
Whiplash has been difficult to study because its pathoanatomy has remained poorly known, however, the facet joints have been recently isolated as a site of pain in many people that are whiplash-injured.
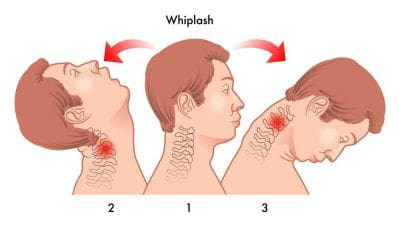
In a typical rear-end collision, the occupant’s pelvis, chest, and head are hastened forward in rapid succession. The massive inertia of the head leads to a horizontal translation (retraction) of the initially stationary head relative to the forward-accelerating torso, and this movement induces compression, shear, and ultimately tension in the cervical spine.
Recent studies have localized the chronic pain of several whiplash patients to the facet joints. Subsequent experiments involving both human subjects and cadaveric cells have demonstrated that harm to the capsular ligaments may play a part in the pathoanatomy of whiplash injury.
Contents
Kinematics of Whiplash Injuries
Biomechanical studies of whiplash injury have used human subjects, animals, cadavers, and mathematical models to investigate possible mechanisms of whiplash injury. Researcher ignorance of the tissues responsible for the pain has often limited the insights. Recent studies, however, has identified a candidate tissue for whiplash injury, and it has provided a focus for research into the mechanics of whiplash injury.
The comprehension of injury mechanics begins with an appreciation of how individuals respond to the kinds of perturbations that create whiplash injury. Rear-end collisions, where an occupant’s vehicle is struck from behind and hastened forward, have been associated with an increased risk of whiplash injury and a higher frequency of symptoms compared to other crash directions. As a result, perturbations that simulate a collision have been used by most biomechanical experiments conducted to investigate whiplash injury. Many research groups have studied subjects exposed to whiplash perturbations, and despite differences in subjects, vehicles, seats, and the crashes used with these groups, a stereotyped reaction has been observed in normally seated subjects.

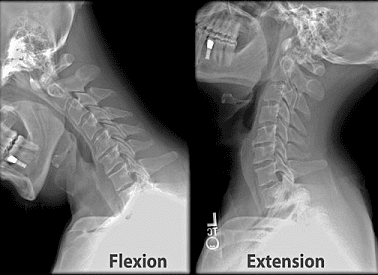
The pelvis is hastened forward, due to a combination of occupant posture and seat compliance, acceleration of the torso lags behind acceleration of the pelvis. This difference in motion between the pelvis and upper torso produces a small rotation of the torso and leads to an initial flexion of the neck, despite the fact that the head is still effectively stationary at this stage in the induced kinematic response. As the torso accelerates forward relative to the head, a horizontal translation develops between the base of the head and the spine, causing the lower vertebrae of the spine to extend. The horizontal shear stiffness of the upright spine is inadequate to overcome the rotational and transitional inertia of the head, and because of this, the upper cervical segments bend. The changing configuration of the vertebrae results in the cervical spine being better able to encourage horizontal forces, and these forces both accelerate the bottom of the skull forward and establish a rearward rotation (expansion) of the head.
In the presence of a properly positioned head restraint, both the head extension angle and the horizontal translation between the torso and head (retraction) are arrested and reversed by the combination of an external force applied to the head from the head restraint and inner forces developed by both the ligamentous cervical spine and the reflex contraction of the cervical muscles.
Larger extension and retraction motions occur, and head motion could be arrested and reversed by inner ligamentous and muscle forces if no head restraint is present or if there exists a gap between the back of the head and the head restraint. The positions of the head and head restraint at effect can therefore have a substantial influence on the magnitude of the head and neck kinematics, and ultimately on the size of the loads applied to the tissues of the cervical spine.
After the interaction with the seat back and head restraint, the head and chest rebound forward. Forward torso motion could be limited by a seatbelt, whereas forward motion of the mind seems to be controlled by sustained activation of the posterior neck muscles.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
By Dr. Alex Jimenez
Additional Topics: Automobile Accident Injuries
Whiplash, among other automobile accident injuries, are frequently reported by victims of an auto collision, regardless of the severity and grade of the accident. The sheer force of an impact can cause damage or injury to the cervical spine, as well as to the rest of the spine. Whiplash is generally the result of an abrupt, back-and-forth jolt of the head and neck in any direction. Fortunately, a variety of treatments are available to treat automobile accident injuries.

TRENDING TOPIC: EXTRA EXTRA: New PUSH 24/7�? Fitness Center
General Disclaimer, Licenses and Board Certifications *
Professional Scope of Practice *
The information herein on "Kinematics of Whiplash Associated Disorders" is not intended to replace a one-on-one relationship with a qualified health care professional or licensed physician and is not medical advice. We encourage you to make healthcare decisions based on your research and partnership with a qualified healthcare professional.
Blog Information & Scope Discussions
Welcome to El Paso's Premier Wellness and Injury Care Clinic & Wellness Blog, where Dr. Alex Jimenez, DC, FNP-C, a Multi-State board-certified Family Practice Nurse Practitioner (FNP-BC) and Chiropractor (DC), presents insights on how our multidisciplinary team is dedicated to holistic healing and personalized care. Our practice aligns with evidence-based treatment protocols inspired by integrative medicine principles, similar to those on this site and on our family practice-based chiromed.com site, focusing on naturally restoring health for patients of all ages.
Our areas of multidisciplinary practice include Wellness & Nutrition, Chronic Pain, Personal Injury, Auto Accident Care, Work Injuries, Back Injury, Low Back Pain, Neck Pain, Migraine Headaches, Sports Injuries, Severe Sciatica, Scoliosis, Complex Herniated Discs, Fibromyalgia, Complex Injuries, Stress Management, Functional Medicine Treatments, and in-scope care protocols.
Our information scope is multidisciplinary, focusing on musculoskeletal and physical medicine, wellness, contributing etiological viscerosomatic disturbances within clinical presentations, associated somato-visceral reflex clinical dynamics, subluxation complexes, sensitive health issues, and functional medicine articles, topics, and discussions.
We provide and present clinical collaboration with specialists from various disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for musculoskeletal injuries or disorders.
Our videos, posts, topics, and insights address clinical matters and issues that are directly or indirectly related to our clinical scope of practice.
Our office has made a reasonable effort to provide supportive citations and has identified relevant research studies that support our posts. We provide copies of supporting research studies upon request to regulatory boards and the public.
We understand that we cover matters that require an additional explanation of how they may assist in a particular care plan or treatment protocol; therefore, to discuss the subject matter above further, please feel free to ask Dr. Alex Jimenez, DC, APRN, FNP-BC, or contact us at 915-850-0900.
We are here to help you and your family.
Blessings
Dr. Alex Jimenez, DC, MSACP, APRN, FNP-BC*, CCST, IFMCP, CFMP, ATN
email: [email protected]
Multidisciplinary Licensing & Board Certifications:
Licensed as a Doctor of Chiropractic (DC) in Texas & New Mexico*
Texas DC License #: TX5807, Verified: TX5807
New Mexico DC License #: NM-DC2182, Verified: NM-DC2182
Multi-State Advanced Practice Registered Nurse (APRN*) in Texas & Multi-States
Multi-state Compact APRN License by Endorsement (42 States)
Texas APRN License #: 1191402, Verified: 1191402 *
Florida APRN License #: 11043890, Verified: APRN11043890 *
Colorado License #: C-APN.0105610-C-NP, Verified: C-APN.0105610-C-NP
New York License #: N25929, Verified N25929
License Verification Link: Nursys License Verifier
* Prescriptive Authority Authorized
ANCC FNP-BC: Board Certified Nurse Practitioner*
Compact Status: Multi-State License: Authorized to Practice in 40 States*
Graduate with Honors: ICHS: MSN-FNP (Family Nurse Practitioner Program)
Degree Granted. Master's in Family Practice MSN Diploma (Cum Laude)
Dr. Alex Jimenez, DC, APRN, FNP-BC*, CFMP, IFMCP, ATN, CCST
My Digital Business Card
Licenses and Board Certifications:
DC: Doctor of Chiropractic
APRNP: Advanced Practice Registered Nurse
FNP-BC: Family Practice Specialization (Multi-State Board Certified)
RN: Registered Nurse (Multi-State Compact License)
CFMP: Certified Functional Medicine Provider
MSN-FNP: Master of Science in Family Practice Medicine
MSACP: Master of Science in Advanced Clinical Practice
IFMCP: Institute of Functional Medicine
CCST: Certified Chiropractic Spinal Trauma
ATN: Advanced Translational Neutrogenomics
Memberships & Associations:
TCA: Texas Chiropractic Association: Member ID: 104311
AANP: American Association of Nurse Practitioners: Member ID: 2198960
ANA: American Nurse Association: Member ID: 06458222 (District TX01)
TNA: Texas Nurse Association: Member ID: 06458222
NPI: 1205907805
| Primary Taxonomy | Selected Taxonomy | State | License Number |
|---|---|---|---|
| No | 111N00000X - Chiropractor | NM | DC2182 |
| Yes | 111N00000X - Chiropractor | TX | DC5807 |
| Yes | 363LF0000X - Nurse Practitioner - Family | TX | 1191402 |
| Yes | 363LF0000X - Nurse Practitioner - Family | FL | 11043890 |
| Yes | 363LF0000X - Nurse Practitioner - Family | CO | C-APN.0105610-C-NP |
| Yes | 363LF0000X - Nurse Practitioner - Family | NY | N25929 |
Dr. Alex Jimenez, DC, APRN, FNP-BC*, CFMP, IFMCP, ATN, CCST
My Digital Business Card






