Diets: The statistics are sobering. The typical American diet far exceeds the daily recommended intake levels in calories from sugars and solid fats, sodium, refined grains, and saturated fat. It is also lacking in the recommended amounts of fruits, vegetables, dairy, whole grains, and oils. The result is obesity and experts project that by 2030, in the United States alone, half of all adults will be obese.
That�s when people start dieting � and that is what gets them into trouble.
Diet vs. Lifestyle Change
Bottom line, diets are temporary. There are some serious consequences that can come from dieting, especially fad or crash diets. The effects of these types of diets can also seriously impact your chiropractic care, hindering your progress.
Also, because diets are temporary, once you return to your regular eating habits the weight usually comes back.
A lifestyle change is a far better choice. It involves making smart, healthy eating choices � choices that you maintain for the rest of your life. This also impacts your chiropractic care by strengthening your body and keeping it healthy so that it is in an optimal state for healing and responds well to treatment.
Types Of Diets
There are all sorts of diets out there. Some are blatantly unhealthy but others are sneaky. They come with claims of being healthy, of being created or endorsed by doctors, or include tons of vitamin supplements but very limited food intake. It is important to be able to spot these destructive fad diets so you don�t get suckered into their hype.
Some of the most common types of fad diets include high protein, low or no carb, liquid, cabbage, grapefruit, broth or juice, and food combining. Some of these can cause serious health problems including vital organ damage. Others can cause vitamin deficiencies and dehydration. None of them can (or should) be maintained over a long period of time, much less the rest of your life.
The Dangers Of Diets
Unhealthy dieting can come with some pretty scary dangers. Because they typically omit key foods or food groups your body can become imbalanced. Some of the dangers of dieting include dehydration, fatigue, weakness, vitamin and mineral deficiency, headaches, nausea, diarrhea, constipation, mental fogginess, loss of muscle mass, organ damage, and even heart attack and stroke.
One popular diet restricts carbs, often cutting them out completely. This includes all whole grains (which have vital minerals and fiber) as well as many fruits and vegetables. The result is a diet that is mostly protein and fat.
While the dieter may lose some weight on this plan, it is at a great cost. The extremely high intake of protein which exceeds the levels that the body should have can cause liver and kidney failure. The omission of vital grains, fruits, and vegetables can lead to serious vitamin deficiencies while the increased fat intake can lead to heart attack and stroke.
If a diet eliminates any of the key foods (lean meats, whole grains, fruits, and vegetables), it advocates losing more than 2 or 3 pounds a week, or it restricts caloric intake to less than 1,200 calories a day it is potentially unhealthy and should only be done 1) under a doctor�s close supervision, and 2) on a very temporary basis.
Healthy Eating Is A Lifestyle
When you make the life changing commitment to adopt a healthy eating lifestyle you open yourself up to a world of better health, more energy, and better focus. Your body will heal faster and you will feel better.
A diet of fresh fruits and vegetables, lean meats, fresh fish, and whole grains, along with lots of water should become a way of life. It is far healthier than the temporary diets that are out there and more effective too.
If you or a loved one need additional dietary guidance, give us a call. Our Doctor of Chiropractic is here to help!
Chronic fatigue syndrome (CFS) is a condition that is not as straightforward as other illnesses. The symptoms can often mimic other states, including some that are pretty serious, so they must all be ruled out before a diagnosis of CFS can be determined.
This is usually not a quick process, so the patient is left dealing with troubling and often debilitating symptoms and no real answers for months or even years. By the time a patient receives a diagnosis of CFS, they are usually physically and emotionally exhausted.
Overview Of Chronic Fatigue Syndrome
According to the Centers for Disease Control (CDC), more than one million people in the United States have CFS. It is more prevalent in the U.S. than lupus, multiple sclerosis, and many types of cancer.
It is found more often in women than men; women are four times more likely to get it. While anyone of any age can get CFS, it seems to be most common in people in their 40s and 50s. Researchers have found no evidence to suggest that CFS is contagious, but they believe there may be a genetic or familial link.
Complications that can come from CFS include depression, increased absence from work, lifestyle restrictions, and inability to carry out normal daily activities like caring for children, housekeeping, or wedding functions. It can cause significant social isolation and loneliness.
Chiropractic For Chronic Fatigue Syndrome
Many people have found that chiropractic for CFS helps reduce the pain that accompanies the condition and increases injury in some patients. The chiropractor uses spinal manipulation to treat the CFS patient, allowing many symptoms associated with the disease without invasive treatments or medication.
Many CFS patients report more energy, less pain or no pain, greater flexibility, increased mobility, and reduced inflammation of joints after just a few chiropractic adjustments. Often, the patient will be recommended to attend several sessions a week for spinal adjustments and counseling on supplements and diet. All these treatments work together to relieve the symptoms, strengthen the immune system, and help the patient feel more in control of their body and condition.
Whole Patient Treatment
One of the benefits of chiropractic treatment for CFS is that it treats the whole patient, not just the symptoms. A doctor of chiropractic may recommend various chiropractic services such as spinal adjustments. Still, they will also sit with the patient and discuss that patient’s diet, daily routine, and any medications or supplements they are taking.
The chiropractor will then make dietary recommendations, including supplements that help CFS, such as:
Omega 3 fatty acids
Eiscosapentaenoic acid (EPA)
Docosahexaenoic acid (DHA)
Magnesium
Malic Acid
Linoleic Acid
Depending on the patient, they may also recommend a liver detox program and a more structured diet and exercise program.
Hope For Patients With CFS
Chiropractic care can give much-needed hope to patients with CFS. The whole patient care they receive helps not only the physical and emotional suffering as well.
The changes in diet, recommended supplements, and chiropractic treatments help the patient’s physical symptoms but also address the emotional ones, particularly depression and frustration. It is essential that patients with CFS know that there is someone who hears them, understands their difficulties, and wants to help them on every level, not just symptom control. Chiropractic care addresses all of these for optimal whole patient care.
Clinic News – Dr. Jimenez Takes A Look At Stress Management
Constipation is an uncomfortable and common side effect of lower back and leg pain conditions. Sciatic nerve pain can occur at the same time as constipation does, but can also alternate where constipation ensues followed by sciatica.
Finding lasting relief is crucial, but understanding the exact reasons why the symptoms occur is just as important. These two conditions can be related or they may be completely coincidental. But the more they occur together, or in succession, there is greater chance that some structural or body connection is happening between the two.
The Facts: Sciatica & Constipation
Investigate why the source process may be the same for both conditions in some.
Constipation,�known as a recurrent and chronic health concern which plagues some people their entire lives. It can be caused by a variety of anatomical reasons, but many of these are fairly easy to diagnose, despite being difficult to cure using traditional medical therapy.
Sciatica is very much the same in that it can be chronic, recurrent and sometimes treatment-resistant.
What these disorders have in common is that they are often linked by nerve compression conditions within the spine. The source can be central or foraminal stenosis, which leads to compression of one or more of the lumbar nerve roots.
It is also possible for cervical central spinal stenosis to cause sciatica and may contribute to constipation, as well.
Both conditions are associated with the mind and body processes, that is physical illness caused or aggravated by mental factors, i.e. stress or some type of conflict. Constipation can be linked to conscious and subconscious emotional issues, while sciatica is just starting to receive the same recognition as a possible mind and body disorder.
Constipation/Sciatica: Solutions
Sciatica cases where constipation is also present involves the nerve roots in the lower spinal regions. These types of symptomatic expressions will be blamed on a variety of structural abnormalities in the lumbosacral region, which include degenerative discdisease, herniated discs and spinal osteoarthritis.
An alternative explanation for many cases of constipation accompanied by sciatica is regional oxygen deprivation. The solution to this condition is the treatment option invented by Dr. John Sarno. This simple treatment can usually solve even the most harmful of sciatica concerns. But the therapy remains controversial as it helps some and not others.
Sciatica/Constipation: Analysis
Once the symptoms have been diagnosed, if symptoms are structural, then treatments should resolve them or at least help in controlling the pain. If various treatments have been utilized with no relief, then it could be misdiagnosis.
Another anatomical condition that could be responsible for the symptoms or the cause could be a combination of the aforementioned mind and body issues working together. An epidemic problem that the healthcare system and one of the underlying reasons why so many with back, neck and sciatica pain never find a lasting cure. Don’t be surprised if to find out the pain was inaccurately diagnosed. This happens to millions every day.
Constipation can also be a result of serious internal diseases or organ malfunctions. Request a complete workup, which includes appropriate diagnostic testing for any significant or chronic constipation case.
Sometimes, this combination of symptoms may indicate the first signs of cauda equina syndrome.�This is a medical emergency and must be treated immediately.
Many will disregard any notion that sciatica is caused by constipation. Constipation can cause sciatica check other websites. Doctors do agree that constipation is one of a many of causes of sciatica.
But the bowels and the lower back are different parts of the body. It is important to understand that all parts of the body are connected in some way or other.
Sciatica?
If there is pain in the lower back near the buttocks and that pain travels down one or both legs, then chances are sciatica is present. Sciatica has become a common lower back pain that doctors, chiropractors, acupuncturists and physical therapists treat frequently. The pain is characterized with a combination of dull and sharp aches that create a feeling of pins and needles. With nerve conditions pins and needles are the most common type of pain.
Sciatica is the result of sciatic nerve compression. Constipation is a non-spinal condition that can cause sciatica. Just trying to use the bathroom can cause pain by irritating the sciatic nerve.
Sciatica happens when the sciatic nerve, which is the largest in the body, is compressed by an external pressure. Women in child birth and men who carry their wallets in the back pocket can experience sciatica.
Sciatica is treatable; if experiencing constipation and lower back pain at the same time, ask a doctor to test for sciatica. Doctors will order a CT scan, MRI, X-Ray or nerve conduction test.
Solving The Problem:
Experiencing sciatica related to constipation, then the first course of action is diet change. A fiber-infused diet that combines fruits and vegetables can relieve constipation. Or consider a fiber supplement.
Pain Reduction:
While waiting for constipation relief, there are various ways to reduce pain.
Take aspirin or ibuprofen, Anti-inflammatory medications reduce nerve and muscle inflammation, which alleviate nerve irritation.
Alternate hot and cold compresses, which reduce inflammation and sooth the pain. Can also be applied to the legs if the pain travels down the body.
Consider a firm mattress to support the back and alleviate any sciatica that may be the result from back strain.
A doctor may recommend several days of rest in order to allow the nerve damage time to heal.
Rules To Remember:
Do not bend or sit in a soft chair. Back support is critical.
Do not ignore the pain. Nerve pain heals within a week or gets worse.
Move slowly when standing or getting in and out of bed.
No heavy lifting & sometimes no lifting at all.
Good Nutrition & Chiropractic Treatment Contribute To Overall Well-Being
Manual therapy migraine treatment, or manipulative therapy, is a physical treatment approach which utilizes several specific hands-on techniques to treat a variety of injuries and/or conditions. Manual therapy is commonly used by chiropractors, physical therapists and massage therapists, among other qualified and experienced healthcare professionals, to diagnose and treat soft tissue and joint pain. Many healthcare specialists recommend manual therapy, or manipulative therapy as a treatment for migraine headache pain. The purpose of the following article is to educate patients on the effects of manual therapies for migraine treatment.
Manual Therapies for Migraine: a Systematic Review
Abstract
Migraine occurs in about 15% of the general population. Migraine is usually managed by medication, but some patients do not tolerate migraine medication due to side effects or prefer to avoid medication for other reasons. Non-pharmacological management is an alternative treatment option. We systematically reviewed randomized clinical trials (RCTs) on manual therapies for migraine. The RCTs suggest that massage therapy, physiotherapy, relaxation and chiropractic spinal manipulative therapy might be equally effective as propranolol and topiramate in the prophylactic management of migraine. However, the evaluated RCTs had many methodological shortcomings. Therefore, any firm conclusion will require future, well-conducted RCTs on manual therapies for migraine.
Migraine is usually managed by medication, but some patients do not tolerate acute and/or prophylactic medicine due to side effects, or contraindications due to co-morbidity of myocardial disorders or asthma among others. Some patients wish to avoid medication for other reasons. Thus, non-pharmacological management such as massage, physiotherapy and chiropractic may be an alternative treatment option. Massage therapy in Western cultures uses classic massage, trigger points, myofascial release and other passive muscle stretching among other treatment techniques which are applied to abnormal muscle tissue. Modern physiotherapy focuses on rehabilitation and exercise, while manual treatment emphasis postural corrections, soft tissue work, stretching, active and passive mobilization and manipulation techniques. Mobilization is commonly defined as movement of joints within the physiological range of motion [1]. The two most common chiropractic techniques are the diversified and Gonstead, which are used by 91 and 59% of chiropractors [2]. Chiropractic spinal manipulation (SM) is a passive-controlled maneuver which uses a directional high-velocity, low-amplitude thrusts directed at a specific joint past the physiological range of motion, without exceeding the anatomical limit [1]. The application and duration of the different manual treatments varies among those who perform it. Thus, manual treatment is not necessarily as uniform as, for instance, specific treatment with a drug in a certain dose.
This paper systematically review randomized controlled trials (RCTs) assessing the efficacy of manual therapies on migraine, i.e., massage, physiotherapy and chiropractic.
Method
The literature search was done on CINAHL, Cochrane, Medline, Ovid and PubMed. Search words were migraine and chiropractic, manipulative therapy, massage therapy, osteopathic treatment, physiotherapy or spinal mobilization. All RCTs written in English using manual therapy on migraine were evaluated. Migraine was preferentially classified according to the criteria of the International Headache Societies from 1988 or its revision from 2004, although it was not an absolute requirement [3, 4]. The studies had to evaluate at least one migraine outcome measure such as pain intensity, frequency, or duration. The methodological quality of the included RCT studies was assessed independently by the authors. The evaluation covered study population, intervention, measurement of effect, data presentation and analysis (Table 1). The maximum score is 100 points and ?50 points considered to be methodology of good quality [5�7].
Results
The literature search identified seven RCT on migraine that met our inclusion criteria, i.e., two massage therapy studies [8, 9], one physiotherapy study [10] and four chiropractic spinal manipulative therapy studies (CSMT) [11�14], while we found no RCTs studies on spinal mobilization or osteopathic as a intervention for migraine.
Methodological Quality of the RCTs
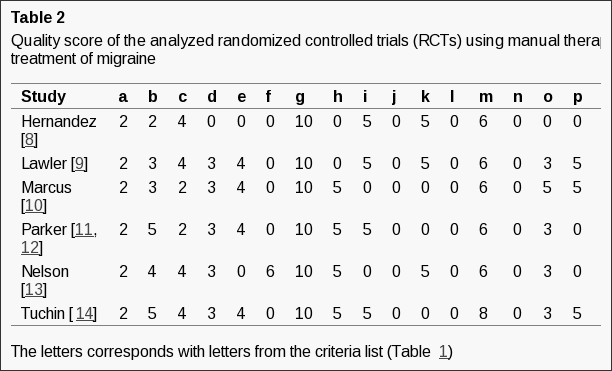
Table 2 shows the authors average methodological score of the included RCT studies [8�14]. The average score varied from 39 to 59 points. Four RCTs were considered to have a good quality methodology score (?50), and three RCTs had a low score.
Randomized Controlled Trials
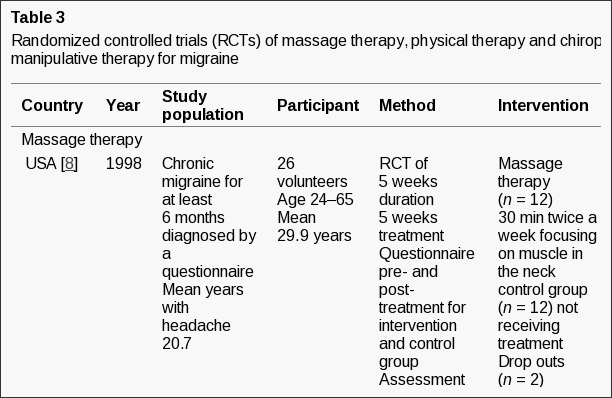
Table 3 shows details and the main results of the different RCT studies [8�14].
Massage Therapy
An American study included 26 participants with chronic migraine diagnosed by questionnaire [8]. Massage therapy had a statistically significant effect on pain intensity as compared with controls. Pain intensity was reduced 71% in the massage group and unchanged in the control group. Interpretation of the data is otherwise difficult and results on migraine frequency and duration are missing.
A New Zealand study included 48 migraineurs diagnosed by questionnaire [9]. The mean duration of a migraine attack was 47 h, and 51% of the participants had more than one attack per month. The study included a 3 week follow-up period. The migraine frequency was significantly reduced in the massage group as compared with the control group, while the intensity of attacks was unchanged. Results on migraine duration are missing. Medication use was unchanged, while sleep quality was significantly improved in the massage group (p < 0.01), but not in the control group.
Physical Therapy
An American physical therapy study included female migraineurs with frequent attacks diagnosed by a neurologist according to the criteria of the International Headache Society [3, 10]. Clinical effect was defined as >50% improvement in headache severity. Clinical effect was observed in 13% of the physical therapy group and 51% of the relaxation group (p < 0.001). The mean reduction in headache severity was 16 and 41% from baseline to post-treatment in the physical therapy and relaxation groups. The effect was maintained at 1 year follow-up in both groups. A second part of the study offered persons without clinical effect in the first part of the study, the other treatment option. Interestingly, clinical effect was observed in 55% of those whom received physical therapy in the second round who had no clinical effect from relaxation, while 47% had clinical effect from relaxation in the second round. The mean reduction in headache severity was 30 and 38% in the physical therapy and relaxation groups. Unfortunately, the study did not include a control group.
Chiropractic Spinal Manipulative Treatment
An Australian study included migraineurs with frequent attacks diagnosed by a neurologist [11]. The participants were divided into three study groups; cervical manipulation by chiropractor, cervical manipulation by physiotherapist or physician, and cervical mobilization by physiotherapist or physician. The mean migraine attack duration was skewed in the three groups, as it was much longer in cervical manipulation by chiropractor (30.5 h) than cervical manipulations by physiotherapist or physician (12.2 h) and cervical mobilization groups (14.9 h). The study had several investigators and the treatment within each group was beside the mandatory requirements free for the therapists. No statistically significant differences were found between the three groups. Improvement was observed in all three groups post-treatment (Table 3). Prior to the trial, chiropractors were confident and enthusiastic about the efficacy of cervical manipulation, while physiotherapists and physicians were doubtful about the relevance. The study did not include a control group although cervical mobilization is mentioned as the control group in the paper. A follow-up 20 months after the trial showed further improvement in the all three groups (Table 3) [12].
An American study included 218 migraineurs diagnosed according to the criteria of the International Headache Society by chiropractors [13]. The study had three treatment groups, but no control group. The headache intensity on days with headaches was unchanged in all three groups. The mean frequency was reduced equally in the three groups (Table 3). Over the counter (OTC) medication was reduced from baseline to 4 weeks post-treatment with 55% in the CSMT group, 28% in the amitriptyline group and 15% in the combined CSMT and amitriptyline group.
The second Australian study was based on questionnaire diagnoses on migraine [14]. The participants had migraine for mean 18.1 years. The effect of CSMT was significant better than the control group (Table 3). The mean reduction of migraine frequency, intensity and duration from baseline to follow-up were 42, 13, and 36% in CSMT group, and 17, 5, and 21% in the control group (data calculated by the reviewers based on figures from the paper).
Discussion
Methodological Considerations
The prevalence of migraine was similar based on a questionnaire and a direct physician conducted interview, but it was due to equal positive and negative misclassification by the questionnaire [15]. A precise headache diagnosis requires an interview by a physicians or other health professional experienced in headache diagnostics. Three of the seven RCTs ascertained participants by a questionnaire, with the diagnostic uncertainty introduced by this (Table 3).
The second American study included participants with at least four headache days per months [13]. The mean headache severity on days with headache at baseline varied from 4.4 to 5.0 on a 0�10 box scale in the three treatment groups. This implies that the participants had co-occurrence of tension-type headache, since tension-type headache intensity usually vary between 1 and 6 (mild or moderate), while migraine intensity can vary between 4 and 9 (moderate or severe), but usually it is a severe pain between 7 and 9 [16, 17]. The headache severity on days with headache was unchanged between baseline and at follow-up, indicating that the effect observed was not exclusively due to an effect on migraine, but also an effect on tension-type headache.
RCTs that include a control group are advantageous to RCTs that compare two active treatments, since the effect in the placebo group rarely is zero and often varies. An example is RCTs on acute treatment of migraine comparing the efficacy of subcutaneous sumatriptan and placebo showed placebo responses between 10 and 37%, while the therapeutic effect, i.e., the efficacy of sumatriptan minus the efficacy of placebo was similar [18, 19]. Another example is a RCT on prophylactic treatment of migraine, comparing topiramate and placebo [20]. The attack reduction increased along with increasing dose of topiramate 50, 100 and 200 mg/day. The mean migraine attack frequency was reduced from 1.4 to 2.5 attacks per month in the topiramate groups and 1.1 attacks per month in the placebo group from baseline, with mean attack frequencies varying from 5.1 to 5.8 attacks per month in the four groups.
Thus, interpretation of the efficacy in the four RCTs without a control group is not straight forward [9�12]. The methodological quality of all seven RCTs had room for improvement as the maximum score 100 was far from expectation, especially a precise migraine diagnosis is important.
Several of the studies relatively include a few participants, which might cause type 2 errors. Thus, power calculation prior to the study is important in the future studies. Furthermore, the clinical guidelines from the International Headache Society should be followed, i.e., frequency is a primary end point, while duration and intensity can be secondary end points [21, 22].
Dr. Alex Jimenez’s Insight
Manual therapies, such as massage therapy, physical therapy and chiropractic spinal manipulative treatment are several well-known migraine treatment approaches recommended by healthcare professionals to help improve as well as manage the painful symptoms associated with the condition. Patients who are unable to use drugs and/or medications, including those who may prefer to avoid using these, can benefit from manual therapies for migraine treatment, according to the following article. Evidence-based research studies have determined that manual therapies might be equally as effective for migraine treatment as drugs and/or medications. However, the systematic review determined that future, well-conducted randomized clinical trials on the use of manual therapies for migraine headache pain are required to conclude the findings.
Results
The two RCTs on massage therapy included relatively a few participants, along with shortcomings mentioned in Table 3 [8, 9]. Both studies showed that massage therapy was significantly better than the control group, by reducing migraine intensity and frequency, respectively. The 27�28% (34�7% and 30�2%) therapeutic gain in migraine frequency reduction by massage therapy is comparable with the 6, 16 and 29% therapeutic gain in migraine frequency reduction by prophylactic treatment with topiramate 50, 100 and 200 mg/day [20].
The single study on physiotherapy is large, but do not include a control group [10]. The study defined responders to have 50% or more reduction in migraine intensity. The responder rate to physical therapy was only 13% in the first part of the study, while it was 55% in the group that did not benefit from relaxation, while the responder rate to relaxation was 51% in the first part of the study and 47% in the group that did not benefit from physical therapy. A reduction in migraine intensity often correlates with reduced migraine frequency. For comparison, the responder rate was 39, 49, 47 and 23% among those who received topiramate 50, 100 and 200 mg/day and placebo as defined by 50% or more reduction in migraine frequency [20]. A meta-analysis of 53 studies on prophylactic treatment with propranolol showed a mean 44% reduction in migraine activity [23]. Thus, it seems that physical therapy and relaxation has equally good effect as topiramate and propranolol.
Only one of the four RCTs on chiropractic spinal manipulative therapy (CSMT) included a control group, while the other studies compared with other active treatment [11�14]. The first Australian study showed that the migraine frequency was reduced in all three groups when baseline was compared with 20 months post trail [11, 12]. The chiropractors were highly motivated to CSMT treatment, while physicians and physiotherapist were more sceptical, which might have influenced on the result. An American study showed that CSMT, amitriptyline and CSMT + amitriptyline reduced the migraine frequency 33, 22 and 22% from baseline to post-treatment (Table 3). The second Australian study found that migraine frequency was reduced 35% in the CSMT group, while it was reduced 17% in the control group. Thus, the therapeutic gain is equivalent to that of topiramate 100 mg/day and the efficacy is equivalent to that of propranolol [20, 23].
Three case reports raise concerns about chiropractic cervical SMT, but a recent systematic review found no robust data concerning the incidence or the prevalence of adverse reactions following chiropractic cervical SMT [24�27]. When to refer migraine patients to manual therapies? Patients not responding or tolerating prophylactic medication or who wish to avoid medication for other reasons, can be referred to massage therapy, physical therapy or chiropractic spinal manipulative therapy, as these treatments are safe with a few adverse reactions [27�29].
Conclusion
Current RCTs suggest that massage therapy, physiotherapy, relaxation and chiropractic spinal manipulative therapy might be equally efficient as propranolol and topiramate in the prophylactic management of migraine. However, a firm conclusion requires, in future, well-conducted RCTs without the many methodological shortcomings of the evaluated RCTs on manual therapies. Such studies should follow clinical trial guidelines from the International Headache Society [21, 22].
Conflict of Interest
None declared.
Open Access: This article is distributed under the terms of the Creative Commons Attribution License which permits any use, distribution and reproduction in any medium, provided the original author(s) and source are credited.
In conclusion,�chiropractors, physical therapists and massage therapists, among other qualified and experienced healthcare professionals, recommend manual therapies as a treatment for migraine headache pain. The purpose of the article was to�educate patients on the effects of manual therapies for migraine treatment. Furthermore, the systematic review determined that�future, well-conducted randomized clinical trials are required to conclude the findings. Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Neck Pain
Neck pain is a common complaint which can result due to a variety of injuries and/or conditions. According to statistics, automobile accident injuries and whiplash injuries are some of the most prevalent causes for neck pain among the general population. During an auto accident, the sudden impact from the incident can cause the head and neck to jolt abruptly back-and-forth in any direction, damaging the complex structures surrounding the cervical spine. Trauma to the tendons and ligaments, as well as that of other tissues in the neck, can cause neck pain and radiating symptoms throughout the human body.
1. Esposito S, Philipson S. Spinal adjustment technique the chiropractic art. Alexandria: Craft Printing; 2005.
2. Cooperstein R, Gleberson BJ. Technique systems in chiropractic. 1. New York: Churchill Livingstone; 2004.
3. Headache Classification Committee of the International Headache Society (1988) Classification and diagnostic criteria for headache disorders, cranial neuralgias and facial pain. Headache Classification Committee of the International Headache Society. Cephalalgia 8 (suppl 7):1�96 [PubMed]
4. Headache Classification Subcommittee of the International Society (2004) The international classification of headache disorders, 2nd edn, Cephalagia 24 (suppl 1):1�160 [PubMed]
5. Ter Riet G, Kleijnen J, Knipschild P. Acupuncture and chronic pain: a criteria-based meta-analysis. J Clin Epidemiol. 1990;43:1191�1199. doi: 10.1016/0895-4356(90)90020-P. [PubMed][Cross Ref]
6. Koes BW, Assendelft WJ, Heijden GJ, Bouter LM, Knipschild PG. Spinal manipulation and mobilisation for back and neck pain: a blinded review. BMJ. 1991;303:1298�1303. doi: 10.1136/bmj.303.6813.1298. [PMC free article][PubMed][Cross Ref]
7. Fernandez-de-las-Penas C, Alonso-Blanco C, San-Roman J, Miangolarra-Page JC. Methodological quality of randomized controlled trials of spinal manipulation and mobilization in tension-type headache, migraine, and cervicogenic headache. J Orthop Sports Phys Ther. 2006;36:160�169. [PubMed]
8. Hernandez-Rief M, Dieter J, Field T, Swerdlow B, Diego M. Migraine headache reduced by massage therapy. Int J Neurosci. 1998;96:1�11. doi: 10.3109/00207459808986453. [Cross Ref]
9. Lawler SP, Cameron LD. A randomized, controlled trial of massage therapy as a treatment for migraine. Ann Behav Med. 2006;32:50�59. doi: 10.1207/s15324796abm3201_6. [PubMed][Cross Ref]
10. Marcus DA, Scharff L, Mercer S, Turk DC. Nonpharmacological treatment for migraine: incremental utility of physical therapy with relaxation and thermal biofeedback. Cephalalgia. 1998;18:266�272. doi: 10.1046/j.1468-2982.1998.1805266.x. [PubMed][Cross Ref]
11. Parker GB, Tupling H, Pryor DS. A controlled trial of cervical manipulation of migraine. Aust NZJ Med. 1978;8:589�593. [PubMed]
12. Parker GB, Pryor DS, Tupling H. Why does migraine improve during a clinical trial? Further results from a trial of cervical manipulation for migraine. Aust NZJ Med. 1980;10:192�198. [PubMed]
13. Nelson CF, Bronfort G, Evans R, Boline P, Goldsmith C, Anderson AV. The efficacy of spinal manipulation, amitriptyline and the combination of both therapies for the prophylaxis of migraine headache. J Manipulative Physiol Ther. 1998;21:511�519. [PubMed]
14. Tuchin PJ, Pollard H, Bonello R. A randomized controlled trial of chiropractic spinal manipulative therapy for migraine. J Manipulative Physiol Ther. 2000;23:91�95. doi: 10.1016/S0161-4754(00)90073-3. [PubMed][Cross Ref]
15. Rasmussen BK, Jensen R, Olesen J. Questionnaire versus clinical interview in the diagnosis of headache. Headache. 1991;31:290�295. doi: 10.1111/j.1526-4610.1991.hed3105290.x. [PubMed][Cross Ref]
16. Lundquist YC, Benth JS, Grande RB, Aaseth K, Russell MB. A vertical VAS is a valid instrument for monitoring headache pain intensity. Cephalalgia. 2009;29:1034�1041. doi: 10.1111/j.1468-2982.2008.01833.x. [PubMed][Cross Ref]
17. Rasmussen BK, Olesen J. Migraine with aura and migraine without aura: an epidemiological study. Cephalalgia. 1992;12:221�228. doi: 10.1046/j.1468-2982.1992.1204221.x. [PubMed][Cross Ref]
18. Ensink FB. Subcutaneous sumatriptan in the acute treatment of migraine. Sumatriptan International Study Group. J Neurol. 1991;238(suppl 1):S66�S69. doi: 10.1007/BF01642910. [PubMed][Cross Ref]
19. Russell MB, Holm-Thomsen OE, Rishoj NM, Cleal A, Pilgrim AJ, Olesen J. A randomized double-blind placebo-controlled crossover study of subcutaneous sumatriptan in general practice. Cephalalgia. 1994;14:291�296. doi: 10.1046/j.1468-2982.1994.1404291.x. [PubMed][Cross Ref]
20. Brandes JL, Saper JR, Diamond M, Couch JR, Lewis DW, Schmitt J, Neto W, Schwabe S, Jacobs D, MIGR-002 Study Group Topiramate for migraine prevention: a randomized controlled trial. JAMA. 2004;291:965�973. doi: 10.1001/jama.291.8.965. [PubMed][Cross Ref]
21. Tfelt-Hansen P, Block G, Dahl�f C, Diener HC, Ferrari MD, Goadsby PJ, Guidetti V, Jones B, Lipton RB, Massiou H, Meinert C, Sandrini G, Steiner T, Winter PB, International Headache Society Clinical trials Subcommittee Guidelines for controlled trials of drugs in migraine: 2nd ed. Cephalalgia. 2000;20:765�786. doi: 10.1046/j.1468-2982.2000.00117.x. [PubMed][Cross Ref]
22. Silberstein S, Tfelt-Hansen P, Dodick DW, Limmroth V, Lipton RB, Pascual J, Wang SJ, Task Force of the International Headache Society Clinical Trials Subcommittee Guidelines for controlled trials of prophylactic treatment of chronic migraine in adults. Cephalalgia. 2008;28:484�495. doi: 10.1111/j.1468-2982.2008.01555.x. [PubMed][Cross Ref]
23. Holroyd KA, Penzien DB, Cordingley GE. Propranolol in the management of recurrent migraine: a meta-analytic review. Headache. 1991;31:333�340. doi: 10.1111/j.1526-4610.1991.hed3105333.x. [PubMed][Cross Ref]
24. Khan AM, Ahmad N, Li X, Korsten MA, Rosman A. Chiropractic sympathectomy: carotid artery dissection with oculosympathetic palsy after chiropractic manipulation of the neck. Mt Sinai J Med. 2005;72:207�210. [PubMed]
25. Morelli N, Gallerini S, Gori S, Chiti A, Cosottini M, Orlandi G, Murri L. Intracranial hypotension syndrome following chiropractic manipulation of the cervical spine. J Headache Pain. 2006;7:211�213. doi: 10.1007/s10194-006-0308-0. [PMC free article][PubMed][Cross Ref]
26. Marx P, P�schmann H, Haferkamp G, Busche T, Neu J. Manipulative treatment of the cervical spine and stroke. Fortschr Neurol Psychiatr. 2009;77:83�90. doi: 10.1055/s-0028-1109083. [PubMed][Cross Ref]
27. Gouveia LO, Gastanho P, Ferreira JJ. Safety of chiropractic intervention. A systematic review. Spine. 2009;34:E405�E413. doi: 10.1097/BRS.0b013e3181a16d63. [PubMed][Cross Ref]
28. Ernst E. The safety of massage therapy. Rheumatology. 2003;42:1101�1106. doi: 10.1093/rheumatology/keg306. [PubMed][Cross Ref]
29. Zeppos L, Patman S, Berney S, Adsett JA, Bridson JM, Paratz JD. Physiotherapy in intensive care is safe: an observational study. Aust J Physiother. 2007;53:279�283. [PubMed]
These assessment and treatment recommendations represent a synthesis of information derived from personal clinical experience and from the numerous sources which are cited, or are based on the work of researchers, clinicians and therapists who are named (Basmajian 1974, Cailliet 1962, Dvorak & Dvorak 1984, Fryette 1954, Greenman 1989, 1996, Janda 1983, Lewit 1992, 1999, Mennell 1964, Rolf 1977, Williams 1965).
Clinical Application of Neuromuscular Techniques: the Subscapularis Muscle
The subscapularis is a large triangular muscle which fills the subscapular fossa and inserts into the lesser tubercle of the humerus and the front of the capsule of the shoulder-joint.
The subscapularis rotates the head of the humerus medially (internal rotation) and adducts it; when the arm is raised, it draws the humerus forward and downward. It is a powerful defense to the front of the shoulder-joint, preventing displacement of the head of the humerus.
Damage or trauma from an injury or an aggravated condition can cause shortness in the subscapularis muscle. The following assessments and treatments can help improve structure and function.
Assessment of Shortness in the Subscapularis Muscle
Subscapularis shortness test (a) Direct palpation of subscapularis is required to define problems in it, since pain patterns in the shoulder, arm, scapula and chest may all derive from subscapularis or from other sources.
The patient is supine and the practitioner grasps the affected side hand and applies traction while the fingers of the other hand palpate over the edge of latissimus dorsi in order to make contact with the ventral surface of the scapula, where subscapularis can be palpated. There may be a marked reaction from the patient when this is touched, indicating acute sensitivity.
Subscapularis shortness test (b) (as seen on Fig. 4.39 below) The patient is supine with the arm abducted to 90�, the elbow flexed to 90�, and the forearm in external rotation, palm upwards. The whole arm is resting at the restriction barrier, with gravity as its counterweight.
If subscapularis is short the forearm will be unable to rest easily parallel with the floor but will be somewhat elevated.
Figure 4.39A, B Assessment and MET self-treatment position for subscapularis. If the upper arm cannot rest parallel to the floor, possible shortness of subscapularis is indicated.
Care is needed to prevent the anterior shoulder becoming elevated in this position (moving towards the ceiling) and so giving a false normal picture.
Assessment of Weakness in the Subscapularis Muscle
The patient is prone with humerus abducted to 90� and elbow flexed to 90�. The humerus should be in internal rotation so that the forearm is parallel with the trunk, palm towards ceiling. The practitioner stabilises the scapula with one hand and with the other applies pressure to the patient�s wrist and forearm as though taking the humerus towards external rotation, while the patient resists.
The relative strength is judged and the method discussed by Norris (1999) should used to increase strength (isotonic eccentric contraction performed slowly).
MET Treatment of the Subscapularis Muscle
The patient is supine with the arm abducted to 90�, the elbow flexed to 90�, and the forearm in external rotation, palm upwards. The whole arm is resting at the restriction barrier, with gravity as its counterweight. (Care is needed to prevent the anterior shoulder becoming elevated in this position (moving towards the ceiling) and so giving a false normal picture.)
The patient raises the forearm slightly, against minimal resistance from the practitioner, for 7�10 seconds and, following relaxation, gravity or slight assistance from the operator takes the arm into greater external rotation, through the barrier, where it is held for not less than 20 seconds.
Dr. Alex Jimenez offers an additional assessment and treatment of the hip flexors as a part of a referenced clinical application of neuromuscular techniques by Leon Chaitow and Judith Walker DeLany. The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
By Dr. Alex Jimenez
Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.
Migraine pain is among one of the most common and debilitating conditions of the human population. As a result, many migraine cases are often misdiagnosed, leading to their improper treatment. With the proper treatment, however, a patient’s overall health and wellness as well as their quality of life may improve considerably. In addition, patient education is essential to help patients take appropriate self-care measures and for them to learn how to cope with the chronic nature of their condition. Chiropractic spinal manipulative therapy and the use of medication has been previously compared to determine the effectiveness of each for migraine pain. The purpose of the following article is to demonstrate the efficacy of each migraine pain treatment.
A Case Series of Migraine Changes Following a Manipulative Therapy Trial
Abstract
Objective: To present the characteristics of four cases of migraine, who were included as participants in a prospective trial on chiropractic spinal manipulative therapy for migraine.
Method: Participants in a migraine research trial, were reviewed for the symptoms or clinical features and their response to manual therapy.
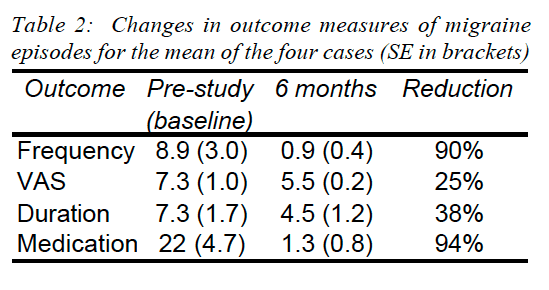
Results: The four selected cases of migraine responded dramatically to SMT, with numerous self reported symptoms being either eliminated or substantially reduced. Average frequency of episodes was reduced on average by 90%, duration of each episode by 38%, and use of medication was reduced by 94%. In addition, several associated symptoms were substantially reduced, including nausea, vomiting, photophobia and phonophobia.
Discussion: The various cases are presented to assist practitioners making a more informed prognosis.
Migraine, in its various forms, affects approximately 12 to 15% of people throughout the world, with an estimated incidence in the USA of 6% of males and 18% of females (1). Depending on the severity of a migrainous attack it is apparent that most, if not all, of the body systems can be affected (2). Consequently migraine poses a substantial threat to regular sufferers, which debilitates them to varying degrees from slight to severe (3).
One early definition of migraine highlights some potential difficulties in research assessing treatment for migraine. �A familial disorder characterised by recurrent attacks of headache widely variable in intensity, frequency and duration. Attacks are commonly unilateral and are usually associated with anorexia, nausea and vomiting. In some cases they are preceded by, or associated with neurological and mood disturbances. All of the above characteristics are not necessarily present in each attack or in each patient� (4). (Migraine and headache of the World Federation of Neurology in 1969).
Some of the more common symptoms of migraine include headache, an aura, scotoma, photophobia, phonophobia, scintillations, nausea and/or vomiting (5).
The source of pain in migraines is to found in the intra- and extracranial blood vessels (6). The blood vessel walls are pain sensitive to distension, traction or displacement. The idiopathic dilation of cranial blood vessels, together with an increase in a pain-threshold-lowering substance, result in headache for migraine headache (7).
Migraine has been shown to be reduced following chiropractic spinal manipulative therapy (8-18). In addition, other research suggests a potential role of musculoskeletal conditions in the aetiology of migraine (19-22). A misdiagnosis of migraine or cervicogenic headache could give a misleading positive result for improvement (23). Therefore, an accurate diagnosis needs to be made, based on standard accepted taxonomy.
A new classification system of headaches has been developed by the Headache Classification Committee of the International Headache Society (IHS), which contains a main category covering migraine (24). However, this taxonomy system still has several areas of potential overlap or controversy regarding the diagnosis of the headache (23).
This paper presents three cases of migraine with aura (MA) and one of migraine without aura (MW), detailing their symptoms, clinical features and response to chiropractic Spinal Manulative Therapy (SMT). The authors hope to enhance practitioners knowledge for migraine conditions that may respond favourably with SMT.
Features of Migraine
The IHS defines migraines as having at least two of the following: unilateral location, pulsating quality, moderate or severe intensity, aggravated by routine physical activity. During the headache the person must also experience either nausea &/or vomiting, and photophobia &/or phonophobia (24). In addition, there is no suggestion either by history, physical or neurological examination that the person has a headache listed in groups 5-11 of their classification system (23-25).
A previous study by the author has detailed features of the different classifications of migraine (8). The aura is the distinguishing feature between the old classifications of common (MW) and classic migraine (MA) (24). It has�been described by migraine sufferers as an opaque object, or a zigzag line around a cloud, even cases of tactile hallucinations have been recorded (6,7). The most common auras consist of homonymous visual disturbances, unilateral parathesias &/or numbness, unilateral weakness, aphasia or unclassifiable speech difficulty.
The potential mechanisms for the different migraine types are poorly understood. There have been a number of aetiologies proposed in the literature, but none seem to be able to explain all the potential symptoms experienced by migraine sufferers (26). The IHS describe changes in blood composition and platelet function as a triggering role. Processes which occur in the brain act via the trigemino-vascular system and the intra and extracranial vasculature and perivascular spaces (24).
Methodology
Based on a previous reported study (9) which involved 32 subjects who received chiropractic SMT for MA, three cases are presented which were selected due to the significant changes the patient experienced.
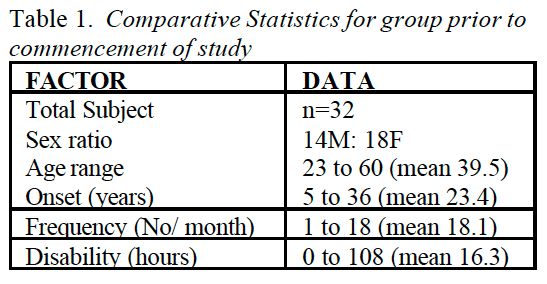
People with migraines were advertised for participation in the study, via the radio and newspapers within a local region of Sydney. All applicants completed a questionnaire, developed from Vernon (27) and has been reported in a previous study (9).
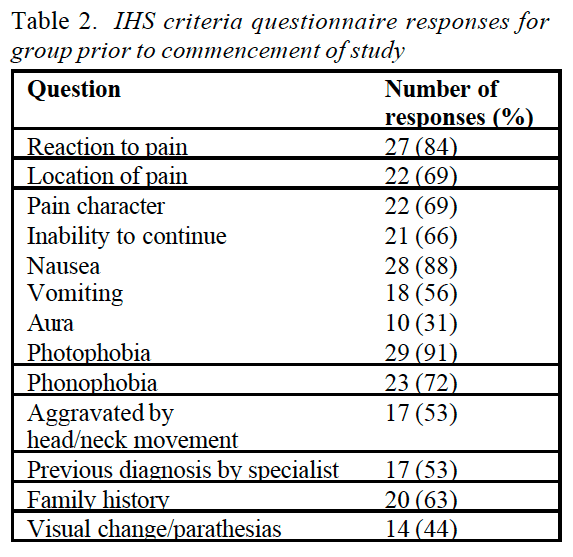
The participants to take part in the trial were selected according to responses in the questionnaire of specific symptoms. The criteria for MA diagnosis was compliance with at least 5 out of the following indicators: reaction to pain requiring cessation of activities or the need to seek a quiet dark area; pain located around the temples; pain described as throbbing; associated symptoms of nausea, vomiting, aura, photophobia or phonophobia; migraine precipitated by weather changes; migraine aggravated by head or neck movements; previous diagnosis of migraine by a specialist; and a family history of migraine.
Participants also had to experience migraine at least once a month, but not daily and the migraines could not have been initiated by trauma. Participants were excluded from the study if there were contra-indications to SMT, such as meningitis or cerebral aneurysm. In addition, participants with temporal arteritis, benign intracranial hypertension or space occupying lesions, were also excluded due to safety aspects.
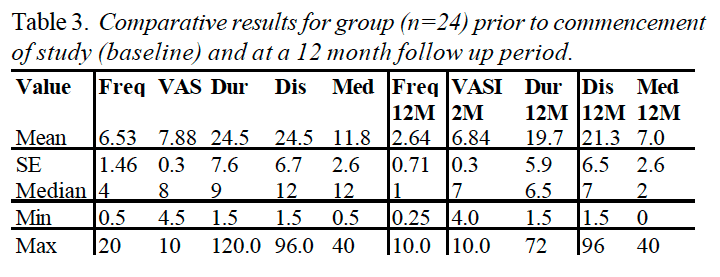
The trial was conducted over six months, and consisted of 3 stages: two months pre-treatment, two months treatment, and two months post treatment. Participants completed diaries during the entire trial noting the�frequency, intensity, duration, disability, associated symptoms and use of medication for each migraine episode. In addition, clinic records were compared to their diary entries of migraine episodes. Concurrently, the subjects were contacted by telephone by the author every two weeks and asked to describe the migraine episodes for comparison to their diaries.
A detailed history of the patients� subjective pain features was taken during the initial consultation. This included the type of pain, duration, onset, severity, radiation, aggravating and relieving factors. The history also included medical features, a systems review for potential pathologies, previous treatments and its effects. Assessment of subluxation included: orthopaedic and neurological testing, segmental springing, mobility measures such as visual estimation of range of motion, assessment of previous radiographs, specific chiropractic vertebral testing procedures, as well as response of the patient to SMT.
In addition, several vascular investigations were performed where indicated, which include: vertebral artery test, manipulative provocation test, blood pressure assessment, and abdominal aortic aneurysm screening.
During the treatment period, the subjects continued to record migraine episodes in their diary, and receive telephone calls from the authors. Treatment consisted of short amplitude, high velocity spinal manipulative thrusts, or areas of fixation determined by the physical examination. Comparison was made of initial baseline episodes of migraine prior to commencement of the study and at six months following its cessation.
Case 1
A 25 year old, 65kg Caucasian male presented with neck pain which had commenced in early childhood, that he felt may have been related to his prolonged birth. During the history the patient stated that he suffered a regular migraine headaches (3-4 per week) which he supposed was related to a motor vehicle accident, two years prior to his presentation. He reported that his �migraine� symptoms were a unilateral throbbing headache, an aura, nausea, vomiting, vertigo, and photophobia. Sleep tended to alleviate the symptoms and he required Allegren medication (25mg) on a daily basis.
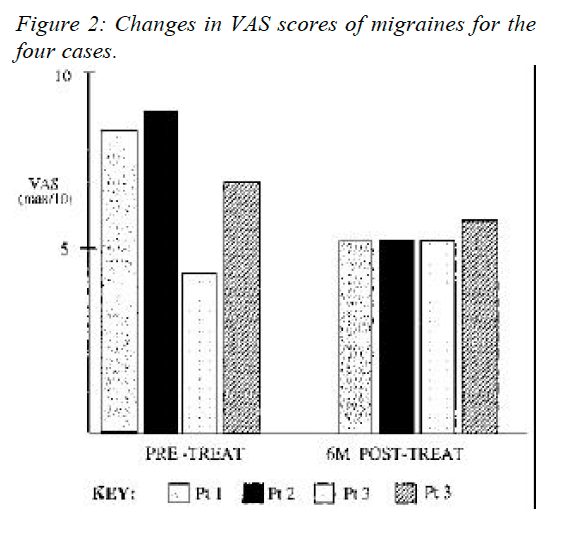
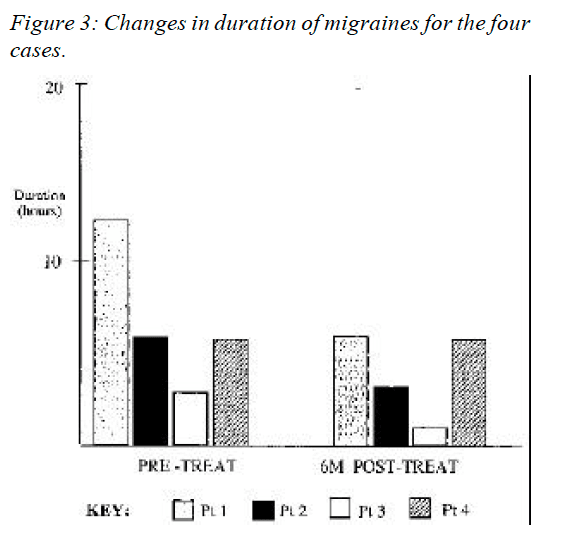
From diaries the patient was required to complete in the study, a migraine would occur 14 times a month, last an average 12.5 hours and he could perform duties after 8 hours. In addition a visual analogue scale score (VAS) for an average episode was 8.5 out of a possible maximum score of ten, corresponding to a description of �terrible� pain.
On examination, he was found to have sensitive suboccipital and upper cervical musculature, and decreased range of motion at the joint between the occiput and first cervical vertebra, the atlanto-occipital facet joint (Occ-C1), coupled with pain on flexion and extension of the cervical spine. He also had significant reduction in thoracic spine motion and an increase in thoracic kyphosis.
Treatment
The patient received chiropractic adjustments (described above) to his Occ-C1 joint, upper thoracic spine and the affected hypertonic musculature. An initial course of 16 diversified chiropractic treatments was conducted as part of a research program that the patient was participating in. The program involved recording several features for every migraine episode, including visual analogue scores, duration, medication and time before they could return to normal activities. In addition, he was shown some stretches and other exercises for his neck muscles and proved compliant.
Outcome
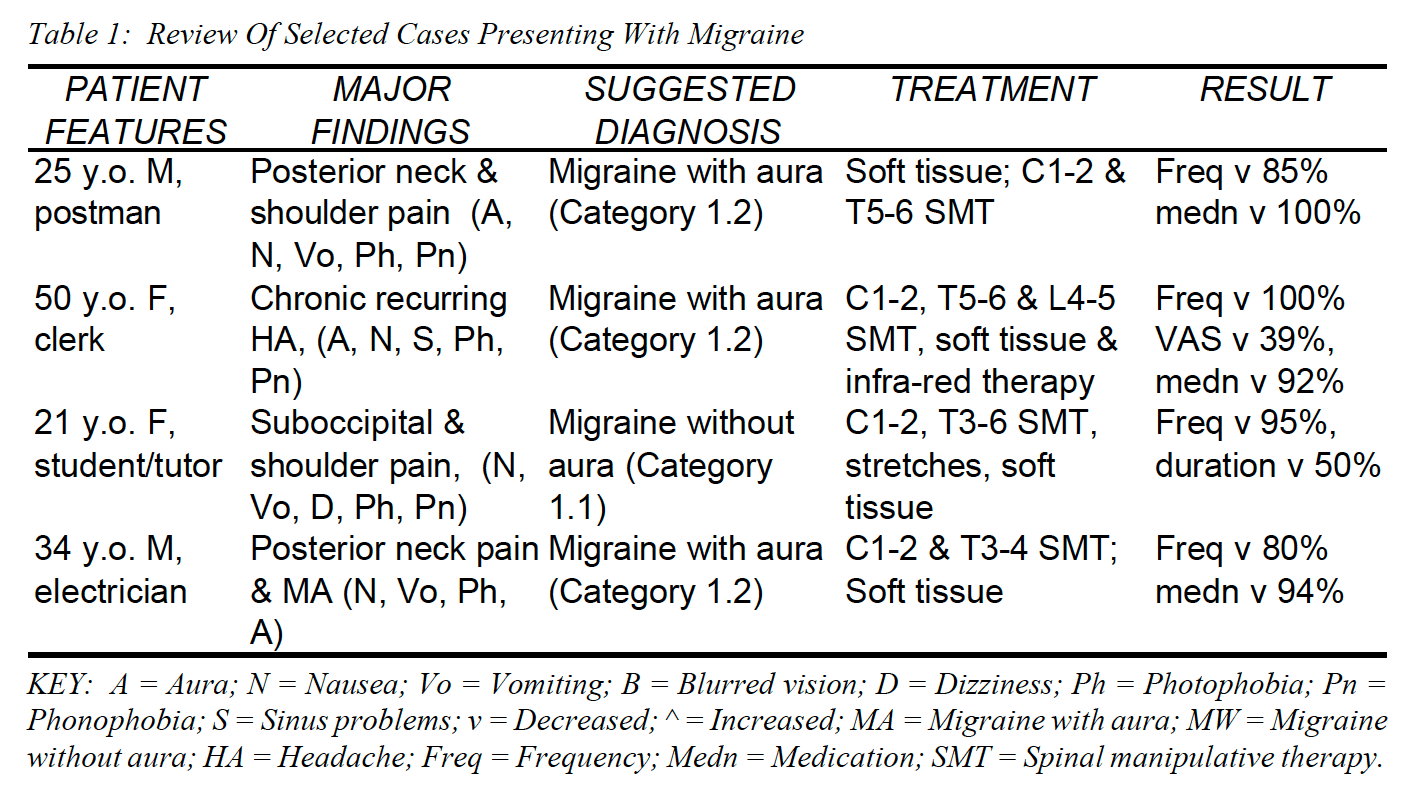
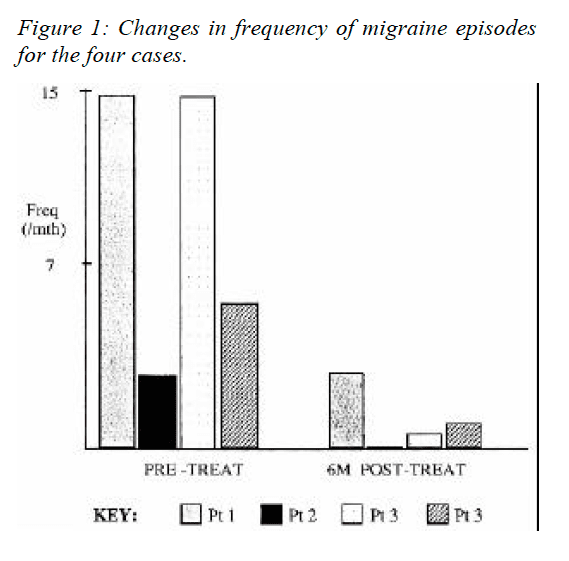
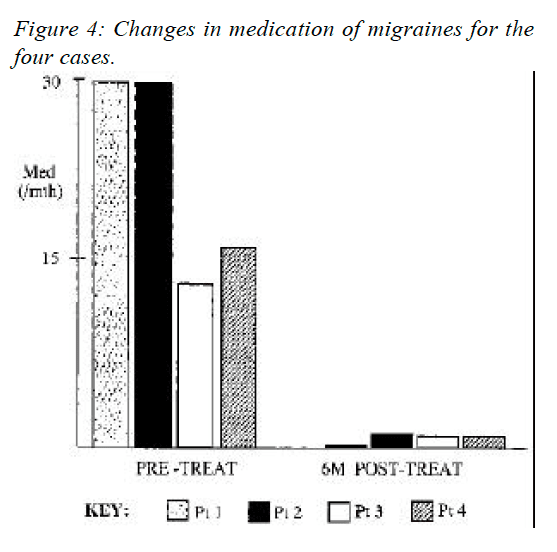
The patient reported a dramatic improvement after the course of treatment and had noticeably reduced frequency and intensity of migraines. This had continued when the patient was contacted at a period of 6 months after the study had ceased (Fig 1). At that point the patient reported having 2 migraines a month, with a VAS score of 5 out of ten, and the average duration had fallen to 7 hours (Fig�s 1-3). In addition, he now used no medication and noted that he no longer experienced nausea, vomiting, photophobia or phonophobia (Table 1).
Case 2
A 43 year old female university clerk presented complaining of chronic recurring headaches each lasting on average five days, sinus trouble due to allergy, and disturbed vision. The patient stated she experienced �migraines� which had been occurring since the age of eight. During the migraines she experienced nausea, visual disturbances, photophobia, phonophobia and scotoma. The pain usually began around her right eye but would often change to the left temple. She did not describe the pain as throbbing and the pain only stopped activities on a few occasions each year.
The patient stated she experienced the migraines once a month, except during springtime, when the migraines would occur at least once a week. She had been prescribed hormone replacement therapy (HRT) for twelve months following menopause, which had not changed the migraines. She also reported a VAS score of eight for an average episode and that an average episode lasted between six to eight hours.
In her history she reported that she had experienced many falls while horse riding between the ages of eight to ten. However, she believed that no bones were broken at the time of the falls, although this was not confirmed by radiographs at the time of injury. She had two children and was active, currently playing tennis, walking and was a keen gardener. Her past treatment included non- prescription medication for her sinus problems (Teldane),�however this did not seem to relieve the migraine. The patient stated she had previously had pethadine injections due to the severity of the migraines.
On examination she had an increased thoracic kyphosis, associated Trapezius hypertonicity and trigger points. She exhibited slight scoliosis (negative on Adams test) in the lumbar and thoracic regions. The patient also had moderate limitation in cervical spine mobility, notably in left lateral flexion and right rotation.
Treatment
Treatment consisted of diversified chiropractic spinal adjustments, especially to the C1-2, T5-6, L4-5 joints to correct the restriction of movement. Vibrator massage, and infra-red therapy were used to complement the�treatment, releasing muscles spasm of the region before the adjustments were delivered. The patient was given 14 treatments over the two months of the research trial. Following the initial treatment she experienced some moderate neck pain which resolved following the next session.
Outcome
When contacted six months following the study, the patient stated the migraines had not experienced a migraine in the last four months. The last episode she had noted a VAS score reduced to four, the average duration had reduced to three days and she had now reduced her medication to nil (Fig�s 1-4). In addition, she now experienced minor nausea, no photophobia or phonophobia, and she had substantially improved neck�mobility. She had continued to have chiropractic treatment at a frequency of once a month, following the end of the research trial.
Case 3
A 21 year old female, 171cm tall Caucasian presented with a chief complaint of severe migraines. Each episode lasted two to four hours, at a frequency of three to four episodes per week, and they had occurred for five years. The patient reported moderate posterior neck and shoulder pain, associated with the migraines. She also believed the initial migraine to be induced by stress and subsequent episodes were also aggravated by emotional stress. The patient reported no other health problems except very mild hypotension, for which she was not taking medication.
The patient�s migraines were located in the frontal, temporal and occipital regions bilaterally. No symptoms occurred premonitory to the onset of her migraines, nor did she experience visual disturbances prior to or during the migraine episodes. She described the pain as a constant dull ache, which was local and she did not complain of any parathesias.
At the initial visit, she rated each migraine between 4 and 5 on a VAS of 1-10. She also noted she experienced nausea, vomiting, dizziness, photophobia and phonophobia.
The cervical ranges of motion were restricted, predominantly in right rotation. Palpation findings were obvious at trapezius, suboccipital and supra scapulae muscles due to increased tone, colour and temperature. Motion palpation indicated restricted movement of the C1-2 facet joint on the right side. Further palpation of the supra scapular and suboccipital indicated myofibrotic tissue. Neurological tests such as Rhombergs, and vertebrobasilar (Maines) test, were negative.
Treatment
The initial treatment was muscle stripping technique aided by a masseter machine massage across the muscle fibres of the trapezius, suprascapularis and temporal regions. The patient also had a cervical adjustment of C1- 2, and adjustment to the T3-4 & T4-5 segments.
The patient was seen three days later, at which point she reported that her neck was less painful. However, she still complained of right neck pain and dizziness. Examination revealed passive motion restriction at C1-2 motion segment. Her thoracic spine was found to be restricted at segment T5-6. In addition, she had mild to moderate hypertonicity in suboccipital and cervical paraspinal muscles and supra scapular area. She was again treated�with adjustments and soft tissue technique. The C1-2 restriction to the right was adjusted with a cervical adjustment. The T5-6 restriction was also adjusted and the myofibrotic tissues were treated with the masseter.
The patient returned four days later. She reported that her migraine had improved. She no longer experienced the symptoms of a non-classical migraine. However, the pressure sensation was still present around her head, but less so than prior to the commencement of treatment. No neck pain was reported. Examination revealed a passive motion restriction of C1-2 motion segment. There was hypertonicity in the suboccipital and supra scapular muscles. The patient was treated with a cervical adjustment at C1-2 and muscle work on the above muscle groups. Neck stretching exercises were also advised.
The patient was seen a total of thirteen times over a two month period, and stated that her migraine episodes had reduced significantly at the last treatment. In addition, she was no longer experiencing neck pain. Examination revealed passive motion restriction at the C1-2 motion segment, which was reduced by adjustment.
Outcome
The patient was contacted six months after the trial for a follow-up, at which point she reported she had experienced a reduction of migraine episodes to once every two months. However, her VAS scores for an average episode was now 5.5, but the duration of an average episode was reduced by 50%. In addition, she noted a reduction in photophobia and phonophobia, but still experienced some dizziness. The patient also noted a reduction in use of medication from three Nurofen a week (12 per month) to three per month, representing a 75% reduction (Fig�s 1- 4).
Case 4
A 34 year old, 75kg Caucasian male presented with neck pain and migraines which had commenced after he had hit his head whilst surfing at a beach. This incident occurred when the patient was 19 years old but the patient said the migraines had peaked at 25 years of age. The patient stated that at 25 years of age he suffered a�migraine headaches (three to four times per week) but now in the last year prior to his presentation he experienced them twice a week. He reported that his migraines started in the suboccipital region, and radiated to his right eye. He also reported they were a unilateral throbbing headache, an aura, nausea, vomiting, vertigo, and photophobia. The patient stated taking aspirin and mersyndol medication approximately four to five times a week.
The patient reported that an average episode lasted twelve to eighteen hours and he could perform duties after eight to ten hours. In addition a visual analogue scale score (VAS) for an average episode was 7.0 out of a possible maximum score of ten, corresponding to a description of �moderate� pain. He also reported that he had osteopathic treatment approximately three years earlier, which had given some short term relief, however, physiotherapy had proven ineffective.
On examination, he was found to have significant reduction in thoracic spine motion and an increase in thoracic kyphosis, and decreased range of motion at the joint between the first and second cervical vertebra (C1- 2), the atlanto-occipital facet joint (Occ-C1), coupled with pain on flexion and extension of the cervical spine. He also had sensitive suboccipital and upper cervical musculature, especially the upper Trapezius muscle.
Treatment
The patient received chiropractic diversified adjustments to his C1-2 joint, upper thoracic spine and the affected hypertonic musculature. After a course of 14 treatments (conducted as part of a research program) the patient found he was experiencing one migraine per fortnight. The patient also reported that the nausea had decreased and that the aura was less significant.
The patient reported the improvement after the initial treatment had continued when the patient was contacted 6 months after the study had ceased. At that point the patient reported having one migraine a month, and that the VAS score had fallen to 6 out of ten. However, the average duration and return to normal activities time had remain the same as before the treatment had commenced. The patient reported that he now used only one medication per month and that he no longer experienced nausea, vomiting, and the aura (Fig�s 1-4).
Dr. Alex Jimenez’s Insight
“How does the effectiveness of chiropractic care and the use of medication vary when it comes to migraine pain?”�Chiropractic migraine pain treatment, such as chiropractic spinal manipulative treatment or spinal manipulation, is commonly utilized to help improve as well as manage migraine symptoms. Many healthcare professionals also frequently use medication, such as amitriptyline, to help relieve migraine symptoms although this treatment option may only temporarily relieve the symptoms rather than treat the condition from the source. Chiropractic care and the use of medication can be used together to help increase the relief of the treatments, as recommended by a healthcare professional. Several evidence-based studies, like the ones in the article, have demonstrated the effectiveness of chiropractic migraine pain treatment, however, more research studies are required to determine their specific result on migraine pain management. Furthermore, other research studies have shown that medication may be as effective as chiropractic spinal manipulative treatment but was associated with more side effects. Common side effects of medications like amitriptyline include: drowsiness, dizziness, dry mouth, blurred vision, constipation, trouble urinating or weight gain. Additional assessments on the effectiveness of spinal manipulation and amitriptyline is needed.
Conclusion
These four case studies highlight an apparent significant reduction in disability associated with migraines (Table 1). The conclusions are limited however, because the study does not contain a control group for comparison of placebo effect. Therefore chiropractic SMT appears to have significantly reduced migraine disability for these individuals.
Practitioners need to be critically aware of diagnostic criteria when presenting studies or case studies on effectiveness of their treatment (8). This is especially important in presentation of migraine and manipulative therapy research (12, 23).
Changes in outcome measures of migraine episodes for the mean of the four cases revealed some interesting findings (Table 2 ). As can be seen in the table, the frequency of episodes and the use of medication were substantially reduced for the four cases. However, one cannot conclude that this could be the case for other migraine sufferers due to the small number of cases presented.
Acknowledgement
The author greatly appreciates the contribution of Dr Dave Mealing in the preparation of the paper.
A Randomized Controlled Trial of Chiropractic Spinal Manipulative Therapy for Migraine.
Abstract
Objective: To assess the efficacy of chiropractic spinal manipulative therapy (SMT) in the treatment of migraine.
Design: A randomized controlled trial of 6 months’ duration. The trial consisted of 3 stages: 2 months of data collection (before treatment), 2 months of treatment, and a further 2 months of data collection (after treatment). Comparison of outcomes to the initial baseline factors was made at the end of the 6 months for both an SMT group and a control group.
Setting: Chiropractic Research Center of Macquarie University.
Participants: One hundred twenty-seven volunteers between the ages of 10 and 70 years were recruited through media advertising. The diagnosis of migraine was made on the basis of the International Headache Society standard, with a minimum of at least one migraine per month.
Interventions: Two months of chiropractic SMT (diversified technique) at vertebral fixations determined by the practitioner (maximum of 16 treatments).
Main Outcome Measures: Participants completed standard headache diaries during the entire trial noting the frequency, intensity (visual analogue score), duration, disability, associated symptoms, and use of medication for each migraine episode.
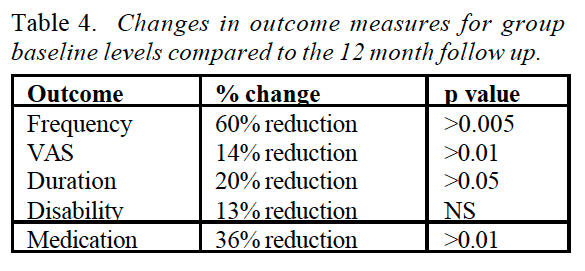
Results: The average response of the treatment group (n = 83) showed statistically significant improvement in migraine frequency (P < .005), duration (P < .01), disability (P < .05), and medication use (P< .001) when compared with the control group (n = 40). Four persons failed to complete the trial because of a variety of causes, including change in residence, a motor vehicle accident, and increased migraine frequency. Expressed in other terms, 22% of participants reported more than a 90% reduction of migraines as a consequence of the 2 months of SMT. Approximately 50% more participants reported significant improvement in the morbidity of each episode.
Conclusion: The results of this study support previous results showing that some people report significant improvement in migraines after chiropractic SMT. A high percentage (>80%) of participants reported stress as a major factor for their migraines. It appears probable that chiropractic care has an effect on the physical conditions related to stress and that in these people the effects of the migraine are reduced.
Spinal Manipulation vs. Amitriptyline for the Treatment of Chronic Tension-Type Headaches: a Randomized Clinical Trial
Abstract
Objective: To compare the effectiveness of spinal manipulation and pharmaceutical treatment (amitriptyline) for chronic tension-type headache.
Design: Randomized controlled trial using two parallel groups. The study consisted of a 2-wk baseline period, a 6-wk treatment period and a 4-wk posttreatment, follow-up period.
Setting: Chiropractic college outpatient clinic.
Patients: One hundred and fifty patients between the ages of 18 and 70 with a diagnosis of tension-type headaches of at least 3 months’ duration at a frequency of at least once per wk.
Interventions: 6 wk of spinal manipulative therapy provided by chiropractors or 6 wk of amitriptyline treatment managed by a medical physician.
Main Outcome Measures: Change in patient-reported daily headache intensity, weekly headache frequency, over-the-counter medication usage and functional health status (SF-36).
Results: A total of 448 people responded to the recruitment advertisements; 298 were excluded during the screening process. Of the 150 patients who were enrolled in the study, 24 (16%) dropped out: 5 (6.6%) from the spinal manipulative therapy and 19 (27.1%) from the amitriptyline therapy group. During the treatment period, both groups improved at very similar rates in all primary outcomes. In relation to baseline values at 4 wk after cessation of treatment, the spinal manipulation group showed a reduction of 32% in headache intensity, 42% in headache frequency, 30% in over-the-counter medication usage and an improvement of 16% in functional health status. By comparison, the amitriptyline therapy group showed no improvement or a slight worsening from baseline values in the same four major outcome measures. Controlling for baseline differences, all group differences at 4 wk after cessation of therapy were considered to be clinically important and were statistically significant. Of the patients who finished the study, 46 (82.1%) in the amitriptyline therapy group reported side effects that included drowsiness, dry mouth and weight gain. Three patients (4.3%) in the spinal manipulation group reported neck soreness and stiffness.
Conclusions: The results of this study show that spinal manipulative therapy is an effective treatment for tension headaches. Amitriptyline therapy was slightly more effective in reducing pain at the end of the treatment period but was associated with more side effects. Four weeks after the cessation of treatment, however, the patients who received spinal manipulative therapy experienced a sustained therapeutic benefit in all major outcomes in contrast to the patients that received amitriptyline therapy, who reverted to baseline values. The sustained therapeutic benefit associated with spinal manipulation seemed to result in a decreased need for over-the-counter medication. There is a need to assess the effectiveness of spinal manipulative therapy beyond four weeks and to compare spinal manipulative therapy to an appropriate placebo such as sham manipulation in future clinical trials.
In conclusion,�the following research studies demonstrated the effectiveness of chiropractic spinal manipulative therapy while one research study compared it with the use of amitriptyline for migraine. The article concludes that both chiropractic migraine pain treatment as well as medication were significantly effective in the improvement of migraine headache, however, amitriptyline is reported to present various side effects. Finally, patients may choose the best possible treatment for their migraine pain, as recommended by a healthcare professional. Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Neck Pain
Neck pain is a common complaint which can result due to a variety of injuries and/or conditions. According to statistics, automobile accident injuries and whiplash injuries are some of the most prevalent causes for neck pain among the general population. During an auto accident, the sudden impact from the incident can cause the head and neck to jolt abruptly back-and-forth in any direction, damaging the complex structures surrounding the cervical spine. Trauma to the tendons and ligaments, as well as that of other tissues in the neck, can cause neck pain and radiating symptoms throughout the human body.
1. Lipton RB, Stewart WF. Migraine in the United States: a review of epidemiology and health care use. Neurology 1993; 43(Suppl 3): S6-10.
2. Stewart WF, Lipton RB, Celentous DD, et al. Prevalence of migraine headache in the United States. JAMA 1992; 267: 64-9.
3. King J. Migraine in the Workplace. Brainwaves. Australian Brain Foundation 1995. Hawthorn, Victoria.
4. Wolff�s Headache and other head pain. Revised by Dalessio DJ. 3rd Ed 1972 Oxford University Press, New York.
5. Linet OS, Stewart WF, Celentous DD, et al. An epidemiological study of headaches among adolescents and young adults. JAMA 1989; 261: 221-6.
6. Anthony M. Migraine and its Management, Australian Family Physician 1986; 15(5): 643-9.
7. Sjasstad O, Fredricksen TA, Sand T. The localisation of the initial pain of attack: a comparison between classic migraine and cervicogenic headache. Functional Neurology 1989; 4: 73-8
8. Tuchin PJ, Bonello R. Classic migraine or not classic migraine, that is the question. Aust Chiro & Osteo 1996; 5: 66-74.
9. Tuchin PJ. The Efficacy Of Chiropractic Spinal Manipulative Therapy (SMT) In The Treatment Of Migraine – A Pilot Study. Aust Chiro & Osteo 1997; 6: 41-7.
10. Parker GB, Tupling H, Pryor DS. A Controlled Trial of Cervical Manipulation for Migraine, Aust NZ J Med 1978; 8: 585-93.
11. Hasselburg PD. Commission of Inquiry Into Chiropractic. Chiropractic in New Zealand. 1979 Government Printing Office New Zealand.
12. Parker GB, Tupling H, Pryor DS. Why Does Migraine Improve During a Clinical Trial? Further Results from a Trial of Cervical Manipulation for Migraine. Aust NZ J Med 1980; 10: 192-8.
13. Vernon H, Dhami MSI. Vertebrogenic Migraine, J Canadian Chiropractic Assoc 1985; 29(1): 20-4.
14. Wight JS. Migraine: A Statistical Analysis of Chiropractic Treatment. J Am Chiro Assoc 1978; 12: 363-7.
15. Vernon H, Steiman I, Hagino C. Cervicogenic Dysfunction in muscle contraction headache and migraine: a descriptive study. J Manipulative Physiol Ther 1992; 15: 418-29.
16. Whittingham W, Ellis WS, Molyneux TP. The effect of manipulation (Toggle recoil technique) for headaches with upper cervical joint dysfunction: a case study. J Manipulative Physiol Ther. 1994; 17(6): 369-75.
17. Lenhart LJ. Chiropractic Management of Migraine without Aura: A case study. JNMS 1995; 3: 20-6.
18. Tuchin PJ, Scwafer T, Brookes M. A Case Study of Chronic Headaches. Aust Chiro Osteo 1996; 5: 47- 53.
19. Nelson CF. The tension headache, migraine continuum: A hypothesis. J Manipulative Physiol Ther 1994; 17(3): 157-67.
20. Kidd R, Nelson C. Musculoskeletal dysfunction of the neck in migraine and tension headache. Headache 1993; 33: 566-9.
21. Milne E. The Mechanism and treatment of migraine and other disorders of cervical and postural dysfunction. Cephalgia 1989; 9(Suppl 10): 381-2.
22. Young K, Dharmi M. The Efficacy Of cervical manipulation as opposed to pharmacological therapeutics in the treatment of migraine patients. Transactions of the Consortium for Chiropractic Research. 1987.
23. Marcus DA. Migraine and tension type headaches: the questionable validity of current classification systems. Pain 1992; 8: 28-36.
24. Headache Classification Committee of the International Headache, Society. Classification and diagnostic criteria for headache disorders, cranial neuralgias and facial pain. Cephalgia 1988; 9(Suppl 7): 1-93.
25. Rasmussen BK, Jensen R, Schroll M, Olsen J. Interactions between migraine and tension type headaches in the general population. Arch Neurol 1992; 49: 914-8.
26. Vernon H. Upper Cervical Syndrome: Cervical Diagnosis and Treatment. In Vernon H. (Ed): Differential Diagnosis of Headache. 1988 Baltimore, Williams and Wilkins.
27. Vernon HT. Spinal manipulation and headache of cervical origin. J Manipulative Physiol Ther 1989; 12: 455-68.
A migraine is commonly identified by a moderate to severe throbbing pain or a pulsing sensation, usually on one side of the head, often accompanied by nausea, vomiting and extreme sensitivity to light and sound. Migraine headache pain can last for hours to even days and the symptoms can become so severe they may be disabling. Many doctors can treat varying intensities of head pain, however, the use of drugs and/or medications may only temporarily relieve the painful symptoms. Evidence-based research studies like the one described below, have determined that chiropractic spinal manipulative therapy may effectively improve migraine headaches. The purpose of the article is to educate patients on migraine headache chiropractic treatment.
A Twelve Month Clinical Trial of Chiropractic Spinal Manipulative Therapy for Migraine
Abstract
Objective: To assess the efficacy of Chiropractic spinal manipulative therapy (SMT) in the treatment of migraine.
Design: A prospective clinical trial of twelve months duration. The trial consisted of 3 stages: two month pre- treatment, two month treatment, and two months post treatment. Comparison of outcomes to the initial baseline factors was made and also 6 months after the cessation of the study.
Setting: Chiropractic Research Centre of Macquarie University
Participants: Thirty two volunteers, between the ages of 20 to 65 were recruited through media advertising. The diagnosis of migraine was based on a self reported detailed questionnaire, with minimum of one migraine per month.
Interventions: Two months of chiropractic SMT at vertebral fixations determined by the practitioner, through orthopedic and chiropractic testing.
Main Outcome Measures: Participants completed diaries during the entire trial noting the frequency, intensity (visual analogue score), duration, disability, associated symptoms and use of medication for each migraine episode.
Results: The initial 32 participants showed statistically significant (p < 0.05) improvement in migraine frequency, VAS, disability, and medication use, when compared to initial baseline levels. A further assessment of outcomes after a six month follow up (based on 24 participants), continued to show statistically significant improvement in migraine frequency (p < 0.005), VAS (p < 0.01), disability (p < 0.05), and medication use (p < 0.01), when compared to initial baseline levels. In addition, information was collected regarding any changes in neck pain following chiropractic SMT. The results indicated that 14 participants (58%) reported no increase in neck pain as a consequence of the two months of SMT. Five participants (21%) reported a slight increase, three participants (13%) reported mild pain, and two participants (8%) reported moderate pain.
Conclusion: The results of this study support the hypothesis that Chiropractic SMT is an effective treatment for migraine, in some people. However, a larger controlled study is required.
The cervical spine as a cause of headache has been well described in the literature (1,2). The Headache Classification Committee of the International Headaches Society, has defined cervicogenic headache, in addition to the other types of headaches, including migraine and tension type headache (3).
However, the role of spinal conditions (especially the cervical spine) and their associated treatment for migraine does not have a well established causal relationship or clear aetiological pathway (4-7). In addition, migraine often has uncertain or overlapping diagnostic criteria thus making the role of the cervical spine as an aetiological factor even more uncertain (8,9).
Migraines are a common and debilitating conditions yet because of this uncertain aetiology, the most appropriate long term treatment has not been established (9,10). Most aetiological models relate to vascular causes of migraine, where episodes seem to be initiated by a decreased blood flow to the cerebrum followed by extracranial vasodilatation during the headache phase (11,12). However, other aetiological models seem connected with vascular changes related to neurological causes and associated serotonergic disturbances (10). Therefore, previous treatments have focused on pharmacological modification of blood flow or serotonin antagonist block (11).
This paper will evaluate the efficacy of chiropractic spinal manipulative treatment during a prospective clinical trial of twelve months duration.
Chiropractic Treatment
Chiropractic SMT is defined as a passive manual manoeuvre during which the three joint complex is carried beyond the normal physiological range of movement without exceeding the boundaries of anatomical integrity (4). SMT requires a dynamic force in a specific direction, usually with a short amplitude to correct a problem of reduced vertebral motion or positional fault. Treatment usually consists of short amplitude, high velocity spinal manipulative thrusts (diversified technique), on areas of vertebral fixation determined by a clinical history and physical examinations.
The most commonly used factors to locate vertebral fixation (denoted vertebral subluxation complex by�chiropractors) are a clinical history relating to mechanical pain patterns and medical details to excluded possible non- mechanical causes (4). These findings would then be confirmed by a thorough physical examination, by assessing which tests/signs (orthopaedic and chiropractic) were able to reproduce the presenting symptom (7).
Studies in effectiveness and cost-effectiveness of treatment for back pain have found significant benefit for chiropractic spinal manipulative therapy (SMT). These studies have been detailed in a previous publication by this author on chiropractic in the workers compensation system (13). In addition, numerous studies have identified improvement in neck pain and headache following chiropractic SMT (4,7,14-17).
This paper will test an hypothesis that spinal conditions appear to contribute to the aetiology and morbidity of migraine.
Methodology
The study was twelve month prospective clinical trial which involved 32 subjects who received a two month course of chiropractic SMT. Treatment consisted of short amplitude, high velocity spinal manipulative thrusts (chiropractic adjustive technique), on areas of vertebral subluxation determined by the physical examination.
Participants were recruited via the radio and newspapers in the Sydney region. Applicants completed a previously reported questionnaires, and were selected according to responses in the following symptoms. The participants needed to a minimum of 5 of the following IHS indicators: reaction to pain requiring cessation of activities, the need to seek a quiet dark area, unilateral pain located parieto- temporal, pain described as pulsating/throbbing, associated symptoms of nausea &/or vomiting, photophobia &/or phonophobia, migraine aggravated by head or neck movements, and a family history of migraine (3).
Inclusion was also based on participants experiencing at least one migraine a month. Exclusion was based on non- migraine indicators of a daily migraine or the initiating factor being trauma. Participants were also excluded from the study if there were contra-indications to SMT, such as meningitis or cerebral aneurysm. In addition, participants with temporal arteritis, benign intracranial hypertension or space occupying lesions were also excluded due to safety aspects.
Participants completed diaries during the initial six month trial noting the frequency, VAS, duration, disability, associated symptoms and use of medication for each migraine episode. Participants were instructed how to complete the diary which contained a table and an�instruction sheet. Participants had to note the date of the migraine, an intensity score based on a visual analogue scale, the hours the migraine lasted and the time before they could return to normal activities. In addition, participants noted associated symptoms using a letter abbreviation and they noted the type and strength of medication for each migraine episode.
Patient’s blinding was achieved by participants being informed that they may be randomly assigned to a control group which would receive a placebo (non effective) treatment. Concurrently, the practitioners were “blinded” to previous treatment results, assignment of control procedures and other outcome measures.
The first aspect of the trial was conducted over six months, and consisted of 3 stages: two months pre-treatment, two months treatment, and two months post treatment. Participants were contacted by the author a further six months after the initial trial and asked to complete another questionnaire regarding their current migraine episodes for comparison to baseline data. The follow up questionnaire sought information on the same outcome measures, as detailed in the diaries described above.
Comparison was made to initial baseline outcome measurements of migraine preceding commencement of SMT, data at the end of the two months post SMT, and to the six month follow up data. Statistical analysis involved comparing the changes of the different outcome measurements of frequency, VAS, duration, disability, and medication use throughout the trial. Statistical tests employed were a paired t test to test for significant difference between each group and a one way analysis of variance (ANOVA) to test for changes for all groups.
Dr. Alex Jimenez’s Insight
“How can chiropractic spinal manipulative therapy help manage my migraine headache pain?”�Although researchers today don’t know the definitive cause behind these complex headaches, many healthcare professionals believe migraines are often the result of an underlying issue along the cervical spine, or neck. If you suffer from migraine headache pain, chiropractic treatment can help correct spinal misalignments, or subluxations, in the cervical spine to improve the severity of the headache and decrease their frequency. It’s not necessary to rely on drugs and/or medications to relieve the painful symptoms, however, these may be used if properly directed by a healthcare professional. Rather than focusing on the head pain alone, a doctor of chiropractic will target the source of the issue and help improve your overall health and wellness.
Results
Thirty two participants, between the ages of 23 to 60, joined the study with there being 14 males and 18 females. Table 1 gives the comparative descriptive statistics for the group. The length of time the person had migraines ranged between 5 to 36 years for the group, with the average being 18.1 years. The duration of a typical migraine episode ranged between 0.75 to 108 hours for the group, with the average being 23.3 hours. The disability (length of time before the person could return to normal activities) of a typical migraine ranged between 0 to 108 hours for the group, with the average being 25.0 hours.
The percentage response for each of the diagnostic criteria of the IHS guidelines is detailed in table 2 (Table 2). The highest responses were for photophobia (91%), nausea (88%), reaction to pain requiring the person to seek a quiet dark area (84%), phonophobia (72%), throbbing pain characteristic (69%), parieto-temporal pain location (69%), inability to continue normal activities (66%), and family history (63%).
The IHS diagnostic criteria with the lowest responses were aura (31%), migraines aggravated by head or neck movement (53%), and vomiting (56%). A moderate number (44%) of people did not indicate aura as a feature, however, they described either homonymous visual changes or parasthesias. Therefore, the number of people experiencing migraine with aura (MA) for this group was twenty four (75%) of a total group of thirty two.
The group showed statistically significant improvement (p < 0.05) in migraine frequency, VAS, duration and disability, when compared to initial baseline levels. The frequency rates reduced by 46% for the group, severity reduced by 12%, duration reduced by 20%, disability reduced by 14% only one participant (3.1 %) reported that their migraine episodes were worse after the two months of SMT, but this was not sustained at the two month post treatment follow up period. Table 3 demonstrates variate scores in each of the six diary categories for the three phases of the trial.
From the initial thirty two participants who entered the study, four participants failed to complete the entire trial, one due to alteration in work situation, one due to a fractured ankle, one due to soreness after SMT, and one ACO�following a perceived worsening of their migraine due to chiropractic SMT. In addition, four people failed to return their six month follow up data, and were excluded from the assessment. Therefore the assessment of changes in migraine at the twelve month period was based on 24 participants. Table 4 gives the comparative statistics for this group at the end of the 12 month period.
The average response at twelve months (n=24) showed statistically significant improvement in migraine frequency (p < 0.005), VAS (p < 0.01), duration (p < 0.05), and medication use (p < 0.01), when compared to initial baseline levels (Figure ????). The greatest area for improvement was with the frequency of episodes (60% reduction), and the associated severity of each migraine (14% reduction). In addition, the duration of the migraine (20% reduction) and the use of medication, reduced significantly following the SMT intervention (36% reduction). Table 3 shows mean variate scores for the three phases of the trial and statistical significance by analysis of variance (ANOVA).
Another additional result related to associated neck pain. Fourteen participants (58%) reported no increase in neck pain as a consequence of the two months of SMT. Five participants (21%) reported slight pain, three participants (13%) reported mild pain, and two participants (8%) reported moderate pain.
Discussion
The majority of participants were chronic migraine sufferers, on average they had experienced migraines for 18.1 years. However, the results have demonstrated a significant (p< 0.005) reduction in their migraine episodes and their associated disability. The mean number of migraines per month reduced from 7.6 to 2.6 episodes.
A twelve month study gives the results substantial significance because a criticism of early studies were that the length of the trial was too short to allow for the cyclical nature of migraines (18). However, the study was limited in the sample size and the fact that the trial was a pragmatic study which did not consider what aspects of chiropractic SNIT had contributed to the improvement in the migraines.
In addition, the study was limited due to the lack of a control group. However, it could be argued that participants acted as their own form of control, due to the�baseline two months data collection, especially given the fact that this group were chronic migraine sufferers.
A further limitation of this study, as with other studies of migraine or headaches was that there is substantial overlap in diagnosis and classification of migraines. The questionnaire used in this study proved to have good reliability, however, there is strong suggestion that many headache sufferers may have more than one type of headache (6-9). An advantage with the design of this study is that regardless of the exact “diagnosis” of the migraine, self reported improvement of outcome measures allow assessment of the validity of the therapy in question (4).
This study appears to confirm that there are a number of precipitating or aggravating factors involved in migraine episodes and therefore a single treatment regime may prove ineffective in the long term (4,5,9,15).
Practitioners need to be aware of the various treatment strategies and their relative advantages or limitations.
Importantly, many of the associated symptoms suffered by participants on the trial were reported to be decreased following the SMT. The associated symptoms which decreased following the trial included nausea (41% of participants felt reduction), photophobia (31 % felt reduction), vomiting (25% felt reduction), and phonophobia (25% felt reduction). Commonly reported side effects which often increase following pharmaceutical trials include nausea, vomiting, fatigue, chest pain, paraesthesia, somnolence, syncope, vertigo and less commonly atrial fibrillation. In addition, recent evidence has identified sumatriptan to be a potential cause of birth defects and myocardial infarction (19,20).
Whilst not a factor noted by the IHS, stress as either an aggravating or precipitating factor was cited by 73% of participants. In addition, 66% of people reported neck pain at the time of the migraine, with a further 31 % of people reporting upper back pain (some people noted both simultaneously).
Interestingly, five people at the end of the 12 months followup had no migraines and had decreased need for medication by 100% following chiropractic SMT. No patients reported that their migraines had increased as a result of the SMT trial.
Conclusion
The results of this study support the hypothesis that Chiropractic SMT is an effective treatment for migraine, in some people. However, due to the multifactorial nature of migraine, and the finding that episodes usually reduce following any intervention, further larger controlled study is required.
A prospective randomised controlled trial utilising detuned EPT (interferential), a sham manipulation group and an SMT group is nearing conclusion. It is anticipated this trial will provide further information of the efficacy of Chiropractic SMT in the treatment of migraine with aura.
In conclusion,�because migraine headache pain can be significantly debilitating, it’s essential for patients who suffer from this complex type of head pain to understand the effectiveness of chiropractic spinal manipulative therapy. According to the results of the research study above, migraine headache chiropractic treatment can be effectively used to as migraine treatment. Regardless of the results of the twelve month clinical trial, further research studies are still required. Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Neck Pain
Neck pain is a common complaint which can result due to a variety of injuries and/or conditions. According to statistics, automobile accident injuries and whiplash injuries are some of the most prevalent causes for neck pain among the general population. During an auto accident, the sudden impact from the incident can cause the head and neck to jolt abruptly back-and-forth in any direction, damaging the complex structures surrounding the cervical spine. Trauma to the tendons and ligaments, as well as that of other tissues in the neck, can cause neck pain and radiating symptoms throughout the human body.
1. Bogduk N. Cervical causes of headache and dizziness. In: Greive GP (ed) Modern manual therapy of the vertebral column. 2nd ed 1994. Churchill Livingstone, Edinburgh. p3l7-31.
2. Jull GA. Cervical Headache: a review. In: Greive GP (ed) Modem manual therapy of the vertebral column. 2nd ed 1994. Churchill Livingstone, Edinburgh. p 333-34,6
3. Headache Classification Committee of the International Headache, Society. Classification and diagnostic criteria for headache disorders, cranial neuralgias and facial pain. Cephalgia 1988, 9. Suppl. 7: 1-93.
4. Tuchin PJ. The efficacy of chiropractic spinal manipulative therapy (SMT) in the treatment of migraine – a pilot study. Aust Chiro & Osteo 1997; 6: 41-7.
5. Milne E. The mechanism and treatment of migraine and other disorders of cervical and postural dysfunction. Cephaigia 1989; 9, Suppi 10: 381-2.
6. Kidd R, Nelson C. Musculoskeletal dysfunction of the neck in migraine and tension headache. Headache 1993; 33: 566-9.
7. Tuchin PJ, Bonello R. Classic migraine or not classic migraine, that is the question. Aust Chiro & Osteo 1996; 5: 66-74.
8. Marcus DA. Migraine and tension type headaches: the questionable validity of current classification systems. 1992; Pain 8: 28-36.
9. Rasmussen BK, Jensen R, Schroll M, Olsen J. Interactions between migraine and tension type headaches in the general population. Arch Neurol 1992; 49: 914-8.
10. Lance JW. A concept of migraine and the search for the ideal headache drug. Headache 1990; 1: 17-23.
11. Dalassio D. The pathology of migraine. Clin J Pain 1990 6: 235-9.
12. Moskowitz MA. Basic mechanisms in vascular headache. Neurol Clin 1990; 16: 157-68
13. Tuchin PJ, Bonello R. Preliminary Findings of Analysis of Chiropractic Utilisation and Cost in the Workers Compensation System of New South Wales. J Manipulative Physiol Ther 1995; lg: 503-11.
14. Tuchin PJ, Scwafer T, Brookes M. A Case Study of Chronic Headaches. Aust Chiro & Osteo 1996; 5: 47-53.
15. Parker GB, Tupling H, Pryor DS. A Controlled Trial of Cervical Manipulation for Migraine. Aust NZ J Med 1978; 8: 585-93.
16. Young K, Dharmi M. The efficacy of cervical manipulation as opposed to pharmacological therapeutics in the treatment of migraine patients. Transactions of the Consortium for Chiropractic Research. 1987.
17. Vernon H, Steiman I, Hagino C. Cervicogenic dysfunction in muscle contraction headache and migraine: a descriptive study. J Manipulative Physiol Ther 1992; 15: 418-29
18. Parker GB, Tupling H, Pryor DS. Why does migraine improve during a clinical trial? Further results from a trial of cervical manipulation for migraine. Aust NZ J Med 1980; 10: 192-8.
19. Ottervanger JP, Stricker BH. Cardiovascular adverse reactions to sumatriptan: cause for concern? CNS Drugs 1995; 3: 90-8.
20. Simmons VE, Blakeborough P. The safety profile of sumatriptan. Rev Contemp Pharmacother 1994; 5: 319-28.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine




 Investigate why the source process may be the same for both conditions in some.
Investigate why the source process may be the same for both conditions in some. Sciatica cases where constipation is also present involves the nerve roots in the lower spinal regions. These types of symptomatic expressions will be blamed on a variety of structural abnormalities in the lumbosacral region, which include degenerative disc disease, herniated discs and spinal osteoarthritis.
Sciatica cases where constipation is also present involves the nerve roots in the lower spinal regions. These types of symptomatic expressions will be blamed on a variety of structural abnormalities in the lumbosacral region, which include degenerative disc disease, herniated discs and spinal osteoarthritis.