal
Chagas disease (Trypanosoma Cruzi infection) with the destruction of the Myenteric plexus neurons of the GI system (megacolon & esophagus)
However, the heart is the M/C affected organ
Clinically: Dysphagia for both solids and liquids, in comparison to dysphagia for solids only in cases of esophageal carcinoma. Chest pain and regurgitation. M/C mid esophageal squamous cell carcinoma in approximately 5% due to chronic irritation of the mucosa by stasis of food and secretions. Aspiration pneumonia may develop. Candida esophagitis
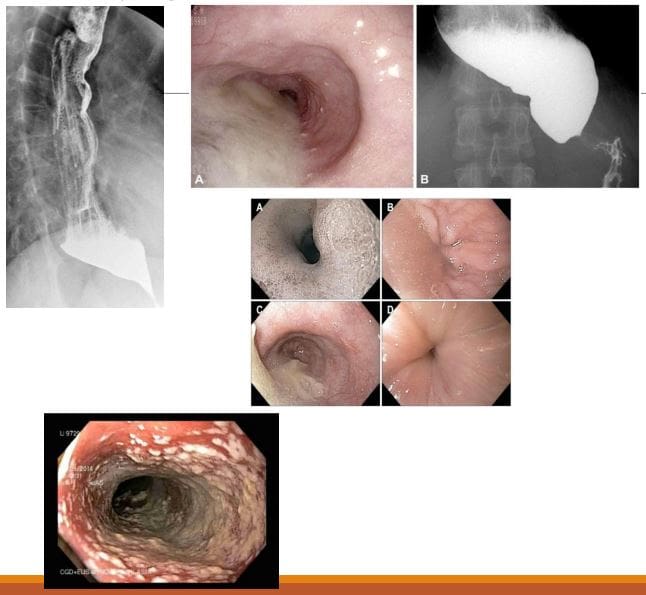
Imaging: �Bird -beak� on upper GI barium swallow, dilated esophagus, loss of peristalsis. An endoscopic exam is crucial.
Rx: difficult. Calcium channel blockers (short -term).Pneumatic dilatation, effective in 85% of patients with 3 -5% risk of bleeding/perforation. Botulinum toxin injection lasts only approx. 12 months per treatment. May scar the submucosa leading to increased risk of perforation during subsequent myotomy. Surgical myotomy (Heller myotomy)
10 -30% of patients develop gastroesophageal reflux (GERD)
Presbyesophagus: used to describe the manifestations of degenerating motor function in the aging esophagus >80-y.o. Due to interruption of the reflex arc with decreased sensitivity to distension and alteration in peristalsis.
Patients may complain of dysphagia or chest pain, but most are asymptomatic
Diffuse/distal esophageal spasm (DES) is a motility disorder of the esophagus that may appear as a corkscrew or rosary bead esophagus on barium swallow.
2% of non-cardiac chest pain
Manometry is the gold-standard diagnostic test.
Zenker diverticulum (ZD) aka pharyngeal pouch
An outpouching at the level of the hypopharynx, just proximal to the upper esophageal sphincter, known as the Killian dehiscence or Killian triangle
Patients are 60-80 y.o and present with dysphagia, regurgitation, halitosis, globus sensation
May complicate with aspiration and pulmonary abnormalities
Patients may accumulate medications
ZD- is a pseudodiverticulum or pulsion diverticulum resulting from herniation of the submucosa through the Killian dehiscence, forming a sac where food and other contents may accumulate.
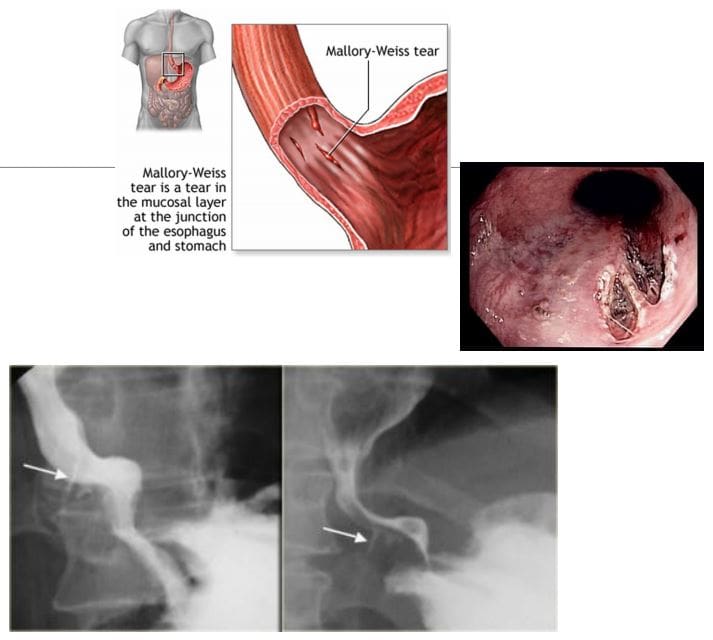
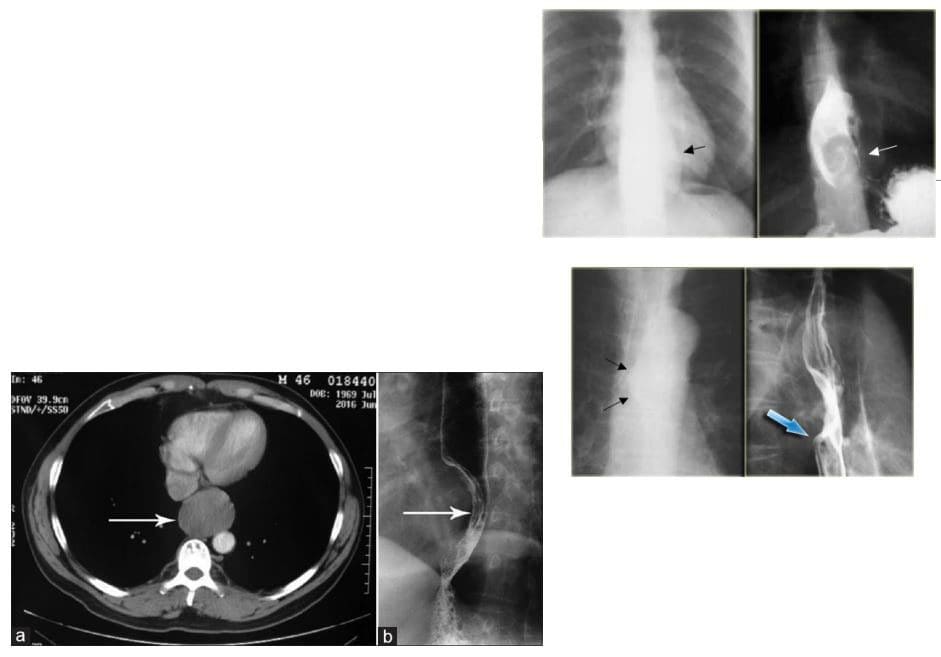
Mallory-Weiss syndrome refers to mucosal and submucosal tears of the distal oesophageal venous plexus associated with violent retching/vomiting and projection of gastric contents against the lower esophagus. Alcoholics are at particular risk. Cases present with painless hematemesis. Treatment is typically supportive.
Dx: imaging plays little role, but contrast esophagram may demonstrate some mucosal tears filled by contrast (bottom right image). CT scanning may help to exclude other causes of upper GI bleeding
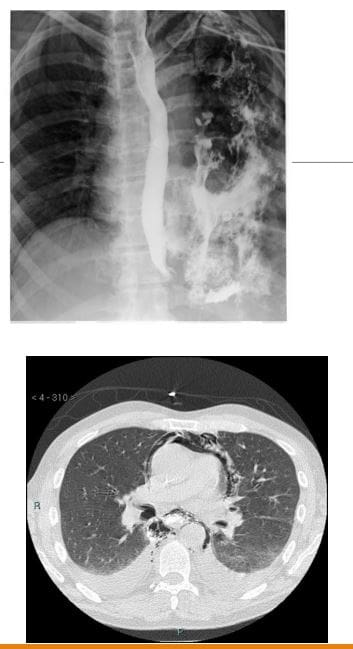
Boerhaave syndrome: esophageal rupture secondary to forceful vomiting
Mechanisms involve forceful expulsion of gastric contents especially with large undigested foods when esophagus forcefully contracts against closed glottis with 90% occurring along left posterolateral wall
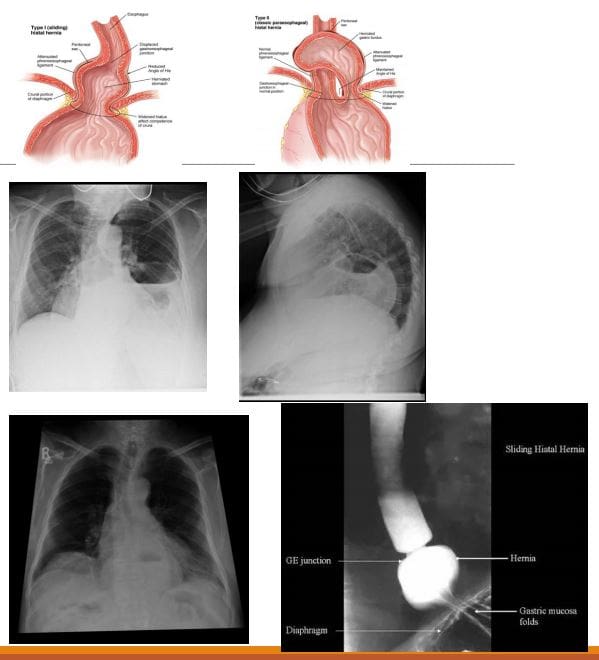
Hiatus hernias (HH): herniation of abdominal contents through the esophageal hiatus of the diaphragm into the thoracic cavity.
Many patients with HH are asymptomatic, and it is an incidental finding. However, symptoms may include epigastric/chest pain, postprandial fullness, nausea and vomiting
Sometimes HH is considered synonymous with gastro-oesophageal reflux disease (GORD), but there is a poor correlation between the two conditions!
2-types: sliding hiatus hernia 90% & rolling (paraoesophageal) hernia 10%. The latter may strangulate leading to ischemia and complications.
Esophageal Leiomyoma is the M/C benign esophageal neoplasm. It is often large but yet non-obstructive. Gastrointestinal stromal tumors (GIST) are the least common in the esophagus. Should be differentiated from Esophageal carcinomas.
Imaging: contrast esophagram, upper GI barium swallow, CT scanning. Gastroesophagoscopy is the Dx method of choice.
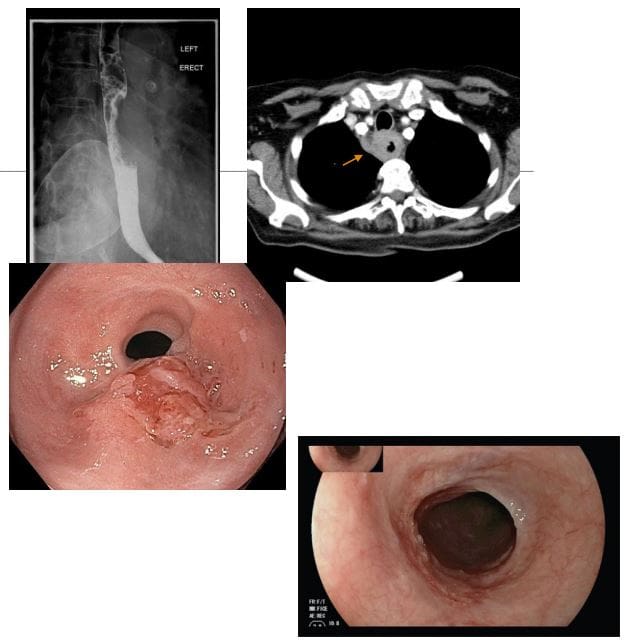
Esophageal carcinoma: presented with increasing dysphagia, initially to solids and progressing to liquids with obstruction in more advanced cases
<1% of all cancers and 4-10% of all GI malignancies. There is recognized male preponderance with the squamous cell subtype due to smoking and alcohol. Barrett esophagus and adenocarcinoma
M: F 4:1. Black individuals are more susceptible than White individuals 2:1. Poor prognosis!
A barium swallow can be sensitive in identifying esophageal mass. Gastroesophagoscopy (endoscopy) confirms the diagnosis with tissue biopsy
Overall the most common malignancy is 2ndary gastric fundal carcinoma invading distal esophagus
Squamous cell is typically found in the mid esophagus, Adenocarcinoma in the distal region
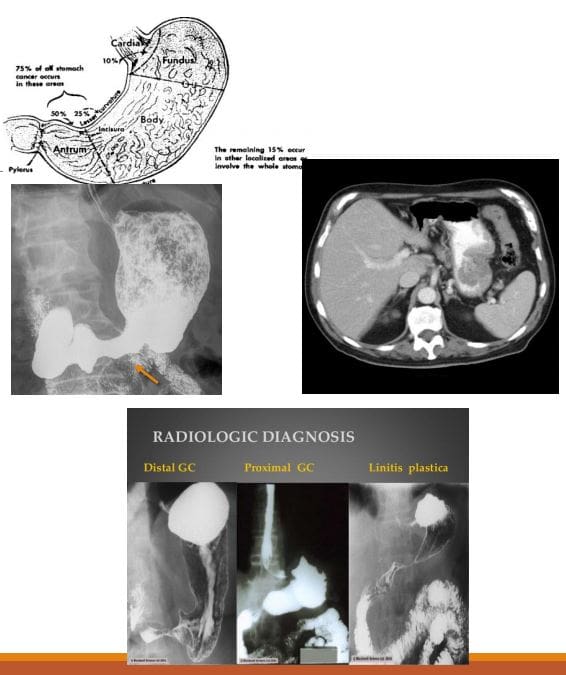
Gastric carcinoma: primary malignancy of gastric epithelium. Rare before the age of 40. The median age at diagnosis in the United States is 70 years for males and 74 years for females. Japan, South Korea, Chile, and Eastern European countries have one of the highest rates of stomach cancer in the world. Stomach cancer rates are declining worldwide. Gastric cancer is the 5th causes of cancer-related death. Association with Helicobacter pylori infection 60- 80%, but only 2% population with H. Pyloris develop Stomach cancer. 8-10% have an inherited familial component.
Gastric Lymphoma is also linked to H. Pyloris infection. Gastrointestinal Stromal Cell Tumour or GIST is another neoplasm affecting the stomach
Clinically: No symptoms when it is superficial and potentially curable. Up to 50% of patients may have non-specific GI complaints. Patients may present with anorexia and weight loss (95%) as well as vague abdominal pain. Nausea, vomiting, and early satiety d/t obstruction may occur with bulky tumors or infiltrative lesions that impair stomach distension.
Prognosis: Most gastric cancers diagnosed late and may reveal local invasion with regional adenopathy, liver, and mesenteric spread. A 5-year survival rate of 20% or less. In Japan and S. Korea, early screening programmes increased survival to 60%
Imaging: Barium upper GI study, CT scanning. Endoscopic examination is the method of choice for the diagnosis. On imaging, Gastric cancer may appear as an exophytic (polypoid) mass or Fungative type, Ulcerative or Infiltrative/diffuse type (Linitis Plastica). CT scanning is important to evaluate local invasion (nodes, mesentery, liver, etc.)
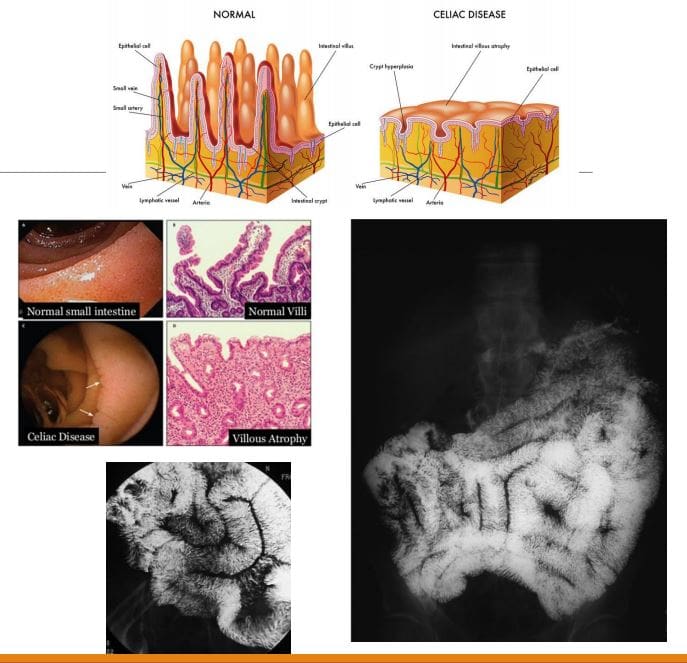
Celiac disease aka non-tropical sprue aka Gluten-sensitive enteropathy: A T-cell mediated autoimmune chronic gluten-induced mucosal damage resulting in loss of villi in the proximal small bowel and gastrointestinal malabsorption (i.e., sprue). Considered in some cases of iron deficiency anemia of undetermined cause. Common in Caucasians (1 in 200) but rare in Asian and black individuals. Two peaks: a small cluster in early childhood. Typically in 3rd and 4th decades of life.
Clinically: Abdominal pain is the m/c symptom, malabsorption of nutrients/vitamins: IDA and guaiac-positive stools, diarrhea, constipation, steatorrhea, weight loss, osteoporosis/osteomalacia, dermatitis herpetiformis. Increased association with T-cell lymphoma, Increased association with esophageal squamous cell carcinoma, SBO
Dx: Upper GI endoscopy with multiple duodenal biopsies is considered a diagnostic standard for celiac disease. Histology reveals T-cell infiltration and lymphoplasmacytosis, Villi atrophy, Crypts hyperplasia, Submucosa, and Serosa are spared. Rx: elimination of gluten-containing products
Imaging: Not required for Dx but on Barium swallow fluoroscopy: mucosal atrophy and obliteration of mucosal folds (advanced cases only). SB dilation is the most typical finding. Nodularity of the duodenum (bubbly duodenum). Reversal of jejunal and ileal mucosal folds:
�The jejunum looks like ileum, the ileum looks like the jejunum, and the duodenum looks like hell.�
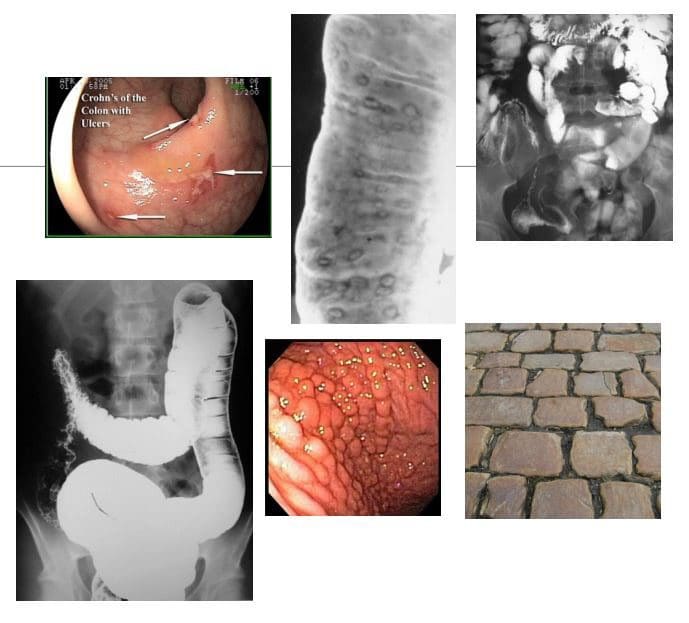
CD: chronic relapsing-remitting autoimmune inflammation that affects any part of the GI tract from the mouth to the anus but at onset most typically involves the terminal ileum. M/C presentation: abdominal pain/cramping and diarrhea. Path: granulomata formation that unlike UC is transmural, potentially leading to strictures. Areas affected by the inflammation are typically patchy
Complications are numerous: malabsorption of nutrients/vitamins (anemia, osteoporosis, developmental delay in children, susceptibility to GI malignancy, bowel obstruction, fistula formation, extra-abdominal manifestations: uveitis, arthritis, AS, erythema nodosum and others. 10- 20% may require abdominal surgery after 10-years of CD usually for strictures, fistiluzation, BO.
Dx: clinical, CBC, CMP, CRP, ESR, serological tests: DDx of IBD: anti-Saccharomyces cerevisiae antibodies (ASCA), perinuclear antineutrophil cytoplasmic antibody (p-ANCA) histologically or in serum. Fecal Calprotectin test helps to DDx IBS and evaluate response to treatment, disease activity/relapses.
Dx of choice: endoscopy, ileoscopy, and multiple biopsies may reveal endoscopic and histological changes. Video capsule endoscopy (VCE), Imaging may help with Dx of complications. Rx: immunomodulatory drugs, complementary medicine, diet, probiotics, operative. No cure but the aim is to induce remission, control symptoms and prevent/treat complications
Imaging Dx: KUB to DDx SBO, Barium enema (single and double contrast), small bowel follow through. Findings: skip lesions, aphthous/deep ulcerations, fistula/sinus tracts, String sign, creeping fat pushed loops of LB, cobblestone appearance d/t fissures/ulcers pushing mucosa, CT scanning with oral and IV contrast.
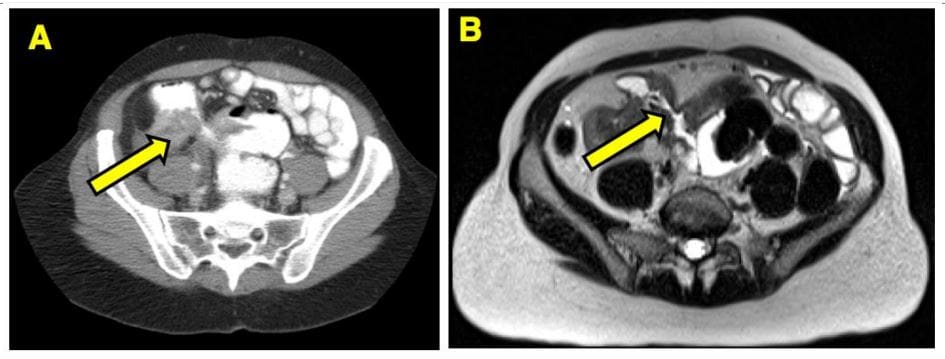
Imaging from a Crohn’s patient who had a small bowel resection for obstruction.
(B) MRE of the same area shows a fibrostenotic stricture
UC: characteristically involves only the colon but backwash ileitis may develop. Onset is typically at 15-40s and is more prevalent in males, but the onset after the age of 50 is also common. More common in North America and Europe (hygiene hypothesis). Etiology: A combination of environmental, genetic and gut microbiome changes are involved. Smoking and early appendectomy tend to show a negative association with UC, unlike in CD considered some of the risk factors.
Clinical Features: Rectal bleeding (common), diarrhea, rectal mucous discharge, tenesmus (occasionally), lower abdominal pain and severe dehydration from purulent rectal discharge (in severe cases, especially in the elderly), fulminant colitis and toxic megacolon can be fetal but are rare complications. Pathology: No granulomata. Ulcerations affect mucosa and submucosa. Pseudopolyps present as elevated spared mucosa.
An initial process always affects the rectum and remain a local disease (proctitis) in (25%). 30% Proximal disease extension may occur. UC may present as left-sided (55%) and pancolitis (10%). Majority of cases are mild to moderate
Imaging: not required for Dx but barium enema may reveal ulcerations, thumbprinting, in advanced cases loss of haustra and narrowing of the colon producing �lead-pipe colon.� CT scanning may help with Dx seen as mucosal thickening detected only in moderate and severe cases. CT may help with of Dx of complications. Plain film image reveals �lead-pipe colon� and sacroiliitis as Enteropathic arthritis (AS)
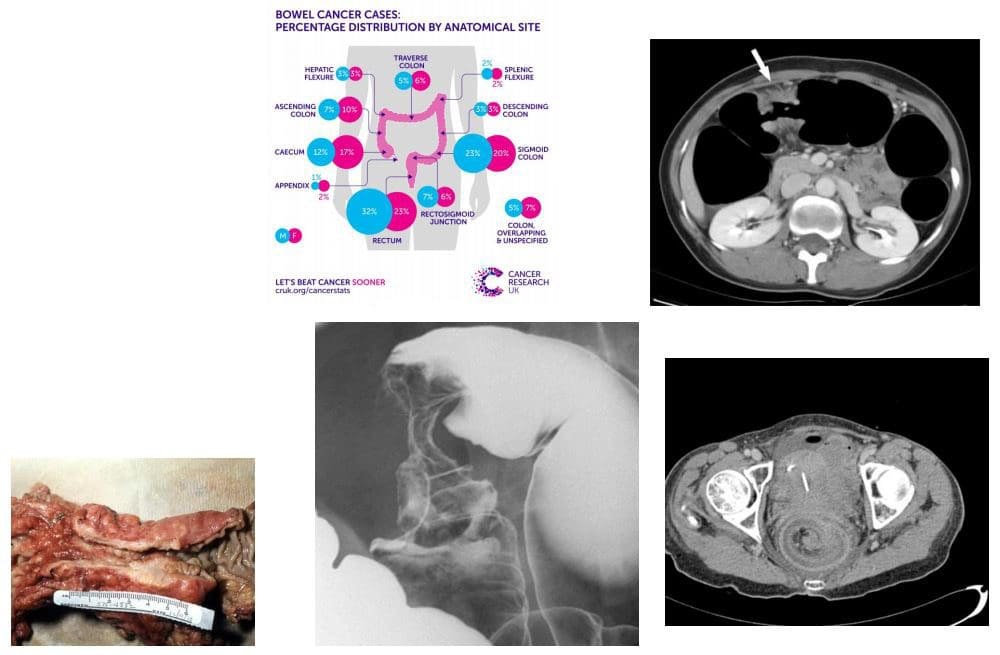
Colorectal carcinoma (CRC) m/c cancer of the GI tract and the 2nd most frequent malignancy in adults. Dx: endoscopy and biopsy. CT is the modalities most frequently used for staging. Surgical resection may be curative although the five-year survival rate is 40- 50% depending on staging. Risk factors: low fiber and high fat and animal protein diet, obesity (especially in men), chronic ulcerative colitis. Colonic adenomas (polyps). Familial adenomatous polyposis syndromes (Gardener syndrome) and Lynch syndrome as non-familial polyposis.
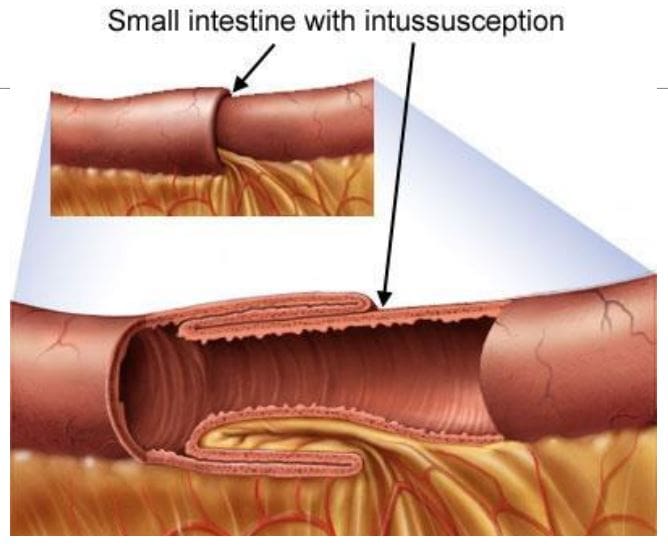
Clinically: insidious onset with altered bowel habits, fresh blood or melena, iron deficiency anemia from chronic occult blood loss especially in the right-sided tumors. Bowel obstruction, intussusception, heavy bleeding and metastatic disease especially to the Liver may be initial presentation. Path: 98% are adenocarcinomas, arise from pre-existing colonic adenomas (neoplastic polyps) with malignant transformation. The five-year survival rate is 40-50%, with stage at operation the single most important factor affecting prognosis. M/C rectosigmoid tumors (55%),
N.B. Some adenocarcinomas esp. mucinous types typically presented late and usually carry poor prognosis due to late presentation and mucin secretion and local/distant spread
Imaging: Barium enema is sensitivities for polyps >1 cm, single contrast: 77-94%, double contrast: 82-98%. Colonoscopy is a modality of choice for prevention, detection, and identification of colorectal carcinoma. Contrast-enhanced CT scanning is used for staging and prognosis evaluation of mets.
Screening: colonoscopy: men 50 y.o.-10-years if normal, 5-years if polypectomy, FOB, 1st degree relative with CA begin surveillance at 40 y.o
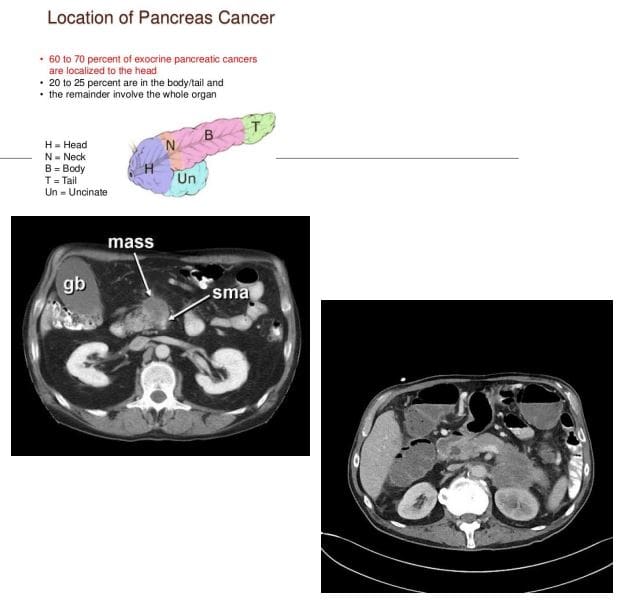
Pancreatic Cancer: ductal epithelial adenocarcinoma (90%), very poor prognosis with high mortality. 3rd M/C abdominal cancer. Colon is #1, stomach #2. Pancreatic cancer accounts for 22% of all deaths due to gastrointestinal malignancy, and 5% of all cancer deaths. 80% of cases in 60+. Cigarette smoking is the strongest environmental risk factor, a diet rich in animal fats and protein. Obesity. Family history. M/C detected in the head and uncinate process.
Dx: CT scanning is crucial. Invasion of Superior Mesenteric Artery (SMA) indicates unresectable disease. 90% of pancreatic adenocarcinomas are unresectable at Dx. Most patients die within 1-year of Dx. Clinically: painless jaundice, abd. Pain, Courvoisier�s gallbladder: painless jaundice and enlarged gallbladder, Trousseau�s syndrome: migratory thrombophlebitis, new onset diabetes mellitus, regional and distant metastasis.
CT Dx: pancreatic mass with strong desmoplastic reaction, poor enhancement, and slightly lower attenuation compared to the adjacent normal gland, SMA invasion.
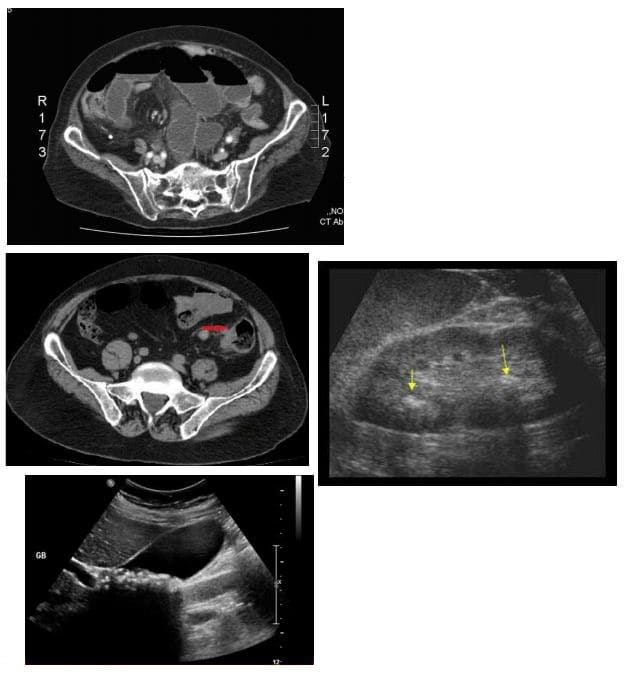
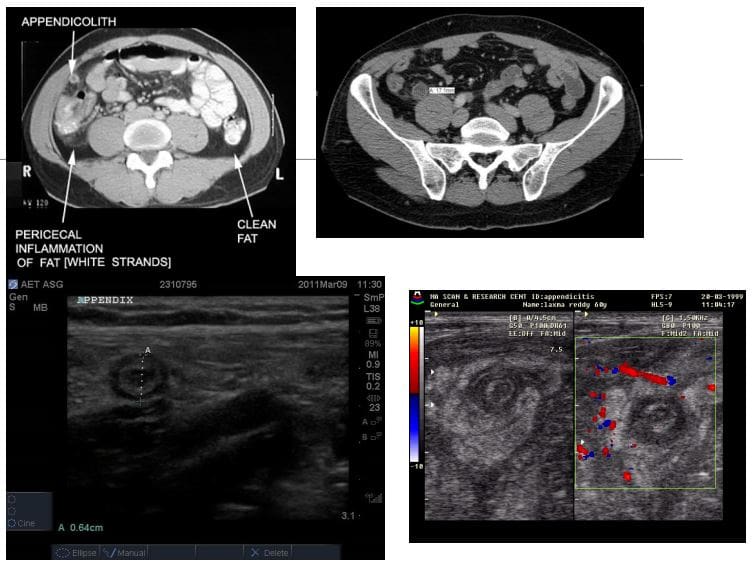
Appendicitis: very common condition in general radiology practice and is a major cause of abdominal surgery in young patients
CT is the most sensitive modality to detect appendicitis
Ultrasound should be employed in younger patients and children
KUB Radiographs should play no role in the diagnosis of appendicitis
On imaging, appendicitis reveals inflamed appendix with wall thickening, enlargement, and periappendiceal fat stranding. Similar findings of wall thickening and enlargement are noted on US. Typical �target sign� is noted on short axis US probe position.
If the appendix is retro-caecal than US may fail to provide accurate Dx and CT scanning may be required
Rx: operative to avoid complications
Small bowel obstruction (SBO)-80% of all mechanical intestinal obstruction; the remaining 20% result from large bowel obstruction. It has a mortality rate of 5.5%
M/C cause: any Hx of previous abdominal surgery and adhesions
Classical presentation is constipation, increasing abdominal distension with nausea and vomiting
Radiographs are only 50% sensitive for SBO
CT will demonstrate the cause of SBO in 80% of cases
There are variable criteria for maximal small bowel obstruction, but 3.5 cm is a conservative estimate of dilated bowel
On Abd x-ray: supine vs. upright. Dilated bowel, stretched valvulae conivente (mucosal folds), alternative air-fluid levels �step ladder.� Absent gas in the rectum/colon
Rx: operative as �acute abdomen.�
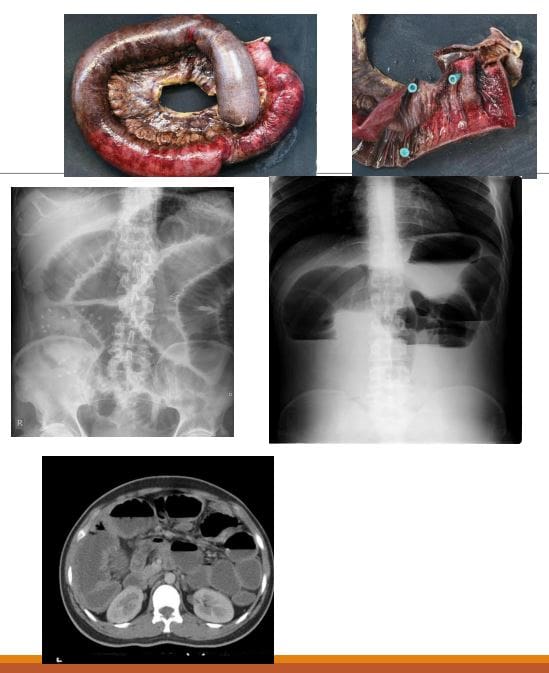
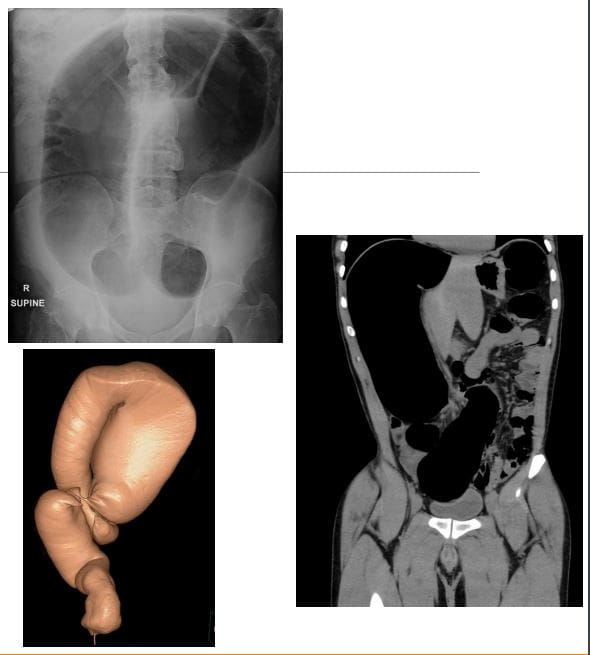
Volvulus-m/c in the Sigmoid colon esp. in elderly. The main reason: chronic constipation with redundant sigmoid twisting on sigmoid mesocolon. Leads to Large bowel obstruction (LBO). Other common causes: a colon tumor. Sigmoid vs. Caecum volvulus
Clinically: signs of LBO with constipation, abdominal bloating, pain, nausea, and vomiting. Onset may be acute or chronic
Radiographically: loss of haustra in the LB, LB distension (>6-cm), �coffee bean sign� next slide, the lower end of volvulus points to the pelvis
N.B: Rule of thumb for dilated bowel should be 3-6-9 where 3-cm SB, 6-cm LB & 9-cm Coecum
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine