How Chiropractic Care Helps Gut Injuries After Car Accidents: Restoring Spinal Alignment for Digestive Relief
Car accidents often cause visible injuries like whiplash or back pain. But in some cases, they can also lead to unexpected symptoms, including digestive problems. Bloating, cramping, nausea, and constipation may not seem connected to an auto injury—but there’s a deeper link between the spine and the gut.
At El Paso Back Clinic, Dr. Alexander Jimenez, DC, APRN, FNP-BC, specializes in understanding how musculoskeletal injuries caused by car accidents can contribute to gut dysfunction. His integrative approach utilizes chiropractic adjustments, diagnostic imaging, and medical evaluation to help patients recover not only from back pain but also from internal symptoms that impact their quality of life.
Car Accidents and Digestive Problems: What’s the Link?
When a car accident occurs, the force of impact can damage the spine, muscles, and nerves. These injuries can lead to inflammation, spinal misalignment, and nerve compression—especially in the thoracic and lumbar spine, which are closely tied to digestion. Even if the abdomen wasn’t hit directly, nerve disruptions from the spine may still affect how the digestive system works.
The autonomic nervous system, which regulates internal organs, often becomes unbalanced following trauma. This can trigger symptoms like:
Nausea or vomiting
Constipation or diarrhea
Loss of appetite
Acid reflux or bloating
Misalignments in the spine—called subluxations—can also compress nerves that travel to the stomach and intestines, slowing down their normal function and increasing gut distress.
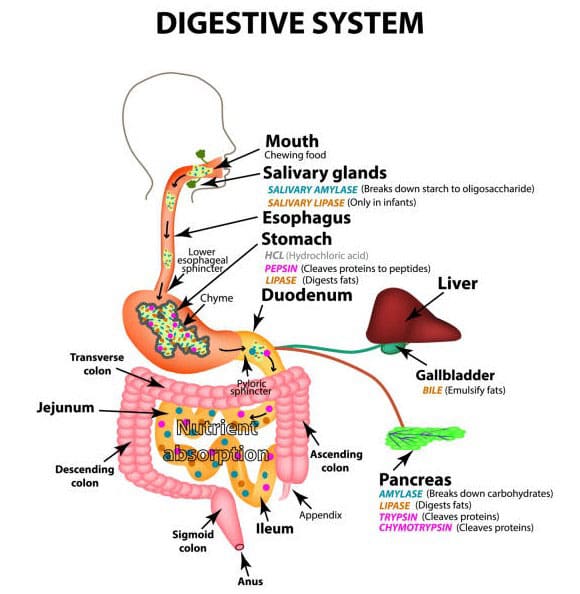
The spine doesn’t just support posture—it also protects the spinal cord and the nerves that control digestion. When an accident misaligns the vertebrae, it can pinch or irritate these nerves. For example:
T6–T9 vertebrae affect the stomach and small intestines
L1–L3 vertebrae impact the large intestine and colon
The vagus nerve, connected through the cervical spine, helps regulate digestion
When these nerves are compressed, the digestive system may not receive the right signals. This can lead to discomfort and dysfunction even without a direct abdominal injury.
Chiropractic adjustments aim to realign the spine, restore nerve flow, and reduce inflammation, thereby supporting the body’s natural ability to regulate digestion.
Dr. Alexander Jimenez’s Approach at El Paso Back Clinic
Dr. Alexander Jimenez brings a unique combination of chiropractic and medical expertise to patient care. As a Doctor of Chiropractic and a board-certified Family Nurse Practitioner (APRN, FNP-BC), he provides a dual-scope model that integrates:
Advanced spinal and musculoskeletal assessments
Diagnostic imaging (MRI, X-ray, CT scans)
Functional medicine support
Legal-medical documentation for personal injury claims
Nutritional and inflammatory evaluations
Dr. Jimenez and his team assess not just back and neck pain, but also internal systems that may be affected by spinal trauma. Patients reporting digestive issues after an accident often undergo evaluations that include spinal palpation, nerve testing, and postural analysis to uncover hidden contributors to their symptoms.
Whiplash is one of the most common injuries from rear-end car accidents. While it mainly affects the cervical spine, it can also disrupt the vagus nerve, which runs from the brainstem down into the digestive system. The vagus nerve plays a key role in the following functions:
Stomach acid production
Intestinal movement
Appetite regulation
Nutrient absorption
Misalignment of the neck can impair vagus nerve function, leading to symptoms such as reflux, indigestion, or slowed digestion. Realigning the cervical spine through chiropractic care may help relieve this nerve pressure and restore better digestive function.
Chiropractic Adjustments: Drug-Free Digestive Support
After a car accident, patients are often prescribed medications like antacids, laxatives, or anti-inflammatories to manage symptoms. While helpful in the short term, these don’t address the root cause of the digestive issues—especially when spinal misalignment is involved.
Chiropractic care is a drug-free, non-invasive solution that aims to correct the structural problems contributing to gut symptoms. At El Paso Back Clinic, chiropractic adjustments are tailored to each individual’s injuries and nervous system balance. Improvements in digestion may occur as the spine realigns and nerve signals are restored.
A Comprehensive Recovery Plan: Integrating Chiropractic and Functional Medicine
Dr. Jimenez takes a comprehensive approach to post-accident recovery. His patients often receive an individualized plan that includes:
Spinal and soft tissue adjustments
Anti-inflammatory nutritional guidance
Postural and core strengthening
Functional diagnostic testing
Emotional stress evaluation
By combining chiropractic care with functional medicine and injury rehabilitation strategies, El Paso Back Clinic helps patients heal from both external trauma and internal dysfunction. If gut issues are not resolving, additional imaging or laboratory tests may be recommended to rule out complications, such as internal bruising, hernias, or organ damage.
Legal and Documentation Support for Digestive Symptoms
Digestive issues related to car accidents are often harder to document than broken bones or visible injuries. But they still affect daily life—and they deserve attention in personal injury cases. Dr. Jimenez provides detailed documentation that supports legal claims and insurance coverage, including:
Injury diagnosis and symptom correlation
Imaging and nerve testing reports
Treatment progress updates
Functional impairment assessments
Collaborative notes for legal teams
This ensures that patients not only recover physically but also receive the support and recognition they need in their legal processes.
The sooner chiropractic care begins after a car accident, the better the outcomes—especially for preventing long-term gut issues. Delayed care can allow inflammation to worsen, nerves to become more irritated, and spinal misalignments to solidify into chronic dysfunction.
At El Paso Back Clinic, early evaluations include:
Spinal alignment assessments
Postural screenings
Neurological testing
Inflammatory marker checks
Digestive function reviews
Early detection and treatment help reduce the risk of chronic constipation, irritable bowel symptoms, or abdominal adhesions.
Conclusion: Restoring Digestive Health Through the Spine
Although chiropractors don’t treat the digestive system directly, they can help alleviate symptoms by addressing spinal misalignments that affect gut function. After a car accident, many patients at El Paso Back Clinic report digestive problems that may stem from nerve interference, muscle tension, or autonomic imbalance.
Dr. Alexander Jimenez, with his dual-scope expertise, provides comprehensive care that includes chiropractic adjustments, functional evaluations, and documentation of injuries. His integrative team assists patients in recuperating from car accidents, not only in terms of structure but also in terms of internal health.
If you’ve experienced digestive discomfort following a motor vehicle accident, don’t overlook the role of your spine. A proper evaluation could be the key to lasting relief.
Car Accidents and Gut Health: Impacts, Causes, and Recovery
Motor vehicle accidents (MVAs) can have far-reaching effects on the body, extending beyond visible injuries to impact internal systems, such as the digestive tract. While back and neck pain are commonly associated with car accidents, gut health issues—ranging from immediate abdominal pain to delayed digestive problems—are often overlooked. These issues can stem from direct physical trauma, emotional stress, medication side effects, and disruptions to the gut-brain axis. In El Paso, Texas, Dr. Alexander Jimenez, a renowned chiropractor and nurse practitioner, has extensively documented the connection between motor vehicle accidents (MVAs) and gut health through his clinical observations. This blog post examines the impact of car accidents on gut health, the role of stress and medications, and Dr. Jimenez’s integrative approach to treatment, which emphasizes advanced diagnostics and personalized care for personal injury cases.
Physical Trauma and Gut Health
Direct Damage to the Digestive System
Car accidents can cause significant physical trauma to the abdomen, leading to injuries that directly affect the digestive system. Blunt force trauma from seat belts, airbags, or steering wheel impact can result in internal bruising, organ damage, or intestinal perforations. According to MD Searchlight (2024), intestinal trauma can be penetrating (e.g., from sharp objects) or blunt (e.g., from impact), both of which can disrupt the integrity of the digestive tract, causing immediate or delayed symptoms like abdominal pain, bloating, or diarrhea (MD Searchlight, 2024).
Seat Belt Syndrome: This term refers to injuries resulting from the sudden force of a seat belt against the abdomen during a crash. While seat belts save lives, they can cause bruising, lacerations, or more severe issues like bowel obstructions or internal bleeding (AICA Orthopedics, 2020). For example, the pressure from a seat belt can lead to small bowel perforations, which may not manifest symptoms until days or weeks later.
Internal Bleeding and Organ Damage: The Michigan Auto Law (2025) highlights that stomach pain and diarrhea after an accident can signal internal bleeding or organ rupture, which are life-threatening if untreated (Michigan Auto Law, 2025). Organs like the liver, spleen, or pancreas can sustain damage, leading to complications such as peritonitis (inflammation of the abdominal lining) or sepsis.
Delayed Symptoms: AICA Orthopedics (2024) notes that delayed stomach pain is common due to the adrenaline rush during an accident, which can mask initial symptoms. Injuries such as gastrointestinal perforations or pancreatitis may not become apparent until inflammation worsens, necessitating immediate medical evaluation (AICA Orthopedics, 2024).
Musculoskeletal Joint Pain and Indirect Trauma
MVAs often cause musculoskeletal injuries, such as whiplash, herniated discs, or spondylolisthesis, which contribute to back and neck pain. These injuries can indirectly affect gut health by altering posture, increasing stress, or necessitating medications that disrupt digestion. Dr. Alexander Jimenez explains that spinal misalignments from accidents can compress nerves that regulate digestive functions, leading to symptoms like constipation or irritable bowel syndrome (El Paso Back Clinic, n.d.).
Whiplash and Abdominal Pain: While whiplash primarily affects the neck, the jerking motion can strain abdominal muscles or compress internal organs, causing digestive discomfort (The Barnes Firm, 2020). This connection underscores the systemic impact of MVAs on the body.
Chronic Pain and Gut Health: Chronic back or neck pain from MVAs can elevate stress levels, disrupting the gut-brain axis and exacerbating gastrointestinal issues. Janicek Law (2023) emphasizes that chronic pain can lead to inflammation, which in turn further impairs gut function (Janicek Law, 2023).
The gut-brain axis is a bidirectional communication system between the brain and the gut, mediated by the vagus nerve, neurotransmitters, and gut microbiota. MVAs can induce significant emotional stress, triggering physiological changes that disrupt this axis. Khiron Clinics (2023) explains that trauma elevates cortisol levels, thereby increasing gut permeability and allowing bacteria to enter the bloodstream, which can lead to inflammation and digestive issues (Khiron Clinics, 2023).
Stress-Induced Gut Issues: The fear and anxiety following an accident can inhibit the vagus nerve, reducing its ability to regulate digestion. This can lead to symptoms like nausea, diarrhea, or constipation (LinkedIn, 2019). Animal studies cited in LinkedIn (2019) show that stress can cause gastrointestinal issues and even mimic post-traumatic stress disorder (PTSD) symptoms, highlighting the gut-brain connection (LinkedIn, 2019).
Traumatic Brain Injury (TBI) and Gut Health: MVAs can cause TBIs, ranging from mild concussions to severe brain damage. Heuer Fischer (n.d.) notes that traumatic brain injuries (TBIs) disrupt the gut microbiome, leading to dysbiosis—a gut bacterial imbalance—which impairs digestion and promotes inflammation (Heuer Fischer, n.d.). PMC (2021) notes that dysbiosis caused by TBI increases gut permeability, thereby exacerbating inflammation throughout the body (PMC, 2021).
Clinical Observations by Dr. Jimenez
Dr. Jimenez’s work emphasizes the interplay between emotional stress, traumatic brain injuries (TBIs), and gut health. His clinical observations at Injury Medical & Chiropractic Clinic indicate that patients with MVAs often present with both musculoskeletal pain and gastrointestinal symptoms, such as bloating or irregular bowel movements (Dr. Alex Jimenez, n.d.). He attributes these issues to stress-induced disruptions in the gut-brain axis, compounded by physical injuries.
Dr. Alex Jimenez. (n.d.). Traumatic brain injuries & gut issues. Retrieved from https://dralexjimenez.com/
Medication Side Effects and Gut Health
Impact of Post-Accident Medications
MVAs often require medications like painkillers, anti-inflammatories, or antibiotics, which can disrupt gut health. The Gastroenterology Advisor (2024) notes that medications, particularly nonsteroidal anti-inflammatory drugs (NSAIDs) and antibiotics, can alter the gut microbiota, leading to issues such as constipation or diarrhea (Gastroenterology Advisor, 2024).
NSAIDs: Commonly prescribed for back and neck pain, NSAIDs can irritate the stomach lining, causing gastritis or ulcers. This is particularly problematic for MVA patients with pre-existing gut sensitivities.
Antibiotics: If surgery or infections (e.g., from intestinal perforations) are involved, antibiotics may be prescribed. These can deplete beneficial gut bacteria, leading to dysbiosis and symptoms like bloating or diarrhea (PMC, 2018).
Opioids: Used for severe pain, opioids slow gut motility, causing constipation or even bowel obstructions. Chiropractor Snellville (2023) highlights that prolonged opioid use can exacerbate digestive issues in MVA patients (Chiropractor Snellville, 2023).
Dr. Jimenez’s Approach to Medication Management
Dr. Jimenez advocates for a functional medicine approach, minimizing reliance on medications that harm gut health. He integrates dietary recommendations and probiotics to restore gut microbiota, particularly for patients on long-term pain management (Dr. Alex Jimenez, n.d.). His personalized nutrition plans aim to reduce inflammation and support digestive recovery.
Dr. Alex Jimenez. (n.d.). Post-automobile accident recovery and healing foods. Retrieved from https://dralexjimenez.com/
Dr. Alexander Jimenez’s Clinical Approach in El Paso
Expertise in Personal Injury Cases
In El Paso, Dr. Alexander Jimenez is a leading expert in treating motor vehicle accident (MVA)-related injuries, combining his expertise as a chiropractor and nurse practitioner. With over 20 years of experience, he has treated numerous patients with musculoskeletal and gastrointestinal issues stemming from car accidents (El Paso Back Clinic, n.d.). His integrative approach includes chiropractic adjustments, functional medicine, and nutritional counseling to address both physical and systemic effects of injuries.
Personal Injury Documentation: Dr. Jimenez collaborates with personal injury attorneys to provide detailed medical documentation, ensuring patients receive appropriate legal compensation. His reports link symptoms like back pain, neck pain, and digestive issues to the accident, strengthening legal claims (Dr. Alex Jimenez, n.d.).
Advanced Diagnostics and Dual-Scope Procedures
Dr. Jimenez utilizes advanced imaging techniques (e.g., X-rays, CT scans, and MRIs) and dual-scope procedures (e.g., endoscopy and colonoscopy) to accurately diagnose MVA-related injuries. These tools help identify internal damage, such as intestinal perforations or organ trauma, that may not be evident through physical exams alone (Dr. Alex Jimenez, n.d.).
Clinical Rationale: His use of diagnostics ensures precise identification of injuries, guiding targeted treatments. For example, imaging can reveal herniated discs causing nerve compression, which may contribute to digestive issues. Dual-scope procedures are particularly useful for detecting gastrointestinal trauma, such as tears in the intestinal wall, which can lead to sepsis if untreated.
Holistic Treatment Plans: Dr. Jimenez’s treatment plans combine chiropractic care for musculoskeletal pain, visceral manipulation for gut health, and dietary adjustments to reduce inflammation. His approach addresses the root causes of symptoms, promoting long-term recovery (El Paso Back Clinic, n.d.).
Citations
Dr. Alex Jimenez. (n.d.). Car accident specialist in El Paso, TX. Retrieved from https://dralexjimenez.com/
Seek Medical Attention: Even if symptoms are not immediate, a thorough medical evaluation is crucial to rule out internal injuries. The Barnes Firm (2020) emphasizes that prompt care can prevent complications like organ failure or sepsis (The Barnes Firm, 2020).
Monitor Symptoms: Watch for delayed symptoms, such as stomach pain, diarrhea, or bloating, which may indicate serious issues (AICA Orthopedics, 2024).
Consult a Specialist: Specialists, such as Dr. Jimenez, can provide comprehensive care that addresses both physical and gastrointestinal symptoms.
Long-Term Recovery
Chiropractic Care: Regular adjustments can alleviate back and neck pain, reducing stress on the digestive system.
Dietary Adjustments: Dr. Jimenez recommends anti-inflammatory diets rich in probiotics to restore gut health (Dr. Alex Jimenez, n.d.).
Stress Management: Techniques such as meditation or yoga can help reduce cortisol levels, thereby supporting the gut-brain axis (Khiron Clinics, 2023).
Preventing Future Injuries
Proper Seat Belt Use: Ensure seat belts are worn correctly to minimize abdominal trauma.
Safe Driving Practices: Avoid distractions and follow traffic rules to reduce the risk of accidents.
Vehicle Safety Features: Utilize airbags and advanced safety systems to enhance protection (PMC, n.d.).
Car accidents can profoundly affect gut health through physical trauma, emotional stress, and medication side effects. Direct injuries like seat belt syndrome or internal bleeding can cause immediate or delayed digestive issues, while stress and TBIs disrupt the gut-brain axis, leading to long-term complications. Medications used to manage pain or infections can further impair gut microbiota, exacerbating symptoms. In El Paso, Dr. Alexander Jimenez’s integrative approach—combining chiropractic care, advanced diagnostics, and functional medicine—offers a comprehensive solution for MVA victims. His use of imaging and dual-scope procedures ensures accurate diagnoses, while his collaboration with legal professionals supports patients’ compensation claims. By addressing both physical and systemic effects, Dr. Jimenez helps patients achieve holistic recovery, emphasizing the importance of seeking prompt medical care after a motor vehicle accident (MVA).
Can incorporating sauerkraut into one’s diet help promote healthy gut bacteria?
Sauerkraut
Sauerkraut, a fermented cabbage food, is a great source of probiotics and fiber, both of which can contribute to gut health. It’s a living food containing various microbial strains and can help improve digestion, reduce inflammation, and improve overall gut health. (Shahbazi R. et al., 2021)
Fermented foods like sauerkraut have live cultures that promote the growth of beneficial probiotics, bacteria that provide powerful health benefits. Probiotics also help make foods more digestible, increasing the gut’s ability to absorb the vitamins and minerals they contain. A study found that fermented cabbage may help protect intestinal cells from inflammatory damage more than raw cabbage. (Wei L., & Marco M. L., 2025)
Homemade sauerkraut likely contains more live cultures than store-bought since processing may destroy some of the healthy bacteria. (National Institutes of Health Office of Dietary Supplements, 2023) Depending on which supplement is chosen, sauerkraut may have a greater diversity of probiotic strains. This is because an oral supplement has a known quantity and strain of probiotics. Individuals who want to add probiotics to their diet for potential gut health benefits should take a food-first approach, which is generally recommended over oral supplements. (National Institutes of Health, 2025)
Look at the Benefits
Probiotics
Sauerkraut contains lactic acid bacteria, which are beneficial bacteria that can help support the immune system and reduce inflammation. (Healthline, 2023)
Fiber
Sauerkraut is a robust source of fiber, which aids in digestion and can help you feel full longer.
Digestion
The probiotics in sauerkraut can improve digestion by promoting a healthy gut microbiome. (Medical News Today, 2023)
Consult with a doctor before adding sauerkraut to your diet if you are taking monoamine oxidase inhibitors (MAOIs).
Start small and learn how you like to eat sauerkraut, which can be as a condiment, side dish, or sandwich ingredient.
Injury Medical Chiropractic and Functional Medicine Clinic
As a Family Practice Nurse Practitioner, Dr. Jimenez combines advanced medical expertise with chiropractic care to address various conditions. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop highly effective treatment plans through an integrated approach for each patient and restore health and function to the body through nutrition and wellness, functional medicine, acupuncture, electroacupuncture, and integrated medicine protocols. We focus on what works for you to relieve pain, restore function, prevent injury, and mitigate issues through adjustments that help the body realign itself. The clinic can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal problems.
Body In Balance: Chiropractic, Fitness, and Nutrition
References
Shahbazi, R., Sharifzad, F., Bagheri, R., Alsadi, N., Yasavoli-Sharahi, H., & Matar, C. (2021). Anti-Inflammatory and Immunomodulatory Properties of Fermented Plant Foods. Nutrients, 13(5), 1516. https://doi.org/10.3390/nu13051516
Healthline. (2023). 8 Surprising Benefits of Sauerkraut (Plus How to Make It). https://www.healthline.com/nutrition/benefits-of-sauerkraut#nutrients
Medical News Today. (2023). What are the benefits of eating sauerkraut? https://www.medicalnewstoday.com/articles/health-benefits-of-sauerkraut
Wei, L., & Marco, M. L. (2025). The fermented cabbage metabolome and its protection against cytokine-induced intestinal barrier disruption of Caco-2 monolayers. Applied and environmental microbiology, e0223424. Advance online publication. https://doi.org/10.1128/aem.02234-24
National Institutes of Health Office of Dietary Supplements. (2023). Probiotics. Retrieved from https://ods.od.nih.gov/factsheets/Probiotics-Consumer/
National Institutes of Health. (2025). Probiotics. Retrieved from https://ods.od.nih.gov/factsheets/Probiotics-HealthProfessional/
U.S. Department of Agriculture. (2018). Sauerkraut, canned, solids and liquids. Retrieved from https://fdc.nal.usda.gov/food-details/169279/nutrients
For individuals dealing with digestive issues and conditions, can incorporating Tai Chi help improve gut health?
Tai Chi For Gut Health
Tai Chi is an exercise that has been referred to as moving meditation. The practice is rooted in Chinese medicine, which fuses martial arts and meditation. The art of Tai Chi is used to improve physical health. It can also positively impact gut health by improving digestive function, reducing inflammation, and influencing the gut microbiota composition. The slow, controlled movements and deep breathing can stimulate abdominal and pelvic organs, promoting digestion. Additionally, it has been shown to reduce inflammation in the gut and increase the diversity of gut bacteria, including beneficial butyrate-producing bacteria. (Kang D., Wang X., & Wang J., 2023)
Types
The idea is to slow down your mind and body by repeating rhythmic choreography and breathwork for about 30 to 60 minutes, culminating in finding a sense of inner peace and tranquility.
Primary Forms/Styles
These include Chen, Yang, Wu, Sun, and Wu/Hao. Each follows the same origins and principles with variations. (Tai Chi for Health Institute, 2007)
Chen Style
Considered the oldest and original style, the Chen style is characterized by explosive power, low stances, and a combination of fast and slow movements, including jumping, kicking, and striking.
Chen also utilizes a movement called “silk reeling,” a spiral-esque, flowing movement that starts at the feet and moves into the hands.
Yang Style
Yang is often considered the most popular form of Tai Chi and is practiced worldwide.
Yang Tai Chi focuses more on improving flexibility through grand, sweeping movements executed slowly and gracefully.
Wu Style
Wu Tai Chi emphasizes small, compact movements and a medium stance. Its focus is on extending the body by leaning forward and backward.
Sun Style
Sun Tai Chi combines elements of Tai Chi, Xing Yi, and Ba Gua, resulting in a unique style with fluid, circular movements.
Hao Style
This style is characterized by small-frame movements focusing on accurate position and internal strength.
Tai Chi can indirectly benefit gut health by reducing stress levels.
Its emphasis on slow movements and deep breathing can help reduce stress.
Combining meditative practices with physical movement can help calm the mind, improve focus, and even trigger the release of endorphins.
Improved Digestion
Gentle, flowing movements, particularly those involving the diaphragm, can massage and stimulate the abdominal and pelvic organs, aiding the digestive process.
Reduced Inflammation
Tai Chi can help reduce gut inflammation, a common issue in conditions like inflammatory bowel disease (IBD).
Gut Microbiota Changes
Tai Chi has been found to positively influence the gut microbiota composition, increasing the diversity and abundance of beneficial bacteria.
Improved Gut Barrier Function
Tai Chi may help improve the integrity of the gut barrier, which is essential for preventing harmful substances from entering the bloodstream and causing inflammation.
Increased Butyrate Production
Tai Chi can promote the growth of butyrate-producing bacteria, which are important for intestinal health and can reduce inflammation.
Overall Health Benefits
Increases Cognitive Function
In addition to improving your mental well-being, Tai Chi has also been found to boost cognitive abilities.
A meta-analysis stated that physical exercise, in general, improves cognitive function, and researchers specifically recommended Tai Chi for elderly individuals since it’s a gentler and more accessible form of physical exercise that also combines mental exercises through repeated choreography. (Yin Wu, et al., 2013)
Increases Flexibility and Agility
Similar to yoga, Tai Chi often involves body extensions that can improve flexibility and agility.
This is useful in daily activities and makes you more agile and capable in other sports.
Improves Balance and Coordination
In addition to improving flexibility and agility, the intricate movements can help balance and coordination.
This skill is useful in daily life.
It can help with fine motor skills and even prevent trips, stumbles, falls, and other sports.
Enhances Strength and Stamina
As with any form of physical exercise, Tai Chi can build upon existing strength and stamina.
With ongoing practice, individuals become leaner, their muscles are more defined, and they can exercise longer.
Injury Medical Chiropractic & Functional Medicine Clinic
Talk to a healthcare provider to learn what interventions would help the most. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, and prevent injury. Regarding musculoskeletal pain, specialists like chiropractors, acupuncturists, and massage therapists can help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal issues.
Body Maintenance
References
Kang, D., Wang, X., & Wang, J. (2023). Intervention study of tai chi training on the intestinal flora of college student basketball players. Medicine, 102(36), e35044. https://doi.org/10.1097/MD.0000000000035044
Wu Y, W. Y., Burgess EO, Wu J. (2013). The effects of Tai Chi exercise on cognitive function in older adults: A meta-analysis. Journal of Sport and Health Science, 2(4), 193-203. https://doi.org/https://doi.org/10.1016/j.jshs.2013.09.001
Tai Chi for Health Institute. (2018). History of Tai Chi. https://taichiforhealthinstitute.org/history-of-tai-chi/#:~:text=Based%20on%20Qigong%20and%20martial%20art%20techniques,It%20contains%20explosive%20power%20and%20low%20stances.
Enzymes’ function is to help trigger bodily processes ranging from digestion to blood clotting to growth. What is the best way to support enzyme production?
Enzymes
Enzymes are proteins that act as biological catalysts. They cause and speed up crucial chemical reactions and help the body complete necessary chemical reactions. They are vital for many biological processes, including digestion, metabolism, and molecule building and breaking down. This includes breaking down food, facilitating growth, and forming blood clots. Too little of a certain type can lead to serious health implications like a fatal buildup of toxins. Individuals missing a certain kind of enzyme or having too little of it can develop serious health conditions.
Function
They help speed up chemical reactions in the body (National Human Genome Research Institute, 2025). They facilitate chemical reactions in everything from digesting food to muscle growth. Enzymes facilitate this by binding to a cell, creating the reactions needed. With enzyme binding, chemical reactions can occur without destroying the cell. (Nemours KidsHealth, 2023) Each cell in the body has thousands of enzymes to help facilitate all the complex reactions to maintain health. (National Human Genome Research Institute, 2025)
Factors Affecting Production
In healthy individuals, the body produces the enzymes it needs. However, metabolic disorders can occur if the body does not produce enough of a certain type. (Kennedy Krieger Institute, 2025) These disorders can be serious and are usually caused by a genetic malfunction that impacts production.
Types
There are thousands of different types. Digestive enzymes, for example, aid in the breakdown of food and convert it into energy. Common enzymes that are critical for health include (Nemours KidsHealth, 2023)
Amylase
Digestive helps break down starches.
Aspartate aminotransaminase (AST) and Alanine Aminotransaminase (ALT)
Help the liver convert sugar into energy.
Creatine Kinase (CK)
Helps muscles create energy.
DNA Polymerase
Facilitates growth by allowing DNA to duplicate.
Glucose-6-Phosphate Dehydrogenase
Keeps red blood cells healthy by preventing damage to the cell.
Lipase
A digestive enzyme that helps break down fats and oils.
Protease
Digestive helps break down proteins.
Thrombin
Causes blood to clot.
Deficiencies
If the body doesn’t make enough of a certain enzyme, it cannot undergo the bodily processes that the enzyme helps facilitate. This can lead to a variety of symptoms. Some are minor, like not being able to eat lactose. Others are serious, like developmental delays caused by the build-up of toxins. (Kennedy Krieger Institute, 2025) Usually, these deficiencies are caused by genetics.
Types
There are various deficiencies. Some are very rare, while others can lead to conditions such as: (Nemours KidsHealth, 2023)
Lactose Intolerance
This is caused by not having enough of the enzyme that breaks down lactose, a sugar found in milk, leading to gas and bloating.
Tay-Sachs Disease
An often fatal disease caused by a missing hexosaminidase, which is responsible for breaking down fats
Gilbert’s Syndrome
This is caused by a missing enzyme that removes waste product (bilirubin) from the blood, leading to bilirubin buildup and
Jaundice or yellowing of the skin and whites of the eyes
Galactosemia
This leads to slow growth and trouble gaining weight, which is caused by the missing galactose-1-phosphate uridylyltransferase (GALT), which helps break down a sugar called galactose.
Phenylketonuria (PKU)
This is caused by having too little phenylalanine hydroxylase, which breaks down a protein called phenylalanine, causing brain damage.
Morquio Syndrome
This is caused by having too few enzymes that break down glycosaminoglycans, a type of sugar molecule.
This leads to bone and growth abnormalities.
Wilson’s Disease
A liver disease is caused by a missing protein that helps break down copper in the body.
Enzyme Production Support
Eat a healthy, well-balanced diet of fruits and vegetables to support enzyme production. Avoid processed foods, especially those that are very fatty (Johns Hopkins Medicine, 2025). The body produces all the necessary enzymes unless the individual has a genetic condition. Supplements aren’t usually required, but they can help with lactose intolerance or digestion in cystic fibrosis patients. (Nemours KidsHealth, 2023)
One supplement type, pancreatic enzyme replacement therapy (PERT), is available. PERT is an FDA-regulated prescription medication prescribed to patients with serious illnesses such as cystic fibrosis. (U.S. Food and Drug Administration, 2019)
Injury Medical Chiropractic & Functional Medicine Clinic
Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, and prevent injury. Regarding musculoskeletal pain, specialists like chiropractors, acupuncturists, and massage therapists can help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal issues.
Chiropractic Care and Metabolism: The Hidden Link
References
National Human Genome Research Institute. (2025). Enzyme. Retrieved from https://www.genome.gov/genetics-glossary/Enzyme
U.S. Food and Drug Administration. (2019). FDA approves new breakthrough therapy for cystic fibrosis. Retrieved from https://www.fda.gov/news-events/press-announcements/fda-approves-new-breakthrough-therapy-cystic-fibrosis
For individuals struggling with constipation, a common digestive issue, could performing abdominal self-massage help bring relief?
Abdominal Self Massage
Constipation refers to having a bowel movement fewer than three times per week. In addition to stress, certain lifestyle issues can lead to constipation, including not getting enough fiber, exercise, and proper hydration. Many also experience constipation while traveling. Abdominal self-massage involves gently massaging the stomach with your hands, either in a circular motion or with strokes, to improve digestion, relieve constipation, and reduce bloating. Performing self-massage on and around the abdomen can help ease constipation in several ways, such as stimulating the muscles, producing bowel movements, and soothing chronic stress. (Sinclair M. 2011)
Massage and Constipation
Abdominal massage can provide several benefits, including:
Stimulates and Improves Digestion
Massage stimulates the muscles and nerves that control digestion, promoting bowel movements and reducing constipation.
Reduces Bloating
Massaging the abdomen may help to reduce bloating and gas by gently moving fluids and gases through the digestive system.
In addition, it can help soften stool, speed up the movement of stool through the gut, and reduce the need to use laxatives. (University of Michigan Medicine, 2021)
Relieves Constipation
Abdominal massage can help with constipation by encouraging bowel movements.
Reduces Pain and Discomfort
Some find that abdominal massage helps to reduce pain and discomfort related to digestive issues.
Massage can help relax tense abdominal muscles and reduce pain associated with conditions like irritable bowel syndrome (IBS).
Improved lymphatic drainage
Massage helps move lymphatic fluid, which carries waste products and toxins away from the abdominal area.
Research
Although massage isn’t a standard treatment for constipation, some research shows it may help restore regularity. A report reviewed several clinical trials focusing on abdominal massage and its use as a treatment for chronic constipation. The results showed that abdominal massage may provide relief by promoting peristalsis, a series of muscle contractions that help move food through the digestive tract. The report also found that massage may help lessen colonic transit time, which is when digested food passes through the colon or last segment of the digestive tract. The report determined that abdominal massage can help alleviate constipation-related pain and discomfort. (Sinclair M. 2011)
In clinical trials, individuals with constipation reported improved quality of life after abdominal self-massage. However, some research suggests that using abdominal massage for constipation relief will not decrease the use of laxatives, the most commonly used treatment. (Lämås K. et al., 2009)
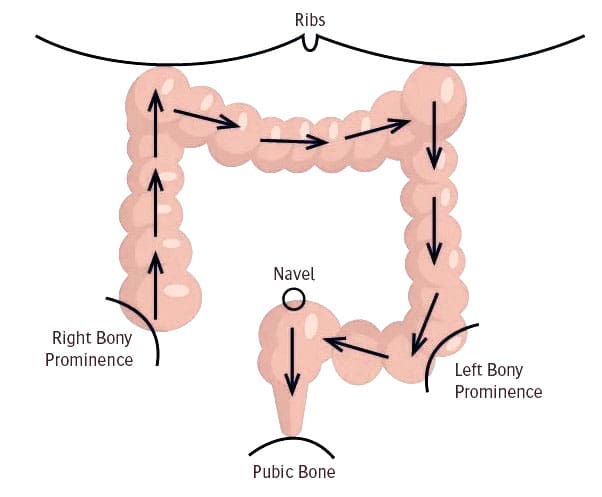
How to Massage
Various massage techniques may help relieve constipation and promote bowel movements. These are typically performed while lying down.
One technique involves placing the palm on the abdomen and making small, circular, clockwise motions around your belly button.
Individuals can also widen these circles so that the massage covers their entire abdomen.
Another technique begins by placing your hand below your breastbone, then gliding that hand down the length of your abdomen in one smooth stroke.
Repeat the movement with the other hand and continue this cycle for a few minutes.
When practicing self-massage, use light and gentle pressure, then gradually increase the pressure.
If you experience pain or tenderness, lighten up and return to a comfortable pressure level.
Try performing massage twice daily, aiming for a 20-minute session. Incorporating deep breathing into each session may also help. Before trying a massage or any home remedy, it is recommended to discuss it with a healthcare provider to see if it’s appropriate and safe. Pregnant women, for example, should avoid any massage on their abdomen. Constipation can sometimes signal an underlying condition that requires medical treatment, such as an underactive thyroid. Other symptoms like abdominal pain may be present, but sometimes constipation may be the only symptom.
Other Remedies
Self-massage alone is unlikely to treat chronic constipation; the goal should be to improve overall digestion to keep the organs functioning properly. To maintain regularity, it’s essential to drink plenty of water daily, eat enough fiber-rich foods, and engage in physical activity. Other alternative treatments include therapies like:
Acupressure
Biofeedback
Probiotics
Before trying self-massage, consult a medical caregiver to ensure it is safe and correct for the individual. Abdominal massage may not help with painful bloating caused by disease, infection, or other reasons.
Injury Medical Chiropractic & Functional Medicine Clinic
Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, and prevent injury. Regarding musculoskeletal pain, specialists like chiropractors, acupuncturists, and massage therapists can help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal issues.
Massage Therapy Rehabilitation
References
Sinclair M. (2011). The use of abdominal massage to treat chronic constipation. Journal of bodywork and movement therapies, 15(4), 436–445. https://doi.org/10.1016/j.jbmt.2010.07.007
University of Michigan Medicine. (2021). Self-abdominal massage. https://www.med.umich.edu/1libr/MBCP/AbdominalSelfmassage.pdf
Lämås, K., Lindholm, L., Stenlund, H., Engström, B., & Jacobsson, C. (2009). Effects of abdominal massage in management of constipation–a randomized controlled trial. International journal of nursing studies, 46(6), 759–767. https://doi.org/10.1016/j.ijnurstu.2009.01.007
Looking for GI disorder treatment? Learn about the latest strategies and methods to manage your condition effectively.
What Are GI Disorders?
How often does a huge lunch leave you feeling bloated? Have you ever had gastrointestinal inflammation or constipation? Or do you have muscles and joints that are stiff? Environmental variables may disrupt the gastrointestinal system and produce several overlapping risk profiles in the body by extending their effect onto the musculoskeletal system. This can result in pain-like sensations that often resemble musculoskeletal illnesses, although many individuals are unaware of this. Depending on their severity, gastrointestinal (GI) problems are often frequent and may be difficult to treat, with major medical and social repercussions. In 2018, Malone et al. Gastric reflux disease (GERD), small intestinal bacterial overgrowth (SIBO), and irritable bowel syndrome (IBS) are a few prevalent GI disorders. In the musculoskeletal system, GI issues may be a contributing factor to persistent discomfort, inflexible joints, and muscular dysfunction. Understanding the relationship between the stomach and the musculoskeletal system helps many people find practical, non-surgical solutions that may alleviate pain and enhance their quality of life.
How GI Disorders Affect The Gut & Musculoskeletal System
Many individuals question how environmental variables might impact their muscles and intestines, and they play a significant role in the development of GI illnesses. One environmental component that might have an impact on the muscles and intestines is stress. A person’s physical and mental health may be impacted by stress, which can alter how the gut bacteria react and result in gastrointestinal diseases. In 2011, Konturek et al.
Inflammation & Systemic Effects
When GI illnesses begin to impact the body, they lead to inflammation and adhere to the afflicted region, resulting in problems with the stomach. When the gut system is affected by inflammation, it may cause low-grade inflammation, compromise the integrity of the gut barrier, and interfere with normal food and nutrient digestion. In 2024, Cassini et al. This may result in inflammatory chronic gastrointestinal disorders such as ulcerative colitis or Crohn’s disease. This may then cause cytokines and inflammatory mediators to be released into the bloodstream, which can lead to systemic inflammation in the musculoskeletal system, resulting in symptoms including tiredness, joint stiffness, and muscle soreness.
Nutrient Malabsorption & Deficiencies
Chronic diarrhea, IBD, and celiac disease may all affect how nutrients are absorbed, resulting in vitamin and mineral deficiencies that can cause joint pain, weakness, and cramping in the muscles that are often confused with fibromyalgia or arthritis.
Gut Dysbiosis & The Nervous System
The neurological system and the digestive system, often referred to as the “second brain,” have a special interaction. Dysbiosis, or an imbalance in gut bacteria, may lead to the development of a leaky gut since the gut contains trillions of bacteria and aids in the transportation of nutrients from meals to other bodies. Toxins may enter the circulation and set off the immune system as a result. This results in systemic inflammation and musculoskeletal pain, which impacts the quality of life and pain of the musculoskeletal system from the stomach. (Casini and others, 2024) In addition, the gut-brain axis regulates muscular contraction and pain perception.
Visceral-Somatic Reflexes & Referred Pain
Referred pain patterns, in which the musculoskeletal system experiences visceral discomfort, may be caused by GI problems. Visceral pain hypersensitivity manifests as persistent stomach pain or discomfort (Farmer & Aziz, 2009). For instance, IBS might result in lower back and pelvic pain because of visceral-somatic responses, but GERD can produce chest and upper back pain.
Fighting Inflammation Naturally: Video
Functional & Nonsurgical Approaches To Reduce GI Pain
The following non-surgical, evidence-based methods may be used to treat musculoskeletal and intestinal discomfort:
Dietary Modifications
A nutritious diet is a good place to start when making little adjustments to enhance gut health. A balanced diet may help the body develop, mend, and produce energy. It can also influence and control a number of vital bodily processes, including hormones in the gastrointestinal tract. El-Salhy, 2019. By avoiding trigger meals that result in overlapping pain sensations, including foods high in omega-3s and polyphenols may help lessen the inflammatory effects from the stomach. GI issues may be treated using the following diets:
Elimination and Anti-Inflammatory Diet
Diet of FODMAP.
Pro-& Prebiotics
Probiotics and prebiotics may aid in the restoration and balancing of the gut flora in terms of gut health. Prebiotics use foods high in fiber to nourish the good bacteria in the stomach and promote gut health, while probiotics include good bacteria that help balance the gut microbiota and lower inflammation. By combining these two, intestinal inflammation may be avoided by reestablishing the dynamic equilibrium between the host defense systems and microbiota in the intestinal mucosa. (Dhaneshwar & Roy, 2023)
Stress Management
Reducing environmental stresses that lead to gastrointestinal illnesses and musculoskeletal discomfort also helps the body relax and ease tight muscles. Among the methods individuals may use are:
Meditation and Mindfulness: Progressive muscular relaxation, yoga, and deep breathing may all help people feel less discomfort and less sensitive to their stomachs.
Cognitive behavioral therapy, or CBT, may help enhance pain tolerance and manage GI symptoms brought on by stress.
Manual Therapies
GI conditions linked to musculoskeletal discomfort may be reduced using manual therapy. In order to assist strengthen and stretch weak muscle groups and lessen the body’s inflammatory effects, massage therapists, physical therapists, and chiropractors may use a variety of treatments. Among these treatments are:
Osteopathic Manipulative Therapy (OMT): Enhances gastrointestinal motility and relieves referred pain.
Visceral manipulation is a manual treatment that eases musculoskeletal tension and improves digestion by releasing abdominal limitations.
Massage therapy may ease back and abdominal muscular tension and lessen gastrointestinal symptoms associated with stress.
Acupuncture
By activating the autonomic nervous system, acupuncture has been shown to enhance stomach motility and lessen discomfort associated with IBS. To alleviate a patient, acupuncturists insert tiny, thin needles into different bodily acupoints. Neuromodulation, intestinal barrier restoration, and gut microbiota adjustment are all part of acupuncture. (Li and others, 2023)
Conclusion
The musculoskeletal system and gastrointestinal illnesses interact in a unique way because their risk profiles overlap and correlate. Treatments to lessen GI issues may be more successful when this relationship is understood. Functional, non-surgical methods including movement-based treatments, manual therapies, stress management, gut microbiota maintenance, and dietary modifications may provide comprehensive relief from GI-related musculoskeletal pain. These little adjustments to a person’s daily schedule, such as regular exercise or a balanced diet, may help address the underlying cause of dysfunction and provide long-lasting relief and enhanced wellbeing.
Injury Medical & Functional Medicine Clinic
We associate with certified medical providers who understand the importance of the effects of GI disorders on not only the gut system but also the musculoskeletal system. While asking important questions to our associated medical providers, we advise patients to implement small changes like physical activities and small dietary changes to their diet to reduce the chances of GI disorders from returning. Dr. Alex Jimenez, D.C., envisions this information as an academic service. Disclaimer.
References
Casini, I., Massai, L., Solomita, E., Ortenzi, K., Pieretti, S., & Aloisi, A. M. (2024). Gastrointestinal Conditions Affect Chronic Pain and Quality of Life in Women. Int J Environ Res Public Health, 21(11). https://doi.org/10.3390/ijerph21111435
El-Salhy, M. (2019). Nutritional Management of Gastrointestinal Diseases and Disorders. Nutrients, 11(12). https://doi.org/10.3390/nu11123013
Farmer, A. D., & Aziz, Q. (2009). Visceral pain hypersensitivity in functional gastrointestinal disorders. Br Med Bull, 91, 123-136. https://doi.org/10.1093/bmb/ldp026
Konturek, P. C., Brzozowski, T., & Konturek, S. J. (2011). Stress and the gut: pathophysiology, clinical consequences, diagnostic approach and treatment options. J Physiol Pharmacol, 62(6), 591-599. https://www.ncbi.nlm.nih.gov/pubmed/22314561
Li, X., Liu, S., Liu, H., & Zhu, J. J. (2023). Acupuncture for gastrointestinal diseases. Anat Rec (Hoboken), 306(12), 2997-3005. https://doi.org/10.1002/ar.24871
Malone, M., Waheed, A., & Samiullah, S. (2018). Functional Gastrointestinal Disorders: Functional Lower Gastrointestinal Disorders in Adults. FP Essent, 466, 21-28. https://www.ncbi.nlm.nih.gov/pubmed/29528206
Roy, S., & Dhaneshwar, S. (2023). Role of prebiotics, probiotics, and synbiotics in management of inflammatory bowel disease: Current perspectives. World J Gastroenterol, 29(14), 2078-2100. https://doi.org/10.3748/wjg.v29.i14.2078
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine