Stomach pain, burning, or aching 1-4 hours after eating?
Unpredictable abdominal pain?
Gas immediately following after a meal?
Excessive belching, burping, or bloating?
If you are experiencing any of these situations, then try these top ten superfoods to prevent inflammation in your body.
Superfoods lack any formal criteria, and people wonder what makes a food a superfood. Medical experts agreed that foods with the title “superfood” have health benefits that go far beyond what is listed on their nutrition labels. There is a wide range of health-promoting superfoods that can be incorporated into a person’s diet in several different ways. Eating superfood alone will not make anyone healthier overnight, but adding them to an already balanced diet can give anyone a mega-dose of added health benefits to their body.
Getting to Know Superfoods
According to the Merriam-Webster Dictionary, a superfood is defined as “a food that rich in compounds and considered beneficial to a person’s health. It can be any foods that have antioxidants, fatty acids, or fibers in their nutrient compounds. While the Oxford Dictionary defines a superfood as �a nutrient-rich food that is considered to be especially beneficial for health and well-being.�
Here are the top ten superfoods that have been scientifically proven to help optimize the body’s ability to function correctly. These superfoods are not only super healthy, but they are affordable and readily available in the grocery stores, online, and at farmer’s markets.
A�ai Berries
A�ai berries are high in antioxidants. They also contain B vitamins, magnesium, potassium, healthy fats, and phosphorus. The a�ai berry is one of the most well-known superfoods that is beneficial for the body’s microbiome. Studies have shown that a�ai berries have anti-inflammatory properties, help improve the cognitive function, maintaining healthy blood sugar levels, and protect against heart diseases. The berries themselves have also been suggested to help slow down age-related memory loss in individuals.
Studies have shown that the health benefits of the a�ai berries are that the berries contain a range of polyphenols that protects cellular oxidative damage in vitro and can provide ant-inflammatory signaling in the body by reducing the production of free radicals by inflammatory cells. Chronic inflammation in the body can lead to diseases like fibromyalgia. So consuming this berry can help lower the risk of inflammation in the body.
Plant-based protein
Plant proteins are abundant, branched-chain containing essential amino acids, and are exceptionally high in lysine. Research has been shown that lysine can help balance blood glucose in the body. Lysine even can increase muscle strength and combat anxiety in the body.
Plant-based proteins that contain carotenoids and flavonoids can modulate inflammatory responses in the body as well as the immunological process as well. Plant foods have anti-inflammatory potential that everyone needs in their diet to reduce inflammatory responses that is in the body.
Salmon
Salmon is a superfood that has one of the highest sources for omega-3 fatty acids. Omega-3 fatty acids have been shown to lower the risk of developing coronary heart diseases, lowers metabolic syndrome, and diabetes. Studies have been shown that fish oil has also been known to help combat late-onset Alzheimer�s disease.
Consuming salmon or any foods that contain omega-3s may help alleviate oxidative stress that the body may have picked up. Omega-3s even play a role in lowering the risk of inflammation on individuals who have to develop fibromyalgia. Since it associates with pro-inflammatory cytokines, eating omega-3 fatty foods can help lower the inflammation and alleviate it as well.
Avocados
Avocados are a nutrient-rich superfood, high fiber fruits that play a significant role in combating chronic diseases in the body. Eating avocados regularly have been known to lower the risk of heart disease, metabolic syndrome, diabetes, and certain cancers.
Since avocados are a nutrient-dense source of MUFA (monounsaturated fatty acids), the fruit can be used to replace SFA (saturated fatty acids) in a diet to lower LDL-C (low-density lipoprotein cholesterol) in the body.
Kale
Kale has an excellent source of nutrients like zinc, folate, magnesium, calcium, vitamin C, fiber, and iron. Research has shown that dark leafy greens can reduce the risk of chronic illnesses like type 2 diabetes and heart disease.
Olive oil
Olive oil is a superfood that has been shown to provide a range of various health benefits. Extra virgin olive oil is associated with reducing the risk of cardiovascular disease and mortality on individuals that have a high cardiovascular risk.
Olive oil has a monounsaturated fat called oleic acid, which helps reduce inflammation in the body.
Sweet potato
Sweet potato is the superfood root vegetable that is full of nutrients that are beneficial to the body. They are an excellent source of carotenoids, fiber, potassium, vitamin C, and vitamin A.
Consuming sweet potato is beneficial for the body due to reducing the risk of inflammation and DNA damage. Since it contains high levels of antioxidants, it may also prevent cell damage as well in the body.
Fermented Foods
Fermented foods like yogurt, kefir sauerkraut, and many others are heavily sought after superfoods by consumers. This is because fermented foods have a range of fantastic health benefits like antioxidants, anti-microbial, anti-fungal, anti-inflammatory, andante-diabetic properties.
Green tea
Green tea is a lightly caffeinated beverage that has a broad spectrum of health benefits for the body. It is rich with antioxidants and polyphenolic compounds that can protect the body against chronic diseases and be a useful tool for bodyweight management.
Seaweed
Seaweed is packed with several nutrients like folate, vitamin K iodine, and fiber that is beneficial for the body. It plays an essential role by helping lowering blood pressure and to treat several chronic illnesses. Studies have shown that due to their potential beneficial activities such as anti-inflammatory and anti-diabetic effects that are beneficial to prevent flare-ups in the white adipose tissue and systemic IR.
Conclusion
Superfoods are an essential additive boost to any healthy diet. These ten superfoods contain anti-inflammatory properties that are beneficial to the body to prevent the risk of inflammation in the body. Eating these foods combine with these products will provide relief from oxidative stress and inflammation that the body may encounter, as well as providing support to the endocrine system.
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues as well as functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or chronic disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at�915-850-0900�.
References:
Basu, Arpita, et al. �Dietary Factors That Promote or Retard Inflammation.� Arteriosclerosis, Thrombosis, and Vascular Biology, U.S. National Library of Medicine, May 2006, www.ncbi.nlm.nih.gov/pubmed/16484595.
Dellwo, Adrienne. �The Potential Benefits of Omega-3 for Fibromyalgia & CFS.� Verywell Health, Verywell Health, 7 July 2019, www.verywellhealth.com/omega-3-for-fibromyalgia-and-chronic-fatigue-syndrome-715987.
Felman, Adam. �Fibromyalgia: Symptoms, Causes, and Treatment.� Medical News Today, MediLexicon International, 5 Jan. 2018, www.medicalnewstoday.com/articles/147083.php.
Jensen, Gitte S, et al. �Pain Reduction and Improvement in Range of Motion after Daily Consumption of an A�ai (Euterpe Oleracea Mart.) Pulp-Fortified Polyphenolic-Rich Fruit and Berry Juice Blend.� Journal of Medicinal Food, Mary Ann Liebert, Inc., 2011, www.ncbi.nlm.nih.gov/pmc/articles/PMC3133683/.
Oh, Ji-Hyun, et al. �Anti-Inflammatory and Anti-Diabetic Effects of Brown Seaweeds in High-Fat Diet-Induced Obese Mice.� Nutrition Research and Practice, The Korean Nutrition Society and the Korean Society of Community Nutrition, Feb. 2016, www.ncbi.nlm.nih.gov/pmc/articles/PMC4742310/.
Smriga, Miro, et al. �Lysine Fortification Reduces Anxiety and Lessens Stress in Family Members in Economically Weak Communities in Northwest Syria.� Proceedings of the National Academy of Sciences of the United States of America, National Academy of Sciences, 1 June 2004, www.ncbi.nlm.nih.gov/pubmed/15159538.
Tanaka, Takuji, et al. �Cancer Chemoprevention by Carotenoids.� Molecules (Basel, Switzerland), MDPI, 14 Mar. 2012, www.ncbi.nlm.nih.gov/pubmed/22418926.
Unknown, Unknown. �What Are Superfoods? Top 10 Superfoods.� Fullscript, 4 Mar. 2019, fullscript.com/blog/superfoods.
Unni, Uma S, et al. �The Effect of a Controlled 8-Week Metabolic Ward Based Lysine Supplementation on Muscle Function, Insulin Sensitivity and Leucine Kinetics in Young Men.� Clinical Nutrition (Edinburgh, Scotland), U.S. National Library of Medicine, Dec. 2012, www.ncbi.nlm.nih.gov/pubmed/22524975.
Wang, Li, et al. �Effect of a Moderate Fat Diet with and without Avocados on Lipoprotein Particle Number, Size and Subclasses in Overweight and Obese Adults: a Randomized, Controlled Trial.� Journal of the American Heart Association, Blackwell Publishing Ltd, 7 Jan. 2015, www.ncbi.nlm.nih.gov/pubmed/25567051.
Wang, Ping-Yu, et al. �Higher Intake of Fruits, Vegetables or Their Fiber Reduces the Risk of Type�2 Diabetes: A Meta-Analysis.� Journal of Diabetes Investigation, John Wiley and Sons Inc., Jan. 2016, www.ncbi.nlm.nih.gov/pubmed/26816602.
Watzl, Bernhard. �Anti-Inflammatory Effects of Plant-Based Foods and of Their Constituents.� International Journal for Vitamin and Nutrition Research. Internationale Zeitschrift Fur Vitamin- Und Ernahrungsforschung. Journal International De Vitaminologie Et De Nutrition, U.S. National Library of Medicine, Dec. 2008, www.ncbi.nlm.nih.gov/pubmed/19685439.
?anlier, Nevin, et al. �Health Benefits of Fermented Foods.� Critical Reviews in Food Science and Nutrition, U.S. National Library of Medicine, 2019, www.ncbi.nlm.nih.gov/pubmed/28945458.
If you are experiencing any of these situations, then try considering intermittent fasting.
Since becoming popular in recent years, intermittent fasting is a dietary approach that lots of individuals have been using in their healthy lifestyle. During the time of the hunter-gatherer society, people have used this method for centuries as a way of survival. Studies have been shown that people used it for medicinal purposes throughout history as a medicinal remedy. Ancient Rome, Greek and Chinese civilizations used intermittent fasting in their daily lives. Fasting has even been used for spiritual reasons in certain religions, like Buddhism, Islam, and Christianity as individuals use it as a way to reflect on themselves and be closer to their deities.
What is Fasting?
Fasting is where a person does not consume food or beverages at least for twelve hours during the day. When a person starts fasting, they will notice that their metabolism and their hormones will change in their bodies. There is upcoming research that intermittent fasting can promote amazing health benefits to the body. The health benefits that intermittent fasting provides are weight loss, protective effects in the brain, decreased inflammation and improving blood glucose and insulin levels in the body.
The Different Methods
There are other methods of fasting that involves fasting from food for several days or weeks. With these different methods, they involve a shorter period that is between 16 to 24 hours. Several types of intermittent fasting are determined by the feeding window duration (when to eat the food) and the fasting window (when to avoid the food). Here are some of the other methods of fasting, which includes:
Time-restricted feeding (TRF): This type of fasting has a feeding window period from 4 to 12 hours. For the remainder of the day, water is the only thing that is allowed to be consumed. The common variation to eat this type of fasting is 16/8. This means that a person has to fast at least 16 hours every day.
Early time-restricted feeding (eTRF): This is a different variety of time-restricted fasting that is from 8 a.m. to 2 p.m. After the 6 hours are up, the rest of the day is made up of this fasting period.
Alternate day fasting (ADF): This type of fasting involves a person eating one day and the next day they completely fast. They alternate between eating and fasting each day to get the benefits.
