For individuals into sports, fitness enthusiasts, and those that engage in physical activities, musculoskeletal injuries are common. Can using ice tape help during the initial or acute phase of injury decrease inflammation and swelling to expedite recovery and return to activities sooner?
Ice Tape
After a musculoskeletal injury, individuals are recommended to follow the R.I.C.E. method to help reduce swelling and inflammation. R.I.C.E. is the acronym for Rest, Ice, Compression, and Elevation. (Michigan Medicine. University of Michigan. 2023) The cold helps to decrease pain, lower tissue temperature, and decrease swelling around the site of the injury. By controlling the inflammation with ice and compression early after injury, individuals can maintain the appropriate range of motion and mobility around the injured body part. (Jon E. Block. 2010) There are different ways to apply ice to an injury.
Store-bought ice bags and cold packs.
Soaking the injured body part in a cold whirlpool or tub.
Making reusable ice packs.
A compression bandage can be used together with the ice.
Ice Tape is a compression bandage that provides cold therapy all at once. After an injury, applying it can help decrease the pain and swelling during the acute inflammatory phase of healing. (Matthew J. Kraeutler et al., 2015)
How The Tape Works
The tape is a flexible bandage that is infused with therapeutic cooling gel. When applied to an injured body part and exposed to air, the gel activates, generating a cold sensation around the area. The therapeutic medicinal effect can last five to six hours. Combined with a flexible bandage, it provides ice therapy and compression. The ice tape can be used straight out of the package but can also be stored in the refrigerator to increase the cold effect. Depending on the maker’s instructions, the tape should not be stored in the freezer as this can make it too hard to wrap around the injured area.
Advantages
The benefits include the following:
Easy to Use
The product is easy to use.
Take out the tape, and start wrapping it around the injured body part.
Fasteners Not Required
The wrap sticks to itself, so the tape stays in place without using clips or fasteners.
Easy to Cut
The standard roll is 48 inches long by 2 inches wide.
Most injuries require enough to wrap around the injured area.
Scissors cut the exact amount needed, and store the rest in the resealable bag.
Reusable
After 15 to 20 minutes of application, the product can be easily removed, rolled up, stored in the bag, and used again.
The tape can be used multiple times.
The tape begins to lose its cooling quality after several uses.
Portable
The tape does not need to be placed in a cooler when traveling.
It is easily portable and perfect for a quick ice and compression application immediately after an injury.
It can decrease pain and inflammation and kept at the workplace.
Disadvantages
A few disadvantages include the following:
Chemical Odor
The gel on the flexible wrap can have a medicine odor.
It is not quite as powerful smelling as pain creams, but the chemical odor could bother some individuals.
Might Not Be Cold Enough
The tape works for immediate pain relief and inflammation, but it may not get cold enough for the user when applied right from the package at room temperature.
However, it can be placed in a refrigerator to increase the coldness and may provide a more therapeutic cooling effect, especially for those dealing with tendinitis or bursitis.
Stickiness Could Be Distracting
The tape could be a bit sticky for some.
This sticky factor can be a minor annoyance.
However, it just feels sticky when being applied.
A couple of flecks of the gel may get left behind when removed.
The ice tape can also stick to clothing.
For individuals looking for a quick, on-the-go cooling therapy for injured or aching body parts, ice tape may be an option. It could be good to have on hand to provide cooling compression if a minor injury occurs while participating in athletics or physical activities and relief for overuse or repetitive strain injuries.
Block J. E. (2010). Cold and compression in the management of musculoskeletal injuries and orthopedic operative procedures: a narrative review. Open access journal of sports medicine, 1, 105–113. https://doi.org/10.2147/oajsm.s11102
Kraeutler, M. J., Reynolds, K. A., Long, C., & McCarty, E. C. (2015). Compressive cryotherapy versus ice-a prospective, randomized study on postoperative pain in patients undergoing arthroscopic rotator cuff repair or subacromial decompression. Journal of shoulder and elbow surgery, 24(6), 854–859. https://doi.org/10.1016/j.jse.2015.02.004
For individuals experiencing a turf toe injury, can knowing the symptoms help athletes and non-athletes with treatment, recovery time, and returning to activities?
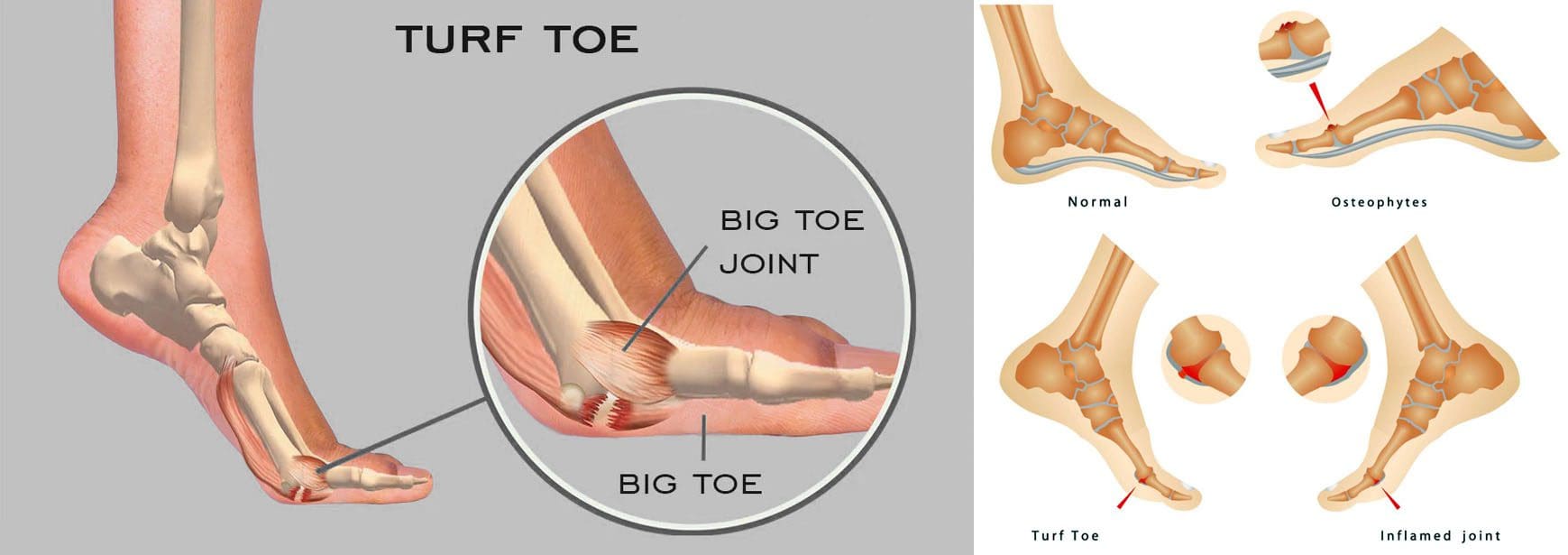
Turf Toe Injury
A turf toe injury affects the soft tissue ligaments and tendons at the base of the big toe under the foot. This condition usually occurs when the toe is hyperextended/forced upward, such as when the ball of the foot is on the ground and the heel is lifted. (American Academy of Orthopaedic Surgeons. 2021) The injury is common among athletes who play sports on artificial turf, which is how the injury got its name. However, it can also affect non-athletes, like individuals working on their feet all day.
Recovery time after turf toe injury depends on the severity and the type of activities the individual plans to return to.
Returning to high-level sports activities after a severe injury can take six months.
These injuries vary in severity but usually improve with conservative treatment. In severe cases, surgery could be required.
Pain is the primary issue that stops physical activities after a grade 1 injury, while grades 2 and 3 can take weeks to months to heal completely.
Meaning
A turf toe injury refers to a metatarsophalangeal joint strain. This joint comprises ligaments that connect the bone on the sole of the foot, below the big toe/proximal phalanx, to the bones that connect the toes to the larger bones in the feet/metatarsals. The injury is usually caused by hyperextension that often results from a pushing-off motion, like running or jumping.
If experiencing turf toe symptoms, see a healthcare provider for a proper diagnosis so they can develop a personalized treatment plan. They will perform a physical exam to assess pain, swelling, and range of motion. (American Academy of Orthopaedic Surgeons. 2021) If the healthcare provider suspects tissue damage, they may recommend imaging with X-rays and (MRI) to grade the injury and determine the proper course of action.
Grades 2 and 3 come with partial or complete tissue tearing, severe pain, and swelling. Treatments for more severe turf toe can include: (Ali-Asgar Najefi et al., 2018)
Limited weight bearing
Using assistive devices like crutches, a walking boot, or a cast.
Physical therapy also includes proprioception and agility training exercises, orthotics, and wearing recommended shoes for specific physical activities. (Lisa Chinn, Jay Hertel. 2010)
A physical therapist can also help ensure that the individual does not return to physical activities before the injury is fully healed and prevent the risk of re-injury.
Grade 1 – Subjective as it varies depending on the individual’s pain tolerance.
Grade 2 – Four to six weeks of immobilization.
Grade 3 – Eight weeks minimum of immobilization.
It can take up to six months to return to normal function.
Returning To Normal Activities
After a grade 1 turf toe injury, individuals can return to normal activities once the pain is under control. Grades 2 and 3 take longer to heal. Returning to sports activities after a grade 2 injury can take around two or three months, while grade 3 injuries and cases that require surgery can take up to six months. (Ali-Asgar Najefi et al., 2018)
Sports Chiropractic Treatment
References
American Academy of Orthopaedic Surgeons. (2021). Turf toe.
American College of Foot and Ankle Surgeons. Foot Health Facts. (2023). RICE protocol.
Najefi, A. A., Jeyaseelan, L., & Welck, M. (2018). Turf toe: A clinical update. EFORT open reviews, 3(9), 501–506. https://doi.org/10.1302/2058-5241.3.180012
Pinter, Z. W., Farnell, C. G., Huntley, S., Patel, H. A., Peng, J., McMurtrie, J., Ray, J. L., Naranje, S., & Shah, A. B. (2020). Outcomes of Chronic Turf Toe Repair in Non-athlete Population: A Retrospective Study. Indian journal of orthopaedics, 54(1), 43–48. https://doi.org/10.1007/s43465-019-00010-8
Chinn, L., & Hertel, J. (2010). Rehabilitation of ankle and foot injuries in athletes. Clinics in sports medicine, 29(1), 157–167. https://doi.org/10.1016/j.csm.2009.09.006
Athletes and physically active individuals who participate in activities, exercises, and sports that involve kicking, pivoting, and/or shifting directions can develop pelvis overuse injury of the pubic symphysis/joint at the front of the pelvis known as osteitis pubis. Can recognizing the symptoms and causes help in treatment and prevention?
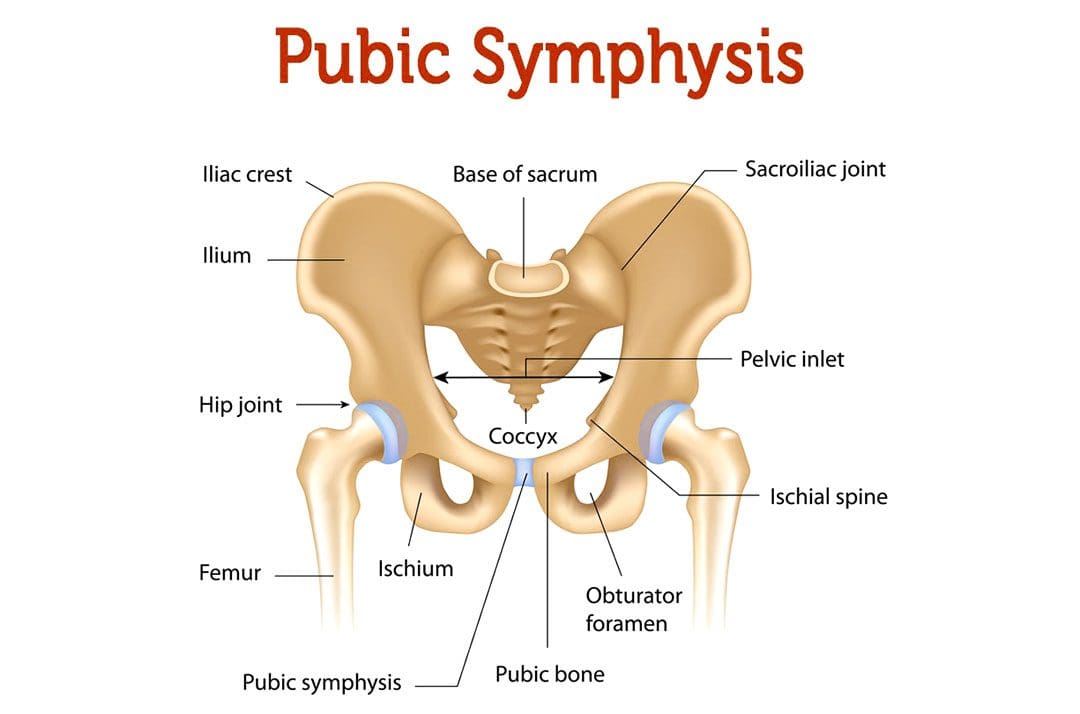
Osteitis Pubis Injury
Osteitis pubis is the inflammation of the joint that connects the pelvic bones, called the pelvic symphysis, and the structures around it. The pubic symphysis is a joint in front of and below the bladder. It holds the two sides of the pelvis together in the front. The pubis symphysis has very little motion, but when abnormal or continued stress is placed on the joint, groin and pelvic pain can present. An osteitis pubis injury is a common overuse injury in physically active individuals and athletes but can also occur as the result of physical trauma, pregnancy, and/or childbirth.
Symptoms
The most common symptom is pain over the front of the pelvis. The pain is most often felt in the center, but one side may be more painful than the other. The pain typically radiates/spreads outward. Other signs and symptoms include: (Patrick Gomella, Patrick Mufarrij. 2017)
Lower abdominal pain in the center of the pelvis
Limping
Hip and/or leg weakness
Difficulty climbing stairs
Pain when walking, running, and/or shifting directions
Clicking or popping sounds with movement or when shifting directions
Pain when lying down on the side
Pain when sneezing or coughing
Osteitis pubis can be confused with other injuries, including a groin strain/groin pull, a direct inguinal hernia, ilioinguinal neuralgia, or a pelvic stress fracture.
Causes
An osteitis pubis injury usually occurs when the symphysis joint is exposed to excessive, continued, directional stress and overuse of the hip and leg muscles. Causes include: (Patrick Gomella, Patrick Mufarrij. 2017)
Sports activities
Exercising
Pregnancy and childbirth
Pelvic injury like a severe fall
Diagnosis
The injury is diagnosed based on a physical examination and imaging tests. Other tests may be used to rule out other possible causes.
The physical exam will involve manipulation of the hip to place tension on the rectus abdominis trunk muscle and adductor thigh muscle groups.
Pain during the manipulation is a common sign of the condition.
Individuals may be asked to walk to look for irregularities in gait patterns or to see if symptoms occur with certain movements.
X-rays will typically reveal joint irregularities as well as sclerosis/thickening of the pubic symphysis.
Magnetic resonance imaging – MRI may reveal joint and surrounding bone inflammation.
Some cases will show no signs of injury on an X-ray or MRI.
Treatment
Effective treatment can take several months or longer. Because inflammation is the underlying cause of symptoms, the treatment will often involve: (Tricia Beatty. 2012)
Rest
Allows the acute inflammation to subside.
During recovery, sleeping flat on the back may be recommended to reduce pain.
Ice and Heat Applications
Ice packs help reduce inflammation.
The heat helps ease pain after the initial swelling has gone down.
Physical Therapy
Physical therapy can be extremely helpful in treating the condition to help regain strength and flexibility. (Alessio Giai Via, et al., 2019)
Anti-inflammatory Medication
Over-the-counter nonsteroidal anti-inflammatory medications – NSAIDs like ibuprofen and naproxen can reduce pain and inflammation.
Assistive Walking Devices
If the symptoms are severe, crutches or a cane may be recommended to reduce stress on the pelvis.
Cortisone
There have been attempts to treat the condition with cortisone injections, but the evidence supporting its use is limited and needs further research. (Alessio Giai Via, et al., 2019)
Prognosis
Once diagnosed, the prognosis for full recovery is optimal but can take time. It can take some individuals six months or more to return to pre-injury level of function, but most return by around three months. If conservative treatment fails to provide relief after six months, surgery could be recommended. (Michael Dirkx, Christopher Vitale. 2023)
Sports Injuries Rehabilitation
References
Gomella, P., & Mufarrij, P. (2017). Osteitis pubis: A rare cause of suprapubic pain. Reviews in urology, 19(3), 156–163. https://doi.org/10.3909/riu0767
Beatty T. (2012). Osteitis pubis in athletes. Current sports medicine reports, 11(2), 96–98. https://doi.org/10.1249/JSR.0b013e318249c32b
Via, A. G., Frizziero, A., Finotti, P., Oliva, F., Randelli, F., & Maffulli, N. (2018). Management of osteitis pubis in athletes: rehabilitation and return to training – a review of the most recent literature. Open access journal of sports medicine, 10, 1–10. https://doi.org/10.2147/OAJSM.S155077
Dirkx M, Vitale C. Osteitis Pubis. [Updated 2022 Dec 11]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK556168/
The Q or quadriceps angle is a measurement of pelvic width that is believed to contribute to the risk of sports injuries in women athletes. Can non-surgical therapies and exercises help rehabilitate injuries?
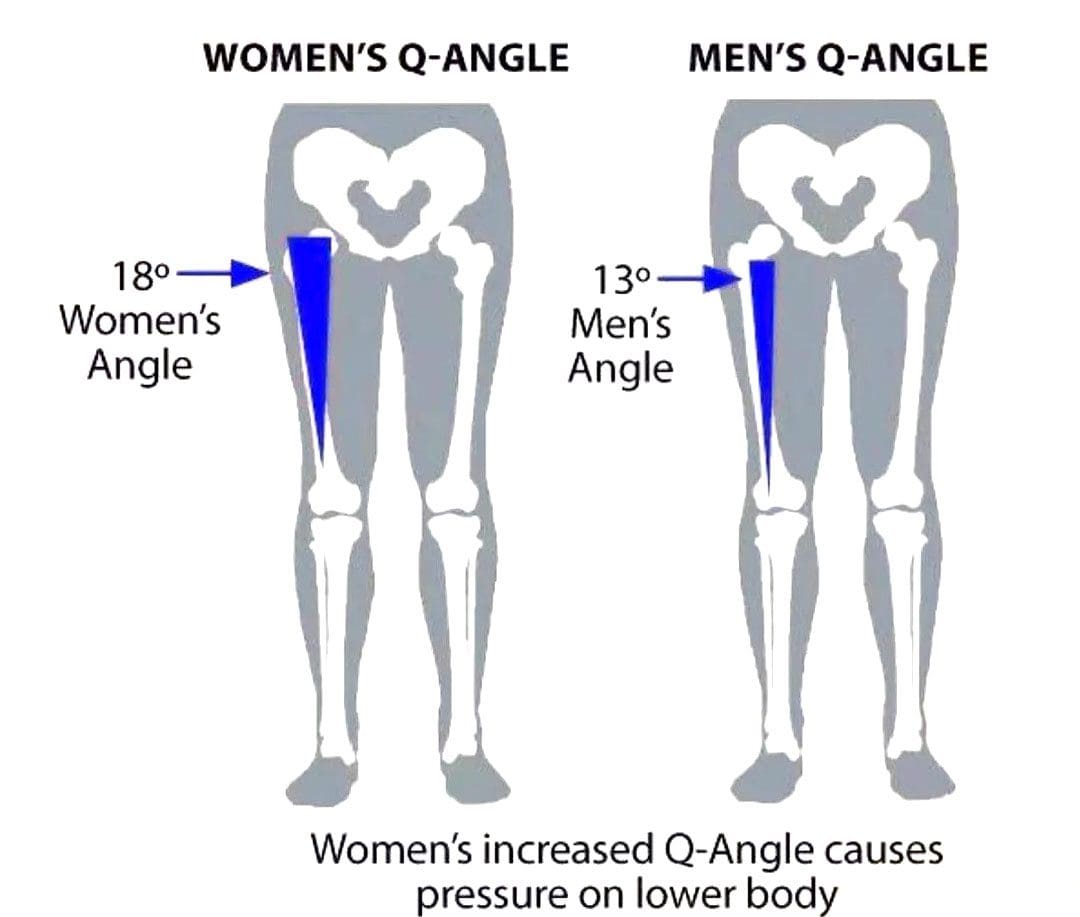
Quadriceps Q – Angle Injuries
The Q angle is the angle where the femur/upper leg bone meets the tibia/lower leg bone. It is measured by two intersecting lines:
One from the center of the patella/kneecap to the anterior superior iliac spine of the pelvis.
The other is from the patella to the tibial tubercle.
On average the angle is three degrees higher in women than men.
Women have biomechanical differences that include a wider pelvis, making it easier to give birth. However, this difference can contribute to knee injuries when playing sports, as an increased Q angle generates more stress on the knee joint, as well as leading to increased foot pronation.
Injuries
Various factors can increase the risk of injury, but a wider Q angle has been linked to the following conditions.
Patellofemoral Pain Syndrome
An increased Q angle can cause the quadriceps to pull on the kneecap, shifting it out of place and causing dysfunctional patellar tracking.
With time, this can cause knee pain (under and around the kneecap), and muscle imbalance.
Foot orthotics and arch supports could be recommended.
Some researchers have found a link, while others have not found the same association. (Wolf Petersen, et al., 2014)
Chondromalacia of the Knee
This is the wearing down of the cartilage on the underside of the kneecap.
An increased Q angle can be a factor that increases stress and causes the knee to lose its stability.
However, this remains controversial, as some studies have found no association between the Q angle and knee injuries.
Chiropractic Treatment
Strengthening Exercises
ACL injury prevention programs designed for women have resulted in reduced injuries. (Trent Nessler, et al., 2017)
The vastus medialis obliquus or VMO is a teardrop-shaped muscle that helps move the knee joint and stabilize the kneecap.
Strengthening the muscle can increase the stability of the knee joint.
Strengthening may require a specific focus on muscle contraction timing.
Closed-chain exercises like wall squats are recommended.
Glute strengthening will improve stability.
Stretching Exercises
Stretching tight muscles will help relax the injured area, increase circulation, and restore range of motion and function.
Muscles commonly found to be tight include the quadriceps, hamstrings, iliotibial band, and gastrocnemius.
Foot Orthotics
Custom-made, flexible orthotics decrease the Q angle and reduce pronation, relieving the added stress on the knee.
A custom orthotic ensures that the foot and leg dynamics are accounted for and corrected.
Motion-control shoes can also help correct overpronation.
Knee Rehabilitation
References
Khasawneh, R. R., Allouh, M. Z., & Abu-El-Rub, E. (2019). Measurement of the quadriceps (Q) angle with respect to various body parameters in young Arab population. PloS one, 14(6), e0218387. https://doi.org/10.1371/journal.pone.0218387
Petersen, W., Ellermann, A., Gösele-Koppenburg, A., Best, R., Rembitzki, I. V., Brüggemann, G. P., & Liebau, C. (2014). Patellofemoral pain syndrome. Knee surgery, sports traumatology, arthroscopy: Official journal of the ESSKA, 22(10), 2264–2274. https://doi.org/10.1007/s00167-013-2759-6
Vaienti, E., Scita, G., Ceccarelli, F., & Pogliacomi, F. (2017). Understanding the human knee and its relationship to total knee replacement. Acta bio-medica : Atenei Parmensis, 88(2S), 6–16. https://doi.org/10.23750/abm.v88i2-S.6507
Mitani Y. (2017). Gender-related differences in lower limb alignment, range of joint motion, and the incidence of sports injuries in Japanese university athletes. Journal of Physical Therapy Science, 29(1), 12–15. https://doi.org/10.1589/jpts.29.12
Nessler, T., Denney, L., & Sampley, J. (2017). ACL Injury Prevention: What Does Research Tell Us? Current reviews in musculoskeletal medicine, 10(3), 281–288. https://doi.org/10.1007/s12178-017-9416-5
Sports activities will result in aches, pains, and injuries that need to be examined by a doctor or specialist for proper diagnosis and treatment. Finding the right sports injury specialist can be one of the most difficult parts of dealing with an injury. The following may help when deciding if a sports chiropractic specialist can help.
Sports Injury Specialist
Sports medicine is the study and practice of medical principles related to the science of sports:
Injury prevention
Injury diagnosis and treatment
Nutrition
Psychology
Sports medicine focuses on the medical and therapeutic aspects of sports physical activity. These individuals can be physicians, surgeons, chiropractors, physical therapists, or providers who regularly work with athletes. Athletes often prefer providers with athletic treatment experience.
Doctor To See First for a Sports Injury
Individuals that belong to an HMO or PPO may find that their primary care physician is the first doctor to see for injury.
A family doctor may not be a sports medicine specialist but may have the expertise to deal with the injury.
Minor musculoskeletal injuries like acute sprains and strains respond well to immediate standard treatments like rest, ice, compression, and elevation.
Individuals with complicated overuse or training injuries, chronic conditions such as tendonitis, or who require surgery will be referred to a specialist.
Family Doctor Treatment
Nearly all family practice physicians can diagnose and treat various sports-related injuries.
Other non-traditional methods to treat conditions and illnesses.
Some may have specific experience in treating sports-related injuries.
Finding the Right Specialist
It is important to find a doctor who can design a treatment plan to heal and rehabilitate the injury properly and get the athlete back to their sport quickly and safely. Medicine is science and art, and injury treatment should be personalized to specific goals of healing and performance. When selecting a healthcare provider to treat injuries or provide advice, personal recommendations from trusted sources are recommended to screen providers. As well as asking other athletes, local teams, gyms, athletic clubs, and healthcare organizations can direct individuals in the right direction. If you can’t find a confident recommendation, look for a certified sports medicine physician online or call the clinic. When calling the office, questions to think about include:
What is your treatment specialty?
What experience do you have treating athletes?
What special training do you have in sports injury care?
What degrees and certifications do you have?
How I Tore My ACL
References
Bowyer, B L et al. “Sports medicine. 2. Upper extremity injuries.” Archives of physical medicine and Rehabilitation vol. 74,5-S (1993): S433-7.
Chang, Thomas J. “Sports Medicine.” Clinics in podiatric medicine and surgery vol. 40,1 (2023): xiii-xiv. doi:10.1016/j.cpm.2022.10.001
Ellen, M I, and J Smith. “Musculoskeletal rehabilitation and sports medicine. 2. Shoulder and upper extremity injuries.” Archives of physical medicine and Rehabilitation vol. 80,5 Suppl 1 (1999): S50-8. doi:10.1016/s0003-9993(99)90103-x
Haskell, William L et al. “Physical activity and public health: updated recommendation for adults from the American College of Sports Medicine and the American Heart Association.” Medicine and science in sports and exercise vol. 39,8 (2007): 1423-34. doi:10.1249/mss.0b013e3180616b27
Sherman, A L, and J L Young. “Musculoskeletal rehabilitation and sports medicine. 1. Head and spine injuries.” Archives of physical medicine and Rehabilitation vol. 80,5 Suppl 1 (1999): S40-9. doi:10.1016/s0003-9993(99)90102-8
Zwolski, Christin, et al. “Resistance Training in Youth: Laying the Foundation for Injury Prevention and Physical Literacy.” Sports Health vol. 9,5 (2017): 436-443. doi:10.1177/1941738117704153
Gymnastics is a demanding and challenging sport. Gymnasts train to be powerful and graceful. Today’s moves have become increasingly technical acrobatic moves with a much higher degree of risk and difficulty. All the stretching, bending, twisting, jumping, flipping, etc., increases the risk of neuromusculoskeletal injuries. Gymnastics injuries are inevitable. Bruises, cuts, and scrapes are common, as are overuse strains and sprains, but severe and traumatic injuries can occur. Injury Medical Chiropractic and Functional Medicine Team can treat and rehabilitate injuries and help to strengthen and prevent injuries. The therapy team will thoroughly evaluate the individual to determine the injury/s severity, identify any weaknesses or limitations, and develop a personalized plan for optimal recovery, stability, and strength.
Gymnastic Injuries
One of the main reasons injuries are more prevalent is because today’s athletes start earlier, spend more time practicing, perform more complex skill sets, and have higher levels of competition. Gymnasts learn to perfect a skill and then train to make their bodies look elegant while executing the routine. These moves require precision, timing, and hours of practice.
Injury Types
Sports injuries are classified as:
Chronic Overuse injuries: These cumulative aches and pains occur over time.
They can be treated with chiropractic and physical therapy and prevented with targeted training and recovery.
Acute Traumatic injuries: These are typically accidents that happen suddenly without warning.
These require immediate first aid.
Most Common Injuries
Gymnasts are taught how to fall and land to lessen the impact on the spine, head, neck, knees, ankles, and wrists.
Back
Common back injuries include muscle strains and spondylolysis.
Bruises and Contusions
Tumbling, twisting, and flipping can result in various bruises and contusions.
Muscle Soreness
This is the sort of muscle soreness experienced 12 to 48 hours after a workout or competition.
Proper rest is necessary for the body to recover fully.
Overtraining Syndrome
Overtraining syndrome happens when individuals train beyond the body’s ability to recover.
Strength and/or flexibility imbalances – one side is stronger.
Chiropractic Care
Our therapists will start with an evaluation and a biomechanical assessment to identify all the factors contributing to the injury. This will consist of a thorough medical history to understand overall health status, training schedule, and the physical demands on the body. The chiropractor will develop a comprehensive program that includes manual and tool-assisted pain relief techniques, mobilization work, MET, core strengthening, targeted exercises, and injury prevention strategies.
Facet Syndrome Chiropractic Treatment
References
Armstrong, Ross, and Nicola Relph. “Screening Tools as a Predictor of Injury in Gymnastics: Systematic Literature Review.” Sports medicine – open vol. 7,1 73. 11 Oct. 2021, doi:10.1186/s40798-021-00361-3
Farì, Giacomo, et al. “Musculoskeletal Pain in Gymnasts: A Retrospective Analysis on a Cohort of Professional Athletes.” International journal of environmental research and public health vol. 18,10 5460. 20 May. 2021, doi:10.3390/ijerph18105460
Kreher, Jeffrey B, and Jennifer B Schwartz. “Overtraining syndrome: a practical guide.” Sports Health vol. 4,2 (2012): 128-38. doi:10.1177/1941738111434406
Meeusen, R, and J Borms. “Gymnastic injuries.” Sports medicine (Auckland, N.Z.) vol. 13,5 (1992): 337-56. doi:10.2165/00007256-199213050-00004
Sweeney, Emily A et al. “Returning to Sport After Gymnastics Injuries.” Current sports medicine reports vol. 17,11 (2018): 376-390. doi:10.1249/JSR.0000000000000533
Westermann, Robert W et al. “Evaluation of Men’s and Women’s Gymnastics Injuries: A 10-Year Observational Study.” Sports Health vol. 7,2 (2015): 161-5. doi:10.1177/1941738114559705
A big part of sports is avoiding and preventing injuries, as injury prevention is far better than rehabilitation and recovery. This is where prehabilitation comes in. Prehabilitation is a personalized, constantly evolving, and developing strengthening exercise program. The program aims to provide sports-specific targeted exercises and activities to maintain athletes’ physical abilities and mental preparedness for their sport. The first step is for an athletic trainer, sports chiropractor, and physical therapist to examine the individual.
Prehabilitation
Everybody is different when it comes to developing an effective prehabilitation program. Every individual’s program should be progressive and re-evaluated to adapt and adjust to the athlete’s needs. The first step is learning to prevent injuries and following basic injury prevention protocols. Knowing what to do when the body sustains an injury, like home treatment and when it’s time to see a doctor.
Athletes
Athletes of all levels are recommended to incorporate a prehabilitation program into their training. As athletes engage in their sport, their bodies adjust to the physical demands of practicing, playing, and training. Imbalances can happen naturally with normal activity but become more pronounced with each practice, game, and training session and often are the cause of injury. The repetitive movements and regular stresses can cause neuromusculoskeletal symptoms to present. This includes:
Tightness of muscle groups.
Pain and discomfort symptoms.
Stabilization issues.
Strength imbalances.
Program
A chiropractic therapist will measure the individual’s range of motion and strength, biomechanics, evaluate medical history, and present health status. Individuals with an injury or a condition can also benefit from prehabilitation.
Each program is personalized and will address total body balance, sports-specific needs, and weaknesses.
The exercises will balance strength, coordination, range of motion, and stabilization.
The premise is looking at and comparing movements from left to right, front to back, and upper to lower body.
Activities can be subtle, focused exercises or a complex movement sequence to stabilize or improve a specific skill.
Programs focus on strengthening and stabilizing the core, abdominals, hips, and back.
Instability is common and often presents from a lack of core training, as athletes tend to focus on what parts of the body their specific sport utilizes, leaving the core without a regular training routine.
A prehabilitation program has to be constantly updated to adjust to the individual’s progress.
Tools like foam rollers, balance boards, weights, and exercise balls are used.
Training
Prehabilitation should start before any acute or chronic injury occurs, but often it takes a few injuries for individuals to decide to get into a prehabilitation program. Depending on an athlete’s training cycle, prehabilitation can be incorporated into practice or as an independent workout and become part of an athlete’s training routine. A session can include the following:
Warm-up and cool-down exercises.
Exercises to perform while resting or waiting during practice.
A targeted workout on specific weaknesses.
A complete workout for days off or active rest days.
Mini workouts for when traveling and recovery days.
For athletes, feeling challenged and motivated can be the difference between success and failure. Working with a trainer, sports chiropractor, and therapists who know sports, understand athletic needs, and communicate well, will contribute to a successful prehabilitation program.
Improving Athletic Performance
References
Durrand, James et al. “Prehabilitation.” Clinical medicine (London, England) vol. 19,6 (2019): 458-464. doi:10.7861/clinmed.2019-0257
Giesche, Florian, et al. “Evidence for the effects of prehabilitation before ACL-reconstruction on return to sport-related and self-reported knee function: A systematic review.” PloS one vol. 15,10 e0240192. 28 Oct. 2020, doi:10.1371/journal.pone.0240192
Halloway S, Buchholz SW, Wilbur J, Schoeny ME. Prehabilitation Interventions for Older Adults: An Integrative Review. Western Journal of Nursing Research. 2015;37(1):103-123. doi:10.1177/0193945914551006
Smith-Ryan, Abbie E et al. “Nutritional Considerations and Strategies to Facilitate Injury Recovery and Rehabilitation.” Journal of athletic training vol. 55,9 (2020): 918-930. doi:10.4085/1062-6050-550-19
Vincent, Heather K, and Kevin R Vincent. “Rehabilitation and Prehabilitation for Upper Extremity in Throwing Sports: Emphasis on Lacrosse.” Current sports medicine reports vol. 18,6 (2019): 229-238. doi:10.1249/JSR.0000000000000606
Vincent, Heather K et al. “Injury Prevention, Safe Training Techniques, Rehabilitation, and Return to Sport in Trail Runners.” Arthroscopy, sports medicine, and rehabilitation vol. 4,1 e151-e162. 28 Jan. 2022, doi:10.1016/j.asmr.2021.09.032
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine

 Ice Tape
Ice Tape