
Core Anatomy
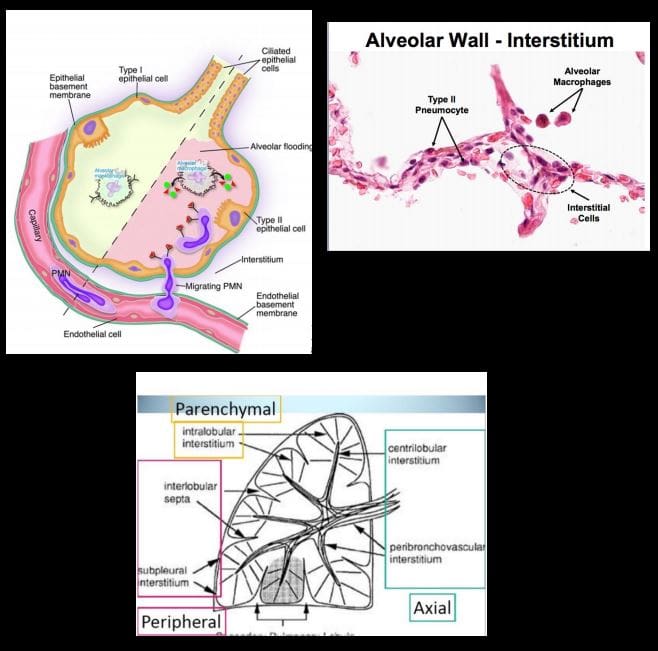
- Note generations of the tracheal-bronchial tree, lobes, segments, and fissures. Note secondary pulmonary lobule (1.5-2-cm)-the basic functional unit of lungs observed on HRCT. Note important structural organization of the alveolar spaces with communications in between (pores of Kohn & canals of Lambert) that permit air drift and by the same mechanism allow exudative or transudative fluid to spread through the lung and stopped at the fissure. Note the anatomy of the pleura: parietal that is a part of the endothoracic fascia and the visceral that forms a lung edge � pleural space in between.
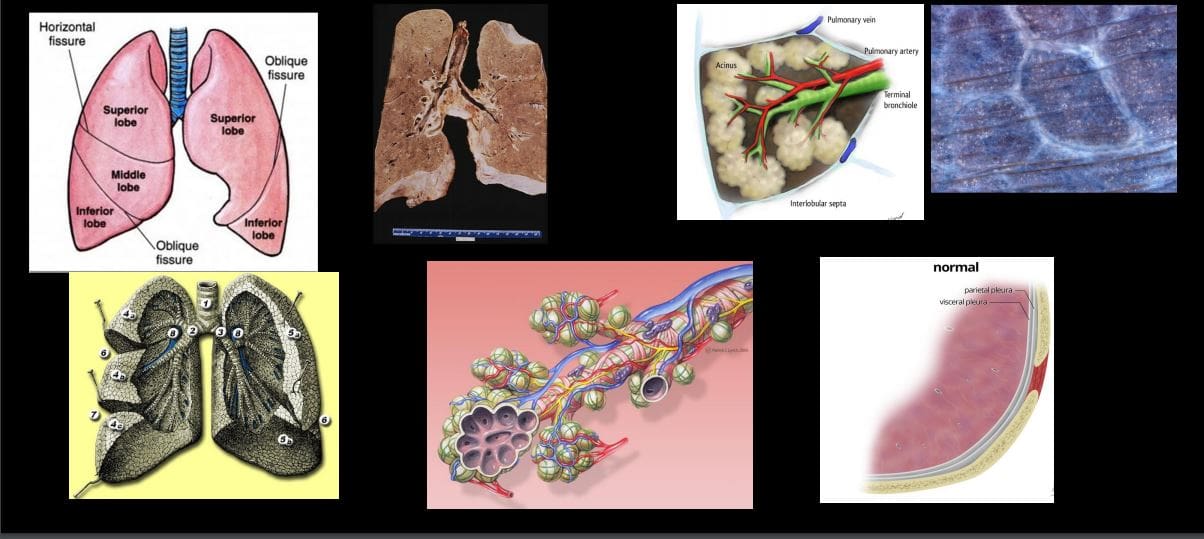
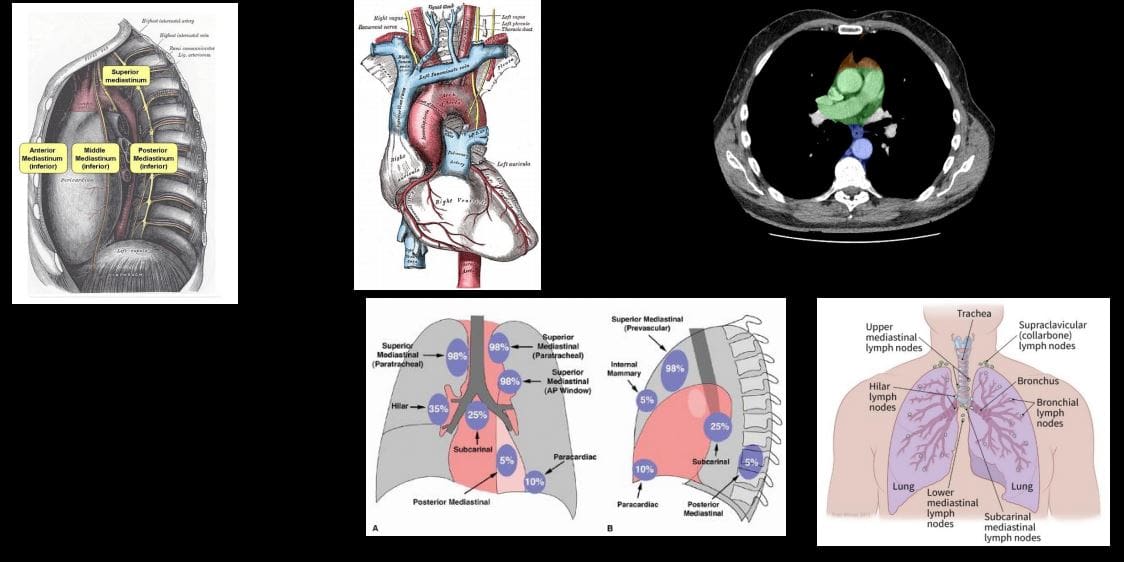
- Mediastinum: surrounded by the pleura and the lung. Accommodates major structures contains numerous lymph nodes (see diagramme showing mediastinal nodes and their involvement in Lymphoma
Contents
General Approach to Investigating Chest Complaints
- Radiographic examination (Chest X-ray CXR); excellent 1st step. Low cost, low radiation exposure, multiple clinical complaints evaluation
- CT scanning: chest CT, High-Resolution CT (HRCT)
- Chest pathology approach:
- Trauma
- Infection
- Neoplasms
- Pulmonary edema
- Pulmonary emphysema
- Atelectasis
- Pleural pathology
- Mediastinum
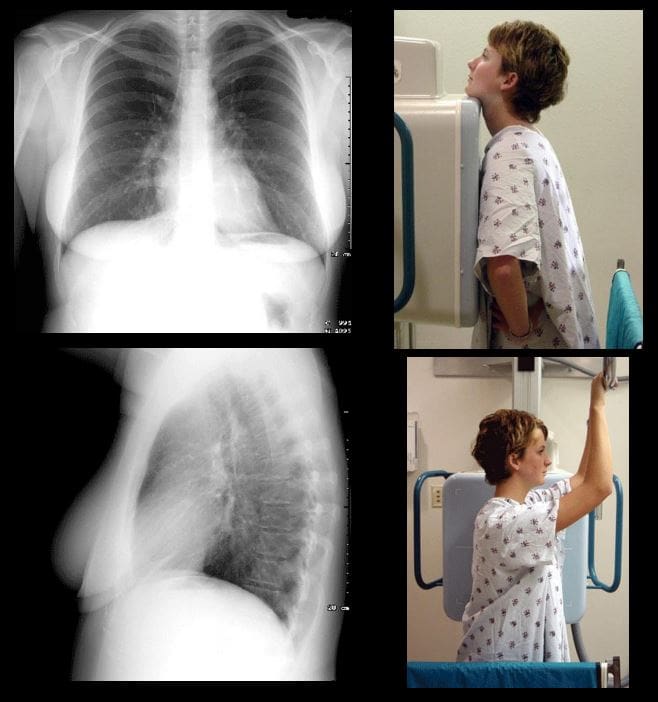
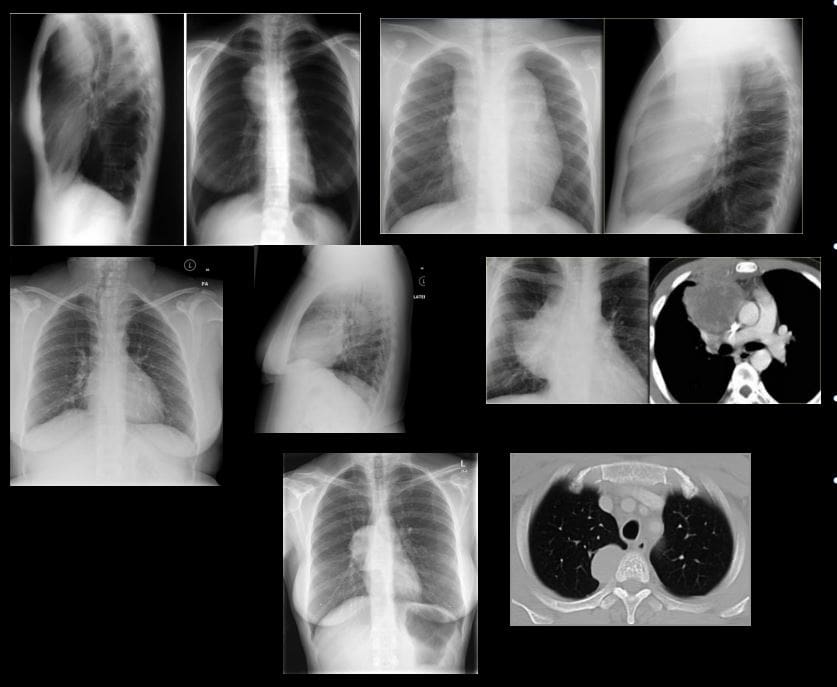
PA & Lateral CXR
- Additional views may be used:
- Lordotic view: helps to evaluate apical regions
- Decubitus views right and left: help to evaluate subtle pleural effusion, pneumothorax and other pathology
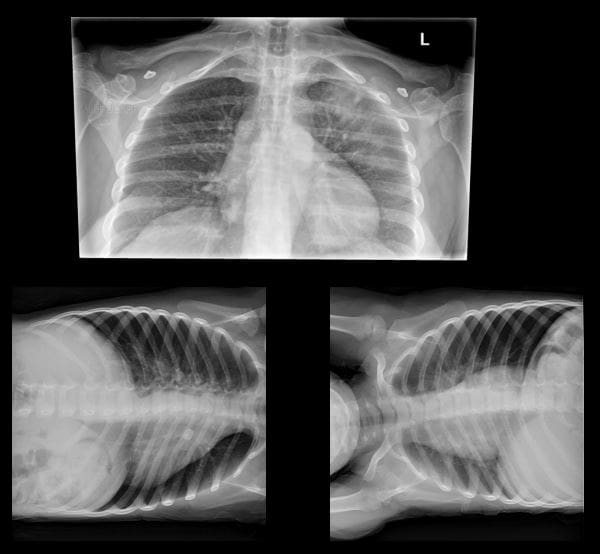
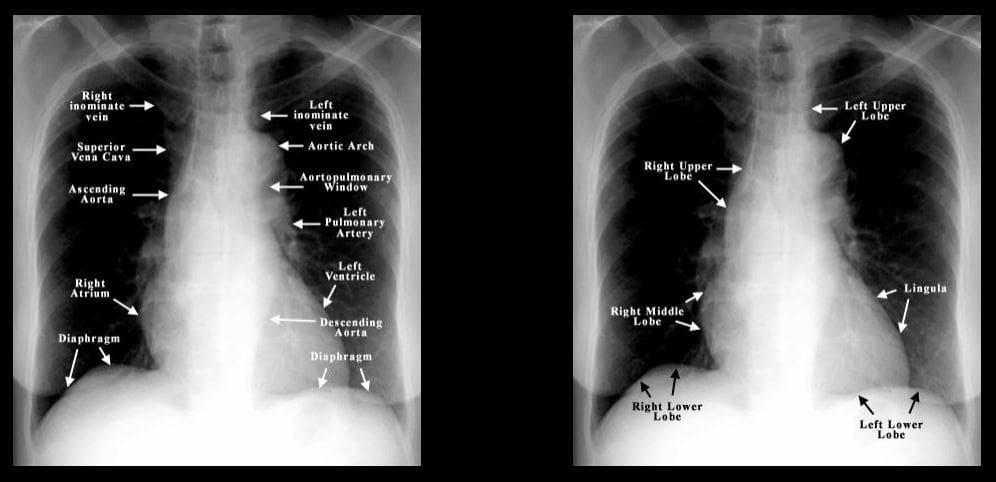
- Normal CXR PA & Lateral views. Ensure good exposure: T-spine discs and vessels through the heart are visualized on PA view. Count 9-10 right posterior ribs to confirm adequate inspiratory effort. Begin a thorough survey using the following approach: Are There Many Lung Lesions A-abdomen/diaphragm, T-thorax wall, M-mediastinum, L-lungs individually, Lungs-both. Develop a good search pattern
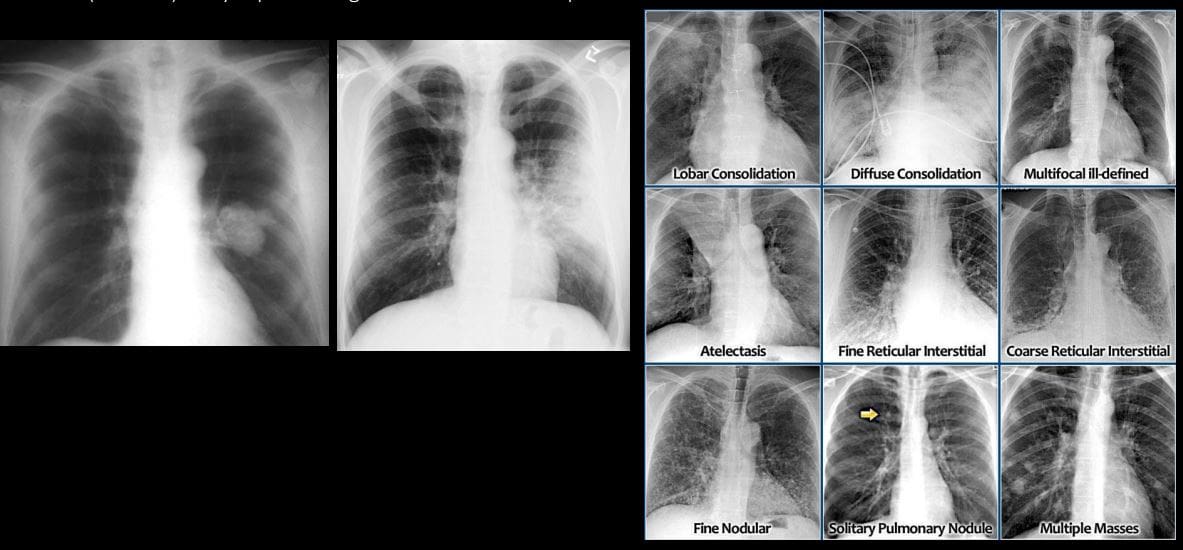
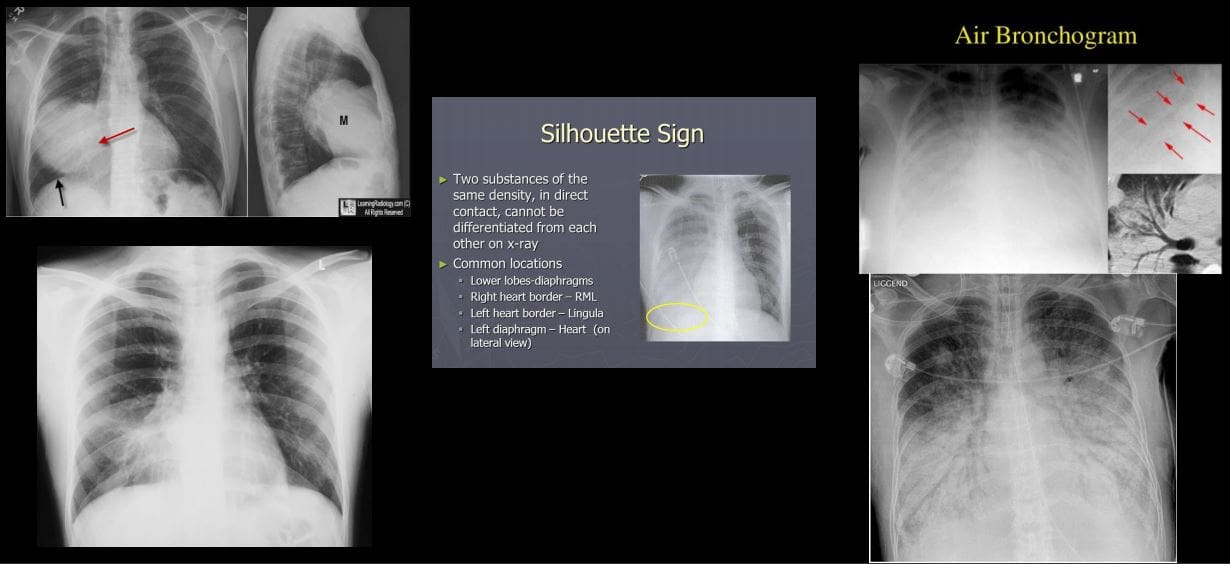
- 1) Airspace disease aka alveolar lung disease? Filling of the lung’s alveoli, acini and subsequently the entire lobe with fluid or substance of any composition (blood, pus, water, proteinaceous material or even cells) Radiographically: lobar or segmental distribution, airspace nodules may be noted, tendency to coalesce, air bronchograms and silhouette sign present. Batwing (butterfly) distribution noted as in (CHF). Rapidly changing over time, i.e., increase or decrease (days)
- 2) Interstitial disease: infiltration of pulmonary interstitium (alveoli septum, lung parenchyma, vessel walls, etc.) by for example by viruses, small bacteria, protozoans. Also infiltration by cells such as inflammatory/malignant cells (e.g., lymphocytes) Presented as an accentuation of lung interstitium with a reticular, nodular, mixed reticulonodular pattern. Different etiologies: inflammatory autoimmune diseases, fibrosing lung disease, occupational lung disease, viral/mycoplasma infection, TB, sarcoidosis lymphoma/leukemia and many other.
- Recognizing different patterns of pulmonary disease can help with DDx. Mass vs. Consolidation (left). Note different patterns of pulmonary disease: airspace disease as lobar consolidation indicative of pneumonia, diffuse consolidation indicative of pulmonary edema. Atelectasis (collapse and volume loss). Interstitial patterns of pulmonary disease: reticular, nodular or mixed. SPN vs. Multiple focal consolidations (nodules) likely representing mets infiltrates vs. septic infiltrates
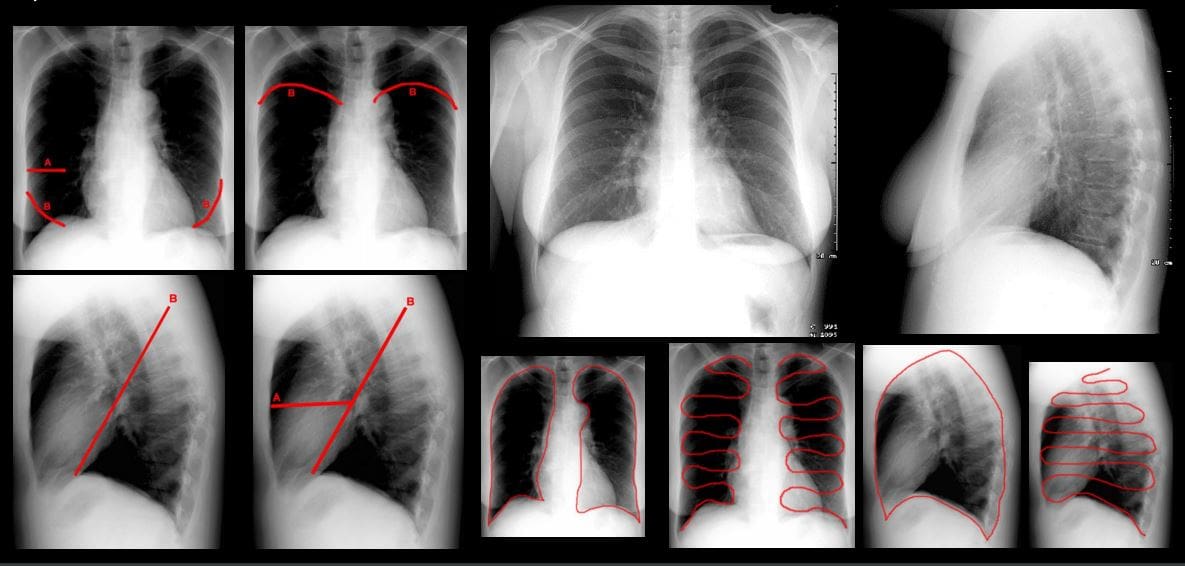
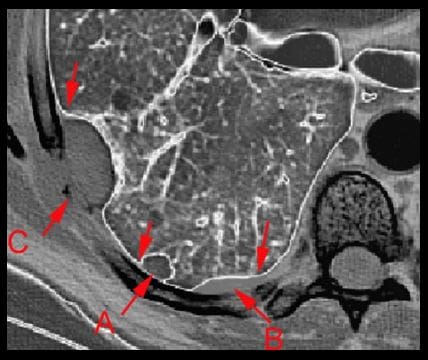
- A = intraparenchymal
- B = pleural
- C = extrapleura
- Recognize important location of chest lesions
- Important signs: Silhouette sign: help with localization and DDx. Example: Bottom left image: radiopacity in the right lung, where is it located? Right MM because the right heart border that is adjacent to right middle lobe is not seen (silhouetted) Air bronchograms: air containing bronchi/bronchioles surrounded by fluid
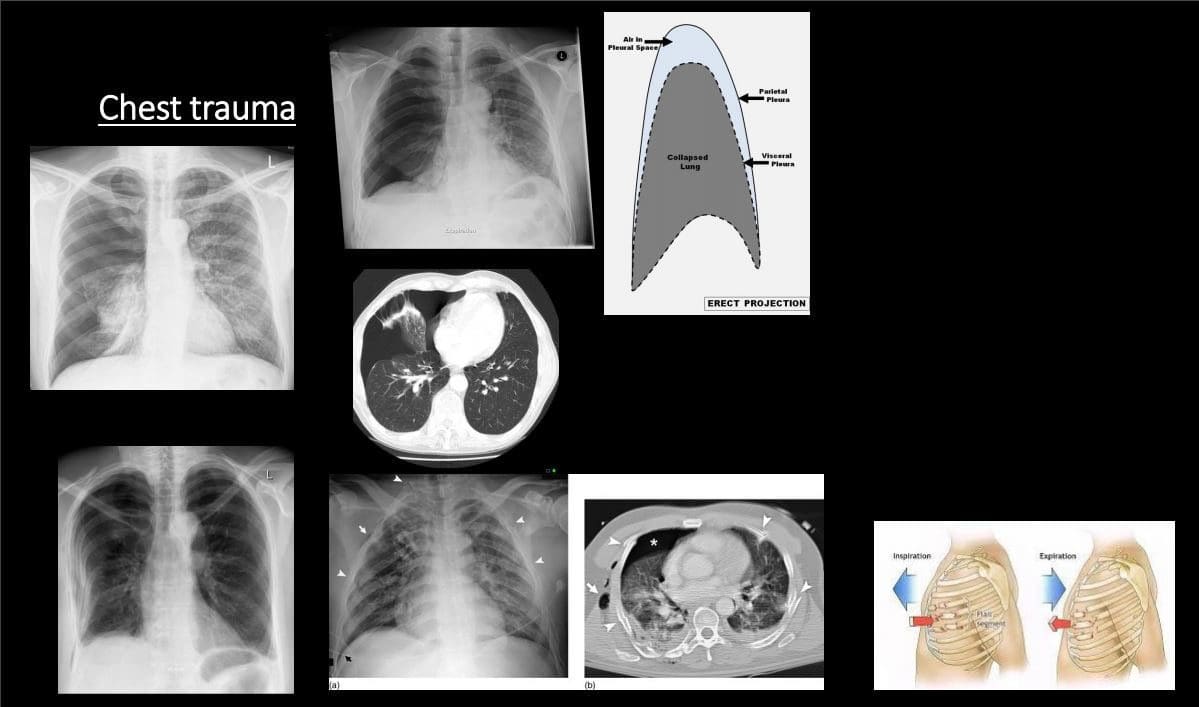
Chest Trauma
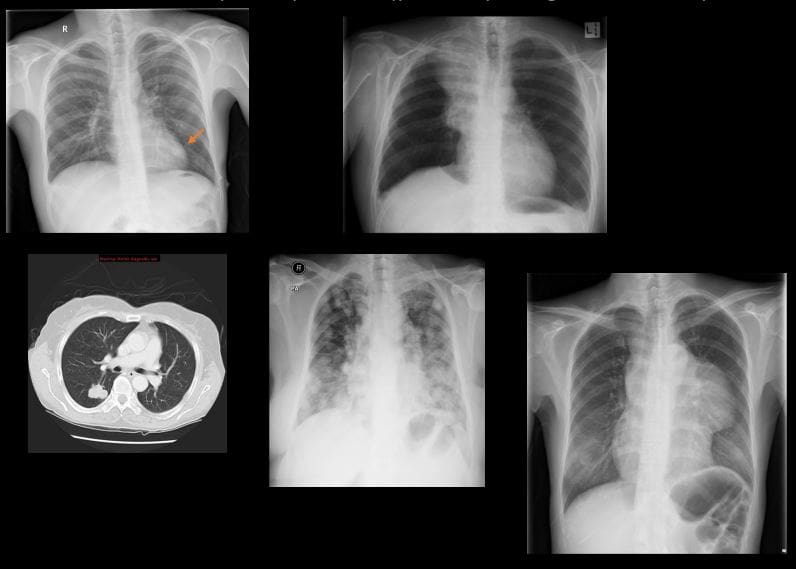
- Pneumothorax (PTX): air (gas) in the pleural space. Many causes. Complications:
- Tension PTX: continuous increase of air in the pleural space that rapidly compresses mediastinum and lung rapidly reducing venous return to the heart. It can be fatal if not treated rapidly
- Spontaneous PTX: primary (young adults (30 -40) especially tall, thin men. Additional causes: Marfan�s syndrome, EDS, Homocystinuria, a – 1 -antitrypsin deficiency. Secondary: older pts with parenchymal disease: neoplasms, abscess, emphysema, lung fibrosis and honeycombing, catamenial PTX d/t endometriosis and others.
- Traumatic pneumothorax: lung laceration, blunt trauma, iatrogenic (chest tubes, etc.) acupuncture, etc.
- CXR: note visceral pleural line aka lung edge. An Absence of pulmonary tissue/vessels beyond the visceral pleural line. Subtle pneumothorax can be missed. On erect position, air rises and PTX should be sought at the top.
- Rib fractures: v.common. Traumatic or pathological (e.g., mets, MM) Rib series x – rays are not very useful because CXR and/or CT scanning are more important to evaluate posttraumatic PTX (bottom left) lung laceration and another major path
Infection
- Pneumonia: bacterial vs. viral or fungal or in the immunocompromised host (e.g., Cryptococcus in HIV/AIDS) Pulmonary TB
- Pneumonia: community-acquired vs. hospital-acquired. Typical bacterial pneumonia or Lobar (non-segmental) pneumonia with purulent material filling the alveoli and spreading to the entire lobe. M/C organismStreptococcus Pneumonia or the Pneumococcus
- Others: (Staph, Pseudomonas, Klebsiella esp. in alcoholics potentially leading to necroSIS/lung gangrene) Mycoplasma (20-30s) aka walking pneumonia, etc.
- Clinically: a productive cough, fever, pleuritic chest pain sometimes hemoptysis.
- CXR: confluent airspace opacity confined to the entire lobe. Air bronchograms. Silhouette sign help with location.
- Viral: Influenza, VZV, HSV, EBV, RSV, etc. presents as interstitial lung disease that can be bilateral. May lead to respiratory compromise
- Atypical pneumonia and Fungal Pneumonia: Mycoplasma, Legionnaire’s disease, and some fungal/Cryptococcus pneumonia may present with interstitial lung disease.
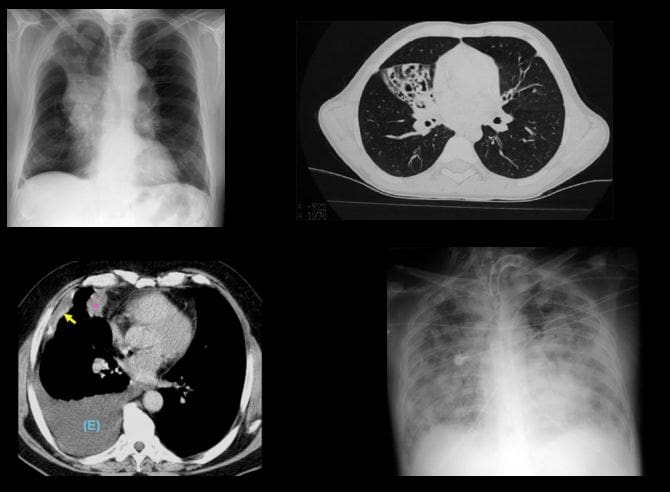
- Pulmonary abscess: an infectious collection of purulent material in the lungs that often necrotizes. May lead to significant pulmonary and system complications/life-threatening.
- On CXR or CT: round collection with thick borders and central necrosis containing air-fluid level. DDx from empyema that distorts the lung and pleural-based
- Rx: antibiotics, antifungal, antiviral agents.
- Pneumonia needs to be followed up with repeat CXR to ensure complete resolution
- Lack of radiographic improvement of pneumonia may represent declined immunity, antibiotic resistance, underlying lung carcinoma or other complicating factors
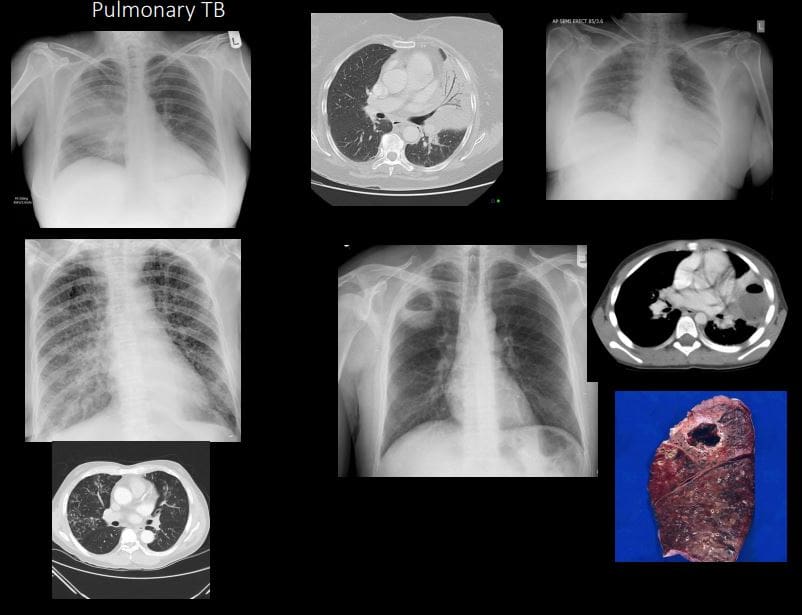
Pulmonary TB
- Common infection worldwide (3rd world countries). 1 in 3 persons worldwide is affected by TB. TB is caused by Mycobacterium TB or Mycobacterium Bovis. Intracellular bacillus. Macrophage plays a key role.
- Primary Pulmonary TB & Post-primary TB. Requires repeated exposure through inhalation. In most immunocompetent hosts, the active infection does not develop
- TB presents as 1) cleared by the host, 2) suppressed into Latent Tuberculosis Infection (LTBI) 3) cause active disease TB. Patients with LTBI are not spreading TB.
- Imaging: CXR, HRCT. Primary TB: pulmonary airspace consolidation (60%) lower lobes, lymphadenopathy (95%- hilar & paratracheal), pleural effusion (10%). The Spread of primary TB most likely in immunocompromised and children.
- Milliary TB: pulmonary and system complication dissemination that can be fatal
- Post-primary (secondary) or reactivation infection: Mostly in the Apices and posterior segments of the upper lobes )high PO2), 40%-cavitating lesions, patchy or confluent airspace disease, fibrocalcific. Latent features: nodal calcifications.
- Dx: Acid-fast bacilli (AFB) smear and culture (sputum). HIV serology in all patients with TB and unknown HIV status
- Rx: 4-drug regimen: isoniazid, rifampin, pyrazinamide, and either ethambutol or streptomycin.
Pulmonary Neoplasms (primary lung cancer vs. pulmonary metastasis)
- Lung cancer: m/c cancer in men and 6th most frequent cancer in women. Strong association with carcinogens inhalation. Clinically: late discovery, depending on the location of the tumor. Pathology (types): Small cell (SCC) vs. Non-small cell carcinoma
- Small cell: (20%) develops from neuroendocrine aka Kultchitsky cell, thus may secrete biologically active substances presenting with paraneoplastic syndrome. Typically located centrally (95%) at or near the mainstem/lobar bronchus. Most show poor prognosis and unresectable.
- Non-small cell: Lung adenocarcinoma (40%) (M/C lung cancer), M/C in women and non-smokers. Others: Squamous cell (may present with cavitating lesion), Large cell and some others
- Plain film (CXR): new or enlarged focal lesion, widened mediastinum suggestive of lymph node involvement, pleural effusion, atelectasis, and consolidation. SPN-may represents potential lung cancer especially if it contains irregular borders, feeding vessels, thick wall, in the upper lungs. Multiple lung nodules are likely to represent metastasis.
- Best Modality: HRCT with contrast.
- Other chest neoplasms: Lymphoma is v. common in the chest especially in mediastinal and internal mammary notes.
- Overall M/C pulmonary neoplasms are a metastasis. Some tumors show a higher predilection for lung mets, e.g., Melanoma, but any cancer can metastasize to the lungs. Some mets referred as �Cannonball� metastasis
- Rx: radiation, chemotherapy, resection
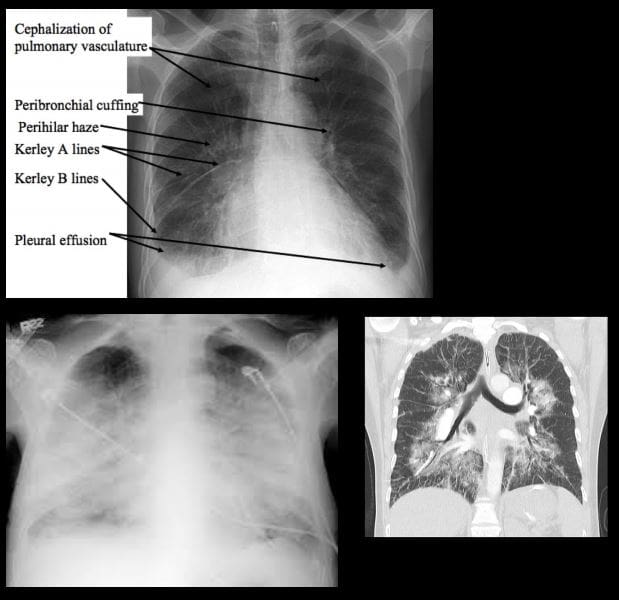
- Pulmonary edema: a general term defines abnormal fluid accumulation outside vascular structures. Broadly divided into Cardiogenic (e.g., CHF, mitral regurgitation) and Non-cardiogenic with a multitude of causes (e.g., fluid overload, post-transfusion, neurological causes, ARDS, near drowning/asphyxiation, heroin overdose, and others)
- Causes: increased in Hydrostatic pressure vs. decreased in oncotic pressure.
- Imaging: CXR and CT: 2-types Interstitial and Alveolar flooding. Imaging presentation depends on stages
- In CHF: Stage 1: redistribution of vascular flow (10- 18-mm Hg) noted as �cephalization� of the pulmonary vasculature. Stage 2: Interstitial edema (18-25-mm Hg) Interstitial edema: peribronchial cuffing, Kerley lines (lymphatics filled with fluid) A, B, C lines. Stage 3: Alveolar edema: airspace disease: patchy consolidations developing into diffuse airspace disease: Batwing edema, air bronchograms
- Rx: 3 main goals: Initial O2 to keep O2 at 90% saturation
- Next: (1) reduction of pulmonary venous return (preload reduction), (2) reduction of systemic vascular resistance (afterload reduction), and (3) inotropic support. Treat underlying causes (e.g., CHF)
- Lung atelectasis: incomplete expansion of pulmonary parenchyma. The term “collapsed lung” is typically reserved for when the entire lung is collapsed
- 1) Resorptive (obstructive) atelectasis occurs as a result of complete obstruction of an airway (e.g. tumor, inhaled objects, etc.)
- 2) Passive (relaxation) atelectasis occurs when contact between the parietal and visceral pleura is disrupted (pleural effusion & pneumothorax)
- 3) Compressive atelectasis occurs as a result of any thoracic space-occupying lesion compressing the lung and forcing air out of the alveoli
- 4) Cicatricial atelectasis: occur as a result of scarring or fibrosis that reduces lung expansion as in granulomatous disease, necrotizing pneumonia, and radiation fibrosis
- 5) Adhesive lung atelectasis occurs from surfactant deficiency and alveolar collapse
- 6) Plate-like or discoid often developed after following general anesthesia
- 7) Imaging features: lung collapse, migration of lung fissures, deviation of the mediastinum, rising of the diaphragm, hyperinflation of adjacent unaffected lung
- Mediastinum: pathology can be divided into those that result in a focal mass or those that result in diffuse disease involving the mediastinum. Additionally, air may track into the mediastinum in pneumomediastinum. Knowledge of mediastinal anatomy helps the Dx.
- Anterior mediastinal masses: thyroid, thymus, teratoma/germ cell tumors, lymphoma, lymphadenopathy, ascending aortic aneurysms
- Middle mediastinal masses: lymphadenopathy, vascular, bronchial lesions etc.
- Posterior mediastinal masses: neurogenic tumours, aortic aneurysms, esophageal masses, spinal masses, aortic chain adenopathy
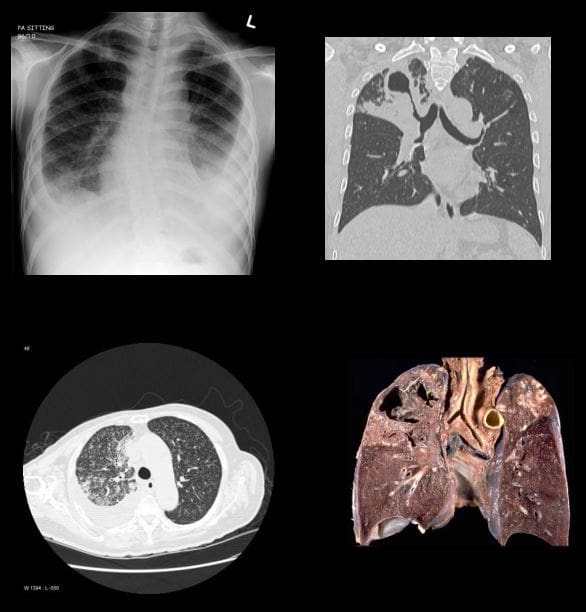
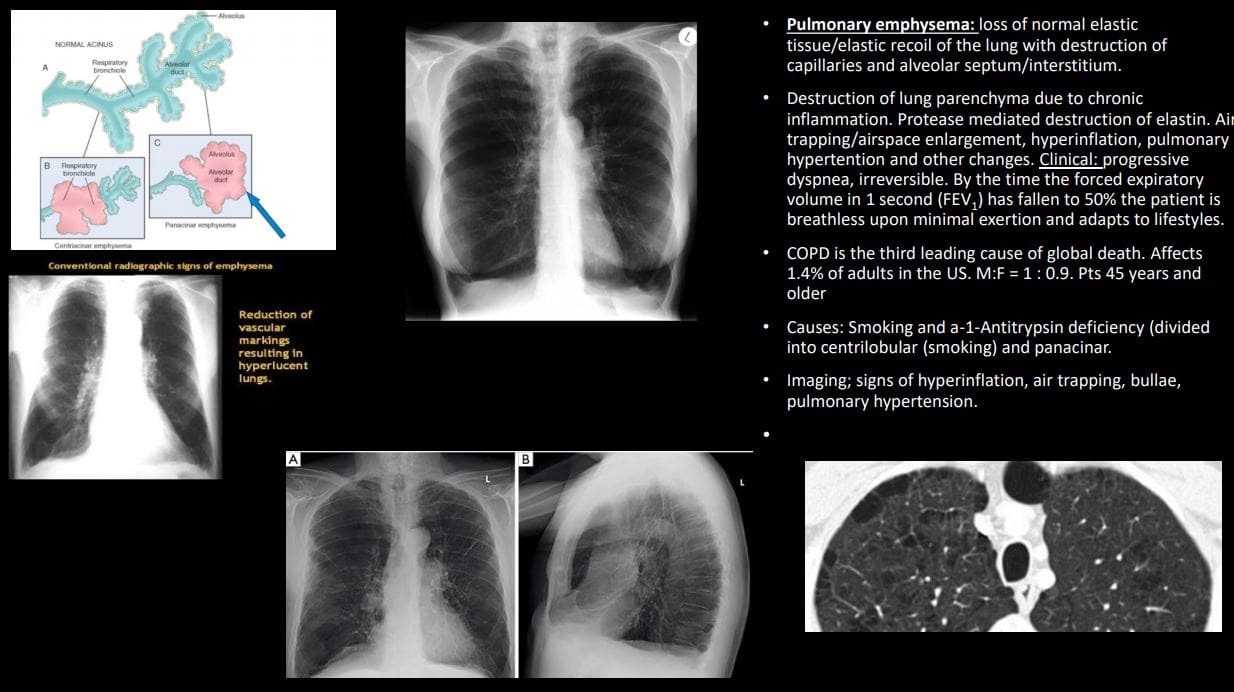
- Pulmonary emphysema: loss of normal elastic tissue/elastic recoil of the lung with the destruction of capillaries and alveolar septum/interstitium.
- Destruction of lung parenchyma due to chronic inflammation. Protease-mediated destruction of elastin. Air trapping/airspace enlargement, hyperinflation, pulmonary hypertension, and other changes. Clinical: progressive dyspnea, irreversible. By the time the forced expiratory volume in 1 second (FEV1 ) has fallen to 50% the patient is breathless upon minimal exertion and adapts to lifestyles.
- COPD is the third leading cause of global death. Affects 1.4% of adults in the US. M:F = 1 : 0.9. Pts 45 years and older
- Causes: Smoking and a-1-Antitrypsin deficiency (divided into centrilobular (smoking) and panacinar.
- Imaging; signs of hyperinflation, air trapping, bullae, pulmonary hypertension.
General Disclaimer, Licenses and Board Certifications *
Professional Scope of Practice *
The information herein on "Diseases Of The Chest Approach To Diagnostic Imaging" is not intended to replace a one-on-one relationship with a qualified health care professional or licensed physician and is not medical advice. We encourage you to make healthcare decisions based on your research and partnership with a qualified healthcare professional.
Blog Information & Scope Discussions
Welcome to El Paso's Premier Wellness and Injury Care Clinic & Wellness Blog, where Dr. Alex Jimenez, DC, FNP-C, a Multi-State board-certified Family Practice Nurse Practitioner (FNP-BC) and Chiropractor (DC), presents insights on how our multidisciplinary team is dedicated to holistic healing and personalized care. Our practice aligns with evidence-based treatment protocols inspired by integrative medicine principles, similar to those on this site and on our family practice-based chiromed.com site, focusing on naturally restoring health for patients of all ages.
Our areas of multidisciplinary practice include Wellness & Nutrition, Chronic Pain, Personal Injury, Auto Accident Care, Work Injuries, Back Injury, Low Back Pain, Neck Pain, Migraine Headaches, Sports Injuries, Severe Sciatica, Scoliosis, Complex Herniated Discs, Fibromyalgia, Complex Injuries, Stress Management, Functional Medicine Treatments, and in-scope care protocols.
Our information scope is multidisciplinary, focusing on musculoskeletal and physical medicine, wellness, contributing etiological viscerosomatic disturbances within clinical presentations, associated somato-visceral reflex clinical dynamics, subluxation complexes, sensitive health issues, and functional medicine articles, topics, and discussions.
We provide and present clinical collaboration with specialists from various disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for musculoskeletal injuries or disorders.
Our videos, posts, topics, and insights address clinical matters and issues that are directly or indirectly related to our clinical scope of practice.
Our office has made a reasonable effort to provide supportive citations and has identified relevant research studies that support our posts. We provide copies of supporting research studies upon request to regulatory boards and the public.
We understand that we cover matters that require an additional explanation of how they may assist in a particular care plan or treatment protocol; therefore, to discuss the subject matter above further, please feel free to ask Dr. Alex Jimenez, DC, APRN, FNP-BC, or contact us at 915-850-0900.
We are here to help you and your family.
Blessings
Dr. Alex Jimenez, DC, MSACP, APRN, FNP-BC*, CCST, IFMCP, CFMP, ATN
email: [email protected]
Multidisciplinary Licensing & Board Certifications:
Licensed as a Doctor of Chiropractic (DC) in Texas & New Mexico*
Texas DC License #: TX5807, Verified: TX5807
New Mexico DC License #: NM-DC2182, Verified: NM-DC2182
Multi-State Advanced Practice Registered Nurse (APRN*) in Texas & Multi-States
Multi-state Compact APRN License by Endorsement (42 States)
Texas APRN License #: 1191402, Verified: 1191402 *
Florida APRN License #: 11043890, Verified: APRN11043890 *
Colorado License #: C-APN.0105610-C-NP, Verified: C-APN.0105610-C-NP
New York License #: N25929, Verified N25929
License Verification Link: Nursys License Verifier
* Prescriptive Authority Authorized
ANCC FNP-BC: Board Certified Nurse Practitioner*
Compact Status: Multi-State License: Authorized to Practice in 40 States*
Graduate with Honors: ICHS: MSN-FNP (Family Nurse Practitioner Program)
Degree Granted. Master's in Family Practice MSN Diploma (Cum Laude)
Dr. Alex Jimenez, DC, APRN, FNP-BC*, CFMP, IFMCP, ATN, CCST
My Digital Business Card
Licenses and Board Certifications:
DC: Doctor of Chiropractic
APRNP: Advanced Practice Registered Nurse
FNP-BC: Family Practice Specialization (Multi-State Board Certified)
RN: Registered Nurse (Multi-State Compact License)
CFMP: Certified Functional Medicine Provider
MSN-FNP: Master of Science in Family Practice Medicine
MSACP: Master of Science in Advanced Clinical Practice
IFMCP: Institute of Functional Medicine
CCST: Certified Chiropractic Spinal Trauma
ATN: Advanced Translational Neutrogenomics
Memberships & Associations:
TCA: Texas Chiropractic Association: Member ID: 104311
AANP: American Association of Nurse Practitioners: Member ID: 2198960
ANA: American Nurse Association: Member ID: 06458222 (District TX01)
TNA: Texas Nurse Association: Member ID: 06458222
NPI: 1205907805
| Primary Taxonomy | Selected Taxonomy | State | License Number |
|---|---|---|---|
| No | 111N00000X - Chiropractor | NM | DC2182 |
| Yes | 111N00000X - Chiropractor | TX | DC5807 |
| Yes | 363LF0000X - Nurse Practitioner - Family | TX | 1191402 |
| Yes | 363LF0000X - Nurse Practitioner - Family | FL | 11043890 |
| Yes | 363LF0000X - Nurse Practitioner - Family | CO | C-APN.0105610-C-NP |
| Yes | 363LF0000X - Nurse Practitioner - Family | NY | N25929 |
Dr. Alex Jimenez, DC, APRN, FNP-BC*, CFMP, IFMCP, ATN, CCST
My Digital Business Card