Period fasting (cycling fasting): This type of fasting involves one or two days fasting per week and for the fifth or sixth days of eating as much as a person desire. The variety of period fasting can be a 5:2 or a 6:1.
Modified fasting: This type of fasting has some methods of intermittent fasting that are similar to alternate-day fasting, but this fasting can be modified for anyone. A person can consume very-low-calorie substances during the fasting window period.
How Does It Work?
Intermittent fasting is the result of changes in the body as the hormone patterns and energy metabolism are being affected. Once a person finishes consuming food, the contents are being broken down and transforming into nutrients, so it can be absorbed into the digestive tract. What happens is that the carbohydrates are broken down and turn into glucose and absorb into the bloodstream, distributing it into the body’s tissue as the essential source of energy. The insulin hormone then helps regulate the blood glucose levels by signaling cells to take the sugars from the blood and turning into fuel for the body to function properly.
With intermittent fasting, a person is done with a meal and their glucose levels are depleted from the body. For the energy to meet its requirements the body has to break down the glycogen that is found in the liver and skeletal muscles causing gluconeogenesis. Gluconeogenesis is when the liver produces glucose sugars from non-carbohydrate sources in the body. Then once the insulin levels are low after 18 hours of fasting, a process called lipolysis begins. What lipolysis does is that the body begins to break down the fat components into free fatty acids. When there is a low quantity of glucose for the body to consume for energy, the body itself with start using fatty acids and ketones for energy. Ketosis is a metabolic state where liver cells start to help fatty acids breakdown and converting them into ketone acetoacetate and beta-hydro butyrate.
The muscle cells and neuron cells use these ketones to generate ATP (adenosine triphosphate) which is the main carrier for energy. Research has stated that the usage and availability of fatty acids combined with ketones as an energy replacement for glucose are beneficial for vital body tissues. This includes the heart, the liver, the pancreas, and the brain.
The four metabolic states are induced by fasting are referred to as the fast-fed cycle, and they are:
The fed state
The post-absorptive state
The fasting state
The starvation state
The physiological effect of intermittent fasting can also be achieved by following a ketogenic diet, which is very high fat and low carbohydrate diet. This diet’s purpose is to shift the body’s metabolic state into ketosis.
The Benefits of Fasting
There are tons of research that have demonstrated how intermittent fasting has a wide variety of health benefits, including:
Weight loss
Type 2 diabetes prevention and management
Improved cardiometabolic risk factors
Cellular cleansing
Decreased inflammation
Neuroprotection
Studies have been shown that several proposed mechanisms are responsible for these health effects of intermittent fasting and have proven to be beneficial to a person’s lifestyle.
Conclusion
Intermittent fasting has been practiced for centuries and has gain popularity in recent years. It involves abstaining from consuming foods for at least 12 consecutive hours by turning the fat cells into energy for the body to function. The health benefits that intermittent fasting provides is beneficial for an individual who is trying to maintain a healthy lifestyle. Some products help provide support to the gastrointestinal system as well as making sure that sugar metabolism is at a healthy level for the body to function.
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
References:
Dhillon, Kiranjit K. �Biochemistry, Ketogenesis.� StatPearls [Internet]., U.S. National Library of Medicine, 21 Apr. 2019, www.ncbi.nlm.nih.gov/books/NBK493179/#article-36345.
Hue, Louis, and Heinrich Taegtmeyer. �The Randle Cycle Revisited: a New Head for an Old Hat.� American Journal of Physiology. Endocrinology and Metabolism, American Physiological Society, Sept. 2009, www.ncbi.nlm.nih.gov/pmc/articles/PMC2739696/.
Stockman, Mary-Catherine, et al. �Intermittent Fasting: Is the Wait Worth the Weight?� Current Obesity Reports, U.S. National Library of Medicine, June 2018, www.ncbi.nlm.nih.gov/pmc/articles/PMC5959807/.
Zubrzycki, A, et al. �The Role of Low-Calorie Diets and Intermittent Fasting in the Treatment of Obesity and Type-2 Diabetes.� Journal of Physiology and Pharmacology: an Official Journal of the Polish Physiological Society, U.S. National Library of Medicine, Oct. 2018, www.ncbi.nlm.nih.gov/pubmed/30683819.
Like you have been diagnosed with Celiac Disease, Irritable Bowel Syndrome, Diverticulosis/Diverticulitis, or Leaky Gut Syndrome?
Excessive belching, burping, or bloating?
Abnormal distention after certain probiotics or natural supplements?
Suspicion of nutritional malabsorption?
Do digestive problems subside with relaxation?
If you are experiencing any of these situations, then you might be experiencing gut problems and might have to try the 4R Program.
Food sensitivities, rheumatoid arthritis, and anxiety have been associated with impaired gastrointestinal permeability. These various conditions can happen from many factors that can impact the digestive tract. If left untreated it can potentially be the result of dysfunction of the intestinal permeability barrier, causing inflammation, and severe health conditions that the gut can develop. The 4R program is used to restore a healthy gut in the body and involves four steps. They are: remove, replace, reinoculated, and repair.
Intestinal Permeability
The intestinal permeability helps protects the body and makes sure that harmful bacteria do not enter the gut. It protects the body from potential environmental factors that can be harmful and are entering through the digestive tract. It can be either toxin, pathogenic microorganisms, and other antigens that can harm the digestive tract causing problems. The intestinal lining is consisting of a layer of epithelial cells that are separated by tight junctions. In a healthy gut, the tight junction regulates the intestinal permeability by selectively allowing substances to enter and travel across the intestinal barrier and preventing harmful factors from being absorbed.
Certain environmental factors can damage the tight junction, and the result is that it can increase the intestinal permeability, which causes intestinal hyperpermeability or leaky gut in the body. Contributing factors can increase intestinal permeability like an excessive amount of saturated fats and alcohol, deficiencies in nutrients, chronic stress, and infectious diseases.
With an increased intestinal permeability in the gut, it can enable antigens to cross the gut mucosa and enter the bloodstream causing an immune response and inflammation to the body. There are certain gastrointestinal conditions that are associated with intestinal hyperpermeability and if left untreated it can trigger certain autoimmune conditions that can cause harm to the body.
4Rs Program
The 4Rs is a program that healthcare professionals advise their patients to use when they are addressing disruptive digestive issues and help support gut healing.
Removing the Problem
The first step in the 4Rs program is to remove harmful pathogens and inflammation triggers that are associated with increased intestinal permeability. Triggers like stress and chronic alcohol consumption can do much harm to an individual’s body. So targeting these harmful factors from the body is to treat it with medication, antibiotics, supplements, and the removal of inflammatory foods from the diet is advised, including:
– Alcohol
– Gluten
– Food additives
– Starches
– Certain fatty acids
– Certain foods that a person is sensitive to
Replacing the Nutrients
The second step of the 4Rs program is to replace the nutrients that are causing the gut problems through inflammation. Certain nutrients can help reducing inflammation in the gut while making sure that the digestive tract is being supported. There are some anti-inflammatory foods that are nutritious. These include:
– High-fiber foods
– Omega-3s
– Olive oil
– Mushrooms
– Anti-inflammatory herbs
There are certain supplements can be used to support digestive function by assisting and absorbing the nutrients to promote a healthy gut. What the digestive enzymes do is that they assist in helping to break down fats, proteins, and carbohydrates in the gut. This will help benefit individuals that have an impaired digestive tract, food intolerances, or having celiac disease. Supplements like bile acid supplements can help assist in nutrient absorption by merging lipids together. Studies have stated that bile acids have been used to treat the liver, gallbladder, and bile duct while preventing gallstone formation after bariatric surgery.
Reinoculated The Gut
The third step is of the 4rs program to reinoculated the gut microbe with beneficial bacteria to promote a healthy gut function. Studies have been shown that probiotic supplements have been used to improve the gut by restoring beneficial bacteria. With these supplements, they provide the gut an enhancement by secreting anti-inflammatory substances into the body, help support the immune system, altering the body’s microbial composition, and reducing the intestinal permeability in the gut system.
Since probiotics are found in fermented foods and are considered as a transient since they are not persistent in the gastrointestinal tract and are beneficial. Surprisingly, they still have an impact on human health due to influencing the gut by producing vitamins and anti-microbial compounds, thus providing diversity and gut function.
Repairing the Gut
The last step of the 4Rs program is to repair the gut. This step involves repairing the intestinal lining of the gut with specific nutrients and herbs. These herbs and supplements can help decrease intestinal permeability and inflammation in the body. Some of these herbs and supplements include:
– Aloe vera
– Chios mastic gum
– DGL (Deglycyrrhizinated licorice)
– Marshmallow root
– L-glutamine
– Omega-3s
� Polyphenols
– Vitamin D
– Zinc
Conclusion
Since many factors can adversely affect the digestive system in a harmful way and can be the contributor to several health conditions. The main goal of the 4Rs program is to minimize these factors that are harming the gut and reducing inflammation and increased intestinal permeability. When the patient is being introduced to the beneficial factors that the 4Rs provide, it can lead to a healthy, healed gut. Some products are here to help support the gastrointestinal system by supporting the intestines, improving the sugar metabolism, and targeting the amino acids that are intended to support the intestines.
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
References:
De Santis, Stefania, et al. �Nutritional Keys for Intestinal Barrier Modulation.� Frontiers in Immunology, Frontiers Media S.A., 7 Dec. 2015, www.ncbi.nlm.nih.gov/pmc/articles/PMC4670985/.
Ianiro, Gianluca, et al. �Digestive Enzyme Supplementation in Gastrointestinal Diseases.� Current Drug Metabolism, Bentham Science Publishers, 2016, www.ncbi.nlm.nih.gov/pmc/articles/PMC4923703/.
Mu, Qinghui, et al. �Leaky Gut As a Danger Signal for Autoimmune Diseases.� Frontiers, Frontiers, 5 May 2017, www.frontiersin.org/articles/10.3389/fimmu.2017.00598/full.
Rezac, Shannon, et al. �Fermented Foods as a Dietary Source of Live Organisms.� Frontiers in Microbiology, Frontiers Media S.A., 24 Aug. 2018, www.ncbi.nlm.nih.gov/pmc/articles/PMC6117398/.
Sander, Guy R., et al. �Rapid Disruption of Intestinal Barrier Function by Gliadin Involves Altered Expression of Apical Junctional Proteins.� FEBS Press, John Wiley & Sons, Ltd, 8 Aug. 2005, febs.onlinelibrary.wiley.com/doi/full/10.1016/j.febslet.2005.07.066.
Sartor, R Balfour. �Therapeutic Manipulation of the Enteric Microflora in Inflammatory Bowel Diseases: Antibiotics, Probiotics, and Prebiotics.� Gastroenterology, U.S. National Library of Medicine, May 2004, www.ncbi.nlm.nih.gov/pubmed/15168372.
If you are suffering from any of these symptoms, then you might be experiencing an allergy attack in your body.
The Rise of Allergies
The rise of allergies has not gone unnoticed amongst the young and the old. The allergy disease has affected over 30% of individuals in many communities, particularly young children, have underscored the need for effective prevention strategies in their early lives. Some individuals will blame the increase in toxin exposure while others blame the food, but mostly everyone will admit that the answers to how the allergy disease comes from are still unclear. Whether it be food, environmental factors, or skin allergies, the common denominator that causes the allergies to develop is in the immune system, especially in its inflammatory department.
The body�s immune system is linked to the entire body microbiome, and it also resides in the gastrointestinal tract. It has been said that the health and function of the immune system are directly associated with the diversity as well as the health of the microbiome. So it is reasonable to consider the microbiome when healthcare professionals are seeking to solve the allergy enigma.
Types of Allergic Reactions
With most allergy reactions, they are manifested in either the gastrointestinal tract, respiratory tract, or the skin. It is not a surprise that these organ systems are also where the body’s microbiome is the most heavily concentrated. A variety of bacterial species make their homes in these organ systems since these three organ systems represent the primary portals of entry for these pathogens.
It is logically that the microbiome of the body is so heavily concentrated as it functions as the first line of defense against invading pathogens and antigens. When there is a weak microbiome, or it lacks biodiversity, it will become a weak defense system, and the immune system is required to “pick up the slack” by identifying and protecting the body against these foreign invaders, which includes the common allergens that a person can get.
Skin Allergies
Skin allergies are where the skin becomes red, bumpy, and itchy rashes to become irritating, painful, and embarrassing for some people. Rashes can be caused by many factors, including exposure to certain plants, an allergic reaction to specific medication or food, or by illnesses like measles or chickenpox. Eczema, hives, and contact dermatitis are the three types of skin rashes. Eczema and hives are the two most common types of skin rashes and are related to allergies.
Eczema: Also known as atopic dermatitis, can affect between 10 to 20 percent of children and 1 to 3 percent of adults. People with eczema will experience dry, red, irritated, and itchy skin. When it is infected, the skin may have small fluid-filled bumps that can ooze clear or yellowish liquid. Anyone with eczema can often have a family history of allergies.
Hives: Also known as urticaria, this skin rash is raised, red bumps or welts that appear on the body. Hives can cause two conditions, and they are acute urticaria and chronic urticaria. Acute urticaria is most commonly caused by exposure to an allergen or by an infection, while the causes of chronic urticaria are still mostly unknown.
Contact dermatitis: This skin rash is a reaction that appears when the skin comes in contact with an irritant or an allergen. Soaps, laundry products, shampoos, Excessive exposure to water, or the sun are some of the factors that can cause contact dermatitis. The symptoms can include rashes, blisters, itching, and burning.
Food Allergies
Anyone with a food allergy has an immune system that reacts to specific proteins found in food. Their immune system starts attacking these compounds as if they were harmful pathogens like a bacterium or a virus. Food allergies can affect 250 million to 550 million people in developed and developing countries.
The symptoms can range from mild to severe and can affect individuals differently. The most common signs and symptoms of an individual’s experience include:
The skin may become itchy or blotchy
Lips and face might swell
Tingling in the mouth
Burning sensation on the lips and mouth
Wheezing
Runny nose
Studies have found out that many people who think they have a food allergy may have a food intolerance. These two are entirely different because food intolerances do not involve the IgE antibodies, and the symptoms may be immediate, delayed, or similar to food allergies. Food intolerances occur due to proteins, chemicals, and other factors that can compromise the intestinal permeability. While food allergies mean that even a small amount of food is going to trigger the immune system, causing an allergic reaction.
Seasonal Allergies
Seasonal allergies are one of the most common allergic reactions that people get. About 8 percent of Americans experience it, according to the American Academy of Allergy, Asthma, and Immunology, and it is commonly known as hay fever. Hay fever occurs when the immune system overreacts to outdoor allergens like pollen, weeds, cut grasses, and wind-pollinated plants.� Seasonal allergies are less common in the winter; however, it is possible to experience allergic rhinitis year-round, depending on where the individual lives and on the allergy triggers they may have.
Symptoms of seasonal allergies can range from mild to severe, including:
Sneezing
Runny or stuffy nose
Water and itchy eyes
Itchy throat
Ear congestion
Postnasal drainage
Conclusion
Allergies are a disease that attacks the immune system and can be triggered by many factors, whether it be from food, environmental factors, or the toxins that a person is exposed to. There are ways to lower the allergy symptoms through medicine or foods that have prebiotics and probiotic nutrients that can reduce the reactions. Some products can help support the immune system and can offer nutrients to the gastrointestinal tract and metabolic support.
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues as well as functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or chronic disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
References:
Brosseau, Carole, et al. �Prebiotics: Mechanisms and Preventive Effects in Allergy.� Nutrients, MDPI, 8 Aug. 2019, www.ncbi.nlm.nih.gov/pubmed/31398959.
Kerr, Michael. �Seasonal Allergies: Symptoms, Causes, and Treatment.� Healthline, 7 May, 2018, www.healthline.com/health/allergies/seasonal-allergies.
Molinari, Giuliano, et al. �Respiratory Allergies: a General Overview of Remedies, Delivery Systems, and the Need to Progress.� ISRN Allergy, Hindawi Publishing Corporation, 12 Mar. 2014, www.ncbi.nlm.nih.gov/pmc/articles/PMC3972928/.
Newman, Tim. �Food Allergies: Symptoms, Treatments, and Causes.� Medical News Today, MediLexicon International, 17 July 2017, www.medicalnewstoday.com/articles/14384.php.
Team, DFH. �Attack Allergies with Prebiotics.� Designs for health, 24 Oct. 2019, blog.designsforhealth.com/node/1133.
Let’s be honest, making a change to your lifestyle is hard. Whether that is due to lack of time, motivation, or not knowing where to begin, there is one thing that makes it easier: accountability. This is where health coaching comes into play. Going through the process with someone and having another individual to talk about it with,� makes the change seem more achievable. The bottom line is that people need support. When it comes to changing one’s lifestyle and adapting new healthy behaviors, individuals who have support are more successful.
What Is A Health Coach?�
A health coach can be defined by The Institute for Integrative Nutrition as, ” a wellness authority and supportive mentor who motivates individuals to cultivate positive health choices. Health coaches educate and support clients to achieve their health goals through lifestyle and behavior adjustments.�
Health coaches are becoming more and more essential as modern medicine continues to improve. Now more than ever, the medical field is advancing at high rate speeds and practitioners do not always have the available time some patients need. Here is where health coaches come into play. Essentially, the position of a health coach was created to fill the void in many doctor offices.� Many doctors contribute but do not have the time or resources to help each patient build healthy habits on a day to day basis. However, health coaches are available to be a supportive mentor who help and guide patients in making healthy lifestyle changes.
What Does A Health Coach Do?�
Health coaches play a vital role in modern medicine. Health coaches can work in multiple settings including for a doctor, a spa, a gym, wellness centers, or even have their own private practice. Health coaches help individuals make lasting changes and keep patients on track to feel their best. In addition to this, health coaches motivate, push, encourage, and create plans with patients to optimize energy and decrease stress and fatigue.
Health coaches are not just for diet and exercise help, but for other aspects of life as well. Health coaches are able to help with stress, sleep, relationships, habits, and even one’s career.
Health coaches work with individuals to go through the problem areas in their life and give them tools to improve their lifestyles. By working with a health coach, the individual begins to learn and create habits that will affect and improve their lives while also giving them the essential life skills they can use for a lifetime.� One of the main things that coaches do is aid patients in setting goals. For many, goals are set but are not attainable, healthy, nor realistic. Health coaches work to break down these goals with patients into smaller, more reachable goals. This helps patients push themselves and not get discouraged because they are hitting these smaller marks along the way.
Aside from setting goals, health coaches also prepare the patient for the emotional fallout that can occur. As mentioned earlier, lifestyle changes are not easy and do not occur overnight. This being said, it is normal to have negative emotions regarding the subject along the way. Health coaches are prepared for this and will help you to not only work through them but learn to adapt to these situations and how to overcome the barriers.
How Can You Benefit?�
In the United States, over half of the adult population is affected by at least one chronic disease, many having to do with joint inflammation (Pecoraro, 2019).� Integrative health coaching allows patients to visualize their goals and work with their health coach to properly identify their values and create action steps to achieve optimal health and wellbeing.
People can utilize health coaches at any moment in time. However, many people choose to have a health coach help them after they receive a diagnosis or are overall unhappy in their health and lifestyle choices.
Health coaches are respectful of the personal knowledge one has of their own life and body. Thus, letting the patient have a say in their plan and protocol. This is beneficial because if a patient is included in the creation of their health plan, they are more likely to comply and make it attainable. Not only does this build trust in the professional relationship, but it allows a health coach to consider all areas in the patient’s life.
Individuals can benefit by learning to lessen health issues, problem solve, and gain a new perspective on their life.
A health coach can do a lot more than just aid in diet and exercise. As one can see, health coaches are helpful in many different aspects of one’s life. The qualifications for a health coach can vary. Personally, I have a bachelors degree in Exercise Science with an emphasis in Health Education from Grand Canyon University. In addition to this, I gained my Exercise Physiologist Certification through the American College of Sports Medicine (ACSM). With this background, I am knowledgeable in the pillars of health and how to successfully guide an individual. Almost every person can benefit from a health coach in at least one way. – Kenna Vaughn, Senior Health Coach
The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or chronic disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
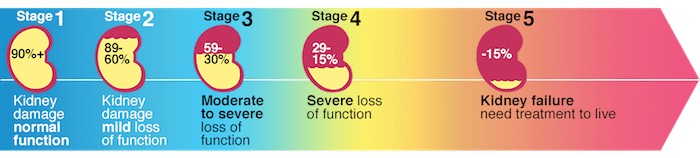
If you are experiencing any of these situations, then you might be experiencing chronic kidney disease.
About over 10% of the adult population suffers from CKD (chronic kidney disease), and the two leading underlying causes of the end-stage of chronic kidney disease are type 2 diabetes and hypertension. Other chronic ailments like dysbiosis of the gut microbiome, inflammation, oxidative stress, as well as environmental toxins and PPI (proton pump inhibitor). All these chronic ailments have been linked to chronic kidney disease in the body.
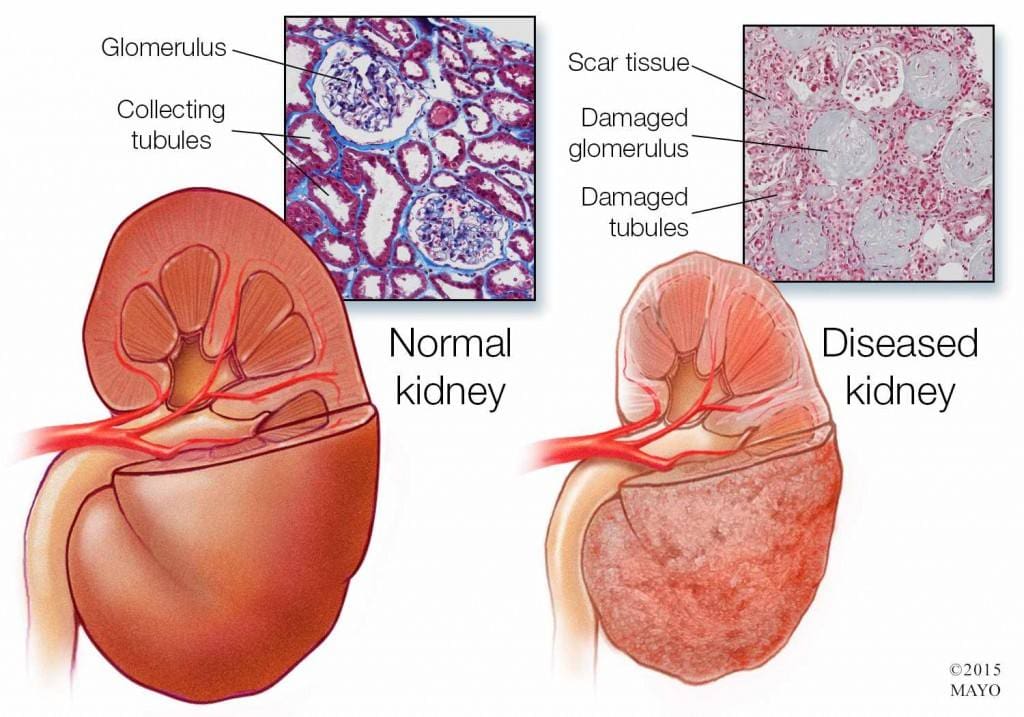
Chronic Kidney Disease
Chronic kidney disease is a slow and progressive loss of kidney function over several years. Also known as chronic renal failure, it much more widespread, and it often goes undetected and undiagnosed until the disease is well advanced. It is not unusual for anyone to realize they have chronic kidney failure when their kidneys are functioning only at 25% than average. As it advances and the kidney’s function is severely impaired, dangerous levels of waste and fluid can rapidly build up in the body.
Chronic kidney failure is different from acute kidney failure due to being a slow and gradually progressive disease. When the disease is fairly well advanced, the conditions are more severe than the signs and symptoms are noticeable, making most of the damage irreversible. Here are some of the most common signs and symptoms of chronic kidney disease include:
Anemia
Blood in urine
Dark urine
Edema- swollen feet, hands, ankles, and face
Fatigue
Hypertension
More frequent urination, especially at night
Muscle cramps and twitches
Pain on the side or mid to lower back
Dietary Fibers for CKD
Researchers have investigated that the role of dietary fibers and the gut microbiome is in renal diets. When there is a dysbiosis in the gut microbiome, it can be a risk factor for the development of chronic kidney disease, thus reducing the renal function. That function will significantly contribute to dysbiosis. The current renal dietary recommendations include a reduction of protein intake with an increase in complex carbohydrates and fiber.
A systemic review did a test that included 14 controlled trials and 143 participants that had chronic kidney disease. The test demonstrated that all 143 participants had a reduction in serum creatinine and urea that is associated with dietary fiber intake, which occurs in a dose-dependent matter. These participants had an average intake of 27 grams of fiber per day in their diet. It is also an essential note that creatinine is metabolized in the intestinal bacteria in the body.
A high fiber diet can lead to the production of SCFAs (short-chain fatty acids) in the gastrointestinal tract. They play an essential role in T regulatory cell activation, which regulates the intestinal immune system. When there is dysregulation in the immune system, it can cause an increase of inflammation that may occur in chronic kidney disease. With a high fiber diet, the intake is associated with lowering the risk of inflammation and the mortality in kidney disease.
Increasing fiber intake is relatively easy with some of these high fiber foods that are both healthy and nutritious and can help individual’s that have kidney disease. These include:
Pears
Strawberries
Avocados
Apples
Carrots
Beets
Broccoli
Lentils
Research has previously demonstrated that a high fiber diet for CDK patients is characterized by the control increase of plant-origin protein and animal-origin foods. This is useful for individuals to limit the consumption of processed food products because of modern conservation processes, which has the purpose of eliminating pathogenic bacteria. People who have chronic kidney disease that go on a high fiber diet have been linked to better kidney function and lowering the risk of inflammation and mortality.
Some individuals may experience some gastrointestinal side effects when they are trying to increase their fiber intake.�Research has been stated that patients should consider resistant starches since it has shown no side effects with the recommended doses.
Conclusion
Chronic kidney disease is a slow and progressive loss of kidney function. The signs and symptoms are noticeable as the disease progress in the later stages. With a high fiber diet, individuals can lower the risk of inflammation and mortality of CDK. When this disease causes inflammation and chronic illness in the kidneys, complications can travel through the entire body. The high fiber diet can also be beneficial for the gut microbiome to function correctly, and some products can help lower the stress hormones and make sure that the body’s hypothalamic-pituitary-adrenal axis is functioning correctly.
October is Chiropractic Health Month. To learn more about it, check out Governor Abbott�s bill on our website to get full details on this historic moment.
The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or chronic disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
References:
D�Alessandro, Claudia. �Dietary Fiber and Gut Microbiota in Renal Diets.� MDPI, Multidisciplinary Digital Publishing Institute, 9 Sept. 2019, www.mdpi.com/2072-6643/11/9/2149/htm.
Gunnars, Kris. �22 High-Fiber Foods You Should Eat.� Healthline, 10 Aug. 2018, www.healthline.com/nutrition/22-high-fiber-foods.
Jurgelewicz, Michael. �New Article Investigates the Role of Dietary Fiber and the Gut Microbiome in Chronic Kidney Disease.� Designs for Health, 13 Sept. 2019, blog.designsforhealth.com/node/1105.
Khosroshahi, H T, et al. �Effects of Fermentable High Fiber Diet Supplementation on Gut Derived and Conventional Nitrogenous Product in Patients on Maintenance Hemodialysis: a Randomized Controlled Trial.� Nutrition & Metabolism., U.S. National Library of Medicine, 12 Mar. 2019, www.ncbi.nlm.nih.gov/pubmed/?term=30911321.
Krishnamurthy, Vidya M Raj, et al. �High Dietary Fiber Intake Is Associated with Decreased Inflammation and All-Cause Mortality in Patients with Chronic Kidney Disease.� Kidney International, U.S. National Library of Medicine, Feb. 2012, www.ncbi.nlm.nih.gov/pmc/articles/PMC4704855/.
Newman, Tim. �Chronic Kidney Disease: Symptoms, Causes, and Treatment.� Medical News Today, MediLexicon International, 13 Dec. 2017, www.medicalnewstoday.com/articles/172179.php.
Staff, Mayo Clinic. �Chronic Kidney Disease.� Mayo Clinic, Mayo Foundation for Medical Education and Research, 15 Aug. 2019, www.mayoclinic.org/diseases-conditions/chronic-kidney-disease/symptoms-causes/syc-20354521.
If you are experiencing any of these situations, then you might be experiencing a low intake of fiber in your diet, causing inflammation.
Throughout several decades, Americans have lost much diversity in their diets, impacting their gut microbiome, and the contribution to the autoimmune disorder epidemic. The vast majority of people have a less than perfect diet that is consists of high in calories, short on nutrients, and low on fiber intake. Research has stated that about only 10 percent of Americans have met their daily fiber requirements.
The diet is a significant environmental trigger in autoimmune diseases. Dietary approaches can provide the most effective means of an individual to returning balance and the dysfunction with the gastrointestinal system. Researchers have found out that the role of dietary fibers can help with rheumatoid arthritis as there is new and developing research on this discovery.
What is Rheumatoid Arthritis?
Rheumatoid arthritis is a long term, progressive, and disabling autoimmune disease. It causes inflammation, swelling, and pain in and around the joints and organs of the body. It affects up to 1 percent of the world’s population and over 1.3 million people in America, according to the Rheumatoid Arthritis Support Network.
Rheumatoid arthritis is also a systemic disease, which means that it affects the whole body, not just the joints. It occurs when an individual’s immune system mistakes their body’s healthy tissues for foreign invaders. As the immune system responds to this, inflammation occurs in the target tissue or organ. Symptoms of rheumatoid arthritis can include:
Pain, swelling, and stiffness in more than one joint
Symmetrical joint involvement
Joint deformity
Unsteadiness when walking
Fever
A general feeling of being unwell
Loss of function and mobility
Weight loss
Weakness
Fiber and Inflammation
Individuals who eat healthily knows that eating fibers in their diet can help reduce the risk of developing various conditions. The AHAEP (American Heart Association Eating Plan) has stated that people should be eating a variety of food fiber sources in their diet. The total dietary fiber intake that a person should be eating is 25 to 30 grams a day from foods, not supplements. Currently, adults in the United States eat about 15 grams a day on their fiber, which is half of the recommended amount.
Eating a high fiber diet can provide many rewards to the body. Eating fruits, vegetables, beans, nuts, and whole grains can provide a boost of vitamins, minerals, protein, and healthy nutrients in the body. Studies have been shown that eating a high fiber diet can help lower the markers of inflammation, which is a critical factor in many forms of arthritis.
The body needs two types of fibers, which are soluble and insoluble. Soluble fibers are mixed with water to form a gel-like consistency, which slows digestion and helps the body absorb nutrients better and helps lower total cholesterol and LDL cholesterol. Insoluble fibers help the digestive system run more efficiently as it adds bulk to stool, which can help prevent constipation.
There have been a few studies that found that people who eat high fiber diets have lower CRP (C-reactive protein) levels in their blood. CRP is a marker for inflammation and is linked to rheumatoid arthritis. When a person eats a high fiber diet, it not only reduces inflammation to their bodies, but it helps lower the body weight as well. High fiber-rich foods feed the beneficial bacteria living in the gut, and then it is releasing substances to the body, promoting lower levels of inflammation.
A study has been shown that patients with rheumatoid arthritis that they consumed either a high fiber bar or cereal for 28 days while continuing with their current medication had decreased levels of inflammation. Researchers noticed that they had an increase of T regulatory cell numbers, a positive Th1/Th17 ratio, a decrease in bone erosion, and a healthy gut microbiome.
Gut Health and Inflammation
The gut plays a crucial role in the immune function as well as digesting and absorbing food in the body. The intestinal barrier provides an effective protective barrier from pathogenic bacteria but also being a healthy environment for beneficial bacteria. With a high fiber diet, it can lead to the production of SCFAs (short-chain fatty acids) in the gastrointestinal tract, thus playing an essential role in T regulatory cell activation, which regulates the intestinal immune system. When inflammation comes to play in the gut, it can disrupt the intestinal permeability barrier and cause a disruption, leading to leaky gut. Probiotics and a high fiber diet can help prevent inflammation and provide a healthy gut function.
Conclusion
Eating a high fiber diet is essential to prevent inflammation, not on the joints, but everywhere in the body. Even though individuals eat half of the recommended amount of fiber in their diets, due to their hectic lifestyle, eating a high fiber diet is beneficial. Incorporating fiber in their diet gradually is ideal as well as drinking water with the fibers to make the process work more effectively in the body. Some products can help aid the body by supporting not only the gastrointestinal function and muscular system but making sure that the skin, hair, nail, and joints are healthy as well.
October is Chiropractic Health Month. To learn more about it, check out Governor Abbott�s declaration on our website to get full details on this historic moment.
The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or chronic disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
References:
at UCSF Medical Center, Healthcare Specialist. �Increasing Fiber Intake.� UCSF Medical Center, 2018, www.ucsfhealth.org/education/increasing_fiber_intake/.
Brazier, Yvette. �Rheumatoid Arthritis (RA): Symptoms, Causes, and Complications.� Medical News Today, MediLexicon International, 16 Oct. 2018, www.medicalnewstoday.com/articles/323361.php.
Hakansson, Asa, and Goran Molin. �Gut Microbiota and Inflammation.� Nutrients, MDPI, June 2011, www.ncbi.nlm.nih.gov/pmc/articles/PMC3257638/.
Jurgelewicz, Michael. �New Study Demonstrates the Role of Fiber in Rheumatoid Arthritis.� Designs for Health, 11 Oct. 2019, blog.designsforhealth.com/node/1125.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine