
Clinical Prediction Rules:
Contents
“Clinical decision rules, spinal pain classification and prediction of treatment outcome: A discussion of recent reports in the rehabilitation literature”
Abstract
Clinical decision rules are an increasingly common presence in the biomedical literature and represent one strategy of enhancing clinical-decision making to improve the efficiency and effectiveness of healthcare delivery. In the context of rehabilitation research, clinical decision rules have been predominantly aimed at classifying patients by predicting their treatment response to specific therapies. Traditionally, recommendations for developing clinical decision rules propose a multistep process (derivation, validation, impact analysis) using the defined methodology. Research efforts aimed at developing a diagnosis-based clinical decision rule have departed from this convention. Recent publications in this line of research have used the modified terminology diagnosis-based clinical decision guide. Modifications to terminology and methodology surrounding clinical decision rules can make it more difficult for clinicians to recognize the level of evidence associated with a decision rule and understand how this evidence should be implemented to inform patient care. We provide a brief overview of clinical decision rule development in the context of the rehabilitation literature and two specific papers recently published in Chiropractic and Manual Therapies.
Clinical Prediction Rules
- Healthcare has undergone an important paradigm shift toward evidence-based practice. An approach thought to enhance clinical decision-making by integrating the best available evidence with clinical expertise and patients’ preferences.
- Ultimately, the goal of evidence-based practice is to improve healthcare delivery. However, the translation of scientific evidence into practice has proven a challenging endeavor.
- Clinical decision rules (CDRs), also known as clinical prediction rules, are increasingly common in the rehabilitation literature.
- These are tools designed to inform clinical decision-making by identifying potential predictors of diagnostic test outcome, prognosis, or therapeutic response.
- In the rehabilitation literature, CDRs are most commonly used to predict a patient’s response to treatment. They have been proposed to identify clinically relevant subgroups of patients presenting with otherwise heterogeneous disorders such as non-specific neck or low back pain, which is the perspective on which we intend to focus.
Clinical Prediction Rules
- The ability to classify or subgroup patients with heterogeneous disorders such as spinal pain has been highlighted as a research priority and, consequently, the focus of much research effort. The appeal of such classification approaches is their potential for improved treatment efficiency and effectiveness by matching patients with optimal therapies. In the past, patient classification has relied on implicit approaches founded in tradition or unsystematic observations. The use of CDRs to inform classification is one attempt at a more evidence-driven approach, less dependent on unfounded theory.
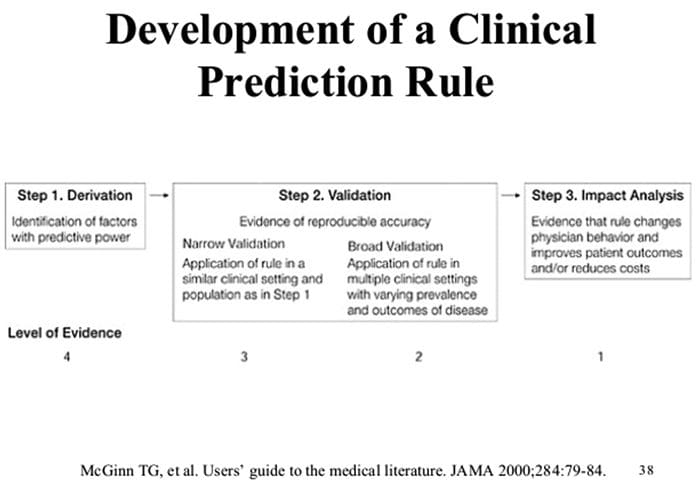
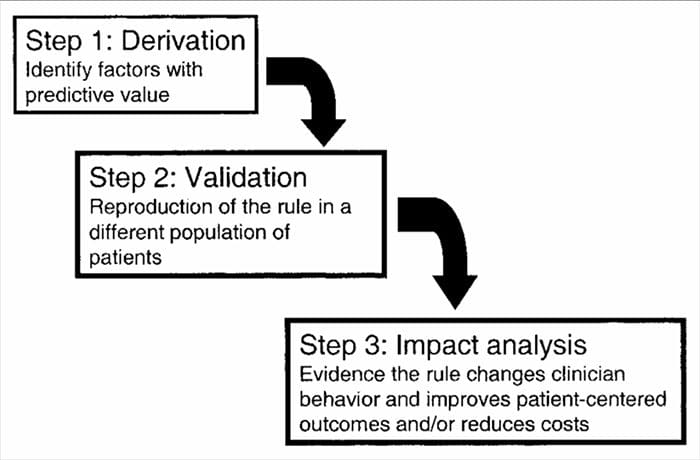
- CDRs are developed in a multistep process involving studies of derivation, validation, and analysis of impact, with each having a defined purpose and methodological criteria. As with all forms of evidence used to make decisions about patients, attention to appropriate study methodology is critical to assessing the potential benefits of implementation.
Benefits Of Clinical Prediction Rules
- It can accommodate more factors than the human brain can take into account
- CDR/CPR model will always give the same result (mathematical equation)
- It can be more accurate than clinical judgment.
Clinical Uses Of Clinical Prediction Rules
- Diagnosis � Pretest probability
- Prognosis � Predict risk of outcomes of disease
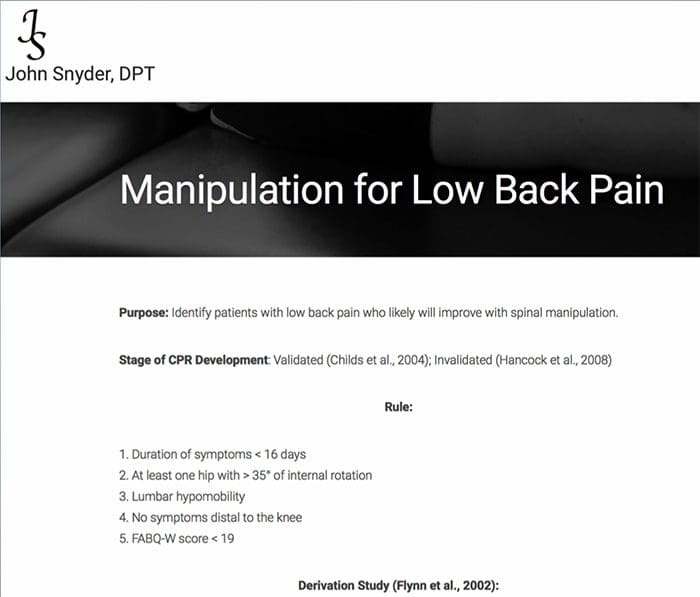
https://johnsnyderdpt.com/for-clinicians/clinical-prediction-rules/manipulation-for-low-back-pain
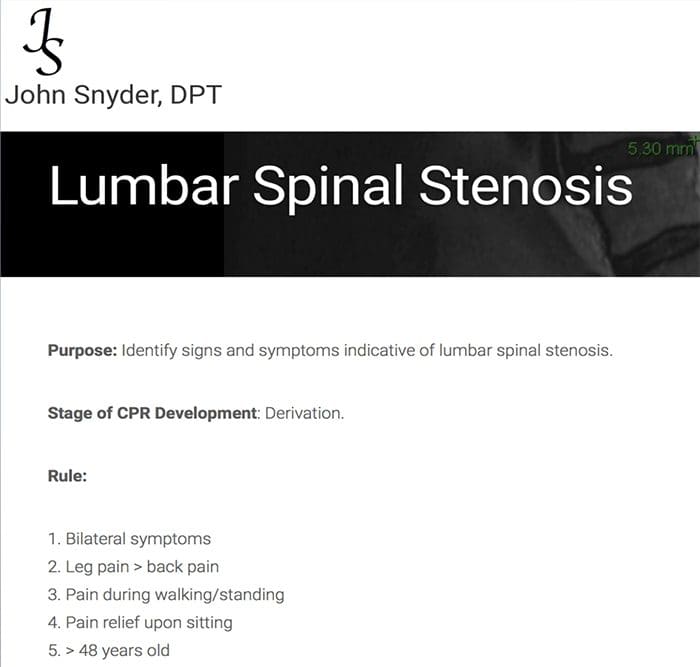
https://johnsnyderdpt.com/for-clinicians/clinical-prediction-rules/lumbar-spinal-stenosis/
Dr. John Snyder’s Website
Flynn Clinical Prediction Rule Video
CDR Analysis Of Impact
Ultimately, the usefulness of a CDR lies not with its accuracy but with its ability to improve clinical outcomes and enhance the efficiency of care.[15] Even when a CDR demonstrates broad validation, this does not ensure that it will change clinical decision-making or that the changes it produces will result in better care.
The changes it produces will result in better care. McGinn et al.[2] identified three explanations for the failure of a CDR at this stage. First, if clinician judgment is as accurate as a CDR-informed decision, there is no benefit to its use. Second, the application of a CDR may involve cumbersome calculations or procedures which discourage clinicians from utilizing the CDR. Third, using the CDR may not be feasible in all environments or circumstances. In addition, we would include the reality that experimental studies may involve patients that are not entirely representative of those seen in routine care and that this may limit the actual value of a CDR. Therefore, to fully understand the utility of a CDR and its ability to improve healthcare delivery, it is necessary to undertake a pragmatic examination of its feasibility and impact when applied in an environment reflecting real-world practice. This can be undertaken with different study designs such as randomized trials, cluster-randomized trials, or other approaches such as examining the impact of a CDR before and after its implementation.
Prevalence of classification methods for patients with lumbar impairments using the McKenzie syndromes, pain pattern, manipulation, and stabilization clinical prediction rules.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3113271/
Objectives
Aims were (1) to determine the proportion of patients with lumbar impairments who could be classified at intake by McKenzie syndromes (McK) and pain pattern classification (PPCs) using Mechanical Diagnosis and Therapy (MDT) assessment methods, manipulation, and stabilization clinical prediction rules (CPRs) and (2) for each Man CPR or Stab CPR category, determine classification prevalence rates using McK and PPC.
CPRs are sophisticated probabilistic and prognostic models where a group of identified patient characteristics and clinical signs and symptoms are statistically associated with meaningful prediction of patient outcomes.
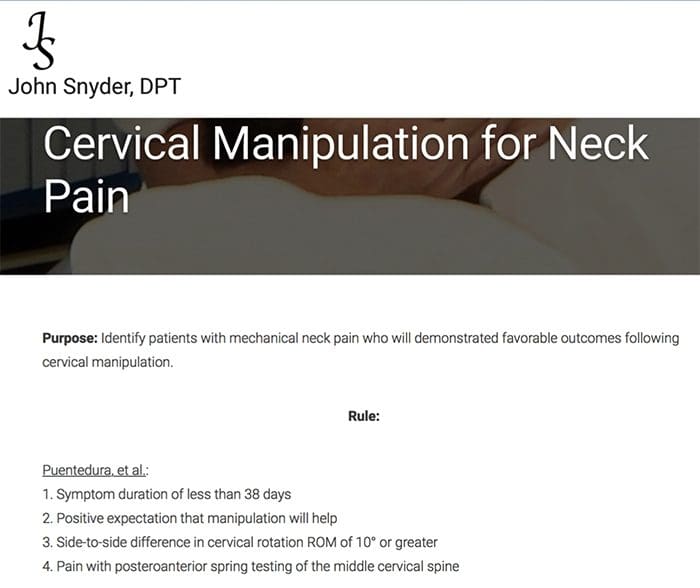
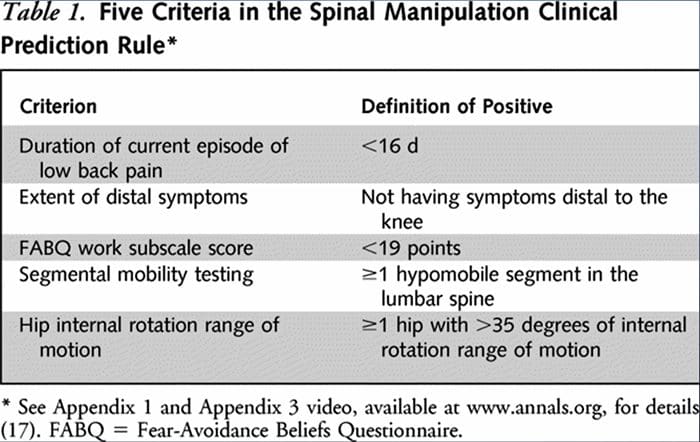
Two separate CPRs were developed by researchers for identifying patients who would respond favorably to manipulation.33,34 Flynn et al. developed the original manipulation CPR using five criteria, i.e., no symptoms below the knee, recent onset of symptoms (<16 days), low fear-avoidance belief questionnaire36 score for work (<19), hypomobility of the lumbar spine, and hip internal rotation ROM (>35 for at least one hip).33
Flynn’s CPR was subsequently modified by Fritz et al. to two criteria, that included no symptoms below the knee and recent onset of symptoms (<16 days), as a pragmatic alternative to reduce clinician burden for identifying patients in primary care most likely to respond to thrust manipulation.34 positively
“Potentia.l Pitfalls Of Clinical Prediction Rules”
What Are Clinical Prediction Rules?
A clinical prediction rule (CPR) is a combination of clinical findings that have statistically demonstrated meaningful predictability in determining a selected condition or prognosis of a patient who has been provided with a specific treatment 1,2. CPRs are created using multi-variate statistical methods, are designed to examine the predictive ability of selected groupings of clinical variables3,4, and are intended to help clinicians make quick decisions that may normally be subject to underlying biases5. The rules are algorithmic in nature and involve condensed information that identifies the smallest number of statistically diagnostic indicators to the targeted condition6.
Clinical prediction rules are generally developed using a 3-step method14. First, CPRs have derived us prospectively-
ing multivariate statistical methods to examine the predictive ability of selected groupings of clinical variables3. The second step involves validating the CPR in a randomized controlled trial to reduce the risk that the predictive factors developed during the derivation phase were selected by chance14. The third step involves conducting an impact analysis to determine how the CPR improves care, reduces costs, and accurately defines the targeted objective14.
Although there is little debate that carefully constructed CPRs can improve clinical practice, to my knowledge, there are no guidelines that specify methodological requirements for CPRs for infusion into all clinical practice environments. Guidelines are created to improve the rigor of study design and reporting. The following editorial outlines potential methodological pitfalls in CPRs that may significantly weaken the transferability of the algorithm. Within the field of rehabilitation, most CPRs have been prescriptive; thus, my comments here are reflective of prescriptive CPRs.
Methodological Pitfalls
CPRs are designed to specify a homogenous set of characteristics from a heterogeneous population of prospectively selected consecutive patients5,15. Typically, the resulting applicable population is a small subset of a larger sample and may only represent a small percentage of the clinician’s actual daily caseload. The setting and location of the larger sample should be generalizable15,16, and subsequent validity studies require assessment of the CPR in different patient groups, in different environments, and with a typical patient group seen by most clinicians16. Because many CPRs are developed based on a very distinct group that may or may not reflect a typical population of patients, the spectrum transportability17 of many current CPR algorithms may be limited.
Clinical prediction rules use outcome measures to determine the effectiveness of the intervention. Outcome measures must have a single operational definition5 and require enough responsiveness to capture appropriate change in the condition14 truly; in addition, these measures should have a well-constructed cut-off score16,18 and be collected by a blinded administrator15. The selection of an appropriate anchor score for measurement of actual change is currently debated19-20. Most outcome measures use a patient recall-based questionnaire such as a global rating of change score (GRoC), which is appropriate when used in the short term but suffers from recall bias when used in long-term analyses19-21.
A potential drawback for CPRs is the failure to maintain the quality of the tests and measures used as predictors in the algorithm. Therefore, the perspective test and measures should be independent of one another during modeling16; each should be performed in a meaningful, acceptable manner4; clinicians or data administrators should be blinded to the patient’s outcomes measures and condition22.
Sources
Potential Pitfalls Of Clinical Prediction Rules; The Journal of Manual & Manipulative Therapy Volume 16 Number Two [69]
Jeffrey J Hebert and Julie M Fritz; Clinical decision rules, spinal pain classification and prediction of treatment outcome: A discussion of recent reports in the rehabilitation literature
General Disclaimer, Licenses and Board Certifications *
Professional Scope of Practice *
The information herein on "Clinical Prediction Rules For Back And Spinal Pain Syndromes" is not intended to replace a one-on-one relationship with a qualified health care professional or licensed physician and is not medical advice. We encourage you to make healthcare decisions based on your research and partnership with a qualified healthcare professional.
Blog Information & Scope Discussions
Welcome to El Paso's Premier Wellness and Injury Care Clinic & Wellness Blog, where Dr. Alex Jimenez, DC, FNP-C, a Multi-State board-certified Family Practice Nurse Practitioner (FNP-BC) and Chiropractor (DC), presents insights on how our multidisciplinary team is dedicated to holistic healing and personalized care. Our practice aligns with evidence-based treatment protocols inspired by integrative medicine principles, similar to those on this site and on our family practice-based chiromed.com site, focusing on naturally restoring health for patients of all ages.
Our areas of multidisciplinary practice include Wellness & Nutrition, Chronic Pain, Personal Injury, Auto Accident Care, Work Injuries, Back Injury, Low Back Pain, Neck Pain, Migraine Headaches, Sports Injuries, Severe Sciatica, Scoliosis, Complex Herniated Discs, Fibromyalgia, Complex Injuries, Stress Management, Functional Medicine Treatments, and in-scope care protocols.
Our information scope is multidisciplinary, focusing on musculoskeletal and physical medicine, wellness, contributing etiological viscerosomatic disturbances within clinical presentations, associated somato-visceral reflex clinical dynamics, subluxation complexes, sensitive health issues, and functional medicine articles, topics, and discussions.
We provide and present clinical collaboration with specialists from various disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for musculoskeletal injuries or disorders.
Our videos, posts, topics, and insights address clinical matters and issues that are directly or indirectly related to our clinical scope of practice.
Our office has made a reasonable effort to provide supportive citations and has identified relevant research studies that support our posts. We provide copies of supporting research studies upon request to regulatory boards and the public.
We understand that we cover matters that require an additional explanation of how they may assist in a particular care plan or treatment protocol; therefore, to discuss the subject matter above further, please feel free to ask Dr. Alex Jimenez, DC, APRN, FNP-BC, or contact us at 915-850-0900.
We are here to help you and your family.
Blessings
Dr. Alex Jimenez, DC, MSACP, APRN, FNP-BC*, CCST, IFMCP, CFMP, ATN
email: [email protected]
Multidisciplinary Licensing & Board Certifications:
Licensed as a Doctor of Chiropractic (DC) in Texas & New Mexico*
Texas DC License #: TX5807, Verified: TX5807
New Mexico DC License #: NM-DC2182, Verified: NM-DC2182
Multi-State Advanced Practice Registered Nurse (APRN*) in Texas & Multi-States
Multi-state Compact APRN License by Endorsement (42 States)
Texas APRN License #: 1191402, Verified: 1191402 *
Florida APRN License #: 11043890, Verified: APRN11043890 *
Colorado License #: C-APN.0105610-C-NP, Verified: C-APN.0105610-C-NP
New York License #: N25929, Verified N25929
License Verification Link: Nursys License Verifier
* Prescriptive Authority Authorized
ANCC FNP-BC: Board Certified Nurse Practitioner*
Compact Status: Multi-State License: Authorized to Practice in 40 States*
Graduate with Honors: ICHS: MSN-FNP (Family Nurse Practitioner Program)
Degree Granted. Master's in Family Practice MSN Diploma (Cum Laude)
Dr. Alex Jimenez, DC, APRN, FNP-BC*, CFMP, IFMCP, ATN, CCST
My Digital Business Card
Licenses and Board Certifications:
DC: Doctor of Chiropractic
APRNP: Advanced Practice Registered Nurse
FNP-BC: Family Practice Specialization (Multi-State Board Certified)
RN: Registered Nurse (Multi-State Compact License)
CFMP: Certified Functional Medicine Provider
MSN-FNP: Master of Science in Family Practice Medicine
MSACP: Master of Science in Advanced Clinical Practice
IFMCP: Institute of Functional Medicine
CCST: Certified Chiropractic Spinal Trauma
ATN: Advanced Translational Neutrogenomics
Memberships & Associations:
TCA: Texas Chiropractic Association: Member ID: 104311
AANP: American Association of Nurse Practitioners: Member ID: 2198960
ANA: American Nurse Association: Member ID: 06458222 (District TX01)
TNA: Texas Nurse Association: Member ID: 06458222
NPI: 1205907805
| Primary Taxonomy | Selected Taxonomy | State | License Number |
|---|---|---|---|
| No | 111N00000X - Chiropractor | NM | DC2182 |
| Yes | 111N00000X - Chiropractor | TX | DC5807 |
| Yes | 363LF0000X - Nurse Practitioner - Family | TX | 1191402 |
| Yes | 363LF0000X - Nurse Practitioner - Family | FL | 11043890 |
| Yes | 363LF0000X - Nurse Practitioner - Family | CO | C-APN.0105610-C-NP |
| Yes | 363LF0000X - Nurse Practitioner - Family | NY | N25929 |
Dr. Alex Jimenez, DC, APRN, FNP-BC*, CFMP, IFMCP, ATN, CCST
My Digital Business Card






