Embrace tofu in your meals for a healthy alternative. Discover its uses and benefits in a balanced diet today.
Introduction
When it comes to improving one’s health and well-being, consuming the correct quantity of nutrient-dense meals not only feeds the body but also gives the musculoskeletal, cardiovascular, and gastrointestinal systems, to mention a few, more nutrients. Minor dietary adjustments may reduce the overlapping risk profiles that environmental variables might produce, which can result in discomfort and agony. Small dietary adjustments may also increase protein intake to support musculoskeletal development and lessen the body’s cardiovascular problems. Tofu is among the most nutrient-dense and adaptable proteins. Today’s article will cover several forms of tofu, their nutritional content, cardiovascular health benefits, and how to include them in a balanced diet.
What Is Tofu?
Made from a soybean slurry and pressed into a solid block, tofu or bean curd is a century-old food from China that has become a staple in East Asia. This versatile food has become a staple source of protein that is becoming more popular globally due to its cooking adaptability and impressive nutritional profile. Tofu comes from soybean seeds as it is bioactive, consisting of soaking, draining, and grinding to a gelatinous block filled with abundant beneficial lipids. Bioactive compounds become a great source of plant-based protein for many individuals. (Dang et al., 2023)
Nutritional Value of Tofu
Since tofu is a great meat alternative for those seeking a plant-based or low-saturated-fat diet as a typical 0.25 block of firm tofu with a serving of 116 grams provides:
Protein: 9g
Calories: 88
Fat: 6g
Saturated Fat: 0.8g
Carbohydrates: 2.2g
Dietary Fibers: 0.3g
Sodium: 8g
Potassium: 140mg
Iron: 34% DV (Daily Value)
Calcium: 40% DV (Daily Value)
Magnesium: 8% DV (Daily Value)
Vitamin B6: 5% DV (Daily Value)
Additionally, the soybean from which tofu is made is a legume that contains no cholesterol, is low in saturated fats, and contains all eight essential amino acids (Montgomery, 2003), making it very appealing to cardiovascular patients.
The Healing Diet: Combat Inflammation & Embrace Wellness- Video
Tofu & Cardiovascular Health
Many do not realize that tofu will benefit cardiovascular health when incorporated into their protein intake. By incorporating tofu into a cardiovascular diet, many will notice lower LDL (low-density lipoprotein) cholesterol. This is due to the hypocholesterolemic effects of the soy protein in tofu. (Messina, 2016) Additionally, tofu has isoflavones that can promote cell proliferation in the body while acting as an antioxidant that can exert anti-inflammatory properties. (Rizzo et al., 2023) Some of the potential benefits of incorporating tofu to support cardiovascular health include:
Rich with healthy heart fats
Reduce cholesterol
Provides support to blood pressure
Weight management
Additionally, with its associated phytochemicals, tofu can help improve lipid profiles when people substitute animal protein with soy to reduce cardiovascular diseases like coronary heart disease and control blood cholesterol levels. (Erdman, 2000)
Types of Tofu
Now, for individuals trying to figure out how to incorporate tofu into various cooking methods and different recipes since it comes in a variety of textures:
Silken Tofu: Silken tofu has a soft and creamy texture, ideal for smoothies, dressings, or desserts.
Soft Tofu: Soft tofu is slightly firmer than silken and similar to Jello. It works well in soups or scrambles.
Firm Tofu: Firm tofu holds its shape well; perfect for stir-fries, grilling, or baking.
Extra-Firm Tofu: Extra-firm tofu is dense and chewy, perfect for recipes that require a desired meatier texture, and best for frying.
Fermented Tofu: Fermented tofu is a preserved, tangy tofu used as a condiment or flavor enhancer in food dishes.
Is Tofu A Good Protein Source?
Tofu can be an excellent alternative to animal protein for vegans or vegetarians looking to reduce their meat intake. Many individuals can incorporate tofu as part of their diet for protein intake to maintain muscle strength and repair due to its essential amino acids that the body needs to function throughout the day.
Adding Tofu Into A Diet?
Tofu is incredibly adaptable as part of a person’s diet as it can absorb the flavors of the ingredients it’s cooked with. Tofu can be boiled, fried, or steamed into healthy dishes while allowing the individual to think more about their nutrition and encouraging them to consider the changes to incorporate in their food habits. (Eze et al., 2018)
Final Thoughts
More than simply an animal protein alternative, tofu is a heart-smart, nutrient-dense meal that can be included into a variety of diets and promote cardiovascular health. Tofu may be included into meals for many individuals who are thinking about increasing their protein intake. This might be their answer to eating healthily and leading a healthier life because of its isoflavones, vital amino acids, and cardiovascular health support.
Injury Medical & Functional Medicine Clinic
We associate with certified medical providers who understand the importance of assessing individuals dealing with cardiovascular issues and are looking for natural alternatives to incorporate plant-based foods into a healthy diet. When asking important questions to our associated medical providers, we advise patients to incorporate tofu into their diet to reduce the effects of cardiovascular disorders related to the body. Dr. Alex Jimenez, D.C., uses this information as an academic service. Disclaimer.
References
Dang, Y., Ren, J., Guo, Y., Yang, Q., Liang, J., Li, R., Zhang, R., Yang, P., Gao, X., & Du, S. K. (2023). Structural, functional properties of protein and characteristics of tofu from small-seeded soybeans grown in the Loess Plateau of China. Food Chem X, 18, 100689. https://doi.org/10.1016/j.fochx.2023.100689
Erdman, J. W., Jr. (2000). AHA Science Advisory: Soy protein and cardiovascular disease: A statement for healthcare professionals from the Nutrition Committee of the AHA. Circulation, 102(20), 2555-2559. https://doi.org/10.1161/01.cir.102.20.2555
Eze, N. M., Okwume, U. G., Eseadi, C., Udenta, E. A., Onyeke, N. G., Ugwu, E. N., Akubue, B. N., Njoku, H. A., & Ezeanwu, A. B. (2018). Acceptability and consumption of tofu as a meat alternative among secondary school boarders in Enugu State, Nigeria: Implications for nutritional counseling and education. Medicine (Baltimore), 97(45), e13155. https://doi.org/10.1097/MD.0000000000013155
Messina, M. (2016). Soy and Health Update: Evaluation of the Clinical and Epidemiologic Literature. Nutrients, 8(12). https://doi.org/10.3390/nu8120754
Rizzo, J., Min, M., Adnan, S., Afzal, N., Maloh, J., Chambers, C. J., Fam, V., & Sivamani, R. K. (2023). Soy Protein Containing Isoflavones Improves Facial Signs of Photoaging and Skin Hydration in Postmenopausal Women: Results of a Prospective Randomized Double-Blind Controlled Trial. Nutrients, 15(19). https://doi.org/10.3390/nu15194113
Learn about gua-sha combined with chiropractic care and how it can improve your well-being through ancient healing techniques.
Introduction
When it comes to many individuals dealing with musculoskeletal pain, it can be due to many environmental factors that can affect the body. Excessive movement can affect different body areas, from overly stressful days to injuries. Some of the more common musculoskeletal issues are neck, shoulder, and back pain. These muscle issues can cause referred pain to the upper and lower extremities while causing the affected muscles to become tight and stiff. When individuals are experiencing musculoskeletal pain, many can incorporate non-surgical treatments to not only relax the body but also reduce the overlapping symptoms of musculoskeletal pain affecting the muscles. One of the most underutilized and effective tools that can help relax the affected muscles is Gua Sha therapy.
What is Gua-Sha?
Gua Sha is a traditional healing technique incorporating a smooth-edged tool made from either jade, rose quartz, or metal to scrape the skin gently. This technique has been used regularly in China and Southeast Asia and has therapeutic properties to restore the body’s chi or energy. “Gua Sha” means scraping stagnant blood to increase circulation beneath the skin. Thus enhancing the immune surveillance function of the affected muscle. (Chu et al., 2021) GuaSha therapy can be a powerful therapeutic tool for reducing inflammation in soft tissues, improving mobility within the extremities, and relieving muscle pain.
How Gua-Sha Helps With Musculoskeletal Pain
Now, when it comes to individuals dealing with musculoskeletal pain, it is often associated with overuse, repetitive movements, injuries, poor posture, or chronic conditions. When these environmental factors start to cause musculoskeletal pain, it can affect different body areas, especially the neck, shoulders, and back. These common areas of musculoskeletal pain can cause localized or referred pain that causes the muscles, fascia, and ligaments to be pain generators due to overuse, leading to myofascial pain and muscle trigger points. (Knezevic et al., 2021) Gua Sha therapy can address these root musculoskeletal causes by:
Breaking up fascia adhesions and scar tissue within the soft tissues
Gua Sha can reduce inflammation in the affected area by improving muscle microcirculation.
Help stimulate the parasympathetic nervous system, providing pain relief
Releasing muscle tension and myofascial trigger points in the upper and lower extremities
Helps to enhance lymphatic drainage, thus reducing swelling and stagnation
In short, Gua Sha can help remove du meridian obstructions, replenish the body’s energy, remove blood stasis, and promote blood circulation for natural healing. (Wang et al., 2020)
Discovering the Benefits of Chiropractic Care- Video
Gua-Sha & Chiropractic Care: A Powerful Combination
When individuals are experiencing musculoskeletal issues within their upper and lower extremities correlated with environmental factors, many will often seek non-surgical treatment for their pain. Some non-surgical treatments, like chiropractic care, can benefit the musculoskeletal system. Chiropractic care emphasizes diagnosing and managing musculoskeletal disorders that use mechanical and manual spinal manipulation. (Trager et al., 2024) Combined with Gua Sha, it can be more effective in promoting healing properties since chiropractic care helps restore joint mobility and realign the spine. Gua-Sha helps break down or scrape the surrounding tissues. For chiropractors, incorporating the Graston technique (another form of Gua Sha) utilizes specialized instruments to modify the affected body area structure and composition of soft tissue. This then enhances fascia mobility while addressing tissue adhesions. (Deshmukh & Phansopkar, 2023)
The Benefits of Chiropractic Care & Gua-Sha
Chiropractic adjustments assist people in maintaining healthy musculoskeletal alignment, significantly reducing discomfort in the muscles, joints, bones, and connective tissues. (Chu et al., 2023) The following are some advantages of using gua sha either by itself or in conjunction with chiropractic care:
Relief from shoulder, back, and neck discomfort
Increase the flexibility and range of motion of your muscles.
Reduced inflammation in the afflicted muscle
Speeds up the body’s recuperation process
As part of an individual’s personalized treatment strategy, Gua-Sha and chiropractic adjustments may assist in addressing the underlying problems that impact the whole kinetic body chain. Gua Sha may be used either before to or after a chiropractic adjustment to help restore tissue flow and function, lessen guarding, promote mobility, and boost the procedure’s efficacy. This, in turn, supports both functional musculoskeletal mobility and long-term repair.
Common Gua-Sha Uses In Musculoskeletal Care
A mild, non-invasive treatment that can be tailored to each person’s tolerance and healing requirements, gua sha therapy is useful for several ailments. This comprises:
Persistent lower back or neck discomfort
Syndrome of Myofascial Pain
Carpal tunnel syndrome
Tendonitis (e.g., Achilles, tennis elbow)
Fascia plantar
Scarring or stiffness after surgery
The malfunctioning of the TMJ and tension headaches
Although Gua Sha treatment has several positive benefits for the musculoskeletal system, not everyone who has particular vascular or skin issues or who bleeds readily should use it. People must speak with their affiliated healthcare professionals to explore a suitable, individualized treatment plan for certain illnesses.
Conclusion
People seeking a natural, non-pharmacological remedy for environmental-induced musculoskeletal discomfort may use Gua Sha in their personalized chiropractic therapy regimen. By promoting soft tissue health and ensuring adequate spinal alignment, this combination may lessen the likelihood that musculoskeletal issues will recur. People who begin to consider their health and well-being will have a whole team to support them on their path to wellness and help them become pain-free with chiropractic adjustments and Gua Sha treatment.
Injury Medical & Functional Medicine Clinic
We associate with certified medical providers who understand the importance of assessing individuals dealing with musculoskeletal pain by incorporating Gua-Sha and chiropractic care. When asking important questions to our associated medical providers, we advise patients to utilize Gua-Sha combined with chiropractic care to reduce musculoskeletal pain and restore soft tissue mobility in the extremities. Dr. Alex Jimenez, D.C., uses this information as an academic service. Disclaimer.
References
Chu, E. C., Lin, A. F. C., & Chu, V. (2023). The Inclusion of Chiropractic Care in the Healthy China Initiative 2030. Cureus, 15(8), e43068. https://doi.org/10.7759/cureus.43068
Chu, E. C. P., Wong, A. Y. L., Sim, P., & Kruger, F. (2021). Exploring scraping therapy: Contemporary views on an ancient healing – A review. J Family Med Prim Care, 10(8), 2757-2762. https://doi.org/10.4103/jfmpc.jfmpc_360_21
Deshmukh, N. S., Jr., & Phansopkar, P. (2023). Effect of the Graston Technique and Cupping Therapy on Pain and Functions in Individuals With Medial Tibial Stress Syndrome: A Randomized Clinical Trial. Cureus, 15(11), e48246. https://doi.org/10.7759/cureus.48246
Knezevic, N. N., Candido, K. D., Vlaeyen, J. W. S., Van Zundert, J., & Cohen, S. P. (2021). Low back pain. The Lancet, 398(10294), 78-92. https://doi.org/10.1016/s0140-6736(21)00733-9
Trager, R. J., Bejarano, G., Perfecto, R. T., Blackwood, E. R., & Goertz, C. M. (2024). Chiropractic and Spinal Manipulation: A Review of Research Trends, Evidence Gaps, and Guideline Recommendations. J Clin Med, 13(19). https://doi.org/10.3390/jcm13195668
Wang, Y. W., Xi, Z. W., Pu, B., Chen, G. Y., Ma, Y. F., Liu, D. L., & Xu, X. (2020). Gua sha therapy for chronic low back pain: A protocol for systematic review. Medicine (Baltimore), 99(40), e20606. https://doi.org/10.1097/MD.0000000000020606
Enzymes’ function is to help trigger bodily processes ranging from digestion to blood clotting to growth. What is the best way to support enzyme production?
Enzymes
Enzymes are proteins that act as biological catalysts. They cause and speed up crucial chemical reactions and help the body complete necessary chemical reactions. They are vital for many biological processes, including digestion, metabolism, and molecule building and breaking down. This includes breaking down food, facilitating growth, and forming blood clots. Too little of a certain type can lead to serious health implications like a fatal buildup of toxins. Individuals missing a certain kind of enzyme or having too little of it can develop serious health conditions.
Function
They help speed up chemical reactions in the body (National Human Genome Research Institute, 2025). They facilitate chemical reactions in everything from digesting food to muscle growth. Enzymes facilitate this by binding to a cell, creating the reactions needed. With enzyme binding, chemical reactions can occur without destroying the cell. (Nemours KidsHealth, 2023) Each cell in the body has thousands of enzymes to help facilitate all the complex reactions to maintain health. (National Human Genome Research Institute, 2025)
Factors Affecting Production
In healthy individuals, the body produces the enzymes it needs. However, metabolic disorders can occur if the body does not produce enough of a certain type. (Kennedy Krieger Institute, 2025) These disorders can be serious and are usually caused by a genetic malfunction that impacts production.
Types
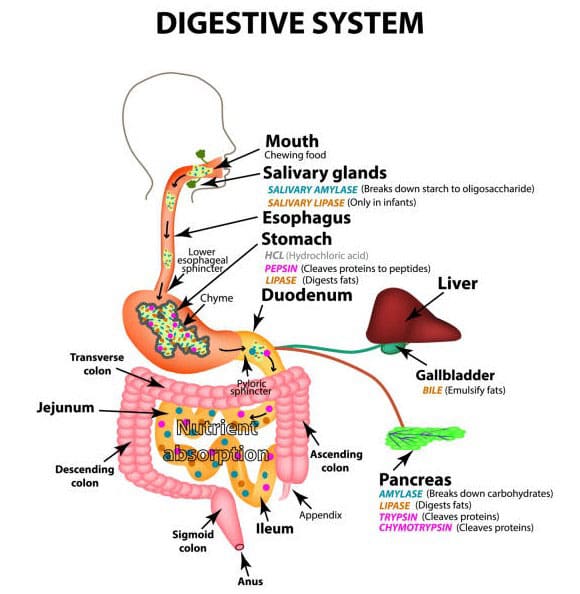
There are thousands of different types. Digestive enzymes, for example, aid in the breakdown of food and convert it into energy. Common enzymes that are critical for health include (Nemours KidsHealth, 2023)
Amylase
Digestive helps break down starches.
Aspartate aminotransaminase (AST) and Alanine Aminotransaminase (ALT)
Help the liver convert sugar into energy.
Creatine Kinase (CK)
Helps muscles create energy.
DNA Polymerase
Facilitates growth by allowing DNA to duplicate.
Glucose-6-Phosphate Dehydrogenase
Keeps red blood cells healthy by preventing damage to the cell.
Lipase
A digestive enzyme that helps break down fats and oils.
Protease
Digestive helps break down proteins.
Thrombin
Causes blood to clot.
Deficiencies
If the body doesn’t make enough of a certain enzyme, it cannot undergo the bodily processes that the enzyme helps facilitate. This can lead to a variety of symptoms. Some are minor, like not being able to eat lactose. Others are serious, like developmental delays caused by the build-up of toxins. (Kennedy Krieger Institute, 2025) Usually, these deficiencies are caused by genetics.
Types
There are various deficiencies. Some are very rare, while others can lead to conditions such as: (Nemours KidsHealth, 2023)
Lactose Intolerance
This is caused by not having enough of the enzyme that breaks down lactose, a sugar found in milk, leading to gas and bloating.
Tay-Sachs Disease
An often fatal disease caused by a missing hexosaminidase, which is responsible for breaking down fats
Gilbert’s Syndrome
This is caused by a missing enzyme that removes waste product (bilirubin) from the blood, leading to bilirubin buildup and
Jaundice or yellowing of the skin and whites of the eyes
Galactosemia
This leads to slow growth and trouble gaining weight, which is caused by the missing galactose-1-phosphate uridylyltransferase (GALT), which helps break down a sugar called galactose.
Phenylketonuria (PKU)
This is caused by having too little phenylalanine hydroxylase, which breaks down a protein called phenylalanine, causing brain damage.
Morquio Syndrome
This is caused by having too few enzymes that break down glycosaminoglycans, a type of sugar molecule.
This leads to bone and growth abnormalities.
Wilson’s Disease
A liver disease is caused by a missing protein that helps break down copper in the body.
Enzyme Production Support
Eat a healthy, well-balanced diet of fruits and vegetables to support enzyme production. Avoid processed foods, especially those that are very fatty (Johns Hopkins Medicine, 2025). The body produces all the necessary enzymes unless the individual has a genetic condition. Supplements aren’t usually required, but they can help with lactose intolerance or digestion in cystic fibrosis patients. (Nemours KidsHealth, 2023)
One supplement type, pancreatic enzyme replacement therapy (PERT), is available. PERT is an FDA-regulated prescription medication prescribed to patients with serious illnesses such as cystic fibrosis. (U.S. Food and Drug Administration, 2019)
Injury Medical Chiropractic & Functional Medicine Clinic
Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, and prevent injury. Regarding musculoskeletal pain, specialists like chiropractors, acupuncturists, and massage therapists can help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal issues.
Chiropractic Care and Metabolism: The Hidden Link
References
National Human Genome Research Institute. (2025). Enzyme. Retrieved from https://www.genome.gov/genetics-glossary/Enzyme
U.S. Food and Drug Administration. (2019). FDA approves new breakthrough therapy for cystic fibrosis. Retrieved from https://www.fda.gov/news-events/press-announcements/fda-approves-new-breakthrough-therapy-cystic-fibrosis
For individuals struggling with constipation, a common digestive issue, could performing abdominal self-massage help bring relief?
Abdominal Self Massage
Constipation refers to having a bowel movement fewer than three times per week. In addition to stress, certain lifestyle issues can lead to constipation, including not getting enough fiber, exercise, and proper hydration. Many also experience constipation while traveling. Abdominal self-massage involves gently massaging the stomach with your hands, either in a circular motion or with strokes, to improve digestion, relieve constipation, and reduce bloating. Performing self-massage on and around the abdomen can help ease constipation in several ways, such as stimulating the muscles, producing bowel movements, and soothing chronic stress. (Sinclair M. 2011)
Massage and Constipation
Abdominal massage can provide several benefits, including:
Stimulates and Improves Digestion
Massage stimulates the muscles and nerves that control digestion, promoting bowel movements and reducing constipation.
Reduces Bloating
Massaging the abdomen may help to reduce bloating and gas by gently moving fluids and gases through the digestive system.
In addition, it can help soften stool, speed up the movement of stool through the gut, and reduce the need to use laxatives. (University of Michigan Medicine, 2021)
Relieves Constipation
Abdominal massage can help with constipation by encouraging bowel movements.
Reduces Pain and Discomfort
Some find that abdominal massage helps to reduce pain and discomfort related to digestive issues.
Massage can help relax tense abdominal muscles and reduce pain associated with conditions like irritable bowel syndrome (IBS).
Improved lymphatic drainage
Massage helps move lymphatic fluid, which carries waste products and toxins away from the abdominal area.
Research
Although massage isn’t a standard treatment for constipation, some research shows it may help restore regularity. A report reviewed several clinical trials focusing on abdominal massage and its use as a treatment for chronic constipation. The results showed that abdominal massage may provide relief by promoting peristalsis, a series of muscle contractions that help move food through the digestive tract. The report also found that massage may help lessen colonic transit time, which is when digested food passes through the colon or last segment of the digestive tract. The report determined that abdominal massage can help alleviate constipation-related pain and discomfort. (Sinclair M. 2011)
In clinical trials, individuals with constipation reported improved quality of life after abdominal self-massage. However, some research suggests that using abdominal massage for constipation relief will not decrease the use of laxatives, the most commonly used treatment. (Lämås K. et al., 2009)
How to Massage
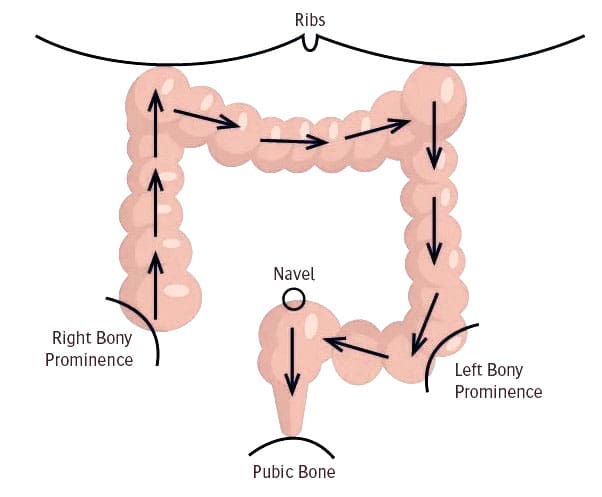
Various massage techniques may help relieve constipation and promote bowel movements. These are typically performed while lying down.
One technique involves placing the palm on the abdomen and making small, circular, clockwise motions around your belly button.
Individuals can also widen these circles so that the massage covers their entire abdomen.
Another technique begins by placing your hand below your breastbone, then gliding that hand down the length of your abdomen in one smooth stroke.
Repeat the movement with the other hand and continue this cycle for a few minutes.
When practicing self-massage, use light and gentle pressure, then gradually increase the pressure.
If you experience pain or tenderness, lighten up and return to a comfortable pressure level.
Try performing massage twice daily, aiming for a 20-minute session. Incorporating deep breathing into each session may also help. Before trying a massage or any home remedy, it is recommended to discuss it with a healthcare provider to see if it’s appropriate and safe. Pregnant women, for example, should avoid any massage on their abdomen. Constipation can sometimes signal an underlying condition that requires medical treatment, such as an underactive thyroid. Other symptoms like abdominal pain may be present, but sometimes constipation may be the only symptom.
Other Remedies
Self-massage alone is unlikely to treat chronic constipation; the goal should be to improve overall digestion to keep the organs functioning properly. To maintain regularity, it’s essential to drink plenty of water daily, eat enough fiber-rich foods, and engage in physical activity. Other alternative treatments include therapies like:
Acupressure
Biofeedback
Probiotics
Before trying self-massage, consult a medical caregiver to ensure it is safe and correct for the individual. Abdominal massage may not help with painful bloating caused by disease, infection, or other reasons.
Injury Medical Chiropractic & Functional Medicine Clinic
Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, and prevent injury. Regarding musculoskeletal pain, specialists like chiropractors, acupuncturists, and massage therapists can help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal issues.
Massage Therapy Rehabilitation
References
Sinclair M. (2011). The use of abdominal massage to treat chronic constipation. Journal of bodywork and movement therapies, 15(4), 436–445. https://doi.org/10.1016/j.jbmt.2010.07.007
University of Michigan Medicine. (2021). Self-abdominal massage. https://www.med.umich.edu/1libr/MBCP/AbdominalSelfmassage.pdf
Lämås, K., Lindholm, L., Stenlund, H., Engström, B., & Jacobsson, C. (2009). Effects of abdominal massage in management of constipation–a randomized controlled trial. International journal of nursing studies, 46(6), 759–767. https://doi.org/10.1016/j.ijnurstu.2009.01.007
Can incorporating nutritional yeast be an option for individuals seeking a healthy vegan and vegetarian cheese substitute?
Nutritional Yeast
Nutritional yeast is a deactivated form of Saccharomyces cerevisiae yeast, commonly known as baker’s or brewer’s yeast. It’s popular in vegan and vegetarian cooking for its savory, cheesy flavor and nutritional benefits. Nutritional yeast is harvested, rinsed, and heat-dried to deactivate it, removing its leavening properties. This means it doesn’t cause food to rise but adds flavor and vital nutrients.
Around 1.5 tablespoons contains 5 grams of carbohydrates, including 3 grams of fiber.
Yeast provides an especially beneficial form of soluble fiber known as beta-glucan, with unique health benefits. (Bashir K. M. I., & Choi J. S. 2017)
Fats
Most brands are naturally fat-free.
Protein
It provides all essential amino acids with 8 grams per 1.5 tablespoons.
Vitamins and Minerals
Most nutritional yeast products are fortified with added B vitamins. Most provide 600% or more B vitamins per 16 grams and 1,000% of the daily value for vitamin B12, depending on the brand. It also has:
Calcium
Thiamin
Iron
Potassium
Nutritional Yeast Health Benefits
Health benefits include:
Reduces Risk of Anemia
Iron is typically the first nutrient to come to mind. However, inadequate folate or vitamin B12 also causes anemia. A common treatment for a vitamin B12 deficiency is injections, but large doses consumed can also be effective. (National Institutes of Health, Office of Dietary Supplements, 2024) Individuals who follow a plant-based or vegan diet often have limited sources of vitamin B12. Most brands of nutritional yeast are fortified with B12, providing more than 500% of the daily value per serving. Because B12 is water-soluble, it won’t cause toxicity when consumed in high doses and can serve as a key source of this essential nutrient.
Supports Heart Health
Nutritional yeast contains beta-glucan, a carbohydrate found in the cell walls of plants, bacteria, and fungi. Higher intakes lead to favorable cardiovascular outcomes, including lowering bad cholesterol and increasing good cholesterol. (Bashir K. M. I., & Choi J. S. 2017) In addition, most brands contain potassium, which reduces blood pressure.
Promote Healthy Immune System Function
More research is needed, but several studies have shown how yeast-derived beta-glucan can strengthen the immune system. (Stier H., Ebbeskotte V., & Gruenwald J. 2014) These benefits are attributed to beta glucan’s bacterial fermentation in the intestines. Beta-glucan may also stimulate the activity of crucial immune system cells, like macrophages.
Prevents Constipation
Fiber is essential. The recommended fiber intake is at least 25 to 35 grams daily. Unfortunately, many do not get enough. Nutritional yeast contributes 3 grams of fiber per 16 grams. Fiber regulates bowel movements by pulling water into the colon and adding bulk and softness to stool. (University of Michigan, 2008)
Using nutritional yeast can help reach an adequate fiber intake.
Diabetes Management
Getting enough fiber helps prevent blood sugar fluctuations. Low-fiber diets have been shown to increase the risk of diabetes in various populations. (Harvard T.H. Chan, School of Public Health, 2022) Fiber slows digestion and increases satiety, controlling hunger and the glycemic response. Fiber is beneficial for preventing diabetes and helping those with diabetes maintain good numbers.
Allergies
Individuals who suspect a yeast or mold allergy see an allergist for a full evaluation.
Yeast overgrowth is another possible condition that is unrelated to yeast allergies.
Yeast overgrowth can occur in compromised immune systems or following antibiotic treatment.
Because yeast is present in many foods, anyone with a true yeast allergy may have to avoid several food items, including baked goods, fermented alcoholic beverages, marmite/vegemite, sourdough bread, and certain multivitamins. (Cunningham E. 2013)
Adverse Effects
Nutritional yeast is inactive and unlikely to cause negative effects. However, for individuals who suffer from irritable bowel syndrome (IBS) or migraines, yeast may be a trigger. (UMass Medical School Center for Applied Nutrition, 2020)
Check the label to see if the product is fortified with added vitamins and minerals or has added sodium.
Nutritional yeast is a dry food product available year-round in supermarkets or sold in a bulk food bin.
Storage, Safety, and Use
Although nutritional yeast is a dry product, it will stay in the refrigerator longer after it has been opened. Store it in an airtight container, and be mindful of the expiration date on the label.
It can be added to savory dishes such as pasta, roasted meats, vegetables, and salads. Ways to use include:
On scrambled eggs.
On top of garlic bread.
Popcorn seasoning.
Add to soups.
In pasta dishes, as a substitute for parmesan cheese.
An alternative to cheese sauce.
Injury Medical Chiropractic and Functional Medicine Clinic
Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop highly effective treatment plans through an integrated approach for each patient and restore health and function to the body through nutrition and wellness, functional medicine, acupuncture, Electroacupuncture, and integrated medicine protocols. We focus on what works for you to relieve pain, restore function, prevent injury, and mitigate issues through adjustments that help the body realign itself. The clinic can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal problems.
Learning About Food Substitutions
References
U.S. Department of Agriculture. FoodData Central. (2019). Nutritional yeast. Retrieved from https://fdc.nal.usda.gov/food-details/1744022/nutrients
Bashir, K. M. I., & Choi, J. S. (2017). Clinical and Physiological Perspectives of β-Glucans: The Past, Present, and Future. International journal of molecular sciences, 18(9), 1906. https://doi.org/10.3390/ijms18091906
National Institutes of Health, Office of Dietary Supplements. (2024). Vitamin B12: Fact sheet for health professionals. Retrieved from https://ods.od.nih.gov/factsheets/VitaminB12-HealthProfessional/
Stier, H., Ebbeskotte, V., & Gruenwald, J. (2014). Immune-modulatory effects of dietary Yeast Beta-1,3/1,6-D-glucan. Nutrition journal, 13, 38. https://doi.org/10.1186/1475-2891-13-38
University of Michigan. (2008). Bowel function anatomy. https://medicine.umich.edu/sites/default/files/content/downloads/bowel-function.pdf
Harvard T.H. Chan, School of Public Health. (2022). Fiber. https://nutritionsource.hsph.harvard.edu/carbohydrates/fiber/
Cunningham E. (2013). Is there a diet for “yeast allergy”? Journal of the Academy of Nutrition and Dietetics, 113(3), 484. https://doi.org/10.1016/j.jand.2013.01.013
UMass Medical School Center for Applied Nutrition. Chan, U., School, M., & Nutrition, C. F. A. (2020). Nutritional yeast: Nourishing or no-go? UM. https://www.umassmed.edu/nutrition/blog/blog-posts/2020/2/nutritional-yeast–nourishing-or-no-go/
Looking for GI disorder treatment? Learn about the latest strategies and methods to manage your condition effectively.
What Are GI Disorders?
How often does a huge lunch leave you feeling bloated? Have you ever had gastrointestinal inflammation or constipation? Or do you have muscles and joints that are stiff? Environmental variables may disrupt the gastrointestinal system and produce several overlapping risk profiles in the body by extending their effect onto the musculoskeletal system. This can result in pain-like sensations that often resemble musculoskeletal illnesses, although many individuals are unaware of this. Depending on their severity, gastrointestinal (GI) problems are often frequent and may be difficult to treat, with major medical and social repercussions. In 2018, Malone et al. Gastric reflux disease (GERD), small intestinal bacterial overgrowth (SIBO), and irritable bowel syndrome (IBS) are a few prevalent GI disorders. In the musculoskeletal system, GI issues may be a contributing factor to persistent discomfort, inflexible joints, and muscular dysfunction. Understanding the relationship between the stomach and the musculoskeletal system helps many people find practical, non-surgical solutions that may alleviate pain and enhance their quality of life.
How GI Disorders Affect The Gut & Musculoskeletal System
Many individuals question how environmental variables might impact their muscles and intestines, and they play a significant role in the development of GI illnesses. One environmental component that might have an impact on the muscles and intestines is stress. A person’s physical and mental health may be impacted by stress, which can alter how the gut bacteria react and result in gastrointestinal diseases. In 2011, Konturek et al.
Inflammation & Systemic Effects
When GI illnesses begin to impact the body, they lead to inflammation and adhere to the afflicted region, resulting in problems with the stomach. When the gut system is affected by inflammation, it may cause low-grade inflammation, compromise the integrity of the gut barrier, and interfere with normal food and nutrient digestion. In 2024, Cassini et al. This may result in inflammatory chronic gastrointestinal disorders such as ulcerative colitis or Crohn’s disease. This may then cause cytokines and inflammatory mediators to be released into the bloodstream, which can lead to systemic inflammation in the musculoskeletal system, resulting in symptoms including tiredness, joint stiffness, and muscle soreness.
Nutrient Malabsorption & Deficiencies
Chronic diarrhea, IBD, and celiac disease may all affect how nutrients are absorbed, resulting in vitamin and mineral deficiencies that can cause joint pain, weakness, and cramping in the muscles that are often confused with fibromyalgia or arthritis.
Gut Dysbiosis & The Nervous System
The neurological system and the digestive system, often referred to as the “second brain,” have a special interaction. Dysbiosis, or an imbalance in gut bacteria, may lead to the development of a leaky gut since the gut contains trillions of bacteria and aids in the transportation of nutrients from meals to other bodies. Toxins may enter the circulation and set off the immune system as a result. This results in systemic inflammation and musculoskeletal pain, which impacts the quality of life and pain of the musculoskeletal system from the stomach. (Casini and others, 2024) In addition, the gut-brain axis regulates muscular contraction and pain perception.
Visceral-Somatic Reflexes & Referred Pain
Referred pain patterns, in which the musculoskeletal system experiences visceral discomfort, may be caused by GI problems. Visceral pain hypersensitivity manifests as persistent stomach pain or discomfort (Farmer & Aziz, 2009). For instance, IBS might result in lower back and pelvic pain because of visceral-somatic responses, but GERD can produce chest and upper back pain.
Fighting Inflammation Naturally: Video
Functional & Nonsurgical Approaches To Reduce GI Pain
The following non-surgical, evidence-based methods may be used to treat musculoskeletal and intestinal discomfort:
Dietary Modifications
A nutritious diet is a good place to start when making little adjustments to enhance gut health. A balanced diet may help the body develop, mend, and produce energy. It can also influence and control a number of vital bodily processes, including hormones in the gastrointestinal tract. El-Salhy, 2019. By avoiding trigger meals that result in overlapping pain sensations, including foods high in omega-3s and polyphenols may help lessen the inflammatory effects from the stomach. GI issues may be treated using the following diets:
Elimination and Anti-Inflammatory Diet
Diet of FODMAP.
Pro-& Prebiotics
Probiotics and prebiotics may aid in the restoration and balancing of the gut flora in terms of gut health. Prebiotics use foods high in fiber to nourish the good bacteria in the stomach and promote gut health, while probiotics include good bacteria that help balance the gut microbiota and lower inflammation. By combining these two, intestinal inflammation may be avoided by reestablishing the dynamic equilibrium between the host defense systems and microbiota in the intestinal mucosa. (Dhaneshwar & Roy, 2023)
Stress Management
Reducing environmental stresses that lead to gastrointestinal illnesses and musculoskeletal discomfort also helps the body relax and ease tight muscles. Among the methods individuals may use are:
Meditation and Mindfulness: Progressive muscular relaxation, yoga, and deep breathing may all help people feel less discomfort and less sensitive to their stomachs.
Cognitive behavioral therapy, or CBT, may help enhance pain tolerance and manage GI symptoms brought on by stress.
Manual Therapies
GI conditions linked to musculoskeletal discomfort may be reduced using manual therapy. In order to assist strengthen and stretch weak muscle groups and lessen the body’s inflammatory effects, massage therapists, physical therapists, and chiropractors may use a variety of treatments. Among these treatments are:
Osteopathic Manipulative Therapy (OMT): Enhances gastrointestinal motility and relieves referred pain.
Visceral manipulation is a manual treatment that eases musculoskeletal tension and improves digestion by releasing abdominal limitations.
Massage therapy may ease back and abdominal muscular tension and lessen gastrointestinal symptoms associated with stress.
Acupuncture
By activating the autonomic nervous system, acupuncture has been shown to enhance stomach motility and lessen discomfort associated with IBS. To alleviate a patient, acupuncturists insert tiny, thin needles into different bodily acupoints. Neuromodulation, intestinal barrier restoration, and gut microbiota adjustment are all part of acupuncture. (Li and others, 2023)
Conclusion
The musculoskeletal system and gastrointestinal illnesses interact in a unique way because their risk profiles overlap and correlate. Treatments to lessen GI issues may be more successful when this relationship is understood. Functional, non-surgical methods including movement-based treatments, manual therapies, stress management, gut microbiota maintenance, and dietary modifications may provide comprehensive relief from GI-related musculoskeletal pain. These little adjustments to a person’s daily schedule, such as regular exercise or a balanced diet, may help address the underlying cause of dysfunction and provide long-lasting relief and enhanced wellbeing.
Injury Medical & Functional Medicine Clinic
We associate with certified medical providers who understand the importance of the effects of GI disorders on not only the gut system but also the musculoskeletal system. While asking important questions to our associated medical providers, we advise patients to implement small changes like physical activities and small dietary changes to their diet to reduce the chances of GI disorders from returning. Dr. Alex Jimenez, D.C., envisions this information as an academic service. Disclaimer.
References
Casini, I., Massai, L., Solomita, E., Ortenzi, K., Pieretti, S., & Aloisi, A. M. (2024). Gastrointestinal Conditions Affect Chronic Pain and Quality of Life in Women. Int J Environ Res Public Health, 21(11). https://doi.org/10.3390/ijerph21111435
El-Salhy, M. (2019). Nutritional Management of Gastrointestinal Diseases and Disorders. Nutrients, 11(12). https://doi.org/10.3390/nu11123013
Farmer, A. D., & Aziz, Q. (2009). Visceral pain hypersensitivity in functional gastrointestinal disorders. Br Med Bull, 91, 123-136. https://doi.org/10.1093/bmb/ldp026
Konturek, P. C., Brzozowski, T., & Konturek, S. J. (2011). Stress and the gut: pathophysiology, clinical consequences, diagnostic approach and treatment options. J Physiol Pharmacol, 62(6), 591-599. https://www.ncbi.nlm.nih.gov/pubmed/22314561
Li, X., Liu, S., Liu, H., & Zhu, J. J. (2023). Acupuncture for gastrointestinal diseases. Anat Rec (Hoboken), 306(12), 2997-3005. https://doi.org/10.1002/ar.24871
Malone, M., Waheed, A., & Samiullah, S. (2018). Functional Gastrointestinal Disorders: Functional Lower Gastrointestinal Disorders in Adults. FP Essent, 466, 21-28. https://www.ncbi.nlm.nih.gov/pubmed/29528206
Roy, S., & Dhaneshwar, S. (2023). Role of prebiotics, probiotics, and synbiotics in management of inflammatory bowel disease: Current perspectives. World J Gastroenterol, 29(14), 2078-2100. https://doi.org/10.3748/wjg.v29.i14.2078
Can drinking parsley tea help improve overall health?
Parsley Tea
Parsley is commonly used as a garnish and to increase flavor in dishes. Some use parsley leaves instead of salt in their food to reduce their sodium intake. It is widely available in grocery stores and can be grown at home. Parsley tea is an herbal tea. Surprisingly, parsley tea benefits health, but not all of this is supported by scientific evidence. There are different kinds of parsley:
Curly leaf (Petroselinum crispum)
Flat leaf (Petroselinum neapolitanum) or Italian parsley.
Parsley is high in vitamins A, B, C, E, and K.
Parsley also provides fiber, iron, copper, calcium, and potassium.
The kind used in tea is up to you, based on flavor preferences.
Benefits
Parsley is believed to have various benefits, some of which are derived from consuming parsley tea. For example, parsley is used to freshen breath; however, adding sugar reduces dental benefits. Many women also suggest that parsley helps to ease menstrual cramps, and others say that consuming parsley or tea helps them eliminate excess water weight. However, further research is needed to support its benefits that include: (Ganea M. et al., 2024)
Asthma
Cough
Digestive problems
Menstrual problems
Fluid retention and swelling (edema)
Urinary tract infections
Kidney stones
Cracked or chapped skin
Bruises
Insect bites
Liver disorders
Tumors
Preparation
The quickest way to enjoy parsley tea is to use a parsley tea bag. Brands are available online and in health food stores. Parsley tea bags are manufactured using dried leaves, which can be stored in a cool, dry place and last much longer than fresh parsley. The herb is inexpensive, and making parsley tea at home is also cheap and easy.
Choose Parsley
Flat or curly.
Remove the leaves from the stems.
Gather about 1/8-1/4 cups of leaves for each cup of tea.
Place the leaves at the bottom of your cup or in a tea infuser.
Note: you can also use a French press to make parsley tea.
To do so, place the loose leaves at the bottom of the French press.
Heat Water
Once boiling, fill the cup or press with hot water.
Allow the Leaves to Steep
For about four minutes.
Steep longer if you prefer a stronger cup.
If you are new to parsley tea, start with a weaker cup and gradually increase the strength as you get used to the taste.
Remove the Parsley Leaves
With a spoon, remove the infuser and discard the leaves.
If you use a press, place the plunger on top and slowly press down to separate the leaves from the tea.
Flavor your tea with lemon or a little sugar (optional).
Side Effects
The FDA generally recognizes parsley as safe (GRAS). However, consuming large amounts—more than you would typically consume in amounts commonly found in food—can be dangerous. Having a cup of tea daily is not considered a large amount, but if you make tea with parsley oil or ground parsley seeds, your intake could be much higher than normal. Individuals who consume too much parsley may experience anemia and liver or kidney problems. (Alyami F. A., & Rabah D. M. 2011) Individuals who have diabetes, fluid retention, high blood pressure, or kidney disease should talk to their doctor to see if consuming parsley is safe for them, as it may cause side effects that can worsen their condition. Patients who undergo surgery are advised to avoid parsley in the two weeks before their procedure.
Injury Medical Chiropractic and Functional Medicine Clinic
Injury Medical Chiropractic and Functional Medicine Clinic focuses on and treats injuries and chronic pain syndromes through personalized care plans that improve ability through flexibility, mobility, and agility programs to relieve pain. Our providers use an integrated approach to create customized care plans for each patient and restore health and function to the body through nutrition and wellness, functional medicine, acupuncture, electroacupuncture, and various medicine protocols. If the individual needs other treatment, they will be referred to a clinic or physician best suited for them. Dr. Jimenez has teamed up with top surgeons, clinical specialists, medical researchers, nutritionists, and health coaches to provide the most effective clinical treatments.
Optimizing Your Wellness
References
Ganea, M., Vicaș, L. G., Gligor, O., Sarac, I., Onisan, E., Nagy, C., Moisa, C., & Ghitea, T. C. (2024). Exploring the Therapeutic Efficacy of Parsley (Petroselinum crispum Mill.) as a Functional Food: Implications in Immunological Tolerability, Reduction of Muscle Cramps, and Treatment of Dermatitis. Molecules (Basel, Switzerland), 29(3), 608. https://doi.org/10.3390/molecules29030608
Alyami, F. A., & Rabah, D. M. (2011). Effect of drinking parsley leaf tea on urinary composition and urinary stones’ risk factors. Saudi journal of kidney diseases and transplantation: an official publication of the Saudi Center for Organ Transplantation, Saudi Arabia, 22(3), 511–514.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine