If you are experiencing any of these situations, then you might be experiencing problems with your stomach acid pH balance.
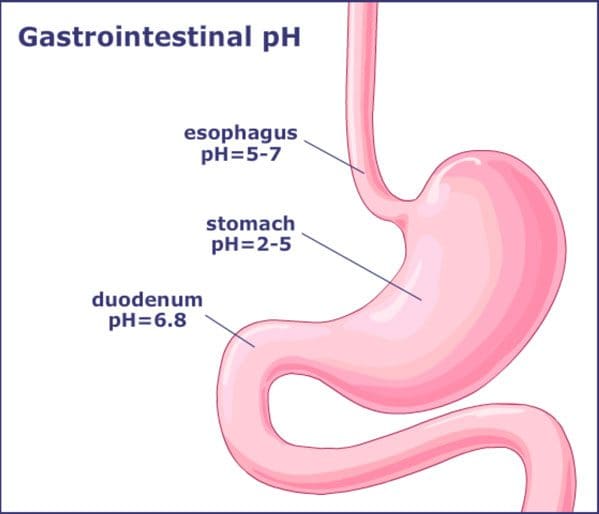
The pH Balance of the Stomach
The stomach produces gastric acids that help breakdown the food contents that a person eats. With the gastric acids, studies stated that its role is diverting the bile and pancreatic juice from the intestines. With humans, the stomach plays a significant role as a biological filter with moderate lifestyle changes. Whether it changes in a person’s diet, hygiene, and medical interventions can alter the stomach’s pH levels.
With the stomach acidity in the body, it is a double-edged sword. High acidity in the stomach can prevent pathogen exposure, but it can also decrease the likelihood of recolonization of beneficial microbes. Low acidity in the stomach is more likely to be colonized by pathogens and can cause gastric infections.
Acid Reflux
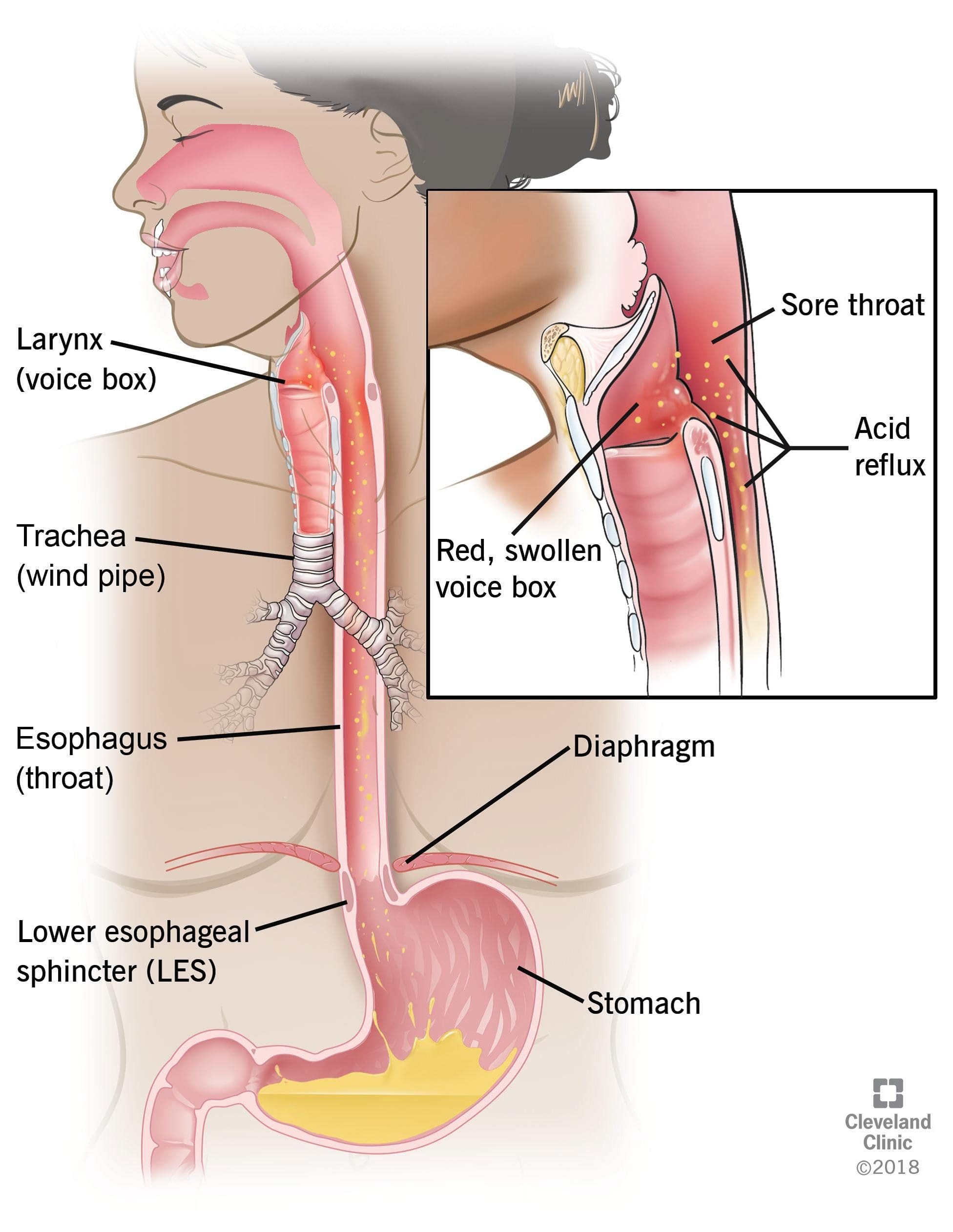
Acid reflux is a common condition that features a burning pain in the lower chest area, and it occurs when stomach acid flows back up into the food pipe. Diseases that are the result of acid reflux is one of the most common gut complaints from individuals and seen by hospital departments in the United States. The stomach contains hydrochloric acid that helps breakdown food and protects it from pathogens such as bacteria.
Even though the lining of the stomach is specially adapted to protect it from hydrochloric acid, the esophagus is not protected from this powerful acid. The gastroesophageal sphincter is a ring of muscle that generally acts as a valve that lets food into the stomach but does not let the food back up into the esophagus. When it fails, the stomach contents will regurgitate into the esophagus, and the symptoms of acid reflux will be felt.
One of the risk factors that acid reflux causes that are not preventable are hiatal hernia. This hernia causes a hole in the diaphragm that allows the upper part of the stomach to enter the chest cavity. Other risk factors include:
Obesity
Smoking (active or passive)
Low levels of physical exercise
Certain medication
Poor diet
Some of the symptoms that acid reflux creates can cause heartburn, and it is uncomfortable when the sensation travels up to the neck and throat. When an individual lays down or bends over, it tends to get the worst and can last for several hours. Some of the symptoms caused by acid reflux include:
Heartburn
Sour taste in the mouth
Regurgitation
Dyspepsia
Difficulty swallowing
Sore throat
Dry cough
Asthma symptoms
Hypochlorhydria
Hypochlorhydria is the medical term for low levels of stomach acid. Individuals with hypochlorhydria are unable to produce enough hydrochloric acid in their stomach and may experience digestive issues, nutritional deficiencies, and gastrointestinal infections.
Some of the common causes of hypochlorhydria are:
Age: Aging can make the stomach produce less acid in the body. A 2013 review stated that adults over the age of 65 are more susceptible to develop that hypochlorhydria.
Stress: Even though everyday stress does not have much effect on the production of stomach acid, chronic stress, however, can contribute to hypochlorhydria.
Medication: Individuals that use long-term antacids or other medication for acid reflux or heartburn may decrease the stomach acid that the body produces.
Bacterial Infection: A bacteria called Helicobacter pylori is a widespread, yet under-appreciated pathogen that can alter the host physiology and subvert the host immune response. It is the primary cause of peptic ulcers and gastric cancers while contributing to a low level of stomach acid.
Zinc deficiency: Zinc is a necessary mineral for stomach acid production. A lack of this mineral can contribute to hypochlorhydria to the body.
Stomach surgery: Surgical procedures like gastric bypass surgery can reduce the amount of the stomach produces.
Symptoms of hypochlorhydria are related to impaired digestion, increase infection, and reduce the absorption of nutrients from food. Symptoms may include:
Bloating
Burping
Upset stomach
Heartburn
Gas
Indigestion
Undigested food in stool
Neurological issues like numbness, tingling, and vision changes
Conclusion
The stomach is producing gastric acids that help break down food components. When environmental factors are in effect, they can alter the stomach’s pH balance and can disrupt the hydrochloric acid. Since stomach acidity is a double edge sword, it can go back and forth on the pH levels. High acidity in the stomach can cause acid reflux to the esophagus and decrease the likelihood of recolonizing beneficial microbes in the gut. Low acidity in the stomach can cause hypochlorhydria and develop digestive issues, nutrient deficiencies, and gastrointestinal infections. These products can help support the gastrointestinal system, as well as supporting the pH-optimized enzymes in both the gastric and intestinal function in the body.
October is Chiropractic Health Month. To learn more about it, check out Governor Abbott�s proclamation on our website to get full details on this historic moment.
The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or chronic disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
Reference:
Beasley, DeAnna E, et al. �The Evolution of Stomach Acidity and Its Relevance to the Human Microbiome.� PloS One, Public Library of Science, 29 July 2015, www.ncbi.nlm.nih.gov/pmc/articles/PMC4519257/.
Britton, Edward, and John T. McLaughlin. �Ageing and the Gut.� Cambridge Core, Cambridge University Press, 12 Nov. 2012, www.cambridge.org/core/journals/proceedings-of-the-nutrition-society/article/ageing-and-the-gut/A85D096755F5F7652C262495ABF302A0/core-reader.
Dix, Megan. �What Is Hypochlorhydria?� Healthline, 12 Mar. 2018, www.healthline.com/health/hypochlorhydria.
Green, G M. �Role of Gastric Juice in Feedback Regulation of Rat Pancreatic Secretion by Luminal Proteases.� Pancreas, U.S. National Library of Medicine, July 1990, www.ncbi.nlm.nih.gov/pubmed/2199966.
Kines, Kasia, and Tina Krupczak. �Nutritional Interventions for Gastroesophageal Reflux, Irritable Bowel Syndrome, and Hypochlorhydria: A Case Report.� Integrative Medicine (Encinitas, Calif.), InnoVision Professional Media, Aug. 2016, www.ncbi.nlm.nih.gov/pmc/articles/PMC4991651/.
Leonard, Jayne. �Hypochlorhydria (Low Stomach Acid): Causes, Symptoms, and Treatment.� Medical News Today, MediLexicon International, 17 July 2018, www.medicalnewstoday.com/articles/322491.php.
MacGill, Markus. �Acid Reflux: Causes, Treatment, and Symptoms.� Medical News Today, MediLexicon International, 13 Nov. 2017, www.medicalnewstoday.com/articles/146619.php.
Ramsay, Philip T, and Aaron Carr. �Gastric Acid and Digestive Physiology.� The Surgical Clinics of North America, U.S. National Library of Medicine, Oct. 2011, www.ncbi.nlm.nih.gov/pubmed/21889024.
Testerman, Traci L, and James Morris. “Beyond the Stomach: An Updated View of Helicobacter Pylori Pathogenesis, Diagnosis, and Treatment.” World Journal of Gastroenterology, Baishideng Publishing Group Inc, 28 Sept. 2014, www.ncbi.nlm.nih.gov/pmc/articles/PMC4177463/.
Wang, Yao-Kuang, et al. �Current Pharmacological Management of Gastroesophageal Reflux Disease.� Gastroenterology Research and Practice, Hindawi Publishing Corporation, 2013, www.ncbi.nlm.nih.gov/pmc/articles/PMC3710614/.
Pain, tenderness, soreness on the left side, under the rib cage
Nausea or vomiting
Stool undigested, foul-smelling, mucus-like, greasy or poorly formed
If you are experiencing any of these situations, then you might be experiencing pancreatic digestive disorders.
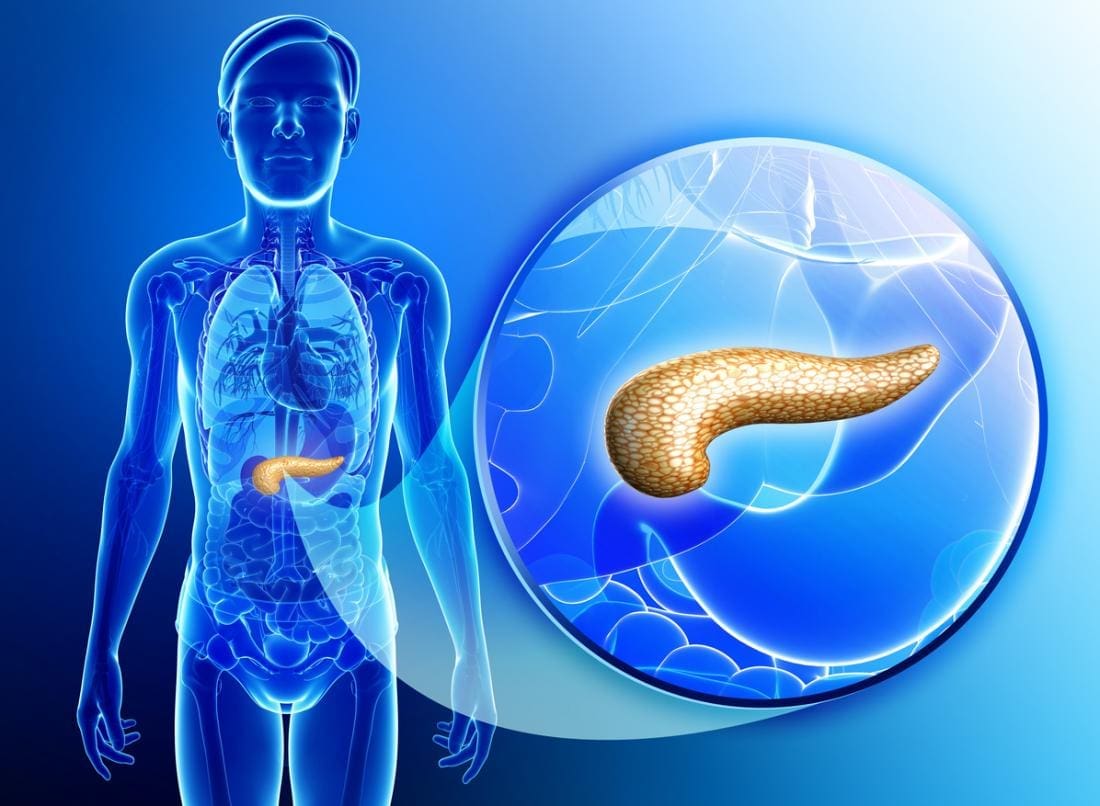
The Pancreas
The pancreas is a gland organ located in the abdomen. It is part of the digestive system, producing insulin and other vital enzymes and hormones that help break down food. It has an endocrine function, due to releasing juices directly into the bloodstream and has an exocrine function that releases juices into the ducts in the body.
One of its many jobs the pancreas does is that it secretes out enzymes into the small intestine and continues to break down that left in the stomach. Another job is that it produces insulin and secretes it into the bloodstream, where it can regulate the body’s glucose or sugar level. When there is a problem with insulin control in the body, it can lead a person to have diabetes. Other health problems include pancreatitis and pancreatic cancer.
Pancreatitis
Pancreatitis is an inflammation in the pancreas. It occurs when the digestive enzymes become activated while irritating the cells in the pancreas. With repeated damages to the pancreas, it can cause either two forms of pancreatitis, which is acute pancreatitis and chronic pancreatitis. Both are very painful and can form scar tissue in the pancreas, causing it to lose its function. A poorly functioning pancreas can cause digestion problems and diabetes. Here are the conditions that can lead to pancreatitis:
Abdominal surgery
Alcoholism
Certain medications
Cystic fibrosis
Gallstones
Obesity
Chronic Pancreatitis
Chronic pancreatitis is a long-term progressive inflammatory disease in the pancreas that can lead to a permanent breakdown of the structure and function of the pancreas in the body. Studies stated that the most common cause of chronic pancreatitis is long term alcohol abuse, it is thought to account for between 70 to 80 percent for all cases, and significantly it affects more men than women.
Common signs and symptoms of chronic pancreatitis include:
Severe upper abdominal pain that is more intense after a meal
Nausea and vomiting
When the disease progresses, the episodes of pain will become more frequent and more severe to individuals. Some individuals eventually suffer from constant abdominal pain, and as chronic pancreatitis progresses, the ability of the pancreas to produce digestive juices will deteriorate, and the following symptoms appear:
Smelly and greasy stool
Bloating
Abdominal cramps
Flatulence
Diabetes
There are numerous complications that an individual can potentially have with chronic pancreatitis. Nutrient malabsorption is one of the most complications since the pancreas is not producing enough digestive enzymes for the body to absorb the nutrients properly, leading to malnutrition. Another possible complication is the development of diabetes, where chronic pancreatitis damages the cells that produce insulin and glucagon to the body. Some individuals will also develop pseudocyst, which is fluid-filled that can form inside or outside the pancreas and can be very dangerous to the body since they can block the essential ducts and blood vessels.
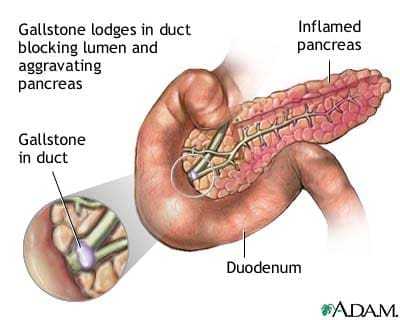
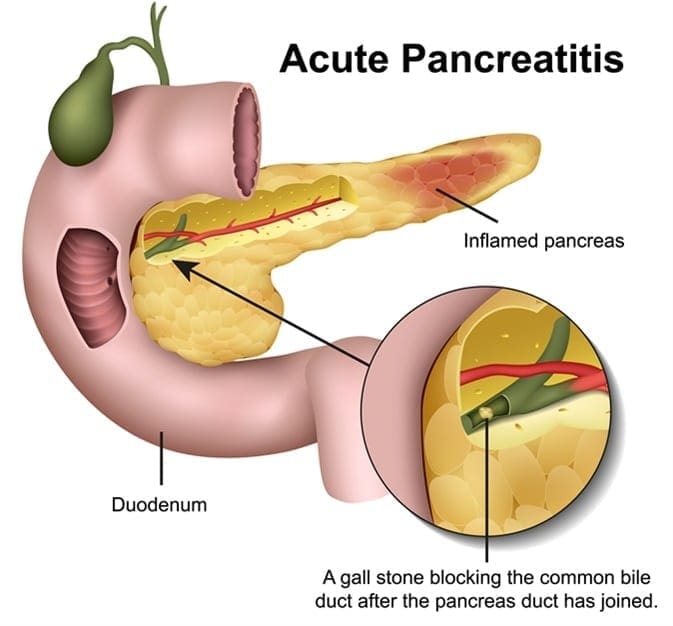
Acute Pancreatitis
Acute pancreatitis is a sudden inflammation of the pancreas. It causes the enzymes to be excessively produced, causing the pancreas gland to be swollen and inflamed. It will make digestion slow down and become painful, making the other body functions be affected as well as making the pancreas be permanently damaged and scarred.
Acute pancreatitis is painful and can develop quickly. It can trigger potentially fatal complications as the mortality rate can range from less than 5 percent to over 30 percent, depending on the severity of the condition and if it reaches to the other organs beyond the pancreas. The most common cause of acute pancreatitis is the production of gallstones in the gallbladder, alcohol misuse, and infections.
When a person has acute pancreatitis, they feel the pain in the lower abdomen and then feel it more gradually as the pain intensified until it is a constant ache. Other symptoms include:
Vomiting and nausea
Diarrhea
Loss of appetite
Pain with coughing, vigorous movements, and deep breathing
Tenderness when the abdomen is touched
Fever
Jaundice, yellowish tinge on the skin and the whites of the eyes
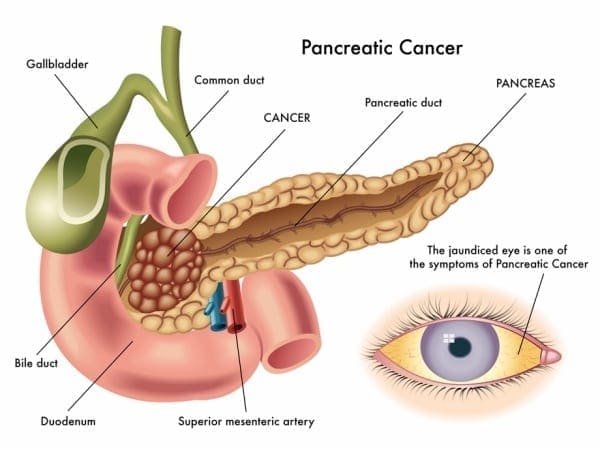
Pancreatic Cancer
Also known as �the silent disease,” pancreatic cancer happens when uncontrolled cell growth begins to form in a part of the pancreas. Tumors develop and interfere with the way the pancreas works. Pancreatic cancer often shows any symptoms until the later stages, and it can be challenging to manage. The signs and symptoms of pancreatic cancer include:
Pain in the upper abdomen that radiates to the back
Unintended weight loss or loss of appetite
Pale or grey fatty stool
Jaundice
New-onset diabetes
Blood clots
Depression
Fatigue
Conclusion
The pancreas is located in the abdomen, and its primary function is to produce insulin and necessary enzymes and hormone to aid the digestion of food. When complications are attacking the pancreas like pancreatic cancer and pancreatitis, it can damage the pancreas to stop producing insulin and can lead to chronic illnesses to spread all over the body. Some products can help support the sugar metabolism that the pancreas creates and offer nutrients and enzymatic cofactors to the gastrointestinal system in the body.
October is Chiropractic Health Month. To learn more about it, check out Governor Abbott�s proclamation on our website to get full details on this historic moment.
The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or chronic disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
Reference:
Banks, Peter A, et al. �The Management of Acute and Chronic Pancreatitis.� Gastroenterology & Hepatology, Millennium Medical Publishing, Feb. 2010, www.ncbi.nlm.nih.gov/pmc/articles/PMC2886461/.
Bartel, Michael. �Acute Pancreatitis – Gastrointestinal Disorders.� MSD Manual Professional Edition, MSD Manuals, July 2019, www.msdmanuals.com/en-gb/professional/gastrointestinal-disorders/pancreatitis/acute-pancreatitis.
Brazier, Yvette. �Acute Pancreatitis: Symptoms, Treatment, Causes, and Complications.� Medical News Today, MediLexicon International, 19 Dec. 2017, www.medicalnewstoday.com/articles/160427.php.
Brazier, Yvette. �Pancreatic Cancer: Symptoms, Causes, and Treatment.� Medical News Today, MediLexicon International, 23 Oct. 2018, www.medicalnewstoday.com/articles/323423.php.
Crosta, Peter. �Pancreas: Functions and Disorders.� Medical News Today, MediLexicon International, 26 May 2017, www.medicalnewstoday.com/articles/10011.php.
Felman, Adam. �Chronic Pancreatitis: Treatments, Symptoms, and Causes.� Medical News Today, MediLexicon International, 19 Dec. 2017, www.medicalnewstoday.com/articles/160459.php.
Health Publishing, Harvard. �Acute Pancreatitis.� Harvard Health, July 2019, www.health.harvard.edu/a_to_z/acute-pancreatitis-a-to-z.
Staff, Mayo Clinic. �Pancreatic Cancer.� Mayo Clinic, Mayo Foundation for Medical Education and Research, 9 Mar. 2018, www.mayoclinic.org/diseases-conditions/pancreatic-cancer/symptoms-causes/syc-20355421.
Staff, Mayo Clinic. �Pancreatitis.� Mayo Clinic, Mayo Foundation for Medical Education and Research, 7 Sept. 2019, www.mayoclinic.org/diseases-conditions/pancreatitis/symptoms-causes/syc-20360227.
If you are experiencing any of these situations, then you might be experiencing some stomach digestive disorders.
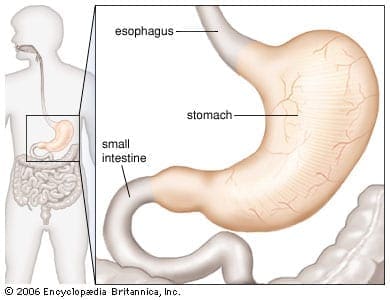
The Stomach
The human stomach�s core function is to aid food to digest when an individual eats. The four critical components of the gastric digestive function are:
A reservoir capacity
Acid secretion
Enzyme secretion
Gastrointestinal motility
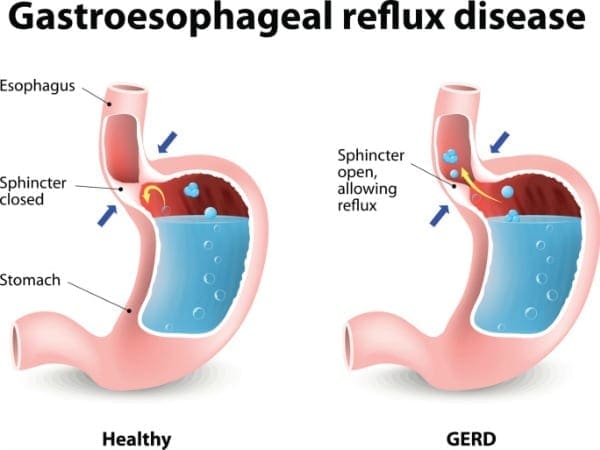
These four components help the stomach function properly in the digestive system and help the body absorb essential nutrients and are responsible for getting rid of waste out of the body. Any disorders like GERD, gallstones, and Crohn’s disease are a few of the many illnesses that can affect not only the stomach but the entire digestive system. It can cause a person to feel discomfort and can be long term if the individual has not treated it.
One of the main symptoms that GERD causes is heartburn. Heartburn is a discomfort feeling that is felt from behind the breastbone as a burning sensation. It tends to get worse on a person if they lay down, bend over, after eating food. Not all individuals with GERD experiences heartburn, there are other possible symptoms such as:
Chest pains
Difficulty swallowing
Bad breath
The sensation of a lump in the throat
Sour taste in the mouth
Respiratory problems
Tooth decay
Gallstones
Gallstones are hardened deposits of digestive fluids that can form in the gallbladder. The gallbladder is a small, pear-shaped organ that’s located on the right side of the abdomen, just beneath the liver. It also holds bile fluid that releases into the small intestines. Gallstones can range in sizes from as small as sand to as large as a golf ball. According to Harvard Health Publications, about 80% of gallstones are made of cholesterol, while the other 20% is made up of calcium salts and bilirubin.
Gallstones can lead to pain in the upper right abdomen. An individual may start to feel gallbladder pains when they eat foods that are high in fat, especially fried foods. Furthermore, if the pain continues, it may lead to an inflamed gallbladder or cholecystitis. They may also experience symptoms like:
Pain on the right-hand side of the body, just below the ribs
Back pain between the shoulder blades
Pain in the right shoulder
Nausea
Dark urine
Clay-colored stool
Stomach pain
Researchers stated that some people develop the chemical imbalance in their gallbladders causes gallstones while others do not. Gallstones are more common among people with obesity, and studies revealed that women can develop gallstones and may require surgery to remove them.
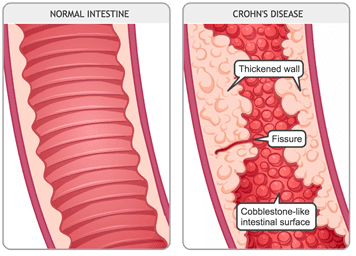
Crohn�s Disease
Crohn�s disease is an inflammatory disease. It causes inflammation in the body’s digestive tract and can cause several chronic illnesses. Inflammation caused by Crohn’s disease can be in different areas of the digestive tract in different people. The inflammation often spreads deep into the layers of the affected bowel tissue, causing pain, and sometimes lead to life-threating complications.
Crohn�s disease symptoms can vary depending on which part of the gut is affected in the body. Specific symptoms can often develop gradually and become worse over time, and it is rare for the symptoms of Crohn’s disease to develop suddenly and dramatically. The symptoms of Crohn’s disease include:
Pain
Ulcers in the gut
Mouth ulcers
Diarrhea
A fever
Fatigue
Loss of appetite
Rectal bleeding and anal fissures
Anemia
The exact causes of Crohn’s disease are still unclear, but researchers theorized that it stems from an abnormal reaction in the immune system. The theory stated that the immune system attacks food, good bacteria, and beneficial substances as if they are unwanted substances. During the attack, the body’s white cells start building up in the lining of the gut and triggers inflammation. It is still unclear whether the abnormal immune system causes Crohn’s disease, but there are environmental factors that can increase the risk of inflammation.
Conclusion
The stomach’s primary function is to digest the food that a person consumes. Four components help aid the stomach to function correctly. When the stomach is dealing with chronic illnesses like Crohn’s disease, gallstones, and GERD, it can lead to inflammation on the intestinal barriers. When it is left untreated, it can lead to life long complicated problems in the body. Some products can help aid the stomach digestion as they help support the gastrointestinal system as well.
October is Chiropractic Health Month. To learn more about it, check out Governor Abbott�s bill on our website to get full details on this historic moment.
The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or chronic disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
Brazier, Yvette. �Cholecystitis: Symptoms, Causes, Diagnosis, and Treatment.� Medical News Today, MediLexicon International, 22 Jan. 2018, www.medicalnewstoday.com/articles/172067.php.
Brazier, Yvette. �Crohn’s Disease: Symptoms, Diet, Treatment, and Causes.� Medical News Today, MediLexicon International, 11 Jan. 2019, www.medicalnewstoday.com/articles/151620.php.
Editorial Team, Healthline, and Heather Cruickshank. �Everything You Need to Know About Acid Reflux and GERD.� Healthline, 7 Dec. 2018, www.healthline.com/health/gerd.
Holland, Kimberly. �Understanding Crohn’s Disease.� Healthline, 2 May, 2019, www.healthline.com/health/crohns-disease.
MacGill, Markus. �GERD: Symptoms, Causes, and Treatment.� Medical News Today, MediLexicon International, 18 Jan. 2018, www.medicalnewstoday.com/articles/14085.php.
Macon, Brindles Lee, et al. �Understanding Gallstones: Types, Pain, and More.� Healthline, 1 June, 2017, www.healthline.com/health/gallstones.
O’Connor, Anthony, and Colm O’Mor�in. �Digestive Function of the Stomach.� Digestive Diseases (Basel, Switzerland), U.S. National Library of Medicine, 2014, www.ncbi.nlm.nih.gov/pubmed/24732181.
Publishing, Harvard Health. �What to Do about Gallstones.� Harvard Health, 2011, www.health.harvard.edu/womens-health/what-to-do-about-gallstones.
Staff, Mayo Clinic. �Crohn’s Disease.� Mayo Clinic, Mayo Foundation for Medical Education and Research, 13 Sept. 2019, www.mayoclinic.org/diseases-conditions/crohns-disease/symptoms-causes/syc-20353304.
Staff, Mayo Clinic. �Gallstones.� Mayo Clinic, Mayo Foundation for Medical Education and Research, 8 Aug. 2019, www.mayoclinic.org/diseases-conditions/gallstones/symptoms-causes/syc-20354214.
Unknown, Unknown. �Definition & Facts for GER & GERD.� National Institute of Diabetes and Digestive and Kidney Diseases, U.S. Department of Health and Human Services, 1 Nov. 2014, www.niddk.nih.gov/health-information/digestive-diseases/acid-reflux-ger-gerd-adults/definition-facts.
Lower abdominal pain relieved by passing stool or gas
Alternating constipation and diarrhea
A hard, dry, or small stool
Use laxatives frequently
If you are experiencing any of these situations, then you must be experiencing gastrointestinal impairments in your body.
Gastrointestinal Impairments
The digestive system is consisting of the gastrointestinal tract, which is home to the intestines, the liver, the colon, the gallbladder, the pancreas, and the stomach. When there is a disruption in the gastrointestinal tract, it can cause inflammation and chronic illnesses that can harm the body. Functional disorders in the digestive tract (GI tract) can look normal in the body, but it doesn’t work correctly.
Many factors can upset the GI tract and its motility, including:
Eating a diet low in fiber
Not getting enough exercise
Traveling or changes in a routine
Eating large amounts of dairy blankets
Stress
Resisting the urge to have a bowel movement
Overusing laxatives
Taking certain medicines
Some of the most common problems that can affect the GI tract are constipation, IBS, and colon cancer.
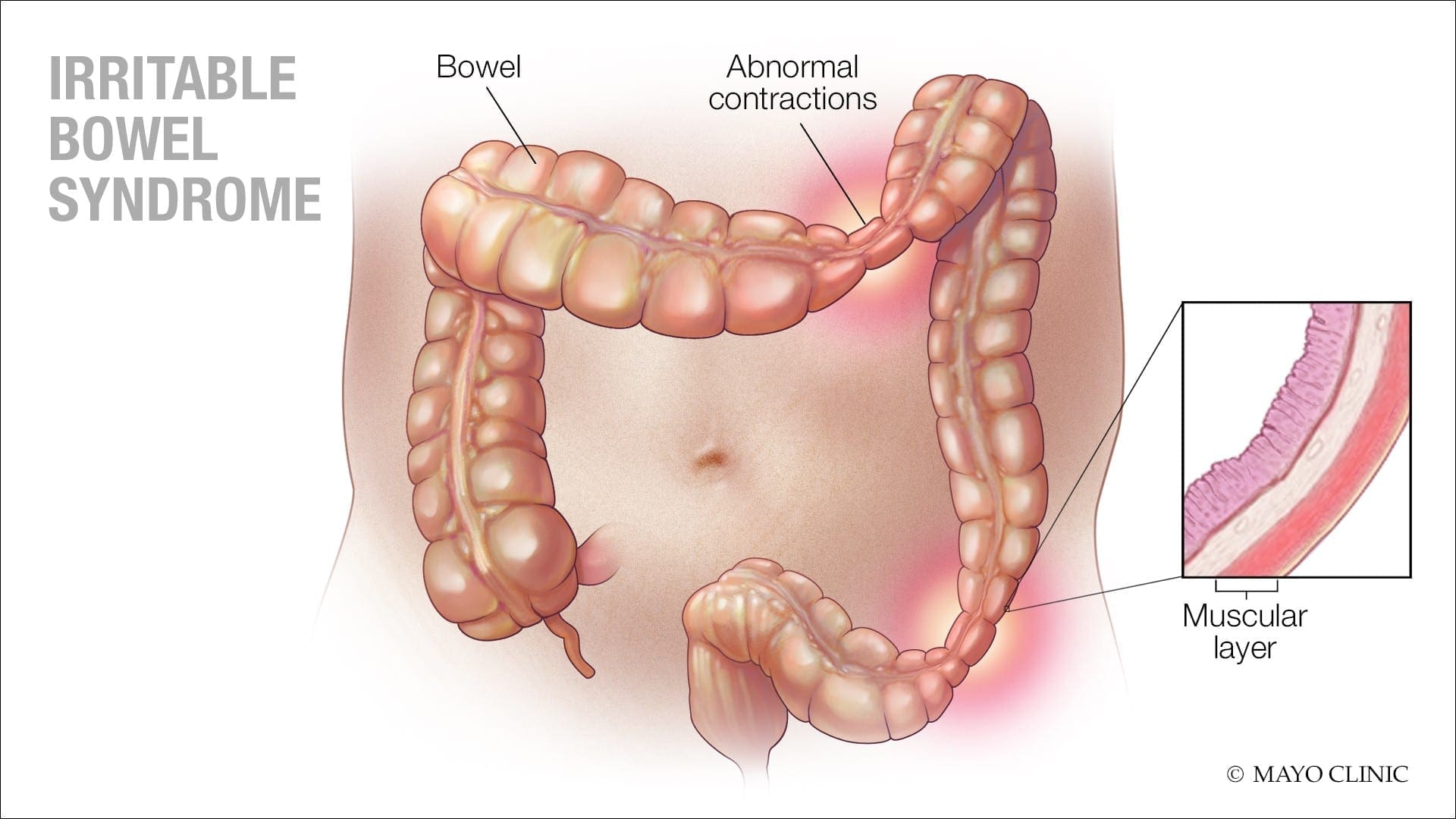
Irritable Bowel Syndrome
IBS (irritable bowel syndrome) is a long term gastrointestinal disorder. It can cause abdominal pain, bloating, mucus in the stool, irregular bowel habits, and can alternate diarrhea and constipation. IBS can cause persistent discomfort to individuals, but they can improve the symptoms over time as they learn to manage the condition.
Some of the symptoms caused by IBS are:
Changes in bowel habits
Abdominal pain and cramping that lessens after using the bathroom
A feeling that the bowels not fully emptied after using the bathroom
Excess gas
The passing of mucus from the rectum
The sudden urgent need to use the bathroom
Swelling or bloating from the abdomen.
Signs and symptoms of IBS can vary between individuals and can often resemble other diseases and conditions. IBS symptoms can often get worst after earing, and a flare-up may last about 2 to 4 days, then the symptoms may either improve or go away entirely, but IBS symptoms can affect different body parts.
These can include:
Frequent urination
Bad breath
Headaches
Joint or muscle pain
Persistent fatigue
Anxiety
Depression
Constipation
Constipation is one of the most common digestive problems that affects around 2.5 million individuals. It is a syndrome that is defined by bowel symptoms (painful or infrequent passage of stool, the hardness of stool, or a feeling of incomplete evacuation) that may occur either in isolation or secondary to another underlying disease like for example, Parkinson’s disease.
The cause of constipation is through the colon. The colon’s main job is to absorb water from leftover food as it passes through the digestive system and creates waste. When the waste is ready to be excreted out, the colon’s muscles propel the waste out through the rectum to eliminate from the body. If the debris remains in the colon for too long, though, it can be tough and challenging to excrete it out of the body.
Some factors can cause constipation; this can include:
Stress
Low-fiber diet
Lack of exercise
Certain medications
Particular diseases like a stroke, Parkinson’s disease, and diabetes
Problems with the colon or rectum
Hormonal issues
Everyone’s definition of a regular bowel movement may be different. Some people can go about three times a day, while others can go to relieve themselves about three times a week. Some of the symptoms of constipation included are:
Fewer than three bowel movements a week
Passing hard, dry stools
Straining or pain during bowel movements
Still feeling full after a bowel movement
Experiencing a rectal blockage
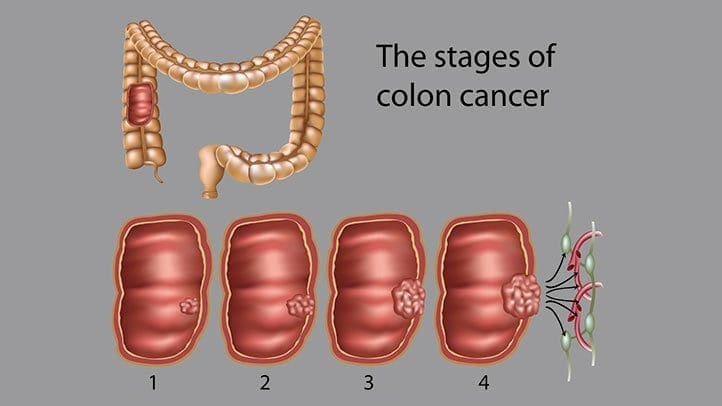
Colon Cancer
Colon cancer is the third most common type of cancer. When tumorous growths develop in the large intestine or the colon, it develops colon cancer in the GI tract. The colon, the one organ where the body draws out water and salt from solid wastes. The waste then moves through the rectum and excretes out of the body through the anus.
Even though colon cancer doesn’t cause any symptoms in the earliest stages, but it can become more noticeable as the disease progresses. Some of the sign and symptoms of colon cancer include:
Diarrhea or constipation
Changes in stool consistency
Loose, narrow stools
Blood in the stool
Abdominal pain
Weakness and fatigue
Iron deficiency
If colon cancer spreads to a new location the gastrointestinal system, it can cause additional problems in the new area.
Conclusion
Having gastrointestinal impairments can cause the body to develop chronic illnesses. There are ways to make sure that the digestive tract is functioning correctly. An individual can change their diets and lifestyle and can make sure that their gut is working properly. When there is a disruption in the GI tract like IBS, constipation, and colon cancer, it can lead to many health problems if the individual is not careful. If an individual prolongs the symptoms, then they will develop life-long issues for their body. Some products help support the intestinal tract and help strengthens the natural defenses and support the intestinal immune function.
October is Chiropractic Health Month. To learn more about it, check out Governor Abbott�s declaration on our website to get full details on this historic moment.
The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or chronic disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
References:
Bharucha, Adil E, et al. �American Gastroenterological Association Technical Review on Constipation.� Gastroenterology, U.S. National Library of Medicine, Jan. 2013, www.ncbi.nlm.nih.gov/pmc/articles/PMC3531555/.
Brazier, Yvette. �Irritable Bowel Syndrome (IBS): Symptoms, Diet, Causes, and Treatment.� Medical News Today, MediLexicon International, 18 Dec. 2017, www.medicalnewstoday.com/articles/37063.php.
Crosta, Peter. �Colon Cancer: Symptoms, Treatment, and Causes.� Medical News Today, MediLexicon International, 28 Aug. 2019, www.medicalnewstoday.com/articles/150496.php.
Sethi, Saurabh. �What You Should Know About Constipation.� Healthline, 23 Aug. 2019, www.healthline.com/health/constipation.
Whitfield, K Lynette, and Robert J Shulman. �Treatment Options for Functional Gastrointestinal Disorders: from Empiric to Complementary Approaches.� Pediatric Annals, U.S. National Library of Medicine, May 2009, www.ncbi.nlm.nih.gov/pmc/articles/PMC2830707/.
The percentage of individuals that are affected by fatigue, headaches, and overall pain is continuously growing. For the most part, these symptoms can all be linked back to a hormone imbalance. Hormone imbalances are more common than individuals realize and can affect people of all ages. Originally, hormone testing was completed through a blood draw (serum testing). However, as science is improving, there are now better, more functional ways of testing.��
As more and more studies are done, it is becoming more clear that salivary testing is superior to serum (blood) testing for hormones. There are two forms in which hormones exist in the human body, free (5%) and protein-bound (95%). Due to the protein-bound hormones being bound, they become too large to pass through into the salivary glands. This meaning that they are not bio-available and can not be delivered to the receptors in the tissues of the body.� The unbound hormones, or free hormones, are the relevant hormones that are found in the saliva. Considering the fact that free hormones are not as abundant, the hormone levels found in saliva are significantly less than those found in serum. However, many patients who are treated with serum hormone results are often overdosed because of the lack of correlation between bio-availability.
Labrix by Doctor’s Data
Similar to the D.U.T.C.H�hormone testing previously discussed, this company Labrix offers a variety of hormone testing as well.
Neurotransmitters:
NeuroBasic: ideal for monitoring therapeutic interventions of neurotransmitter imbalances previously tested or when symptoms are indicating an imbalance. This test measures Serotonin, Dopamine, Epinephrine, Norepinephrine, Glutamate, Glycine, Histamine, and Phenethylamine
Comprehensive Neurotransmitter: best when a comprehensive look at neurotransmitter secretion and metabolism of markers is needed. This test measures Serotonin, GABA, Dopamine, Norepinephrine, Epinephrine, Glutamate, Glycine, Histamine, and Phenethylamineand DOPAC, 3-MT, Normetanephrine, Metanephrine, 5-HIAA, Tryptamine, Tyrosine, Tyramine, and Taurine.
NeuroHormones:�
NeuroHormone Complete Plus:� provides insight on how the HPA axis function may be contributing to patients’ symptoms, such as mood swings, fatigue, and pain. In addition, this test is ideal for those who are at risk for breast cancer, PCOS, or a strong family history of autoimmune disease.�This test is recommended for women only.� This test measures�Estrone, Estradiol, Estriol, Progesterone, Testosterone, DHEA, Cortisol x 4, Serotonin, GABA, Dopamine, Epinephrine, Norepinephrine, Glutamate, Glycine, Histamine, Phenethylamine
NeuroHormone Complete: useful for patients (men or women) who are experiencing any type of mood disorder, addiction, fatigue, chronic illness, confusion, weight issues, low libido, PMS, or chronic pain. This test measures Estradiol, Progesterone, Testosterone, DHEA, Cortisol x 4, Serotonin, GABA, Dopamine, Epinephrine, Norepinephrine, Glutamate, Glycine, Histamine, Phenethylamine.�
NeuroAdrenal: Included in this test is a full diurnal cortisol pattern, DHEA, and 6 primary neurotransmitters to help those with symptoms such as depression, anxiety, addiction, chronic illness, and low libido. This test measures DHEA, Cortisol x 4, Serotonin, GABA, Dopamine, Epinephrine, Norepinephrine, Glutamate, Glycine, Histamine, Phenethylamine
Salivary Hormone:�
Comprehensive Plus: provides an assessment of breast cancer risk. This test is a considerationfor women only who have an increased risk for developing breast cancer, other hormonally sensitive cancers, PCOS or a family history of autoimmune disease. This test measures estrone, estriol, and Estrogen Quotient.
Women’s Helth and breast Profile: includes two risk assessment ratios, the Estrogen Quotient and the Pg/E2 ratio
Comprehensive Hormone: �assessment of hormonal status and endocrine function and includes estradiol, progesterone, testosterone, DHEA and four cortisols. This profile is useful with male and female patients because it looks at the full diurnal cortisol pattern; it is especially important in patients who are experiencing the full diurnal pattern ( weight gain, high blood sugar, elevated lipids, chronic fatigue)
Short Comprehensive: useful in men and women whose primary symptoms are related to sex hormone imbalances (elevated or depressed E2, P or T)
Basic Hormone: a basic evaluation of the sex hormones and a brief glimpse at the adrenal function with the AM cortisol level. Best for men who are experiencing decreased libido, erectile dysfunction, loss os stamina, decreased mental sharpness and metabolic syndrome. Best for women who are experiencing hot flashes, anxiety, night sweats, breast tenderness, irritability, forgetfulness, and acne.�
Comprehensive Adrenal Function: provides insight into the body�s stress response. This test measures sIgA
Adrenal Function: comprehensive view of adrenal function, DHEA, and cortisol levels. This is best for people who are fatigued, nervous, weak, crave sugar, have headaches, irritability, and depression
Diurnal Cortisol: Similar to the test above but for patients who do not need DHEA testing
Melatonin: Provides a snapshot of the sleep/wake cycle during a one day period
Salivary Hormone + CAR :
CAR: has the capability to test all the same markers as above but adds Cortisol Awakening Response “CAR” to all of them.�
For more information regarding testing and hormones tested, please visitlabrix.com��
LABRIX BASIC BOX CONTENTS:
Upon opening every box (no matter the labrix test) the patient will see a requisition form, a billable stamp, and a FedEx envelope. Under these two items, a styrofoam box (insulated cooler) with the imprint “doctorsdata.com” will be present. Once the patient lifts the lid off of the styrofoam box, they will see two more pieces of paper.� The first being a list of symptoms (patient survey) on a white sheet of paper that the patient is to fill out and place back in the styrofoam box and the second a small instruction manual.
Neurotransmitter Tests Breakdown
For the Neurotransmitter Tests, the patient is provided with the basic kit described above. The only sample type required for the neurotransmitter tests is urine.
The contents of the styrofoam box include a small plastic cup, a clear plastic bag consisting of a white tube, a dropper, an absorbent pad, and a Lab-Brix ice pack. The first step is to freeze the ice-pack and keep it frozen until ready to ship.�
In order for this test to have proper results, the patient should collect their sample with their first or second-morning urine upon waking. Then, select on the requisition form which urine ( first or second ) the sample was collected from. It is also important to note on the requisition form what time the patient woke and what time the sample was collected. The urine sample should be collected midstream. Patients will collect their sample in the plastic cup provided, not directly in the tube. Next, the patients will use the dropper provided to transfer 10 ml of the sample from the cup into the tube. Ensure the lid is screwed on tightly and gently rock the tube back and forth for 3-5 seconds to mix the urine with the preservative. The patients will then wrap the absorbent pad around the tube (not inside the tube), and place the sample tube back in the plastic bag. The bag is then to be placed in the freezer for 4-6 hours, and is to be kept frozen until ready to ship!�
Neurotransmitter + Hormone Tests Breakdown
The Neurotransmitter + Hormone analysis tests consist of urine and saliva samples. This basic test kit includes everything above. However, upon opening this styrofoam box the patient will find two plastic bags. The first being a plain plastic clear bag with a dropper, white test tube, and absorbent pad. The second plastic bag is a biohazard bag that has multiple colors on the outside and consists of 4 clear small straws, an absorbent pad, and 4 small saliva collection tubes of various colors.�
The urine sample is instructed to be taken the same way as the neurotransmitter test.
The patient should collect their sample with their first or second-morning urine upon waking. Then, select on the requisition form which urine ( first or second ) the sample was collected from. (Remember, the individual is� to note on the requisition form time they woke and what time the sample was collected). Patients will collect their sample mid-stream in the plastic cup provided, not directly in the tube. Next, use the dropper provided to transfer 10 ml of the sample from the cup into the tube. Be sure to check that the lid is screwed on tightly and gently rock the tube back and forth for 3-5 seconds to mix the urine with the preservative. The patients will then wrap the absorbent pad around the tube (not inside the tube), and place the sample tube back in the plastic bag. The bag is then to be placed in the freezer for 4-6 hours, and is to be kept frozen until ready to ship!��
The salivary collection has a few more steps considering it is 4 samples rather than one. The timing for the salivary testing is critical, so timers are encouraged. As the patient wakes up, a timer should be set for 30 minutes later. This is when the first salivary sample (the pink tube) is to be collected. Before this test, the patient should not eat, drink, brush or floss. The second collection (green tube) is to be taken right before lunch, around noon. The third (orange tube), is to be collected in the evening before dinner, and the final collection (blue tube) before bed at night.�
For all salivary collections, each tube needs to be 3/4 of the way full. The straws provided are the patient’s choice to be used. As soon as the tube is 3/4 of the way full, snap the saliva lid tightly, put into the bag in which it came, and freeze for 4-6 hours, until ready to ship. Patients are to record the date and times of the saliva collections on the bag and requisition form.�
Salivary Hormone
Considering the salivary hormone testing is done using 4 saliva samples, the instructions are the same as the saliva collection in the test mentioned above. However, to review them again,�the timing for the salivary testing is critical, so timers are highly encouraged.
As the patient wakes up, a timer should be set for 30 minutes later. This is when the first salivary sample (the pink tube) is to be collected. Before this test, the patient is not to eat, drink, brush or floss. For the second collection (green tube), it should be collected right before lunch, around noon. The third (orange tube), is to be obtained in the evening before dinner, and the final sample (blue tube) before bed at night.�
For all salivary collections, each tube needs to be 3/4 of the way full. The straws provided are to be used at the patient’s discretion. As soon as the tube is 3/4 of the way full, snap the saliva lid tightly, put into the bag in which it came, and freeze for 4-6 hours, until ready to ship. Patients are to record the date and times of the saliva collections on the bag and requisition form.�
Salivary Hormone + CAR Breakdown
Aside from the basic components, the styrofoam box includes 6 colored salvia collection tubes, 6 straws, and an absorbent pad. The tests that fall under this category require 6 samples throughout the day. It is important to remember to write down the time the samples were collected as well as the time when the patient first woke up. The first sample (yellow tube) is to be taken as soon as the patient is awake but has not gotten out of bed. In order to accomplish this properly, it is best the patient sets the tube next to their bed the night before. This makes it easy to collect first thing in the morning. It is very important that the patient sets an alarm for 30 minutes after they wake up ( second test, pink tube)and for 1 hour after they wake up (third test, lavender tube). These tests are all to be done prior to eating breakfast, brushing and flossing teeth. The fourth collection (green tube) is to be taken before lunch and the fifth (orange tube) before dinner. The sixth and final sample (blue tube) is to be collected at least one hour after dinner. Just as the other saliva samples mentioned above, these tubes are to be filled 3/4 of the way, tightly closed, placed back in the bag they came in and frozen for 4-6 hours, or until they are ready to ship.
SHIPPING INSTRUCTIONS FOR ALL TESTS:
Shipping should be done Monday-Friday as this will ensure the sample will be delivered to the lab on time. Make sure all paperwork is filled out properly and place contents back in the styrofoam box in the following order:�
sealed plastic bag with frozen specimen tubes
frozen ice pack�
requisition form, symptom sheet, and payment (if applicable)�
Next, place the lid back on the box and place the entire styrofoam box in the cardboard collection kit. Close the cardboard box and place it inside the FedEx shipping envelope provided. The patient will then write their name and address on the Billable Stamp and tear off the customer receipt for their records. Then, place on the FedEx envelope. The final step is to schedule a pick-up. In order to do this, the patient will call the FedEx toll-Free number at 1-800-463-3339 and select “schedule a pickup”. This MUST be a scheduled pick up from an address and NOT a dropbox.�
* It is important to note that patients should avoid eating avocados, eggplant, tomatoes, bananas, melons, pineapples, plums, nuts, nut butter, wine, cheese and chocolate 48 hours before and during the testing period as these could impact the results.
* Patients should keep in mind that strenuous exercise, alcohol, coffee, tea, tobacco or any other product containing nicotine is to be avoided 24 hours before and during the collection period.
Labrix is a great company that allows patients a noninvasive way to have their hormone levels checked. Almost every patient who walks in the door can benefit from this test. I highly recommend this test because hormone levels can change based on age, PMS symptoms, fatigue, blood sugar issues, or stress! These results are accurate and have a decently quick turn around time. Gaining insight and taking control of your body is now easier than ever. – Kenna Vaughn, Senior Health Coach
The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or chronic disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
*All information and photos/video content for this article are directly sourced from labrix. Please see labrix for more information and credit.
Do you feel that you must have sweets after meals? Do you get light-headed if you miss a meal? Or feel that craving for sweets during the day? Does your body feels shaky jittery or have tremors? If you are experiencing any of these situations, you may be experiencing LADA.
LADA
Autoimmune diabetes is a heterogeneous disease that can arise at any age. Anyone with adult-onset autoimmune diabetes who does not necessitate insulin therapy for at least six months after being diagnosed may have LADA (latent autoimmune diabetes of adulthood). LADA is a slowly progressing form of autoimmune diabetes, and it has been estimated that 20% of people are diagnosed with having non-obesity-related type 2 diabetes.
LADA occurs when the pancreas stops producing adequate insulin and slowly damages the insulin-producing cells in the pancreas, harming the body�s function. It is clear, however, that the frequency of autoimmune diabetes among adults can be underestimated, and clinical features such as age and severity of symptoms are of no help in identifying patients that have LADA since there is still more research being done to treat LADA. The body mass index and C peptide levels in the general population can increase with age, and these parameters are of limited use in identifying LADA patients.
Different Types of Diabetes
In a person, diabetes is a condition that impairs the body’s ability to process blood glucose, and roughly the estimated number of people over 18 years of age that are diagnosed and undiagnosed with diabetes is about 30.2 million. Without ongoing, careful management, diabetes can lead to a build-up of sugars in the blood, which can increase the risk of dangerous complications, including stroke and heart disease.
There are different kinds of diabetes, including LADA, that can occur, and managing the condition depends on the type of diabetes an individual has.
Type 1 Diabetes
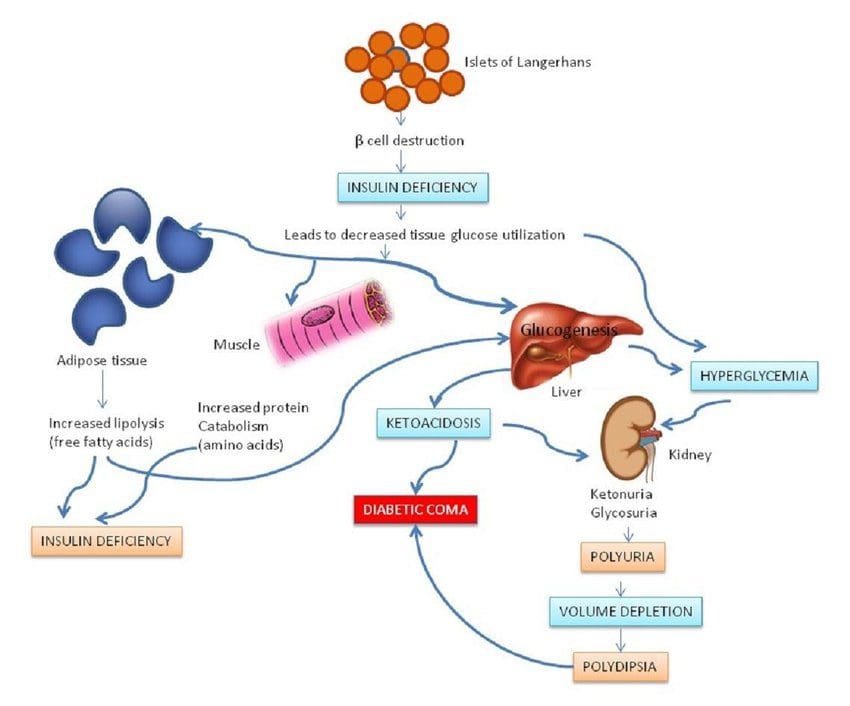
Type 1 diabetes is also known as juvenile diabetes, and the body does not produce enough insulin, and the blood glucose level remains high in the body. People with type 1 diabetes are insulin-dependent and must take artificial insulin daily to stay alive. The immune system attacks a cluster of cells known as islets in the pancreas that would typically produce insulin and stopping or slowing down the insulin production in the body.
When a person receives a diagnosis of type 1 diabetes from healthcare professionals, the islet cells are responsible for insulin secretion from the pancreas may continue to produce the insulin hormone for a while before ceasing. It can also lead to the production of LADA if it is not being monitored.
The physical effects of type 1 diabetes include:
Increased hunger and thirst
Frequent urination
Blurry vision
Tiredness and fatigue
Weight loss without an apparent trigger or causes.
Type 2 Diabetes
Type 2 diabetes is one of the most common forms of diabetes and can appear at any age, affecting over 30 million Americans. It happens when the blood sugar levels rise due to problems with the use or production of insulin.
Studies show that most people do not experience the symptoms in the early stages of type 2 diabetes, and they might have symptoms for many years. For those that do have type 2, diabetes may have acanthosis nigricans. Acanthosis nigricans is a skin condition that causes the skin to become thicker and darker. It often appears mostly on the neck, elbows, knees, knuckles, the folds around the neck and the groin.
Other early symptoms of type 2 diabetes that an individual may have included:
Frequent bladder, kidneys, or skin infections
Cuts that take longer to heal
Fatigue
Extreme hunger
Increased thirst
Urinary frequency
Blurred vision
Mixed Diabetes (Type 1.5)
Mixed diabetes or LADA is an autoimmune condition that shares the characteristics of both type 1 and type 2 diabetes in adults. It is diagnosed during adulthood and sets in the bloodstream gradually; however, unlike type 2, LADA is an autoimmune disease and is not reversible if the person changes their diet and lifestyle. �It can be triggered by the damage done to the pancreas from the antibodies against the insulin-producing cells.
If a person has LADA, their beta cells stop functioning much more quickly than type 2 diabetes. Researchers have found out that an estimated 10 percent of people who have diabetes will have LADA. It stated that the treatment for LADA patients is far less elucidated than the cases for type 1 and type 2 diabetes. Finding a treatment strategy for LADA can reduce the decline of beta-cell function, ensures adequate metabolic treatment so far.
Some of the symptoms that LADA patients may have include:
Frequent thirst
Increased urination, including at night
Unexplained weight loss
Blurred vision
Tingling nerves
If LADA is left untreated, it can lead to diabetic ketoacidosis, which is a condition where the body can not utilize sugar as fuel due to the absence of insulin and starts burning fat. It produces ketones, which are toxic to the body.
Type 3 Diabetes
Type 3 diabetes is known as brain diabetes and has an established linked to Alzheimer’s disease. This type of diabetes is triggered by a type of insulin resistance and an insulin-like growth factor dysfunction that occurs specifically in the brain, causing dementia.
Alzheimer�s disease has characteristics histopathological, molecular, and biochemical abnormalities in the brain’s cell structure. Since it has been linked with type 3 diabetes, characteristic features of type 3 diabetes include impairments in insulin actions and signaling that result in chronic hyperglycemia, irrespective of subtype, etiology, pathogenesis, or insulin availability.
Conclusion
Autoimmune diabetes can affect anyone at any age. It can damage the pancreas walls to stop producing insulin to the body, causing problems for an individual. LADA (latent autoimmune diabetes in adults) is an autoimmune disease that has the characteristics of type 1 and type 2 diabetes that are in adults. There is still more research being done to treat LADA, and there are products that can help support sugar metabolism and maintain blood sugar levels to a healthy range.
October is Chiropractic Health Month. To learn more about it, check out Governor Abbott�s declaration on our website to get full details on this historic moment.
The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or chronic disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
References:
Barhum, Lana. �Type 2 Diabetes: Symptoms, Early Signs, and Complications.� Medical News Today, MediLexicon International, 16 Apr. 2019, www.medicalnewstoday.com/articles/317462.php.
Castro, M. Regina. �Latent Autoimmune Diabetes in Adults (LADA): What Is It?� Mayo Clinic, Mayo Foundation for Medical Education and Research, 10 May 2019, www.mayoclinic.org/diseases-conditions/type-1-diabetes/expert-answers/lada-diabetes/faq-20057880.
de la Monte, Suzanne M, and Jack R Wands. �Alzheimer’s Disease Is Type 3 Diabetes-Evidence Reviewed.� Journal of Diabetes Science and Technology, Diabetes Technology Society, Nov. 2008, www.ncbi.nlm.nih.gov/pmc/articles/PMC2769828/.
Felman, Adam. �Type 1 Diabetes: Overview, Symptoms, and Treatment.� Medical News Today, MediLexicon International, 19 Nov. 2018, www.medicalnewstoday.com/articles/323729.php.
Hals, Ingrid K. �Treatment of Latent Autoimmune Diabetes in Adults: What Is Best?� Current Diabetes Reviews, U.S. National Library of Medicine, 2019, www.ncbi.nlm.nih.gov/pubmed/30009709.
Leonard, Jayne. �Acanthosis Nigricans: Causes, Symptoms, Treatment, and Pictures.� Medical News Today, MediLexicon International, 21 Dec. 2018, www.medicalnewstoday.com/articles/324062.php.
MSN, Rachel Nall RN. �Diabetes: Symptoms, Treatment, and Early Diagnosis.� Medical News Today, MediLexicon International, 8 Nov. 2018, www.medicalnewstoday.com/articles/323627.php.
Pozzilli, Paolo, and Silvia Pieralice. �Latent Autoimmune Diabetes in Adults: Current Status and New Horizons.� Endocrinology and Metabolism (Seoul, Korea), Korean Endocrine Society, June 2018, www.ncbi.nlm.nih.gov/pmc/articles/PMC6021307/.
Prelipcean, Maria S. �What You Need to Know About Type 1.5 Diabetes.� Healthline, 2 Nov. 2018, www.healthline.com/health/type-1-5-diabetes.
Watson, Kathryn. �Type 3 Diabetes and Alzheimer’s Disease: What You Need to Know.� Healthline, 16 Oct. 2019, www.healthline.com/health/type-3-diabetes.
Wint, Carmella, and Marijane Leonard. �What You Should Know About Diabetic Ketoacid.� Healthline, 4 Dec. 2018, www.healthline.com/health/type-2-diabetes/ketoacidosis.
Microbes have multicellular hosts and can have many effects on the host�s health and well-being. Researchers have stated that microbes influence metabolism, immunity, and behavior on the human body. One of the most important but understudied mechanisms that microbes have is that they can involve hormones. In the presence of gut microbiota, specific changes in hormone levels can correlate in the gut. The gut microbiota can produce and secrete hormones, respond to the host hormones, and regulate their expression levels. There is also a link between the endocrine system and the gut microbiota as more information is still being researched.
The Gut to Hormone Connection
Since the human microbiome contains a vast array of microbes and genes that shows a higher complexity. Unlike other organs in the body, the gut microbiota’s function is not fully understood yet but can be disrupted easily by antibiotics, diet, or surgery. The best-characterized function is how the gut microbiota interacts with the endocrine system in the body.
Emerging research has indicated that the gut microbiome plays a central role in regulating estrogen levels within the body. When the estrogen hormone levels are too high or too low, it can lead to the risk of developing estrogen-related diseases like endometriosis, polycystic ovary syndrome, breast cancer, and prostate cancer to males and females.
The gut to hormone connection is essential since the gut is one of the producers to create hormones that travel through the entire body system. With the endocrine system is being involved, it is the first network to produce and transport hormones to the organs that need the hormones to function. When there is an imbalance of hormones in the human body, it can disrupt all the other hormones.
The gut microbiota influences nearly every hormone that the endocrine system creates, including:
The thyroid hormones
Estrogen hormones
Stress hormones
Thyroid Hormones
If the gut has inflammation, then the hormones in the body will create an excessive or low quantity in the body. If the endocrine glands like thyroid, are producing a low quantity of hormones and the gut can be imbalanced and lead to hypothyroidism. When there is low microbial diversity in the gut, studies have shown that the low microbial diversity is linked to high TSH (thyroid-stimulating hormone) levels. The excessive quantity of thyroid hormones can lead to hyperthyroidism. Both hyperthyroidism and hypothyroidism can cause symptoms like irritability, anxiety, poor memory, and many symptoms that can affect the body.
“If you are experiencing excessive belching, burping, bloating, difficult bowel movements difficulty digesting proteins and meats; undigested food found in stools, digestive problems subside with rest and relaxation or any symptoms. Then this article will give you a better understand what is happening with the gut and how hormones can affect the gut system.”
Estrogen Hormones
The gut and an individual’s hormones are meant to be in communication with each other. They not only support each other, but they also work together to make sure the body is running smoothly. Studies have found out that the gut’s intestinal cells have special receptors for hormones that allow them to detect any hormonal shifts that affect the body.
Since estrogen is typically associated with women, it is common that men need the right amount of estrogen levels to function. The gut microbiota is the key regulator of leveling and circulating estrogen in the body. The microbes produce an enzyme called beta-glucuronidase, which then converts the estrogen hormone to its active form.
The gut microbiome can regulate estrogen levels by functioning a specific bacteria in the microbiome called estrobolome. Estrobolome is the aggregates of enteric bacterial genes that are capable of metabolizing estrogen. It might affect women’s risk of developing postmenopausal estrogen receptor-positive breast cancer. The estrobolome is highly essential to keep estrogen levels in the body at a stable state.
In the gut microbiota, both the estrogen and progesterone hormones can impact the guts’ motility and peristalsis ( The rhythmic movement of the intestines that move food through the stomach and out of the body) by playing opposing roles in the guts� motility. Progesterone helps slow down the gut�s motility by relaxing the smooth and slowing transit the time the food is moving out of the body. Estrogen helps increase the contraction of the smooth muscles in the intestines. When the estrogen hormones are leveled right, it can help keep the gut moving smoothly and help increase the diversity of the body�s microbiomes, which is a good thing for the immune system.
Stress Hormones
Stress hormones or cortisol plays a massive part in the gut microbiota. Since cortisol hormones connect to the brain, it sends the signals to the gut and vice versa. If it is a short stressor like getting ready for a presentation or a job interview, the person will feel “butterflies” in their gut. The longer stressors, for example, like having a highly stressful job or feeling anxious consistently, can lead to chronic illnesses in the gut like inflammation or leaky gut. Since the hormone and gut connection is in sync with the gut and brain connection, it is crucial to lowering the cortisol levels to a stable state for a healthy functional body.
Conclusion
The gut and hormone connections are profoundly meaningful since they are linked closely together. When there is a disruption on the gut, it can cause hormones to be imbalanced, causing many disruptions like inflammation and leaky gut. When there is a disruption in the hormones, it can disrupt the gut as well by negatively shifting the gut’s microbiome. So to ensure that the gut is functioning correctly, it is crucial to eat food that contains probiotics and is fermented to keep the gut flora healthy. Some products can help counter the metabolic effects of temporary stress and supporting estrogen metabolism by incorporating other essential nutrients and cofactors to support the endocrine system.
October is Chiropractic Health Month. To learn more about it, check out Governor Abbott�s declaration on our website to get full details on this historic moment.
The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or chronic disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
References:
Author, Guest. �How Your Gut Microbiome Influences Your Hormones.� Bulletproof, 21 Aug. 2019, www.bulletproof.com/gut-health/gut-microbiome-hormones/.
Evans, James M, et al. �The Gut Microbiome: the Role of a Virtual Organ in the Endocrinology of the Host.� The Journal of Endocrinology, U.S. National Library of Medicine, 28 Aug. 2013, www.ncbi.nlm.nih.gov/pubmed/23833275.
Kresser, Chris. �The Gut�Hormone Connection: How Gut Microbes Influence Estrogen Levels.� Kresser Institute, Kresserinstitute.com, 10 Oct. 2019, kresserinstitute.com/gut-hormone-connection-gut-microbes-influence-estrogen-levels/.
Kwa, Maryann, et al. �The Intestinal Microbiome and Estrogen Receptor-Positive Female Breast Cancer.� Journal of the National Cancer Institute, Oxford University Press, 22 Apr. 2016, www.ncbi.nlm.nih.gov/pmc/articles/PMC5017946/.
Neuman, Hadar, et al. �Microbial Endocrinology: the Interplay between the Microbiota and the Endocrine System.� OUP Academic, Oxford University Press, 20 Feb. 2015, academic.oup.com/femsre/article/39/4/509/2467625.
Szkudlinski, Mariusz W, et al. �Thyroid-Stimulating Hormone and Thyroid-Stimulating Hormone Receptor Structure-Function Relationships.� Physiological Reviews, U.S. National Library of Medicine, Apr. 2002, www.ncbi.nlm.nih.gov/pubmed/11917095.
Wieselman, Brie. �Why Your Gut Health and Microbiome Make-or-Break Your Hormone Balance.� Brie Wieselman, 28 Sept. 2018, briewieselman.com/why-your-gut-health-and-microbiome-make-or-break-your-hormone-balance/.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine