Stretching is often an outstanding complement to chiropractic care. Blood flow to the muscles is increased and it helps lower the risk of injury and improves physical performance. More importantly, stretching is good for the joints, helping them function through their full range of motion. Additionally, some studies show that muscles work and move more effectively when they are stretched regularly. These benefits of stretching make it a great practice to incorporate into your daily routine, especially between chiropractic treatments.
The muscles all along the spine respond well to stretching. However, sometimes it is difficult to manipulate specific muscle groups and get a thorough stretch.
The cervical spine is a prime example. Although the neck turns in so many ways, finding positions that provide an effective stretch are surprisingly difficult.
These three stretches effectively work the muscles through the neck and shoulders�and are simple enough to do at home whether you are between chiropractic appointments or if you wake up with a crick in your neck.
Before You Stretch
If you are under a chiropractor�s care, you should check with him or her before you start a stretching program. This is especially important if you have a neck injury or have a spinal condition that causes deterioration or pain.
When you begin stretching, you may feel a little discomfort, but it is important to note that it should never cause pain or worsen it. If this occurs, or if it just doesn�t feel �right,� you should stop immediately and call your chiropractor.
Neck and Trap Stretch
If standing: Stand up straight with your pelvis slightly tucked (not swayback), feet shoulder�s width apart, knees soft.
If sitting: Sit up straight with your feet flat on the floor.
1. Drop your shoulders and roll them slightly back. Let your arms hang down.
2. Reach behind your back and, with your left hand, grasp your right wrist. If you can�t reach to grasp your wrist, grab your fingers. If you can�t reach your fingers, sit in a straight back chair and put your right arm as far behind you as you can and slide your right hand under your right buttock to provide stability.
3. If clasping your hands behind you, gently pull your arm behind you to the left. If unable to reach behind you, drop your right shoulder.
4. At the same time, tilt your head to the left, bringing your ear to your shoulder but don�t raise your left shoulder. You will feel the stretch all along the right muscles of the neck.
5. Hold the stretch for 15 to 30 seconds.
6. Do the same movement for the left side.
7. Repeat the full move 3 to 5 times.
Gentle Neck Extension
If standing: Stand up straight with your pelvis slightly tucked (not swayback), feet shoulder�s width apart, knees soft, hands relaxed and at your sides.
If sitting: Sit up straight with your feet flat on the floor, hands relaxed and at your sides.
If lying down: Lie flat on the floor. If necessary, put a pillow under your knees to take pressure off of the lower back. Stretch your arms down by your side.
1. Push your shoulders down towards your feet.
2. Tuck your chin to your chest but don�t let your shoulders lift.
3. Slowly raise your chin, feeling the stretch along the front of your neck. Hold the position for 20 to 30 seconds.
4. Return your head to its normal, upright position for 30 seconds. Repeat the entire movement 5 to 7 times.
Stretch for Traps
If standing: Stand up straight with your pelvis slightly tucked (not swayback), feet shoulder�s width apart, knees soft, hands relaxed and at your sides.
If sitting: Sit up straight with your feet flat on the floor, hands relaxed and at your sides.
If lying down: Lie flat on the floor. If necessary, put a pillow under your knees to take pressure off of the lower back. Stretch your arms down by your side.
1. Start with your head in the normal, upright position.
2. Bend your neck to the right side, moving your ear towards your shoulder.
3. Raise your left hand to your head and apply gentle pressure to facilitate the stretch while drawing up your left shoulder. Hold for 20 seconds.
4. Return to your starting position.
5. Repeat the same movement on the right side.
6. Do 3 to 5 sets.
Neck Pain Chiropractic Treatment
XYMOGEN 6 Day Detox Kit
6 Day Detox Kit�is designed to renew and enhance the body�s cleansing and detoxification capabilities. It combines four specially selected XYMOGEN formulations: ColonX�, Drainage�, ProbioMax��Daily DF, and OptiCleanse�GHI. When taken together, as recommended within the 6-Day Detox Guide, these complementary formulas work in concert to encourage the various detox-linked systems and organs of the body to process and eliminate waste and toxins.*
6 Day Detox Kit�includes 1 bottle of OptiCleanse GHI Vanilla Delight, 1 bottle of ColonX 60c, 1 carton of ProbioMax Daily DF 30c, 1 bottle of Drainage 1 fl oz, and 1 20 oz Shaker Bottle.
Today we will discuss the fundamentals of functional medicine and how you can build a healthy doctor-patient relationship.
If you visit the doctor because you�ve been experiencing migraines, eczema, irritable bowel syndrome and depression, you�re most likely going to be referred to four different specialists and you may even be prescribed four different drugs and/or medications, at minimum. A functional medicine approach understands that there may be common underlying health issues which can be causing a patient�s symptoms. Once you get to the source of the problem, you can fix the health issues that create the symptoms.
Functional medicine asks, �Why do you have those symptoms and how can we treat the source of the problem and improve your overall health and wellness?� rather than, �What disease do you have and what drug do you use to treat it?�
What is Sick Care vs Health Care?
Hello everyone, my name is Dr. Alex Jimenez. I�m a chiropractor and practicing functional medicine doctor in El Paso, Texas. I�m so happy to introduce you to part one of �Taking Control of Your Healthcare�, where we will discuss the differences between �Sick Care and Health Care�. So, I frequently hear people talk about how difficult it is to find the right doctor, someone who is willing to work with them, who listens to them, and who is open to meeting their demands while teaching them everything they need to know about their problems. A doctor who accepts innovative advances in science and system approaches to determine the source of the problem. This is known as functional medicine, and we will discuss more of that in a minute.
My goal right now is to show you how you can find the right doctor and build the best relationship with them to get the care you deserve. It�s important to ask your doctor several questions to determine if they are the appropriate fit for you, if they�re willing to work with you, to listen to you, and if they�re open to your requests as well as learning about problems they�re not familiar with and following new treatment approaches. By way of instance, if the doctor you choose says that nutrition has nothing to do with disease, then you should probably go find another doctor. Now let�s discuss what questions you should ask your doctor regarding your overall health and wellness in order to be informed about what�s happening in your own body.
I�ve talked to patients who have visited numerous doctors in hopes of finding an answer as to why they�re not feeling well or have some type of disease. Many are frequently referred to one or more specialists and, in some cases, they�re given Prozac, or they�re told that their symptoms are all in their head or sometimes they�re even told that there�s nothing wrong with them after their lab results are all normal. And it�s frequently these same patients who are often sent to various doctors for each part of their body rather than being sent to a doctor who can diagnose and treat their body as a whole. If you go to the doctor and you have migraines, eczema, irritable bowel syndrome, and depression, in most cases, you�re going to be sent to four different specialists and you�re going to be given, at least, four different medicines instead of visiting a specialist who can understand the underlying source of the problem and treat the root of the symptoms.
Have you ever visited a doctor who, after explaining your symptoms to them, said, �Oh, I did a full blood panel and everything came back normal.� This could mean one of two things, either you�re crazy or they�re missing something. And I�m sure they�re often missing something because they�re not looking in the right places for the answers. It�s like the guy who dropped his keys in the street and when his friend sees him looking under a lamppost, he says, �Hey, what are you doing?� He says, �Well, I�m looking for my keys.� �So, where did you lose them.� He says, �Well I lost them down the street.� �Then why are you looking here?� �Well, the light�s better here.� And unfortunately, that happens a lot in medicine. Doctors will look for answers where problems are easy to find. And that is the purpose of this article. To help you understand how you can find the source of the underlying health issues that are making you feel sick.
This reminds me of a case of a woman I saw in my office who had psoriatic arthritis, an autoimmune condition which caused her to have rashes all over her body along with joint pain and swelling. As a result, she was on large amounts of drugs and/or medications which added up to about $60,000 dollars a year or more. She also had other health issues, she had acid reflux, irritable bowel syndrome, pre-diabetes, migraines, insomnia and depression. This woman visited many different specialists and she was taking prescriptions to address each of her symptoms. When it came time for me to see her, all I did was get to the source of the problem.
So, during diagnosis, I said to myself, �Okay, this patient has inflammation, but what�s the cause of her inflammation?� And instead of referring her to numerous other specialists so she could receive medicine for her migraines, acid reflux, depression, etc., I said to myself, �Oh, all of these symptoms are inflammatory, so what�s the root of the inflammation?� Well it turns out that the patient had problems with her gut all along. I then helped her clear out the �bad bugs� in her gut by recommending her an anti-inflammatory diet, I included some supplements, fish oil, vitamin D, probiotics. Honestly, really basic natural remedies. When she returned six weeks later, all of her symptoms had disappeared. She had gotten off all of her prescription medicines and she had lost 20 pounds. I didn�t tell her to stop taking her meds, she just did it on her own. It was absolutely remarkable and that�s what happens when you treat the source of a patient�s underlying health issues. And you don�t have to do a lot to get to the root of the cause.
I understand that it may not always be possible to work with a doctor who�s trained in functional medicine, which we will discuss what that means in a minute, however, it is possible to find a doctor who�s going to be willing to work with you, who�s going to listen, who�s going to have an open mind and who�s going to be your partner during your journey to overall health and wellness. Throughout this article, I�m going to discuss conventional lab testing as well as innovative functional medicine lab testing, demonstrating it all for the purpose of creating well-being rather than viewing it all from the perspective of the disease in order to find the source of a patient�s health issues and correct imbalances through a functional medicine approach.
Taking Control of Your Health Care vs Sick Care
Functional medicine is often referred to as the future of medicine, but it�s currently being offered by many doctors if you visit the right place. The purpose of functional medicine is to diagnose and treat the root cause of a variety of diseases by evaluating the body as a whole, rather than by analyzing each collection of organs independently through separate specialists. Functional medicine treats the whole system, not just the symptoms. Doctors who practice functional medicine frequently ask themselves, �Why does the patient have these symptoms and how can I fix the root causes and improve their overall health and wellness?� rather than �What disease does the patient have and what drug and/or medication do they use to treat it?�
I�ve been a practicing chiropractor for over 25 years. And I�ve witness countless of miracles every day. My patients don�t simply find relief from their symptoms, they truly achieve overall well-being. Unfortunately, our current healthcare system is broken. Many doctors are tremendously affected due to time constraints set by insurance companies to pay bills, causing them to rush through their appointments. In turn, this continuous cycle can frequently end up leaving patients with unanswered questions followed by frustration. Our current healthcare system makes people feel powerless, often keeping them stuck in disease.
As a part of this healthcare system, it�s important that we understand that some diseases are not as easily treatable as a cold. Several diseases also don�t just develop randomly. The majority of diseases which exist today are related to your environment and how these external as well as internal factors alike interact with your genes and lifestyle to influence your health and wellness.
What we know today as the �conventional medicine� approach is typically referred to as the �name it, blame it, and tame it� game. First, the doctor will diagnose the patient and provide them with a label, by way of instance, they say a patient has depression. Now they have the name of the disease. And finally, the doctor will treat the disease with prescription drugs and/or medications. In the end, the patient is left taking an antidepressant. However, depression can be caused by a wide array of factors and the solution isn�t necessarily an antidepressant. Not only is this type of practice outdated, it�s actually considered to be quite unsafe in the long-run. And it�s often not providing patients with the results they need. People are being misdiagnosed and mistreated, frequently being left sick without really getting the proper care they deserve.
Conventional medicine can also be helpful at the very end stages of some diseases as well as for acute diseases. If you have an emergency or you�re feeling very sick, if you break a bone, or if you have a raging infection, conventional medicine, acute care, drugs and/or medications can be the right solution and we should be highly grateful for them. But this is not the approach we need to prevent and cure chronic diseases. If we actually understood how to care for our bodies the way we should, most of us wouldn�t be feeling as sick as we do. And many people will walk around feeling sick, but you don�t have to, it�s not normal. Many doctors now understand that a change is required to turn our entire sick care system into one that actually supports health care.
I would like to empower you to help transform the future of the medicine field by taking your well-being into your own hands. Throughout the next articles I�m going to share with you how you can find a doctor that takes consideration of your personal values and beliefs so you can achieve the results you�re looking for while in a safe and comfortable environment. You can learn how to be your own health advocate and become a true partner with your doctor. And there are many other doctors and functional medicine practitioners like me who are waiting to help.
Furthermore, I�m going to share with you how you can find the best doctor and I�m also going to provide you with many other tools to help you be the leader of your overall health and wellness. How you can take control and make the calls for your own well-being. Including what lab work you should ask your doctor for, and how to understand what the information means and what you should do with it. One of the most common ways doctors utilize labs is to evaluate what goes wrong when a patient isn�t feeling well and to analyze the end of a continuum of disease. If your liver function changes your liver cells may already be dying. If they�re normal, however, many doctors say, �Oh, you�re normal.� But it may actually not be normal. The good news is that you may be able to find imbalances sooner in order to treat them in time.
Although it�s slowly been changing, many doctors have the custom of not giving patients their actual lab tests. And if this isn�t the case, several doctors don�t provide detailed explanations of patient�s lab tests other than, �Your lab tests came back normal,� or �Your cholesterol is a little high,� or, �Your blood sugar is a little high.� As a chiropractor, I believe that everyone should have access to their lab tests and that these should be explained to the patient. We need to start democratizing health care. And this has become more fundamental than ever before.
Now why is this so important? Approximately 133 million Americans are affected by chronic disease and that number is even higher depending on how chronic disease is defined. About one in two individuals in the United States has pre-diabetes or type 2 diabetes. The rate of a variety of diseases, including digestive problems, allergic diseases, heart disease, autoimmune diseases, cancer, obesity, type 2 diabetes, and dementia have all been increasing. Where approximately one in three kids born today will have type 2 diabetes in their lifetime and one in two people over the age of 85 and one in four people over the age of 75, are going to have dementia.
Health issues like these are manifesting throughout our population at a tremendous rate and they can affect everyone, either personally or through the suffering of a loved one. Additionally, chronic diseases have caused a dramatic economic burden within our country.
However, the reason why I�m so happy to share this article with you is because there�s a lot we can do to change the future of our healthcare system. Many doctors and I have the knowledge we need to decrease or even eliminate the suffering of so many people and to save the economy. Every day in my office, I see patients recover their quality of life after they were expecting to suffer their entire lives due to chronic diseases such as, acid reflux, irritable bowel syndrome, headaches, fatigue, and arthritis, among other health issues. Problems like allergies, hormonal issues, obesity, diabetes, heart disease, autoimmune diseases, and depression. And patients can truly get better and thrive, not just cope with or manage their disease. Within a few months, even weeks, of visiting me and my staff, the lives of patients can tremendously change.
Functional medicine looks at how the human body functions as a whole, and its most basic approach is to first understand the factors, genes, and triggers for disease, and how lifestyle and environmental inputs, including diet, stress, toxins, allergens, and microbes, interact with the human body to create imbalances which can commonly lead to chronic health issues.
So, let me take a moment to discuss something. The human body is a system. And this entire system is made up of smaller, �mini-systems� which are all dynamically interacting. But, when one or more of these systems get out of balance, you can become sick. And when these systems get in balance again, you become healthy. And that�s what functional medicine is. Functional medicine is simply understanding what causes imbalances in the human body and treating them to restore balance and provide essential needs to all the systems in the human body. Creating overall health and wellness. It is the science of creating well-being. And doctors achieve this by utilizing a patient�s detailed medical history, combined with targeted lab tests. Doctors who follow a functional medicine approach, like me, by way of instance, generally evaluate your gut and your microbiome, which not many doctors look into. We also want to look at your immune system and whether inflammation is affecting you, something which we refer to as defense and repair. And we want to know how your mitochondria produces energy from food and oxygen. Functional medicine practitioners want to know if you have any dysfunctions in energy production, which is typically the source of numerous diseases, such as Alzheimer�s disease and autism, type 2 diabetes, and fatigue, among many others. We also determine your toxic load and your ability to detoxify, involving the function of other communication systems in your body, such as your hormones. Finally, we evaluate your structural system, from your cells to your biomechanical structures and how these interact with your beliefs, emotions, and more.
I�ve used these procedures, over and over again, to help reverse chronic disease in my patients and educate them on how to achieve long-term health and wellness, all while feeling like the best versions of themselves. We are all given the opportunity to cure or tremendously improve health issues or problems which are often misdiagnosed and mistreated by conventional medicine. Functional medicine provides the opportunity to discover overall well-being at any age.
As a matter of fact, I treated a man named, George, who was 63 years old, weighed 300 pounds, and who had a variety of health problems. He had acid reflux, sinus problems, diabetes, angina heart failure, prostate problems, sexual dysfunction, and edema in his legs. And as a result, he was under a wide array of prescription medicine. He came into my office one day and he said to me, �Can you help me.� I said, �Yes, but you will have to do everything I say.�
So, I recommended him an anti-inflammatory diet, consisting of whole foods and a low intake of sugar, and I advised him to take a variety of supplements in order to optimize his nutrition, all while I guided him into participating on exercises and physical activities. Within a year, it was like a miracle, the patient had lost 155 pounds, he reversed all of his health issues and he stopped using his prescription medicines. Now, he�s planning the rest of his life, when before he came to visit me, he was planning the end of his life. Another patient I treated, named Isabel, struggled with an autoimmune disease. She was only 10 years old and she was already under a pile of drugs, steroids, immunosuppressants, and even chemo drugs. It turns out that her diet and exposure to heavy metals was affecting her gut and causing inflammation. Now, I simply treated the source of her problems and her autoimmune disease went away. She stopped using her prescription medicines and, altogether, her quality of life improved and she thrived.
Functional medicine is an alternative treatment approach which focuses on the interactions between external or environmental factors as well as internal factors associated with the gastrointestinal, endocrine, and immune systems of the human body. Finding the right doctor can make a big difference when it comes to getting health care over sick care. Functional medicine treats the source of the problem rather than treating the symptoms alone. As a chiropractor and functional medicine practitioner, my primary goal is to provide patients with the care they deserve for their health issues as well as to educate them on the fundamentals of functional medicine. The purpose of this article is to help patients find the right doctor and build a healthy doctor-patient relationship. Dr. Alex Jimenez D.C., C.C.S.T. Insight
Sick Care vs Health Care Overview
Over the next few weeks, we�re going to go through some of the fundamental principles and concepts that helped me find the underlying cause of disease through the use of functional medicine. And that will help you achieve overall health and wellness.
In our next article, I�m going to teach you how you can take your own measurements to understand your own well-being and what you can do to improve your vital signs. This procedure is going to help provide you with important baseline data and information to help you better understand your health risks. It�s also going to allow you to evaluate and analyze your own progress as you work towards your ultimate wellness goals.
In the third article, I�m going to try to cover everything about nutrition. I will explain how we can test your nutritional status and how you can utilize food as treatment to start changing your overall health and wellness as soon as possible. Your diet is one of the most effective parts you can control to create a healthier lifestyle. I�ll be sharing tips and tricks for a better nutrition.
Because hormones can impact nearly every aspect of our health, we�re also going to be highlighting them in the fourth article. Unfortunately, a majority of doctors do not understand what optimal hormone levels should look like nor are they aware of the proper methods for testing hormones. I will be preparing you to have an effective conversation with your doctor on which type of hormone test actually matters, what they mean, and what you can do about them.
In article five I�m going to focus on heart health, such as high blood pressure, high cholesterol, and cardiovascular disease. These conditions are extremely common, and unfortunately, conventional medicine frequently tries to treat them by simply controlling the symptoms. Lowering cholesterol, lowering your blood pressure, that does not solve the root cause of the problems. Most of the time, increased levels of blood sugar, obesity and diabetes are the cause of cardiovascular disease. I�m going to demonstrate how we can prevent and reverse these diseases using lifestyle modifications, including nutrition, to improve heart health.
In the sixth article, I�ll be discussing obesity and diabetes, something I�ll be frequently referring to as diabesity. Metabolic disorders ranging from minimal fat and moderate insulin resistance to pre-diabetes to type 2 diabetes. The great thing about these metabolic disorders, however, is that they are completely reversible. But most conventional doctors don�t know it�s reversible. I�m going to help teach you how you can recover a healthy metabolism and how you can reverse the range of problems involved in diabesity, which as you will learn, are a lot of different diseases.
In article seven, I�m going to talk about the immune system, particularly discussing hidden inflammation and disease. As inflammation is described to be the underlying cause of a majority of chronic diseases, we continue to see increasing rates of autoimmune diseases and allergies, which are signs that our immune systems are not functioning properly. However, inflammation is also associated with obesity, type 2 diabetes, heart disease, cancer, dementia, and even depression. I�ll explain how you can talk to your doctor about testing for inflammation, what the markers mean, and how you can care for your immune system on a deeper level.
In article eight, we�re going to move into the topic of the metabolism and mitochondria. Now every one of our cells hold hundreds or thousands of mitochondria, the energy generators of our cells. When these become damaged, we can suffer from a variety of problems, including pain, memory loss, fatigue, and many other symptoms. I�m going to explain how we can care for your mitochondria at the cellular level and why this is a vital piece of optimal health and wellness.
Then, in article nine, we�re going to explore the meaning of detoxification, or the human body�s innate detox system and why this is an essential part of the healing process. From mold to heavy metals, and other toxins, I�m going explain what you need to know to avoid toxins and how you can eliminate those that you are already carrying to optimize your capability to detoxify. With the amount of toxins we�re exposed to on a regular basis, it�s important to identify the causes that may be affecting you and how you can begin eliminating them right away. Fortunately, this is something you can easily do to create a cleaner lifestyle for you and your loved ones.
Finally, in article ten we will be talking about digestion. Digestive health is one of the most commonly discussed topics in functional medicine. Because our digestive system is the center of our health, by diagnosing problems in this system, we can improve everything from mental health, nutrient absorption, and cardiovascular risk to immune system function. In the tenth article, I�m going to guide you through the tests that are available for monitoring your gut health, as well as what you can do to improve your own digestive health, as soon as possible.
I�m so happy you�ll be joining me throughout this series of articles because the future of medicine depends on it. When you learn how you can impact your well-being by being proactive and by creating a partnership with your doctor, everything changes. Through functional medicine, you can also help transform our sick care system into an actual health care system.
So, let�s finish up this article with the questions you want to ask your doctor as you interview them to see if they can be a partner for you and your overall health and wellness. These are just a few high-level questions to start with your discussion. Are you willing to work with me as a partner for my well-being? Also, what�s your point of view on nutrition and health? Do you think food is medicine? Are you willing to give me copies of my test results and explain what they mean? The reason why we�re asking these questions is to make sure that your doctor is willing to work with you and understand the role of functional medicine.
I�m so happy to be a part of your journey to better health and wellness. Thank you very much for joining me today. The scope of our information is limited to chiropractic and spinal health issues as well as functional medicine topics and discussions. To further discuss the subject matter, please feel free to ask Dr. Alex Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topic Discussion:�Acute Back Pain
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief. �
Chronic pain caused by accidents and/or aggravated conditions can often be one of the primary reasons for depression in patients. When painful symptoms induce patients to struggle with their everyday physical activities, their mental health can be tremendously influenced. Chiropractic care utilizes spinal adjustments and manual manipulations which could help restore the initial integrity of the backbone. Patients describe how chiropractic care has helped them recover their well-being and they highly recommend Dr. Alex Jimenez, doctor of chiropractic, as the non-surgical choice for chronic pain and depression, one of a variety of other common health issues.
Chiropractic Relief
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused on treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
We want you to live a life that is fulfilled with more energy, positive attitude, better sleep, less pain, proper body weight and educated on how to maintain this way of life. I have made a life of taking care of every one of my patients.
I assure you, I will only accept the best for you�
If you have enjoyed this video and we have helped you in any way, please feel free to subscribe and recommend�us.
After a slip-and-fall accident,�Aracely Norte was limited�in her ability to work, that affected her quality of life. Due to chronic pain, Aracely had difficulty engaging in regular, everyday responsibilities. After hearing about El Paso, TX. Chiropractor, Dr. Alex Jimenez, from her lawyer, Aracely found relief from her chronic pain. Aracely describes how Dr. Jimenez cared for her injuries while he educated her about her health issues and the treatment he provided her with. Aracely highly recommends Dr. Jimenez as the non-surgical choice for chronic pain. Chronic pain is a common issue which can occur due to a variety of reasons, including injuries and underlying conditions, however, chiropractic care can help eliminate chronic pain symptoms.�
Chiropractic Rehab
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused on treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
We want you to live a life that is fulfilled with more energy, positive attitude, better sleep, less pain, proper body weight and educated on how to maintain this way of life. I have made a life of taking care of every one of my patients.
I assure you, I will only accept the best for you�
If you have enjoyed this video and we have helped you in any way, please feel free to subscribe and recommend�us.
Chronic pain is one of the most prevalent conditions in the United States, affecting an estimated 100 million Americans each year. To put that into perspective, that�s more than the number of people suffering from cancer, heart disease, and diabetes, combined.
Many of these chronic pain sufferers are looking for relief beyond pharmaceuticals which can have unpleasant and even harmful side effects. This has brought them to natural pain management methods like chiropractic care as well as natural substances like curcumin. For many people, these treatment options have brought them relief from the pain and help them return to a more normal lifestyle.
How does it work though? And, more importantly, can it work for you?
What is Curcumin?
Natural herbal turmeric capsules with fresh herb leaves and dry curcumin in paper
Curcumin is a spice that is a relative of ginger and is a component of turmeric. Often in the U.S., the terms curcumin and turmeric are used interchangeably. However, curcumin is what gives turmeric its bright yellow color.
While it is often found in curries and other traditional Indian food, it has also long been used to treat a variety of health issues including inflammation that causes pain in the body. These claims have been backed up by several studies that show the tasty spice has tremendous health benefits to offer.
These studies have shown that curcumin has strong anti-inflammatory properties although why it works is not yet completely understood. This information has prompted further studies to determine the efficacy of curcumin in treating a wide range of conditions including chronic pain.
One study examined the spice�s effects on people suffering from arthritis or joint pain. The results determined that turmeric extract (curcumin) supplements were just as effective as ibuprofen in relieving the pain in patients with knee osteoarthritis. It helped to reduce the inflammation that was causing the pain, bringing the patients much-needed relief.
Taking Curcumin for Better Health
You can get curcumin or turmeric supplements, but there is no standard dosage information available. Your chiropractor can advise you on how much to take and which supplement brands are the best.
You can also use the spice in the foods you eat and gain a good bit of the health properties that way. However, it may be more efficient and more comfortable to take curcumin or turmeric supplements, especially when you are treating inflammation and pain.
Curcumin is generally safe with very few side effects. As with any medication or supplement, some people are sensitive to the spice and may experience diarrhea and nausea.
However, that usually occurs at higher doses or after the patient has been using it for a long time. High doses could also pose a risk if the person has ulcers. It can also irritate the skin is applied topically.
If you are considering incorporating curcumin into your daily diet as a health supplement, you should first talk to your doctor or chiropractor to make sure it is safe for you. Women who are pregnant or nursing should not take the supplements.
People with conditions like diabetes, gallbladder issues, bleeding disorders, kidney disease, or immunity problems should take special care when using the supplement. Also, it can interact with medications like NSAIDs, aspirin, diabetes drugs, statins, blood thinners, and blood pressure medications so talk to your health professional, such as your chiropractor, before taking. They may adjust your dosage or recommend certain nutritional therapies to better support the supplement.
Your chiropractor can help you live a more natural, pain-free life and supplements like curcumin may be a part of that plan. They can help put you on the path to a life well lived.
Many healthcare professionals highly recommend that patients with multiple sclerosis, or MS, avoid dairy. Several research studies have demonstrated a high correlation between MS and dairy, especially cow�s milk. By way of instance, some of the proteins in cow�s milk are targeted by the immune cells of patients with multiple sclerosis. These include butyrophilin and bovine serum albumin, or BSA. Moreover, injecting those same cow�s milk proteins into test animals caused lesions to appear in their central nervous systems.
Some proteins in cow�s milk imitate part of the myelin oligodendrocyte glycoprotein, or MOG, the section of myelin believed to initiate the autoimmune reaction associated with multiple sclerosis. Furthermore, this can trick the immune system into initiating an attack on the MOG, subsequently causing demyelination. Another research study involving more than 135,000 men and women in the United States determined a connection between cow�s milk and the degenerative neurological disorder, Parkinson�s Disease. Researchers have speculated that dairy products, especially cow’s milk, may have a generally toxic effect on nervous tissue.
Lactose intolerance is common throughout the general population, and it is most notably frequent in Mediterranean, Asian, and African populations. People with lactose intolerance experience a variety of symptoms, including bloating, cramps, diarrhea, and nausea. Given the high potential risks for people with MS consuming dairy products, despite a lack of conclusive evidence, healthcare professionals recommend avoiding the consumption of dairy products, among other types of foods. The purpose of the article below is to discuss the nutrition facts in multiple sclerosis, including which types of foods patients with MS should avoid, such as dairy.
Abstract
The question whether dietary habits and lifestyle have influence on the course of multiple sclerosis (MS) is still a matter of debate, and at present, MS therapy is not associated with any information on diet and lifestyle. Here we show that dietary factors and lifestyle may exacerbate or ameliorate MS symptoms by modulating the inflammatory status of the disease both in relapsing-remitting MS and in primary-progressive MS. This is achieved by controlling both the metabolic and inflammatory pathways in the human cell and the composition of commensal gut microbiota. What increases inflammation are hypercaloric Western-style diets, characterized by high salt, animal fat, red meat, sugar-sweetened drinks, fried food, low fiber, and lack of physical exercise. The persistence of this type of diet upregulates the metabolism of human cells toward biosynthetic pathways including those of proinflammatory molecules and also leads to a dysbiotic gut microbiota, alteration of intestinal immunity, and low-grade systemic inflammation. Conversely, exercise and low-calorie diets based on the assumption of vegetables, fruit, legumes, fish, prebiotics, and probiotics act on nuclear receptors and enzymes that upregulate oxidative metabolism, downregulate the synthesis of proinflammatory molecules, and restore or maintain a healthy symbiotic gut microbiota. Now that we know the molecular mechanisms by which dietary factors and exercise affect the inflammatory status in MS, we can expect that a nutritional intervention with anti-inflammatory food and dietary supplements can alleviate possible side effects of immune-modulatory drugs and the symptoms of chronic fatigue syndrome and thus favor patient wellness.
Keywords:complementary alternative medicine, gut microbiota, inflammation, lifestyle, multiple sclerosis, nutrition
Introduction
Multiple sclerosis (MS) is a chronic, inflammatory, and autoimmune disease of the central nervous system (CNS), leading to widespread focal degradation of the myelin sheath, variable axonal and neuronal injury, and disabilities in young adults, mostly women. The disease is characterized by disseminated and heterogeneous perivascular inflammatory processes at the blood�brain barrier (BBB), with involvement of autoreactive T cells, B lymphocytes, macrophages, and microglial cells against brain and spinal cord white matter (McFarland and Martin, 2007; Constantinescu and Gran, 2010; Kutzelnigg and Lassmann, 2014).
Antibodies (Krumbholz et al., 2012), activated complement (Ingram et al., 2014), cytokines, mitochondrial dysfunction (Su et al., 2009), reactive oxygen species (ROS; Gilgun-Sherki et al., 2004), and matrix metalloproteinases (MMPs; Liuzzi et al., 2002; Rossano et al., 2014) may cooperate to yield the pathology.
From the clinical point of view, there are at least two main forms of the disease: the relapsing-remitting MS (RRMS; about 85% of clinical cases) and the primary-progressive MS (PPMS; about 15% of the clinical cases) (Dutta and Trapp, 2014; Lublin et al., 2014). In RRMS, which usually evolves in secondary-progressive MS (SPMS), relapses are associated with increased systemic inflammation and formation of lesions in the brain, followed by more or less complete remissions, whereas the pathogenesis of PPMS is characterized by progressive neurological damages rather than relapses and remissions.
At present, there are at least 10 disease-modifying therapies that have been found to slow disease progression and prevent some disability symptoms, but only in the case of RRMS. However, as the disease is complex in nature and unique in the individual course, no patient responds to therapy in the same way (Loleit et al., 2014). Similarly, there are no truly reliable biomarkers that allow for everyone to evaluate the effectiveness of treatment and it is therefore important to discover novel markers of the disease (Fernandez et al., 2014).
The lack of response to immune-modulatory therapies in the case of PPMS, otherwise effective in the treatment of RRMS, may be due to different pathogenic mechanisms acting in RRMS and PPMS. However, this is not true with regard to inflammation: A significant association between inflammation and neurodegeneration has been observed in the brain not only in acute and relapsing MS but also in the secondary and primary progressive MS (Frischer et al., 2009; Lassmann, 2013), and active MS lesions are always associated with inflammation (Kutzelnigg and Lassmann, 2014). Thus, inflammation must be the target for the treatment of both forms of the disease.
Linking Inflammation with Dietary Habits and Lifestyle
What causes the inflammatory processes in MS? MS is a complex disease, and the genetic and the immunological components are not sufficient to explain its origin. Actually, MS has a multifactorial nature and various environmental factors or metabolic conditions may have a role in its development (Ascherio, 2013): viral infections (Ascherio et al., 2012; Venkatesan and Johnson, 2014), heavy metal poisoning (Latronico et al., 2013; Zanella and Roberti di Sarsina, 2013), smoking (Jafari and Hintzen, 2011), childhood obesity (Munger, 2013), low vitamin D status (Ascherio et al., 2014), or incorrect lifestyle, including wrong dietary habits (Riccio, 2011; Riccio et al., 2011; Riccio and Rossano, 2013).
None of the above-mentioned environmental factors alone can explain the disease; however, the following considerations make more attractive the involvement in MS of dietary habits and lifestyle, rather than infections or smoking, as factors that may influence the course of the disease:
Geographical distribution: MS is more prevalent in Western countries with the highest income and most distant of the equator. Features of these countries are a sedentary lifestyle, a high-calorie diet rich in saturated fats of animal origin (Western diet), and low sunshine exposure (WHO and MSIF, 2008).
Effect of migration: With the migration from an area of high incidence of MS to another place with low incidence before age of 15 years, the low risk is acquired, while the migration after this age does not change the level of risk. This aspect may be linked with nutritional, rather than with infectious or toxicological environmental factors (McLeod et al., 2011).
Low availability of vitamin D: Another environmental factor related to diet and geographical distribution is the availability of vitamin D, which is lower at latitudes with lower exposure to sunlight. Patients with MS have a low content of vitamin D (Ascherio et al., 2014), but this is true also for other chronic inflammatory diseases (Yin and Agrawal, 2014).
Postprandial inflammation: High animal fat/high sugar and refined carbohydrate diet is associated with postprandial inflammation (Erridge et al., 2007; Ghanim et al., 2009; Margioris, 2009).
High body mass index: High body mass index (BMI) before age 20 is associated with 2� increased risk (Hedstr�m et al., 2012). Note that BMI is correlated with gut microbiota status.
Similarity with other inflammatory diseases related to wrong dietary habits: MS has some similarities with inflammatory bowel disease (IBD; Cantorna, 2012): both have low vitamin D and are influenced from environmental factors (Dam et al., 2013). Furthermore, glatiramer acetate (GA, or Copolymer 1/Copaxone) is beneficial in both diseases (Aharoni, 2013) and there is an increased incidence of IBD among MS patients.
How Food Affects the Course of Inflammatory Diseases: A Basic Approach
The observations reported above suggest that the nutritional status may influence the course of MS. However, the question arises of how dietary molecules could exacerbate or ameliorate MS symptoms, and in general how they could favor or downregulate inflammation at molecular level. In particular, it is important to clarify what are the targets of dietary molecules and the molecular mechanisms involved, if any.
Fundamentally, we can say that the food we consume has a broad impact on our development, behavior, health condition, and lifespan by acting on two main targets: (A) the cells of our body and (B) the commensal gut microbiota (Figure 1).
On one hand, different kind and amount of dietary factors can interact with enzymes, transcription factors, and nuclear receptors of human cells. This may induce specific modifications of cellular metabolism toward either catabolism or anabolism and modulate the inflammatory and autoimmune responses in our body (Desvergne et al., 2006).
On the other hand, we have to consider the impact of diet and lifestyle on our intestinal microflora. We are indeed metaorganisms living with trillions (1014) of microbial cells (roughly 10 times the cells of our body) and thousands of different microorganisms known as the gut microbiota. This complex ecosystem is an essential part of our organism and influences both our immune system and our metabolism. Therefore, it has a strong impact on our health.
In health, there is a close mutualistic and symbiotic relationship between gut microbiota and humans, and gut microbiota provides a number of useful metabolic functions, protects against enteropathogens, and contributes to normal immune functions. This is the normal state of the human intestinal microbiota, called eubiosis. Distortion from eubiosis, linked with a decrease of intestinal biodiversity and increase of pathogenic bacteria, is called dysbiosis. The most common consequence of a dysbiotic gut microbiota is the alteration of the mucosal immune system and the rise of inflammatory, immune, metabolic, or degenerative diseases (Chassaing and Gewirtz, 2014).
Different kinds and amounts of dietary factors elicit the selection of specific gut microbial populations changing type and number of microbial species toward eubiosis or dysbiosis, simply acting through the preferential feeding of one or the other microbial population. If our diet favors the change to a dysbiotic gut microbiota, this may lead to gut inflammation, alteration of intestinal immunity, and then to systemic inflammation and chronic inflammatory diseases.
How Dietary Factors Influence the Metabolism of Human Cells and Modulate Inflammation
To understand how dietary molecules can directly influence the metabolism of human cells, it is necessary to describe first what are the enzymes and transcription factors involved in catabolism or anabolism in the cell.
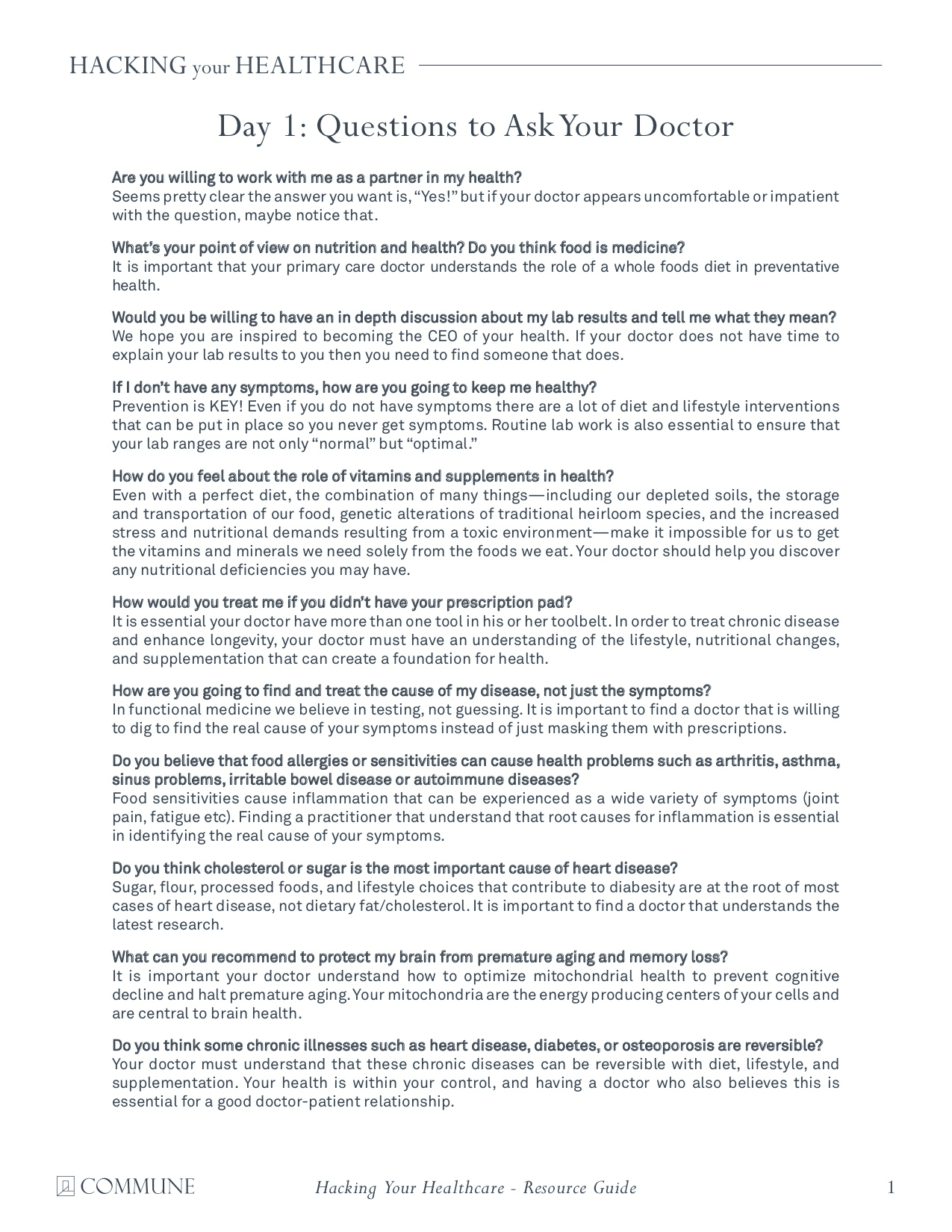
As shown on the left in Figure 2, oxidative metabolism is upregulated by two enzymes and a nuclear receptor. The enzymes are the AMP-activated protein kinase (AMPK; Steinberg and Kemp, 2009) and the Sirtuins (SIRT), a group of histone deacylating enzymes, which are activated by NAD+ (Zhang et al., 2011; Rice et al., 2012). The nuclear receptor is represented by the isotypes of the peroxisome proliferator-activated receptors (PPARs; Desvergne and Wahli, 1999; Burns and VandenHeuvel, 2007).
�
PPAR isotypes upregulate the transcription of genes involved in the beta-oxidation of fatty acids in mitochondria and peroxisomes and form a network with AMPK and Sirtuins pathways. The AMPK-Sirtuins-PPAR pathway is activated by a lifestyle based on calorie restriction and physical exercise, as well as by some bioactive molecules (polyphenols, found in vegetables and fruits, and omega-3 (n-3) long-chain polyunsaturated fatty acids [PUFA], found in fish). Ligand-activated PPAR isotypes form heterodimeric complexes with the retinoid X-receptor (RXR), which, in turn, is activated by 9-cis-retinoic acid (RA).
Conversely, as shown on the right in Figure 2�like on the other dish of an imaginary balance�high intake of energy-dense nutrients leads to the upregulation of anabolism, including lipogenesis and cell growth, through the activation of the sterol regulatory element-binding proteins, SREBP-1c and SREBP-2 (Xu et al., 2013), and the carbohydrate responsive element-binding protein, ChREBP (Xu et al., 2013). SREBP-1c and SREBP-2 are under the control of the nuclear receptors called the liver X receptors (LXR; Mitro et al., 2007; Nelissen et al., 2012). LXR isotypes, which are activated by the cholesterol derivatives oxysterols and glucose, have a relevant role in the synthesis of lipids by activating SREBP-1c and the synthesis of triacylglycerols, while inhibiting SREBP-2 and the synthesis of cholesterol.
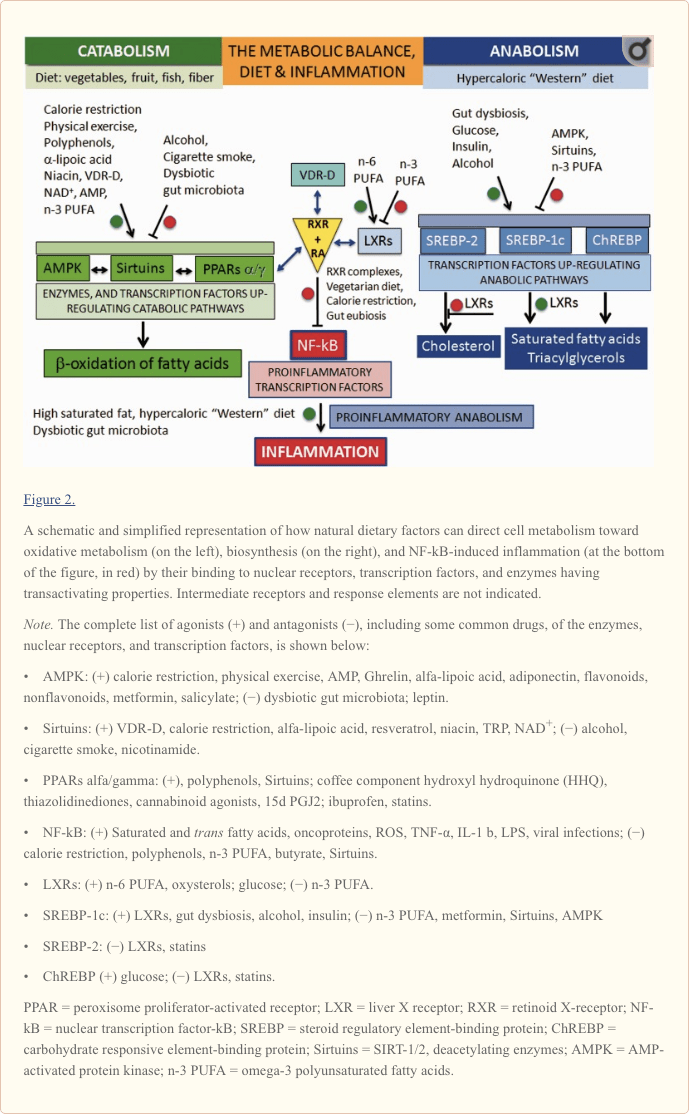
Central to the understanding of the link between diet and inflammation are two transcription factors involved in inflammation and autoimmunity: the nuclear transcription factor-kB (NF-kB) and the activator protein (AP-1; Yan and Greer, 2008). In MS, both NF-kB and AP-1 are activated and induce the expression of several proinflammatory genes and the production of proinflammatory molecules. The cause of their activation in MS is not known but, as shown in Figure 2 for NF-kB, this can be activated not only by viruses, cytokines, and oxidative stress but also by some dietary components such as saturated fatty acids or trans unsaturated fatty acids, which therefore can be considered proinflammatory.
Downregulation of the proinflammatory NF-kB can be achieved by the inhibitory binding of the RA-activated forms of the retinoid X-receptor isotypes (RXRs; P�rez et al., 2012; Zhao et al., 2012; Fragoso et al., 2014).
As shown in the center of Figure 2 and more in detail in Figure 3, the active forms of RA-RXRs are heterodimers resulting from their association with specific ligand-activated nuclear receptors, namely PPARs, LXRs, and vitamin D receptor (VDR).
All three nuclear receptors�PPAR, LXR, and VDR�must be activated by specific ligands. As indicated in Figure 2, the ligands can be specific dietary factors and this clarify how cells respond to changes in nutritional status and regulate energy homeostasis but represents also the molecular key to understanding how nutrients can influence the course of chronic inflammatory diseases (Heneka et al., 2007; Zhang-Gandhi and Drew, 2007; Krishnan and Feldman, 2010; Cui et al., 2011; Schnegg and Robbins, 2011; Gray et al., 2012).
Therefore, each of the three nuclear receptors�PPAR, LXR, and VDR�competes for the binding to RA-RXR and forms hetero-complexes that can inhibit NF-kB and exert a tight control over the expression of inflammatory genes, thus integrating metabolic and inflammatory signaling. It is clear that there is competition between the three receptors PPAR, LXR, and VDR-D, for the binding with RA-RXR, but this competition should have an influence only on metabolism and not on inflammation, because it is not yet known which of the three heterodimers is more effective in inhibiting NF-kB.
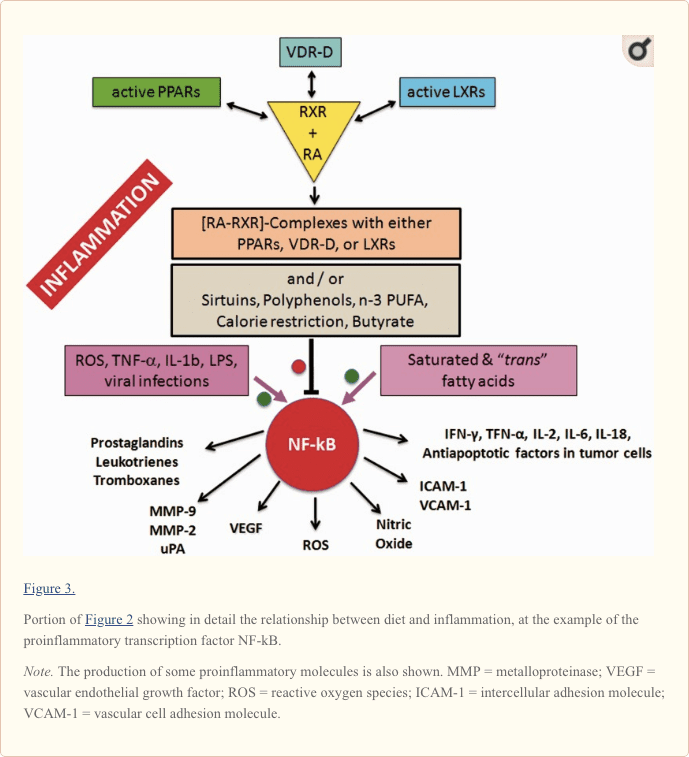
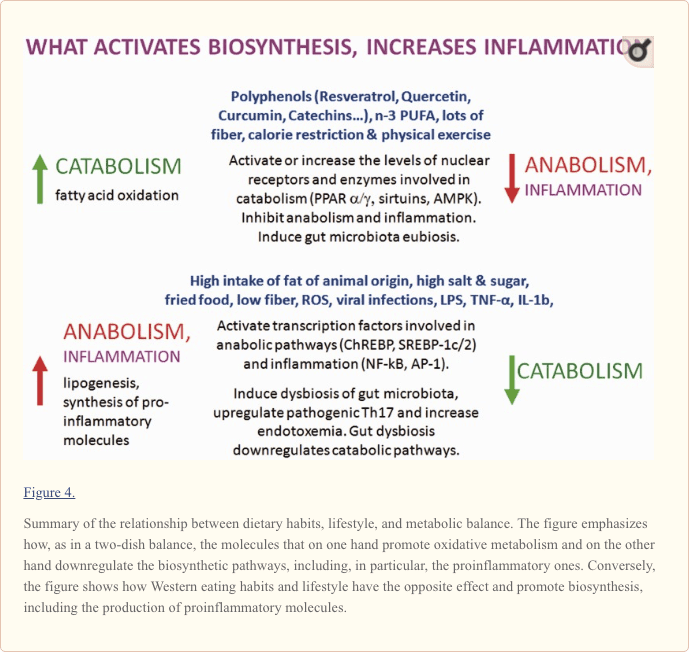
Obviously, the production of proinflammatory molecules in the course of relapses is a biosynthetic process: It is sustained by hypercaloric diets and counteracted by low-calorie diets. In principle, what favors anabolism will promote the inflammatory processes, while what favors catabolism will contrast them (Figure 4).
How Dietary Factors Influence Composition and Biodiversity of Gut Microbiota and Alter Host�Microbiota Relationship
The Link Between Lifestyle, Dietary Habits, and Gut Microbiota Composition
The composition of the intestinal microflora is highly individual and is influenced by many factors such as diet, physical activity, stress, medications, age, and so forth. Each of us has a unique set of at least 100 to 150 species of bacteria.
An easy way to discuss about the effect of food and lifestyle on gut microflora is to restrict the overview to only two dominant bacterial divisions�the Bacteroidetes and the Firmicutes�accounting for about 90% of the total, as it has been shown that the ratio Bacteroidetes/Firmicutes (B/F) is influenced by long-term dietary habits (Cani and Delzenne, 2009; Wu et al., 2011; Lozupone et al., 2012; Tremaroli and B�ckhed, 2012; Panda et al., 2014).
A comparative study of De Filippo et al. (2010) in children from Florence and from Burkina Faso in Africa showed that long-term dietary habits have significant effects on human gut microbiota.
In this study, the Burkina Faso diet was based on the consumption of plant polysaccharides such as millet and sorghum (10 g fibers/day and 662�992 kcal/day), whereas the diet of Italian children was Western style, based on proteins, animal fat, sugar-sweetened drinks, and refined carbohydrates (5.6 g fibers/day and 1,068�1,512 kcal/day). Analysis of fecal samples in the children from Africa showed the prevalence of the Bacteroidetes (73%)�mainly Prevotella and Xylanibacter�and low levels of Firmicutes (12%). On the contrary, a prevalence of Firmicutes (51%) over the Bacteroidetes (27%) was observed in Italian children, but the Bacteroidetes shifted from Prevotella and Xylanibacter to Bacteroides. These latter are usually selected among the Bacteroidetes because they can use also simple sugars in addition to complex glycans, and simple sugars are normal components of Western diets.
In conclusion, the B/F ratio increases in association with a diet rich in complex carbohydrates (nondigestible by our enzymes) because the symbiotic and usually nonharmful Bacteroidetes, such as Prevotella and Xylani bacter, love to have complex glycans to eat. Bacteria consuming complex glycans produce butyrate, which down regulate the activation of proinflammatory NF-kB (Figure 3).
Conversely, Western, energy-dense diets change the gut microbiota profile and increase the population of Firmicutes (including the Mollicutes), more suited to extract and harvest energy, but often pathogenic (Moschen et al., 2012).
The Link Between Dysbiotic Gut Microbiota and Chronic Inflammation
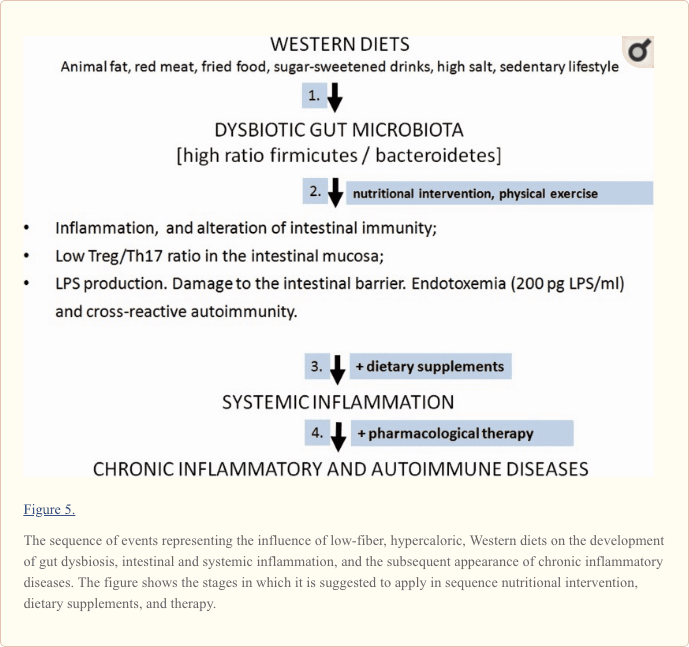
In a dysbiotic gut microbiota, the B/F ratio is low and the possibly pathogenic Firmicutes prevail over Bacteroidetes (Figure 5). The failure of microbial balance and the decrease of biodiversity occurring in dysbiosis lead to the disruption of the complex interplay between the microbiota and its host and contribute to low-grade endotossemia, and chronic intestinal and systemic inflammation. With the onset of systemic inflammation, the risk of chronic inflammatory and immune-mediated diseases increases (Tilg et al., 2009; Brown et al., 2012; Maynard et al., 2012).
Actually, in the presence of a dysbiotic microbiota, gut endotoxin/lipopolysaccharide (LPS) is increased, regulatory T cells (Treg) are defective, and the aryl hydrocarbon receptors and proinflammatory Th17 cells are activated (Cani et al., 2008; Veldhoen et al., 2008).
LPS leads to the dysfunction of the mucosal barrier and affects other tissues when its plasma level increases above 200 pg/ml serum. The increased gut permeability due to the dysbiotic gut microbiota may be exemplified by the passage of IgA and IgG antibodies against gluten and gliadin, also observed in MS patients (Reichelt and Jensen, 2004).
The Link Between Dysbiotic Gut Microbiota and MS
In our previous work, we have proposed that the model linking microbiota alteration�due to Western diet and lifestyle�and the failure of the correct communication between the microbiota and the intestine, leading to low-grade endotoxemia and systemic autoimmune inflammation, might be valid also for the pathogenesis of MS (Fern�ndez et al., 2012; Riccio, 2011). In fact, MS shares with other chronic inflammatory diseases common mechanisms, all probably based on the persistence of low-grade endotoxemia related to wrong lifestyle and dietary habits together with a latent dysbiosis. Moreover, the existence of a gut microbiota-brain axis, which is now more than an emerging concept, suggests that intervention on gut microbiota may be a fruitful strategy for future treatment of complex CNS disorders (Cryan and Dinan, 2012).
The possible direct link between gut microbiota and MS has been shown experimentally by Berer et al. (2011). Using transgenic mice, Berer et al. have shown that gut commensal bacteria can trigger a relapsing-remitting autoimmune disease driven by myelin-specific CD4+ T cells and demyelination, given the availability of MOG�the autoantigen myelin oligodendrocyte glycoprotein. In another study, it was shown that antibiotic treatment directed to alter gut microflora suppresses experimental allergic encephalomyelitis (EAE; Yokote et al., 2008).
These findings suggest that gut microbiota may play a crucial role in the starting phase of MS and may also predispose host susceptibility to other CNS autoimmune diseases as well as to neuropsychiatric disorders such as autism, depression, anxiety, and stress. A new concept of gut microbiota-brain axis is emerging (Wang and Kasper, 2014).
On these grounds, understanding the role of gut microbiota in health and disease can lay the foundation to treat chronic diseases by modifying the composition of gut microbiota through the choice of a correct lifestyle, including dietary habits. Moreover, direct manipulation of the gut microbiota may improve adaptive immune response and reduce inflammatory secretions. For example, because a specific role of intestinal Th17 cells has been suggested in MS immunopathology (Sie et al., 2014), promoting Treg cell differentiation and reducing pathogenic Th17 cells might prevent recurrence of autoimmunity in MS patients (Issazadeh-Navikas et al., 2012).
On these grounds, the discovery that the defect of the Treg/Th17 balance observed in MS models is also present in MS patients, could have important clinical implications, as this defect can be modulated by changes in the microbiota composition, which in turn is modulated by dietary changes (David et al., 2014).
Proinflammatory Dietary Factors
The components of the diet whose intake must be controlled to avoid the rise of inflammatory processes in MS, as well as in other chronic inflammatory diseases, are as follows:
Saturated fatty acids of animal origin;
Unsaturated fatty acids in the trans configuration (hydrogenated fatty acids);
Red meat;
Sweetened drinks, and in general hypercaloric diets rich in refined (low-fiber) carbohydrates, in addition to animal fat;
Increased dietary salt intake;
Cow�s milk proteins of the milk fat globule membrane (MFGM proteins).
Fat of Animal Origin
Saturated fatty acids of animal origin, which are found in foods such as whole milk, butter, cheese, meat, and sausages, are the components of the diet taken into account more frequently for their deleterious influence on the course of MS.
In 1950, Swank suggested that the consumption of saturated animal fat is directly correlated with frequency of MS, but a link between restricted intake of animal fat and remission of MS was reported only in 2003 (Swank and Goodwin, 2003). According to Swank and Goodwin, high-fat diets lead to the synthesis of storage lipids and cholesterol and cause a decrease of membrane fluidity and possible obstruction of capillaries, and the onset or increase of inflammation.
Other more recent studies indicate that the action of saturated fat is controlled at the transcriptional level and influence both gene expression, cell metabolism, development, and differentiation of cells. More in general, the assumption of animal fat is often linked to a high-calorie intake, which is on its own a detrimental factor for many chronic inflammatory diseases. Finally, as described later in this article, an excess of saturated animal fat leads to a dysbiotic intestinal microbiota, dysfunction of intestinal immunity, and low-grade systemic inflammation and represents a possible cause of some human chronic disorders.
Trans Fatty Acids
Trans fatty acids (TFAs) are unsaturated fatty acids that contain at least one nonconjugated double bond in the trans configuration (Bhardwaj et al., 2011).
As products of partial hydrogenation of vegetable oils, they were introduced in the 1960s to replace animal fat, but only much later it was found that they have the same deleterious effect on the metabolism and, as the saturated fatty acids, increase the levels of cholesterol and promote the formation of abdominal fat and weight gain. TFAs intake was found to be positively associated with gut inflammation and the upregulation of proinflammatory citokines in Th17 cell polarization (Okada et al., 2013). Moreover, TFAs interfere with the metabolism of natural unsaturated fatty acids, which have the cis configuration.
TFAs are found in margarine and other treated (hydrogenated) vegetal fat, in meat and dietary products from ruminants and in snacks. They may be present also in French fries and other fried food, as they are also formed in the frying.
Red Meat
Red meat contains more iron heme than white meat. The iron is easily nitrosylated and this facilitates the formation of endogenous nitroso-compounds (NOCs; Joosen et al., 2010). Red meat intake shows indeed a dose�response relation with NOCs formation, whereas there is no such relation for white meat. NOCs are mutagenic: induce nitrosylation and DNA damage. Processed (nitrite-preserved) red meat increases the risk. Heterocyclic amines are formed during cooking of meat at high temperatures, but this is not specific for red meat (Joosen et al., 2010).
Abnormal iron deposits have been found at the sites of inflammation in MS (Williams et al., 2012) and consumption of red meat is associated with higher levels of ?-GT and hs-CRP (Montonen et al., 2013).
Noteworthy, we do not have N-glycolylneuraminic acid (Neu5Gc), a major sialic acid, because an inactivating mutation in the CMAH gene eliminated its expression in humans. Metabolic incorporation of Neu5Gc from dietary sources�particularly red meat and milk products�can create problems, as humans have circulating anti-Neu5Gc antibodies and this implies the possible association with chronic inflammation (Padler-Karavani et al., 2008).
Finally, meat contains arachidonic acid (the omega-6 (n-6) PUFA, which is the precursor of proinflammatory eicosanoids [prostaglandins, thromboxanes, and leukotrienes]) and activates the Th17 pathway (Stenson, 2014).
High Intake of Sugar and Low Intake of Fiber
The high intake of sugar-sweetened beverages and refined cereals, with low fiber content, increases rapidly the number of calories and glucose level. The subsequent increase of insulin production upregulates the biosynthetic pathways and inter alia the production of arachidonic acid and its proinflammatory derivatives.
Increased Dietary Salt Intake
Increased dietary salt intake might be an environmental risk factor for the development of autoimmune diseases, as it has been found that it can induce pathogenic Th17 cells and related proinflammatory cytokines in EAE (Kleinewietfeld et al., 2013; Wu et al., 2013). Th17 cells have been involved in the development of MS.
Cow�s Milk Fat and the Proteins of the Milk Fat Globule Membrane
Milk fat is dispersed in a homogeneous way and protected from oxidation, thanks to a membrane made of lipids and particular proteins called proteins of the milk fat globule membrane (MFGM; Riccio, 2004). These proteins, which account for only 1% of milk proteins, have an informational rather than a nutritional value. In human lactation, they are needed for the correct formation of the digestive, nervous, and immune systems in infants. This flow of information is obviously not relevant, or not required at all, in adulthood and, as well, in the case of cow�s milk taken for human nutrition. In adult age, MFGM proteins of cow�s milk no longer have an informational role and may be eliminated from the diet together with milk fat.
The removal of MFGM proteins from whole cow�s milk is particularly relevant in the case of MS. The most representative MFGM protein (40% of total MFGM proteins), butyrophilin (BTN), is indeed suspected to have a role in MS, as it is very similar to MOG, one of the candidate autoantigen in MS. BTN and MOG share the same behavior in MS experimental models, and MOG/BTN cross-reactive antibodies have been found in MS, in autism and in coronary heart disease (CHD; Riccio, 2004). On these grounds, the patient with MS should avoid the intake of whole cow�s milk and prefer skimmed milk, which, in addition, has no animal fat.
Another point of view is that of Swanson et al. (2013). They have found that BTN or BTN-like molecules might have a regulatory role in immunity and therefore they suggest that BTN or BTN-like molecules could be useful to induce Treg development.
Hypercaloric Diets and Postprandial Inflammation
After each meal, we may experience a transient and moderate oxidative stress and a moderate inflammatory response depending on type and quantity of food. Dietary habits based on a frequent and persistent exposure to meals with high intake of salt/animal fat and trans fat/sugar-sweetened drinks stresses our immune/metabolic system and the subsequent possible failure of homeostasis may lead to immune and metabolic disorders of diverse nature.
Taken together, the diet-dependent stress might be due to following reasons: (a) calorie intake: the higher the calories, the more the oxidative stress induced; (b) glycemic load of a meal: acute postprandial glycemic peaks may induce a release of insulin much higher than necessary; (c) lipid pattern: saturated animal fat, trans fatty acids, and omega-6 (n-6) long-chain PUFA promote postprandial inflammation. As reported in the following sections, postprandial inflammation is attenuated or suppressed by n-3 PUFA and polyphenols, calorie restriction, and physical exercise.
Anti-Inflammatory Natural Bioactive Compounds: Useful to Tackle MS and Prevent Relapses?
Specific bioactive dietary molecules are able to counteract the effects of pathogenic microbial agents and downregulate the expression of inflammatory molecules. Among them, the most important compounds are the polyphenols and carotenoids from vegetables, n-3 PUFA from fish, vitamins D and A, thiol compounds such as lipoic acid, and oligoelements such as selenium and magnesium.
Most of the above-mentioned compounds, with exception of PUFA, which are not antioxidant, are known for their antioxidant properties. The rationale for the use of antioxidants in MS is based on the observation that oxidative stress is one of the most important components of the inflammatory process leading to degradation of myelin and axonal damage. However, it is now known that dietary antioxidants have additional biological properties going far beyond the simple antioxidant activity. Indeed, they are able to counteract the negative effects of microbial agents and saturated or trans fatty acids, downregulating the expression of proinflammatory molecules, oxidative stress, and angiogenesis.
Polyphenols
All polyphenols�which are present in vegetables, cereals, legumes, spices, herbs, fruits, wine, fruit juices, tea, and coffee�have anti-inflammatory, immune-modulatory, anti-angiogenic, and antiviral properties and stimulate the catabolic pathways (Gupta et al., 2014; Wang et al., 2014). They are found in plants in the form of glycosides, esters, or polymers, too large to enter the intestinal membrane. Aglycons released from gut microbiota are conjugated to glucuronides and sulfates in intestine and liver. Their solubility and bioavailability are very poor (�M; Visioli et al., 2011).
From a structural point of view, polyphenols include flavonoids and nonflavonoids molecules (Bravo, 1998). The most important flavonoids are quercetin (onions, apples, citrus fruit, and wine; Min et al., 2007; Sternberg et al., 2008), catechins (green tea; Friedman, 2007), and daidzein and genistein (soy; Castro et al., 2013; Zhou et al., 2014). The most important nonflavonoids are resveratrol (chocolate, peanuts, berries, black grapes, and red wine; Das and Das, 2007; Cheng et al., 2009; Shakibaei et al., 2009), curcumin (spice turmeric of ginger family, curry; Prasad et al., 2014), and hydroxytyrosol (olive oil; Hu et al., 2014).
It has been found that the anti-inflammatory effect of polyphenols in vitro may depend on their chemical structure (Liuzzi et al., 2011). Thus, a mixture of flavonoids and nonflavonoids may be more effective than supplementation with only one polyphenol.
Two examples of the most studied polyphenols are quercetin and resveratrol. Quercetin is present mainly as a glucoside. Most of its effects are additive to those of interferon-?. Quercetin is not toxic, but its oxidation product, quercetin quinone, is very reactive toward the SH groups of proteins and glutathione and may be toxic (Boots et al., 2008). Addition of lipoic acid or N-acetylcysteine can limit the toxic effects.
Resveratrol is glucuronated in the liver and absorbed in this form mainly in the duodenum but only in very limited amount. Depending on its concentration, resveratrol can induce the death of a wide variety of cells by necrosis or apoptosis. In this regard, it is commonly accepted that resveratrol has neuroprotective effects; however, it has been also reported that it can exacerbate experimental MS-like diseases (Sato et al., 2013). These discrepancies can be attributed to the different concentrations used in vitro or bioavailable in vivo, as resveratrol has opposite effects at concentrations of 10?5 M (proliferation of human mesenchimal cells) and 10?4 M (inhibition of proliferation). In our experience, resveratrol has a neurotrophic effect on cortical neurons in culture only at very low concentration, whereas at higher concentration, it may have toxic effect. But in the case of oxidative stress, resveratrol has neuroprotective properties also at the higher concentrations.
Vitamin D, Vitamin A, Carotenoids, Other Vitamins, and Oligoelements
Other compounds and elements that may be useful as supplements in MS are the vitamins D, A, E, C, B12 (Mastronardi et al., 2004), and niacin (Penberthy and Tsunoda, 2009), and oligoelements such as selenium (Boosalis, 2008) and magnesium (Galland, 2010).
Vitamin D has immune-modulatory roles and represents the most promising dietary molecule for the treatment of chronic inflammatory diseases such as MS (Smolders et al., 2008; Pierrot-Deseilligny, 2009; Cantorna, 2012; Ascherio et al., 2014). As already mentioned, it is generally believed that the special geographical distribution of MS in the world can also be attributed to the reduced availability of vitamin D3, due to insufficient exposure to sunlight in some countries, and the lack of active vitamin D may be another possible cause of environmental origin of MS. However, low levels of active vitamin D may be due also to its altered metabolism or function not only to the exposure to sunlight. In fact, the failure of vitamin D3 (cholecalciferol) supplementation to show beneficial effects on body weight or on the course of inflammatory diseases may be due to the persistence of its deficiency despite its administration.
Vitamin D3 (cholecalciferol), formed after exposure to sunshine, is hydroxylated in the liver to 25-(OH) D3 (calcidiol) by the P450 enzymes CYP27A1 or CYP2R1, and subsequently activated in the kidney by CYP27B1 to 1?, 25-(OH)2 D3 (calcitriol). This latter, the active form of vitamin D, is inactivated by CYP24A1 to 1?, 24,25-(OH)3 D3 (calcitroic acid). This means that the levels of active vitamin D depend on the relative rates of its synthesis via CYP27B1 and its modifications via CYP24A1 (Schuster, 2011). High CYP24A1 expression, induced by endogenous compounds and xenobiotics, might lead to low levels of vitamin D and cause or enhance chronic inflammatory diseases and cancer. On these grounds, it is important to follow up the level of vitamin D in the course of vitamin D administration. If vitamin D levels remain low, the expression of CYP24A1 mRNA should be examined, and determination of CYP27B1 and CYP24A1 activities and their inhibition should be tested (Chiellini et al., 2012, K�sa et al., 2013).
Another important aspect regards the VDR. The active metabolite of vitamin D�1?, 25-dihydroxyvitamin D�binds to VDR, and the complex VDR-D controls the expression of several genes involved in processes of potential relevance to chronic diseases. As represented in Figures 2 and and3,3, the VDR-D complex competes with ligand-activated PPARs or LXRs for the binding to RA-RXR. The heterodimeric complexes bind to the proinflammatory transcription factor NFkB and downregulate the synthesis of proinflammatory molecules. In this context, when evaluating the effectiveness of vitamin D supplementation in the course of MS, one should consider the eventual polymorphisms affecting the VDR, which has been recently associated with obesity, inflammation, and alterations of gut permeability (Al-Daghri et al., 2014).
Moreover, the finding that that VDR-D activate the Sirtuin SIRT-1 (An et al., 2010; Polidoro et al., 2013) suggests that vitamin D has an influence also on cell metabolism and therefore may have properties similar to those of many other natural dietary supplements: upregulate oxidative metabolism and downregulate inflammation.
Finally, it should be considered that there are differences between data in humans and experimental models. Actually, in humans, unlike in mice, obesity is associated with poor vitamin D status (Bouillon et al., 2014).
Among the carotenoids, the most important is lycopene (tomato, water melon, and pink grape fruit; Rao and Rao, 2007). Besides to be a very strong antioxidant, lycopene can give beta-carotene and retinoic acid, and the latter can activate the RXR receptor (Figure 2). Although higher intakes of dietary carotenoids, vitamin C, and vitamin E did not reduce the risk of MS in women (Zhang et al., 2001), the relevance of lycopene and vitamin A against inflammation cannot be disregarded.
Omega-3 (n-3) Essential Fatty Acids and Poly-Unsaturated Fatty Acids from Vegetables, Seafood, and Fish Oil
n-3 essential fatty acids (EFA) and PUFA represent a valid alternative to saturated fatty acids of animal origin.
Vegetable and vegetable oils contain the essential fatty acids linoleic acid (n-6) and linolenic acid (n-3). n-6 and n-3 fatty acids have opposite effects and their presence in the diet should be equivalent (Schmitz and Ecker, 2008). However, in Western diets, the ratio n-6/n-3 is increased from 6 to 15 times and this leads to a higher incidence of cardiovascular and inflammatory diseases. In fact, the linoleic acid leads to the formation of arachidonic acid (20:4), the precursor of the proinflammatory eicosanoids prostaglandins-2, leukotrienes-4, and thromboxanes-2. The synthesis of these eicosanoids is favored by insulin, and inhibited by aspirin, as well as by the n-3 long-chain PUFA EPA (eicosapentaenoic acid) and DHA (docosahexaenoic acid), which derive from n-3 linolenic acid.
Both DHA and EPA are found in seafood and fish oil. Both show remarkable anti-inflammatory, anti-thrombotic, and immune-modulatory activities, comparable with those of statins (Calder, 2006; Farooqui et al., 2007). n-3 PUFA inhibit inflammatory processes and the synthesis of fatty acids and cholesterol, and instead they stimulate the oxidation of fatty acids. On this basis, in chronic inflammatory diseases such as MS, n-3 essential fatty acids (EFA) and n-3 PUFA should prevail in the diet over the n-6 fatty acids. It is interesting to note that DHA is present in high concentrations in the brain and its levels decrease in patients with MS.
In cultured microglial cells activated by LPS, fish oil is as effective as interferon-? in inhibiting the expression of MMP-9 (gelatinase B), an important mediator of neuro-inflammation (Liuzzi et al., 2004, 2007). Moreover, n-3 PUFA significantly decreased MMP-9 levels in few clinical trials, indicating that n-3 PUFA may represent a good complementary treatment in the course of MS (Weinstock-Guttman et al., 2005; Mehta et al., 2009; Shinto et al., 2009). Fish oil has been also found to improve motor performances in healthy rat pups (Coluccia et al., 2009).
n-3 PUFA act in synergy with aspirin on AMPK and COX enzymes but with different mechanisms. Noteworthy, in the presence of aspirin, EPA and DHA form new anti-inflammatory bioactive molecules called resolvins, protectins, and maresins, which are able to reduce cellular inflammation and inflammatory pain (Xu et al., 2010; Hong and Lu, 2013; Serhan and Chiang, 2013). This may be a relevant aspect related to the nutritional intervention in MS. Indeed, the inflammatory processes associated to MS could be also due to the low ratio omega-3 (anti-inflammatory)/omega 6 (inflammatory) PUFA and thereby to the low production of adequate amounts of resolution-inducing molecules lipoxins, resolvins, and protectins that suppress inflammation. Hence, administration of omega-3 PUFA together with aspirin or directly of lipoxins, resolvins, and protectins may form a new approach in the prevention and treatment of MS and other neuroinflammatory diseases. Furthermore, other anti-inflammatory and antiangiogenic eicosanoids can also be produced by the P450 CYP enzymes from EPA and DHA (Yanai et al., 2014). In this context, it should be taken into consideration that statins may interfere negatively with the metabolism of n-3 and n-6, as they can decrease the n-3/n-6 ratio. Thus, treatment with statins should be associated with n-3 PUFA supplementation (Harris et al., 2004).
Seeds oils, from sunflower, corn, soybean, and sesame, contain more n-6 fatty acids than n-3 fatty acids and therefore their assumption should be limited in MS, in order to limit the level of proinflammatory eicosanoid production. On the other hand, coconut oil has a high content of saturated fatty acids. Among vegetable oils, olive oil should be preferred for the good ratio between saturated and unsaturated fatty acids, and because it contains the antioxidant hydroxytyrosol.
Thiolic compounds as Dietary Supplements
Compounds containing thiol groups (�SH) such as ?-lipoic acid (ALA), glutathione, and N-acetylcysteine (NAC) should be taken into consideration as possible dietary supplements to be used for the complementary treatment of MS.
As polyphenols, ALA (Salinthone et al., 2008; green plants and animal foods) has immunomodulatory and anti-inflammatory properties. ALA stabilizes the integrity of the BBB and stimulates the production of cAMP and the activity of protein kinase A. Also NAC might be useful in neurological disorders. It passes through the BBB and protects from inflammation (Bavarsad Shahripour et al., 2014).
The Mediterranean Diet
A recent systematic review and meta-analysis of intervention trials provide evidence that Mediterranean diet patterns reduce inflammation and cardiovascular mortality risk and improves endothelial functions (Schwingshackl and Hoffmann, 2014). These findings are as much encouraging as you think that the true Mediterranean diet is a little different from the one currently described.
It is generally agreed that the Mediterranean diet is based on consumption of extra-virgin olive oil, unrefined cereals, legumes, diverse vegetables (in particular tomatoes) and fruits, dairy products (mostly as pecorino cheese, ricotta, mozzarella, and yogurt), fish and fishery products, and low consumption of animal fat and meat. However, currently, the Mediterranean diet tends to a high consumption of pasta and bread, which means a high intake of gluten.
Once, in true Mediterranean diet, in Southern Italy, meat was eaten two or at most three times a week, only olive oil was used for cooking (extra-virgin quality and the most possible raw), but notably the intake of gluten was about half compared with the current intake. The pasta was eaten with the classic home-made tomato sauce, but in alternative, it was most often mixed with other gluten-free foods. The most common recipes were pasta and potatoes; pasta with either green beans, or artichokes, zucchini, eggplant, turnips, or cabbage; pasta with a mix of vegetables and legumes (minestrone: vegetable soup); and pasta with chickpeas, beans, or lentils. The sugar-sweetened drinks of today were not known. A high assumption of gluten-rich food may lead to nonceliac asymptomatic gluten sensitivity, mucosal intestinal damage, changes in gut microbiota, and low-grade intestinal inflammation. In conclusion, the Mediterranean diet is good, but the intake of gluten must be limited and must be whole grains.
Inflammatory and Anti-Inflammatory Lifestyle
Smoking (Proinflammatory)
Only a few studies have been carried out on the impact of smoking on the course of MS and results are conflicting, perhaps because its effects are difficult to ascertain and enucleate from other factors. Weiland et al. (2014) have found no association between smoking and relapse rate or disease activity, but do not exclude that smokers might have a significantly lower health-related quality of life than non-smokers, whereas Manouchehrinia et al. (2013) found that smoking is associated with more severe disease.
However, as it is shown in Figure 2, it can be expected that cigarette smoke may worsen the course of MS, as it may inhibit the anti-inflammatory activity of Sirtuins (Caito et al., 2010). The oxidative and carbonyl stress induced by cigarette smoke can be reversed by resveratrol (Liu et al., 2014).
Alcohol Consumption (Proinflammatory)
Recent studies shows that alcohol (beer, wine, or liquor) consumption is not associated to MS risk (Massa et al., 2013; Hedstr�m et al., 2014). However, as also shown in Figure 2, alcohol may inhibit the Sirtuin SIRT1 and activate the transcriptional activity of SREBP-1c (You et al., 2008), thus promoting the biosynthesis of lipids and inflammation at the expense of oxidative metabolism.
There are other two aspects of ethanol that should be considered. First, the metabolism of ethanol converts a large number of NAD+ molecules to NADH, limiting the availability of NAD+ required for the activity of Sirtuins. Second, as a substrate of the P450 enzymes, ethanol can interfere with the metabolism of drugs, which are transformed by the same enzymes. The result may be the prolongation and the enhancement of drug action. Altogether, alcohol should be considered as a molecule that interferes with the normal metabolism and facilitates the inflammatory process, complicating the possibility of improving the wellbeing of the patient.
Calorie Restriction (Anti-Inflammatory)
High-calorie intake and a meal rich in refined carbohydrates and sugar increase insulin level and favors biosynthesis, including the production of proinflammatory molecules and the production of free radicals. Calorie restriction, obtained by decreasing food intake or by intermittent fasting (one day and the other not), upregulates the level of SIRT1 (Zhang et al., 2011), increases the level of AMP and upregulates AMPK, increases adiponectin levels and upregulate or activate its receptors (Lee and Kwak, 2014), and downregulates oxidative damage, lymphocyte activation, and the progression of experimental models of MS (Piccio et al., 2008, 2013). The effects of calorie restriction can be mimicked by agonists (resveratrol and other polyphenols), acting on the same targets (SIRT1, AMPK).
Physical Exercise (Anti-Inflammatory)
Physical exercise is now an almost accepted practice also for MS patients and is commonly applied in order to decrease the symptoms of chronic fatigue and prevent or slow the onset of disability. However, the importance of physical exercise goes beyond that of simple muscle activity and should be rather considered in a holistic context in which diet, exercise, therapy, and social interchange, all play a role for the wellness of MS patients (Gacias and Casaccia, 2013).
Dietary control and exercise practice have been proposed by the WHO (2010) to attenuate or prevent human chronic diseases.
From a molecular point of view, physical exercise exerts its beneficial effect by acting on the protein kinase AMPK axis and the AMPK�Sirtuins�PPAR-? network, upregulating oxidative metabolism and downregulating biosynthetic pathways and inflammation (Narkar et al., 2008). As AMPK has a key role in energy balance, it is important to mention its agonists. Resveratrol and AMPK agonists such as metformin, a drug used in type 2 diabetes, can mimic or enhance the effect of physical activity and are effective in experimental encephalitis (Nath et al., 2009).
Physical exercise influences the quality of life and may stimulate the production of anti-inflammatory cytokines (Florindo, 2014). Furthermore, physical exercise lowers plasma levels of leptin and reduces gene expression of leptin receptors in the liver (Yasari et al., 2009), while increasing adiponectin levels and adiponectin receptors activity (Lee and Kwak, 2014).
The association of physical exercise with calorie restriction leads to a significant reduction of inflammatory markers (Reed et al., 2010).
Recent studies carried on adult C57BL/6 J male mice have shown that exercise stimulate brain mitochondrial activity, potentiate neuroplasticity, and is associated to mood improvement, as it decrease anxiety-like behaviors in the open field and exert antidepressant-like effects in the tail suspension test (Aguiar et al., 2014). Other studies performed on rats showed that exercise can alter the composition and diversity of gut bacteria (Petriz et al., 2014).
On these grounds, MS patients should practice mild physical exercise (brisk walking, swimming, or even dancing), if possible in the course of a rehabilitation program.
Nutritional Clinical Trials in MS So Far
Unfortunately, nutritional clinical trials in MS are only very few. Some of them were based on diets low in saturated fat, either without supplements (Swank and Goodwin, 2003) or with omega-3 fat supplements (Nordvik et al., 2000; Weinstock-Guttman et al., 2005). Other clinical trials were based on the administration of single dietary supplements only: either vitamin D, or fish oil (n-3 PUFA), or lipoic acid. Clinical trials with single polyphenols were performed only in cancer. Dietary supplements have never been used together and have never been associated with dietary prescription.
Taken together, clinical attempts to clarify the role of nutrition in MS were considered only promising of poor quality or with no clear results (Farinotti et al., 2007, 2012). In particular, as reported by Farinotti et al. in their Cochrane review (2012), supplements such as n-3 PUFA seem to have no major effect on the main clinical outcome in MS, but they may reduce the frequency of relapses over 2 years. Data available were considered to be insufficient or of uncertain quality to assess a real effect from PUFA supplementation. In some studies, slight possible benefits in relapse outcomes were found with omega-6 fatty acids, but data were characterized by the reduced validity of the endpoints. In general, trial quality was found to be poor. Studies on vitamin supplementation were not analyzed as none met the eligibility criteria, mainly due to lack of clinical outcomes. Thus, evidence on the benefits and risks of vitamin supplementation and antioxidant supplements in MS is lacking.
Suggestions for a Nutritional Intervention in MS: The Choice of Diet and Dietary Supplements
At the end, the goal of a nutritional intervention in MS must be the control of inflammation and this, as shown in this review, can be achieved mainly by controlling postprandial inflammation, the composition of gut microbiota and intestinal and systemic inflammation, and immunity. This can be achieved by a long-term dietary intervention, with a hypocaloric diet, prebiotics, probiotics, and dietary supplements.
As reported in this article, healthy dietary molecules, calorie restriction, and exercise are able to direct cell metabolism toward catabolism and downregulate anabolism and inflammation by interacting at different levels with specific enzymes, nuclear receptors, and transcriptional factors. Furthermore, in association with fiber, they can shift gut dysbiosis to eubiosis.
As a result, low-calorie meals (1,600�1,800 kcal) based on vegetables, whole cereals, legumes, fruit, and fish may slow down the progression of the disease and ameliorate the wellness of MS patients, whereas hypercaloric diets with high intake of salt, saturated animal fat, fried food, and sugar-sweetened drinks may lead to the onset of postprandial inflammation and systemic low-grade inflammation.
Diet should be integrated with prebiotics, probiotics, specific vitamins (D, A, B12, and nicotinic acid), oligoelements (magnesium and selenium), and dietary supplements such as polyphenols, n-3 PUFA, and lipoic acid.
Prebiotics for MS should include inulin, bran, lactosucrose, and oligofructose, preferential nutrients for colonocytes and capable to inactivate NF-kB. Probiotics, such as lactococcus lactis, bifidobacterium lactis, and clostridium butyricum, which can improve the intestinal microbial balance, can be used to change the composition of colonic microbiota. The combination of prebiotics and probiotics is highly recommended. Bowel functions and weight should always be under control.
A more drastic therapeutic approach aimed to restore gut eubiosis and downregulate inflammation may be represented by fecal microbiota transplantation (FMT; Smits et al., 2013). The method seems to be very effective but still primitive, not completely safe, and in a way also disgusting. The field should move beyond fecal transplants, identify the organisms that may be essential for a particular condition, and provide those organisms in a much simpler fashion than FMT (�Critical Views in Gastroenterology & Hepatology,� 2014).
Dietary supplements, with the only exception of omega-3 PUFA, which are normal constituents of our body, are useful at the beginning of the nutritional intervention, or in the course of relapses, to facilitate the recovery of a healthy condition, but their use should be restricted to only a limited period of time (3�4 months). This is particularly valid for the polyphenols. Polyphenols are not well-known molecules with regard to their bioavailability and their biological effects and special precautions should be used when supplementing the diet with them. On one hand, they can downregulate the synthesis of proinflammatory molecules in the course of inflammatory processes; on the other hand, they can stimulate cell activity in resting cells, but a persistent stimulation can induce the apoptosis of healthy cells. Taken together, these considerations suggest that administration of purified polyphenols should be performed on the basis of preliminary clinical trials to test their effectiveness as dietary supplements and to determine their long-term safety and the right dosage.
In general, a nutritional intervention with anti-inflammatory food and dietary supplements decreases the biosynthesis of proinflammatory compounds and therewith makes more effective the use of immune-modulatory drugs, and eventually might limit their possible adverse effects, alleviate the symptoms of chronic fatigue syndrome, and favor patient wellness. However, diet and dietary supplements should not be treated as drugs and as a substitute of therapy. Similarly, proinflammatory food is not toxic and there is no need to exclude it completely. You can eat a nice steak or fried food without risk or guilt, if you are in a basically healthy condition. What hurts are the wrong eating habits in the long run.
Multiple sclerosis, or MS, is a chronic, progressive disease involving damage to the myelin sheaths of nerve cells. The epidemiology of MS suggests that various factors are often involved in the clinical expression of the health issue. However, numerous research studies have primarily evaluated the role of diet on the development of multiple sclerosis. For several years, healthcare professionals believed there was a correlation between the consumption of dairy in patients with multiple sclerosis. According to various research studies, a significant correlation between cow milk and the prevalence of multiple sclerosis was found, suggesting a possible role of dairy products in the multifactorial etiology of MS. Dr. Alex Jimenez D.C., C.C.S.T.
Conclusions
So, at first glance, MS does not seem to have any of the characteristics of chronic inflammatory diseases, which could be related to wrong dietary habits and lifestyle, or even to a dysbiotic gut microbiota. There is apparently nothing in an exacerbation of the disease that may be linked to food or the state of the intestinal microbiota. In fact, when we began our studies on the impact of nutrition on MS, there was not even the slightest clue that there could exist a real link between them, and the idea of the involvement of gut microbiota in MS was considered only very speculative. To date, the idea that dietary habits might influence the course of MS is still struggling to establish itself. Not so in cardiovascular diseases and other chronic inflammatory conditions, in which the influence of dietary habits is almost accepted, and not even in cancer, which is increasingly considered as a metabolic disorder (Seyfried et al., 2014).
At present, MS therapy is not associated to any particular diet, probably due to lack of information on the effects of nutrition on the disease. However, the majority of patients with MS is looking for complementary and alternative treatments (CAM), and in particular is trying to change dietary habits, almost without the advice of the physician (Schwarz et al., 2008; Leong et al., 2009). A recent study based on data provided by MS patients in response to a questionnaire on their dietary habits seems to support a significant association of healthy dietary habits with better physical and mental health-related quality of life and a lower level of disability (Hadgkiss et al., 2014). These data reinforce the idea of the need for randomized controlled trials of nutritional intervention for people with MS. It should be emphasized that nutritional treatments should be complementary, but not alternative to therapy, be part of a holistic approach and performed under medical control.
As there are no data available from clinical trials yet, our work is aimed to rationalize dietary choices on the basis of known and established effects of dietary factors and lifestyle at the molecular level. Data reported in Figure 2 are obviously not complete but may be useful to provide guidelines for nutritional interventions. In principle, proinflammatory food upregulate the biosynthetic and inflammatory pathways, as shown on the right and at the bottom of Figure 2, whereas anti-inflammatory food upregulates oxidative metabolism and downregulates anabolism and inflammation.
As shown in this article, the finding that calorie restriction, exercise, and particular dietary factors can influence the degree of inflammatory responses by acting on both cellular metabolism (Figure 2) and composition of gut microbiota (Figure 5), suggests that an appropriate nutritional intervention may ameliorate the course of the disease and may be therefore taken in consideration as a possible complementary treatment in MS. As inflammation is present in both RRMS and PPMS, nutritional advices are indicated for both forms of the disease. This is particularly important in the case of PPMS, for which no cure is presently available. Conversely, as specific dietary habits may be detrimental and may promote a chronic state of low-grade inflammation, a wrong diet may be considered a possible contributory cause of relapses in MS.
Taken together, we have now a better knowledge of the possible influence of dietary factors on cell metabolism and gut microbiota, and on their possible effects on the disease, but, clearly, we are only just beginning to understand the role of nutrition and gut microbiota in MS and much work remains in terms of understanding the nature of the interactions of gut microbiota with the host�s immune system, especially at sites distal to the intestine.
On these grounds, future prospects in MS research should regard the following points: (a) assess gut microbiota composition; (b) evaluate defects in intestinal immune system; (c) clarify the role of polyphenols and vitamin D metabolism; (d) study the impact of dietary factors, herbs, and drugs on AMPK, Sirtuins, PPAR, or directly on NF-kB. Noteworthy, some drugs used to treat type II diabetes, such as the PPAR-? agonists thiazolidinediones (Bernardo et al., 2009), and the AMPK agonist metformin (Nath et al., 2009) have anti-inflammatory effects comparable with those of anti-inflammatory dietary factors; (e) define possible interferences between dietary supplements and MS drugs; (f) promote a campaign aimed to educate about the importance to follow a healthy diet during therapy, for instance, encouraging patients to include fiber or complex carbohydrates in their diet, supplementing with probiotics, choosing n-3 fats over proinflammatory n-6 fats, and limiting meat and animal fat consumption. The choice of good recipes, such as those described by Mollie Katzen (2013), can make the diet more acceptable.
Overall, immune-modulatory conventional MS therapies have been almost successful; however, drugs that can protect and favor repair mechanisms are still missing. We can decide to help people stay healthy by providing nutritional guidance and physical activity opportunities. For the moment, there are only good prospects for improving the wellbeing of patients with MS. We are only at the beginning of the story.
Summary
As both relapsing-remitting MS and primary-progressive MS are inflammatory diseases, they can be influenced by proinflammatory or anti-inflammatory dietary habits and lifestyle through their action on cell metabolism and gut microbiota. Nutritional advice to MS patients may favor their wellness.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is supported by the Italian Foundation for Multiple Sclerosis (FISM) with grants 2007/R/15 for the Project �Healthy and Functional Foods for MS patients,� 2010/R/35 for the Project �The Molecular Basis for Nutritional Intervention in Multiple Sclerosis,� and 2014/S/2 (2014�2015) for the project �Nutritional Facts in Multiple Sclerosis: Why They Are Important and How They Should Be Managed� to P. R.
Many doctors greatly recommend that patients with multiple sclerosis, or MS, avoid dairy because various research studies have demonstrated a high correlation between MS and dairy, especially cow�s milk. This is largely due to the fact that the proteins in cow�s milk are generally targeted by the immune system of patients with multiple sclerosis. Furthermore, some proteins in cow�s milk imitate part of the myelin oligodendrocyte glycoprotein, or MOG, the section of myelin which triggers the autoimmune response in multiple sclerosis that can trick the immune system to attack and destroy the MOG. Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic and spinal health issues. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief. �
Gale Grijalva was a victim of a car crash. As a result, she started to experience severe pain symptoms which tremendously affected her ability to perform her regular tasks. Gale Grijalva describes the conditions that resulted in the auto accident as well as how her symptoms that are specific began to manifest after the incident. Gale Grijalva visited Dr. Alex Jimenez, chiropractor, to receive chiropractic care for her car crash injuries and she was grateful to get the pain relief she deserved. Chiropractic care is an effective and secure, alternative treatment option which focuses on the identification, prevention, and treatment of many different injuries and/or conditions. Gale Grijalva highly recommends Dr. Alex Jimenez as the noninvasive choice for car accident injuries and whiplash, among other problems.
Chiropractic Treatment
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused on treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
We want you to live a life that is fulfilled with more energy, positive attitude, better sleep, less pain, proper body weight and educated on how to maintain this way of life. I have made a life of taking care of every one of my patients.
I assure you, I will only accept the best for you�
If you have enjoyed this video and we have helped you in any way, please feel free to subscribe and recommend�us.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine