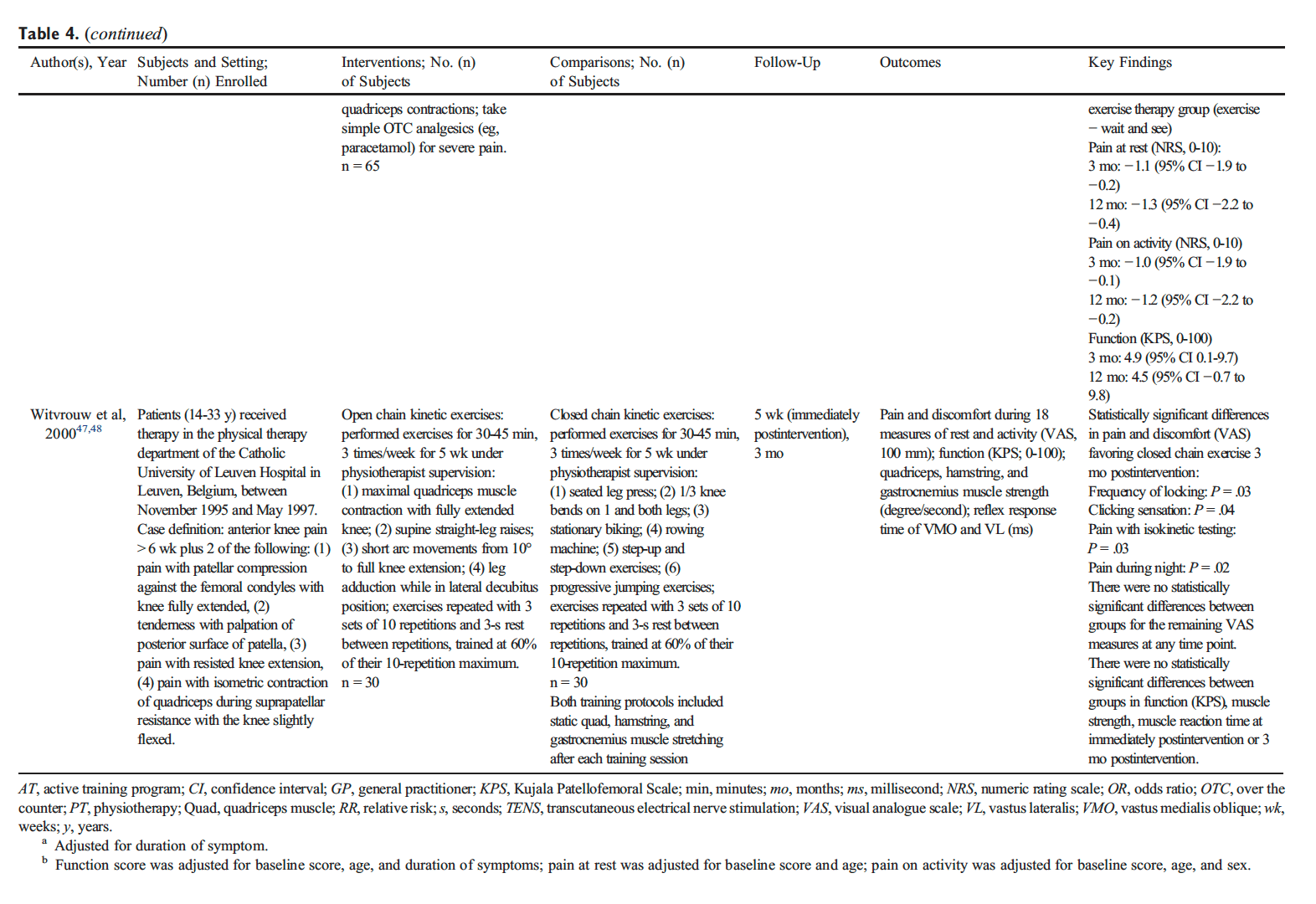
Low back pain, or LBP, is a very common condition which affects the lumbar spine, or the lower section of the spine. Approximately more than 3 million cases of LBP are diagnosed in the United States aline every year and about 80 percent of adults worldwide experience low back pain at some point during their lifetime. Low back pain is generally caused by injury to a muscle (strain) or ligament (sprain) or due to damage from a disease. Common causes of LBP include poor posture, lack of regular exercise,�improper lifting, fracture, herniated discs and/or arthritis. Most cases of low back pain may often go away on their own, however, when LBP becomes chronic, it may be important to seek immediate medical attention. Two therapeutic methods have been utilized to improve LBP. The following article compares the effects of Pilates and McKenzie training on LBP.
A Comparison of the Effects of Pilates and McKenzie Training on Pain and General Health in Men with Chronic Low Back Pain: A Randomized Trial
Abstract
Background: Today, chronic low back pain is one of the special challenges in healthcare. There is no unique approach to treat chronic low back pain. A variety of methods are used for the treatment of low back pain, but the effects of these methods have not yet been investigated adequately.
Aim: The aim of this study was to compare the effects of Pilates and McKenzie training on pain and general health of men with chronic low back pain.
Materials and Methods: Thirty-six patients with chronic low back pain were chosen voluntarily and assigned to three groups of 12 each: McKenzie group, Pilates group, and control group. The Pilates group participated in 1-h exercise sessions, three sessions a week for 6 weeks. McKenzie group performed workouts 1 h a day for 20 days. The control group underwent no treatment. The general health of all participants was measured by the General Health Questionnaire 28 and pain by the McGill Pain Questionnaire.
Results: After therapeutic exercises, there was no significant difference between Pilates and McKenzie groups in pain relief (P = 0.327). Neither of the two methods was superior over the other for pain relief. However, there was a significant difference in general health indexes between Pilates and McKenzie groups.
Conclusion: Pilates and McKenzie training reduced pain in patients with chronic low back pain, but the Pilates training was more effective to improve general health.
Keywords:Chronic back pain, general health, Mckenzie training, pain, Pilates training
Introduction
Low back pain with a history of more than 3 months and without any pathological symptom is called chronic low back pain. For patient with chronic low back pain, the physician should take into consideration the likelihood of muscle pain development with spinal origin, in addition to low back pain with unknown origin. This type of pain may be mechanical (increase in pain with movement or physical pressure) or nonmechanical (increase in pain at the rest time).[1] Low back pain or spine pain is the most common musculoskeletal complication.[2] About 50%�80% of healthy people may experience low back pain during their lifetime, and about 80% of the problems are related to the spine and occur in the lumbar area.[3] Low back pain may be caused by trauma, infection, tumors, etc.[4] Mechanical injuries which are caused by overuse of a natural structure, deformity of an anatomical structure, or the injury in the soft tissue are the most common reasons for back pain. From occupational health perspective, back pain is among the most important reasons for the absence from work and occupational disability;[5] in fact, the longer the period of disease,[6] the less likely it is to improve and return to work.[1] Disability due to low back pain in addition to disturbance in doing daily and social activities has a very negative effect, from social and economic perspectives, on the patient and the community, which makes chronic low back pain highly important.[3] Today, chronic low back pain is one of the critical challenges in medicine. Patients with chronic low back pain are responsible for 80% of the costs paid for the treatment of low back pain that is also the reason for mobility restrictions in most people under 45 years.[7] In the developed countries, the overall cost paid for low back pain per year is 7.1 of total share of the gross national product. Clearly, most of the cost is related to counseling and treatment of patients with chronic low back pain rather than with intermittent and recursive low back pain.[8] The existence of various methods of treatment is because of no single cause of low back pain.[9] A variety of methods such as pharmacotherapy, acupuncture, infusions, and physical methods are the most common interventions for treatment of low back pain. However, the effects of these methods remain to be fully known.[6] An exercise program, developed based on the physical conditions of patients, can promote the quality of life in patients with chronic disease.[10,11,12,13,14]
Literature shows that the effect of exercise in controlling chronic low back pain is under study and there is strong evidence about the fact that movement therapy is effective to treat low back pain.[15] However, no specific recommendations exist about the type of exercise, and the effects of certain types of movement therapies have been determined in few studies.[9] Pilates training consists of the exercises that focus on improving flexibility and strength in all the body organs, without increasing the mass of muscles or destroying them. This training method consists of controlled movements that form a physical harmony between the body and brain, and can raise the ability of the body of people at any age.[16] In addition, people who do Pilates exercise would have better sleep and less fatigue, stress, and nervousness. This training method is based on standing, sitting, and lying positions, without intervals, jumping, and leaping; thus, it may reduce injuries resulting from the joint damage because the exercise movements in the ranges of motion in the above three positions are performed with deep breathing and muscle contraction.[17] McKenzie method, also called mechanical diagnosis and therapy and based on the patient’s active participation, is used and trusted by patients and the people who use this method worldwide. This method is based on physical therapy which has been frequently studied. The distinctive characteristic of this method is the principle of initial assessment.[18] This principle is a reliable and safe method to make a diagnosis that makes the correct treatment planning possible. In this way, the time and energy are not spent for costly tests, rather McKenzie therapists, using a valid indicator, quickly recognize that how much and how this method is fruitful for the patient. More appropriately, McKenzie method is a comprehensive approach based on the correct principles whose full understanding and following is very fruitful.[19] In the recent years, non-pharmacological approaches have attracted the attention of physicians and patients with low back pain.[20] Complementary therapies[21] and treatments with holistic nature (to increase physical and mental well-being) are appropriate to manage physical illness.[13] Complementary therapies can slow down disease progression and improve capacity and physical performance. The aim of the present study is to compare the effect of the Pilates and McKenzie training on pain and general health in men with chronic low back pain.
Materials and Methods
This randomized clinical trial was conducted in Shahrekord, Iran. The total study population screened was 144. We decided to enroll at least 25% of the population, 36 individuals, using a systematic random sampling. First, the participants were numbered and a list was developed. The first case was selected using random number table and then one out of four patients was randomly enrolled. This process continued till a desired number of participants were enrolled. Then, the participants were randomly assigned to experimental (Pilates and McKenzie training) groups and control group. After explaining the research purposes to the participants, they were asked to complete the consent form for participation in the study. Furthermore, the patients were ensured that the research data are kept confidential and used only for research purposes.
Inclusion Criteria
The study population included men aged 40�55 years in Shahrekord, South-West Iran, with chronic back pain, that is, history of more than 3 months of low back pain and no specific disease or other surgery.
Exclusion Criteria
The exclusion criteria were low back arch or so-called army back, serious spinal pathology such as tumors, fractures, inflammatory diseases, previous spinal surgery, nerve root compromise in the lumbar region, spondylolysis or spondylolisthesis, spinal stenosis, neurological disorders, systemic diseases, cardiovascular diseases, and receiving other therapies simultaneously. The examiner who assessed the outcomes was blinded to group assignment. Twenty-four hours before the training, a pretest was administered to all three groups to determine pain and general health; and then, the training began after completion of the McGill Pain Questionnaire (MPQ) and the General Health Questionnaire-28 (GHQ-28). The MPQ can be used to evaluate a person experiencing significant pain. It can be used to monitor the pain over time and to determine the effectiveness of any intervention. Minimum pain score: 0 (would not be seen in a person with true pain), maximum pain score: 78, and the higher the pain score the more severe the pain. Investigators reported that the construct validity and the reliability of the MPQ were reported as a test-retest reliability of 0.70.[22] The GHQ is a self-administered screening questionnaire. Test-retest reliability has been reported to be high (0.78�0 0.9) and inter- and intra-rater reliability have both been shown to be excellent (Cronbach’s ? 0.9�0.95). High internal consistency has also been reported. The lower the score is, the better the general health is.[23]
The participants in the experimental groups started training program under supervision of a sports medicine specialist. The training program consisted of 18 sessions of supervised individual training for both groups, with the sessions held three times per week for 6 weeks. Each training session lasted for an hour and was performed at the Physiotherapy Clinic in the School of Rehabilitation of the Shahrekord University of Medical Sciences in 2014�2015. The first experimental group performed Pilates training for 6 weeks, three times a week about an hour per session. In each session, first, a 5-min warm-up and preparation procedures were run; and at the end, stretching and walking were done to return to the baseline condition. In the McKenzie group, six exercises were used: Four extension-type exercises and two flexion-types. The extension-type exercises were performed in prone and standing positions, and the flexion-type exercises in the supine and sitting positions. Each exercise was run ten times. In addition, the participants conducted twenty daily individual training sessions for an hour.[18] After training of both groups, the participants filled out the questionnaires and then the collected data were presented in both descriptive and inferential statistics. Furthermore, the control group without any training, at the end of a period when other groups have completed, filled the questionnaire. Descriptive statistics were used for central tendency indicators such as mean (� standard deviation) and relevant diagrams were used to describe the data. Inferential statistics, one-way ANOVA and post hoc Tukey’s test, were used to analyze the data. Data analysis was done by SPSS Statistics for Windows, Version 21.0 (IBM Corp. Released 2012. IBM Armonk, NY: IBM Corp). P < 0.05 was considered statistically significant.
Dr. Alex Jimenez’s Insight
Alongside the use of spinal adjustments and manual manipulations for low back pain, chiropractic care commonly utilizes therapeutic exercise methods to improve LBP symptoms, restoring the affected individual’s strength, flexibility and mobility as well as promoting a faster recovery. The Pilates and McKenzie method of training, as mentioned in the article, are compared to determine which therapeutic exercise is best for treating low back pain. As�a Level I Certified Pilates Instructor, Pilates training is implemented with chiropractic treatment to improve LBP more effectively. Patients participating in a therapeutic exercise method alongside a primary form of treatment for low back pain can experience additional benefits. McKenzie training can also be implemented with chiropractic treatment to further improve LBP symptoms. The purpose of this research study is to demonstrate evidence-based information on the benefits of Pilates and McKenzie methods for low back pain as well as to educate patients on which of the two therapeutic exercises should be considered to help treat their symptoms and achieve overall health and wellness.
Level I Certified Pilates Instructors at Our Location
Dr. Alex Jimenez D.C., C.C.S.T | Chief Clinical Director and Level I Certified Pilates Instructor
Truide Torres | Director of Patient Relations Advocate Dept. and Level I Certified Pilates Instructor
Results
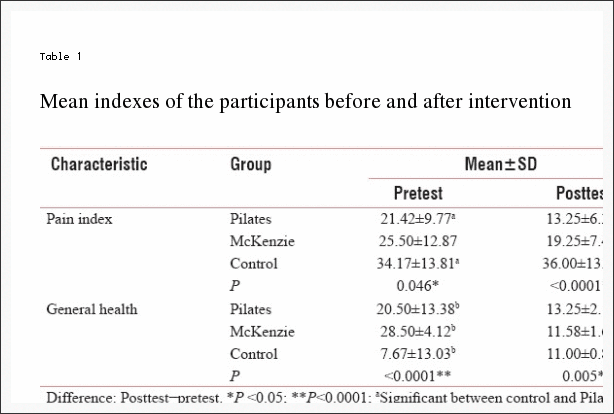
The results showed no significant difference between the case and control groups regarding the gender, marital status, job, educational level, and income. The results showed changes in pain index and general health in the participants before and after Pilates and McKenzie training in the two experimental and even control groups [Table 1].
A significant difference was seen in pain and general health between the control and the two experimental groups at the pre- and post-test, so that the exercise training (both Pilates and McKenzie) resulted in reduced pain and promoted general health; while in the control group, pain increased and general health declined.
Discussion
The results of this study indicate that back pain reduced and general health enhanced after exercise therapy with both Pilates and McKenzie training, but in the control group, pain was intensified. Petersen et al. study on 360 patients with chronic low back pain concluded that at the end of 8 weeks of McKenzie training and high-intensity endurance training and 2 months training at home, pain and disability decreased in McKenzie group at the end of 2 months, but at the end of 8 months, no differences were seen among the treatments.[24]
The results of another study show that McKenzie training is a beneficial method for reducing pain and increasing the movements of the spine in patients with chronic low back pain.[18] Pilates training can be an effective method for improving general health, athletic performance, proprioception, and reduction of pain in patients with chronic low back pain.[25] The improvements in strength seen in the participants in the present study were more likely to be due to decrease in pain inhibition than to neurological changes in muscle firing/recruitment patterns or to morphological (hypertrophic) changes in the muscle. In addition, neither of the treatments was superior over the other in view of reducing the intensity of pain. In the present study, 6 weeks of McKenzie training led to significant reduction in pain levels in men with chronic low back pain. The rehabilitation of patients with chronic low back pain is aimed to restore strength, endurance, and flexibility of soft tissues.
Udermann et al. showed that McKenzie training improved pain, disability, and psychosocial variables in patients with chronic low back pain, and back stretching training did not have any additional effect on pain, disability, and psychosocial variables.[26] The results of another study show that there is a reduction in pain and disability due to McKenzie method for at least 1 week in comparison with the passive treatment in patients with low back pain, but reduction in pain and disability due to McKenzie method in comparison with the active treatment methods is desirable within 12 weeks after treatment. Overall, McKenzie treatment is more effective than passive methods to treat low back pain.[27] One of the popular exercise therapies for patients with low back pain is McKenzie training program. McKenzie method leads to improvement of low back pain symptoms such as pain in the short-term. Moreover, McKenzie therapy is more effective in comparison with passive treatments. This training is designed to mobilize the spine and to strengthen the lumbar muscles. Previous studies have shown that weakness and atrophy in the body central muscles, particularly the transverse abdominal muscle in patients with low back pain.[28] The results of this research also showed that there was a significant difference in the general health indexes between Pilates and McKenzie groups. In the present study, 6 weeks of Pilates and McKenzie training led to a significant reduction in the level of general health (physical symptoms, anxiety, social dysfunction, and depression) in men with chronic low back pain and the general health in Pilates training group improved. The results of most studies show that exercise therapy reduces pain and improves general health in patients with chronic low back pain. Importantly, the agreement about the duration, type, and intensity of the training remains to be achieved and there is no definite training program that can have the best effect on patients with chronic low back pain. Therefore, more research is needed to determine the best duration and treatment method to reduce and improve general health in patients with low back pain. In the Al-Obaidi et al. study, pain, fear, and functional disability improved after 10 weeks of treatment in patients.[5]
Besides that McKenzie training increases the range of motion of lumbar flexion. Overall, neither of the two methods of treatment was superior over the other.[18]
Borges et al. concluded that after 6 weeks of treatment, the average index of pain in experimental group was lower than the control group. Furthermore, the general health of the experimental group exhibited greater improvement than the control group. The results of this research support recommending Pilates training to patients with chronic low back pain.[29] Caldwell et al. on the university students concluded that Pilates training and Tai chi guan improved mental parameters such as self-sufficiency, quality of sleep, and morality of students but had no effect on physical performance.[30] Garcia et al. study on 148 patients with nonspecific chronic low back pain concluded that treating patients with nonspecific chronic low back pain by McKenzie training and back school caused disability to improve after treatment, but quality of life, pain, and the range of motor flexibility did not change. McKenzie treatment is typically more effective on disability than back school program.[19]
The overall findings of this study are supported by the literature, demonstrating that a Pilates program may offer a low-cost, safe alternative to the treatment of low back pain in this specific group of patients. Similar effects have been found in patients with unspecific chronic low back pain.[31]
Our study had good levels of internal and external validity and thus can guide therapists and patients considering therapies of choice for back pain. The trial included a number of features to minimize bias such as prospectively registering and following a published protocol.
Study Limitation
Small sample size enrolled in this study limits the generalization of the study findings.
Conclusion
The results of this study showed that 6-week Pilates and McKenzie training reduced pain in patients with chronic low back pain, but there was no significant difference between the effect of two therapeutic methods on pain and both exercise protocols had the same effect. In addition, Pilates and McKenzie training improved general health; however, according to the mean general health changes after the exercise therapy, it can be argued that the Pilates training has a greater effect in improving general health.
Financial Support and Sponsorship
Nil.
Conflicts of Interest
There are no conflicts of interest.
In conclusion,�when comparing the effects of Pilates and McKenzie training on general health as well as on painful symptoms in men with chronic low back pain, the evidence-based research study determined that both the Pilates and the McKenzie method of training effectively reduced pain in patients with chronic LBP. There was no significant difference between the two therapeutic methods altogether, however, the mean results of the research study demonstrated that Pilates training was more effective towards improving general health in men with chronic low back pain than McKenzie training.� Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Sciatica
Sciatica is referred to as a collection of symptoms rather than a single type of injury or condition. The symptoms are characterized as radiating pain, numbness and tingling sensations from the sciatic nerve in the lower back, down the buttocks and thighs and through one or both legs and into the feet. Sciatica is commonly the result of irritation, inflammation or compression of the largest nerve in the human body, generally due to a herniated disc or bone spur.
1. Bergstr�m C, Jensen I, Hagberg J, Busch H, Bergstr�m G. Effectiveness of different interventions using a psychosocial subgroup assignment in chronic neck and back pain patients: A 10-year follow-up. Disabil Rehabil. 2012;34:110�8. [PubMed]
2. Hoy DG, Protani M, De R, Buchbinder R. The epidemiology of neck pain. Best Pract Res Clin Rheumatol. 2010;24:783�92. [PubMed]
3. Balagu� F, Mannion AF, Pellis� F, Cedraschi C. Non-specific low back pain. Lancet. 2012;379:482�91. [PubMed]
4. Sadock BJ, Sadock VA. Kaplan and Sadock’s Synopsis of Psychiatry: Behavioral Sciences/Clinical Psychiatry. New York: Lippincott Williams & Wilkins; 2011.
5. Al-Obaidi SM, Al-Sayegh NA, Ben Nakhi H, Al-Mandeel M. Evaluation of the McKenzie intervention for chronic low back pain by using selected physical and bio-behavioral outcome measures. PM R. 2011;3:637�46. [PubMed]
6. Dehkordi AH, Heydarnejad MS. Effect of booklet and combined method on parents’ awareness of children with beta-thalassemia major disorder. J Pak Med Assoc. 2008;58:485�7. [PubMed]
7. van der Wees PJ, Jamtvedt G, Rebbeck T, de Bie RA, Dekker J, Hendriks EJ. Multifaceted strategies may increase implementation of physiotherapy clinical guidelines: A systematic review. Aust J Physiother. 2008;54:233�41. [PubMed]
8. Maas ET, Juch JN, Groeneweg JG, Ostelo RW, Koes BW, Verhagen AP, et al. Cost-effectiveness of minimal interventional procedures for chronic mechanical low back pain: Design of four randomised controlled trials with an economic evaluation. BMC Musculoskelet Disord. 2012;13:260. [PMC free article][PubMed]
9. Hernandez AM, Peterson AL. Handbook of Occupational Health and Wellness. Springer: 2012. Work-related musculoskeletal disorders and pain; pp. 63�85.
10. Hassanpour Dehkordi A, Khaledi Far A. Effect of exercise training on the quality of life and echocardiography parameter of systolic function in patients with chronic heart failure: A randomized trial. Asian J Sports Med. 2015;6:e22643. [PMC free article][PubMed]
11. Hasanpour-Dehkordi A, Khaledi-Far A, Khaledi-Far B, Salehi-Tali S. The effect of family training and support on the quality of life and cost of hospital readmissions in congestive heart failure patients in Iran. Appl Nurs Res. 2016;31:165�9. [PubMed]
12. Hassanpour Dehkordi A. Influence of yoga and aerobics exercise on fatigue, pain and psychosocial status in patients with multiple sclerosis: A Randomized Trial. J Sports Med Phys Fitness. 2015 [Epub ahead of print] [PubMed]
13. Hassanpour-Dehkordi A, Jivad N. Comparison of regular aerobic and yoga on the quality of life in patients with multiple sclerosis. Med J Islam Repub Iran. 2014;28:141. [PMC free article][PubMed]
14. Heydarnejad S, Dehkordi AH. The effect of an exercise program on the health-quality of life in older adults. A randomized controlled trial. Dan Med Bull. 2010;57:A4113. [PubMed]
15. van Middelkoop M, Rubinstein SM, Verhagen AP, Ostelo RW, Koes BW, van Tulder MW. Exercise therapy for chronic nonspecific low-back pain. Best Pract Res Clin Rheumatol. 2010;24:193�204. [PubMed]
16. Critchley DJ, Pierson Z, Battersby G. Effect of pilates mat exercises and conventional exercise programmes on transversus abdominis and obliquus internus abdominis activity: Pilot randomised trial. Man Ther. 2011;16:183�9. [PubMed]
17. Kloubec JA. Pilates for improvement of muscle endurance, flexibility, balance, and posture. J Strength Cond Res. 2010;24:661�7. [PubMed]
18. Hosseinifar M, Akbari A, Shahrakinasab A. The effects of McKenzie and lumbar stabilization exercises on the improvement of function and pain in patients with chronic low back pain: A randomized controlled trial. J Shahrekord Univ Med Sci. 2009;11:1�9.
19. Garcia AN, Costa Lda C, da Silva TM, Gondo FL, Cyrillo FN, Costa RA, et al. Effectiveness of back school versus McKenzie exercises in patients with chronic nonspecific low back pain: A randomized controlled trial. Phys Ther. 2013;93:729�47. [PubMed]
20. Hassanpour-Dehkordi A, Safavi P, Parvin N. Effect of methadone maintenance treatment of opioid dependent fathers on mental health and perceived family functioning of their children. Heroin Addict Relat Clin. 2016;18(3):9�14.
21. Shahbazi K, Solati K, Hasanpour-Dehkordi A. Comparison of hypnotherapy and standard medical treatment alone on quality of life in patients with irritable bowel syndrome: A Randomized Control Trial. J Clin Diagn Res. 2016;10:OC01�4. [PMC free article][PubMed]
22. Ngamkham S, Vincent C, Finnegan L, Holden JE, Wang ZJ, Wilkie DJ. The McGill Pain Questionnaire as a multidimensional measure in people with cancer: An integrative review. Pain Manag Nurs. 2012;13:27�51. [PMC free article][PubMed]
23. Sterling M. General health questionnaire-28 (GHQ-28) J Physiother. 2011;57:259. [PubMed]
24. Petersen T, Kryger P, Ekdahl C, Olsen S, Jacobsen S. The effect of McKenzie therapy as compared with that of intensive strengthening training for the treatment of patients with subacute or chronic low back pain: A randomized controlled trial. Spine (Phila Pa 1976) 2002;27:1702�9. [PubMed]
25. Gladwell V, Head S, Haggar M, Beneke R. Does a program of pilates improve chronic non-specific low back pain? J Sport Rehabil. 2006;15:338�50.
26. Udermann BE, Mayer JM, Donelson RG, Graves JE, Murray SR. Combining lumbar extension training with McKenzie therapy: Effects on pain, disability, and psychosocial functioning in chronic low back pain patients. Gundersen Lutheran Med J. 2004;3:7�12.
27. Machado LA, Maher CG, Herbert RD, Clare H, McAuley JH. The effectiveness of the McKenzie method in addition to first-line care for acute low back pain: A randomized controlled trial. BMC Med. 2010;8:10. [PMC free article][PubMed]
28. Kilpikoski S. The McKenzie Method in Assessing, Classifying and Treating Non-Specific Low Back Pain in Adults with Special Reference to the Centralization Phenomenon. Jyv�skyl� University of Jyv�skyl� 2010
29. Borges J, Baptista AF, Santana N, Souza I, Kruschewsky RA, Galv�o-Castro B, et al. Pilates exercises improve low back pain and quality of life in patients with HTLV-1 virus: A randomized crossover clinical trial. J Bodyw Mov Ther. 2014;18:68�74. [PubMed]
30. Caldwell K, Harrison M, Adams M, Triplett NT. Effect of pilates and taiji quan training on self-efficacy, sleep quality, mood, and physical performance of college students. J Bodyw Mov Ther. 2009;13:155�63. [PubMed]
31. Altan L, Korkmaz N, Bingol U, Gunay B. Effect of pilates training on people with fibromyalgia syndrome: A pilot study. Arch Phys Med Rehabil. 2009;90:1983�8. [PubMed]
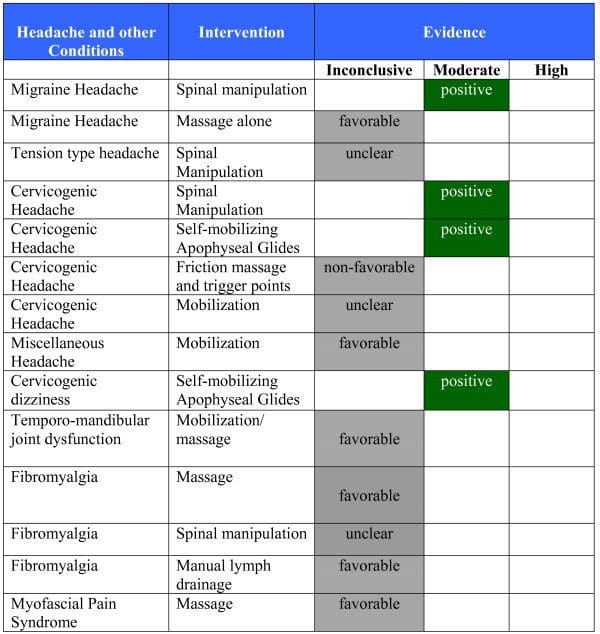
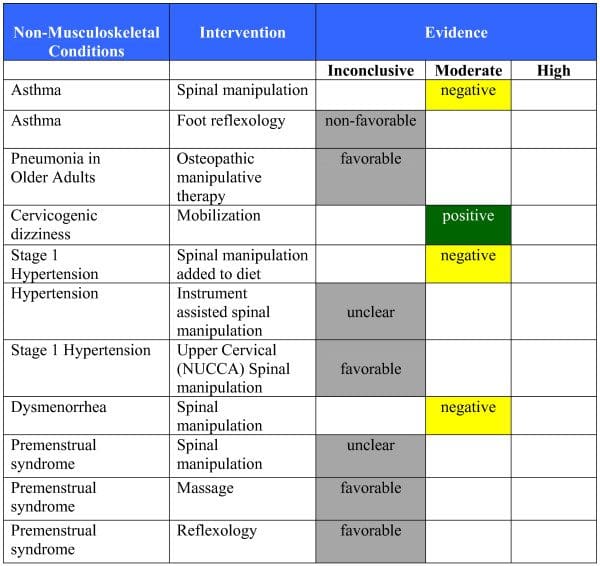
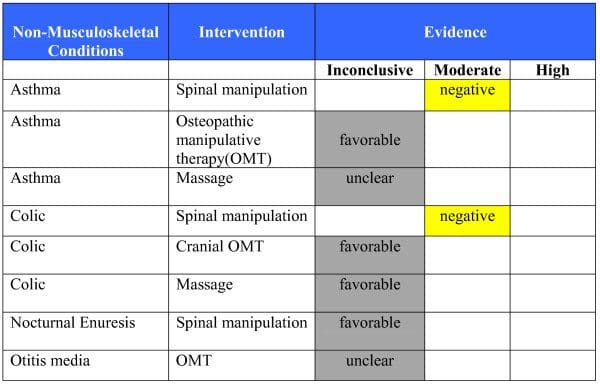
Chiropractic Management of Low Back Pain and Low Back-Related Leg Complaints: A Literature Synthesis
Chiropractic care is a well-known complementary and alternative treatment option frequently used to diagnose, treat and prevent injuries and conditions of the musculoskeletal and nervous systems. Spinal health issues are among some of the most common reasons people seek chiropractic care, especially for low back pain and sciatica complaints. While there are many different types of treatments available to help improve low back pain and sciatica symptoms, many individuals will often prefer natural treatment options over the use of drugs/medications or surgical interventions. The following research study demonstrates a list of evidence-based chiropractic treatment methods and their effects towards improving a variety of spinal health issues.
Abstract
Objectives: The purpose of this project was to review the literature for the use of spinal manipulation for low back pain (LBP).
Methods: Asearch strategymodified fromthe Cochrane Collaboration reviewforLBP was conducted through the following databases: PubMed, Mantis, and the Cochrane Database. Invitations to submit relevant articles were extended to the profession via widely distributed professional news and association media. The Scientific Commission of the Council on Chiropractic Guidelines and Practice Parameters (CCGPP) was charged with developing literature syntheses, organized by anatomical region, to evaluate and report on the evidence base for chiropractic care. This article is the outcome of this charge. As part of the CCGPP process, preliminary drafts of these articles were posted on the CCGPP Web site www.ccgpp.org (2006-8) to allow for an open process and the broadest possible mechanism for stakeholder input.
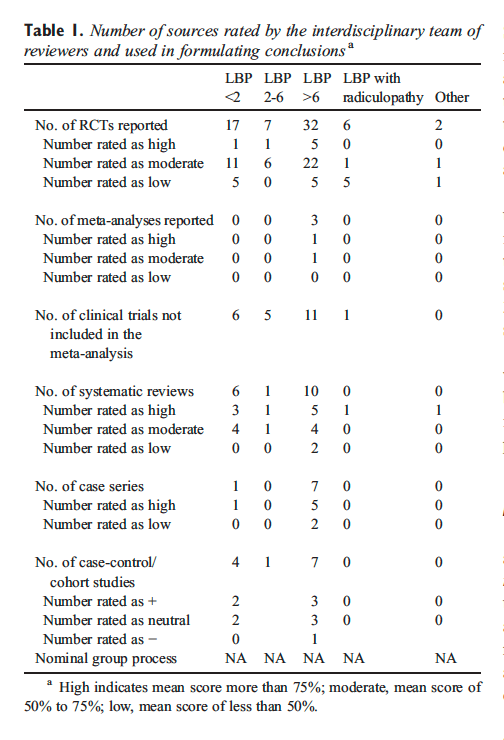
Results: A total of 887 source documents were obtained. Search results were sorted into related topic groups as follows: randomized controlled trials (RCTs) of LBP and manipulation; randomized trials of other interventions for LBP; guidelines; systematic reviews and meta-analyses; basic science; diagnostic-related articles, methodology; cognitive therapy and psychosocial issues; cohort and outcome studies; and others. Each group was subdivided by topic so that team members received approximately equal numbers of articles from each group, chosen randomly for distribution. The team elected to limit consideration in this first iteration to guidelines, systematic reviews, meta-analyses, RCTs, and coh ort studies. This yielded a total of 12 guidelines, 64 RCTs, 13 systematic reviews/meta-analyses, and 11 cohort studies.
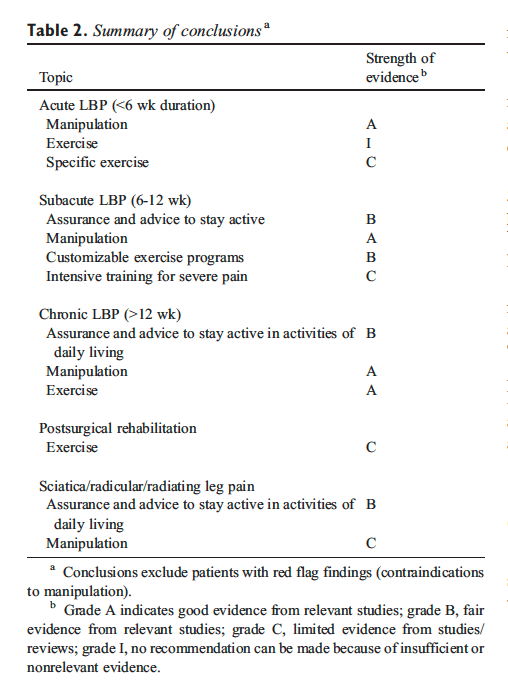
Conclusions: As much or more evidence exists for the use of spinal manipulation to reduce symptoms and improve function in patients with chronic LBP as for use in acute and subacute LBP. Use of exercise in conjunction with manipulation is likely to speed and improve outcomes as well as minimize episodic recurrence. There was less evidence for the use of manipulation for patients with LBP and radiating leg pain, sciatica, or radiculopathy. (J Manipulative Physiol Ther 2008;31:659-674)
The Council on Chiropractic Guidelines and Practice Parameters (CCGPP) was formed in 1995 by the Congress of Chiropractic State Associations with assistance from the American Chiropractic Association, Association of Chiropractic Colleges, Council on Chiropractic Education, Federation of Chiropractic Licensing�Boards, Foundation for the Advancement of Chiropractic Sciences, Foundation for Chiropractic Education and Research, International Chiropractors Association, National Association of Chiropractic Attorneys, and the National Institute for Chiropractic Research. The charge to the CCGPP was to create a chiropractic �best practices� document. The Council on Chiropractic Guidelines and Practice Parameters was delegated to examine all existing guidelines, parameters, protocols, and best practices in the United States and other nations in the construction of this document.
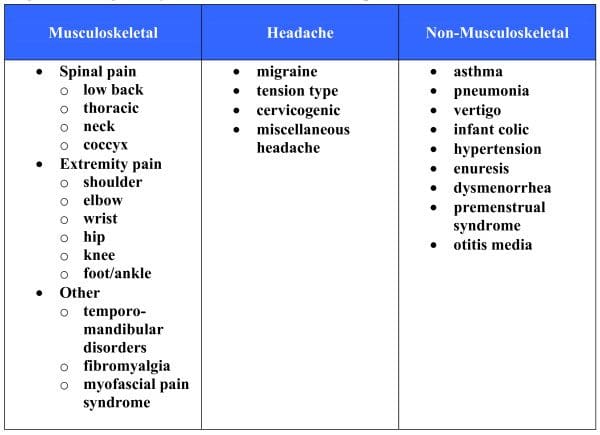
Toward that end, the Scientific Commission of CCGPP was charged with developing literature syntheses, organized by region (neck, low back, thoracic, upper and lower extremity, soft tissue) and the nonregional categories of nonmusculoskeletal, prevention/health promotion, special populations, subluxation, and diagnostic imaging.
The purpose of this work is to provide a balanced interpretation of the literature to identify safe and effective treatment options in the care of patients with low back pain (LBP) and related disorders. This evidence summary is intended to serve as a resource for practitioners to assist them in consideration of various care options for such patients. It is neither a replacement for clinical judgment nor a prescriptive standard of care for individual patients.
Methods
Process development was guided by experience of commission members with the RAND consensus process, Cochrane collaboration, Agency for Health Care and Policy Research, and published recommendations modified to the needs of the council.
Identification and Retrieval
The domain for this report is that of LBP and low backrelated leg symptoms. Using surveys of the profession and publications on practice audits, the team selected the topics for review by this iteration.
Topics were selected based on the most common disorders seen and most common classifications of treatments used by chiropractors based on the literature. Material for review was obtained through formal hand searches of published literature and of electronic databases, with assistance from a professional chiropractic college librarian. A search strategy was developed, based upon the CochraneWorking Group for Low Back Pain. Randomized controlled trials (RCTs), systematic reviews/meta-analyses, and guidelines published through 2006 were included; all other types of studies were included through 2004. Invitations to submit relevant articles were extended to the profession via widely distributed professional news and association media. Searches focused on guidelines, meta-analyses, systematic reviews, randomized clinical trials, cohort studies, and case series.
Evaluation
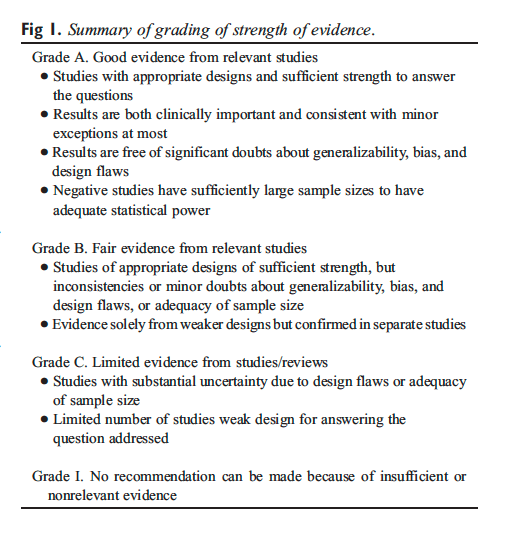
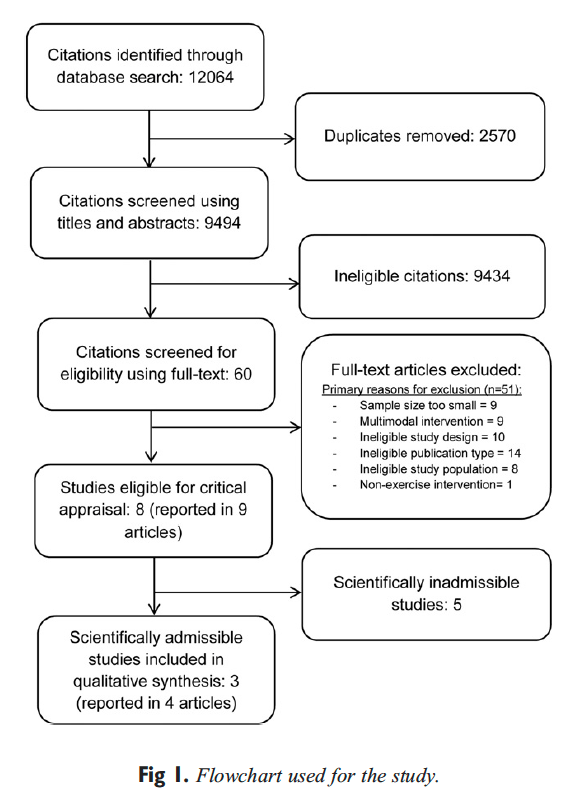
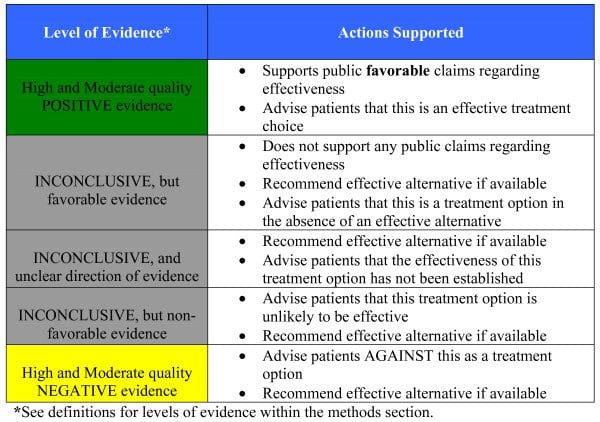
Standardized and validated instruments used by the Scottish Intercollegiate Guidelines Network were used to evaluate RCTs and systematic reviews. For guidelines, the Appraisal of Guidelines for Research and Evaluation instrument was used. A standardized method for grading the strength of the evidence was used, as summarized in Figure 1. Each team’s multidisciplinary panel conducted the review and evaluation of the evidence.
Search results were sorted into related topic groups as follows: RCTs of LBP and manipulation; randomized trials of other interventions for LBP; guidelines; systematic reviews and meta-analyses; basic science; diagnosticrelated articles; methodology; cognitive therapy and psychosocial issues; cohort and outcome studies; and others. Each group was subdivided by topic so that team members received approximately equal numbers of articles from each group, chosen randomly for distribution. On the basis of the CCGPP formation of an iterative process and the volume of work available, the team elected to limit consideration in this first iteration to guidelines, systematic reviews, meta-analyses, RCTs, and cohort studies.
Dr. Alex Jimenez’s Insight
How does chiropractic care benefit people with low back pain and sciatica?�As a chiropractor experienced in the management of a variety of spine health issues, including low back pain and sciatica, spinal adjustments and manual manipulations, as well as other non-invasive treatment methods, can be safely and effectively implemented towards the improvement of back pain symptoms. The purpose of the following research study is to demonstrate the evidence-based effects of chiropractic in the treatment of injuries and conditions of the musculoskeletal and nervous systems. The information in this article can educate patients on how alternative treatment options can help improve their low back pain and sciatica. As a chiropractor, patients may also be referred to other healthcare professionals, such as physical therapists, functional medicine practitioners and medical doctors, to help them further manage their low back pain and sciatica symptoms. Chiropractic care can be used to avoid surgical interventions for spine health issues.
Results and Discussion
A total of 887 source documents were initially obtained. This included a total of 12 guidelines, 64 RCTs, 20 systematic reviews/meta-analyses, and 12 cohort studies. Table 1 provides an overall summary of the number of studies evaluated.
Assurance and Advice
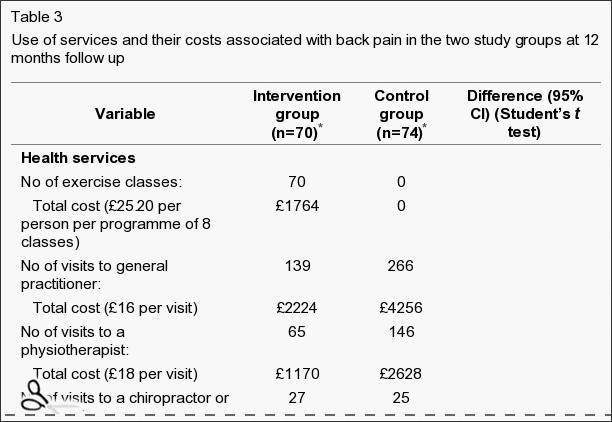
The search strategy used by the team was that developed by van Tulder et al, and the team identified 11 trials. Good evidence indicates that patients with acute LBP on bed rest have more pain and less functional recovery than those who stay active. There is no difference in pain and functional status between bed rest and exercises. For sciatica patients, fair evidence shows no real difference in pain and functional status between bed rest and staying active. There is fair evidence of no difference in pain intensity between bed rest and physiotherapy but small improvements in functional status. Finally, there is little difference in pain intensity or functional status between shorter-term or longer-term bed rest.
A Cochrane review by Hagen et al demonstrated small advantages in short-term and long-term for staying active over bed rest, as did a high-quality review by the Danish Society of Chiropractic and Clinical Biomechanics, including 4 systematic reviews, 4 additional RCTS, and 6 guidelines, on acute LBP and sciatica. The Cochrane review by Hilde et al included 4 trials and concluded a small beneficial effect for staying active for acute, uncomplicated LBP, but no benefit for sciatica. Eight studies on staying active and 10 on bed rest were included in an analysis by the group of Waddell. Several therapies were coupled with advice to stay active and include analgesic medication, physical therapy, back school, and behavioral counseling. Bed rest for acute LBP was similar to no treatment and placebo and less effective than alternative treatment. Outcomes considered across the studies were rate of recovery, pain, activity levels, and work time loss. Staying active was found to have a favorable effect.
Review of 4 studies not covered elsewhere assessed the use of brochures/booklets. The trend was for no differences in outcome for pamphlets. One exception was noted�that those who received manipulation had less bothersome symptoms at 4 weeks and significantly less disability at 3 months for those who received a booklet encouraging staying active.
In summary, assuring patients that they are likely to do well and advising them to stay active and avoid bed rest is a best practice for management of acute LBP. Bed rest for short intervals may be beneficial for patients with radiating leg pain who are intolerant of weight bearing.
Adjustment/Manipulation/Mobilization Vs Multiple Modalities
This review considered literature on high-velocity, lowamplitude (HVLA) procedures, often termed adjustment or manipulation, and mobilization. The HVLA procedures use thrusting maneuvers applied quickly; mobilization is applied cyclically. The HVLA procedure and mobilization may be mechanically assisted; mechanical impulse devices are considered HVLA, and flexion-distraction methods and continuous passive motion methods are within mobilization.
The team recommends adopting the findings of the systematic review by Bronfort et al, with a quality score (QS) of 88, covering literature up to 2002. In 2006, the Cochrane collaboration reissued an earlier (2004) review of spinal manipulative therapy (SMT) for back pain performed by Assendelft et al. This reported on 39 studies up to 1999, several overlapping with those reported by Bronfort et al using different criteria and a novel analysis. They report no difference in outcome from treatment with manipulation vs alternatives. As several additional RCTs had appeared in the interim, the rationale for reissuing the older review without acknowledging new studies was unclear.
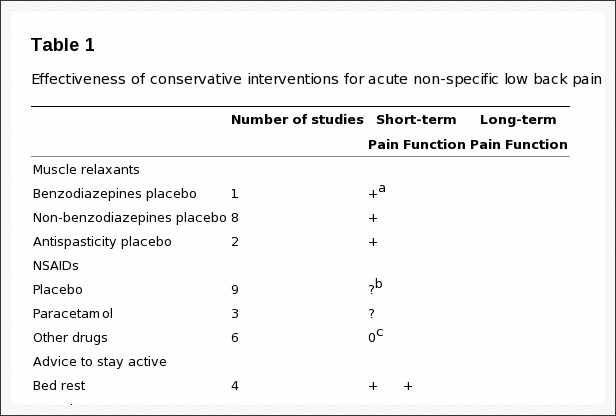
Acute LBP. There was fair evidence that HVLA has better short-term efficacy than mobilization or diathermy and limited evidence of better short-term efficacy than diathermy, exercise, and ergonomic modifications.
Chronic LBP. The HVLA procedure combined with strengthening exercise was as effective for pain relief as nonsteroidal antiinflammatory dugs with exercise. Fair evidence indicated that manipulation is better than physical therapy and home exercise for reducing disability. Fair evidence shows that manipulation improves outcomes more than general medical care or placebo in the short-term and to physical therapy in the long-term. The HVLA procedure had better outcomes than home exercise, transcutaneous�electrical nerve stimulation, traction, exercise, placebo and sham manipulation, or chemonucleolysis for disk herniation.
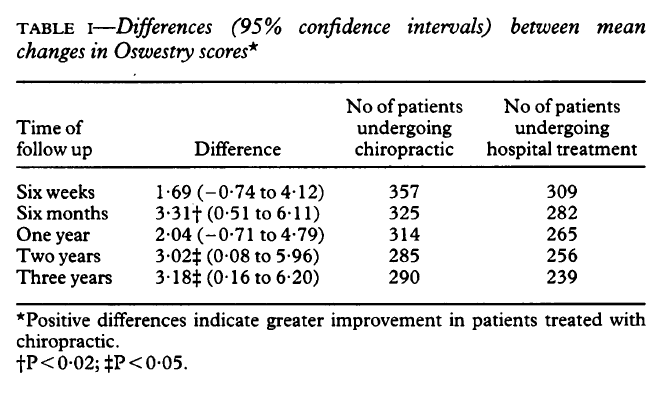
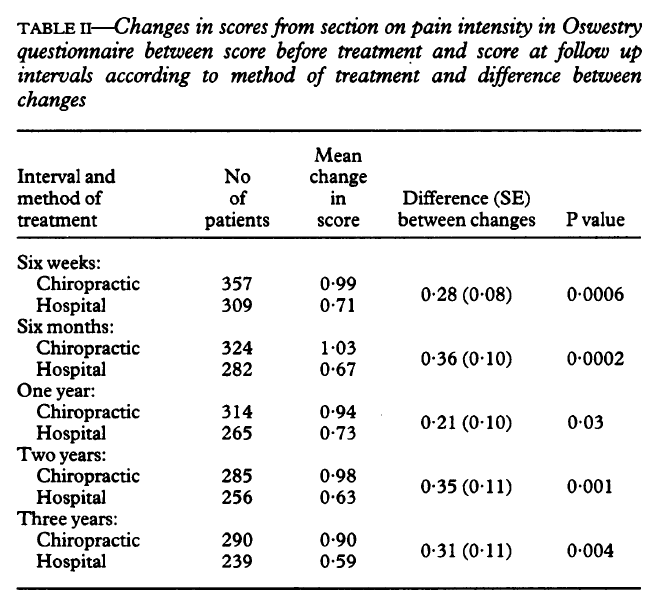
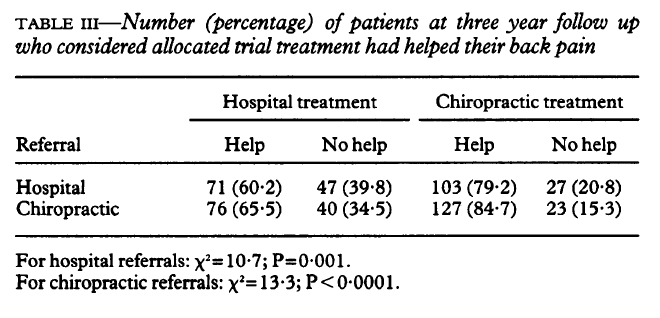
Mixed (Acute and Chronic) LBP. Hurwitz found that HVLA was the same as medical care for pain and disability; adding physical therapy to manipulation did not improve outcomes. Hsieh found no significant value for HVLA over back school or myofascial therapy. A short-term value of manipulation over a pamphlet and no difference between manipulation and McKenzie technique were reported by Cherkin et al. Meade contrasted manipulation and hospital care, finding greater benefit for manipulation over both short-term and long-term. Doran and Newell found that SMT resulted in greater improvement than physical therapy or corsets.
Acute LBP
Sick List Comparisons. Seferlis found that sick patients listed were significantly improved symptomatically after 1 month regardless of the intervention, including manipulation. Patients were more satisfied and felt that they were provided better explanations about their pain from practitioners who used manual therapy (QS, 62.5). Wand et al examined the effects of sick-listing oneself and noted that a group receiving assessment, advice, and treatment improved better than did a group getting assessment, advice, and who were put on a wait list for a 6-week period. Improvements were observed in disability, general health, quality of life, and mood, though pain and disability were not different at longterm follow-up (QS, 68.75).
Physiologic Therapeutic Modality and Exercise. Hurley and colleagues tested the effects of manipulation combined with interferential therapy compared to either modality alone. Their results showed all 3 groups improved function to the same degree, both at 6-month and at 12-month follow-up (QS, 81.25). Using a single-blinded experimental design to compare manipulation to massage and low-level electrostimulation, Godfrey et al found no differences between groups at the 2 to 3-week observation time frame (QS, 19). In the study by Rasmussen, results showed that 94% of the patients treated with manipulation were symptom-free within 14 days, compared to 25% in the group that received short-wave diathermy. Sample size was small, however, and as a result, the study was underpowered (QS, 18). The Danish systematic review examined 12 international sets of guidelines, 12 systematic reviews, and 10 randomized clinical trials on exercise. They found no specific exercises, regardless of type, that were useful for the treatment of acute LBP with the exception of McKenzie maneuvers.
Sham and Alternate Manual Method Comparisons. The study of Hadler balanced for effects of provider attention and physical contact with a first effort at a manipulation sham procedure. Patients in the group that entered the trial with greater prolonged illness at the outset were reported to have benefited from the manipulation. Similarly, they improved faster and to a greater degree (QS, 62.5). Hadler demonstrated that there was a benefit for a single session of manipulation compared to a session of mobilization (QS, 69). Erhard reported that the rate of positive response to manual treatment with a hand-heel rocking motion was greater than with extension exercises (QS, 25). Von Buerger examined the use of manipulation for acute LBP, comparing rotational manipulation to soft tissue massage. He found that the manipulation group responded better than the soft tissue group, although the effects occurred mainly in the short-term. The results were also hampered by the nature of the forced multiple choice selections on the data forms (QS, 31). Gemmell compared 2 forms of manipulation for LBP of less than 6 weeks of duration as follows: Meric adjusting (a form of HVLA) and Activator technique (a form of mechanically assisted HVLA). No difference was observed, and both helped to reduce pain intensity (QS, 37.5). MacDonald reported a short-term benefit in disability measures within the first 1 to 2 weeks of starting therapy for the manipulation group that disappeared by 4 weeks in a control group (QS, 38). The work of Hoehler, although containing mixed data for patients with acute and chronic LBP, is included here because a larger proportion of patients with acute LBP were involved in the study. Manipulation patients reported immediate relief more often, but there were no differences between groups at discharge (QS, 25).
Medication. Coyer showed that 50% of the manipulation group was symptom-free within 1 week and 87% were discharged symptom-free in 3 weeks, compared to 27% and 60%, respectively, of the control group (bed rest and analgesics) (QS, 37.5). Doran and Newell compared manipulation, physiotherapy, corset, or analgesic medication, using outcomes that examined pain and mobility. There were no differences between groups over time (QS, 25). Waterworth compared manipulation to conservative physiotherapy and 500 mg of diflunisal twice per day for 10 days. Manipulation showed no benefit for the rate of recovery (QS, 62.5). Blomberg compared manipulation to steroid injections and to a control group receiving conventional activating therapy. After 4 months, the manipulation group had less restricted motion in extension, less restriction in side-bending to both sides, less local pain on extension and right sidebending, less radiating pain, and less pain when performing a straight leg raise (QS, 56.25). Bronfort found no outcome differences between chiropractic care compared to medical care at 1 month of treatment, but there were noticeable improvements in the chiropractic group at both 3 and 6-month follow-up (QS, 31).
Subacute Back Pain
Staying Active. Grunnesjo compared combined effects of manual therapy with advice to stay active to advice alone in patients with acute and subacute LBP. The addition of�manual therapy appeared to reduce pain and disability more effectively than the �stay active� concept alone (QS, 68.75).
Physiologic Therapeutic Modality and Exercise. Pope demonstrated that manipulation offered better pain improvement than transcutaneous electrical nerve stimulation (QS 38). Sims-Williams compared manipulation to �physiotherapy.� Results demonstrated a short-term benefit for manipulation on pain and ability to do light work. Differences between groups waned at 3 and 12-month follow-ups (QS, 43.75, 35). Skargren et al compared chiropractic to physiotherapy for patients with LBP who had no treatment for the prior month. No differences in health improvements, costs, or recurrence rates were noted between the 2 groups. However, based on Oswestry scores, chiropractic performed better for patients who had pain for less than 1 week, whereas the physiotherapy seemed to be better for those who had pain for more than 4 weeks (QS, 50).
The Danish systematic review examined 12 international sets of guidelines, 12 systematic reviews, and 10 randomized clinical trials on exercise. Results suggested that exercise, in general, benefits patients with subacute back pain. Use of a basic program that can be readily modified to meet individual patient needs is recommended. Issues of strength, endurance, stabilization, and coordination without excessive loading can all be addressed without the use of high-tech equipment. Intensive training consisting of greater than 30 and less than 100 hours of training are most effective.
Sham and Alternate Manual Method Comparisons. Hoiriis compared efficacy of chiropractic manipulation to placebo/ sham for subacute LBP. All groups improved on measures of pain, disability, depression, and Global Impression of Severity. Chiropractic manipulation scored better than placebo in reducing pain and Global Impression of Severity scores (QS, 75). Andersson and colleagues compared osteopathic manipulation to standard care to patients with subacute LBP, finding that both groups improved for a 12-week period at about the same rate (QS, 50).
Medication Comparisons. In a separate treatment arm of the study of Hoiriis, the relative efficacy of chiropractic manipulation to muscle relaxants for subacute LBP was studied. In all groups, pain, disability, depression, and Global Impression of Severity decreased. Chiropractic manipulation was more effective than muscle relaxants in reducing Global Impression of Severity scores (QS, 75).
Chronic LBP
Staying Active Comparisons. Aure compared manual therapy to exercise in patients with chronic LBP who were sick listed. Although both groups showed improvements in pain intensity, functional disability, general health, and return to work, the manual therapy group showed significantly greater improvements than did the exercise group for all outcomes. Results were consistent for both the short-term and the longterm (QS, 81.25).
Physician Consult/Medical Care/Education. Niemisto compared combined manipulation, stabilization exercise, and physician consultation to consultation alone. The combined intervention was more effective in reducing pain intensity and disability (QS, 81.25). Koes compared general practitioner treatment to manipulation, physiotherapy, and a placebo (detuned ultrasound). Assessments were made at 3, 6, and 12 weeks. The manipulation group had a quicker and larger improvement in physical function compared to the other therapies. Changes in spinal mobility in the groups were small and inconsistent (QS, 68). In a follow-up report, Koes found during subgroup analysis that improvement in pain was greater for manipulation than for other treatments at 12 months when considering patients with chronic conditions, as well as those who were younger than 40 years (QS, 43). Another study by Koes showed that many patients in the nonmanipulation treatment arms had received additional care during follow-up. Yet, improvement in the main complaints and in physical functioning remained better in the manipulation group (QS, 50). Meade observed that chiropractic treatment was more effective than hospital outpatient care, as assessed using the Oswestry Scale (QS, 31). An RCT conducted in Egypt by Rupert compared chiropractic manipulation, after medical and chiropractic evaluation. Pain, forward flexion, active, and passive leg raise all improved to a greater degree in the chiropractic group; however, the description of alternate treatments and outcomes was ambiguous (QS, 50).
Triano compared manual therapy to educational programs for chronic LBP. There was greater improvement in pain, function, and activity tolerance in the manipulation group, which continued beyond the 2-week treatment period (QS, 31).
Physiologic Therapeutic Modality. A negative trial for manipulation was reported by Gibson (QS, 38). Detuned diathermy was reported to achieve better results over manipulation, although there were baseline differences between groups. Koes studied the effectiveness of manipulation, physiotherapy, treatment by a general practitioner, and a placebo of detuned ultrasound. Assessments were made at 3, 6, and 12 weeks. The manipulation group showed a quicker and better improvement in physical function capacity compared to the other therapies. Flexibility differences between groups were not significant (QS, 68). In a follow-up report, Koes found that a subgroup analysis demonstrated that improvement in pain was greater for those treated with manipulation, both for younger (b40) patients and those with chronic conditions at 12-month follow-up (QS, 43). Despite many patients in the nonmanipulation groups received additional care during follow-up, improvements remained better in the manipulation group than in the physical therapy group (QS, 50). In a separate report by the same group, there were improvements in both the physiotherapy and manual therapy groups with regard to severity of complaints and global perceived effect compared to general practitioner care;�however, the differences between the 2 groups was not significant (QS, 50). Mathews et al found that manipulation hastened recovery from LBP more than the control did.
Exercise Modality. Hemilla observed that SMT led to better long-term and short-term disability reduction compared to physical therapy or home exercise (QS, 63). A second article by the same group found that neither bone-setting nor exercise differed significantly from physical therapy for symptom control, though bone-setting was associated with improved lateral and forward-bending of the spine more than exercise (QS, 75). Coxhea reported that HVLA provided better outcomes when compared to exercise, corsets, traction, or no exercise when studied in the short-term (QS, 25). Conversely, Herzog found no differences between manipulation, exercise, and back education in reducing either pain or disability (QS, 6). Aure compared manual therapy to exercise in patients with chronic LBP who were also sick listed. Although both groups showed improvements in pain intensity, functional disability, and general health and returned to work, the manual therapy group showed significantly greater improvements than did the exercise group for all outcomes. This result persisted for both the short-term and the long-term (QS, 81.25). In the article by Niemisto and colleagues, the relative efficacy of combined manipulation, exercise (stabilizing forms), and physician consultation compared to consultation alone was investigated. The combined intervention was more effective in reducing pain intensity and disability (QS, 81.25). The United Kingdom Beam study found that manipulation followed by exercise achieved a moderate benefit at 3 months and a small benefit at 12 months. Likewise, manipulation achieved a small to moderate benefit at 3 months and a small benefit at 12 months. Exercise alone had a small benefit at 3 months but no benefit at 12 months. Lewis et al found improvement occurred when patients were treated by combined manipulation and spinal stabilization exercises vs use of a 10-station exercise class.
The Danish systematic review examined 12 international sets of guidelines, 12 systematic reviews, and 10 randomized clinical trials on exercise. Results suggested that exercise, in general, benefits patients with chronic LBP. No clear superior method is known. Use of a basic program that can be readily modified to meet individual patient needs is recommended. Issues of strength, endurance, stabilization, and coordination without excessive loading can all be addressed without the use of high-tech equipment. Intensive training consisting of greater than 30 and less than 100 hours of training are most effective. Patients with severe chronic LBP, including those off work, are treated more effectively with a multidisciplinary rehabilitation program. For post surgical rehabilitation, patients starting 4 to 6 weeks after disk surgery under intensive training receive greater benefit than with light exercise programs.
Sham and Alternate Manual Methods. Triano found that SMT produced significantly better results for pain and disability relief for the short-term, than did sham manipulation (QS, 31). Cote found no difference over time or for comparisons within or between the manipulation and mobilization groups (QS, 37.5). The authors posed that failure to observe differences may have been due to low responsiveness to change in the instruments used for algometry, coupled with a small sample size. Hsieh found no significant value for HVLA over back school or myofascial therapy (QS, 63). In the study by Licciardone, a comparison was made between osteopathic manipulation (which includes mobilization and soft tissue procedures as well as HVLA), sham manipulation, and a no-intervention control for patients with chronic LBP. All groups showed improvement. Sham and osteopathic manipulation were associated with greater improvements than seen in the no-manipulation group, but no difference was observed between the sham and manipulation groups (QS, 62.5). Both subjective and objective measures showed greater improvements in the manipulation group compared to a sham control, in a report by Waagen (QS, 44). In the work of Kinalski, manual therapy reduced the time of treatment of patients with LBP and concomitant intervertebral disk lesions. When disk lesions were not advanced, a decreased muscular hypertonia and increased mobility was noted. This article, however, was limited by a poor description of patients and methods (QS, 0).
Harrison et al reported a nonrandomized cohort controlled trial of treatment of chronic LBP consisting of 3-point bending traction designed to increase curvature of the lumbar spine. The experimental group received HVLA for pain control during the first 3 weeks (9 treatments). The control group received no treatment. Follow-up at a mean of 11 weeks showed no change in pain or curvature status for controls but a significant increase in curvature and reduction of pain in the experimental group. Average number of treatments to achieve this result was 36. Long-term followup at 17 months showed retention of benefits. No report of relationship between clinical changes and structural change was given.
Haas and colleagues examined the dose-response patterns of manipulation for chronic LBP. Patients were randomly allocated to groups receiving 1, 2, 3, or 4 visits per week for 3 weeks, with outcomes recorded for pain intensity and functional disability. A positive and clinically important effect of the number of chiropractic treatments on pain intensity and disability at 4 weeks was associated with the groups receiving the higher rates of care (QS, 62.5). Descarreaux et al extended this work, treating 2 small groups for 4 weeks (3 times per week) after 2 baseline evaluations separated by 4 weeks. One group was then treated every 3 weeks; the other did not. Although both groups had lower Oswestry scores at 12 weeks, at 10 months, the improvement only persisted for the extended SMT group.
Medication. Burton and colleagues demonstrated that HVLA led to greater short-term improvements in pain and disability than did chemonucleolysis for managing disk�herniation (QS, 38). Bronfort studied SMT combined with exercise vs a combination of nonsteroidal antiinflammatory drugs and exercise. Similar results were obtained for both groups (QS, 81). Forceful manipulation coupled with sclerosant therapy (injection of a proliferant solution composed of dextrose-glycerine-phenol) was compared to lower force manipulation combined with saline injections, in a study by Ongley. The group receiving forceful manipulation with sclerosant fared better than the alternate group, but effects cannot be separated between the manual procedure and the sclerosant (QS, 87.5). Giles and Muller compared HVLA procedures to medication and acupuncture. Manipulation showed greater improvement in frequency of back pain, pain scores, Oswestry, and SF-36 compared to the other 2 interventions. Improvements lasted for 1 year. Weaknesses of the study were use of a compliers-only analysis as intention to treat for the Oswestry, and Visual Analogue Scale (VAS) was not significant.
Sciatica/Radicular/Radiating Leg Pain
Staying Active/Bed Rest. Postacchini studied a mixed group of patients with LBP, with and without radiating leg pain. Patients could be classified as acute or chronic and were evaluated at 3 weeks, 2 months, and 6 months postonset. Treatments included manipulation, drug therapy, physiotherapy, placebo, and bed rest. Acute back pain without radiation and chronic back pain responded well to manipulation; however, in none of the other groups did manipulation fare as well as other interventions (QS, 6).
Physician Consult/Medical Care/Education. Arkuszewski looked at patients with lumbosacral pain or sciatica. One group received drugs, physiotherapy, and manual examination, whereas the second added manipulation. The group receiving manipulation had a shorter treatment time and a more marked improvement. At 6-month follow-up, the manipulation group showed better neuromotor system function and a better ability to continue employment. Disability was lower in the manipulation group (QS, 18.75).
Physiologic Therapeutic Modality. Physiotherapy combined with manual manipulation and medication was examined by Arkuszewski, in contrast to the same scheme with manipulation added, as noted above. Outcomes from manipulation were better for neurologic and motor function as well as disability (QS, 18.75). Postacchini looked at patients with acute or chronic symptoms evaluated at 3 weeks, 2 months, and 6 months postonset. Manipulation was not as effective for managing the patients with radiating leg pain as the other treatment arms (QS, 6). Mathews and colleagues examined multiple treatments including manipulation, traction, sclerosant use, and epidural injections for back pain with sciatica. For patients with LBP and restricted straight leg raise test, manipulation conferred highly significant relief, more so than alternate interventions (QS, 19). Coxhead et al included among their subjects patients who had radiating pain at least to the buttocks. Interventions included traction, manipulation, exercise, and corset, using a factorial design. After 4 weeks of care, manipulation showed a significant degree of benefit on one of the scales used to assess progress. There were no real differences between groups at 4 months and 16 months posttherapy, however (QS, 25).
Exercise Modality. In the case of LBP after laminectomy, Timm reported that exercises conferred benefit both for pain relief and cost-effectiveness (QS, 25). Manipulation had only a small influence on improvement of either symptoms or function (QS, 25). In the study by Coxhead et al, radiating pain to at least the buttocks was better after 4 weeks of care for manipulation, in contrast to other treatments that disappeared 4 months and 16 months posttherapy (QS, 25).
Sham and Alternate Manual Method. Siehl looked at the use of manipulation under general anesthesia for patients with LBP and unilateral or bilateral radiating leg pain. Only temporary clinical improvement was noted when traditional electromyographic evidence of nerve root involvement was present. With negative electromyography, manipulation was reported to provide lasting improvement (QS, 31.25) Santilli and colleagues compared HVLA to soft tissue pressing without any sudden thrust in patients with moderate acute back and leg pain. The HVLA procedures were significantly more effective in reducing pain, reaching a pain-free status, and the total number of days with pain. Clinically significant differences were noted. The total number of treatment sessions was capped at 20 on a dosage of 5 times per week with care depending on pain relief. Follow-up showed relief persisting through 6 months.
Medication. Mixed acute and chronic back pain with radiation treated in a study using multiple treatment arms were evaluated at 3 weeks, 2 months, and 6 months postonset by the group of Postacchini. Medication management fared better than did manipulation when radiating leg pain was present (QS, 6). Conversely, for the work of Mathews and colleagues, the group of patients with LBP and limited straight leg raise test responded more to manipulation than to epidural steroid or sclerosants (QS, 19).
Disk Herniation
Nwuga studied 51 subjects who were having a diagnosis of prolapsed intervertebral disk and who had been referred for physical therapy. Manipulation was reported to be superior to conventional therapy (QS, 12.5). Zylbergold found that there were no statistical differences between 3 treatments�lumbar flexion exercises, home care, and manipulation. Short-term follow-up and a small sample size were posed by the author as a basis for failing to reject the null hypothesis (QS, 38).
Exercise
Exercise is one of the most well-studied forms of treatment of low back disorders. There are many different approaches to�exercise. For this report, it is important only to differentiate multidisciplinary rehabilitation. These programs are designed for patients with especially chronic condition with significant psychosocial problems. They involve trunk exercise, functional task training including work simulation/vocational training, and psychological counseling.
In a recent Cochrane review on exercise for the treatment of nonspecific LBP (QS, 82), effectiveness of exercise therapy in patients classified as acute, subacute, and chronic was compared to no treatment and alternate treatments. Outcomes included the assessment of pain, function, return to work, absenteeism, and/or global improvements. In the review, 61 trials met the inclusion criteria, most of which dealt with chronic (n = 43), whereas smaller numbers addressed acute (n = 11) and subacute (n = 6) pain. The general conclusions were as follows:
exercise is not effective as a treatment of acute LBP,
evidence that exercise was effective in chronic populations relative to comparisons made at follow-up periods,
mean improvements of 13.3 points for pain and 6.9 points for function were observed, and
there is some evidence that graded-activity exercise is effective for subacute LBP but only in the occupational setting
The review examined population and intervention characteristics, as well as outcomes to reach its conclusions. Extracting data on return to work, absenteeism, and global improvement proved so difficult that only pain and function could be quantitatively described.
Eight studies scored positively on key validity criteria. With regard to clinical relevance, many of the trials presented inadequate information, with 90% reporting the study population but only 54% adequately describing the exercise intervention. Relevant outcomes were reported in 70% of the trials.
Exercise for Acute LBP. Of the 11 trials (total n = 1192), 10 had nonexercise comparison groups. The trials presented conflicting evidence. Eight low-quality trials showed no differences between exercise and usual care or no treatment. Pooled data showed that there was no difference in shortterm pain relief between exercise and no treatment, no difference in early follow-up for pain when compared to other interventions, and no positive effect of exercise on functional outcomes.
Subacute LBP. In 6 studies (total n = 881), 7 exercise groups had a nonexercise comparison group. The trials offered mixed results with regard to evidence of effectiveness, with fair evidence of effectiveness for a graded-exercise activity program as the only notable finding. Pooled data did not show evidence to either support or refute the use of exercise for subacute LBP, either for decreasing pain or improving function.
Chronic LBP. There were 43 trials included in this group (total n = 3907). Thirty-three of the studies had nonexercise comparison groups. Exercise was at least as effective as other conservative interventions for LBP, and 2 high-quality studies and 9 lower-quality studies found exercise to be more effective. These studies used individualized exercise programs, focusing mainly on strengthening or trunk stabilization. There were 14 trials that found no difference between exercise and other conservative interventions; of these, 2 were rated highly and 12 rated lower. Pooling the data showed a mean improvement of 10.2 (95% confidence interval [CI], 1.31-19.09) points on a 100-mm pain scale for exercise compared to no treatment and 5.93 (95% CI, 2.21- 9.65) points compared to other conservative treatments. Functional outcomes also showed improvements as follows: 3.0 points at earliest follow-up compared to no treatment (95% CI, ?0.53 to 6.48) and 2.37 points (95% CI, 1.04-3.94) compared to other conservative treatments.
Indirect subgroup analysis found that trials examining health care study populations had higher mean improvements in pain and physical functioning compared to their comparison groups or to trials set in occupational or general populations.
The review authors offered the following conclusions:
In acute LBP, exercises are not more effective than other conservative interventions. Meta-analysis showed no advantage over no treatment of pain and functional outcomes over the short or long-term.
There is fair evidence of effectiveness of a gradedactivity exercise program in subacute LBP in occupational settings. The effectiveness for other types of exercise therapy in other populations is unclear.
In chronic LBP, there is good evidence that exercise is at least as effective as other conservative treatments. Individually designed strengthening or stabilizing programs appear to be effective in health care settings. Meta-analysis found functional outcomes significantly improved; however, the effects were very small, with a less than 3-point (of 100) difference between the exercise and comparison groups at earliest follow-up. Pain outcomes were also significantly improved in groups receiving exercises relative to other comparisons, with a mean of approximately 7 points. Effects were similar over longer follow-up, though confidence intervals increased. Mean improvements in pain and functioning may be clinically meaningful in studies from health care populations in which improvements were significantly greater than those observed in studies from general or mixed populations.
The Danish group review of exercise was able to identify 5 systematic reviews and 12 guidelines that discussed exercise for acute LBP, 1 systematic review and 12 guidelines for subacute, and 7 systematic reviews and 11 guidelines for chronic. Furthermore, they identified 1 systematic review that selectively evaluated for postsurgical�cases. Conclusions were essentially the same as the Cochrane review, with the exceptions that there was limited support for McKenzie maneuvers for patients with acute condition and for intensive rehabilitation programs for 4 to 6 weeks after disk surgery over light exercise programs.
Natural and Treatment History for LBP
Most studies have demonstrated that nearly half of LBP will improve within 1 week, whereas nearly 90% of it will be gone by 12 weeks. Even more, Dixon demonstrated that perhaps as much as 90% of LBP will resolve on its own, without any intervention whatsoever. Von Korff demonstrated that a significant number of patients with acute LBP will have persistent pain if they are observed up to 2 years.
Phillips found that nearly 4 of 10 people will have LBP after an episode at 6 months from onset, even if the original pain has disappeared because more than 6 in 10 will have at least 1 relapse during the first year after an episode. These initial relapses occur within 8 weeks most commonly and may reoccur over time, though in decreasing percentages.
Workers’ compensation injury patients were observed for 1 year to examine symptom severity and work status. Half of those studied lost no work time in the first month after injury, but 30% did lose time from work due to their injury over the course of 1 year. Of those who missed work in the first month due to their injury and had already been able to return to work, nearly 20% had absence later in that same year. This implies that assessing return to work at 1 month after injury will fail to give an honest depiction of the chronic, episodic nature of LBP. Although many patients have returned to work, they will later experience continuing problems and work-related absences. Impairment present at more than 12 weeks postinjury may be far higher than what has been previously reported in the literature, where rates of 10% are common. In fact, the rates may go up to 3 to 4 times higher.
In a study by Schiotzz-Christensen and colleagues, the following was noted. In relation to sick leave, LBP has a favorable prognosis, with a 50% return to work within the first 8 days and only 2% on sick leave after 1 year. However, 15% had been on sick leave during the following year and about half continued to complain of discomfort. This suggested that an acute episode of LBP significant enough to cause the patient to seek a visit to a general practitioner is followed by a longer period of low-grade disability than previously reported. Also, even for those who returned to work, up to 16% indicated that they were not functionally improved. In another study looking at outcomes after 4 weeks after initial diagnosis and treatment, only 28% of patients did not experience any pain. More strikingly, the persistence of pain differed between groups that had radiating pain and those that did not, with 65% of the former feeling improvement at 4 weeks, vs 82% of the latter. The general findings from this study differ from others in that 72% of patients still experienced pain 4 weeks after initial diagnosis.
Hestbaek and colleagues reviewed a number of articles in a systematic review. The results showed that the reported proportion of patients who still experienced pain after 12 months after onset was 62% on average, with 16% sick-listed 6 months after onset, and with 60% experiencing relapse of work absence. Also, they found that the mean reported prevalence of LBP in patients who had past episodes of LBP was 56%, compared to just 22% for those who had no such history. Croft and colleagues performed a prospective study looking at the outcomes of LBP in general practice, finding that 90% of patients with LBP in primary care had stopped consulting with symptoms within 3 months; however, most were still experiencing LBP and disability 1 year after the initial visit. Only 25% had fully recovered within that same year.
There are even different results in the study by Wahlgren et al. Here, most patients continued to experience pain at both 6 and 12 months (78% and 72%, respectively). Only 20% of the sample had fully recovered by 6 months and only 22% by 12 months.
Von Korff has provided a lengthy list of data he considers relevant to assessing the clinical course of back pain as follows: age, sex, race/ethnicity, years of education, occupation, change in occupation, employment status, disability insurance status, litigation status, recency/age at first onset of back pain, recency/age when care was sought, recency of back pain episode, duration of current/most recent episode of back pain, number of back pain days, current pain intensity, average pain intensity, worst pain intensity, ratings of interference with activities, activity limitation days, clinical diagnosis for this episode, bed rest days, work loss days, recency of back pain flare-up, and duration of the most recent flare-up.
In a practice-based observational study by Haas et al of almost 3000 patients with acute and chronic condition treated by chiropractors and primary care medical doctors, pain was noted in patients with acute and chronic condition up to 48 months after enrollment. At 36 months, 45% to 75% of patients reported at least 30 days of pain in the prior year, and 19% to 27% of patients with chronic condition recalled daily pain over the previous year.
The variability noted in these and many other studies can be explained in part by the difficulty in making an adequate diagnosis, by the different classification schemes used in classifying LBP, by the different outcome tools used in each study and by many other factors. It also points up the extreme difficulty in getting a handle on the day-to-day reality for those who have LBP.
Common Markers and Rating Complexity for LBP
What Are the Relevant Benchmarks for Evaluating Process of Care?. One benchmark is described above, that being natural history. Complexity and risk stratification are important, as�are cost issues; however, cost-effectiveness is beyond the scope of this report.
It is understood that patients with uncomplicated LBP improve faster than those with various complications, the most notable of which is radiating pain. Many factors may influence the course of back pain, including comorbidity, ergonomic factors, age, the level of fitness of the patient, environmental factors, and psychosocial factors. The latter is receiving a great deal of attention in the literature, though as noted elsewhere in this book, such consideration may not be justified. Any of these factors, alone or in combination, may hamper or retard the recovery period after injury.
It seems that biomechanical factors play an important role in the incidence of first-time episodes of LBP and its attendant problems such as work loss; psychosocial factors come into play more in subsequent episodes of LBP. The biomechanical factors can lead to tissue tearing, which then create pain and limited ability for years to follow. This tissue damage cannot be seen on standard imaging and may only be apparent upon dissection or surgery.
abnormal joint motion or decreased body mechanics;
prolonged static posture or poor motor control;
work-related such as vehicle operation, sustained loads, materials handling;
employment history and satisfaction; and
wage status.
IJzelenberg and Burdorf investigated whether demographic, work-related physical, or psychosocial risk factors involved in the occurrence of musculoskeletal conditions determine subsequent health care use and sick leave. They found that within 6 months, nearly one third of industrial workers with LBP (or neck and upper extremity problems) had a recurrence of sick leave for that same problem and a 40% recurrence of health care use. Work-related factors associated with musculoskeletal symptoms were similar to those associated with health care use and sick leave; but, for LBP, older age and living alone strongly determined whether patients with these problems took any sick leave. The 12- month prevalence of LBP was 52%, and of those with symptoms at baseline, 68% had a recurrence of the LBP. Jarvik and colleagues add depression as an important predictor of new LBP. They found the use of MRI to be a less important predictor of LBP than depression.
What Are the Relevant Outcome Measures?. The Clinical Practice Guidelines formulated by the Canadian Chiropractic Association and the Canadian Federation of Chiropractic Regulatory Boards note that there are a number of outcomes that may be used to demonstrate change as a result of treatment. These should be both reliable and valid. According to the Canadian guidelines, appropriate standards are useful in chiropractic practice because they are able to perform the following:
consistently evaluate the effects of care over time;
help indicate the point of maximum therapeutic improvement;
uncover problems related to care such as noncompliance;
document improvement to the patient, doctor, and third parties;
suggest modifications of the goals of treatment if necessary;
quantify the clinical experience of the doctor;
justify the type, dose, and duration of care;
help provide a database for research; and
assist in establishing standards of treatment of specific conditions.
The broad general classes of outcomes include functional outcomes, patient perception outcomes, physiologic outcomes, general health assessments, and subluxation syndrome outcomes. This chapter addresses only functional and patient perception outcomes assessed by questionnaires and functional outcomes assessed by manual procedures.
Functional Outcomes. These are outcomes that measure the patient’s limitations in going about his or her normal daily activities. What is being looked at is the effect of a condition or disorder on the patient (ie, LBP, for which a specific diagnosis may not be present or possible) and its outcome of care. Many such outcome tools exist. Some of the better known include the following:
Roland Morris Disability Questionnaire,
Oswestry Disability Questionnaire,
Pain Disability Index,
Neck Disability Index,
Waddell Disability Index, and
Million Disability Questionnaire.
These are only some of the existing tools for assessing function.
In the existing RCT literature for LBP, functional outcomes have been shown to be the outcome that demonstrates the greatest change and improvement with SMT. Activities of daily living, along with patient selfreporting of pain, were the 2 most notable outcomes to show such improvement. Other outcomes fared less well, including trunk range of motion (ROM) and straight leg raise.
In the chiropractic literature, the outcome inventories used most frequently for LBP are the Roland Morris Disability Questionnaire and the Oswestry Questionnaire. In a study in 1992, Hsieh found that both tools provided consistent results over the course of his trial, although the results from the 2 questionnaires differed.
Patient Perception Outcomes. Another important set of outcomes involve patient perception of pain and their satisfaction with care. The first involves measuring changes in pain perception over time of its intensity, duration, and frequency. There are a number of valid tools available that can accomplish this, including the following:
Visual analog scale�this is a 10-cm line that has pain descriptions noted at both ends of that line representing no pain to intolerable pain; the patient is asked to mark a point on that line that reflects their perceived pain intensity. There are a number of variants for this outcome, including the Numerical Rating Scale (where the patient provides a number between 0 and 10 to represent the amount of pain they have) and the use of pain levels from 0 to 10 depicted pictorially in boxes, which the patient may check. All of these appear to be equally reliable, but for ease of use, either the standard VAS or Numerical Rating Scale is commonly used.
Pain diary�these may be used to help monitor a variety of different pain variables (for example, frequency, which the VAS cannot measure). Different forms may be used to collect this information, but it is typically completed on a daily basis.
McGill Pain Questionnaire�this scale helps quantify several psychologic components of pain as follows: cognitive-evaluative, motivational-affective, and sensory discriminative. In this instrument, there are 20 categories of words that describe the quality of pain. From the results, 6 different pain variables can be determined.
All of the above instruments have been used at various times to monitor the progress of treatment of back pain with SMT.
Patient satisfaction addresses both the effectiveness of care as well as the method of receiving that care. There are numerous methods of assessing patient satisfaction, and not all of them were designed to be specifically used for LBP or for manipulation. However, Deyo did develop one for use with LBP. His instrument examines the effectiveness of care, information, and caring. There is also the Patient Satisfaction Questionnaire, which assesses 8 separate indices (such as efficacy/outcomes or professional skill, for example). Cherkin noted that the Visit Specific Satisfaction Questionnaire can be used for chiropractic outcome assessment.
Recent work has shown that patient confidence and satisfaction with care are related to outcomes. Seferlis found that patients were more satisfied and felt that they were provided better explanations about their pain from practitioners who used manual therapy. Regardless of treatment, highly satisfied patients at 4 weeks were more likely than less satisfied patients to perceive greater pain improvement throughout 18-month follow-up in a study by Hurwitz et al. Goldstein and Morgenstern found a weak association between treatment confidence in the therapy they received and greater improvement in LBP. A frequent assertion is that benefits observed from application of manipulation methods are a result of physician attention and touching. Studies directly testing this hypothesis were conducted by Hadler et al in patients with acute condition and by Triano et al in patients with subacute and chronic condition. Both studies compared manipulation to a placebo control. In the study of Hadler, the control balanced for provider time attention and frequency, whereas Triano et al also added an education program with home exercise recommendations. In both cases, results demonstrated that although attention given to patients was associated with improvement over time, patients receiving manipulation procedures improved more quickly.
General Health Outcome Measures. This has traditionally been a difficult outcome to effectively measure but a number of more recent instruments are demonstrating that it can be done reliably. The 2 major instruments for doing so are the Sickness Impact Profile and the SF-36. The first assesses dimensions such as mobility, ambulation, rest, work, social interaction, and so on; the second looks primarily at well being, functional status, and overall health, as well as 8 other health concepts, to ultimately determine 8 indices that can be used to determine overall health status. Items here include physical functioning, social functioning, mental health, and others. This tool has been used in many settings and has also been adapted into shorter forms as well.
Physiologic Outcome Measures. The chiropractic profession has a number of physiologic outcomes that are used with regard to the patient care decision-making process. These include such procedures as ROM testing, muscle function testing, palpation, radiography, and other less common procedures (leg length analysis, thermography, and others). This chapter addresses only the physiologic outcomes assessed manually.
Range of Motion. This examination procedure is used by nearly every chiropractor and is used to assess impairment because it is related to spinal function. It is possible to use ROM as a means to monitor improvement in function over time and, therefore, improvement as it relates to the use of SMT. One can assess regional and global lumbar motion, for example, and use that as one marker for improvement.
Range of motion can be measured via a number of different means. One can use standard goniometers, inclinometers, and more sophisticated tools that require the use of specialized equipment and computers. When doing so, it is important to consider the reliability of each individual method. A number of studies have assessed various devices as follows:
Zachman found the use of the rangiometer moderately reliable,
Nansel found that using 5 repeated measures of cervical spine motion with an inclinometer to be reliable,
Liebenson found that the modified Schrober technique, along with inclinometers and flexible spinal rulers had the best support from the literature,
Triano and Schultz found that ROM for the trunk, along with trunk strength ratios and myoelectrical activity, was good indicator for LBP disability, and
a number of studies found that the kinematic measurement of ROM for spinal mobility is reliable.
Muscle Function. Evaluating muscle function may be done using an automated system or by manual means. Although manual muscle testing has been a common diagnostic practice within the chiropractic profession, there are few studies demonstrating clinical reliability for the procedure, and these are not considered to be of high quality.
Automated systems are more reliable and are capable of assessing muscle parameters such as strength, power, endurance, and work, as well as assess different modes of muscle contraction (isotonic, isometric, isokinetic). Hsieh found that a patient-initiated method worked well for specific muscles, and other studies have shown the dynamometer to have good reliability.
Leg Length Inequality. Very few studies of leg length have shown acceptable levels of reliability. The best methods for assessing reliability and validity of leg length involve radiographic means and are therefore subject to exposure to ionizing radiation. Finally, the procedure has not been studied as to validity, making the use of this as an outcome questionable.
Soft Tissue Compliance. Compliance is assessed by both manual and mechanical means, using the hand alone or using a device such as an algometer. By assessing compliance, the chiropractor is looking to assess muscle tone.
Early tests of compliance by Lawson demonstrated good reliability. Fisher found increases in tissue compliance with subjects involved in physical therapy. Waldorf found that prone segmental tissue compliance had good test/retest variation of less than 10%.
Pain tolerance assessed using these means has been found reliable, and Vernon found it was a useful measure in assessing the cervical paraspinal musculature after adjusting. The guidelines group from the Canadian Chiropractic Association and the Canadian Federation of Chiropractic Regulatory Boards concluded that �the assessments are safe and inexpensive and appear to be responsive to conditions and treatments commonly seen in chiropractic practice.�
Conclusion
Existing research evidence regarding the usefulness of spinal adjusting/manipulation/mobilization indicates the following:
As much or more evidence exists for the use of SMT to reduce symptoms and improve function in patients with chronic LBP as for use in acute and subacute LBP.
Use of exercise in conjunction with manipulation is likely to speed and improve outcomes as well as minimize episodic recurrence.
There was less evidence for the use of manipulation for patients with LBP and radiating leg pain, sciatica, or radiculopathy.
Cases with high severity of symptoms may benefit by referral for comanagement of symptomswith medication.
There was little evidence for the use of manipulation for other conditions affecting the low back and very few articles to support a higher rating.
Exercise and reassurance have been shown to be of value primarily in chronic LBP and low back problems associated with radicular symptoms. A number of standardized, validated tools are available to help capture meaningful clinical improvement over the course of low back care. Typically, functional improvement (as opposed to simple reported reduction in pain levels) may be clinically meaningful for monitoring responses to care. The literature reviewed remains relatively limited in predicting responses to care, tailoring specific combinations of intervention regimens (although the combination of manipulation and exercise may be better than exercise alone), or formulating condition-specific recommendations for frequency and�duration of interventions. Table 2 summarizes the recommendations of the team, based on the review of the evidence.
Practical Applications
Evidence exists for the use of spinal manipulation to reduce symptoms and improve function in patients with chronic, acute, and subacute LBP.
Exercise in conjunction with manipulation is likely to speed and improve outcomes and minimize recurrence
In conclusion,�more evidence-based research studies have become available regarding the effectiveness of chiropractic care for low back pain and sciatica. The article also demonstrated that exercise should be used together with chiropractic to help speed up the rehabilitation process and further improve recovery. In most cases, chiropractic care can be used for the management of low back pain and sciatica, without the need for surgical interventions. However, if surgery is required to achieve recovery, a chiropractor may refer the patient to the next best healthcare professional. Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Sciatica
Sciatica is referred to as a collection of symptoms rather than a single type of injury or condition. The symptoms are characterized as radiating pain, numbness and tingling sensations from the sciatic nerve in the lower back, down the buttocks and thighs and through one or both legs and into the feet. Sciatica is commonly the result of irritation, inflammation or compression of the largest nerve in the human body, generally due to a herniated disc or bone spur.
Leape, LL, Park, RE, Kahan, JP, and Brook, RH. Group judgments of appropriateness: the effect of panel composition. Qual Assur Health Care. 1992; 4: 151�159
Bigos S, Bowyer O, Braen G, et al. Acute low back problems in adults. Rockville (Md): Agency for Health Care Policy and Research, Public Health Service, U.S. Dept of Health and Human Services; 1994.
National Health and Medical Research Council. A guide to the development, implementation and evaluation of clinical practice guidelines. AusInfo, Canberra, Australia; 1999
McDonald, WP, Durkin, K, and Pfefer, M. How chiropractors think and practice: the survey of North American Chiropractors. Semin Integr Med. 2004; 2: 92�98
Hurwitz, E, Coulter, ID, Adams, A, Genovese, BJ, and Shekelle, P. Use of chiropractic services from 1985 through 1991 in the United States and Canada. Am J Public Health. 1998; 88: 771�776
Coulter, ID, Hurwitz, E, Adams, AH, Genovese, BJ, Hays, R, and Shekelle, P. Patients using chiropractors in North America. Who are they, and why are they in chiropractic care?. Spine. 2002; 27: 291�296
Bronfort, G, Haas, M, Evans, RL, and Bouter, LM. Efficacy of spinal manipulation and mobilization for low back pain and neck pain: a systematic review and best evidence synthesis. Spine J. 2004; 4: 335�356
Petrie, JC, Grimshaw, JM, and Bryson, A. The Scottish Intercollegiate Guidelines Network Initiative: getting validated guidelines into local practice. Health Bull (Edinb). 1995; 53: 345�348
Cluzeau, FA and Littlejohns, P. Appraising clinical practice guidelines in England and Wales: the development of a methodologic framework and its application to policy. Jt Comm J Qual Improv. 1999; 25: 514�521
Stroup, DF, Berlin, JA, Morton, SC et al. Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA. 2000; 283: 2008�2012
Shekelle, P, Morton, S, Maglione, M et al. Ephedra and ephedrine for weight loss and athletic performance enhancement: clinical efficacy and side effects. Evidence Report/Technology Assessment No. 76 [Prepared by Southern California Evidence-based Practice Center, RAND, under contract no. 290-97-0001, Task Order No. 9]. AHRQ Publication No. 03-E022. Agency for Health Care Research and Quality, Rockville (Md); 2003
van Tulder, MW, Koes, BW, and Bouter, LM. Conservative treatment of acute and chronic nonspecific low back pain: a systematic review of randomized controlled trials of the most common interventions. Spine. 1997; 22: 2128�2156
Hagen, KB, Hilde, G, Jamtvedt, G, and Winnem, M. Bed rest for acute low back pain and sciatica (Cochrane Review). in: The Cochrane Library. vol. 2. Update Software, Oxford; 2000
(L�ndesmerter og kiropraktik. Et dansk evidensbaseret kvalitetssikringsprojekt)in: Danish Society of Chiropractic and Clinical Biomechanics (Ed.) Low back pain and Chiropractic. A Danish evidence-based quality assurance project report. 3rd ed.�Danish Society of Chiropractic and Clinical Biomechanics, Denmark; 2006
Hilde, G, Hagen, KB, Jamtvedt, G, and Winnem, M. Advice to stay active as a single treatment for low back pain and sciatica. Cochrane Database Syst Rev. 2002; : CD003632
Waddell, G, Feder, G, and Lewis, M. Systematic reviews of bed rest and advice to stay active for acute low back pain. Br J Gen Pract. 1997; 47: 647�652
Hurwitz, EL, Morgenstern, H, Harber, P et al. Second prize: the effectiveness of physical modalities among patients with low back pain randomized to chiropractic care: findings from the UCLA low back pain study. J Manipulative Physiol Ther. 2002; 25: 10�20
Hsieh, CY, Phillips, RB, Adams, AH, and Pope, MH. Functional outcomes of low back pain: comparison of four treatment groups in a randomized clinical trial. J Manipulative Physiol Ther. 1992; 15: 4�9
Cherkin, DC, Deyo, RA, Battie, M, Street, J, and Barlow, W. A comparison of physical therapy, chiropractic manipulation, and provision of an educational booklet for low back pain. N Engl J Med. 1998; 339: 1021�1029
Meade, TW, Dyer, S, Browne, W, Townsend, J, and Frank, AO. Low back pain of mechanical origin: randomized comparison of chiropractic and hospital outpatient treatment. Br Med J. 1990; 300: 1431�1437
Meade, TW, Dyer, S, Browne, W, and Frank, AO. Randomized comparison of chiropractic and hospital outpatient management for low back pain: results from extended follow-up. Br Med J. 1995; 311: 349�351
Seferlis, T, Nemeth, G, Carlsson, AM, and Gillstrom, P. Conservative treatment in patients sick-listed for acute low-back pain: a prospective randomized study with 12 months’ follow up. Eur Spine J. 1998; 7: 461�470
Wand, BM, Bird, C, McAuley, JH, Dore, CJ, MacDowell, M, and De Souza, L. Early intervention for the management of acute low back pain. Spine. 2004; 29: 2350�2356
Hurley, DA, McDonough, SM, Dempster, M, Moore, AP, and Baxter, GD. A randomized clinical trial of manipulative therapy and interferential therapy for acute low back pain. Spine. 2004; 29: 2207�2216
Hadler, NM, Curtis, P, Gillings, DB, and Stinnett, S. A benefit of spinal manipulation as adjunctive therapy for acute low-back pain: a stratified controlled trial. Spine. 1987; 12: 703�706
Hadler, NM, Curtis, P, Gillings, DB, and Stinnett, S. Der nutzen van manipulationen als zusatzliche therapie bei akuten lumbalgien: eine gruppenkontrollierte studie. Man Med. 1990; 28: 2�6
Erhard, RE, Delitto, A, and Cibulka, MT. Relative effectiveness of an extension program and a combined program of manipulation and flexion and extension exercises in patients with acute low back syndromes. Phys Ther. 1994; 174: 1093�1100
Gemmell, H and Jacobson, BH. The immediate effect of Activator vs. Meric adjustment on acute low back pain: a randomized controlled trial. J Manipulative Physiol Ther. 1995; 18: 5453�5456
Waterworth, RF and Hunter, IA. An open study of diflunisal, conservative and manipulative therapy in the management of acute mechanical low back pain. N Z Med J. 1985; 98: 372�375
Blomberg, S, Hallin, G, Grann, K, Berg, E, and Sennerby, U. Manual therapy with steroid injections- a new approach to treatment of low back pain: a controlled multicenter trial with an evaluation by orthopedic surgeons. Spine. 1994; 19: 569�577
Bronfort, G. Chiropractic versus general medical treatment of low back pain: a small scale controlled clinical trial. Am J Chiropr Med. 1989; 2: 145�150
Grunnesjo, MI, Bogefledt, JP, Svardsudd, KF, and Blomberg, SIE. A randomized controlled clinical trial of stay-active care versus manual therapy in addition to stay-active care: functional variables and pain. J Manipulative Physiol Ther. 2004; 27: 431�441
Pope, MH, Phillips, RB, Haugh, LD, Hsieh, CY, MacDonald, L, and Haldeman, S. A prospective, randomized three-week trial of spinal manipulation, transcutaneous muscle stimulation, massage and corset in the treatment of subacute low back pain. Spine. 1994; 19: 2571�2577
Sims-Williams, H, Jayson, MIV, Young, SMS, Baddeley, H, and Collins, E. Controlled trial of mobilization and manipulation for patients with low back pain in general practice. Br Med J. 1978; 1: 1338�1340
Sims-Williams, H, Jayson, MIV, Young, SMS, Baddeley, H, and Collins, E. Controlled trial of mobilization and manipulation for low back pain: hospital patients. Br Med J. 1979; 2: 1318�1320
Skargren, EI, Carlsson, PG, and Oberg, BE. One-year follow-up comparison of the cost and effectiveness of chiropractic and physiotherapy as primary management for back pain: subgroup analysis, recurrent, and additional health care utilization. Spine. 1998; 23: 1875�1884
Andersson, GBJ, Lucente, T, Davis, AM, Kappler, RE, Lipton, JA, and Leurgens, S. A comparison of osteopathic spinal manipulation with standard care for patients with low back pain. N Engl J Med. 1999; 341: 1426�1431
Aure, OF, Nilsen, JH, and Vasseljen, O. Manual therapy and exercise therapy in patients with chronic low back pain: a randomized, controlled trial with 1-year follow-up. Spine. 2003; 28: 525�538
Niemisto, L, Lahtinen-Suopanki, T, Rissanen, P, Lindgren, KA, Sarno, S, and Hurri, H. A randomized trial of combined manipulation, stabilizing exercises, and physical consultation compared to physician consultation alone for chronic low back pain. Spine. 2003; 28: 2185�2191
Koes, BW, Bouter, LM, van Mameren, H, Essers, AHM, Verstegen, GMJR, Hafhuizen, DM, Houben, JP, and Knipschild, P. A blinded randomized clinical trial of manual therapy and physiotherapy for chronic back and neck complaints: physical outcome measures. J Manipulative Physiol Ther. 1992; 15: 16�23
Koes, BW, Bouter, LM, van mameren, H, Essers, AHM, Verstegen, GJMG, Hofhuizen, DM, Houben, JP, and Knipschild, PG. A randomized trial of manual therapy and physiotherapy for persistent back and neck complaints: subgroup analysis and relationship between outcome measures. J Manipulative Physiol Ther. 1993; 16: 211�219
Koes, BM, Bouter, LM, van Mameren, H, Essers, AHM, Verstegen, GMJR, hofhuizen, DM, Houben, JP, and Knipschild, PG. Randomized clinical trial of manipulative therapy and physiotherapy for persistent back and neck complaints: results of a one-year follow-up. Br Med J. 1992; 304: 601�605
Triano, JJ, McGregor, M, Hondras, MA, and Brennan, PC. Manipulative therapy versus education programs in chronic low back pain. Spine. 1995; 20: 948�955
Gibson, T, Grahame, R, Harkness, J, Woo, P, Blagrave, P, and Hills, R. Controlled comparison of short-wave diathermy treatment with osteopathic treatment in non-specific low back pain. Lancet. 1985; 1: 1258�1261
Koes, BW, Bouter, LM, van Mameren, H, Essers, AHM, Verstegen, GMJR, Hofhuizen, DM, Houben, JP, and Knipschild, PG. The effectiveness of manual therapy, physiotherapy, and treatment by the general practitioner for nonspecific back and neck complaints: a randomized clinical trial. Spine. 1992; 17: 28�35
Hemilla, HM, Keinanen-Kiukaanniemi, S, Levoska, S, and Puska, P. Long-term effectiveness of bone-setting, light exercise therapy, and physiotherapy for prolonged back pain: a randomized controlled trial. J Manipulative Physiol Ther. 2002; 25: 99�104
Hemilla, HM, Keinanen-Kiukaanniemi, S, Levoska, S, and Puska, P. Does folk medicine work? A randomized clinical trial on patients with prolonged back pain. Arch Phys Med Rehabil. 1997; 78: 571�577
Coxhead, CE, Inskip, H, Meade, TW, North, WR, and Troup, JD. Multicentre trial of physiotherapy in the management of sciatic symptoms. Lancet. 1981; 1: 1065�1068
Herzog, W, Conway, PJ, and Willcox, BJ. Effects of different treatment modalities on gait symmetry and clinical measurements for sacroiliac joint patients. J Manipulative Physiol Ther. 1991; 14: 104�109
Brealey, S, Burton, K, Coulton, S et al. UK Back Pain Exercise and Manipulation (UK BEAM) trial�national randomized trial of physical treatments for back pain in primary care: objectives, design and interventions [ISRCTN32683578]. BMC Health Serv Res. 2003; 3: 16
Lewis, JS, Hewitt, JS, Billington, L, Cole, S, Byng, J, and Karayiannis, S. A randomized clinical trial comparing two physiotherapy interventions for chronic low back pain. Spine. 2005; 30: 711�721
Cote, P, Mior, SA, and Vernon, H. The short-term effect of a spinal manipulation on pain/pressure threshold is patients with chronic mechanical low back pain. J Manipulative Physiol Ther. 1994; 17: 364�368
Waagen, GN, Haldeman, S, Cook, G, Lopez, D, and DeBoer, KF. Short term of chiropractic adjustments for the relief of chronic low back pain. Manual Med. 1986; 2: 63�67
Kinalski, R, Kuwik, W, and Pietrzak, D. The comparison of the results of manual therapy versus physiotherapy methods used in treatment of patients with low back pain syndromes. J Man Med. 1989; 4: 44�46
Harrison, DE, Cailliet, R, Betz, JW, Harrison, DD, Colloca, CJ, Hasas, JW, Janik, TJ, and Holland, B. A non-randomized clinical control trial of Harrison mirror image methods (lateral translations of the thoracic cage) in patients with chronic low back pain. Eur Spine J. 2005; 14: 155�162
Descarreaux, M, Normand, MC, Laurencelle, L, and Dugas, C. Evaluation of a specific home exercise program for low back pain. J Manipulative Physiol Ther. 2002; 25: 497�503
Burton, AK, Tillotson, KM, and Cleary, J. Single-blind randomized controlled trial of hemonucelolysis and manipulation in the treatment of symptomatic lumbar disc herniation. Eur Spine J. 2000; 9: 202�207
Giles, LGF and Muller, R. Chronic spinal pain syndromes: a clinical pilot trial comparing acupuncture, a nonsteroidal anti-inflammatory drug, and spinal manipulation. J Manipulative Physiol Ther. 1999; 22: 376�381
Timm, KE. A randomized-control study of active and passive treatments for chronic low back pain following L5 laminectomy. J Orthop Sports Phys Ther. 1994; 20: 276�286
Siehl, D, Olson, DR, Ross, HE, and Rockwood, EE. Manipulation of the lumbar spine under general anesthesia: evaluation by electromyography and clinical-neurologic examination of its use for lumbar nerve root compression syndrome. J Am Osteopath Assoc. 1971; 70: 433�438
Santilli, V, Beghi, E, and Finucci, S. Chiropractic manipulation in the treatment of acute back pain and sciatica with disc protrusion: a randomized double-blind clinical trial of active and simulated spinal manipulations. ([Epub 2006 Feb 3])Spine J. 2006; 6: 131�137
Nwuga, VCB. Relative therapeutic efficacy of vertebral manipulation and conventional treatment in back pain management. Am J Phys Med. 1982; 61: 273�278
Hayden, JA, van Tulder, MW, and Tomlinson, G. Systematic review: strategies for using exercise therapy to improve outcomes in chronic low back pain. Ann Intern Med. 2005; 142: 776�785
Butler, RJ, Johnson, WG, and Baldwin, ML. Measuring success in managing work-disability. Why return to work doesn’t work. Ind Labor Relat Rev. 1995; : 1�24
Schiotzz-Christensen, B, Nielsen, GL, Hansen, VK, Schodt, T, Sorenson, HT, and Oleson, F. Long-term prognosis of acute low back pain in patients seen in general practice: a 1-year prospective follow-up study. Fam Pract. 1999; 16: 223�232
Chavannes, AW, Gubbles, J, Post, D, Rutten, G, and Thomas, S. Acute low back pain: patients’ perception of pain after initial diagnosis and treatment in general practice. J R Coll Gen Pract. 1986; 36: 271�273
Hestbaek, L, Leboeuf-Yde, C, and Manniche, C. Low back pain: what is the long-term course? A review of studies of general patient populations. Eur Spine J. 2003; 12: 149�165
Croft, PR, MacFarlane, GJ, Papageorgiou, AC, Thomas, E, and Silman, AJ. Outcome of low back pain in general practice: a prospective study. Br Med J. 1998; 316: 1356�1359
Haas, M, Goldberg, B, Aickin, M, Ganger, B, and Attwood, M. A practice-based study of patients with acute and chronic low back pain attending primary care and chiropractic physicians: two-week to 48-month follow-up. J Manipulative Physiol Ther. 2004; 27: 160�169
Spitzer, WO, LeBlanc, FE, and Dupuis, M. Scientific approach to the assessment and management of activity-related spinal disorders: a monograph for physicians: report of the Quebec Task Force on Spinal Disorders. Spine. 1987; 12: S1�S59
Jarvik, C, Hollingworth, W, Martin, B et al. Rapid magnetic resonance imaging vs. radiographs for patients with low back pain: a randomized controlled trial. JAMA. 2003; 289: 2810�2818
Henderson, D, Chapman-Smith, DA, Mior, S, and Vernon, H. Clinical Guidelines for Chiropractic Practice in Canada. Canadian Chiropractic Association, Toronto (ON); 1994
Hsieh, C, Phillips, R, Adams, A, and Pope, M. Functional outcomes of low back pain: comparison of four treatment groups in a randomized controlled trial. J Manipulative Physiol Ther. 1992; 15: 4�9
Deyo, RA, Walsh, NE, Martin, DC, Schoenfeld, LS, and Ramamurthy, S. A controlled trial of transcutaneous electrical nerve stimulation (TENS) and exercise for chronic low back pain. N Engl J Med. 1990; 322: 1627�1634
Elnaggar, IM, Nordin, M, Sheikhzadeh, A, Parnianpour, M, and Kahanovitz, N. Effects of spinal flexion and extension exercises on low-back pain and spinal mobility in chronic mechanical low-back pain patients. Spine. 1991; 16: 967�97299
Hurwitz, EL, Morgenstern, H, Kominski, GF, Yu, F, and Chiang, LM. A randomized trial of chiropractic and medical care for patients with low back pain: eighteen-month follow-up outcomes from the UCLA low back pain study. Spine. 2006; 31: 611�621
Goldstein, MS, Morgenstern, H, Hurwitz, EL, and Yu, F. The impact of treatment confidence on pain and related disability among patients with low-back pain: results from the University of California, Los Angeles, low-back pain study. Spine J. 2002; 2: 391�399
Zachman, A, Traina, A, Keating, JC, Bolles, S, and Braun-Porter, L. Interexaminer reliability and concurrent validity of two instruments for the measurement of cervical ranges of motion. J Manipulative Physiol Ther. 1989; 12: 205�210
Triano, J and Schultz, A. Correlation of objective measures of trunk motion and muscle function with low-back disability ratings. Spine. 1987; 12: 561�565
Nicholas, J, Sapega, A, Kraus, H, and Webb, J. Factors influencing manual muscle tests in physical therapy. The magnitude and duration of force applied. J Bone Joint Surg Am. 1987; 60: 186�190
Waldorf, T, Devlin, L, and Nansel, D. The comparative assessment of paraspinal tissue compliance on asymptomatic female and male subjects in both prone and standing positions. J Manipulative Physiol Ther. 1991; 4: 457�461
Ohrbach, R and Gale, E. Pressure pain threshold in normal muscles: reliability, measurement effects, and topographic differences. Pain. 1989; 37: 257�263
Vernon, H. Applying research-based assessments of pain and loss of function to the issue of developing standards of care in chiropractic. Chiropr Technique. 1990; 2: 121�126
Based on statistical findings, approximately more than three million people in the United States are injured in an automobile accident every year. In fact, auto accidents are considered to be one of the most common causes for trauma or injury. Neck injuries, such as whiplash, frequently occur due to the sudden back-and-forth movement of the head and neck from the force of the impact. The same mechanism of injury can also cause soft tissue injuries in other parts of the body, including the lower back as well as the lower extremities. Neck, hip, thigh and knee injuries are common types of injuries resulting from auto accidents.
Abstract
Objective: The purpose of this systematic review was to determine the effectiveness of exercise for the management of soft tissue injuries of the hip, thigh, and knee.
Methods: We conducted a systematic review and searched MEDLINE, EMBASE, PsycINFO, the Cochrane Central Register of Controlled Trials, and CINAHL Plus with Full Text from January 1, 1990, to April 8, 2015, for randomized controlled trials (RCTs), cohort studies, and case-control studies evaluating the effect of exercise on pain intensity, self-rated recovery, functional recovery, health-related quality of life, psychological outcomes, and adverse events. Random pairs of independent reviewers screened titles and abstracts and assessed risk of bias using the Scottish Intercollegiate Guidelines Network criteria. Best evidence synthesis methodology was used.
Results: We screened 9494 citations. Eight RCTs were critically appraised, and 3 had low risk of bias and were included in our synthesis. One RCT found statistically significant improvements in pain and function favoring clinicbased progressive combined exercises over a �wait and see� approach for patellofemoral pain syndrome. A second RCT suggests that supervised closed kinetic chain exercises may lead to greater symptom improvement than open chain exercises for patellofemoral pain syndrome. One RCT suggests that clinic-based group exercises may be more effective than multimodal physiotherapy in male athletes with persistent groin pain.
Conclusion: We found limited high-quality evidence to support the use of exercise for the management of soft tissue injuries of the lower extremity. The evidence suggests that clinic-based exercise programs may benefit patients with patellofemoral pain syndrome and persistent groin pain. Further high-quality research is needed. (J Manipulative Physiol Ther 2016;39:110-120.e1)
Soft tissue injuries of the lower limb are common. In the United States, 36% of all injuries presenting to emergency departments are sprains and/or strains of the lower extremity. Among Ontario workers, approximately 19% of all approved lost time compensation claims are related to lower extremity injuries. Moreover, 27.5% of Saskatchewan adults injured in a traffic collision report pain in the lower extremity. Soft tissue injuries of the hip, thigh, and knee are costly and place a significant economic and disability burden on workplaces and compensation systems. According to the US Department of Labor Bureau of Statistics, the median time off work for lower extremity injuries was 12 days in 2013. Knee injuries were associated with the longest work absenteeism (median, 16 days).
Most soft tissue injuries of the lower limb are managed conservatively, and exercise is commonly used to treat these injuries. Exercise aims to promote good physical health and restore normal function of the joints and surrounding soft tissues through concepts which include range of motion, stretching, strengthening, endurance, agility, and proprioceptive exercises. However, the evidence about the effectiveness of exercise for managing soft tissue injuries of the lower limb is unclear.
Previous systematic reviews have investigated the effectiveness of exercise for the management of soft tissue injuries of the lower extremity. Reviews suggest that exercise is effective for the management of patellofemoral pain syndrome and groin injuries but not for patellar tendinopathy. To our knowledge, the only review reporting on the effectiveness of exercise for acute hamstring injuries found little evidence to support stretching, agility, and trunk stability exercises.
The purpose of our systematic review was to investigate the effectiveness of exercise compared to other interventions, placebo/sham interventions, or no intervention in improving self-rated recovery, functional recovery (eg, return to activities, work, or school), or clinical outcomes (eg, pain, health-related quality of life, depression) of patients with soft tissue injuries of the hip, thigh, and knee.
Methods
Registration
This systematic review protocol was registered with the International Prospective Register of Systematic Reviews on March 28, 2014 (CRD42014009140).
Eligibility Criteria
Population. Our review targeted studies of adults (?18 years) and/or children with soft tissue injuries of the hip, thigh, or knee. Soft tissue injuries include but are not limited to grade I to II sprains/strains; tendonitis; tendinopathy; tendinosis; patellofemoral pain (syndrome); iliotibial band syndrome; nonspecific hip, thigh, or knee pain (excluding major pathology); and other soft tissue injuries as informed by available evidence. We defined the grades of sprains and strains according to the classification proposed by the American Academy of Orthopaedic Surgeons (Tables 1 and 2). Affected soft tissues in the hip include the supporting ligaments and muscles crossing the hip joint into the thigh (including the hamstrings, quadriceps, and adductor muscle groups). Soft tissues of the knee include the supporting intra-articular and extra-articular ligaments and muscles crossing the knee joint from the thigh including the patellar tendon. We excluded studies of grade III sprains or strains, acetabular labral tears, meniscal tears, osteoarthritis, fractures, dislocations, and systemic diseases (eg, infection, neoplasm, inflammatory disorders).
Interventions. We restricted our review to studies that tested the isolated effect of exercise (ie, not part of a multimodal program of care). We defined exercise as any series of movements aimed at training or developing the body by routine practice or as physical training to promote good physical health.
Comparison Groups. We included studies that compared 1 or more exercise interventions to one another or one exercise intervention to other interventions, wait list, placebo/sham interventions, or no intervention.
Outcomes. To be eligible, studies had to include one of the following outcomes: (1) self-rated recovery; (2) functional recovery (eg, disability, return to activities, work, school, or sport); (3) pain intensity; (4) health-related quality of life; (5) psychological outcomes such as depression or fear; and (6) adverse events.
Study Characteristics. Eligible studies met the following criteria: (1) English language; (2) studies published between January 1, 1990, and April 8, 2015; (3) randomized controlled trials (RCTs), cohort studies, or case-control studies which are designed to assess the effectiveness and safety of interventions; and (4) included an inception cohort of a minimum of 30 participants per treatment arm with the specified condition for RCTs or 100 participants per group with the specified condition in cohort studies or case-control studies. Studies including other grades of sprains or strains in the hip, thigh, or knee had to provide separate results for participants with grades I or II sprains/strains to be included.
We excluded studies with the following characteristics: (1) letters, editorials, commentaries, unpublished manuscripts, dissertations, government reports, books and book chapters, conference proceedings, meeting abstracts, lectures and addresses, consensus development statements, or guideline statements; (2) study designs including pilot studies, cross-sectional studies, case reports, case series, qualitative studies, narrative reviews, systematic reviews (with or without meta-analyses), clinical practice guidelines, biomechanical studies, laboratory studies, and studies not reporting on methodology; (3) cadaveric or animal studies; and (4) studies on patients with severe injuries (eg, grade III sprains/strains, fractures, dislocations, full ruptures, infections, malignancy, osteoarthritis, and systemic disease).
Information Sources
We developed our search strategy with a health sciences librarian (Appendix 1). The Peer Review of Electronic Search Strategies (PRESS) Checklist was used by a second librarian to review the search strategy for completeness and accuracy. We searched MEDLINE and EMBASE, considered to be the major biomedical databases, and PsycINFO, for psychological literature through Ovid Technologies, Inc; CINAHL Plus with Full Text for nursing and allied health literature through EBSCOhost; and the Cochrane Central Register of Controlled Trials through Ovid Technologies, Inc, for any studies not captured by the other databases. The search strategy was first developed in MEDLINE and subsequently adapted to the other bibliographic databases. Our search strategies combined controlled vocabulary relevant to each database (eg, MeSH for MEDLINE) and text words relevant to exercise and soft tissue injuries of the hip, thigh, or knee including grade I to II sprain or strain injuries (Appendix 1). We also hand searched the reference lists of previous systematic reviews for any additional relevant studies.
Study Selection
A 2-phase screening process was used to select eligible studies. Random pairs of independent reviewers screened citation titles and abstracts to determine the eligibility of studies in phase 1. Screening resulted in studies being classified as relevant, possibly relevant, or irrelevant. In phase 2, the same pairs of reviewers independently screened the possibly relevant studies to determine eligibility. Reviewers met to reach consensus on the eligibility of studies and resolve disagreements. A third reviewer was used if consensus could not be reached.
Assessment of Risk of Bias
Independent reviewers were randomly paired to critically appraise the internal validity of eligible studies using the Scottish Intercollegiate Guidelines Network (SIGN) criteria. The impact of selection bias, information bias, and confounding on the results of a study was qualitatively evaluated using the SIGN criteria. These criteria were used to guide reviewers in making an informed overall judgment on the internal validity of studies. This methodology has been previously described. A quantitative score or a cutoff point to determine the internal validity of studies was not used for this review.
The SIGN criteria for RCTs were used to critically appraise the following methodological aspects: (1) clarity of the research question, (2) randomization method, (3) concealment of treatment allocation, (4) blinding of treatment and outcomes, (5) similarity of baseline�characteristics between/among treatment arms, (6) cointervention contamination, (7) validity and reliability of outcome measures, (8) follow-up rates, (9) analysis according to intention-to-treat principles, and (10) comparability of results across study sites (where applicable). Consensus was reached through reviewer discussion. Disagreements were resolved by an independent third reviewer when consensus could not be reached. The risk of bias of each appraised study was also reviewed by a senior epidemiologist (PC). Authors were contacted when additional information was needed to complete the critical appraisal. Only studies with low risk of bias were included in our evidence synthesis.
Data Extraction and Synthesis of Results
Data were extracted from studies (DS) with low risk of bias to create evidence tables. A second reviewer independently checked the extracted data. We stratified results based on the duration of the condition (recent onset [0-3 months], persistent [N3 months], or variable duration [recent onset and persistent combined]).
We used standardized measures to determine the clinical importance of changes reported in each trial for common outcome measures. These include a between-group difference of 2/10 points on the Numeric Rating Scale (NRS), 2/10 cm difference on the Visual Analog Scale (VAS), and 10/100 point difference on the Kujala Patellofemoral scale, otherwise known as the Anterior Knee Pain Scale.
Statistical Analyses
Agreement between reviewers for the screening of articles was computed and reported using the ? statistic and 95% confidence interval (CI). Where available, we used data provided in the studies with a low risk of bias to measure the association between the tested interventions and the outcomes by computing the relative risk (RR) and its 95% CI. Similarly, we computed differences in mean changes between groups and 95% CI to quantify the effectiveness of interventions. The calculation of 95% CIs was based on the assumption that baseline and follow-up outcomes were highly correlated (r = 0.80).
Reporting
This systematic review was organized and reported based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement.
Dr. Alex Jimenez’s Insight
As a doctor of chiropractic, automobile accident injuries are one of the most common reasons people seek chiropractic care. From neck injuries, such as whiplash, to headaches and back pain, chiropractic can be utilized to safely and effectively restore the integrity of the spine after a car crash. A chiropractor like myself will often use a combination of spinal adjustments and manual manipulations, as well as a variety of other non-invasive treatment methods,�to gently correct any spinal misalignments resulting from an auto accident injury. Whiplash and other types of neck injuries occur when the complex structures along the cervical spine are stretched beyond their natural range of movement due to the sudden back-and-forth movement of the head and neck from the force of the impact. Back injury, particularly in the lower spine, are also common as a result of an automobile accident. When the complex structures along the lumbar spine are damaged or injured, symptoms of sciatica may radiate down the lower back, into the buttocks, hips, thighs, legs and down into the feet. Knee injuries may also occur upon impact during an auto accident. Exercise is frequently used with chiropractic care to help promote recovery as well as improve strength, flexibility and mobility. Rehabilitation exercises are offered to patients to further restore the integrity of their body. The following research studies demonstrate that exercise, compared to non-invasive treatment options, is a safe and effective treatment method for individuals suffering with neck and lower extremity injury from a car crash.
Results
Study Selection
We screened 9494 citations based on the title and abstract (Figure 1). Of these, 60 full-text publications were screened, and 9 articles were critically appraised. The primary reasons for ineligibility during full text screening were (1) ineligible study design, (2) small sample size (n b 30 per treatment arm), (3) multimodal interventions not allowing isolation of the effectiveness of exercise, (4) ineligible study population, and (5) interventions not meeting our definition of exercise (Figure 1). Of those critically appraised, 3 studies (reported in 4 articles) had low risk of bias and were included in our synthesis. The interrater agreement for the screening of the articles was ? = 0.82 (95% CI, 0.69-0.95). The percentage agreement for the critical appraisal of studies was 75% (6/8 studies). Disagreement was resolved through discussion for 2 studies. We contacted authors from 5 studies during critical appraisal to request additional information and 3 responded.
Study Characteristics
The studies with low risk of bias were RCTs. One study, conducted in the Netherlands, examined the effectiveness of a standardized exercise program compared to a �wait and see� approach in participants with patellofemoral pain syndrome of variable duration. A second study, with outcomes reported in 2 articles, compared the benefit of closed vs open kinetic chain exercises in individuals with�variable duration patellofemoral pain syndrome in Belgium. The final study, conducted in Denmark, investigated active training compared to a multimodal physiotherapy intervention for the management of persistent adductor-related groin pain.
Two RCTs used exercise programs that combined strengthening exercises with balance or agility training for the lower extremity. Specifically, the strengthening exercises consisted of both isometric and concentric contractions of the quadriceps, hip adductor, and gluteal muscles for the management of patellofemoral pain46 and hip adductors and muscles of the trunk and pelvis for adductor-related groin pain. The exercise programs ranged from 646 to 1243 weeks in duration and were supervised and clinic based with additional daily home exercises. The exercise programs were compared to a �wait and see� approach or to multimodal physiotherapy. The third RCT compared 2 different 5-week protocols which combined either closed or open kinetic chain strengthening and stretching exercises for the lower extremity musculature.
Meta-analysis was not performed due to heterogeneity of accepted studies with respect to patient populations, interventions, comparators, and outcomes. Principles of best evidence synthesis were used to develop evidence statements and perform a qualitative synthesis of findings from studies with low risk of bias.
Risk of Bias Within Studies
The studies with low risk of bias had a clearly defined research question, used appropriate blinding methods where possible, reported adequate similarity of baseline characteristics between treatment arms, and performed an intention-to-treat analyses where applicable (Table 3). The RCTs had follow-up rates greater than 85%. However, these studies also had methodological limitations: insufficient detail describing methods for allocation concealment (1/3), insufficient detail describing methods of randomization (1/3), the use of outcome measures that have not been demonstrated to be valid or reliable (ie, muscle length and successful treatment) (2/3), and clinically important differences in baseline characteristics (1/3).
Of 9 relevant articles, 5 were deemed to have high risk of bias. These studies had the following limitations: (1) poor or unknown randomization methods (3/5); (2) poor or unknown allocation concealment methods (5/ 5); (3) outcome assessor not blinded (4/ 5); (4) clinically important differences in baseline characteristics (3/5); (5) dropouts not reported, insufficient information regarding dropouts per group or large differences in dropout rates between treatment arms (N15%) (3/5); and (6) a lack of information about or no intention-to-treat analysis (5/5).
Summary of Evidence
Patellofemoral Pain Syndrome of Variable Duration. Evidence from 1 RCT suggests that a clinic-based progressive exercise program may provide short- and long-term benefit over usual care for the management of patellofemoral pain syndrome of variable duration. van Linschoten et al randomized participants with a clinical diagnosis of patellofemoral pain syndrome of 2 months to 2 years duration to (1) a clinic-based exercise program (9 visits over 6 weeks) consisting of progressive, static, and dynamic strengthening exercises for the quadriceps, adductor, and gluteal muscles and balance and flexibility exercises, or (2) a usual care �wait and see� approach. Both groups received standardized information, advice, and home-based isometric exercises for the quadriceps based on recommendations from Dutch General Practitioner guidelines (Table 4). There�were statistically significant differences favoring the exercise group for (1) pain (NRS) at rest at 3 months (mean change difference 1.1/10 [95% CI, 0.2-1.9]) and 6 months (mean change difference 1.3/10 [95% CI, 0.4-2.2]); (2) pain (NRS) with activity at 3 months (mean change difference 1.0/10 [95% CI, 0.1-1.9]) and 6 months (mean change difference 1.2/10 [95% CI, 0.2-2.2]); and (3) function (Kujala Patellofemoral Scale [KPS]) at 3 months (mean change difference 4.9/100 [95% CI, 0.1-9.7]). However, none of these differences were clinically important. Furthermore, there were no significant differences in the proportion of participants reporting recovery (fully recovered, strongly recovered), but the exercise group was more likely to report improvement at 3-month follow-up (odds ratio [OR], 4.1 [95% CI, 1.9-8.9]).
Evidence from a second RCT suggests that physiotherapist- supervised closed kinetic chain leg exercises (where the foot remains in constant contact with a surface) may provide short-term benefit compared to supervised open kinetic chain exercises (where the limb moves freely) for some patellofemoral pain syndrome symptoms (Table 4). All participants trained for 30 to 45 minutes, 3 times per week for 5 weeks. Both groups were instructed to perform static lower limb stretching after each training session. Those randomized to closed chain exercises performed supervised (1) leg presses, (2) knee bends, (3) stationary biking, (4) rowing, (5) step-up and step-down exercises, and (6) progressive jumping exercises. Open chain exercise participants performed (1) maximal quad muscle contraction, (2) straight-leg raises, (3) short arc movements from 10� to full knee extension, and (4) leg adduction. Effect sizes were not reported, but the authors reported statistically significant differences favoring closed kinetic chain exercise at 3 months for (1) frequency of locking (P = .03), (2) clicking sensation (P = .04), (3) pain with isokinetic testing (P = .03), and (4) pain during night (P = .02). The clinical significance of these results is unknown. There were no statistically significant differences between groups for any other pain or functional measures at any follow-up period.
Persistent Adductor-Related Groin Pain
Evidence from 1 RCT suggests that a clinic-based group exercise program is more effective than a multimodal program of care for persistent adductor-related groin pain. H�lmich et al studied a group of male athletes with a clinical diagnosis of adductor-related groin pain of greater than 2 months duration (median duration, 38-41 weeks; range, 14-572 weeks) with or without osteitis pubis. Participants were randomized to (1) a clinic-based group exercise program (3 sessions per week for 8-12 weeks) consisting of isometric and concentric resistance strengthening exercises for the adductors, trunk, and pelvis; balance and agility exercises for the lower extremity; and stretching for the abdominals, back, and lower extremity (with the exception of the adductor muscles) or (2) a multimodal physiotherapy program (2 visits per week for 8-12 weeks) consisting of laser; transverse friction massage; transcutaneous electrical nerve stimulation (TENS); and stretching for the adductors, hamstrings, and hip flexors (Table 4). Four months after the intervention, the exercise group was more likely to report that their condition was �much better� (RR, 1.7 [95% CI, 1.0-2.8]).
Adverse Events
None of the included studies commented on the frequency or nature of adverse events.
Discussion
Summary of Evidence
Our systematic review examined the effectiveness of exercise for the management of soft tissue injuries of the hip, thigh, or knee. Evidence from 1 RCT suggests that a clinic-based progressive combined exercise program may offer additional short- or long-term benefit compared to providing information and advice for the management of patellofemoral pain syndrome of variable duration. There is also evidence that supervised closed kinetic chain exercises may be beneficial for some patellofemoral pain syndrome symptoms compared to open kinetic chain exercises. For persistent adductor-related groin pain, evidence from 1 RCT suggests that a clinic-based group exercise program is more effective than a multimodal program of care. Despite the common and frequent use of exercise prescription, there is limited high-quality evidence to inform the use of exercise for the management of soft tissue injuries of the lower extremity. Specifically, we did not find high-quality studies on exercise for the management of some of the more commonly diagnosed conditions including patellar tendinopathy, hamstring sprain and strain injuries, hamstring tendinopathy, trochanteric bursitis, or capsular injuries of the hip.
Previous Systematic Reviews
Our results are consistent with findings from previous systematic reviews, concluding that exercise is effective for the management of patellofemoral pain syndrome and groin pain. However, the results from previous systematic reviews examining the use of exercise for the management of patellar tendinopathy and acute hamstring injuries are inconclusive. One review noted strong evidence for use of eccentric training, whereas others reported uncertainty of whether isolated eccentric exercises were beneficial for tendinopathy compared to other forms of exercise. Furthermore, there is limited evidence of a positive effect from stretching, agility and trunk stability exercises, or slump stretching for the management of acute�hamstring injuries. Differing conclusions between systematic reviews and the limited number of studies deemed admissible in our work may be attributed to differences in methodology. We screened reference lists of previous systematic reviews, and most studies included in the reviews did not meet our inclusion criteria. Many studies accepted in other reviews had small sample sizes (b30 per treatment arm). This increases the risk of residual confounding while also reducing the effect size precision. Furthermore, a number of systematic reviews included case series and case studies. These types of studies are not designed to assess the effectiveness of interventions. Finally, previous reviews included studies where exercise was part of a multimodal intervention, and as a consequence, the isolated effect of exercise could not be ascertained. Of the studies that satisfied our selection criteria, all were critically appraised in our review, and only 3 had low risk of bias and were included in our synthesis.
Strengths
Our review has many strengths. First, we developed a rigorous search strategy that was independently reviewed by a second librarian. Second, we defined clear inclusion and exclusion criteria for the selection of possibly relevant studies and only considered studies with adequate sample sizes. Third, pairs of trained reviewers screened and critically appraised eligible studies. Fourth, we used a valid set of criteria (SIGN) to critically appraise studies. Finally, we restricted our synthesis to studies with low risk of bias.
Limitations and Recommendations for Future Research
Our review also has limitations. First, our search was limited to studies published in the English language. However, previous reviews have found that the restriction of systematic reviews to English language studies has not led to a bias in reported results. Second, despite our broad definition of soft tissue injuries of the hip, thigh, or knee, our search strategy may not have captured all potentially relevant studies. Third, our review may have missed potentially relevant studies published before 1990. We aimed to minimize this by hand searching the reference lists of previous systematic reviews. Finally, critical appraisal requires scientific judgment that may differ between reviewers. We minimized this potential bias by training reviewers in the use of the SIGN tool and using a consensus process to determine study admissibility. Overall, our systematic review highlights a deficit of strong research in this area.
High-quality studies on the effectiveness of exercise for the management of soft tissue injuries of the lower extremity are needed. Most studies included in our review (63%) had a high risk of bias and could not be included in our synthesis. Our review identified important gaps in the literature. Specifically, studies are needed to inform the specific effects of exercises, their long-term effects, and the optimal doses of intervention. Furthermore, studies are needed to determine the relative effectiveness of different types of exercise programs and if the effectiveness varies for soft tissue injuries of the hip, thigh, and knee.
Conclusion
There is limited high-quality evidence to inform the use of exercise for the management of soft tissue injuries of the hip, thigh, and knee. The current evidence suggests that a clinic-based progressive combined exercise program may lead to improved recovery when added to information and advice on resting and avoiding pain provoking activities for the management of patellofemoral pain syndrome. For persistent adductor-related groin pain, a supervised clinic- based group exercise program is more effective than multimodal care in promoting recovery.
Funding Sources and Potential Conflicts of Interest
This study was funded by the Ontario Ministry of Finance and the Financial Services Commission of Ontario (RFP no. OSS_00267175). The funding agency was not involved in the collection of data, data analysis, interpretation of data, or drafting of the manuscript. The research was undertaken, in part, thanks to funding from the Canada Research Chairs program. Pierre C�t� has previously received funding from a Grant from the Ontario Ministry of Finance; consulting for the Canadian Chiropractic Protective Association; speaking and/or teaching arrangements for the National Judicial Institute and Soci�t� des M�decins Experts du Quebec; trips/travel, European Spine Society; board of directors, European Spine Society; grants: Aviva Canada; fellowship support, Canada Research Chair Program�Canadian Institutes of Health Research. No other conflicts of interest were reported for this study.
Contributorship Information
Concept development (provided idea for the research): D.S., C.B., P.C., J.W., H.Y., S.V.
Design (planned the methods to generate the results): D.S., C.B., P.C., H.S., J.W., H.Y., S.V.
Supervision (provided oversight, responsible for organization and implementation, writing of the manuscript): D.S., P.C.
Data collection/processing (responsible for experiments, patient management, organization, or reporting data): D.S., C.B., H.S., J.W., D.e.S., R.G., H.Y., K.R., J.C., K.D., P.C., P.S., R.M., S.D., S.V.
Analysis/interpretation (responsible for statistical analysis, evaluation, and presentation of the results): D.S., C.B., P.C., H.S., M.S., K.R., L.C.
Literature search (performed the literature search): A.T.V.
Writing (responsible for writing a substantive part of the manuscript): D.S., C.B., P.C., H.S.
Critical review (revised manuscript for intellectual content, this does not relate to spelling and grammar checking): D.S., P.C., H.S., J.W., D.e.S., R.G., M.S., A.T.V., H.Y., K.R., J.C., K.D., L.C., P.S., S.D., R.M., S.V.
Practical Applications
There is evidence to suggest that clinic-based exercises may benefit patients with patellofemoral pain syndrome or adductor-related groin pain.
Supervised progressive exercises may be beneficial for patellofemoral pain syndrome of variable duration compared to information/advice.
Supervised closed kinetic chain exercises may provide more benefit compared to open kinetic chain exercises for some patellofemoral pain syndrome symptoms.
Self-rated improvement in persistent groin pain is higher after a clinic-based group exercise program compared to multimodal physiotherapy.
Are Non-Invasive Interventions Effective for the Management of Headaches Associated with Neck Pain?
Furthermore,�other non-invasive interventions, as well as non-pharmacological interventions, are also commonly utilized to help treat symptoms of neck pain and headaches associated with neck injuries, such as whiplash, caused by automobile accidents. As mentioned before, whiplash is one of the most common types of neck injuries resulting from auto accidents. Chiropractic care, physical therapy and exercise, can be used to improve the symptoms of neck pain, according to the following research studies.
Abstract
Purpose
To update findings of the 2000�2010 Bone and Joint Decade Task Force on Neck Pain and its Associated Disorders and evaluate the effectiveness of non-invasive and non-pharmacological interventions for the management of patients with headaches associated with neck pain (i.e., tension-type, cervicogenic, or whiplash-related headaches).
Methods
We searched five databases from 1990 to 2015 for randomized controlled trials (RCTs), cohort studies, and case�control studies comparing non-invasive interventions with other interventions, placebo/sham, or no interventions. Random pairs of independent reviewers critically appraised eligible studies using the Scottish Intercollegiate Guidelines Network criteria to determine scientific admissibility. Studies with a low risk of bias were synthesized following best evidence synthesis principles.
Results
We screened 17,236 citations, 15 studies were relevant, and 10 had a low risk of bias. The evidence suggests that episodic tension-type headaches should be managed with low load endurance craniocervical and cervicoscapular exercises. Patients with chronic tension-type headaches may also benefit from low load endurance craniocervical and cervicoscapular exercises; relaxation training with stress coping therapy; or multimodal care that includes spinal mobilization, craniocervical exercises, and postural correction. For cervicogenic headaches, low load endurance craniocervical and cervicoscapular exercises; or manual therapy (manipulation with or without mobilization) to the cervical and thoracic spine may also be helpful.
Conclusions
The management of headaches associated with neck pain should include exercise. Patients who suffer from chronic tension-type headaches may also benefit from relaxation training with stress coping therapy or multimodal care. Patients with cervicogenic headache may also benefit from a course of manual therapy.
We would like to acknowledge and thank all of the individuals who have made important contributions to this review: Robert Brison, Poonam Cardoso, J. David Cassidy, Laura Chang, Douglas Gross, Murray Krahn, Michel Lacerte, Gail Lindsay, Patrick Loisel, Mike Paulden, Roger Salhany, John Stapleton, Angela Verven, and Leslie Verville. We would also like to thank Trish Johns-Wilson at the University of Ontario Institute of Technology for her review of the search strategy.
Compliance with Ethical Standards
Conflict of Interest
Dr. Pierre C�t� has received a grant from the Ontario government, Ministry of Finance, funding from the Canada Research Chairs program, personal fees from National Judicial Institute for lecturing, and personal fees from European Spine Society for teaching. Drs. Silvano Mior and Margareta Nordin have received reimbursement for travel expenses to attend meetings for the study. The remaining authors report no declarations of interest.
Funding
This work was supported by the Ontario Ministry of Finance and the Financial Services Commission of Ontario [RFP# OSS_00267175]. The funding agency had no involvement in the study design, collection, analysis, interpretation of data, writing of the manuscript or decision to submit the manuscript for publication. The research was undertaken, in part, thanks to funding from the Canada Research Chairs program to Dr. Pierre C�t�, Canada Research Chair in Disability Prevention and Rehabilitation at the University of Ontario Institute of Technology.
In conclusion,�exercise included in chiropractic care and other non-invasive interventions should be utilized as an essential part of treatment to further help improve the symptoms of neck injury as well as that of hip, thigh and knee injury. According to the above research studies, exercise, or physical activity, is beneficial towards speeding up recovery time for patients with automobile accident injuries and for restoring strength, flexibility and mobility to the affected structures of the spine. Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Sciatica
Sciatica is referred to as a collection of symptoms rather than a single type of injury or condition. The symptoms are characterized as radiating pain, numbness and tingling sensations from the sciatic nerve in the lower back, down the buttocks and thighs and through one or both legs and into the feet. Sciatica is commonly the result of irritation, inflammation or compression of the largest nerve in the human body, generally due to a herniated disc or bone spur.
1. Lambers K, Ootes D, Ring D. Incidence of patients with lower
extremity injuries presenting to US emergency departments by
anatomic region, disease category, and age. Clin Orthop Relat
Res 2012;470(1):284-90.
2. Workplace Safety and Insurance Board. By the numbers: 2014
WSIB statistical report. Injury profile�schedule 1; historical
and supplementary data on leading part of body injuries.
[cited June 22, 2015]; Available from: http://www.
wsibstatistics.ca/en/s1injury/s1part-of-body/ 2014.
3. Hincapie CA, Cassidy JD, C�t� P, Carroll LJ, Guzman J.
Whiplash injury is more than neck pain: a population-based
study of pain localization after traffic injury. J Occup Environ
Med 2010;52(4):434-40.
4. Bureau of Labor Statistics US Department of Labor. Nonfatal
occupational injuries and illnesses requiring days away from
work. Table 5. Washington, DC 2014 [June 22, 2015];
Available from: http://www.bls.gov/news.release/archives/
osh2_12162014.pdf 2013.
5. New ZealandGuidelinesDevelopmentGroup. The diagnosis and
management of soft tissue knee injuries: internal derangements.
Best practice evidence-based guideline. Wellington: Accident
Compensation Corporation; 2003 [[June 22, 2015]; Available
from: http://www.acc.co.nz/PRD_EXT_CSMP/groups/
external_communications/documents/guide/wcmz002488.pdf].
6. Bizzini M, Childs JD, Piva SR, Delitto A. Systematic review of
the quality of randomized controlled trials for patellofemoral pain
syndrome. J Orthop Sports Phys Ther 2003;33(1):4-20.
7. Crossley K, Bennell K, Green S, McConnell J. A systematic
review of physical interventions for patellofemoral pain
syndrome. Clin J Sport Med 2001;11(2):103-10.
8. Harvie D, O�Leary T, Kumar S. A systematic review of
randomized controlled trials on exercise parameters in the
treatment of patellofemoral pain: what works? J Multidiscip
Healthc 2011;4:383-92.
9. Lepley AS, Gribble PA, Pietrosimone BG. Effects of electromyographic
biofeedback on quadriceps strength: a systematic
review. J Strength Cond Res 2012;26(3):873-82.
10. Peters JS, Tyson NL. Proximal exercises are effective in treating
patellofemoral pain syndrome: a systematic review. Int J Sports
Phys Ther 2013;8(5):689-700.
11. Wasielewski NJ, Parker TM, Kotsko KM. Evaluation of
electromyographic biofeedback for the quadriceps femoris: a
systematic review. J Athl Train 2011;46(5):543-54.
12. Kristensen J, Franklyn-Miller A. Resistance training in musculoskeletal
rehabilitation: a systematic review. Br J Sports Med
2012;46(10):719-26.
13. Larsson ME, Kall I, Nilsson-Helander K. Treatment of patellar
tendinopathy�a systematic review of randomized controlled
trials. Knee Surg Sports Traumatol Arthrosc 2012;20(8):1632-46.
14. Malliaras P, Barton CJ, Reeves ND, Langberg H. Achilles and
patellar tendinopathy loading programmes: a systematic review
comparing clinical outcomes and identifying potential mechanisms
for effectiveness. Sports Med 2013;43(4):267-86.
15. Wasielewski NJ, KotskoKM. Does eccentric exercise reduce pain
and improve strength in physically active adults with symptomatic
lower extremity tendinosis? A systematic review. J Athl Train
2007;42(3):409-21.
16. Reurink G, Goudswaard GJ, Tol JL, Verhaar JA, Weir A, Moen
MH. Therapeutic interventions for acute hamstring injuries: a
systematic review. Br J Sports Med 2012;46(2):103-9.
17. American Academy of Orthopaedic Surgeons. Sprains, strains,
and other soft-tissue injuries. [updated July 2007 March 11,
2013]; Available from: http://orthoinfo.aaos.org/topic.cfm?topic=
A00304 2007.
18. Abenhaim L, Rossignol M, Valat JP, et al. The role of activity in
the therapeutic management of back pain. Report of
the International Paris Task Force on Back Pain. Spine 2000;
25(4 Suppl):1S-33S.
19. McGowan J, Sampson M, Lefebvre C. An evidence
based checklist for the Peer Review of Electronic Search Strategies
(PRESS EBC). Evid Based Library Inf Pract 2010;5(1):149-54.
20. Sampson M, McGowan J, Cogo E, Grimshaw J, Moher D,
Lefebvre C. An evidence-based practice guideline for the peer
review of electronic search strategies. J Clin Epidemiol 2009;
62(9):944-52.
21. Almeida MO, Silva BN, Andriolo RB, Atallah AN, Peccin MS.
Conservative interventions for treating exercise-related musculotendinous,
ligamentous and osseous groin pain. Cochrane
Database Syst Rev 2013;6:CD009565.
22. Ellis R, Hing W, Reid D. Iliotibial band friction syndrome�a
systematic review. Man Ther 2007;12(3):200-8.
23. Machotka Z, Kumar S, Perraton LG. A systematic review of the
literature on the effectiveness of exercise therapy for groin pain in
athletes. SportsMed Arthrosc Rehabil Ther Technol 2009;1(1):5.
24. Moksnes H, Engebretsen L, Risberg MA. The current evidence
for treatment of ACL injuries in children is low: a systematic
review. J Bone Joint Surg Am 2012;94(12):1112-9.
25. Harbour R, Miller J. A new system for grading recommendations
in evidence based guidelines. BMJ 2001;323(7308):
334-6.
26. Carroll LJ, Cassidy JD, Peloso PM, Garritty C, Giles-Smith L.
Systematic search and review procedures: results of the WHO
Collaborating Centre Task Force on Mild Traumatic Brain
Injury. J Rehabil Med 2004(43 Suppl):11-4.
27. Carroll LJ, Cassidy JD, Peloso PM, et al. Methods for the best
evidence synthesis on neck pain and its associated disorders: the
Bone and Joint Decade 2000-2010 Task Force on Neck Pain
and Its Associated Disorders. JManipulative Physiol Ther 2009;
32(2 Suppl):S39-45.
28. C�t� P, Cassidy JD, Carroll L, Frank JW, Bombardier C. A
systematic review of the prognosis of acute whiplash and a new
conceptual framework to synthesize the literature. Spine (Phila
Pa 1976) 2001;26(19):E445-58.
29. Hayden JA, Cote P, Bombardier C. Evaluation of the quality of
prognosis studies in systematic reviews. Ann Intern Med 2006;
144(6):427-37.
30. Hayden JA, van der Windt DA, Cartwright JL, Cote P,
Bombardier C. Assessing bias in studies of prognostic factors.
Ann Intern Med 2013;158(4):280-6.
31. Spitzer WO, Skovron ML, Salmi LR, et al. Scientific
monograph of the Quebec Task Force on Whiplash-Associated
Disorders: redefining �whiplash� and its management. Spine
1995;20(8 Suppl):1S-73S.
32. van der Velde G, van Tulder M, Cote P, et al. The sensitivity of
review results to methods used to appraise and incorporate trial
quality into data synthesis. Spine (Phila Pa 1976) 2007;32(7):
796-806.
33. Slavin RE. Best evidence synthesis: an intelligent alternative to
meta-analysis. J Clin Epidemiol 1995;48(1):9-18.
34. Hinman RS, McCrory P, Pirotta M, et al. Efficacy of
acupuncture for chronic knee pain: protocol for a randomised
controlled trial using a Zelen design. BMCComplement Altern
Med 2012;12:161.
35. Crossley KM, Bennell KL, Cowan SM, Green S. Analysis of
outcome measures for persons with patellofemoral pain: which
are reliable and valid? Arch Phys Med Rehabil 2004;85(5):
815-22.
36. Cohen J. A coefficient of agreement for nominal scales. Educ
Psychol Meas 1960;20(1):37-46.
37. Abrams KR, Gillies CL, Lambert PC. Meta-analysis of
heterogeneously reported trials assessing change from baseline.
Stat Med 2005;24(24):3823-44.
38. Follmann D, Elliott P, Suh I, Cutler J. Variance imputation for
overviews of clinical trials with continuous response. J Clin
Epidemiol 1992;45(7):769-73.
39. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred
reporting items for systematic reviews and meta-analyses: the
PRISMA statement. BMJ 2009;339:b2535.
40. Askling CM, Tengvar M, Thorstensson A. Acute hamstring
injuries in Swedish elite football: a prospective randomised
controlled clinical trial comparing two rehabilitation protocols.
Br J Sports Med 2013;47(15):953-9.
41. Dursun N, Dursun E, Kilic Z. Electromyographic biofeedbackcontrolled
exercise versus conservative care for patellofemoral
pain syndrome. Arch Phys Med Rehabil 2001;82(12):1692-5.
42. Harrison EL, Sheppard MS, McQuarry AM. A randomized
controlled trial of physical therapy treatment programs in
patellofemoral pain syndrome. Physiother Can 1999;1999:93-100.
43. Holmich P, Uhrskou P, Ulnits L, et al. Effectiveness of active
physical training as treatment for long-standing adductor-related
groin pain in athletes: randomised trial. Lancet 1999;353(9151):
439-43.
44. Lun VM, Wiley JP, Meeuwisse WH, Yanagawa TL. Effectiveness
of patellar bracing for treatment of patellofemoral pain
syndrome. Clin J Sport Med 2005;15(4):235-40.
45. Malliaropoulos N, Papalexandris S, Papalada A, Papacostas E.
The role of stretching in rehabilitation of hamstring injuries: 80
athletes follow-up. Med Sci Sports Exerc 2004;36(5):756-9.
46. van Linschoten R, van Middelkoop M, Berger MY, et al.
Supervised exercise therapy versus usual care for patellofemoral
pain syndrome: an open label randomised controlled trial. BMJ
2009;339:b4074.
47. Witvrouw E, Cambier D, Danneels L, et al. The effect of exercise
regimens on reflex response time of the vasti muscles in patients
with anterior knee pain: a prospective randomized intervention
study. Scand J Med Sci Sports 2003;13(4):251-8.
48. Witvrouw E, Lysens R, Bellemans J, Peers K, Vanderstraeten G.
Open versus closed kinetic chain exercises for patellofemoral
pain. A prospective, randomized study. Am J Sports Med 2000;
28(5):687-94.
49. Johnson AP, Sikich NJ, Evans G, et al. Health technology
assessment: a comprehensive framework for evidence-based
recommendations in Ontario. Int J Technol Assess Health Care
2009;25(2):141-50.
Back pain is one of the most common causes people visit their healthcare professional every year. A primary care physician is often the first doctor who can provide treatment for a variety of injuries and/or conditions, however, among those individuals seeking complementary and alternative treatment options for back pain, most people choose chiropractic care. Chiropractic care focuses on the diagnosis, treatment and prevention of trauma and disease of the musculoskeletal and nervous systems, by correcting misalignments of the spine through the use of spinal adjustments and manual manipulations.
Approximately 35% of individuals seek chiropractic treatment for back pain caused by automobile accidents, sports injuries, and a variety of muscle strains. When people suffer an trauma or injury as a result of an accident, however, they may first receive treatment for their symptoms of back pain in a hospital. Hospital outpatient care describes treatment which does not require an overnight stay at a medical facility. A research study conducted an analysis comparing the effects of chiropractic care and hospital outpatient management for back pain. The results are described in detail below.
Abstract
Objective: To compare the effectiveness over three years of chiropractic and hospital outpatient management for low back pain.
Design: Randomised allocation of patients to chiropractic or hospital outpatient management.
Setting: Chiropractic clinics and hospital outpatient departments within reasonable travelling distance of each other in I I centres.
Subjects: 741 men and women aged 18-64 years with low back pain in whom manipulation was not contraindicated.
Outcome measures: Change in total 0swestry questionnaire score and in score for pain and patient satisfaction with allocated treatment.
Results: According to total 0swestry scores improvement in all patients at three years was about 291/6 more in those treated by chiropractors than in those treated by the hospitals. The beneficial effect of chiropractic on pain was particularly clear. Those treated by chiropractors had more further treatments for back pain after the completion of trial treatment. Among both those initially referred from chiropractors and from hospitals more rated chiropractic helpful at three years than hospital management.
Conclusions: At three years the results confirm the findings of an earlier report that when chiropractic or hospital therapists treat patients with low back pain as they would in day to day practice those treated by chiropractic derive more benefit and long term satisfaction than those treated by hospitals.
Introduction
In 1990 we reported greater improvement in patients with low back pain treated by chiropractic compared with those receiving hospital outpatient management. The trial was “pragmatic” in allowing the therapists to treat patients as they would in day to day practice. At the time of our first report not all patients had been in the trial for more than six months. This paper presents the full results up to three years for all patients for whom follow up information from Oswestry questionnaires and for other outcomes was available for analysis. We also present data on pain from the questionnaire, which is by definition the main complaint prompting referral or self referral.
Methods
Methods were fully described in our first report. Patients initially referred or presenting either to a chiropractic clinic or in hospital were randomly allocated to be treated either by chiropractic or in hospital. A total of 741 patients started treatment. Progress was measured with the Oswestry questionnaire on back pain, which gives scores for I 0 sections for example, intensity of pain and difficulty with lifting, walking, and travelling. The result is expressed on a scale ranging from 0 (no pain or difficulties) to 100 (highest score for pain and greatest difficulty on all items). For an individual item, such as pain, scores range from 0 to 10. The main outcome measures are the changes in Oswestry score from before treatment to each follow up. At one, two, and three years patients were also asked about further treatment since the completion of their trial treatment or since the previous annual questionnaire. At the three year follow up patients were asked whether they thought their allocated trial treatment had helped their back pain.
In the random allocation of treatment minimisation was used within each centre to establish groups for the analysis of results according to initial referral clinic, length of current episode (more or less than ‘a month), presence or absence of a history of back pain, and an Oswestry score at entry of > 40 or <=40%.
Results were analysed on an intention to treat basis (subject to the availability of data at follow up as well as at entry for individual patients). Differences between mean changes were tested by unpaired t tests, and X2 tests were used to test for differences in proportions between the two treatment groups.
Dr. Alex Jimenez’s Insight
Chiropractic is a natural form of health care which purpose is to restore and maintain the function of the musculoskeletal and nervous systems, promoting spinal health and allowing the body to heal itself naturally. Our philosophy emphasizes on the treatment of the human body as a whole, rather than on the treatment of a single injury and/or condition. As an experienced chiropractor, my goal is to properly assess patients in order to determine which type of treatment will most effectively heal their individual type of health issue. From spinal adjustments and manual manipulations to physical activity, chiropractic care can help correct spinal misalignments that cause back pain.
Results
Follow up Oswestry questionnaires were returned by a consistently higher proportion of patients allocated to chiropractic than to hospital treatment. At six weeks, for example, they were returned by 95% and 89% of chiropractic and hospital patients, respectively and at three years by 77% and 70%.
Mean (SD) scores before treatment were 29-8 (14-2) and 28-5 (14-1) in the chiropractic and hospital treatment groups, respectively. Table I shows the differences between the mean changes in total Oswestry scores according to randomly allocated treatment group. The difference at each follow up is the mean change for the chiropractic group minus the mean change for the hospital group.
Positive differences therefore reflect more improvement (due to a greater change in score) in those treated by chiropractic than in hospital (negative differences the reverse). The 3-18 percentage point difference at three years in table I represents a 29% greater improvement in patients treated with chiropractic compared with hospital treatment, the absolute improvement in the two groups at this time being 14-1 and 10-9 percentage points, respectively. As in the first report those with short current episodes, a history of back pain, and initially high Oswestry scores tended to derive most benefit from chiropractic. Those referred by chiropractors consistently derived more benefit from chiropractic than those referred by hospitals.
Table II shows changes between the scores on pain intensity before treatment and the corresponding scores at the various follow up intervals. All these changes were positive that is, indicated improvement but were all significantly greater in those treated by chiropractic, including the changes early on that is, at six weeks and six months, when the proportions returning questionnaires were high. As with the results based on the full Oswestry score the improvement due to chiropractic was greatest in those initially referred by chiropractors, although there was also a non-significant improvement (ranging from 9% at six months to 34% at three years) due to chiropractic at each follow up interval in those referred by hospitals.
Other scores for individual items on the Oswestry index to show significant improvement attributable to chiropractic were ability to sit for more than a short time and sleeping (P=0’004 and 0 03, respectively, at three years), though the differences were not as consistent as for pain. Other scores (personal care, lifting, walking, standing, sex life, social life, and travelling) also nearly all improved more in the patients treated with chiropractic, though most of the differences were small compared with the differences for pain.
Higher proportions of patients allocated to chiropractic sought further treatment (of any kind) for back pain after completion of trial treatment than those managed in hospital. For example, between one and two years after trial entry 122/292 (42%) patients treated with chiropractic compared with 80/258 (3 1%) of hospital treated patients did so (Xl=6 8, P=0 0 1).
Table III shows the proportions of patients at three years who thought their allocated trial treatment had helped their back pain. Among those initially referred by hospitals as well as among those initially referred by chiropractors higher proportions treated by chiropractic considered that treatment had helped compared with those treated in hospital.
Key Messages
Back pain often remits spontaneously
Effective treatments for non-remitting episodes need to be more clearly identified
Chiropractic seems to be more effective than hospital management, possibly because more treatments are spread over longer time periods
A growing number of NHS purchasers are making complementary treatments, including chiropractic, available
Further trials to identify the effective components of chiropractic are needed
Discussion
The results at six weeks and six months shown in table I are identical with those in our first report, as all patients had then been followed up for six months. The findings at one year are similar as many patients had also been followed up then. The considerably larger numbers of patients with data now available at two and three years show smaller benefits at these intervals than previously, though these still significantly favour chiropractic. The substantial benefit of chiropractic on intensity of pain is evident early on and then persists. The consistently larger proportions lost to follow up throughout the trial in those treated in hospital than in those treated by chiropractic suggests greater satisfaction with chiropractic. This conclusion is supported (table III) by the higher proportions in each referral group considering chiropractic helpful by comparison with hospital treatment.
The main criticism of the trial after our first report centred on its “pragmatic” nature, particularly the larger number of chiropractic than hospital treatments and the longer period over which the chiropractic treatments were spread and which were deliberately allowed. These considerations and any consequences of the higher proportions of patients allocated to chiropractic who received further treatment in the later stages of follow up, however, do not apply to the results at six weeks and only apply to a limited extent at six months, when the proportions followed up were high and extra treatment had either not occurred at all or was not yet extensive. Benefits atributable to chiropractic were already evident (especially on pain, table II) at these shorter intervals.
We believe there is now more support for the need for “fastidious” trials focusing on specific components of management and on their feasibility. Meanwhile, the results of our trial show that chiropractic has a valuable part to play in the management of low back pain.
We thank Dr Iain Chalmers for commenting on an earlier draft of the paper. We thank the nurse coordinators, medical staff, physiotherapists, and chiropractors in the 11 centres for their work, and Dr Alan Breen of the British Chiropractic Association for his help. The centres were in Harrow Taunton, Plymouth, Bournemouth and Poole, Oswestry, Chertsey, Liverpool, Chelmsford, Birmingham, Exeter, and Leeds. Without the assistance of many staff members in each the trial could not have been completed.
Funding: Medical Research Council, the National Back Pain Association, the European Chiropractors Union, and the King Edward’s Hospital Fund for London.
Conflict of interest: None.
In conclusion,�after three years, the results of the research study comparing chiropractic care and hospital outpatient management for low back pain determined that people treated by chiropractic experienced more benefits as well as long-term satisfaction than those treated by hospitals. Because back pain is one of the most common�causes people visit their healthcare professional every year, its essential to seek the most effective type of health care. Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
References
Meade TW, Dyer S, Browne W, Townsend J, Frank AO. Low back pain of mechanical origin: randomised comparison of chiropractic and hospital outpatient treatment.�BMJ.�1990 Jun 2;300(6737):1431�1437.�[PMC free article]�[PubMed]
Fairbank JC, Couper J, Davies JB, O’Brien JP. The Oswestry low back pain disability questionnaire.�Physiotherapy.�1980 Aug;66(8):271�273.�[PubMed]
Pocock SJ, Simon R. Sequential treatment assignment with balancing for prognostic factors in the controlled clinical trial.�Biometrics.�1975 Mar;31(1):103�115.�[PubMed]
Additional Topics: Sciatica
Sciatica is referred to as a collection of symptoms rather than a single type of injury or condition. The symptoms are characterized as radiating pain, numbness and tingling sensations from the sciatic nerve in the lower back, down the buttocks and thighs and through one or both legs and into the feet. Sciatica is commonly the result of irritation, inflammation or compression of the largest nerve in the human body, generally due to a herniated disc or bone spur.
In association with professional experience in fitness and chiropractic care,�symptoms of back pain have been determined to improve in people who participate in physical activity and exercise, as directed by a physiotherapist, or physical therapist, or any other healthcare professional, such as a chiropractor. Various complementary and alternative treatment options for back pain also involve the use of functional fitness therapy, however, additional evidence-based research studies on the effectiveness of physical activity and exercise are still needed.
On a personal note, chiropractic care utilizes spinal adjustments and manual manipulations to carefully correct misalignments on the spine, or spinal subluxations. Along with chiropractic treatment, a doctor of chiropractor may also recommend a series of stretches and exercises to help increase flexibility, strength and mobility, improving the overall function of the spine. Physical activity for low back pain has been evaluated in the randomized controlled trial below.
Abstract
Objective
To evaluate effectiveness of an exercise programme in a community setting for patients with low back pain to encourage a return to normal activities.
Design
Randomised controlled trial of progressive exercise programme compared with usual primary care management. Patients� preferences for type of management were elicited independently of randomisation.
Participants
187 patients aged 18-60 years with mechanical low back pain of 4 weeks to 6 months� duration.
Interventions
Exercise classes led by a physiotherapist that included strengthening exercises for all main muscle groups, stretching exercises, relaxation session, and brief education on back care. A cognitive-behavioural approach was used.
Main Outcome Measures
Assessments of debilitating effects of back pain before and after intervention and at 6 months and 1 year later. Measures included Roland disability questionnaire, Aberdeen back pain scale, pain diaries, and use of healthcare services.
Results
At 6 weeks after randomisation, the intervention group improved marginally more than the control group on the disability questionnaire and reported less distressing pain. At 6 months and 1 year, the intervention group showed significantly greater improvement in the disability questionnaire score (mean difference in changes 1.35, 95% confidence interval 0.13 to 2.57). At 1 year, the intervention group also showed significantly greater improvement in the Aberdeen back pain scale (4.44, 1.01 to 7.87) and reported only 378 days off work compared with 607 in the control group. The intervention group used fewer healthcare resources. Outcome was not influenced by patients� preferences.
Conclusions
The exercise class was more clinically effective than traditional general practitioner management, regardless of patient preference, and was cost effective.
Key Messages
Patients with back pain need to return to normal activities as soon as possible but are often afraid that movement or activity may be harmful
An exercise programme led by a physiotherapist in the community and based on cognitive-behavioural principles helped patients to cope better with their pain and function better even one year later
Patients� preferences for type of management did not affect outcome
Patients in the intervention group tended to use fewer healthcare resources and took fewer days off work
This type of exercise programme should be more widely available
Introduction
Low back pain is common and, although it may settle quickly, recurrence rates are about 50% in the following 12 months. Recent management guidelines recommend that an early return to physical activities should be encouraged, but patients are often afraid of movement after an acute onset of back pain. Trials of specific exercise programmes for acute back pain have not shown them to be effective, but a specific exercise programme may have to be tailored to suit the individual patient and so is less likely to be effective for a heterogeneous group of patients.
However, there is some evidence that a general exercise programme, which aims to increase individuals� confidence in the use of their spine and overcome the fear of physical activity, can be effective for patients with chronic back pain (of more than six months� duration). A recent randomised trial of a supervised exercise programme in a hospital setting reported significantly better outcomes at six months and two years for the exercise group compared with the control group. Whether this approach would be effective and cost effective for patients with low back pain of less than six months� duration in a primary care setting is unknown.
An important methodological problem occurs when it is not possible to blind subjects to the treatment they receive, since outcome is probably directly influenced by their preconceived ideas regarding the effectiveness of intervention. Thus, in trials where a double blind procedure is not feasible, participants who are not randomised to their treatment of choice may be disappointed and suffer from resentful demoralisation, whereas those randomised to their preferred treatment may have a better outcome irrespective of the physiological efficacy of the intervention. However, this problem may be partly ameliorated if patients� treatment preferences are elicited before randomisation, so that they can be used to inform the analysis of costs and outcomes.
In this paper, we report a fully randomised trial for the treatment of subacute low back pain in which the analysis was informed by patient preference.
Subjects and Methods
Recruitment of Subjects
Eighty seven general practitioners agreed to participate in the study, and the principal investigator (JKM) visited each practice to discuss participation. Selection of general practitioners was based in the York area and restricted by the need to provide easy access for patients to the classes. Only one invited practice declined to participate. Single handed practices were not invited. The general practitioners referred patients directly to the research team or sent a monthly list of patients who had consulted with back pain. Inclusion criteria were patients with mechanical low back pain of at least four weeks� duration but less than six months, aged between 18 and 60, declared medically fit by their general practitioner to undertake the exercise, and who had consulted one of the general practitioners participating in the study. Patients with any potentially serious pathology were excluded, as were any who would have been unable to attend or participate in the classes. The exclusion criteria were the same as described by Frost et al except that concurrent physiotherapy rather than previous physiotherapy was an exclusion criterion in this trial.
Evaluation
Patients who seemed eligible were contacted by telephone and if they were interested in participating in the study were invited to an initial interview, at which the study and its implications for participants were explained. Patients who met all the eligibility criteria and consented to participate attended a first assessment a week later.
This included a physical examination (to exclude possible serious spinal pathology) and collection of baseline data by means of validated measures of health status. The main outcome measures were the Roland back pain disability questionnaire, which measures functional limitations due to back pain, and the Aberdeen back pain scale, which is more a measure of clinical status. The Roland disability questionnaire consists of a 24 point scale: a patient scoring three points on the scale means that he or she reports, for example, �Because of my back I am not doing any of the jobs that I usually do around the house, I use a handrail to get upstairs, and I lie down to rest more often.� We also administered the EuroQoL health index (EQ-5D) and the fear and avoidance beliefs questionnaire (FABQ).
The second assessment was carried out at the patients� general practice six weeks after randomisation to treatment. The brief physical examination was repeated, and the patients were asked to complete the same outcome questionnaires.
In addition, patients were asked to complete pain diaries in the week before their first assessment and in the week before their second assessment. The diaries were used to assess subjective pain reports and asked �How strong is the pain?� and �How distressing is the pain?�
We also evaluated patients at six and 12 months� follow up by sending them outcome questionnaires to complete and return.
Randomisation and Treatments
A pre-prepared randomisation list was generated from a random numbers table and participants were stratified by practice in blocks of six. The trial coordinator ensured concealment of allocation from the clinical researchers by providing the research physiotherapist with a sealed envelope for a named patient before baseline assessment. A note inside the envelope invited the participant either to attend exercise classes or to continue with the current advice or treatment offered by his or her general practitioner. (One of the referring general practitioners used manipulation as usual treatment on most of his patients so that up to 37 patients in each arm of the study could also have received manipulation.) Each patient had an equal chance of being allocated to the intervention or the control group. Before patients were given their envelope they were asked whether they had any preference for the treatment assignment. The participants opened the envelope after leaving the surgery.
Intervention group�The exercise programme consisted of eight sessions, each lasting an hour, spread out over four weeks, with up to 10 participants in each class. The programme was similar to the Oxford fitness programme and included stretching exercises, low impact aerobic exercises, and strengthening exercises aimed at all the main muscle groups. The overall aim was to encourage normal movement of the spine. No special equipment was needed. Participants were discouraged from viewing themselves as invalids and from following the precept of �Let pain be your guide.� They were encouraged to improve their individual record and were selectively rewarded with attention and praise. Although partly based on a traditional physiotherapy approach, the programme used cognitive-behavioural principles. One simple educational message encouraging self reliance was delivered at each class. Participants were told that they should regard the classes as a stepping stone to increasing their own levels of activity.
Controls�Patients allocated to the control group continued under the care of their doctor and in some cases were referred to physiotherapy as usual. No attempt was made to regulate the treatment they received, but it was recorded.
Economic Analysis
We recorded patients� use of healthcare services using a combination of retrospective questionnaires and prospective diary cards, which they returned at 6 and 12 months� follow up. From this information we estimated the cost of each patient�s treatment. We compared the mean costs of treatment for the two groups by using Student�s t tests and standard confidence intervals. However, as cost data were highly positively skewed, these results were checked with a non-parametric �bootstrap.� The economic evaluation addressed both costs to the NHS and the costs to society. Participants were not charged for the classes, in line with any treatment currently available on the NHS.
Statistical Analysis
Our original intention was to recruit 300 patients, which, given a standard deviation of 4, would have provided 90% power at the 5% significance level to detect a 1.5 point difference between the two groups in the mean change on the Roland disability questionnaire. However, recruitment of patients to the study proved much slower than expected, and, because of the limitations of study resources, recruiting was stopped after 187 patients had been included into the study. This smaller sample reduced the power to detect such a difference to 72%, but there was still 90% power to detect a 2 point difference in outcome.
Our analysis was based on intention to treat. We estimated the effects of treatment on the outcome measures by means of analysis of covariance, with the change in scores as the dependent variable and adjustment being made for baseline score and patient preference. We used Student�s t tests to analyse the data from the pain diaries as the baseline scores were quite similar.
Dr. Alex Jimenez’s Insight
In consideration with the research study regarding a randomized controlled trial coordinated to determine the effectiveness of functional fitness towards the improvement of low back pain, we supplement our philosophies of overall health and wellness to our patients and we make sure to take their recovery and rehabilitation to the next level. Our fitness and chiropractic care treatment goes beyond many other medically advanced methods. The proprietary treatment methods offered at our clinic promote true well-being and fitness practices with a primary goal on the calibration of the human body. The outcome measures of the randomized controlled trial on exercise for low back pain involved two groups of participants, an intervention group and a control group. The results are recorded below.
Results
Study Population
Of the 187 patients included in the trial, 89 were randomised to the intervention and 98 to the control group. The figure shows their progress through the trial. In both groups those with the most severe back pain at randomisation were less likely to return follow up questionnaires: the mean Roland disability questionnaire score for responders at one year follow up was 5.80 (SD 3.48) compared with a mean score of 9.06 (4.58) for non responders respectively (P=0.002).
Baseline Characteristics
The clinical and demographic characteristics of the patients in the two groups were fairly well balanced at randomisation (Table 1), although those allocated to the intervention group tended to report more disability on the Roland disability questionnaire than did the control group. Most patients (118, 63%), when asked, would have preferred to be allocated to the exercise programme. Attendance of the classes was considered quite good, with 73% of the intervention group attending between six and eight of the classes. Four people failed to attend any classes and were included in the intention to treat analysis. No patients allocated to the control group took part in the exercise programme.
Table 1: Baseline characteristics of patients with mechanical low back pain included in study. Values are means (standard deviations) unless stated otherwise.
Clinical Outcomes
Table ?2 shows the mean changes in outcome measures over time, from randomisation to final follow up at one year. After adjustment for baseline scores, the intervention group showed greater decreases in all measures of back pain and disability compared with the controls. At six weeks after randomisation, patients in the intervention group reported less distressing pain than the control group (P=0.03) and a marginally significant difference on the Roland disability questionnaire scores. Other variables were not significantly different, but the differences in change were all in favour of the intervention group. At six months the difference of the mean change scores of the Roland disability questionnaire was significant, and at one year the differences in changes of both the Roland disability questionnaire and the Aberdeen back pain scale were significant (Table ?2). Most of the intervention group improved by at least three points on the Roland disability questionnaire: 53% (95% confidence interval 42% to 64%) had done so at six weeks, 60% (49% to 71%) at six months, and 64% (54% to 74%) at one year. A smaller proportion of the control group achieved this clinically important improvement: 31% (22% to 40%) at six weeks, 40% (29% to 50%) at six months, and 35% (25% to 45%) at one year.
Table 2: Changes in back pain scores from baseline values in intervention and control groups at 6 weeks, 6 months, and 1 year follow up.
Patients� Preference
We examined the effect of patients� baseline preference for treatment on outcome after adjusting for baseline scores and main effects. Preference did not significantly affect response to treatment. The intervention had similar effects on both costs and outcomes regardless of baseline preference. For example, the change in the Roland disability questionnaire score at 12 months in the control group was ?1.93 for patients who preferred intervention and ?1.18 for those who were indifferent (95% confidence interval of difference ?1.05 to 2.55), and in the intervention group the change in score was ?3.10 for those who preferred intervention and ?3.15 for those who were indifferent ((95% confidence interval of difference ?1.47 to 3.08). As the interaction term (preference by random allocation) was non-significant, the results shown in Table ?2 exclude the preference term.
Economic Evaluation
Patients in the intervention group tended to use fewer healthcare and other resources compared with those in the control group (Table ?3). However, the mean difference, totalling �148 per patient, was not significant: the 95% confidence interval suggests there could have been a saving of as much as �442 per patient in the intervention group or an additional cost of up to �146. Patients in the control group took a total of 607 days off work during the 12 months after randomisation compared with 378 days taken off by the intervention group.
Table 3: Use of services and their costs associated with back pain in the two study groups at 12 months follow up.
Discussion
Our results support the hypothesis that a simple exercise class can lead to long term improvements for back pain sufferers. Studies have shown that a similar programme for patients with chronic back pain can be effective in the hospital setting. In this study we show the clinical effectiveness for patients with subacute or recurrent low back pain who were referred by their general practitioner to a community programme.
Current management guidelines for low back pain recommend a return to physical activity and taking exercise. In particular, they recommend that patients who are not improving at six weeks after onset of back pain, which may be a higher proportion than previously realised, should be referred to a reactivation programme. The programme we evaluated fits that requirement well. It shows participants how they can safely start moving again and increase their levels of physical activity. It is simple and less costly than individual treatment.
It seemed to have beneficial effects even one year later, as measured by functional disability (Roland disability questionnaire) and clinical status (Aberdeen back pain scale). The mean changes in scores on these instruments were small, with many patients reporting mild symptoms on the day of entry to the trial. However, a substantially larger proportion of participants in the exercise classes gained increases of over three points on the Roland disability questionnaire at six weeks, six months, and one year, which might be clinically important. At six weeks, participants in the exercise classes reported significantly less distressing pain compared with the control group, although the intensity of pain was not significantly different. This is consistent with findings from a study of chronic back pain patients in Oxford, in which changes in distressing pain were much greater than were the changes in intensity of pain.
People with back pain who use coping strategies that do not avoid movement and pain have less disability. In our study the participants in the exercise classes were able to function better according to Roland disability questionnaire scores than the control group at six months and one year after randomisation to treatment, and at one year they also showed a significantly greater improvement in clinical status as measured by the Aberdeen back pain scale. This increase in differences in effect between the intervention and control groups over time is consistent with the results from long term follow up in comparable back pain trials.
Study Design
The design of this study was a conventional randomised controlled trial in that all eligible patients were randomised. However, the participants were asked to state their preferred treatment before they knew of their allocation. A study of antenatal services showed that preferences can be an important determinant of outcome, but we did not find any strong effect of preference on the outcome, although a much larger sample size would be needed to confidently exclude any modest interaction between preference and outcome. This information may be useful to clinicians in that it suggests that exercise classes are effective even in patients who are not highly motivated. Our trial design, of asking patients for their preferences at the outset, has substantial advantages over the usual patient preference design, in which costs and outcomes cannot be reliably controlled for confounding by preference.
Conclusions
Our exercise programme did not seem to influence the intensity of pain but did affect the participants� ability to cope with the pain in the short term and even more so in the longer term. It used a cognitive-behavioural model, shifting the emphasis away from a disease model to a model of normal human behaviour, and with minimal extra training a physiotherapist can run it. Patients� preferences did not seem to influence the outcome.
Figure 1: Flow chart describing patients’ progress through the trial.
Footnotes
Funding: This research was funded by the Arthritis Research Campaign, the Northern and Yorkshire Regional Health Authority, and the National Back Pain Association.
Competing interests: None declared.
In conclusion,�the participation of patients in functional fitness and/or exercise as recommended by a physiotherapist, or physical therapist, or any other healthcare professional, such as a chiropractor, is essential towards the improvement of their symptoms of low back pain. The exercise programme helped patients better cope with their symptoms of back pain where the intervention group showed that they used fewer healthcare resources and took fewer day off work, according to the outcome measures of the research study. Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Sciatica
Sciatica is referred to as a collection of symptoms rather than a single type of injury or condition. The symptoms are characterized as radiating pain, numbness and tingling sensations from the sciatic nerve in the lower back, down the buttocks and thighs and through one or both legs and into the feet. Sciatica is commonly the result of irritation, inflammation or compression of the largest nerve in the human body, generally due to a herniated disc or bone spur.
3.�Waddell G, Feder G, McIntosh A, Lewis M, Hutchinson A.�Low back pain evidence review.�London: Royal College of General Practitioners; 1996.
4.�Malmivaara A, Hakkinen U, Aro T, Heinrichs M, Koskenniemi L, Kuosma E, et al. The treatment of acute low back pain�bed rest, exercises or ordinary activity?�N Engl J Med.�1995;332:351�355.[PubMed]
5.�Faas A, Chavannes A, van Eijk JTM, Gubbels J. A randomized, placebo-controlled trial of exercise therapy in patients with acute low back pain.�Spine.�1993;18:1388�1395.�[PubMed]
6.�Frost H, Klaber Moffett J, Moser J, Fairbank J. Evaluation of a fitness programme for patients with chronic low back pain.�BMJ.�1995;310:151�154.�[PMC free article]�[PubMed]
7.�Frost H, Lamb S, Klaber Moffett J, Fairbank J, Moser J. A fitness programme for patients with chronic low back pain: 2 year follow-up of a randomised controlled trial.�Pain.�1998;75:273�279.�[PubMed]
8.�McPherson K, Britton A, Wennberg J. Are randomised controlled trials controlled? Patient preferences and unblind trials.�J R Soc Med.�1997;90:652�656.�[PMC free article]�[PubMed]
9.�Bradley C. Designing medical and educational studies.�Diabetes Care.�1993;16:509�518.�[PubMed]
10.�Clement S, Sikorski J, Wilson J, Candy B. Merits of alternative strategies for incorporating patient preferences into clinical trials must be considered carefully [letter]�BMJ.�1998;317:78.�[PubMed]
11.�Torgerson D, Klaber Moffett J, Russell I. Patient preferences in randomised trials: threat or opportunity?�J Health Serv Res Policy.�1996;1(4):194�197.�[PubMed]
12.�Roland M, Morris R. A study of the natural causes of back pain. Part 1: Development of a reliable and sensitive measure of disability in low-back pain.�Spine.�1983;8:141�144.�[PubMed]
13.�Ruta D, Garratt A, Wardlaw D, Russell I. Developing a valid and reliable measure of health outcome for patients with low back pain.�Spine.�1994;19:1887�1896.�[PubMed]
14.�Brooks R.with EuroQoL Group.�EuroQoL: the current state of play�Health Policy�19963753�72.[PubMed]
15.�Waddell G, Newton M, Henderson I, Somerville D, Main C. A fear-avoidance beliefs questionnaire (FABQ) and the role of fear-avoidance beliefs in chronic low back pain and disability.�Pain.�1993;52:157�168.�[PubMed]
16.�Jensen M, McFarland C. Increasing the reliability and validity of pain intensity measurement in chronic pain patients.�Pain.�1993;55:195�203.�[PubMed]
17.�Efron B, Tibshirani R.�An introduction to bootstrap.�New York: Chapman and Hall; 1993.
18.�Williams D, Keefe F. Pain beliefs and use of cognitive-behavioral coping strategies.�Pain.�1991;46:185�190.�[PubMed]
19.�Estlander A, Harkapaa K. Relationships between coping strategies, disability and pain levels in patients with chronic low back pain.�Scand J Behav Ther.�1989;18:56�69.
20.�Holmes J, Stevenson C. Differential effects of avoidant and attentional coping strategies on adaption to chronic and recent-onset pain.�Health Psychology.�1990;9:577�584.�[PubMed]
21.�Rosenstiel A, Keefe F. The use of coping strategies in chronic low back pain patients: relationship to patient characteristics and current adjustments.�Pain.�1983;17:33�44.�[PubMed]
22.�Slade P, Troup J, Lethem J, Bentley G. The fear avoidance model of exaggerated pain perception II Preliminary studies of coping strategies for pain.�Behav Res Ther.�1983;21:409�416.�[PubMed]
23.�Meade T, Dyer S, Browne W, Frank A. Randomised comparison of chiropractic and hospital outpatient management for low back pain: results from extended follow up.�BMJ.�1995;311:349�351.[PMC free article]�[PubMed]
24.�Cherkin D, Deyo R, Battie M, Street J, Barlow W. A comparison of physical therapy, chiropractic manipulation, and provision of an educational booklet for the treatment of patients with low back pain.�N Engl J Med.�1998;339:1021�1029.�[PubMed]
Attributed from a personal perspective, as a practicing chiropractor with experience on a variety of spinal injuries and conditions, back pain is one of the most common health issues reported among the general population, affecting about 8 out of 10 individuals at some point throughout their lives. While many different types of treatments are currently available to help improve the symptoms of back pain, health care based on clinical and experimental evidence has caused an impact on the type of treatment individuals will receive for their back pain. Many patients in health care are turning to non-invasive treatment modalities for their back pain as a result of growing evidence associated with its safety and effectiveness.
On a further note, non-invasive treatment modalities are defined as conservative procedures which do not require incision into the body, where no break in the skin is created and there is no contact with the mucosa or internal body cavity beyond a natural or artificial body orifice, or the removal of tissue. The clinical and experimental methods and results of a variety of non-invasive treatment modalities on back pain have been described and discussed in detail below.
Abstract
At present, there is an increasing international trend towards evidence-based health care. The field of low back pain (LBP) research in primary care is an excellent example of evidence-based health care because there is a huge body of evidence from randomized trials. These trials have been summarized in a large number of systematic reviews. This paper summarizes the best available evidence from systematic reviews conducted within the framework of the Cochrane Back Review Group on non-invasive treatments for non-specific LBP. Data were gathered from the latest Cochrane Database of Systematic Reviews 2005, Issue 2. The Cochrane reviews were updated with additional trials, if available. Traditional NSAIDs, muscle relaxants, and advice to stay active are effective for short-term pain relief in acute LBP. Advice to stay active is also effective for long-term improvement of function in acute LBP. In chronic LBP, various interventions are effective for short-term pain relief, i.e. antidepressants, COX2 inhibitors, back schools, progressive relaxation, cognitive�respondent treatment, exercise therapy, and intensive multidisciplinary treatment. Several treatments are also effective for short-term improvement of function in chronic LBP, namely COX2 inhibitors, back schools, progressive relaxation, exercise therapy, and multidisciplinary treatment. There is no evidence that any of these interventions provides long-term effects on pain and function. Also, many trials showed methodological weaknesses, effects are compared to placebo, no treatment or waiting list controls, and effect sizes are small. Future trials should meet current quality standards and have adequate sample size.
Keywords: Non-specific low back pain, Non-invasive treatment, Primary care, Effectiveness, Evidence review
Introduction
Low back pain is most commonly treated in primary health care settings. Clinical management of acute as well as chronic low back pain (LBP) varies substantially among health care providers. Also, many different primary health care professionals are involved in the management of LBP, such as general practitioners, physical therapists, chiropractors, osteopaths, manual therapists, and others. There is a need to increase consistency in the management of LBP across professions.
At present, there is an increasing international trend towards evidence-based health care. Within the framework of evidence-based health care, clinicians should conscientiously, explicitly, and judiciously use the best current evidence in making decisions about the care of individual patients. The field of LBP research in primary care is an excellent example of evidence-based health care because there is a huge body of evidence. At present, more than 500 randomized controlled trials (RCTs) have been published, evaluating all types of conservative and alternative treatments for LBP that are commonly used in primary care. These trials have been summarized in a large number of systematic reviews. The Cochrane Back Review Group (CBRG) offers a framework for conducting and publishing systematic reviews in the fields of back and neck pain. However, method guidelines have also been developed and published by the CBRG to improve the quality of reviews in this field and to facilitate comparison across reviews and enhance consistency among reviewers. This paper summarizes the best available evidence from systematic reviews conducted within the framework of the CBRG on non-invasive treatments for non-specific LBP.
Objectives
To determine the effectiveness of non-invasive (pharmaceutical and non-pharmaceutical) interventions compared to placebo (or sham treatment, no intervention and waiting list control) or other interventions for acute, subacute, and chronic non-specific LBP. Trials comparing various types of the same interventions (e.g. various types of NSAIDs or various types of exercises) were excluded. The evidence on complementary and alternative medicine interventions (acupuncture, botanical medicines, massage, and neuroreflexotherapy) has been published elsewhere. Evidence on surgical and other invasive interventions for LBP will be presented in another paper in the same issue of the European Spine Journal.
Methods
The results of systematic reviews conducted within the framework of the CBRG were used. Most of these reviews were published, but preliminary results from one Cochrane review on patient education (A. Engers et al., submitted for publication) that has been submitted for publication were also used. Because no Cochrane review was available, we used two recently published systematic reviews for the evidence summary on antidepressants. The Cochrane review on work conditioning, work hardening, and functional restoration was not taken into account because all trials included in this review were also included in the reviews on exercise therapy and multidisciplinary treatment. The Cochrane reviews were updated with additional trials, if available, using Clinical Evidence as source (www.clinicalevidence.com). This manuscript consists of two parts: one on evidence of pharmaceutical interventions and the other on evidence of non-pharmaceutical interventions for non-specific LBP.
Search Strategy and Study Selection
The following search strategy was used in the Cochrane reviews:
A computer aided search of the Medline and Embase databases since their beginning.
A search of the Cochrane Central Register of Controlled Trials (Central).
Screening references given in relevant systematic reviews and identified trials.
Personal communication with content experts in the field.
Two reviewers independently applied the inclusion criteria to select the potentially relevant trials from the titles, abstracts, and keywords of the references retrieved by the literature search. Articles for which disagreement existed, and articles for which title, abstract, and keywords provided insufficient information for a decision on selection were obtained to assess whether they met the inclusion criteria. A consensus method was used to resolve disagreements between the two reviewers regarding the inclusion of studies. A third reviewer was consulted if disagreements were not resolved in the consensus meeting.
Inclusion Criteria
Study design. RCTs were included in all reviews.
Participants. Participants of trials that were included in the systematic reviews usually had acute (less than 6 weeks), subacute (6�12 weeks), and/or chronic (12 weeks or more) LBP. All reviews included patients with non-specific LBP.
Interventions. All reviews included one specific intervention. Typically any comparison group was allowed, but comparisons with no treatment/placebo/waiting list controls and other interventions were separately presented.
Outcomes. The outcome measures included in the systematic reviews were outcomes of symptoms (e.g. pain), overall improvement or satisfaction with treatment, function (e.g. back-specific functional status), well-being (e.g. quality of life), disability (e.g. activities of daily living, work absenteeism), and side effects. Results were separately presented for short-term and long-term follow-up.
Methodological Quality Assessment
In most reviews, the methodological quality of trials included in the reviews was assessed using the criteria recommended by the CBRG. The studies were not blinded for authors, institutions, or the journals in which the studies were published. The criteria were: (1) adequate allocation concealment, (2) adequate method of randomization, (3) similarity of baseline characteristics, (4) blinding of patients, (5) blinding of care provider, (6) equal co-interventions, (7) adequate compliance, (8) identical timing of outcome assessment, (9) blinded outcome assessment, (10) withdrawals and drop outs adequate, and (11) intention-to-treat analysis. All items were scored as positive, negative, or unclear. High quality was typically defined as fulfilling 6 or more of the 11 quality criteria. We refer readers to the original Cochrane reviews for details of the quality of trials.
Data Extraction
The data that were extracted and presented in tables included characteristics of participants, interventions, outcomes, and results. We refer readers to the original Cochrane reviews for summaries of trial data.
Data Analysis
Some reviews conducted a meta-analysis using statistical methods to analyse and summarize the data. If relevant valid data were lacking (data were too sparse or of inadequate quality) or if data were statistically too heterogeneous (and the heterogeneity could not be explained), statistical pooling was avoided. In these cases, reviewers performed a qualitative analysis. In the qualitative analyses, various levels of evidence were used that took into account the participants, interventions, outcomes, and methodological quality of the original studies. If only a subset of available trials provided sufficient data for inclusion in a meta-analysis (e.g. only some trials reported standard deviations), both a quantitative and qualitative analysis was used.
Dr. Alex Jimenez’s Insight
The purpose of the following research study was to determine which of the various non-invasive treatment modalities used could be safe and most effective towards the prevention, diagnosis and treatment of acute, subacute and chronic non-specific low back pain, as well as general back pain. All of the systematic reviews included participants with some type of non-specific low back pain, or LBP, where each received health care for one specific intervention. The outcome measures included in the systematic reviews were based on symptoms, overall improvement or satisfaction with treatment, function, well-being, disability and side effects. The data of the results was extracted and presented in Tables 1 and 2. The researchers of the study performed a qualitative analysis of all the presented clinical and experimental data before demonstrating it in this article. As a healthcare professional, or patient with back pain, the information in this research study may help determine which non-invasive treatment modality should be considered to achieve the desired recovery outcome measures.
Results
Pharmaceutical Interventions
Antidepressants
There are three reasons for using antidepressants in the treatment of LBP. The first reason is that chronic LBP patients often also cope with depression, and treatment with antidepressants may elevate mood and increase pain tolerance. Second, many antidepressant drugs are sedating, and it has been suggested that part of their value for managing chronic pain syndromes simply could be improving sleep. The third reason for the use of antidepressants in chronic LBP patients is their supposed analgesic action, which occurs at lower doses than the antidepressant effect.
Effectiveness of antidepressants for acute LBP No trials were identified.
Effectiveness of antidepressants for chronic LBP Antidepressants versus placebo. We found two systematic reviews including a total of nine trials. One review found that antidepressants significantly increased pain relief compared with placebo but found no significant difference in functioning [pain: standardized mean difference (SMD) 0.41, 95% CI 0.22�0.61; function: SMD 0.24, 95% CI -0.21 to +0.69]. The other review did not statistically pool data but had similar results.
Adverse effects Adverse effects of antidepressants include dry mouth, drowsiness, constipation, urinary retention, orthostatic hypotension, and mania. One RCT found that the prevalence of dry mouth, insomnia, sedation, and orthostatic symptoms was 60�80% with tricyclic antidepressants. However, rates were only slightly lower in the placebo group and none of the differences were significant. In many trials, the reporting of side effects was insufficient.
Muscle Relaxants
The term �muscle relaxants� is very broad and includes a wide range of drugs with different indications and mechanisms of action. Muscle relaxants can be divided into two main categories: antispasmodic and antispasticity medications.
Antispasmodics are used to decrease muscle spasm associated with painful conditions such as LBP. Antispasmodics can be subclassified into benzodiazepines and non-benzodiazepines. Benzodiazepines (e.g. diazepam, tetrazepam) are used as anxiolytics, sedatives, hypnotics, anticonvulsants, and/or skeletal muscle relaxants. Non-benzodiazepines include a variety of drugs that can act at the brain stem or spinal cord level. The mechanisms of action with the central nervous system are still not completely understood.
Antispasticity medications are used to reduce spasticity that interferes with therapy or function, such as in cerebral palsy, multiple sclerosis, and spinal cord injuries. The mechanism of action of the antispasticity drugs with the peripheral nervous system (e.g. dantrolene sodium) is the blockade of the sarcoplasmic reticulum calcium channel. This reduces calcium concentration and diminishes actin�myosin interaction.
Effectiveness of muscle relaxants for acute LBP Benzodiazepines versus placebo. One study showed that there is limited evidence (one trial; 50 people) that an intramuscular injection of diazepam followed by oral diazepam for 5 days is more effective than placebo for patients with acute LBP on short-term pain relief and better overall improvement, but is associated with substantially more central nervous system side effects.
Non-benzodiazepines versus placebo. Eight studies were identified. One high quality study on acute LBP showed that there is moderate evidence (one trial; 80 people) that a single intravenous injection of 60 mg orphenadrine is more effective than placebo in immediate relief of pain and muscle spasm for patients with acute LBP.
Three high quality and one low quality trial showed that there is strong evidence (four trials; 294 people) that oral non-benzodiazepines are more effective than placebo for patients with acute LBP on short-term pain relief, global efficacy, and improvement of physical outcomes. The pooled RR and 95% CIs for pain intensity was 0.80 (0.71�0.89) after 2�4 days (four trials; 294 people) and 0.58 (0.45�0.76) after 5�7 days follow-up (three trials; 244 people). The pooled RR and 95% CIs for global efficacy was 0.49 (0.25�0.95) after 2�4 days (four trials; 222 people) and 0.68 (0.41�1.13) after 5�7 days follow-up (four trials; 323 people).
Antispasticity drugs versus placebo. Two high quality trials showed that there is strong evidence (two trials; 220 people) that antispasticity muscle relaxants are more effective than placebo for patients with acute LBP on short-term pain relief and reduction of muscle spasm after 4 days. One high quality trial also showed moderate evidence on short-term pain relief, reduction of muscle spasm, and overall improvement after 10 days.
Effectiveness of muscle relaxants for chronic LBP Benzodiazepines versus placebo. Three studies were identified. Two high quality trials on chronic LBP showed that there is strong evidence (two trials; 222 people) that tetrazepam 50 mg t.i.d. is more effective than placebo for patients with chronic LBP on short-term pain relief and overall improvement. The pooled RRs and 95% CIs for pain intensity were 0.82 (0.72�0.94) after 5�7 days follow-up and 0.71 (0.54�0.93) after 10�14 days. The pooled RR and 95% CI for overall improvement was 0.63 (0.42�0.97) after 10�14 days follow-up. One high quality trial showed that there is moderate evidence (one trial; 50 people) that tetrazepam is more effective than placebo on short-term decrease of muscle spasm.
Non-benzodiazepines versus placebo. Three studies were identified. One high quality trial showed that there is moderate evidence (one trial; 107 people) that flupirtin is more effective than placebo for patients with chronic LBP on short-term pain relief and overall improvement after 7 days, but not on reduction of muscle spasm. One high quality trial showed that there is moderate evidence (one trial; 112 people) that tolperisone is more effective than placebo for patients with chronic LBP on short-term overall improvement after 21 days, but not on pain relief and reduction of muscle spasm.
Adverse effects Strong evidence from all eight trials on acute LBP (724 people) showed that muscle relaxants are associated with more total adverse effects and central nervous system adverse effects than placebo, but not with more gastrointestinal adverse effects; RRs and 95% CIs were 1.50 (1.14�1.98), 2.04 (1.23�3.37), and 0.95 (0.29�3.19), respectively. The most commonly and consistently reported adverse events involving the central nervous system were drowsiness and dizziness. For the gastrointestinal tract this was nausea. The incidence of other adverse events associated with muscle relaxants was negligible.
NSAIDs
The rationale for the treatment of LBP with NSAIDs is based both on their analgesic potential and their anti-inflammatory action.
Effectiveness of NSAIDs for acute LBP NSAIDs versus placebo. Nine studies were identified. Two studies reported on LBP without radiation, two on sciatica, and the other five on a mixed population. There was conflicting evidence that NSAIDs provide better pain relief than placebo in acute LBP. Six of the nine studies which compared NSAIDs with placebo for acute LBP reported dichotomous data on global improvement. The pooled RR for global improvement after 1 week using the fixed effects model was 1.24 (95% CI 1.10�1.41), indicating a statistically significant effect in favour of NSAIDs compared to placebo. The pooled RR (three trials) for analgesic use using the fixed effects model was 1.29 (95% CI 1.05�1.57), indicating significantly less use of analgesics in the NSAIDs group.
NSAIDs versus paracetamol/acetaminophen. There were no differences between NSAIDs and paracetamol reported in two studies, but one study reported better outcomes for two of the four types of NSAIDs. There is conflicting evidence that NSAIDs are more effective than paracetamol for acute LBP.
NSAIDs versus other drugs. Six studies reported on acute LBP, of which five did not find any differences between NSAIDs and narcotic analgesics or muscle relaxants. Group sizes in these studies ranged from 19 to 44 and, therefore, these studies simply may have lacked power to detect a statistically significant difference. There is moderate evidence that NSAIDs are not more effective than other drugs for acute LBP.
Effectiveness of NSAIDs for chronic LBP NSAIDs versus placebo. One small cross-over study (n=37) found that naproxen sodium 275 mg capsules (two capsules b.i.d.) decreased pain more than placebo at 14 days.
COX2 inhibitors versus placebo. Four additional trials were identified. There is strong evidence that COX2 inhibitors (etoricoxib, rofecoxib and valdecoxib) decreased pain and improved function compared with placebo at 4 and 12 weeks, but effects were small.
Adverse effects NSAIDs may cause gastrointestinal complications. Seven of the nine studies which compared NSAIDs with placebo for acute LBP reported data on side effects. The pooled RR for side effects using the fixed effects model was 0.83 (95% CI 0.64�1.08), indicating no statistically significant difference. One systematic review of the harms of NSAIDs found that ibuprofen and diclofenac had the lowest gastrointestinal complication rate, mainly because of the low doses used in practice (pooled OR for adverse effects vs. placebo 1.30, 95% CI 0.91�1.80). COX2 inhibitors have been shown to have less gastrointestinal side effects in osteoarthritis and rheumatoid arthritis studies. However, increased cardiovascular risk (myocardial infarction and stroke) has been reported with long-term use.
Non-Pharmaceutical Interventions
Advice to Stay Active
Effectiveness of advice to stay active for acute LBP Stay active versus bed rest. The Cochrane review found four studies that compared advice to stay active as single treatment with bed rest. One high quality study showed that advice to stay active significantly improved functional status and reduced sick leave after 3 weeks compared with advice to rest in bed for 2 days. It also found a significant reduction of pain intensity in favour of the stay active group at intermediate follow-up (more than 3 weeks). The low quality studies showed conflicting results. The additional trial (278 people) found no significant differences in pain intensity and functional disability between advice to stay active and bed rest after 1 month. However, it found that advice to stay active significantly reduced sick leave compared with bed rest up to day 5 (52% with advice to stay active vs. 86% with bed rest; P<0.0001).
Stay active versus exercise. One trial found short-term improvement in functional status and reduction in sick leave in favour of advice to stay active. A significant reduction in sick leave in favour of the stay active group was also reported at long-term follow-up.
Effectiveness of advice to stay active for chronic LBP No trials identified.
Adverse effects No trials reported side effects.
Back Schools
The original �Swedish back school� was introduced by Zachrisson Forsell in 1969. It was intended to reduce the pain and prevent recurrences. The Swedish back school consisted of information on the anatomy of the back, biomechanics, optimal posture, ergonomics, and back exercises. Four small group sessions were scheduled during a 2-week period, with each session lasting 45 min. The content and length of back schools has changed and appears to vary widely today.
Effectiveness of back schools for acute LBP Back schools versus waiting list controls or �placebo� interventions. Only one trial compared back school with placebo (shortwaves at the lowest intensity) and showed better short-term recovery and return to work for the back school group. No other short- or long-term differences were found.
Back schools versus other interventions. Four studies (1,418 patients) showed conflicting evidence on the effectiveness of back schools compared to other treatments for acute and subacute LBP on pain, functional status, recovery, recurrences, and return to work (short-, intermediate-, and long-term follow-up).
Effectiveness of back schools for chronic LBP Back schools versus waiting list controls or �placebo� interventions. There is conflicting evidence (eight trials; 826 patients) on the effectiveness of back schools compared to waiting list controls or placebo interventions on pain, functional status, and return to work (short-, intermediate-, and long-term follow-up) for patients with chronic LBP.
Back schools versus other treatments. Six studies were identified comparing back schools with exercises, spinal or joint manipulation, myofascial therapy, and some kind of instructions or advice. There is moderate evidence (five trials; 1,095 patients) that a back school is more effective than other treatments for patients with chronic LBP for pain and functional status (short- and intermediate-term follow-up). There is moderate evidence (three trials; 822 patients) that there is no difference in long-term pain and functional status.
Adverse effects None of the trials reported any adverse effects.
Bed Rest
One rationale for bed rest is that many patients experience relief of symptoms in a horizontal position.
Effectiveness of bed rest for acute LBP Twelve trials were included in the Cochrane review. Some trials were on a mixed population of patients with acute and chronic LBP or on a population of patients with sciatica.
Bed rest versus advice to stay active. Three trials (481 patients) were included in this comparison. The results of two high quality trials showed small but consistent and significant differences in favour of staying active, at 3- to 4-week follow-up [pain: SMD 0.22 (95% CI 0.02�0.41); function: SMD 0.31 (95% CI 0.06�0.55)], and at 12-week follow-up [pain: SMD 0.25 (95% CI 0.05�0.45); function: SMD 0.25 (95% CI 0.02�0.48)]. Both studies also reported significant differences in sick leave in favour of staying active. There is strong evidence that advice to rest in bed is less effective than advice to stay active for reducing pain and improving functional status and speeding-up return to work.
Bed rest versus other interventions. Three trials were included. Two trials compared advice to rest in bed with exercises and found strong evidence that there was no difference in pain, functional status, or sick leave at short- and long-term follow-up. One study found no difference in improvement on a combined pain, disability, and physical examination score between bed rest and manipulation, drug therapy, physiotherapy, back school, or placebo.
Short bed rest versus longer bed rest. One trial in patients with sciatica reported no significant difference in pain intensity between 3 and 7 days of bed rest, measured 2 days after the end of treatment.
Effectiveness of bed rest for chronic LBP There were no trials identified.
Adverse effects No trials reported adverse effects.
Behavioural Treatment
The treatment of chronic LBP not only focuses on removing the underlying organic pathology, but also tries to reduce disability through the modification of environmental contingencies and cognitive processes. In general, three behavioural treatment approaches can be distinguished: operant, cognitive, and respondent. Each of these approaches focus on the modification of one of the three response systems that characterize emotional experiences: behaviour, cognition, and physiological reactivity.
Operant treatments include positive reinforcement of healthy behaviours and consequent withdrawal of attention towards pain behaviours, time-contingent instead of pain-contingent pain management, and spousal involvement. The operant treatment principles can be applied by all health care disciplines involved with the patient.
Cognitive treatment aims to identify and modify patients� cognitions regarding their pain and disability. Cognition (the meaning of pain, expectations regarding control over pain) can be modified directly by cognitive restructuring techniques (such as imagery and attention diversion), or indirectly by the modification of maladaptive thoughts, feelings, and beliefs.
Respondent treatment aims to modify the physiological response system directly, e.g. by reduction of muscular tension. Respondent treatment includes providing the patient with a model of the relationship between tension and pain, and teaching the patient to replace muscular tension by a tension-incompatible reaction, such as the relaxation response. Electromyographic (EMG) biofeedback, progressive relaxation, and applied relaxation are frequently used.
Behavioural techniques are often applied together as part of a comprehensive treatment approach. This so-called cognitive�behavioural treatment is based on a multidimensional model of pain that includes physical, affective, cognitive, and behavioural components. A large variety of behavioural treatment modalities are used for chronic LBP because there is no general consensus about the definition of operant and cognitive methods. Furthermore, behavioural treatment often consists of a combination of these modalities or is applied in combination with other therapies (such as medication or exercises).
Effectiveness of behavioural therapy for acute LBP One RCT (107 people) identified by the review found that cognitive�behavioural therapy reduced pain and perceived disability after 9�12 months compared with traditional care (analgesics plus back exercises until pain had subsided).
Effectiveness of behavioural therapy for chronic LBP Behavioural treatment versus waiting list controls. There is moderate evidence from two small trials (total of 39 people) that progressive relaxation has a large positive effect on pain (1.16; 95% CI 0.47�1.85) and behavioural outcomes (1.31; 95% CI 0.61�2.01) in the short-term. There is limited evidence that progressive relaxation has a positive effect on short-term back-specific and generic functional status.
There is moderate evidence from three small trials (total of 88 people) that there is no significant difference between EMG biofeedback and waiting list control on behavioural outcomes in the short-term. There is conflicting evidence (two trials; 60 people) on the effectiveness of EMG versus waiting list control on general functional status.
There is conflicting evidence from three small trials (total of 153 people) regarding the effect of operant therapy on short-term pain intensity, and moderate evidence that there is no difference [0.35 (95% CI -0.25 to 0.94)] between operant therapy and waiting list control for short-term behavioural outcomes. Five studies compared combined respondent and cognitive therapy with waiting list controls. There is strong evidence from four small trials (total of 134 people) that combined respondent and cognitive therapy has a medium sized, short-term positive effect on pain intensity. There is strong evidence that there are no differences [0.44 (95% CI -0.13 to 1.01)] on short-term behavioural outcomes.
Behavioural treatment versus other interventions. There is limited evidence (one trial; 39 people) that there are no significant differences between behavioural treatment and exercise on pain intensity, generic functional status and behavioural outcomes, either post-treatment, or at 6- or 12-month follow-up.
Adverse effects None reported in the trials.
Exercise Therapy
Exercise therapy is a management strategy that is widely used in LBP; it encompasses a heterogeneous group of interventions ranging from general physical fitness or aerobic exercise, to muscle strengthening, to various types of flexibility and stretching exercises.
Effectiveness of exercise therapy for acute LBP Exercise versus no treatment. The pooled analysis failed to show a difference in short-term pain relief between exercise therapy and no treatment, with an effect of -0.59 points/100 (95% CI -12.69 to 11.51).
Exercise versus other interventions. Of 11 trials involving 1,192 adults with acute LBP, 10 had non-exercise comparisons. These trials provide conflicting evidence. The pooled analysis showed that there was no difference at the earliest follow-up in pain relief when compared to other conservative treatments: 0.31 points (95% CI -0.10 to 0.72). Similarly, there was no significant positive effect of exercise on functional outcomes. Outcomes show similar trends at short-, intermediate-, and long-term follow-up.
Effectiveness of exercise therapy for subacute LBP Exercise versus other interventions. Six studies involving 881 subjects had non-exercise comparisons. Two trials found moderate evidence of reduced work absenteeism with a graded activity intervention compared to usual care. The evidence is conflicting regarding the effectiveness of other exercise therapy types in subacute LBP compared to other treatments.
Effectiveness of exercise therapy for chronic LBP Exercise versus other interventions. Thirty-three exercise groups in 25 trials on chronic LBP had non-exercise comparisons. These trials provide strong evidence that exercise therapy is at least as effective as other conservative interventions for chronic LBP. Two exercise groups in high quality studies and nine groups in low quality studies found exercise more effective than comparison treatments. These studies, mostly conducted in health care settings, commonly used exercise programs that were individually designed and delivered (as opposed to independent home exercises). The exercise programs commonly included strengthening or trunk stabilizing exercises. Conservative care in addition to exercise therapy was often included in these effective interventions, including behavioural and manual therapy, advice to stay active, and education. One low quality trial found a group-delivered aerobics and strengthening exercise program resulted in less improvement in pain and function outcomes than behavioural therapy. Of the remaining trials, 14 (2 high quality and 12 low quality) found no statistically significant or clinically important differences between exercise therapy and other conservative treatments; 4 of these trials were inadequately powered to detect clinically important differences on at least one outcome. Trials were rated low quality most commonly because of inadequate assessor blinding.
Meta-analysis of pain outcomes at the earliest follow-up included 23 exercise groups with an independent comparison and adequate data. Synthesis resulted in a pooled weighted mean improvement of 10.2 points (95% CI 1.31�19.09) for exercise therapy compared to no treatment, and 5.93 points (95% CI 2.21�9.65) compared to other conservative treatment [vs. all comparisons 7.29 points (95% CI 3.67�0.91)]. Smaller improvements were seen in functional outcomes with an observed mean positive effect of 3.15 points (95% CI -0.29 to 6.60) compared to no treatment, and 2.37 points (95% CI 0.74�4.0) versus other conservative treatment at the earliest follow-up [vs. all comparisons 2.53 points (95% CI 1.08�3.97)].
Adverse effects Most trials did not report any side effects. Two studies reported cardiovascular events that were considered not to be caused by the exercise therapy.
Lumbar Supports
Lumbar supports are provided as treatment to people suffering from LBP with the aim of making the impairment and disability vanish or decrease. Different desired functions have been suggested for lumbar supports: (1) to correct deformity, (2) to limit spinal motion, (3) to stabilize part of the spine, (4) to reduce mechanical uploading, and (5) miscellaneous effects: massage, heat, placebo. However, at the present time the putative mechanisms of action of a lumbar support remain a matter of debate.
Effectiveness of lumbar supports for acute LBP No trials were identified.
Effectiveness of lumbar supports for chronic LBP No RCT compared lumbar supports with placebo, no treatment, or other treatments for chronic LBP.
Effectiveness of lumbar supports for a mixed population of acute, subacute, and chronic LBP Four studies included a mix of patients with acute, subacute, and chronic LBP. One study did not give any information about the duration of the LBP complaints of the patients. There is moderate evidence that a lumbar support is not more effective in reducing pain than other types of treatment. Evidence on overall improvement and return to work was conflicting.
Adverse effects Potential adverse effects associated with prolonged lumbar support use include decreased strength of the trunk musculature, a false sense of security, heat, skin irritation, skin lesions, gastrointestinal disorders and muscle wasting, higher blood pressure and higher heart rates, and general discomfort.
Multidisciplinary Treatment Programmes
Multidisciplinary treatments for back pain evolved from pain clinics. Initially, multidisciplinary treatments focused on a traditional biomedical model and in the reduction of pain. Current multidisciplinary approaches to chronic pain are based on a multifactorial biopsychosicial model of interrelating physical, psychological, and social/occupational factors. The content of multidisciplinary programs varies widely and, at present, it is unclear what the optimal content is and who should be involved.
Effectiveness of multidisciplinary treatment for subacute LBP No trials identified.
Effectiveness of multidisciplinary treatment for subacute LBP Multidisciplinary treatment versus usual care. Two RCTs on subacute LBP were included. The study population in both studies consisted of workers on sick leave. In one study the patients in the intervention group returned to work sooner (10 weeks) compared with the control group (15 weeks) (P=0.03). The intervention group also had fewer sick leave during follow-up than the control group (mean difference=-7.5 days, 95% CI -15.06 to 0.06). There was no statistically significant difference in pain intensity between the intervention and control group, but subjective disability had decreased significantly more in the intervention group than in the control group (mean difference=-1.2, 95% CI -1.984 to -0.416). In the other study, the median duration of absence from regular work was 60 days for the group with a combination of occupational and clinical intervention, 67 days with the occupational intervention group, 131 days with the clinical intervention group, and 120.5 days with the usual care group (P=0.04). Return to work was 2.4 times faster in the group with both an occupational and clinical intervention (95% CI 1.19�4.89) than the usual care group, and 1.91 times faster in the two groups with occupational intervention than the two groups without occupational interventions (95% CI 1.18�3.1). There is moderate evidence that multidisciplinary treatment with a workplace visit and comprehensive occupational health care intervention is effective with regard to return to work, sick leave, and subjective disability for patients with subacute LBP.
Effectiveness of multidisciplinary treatment for chronic LBP Multidisciplinary treatment versus other interventions. Ten RCTs with a total of 1,964 subjects were included in the Cochrane review. Three additional papers reported on long-term outcomes of two of these trials. All ten trials excluded patients with significant radiculopathy or other indication for surgery. There is strong evidence that intensive multidisciplinary treatment with a functional restoration approach improves function when compared with inpatient or outpatient non-multidisciplinary treatments. There is moderate evidence that intensive multidisciplinary treatment with a functional restoration approach reduces pain when compared with outpatient non-multidisciplinary rehabilitation or usual care. There is contradictory evidence regarding vocational outcomes. Five trials evaluating less intensive multidisciplinary treatment programmes could not demonstrate beneficial effects on pain, function, or vocational outcomes when compared with non-multidisciplinary outpatient treatment or usual care. One additional RCT was found that showed no difference between multidisciplinary treatment and usual care on function and health related quality of life after 2 and 6 months.
The reviewed studies provide evidence that intensive (>100 h of therapy) MBPSR with a functional restoration approach produces greater improvements in pain and function for patients with disabling chronic LBP than non-multidisciplinary rehabilitation or usual care. Less intensive treatments did not seem effective.
Adverse effects No adverse effects were reported.
Spinal Manipulation
Spinal manipulation is defined as a form of manual therapy which involves movement of a joint past its usual end range of motion, but not past its anatomic range of motion. Spinal manipulation is usually considered as that of long lever, low velocity, non-specific type manipulation as opposed to short lever, high velocity, specific adjustment. Potential hypotheses for the working mechanism of spinal manipulation are: (1) release for the entrapped synovial folds, (2) relaxation of hypertonic muscle, (3) disruption of articular or periarticular adhesion, (4) unbuckling of motion segments that have undergone disproportionate displacement, (5) reduction of disc bulge, (6) repositioning of miniscule structures within the articular surface, (7) mechanical stimulation of nociceptive joint fibres, (8) change in neurophysiological function, and (9) reduction of muscle spasm.
Effectiveness of spinal manipulation for acute LBP Spinal manipulation versus sham. Two trials were identified. Patients receiving treatment that included spinal manipulation had statistically significant and clinically important short-term improvements in pain (10-mm difference; 95% CI 2�17 mm) compared with sham therapy. However, the improvement in function was considered clinically relevant but not statistically significant (2.8-mm difference on the Roland Morris scale; 95% CI -0.1 to 5.6).
Spinal manipulation versus other therapies. Twelve trials were identified. Spinal manipulation resulted in statistically significant more short-term pain relief compared with other therapies judged to be ineffective or possibly even harmful (4-mm difference; 95% CI 1�8 mm). However, the clinical significance of this finding is questionable. The point estimate of improvement in short-term function for treatment with spinal manipulation compared with the ineffective therapies was considered clinically significant but was not statistically significant (2.1-point difference on the Roland Morris scale; 95% CI -0.2 to 4.4). There were no differences in effectiveness between patients treated with spinal manipulation and those treated with any of the conventionally advocated therapies.
Effectiveness of spinal manipulation for chronic LBP Spinal manipulation versus sham. Three trials were identified. Spinal manipulation was statistically significantly more effective compared with sham manipulation on short-term pain relief (10 mm; 95% CI 3�17 mm) and long-term pain relief (19 mm; 95% CI 3�35 mm). Spinal manipulation was also statistically significantly more effective on short-term improvement of function (3.3 points on the Roland and Morris Disability Questionnaire (RMDQ); 95% CI 0.6�6.0).
Spinal manipulation versus other therapies. Eight trials were identified. Spinal manipulation was statistically significantly more effective compared with the group of therapies judged to be ineffective or perhaps harmful on short-term pain relief (4 mm; 95% CI 0�8), and short-term improvement in function (2.6 points on the RMDQ; 95% CI 0.5�4.8). There were no differences in short- and long-term effectiveness compared with other conventionally advocated therapies such as general practice care, physical or exercise therapy, and back school.
Adverse effects In the RCTs identified by the review that used a trained therapist to select people and perform spinal manipulation, the risk of serious complications was low. An estimate of the risk of spinal manipulation causing a clinically worsened disk herniation or cauda equina syndrome in a patient presenting with lumbar disk herniation is calculated from published data to be less than 1 in 3.7 million.
Traction
Lumbar traction uses a harness (with velcro strapping) that is put around the lower rib cage and around the iliacal crest. Duration and level of force exerted through this harness can be varied in a continuous or intermittent mode. Only in motorized and bed rest traction can the force be standardized. With other techniques total body weight and the strength of the patient or therapist determine the forces exerted. In the application of traction force, consideration must be given to counterforces such as lumbar muscle tension, lumbar skin stretch and abdominal pressure, which depend on the patient�s physical constitution. If the patient is lying on the traction table, the friction of the body on the table provides the main counterforce during traction. The exact mechanism through which traction might be effective is unclear. It has been suggested that spinal elongation, through decreasing lordosis and increasing intervertebral space, inhibits nociceptive impulses, improves mobility, decreases mechanical stress, reduces muscle spasm or spinal nerve root compression (due to osteophytes), releases luxation of a disc or capsule from the zygo-apophysial joint, and releases adhesions around the zygo-apophysial joint and the annulus fibrosus. So far, the proposed mechanisms have not been supported by sufficient empirical information.
Thirteen of the studies identified in the Cochrane review included a homogeneous population of LBP patients with radiating symptoms. The remaining studies included a mix of patients with and without radiation. There were no studies exclusively involving patients who had no radiating symptoms.
Five studies included solely or primarily patients with chronic LBP of more than 12 weeks; in one study patients were all in the subacute range (4�12 weeks). In 11 studies the duration of LBP was a mixture of acute, subacute, and chronic. In four studies duration was not specified.
Effectiveness of traction for acute LBP No RCTs included primarily people with acute LBP. One study was identified that included patients with subacute LBP, but this population consisted of a mix of patients with and without radiation.
Effectiveness of traction for chronic LBP One trial found that continuous traction is not more effective on pain, function, overall improvement, or work absenteeism than placebo. One RCT (42 people) found no difference in effectiveness between standard physical therapy including continuous traction and the same program without traction. One RCT (152 people) found no significant difference between lumbar traction plus massage and interferential treatment in pain relief, or improvement of disability 3 weeks and 4 months after the end of treatment. This RCT did not exclude people with sciatica, but no further details of the proportion of people with sciatica were reported. One RCT (44 people) found that autotraction is more effective than mechanical traction on global improvement, but not on pain and function, in chronic LBP patients with or without radiating symptoms. However, this trial had several methodological problems that may be associated with biased results.
Adverse effects Little is known about the adverse effects of traction. Only a few case reports are available, which suggest that there is some danger for nerve impingement in heavy traction, i.e. lumbar traction forces exceeding 50% of the total body weight. Other risks described for lumbar traction are respiratory constraints due to the traction harness or increased blood pressure during inverted positional traction. Other potential adverse effects of traction include debilitation, loss of muscle tone, bone demineralization, and thrombophlebitis.
Transcutaneous Electrical Nerve Stimulation
Transcutaneous electrical nerve stimulation (TENS) is a therapeutic non-invasive modality mainly used for pain relief by electrically stimulating peripheral nerves via skin surface electrodes. Several types of TENS applications, differing in intensity and electrical characteristics, are used in clinical practice: (1) high frequency, (2) low frequency, (3) burst frequency, and (4) hyperstimulation.
Effectiveness of TENS for acute LBP: No trials were identified.
Effectiveness of TENS for chronic LBP The Cochrane review included two RCTs of TENS for chronic LBP. The results of one small trial (N=30) showed a significant decrease in subjective pain intensity with active TENS treatment compared to placebo over the course of the 60-min treatment session. The pain reduction seen at the end of stimulation was maintained for the entire 60-min post-treatment time interval assessed (data not shown). Longer term follow-up was not conducted in this study. The second trial (N=145) demonstrated no significant difference between active TENS and placebo for any of the outcomes measured, including pain, functional status, range of motion, and use of medical services.
Adverse effects In a third of the participants in one trial, minor skin irritation occurred at the site of electrode placement. These adverse effects were observed equally in the active TENS and placebo groups. One participant randomized to placebo TENS developed severe dermatitis 4 days after beginning therapy and was required to withdraw (Tables 1, ?2).
Table 1: Effectiveness of conservative interventions for acute non-specific low back pain.
Table 2: Effectiveness of conservative interventions for chronic non-specific low back pain.
Discussion
The best available evidence for conservative treatments for non-specific LBP summarized in this paper shows that some interventions are effective. Traditional NSAIDs, muscle relaxants, and advice to stay active are effective for short-term pain relief in acute LBP. Advice to stay active is also effective for long-term improvement of function in acute LBP. In chronic LBP, various interventions are effective for short-term pain relief, i.e. antidepressants, COX2 inhibitors, back schools, progressive relaxation, cognitive�respondent treatment, exercise therapy, and intensive multidisciplinary treatment. Several treatments are also effective for short-term improvement of function in chronic LBP, namely COX2 inhibitors, back schools, progressive relaxation, exercise therapy, and multidisciplinary treatment. There is no evidence that any of these interventions provides long-term effects on pain and function. Also, many trials showed methodological weaknesses, effects are compared to placebo, no treatment or waiting list controls, and effect sizes are small. Future trials should meet current quality standards and have adequate sample size. However, in summary, there is evidence that some interventions are effective while evidence for many other interventions is lacking or there is evidence that they are not effective.
During the last decade, various clinical guidelines on the management of acute LBP in primary care have been published that have used this evidence. At present, guidelines exist in at least 12 different countries: Australia, Denmark, Finland, Germany, Israel, the Netherlands, New Zealand, Norway, Sweden, Switzerland, the United Kingdom, and the United States. Since the available evidence is international, one would expect that each country�s guidelines would give more or less similar recommendations regarding diagnosis and treatment. Comparison of clinical guidelines for the management of LBP in primary care from 11 different countries showed that the content of the guidelines regarding therapeutic interventions is quite similar. However, there were also some discrepancies in recommendations across guidelines. Differences in recommendations between guidelines may be due to incompleteness of the evidence, different levels of evidence, magnitude of effects, side effects and costs, differences in health care systems (organization/financial), or differences in membership of guidelines committees. More recent guidelines may have included more recently published trials and, therefore, may end up with slightly different recommendations. Also, guidelines may have been based on systematic reviews that included trials in different languages; the majority of existing reviews have considered only studies published in a few languages, and several, only those published in English. Recommendations in guidelines are not only based on scientific evidence, but also on consensus. Guideline committees may consider various arguments differently, such as the magnitude of the effects, potential side effects, cost-effectiveness, and current routine practice and available resources in their country. Especially as we know that effects in the field of LBP, if any, are usually small and short-term effects only, interpretation of effects may vary among guideline committees. Also, guideline committees may differently weigh other aspects such as side effects and costs. The constitution of the guideline committees and the professional bodies they represent may introduce bias�either for or against a particular treatment. This does not necessarily mean that one guideline is better than the other or that one is right and the other is wrong. It merely shows that when translating the evidence into clinically relevant recommendations more aspects play a role, and that these aspects may vary locally or nationally.
Recently European guidelines for the management of LBP were developed to increase consistency in the management of non-specific LBP across countries in Europe. The European Commission has approved and funded this project called �COST B13�. The main objectives of this COST action were developing European guidelines for the prevention, diagnosis and treatment of non-specific LBP, ensuring an evidence-based approach through the use of systematic reviews and existing clinical guidelines, enabling a multidisciplinary approach, and stimulating collaboration between primary health care providers and promoting consistency across providers and countries in Europe. Representatives from 13 countries participated in this project that was conducted between 1999 and 2004. The experts represented all relevant health professions in the field of LBP: anatomy, anaesthesiology, chiropractic, epidemiology, ergonomy, general practice, occupational care, orthopaedic surgery, pathology, physiology, physiotherapy, psychology, public health care, rehabilitation, and rheumatology. Within this COST B13 project four European guidelines were developed on: (1) acute LBP, (2) chronic LBP, (3) prevention of LBP, and (4) pelvic girdle pain. The guidelines will soon be published as a supplement to the European Spine Journal.
Contributor Information
Maurits W. van Tulder, Bart Koes, Antti Malmivaara: Ncbi.nlm.nih.gov
In conclusion,�the clinical and experimental evidence above for non-invasive treatment modalities on back pain demonstrated that several of the treatments are safe and effective. While the results of a variety of the methods used to improve back pain symptoms were proven to be efficient, many other treatment modalities requires additional evidence and others were reported to not be effective towards improving symptoms of back pain.�The main objective of the research study was to determine the safest and most effective guideline for the prevention, diagnosis and treatment of non-specific back pain.�Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Sciatica
Sciatica is referred to as a collection of symptoms rather than a single type of injury or condition. The symptoms are characterized as radiating pain, numbness and tingling sensations from the sciatic nerve in the lower back, down the buttocks and thighs and through one or both legs and into the feet. Sciatica is commonly the result of irritation, inflammation or compression of the largest nerve in the human body, generally due to a herniated disc or bone spur.
1.�Alaranta H, Rytokoski U, Rissanen A, Talo S, Ronnemaa T, Puukka P, Karppi SL, Videman T, Kallio V, Slatis P. Intensive physical and psychosocial training program for patients with chronic low back pain.�A controlled trial. Spine.�1994;19:1340�1349.�[PubMed]
2.�Alcoff J, Jones E, Rust P, Newman R. Controlled trial of imipramine for chronic low back pain.�J Fam Pract.�1982;14:841�846.�[PubMed]
3.�Alexandre NM, Moraes MA, Correa Filho HR, Jorge SA. Evaluation of a program to reduce back pain in nursing personnel.�Rev Salud Publica.�2001;35:356�361.�[PubMed]
4.�Amlie E, Weber H, Holme I. Treatment of acute low back pain with piroxicam: results of a double-blind placebo-controlled trial.�Spine.�1987;12:473�476. doi: 10.1097/00007632-198706000-00010.�[PubMed][Cross Ref]
5.�Arbus L, Fajadet B, Aubert D, Morre M, Goldfinger E. Activity of tetrazepam in low back pain.�Clin Trials J.�1990;27:258�267.
6.�Assendelft WJ, Morton SC, Yu EI, Suttorp MJ, Shekelle P. Spinal manipulative therapy for low back pain. A meta-analysis of effectiveness relative to other therapies.�Ann Intern Med.�2003;138:871�881.[PubMed]
7.�Atkinson JH, Slater MA, Williams RA. A placebo-controlled randomized clinical trial of nortriptyline for chronic low back pain.�Pain.�1998;76:287�296. doi: 10.1016/S0304-3959(98)00064-5.�[PubMed][Cross Ref]
8.�Atkinson JH, Slater MA, Wahlgren DR. Effects of noradrenergic and serotonergic antidepressants on chronic low back pain intensity.�Pain.�1999;83:137�145. doi: 10.1016/S0304-3959(99)00082-2.�[PubMed][Cross Ref]
9.�Babej-Dolle R, Freytag S, Eckmeyer J, Zerle G, Schinzel S, Schmeider G, Stankov G. Parenteral dipyrone versus diclofenac and placebo in patients with acute lumbago or sciatic pain: randomized observer-blind multicenter study.�Int J Clin Pharmacol Ther.�1994;32:204�209.�[PubMed]
10.�Baptista R, Brizzi J, Dutra F, Josef H, Keisermann M, de Lucca R (1988) Terapeutica da lombalgia com a tizanidina (DS 103-282), un novo agente mioespasmolitico. Estudo multicentrico, duplo-cego e comparativo. Folha Medica
11.�Barrata R. A double-blind study of cyclobenzaprine and placebo in the treatment of acute muskuloskeletal conditions of the low back.�Curr Ther Res.�1982;32:646�652.
12.�Basler H, Jakle C, Kroner-Herwig B. Incorporation of cognitive�behavioral treatment into the medical care of chronic low back patients: a controlled randomized study in German pain treatment centers.�Patient Educ Couns.�1997;31:113�124. doi: 10.1016/S0738-3991(97)00996-8.�[PubMed]�[Cross Ref]
13.�Basmajian J. Cyclobenzaprine hydrochloride effect on skeletal muscle spasm in the lumbar region and neck: two double-blind controlled clinical and laboratory studies.�Arch Phys Med Rehabil.�1978;59:58�63.[PubMed]
14.�Basmajian JV. Acute back pain and spasm: a controlled multicenter trial of combined analgesic and antispasm agents.�Spine.�1989;14:438�439. doi: 10.1097/00007632-198904000-00019.�[PubMed][Cross Ref]
15.�Bendix AF, Bendix T, Ostenfeld S, Bush E, Andersen A. Active treatment programs for patients with chronic low back pain: a prospective randomized, observer-blinded study.�Eur Spine J.�1995;4:148�152. doi: 10.1007/BF00298239.�[PubMed]�[Cross Ref]
16.�Bendix AF, Bendix T, Vaegter KV, Lund C, Frolund L, Holm L. Multidisciplinary intensive treatment for chronic low back pain: a randomized, prospective study.�Cleve Clin J Med.�1996;63:62�69.�[PubMed]
17.�Bendix AE, Bendix T, Lund C, Kirkbak S, Ostenfeld S. Comparison of three intensive programs for chronic low back pain patients: a prospective, randomized, observer-blinded study with one-year follow-up.�Scand J Rehabil Med.�1997;29:81�89.�[PubMed]
18.�Bendix AE, Bendix T, Haestrup C, Busch E. A prospective, randomized 5-year follow-up study of functional restoration in chronic low back pain patients.�Eur Spine J.�1998a;7:111�119. doi: 10.1007/s005860050040.�[PubMed]�[Cross Ref]
19.�Bendix AE, Bendix T, Labriola M, Boekgaard P. Functional restoration for chronic low back pain. Two-year follow-up of two randomized clinical trials.�Spine.�1998b;23:717�725. doi: 10.1097/00007632-199803150-00013.�[PubMed]�[Cross Ref]
20.�Bendix T, Bendix A, Labriola M, Haestrup C, Ebbehoj N. Functional restoration versus outpatient physical training in chronic low back pain: a randomized comparative study.�Spine.�2000;25:2494�2500. doi: 10.1097/00007632-200010010-00012.�[PubMed]�[Cross Ref]
21.�Bergquist-Ullman M, Larsson U. Acute low-back pain in industry.�Acta Orthop Scand.�1977;170(Suppl.):1�117.�[PubMed]
22.�Berry H, Hutchinson D. A multicentre placebo-controlled study in general practice to evaluate the efficacy and safety of tizanidine in acute low-back pain.�J Int Med Res.�1988;16:75�82.�[PubMed]
23.�Berry H, Bloom B, Hamilton EBD, Swinson DR. Naproxen sodium, diflunisal, and placebo in the treatment of chronic back pain.�Ann Rheum Dis.�1982;41:129�132. doi: 10.1136/ard.41.2.129.[PMC free article]�[PubMed]�[Cross Ref]
24.�Beurskens AJ, Vet HC, K�ke AJ, Lindeman E, Regtop W, Heijden GJ, Knipschild PG. Efficacy of traction for non-specific low back pain: a randomised clinical trial.�Lancet.�1995;346:1596�1600. doi: 10.1016/S0140-6736(95)91930-9.�[PubMed]�[Cross Ref]
25.�Beurskens AJ, Vet HC, K�ke AJ, Regtop W, Heijden GJ, Lindeman E, Knipschild PG. Efficacy of traction for nonspecific low back pain. 12-week and 6-month results of a randomized clinical trial.�Spine.�1997;22:2756�2762. doi: 10.1097/00007632-199712010-00011.�[PubMed]�[Cross Ref]
26.�Bianchi M.�Evaluation of cyclobenzaprine for skeletal muscle spasm of local origin. Clinical evaluation of flexeril (cyclobenzaprine HCL/MSD)�Minneapolis: Postgraduate Medicine Communications; 1978. pp. 25�29.
27.�Bigos S, Bowyer O, Braen G (1994) Acute low back problems in adults. Clinical Practice Guideline No. 14. AHCPR Publication No. 95-0642. Agency for Health Care Policy and Research, Public Health Service, US Department of Health and Human Services, Rockville
28.�Bihaug O. Autotraksjon for ischialgpasienter. En kontrollert sammenlikning mellom effekten av Auto-traksjon-B og isometriske ovelser ad modum Hume endall og Jenkins.�Fysioterapeuten.�1978;45:377�379.
29.�Birbara CA, Puopolo AD, Munoz DR. Treatment of chronic low back pain with etoricoxib, a new cyclo-oxygenase-2 selective inhibitor: improvement in pain and disability: a randomised, placebo-controlled, 3-month trial.�J Pain.�2003;4:307�315. doi: 10.1016/S1526-5900(03)00633-3.�[PubMed][Cross Ref]
30.�Blomberg S, Hallin G, Grann K, Berg E, Sennerby U. Manual therapy with steroid injections�a new approach to treatment of low back pain. A controlled multicenter trial with an evaluation by orthopedic surgeons.�Spine.�1994;19:569�577. doi: 10.1097/00007632-199403000-00013.�[PubMed]�[Cross Ref]
31.�Bombardier C, Laine L, Reicin A, Shapiro D, Burgos-Vargas R, Davis B, Day R, Ferraz MB, Hawkey CJ, Hochberg MC, Kvien TK, Schnitzer TJ, Study Group VIGOR. Comparison of upper gastrointestinal toxicity of rofecoxib and naproxen in patients with rheumatoid arthritis. VIGOR Study Group.�N Engl J Med.�2000;343:1520�1528. doi: 10.1056/NEJM200011233432103.�[PubMed]�[Cross Ref]
32.�Borman P, Keskin D, Bodur H. The efficacy of lumbar traction in the management of patients with low back pain.�Rheumatol Int.�2003;23:82�86.�[PubMed]
33.�Bouter LM, Pennick V, Bombardier C, Editorial Board of the Back Review Group Cochrane Back Review Group.�Spine.�2003;28:1215�1218. doi: 10.1097/00007632-200306150-00002.�[PubMed][Cross Ref]
34.�Braun H, Huberty R. Therapy of lumbar sciatica. A comparative clinical study of a corticoid-free monosubstance and a corticoid containing combination drug.�Med Welt.�1982;33:490�491.�[PubMed]
35.�Bronfort G, Goldsmith CH, Nelson CF, Boline PD, Anderson AV. Trunk exercise combined with spinal manipulative or NSAID therapy for chronic low back pain: a randomized, observer-blinded clinical trial.�J Manipulative Physiol Ther.�1996;19:570�582.�[PubMed]
36.�Brown FL, Bodison S, Dixon J, Davis W, Nowoslawski J. Comparison of diflunisal and acetaminophen with codeine in the treatment of initial or recurrent acute low back pain.�Clin Ther.�1986;9(Suppl. c):52�58.[PubMed]
37.�Bru E, Mykletun R, Berge W, Svebak S. Effects of different psychological interventions on neck, shoulder and low back pain in female hospital staff.�Psychol Health.�1994;9:371�382. doi: 10.1080/08870449408407495.�[Cross Ref]
38.�Calmels P, Fayolle-Minon I. An update on orthotic devices for the lumbar spine based on a review of the literature.�Rev Rhum.�1996;63:285�291.�[PubMed]
39.�Casale R. Acute low back pain: symptomatic treatment with a muscle relaxant drug.�Clin J Pain.�1988;4:81�88.
40.�Cherkin DC, Deyo RA, Battie M, Street J, Barlow W. A comparison of physical therapy, chiropractic manipulation, and provision of an educational booklet for the treatment of patients with low back pain.�N Engl J Med.�1998;339:1021�1029. doi: 10.1056/NEJM199810083391502.�[PubMed]�[Cross Ref]
41.�Chok B, Lee R, Latimer J, Seang BT. Endurance training of the trunk extensor muscles in people with subacute low back pain.�Phys Ther.�1999;79:1032�1042.�[PubMed]
42.�Clarke J, van Tulder M, Blomberg S, Bronfort G, van der Heijden G, de Vet HCW (2005) Traction for low back pain: a systematic review within the framework of the Cochrane Collaboration. In: The Cochrane Library, Issue 3. Update Software, Oxford
43.�Coats TL, Borenstein DG, Nangia NK, Brown MT. Effects of valdecoxib in the treatment of chronic low back pain: results of a randomized, placebo-controlled trial.�Clin Ther.�2004;26:1249�1260. doi: 10.1016/S0149-2918(04)80081-X.�[PubMed]�[Cross Ref]
44.�Coomes NE. A comparison between epidural anaesthesia and bed rest in sciatica.�Br Med J.�1961;Jan:20�24.�[PMC free article]�[PubMed]
45.�Coxhead CE, Inskip H, Meade TW, North WRS, Troup JDG. Multicentre trial of physiotherapy in the management of sciatic symptoms.�Lancet.�1981;1:1065�1068. doi: 10.1016/S0140-6736(81)92238-8.[PubMed]�[Cross Ref]
46.�Cramer GD, Humphreys CR, Hondras MA, McGregor M, Triano JJ. The Hmax/Mmax ratio as an outcome measure for acute low back pain.�J Manipulative Physiol Ther.�1993;16:7�13.�[PubMed]
47.�Dalichau S, Scheele K. Effects of elastic lumbar belts on the effect of a muscle training program for patients with chronic back pain [German]�Zt Orthop Grenzgeb.�2000;138:8�16. doi: 10.1055/s-2000-10106.�[PubMed]�[Cross Ref]
48.�Dalichau S, Scheele K, Perrey RM, Elliehausen H-J, Huebner J. Ultraschallgest�tzte Haltungs- und Bewegungsanalyse der Lendenwirbels�ule zum Nachweis der Wirksamkeit einer R�ckenschule.�Zbl Arbeitsmedizin.�1999;49:148�156.
49.�Dapas F. Baclofen for the treatment of acute low-back syndrome.�Spine.�1985;10:345�349. doi: 10.1097/00007632-198505000-00010.�[PubMed]�[Cross Ref]
50.�Davies JE, Gibson T, Tester L. The value of exercises in the treatment of low back pain.�Rheumatol Rehabil.�1979;18:243�247.�[PubMed]
51.�Deyo RA, Diehl AK, Rosenthal M. How many days of bed rest for acute low back pain? A randomized clinical trial.�N Engl J Med.�1986;315:1064�1070.�[PubMed]
52.�Deyo RA, Walsh NE, Martin DC, Schoenfeld LS, Ramamurthy S. A controlled trial of transcutaneous electrical nerve stimulation (TENS) and exercise for chronic low back pain.�N Engl J Med.�1990;322:1627�1634.�[PubMed]
53.�Dickens C, Jayson M, Sutton C. The relationship between pain and depression in a trial using paroxetine in sufferers of chronic low back pain.�Psychosomatics.�2000;41:490�499. doi: 10.1176/appi.psy.41.6.490.�[PubMed]�[Cross Ref]
54.�Donchin M, Woolf O, Kaplan L, Floman Y. Secondary prevention of low-back pain.�A clinical trial. Spine.�1990;15:1317�1320.�[PubMed]
55.�Doran DML, Newell DJ. Manipulation in treatment of low back pain: a multicentre study.�Br Med J.�1975;2:161�164.�[PMC free article]�[PubMed]
56.�Evans DP, Burke MS, Lloyd KN, Roberts EE, Roberts GM. Lumbar spinal manipulation on trial. Part 1: clinical assessment.�Rheumatol Rehabil.�1978;17:46�53.�[PubMed]
57.�Evans DP, Burke MS, Newcombe RG. Medicines of choice in low back pain.�Curr Med Res Opin.�1980;6:540�547.�[PubMed]
58.�Faas A, Chavannes AW, Eijk JTM, Gubbels JW. A randomized placebo-controlled trial of exercise therapy in patients with acute low back pain.�Spine.�1993;18:1388�1395.�[PubMed]
59.�Faas A, Eijk JTM, Chavannes AW, Gubbels JW. A randomized trial of exercise therapy in patients with acute low back pain.�Spine.�1995;20:941�947. doi: 10.1097/00007632-199504150-00012.�[PubMed][Cross Ref]
60.�Farrell JP, Twomey LT. Acute low back pain: comparison of two conservative treatment approaches.�Med J Aust.�1982;1:160�164.�[PubMed]
61.�Fordyce WE, Brockway JA, Bergman JA, Spengler D. Acute back pain: a control group comparison of behavioural versus traditional management methods.�J Behav Med.�1986;9:127�140. doi: 10.1007/BF00848473.�[PubMed]�[Cross Ref]
62.�Frost H, Klaber Moffett JA, Moser JS, Fairbank JCT. Randomised controlled trial for evaluation of fitness programme for patients with chronic low back pain.�Br Med J.�1995;310:151�154.[PMC free article]�[PubMed]
63.�Frost H, Lamb SE, Klaber Moffett JA, Fairbank JCT, Moser JS. A fitness programme for patients with chronic low back pain: 2-year follow-up of a randomised controlled trial.�Pain.�1998;75:273�279. doi: 10.1016/S0304-3959(98)00005-0.�[PubMed]�[Cross Ref]
64.�Frost H, Lamb SE, Doll HA, Taffe Carver P, Stewart-Brown S. Randomized controlled trial of physiotherapy compared with advice for low back pain.�Br Med J.�2004;329:708�711. doi: 10.1136/bmj.38216.868808.7C.�[PMC free article]�[PubMed]�[Cross Ref]
65.�Galantino ML, Bzdewka TM, Eissler-Russo JL, Holbrook ML, Mogck EP, Geigle P. The impact of modified hatha yoga on chronic low back pain: a pilot study.�Altern Ther Health Med.�2004;10:56�59.[PubMed]
66.�Gemignani G, Olivieri I, Ruju G, Pasero G. Transcutaneous electrical nerve stimulation in ankylosing spondylitis: a double-blind study.�Arthritis Rheum.�1991;34:788�789. doi: 10.1002/art.1780340624.[PubMed]�[Cross Ref]
67.�Gibson T, Grahame R, Harkness J, Woo P, Blagrave P, Hills R (1985) Controlled comparison of short-wave diathermy treatment with osteopathic treatment in non-specific low back pain. Lancet 1258�1261[PubMed]
68.�Gilbert JR, Taylor DW, Hildebrand A, Evans C. Clinical trial of common treatments for low back pain in family practice.�Br Med J Clin Res Ed.�1985;291:791�794.�[PMC free article]�[PubMed]
69.�Glomsr�d B, L�nn JH, Soukup MG, B� K, Larsen S. Active back school, prophylactic management for low back pain: three-year follow-up of a randomized controlled trial.�J Rehabil Med.�2001;33:26�30. doi: 10.1080/165019701300006506.�[PubMed]�[Cross Ref]
70.�Glover JR, Morris JG, Khosla T. Back pain: a randomized clinical trial of rotational manipulation of the trunk.�Br J Ind Med.�1974;31:59�64.�[PMC free article]�[PubMed]
71.�Godfrey CM, Morgan PP, Schatzker J. A randomized trial of manipulation for low-back pain in a medical setting.�Spine.�1984;9:301�304. doi: 10.1097/00007632-198404000-00015.�[PubMed]�[Cross Ref]
72.�Gold R. Orphenadrine citrate: sedative or muscle relaxant?�Clin Ther.�1978;1:451�453.
73.�Goldie I. A clinical trial with indomethacin (indomee) in low back pain and sciatica.�Acta Orthop Scand.�1968;39:117�128.�[PubMed]
74.�Goodkin K, Gullion CM, Agras WS. A randomised double blind, placebo-controlled trial of trazodone hydrochloride in chronic low back pain syndrome.�J Clin Psychopharmacol.�1990;10:269�278. doi: 10.1097/00004714-199008000-00006.�[PubMed]�[Cross Ref]
75.�Gur A, Karakoc M, Cevik R, Nas K, Sarac AJ, Karakoc M. Efficacy of low power laser therapy and exercise on pain and functions in chronic low back pain.�Lasers Surg Med.�2003;32:233�238. doi: 10.1002/lsm.10134.�[PubMed]�[Cross Ref]
76.�Guzman J, Esmail R, Karjalainen K. Multidisciplinary rehabilitation for chronic low back pain: systematic review.�Br Med J.�2001;322:1511�1516. doi: 10.1136/bmj.322.7301.1511.�[PMC free article][PubMed]�[Cross Ref]
77.�Hadler NM, Curtis P, Gillings DB, Stinnett S. A benefit of spinal manipulation as adjunctive therapy for acute low-back pain: a stratified controlled trial.�Spine.�1987;12:703�705. doi: 10.1097/00007632-198709000-00012.�[PubMed]�[Cross Ref]
78.�Hagen KB, Hilde G, Jamtvedt G (2003) Bed rest for acute low back pain and sciatica (Cochrane Review). In: The Cochrane Library, Issue 1. Update Software, Oxford
79.�Hameroff SR, Weiss JL, Lerman JC. Doxepin�s effects on chronic pain and depression: a controlled study.�J Clin Psychiatry.�1984;45:47�52.�[PubMed]
80.�Hansen FR, Bendix T, Skov P, Jensen CV, Kristensen JH, Krohn L. Intensive, dynamic back-muscle exercises, conventional physiotherapy, or placebo-control treatment of low back pain: a randomized, observer-blind trial.�Spine.�1993;18:98�107. doi: 10.1097/00007632-199301000-00015.�[PubMed][Cross Ref]
81.�H�rk�p�� K, J�rvikoski A, Mellin G, Hurri H. A controlled study on the outcome of inpatient and outpatient treatment of low-back pain. Part I.�Scand J Rehabil Med.�1989;21:81�89.�[PubMed]
82.�H�rk�p�� K, Mellin G, J�rvikoski A, Hurri H. A controlled study on the outcome of inpatient and outpatient treatment of low-back pain. Part III.�Scand J Rehabil Med.�1990;22:181�188.�[PubMed]
83.�Hayden JA, Tulder MW, Malmivaara AV, Koes BW. Meta-analysis: exercise therapy for nonspecific low back pain.�Ann Intern Med.�2005;142:765�775.�[PubMed]
84.�Hemmila HM, Keinanen-Kiukaanniemi SM, Levoska S. Does folk medicine work? A randomized clinical trial on patients with prolonged back pain.�Arch Phys Med Rehabil.�1997;78:571�577. doi: 10.1016/S0003-9993(97)90420-2.�[PubMed]�[Cross Ref]
85.�Hemmila H, Keinanen-Kiukaanniemi SM, Levoska S, Puska P. Long-term effectiveness of bone-setting, light exercise therapy, and physiotherapy for prolonged back pain: a randomized controlled trial.�J Manipulative Physiol Ther.�2002;25:99�104. doi: 10.1067/mmt.2002.122329.�[PubMed]�[Cross Ref]
86.�Henry D, Lim LLY, Rodriguez LAG. Variability in risk of gastrointestinal complications with individual non-steroidal anti-inflammatory drugs: results of a collaborative meta-analysis.�Br Med J.�1996;312:1563�1566.�[PMC free article]�[PubMed]
87.�Herzog W, Conway PJW, Willcox BJ. Effects of different treatment modalities on gait symmetry and clinical measures for sacroiliac joint patients.�J Manipulative Physiol Ther.�1991;14:104�109.�[PubMed]
88.�Heymans MW, Tulder MW, Esmail R, Bombardier C, Koes BW. Back schools for nonspecific low back pain: a systematic review within the framework of the Cochrane Collaboration Back Review Group.�Spine.�2005;30:2153�2163. doi: 10.1097/01.brs.0000182227.33627.15.�[PubMed]�[Cross Ref]
89.�Hides JA, Jull GA, Richardson CA. Long-term effects of specific stabilizing exercises for first-episode low back pain.�Spine.�2001;26:E243�E248. doi: 10.1097/00007632-200106010-00004.�[PubMed][Cross Ref]
90.�Hilde G, Hagen KB, Jamtvedt G (2003) Advice to stay active as a single treatment for low back pain and sciatica (Cochrane Review). In: The Cochrane Library, Issue 1. Update Software, Oxford�[PubMed]
91.�Hildebrandt VH, Proper KI, van den BR, Douwes M, Heuvel SG, Buuren S. Cesar therapy is temporarily more effective in patients with chronic low back pain than the standard treatment by family practitioner: randomized, controlled and blinded clinical trial with 1 year follow-up [Dutch]�Ned Tijdschr Geneesk.�2000;144:2258�2264.�[PubMed]
92.�Hindle T. Comparison of carisoprodol, butabarbital, and placebo in treatment of the low back syndrome.�Calif Med.�1972;117:7�11.�[PMC free article]�[PubMed]
93.�Hofstee DJ, Gutenbeek JMM, Hoogland PH, Houwelingen HC, Kloet A, L�tters F, Tans JTJ. Westeinde sciatica trial: randomized controlled study of bed rest and physiotherapy for acute sciatica.�J Neurosurg.�2002;96:45�49.�[PubMed]
94.�Hsieh CJ, Phillips RB, Adams AH, Pope MH. Functional outcomes of low back pain: comparison of four treatment groups in a randomized controlled trial.�J Manipulative Physiol Ther.�1992;15:4�9.[PubMed]
95.�Hurri H. The Swedish back school in chronic low-back pain. Part I. Benefits.�Scand J Rehabil Med.�1989;21:33�40.�[PubMed]
96.�Indahl A, Velund L, Reikeraas O. Good prognosis for low back pain when left untampered. A randomized clinical trial.�Spine.�1995;20:473�477.�[PubMed]
97.�Indahl A, Haldorsen EH, Holm S, Reikeras O, Ursin H. Five-year follow-up study of a controlled clinical trial using light mobilization and an informative approach to low back pain.�Spine.�1998;23:2625�2630. doi: 10.1097/00007632-199812010-00018.�[PubMed]�[Cross Ref]
98.�Jacobs JH, Grayson MF. Trial of anti-inflammatory agent (indomethacin) in low back pain with and without redicular involvement.�Br Med J.�1968;3:158�160.�[PMC free article]�[PubMed]
99.�Jenkins DG, Ebbutt AF, Evans CD. Tofranil in the treatment of low back pain.�J Int Med Res.�1976;4:28�40.�[PubMed]
100.�J�ckel WH, Cziske R, Gerdes N, Jacobi E. �berpr�fung der Wirksamkeit station�rer Rehabilitationsma�nahmen bei Patienten mit chronishen Kreuzschmerzen: eine prospective randomisierte, kontrollierte Studie.�Rehabilitation.�1990;29:129�133.�[PubMed]
101.�Kankaanpaa M, Taimela S, Airaksinen O, Hanninen O. The efficacy of active rehabilitation in chronic low back pain. Effect on pain intensity, self-experienced disability, and lumbar fatigability.�Spine.�1999;24:1034�1042. doi: 10.1097/00007632-199905150-00019.�[PubMed]�[Cross Ref]
102.�Katz N, Ju WD, Krupa DA. Efficacy and safety of rofecoxib in patients with chronic low back pain: results from two 4-week, randomised, placebo-controlled, parallel-group. Double-blind trials.�Spine.�2003;28:851�859. doi: 10.1097/00007632-200305010-00002.�[PubMed]�[Cross Ref]
103.�Keijsers JFEM, Groenman NH, Gerards FM, Oudheusden E, Steenbakkers M. A back school in the Netherlands: evaluating the results.�Patient Educ Couns.�1989;14:31�44. doi: 10.1016/0738-3991(89)90005-0.�[PubMed]�[Cross Ref]
104.�Keijsers JFME, Steenbakkers WHL, Meertens RM, Bouter LM, Kok GJ. The efficacy of the back school: a randomized trial.�Arthritis Care Res.�1990;3:204�209.
105.�Klaber Moffett JA, Chase SM, Portek I, Ennis JR. A controlled prospective study to evaluate the effectiveness of a back school in the relief of chronic low-back pain.�Spine.�1986;11:120�122. doi: 10.1097/00007632-198603000-00003.�[PubMed]�[Cross Ref]
106.�Klaber Moffett J, Torgerson D, Bell-Syer S, Jackson D, Llewlyn-Phillips H, Farrin A. Randomised controlled trial of exercise for low back pain: clinical outcomes, costs, and preferences.�Br Med J.�1999;319:279�283.�[PMC free article]�[PubMed]
107.�Klinger N, Wilson R, Kanniainen C., Wagenknecht K, Re O, Gold R. Intravenous orphenadrine for the treatment of lumbar paravertebral muscle strain.�Curr Ther Res.�1988;43:247�254.
108.�Koes BW, Bouter LM, Mameren H, Essers AHM, Verstegen CMJR, Hofhuizen DM, Houben JP, Knipschild PG. Randomised clinical trial of manual therapy and physiotherapy for persistent back and neck complaints: results of one year follow-up.�Br Med J.�1992;304:601�605.�[PMC free article]�[PubMed]
109.�Koes BW, Tulder MW, Ostelo R, Kim Burton A, Waddell G. Clinical guidelines for the management of low back pain in primary care: an international comparison.�Spine.�2001;26:2504�2513. doi: 10.1097/00007632-200111150-00022.�[PubMed]�[Cross Ref]
110.�Konrad K, Tatrai T, Hunka A, Vereckei E, Korondi L. Controlled trial of balneotherapy in treatment of low back pain.�Ann Rheum Dis.�1992;51:820�822. doi: 10.1136/ard.51.6.820.�[PMC free article][PubMed]�[Cross Ref]
111.�Kuukkanen TM, Malkia EA. An experimental controlled study on postural sway and therapeutic exercise in subjects with low back pain.�Clin Rehabil.�2000;14:192�202. doi: 10.1191/026921500667300454.�[PubMed]�[Cross Ref]
112.�Lacey PH, Dodd GD, Shannon DJ. A double-blind placebo controlled study of piroxicam in the management of acute musculoskeletal disorders.�Eur J Rheumatol Inflamm.�1984;7:95�104.�[PubMed]
113.�Lankhorst GJ, Stadt RJ, Vogelaar TW, Korst JK, Prevo AJH. The effect of the Swedish back school in chronic idiopathic low-back pain.�Scand J Rehabil Med.�1983;15:141�145.�[PubMed]
114.�Larsson U, Ch�ler U, Lindstr�m A. Auto-traction for treatment of lumbago-sciatica. A multicenter controlled investigation.�Acta Orthop Scand.�1980;51:791�798. doi: 10.3109/17453678008990875.[PubMed]�[Cross Ref]
115.�Leclaire R, Esdaile JM, Suissa S, Rossignol M, Proulx R, Dupuis M. Back school in a first episode of compensated acute low back pain: a clinical trial to assess efficacy and prevent relapse.�Arch Phys Med Rehabil.�1996;77:673�679. doi: 10.1016/S0003-9993(96)90007-6.�[PubMed]�[Cross Ref]
116.�Lepisto P. A comparative trial of dS 103-282 and placebo in the treatment of acute skeletal muscle spasms due to disorders of the back.�Ther Res.�1979;26:454�459.
117.�Letchuman R, Deusinger RH. Comparison of sacrospinalis myoelectric activity and pain levels in patients undergoing static and intermittent lumbar traction.�Spine.�1993;18:1361�1365. doi: 10.1097/00007632-199308000-00017.�[PubMed]�[Cross Ref]
118.�Lidstrom A, Zachrisson M. Physical therapy on low back pain and sciatica.�Scand J Rehabil Med.�1970;2:37�42.�[PubMed]
119.�Lindequist SL, Lundberg B, Wikmark R, Bergstad B, Loof G, Ottermark AC. Information and regime at low-back pain.�Scand J Rehabil Med.�1984;16:113�116.�[PubMed]
120.�Lindstrom I, Ohlund C, Eek C, Wallin L, Peterson LE, Fordyce WE. The effect of graded activity on patients with subacute low back pain: a randomized prospective clinical study with an operant-conditioning behavioural approach.�Phys Ther.�1992;72:279�293.�[PubMed]
121.�Linton SJ, Bradley LA, Jensen I, Spangfort E, Sundell L. The secondary prevention of low back pain: a controlled study with follow-up.�Pain.�1989;36:197�207. doi: 10.1016/0304-3959(89)90024-9.�[PubMed][Cross Ref]
122.�Ljunggren E, Weber H, Larssen S. Autotraction versus manual traction in patients with prolapsed lumbar intervertebral discs.�Scand J Rehabil Med.�1984;16:117�124.�[PubMed]
123.�Loisel P, Abenhaim L, Durand P, Esdaile J, Suissa S, Gosselin L, Simard R, Turcotte J, Lemaire J. A population-based, randomized clinical trial on back pain management.�Spine.�1997;22:2911�2918. doi: 10.1097/00007632-199712150-00014.�[PubMed]�[Cross Ref]
124.�L�nn JH, Glomsr�d B, Soukup MG, B� K, Larsen S. Active back school: prophylactic management for low back pain. A randomized controlled 1-year follow-up study.�Spine.�1999;24:865�871. doi: 10.1097/00007632-199905010-00006.�[PubMed]�[Cross Ref]
126.�McGill SM. Abdominal belts in industry: a position paper on their assets, liabilities and use.�Am Ind Hyg Assoc.�1993;54:752�754.�[PubMed]
127.�Malmivaara A, H�kkinen U, Aro T, Heinrichs M-L, Koskenniemi L, Kuosma E, Lappi S, Paloheimo R, Servo C, Vaaranen V, Hernberg S. The treatment of acute low back pain�bed rest, exercises, or ordinary activity.�N Eng J Med.�1995;332:351�355. doi: 10.1056/NEJM199502093320602.�[PubMed][Cross Ref]
128.�Marchand S, Charest J, Li J, Chenard JR, Lavignolle B, Laurencelle L. Is TENS purely a placebo effect? A controlled study on chronic low back pain.�Pain.�1993;54:99�106. doi: 10.1016/0304-3959(93)90104-W.�[PubMed]�[Cross Ref]
129.�Mathews JA, Hickling J. Lumbar traction: a double-blind controlled study for sciatica.�Rheumatol Rehabil.�1975;14:222�225. doi: 10.1093/rheumatology/14.4.222.�[PubMed]�[Cross Ref]
130.�Mathews JA, Mills SB, Jenkins VM. Back pain and sciatica: controlled trials of manipulation, traction, sclerosant and epidural injections.�Br J Rheumatol.�1987;26:416�423. doi: 10.1093/rheumatology/26.6.416.�[PubMed]�[Cross Ref]
131.�Mathews W, Morkel M, Mathews J. Manipulation and traction for lumbago and sciatica: physiotherapeutic techniques used in two controlled trials.�Physiother Pract.�1988;4:201�206.
132.�Mellin G, Hurri H, H�rk�p�� K, J�rvikoski A. A controlled study on the outcome of inpatient and outpatient treatment of low back pain. Part II.�Scand J Rehabil Med.�1989;21:91�95.�[PubMed]
133.�Mellin G, H�rk�p�� K, Hurri H, J�rvikoski A. A controlled study on the outcome of inpatient and outpatient treatment of low back pain. Part IV.�Scand J Rehabil Med.�1990;22:189�194.�[PubMed]
134.�Milgrom C, Finestone A, Lev B, Wiener M, Floman Y. Overexertional lumbar and thoracic back pain among recruits: a prospective study of risk factors and treatment regimens.�J Spinal Disord.�1993;6:187�193. doi: 10.1097/00002517-199306030-00001.�[PubMed]�[Cross Ref]
135.�Milne S, Welch V, Brosseau L (2004) Transcutaneous electrical nerve stimulation (TENS) for chronic low back pain. In: The Cochrane Library, Issue 4. Update Software, Oxford
136.�Mitchell RI, Carmen GM. The functional restoration approach to the treatment of chronic pain in patients with soft tissue and back injuries.�Spine.�1994;19:633�642. doi: 10.1097/00007632-199403001-00001.�[PubMed]�[Cross Ref]
137.�Moll W. Zur therapie akuter lumbovertebraler syndrome durch optimale medikamentose muskelrelaxation mittels diazepam.�Med Welt.�1973;24:1747�1751.�[PubMed]
138.�Moseley L. Combined physiotherapy and education is efficacious for chronic low back pain.�Aust J Physiother.�2002;48:297�302.�[PubMed]
139.�Newton-John TR, Spence SH, Schotte D. Cognitive�behavioural therapy versus EMG biofeedback in the treatment of chronic low back pain.�Behav Res Ther.�1995;33:691�697. doi: 10.1016/0005-7967(95)00008-L.�[PubMed]�[Cross Ref]
140.�Niemist� L, Lahtinen-Suopanki T, Rissanen P, Lindgren K-A, Sarna S, Hurri H. A randomized trial of combined manipulation, stabilizing exercises, and physician consultation compared to physician consultation alone for chronic low back pain.�Spine.�2003;28:2185�2191. doi: 10.1097/01.BRS.0000085096.62603.61.�[PubMed]�[Cross Ref]
141.�Nicholas MK, Wilson PH, Goyen J. Operant�behavioural and cognitive�behavioural treatment for chronic low back pain.�Behav Res Ther.�1991;29:225�238. doi: 10.1016/0005-7967(91)90112-G.[PubMed]�[Cross Ref]
142.�Nicholas MK, Wilson PH, Goyen J. Comparison of cognitive�behavioral group treatment and an alternative non-psychological treatment for chronic low back pain.�Pain.�1992;48:339�347. doi: 10.1016/0304-3959(92)90082-M.�[PubMed]�[Cross Ref]
143.�Nouwen A. EMG biofeedback used to reduce standing levels of paraspinal muscle tension in chronic low back pain.�Pain.�1983;17:353�360. doi: 10.1016/0304-3959(83)90166-5.�[PubMed]�[Cross Ref]
144.�Oliphant D. Safety of spinal manipulation in the treatment of lumbar disk herniations: a systematic review and risk assessment.�J Manipulative Physiol Ther.�2004;27:197�210. doi: 10.1016/j.jmpt.2003.12.023.�[PubMed]�[Cross Ref]
145.�Ongley MJ, Klein RG, Dorman TA, Eek BC, Hubert LJ. A new approach to the treatment of chronic low back pain.�Lancet.�1987;2:143�146. doi: 10.1016/S0140-6736(87)92340-3.�[PubMed]�[Cross Ref]
146.�Ostelo RW, van Tulder MW, Vlaeyen JW, Linton SJ, Morley SJ, Assendelft WJ (2005) Behavioural treatment for chronic low-back pain. In: The Cochrane Library, Issue 1. Update Software, Oxford[PubMed]
147.�Pal P, Mangion P, Hossian MA, Diffey L. A controlled trial of continuous lumbar traction in the treatment of back pain and sciatica.�Br J Rheumatol.�1986;25:181�183. doi: 10.1093/rheumatology/25.2.181.�[PubMed]�[Cross Ref]
148.�Pallay RM, Seger W, Adler JL, Ettlinger RE, Quaidoo EA, Lipetz R, O�Brien K, Mucciola L, Skalky CS, Petruschke RA, Bohidar NR, Geba GP. Etoricoxib reduced pain and disability and improved quality of life in patients with chronic low back pain: a 3 month, randomized, controlled trial.�Scand J Rheumatol.�2004;33:257�266. doi: 10.1080/03009740410005728.�[PubMed]�[Cross Ref]
149.�Penrose KW, Chook K, Stump JL. Acute and chronic effects of pneumatic lumbar support on muscular strength, flexibility, and functional impairment index.�Sports Train Med Rehabil.�1991;2:121�129.
150.�Penttinen J, Nevala-Puranen N, Airaksinen O, Jaaskelainen M, Sintonen H, Takala J. Randomized controlled trial of back school with and without peer support.�J Occup Rehabil.�2002;12:21�29. doi: 10.1023/A:1013594103133.�[PubMed]�[Cross Ref]
151.�Pheasant H, Bursk A, Goldfarb J, Azen SP, Weiss JN, Borelli L. Amitriptyline and chronic low back pain: a randomised double-blind crossover study.�Spine.�1983;8:552�557. doi: 10.1097/00007632-198307000-00012.�[PubMed]�[Cross Ref]
152.�Postacchini F, Facchini M, Palieri P. Efficacy of various forms of conservative treatment in low-back pain. A comparative study�. Neuro-Orthopedics.�1988;6:28�35.
153.�Pratzel HG, Alken R-G, Ramm S. Efficacy and tolerance of repeated oral doses of tolperisone hydrochloride in the treatment of painful reflex muscle spasm: results of a prospective placebo-controlled double-blind trial.�Pain.�1996;67:417�425. doi: 10.1016/0304-3959(96)03187-9.�[PubMed]�[Cross Ref]
154.�Preyde M. Effectiveness of massage therapy for subacute low-back pain: a randomized controlled trial.�Can Med Assoc J.�2000;162:1815�1820.�[PMC free article]�[PubMed]
155.�Rasmussen GG. Manipulation in treatment of low back pain: a randomized clinical trial.�Man Med.�1979;1:8�10.
156.�Rasmussen-Barr E, Nilsson-Wikmar L, Arvidsson I. Stabilizing training compared with manual treatment in sub-acute and chronic low-back pain.�Man Ther.�2003;8:233�241. doi: 10.1016/S1356-689X(03)00053-5.�[PubMed]�[Cross Ref]
157.�Reust P, Chantraine A, Vischer TL. Traitement par tractions mecaniques des lombosciatalgies avec ou sans d�ficit neurologique.�Schweiz Med Wochenschr.�1988;118:271�274.�[PubMed]
158.�Risch SV, Norvell NK, Pollock Ml, Risch ED, Langer H, Fulton M. Lumbar strengthening in chronic low back pain patients: physiologic and psychological benefits.�Spine.�1993;18:232�238. doi: 10.1097/00007632-199302000-00010.�[PubMed]�[Cross Ref]
159.�Rozenberg S, Delval C, Rezvani Y. Bed rest or normal activity for patients with acute low back pain: a randomized controlled trial.�Spine.�2002;27:1487�1493. doi: 10.1097/00007632-200207150-00002.[PubMed]�[Cross Ref]
160.�Sackett D (1997) Evidence based medicine. Churchill Livingstone
161.�Salerno SM, Browning R, Jackson JL. The effect of antidepressant treatment in chronic back pain: a meta-analysis.�Arch Intern Med.�2002;162:19�24. doi: 10.1001/archinte.162.1.19.�[PubMed]�[Cross Ref]
162.�Salzmann E, Pforringer W, Paal G, Gierend M. Treatment of chronic low-back syndrome with tetrazepam in a placebo controlled double-blind trial.�J Drug Dev.�1992;4:219�228.
163.�Schonstein E, Kenny D, Keating J, Koes B, Herbert RD. Physical conditioning programs for workers with back and neck pain: a Cochrane systematic review.�Spine.�2003;28:E391�E395. doi: 10.1097/01.BRS.0000092482.76386.97.�[PubMed]�[Cross Ref]
164.�Serferlis T, Lindholm L, Nemeth G. Cost-minimization analysis of three conservative treatment programmes in 180 patients sick-listed for acute low-back pain.�Scand J Prim Health Care.�2000;18:53�57. doi: 10.1080/02813430050202578.�[PubMed]�[Cross Ref]
165.�Silverstein FE, Faich G, Goldstein JL, Simon LS, Pincus T, Whelton A, Makuch R, Eisen G, Agrawal NM, Stenson WF, Burr AM, Zhao WW, Kent JD, Lefkowith JB, Verburg KM, Geis GS. Gastrointestinal toxicity with celecoxib vs nonsteroidal anti-inflammatory drugs for osteoarthritis and rheumatoid arthritis: the CLASS study. A randomized controlled trial. Celecoxib long-term arthritis safety study.�JAMA.�2000;284:1247�1255. doi: 10.1001/jama.284.10.1247.�[PubMed]�[Cross Ref]
166.�Skargren EI, Oberg BE, Carlsson PG, Gade M. Cost and effectiveness analysis of chiropractic and physiotherapy treatment for low back and neck pain.�Six-month follow-up. Spine.�1997;22:2167�2177.[PubMed]
167.�Soukup MG, Glomsrod B, Lonn JH, Bo K, Larsen S, Fordyce WE. The effect of a Mensendieck exercise program as secondary prophylaxis for recurrent low back pain: a randomized, controlled trial with 12-month follow-up.�Spine.�1999;24:1585�1592. doi: 10.1097/00007632-199908010-00013.�[PubMed][Cross Ref]
168.�Soukup M, Lonn J, Glomsrod B, Bo K, Larsen S. Exercises and education as secondary prevention for recurrent low back pain.�Physiother Res Int.�2001;6:27�39. doi: 10.1002/pri.211.�[PubMed]�[Cross Ref]
169.�Staal JB, Hlobil H, Twisk JWR, Smid T, K�ke AJA. Graded activity for low back pain in occupational health care: a randomized controlled trial.�Ann Intern Med.�2004;140:77�84.�[PubMed]
170.�Staiger O, Barak G, Sullivan MD, Deyo RA. Systematic review of antidepressants in the treatment of chronic low back pain.�Spine.�2003;28:2540�2545. doi: 10.1097/01.BRS.0000092372.73527.BA.[PubMed]�[Cross Ref]
171.�Stankovic R, Johnell O. Conservative treatment of acute low back pain. A prospective randomized trial: McKenzie method of treatment versus patient education in �Mini Back School��Spine.�1990;15:120�123. doi: 10.1097/00007632-199002000-00014.�[PubMed]�[Cross Ref]
172.�Stankovic R, Johnell O. Conservative treatment of acute low-back pain: a 5-year follow-up study of two methods of treatment.�Spine.�1995;20:469�472. doi: 10.1097/00007632-199502001-00010.�[PubMed][Cross Ref]
173.�Storheim K, Brox JI, Holm I, Koller AK, Bo K. Intensive group training versus cognitive intervention in sub-acute low back pain: short-term results of a single-blind randomized controlled trial.�J Rehabil Med.�2003;35:132�140. doi: 10.1080/16501970310010484.�[PubMed]�[Cross Ref]
174.�Stuckey SJ, Jacobs A, Goldfarb J. EMG biofeedback training, relaxation training, and placebo for the relief of chronic back pain.�Percept Mot Skills.�1986;63:1023�1036.�[PubMed]
175.�Sweetman BJ, Baig A, Parsons DL. Mefenamic acid, chlormezanone-paracetamol, ethoheptazine-aaspirin-meprobamate: a comparative study in acute low back pain.�Br J Clin Pract.�1987;41:619�624.[PubMed]
176.�Sweetman BJ, Heinrich I, Anderson JAD. A randomized controlled trial of exercises, short wave diathermy, and traction for low back pain, with evidence of diagnosis-related response to treatment.�J Ortho Rheumatol.�1993;6:159�166.
177.�Szpalski M, Hayez JP. How many days of bed rest for acute low back pain? Objective assessment of trunk function.�Eur Spine J.�1992;1:29�31. doi: 10.1007/BF00302139.�[PubMed]�[Cross Ref]
178.�Szpalski M, Hayez JP. Objective functional assessment of the efficacy of tenoxicam in the treatment of acute low back pain: a double blind placebo-controlled study.�Br J Rheumatol.�1994;33:74�78. doi: 10.1093/rheumatology/33.1.74.�[PubMed]�[Cross Ref]
179.�Tesio L, Merlo A. Autotraction versus passive traction: an open controlled study in lumbar disc herniation.�Arch Phys Med Rehabil.�1993;74:871�876. doi: 10.1016/0003-9993(93)90015-3.�[PubMed][Cross Ref]
180.�Topol EJ. Failing the public health�rofecoxib, Merck, and the FDA.�N Engl J Med.�2004;351:1707�1709. doi: 10.1056/NEJMp048286.�[PubMed]�[Cross Ref]
181.�Torstensen TA, Ljunggren AE, Meen HD, Odland E, Mowinckel P, Geijerstam SA. Efficiency and costs of medical exercise therapy, conventional physiotherapy, and self-exercise in patients with chronic low back pain: a pragmatic, randomized, single-blinded, controlled trial with 1-year follow-up.�Spine.�1998;23:2616�2624. doi: 10.1097/00007632-199812010-00017.�[PubMed]�[Cross Ref]
182.�Triano JJ, McGregor M, Hondras MA, Brennan PC. Manipulative therapy versus education in chronic low back pain.�Spine.�1995;20:948�955. doi: 10.1097/00007632-199504150-00013.�[PubMed]�[Cross Ref]
183.�Turner JA. Comparison of group progressive-relaxation training and cognitive�behavioral group therapy for chronic low back pain.�J Consult Clin Psychol.�1982;50:757�765. doi: 10.1037/0022-006X.50.5.757.�[PubMed]�[Cross Ref]
184.�Turner JA, Clancy S. Comparison of operant�behavioral and cognitive�behavioral group treatment for chronic low back pain.�J Consult Clin Psychol.�1988;56:261�266. doi: 10.1037/0022-006X.56.2.261.[PubMed]�[Cross Ref]
185.�Turner JA, Jensen MP. Efficacy of cognitive therapy for chronic low back pain.�Pain.�1993;52:169�177. doi: 10.1016/0304-3959(93)90128-C.�[PubMed]�[Cross Ref]
186.�Turner JA, Clancy S, McQuade KJ, Cardenas DD. Effectiveness of behavioral therapy for chronic low back pain: a component analysis.�J Consult Clin Psychol.�1990;58:573�579. doi: 10.1037/0022-006X.58.5.573.�[PubMed]�[Cross Ref]
187.�Underwood MR, Morgan J. The use of a back class teaching extension exercises in the treatment of acute low back pain in primary care.�Fam Pract.�1998;15:9�15. doi: 10.1093/fampra/15.1.9.�[PubMed][Cross Ref]
188.�Valle-Jones JC, Walsh H, O�Hara J, O�Hara H, Davey NB, Hopkin-Richards H. Controlled trial of a back support in patients with non-specific low back pain.�Curr Med Res Opin.�1992;12:604�613.[PubMed]
189.�Heijden GJMG, Beurskens AJHM, Dirx MJM, Bouter LM, Lindeman E. Efficacy of lumbar traction: a randomised clinical trial.�Physiotherapy.�1995;81:29�35. doi: 10.1016/S0031-9406(05)67032-0.[Cross Ref]
190.�Tulder MW, Scholten RJPM, Koes BW, Deyo RA. Non-steroidal anti-inflammatory drugs for low back pain: a systematic review within the framework of the Cochrane Collaboration.�Spine.�2000;25:2501�2513. doi: 10.1097/00007632-200010010-00013.�[PubMed]�[Cross Ref]
191.�Tulder M, Furlan A, Bombardier C, Bouter L. Updated method guidelines for systematic reviews in the Cochrane Collaboration Back Review Group.�Spine.�2003a;28:1290�1299. doi: 10.1097/00007632-200306150-00014.�[PubMed]�[Cross Ref]
192.�Tulder MW, Touray T, Furlan AD, Solway S, Bouter LM. Muscle relaxants for nonspecific low back pain: a systematic review within the framework of the Cochrane Collaboration.�Spine.�2003b;28:1978�1992. doi: 10.1097/01.BRS.0000090503.38830.AD.�[PubMed]�[Cross Ref]
193.�Tulder M, Furlan A, Gagnier J. Complementary and alternative therapies for low back pain.�Ballieres Best Pract Rheumatol.�2005;19:639�654. doi: 10.1016/j.berh.2005.03.006.�[PubMed]�[Cross Ref]
194.�Videman T, Heikkila J, Partanen T. Double-blind parallel study of meptazinol versus diflunisal in the treatment of lumbago.�Curr Med Res Opin.�1984;9:246�252.�[PubMed]
195.�Vollenbroek-Hutten MMR, Hermens HJ, Wever D, Gorter M, Rinket J, IJzerman MJ. Differences in outcome of a multidisciplinary treatment between subgroups of chronic low back pain patients defined using two multiaxial assessment instruments: the multidimensional pain inventory and lumbar dynamometry.�Clin Rehabil.�2004;18:566�579. doi: 10.1191/0269215504cr772oa.�[PubMed]�[Cross Ref]
196.�Vroomen PJAJ, Marc CTFM, Wilmink JT, Kester ADM, Knottnerus JA. Lack of effectiveness of bed rest for sciatica.�N Engl J Med.�1999;340:418�423. doi: 10.1056/NEJM199902113400602.�[PubMed][Cross Ref]
197.�Waagen GN, Haldeman S, Cook G, Lopez D, DeBoer KF. Short term trial of chiropractic adjustments for the relief of chronic low back pain.�Manual Med.�1986;2:63�67.
198.�Waddell G. A new clinical model for the treatment of low-back pain.�Spine.�1987;12:632�644. doi: 10.1097/00007632-198709000-00002.�[PubMed]�[Cross Ref]
199.�Walker L, Svenkerud T, Weber H. Traksjonsbehandling ved lumbago-ischias. En kontrollert undersolske med Spina-trac.�Fysioterapeuten.�1982;49:161�163.
200.�Ward N, Bokan JA, Phillips M, Benedetti C, Butler S, Spengler D. Antidepressants in concomitant chronic back pain and depression: doxepin and desipramine compared.�J Clin Psychiatry.�1984;45:54�57.[PubMed]
201.�Waterworth RF, Hunter A. An open study of diflunisal, conservative and manipulative therapy in the management of acute mechanical low back pain.�N Z Med J.�1985;95:372�375.�[PubMed]
202.�Weber H. Traction therapy in sciatica due to disc prolapse.�J Oslo City Hosp.�1973;23:167�176.[PubMed]
203.�Weber H, Aasand G. The effect of phenylbutazone on patients with acute lumbago-sciatica: a double blind trial.�J Oslo City Hosp.�1980;30:69�72.�[PubMed]
204.�Weber H, Ljunggren E, Walker L. Traction therapy in patients with herniated lumbar intervertebral discs.�J Oslo City Hosp.�1984;34:61�70.�[PubMed]
205.�Weber H, Holme I, Amlie E. The natural course of acute sciatica with nerve root symptoms in a double-blind placebo-controlled trial evaluating the effect of piroxicam.�Spine.�1993;18:1433�1438. doi: 10.1097/00007632-199312000-00021.�[PubMed]�[Cross Ref]
206.�Werners R, Pynsent PB, Bulstrode CJK. Randomized trial comparing interferential therapy with motorized lumbar traction and massage in the management of low back pain in a primary care setting.�Spine.�1999;24:1579�1584. doi: 10.1097/00007632-199908010-00012.�[PubMed]�[Cross Ref]
207.�Wiesel SW, Cuckler JM, Deluca F, Jones F, Zeide MS, Rothman RH. Acute low back pain: an objective analysis of conservative therapy.�Spine.�1980;5:324�330. doi: 10.1097/00007632-198007000-00006.�[PubMed]�[Cross Ref]
208.�Wilkinson MJ. Does 48 hours� bed rest influence the outcome of acute low back pain?�Br J Gen Pract.�1995;45:481�484.�[PMC free article]�[PubMed]
209.�W�rz R, Bolten W, Heller J, Krainick U, Pergande G. Flupirtin im vergleich zu chlormezanon und placebo bei chronische muskuloskelettalen ruckenschmerzen.�Fortschritte der Therapie.�1996;114(35�36):500�504.�[PubMed]
210.�Wreje U, Nordgren B, Aberg H. Treatment of pelvic joint dysfunction in primary care�a controlled study.�Scand J Prim Health Care.�1992;10:310�315. doi: 10.3109/02813439209014080.�[PubMed][Cross Ref]
211.�Yelland MJ, Glasziou PP, Bogduk N, Schluter PJ, McKernon M. Prolotherapy injections, saline injections, and exercises for chronic low-back pain: a randomized trial.�Spine.�2004;29:9�16. doi: 10.1097/01.BRS.0000105529.07222.5B.�[PubMed]�[Cross Ref]
212.�Zachrisson Forsell M. The back school.�Spine.�1981;6:104�106. doi: 10.1097/00007632-198101000-00022.�[PubMed]�[Cross Ref]
213.�Zylbergold RS, Piper MC. Lumbar disc disease: comparative analysis of physical therapy treatments.�Arch Phys Med Rehabil.�1981;62:176�179.�[PubMed]
Understanding clinical and experimental evidence,�manual therapies, or manipulative therapies, are physical treatments that utilize skilled, hands-on techniques, such as manipulation and/or mobilization, used by a physical therapist, among other healthcare professionals, to diagnose and treat a variety of musculoskeletal and non-musculoskeletal injuries and conditions. Spinal manipulation/mobilization has been determined to be effective for back pain, neck pain, headache and migraine, as well as for several types of joint pain, including various other disorders in adults.
For additional notice, the following research study is a comprehensive summary of the scientific evidence regarding the effectiveness of manual therapies for the management of a variety of musculoskeletal and non-musculoskeletal injuries and conditions. The conclusions are based on the results of randomized clinical trials, widely accepted and primarily UK and United States evidence-based guidelines and the results of other randomized clinical trials not yet included.
Background
The impetus for this report stems from the media debate in the United Kingdom (UK) surrounding the scope of chiropractic care and claims regarding its effectiveness particularly for non-musculoskeletal conditions.
The domain of evidence synthesis is always embedded within the structure of societal values. What constitutes evidence for specific claims is framed by the experience, knowledge, and standards of communities. This varies substantially depending on jurisdictional restrictions by country and region. However, over the last several decades a strong international effort has been made to facilitate the systematic incorporation of standardized synthesized clinical research evidence into health care decision making.
Evidence-Based Healthcare (EBH)
EBH is about doing the right things for the right people at the right time. It does so by promoting the examination of best available clinical research evidence as the preferred process of decision making where higher quality evidence is available. This reduces the emphasis on unsystematic clinical experience and pathophysiological rationale alone while increasing the likelihood of improving clinical outcomes. The fact that randomized clinical trial (RCT) derived evidence of potentially effective interventions in population studies may not be translated in a straight forward manner to the management of individual cases is widely recognized. However, RCTs comprise the body of information best able to meet existing standards for claims of benefit from care delivery. The evidence provided by RCTs constitutes the first line of recommended action for patients and contributes, along with informed patient preference, in guiding care. Practice, as opposed to claims, is inherently interpretative within the context of patient values and ethical defensibility of recommendations. Indeed, the need to communicate research evidence, or its absence, to patients for truly informed decision-making has become an important area of health care research and clinical practice.
While some may argue that EBH is more science than art, the skill required of clinicians to integrate research evidence, clinical observations, and patient circumstances and preferences is indeed artful. It requires creative, yet informed improvisation and expertise to balance the different types of information and evidence, with each of the pieces playing a greater or lesser role depending on the individual patient and situation.
It has become generally accepted that providing evidence-based healthcare will result in better patient outcomes than non-evidence-based healthcare. The debate of whether or not clinicians should embrace an evidence-based approach has become muted. Put simply by one author: “…anyone in medicine today who does not believe in it (EBH) is in the wrong business.” Many of the criticisms of EBH were rooted in confusion over what should be done when good evidence is available versus when evidence is weak or nonexistent. From this, misunderstandings and misperceptions arose, including concerns that EBH ignores patient values and preferences and promotes a cookbook approach. When appropriately applied, EBH seeks to empower clinicians so they can develop fact-based independent views regarding healthcare claims and controversies. Importantly, it acknowledges the limitations of using scientific evidence alone to make decisions and emphasizes the importance of patients’ values and preferences in clinical decision making.
The question is no longer “should” we embrace EBH but “how”? With EBH comes the need for new skills including: efficient literature search strategies and the application of formal rules of evidence in evaluating the clinical literature. It is important to discern the role of the health care provider as an advisor who empowers informed patient decisions. This requires a healthy respect for which scientific literature to use and how to use it. “Cherry-picking” only those studies which support one’s views or relying on study designs not appropriate for the question being asked does not promote doing the right thing for the right people at the right time.
Perhaps most critical is the clinician’s willingness to change the way they practice when high quality scientific evidence becomes available. It requires flexibility born of intellectual honesty that recognizes one’s current clinical practices may not�really�be in the best interests of the patient. In some cases this will require the abandonment of treatment and diagnostic approaches once believed to be helpful. In other cases it will require the acceptance and training in new methods. The ever-evolving scientific knowledge base demands that clinicians be accepting of the possibility that what is “right” today might not be “right” tomorrow. EBH requires that clinicians’ actions are influenced by the evidence. Importantly a willingness to change must accompany the ability to keep up to date with the constant barrage of emerging scientific evidence.
Purpose
The purpose of this report is to provide a brief and succinct summary of the scientific evidence regarding the effectiveness of manual treatment as a therapeutic option for the management of a variety of musculoskeletal and non-musculoskeletal conditions based on the volume and quality of the evidence. Guidance in translating this evidence to application within clinical practice settings is presented.
Methods
For the purpose of this report, manual treatment includes spinal and extremity joint manipulation or mobilization, massage and various soft tissue techniques. Manipulation/mobilization under anaesthesia was not included in the report due to the procedure’s invasive nature. The conclusions of the report are based on the results of the most recent and most updated (spans the last five to ten years) systematic reviews of RCTs, widely accepted evidence-based clinical guidelines and/or technology assessment reports (primarily from the UK and US if available), and all RCTs not yet included in the first three categories. While critical appraisal of the included reviews and guidelines would be ideal, it is beyond the scope of the present report. The presence of discordance between the conclusions of systematic reviews is explored and described. The conclusions regarding effectiveness are based on comparisons with placebo controls (efficacy) or commonly used treatments which may or may not have been shown to be effective (relative effectiveness), as well as comparison to no treatment. The strength/quality of the evidence relating to the efficacy/effectiveness of manual treatment is graded according to an adapted version of the latest grading system developed by the US Preventive Services Task Force (see�http://www.ahrq.gov/clinic/uspstf/grades.htm). The evidence grading system used for this report is a slight modification of the system used in the 2007 Joint Clinical Practice Guideline on low back pain from the American College of Physicians and the American Pain Society.
Through a search strategy using the databases MEDLINE (PubMed), Ovid, Mantis, Index to Chiropractic Literature, CINAHL, the specialized databases Cochrane Airways Group trial registry, Cochrane Complementary Medicine Field, and Cochrane Rehabilitation Field, systematic reviews and RCTs as well as evidence-based clinical guidelines were identified. Search restrictions were human subjects, English language, peer-reviewed and indexed journals, and publications before October 2009. In addition, we screened and hand searched reference citations located in the reviewed publications. The description of the search strategy is provided in Additional file�1�(Medline search strategy).
Although findings from studies using a nonrandomized design (for example observational studies, cohort studies, prospective clinical series and case reports) can yield important preliminary evidence, the primary purpose of this report is to summarize the results of studies designed to address efficacy, relative efficacy or relative effectiveness and therefore the evidence base was restricted to RCTs. Pilot RCTs not designed or powered to assess effectiveness, and RCTs designed to test the immediate effect of individual treatment sessions were not part of the evidence base in this report.
The quality of RCTs, which have not been formally quality-assessed within the context of systematic reviews or evidence based guidelines, was assessed by two reviewers with a scale assessing the risk of bias recommended for use in Cochrane systematic reviews of RCTs. Although the Cochrane Collaboration handbook�http://www.cochrane.org/resources/handbook/�discourages that scoring be applied to the risk of bias tool, it does provide suggestion for how trials can be summarized. We have been guided by that suggestion and the adapted evidence grading system used in this report requires that we assess the validity and impact of the latest trial evidence. These additional trials are categorized as higher, moderate, or lower-quality as determined by their attributed risk of bias. For details, see Additional file�2�(The Cochrane Collaboration tool for assessing risk of bias and the rating of the bias for the purpose of this report).
The overall evidence grading system allows the strength of the evidence to be categorized into one of three categories:�high quality evidence, moderate quality evidence, and inconclusive (low quality) evidence. The operational definitions of these three categories follow below:
High quality evidence
The available evidence usually includes consistent results from well-designed, well conducted studies in representative populations which assess the effects on health outcomes.
The evidence is based on at least two consistent higher-quality (low risk of bias) randomized trials. This conclusion is therefore unlikely to be strongly affected by the results of future studies.
Moderate quality evidence
The available evidence is�sufficient�to determine the effectiveness relative to health outcomes, but confidence in the estimate is constrained by such factors as:
� The number, size, or quality of individual studies.
� Inconsistency of findings across individual studies.
� Limited generalizability of findings to routine practice.
� Lack of coherence in the chain of evidence.
The evidence is based on at least one higher-quality randomized trial (low risk of bias) with sufficient statistical power, two or more higher-quality (low risk of bias) randomized trials with some inconsistency; at least two consistent, lower-quality randomized trials (moderate risk of bias). As more information becomes available, the magnitude or direction of the observed effect could change, and this change may be large enough to alter the conclusion.
Inconclusive (low quality) evidence
The available evidence is�insufficient�to determine effectiveness relative to health outcomes. Evidence is insufficient because of:
� The limited number or power of studies.
� Important flaws in study design or methods (only high risk of bias studies available).
� Unexplained inconsistency between higher-quality trials.
� Gaps in the chain of evidence.
� Findings not generalizable to routine practice.
� Lack of information on important health outcomes
For the purpose of this report a determination was made whether the inconclusive evidence appears favorable or non-favorable or if a direction could even be established (unclear evidence).
Additionally, brief evidence statements are made regarding other non-pharmacological, non-invasive physical treatments (for example exercise) and patient educational interventions, shown to be effective and which can be incorporated into evidence-based therapeutic management or co-management strategies in chiropractic practices. These statements are based on conclusions of the most recent and most updated (within last five to ten years) systematic reviews of randomized clinical trials and widely accepted evidence-based clinical guidelines (primarily from the UK and US if available) identified through our search strategy.
Translating Evidence to Action
Translating evidence requires the communication of salient take-home messages in context of the user’s applications. There are two message applications for information derived from this work. First, the criteria for sufficiency of evidence differ depending on the context of the considered actions. Sufficient evidence to proffer claims of effectiveness is defined within the socio-political context�of ethics and regulation. Separate is the second application of evidence to inform decision making for individual patients. Where there is strength of evidence and the risk of bias is small, the preferred choices require little clinical judgment. Alternatively, when evidence is uncertain and/or there is higher risk of bias, then greater emphasis is placed on the patient as an active participant. This requires the clinician to effectively communicate research evidence to patients while assisting their informed decision-making.
In summary, the information derived within this report are directed to two applications 1) the determination of supportable public claims of treatment effectiveness for chiropractic care within the context of social values; and 2) the use of evidence information as a basis for individualized health care recommendations using the hierarchy of evidence (Figure 1).
Figure 1 Translating evidence to action.
Dr. Alex Jimenez’s Insight
The purpose of the research study was to provide substantial clinical and experimental evidence on the effectiveness of manual therapies, or manipulative therapies. Systematic reviews of randomized clinical trials, or RCTS, helped demonstrate the strength and quality of the evidence regarding the effectiveness of these, such as manipulation and/or mobilization. The results of the research study provide two additional purposes: to determine supportable public claims of treatment effectiveness for chiropractic care within the context of social values; and to utilize the information from the evidence as a basis for individualized healthcare recommendations using the hierarch of evidence. Detailed results of each research study method and conclusive outcome is recorded below regarding the effectiveness of manual therapies, including spinal manipulation and/or mobilization, among others.
Results
By September 2009, 26 categories of conditions were located containing RCT evidence for the use of manual therapy: 13 musculoskeletal conditions, four types of chronic headache and nine non-musculoskeletal conditions (Figure 2). We identified 49 recent relevant systematic reviews and 16 evidence-based clinical guidelines plus an additional 46 RCTs not yet included within the identified systematic reviews and guidelines. A number of other non-invasive physical treatments and patient education with evidence of effectiveness were identified including exercise, yoga, orthoses, braces, acupuncture, heat, electromagnetic field therapy, TENS, laser therapy, cognitive behavioral therapy and relaxation. The report presents the evidence of effectiveness or ineffectiveness of manual therapy as evidence summary statements at the end of the section for each condition and in briefer summary form in Figures 3, 4, 5, 6, and 7. Additionally, definitions and brief diagnostic criteria for the conditions reviewed are provided. Diagnostic imaging for many conditions is indicated by the presence of “red flags” suggestive of serious pathology. Red flags may vary depending on the condition under consideration, but typically include fractures, trauma, metabolic disorders, infection, metastatic disease, and other pathological disease processes contraindicative to manual therapy.
Figure 2 Categories of conditions included in this report.
Figure 3 Evidence summary of spinal conditions in adults.
Figure 4 Evidence summary of extremity conditions in adults.
Figure 5 Evidence summary of headache and other conditions in adults.
Figure 6 Evidence summary of non musculoskeletal conditions in adults.
Figure 7 Evidence summary of non musculoskeletal conditions in pediatrics.
Non-specific Low Back Pain (LBP)
Definition
Non-specific LBP is defined as soreness, tension, and/or stiffness in the lower back region for which it is not possible to identify a specific cause of pain.
Diagnosis
Diagnosis of non-specific LBP is derived from the patient’s history with an unremarkable neurological exam and no indicators of potentially serious pathology. Imaging is only indicated in patients with a positive neurological exam or presence of a “red flag”.
Evidence base for manual treatment
Systematic reviews (most recent)
Since 2004, five systematic reviews made a comprehensive evaluation of the benefit of spinal manipulation for non-specific LBP. Approximately 70 RCTs were summarized. The reviews found that spinal manipulation was superior to sham intervention and similar in effect to other commonly used efficacious therapies such as usual care, exercise, or back school. For sciatica/radiating leg pain, three reviews�found manipulation to have limited evidence. Furlan et al�concluded massage is beneficial for patients with subacute and chronic non-specific low-back pain based on a review of 13 RCTs.
Evidence-based clinical guidelines
Since 2006, four guidelines make recommendations regarding the benefits of manual therapies for the care of LBP: NICE, The American College of Physicians/American Pain Society , European guidelines for chronic LBP, and European guidelines for acute LBP. The number of RCTs included within the various guidelines varied considerably based on their scope, with the NICE guidelines including eight trials and The American College of Physicians/American Pain Society guidelines including approximately 70 trials. These guidelines in aggregate recommend spinal manipulation/mobilization as an effective treatment for acute, subacute, and chronic LBP. Massage is also recommended for the treatment of subacute and chronic LBP.
Recent randomized clinical trials not included in above
Hallegraeff et al�compared a regimen of spinal manipulation plus standard physical therapy to standard physical therapy for acute LBP. Overall there were no differences between groups for pain and disability post treatment. Prediction rules may have affected outcomes. This study had a high risk of bias.
Rasmussen et al found patients receiving extension exercise or receiving extension exercise plus spinal manipulation experienced a decrease in chronic LBP, but no differences were noted between groups. This study had a high risk of bias.
Little et al�found Alexander technique, exercise, and massage were all superior to control (normal care) at three months for chronic LBP and disability. This study had a moderate risk of bias.
Wilkey et al found chiropractic management was superior to NHS pain clinic management for chronic LBP at eight weeks for pain and disability outcomes. This study had a high risk of bias.
Bogefeldt et al found manual therapy plus advice to stay active was more effective than advice to stay active alone for reducing sick leave and improving return to work at 10 weeks for acute LBP. No differences between the groups were noted at two years. This study had a low risk of bias.
Hancock et al found spinal mobilization in addition to medical care was no more effective than medical care alone at reducing the number of days until full recovery for acute LBP. This study had a low risk of bias.
Ferreira et al found spinal manipulation was superior to general exercise for function and perceived effect at eight weeks in chronic LBP patients, but no differences were noted between groups at six and 12 months. This study had a moderate risk of bias.
Eisenberg et al found that choice of complementary therapies (including chiropractic care) in addition to usual care was no different from usual care in bothersomeness and disability for care of acute LBP. The trial did not report findings for any individual manual therapy. This study had a low risk of bias.
Hondras et al found lumbar flexion-distraction was superior to minimal medical care at 3,6,9,12, and 24 weeks for disability related to subacute or chronic LBP, but spinal manipulation was superior to minimal medical care only at three weeks. No differences between spinal manipulation and flexion-distraction were noted for any reported outcomes. Global perceived improvement was superior at 12 and 24 weeks for both manual therapies compared to minimal medical care. This study had a low risk of bias.
Mohseni-Bandpei et al showed that patients receiving manipulation/exercise for chronic LBP reported greater improvement compared with those receiving ultrasound/exercise at both the end of the treatment period and at 6-month follow-up. The study had a high risk of bias.
Beyerman et al evaluated the efficacy of chiropractic spinal manipulation, manual flexion/distraction, and hot pack application for the treatment of LBP of mixed duration from osteoarthritis (OA) compared with moist heat alone. The spinal manipulation group reported more and faster short term improvement in pain and range of motion. The study had a high risk of bias.
Poole et al showed that adding either foot reflexology or relaxation training to usual medical care in patients with chronic LBP is no more effective than usual medical care alone in either the short or long term. The study had a moderate risk of bias.
Zaproudina et al found no differences between groups (bonesetting versus exercise plus massage) at one month or one year for pain or disability. The global assessment score of improvement was superior for the bonesetting group at one month. This study had a high risk of bias.
Evidence Summary (See Figure 3)
? High quality evidence that spinal manipulation/mobilization is an effective treatment option for subacute and chronic LBP in adults.
? Moderate quality evidence that spinal manipulation/mobilization is an effective treatment option for subacute and chronic LBP in older adults.
? Moderate quality evidence that spinal manipulation/mobilization is an effective treatment option for acute LBP in adults.
? Moderate evidence that adding spinal mobilization to medical care does not improve outcomes for acute LBP in adults.
? Moderate quality evidence that massage is an effective treatment for subacute and chronic LBP in adults.
? Inconclusive evidence in a favorable direction regarding the use of manipulation for sciatica/radiating leg pain.
? Inconclusive evidence in a non-favorable direction regarding the addition of foot reflexology to usual medical care for chronic LBP.
Other effective non-invasive physical treatments or patient education
Advice to stay active, interdisciplinary rehabilitation, exercise therapy, acupuncture, yoga, cognitive-behavioral therapy, or progressive relaxation for chronic LBP and superficial heat for acute LBP.
Non-specific mid back pain
Definition
Non-specific thoracic spine pain is defined as soreness, tension, and/or stiffness in the thoracic spine region for which it is not possible to identify a specific cause of pain.
Diagnosis
Diagnosis of non-specific thoracic spine pain is derived from the patient’s history with an unremarkable neurological exam and no indicators of potentially serious pathology. Imaging is only indicated in patients with a positive neurological exam or presence of a “red flag”.
Evidence base for manual treatment
Systematic reviews (most recent)
No systematic reviews addressing the role of manual therapy in thoracic spine pain that included randomized clinical trials were located.
Evidence-based clinical guidelines
The Australian acute musculoskeletal pain guidelines group concludes there is evidence from one small pilot study that spinal manipulation is effective compared to placebo for thoracic spine pain.
Recent randomized clinical trials not included in above
Multiple randomized clinical trials investigating the use of thoracic spinal manipulation were located; however, most of the trials assessed the effectiveness of thoracic manipulation for neck or shoulder pain.
Evidence Summary (See Figure 3)
? Inconclusive evidence in a favorable direction regarding the use of spinal manipulation for mid back pain.
Other effective non-invasive physical treatments or patient education
None
Mechanical neck pain
Definition
Mechanical neck pain is defined as pain in the anatomic region of the neck for which it is not possible to identify a specific pathological cause of pain. It generally includes neck pain, with or without pain in the upper limbs which may or may not interfere with activities of daily living (Grades I and II). Signs and symptoms indicating significant neurologic compromise (Grade III) or major structural pathology (Grade IV including fracture, vertebral dislocation, neoplasm, etc.) are NOT included.
Diagnosis
Diagnosis of mechanical neck pain is derived from the patient’s history. Imaging is only indicated in patients with a positive neurological exam or presence of a “red flag”.
Evidence base for manual treatment
Systematic reviews (most recent)
The recently published best evidence synthesis by the Bone and Joint Decade 2000-2010 Task Force on Neck Pain and Its Associated Disorders represents the most recent and comprehensive systematic review of the literature for non-invasive interventions, including manual treatment, for neck pain. For whiplash associated disorders, they concluded that mobilization and exercises appear more beneficial than usual care or physical modalities. For Grades I and II neck pain, they concluded that the evidence suggests that manual treatment (including manipulation and mobilization) and exercise interventions, low-level laser therapy and perhaps acupuncture are more effective than no treatment, sham or alternative interventions. No one type of treatment was found to be clearly superior to any other. They also note that manipulation and mobilization yield comparable results. Conclusions regarding massage could not be made due to lack of evidence.
Since 2003, there were five other systematic reviews. One found that spinal manipulation was effective for non-specific neck pain alone and in combination with exercise, while two found effectiveness only for the combination of spinal manipulation and exercise. Differences between review conclusions are expected. It is likely they can be attributed to additional primary studies and diversity in review strategies, including inclusion criteria, methodological quality scoring, and evidence determination.
Evidence-based clinical guidelines
The American Physical Therapy Association’s guidelines on neck pain recommends utilizing cervical manipulation and mobilization procedures to reduce neck pain based on strong evidence.�They found cervical manipulation and mobilization with exercise to be more effective for reducing neck pain and disability than manipulation and mobilization alone. Thoracic spine manipulation is also recommended for reducing pain and disability in patients with neck and neck-related arm pain based on weak evidence.
Recent randomized clinical trials not included in above
H�kkinen et al used a cross-over design to compare manual therapy and stretching for chronic neck pain. Manual therapy was more effective than stretching at four weeks, but no difference between the two therapies was noted at 12 weeks. This study had a high risk of bias.
Gonz�lez-Iglesias et al examined the effectiveness of adding general thoracic spine manipulation to electrotherapy/thermal therapy for acute neck pain. In two separate trials they found an advantage for the manipulation group in terms of pain and disability. The trials had moderate to low risk of bias.
Walker et al compared manual therapy with exercise to advice to stay active and placebo ultrasound. The manual therapy group reported less pain (in the short term) and more improvement and less disability (in the long term) than the placebo group. This study had a low risk of bias.
Cleland et al�showed that thoracic spine thrust mobilization/manipulation results in a significantly greater short-term reduction in pain and disability than does thoracic non-thrust mobilization/manipulation in people with mostly subacute neck pain. The study had a low risk of bias.
Fernandez et al�found that adding thoracic manipulation to a physical therapy program was effective in treating neck pain due to whiplash injury. The study had a high risk of bias.
Savolainen et al�compared the effectiveness of thoracic manipulations with instructions for physiotherapeutic exercises for the treatment of neck pain in occupational health care. The effect of the manipulations was more favorable than the personal exercise program in treating the more intense phase of pain. The study had a moderate risk of bias.
Zaproudina et al�assessed the effectiveness of traditional bone setting (mobilization) of joints of extremities and the spine for chronic neck pain compared with conventional physiotherapy or massage. The traditional bone setting was superior to the other two treatments in both in the short and long term. The study had a moderate risk of bias.
Sherman et al compared massage therapy to self-care for chronic neck pain. Massage was superior to self-care at 4 weeks for both neck disability and pain. A greater proportion of massage patients reported a clinically significant improvement in disability than self-care patients at four weeks, and more massage patients reported a clinically significant improvement in pain at four and 10 weeks. No statistically significant differences between groups were noted at 26 weeks. This study had a low risk of bias.
Evidence Summary (See Figure 3)
? Moderate quality evidence that mobilization combined with exercise is effective for acute whiplash-associated disorders.
? Moderate quality evidence that spinal manipulation/mobilization combined with exercise is effective for chronic non-specific neck pain.
? Moderate quality evidence that thoracic spinal manipulation/mobilization is effective for acute/subacute non-specific neck pain.
? Moderate quality evidence that spinal manipulation is similar to mobilization for chronic non-specific neck pain.
? Moderate quality evidence that massage therapy is effective for non-specific chronic neck pain.
? Inconclusive evidence in a favorable direction for cervical spinal manipulation/mobilization alone for neck pain of any duration.
Other effective non-invasive physical treatments or patient education
Exercise, low-level laser therapy, acupuncture
Coccydynia
Definition
Coccydynia is defined as symptoms of pain in the region of the coccyx.
Diagnosis
Diagnosis of coccydynia is derived from the patient’s history and exam with no indicators of potentially serious pathology. Imaging is only indicated in patients with a presence of a “red flag”.
Evidence base for manual treatment
Systematic reviews (most recent)
None located
Evidence-based clinical guidelines
None located
Recent randomized clinical trials not included in above
Maigne et al found manipulation was more effective than placebo for pain relief and disability in the treatment of coccydynia at one month. This study had a moderate risk of bias.
Evidence Summary (See Figure 3)
? Inconclusive evidence in a favorable direction for the use of spinal manipulation in the treatment of coccydynia.
Other effective non-invasive physical treatments or patient education
None
Shoulder pain
Definition
Shoulder pain is defined as soreness, tension, and/or stiffness in the anatomical region of the shoulder and can be secondary to multiple conditions including, but not limited to rotator cuff disease and adhesive capsulitis.
Diagnosis
Diagnosis of shoulder pain is derived mainly from the patient’s history and physical exam with no indicators of potentially serious pathology. Imaging studies are confirmatory for diagnoses of rotator cuff disorders, osteoarthritis, glenohumeral instability, and other pathologic causes of shoulder pain.
Evidence base for manual treatment
Systematic reviews (most recent)
Two systematic reviews evaluated the benefit of manual therapy for shoulder pain. Six RCTs evaluating the effectiveness of manual therapy for the treatment of shoulder pain were included. Five of the trials evaluated mobilization�while one trial evaluated the use of manipulation and mobilization�for shoulder pain. The review concluded there is weak evidence that mobilization added benefit to exercise for rotator cuff disease.
Evidence-based clinical guidelines
The Philadelphia Panel’s evidence based clinical practice guidelines on selected rehabilitation interventions for shoulder pain concluded there is insufficient evidence regarding the use of therapeutic massage for shoulder pain.
Recent randomized clinical trials not included in above
Vermeulen et al�found that high-grade mobilization techniques were more effective than low-grade mobilization techniques for active range of motion (ROM), passive ROM, and shoulder disability for adhesive capsulitis at three to 12 months. No differences were noted for pain or mental and physical general health. Both groups showed improvement in all outcome measures. This study had low risk of bias.
van den Dolder and Roberts�found massage was more effective than no treatment for pain, function, and ROM over a two week period in patients with shoulder pain. This study had moderate risk of bias.
Bergman et al�found no differences between groups during the treatment period (6 wks). More patients reported being “recovered” in the usual care plus manipulative/mobilization group at 12 and 52 weeks compared to usual care alone. This study had low risk of bias.
Johnson et al�found no differences in pain or disability between anterior and posterior mobilization for the care of adhesive capsulitis. This study had a high risk of bias.
Guler-Uysal et al�concluded that deep friction massage and mobilization exercises was superior in the short term to physical therapy including diathermy for adhesive capsulitis. The study had a high risk of bias.
? Moderate quality evidence that high-grade mobilization is superior to low-grade mobilization for reduction of disability, but not for pain, in adhesive capsulitis.
? Inconclusive evidence in an unclear direction for a comparison of anterior and posterior mobilization for adhesive capsulitis.
? Moderate evidence favors the addition of manipulative/mobilization to medical care for shoulder girdle pain and dysfunction.
? Inconclusive evidence in a favorable direction for massage in the treatment of shoulder pain.
? Inconclusive evidence in a favorable direction for mobilization/manipulation in the treatment of rotator cuff pain.
Other effective non-invasive physical treatments or patient education
Exercise therapy
Lateral epicondylitis
Definition
Lateral epicondylitis is defined as pain in the region of the lateral epicondyle which is exacerbated by active and resistive movements of the extensor muscles of the forearm.
Diagnosis
Diagnosis is made solely from the patient’s history and clinical examination.
Evidence base for manual treatment
Systematic reviews (most recent)
Three systematic reviews evaluating the benefit of manual therapy for lateral epicondylitis have been identified. Eight RCTs were included�in the systematic reviews examining the effect of various manual therapies including elbow�and wrist manipulation, cervical spine�and elbow mobilization, and cross-friction massage. Bisset et al�concluded there is some evidence of positive initial effects of manual techniques (massage/mobilization) for lateral epicondylitis, but no long term evidence. Smidt et al�concluded there is insufficient evidence to draw conclusions on the effectiveness of mobilization techniques for lateral epicondylitis.
Evidence-based clinical guidelines
None located
Recent randomized clinical trials not included in above
Verhaar et al showed that corticosteroid injection was superior to Cyriax physiotherapy for the number of pain free subjects at six weeks. No differences between groups were noted at one year. This study had a high risk of bias.
Bisset et al�found corticosteroid injections were superior to elbow mobilization with exercise which was superior to wait and see approaches for pain-free grip strength, pain intensity, function, and global improvement at six weeks. However, both elbow mobilization with exercise and the wait and see approach were superior to corticosteroid injections at six months and one year for all of the previously reported outcomes. This study had a low risk of bias.
Nourbakhsh and Fearon�found oscillating energy manual therapy (tender point massage) was superior to placebo manual therapy for pain intensity and function. This study had a high risk of bias due to sample size (low risk of bias otherwise).
Evidence Summary (See Figure 4)
? Moderate quality evidence that elbow mobilization with exercise is inferior to corticosteroid injections in the short term and superior in the long term for lateral epicondylitis.
? Inconclusive evidence in a favorable direction regarding the use of manual oscillating tender point therapy of the elbow for lateral epicondylitis.
Other effective non-invasive physical treatments or patient education
Laser therapy, acupuncture
Carpal tunnel syndrome
Definition
Carpal tunnel syndrome is defined as compression of the median nerve as it passes through the carpal tunnel in the wrist.
Diagnosis
Diagnosis of carpal tunnel syndrome is made from the patient’s history, physical exam, and confirmatory electrodiagnostic tests.
Evidence base for manual treatment
Systematic reviews (most recent)
Since 2003, four systematic reviews evaluated the benefit of manual therapy for carpal tunnel syndrome. Two RCTs evaluating the effectiveness of manual therapy were included. One of the trials examined the use of spinal and upper extremity manipulation, while the other trial examined the use of wrist manipulation for carpal tunnel syndrome. The reviews concluded uncertain or limited evidence for manipulation/mobilization.
Evidence-based clinical guidelines
The American Academy of Orthopaedic Surgeons clinical practice guideline on the treatment of carpal tunnel syndrome�made no recommendations for or against the use of manipulation or massage therapy due to insufficient evidence.
Recent randomized clinical trials not included in above
None
Evidence Summary (See Figure 4)
? Inconclusive evidence in a favorable direction for manipulation/mobilization in the treatment of carpal tunnel syndrome.
Other effective non-invasive physical treatments or patient education
Splinting
Hip pain
Definition
Hip pain is defined as soreness, tension, and/or stiffness in the anatomical region of the hip and can be secondary to multiple conditions including hip osteoarthritis.
Diagnosis
Diagnosis of hip pain is derived from the patient’s history and physical exam with an unremarkable neurological exam and no indicators of potentially serious pathology. Imaging studies are confirmatory for diagnoses of moderate or severe osteoarthritis.
Evidence base for manual treatment
Systematic reviews (most recent)
One systematic review evaluating manual therapy for hip pain has been published. One RCT evaluating the effectiveness of hip manipulation for the treatment of hip osteoarthritis was included in the published systematic review. The review concluded there is limited evidence for manipulative therapy combined with multimodal or exercise therapy for hip osteoarthritis.
Evidence-based clinical guidelines
The NICE national clinical guidelines for care and management of adults with osteoarthritis�recommends manipulation and stretching should be considered as an adjunct to core treatment, particularly for osteoarthritis of the hip. This recommendation is based on the results of one RCT.
The orthopaedic section of the American Physical Therapy Association’s guidelines on hip pain and mobility deficits�recommends clinicians should consider the use of manual therapy procedures to provide short-term pain relief and improve hip mobility and function in patients with mild hip osteoarthritis based on moderate evidence.
Recent randomized clinical trials not included in above
Licciardone et al found decreased rehabilitation efficiency with osteopathic manipulative therapy (OMT) compared to sham OMT following hip arthroplasty. No other significant differences were found between the two groups. This study had a high risk of bias.
Evidence Summary (See Figure 4)
? Moderate quality evidence that hip manipulation is superior to exercise for the treatment of the symptoms of hip osteoarthritis.
? Inconclusive evidence in a non-favorable direction regarding osteopathic manipulative therapy for rehabilitation following total hip arthroplasty.
Other effective non-invasive physical treatments or patient education
Exercise therapy, advice about weight loss, and appropriate footwear
Knee pain
Definition
Knee pain is defined as soreness, tension, and/or stiffness in the anatomical region of the knee and can be secondary to multiple conditions including knee osteoarthritis or patellofemoral pain syndrome.
Diagnosis
Diagnosis of knee pain is derived from the patient’s history and physical exam with an unremarkable neurological exam and no indicators of potentially serious pathology. Imaging studies are confirmatory for diagnoses of moderate or severe osteoarthritis.
Evidence base for manual treatment
Systematic reviews (most recent)
As of September 2009, one systematic review evaluating the benefit of manual therapy for knee pain has been identified . Ten RCT’s evaluating the effectiveness of manual therapy for the treatment of knee pain were included in the published systematic review. Both osteoarthritis knee pain and patellofemoral pain syndrome were included in the conditions reviewed. Various manual therapy techniques including spinal mobilization,�spinal manipulation, knee mobilization, and knee manipulation were examined within the review. The review concludes there is fair evidence for manipulative therapy of the knee and/or full kinetic chain (Sacro-iliac to foot), combined with multimodal or exercise therapy for knee osteoarthritis and patellofemoral pain syndrome.
Evidence-based clinical guidelines
The NICE national clinical guidelines for care and management of adults with osteoarthritis�recommends manipulation and stretching should be considered as an adjunct to core treatment.
Recent randomized clinical trials not included in above
Pollard et al�assessed a manual therapy protocol compared to non-forceful manual contact (control). They concluded that a short term of manual therapy significantly reduced pain compared to the control group. This study had a high risk of bias.
Perlman et al�found massage therapy was more effective than wait list control for osteoarthritis related knee pain, stiffness, and function. This study had a high risk of bias.
Licciardone et al�assessed osteopathic manipulative treatment following knee arthroplasty. This study found decreased rehabilitation efficiency with OMT compared to sham OMT; otherwise, no significant differences were found between the two groups. This study had a high risk of bias.
? Moderate quality evidence that manual therapy of the knee and/or full kinetic chain (SI to foot) combined with multimodal or exercise therapy is effective for the symptoms of knee osteoarthritis.
? Moderate quality evidence that manual therapy of the knee and/or full kinetic chain (SI to foot) combined with multimodal or exercise therapy is effective for patellofemoral pain syndrome.
? Inconclusive evidence in a favorable direction that massage therapy is effective for the symptoms of knee osteoarthritis.
? Inconclusive evidence in a non-favorable direction for the effectiveness of osteopathic manipulative therapy for rehabilitation following total hip or knee arthroplasty.
Other effective non-invasive physical treatments or patient education
Exercise therapy, advice about weight loss, appropriate footwear, pulsed electromagnetic field therapy, acupuncture, and TENS
Ankle and foot conditions
Definition
A variety of conditions are included under ankle and foot conditions including ankle sprains, plantar fasciitis, morton’s neuroma, hallux limitus/rigidus, and hallux abducto valgus.
Diagnosis
The diagnosis of ankle/foot conditions relies mainly on the patient’s history and physical examination. Imaging studies are indicated for morton’s neuroma or in the presence of potential pathology.
Evidence base for manual treatment
Systematic reviews (most recent)
As of September 2009, two systematic reviews evaluating the benefit of manual therapy for ankle and foot conditions have been published. The ankle and foot conditions reviewed included ankle sprain, plantar fasciitis, morton’s neuroma, hallux limitus, and hallux abducto valgus. Thirteen RCTs evaluating the effectiveness of manual therapy for the treatment of various ankle and foot conditions were included in the published systematic reviews. Of the thirteen trials, six examined the use of ankle/foot manipulation, six examined the use of ankle/foot mobilization, and one trial examined the combined use of manipulation and mobilization.
The review by Brantingham et al concluded there is fair evidence for manipulative therapy of the ankle and/or foot combined with multimodal or exercise therapy for ankle inversion sprain. The same authors found limited evidence for manipulative therapy combined with multimodal or exercise therapy for plantar fasciitis, metatarsalgia, and hallux limitus and insufficient evidence for the use of manual therapy for hallux abducto valgus.
The review by van der Wees et al concluded it is likely that manual mobilization has an initial effect on dorsiflexion range of motion after ankle sprains.
Evidence-based clinical guidelines
None making recommendations based on RCTs were located
Recent randomized clinical trials not included in above
Wynne et al found an osteopathic manipulative therapy group had greater improvement in plantar fasciitis symptoms versus placebo control. This study had a high risk of bias.
Cleland et al compared manual therapy with exercise to electrotherapy with exercise for patients with plantar heel pain. They found manual therapy plus exercise was superior. This study had a low risk of bias.
Lin et al found the addition of manual therapy (mobilization) to a standard physiotherapy program provided no additional benefit compared to the standard physiotherapy program alone for rehabilitation following ankle fracture. This study had a low risk of bias.
Evidence Summary (See Figure 4)
? Moderate quality evidence that mobilization is of no additional benefit to exercise in the rehabilitation following ankle fractures.
? Moderate quality evidence that manual therapy of the foot and/or full kinetic chain (SI to foot) combined with exercise therapy is effective for plantar fasciitis.
? Inconclusive evidence in a favorable direction for the effectiveness of manual therapy with multimodal or exercise therapy for ankle sprains.
? Inconclusive evidence in a favorable direction regarding the effectiveness of manual therapy for morton’s neuroma, hallux limitus, and hallux abducto valgus.
Other effective non-invasive physical treatments or patient education
Stretching and foot orthoses for plantar fasciitis, ankle supports for ankle sprains
Temporomandibular disorders
Definition
Temporomandibular disorders consist of a group of pathologies affecting the masticatory muscles, temporomandibular joint, and related structures.
Diagnosis
Diagnosis of temporomandibular disorders is derived from the patient’s history and physical exam with no indicators of potentially serious pathology.
Evidence base for manual treatment
Systematic reviews (most recent)
As of September 2009, two systematic reviews evaluating the benefit of manual therapy for temporomandibular dysfunction have been published. Three RCTs evaluating the effectiveness of manual therapy were included in the published systematic reviews. Two of the trials examined the effectiveness of mobilization�and one trial assessed massage. The reviews conclude there is limited evidence for the use of manual therapy in the treatment of temporomandibular dysfunction.
Evidence-based clinical guidelines
None located
Recent randomized clinical trials not included in above
Monaco et al�examined the effects of osteopathic manipulative treatment on mandibular kinetics compared to a no treatment control group; however, no between group analysis was performed. This study had a high risk of bias.
Ismail et al�found physical therapy including mobilization in addition to splint therapy was superior to splint therapy alone after three months of treatment for active mouth opening. No differences were found between groups for pain. This study had a moderate risk of bias.
? Inconclusive evidence in a favorable direction regarding mobilization and massage for temporomandibular dysfunction.
Other effective non-invasive physical treatments or patient education
None
Fibromyalgia
Definition
Fibromyalgia syndrome (FMS) is a common rheumatological condition characterized by chronic widespread pain and reduced pain threshold, with hyperalgesia and allodynia.
Diagnosis
Diagnosis of fibromyalgia is made primarily from the patient’s history and physical exam. The American College of Rheumatology have produced classification criteria for fibromyalgia including widespread pain involving both sides of the body, above and below the waist for at least three months and the presence of 11 out of 18 possible pre-specified tender points.
Evidence base for manual treatment
Systematic reviews (most recent)
Since 2004, three systematic reviews evaluating the benefit of manual therapy for fibromyalgia have been published. Six RCTs evaluating the effectiveness of manual therapy for the treatment of fibromyalgia were included in the published systematic reviews. Five of the studies assessed the effectiveness of spinal manipulation for fibromyalgia, while one assessed the effectiveness of massage.
Schneider et al�conclude there is moderate level evidence from several RCTs and a systematic review�that massage is helpful in improving sleep and reducing anxiety in chronic pain; however, few of the studies included in the systematic review�specifically investigated fibromyalgia.
Ernst�states that the current trial evidence is insufficient to conclude that chiropractic is an effective treatment of fibromyalgia.
Goldenberg et al�conclude there is weak evidence of efficacy for chiropractic, manual, and massage therapy in the treatment of fibromyalgia.
Evidence-based clinical guidelines
The 2007 a multidisciplinary task force with members from 11 European countries published evidence based recommendation for FMS. The task force notes the clinical trial evidence for manual therapy is lacking.
Randomized clinical trials not included in above
Ekici et al found improvement was higher in the manual lymph drainage group compared to connective tissue massage on the fibromyalgia impact questionnaire, but no differences were noted between groups for pain, pain pressure threshold, or health related quality of life. This study had a moderate risk of bias.
Evidence Summary (See Figure 5)
? Inconclusive evidence in a favorable direction regarding the effectiveness of massage and manual lymph drainage for the treatment of fibromyalgia.
? Inconclusive evidence in an unclear direction regarding the effectiveness of spinal manipulation for the treatment of fibromyalgia.
Other effective non-invasive physical treatments or patient education
Heated pool treatment with or without exercise, supervised aerobic exercise
Myofascial Pain Syndrome
Definition
Myofascial pain syndrome is a poorly defined condition that requires the presence of myofascial trigger points.
Diagnosis
Diagnosis of myofascial pain syndrome is made exclusively from the patient’s history and physical exam.
Evidence base for manual treatment
Systematic reviews (most recent)
As of September 2009, one systematic review evaluating the benefit of manual therapy for myofascial pain syndrome was identified, which concludes there is limited evidence to support the use of some manual therapies for providing long-term relief of pain at myofascial trigger points. Fifteen RCTs evaluating the effectiveness of manual therapy for the treatment of myofascial pain syndrome were included in the published systematic review. Only two of the truly randomized trials assessed the effectiveness of manual therapy beyond the immediate post-treatment period. One trial assessed the effectiveness of massage combined with other therapies, while the other trial assessed the effectiveness of self-treatment with ischemic compression.
Evidence-based clinical guidelines
None
Recent randomized clinical trials not included in above
None
Evidence Summary (See Figure 5)
? Inconclusive evidence in a favorable direction regarding the effectiveness of massage for the treatment of myofascial pain syndrome.
Other effective non-invasive physical treatments or patient education
Laser, acupuncture
Migraine Headache
Definition
Migraine headache is defined as recurrent/episodic moderate or severe headaches which are usually unilateral, pulsating, aggravated by routine physical activity, and are associated with either nausea, vomiting, photophobia, or phonophobia.
Diagnosis
Diagnosis of migraine headaches is made primarily from the patient’s history and a negative neurological exam. Neuroimaging is only indicated in patients with a positive neurological exam or presence of a “red flag”.
Evidence base for manual treatment
Systematic reviews (most recent)
Since 2004, two systematic reviews evaluated the benefit of manual therapy for migraine headache. The reviews evaluated three RCTs on spinal manipulation. Astin and Ernst�concluded that due to methodological limitations of the RCTs, it is unclear whether or not spinal manipulation is an effective treatment for headache disorders. In contrast, the conclusion from a Cochrane review�was that spinal manipulation is an effective option for the care of migraine headache. The conclusions of the two reviews differed in methodology for determining RCT quality and the strength of evidence. Astin and Ernst�evaluated study quality using a scale that is no longer recommended by the Cochrane Collaboration and did not apply evidence rules for their conclusions. The Cochrane review used a pre-specified, detailed protocol for synthesizing the evidence from the quality, quantity, and results of RCTs.
Evidence-based clinical guidelines
The SIGN guidelines�for the diagnosis and management of headache in adults concludes the evidence of effectiveness for manual therapy is too limited to lead to a recommendation.
Recent randomized clinical trials not included in above
Lawler and Cameron�found that massage therapy significantly reduced migraine frequency in the short term compared to filling out a diary with no other treatment. This study had a high risk of bias.
? Moderate quality evidence that spinal manipulation has an effectiveness similar to a first-line prophylactic prescription medication (amitriptyline) for the prophylactic treatment of migraine.
? Inconclusive evidence in a favorable direction comparing spinal manipulation to sham interferential.
? Inconclusive evidence in a favorable direction regarding the use of massage therapy alone.
Other effective non-invasive physical treatments or patient education
Tension-type headache is defined as a headache that is pressing/tightening in quality, mild/moderate in intensity, bilateral in location, and does not worsen with routine physical activity.
Diagnosis
Diagnosis of tension-type headaches is made primarily from the patient’s history and a negative neurological exam. Neuroimaging is only indicated in patients with a positive neurological exam or presence of a “red flag”.
Evidence base for manual treatment
Systematic reviews (most recent)
Since 2002, five systematic reviews evaluated the benefit of manual therapy for tension-type headache. Eleven RCTs were included in the published systematic reviews. Three of the RCTs assessed the effectiveness of spinal manipulation, six of the trials evaluated the use of combined therapies including a form of manual therapy, one trial evaluated a craniosacral technique, and the remaining trial compared connective tissue manipulation to mobilization. The reviews generally conclude there is insufficient evidence to draw inference on the effectiveness of manual therapy in the treatment of tension-type headache. An exception is the Cochrane review�which found that some inference regarding spinal manipulation could be made from two trials with low risk of bias. One trial�showed that for the prophylactic treatment of chronic tension-type headache, amitriptyline (an effective drug) is more effective than spinal manipulation during treatment. However, spinal manipulation is superior in the short term after cessation of both treatments, but this could be due to a rebound effect of the medication withdrawal. The other trial�showed that spinal manipulation in addition to massage is no more effective than massage alone for the treatment of episodic tension-type headache.
Evidence-based clinical guidelines
The SIGN guideline�for the diagnosis and management of headache in adults draws no conclusions.
Recent randomized clinical trials not included in above
Anderson and Seniscal�found that participants receiving osteopathic manipulation in addition to relaxation therapy had significant improvement in headache frequency compared to relaxation therapy alone. This study had a moderate risk of bias.
Evidence Summary (See Figure 5)
? Moderate quality evidence that spinal manipulation in addition to massage is no more effective than massage alone for the treatment of episodic tension-type headache.
? Inconclusive evidence in an unclear direction regarding the use of spinal manipulation alone or in combination with therapies other than massage for most forms of tension-type headache.
Other effective non-invasive physical treatments or patient education
Acupuncture, biofeedback
Cervicogenic Headache
Definition
Cervicogenic headache is defined as unilateral or bilateral pain localized to the neck and occipital region which may project to regions on the head and/or face. Head pain is precipitated by neck movement, sustained awkward head positioning, or external pressure over the upper cervical or occipital region on the symptomatic side.
Diagnosis
Diagnosis of cervicogenic headaches is made primarily from the patient’s history and a negative neurological exam. Neuroimaging is only indicated in patients with a positive neurological exam or presence of a “red flag”.
Evidence base for manual treatment
Systematic reviews (most recent)
Since 2002, four systematic reviews have been published on manual therapy for cervicogenic headache. The reviews made inference based on six RCTs that evaluated a range of manual therapy treatments including spinal manipulation, mobilization, and friction massage. Astin and Ernst�concluded that due to methodological limitations of the RCTs, it is unclear whether or not spinal manipulation is an effective treatment for headache disorders. In contrast, a Cochrane review concluded that spinal manipulation is an effective option for the care of cervicogenic headache. The conclusions of the two reviews differed in methodology for determining RCT quality and the strength of evidence. Ernst evaluated study quality using a scale that is no longer recommended by the Cochrane Collaboration and did not apply evidence rules for their conclusions. The Cochrane review�used a pre-specified, detailed protocol for synthesizing the evidence from the quality, quantity, and results of RCTs.
Evidence-based clinical guidelines
The SIGN guidelines�for the diagnosis and management of headache in adults concluded spinal manipulation should be considered in patients with cervicogenic headache.
Recent randomized clinical trials not included in above
Hall et al�evaluated the efficacy of apophyseal glide of the upper cervical region in comparison to a sham control. They found a large clinically important and statistically significant advantage of the intervention over sham for pain intensity. The study had a low risk of bias.
? Moderate quality evidence that spinal manipulation is more effective than placebo manipulation, friction massage, and no treatment.
? Moderate quality evidence that spinal manipulation is similar in effectiveness to exercise.
? Moderate quality evidence that self-mobilizing natural apophyseal glides are more effective than placebo.
? Inclusive evidence that deep friction massage with trigger point therapy is inferior to spinal manipulation.
? Inconclusive evidence in an unclear direction for the use of mobilization.
Other effective non-invasive physical treatments or patient education
Neck exercises
Miscellaneous Headache
Definition
Headaches not classified as tension-type, migraine, or cervicogenic in nature according to the International Headache Society’s 2004 diagnostic criteria.
Evidence base for manual treatment
Systematic reviews (most recent)
One systematic review (2004) evaluated the benefit of manual therapy for other types of chronic headache. One RCT evaluating the use of mobilization for post-traumatic (post-concussive) headache was included. The review found the evidence to be inconclusive.
Evidence-based clinical guidelines
None
Recent randomized clinical trials not included in above
? Inconclusive evidence in a favorable direction regarding mobilization for post-traumatic headache.
Other effective non-invasive physical treatments or patient education
None
Asthma
Definition
Asthma is a common, complex chronic disorder of the airways that is characterized by variable and recurring symptoms, airflow obstruction, bronchial hyperresponsiveness, and an underlying inflammation.
Diagnosis
The diagnosis is made through the combination of the patient’s history, upper respiratory physical exam, and pulmonary function testing (spirometry). Patient administered peak flow measurement is often used to monitor effects of treatment.
Evidence base for manual treatment
Systematic reviews
Since 2002, four systematic reviews, one a Cochrane review, on manual therapy for asthma have been published. Of the total of five RCTs on the effectiveness of manual therapy�available from the searched literature, two investigated chiropractic spinal manipulation for chronic asthma, one in adults�and the other in children. Two trials assessed the effectiveness on chronic asthma in children, one examined osteopathic manipulative/manual therapy, and the other massage. The fifth trial evaluated the effect of foot manual reflexology for change in asthma symptoms and lung function in adults. The four systematic reviews collectively concluded that the evidence indicates that none of the manual therapy approaches have been shown to be superior to a suitable sham manual control on reducing severity and improving lung function but that clinically important improvements occur over time during both active and sham treatment.
Evidence-based clinical guidelines
The asthma guidelines by The US National Heart, Lung, and Blood Institutes�and by The British Thoracic Society�both conclude that there is insufficient evidence to recommend the use of chiropractic or related manual techniques in the treatment of asthma.
Recent randomized clinical trials not included in above
None
Evidence Summary (See Figures 6 & 7)
? There is moderate quality evidence that spinal manipulation is not effective (similar to sham manipulation) for the treatment of asthma in children and adults on lung function and symptom severity.
? There is inconclusive evidence in a non-favorable direction regarding the effectiveness of foot manual reflexology for change in asthma symptoms and lung function in adults.
? There is inconclusive evidence in a favorable direction regarding the effectiveness of osteopathic manipulative treatment for change in asthma symptoms and lung function in children.
? There is inconclusive evidence in an unclear direction regarding the effectiveness of massage for change in asthma symptoms and lung function in children.
Other effective non-invasive physical treatments or patient education
Education and advice on self-management, maintaining normal activity levels, control of environmental factors and smoking cessation
Pneumonia
Definition
Pneumonia is defined as an acute inflammation of the lungs caused by infection.
Diagnosis
Diagnosis of pneumonia relies primarily on chest radiography in conjunction with the patient’s history, examination, and laboratory findings.
Evidence base for manual treatment
Systematic reviews (most recent)
Since 2007, one systematic review evaluating the benefit of manual therapy for pneumonia has been published. One RCT evaluating the effectiveness of manual therapy for the treatment of pneumonia was included in the published systematic review. The included trial assessed the effectiveness of osteopathic spinal manipulation for acute pneumonia in hospitalized elderly adults. The review concluded there is promising evidence for the potential benefit of manual procedures for hospitalized elderly patients with pneumonia. Our risk of bias assessment places this trial in the moderate risk of bias category.
? There is inconclusive evidence in a favorable direction regarding the effectiveness of osteopathic manual treatment for the treatment of acute pneumonia in elderly hospitalized patients.
Other effective non-invasive physical treatments or patient education
Cases of pneumonia that are of public health concern should be reported immediately to the local health department. Respiratory hygiene measures, including the use of hand hygiene and masks or tissues for patients with cough, should be used in outpatient settings as a means to reduce the spread of respiratory infections.
Vertigo
Definition
Vertigo is defined as a false sensation of movement of the self or the environment. Vertigo is a sensation and not necessarily a diagnosis as there are multiple underlying pathologies responsible for vertigo.
Diagnosis
Diagnosis of vertigo relies primarily on the patient’s history and clinical examination. Potential causes of vertigo include both pathological disorders such as vertebrobasilar insufficiency or central nervous system lesions as well as more benign causes such as cervicogenic vertigo or benign paroxysmal positional vertigo.
Evidence base for manual treatment
Systematic reviews (most recent)
Since 2004, two systematic reviews evaluating the benefit of manual therapy for vertigo have been published.�One RCT evaluating the effectiveness of mobilization and soft-tissue massage for the treatment of cervicogenic vertigo was included in both published systematic reviews. One review concluded limited evidence of effectiveness. The other concluded effectiveness, but the inference was on the inclusion of other types of evidence.
Evidence-based clinical guidelines
None addressing the use of manual therapy
Recent randomized clinical trials not included in above
Reid et al�compared sustained natural apophyseal glides (SNAGs), delivered manually by a therapist, to detuned laser treatment for the treatment of cervicogenic dizziness. Patients receiving SNAGs reported less dizziness, disability and cervical pain after six weeks, but not at 12 weeks. This study had a low risk of bias.
? Moderate quality evidence that manual treatment (specifically sustained natural apophyseal glides) is an effective treatment for cervicogenic dizziness, at least in the short term.
Other effective non-invasive physical treatments or patient education
Particle repositioning maneuvers for benign paroxysmal positional vertigo, vestibular rehabilitation
Infantile Colic
Definition
Colic is a poorly defined condition characterized by excessive, uncontrollable crying in infants.
Diagnosis
The diagnosis of colic is based solely on the patient’s history and the absence of other explanations for the excessive crying. The “rule of threes” is the most common criteria used in making a diagnosis of colic. The rule of three’s is defined as an otherwise healthy and well fed infant with paroxysms of crying and fussing lasting for a total of three hours a day and occurring more than three days a week for at least three weeks.
Evidence base for manual treatment
Systematic reviews (most recent)
Since 2003, six systematic reviews evaluating the benefit of manual therapy for infantile colic have been published. Two of the systematic reviews evaluated the effectiveness of manual therapy for non-musculoskeletal�and pediatric�conditions as a whole but fail to draw specific conclusions regarding the use of manual therapy for infantile colic. Of the eight RCTs evaluating the effectiveness of manual therapy for the treatment of colic, five were included in the published systematic reviews. All five of the trials assessed the effectiveness of chiropractic spinal manipulation for infantile colic. All four systematic reviews concluded there is no evidence manual therapy is more effective than sham therapy for the treatment of colic.
Evidence-based clinical guidelines
No clinical guidelines located
Randomized clinical trials not included in above
Hayden et al�found cranial osteopathy was more effective than no treatment for crying duration. This study had a high risk of bias
Huhtala et al�found no difference between groups treated with massage therapy or given a crib vibrator for crying duration. This study had a high risk of bias.
Arikan et al�found all four interventions (massage, sucrose solution, herbal tea, hydrolysed formula) showed improvement compared to a no treatment control group. This study had a moderate risk of bias.
Evidence Summary (See Figure 7)
? Moderate quality evidence that spinal manipulation is no more effective than sham spinal manipulation for the treatment of infantile colic.
? Inconclusive evidence in a favorable direction regarding the effectiveness of cranial osteopathic manual treatment and massage for the treatment of infantile colic.
Other effective non-invasive physical treatments or patient education
Reduce stimulation, herbal tea, and trial of hypoallergenic formula milk
Nocturnal Enuresis
Definition
Nocturnal enuresis is defined as the involuntary loss of urine at night, in the absence of organic disease, at an age when a child could reasonably be expected to be dry (typically at the age of five).
Diagnosis
The diagnosis of nocturnal enuresis is derived mainly from the patient’s history given the absence of other organic causes including congenital or acquired defects of the central nervous system. Psychological factors can be contributory in some children requiring proper assessment and treatment.
Evidence base for manual treatment
Systematic reviews (most recent)
Since 2005, two systematic reviews, one a Cochrane review, evaluating the benefit of manual therapy for nocturnal enuresis were published. The systematic reviews included a total of two randomized clinical trials. Both of the included trials examined the use of spinal manipulation for nocturnal enuresis. Both reviews concluded there is insufficient evidence to make conclusions about the effectiveness of spinal manipulation for the treatment of enuresis.
Evidence-based clinical guidelines
None addressing manual therapy as a treatment option
? Inconclusive evidence in a favorable direction regarding the effectiveness of chiropractic care for the treatment of enuresis.
Other effective non-invasive physical treatments or patient education
Education, simple behavioral interventions, and alarm treatment
Otitis Media
Definition
Otitis media is characterized by middle ear inflammation which can exist in an acute or chronic state and can occur with or without symptoms.
Diagnosis
Diagnosis of otitis media relies on otoscopic signs and symptoms consistent with a purulent middle ear effusion in association with systemic signs of illness.
Evidence base for manual treatment
Systematic reviews (most recent)
Hawk et al�found promising evidence for the potential benefit of spinal manipulation/mobilization procedures for children with otitis media. This was based on one trial. Two other reviews specifically addressed spinal manipulation by chiropractors for non-musculoskeletal�and pediatric�conditions. Both found insufficient evidence to comment on manual treatment effectiveness or ineffectiveness for otitis media.
Evidence-based clinical guidelines
The American Academy of Pediatrics 2004 guidelines on the diagnosis and management of acute otitis media�concluded no recommendation for complementary and alternative medicine for the treatment of acute otitis media can be made due to limited data.
Recent randomized clinical trials not included in above
Wahl et al investigated the efficacy of osteopathic manipulative treatment with and without Echinacea compared to sham and placebo for the treatment of otitis media. The study found that a regimen of up to five osteopathic manipulative treatments does not significantly decrease the risk of acute otitis media episodes. This study had a high risk of bias.
? Inconclusive evidence in an unclear direction regarding the effectiveness of osteopathic manipulative therapy for otitis media.
Other effective non-invasive physical treatments or patient education
Patient education and “watch and wait” approach for 72 hours for acute otitis media
Hypertension
Definition
Hypertension is defined as the sustained elevation of systolic blood pressure over 140 mmHg, diastolic blood pressure over 90 mm Hg, or both.
Diagnosis
Diagnosis of hypertension is made by the physical exam, specifically sphygmomanometry. The patient’s history, clinical exam and laboratory tests help identify potential etiologies.
Evidence base for manual treatment
Systematic reviews (most recent)
Since 2007, one systematic review evaluating the benefit of manual therapy for hypertension has been published (Hawk et al). Two RCTs evaluating the effectiveness of manual therapy for the treatment of stage I hypertension were included in this systematic review. One of the included trials evaluated the use of spinal manipulation and the other evaluated the use of instrument assisted spinal manipulation. The review found no evidence of effectiveness for spinal manipulation.
Evidence-based clinical guidelines
None addressing the use of manual therapy
Recent randomized clinical trials not included in above
A study by Bakris et al found NUCCA upper cervical manipulation to be more effective than sham manipulation in lowering blood pressure in patients with Stage I hypertension. This study had a high risk of bias.
Evidence Summary (See Figure 6)
? Moderate quality evidence that diversified spinal manipulation is not effective when added to a diet in the treatment of stage I hypertension.
? Inconclusive evidence in a favorable direction regarding upper cervical NUCCA manipulation for stage I hypertension .
? Inconclusive evidence in an unclear direction regarding instrument assisted spinal manipulation for hypertension.
Other effective non-invasive physical treatments or patient education
Advice on lifestyle interventions including diet, exercise, moderate alcohol consumption and smoking cessation
Relaxation therapies including biofeedback, meditation, or muscle relaxation
Dysmenorrhea
Definition
Dysmenorrhea is defined as painful menstrual cramps of uterine origin. Dysmenorrhea is grouped into two categories, primary and secondary dysmenorrhea. Secondary dysmenorrhea is painful menstruation associated with a pelvic pathology like endometriosis, while primary dysmenorrhea is painful menstruation in the absence of pelvic disease.
Diagnosis
Diagnosis of primary dysmenorrhea is made from the patient’s history. Diagnosis of secondary dysmenorrhea requires further investigation including a pelvic exam and potential ultrasound or laparoscopy.
Evidence base for manual treatment
Systematic reviews (most recent)
We identified two systematic reviews evaluating the benefit of manual therapy for dysmenorrhea. Five studies evaluating the effectiveness of manual therapy for the treatment of dysmenorrhea were included in the systematic reviews. Four of the included trials examined the use of spinal manipulation�and one examined the use of osteopathic manipulative techniques. Based on these trials, the Cochrane review by Proctor et al concluded there is no evidence to suggest that spinal manipulation is effective in the treatment of primary and secondary dysmenorrhea. The review by Hawk et al concluded the evidence was equivocal regarding chiropractic care for dysmenorrhea.
Evidence-based clinical guidelines
We identified consensus guidelines from the Society of Obstetricians and Gynecologists of Canada (SOGC) published in 2005 which included an assessment of manual treatment for primary dysmenorrhea. The authors concluded there is no evidence to support spinal manipulation as an effective treatment for primary dysmenorrhea.
Recent randomized clinical trials not included in above
None
Evidence Summary (See Figure 7)
? Moderate quality evidence that spinal manipulation is no more effective than sham manipulation in the treatment of primary dysmenorrhea.
Other effective non-invasive physical treatments or patient education
High frequency TENS
Premenstrual Syndrome
Definition
Premenstrual syndrome is defined as distressing physical, behavioral, and psychological symptoms, in the absence of organic or underlying psychiatric disease, which regularly recurs during the luteal phase of the menstrual cycle and disappears or significantly regresses by the end of menstruation and is associated with impairment in daily functioning and/or relationships.
Diagnosis
Diagnosis of premenstrual syndrome is made through patient history and the use of a patient diary over two menstrual cycles.
Evidence base for manual treatment
Systematic reviews (most recent)
Since 2007, three systematic reviews evaluating the benefit of manual therapy for premenstrual syndrome have been published. Three RCTs evaluating the effectiveness of manual therapy for the treatment of premenstrual syndrome were included in the reviews. The included trials examined different forms of manual therapy including spinal manipulation, massage therapy, and reflexology. Overall, the reviews concluded that the evidence is “not promising”, “equivocal”, and that high quality studies are needed to draw firm conclusions.
Evidence-based clinical guidelines
None discussing manual therapy
Recent randomized clinical trials not included in above
None
Evidence Summary (See Figure 7)
? Inconclusive evidence in a favorable direction regarding the effectiveness of reflexology and massage therapy for the treatment of premenstrual syndrome.
? Inconclusive evidence in an unclear direction regarding the effectiveness of spinal manipulation for the treatment of premenstrual syndrome.
Other effective non-invasive physical treatments or patient education
Cognitive behavioral therapy
Discussion
Making claims
There are two important questions underlying the medical and media debate surrounding the scope of chiropractic care and claims regarding its effectiveness particularly for non-musculoskeletal conditions: 1) should health professionals be permitted to use generally safe but as yet unproven methods? 2) What claims, if any, can and should be made with respect to the potential value of unproven treatments?
In response to the first question, a reasonable answer is “yes” given that professionals operate within the context of EBH, where it is acknowledged what is known today, might change tomorrow. It requires flexibility born of intellectual honesty that recognizes one’s current clinical practices may not�really�be in the best interests of the patient and as better evidence emerges, clinicians are obligated to change. Further, where evidence is absent, they are open to promoting the development of new knowledge that expands understanding of appropriate health care delivery.
In response to the second question, no claims of efficacy/effectiveness should be made for which there isn’t sufficient evidence. Unsubstantiated claims can be dangerous to patient health. We maintain the best evidence for efficacy/effectiveness that meets society’s standards comes from well-designed RCTs. While other study designs and clinical observations do offer insight into the plausibility and potential value of treatments, the concepts of plausibility and evidence of efficacy/effectiveness should not be confused when making claims.
Clinical Experience versus Clinical effectiveness
Why is it that the results of RCTs often do not confirm the results observed in clinical practice? There are several reasons. One of the problems is that both the provider and the patient are likely to interpret any improvement as being solely a result of the intervention being provided. However this is seldom the case. First, the natural history of the disorder (for example. acute LBP) is expected to partially or completely resolve by itself regardless of treatment. Second, the phenomenon of regression to the mean often accounts for some of the observed improvement in the condition. Regression to the mean is a statistical phenomenon associated with the fact that patients often present to the clinic or in clinical trials at a time where they have relatively high scores on severity outcome measures. If measured repeatedly before the commencement of treatment the severity scores usually regress towards lower more normal average values.
Additionally, there is substantial evidence to show that the ritual of the patient practitioner interaction has a therapeutic effect in itself separate from any specific effects of the treatment applied. This phenomenon is termed contextual effects. The contextual or, as it is often called, non-specific effect of the therapeutic encounter can be quite different depending on the type of provider, the explanation or diagnosis given, the provider’s enthusiasm, and the patient’s expectations. Some researchers have suggested that relying on evidence from RCTs and systematic reviews of RCTs is not adequate to determine whether a treatment is effective or not. The main issue, they contend, is that the intervention when studied in RCTs is too highly protocolized and does not reflect what is going on in clinical practice. They advocate a whole systems research approach that more accurately represents the entire clinical encounter. When using this perspective and systematically synthesizing the literature regarding chiropractic treatment of non-musculoskeletal conditions, also reviewed in this report, they conclude, for example that chiropractic is beneficial to patients with asthma and to children with infantile colic. This conclusion is at odds with the evidence summaries found in this report. We submit that whole systems research approach in this instance is clouding the interpretation of the literature regarding effectiveness as it relates to making claims, and incorrectly giving the consumer the impression that chiropractic care shows effectiveness over and above the contextual effects as it relates to the two examples above.
In a placebo-controlled RCT the question is: does the treatment provided have a specific effect over and above the contextual or non-specific effects. The result of such a trial may show that there is no important difference between the active intervention and the sham intervention. However, the patients may exhibit clinically important changes from baseline in both groups and thus the outcome would be consistent with what clinicians observe in their practice. An example of this is the results of the pragmatic placebo controlled RCT on chiropractic co-management of chronic asthma in adults (care delivered by experienced chiropractors consistent with normal clinical practice), which showed that patients improved equally during both the active and the sham intervention phases of the trial.
The Pieces of The Evidence-Based Healthcare Puzzle
It is essential to recognize what each piece of the EBH puzzle offers. Patient values and preferences do not provide sound evidence of a treatment’s effectiveness and may be misleading. A patient can be satisfied with a treatment, but it still may not be effective. The clinician’s observations, if well documented, can attest to patient improvement while under care and encourage perception of a treatment’s clinical plausibility. However, the narrow focus of attention under non-systematic observations common to practice experience tends to obscure other factors influencing case outcome. Similarly, EBH can be flawed, not because it fails to be scientific, but because-like all sciences-it imports the biases of researchers and clinicians. Well-performed clinical research however, does provide evidence for claims that a treatment is effective when the results are consistently applied to relevant patients. This is because of its reliance on methods for systematic observation and efforts to minimize bias.
Other authors’ work has been used to argue that a range of study types should be included when evaluating a treatment’s efficacy/effectiveness (case series, etc.). We maintain the best evidence that rises to societal standards to support claims of efficacy/effectiveness comes from well-designed RCTs. This is largely due to the powerful effect of successful randomization and design factors intended to minimize bias (all which help ensure that the results are due to the intervention and not some other known or unknown factor). Other evidence may be useful to inform treatment options when conditions for individual patients are not consistent with the best evidence or when better evidence is unavailable. Other types of research are more appropriate for answering related questions including, but not limited to, safety or mechanistic plausibility. This can lead to the refinement of interventions, inform the design of clinical trials, and aid in the interpretation of clinical observations. Similarly, clinical data from epidemiological studies, case reports, and case series can suggest that a treatment is�clinically plausible. That is, clinical observations demonstrate that�it is possible�that an intervention is effective. However, a gain in plausibility, biological or clinical, does NOT constitute proof of a treatment’s efficacy in human populations. Conversely lack of proof (as demonstrated through well performed randomized clinical trials) does not exclude plausibility.
Research on systematic reviews have taught us that individual studies can often lead to a conclusion very different from that of a systematic analysis of all available studies. Moreover, the scientific process is a systematic means of self-correcting investigations that classically begin with observations and hypotheses that support plausibility and/or mechanisms. Ideally, these precede and inform the conduct of RCTs under conditions most likely to yield clear results, often referred to as efficacy studies. Separately, studies that emulate general practice conditions may be used to develop an understanding of effectiveness. Historically, the modern investigation of manual treatment methods represents an aberration in this process. With the advent of social support and funding for research at the end of the 20th�Century, there was an underlying presumption that the long-term practice of these methods provided a sound clinical wisdom on which to ground RCTs, bypassing mechanistic studies. The early emphasis on clinical trials has illuminated the gaps in understanding of appropriate indications for treatment, dosage and duration of care, consistency of treatment application, and the appropriate outcome measures to monitor results. In response, funding agencies in North America have renewed research emphasis on the potential mechanisms of effect. Data from this work is expected to inform future clinical research questions, and subsequently lead to well-grounded studies that are likely to yield more complete evidence regarding appropriate and effective care.
Safety of Manual Treatment
Choosing an intervention should always be tempered by the risk of adverse events or harm. Adverse events associated with manual treatment can be classified into two categories: 1) benign, minor or non-serious and 2) serious. Generally those that are benign are transient, mild to moderate in intensity, have little effect on activities, and are short lasting. Most commonly, these involve pain or discomfort to the musculoskeletal system. Less commonly, nausea, dizziness or tiredness are reported. Serious adverse events are disabling, require hospitalization and may be life-threatening. The most documented and discussed serious adverse event associated with spinal manipulation (specifically to the cervical spine) is vertebrobasilar artery (VBA) stroke. Less commonly reported are serious adverse events associated with lumbar spine manipulation, including lumbar disc herniation and cauda equina syndrome.
Estimates of serious adverse events as a result of spinal manipulation have been uncertain and varied. Much of the available evidence has been relatively poor due to challenges in establishing accurate risk estimates for rare events. Such estimates are best derived from sound population based studies, preferably those that are prospective in nature.
Estimates of VBA stroke subsequent to cervical spine manipulation range from one event in 200,000 treatments to one in several million. In a subsequent landmark population-based study, Cassidy et al revisited the issue using case-control and case-crossover designs to evaluate over 100 million person-years of data. The authors confirmed that VBA stroke is a very rare event in general. They stated, “We found no evidence of excess risk of VBA stroke associated with chiropractic care compared to primary care.” They further concluded, “The increased risk of VBA stroke associated with chiropractic and PCP (primary care physician) visits is likely due to patients with headache and neck pain from VBA dissection seeking care before their stroke.” In regards to benign adverse reactions, cervical spine manipulation has been shown to be associated with an increased risk when compared to mobilization.
Appropriately, the risk-benefit of cervical spine manipulation has been debated. As anticipated, new research can change what is known about the benefit of manual treatment for neck pain. Currently, the evidence suggests that it has some benefit. It has been suggested that the choice between mobilization and manipulation should be informed by patient preference.
Estimates of cervical or lumbar disc herniation are also uncertain, and are based on case studies and case series. It has been estimated that the risk of a serious adverse event, including lumbar disc herniation is approximately 1 per million patient visits. Cauda equina syndrome is estimated to occur much less frequently, at 1 per several million visits.
Safety of Manual Treatment in Children
The true incidence of serious adverse events in children as a result of spinal manipulation remains unknown. A systematic review published in 2007 identified 14 cases of direct adverse events involving neurologic or musculoskeletal events, nine of which were considered serious (eg. subarachnoid hemorrhage, paraplegia, etc.). Another 20 cases of indirect adverse events were identified (delayed diagnosis, inappropriate application of spinal manipulation for serious medical conditions). The review authors note that case reports and case series are a type of “passive” surveillance, and as such don’t provide information regarding incidence. Further, this type of reporting of adverse events is recognized to underestimate true risk.
Importantly, the authors postulate that a possible reason for incorrect diagnosis (for example. delayed diagnosis, inappropriate treatment with spinal manipulation) is due to lack of sufficient pediatric training. They cite their own survey�which found that in a survey of 287 chiropractors and osteopaths, 78% reported one semester or less of formal pediatric education and 72% received no pediatric clinical training. We find this particularly noteworthy.
Limitations of the Report Conclusions
The conclusions in this report regarding the strength of evidence of presence or absence of effectiveness are predicated on the rules chosen for which there are no absolute standards. Different evidence grading systems and rules regarding impact of study quality may lead to different conclusions. However, we have applied a synthesis methodology consistent with the latest recommendations from authoritative organizations involved in setting standards for evidence synthesis. Although we used a comprehensive literature search strategy we may not have identified all relevant RCTs, guidelines, and technology reports. Conditions for which this report concludes the evidence currently shows manual treatment to be effective or even ineffective, sometimes rests on a single RCT with adequate statistical power and low risk of bias. Additional high quality RCTs on the same topics have a substantial likelihood of changing the conclusions. Including only English language reviews and trials may be considered another limitation of this report leading to language bias; however, the impact of excluding non-English trials from meta-analyses and systematic reviews is conflicting, and the incidence of randomized trials published in non-English journals is declining. Another potential limitation of this report is the lack of critical appraisal of the systematic reviews and clinical guidelines included in the report. Systematic reviews and clinical guidelines can differ widely in methodologic quality and risk of bias. While critical appraisal of the included reviews and guidelines would be ideal, it was beyond the scope of the present report. When drawing conclusions about relative effectiveness of different forms of manual treatments it is acknowledged that it has usually not been possible to isolate or quantify the specific effects of the interventions from the non-specific (contextual) effect of patient-provider interaction. It was beyond the scope of this report to assess the magnitude of the effectiveness of the different manual therapies relative to the therapies to which comparisons were made. However, if moderate or high quality evidence of effectiveness was established the therapy was interpreted as a viable treatment option, but not necessarily the most effective treatment available. We recognize that findings from studies using a nonrandomized design (for example. observational studies, cohort studies, prospective clinical series and case reports) can yield important preliminary evidence on potential mechanisms and plausibility of treatment effects. However, the primary purpose of this report is to summarize the results of studies designed to specifically address treatment efficacy and effectiveness from which claims of clinical utility, consistent with that literature, may be considered defensible. Therefore, the evidence base on the effects of care was restricted to RCTs.
Conclusions
Spinal manipulation/mobilization is effective in adults for acute, subacute, and chronic low back pain; for migraine and cervicogenic headache; cervicogenic dizziness; and a number of upper and lower extremity joint conditions. Thoracic spinal manipulation/mobilization is effective for acute/subacute neck pain, and, when combined with exercise, cervical spinal/manipulation is effective for acute whiplash-associated disorders and for chronic neck pain. The evidence is inconclusive for cervical manipulation/mobilization alone for neck pain of any duration, and for any type of manipulation/mobilization for mid back pain, sciatica, tension-type headache, coccydynia, temporomandibular joint disorders, fibromyalgia, premenstrual syndrome, and pneumonia in older adults. Spinal manipulation is not effective for asthma and dysmenorrhea when compared to sham manipulation, or for Stage 1 hypertension when added to an antihypertensive diet. For children, the evidence is inconclusive regarding the effectiveness of spinal manipulation/mobilization for otitis media and enuresis, but shows it is not effective for infantile colic and for improving lung function in asthma when compared to sham manipulation.
The evidence regarding massage shows that for adults it is an effective treatment option for chronic LBP and chronic neck pain. The evidence is inconclusive for knee osteoarthritis, fibromyalgia, myofascial pain syndrome, migraine headache, and premenstrual syndrome. For children, the evidence is inconclusive for asthma and infantile colic.
Competing interests
All authors are trained as doctors of chiropractic but are now full time professional researchers.
Authors’ contributions
GB was responsible for the methodology used to select and summarize the evidence, for organizing and participating in the analysis of the evidence and formulating conclusions and drafting and finalizing the report.
MH participated in analyzing the evidence and formulating conclusions for the majority of the musculoskeletal conditions and the different types of headache.
RE participated in analyzing the evidence and formulating conclusion for part of the musculoskeletal and non-musculoskeletal conditions and providing substantial input to the background and discussion sections.
BL was responsible for retrieving the research articles and providing draft summary statements for all conditions as well as participating in drafting and proof reading the manuscript.
JT was responsible for conceiving and drafting the section on translation of research into action and providing substantial input to the background and discussion sections. All authors have read and approved the final manuscript.
Includes the criteria used for evaluating risk of bias from randomized controlled trials not included within systematic reviews, evidence based guidelines, or health technology assessments.
The UK General Chiropractic Council provided the funding for this scientific evidence report.
Della Shupe, librarian at NWHSU, is acknowledged for helping design and perform the detailed search strategy used for the report.
In conclusion, the results of the above research study determined that manual therapies, such as manipulation and/or mobilization are effective in adults for acute, subacute and chronic low back pain, migraine and cervicogenic headache, cervicogenic dizziness, as well as for several extremity joint conditions and acute/subacute neck pain. The clinical and experimental evidence was inconclusive alone for some cases of neck and back pain, sciatica, tension-type headache coccydynia, temporomandibular joint disorders, fibromyalgia, premenstrual syndrome and pneumonia in older adults.� Manual therapies, such as manipulation and/or mobilization were not effective for asthma and dysmenorrhea and well as for otitis media and enuresis or infantile colic and asthma.
Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Sciatica
Sciatica is referred to as a collection of symptoms rather than a single type of injury or condition. The symptoms are characterized as radiating pain, numbness and tingling sensations from the sciatic nerve in the lower back, down the buttocks and thighs and through one or both legs and into the feet. Sciatica is commonly the result of irritation, inflammation or compression of the largest nerve in the human body, generally due to a herniated disc or bone spur.
Goldberg M. On evidence and evidence-based medicine: lessons from the philosophy of science.�Soc Sci Med.�2006;62:2621�2632. doi: 10.1016/j.socscimed.2005.11.031.�[PubMed]�[Cross Ref]
Nelson LH. In:�In Feminist epistemologies.�Alcoff, Potter E, editor. 1993. Epistemological communities; pp. 121�160.
Lavis JN, Robertson D, Woodside JM, McLeod CB, Abelson J. How can research organizations more effectively transfer research knowledge to decision makers?�Milbank Q.�2003;81:221�222. doi: 10.1111/1468-0009.t01-1-00052.�[PMC free article]�[PubMed]�[Cross Ref]
Straus SE, Tetroe J, Graham I. Defining knowledge translation.�CMAJ.�2009;181:165�168.[PMC free article]�[PubMed]
Muir Gray JA.�Evidence Based Healthcare How to make Health Policy and Management Decisions.2. Harcourt Publishers Limited; 2001.
Guyatt G, Cook D, Haynes B. Evidence based medicine has come a long way.�BMJ.�2004;329:990�991. doi: 10.1136/bmj.329.7473.990.�[PMC free article]�[PubMed]�[Cross Ref]
Lambert H. Accounting for EBM: notions of evidence in medicine.�Soc Sci Med.�2006;62:2633�2645. doi: 10.1016/j.socscimed.2005.11.023.�[PubMed]�[Cross Ref]
Davey Smith G, Egger M. Incommunicable knowledge? Interpreting and applying the results of clinical trials and meta-analyses.�J Clin Epidemiol.�1998;51:289�295. doi: 10.1016/S0895-4356(97)00293-X.�[PubMed]�[Cross Ref]
Schatter A, Fletcher RH. Research evidence and the individual patient.�Quarterly Journal of Medicine.�2003;96:1�5.�[PubMed]
Triano JJ. What constitutes evidence for best practice?�J Manipulative Physiol Ther.�2008;31:637�643. doi: 10.1016/j.jmpt.2008.10.009.�[PubMed]�[Cross Ref]
Greenhalgh T, Hurwitz B. Narrative based medicine; Why study narrative?�BMJ.�1999;318:48�50.[PMC free article]�[PubMed]
Hope T. Evidence-based patient choice and psychiatry.�Evid Based Ment Health.�2002;5:100�101. doi: 10.1136/ebmh.5.4.100.�[PubMed]�[Cross Ref]
Evidence-based patient choice: Inevitable or impossible?�Oxford University Press; 2001.
Shaughnessy AF, Slawson DC, Becker L. Clinical jazz: harmonizing clinical experience and evidence-based medicine.�J Fam Pract.�1998;47:425�428.�[PubMed]
Straus SE. What’s the E for EBM?�BMJ.�2004;328:535�536. doi: 10.1136/bmj.328.7439.535.[PMC free article]�[PubMed]�[Cross Ref]
Marmot MG. Evidence based policy or policy based evidence?�BMJ.�2004;328:906�907. doi: 10.1136/bmj.328.7445.906.�[PMC free article]�[PubMed]�[Cross Ref]
Chou R, Huffman LH. Nonpharmacologic therapies for acute and chronic low back pain: a review of the evidence for an American Pain Society/American College of Physicians clinical practice guideline.�Ann Intern Med.�2007;147:492�504.�[PubMed]
Haynes RB, Devereaux PJ, Guyatt GH. Physicians’ and patients’ choices in evidence based practice.�BMJ.�2002;324:1350. doi: 10.1136/bmj.324.7350.1350.�[PMC free article]�[PubMed]�[Cross Ref]
Gordon EJ. The political contexts of evidence-based medicine: policymaking for daily hemodialysis.�Soc Sci Med.�2006;62:2707�2719. doi: 10.1016/j.socscimed.2005.11.024.�[PubMed]�[Cross Ref]
Savigny P, Watson P, Underwood M. Early management of persistent non-specific low back pain: summary of NICE guidance.�BMJ.�2009;338:b1805. doi: 10.1136/bmj.b1805.�[PubMed]�[Cross Ref]
Chou R, Qaseem A, Snow V, Casey D, Cross JT Jr, Shekelle P. Diagnosis and treatment of low back pain: a joint clinical practice guideline from the American College of Physicians and the American Pain Society.�Ann Intern Med.�2007;147:478�491.�[PubMed]
Airaksinen O, Brox JI, Cedraschi C, Hildebrandt J, Klaber-Moffett J, Kovacs F. Chapter 4. European guidelines for the management of chronic nonspecific low back pain.�Eur Spine J.�2006;15(Suppl 2):S192�S300. doi: 10.1007/s00586-006-1072-1.�[PMC free article]�[PubMed]�[Cross Ref]
van Tulder M, Becker A, Bekkering T, Breen A, Del Real MT, Hutchinson A. Chapter 3. European guidelines for the management of acute nonspecific low back pain in primary care.�Eur Spine J.�2006;15(Suppl 2):S169�S191. doi: 10.1007/s00586-006-1071-2.�[PMC free article]�[PubMed][Cross Ref]
Assendelft WJ, Morton SC, Yu EI, Suttorp MJ, Shekelle PG. Spinal manipulative therapy for low back pain.�Cochrane Database Syst Rev.�2004. p. CD000447.�[PubMed]
van Tulder MW, Koes B, Malmivaara A. Outcome of non-invasive treatment modalities on back pain: an evidence-based review.�Eur Spine J.�2006;15(Suppl 1):S64�S81. doi: 10.1007/s00586-005-1048-6.�[PMC free article]�[PubMed]�[Cross Ref]
Lawrence DJ, Meeker W, Branson R, Bronfort G, Cates JR, Haas M. Chiropractic management of low back pain and low back-related leg complaints: a literature synthesis.�J Manipulative Physiol Ther.�2008;31:659�674. doi: 10.1016/j.jmpt.2008.10.007.�[PubMed]�[Cross Ref]
Bronfort G, Haas M, Evans R, Kawchuk G, Dagenais S. Evidence-informed management of chronic low back pain with spinal manipulation and mobilization.�Spine J.�2008;8:213�225. doi: 10.1016/j.spinee.2007.10.023.�[PubMed]�[Cross Ref]
Bronfort G, Haas M, Evans RL, Bouter LM. Efficacy of spinal manipulation and mobilization for low back pain and neck pain: a systematic review and best evidence synthesis.�Spine J.�2004;4:335�356. doi: 10.1016/j.spinee.2003.06.002.�[PubMed]�[Cross Ref]
Furlan AD, Imamura M, Dryden T, Irvin E. Massage for Low Back Pain: An Updated Systematic Review Within the Framework of the Cochrane Back Review Group.�Spine.�2009;34:1669�1684. doi: 10.1097/BRS.0b013e3181ad7bd6.�[PubMed]�[Cross Ref]
National Institute for Health and Clinical Excellence. Low back pain: Early management of persistent non-specific low back pain.�Clinical guideline.�2009;88
Hallegraeff JM, de Greef M, Winters JC, Lucas C. Manipulative therapy and clinical prediction criteria in treatment of acute nonspecific low back pain.�Percept Mot Skills.�2009;108:196�208. doi: 10.2466/PMS.108.1.196-208.�[PubMed]�[Cross Ref]
Rasmussen J, Laetgaard J, Lindecrona AL, Qvistgaard E, Bliddal H. Manipulation does not add to the effect of extension exercises in chronic low-back pain (LBP). A randomized, controlled, double blind study.�Joint Bone Spine.�2008;75:708�713.�[PubMed]
Little P, Lewith G, Webley F, Evans M, Beattie A, Middleton K. Randomised controlled trial of Alexander technique lessons, exercise, and massage (ATEAM) for chronic and recurrent back pain.�Br J Sports Med.�2008;42:965�968. doi: 10.1136/bjsm.2007.039560.�[PubMed]�[Cross Ref]
Wilkey A, Gregory M, Byfield D, McCarthy PW. A comparison between chiropractic management and pain clinic management for chronic low-back pain in a national health service outpatient clinic.�J Altern Complement Med.�2008;14:465�473. doi: 10.1089/acm.2007.0796.�[PubMed]�[Cross Ref]
Bogefeldt J, Grunnesjo MI, Svardsudd K, Blomberg S. Sick leave reductions from a comprehensive manual therapy programme for low back pain: the Gotland Low Back Pain Study.�Clin Rehabil.�2008;22:529�541. doi: 10.1177/0269215507087294.�[PubMed]�[Cross Ref]
Hancock MJ, Maher CG, Latimer J, McLachlan AJ, Cooper CW, Day RO. Assessment of diclofenac or spinal manipulative therapy, or both, in addition to recommended first-line treatment for acute low back pain: a randomised controlled trial.�Lancet.�2007;370:1638�1643. doi: 10.1016/S0140-6736(07)61686-9.�[PubMed]�[Cross Ref]
Ferreira ML, Ferreira PH, Latimer J, Herbert RD, Hodges PW, Jennings MD. Comparison of general exercise, motor control exercise and spinal manipulative therapy for chronic low back pain: A randomized trial.�Pain.�2007;131:31�37. doi: 10.1016/j.pain.2006.12.008.�[PubMed]�[Cross Ref]
Eisenberg DM, Post DE, Davis RB, Connelly MT, Legedza AT, Hrbek AL. Addition of choice of complementary therapies to usual care for acute low back pain: a randomized controlled trial.�Spine.�2007;32:151�158. doi: 10.1097/01.brs.0000252697.07214.65.�[PubMed]�[Cross Ref]
Hondras MA, Long CR, Cao Y, Rowell RM, Meeker WC. A randomized controlled trial comparing 2 types of spinal manipulation and minimal conservative medical care for adults 55 years and older with subacute or chronic low back pain.�J Manipulative Physiol Ther.�2009;32:330�343. doi: 10.1016/j.jmpt.2009.04.012.�[PubMed]�[Cross Ref]
Mohseni-Bandpei MA, Critchley J, Staunton T. A prospective randomised controlled trial of spinal manipulation and ultrasound in the treatment of chronic low back pain.�Physiotherapy.�2006;92:34�42. doi: 10.1016/j.physio.2005.05.005.�[Cross Ref]
Beyerman KL, Palmerino MB, Zohn LE, Kane GM, Foster KA. Efficacy of treating low back pain and dysfunction secondary to osteoarthritis: chiropractic care compared with moist heat alone.�J Manipulative Physiol Ther.�2006;29:107�114. doi: 10.1016/j.jmpt.2005.10.005.�[PubMed][Cross Ref]
Poole H, Glenn S, Murphy P. A randomised controlled study of reflexology for the management of chronic low back pain.�Eur J Pain.�2007;11:878�887. doi: 10.1016/j.ejpain.2007.01.006.�[PubMed][Cross Ref]
Zaproudina N, Hietikko T, Hanninen OO, Airaksinen O. Effectiveness of traditional bone setting in treating chronic low back pain: a randomised pilot trial.�Complement Ther Med.�2009;17:23�28. doi: 10.1016/j.ctim.2008.08.005.�[PubMed]�[Cross Ref]
Australian Acute Musculoskeletal Pain Guidelines Group.�Evidence-Based Management of Acute Musculoskeletal Pain.�Bowen Hills QLD, Australian Academic Press Pty. Ltd; 2003.
Bussieres AE, Taylor JA, Peterson C. Diagnostic imaging practice guidelines for musculoskeletal complaints in adults-an evidence-based approach-part 3: spinal disorders.�J Manipulative Physiol Ther.�2008;31:33�88. doi: 10.1016/j.jmpt.2007.11.003.�[PubMed]�[Cross Ref]
Schiller L. Effectiveness of spinal manipulative therapy in the treatment of mechanical thoracic spine pain: a pilot randomized clinical trial.�J Manipulative Physiol Ther.�2001;24:394�401. doi: 10.1067/mmt.2001.116420.�[PubMed]�[Cross Ref]
Cleland JA, Childs JD, McRae M, Palmer JA, Stowell T. Immediate effects of thoracic manipulation in patients with neck pain: a randomized clinical trial.�Man Ther.�2005;10:127�135. doi: 10.1016/j.math.2004.08.005.�[PubMed]�[Cross Ref]
Savolainen A, Ahlberg J, Nummila H, Nissinen M. Active or passive treatment for neck-shoulder pain in occupational health care? A randomized controlled trial.�Occup Med (Lond)�2004;54:422�424. doi: 10.1093/occmed/kqh070.�[PubMed]�[Cross Ref]
Allison GT, Nagy BM, Hall T. A randomized clinical trial of manual therapy for cervico-brachial pain syndrome — a pilot study.�Man Ther.�2002;7:95�102. doi: 10.1054/math.2002.0453.�[PubMed][Cross Ref]
Bergman GJ, Winters JC, Groenier KH, Pool JJ, Meyboom-de Jong B, Postema K. Manipulative therapy in addition to usual medical care for patients with shoulder dysfunction and pain: a randomized, controlled trial.�Ann Intern Med.�2004;141:432�439.�[PubMed]
Winters JC, Sobel JS, Groenier KH, Arendzen HJ, Meyboom-de Jong B. Comparison of physiotherapy, manipulation, and corticosteroid injection for treating shoulder complaints in general practice: randomised, single blind study.�BMJ.�1997;314:1320�1325.�[PMC free article]�[PubMed]
Winters JC, Jorritsma W, Groenier KH, Sobel JS, Meyboom-de Jong B, Arendzen HJ. Treatment of shoulder complaints in general practice: long term results of a randomised, single blind study comparing physiotherapy, manipulation, and corticosteroid injection.�BMJ.�1999;318:1395�1396.[PMC free article]�[PubMed]
Haldeman S, Carroll L, Cassidy D, Schubert J, Nygren A. The Bone and Joint Decade 2000-2010 Task Force on Neck Pain and Its Associated Disorders: executive summary.�Spine.�2008;33:S5�S7. doi: 10.1097/BRS.0b013e3181643f40.�[PubMed]�[Cross Ref]
Hurwitz EL, Carragee EJ, Velde G van der, Carroll LJ, Nordin M, Guzman J. Treatment of neck pain: noninvasive interventions: results of the Bone and Joint Decade 2000-2010 Task Force on Neck Pain and Its Associated Disorders.�J Manipulative Physiol Ther.�2009;32:S141�S175. doi: 10.1016/j.jmpt.2008.11.017.�[PubMed]�[Cross Ref]
Childs JD, Cleland JA, Elliott JM, Teyhen DS, Wainner RS, Whitman JM. Neck pain: Clinical practice guidelines linked to the International Classification of Functioning, Disability, and Health from the Orthopedic Section of the American Physical Therapy Association.�J Orthop Sports Phys Ther.�2008;38:A1�A34.�[PubMed]
Ernst E. Chiropractic spinal manipulation for neck pain: a systematic review.�J Pain.�2003;4:417�421. doi: 10.1067/S1526-5900(03)00735-1.�[PubMed]�[Cross Ref]
Gross AR, Hoving JL, Haines TA, Goldsmith CH, Kay T, Aker P. Manipulation and mobilisation for mechanical neck disorders.�Cochrane Database Syst Rev.�2004. p. CD004249.�[PubMed]
Vernon HT, Humphreys BK, Hagino CA. A systematic review of conservative treatments for acute neck pain not due to whiplash.�J Manipulative Physiol Ther.�2005;28:443�448. doi: 10.1016/j.jmpt.2005.06.011.�[PubMed]�[Cross Ref]
Ezzo J, Haraldsson BG, Gross AR, Myers CD, Morien A, Goldsmith CH. Massage for mechanical neck disorders: a systematic review.�Spine (Phila Pa 1976)�2007;32:353�362.�[PubMed]
Hakkinen A, Salo P, Tarvainen U, Wiren K, Ylinen J. Effect of manual therapy and stretching on neck muscle strength and mobility in chronic neck pain.�J Rehabil Med.�2007;39:575�579. doi: 10.2340/16501977-0094.�[PubMed]�[Cross Ref]
Gonzalez-Iglesias J, Fernandez-de-las-Penas C, Cleland JA, Gutierrez-Vega MR. Thoracic spine manipulation for the management of patients with neck pain: a randomized clinical trial.�J Orthop Sports Phys Ther.�2009;39:20�27.�[PubMed]
Gonzalez-Iglesias J, Fernandez-de-las-Penas C, Cleland JA, Alburquerque-Sendin F, Palomeque-del-Cerro L, Mendez-Sanchez R. Inclusion of thoracic spine thrust manipulation into an electro-therapy/thermal program for the management of patients with acute mechanical neck pain: a randomized clinical trial.�Man Ther.�2009;14:306�313. doi: 10.1016/j.math.2008.04.006.�[PubMed][Cross Ref]
Walker MJ, Boyles RE, Young BA, Strunce JB, Garber MB, Whitman JM. The effectiveness of manual physical therapy and exercise for mechanical neck pain: a randomized clinical trial.�Spine (Phila Pa 1976)�2008;33:2371�2378.�[PubMed]
Cleland JA, Glynn P, Whitman JM, Eberhart SL, MacDonald C, Childs JD. Short-term effects of thrust versus nonthrust mobilization/manipulation directed at the thoracic spine in patients with neck pain: a randomized clinical trial.�Phys Ther.�2007;87:431�440. doi: 10.2522/ptj.20060155.�[PubMed][Cross Ref]
Fernandez-de-las-Penas C, Fernandez-Carnero J, Fernandez A, Lomas-Vega R, Miangolarra-Page JC. Dorsal Manipulation in Whiplash Injury Treatment: A Randomized Controlled Trial.�Journal of Whiplash & Related Disorders.�2004;3:55�72. doi: 10.1300/J180v03n02_05.�[Cross Ref]
Zaproudina N, Hanninen OO, Airaksinen O. Effectiveness of traditional bone setting in chronic neck pain: randomized clinical trial.�J Manipulative Physiol Ther.�2007;30:432�437. doi: 10.1016/j.jmpt.2007.05.004.�[PubMed]�[Cross Ref]
Maigne JY, Chatellier G, Faou ML, Archambeau M. The treatment of chronic coccydynia with intrarectal manipulation: a randomized controlled study.�Spine (Phila Pa 1976)�2006;31:E621�E627.[PubMed]
Bussieres AE, Peterson C, Taylor JA. Diagnostic imaging guideline for musculoskeletal complaints in adults-an evidence-based approach-part 2: upper extremity disorders.�J Manipulative Physiol Ther.�2008;31:2�32. doi: 10.1016/j.jmpt.2007.11.002.�[PubMed]�[Cross Ref]
Green S, Buchbinder R, Hetrick S. Physiotherapy interventions for shoulder pain.�Cochrane Database Syst Rev.�2003. p. CD004258.�[PubMed]
Desmeules F, Cote CH, Fremont P. Therapeutic exercise and orthopedic manual therapy for impingement syndrome: a systematic review.�Clin J Sport.�2003;13:176�182. doi: 10.1097/00042752-200305000-00009.�[PubMed]�[Cross Ref]
Bang MD, Deyle GD. Comparison of supervised exercise with and without manual physical therapy for patients with shoulder impingement syndrome.�J Orthop Sports Phys Ther.�2000;30:126�137.[PubMed]
Bulgen DY, Binder AI, Hazleman BL, Dutton J, Roberts S. Frozen shoulder: prospective clinical study with an evaluation of three treatment regimens.�Ann Rheum Dis.�1984;43:353�360. doi: 10.1136/ard.43.3.353.�[PMC free article]�[PubMed]�[Cross Ref]
Conroy DE, Hayes KW. The effect of joint mobilization as a component of comprehensive treatment for primary shoulder impingement syndrome.�J Orthop Sports Phys Ther.�1998;28:3�14.�[PubMed]
Nicholson GG. The effects of passive joint mobilization on pain and hypomobility associated with adhesive capsulitis of the shoulder.�J Orthop Sports Phys Ther.�1985;6:238�246.�[PubMed]
Winters JC, Jorritsma W, Groenier KH, Sobel JS, Meyboom-de Jong B, Arendzen HJ. Treatment of shoulder complaints in general practice: long term results of a randomised, single blind study comparing physiotherapy, manipulation, and corticosteroid injection.�BMJ.�1999;318:1395�1396.[PMC free article]�[PubMed]
Windt DA van der, Koes BW, Deville W, Boeke AJP, de Jong BA, Bouter LM. Effectiveness of corticosteroid injections versus physiotherapy for treatment of painful stiff shoulder in primary care: randomised trial.�BMJ.�1998;317:1292�1296.�[PMC free article]�[PubMed]
Philadelphia Panel evidence-based clinical practice guidelines on selected rehabilitation interventions for shoulder pain.�Phys Ther.�2001;81:1719�1730.�[PubMed]
Vermeulen HM, Rozing PM, Obermann WR, le Cessie S, Vliet Vlieland TP. Comparison of high-grade and low-grade mobilization techniques in the management of adhesive capsulitis of the shoulder: randomized controlled trial.�Phys Ther.�2006;86:355�368.�[PubMed]
Dolder PA van den, Roberts DL. A trial into the effectiveness of soft tissue massage in the treatment of shoulder pain.�Aust J Physiother.�2003;49:183�188.�[PubMed]
Johnson AJ, Godges JJ, Zimmerman GJ, Ounanian LL. The effect of anterior versus posterior glide joint mobilization on external rotation range of motion in patients with shoulder adhesive capsulitis.�J Orthop Sports Phys Ther.�2007;37:88�99.�[PubMed]
Guler-Uysal F, Kozanoglu E. Comparison of the early response to two methods of rehabilitation in adhesive capsulitis.�Swiss Med Wkly.�2004;134:353�358.�[PubMed]
Piligian G, Herbert R, Hearns M, Dropkin J, Landsbergis P, Cherniack M. Evaluation and management of chronic work-related musculoskeletal disorders of the distal upper extremity.�Am J Ind Med.�2000;37:75�93. doi: 10.1002/(SICI)1097-0274(200001)37:1<75::AID-AJIM7>3.0.CO;2-4.[PubMed]�[Cross Ref]
Bisset L, Paungmali A, Vicenzino B, Beller E. A systematic review and meta-analysis of clinical trials on physical interventions for lateral epicondylalgia.�Br J Sports Med.�2005;39:411�422. doi: 10.1136/bjsm.2004.016170.�[PMC free article]�[PubMed]�[Cross Ref]
McHardy A, Hoskins W, Pollard H, Onley R, Windsham R. Chiropractic treatment of upper extremity conditions: a systematic review.�J Manipulative Physiol Ther.�2008;31:146�159. doi: 10.1016/j.jmpt.2007.12.004.�[PubMed]�[Cross Ref]
Smidt N, Assendelft WJ, Arola H, Malmivaara A, Greens S, Buchbinder R. Effectiveness of physiotherapy for lateral epicondylitis: a systematic review.�Ann Med.�2003;35:51�62. doi: 10.1080/07853890310004138.�[PubMed]�[Cross Ref]
Langen-Pieters P, Weston P, Brantingham JW. A randomized, prospective pilot study comparing chiropractic care and ultrasound for the treatment of lateral epicondylitis.�Eur J Chiro.�2003;50:211�8.
Vicenzino B, Collins D, Wright A. The initial effects of a cervical spine manipulative physiotherapy treatment on the pain and dysfunction of lateral epicondylalgia.�Pain.�1996;68:69�74. doi: 10.1016/S0304-3959(96)03221-6.�[PubMed]�[Cross Ref]
Paungmali A, O’Leary S, Souvlis T, Vicenzino B. Hypoalgesic and sympathoexcitatory effects of mobilization with movement for lateral epicondylalgia.�Phys Ther.�2003;83:374�383.�[PubMed]
Struijs PA, Damen PJ, Bakker EW, Blankevoort L, Assendelft WJ, van Dijk CN. Manipulation of the wrist for management of lateral epicondylitis: a randomized pilot study.�Phys Ther.�2003;83:608�616.�[PubMed]
Vicenzino B, Paungmali A, Buratowski S, Wright A. Specific manipulative therapy treatment for chronic lateral epicondylalgia produces uniquely characteristic hypoalgesia.�Man Ther.�2001;6:205�212. doi: 10.1054/math.2001.0411.�[PubMed]�[Cross Ref]
Smidt N, Windt DA van der, Assendelft WJ, Deville WL, Korthals-de Bos IB, Bouter LM. Corticosteroid injections, physiotherapy, or a wait-and-see policy for lateral epicondylitis: a randomised controlled trial.�Lancet.�2002;359:657�662. doi: 10.1016/S0140-6736(02)07811-X.[PubMed]�[Cross Ref]
Drechsler WI, Knarr JF, Snyder-Mackler L. A comparison of two treatment regimens for lateral epicondylitis: a randomized trial of clinical interventions.�J Sport Rehabil.�1997;6:226�234.
Dwars BJ, Feiter Pde, Patka P, Haarman H. Functional treatment of tennis elbow.�Sports Medicine and Health.�1990. pp. 237�241.
Verhaar JA, Walenkamp GH, van Mameren H, Kester AD, Linden AJ van der. Local corticosteroid injection versus Cyriax-type physiotherapy for tennis elbow.�J Bone Joint Surg Br.�1996;78:128�132.[PubMed]
Bisset L, Beller E, Jull G, Brooks P, Darnell R, Vicenzino B. Mobilisation with movement and exercise, corticosteroid injection, or wait and see for tennis elbow: randomised trial.�BMJ.�2006;333:939. doi: 10.1136/bmj.38961.584653.AE.�[PMC free article]�[PubMed]�[Cross Ref]
Nourbakhsh MR, Fearon FJ. The effect of oscillating-energy manual therapy on lateral epicondylitis: a randomized, placebo-control, double-blinded study.�J Hand Ther.�2008;21:4�13. doi: 10.1197/j.jht.2007.09.005.�[PubMed]�[Cross Ref]
Bjordal JM, Lopes-Martins RA, Joensen J, Couppe C, Ljunggren AE, Stergioulas A. A systematic review with procedural assessments and meta-analysis of low level laser therapy in lateral elbow tendinopathy (tennis elbow)�BMC Musculoskelet Disord.�2008;9:75. doi: 10.1186/1471-2474-9-75.[PMC free article]�[PubMed]�[Cross Ref]
Trinh KV, Phillips SD, Ho E, Damsma K. Acupuncture for the alleviation of lateral epicondyle pain: a systematic review.�Rheumatology (Oxford)�2004;43:1085�1090. doi: 10.1093/rheumatology/keh247.�[PubMed]�[Cross Ref]
American Academy of Orthopaedic Surgeons. Clinical practic guidelines on the diagnosis of carpal tunnel syndrome. 2008.
O’Connor D, Marshall S, Massy-Westropp N. Non-surgical treatment (other than steroid injection) for carpal tunnel syndrome.�Cochrane Database Syst Rev.�2003. p. CD003219.�[PubMed]
Goodyear-Smith F, Arroll B. What can family physicians offer patients with carpal tunnel syndrome other than surgery? A systematic review of nonsurgical management.�Ann Fam Med.�2004;2:267�273. doi: 10.1370/afm.21.�[PMC free article]�[PubMed]�[Cross Ref]
Piazzini DB, Aprile I, Ferrara PE, Bertolini C, Tonali P, Maggi L. A systematic review of conservative treatment of carpal tunnel syndrome.�Clin Rehabil.�2007;21:299�314. doi: 10.1177/0269215507077294.�[PubMed]�[Cross Ref]
Davis PT, Hulbert JR, Kassak KM, Meyer JJ. Comparative efficacy of conservative medical and chiropractic treatments for carpal tunnel syndrome: a randomized clinical trial.�J Manipulative Physiol Ther.�1998;21:317�326.�[PubMed]
Tal-Akabi A, Rushton A. An investigation to compare the effectiveness of carpal bone mobilisation and neurodynamic mobilisation as methods of treatment for carpal tunnel syndrome.�Man Ther.�2000;5:214�222. doi: 10.1054/math.2000.0355.�[PubMed]�[Cross Ref]
Cibulka MT, White DM, Woehrle J, Harris-Hayes M, Enseki K, Fagerson TL. Hip pain and mobility deficits–hip osteoarthritis: clinical practice guidelines linked to the international classification of functioning, disability, and health from the orthopaedic section of the American Physical Therapy Association.�J Orthop Sports Phys Ther.�2009;39:A1�25.�[PMC free article]�[PubMed]
Bussieres AE, Taylor JA, Peterson C. Diagnostic imaging practice guidelines for musculoskeletal complaints in adults–an evidence-based approach. Part 1. Lower extremity disorders.�J Manipulative Physiol Ther.�2007;30:684�717. doi: 10.1016/j.jmpt.2007.10.004.�[PubMed]�[Cross Ref]
Brantingham JW, Globe G, Pollard H, Hicks M, Korporaal C, Hoskins W. Manipulative therapy for lower extremity conditions: expansion of literature review.�J Manipulative Physiol Ther.�2009;32:53�71. doi: 10.1016/j.jmpt.2008.09.013.�[PubMed]�[Cross Ref]
Hoeksma HL, Dekker J, Ronday HK, Heering A, van der LN, Vel C. Comparison of manual therapy and exercise therapy in osteoarthritis of the hip: a randomized clinical trial.�Arthritis Rheum.�2004;51:722�729. doi: 10.1002/art.20685.�[PubMed]�[Cross Ref]
National Institute for Health and Clinical Excellence. Osteoarthritis: National clinical guideline for care and management in adults.�Clinical guideline 59.�2008.
Licciardone JC, Stoll ST, Cardarelli KM, Gamber RG, Swift JN Jr, Winn WB. A randomized controlled trial of osteopathic manipulative treatment following knee or hip arthroplasty.�J Am Osteopath Assoc.�2004;104:193�202.�[PubMed]
Hernandez-Molina G, Reichenbach S, Zhang B, Lavalley M, Felson DT. Effect of therapeutic exercise for hip osteoarthritis pain: results of a meta-analysis.�Arthritis Rheum.�2008;59:1221�1228. doi: 10.1002/art.24010.�[PMC free article]�[PubMed]�[Cross Ref]
Deyle GD, Henderson NE, Matekel RL, Ryder MG, Garber MB, Allison SC. Effectiveness of manual physical therapy and exercise in osteoarthritis of the knee. A randomized, controlled trial.�Ann Intern Med.�2000;132:173�181.�[PubMed]
Deyle GD, Allison SC, Matekel RL, Ryder MG, Stang JM, Gohdes DD. Physical therapy treatment effectiveness for osteoarthritis of the knee: a randomized comparison of supervised clinical exercise and manual therapy procedures versus a home exercise program.�Phys Ther.�2005;85:1301�1317.[PubMed]
Crossley K, Bennell K, Green S, Cowan S, McConnell J. Physical therapy for patellofemoral pain: a randomized, double-blinded, placebo-controlled trial.�Am J Sports Med.�2002;30:857�865.[PubMed]
Suter E, McMorland G, Herzog W, Bray R. Conservative lower back treatment reduces inhibition in knee-extensor muscles: a randomized controlled trial.�J Manipulative Physiol Ther.�2000;23:76�80. doi: 10.1016/S0161-4754(00)90071-X.�[PubMed]�[Cross Ref]
Bennell KL, Hinman RS, Metcalf BR, Buchbinder R, McConnell J, McColl G. Efficacy of physiotherapy management of knee joint osteoarthritis: a randomised, double blind, placebo controlled trial.�Ann Rheum Dis.�2005;64:906�912. doi: 10.1136/ard.2004.026526.[PMC free article]�[PubMed]�[Cross Ref]
Moss P, Sluka K, Wright A. The initial effects of knee joint mobilization on osteoarthritic hyperalgesia.�Man Ther.�2007;12:109�118. doi: 10.1016/j.math.2006.02.009.�[PubMed]�[Cross Ref]
Tucker M, Brantingham JW, Myburg C. The relative effectiveness of a non-sterodial anti-inflammatory medicaion (meloxicam) versus manipulation in the treatment of osteoarthritis of the knee.�Eur J Chiro.�2003;50:163�84.
Rowlands B, Brantingham JW. The efficacy of patella mobilisation in patients suffering from patellofemoral pain syndrome.�J Neuromusculoskel System.�1999;7:9.
Stakes N, Myburgh C, Brantingham JW, Moyer R, Jensen M, Globe G. A prospective randomized clinical trial to determine efficacy of combined spinal manipulation and patella mobilization compared to patella mobilization alone in the conservative management of patellofemoral pain syndrome.�J Am Chiro Assoc.�2006;43:11�8.
Taylor K, Brantingham JW. An investigation into the effect of exercise combined with patella mobilisation/manipulation in the treatment of patellofemoral pain syndrome.�Eur J Chiro.�2003;51:17.
Pollard H, Ward G, Hoskins W, Hardy K. The effect of a manual therapy knee protocol on osteoarthritic knee pain: a randomised controlled trial.�JCCA J Can Chiropr Assoc.�2008;52:229�242.�[PMC free article]�[PubMed]
Perlman AI, Sabina A, Williams AL, Njike VY, Katz DL. Massage therapy for osteoarthritis of the knee: a randomized controlled trial.�Arch Intern Med.�2006;166:2533�2538. doi: 10.1001/archinte.166.22.2533.�[PubMed]�[Cross Ref]
Vavken P, Arrich F, Schuhfried O, Dorotka R. Effectiveness of pulsed electromagnetic field therapy in the management of osteoarthritis of the knee: a meta-analysis of randomized controlled trials.�J Rehabil Med.�2009;41:406�411. doi: 10.2340/16501977-0374.�[PubMed]�[Cross Ref]
Hulme J, Robinson V, DeBie R, Wells G, Judd M, Tugwell P. Electromagnetic fields for the treatment of osteoarthritis.�Cochrane Database Syst Rev.�2002. p. CD003523.�[PubMed]
White A, Foster NE’, Cummings M, Barlas P. Acupuncture treatment for chronic knee pain: a systematic review.�Rheumatology (Oxford)�2007;46:384�390. doi: 10.1093/rheumatology/kel413.[PubMed]�[Cross Ref]
Fransen M, McConnell S. Exercise for osteoarthritis of the knee.�Cochrane Database Syst Rev.�2008. p. CD004376.�[PubMed]
Bjordal JM, Johnson MI, Lopes-Martins RA, Bogen B, Chow R, Ljunggren AE. Short-term efficacy of physical interventions in osteoarthritic knee pain. A systematic review and meta-analysis of randomised placebo-controlled trials.�BMC Musculoskelet Disord.�2007;8:51. doi: 10.1186/1471-2474-8-51.�[PMC free article]�[PubMed]�[Cross Ref]
Wees PJ van der, Lenssen AF, Hendriks EJ, Stomp DJ, Dekker J, de Bie RA. Effectiveness of exercise therapy and manual mobilisation in ankle sprain and functional instability: a systematic review.�Aust J Physiother.�2006;52:27�37.�[PubMed]
Vicenzino B, Branjerdporn M, Teys P, Jordan K. Initial changes in posterior talar glide and dorsiflexion of the ankle after mobilization with movement in individuals with recurrent ankle sprain.�J Orthop Sports Phys Ther.�2006;36:464�471. doi: 10.2519/jospt.2006.2265.�[PubMed][Cross Ref]
Eisenhart AW, Gaeta TJ, Yens DP. Osteopathic manipulative treatment in the emergency department for patients with acute ankle injuries.�J Am Osteopath Assoc.�2003;103:417�421.�[PubMed]
Green T, Refshauge K, Crosbie J, Adams R. A randomized controlled trial of a passive accessory joint mobilization on acute ankle inversion sprains.�Phys Ther.�2001;81:984�994.�[PubMed]
Pellow JE, Brantingham JW. The efficacy of adjusting the ankle in the treatment of subacute and chronic grade I and grade II ankle inversion sprains.�J Manipulative Physiol Ther.�2001;24:17�24. doi: 10.1067/mmt.2001.112015.�[PubMed]�[Cross Ref]
Coetzer D, Brantingham JW, Nook B. The relative effectiveness of piroxicam compared to manipulation in the treatment of acute grades 1 and 2 inversion ankle sprains.�J Neuromusculoskel System.�2001;9:9�12.
Collins N. P. Vicenzino B. The initial effects of a Mulligan’s mobilization with movement technique on dorsiflexion and pain in subacute ankle sprains.�Man Ther.�2004;9:77�82. doi: 10.1016/S1356-689X(03)00101-2.�[PubMed]�[Cross Ref]
Lopez-Rodriguez S, Fernandez de-Las-Penas C, Alburquerque-Sendin F, Rodriguez-Blanco C, Palomeque-del-Cerro L. Immediate effects of manipulation of the talocrural joint on stabilometry and baropodometry in patients with ankle sprain.�J Manipulative Physiol Ther.�2007;30:186�192. doi: 10.1016/j.jmpt.2007.01.011.�[PubMed]�[Cross Ref]
Kohne E, Jones A, Korporaal C, Price JL, Brantingham JW, Globe G. A prospective, single-blinded, randomized, controlled clinical trial of the effects of manipulation on proprioception and ankle dorsiflexion in chronic recurrect ankle sprain.�J Am Chiro Assoc.�2007;44:7�17.
Dimou E, Brantingham JW, Wood T. A randomized, controlled trial (with blinded observer) of chiropractic manipulation and Achilles stretching vs orthotics for the treatment of plantar fasciitis.�J Am Chiro Assoc.�2004;41:32�42.
Govender N, Kretzmann H, Price J, Brantingham JW, Globe G. A single-blinded randomized placebo-controlled clinical trial of manipulation and mobilization in the treatment of Morton’s neuroma.�J Am Chiro Assoc.�2007;44:9�18.
Shamus J, Shamus E, Gugel RN, Brucker BS, Skaruppa C. The effect of sesamoid mobilization, flexor hallucis strengthening, and gait training on reducing pain and restoring function in individuals with hallux limitus: a clinical trial.�J Orthop Sports Phys Ther.�2004;34:368�376. doi: 10.1016/S8756-3282(04)00007-9.�[PubMed]�[Cross Ref]
Brantingham JW, Guiry S, Kretzmann H, Globe G, Kite V. A pilot study of the efficacy of a conservative chiropractic protocol using graded mobilization and ice in the treatment of sympomatic hallux abductogalvus bunions.�Clin Chiro.�2005;8:117�33. doi: 10.1016/j.clch.2005.06.001.[Cross Ref]
Brooks SC, Potter BT, Rainey JB. Treatment for partial tears of the lateral ligament of the ankle: a prospective trial.�Br Med J (Clin Res Ed)�1981;282:606�607. doi: 10.1136/bmj.282.6264.606.[PMC free article]�[PubMed]�[Cross Ref]
Wynne MM, Burns JM, Eland DC, Conatser RR, Howell JN. Effect of counterstrain on stretch reflexes, hoffmann reflexes, and clinical outcomes in subjects with plantar fasciitis.�J Am Osteopath Assoc.�2006;106:547�556.�[PubMed]
Cleland JA, Abbott JH, Kidd MO, Stockwell S, Cheney S, Gerrard DF. Manual physical therapy and exercise versus electrophysical agents and exercise in the management of plantar heel pain: a multicenter randomized clinical trial.�J Orthop Sports Phys Ther.�2009;39:573�585.�[PubMed]
Lin CW, Moseley AM, Haas M, Refshauge KM, Herbert RD. Manual therapy in addition to physiotherapy does not improve clinical or economic outcomes after ankle fracture.�J Rehabil Med.�2008;40:433�439. doi: 10.2340/16501977-0187.�[PubMed]�[Cross Ref]
McPoil TG, Martin RL, Cornwall MW, Wukich DK, Irrgang JJ, Godges JJ. Heel pain–plantar fasciitis: clinical practice guildelines linked to the international classification of function, disability, and health from the orthopaedic section of the American Physical Therapy Association.�J Orthop Sports Phys Ther.�2008;38:A1�A18.�[PubMed]
Handoll HH, Rowe BH, Quinn KM, de Bie R. Interventions for preventing ankle ligament injuries.�Cochrane Database Syst Rev.�2001. p. CD000018.�[PubMed]
McNeill C.�Temporomandibular Disorders: Guidelines For Classification, Assessment, and Management.�Quintessence Publishing Co, Inc; 1993. Epidemiology; pp. 19�22.
Dworkin SF, Huggins KH, Wilson L, Mancl L, Turner J, Massoth D. A randomized clinical trial using research diagnostic criteria for temporomandibular disorders-axis II to target clinic cases for a tailored self-care TMD treatment program.�J Orofac Pain.�2002;16:48�63.�[PubMed]
McNeely ML, Armijo OS, Magee DJ. A systematic review of the effectiveness of physical therapy interventions for temporomandibular disorders.�Phys Ther.�2006;86:710�725.�[PubMed]
Medlicott MS, Harris SR. A systematic review of the effectiveness of exercise, manual therapy, electrotherapy, relaxation training, and biofeedback in the management of temporomandibular disorder.�Phys Ther.�2006;86:955�973.�[PubMed]
Taylor M, Suvinen T, Reade P. The effect of grade IV distraction mobilization on patients with temporomandibular pain-dysfunction disorder.�Physiotherapy Theory and Practice.�1994;10:129�136. doi: 10.3109/09593989409036389.�[Cross Ref]
Carmeli E, Sheklow SL, Blommenfeld I. Comparitive study of repositioning splint therapy and passive manual range of motion techniques for anterior displaced temporomandibular discs with unstable excursive reduction.�Physiotherapy.�2001;87:26�36. doi: 10.1016/S0031-9406(05)61189-3.[Cross Ref]
De Laat A, Stappaerts K, Papy S. Counseling and physical therapy as treatment for myofascial pain of the masticatory system.�J Orofac Pain.�2003;17:42�49.�[PubMed]
Monaco A, Cozzolino V, Cattaneo R, Cutilli T, Spadaro A. Osteopathic manipulative treatment (OMT) effects on mandibular kinetics: kinesiographic study.�Eur J Paediatr Dent.�2008;9:37�42.[PubMed]
Ismail F, Demling A, Hessling K, Fink M, Stiesch-Scholz M. Short-term efficacy of physical therapy compared to splint therapy in treatment of arthrogenous TMD.�J Oral Rehabil.�2007;34:807�813. doi: 10.1111/j.1365-2842.2007.01748.x.�[PubMed]�[Cross Ref]
Carville SF, Arendt-Nielsen S, Bliddal H, Blotman F, Branco JC, Buskila D. EULAR evidence-based recommendations for the management of fibromyalgia syndrome.�Ann Rheum Dis.�2008;67:536�541. doi: 10.1136/ard.2007.071522.�[PubMed]�[Cross Ref]
Wolfe F, Smythe HA, Yunus MB, Bennett RM, Bombardier C, Goldenberg DL. The American College of Rheumatology 1990 Criteria for the Classification of Fibromyalgia. Report of the Multicenter Criteria Committee.�Arthritis Rheum.�1990;33:160�172. doi: 10.1002/art.1780330203.[PubMed]�[Cross Ref]
Schneider M, Vernon H, Ko G, Lawson G, Perera J. Chiropractic management of fibromyalgia syndrome: a systematic review of the literature.�J Manipulative Physiol Ther.�2009;32:25�40. doi: 10.1016/j.jmpt.2008.08.012.�[PubMed]�[Cross Ref]
Ernst E. Chiropractic treatment for fibromyalgia: a systematic review.�Clin Rheumatol.�2009;28:1175�1178. doi: 10.1007/s10067-009-1217-9.�[PubMed]�[Cross Ref]
Goldenberg DL, Burckhardt C, Crofford L. Management of fibromyalgia syndrome.�JAMA.�2004;292:2388�2395. doi: 10.1001/jama.292.19.2388.�[PubMed]�[Cross Ref]
Blunt KL, Rajwani MH, Guerriero RC. The effectiveness of chiropractic management of fibromyalgia patients: a pilot study.�J Manipulative Physiol Ther.�1997;20:389�399.�[PubMed]
Tyers S, Smith RB. A comparison of cranial electrotherapy stimulation alone or with chiropractic therapies in the treatment of fibromyalgia.�Am Chiropractor.�2001;23:39�41.
Wise P, Walsh M, Littlejohn G. Efficacy of chiropractic treatment on fibromyalgia syndrome; a randomized controlled trial.�Eur J Chiro.�2002;102:321�5.
Panton LB, Figueroa A, Kingsley JD, Hornbuckle L, Wilson J, St John N. Effects of resistance training and chiropractic treatment in women with fibromyalgia.�J Altern Complement Med.�2009;15:321�328. doi: 10.1089/acm.2008.0132.�[PubMed]�[Cross Ref]
Gamber RG, Shores JH, Russo DP, Jimenez C, Rubin BR. Osteopathic manipulative treatment in conjunction with medication relieves pain associated with fibromyalgia syndrome: results of a randomized clinical pilot project.�J Am Osteopath Assoc.�2002;102:321�325.�[PubMed]
Brattberg G. Connective tissue massage in the treatment of fibromyalgia.�Eur J Pain.�1999;3:235�244. doi: 10.1016/S1090-3801(99)90050-2.�[PubMed]�[Cross Ref]
Richards KC, Gibson R, Overton-McCoy AL. Effects of massage in acute and critical care.�AACN Clin Issues.�2000;11:77�96. doi: 10.1097/00044067-200002000-00010.�[PubMed]�[Cross Ref]
Ekici G, Bakar Y, Akbayrak T, Yuksel I. Comparison of manual lymph drainage therapy and connective tissue massage in women with fibromyalgia: a randomized controlled trial.�J Manipulative Physiol Ther.�2009;32:127�133. doi: 10.1016/j.jmpt.2008.12.001.�[PubMed][Cross Ref]
Busch AJ, Barber KA, Overend TJ, Peloso PM, Schachter CL. Exercise for treating fibromyalgia syndrome.�Cochrane Database Syst Rev.�2007. p. CD003786.�[PubMed]
Vernon H, Schneider M. Chiropractic management of myofascial trigger points and myofascial pain syndrome: a systematic review of the literature.�J Manipulative Physiol Ther.�2009;32:14�24. doi: 10.1016/j.jmpt.2008.06.012.�[PubMed]�[Cross Ref]
Gam AN, Warming S, Larsen LH, Jensen B, Hoydalsmo O, Allon I. Treatment of myofascial trigger-points with ultrasound combined with massage and exercise–a randomised controlled trial.�Pain.�1998;77:73�79. doi: 10.1016/S0304-3959(98)00084-0.�[PubMed]�[Cross Ref]
Dardzinski JA, Ostrov BE, Hamann LS. Myofascial pain unresponsive to standard treatment: successful use of a strain and counterstrain technique with physical therapy.�J Clin Rheumatol.�2000;6:169�174. doi: 10.1097/00124743-200008000-00001.�[PubMed]�[Cross Ref]
Greene C, Debias D, Helig D, Nicholas A, England K, Ehrenfeuchter W. The effect of helium-neon laser and osteopathic manipulation on soft-tissue trigger points.�J Am Osteopath Assoc.�1990;90:638�639.
Hanten WP, Olson SL, Butts NL, Nowicki AL. Effectiveness of a home program of ischemic pressure followed by sustained stretch for treatment of myofascial trigger points.�Phys Ther.�2000;80:997�1003.�[PubMed]
Jaeger B, Reeves JL. Quantification of changes in myofascial trigger point sensitivity with the pressure algometer following passive stretch.�Pain.�1986;27:203�210. doi: 10.1016/0304-3959(86)90211-3.�[PubMed]�[Cross Ref]
Hong CZ, Chen YC, Pon CH, Yu J. Immediate effects of various physical medicine modalities on pain threshold of an active myofascial trigger point.�j musculoskel pain.�1993;1:37�53. doi: 10.1300/J094v01n02_04.�[Cross Ref]
Hou CR, Tsai LC, Cheng KF, Chung KC, Hong CZ. Immediate effects of various physical therapeutic modalities on cervical myofascial pain and trigger-point sensitivity.�Arch Phys Med Rehabil.�2002;83:1406�1414. doi: 10.1053/apmr.2002.34834.�[PubMed]�[Cross Ref]
Hanten WP, Barret M, Gillespie-Plesko M, Jump KA, Olson SL. Effects of active head retraction with retraction/extension and occipital release on the pressure pain threshold of cervical and scapular trigger points.�Physiother Theory Pract.�1997;13:285�291. doi: 10.3109/09593989709036475.[Cross Ref]
Fernandez-de-las-Penas C, Alonso-Blanco C, Fernandez-Carnero J, Miangolarra-Page JC. The immediate effects of ischemic compression technique and transverse friction massage on tenderness of active and latent myofascial trigger points: a pilot study.�J Bodywork Mov Ther.�2009;10:3�9. doi: 10.1016/j.jbmt.2005.05.003.�[Cross Ref]
Terrett AC, Vernon H. Manipulation and pain tolerance. A controlled study of the effect of spinal manipulation on paraspinal cutaneous pain tolerance levels.�Am J Phys Med.�1984;63:217�225.[PubMed]
Vernon HT, Aker P, Burns S, Viljakaanen S, Short L. Pressure pain threshold evaluation of the effect of spinal manipulation in the treatment of chronic neck pain: a pilot study.�J Manipulative Physiol Ther.�1990;13:13�16.�[PubMed]
Cote P, Mior SA, Vernon H. The short-term effect of a spinal manipulation on pain/pressure threshold in patients with chronic mechanical low back pain.�J Manipulative Physiol Ther.�1994;17:364�368.�[PubMed]
Atienza-Meseguer A, Fernandez-de-las-Penas C, Navarro-Poza JL, Rodriguez-Blanco C, Bosca-Gandia JJ. Immediate effects of the strain/counterstrain technique in local pain evoked by tender points in the upper trapezius muscle.�Clin Chiro.�2006;9:112�118. doi: 10.1016/j.clch.2006.06.003.[Cross Ref]
Fryer G, Hodgson L. The effect of manual pressure release on myofascial trigger points in the upper trapezius muscle.�J Bodywork Mov Ther.�2005;9:248�255. doi: 10.1016/j.jbmt.2005.02.002.[Cross Ref]
Cephalalgia.�2. Suppl 1. Vol. 24. 2004. The International Classification of Headache Disorders; pp. 9�160.�[PubMed]
Scotish Intercollegiate Guideline Network. Diagnosis and management of headache in adults. 2008.
Astin JA, Ernst E. The effectiveness of spinal manipulation for the treatment of headache disorders: a systematic review of randomized clinical trials.�Cephalalgia.�2002;22:617�623. doi: 10.1046/j.1468-2982.2002.00423.x.�[PubMed]�[Cross Ref]
Bronfort G, Nilsson N, Haas M, Evans R, Goldsmith CH, Assendelft WJ. Non-invasive physical treatments for chronic/recurrent headache.�Cochrane Database Syst Rev.�2004. p. CD001878.[PubMed]
Parker GB, Pryor DS, Tupling H. Why does migraine improve during a clinical trial? Further results from a trial of cervical manipulation for migraine.�Aust N Z J Med.�1980;10:192�198.�[PubMed]
Tuchin PJ, Pollard H, Bonello R. A randomized controlled trial of chiropractic spinal manipulative therapy for migraine.�J Manipulative Physiol Ther.�2000;23:91�95. doi: 10.1016/S0161-4754(00)90073-3.�[PubMed]�[Cross Ref]
Nelson CF, Bronfort G, Evans R, Boline P, Goldsmith C, Anderson AV. The efficacy of spinal manipulation, amitriptyline and the combination of both therapies for the prophylaxis of migraine headaches.�J Manipulative Physiol Ther.�1998;21:511�519.�[PubMed]
Lawler SP, Cameron LD. A randomized, controlled trial of massage therapy as a treatment for migraine.�Ann Behav Med.�2006;32:50�59. doi: 10.1207/s15324796abm3201_6.�[PubMed][Cross Ref]
Linde K, Allais G, Brinkhaus B, Manheimer E, Vickers A, White AR. Acupuncture for migraine prophylaxis.�Cochrane Database Syst Rev.�2009. p. CD001218.�[PMC free article]�[PubMed]
Nestoriuc Y, Martin A, Rief W, Andrasik F. Biofeedback treatment for headache disorders: a comprehensive efficacy review.�Appl Psychophysiol Biofeedback.�2008;33:125�140. doi: 10.1007/s10484-008-9060-3.�[PubMed]�[Cross Ref]
McCrory DC, Penzien DB, Hasselblad V, Gray RN. Evidence Report: Behavioral and Physical Treatments for Tension-type and Cervicogenic Headache.�FCER Research.�2001.
Lenssinck ML, Damen L, Verhagen AP, Berger MY, Passchier J, Koes BW. The effectiveness of physiotherapy and manipulation in patients with tension-type headache: a systematic review.�Pain.�2004;112:381�388. doi: 10.1016/j.pain.2004.09.026.�[PubMed]�[Cross Ref]
Fernandez-de-las-Penas C, Alonso-Blanco C, Cuadrado ML, Miangolarra JC, Barriga FJ, Pareja JA. Are manual therapies effective in reducing pain from tension-type headache?: a systematic review.�Clin J Pain.�2006;22:278�285. doi: 10.1097/01.ajp.0000173017.64741.86.�[PubMed]�[Cross Ref]
Boline PD, Kassak K, Bronfort G, Nelson C, Anderson AV. Spinal manipulation vs. amitriptyline for the treatment of chronic tension-type headaches: a randomized clinical trial.�J Manipulative Physiol Ther.�1995;18:148�154.�[PubMed]
Bove G, Nilsson N. Spinal manipulation in the treatment of episodic tension-type headache: a randomized controlled trial.�JAMA.�1998;280:1576�1579. doi: 10.1001/jama.280.18.1576.[PubMed]�[Cross Ref]
Hanten WP, Olson SL, hodson JL, imler VL, knab VM, Magee JL. The Effectiveness of CV-4 and Resting Position Techniques on Subjects with Tension-Type Headaches.�The Journal of Manual & Manipulative Therapy.�1999;7:64�70.
Demirturk F, Akarcali I, Akbayrak R, Citak I, Inan L. Results of two different manual therapy techniques in chronic tension-type headache.�The Pain Clinic.�2002;14:121�128. doi: 10.1163/156856902760196333.�[Cross Ref]
Donkin RD, Parkin-Smith GF, Gomes AN. Possible effect of chiropractic manipulation and combined manual traction and manipulation on tension-type headache: a pilot study.�Journal of the Neuromusculoskeletal System.�2002;10:89�97.
Ahonen E, Hakumaki M, Mahlamaki S, Partanen J, Riekkinen P, Sivenius J. Effectiveness of acupuncture and physiotherapy on myogenic headache: a comparative study.�Acupunct Electrother Res.�1984;9:141�150.�[PubMed]
Carlsson J, Fahlcrantz A, Augustinsson LE. Muscle tenderness in tension headache treated with acupuncture or physiotherapy.�Cephalalgia.�1990;10:131�141. doi: 10.1046/j.1468-2982.1990.1003131.x.�[PubMed]�[Cross Ref]
Wylie KR, Jackson C, Crawford PM. Does psychological testing help to predict the response to acupuncture or massage/relaxation therapy in patients presenting to a general neurology clinic with headache?�J Tradit Chin Med.�1997;17:130�139.�[PubMed]
Hoyt WH, Shaffer F, Bard DA, Benesler JS, Blankenhorn GD, Gray JH. Osteopathic manipulation in the treatment of muscle-contraction headache.�JAOA.�1979;78:322�325.�[PubMed]
Jay GW, Brunson J, Branson SJ. The effectiveness of physical therapy in the treatment of chronic daily headaches.�Headache.�1989;29:156�162. doi: 10.1111/j.1526-4610.1989.hed2903156.x.[PubMed]�[Cross Ref]
Marcus DA, Scharff L, Turk DC. Nonpharmacological management of headaches during pregnancy.�Psychosom Med.�1995;57:527�535.�[PubMed]
Anderson RE, Seniscal C. A comparison of selected osteopathic treatment and relaxation for tension-type headaches.�Headache.�2006;46:1273�1280. doi: 10.1111/j.1526-4610.2006.00535.x.�[PubMed][Cross Ref]
Linde K, Allais G, Brinkhaus B, Manheimer E, Vickers A, White AR. Acupuncture for tension-type headache.�Cochrane Database Syst Rev.�2009. p. CD007587.�[PMC free article]�[PubMed]
Sjaastad O, Fredriksen TA, Pfaffenrath V. Cervicogenic headache: diagnostic criteria.�Headache.�1998;38:442�445. doi: 10.1046/j.1526-4610.1998.3806442.x.�[PubMed]�[Cross Ref]
Fernandez-de-las-Penas C, Alonso-Blanco C, Cuadrado ML, Pareja JA. Spinal manipulative therapy in the management of cervicogenic headache.�Headache.�2005;45:1260�1263. doi: 10.1111/j.1526-4610.2005.00253_1.x.�[PubMed]�[Cross Ref]
Bitterli J, Graf R, Robert F, Adler R, Mumenthaler M. Zur Objektivierung der manualtherapeutischen BeeinfluBbarkeit des spondylogenen Kopfschmerzes [Objective criteria for the evaluation of chiropractic treatment of spondylotic headache]�Nervenarzt.�1977;48:259�262.[PubMed]
Howe DH, Newcombe RG, Wade MT. Manipulation of the cervical spine — a pilot study.�J R Coll Gen Pract.�1983;33:574�579.�[PMC free article]�[PubMed]
Ammer K, Hein L, Rathkolb O. [Physical therapy in occipital headaches]�Manuelle Med.�1990;28:65�68.
Jull G, Trott P, Potter H, Zito G, Niere K, Shirley D. A randomized controlled trial of exercise and manipulative therapy for cervicogenic headache.�Spine.�2002;27:1835�1843. doi: 10.1097/00007632-200209010-00004.�[PubMed]�[Cross Ref]
Nilsson N, Christensen HW, Hartvigsen J. The effect of spinal manipulation in the treatment of cervicogenic headache.�J Manipulative Physiol Ther.�1997;20:326�330.�[PubMed]
Whittingham W.�The efficacy of cervical adjustments (Toggle recoil) for chronic cervicogenic headaches [thesis]�Melbourne, Australia: Royal Melbourne Institute of Technology;; 1999.
Hall T, Chan HT, Christensen L, Odenthal B, Wells C, Robinson K. Efficacy of a C1-C2 self-sustained natural apophyseal glide (SNAG) in the management of cervicogenic headache.�J Orthop Sports Phys Ther.�2007;37:100�107.�[PubMed]
Jensen OK, Nielsen FF, Vosmar L. An open study comparing manual therapy with the use of cold packs in the treatment of post-traumatic headache.�Cephalalgia.�1990;10:241�250. doi: 10.1046/j.1468-2982.1990.1005241.x.�[PubMed]�[Cross Ref]
National Heart LaBI. US Guidelines on the Management of Asthma.�Expert Panel Report 3.�2007;3
Scottish Intercollegiate Guidelines Network. British Guideline on the Management of Asthma.�The British Thoracic Society.�2009. pp. 1�132.
Ernst E. Spinal manipulation for asthma: A systematic review of randomised clinical trials.�Respir Med.�2009;103:1791�1795. doi: 10.1016/j.rmed.2009.06.017.�[PubMed]�[Cross Ref]
Hondras MA, Linde K, Jones AP. Manual therapy for asthma.�Cochrane Database Syst Rev.�2001. p. CD001002.�[PubMed]
Balon JW, Mior SA. Chiropractic care in asthma and allergy.�Ann Allergy Asthma Immunol.�2004;93:S55�S60. doi: 10.1016/S1081-1206(10)61487-1.�[PubMed]�[Cross Ref]
Hawk C, Khorsan R, Lisi AJ, Ferrance RJ, Evans MW. Chiropractic care for nonmusculoskeletal conditions: a systematic review with implications for whole systems research.�J Altern Complement Med.�2007;13:491�512. doi: 10.1089/acm.2007.7088.�[PubMed]�[Cross Ref]
Nielsen NH, Bronfort G, Bendix T, Madsen F, Weeke B. Chronic asthma and chiropractic spinal manipulation: a randomized clinical trial.�Clin Exp Allergy.�1995;25:80�88. doi: 10.1111/j.1365-2222.1995.tb01006.x.�[PubMed]�[Cross Ref]
Balon J, Aker PD, Crowther ER, Danielson C, Cox PG, O’Shaughnessy D. A comparison of active and simulated chiropractic manipulation as adjunctive treatment for childhood asthma.�N Engl J Med.�1998;339:1013�1020. doi: 10.1056/NEJM199810083391501.�[PubMed]�[Cross Ref]
Guiney PA, Chou R, Vianna A, Lovenheim J. Effects of osteopathic manipulative treatment on pediatric patients with asthma: a randomized controlled trial.�J Am Osteopath Assoc.�2005;105:7�12.[PubMed]
Field T, Henteleff T, Hernandez-Reif M, Martinez E, Mavunda K, Kuhn C. Children with asthma have improved pulmonary functions after massage therapy.�J Pediatr.�1998;132:854�858. doi: 10.1016/S0022-3476(98)70317-8.�[PubMed]�[Cross Ref]
Brygge T, Heinig JH, Collins P, Ronborg S, Gehrchen PM, Hilden J. Reflexology and bronchial asthma.�Respir Med.�2001;95:173�179. doi: 10.1053/rmed.2000.0975.�[PubMed]�[Cross Ref]
BTS Guidelines for the Management of Community Acquired Pneumonia in Adults.�Thorax.�2001;56(Suppl 4):IV1�64.�[PMC free article]�[PubMed]
Mandell LA, Wunderink RG, Anzueto A, Bartlett JG, Campbell GD, Dean NC. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults.�Clin Infect Dis.�2007;44(Suppl 2):S27�S72. doi: 10.1086/511159.�[PubMed]�[Cross Ref]
Noll DR, Shores JH, Gamber RG, Herron KM, Swift J Jr. Benefits of osteopathic manipulative treatment for hospitalized elderly patients with pneumonia.�J Am Osteopath Assoc.�2000;100:776�782.�[PubMed]
Bhattacharyya N, Baugh RF, Orvidas L, Barrs D, Bronston LJ, Cass S. Clinical practice guideline: benign paroxysmal positional vertigo.�Otolaryngol Head Neck Surg.�2008;139:S47�S81. doi: 10.1016/j.otohns.2008.08.022.�[PubMed]�[Cross Ref]
Reid SA, Rivett DA. Manual therapy treatment of cervicogenic dizziness: a systematic review.�Man Ther.�2005;10:4�13. doi: 10.1016/j.math.2004.03.006.�[PubMed]�[Cross Ref]
Karlberg M, Magnusson M, Malmstrom EM, Melander A, Moritz U. Postural and symptomatic improvement after physiotherapy in patients with dizziness of suspected cervical origin.�Arch Phys Med Rehabil.�1996;77:874�882. doi: 10.1016/S0003-9993(96)90273-7.�[PubMed]�[Cross Ref]
Reid SA, Rivett DA, Katekar MG, Callister R. Sustained natural apophyseal glides (SNAGs) are an effective treatment for cervicogenic dizziness.�Man Ther.�2008;13:357�366. doi: 10.1016/j.math.2007.03.006.�[PubMed]�[Cross Ref]
Hillier SL, Hollohan V. Vestibular rehabilitation for unilateral peripheral vestibular dysfunction.�Cochrane Database Syst Rev.�2007. p. CD005397.�[PubMed]
Wessel MA, Cobb JC, Jackson EB, Harris GS, Detwiler AC. Paroxysmal fussing in infancy, sometimes called “colic”.�Pediatrics.�1954;14:421�434.�[PubMed]
Husereau D, Clifford T, Aker P.�Spinal manipulation for infantile colic.�Vol. 42. Canadian Coordinating office for Health Technology Assessment. Ottawa; 2003.
Brand P, Engelbert R, Helders P. Systematic review of effects of manual therapy in infants with kinetic imbalance due to suboccipital strain (KISS) syndrome.�J Man & Manip Ther.�2005;13:209�214.
Ernst E. Chiropractic manipulation for non-spinal pain–a systematic review.�N Z Med J.�2003;116:U539.�[PubMed]
Gotlib A, Rupert R. Chiropractic manipulation in pediatric health conditions – an updated systematic review.�Chiropr Osteopat.�2008;16:11. doi: 10.1186/1746-1340-16-11.�[PMC free article]�[PubMed][Cross Ref]
Ernst E. Chiropractic spinal manipulation for infant colic: a systematic review of randomised clinical trials.�Int J Clin Pract.�2009;63:1351�1353. doi: 10.1111/j.1742-1241.2009.02133.x.�[PubMed][Cross Ref]
Koonin S, Karpelowsky AS, Yelverton CJ. A comparative study to determine the efficacy of chiropractic spinal manipulative therapy and allopathic medication inthe treatment of infantile colic.�WFC 7th Biennial Congress Proceedings; Orlando. May 1-3, 2003.�pp. 330�1.
Mercer C, Nook B. In:�World Federation of Chiropractic. 5th Biennial Congress, 17-22 May 1999.Haldman S, Murphy B, editor. The efficacy of chiropractic spinal adjustments as a treatment protocol in the management of infant colic; pp. 170�1.
Wiberg JM, Nordsteen J, Nilsson N. The short-term effect of spinal manipulation in the treatment of infantile colic: a randomized controlled clinical trial with a blinded observer.�J Manipulative Physiol Ther.�1999;22:517�522. doi: 10.1016/S0161-4754(99)70003-5.�[PubMed]�[Cross Ref]
Browning M. Comparison of the short-term effects of chiropractic spinal manipulation and occipito-sacral decompression in the treatment of infant colic: a single-blinded, randomised, comparison trial.�Clinical Chiropractic.�2009;11:122�129. doi: 10.1016/j.clch.2008.10.003.�[Cross Ref]
Olafsdottir E, Forshei S, Fluge G, Markestad T. Randomised controlled trial of infantile colic treated with chiropractic spinal manipulation.�Arch Dis Child.�2001;84:138�141. doi: 10.1136/adc.84.2.138.[PMC free article]�[PubMed]�[Cross Ref]
Hayden C, Mullinger B. A preliminary assessment of the impact of cranial osteopathy for the relief of infantile colic.�Complement Ther Clin Pract.�2006;12:83�90. doi: 10.1016/j.ctcp.2005.12.005.[PubMed]�[Cross Ref]
Huhtala V, Lehtonen L, Heinonen R, Korvenranta H. Infant massage compared with crib vibrator in the treatment of colicky infants.�Pediatrics.�2000;105:E84. doi: 10.1542/peds.105.6.e84.�[PubMed][Cross Ref]
Arikan D, Alp H, Gozum S, Orbak Z, Cifci EK. Effectiveness of massage, sucrose solution, herbal tea or hydrolysed formula in the treatment of infantile colic.�J Clin Nurs.�2008;17:1754�1761. doi: 10.1111/j.1365-2702.2008.02504.x.�[PubMed]�[Cross Ref]
Lucassen PL, Assendelft WJ, Gubbels JW, van Eijk JT, van Geldrop WJ, Neven AK. Effectiveness of treatments for infantile colic: systematic review.�BMJ.�1998;316:1563�1569.�[PMC free article][PubMed]
Garrison MM, Christakis DA. A systematic review of treatments for infant colic.�Pediatrics.�2000;106:184�190.�[PubMed]
World Health Organization. The ICD-10 classification of mental and behavioural disorders: Clinical descriptions and diagnostic guidelines. 1992.
Fritz G, Rockney R, Bernet W, Arnold V, Beitchman J, Benson RS. Practice parameter for the assessment and treatment of children and adolescents with enuresis.�J Am Acad Child Adolesc Psychiatry.�2004;43:1540�1550. doi: 10.1097/01.chi.0000142196.41215.cc.�[PubMed]�[Cross Ref]
Glazener CM, Evans JH, Cheuk DK. Complementary and miscellaneous interventions for nocturnal enuresis in children.�Cochrane Database Syst Rev.�2005. p. CD005230.�[PubMed]
Reed WR, Beavers S, Reddy SK, Kern G. Chiropractic management of primary nocturnal enuresis.�J Manipulative Physiol Ther.�1994;17:596�600.�[PubMed]
Leboeuf C, Brown P, Herman A, Leembruggen K, Walton D, Crisp TC. Chiropractic care of children with nocturnal enuresis: a prospective outcome study.�J Manipulative Physiol Ther.�1991;14:110�115.�[PubMed]
Pediatric Society of New Zealand. Best practice evidence based guideline: Nocturnal enuresis. 2005.
Scottish Intercollegiate Guidelines Network. Diagnosis and management of childhood otitis media in primary care. 2003.
Mills MV, Henley CE, Barnes LL, Carreiro JE, Degenhardt BF. The use of osteopathic manipulative treatment as adjuvant therapy in children with recurrent acute otitis media.�Arch Pediatr Adolesc Med.�2003;157:861�866. doi: 10.1001/archpedi.157.9.861.�[PubMed]�[Cross Ref]
Subcommittee on Management of Acute Otitis Media. Diagnosis and management of acute otitis media.�Pediatics.�2004;113:1451�1465. doi: 10.1542/peds.113.5.1451.�[PubMed]�[Cross Ref]
Wahl RA, Aldous MB, Worden KA, Grant KL. Echinacea purpurea and osteopathic manipulative treatment in children with recurrent otitis media: a randomized controlled trial.�BMC Complement Altern Med.�2008;8:56. doi: 10.1186/1472-6882-8-56.�[PMC free article]�[PubMed]�[Cross Ref]
Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL Jr. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report.�JAMA.�2003;289:2560�2572. doi: 10.1001/jama.289.19.2560.�[PubMed][Cross Ref]
National Institute for Health and Clinical Excellence. Hypertension: management of hypertension in adults in primary care.�Clinical Care Guideline.�2006;34
Goertz CH, Grimm RH, Svendsen K, Grandits G. Treatment of Hypertension with Alternative Therapies (THAT) Study: a randomized clinical trial.�J Hypertens.�2002;20:2063�2068. doi: 10.1097/00004872-200210000-00027.�[PubMed]�[Cross Ref]
Yates RG, Lamping DL, Abram NL, Wright C. Effects of chiropractic treatment on blood pressure and anxiety: a randomized, controlled trial.�J Manipulative Physiol Ther.�1988;11:484�488.[PubMed]
Bakris G, Dickholtz M Sr, Meyer PM, Kravitz G, Avery E, Miller M. Atlas vertebra realignment and achievement of arterial pressure goal in hypertensive patients: a pilot study.�J Hum Hypertens.�2007;21:347�352.�[PubMed]
Lefebvre G, Pinsonneault O, Antao V, Black A, Burnett M, Feldman K. Primary dysmenorrhea consensus guideline.�J Obstet Gynaecol Can.�2005;27:1117�1146.�[PubMed]
Proctor ML, Hing W, Johnson TC, Murphy PA. Spinal manipulation for primary and secondary dysmenorrhoea.�Cochrane Database Syst Rev.�2006;3:CD002119.�[PubMed]
Boesler D, Warner M, Alpers A, Finnerty EP, Kilmore MA. Efficacy of high-velocity low-amplitude manipulative technique in subjects with low-back pain during menstrual cramping.�J Am Osteopath Assoc.�1993;93:203�204.�[PubMed]
Snyder BJ, Sanders GE. Evaluation of the Toftness system of chiropractic adjusting for subjects with chronic back pain, chronic tension headaches, or primary dysmenorrhea.�Chiro Tech.�1996;8:3�9.
Kokjohn K, Schmid DM, Triano JJ, Brennan PC. The effect of spinal manipulation on pain and prostaglandin levels in women with primary dysmenorrhea.�J Manipulative Physiol Ther.�1992;15:279�285.�[PubMed]
Tomason PR, Fisher BL, Carpenter PA. Effectiveness of spinal manipulative therapy in treatment of primary dysmenorrhea: A pilot study.�J of Man and Phys Therapeutics.�1979;2:140�145.
Hondras MA, Long CR, Brennan PC. Spinal manipulative therapy versus a low force mimic maneuver for women with primary dysmenorrhea: a randomized, observer-blinded, clinical trial.�Pain.�1999;81:105�114. doi: 10.1016/S0304-3959(99)00004-4.�[PubMed]�[Cross Ref]
Royal College of Obstetricians and Gynaecologists. Management of premenstual syndrome.�Green-top Guideline.�2007;48
Halbreich U, Backstrom T, Eriksson E, O’brien S, Calil H, Ceskova E. Clinical diagnostic criteria for premenstrual syndrome and guidelines for their quantification for research studies.�Gynecol Endocrinol.�2007;23:123�130. doi: 10.1080/09513590601167969.�[PubMed]�[Cross Ref]
Stevinson C, Ernst E. Complementary/alternative therapies for premenstrual syndrome: a systematic review of randomized controlled trials.�Am J Obstet Gynecol.�2001;185:227�235. doi: 10.1067/mob.2001.113643.�[PubMed]�[Cross Ref]
Fugh-Berman A, Kronenberg F. Complementary and alternative medicine (CAM) in reproductive-age women: a review of randomized controlled trials.�Reprod Toxicol.�2003;17:137�152. doi: 10.1016/S0890-6238(02)00128-4.�[PubMed]�[Cross Ref]
Walsh MJ, Polus BI. A randomized, placebo-controlled clinical trial on the efficacy of chiropractic therapy on premenstrual syndrome.�J Manipulative Physiol Ther.�1999;22:582�585. doi: 10.1016/S0161-4754(99)70018-7.�[PubMed]�[Cross Ref]
Hernandez-Reif M, Martinez A, Field T, Quintero O, Hart S, Burman I. Premenstrual symptoms are relieved by massage therapy.�J Psychosom Obstet Gynaecol.�2000;21:9�15. doi: 10.3109/01674820009075603.�[PubMed]�[Cross Ref]
Oleson T, Flocco W. Randomized controlled study of premenstrual symptoms treated with ear, hand, and foot reflexology.�Obstet Gynecol.�1993;82:906�911.�[PubMed]
Reventlow SD, Hvas L, Malterud K. Making the invisible body visible. Bone scans, osteoporosis and women’s bodily experiences.�Soc Sci Med.�2006;62:2720�2731. doi: 10.1016/j.socscimed.2005.11.009.�[PubMed]�[Cross Ref]
Barnett AG, Pols JC van der, Dobson AJ. Regression to the mean: what it is and how to deal with it.�Int J Epidemiol.�2005;34:215�220. doi: 10.1093/ije/dyh299.�[PubMed]�[Cross Ref]
Kaptchuk TJ. The placebo effect in alternative medicine: can the performance of a healing ritual have clinical significance?�Ann Intern Med.�2002;136:817�825.�[PubMed]
Sox HC Jr, Margulies I, Sox CH. Psychologically mediated effects of diagnostic tests.�Ann Intern Med.�1981;95:680�685.�[PubMed]
Kaptchuk TJ. Powerful placebo: the dark side of the randomised controlled trial.�The Lancet.�1998;351:1722�1725. doi: 10.1016/S0140-6736(97)10111-8.�[PubMed]�[Cross Ref]
Kelley JM, Lembo AJ, Ablon JS, Villanueva JJ, Conboy LA, Levy R. Patient and Practitioner Influences on the Placebo Effect in Irritable Bowel Syndrome.�Psychosom Med.�2009;71:789�797. doi: 10.1097/PSY.0b013e3181acee12.�[PMC free article]�[PubMed]�[Cross Ref]
Kaptchuk TJ, Stason WB, Davis RB, Legedza AR, Schnyer RN, Kerr CE. Sham device v inert pill: randomised controlled trial of two placebo treatments.�BMJ.�2006;332:391�397. doi: 10.1136/bmj.38726.603310.55.�[PMC free article]�[PubMed]�[Cross Ref]
Oths K. Communication in a chiropractic clinic: how a D.C. treats his patients.�Cult Med Psychiatry.�1994;18:83�113. doi: 10.1007/BF01384878.�[PubMed]�[Cross Ref]
Adler HM, Hammett VB. The doctor-patient relationship revisited. An analysis of the placebo effect.�Ann Intern Med.�1973;78:595�598.�[PubMed]
Novack DH. Therapeutic aspects of the clinical encounter.�J Gen Intern Med.�1987;2:346�355. doi: 10.1007/BF02596174.�[PubMed]�[Cross Ref]
De Vries R, Lemmens T. The social and cultural shaping of medical evidence: case studies from pharmaceutical research and obstetric science.�Soc Sci Med.�2006;62:2694�2706. doi: 10.1016/j.socscimed.2005.11.026.�[PubMed]�[Cross Ref]
Verhoef MJ, Lewith G, Ritenbaugh C, Boon H, Fleishman S, Leis A. Complementary and alternative medicine whole systems research: beyond identification of inadequacies of the RCT.�Complement Ther Med.�2005;13:206�212. doi: 10.1016/j.ctim.2005.05.001.�[PubMed]�[Cross Ref]
Antman K, Lagakos S, Drazen J. Designing and funding clinical trials of novel therapies.�N Engl J Med.�2001;344:762�763. doi: 10.1056/NEJM200103083441010.�[PubMed]�[Cross Ref]
Hoffer LJ. Proof versus plausibility: rules of engagement for the struggle to evaluate alternative cancer therapies.�CMAJ.�2001;164:351�353.�[PMC free article]�[PubMed]
Khalsa PS, Eberhart A, Cotler A, Nahin R. The 2005 conference on the biology of manual therapies.�J Manipulative Physiol Ther.�2006;29:341�346. doi: 10.1016/j.jmpt.2006.04.002.�[PubMed][Cross Ref]
Rubinstein SM. Adverse events following chiropractic care for subjects with neck or low-back pain: do the benefits outweigh the risks?�J Manipulative Physiol Ther.�2008;31:461�464. doi: 10.1016/j.jmpt.2008.06.001.�[PubMed]�[Cross Ref]
Ernst E. Adverse effects of spinal manipulation: a systematic review.�J R Soc Med.�2007;100:330�338. doi: 10.1258/jrsm.100.7.330.�[PMC free article]�[PubMed]�[Cross Ref]
Rubinstein SM, Peerdeman SM, van Tulder MW, Riphagen I, Haldeman S. A systematic review of the risk factors for cervical artery dissection.�Stroke.�2005;36:1575�1580. doi: 10.1161/01.STR.0000169919.73219.30.�[PubMed]�[Cross Ref]
Michaeli A. A reported occurrence and nature of complications following manipulative physiotherapy in South Afrika.�Aust Physiother.�1993;39:309�315.�[PubMed]
Haldeman S, Carey P, Townsend M, Papadopoulos C. Arterial dissections following cervical manipulation: the chiropractic experience.�CMAJ.�2001;165:905�906.�[PMC free article]�[PubMed]
Cassidy JD, Boyle E, Cote P, He Y, Hogg-Johnson S, Silver F. Risk of vertebrobasilar stroke and chiropractic care: results of a population-based case-control and case-crossover study.�Spine.�2008;33:S176�S183. doi: 10.1097/BRS.0b013e3181644600.�[PubMed]�[Cross Ref]
Hurwitz EL, Morgenstern H, Vassilaki M, Chiang LM. Adverse reactions to chiropractic treatment and their effects on satisfaction and clinical outcomes among patients enrolled in the UCLA Neck Pain Study.�J Manipulative Physiol Ther.�2004;27:16�25. doi: 10.1016/j.jmpt.2003.11.002.[PubMed]�[Cross Ref]
Hurwitz EL, Morgenstern H, Vassilaki M, Chiang LM. Frequency and clinical predictors of adverse reactions to chiropractic care in the UCLA neck pain study.�Spine.�2005;30:1477�1484. doi: 10.1097/01.brs.0000167821.39373.c1.�[PubMed]�[Cross Ref]
Assendelft WJ, Bouter LM, Knipschild PG. Complications of spinal manipulation: a comprehensive review of the literature.�J Fam Pract.�1996;42:475�480.�[PubMed]
Institute for Clinical Systems Improvement.�ICSI Health Care Guidelines: Assessment and management of chronic pain.�Institute for Clinical Systems Improvement; 2005. pp. 1�77.
Haldeman S, Rubinstein SM. Cauda equina syndrome in patients undergoing manipulation of the lumbar spine.�Spine.�1992;17:1469�1473. doi: 10.1097/00007632-199212000-00005.�[PubMed][Cross Ref]
Vohra S, Johnston BC, Cramer K, Humphreys K. Adverse events associated with pediatric spinal manipulation: a systematic review.�Pediatrics.�2007;119:e275�e283. doi: 10.1542/peds.2006-1392.[PubMed]�[Cross Ref]
Stevinson C, Honan W, Cooke B, Ernst E. Neurological complications of cervical spine manipulation.�J R Soc Med.�2001;94:107�110.�[PMC free article]�[PubMed]
Adams D, Amernic H, Humphreys K.�A survey of complementary and alternative medicine practitioners’ knowledge, attitudes, and behavior regarding children in their practice.�San Francisco, CA; p. 206.
Moher D, Pham B, Lawson ML, Klassen TP. The inclusion of reports of randomised trials published in languages other than English in systematic reviews.�Health Technol Assess.�2003;7:1�90.[PubMed]
Juni P, Holenstein F, Sterne J, Bartlett C, Egger M. Direction and impact of language bias in meta-analyses of controlled trials: empirical study.�Int J Epidemiol.�2002;31:115�123. doi: 10.1093/ije/31.1.115.�[PubMed]�[Cross Ref]
Galandi D, Schwarzer G, Antes G. The demise of the randomised controlled trial: bibliometric study of the German-language health care literature, 1948 to 2004.�BMC Med Res Methodol.�2006;6:30. doi: 10.1186/1471-2288-6-30.�[PMC free article]�[PubMed]�[Cross Ref]
Moher D, Tetzlaff J, Tricco AC, Sampson M, Altman DG. Epidemiology and reporting characteristics of systematic reviews.�PLoS Med.�2007;4:e78. doi: 10.1371/journal.pmed.0040078.[PMC free article]�[PubMed]�[Cross Ref]
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine