El Paso, TX. Chiropractor, Dr. Alexander Jimenez continues the discussion on the anatomy of nerve fibers, receptors, spinal tracts and brain pathway/s. As the spinal nerve nears the spinal cord, it splits into the dorsal and ventral roots. The dorsal root only contains the axons of sensory neurons. While the ventral roots contain only the axons of motor neurons. Some of the branches synapse with local neurons in the dorsal root ganglion, posterior (dorsal) horn, and even the anterior (ventral) horn, at the spine where they enter.
Other branches travel short distances up or down the spine to interact with neurons at other levels of the spinal cord. A branch can also turn into the posterior (dorsal) column white matter to connect with the brain. Spinal nerve systems that connect to the brain are contralateral, in that the right side of the body is connected to the left side of the brain and the left side of the body is connected to the right side of the brain.
Cranial nerves convey specific sense information from the head and neck directly to the brain. Whereas spinal information is contralateral, cranial nerve systems are for the most part�ipsilateral, meaning that a cranial nerve on the right side of the head is connected to the right side of the brain. Some cranial nerves contain only sensory axons. Other cranial nerves have both sensory and motor axons, including the trigeminal, facial and glossopharyngeal. General senses of somatosensation for the face travel through the trigeminal system.
PATHWAYS
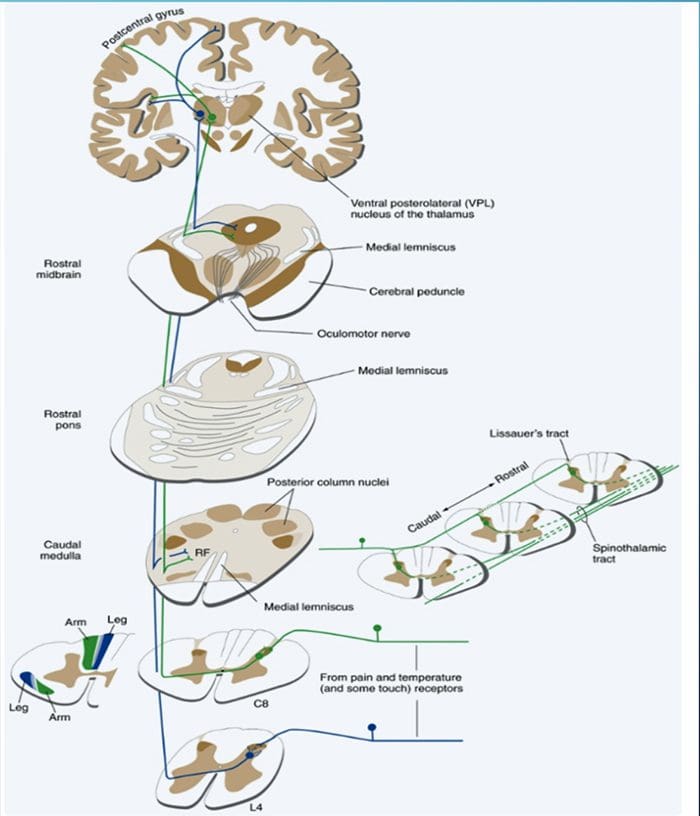
THE POSTERIOR COLUMN� MEDIAL LEMNISCUS SYSTEM CONVEYS INFORMATION ABOUT TOUCH AND LIMB POSITION
POSTERIOR COLUMN MEDIAL LEMNISCAL PATHWAY
The term posterior column refers to the entire contents of a posterior funiculus, exclusive of its share of the propriospinal tract. The posterior columns consist mainly of ascending collaterals of large myelinated primary afferents carrying impulses from various kinds of mechanoreceptors (although substantial numbers of second-order fibers and unmyelinated fibers are also included). This has traditionally been considered the major pathway by which information from low-threshold cutaneous, joint, and muscle receptors reaches the cerebral cortex.
2-Minute Neuroscience: Touch & The Dorsal Columns-Medial Lemniscus
DAMAGE TO THE POSTERIOR COLUMN�MEDIAL LEMNISCUS SYSTEM CAUSES IMPAIRMENT OF PROPRIOCEPTION AND DISCRIMINATIVE TACTILE FUNCTIONS
�As might be expected from the types of afferents contained in the posterior columns, this pathway carries information important for the conscious appreciation of touch, pressure, and vibration and of joint position and movement. However, because input from cutaneous receptors also reaches the cortex by other routes, damage to the posterior columns causes impairment, but not abolition, of tactile perception. Complex discrimination tasks are more severely affected than is the simple detection of stimuli. Other functions, such as proprioception and kinesthesia, are classically considered to be totally lost after posterior column destruction. The result is a distinctive type of ataxia (incoordination of movement); the brain is unable to direct motor activity properly without sensory feedback about the current position of parts of the body. This ataxia is particularly pronounced when the patient�s eyes are closed, preventing visual compensation.�
Given the role of the posterior column, the patient should be screened for any abnormalities regarding their sense of fine touch, vibration, barognosis, graphesthesia, stereognosis, kinaesthesia, two-point discrimination and conscious proprioception:
A common way of testing for fine touch is to ask the patient to recognize common objects placed within a cloth using their touch.
Vibration sense can be tested using a low pitched C128 tuning fork placed along a bony prominence of the desired corresponding spinal level(s) to be tested.
Barognosis refers to the ability to determine the approximate weight of an object.
Graphesthesia refers to the ability to recognize writing on the skin by touch. The practitioner can draw out a letter on the patients skin as a way of testing.
Kinaesthesia refers to ones own sense of body motion (excluding equilibrium which is controlled in part by the inner ear) and is commonly tested using the subject�s ability to detect an externally imposed passive movement, or the ability to reposition a joint to a predetermined position.
Proprioception is often assessed using the Rombergs test. This examination is based on the notion that a person requires at least two of the three following senses to maintain balance while standing: proprioception; vestibular function and vision. A patient who has a defect within their proprioceptive mechanism can still maintain balance by using vestibular function and vision. In the Romberg test, the patient is stood up and asked to close their eyes. A loss of balance is interpreted as a positive Romberg sign.
THE SPINOTHALAMIC TRACT CONVEYS INFORMATION ABOUT PAIN AND TEMPERATURE
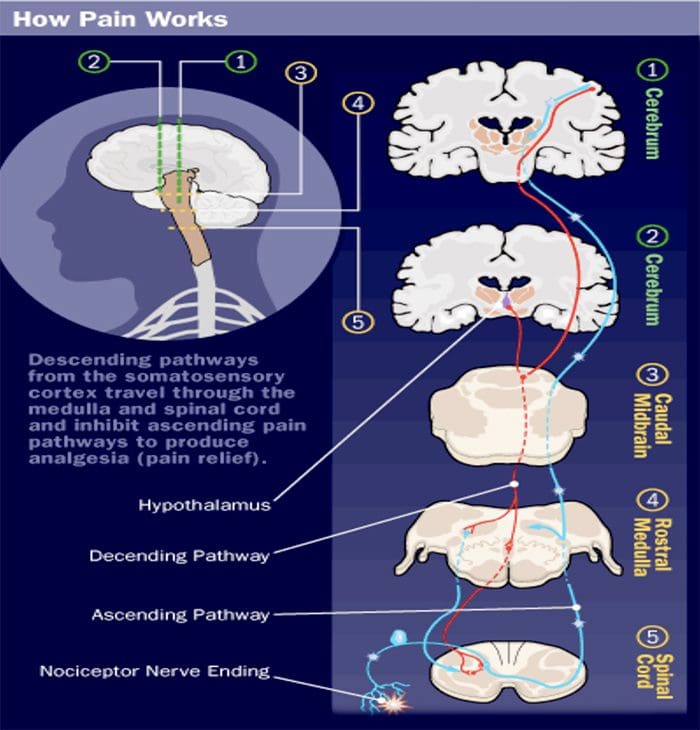
A GOOD BRAIN CAN MODULATE PAIN
SPINOTHALAMIC TRACT
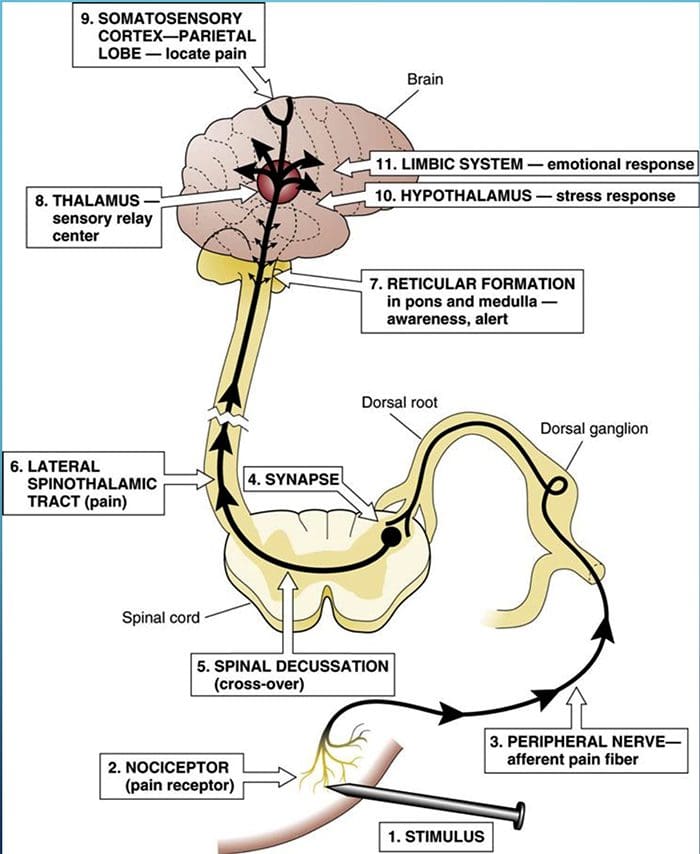
Pain is a complex sensation, in that a noxious stimulus leads not only to the perception of where it occurred but also to things such as a rapid increase in level of attention, emotional reactions, autonomic responses, and a greater likelihood that the event and its circumstances will be remembered. Corresponding to this complexity, multiple pathways convey nociceptive information rostrally from the spinal cord. One of them (the spinothalamic tract) is analogous to the posterior column�medial lemniscus pathway.
SPINOTHALAMIC TRACTS
Two main parts of the Spinothalamic Tract (STT)
Lateral Spinothalamic Tract
Transmission of pain and temperature
Anterior Spinothalamic Tract
Transmission of crude touch and firm pressure
DAMAGE TO THE ANTEROLATERAL SYSTEM CAUSES DIMINUTION OF PAIN AND TEMPERATURE SENSATIONS
Examination:
Given the role of the spinothalamic tract, the patient should be screened for any abnormalities regarding their sense of touch, pain, temperature, and pressure sensation.
Screening for such abnormalities is commonly done using gentle pin pricks and cotton wool, to contrast between sharp and soft, following cutaneous sensory nerve root distributions. Hot and cold discrimination can be ascertained using the cold metal arm of a tuning fork, and a warm palm or heated object.
2 Minute Neuroscience: Pain & The Anterolateral System
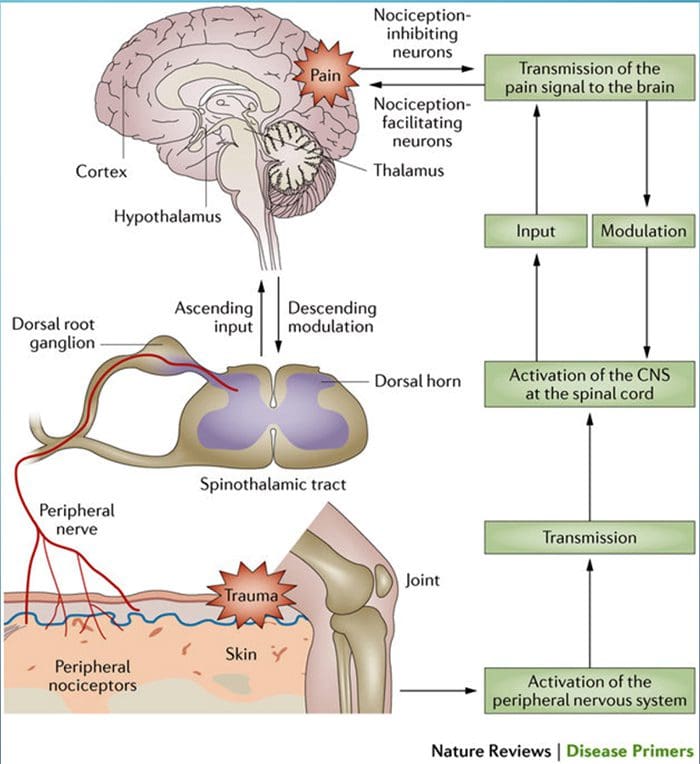
HAUSER ET AL. FIBROMYALGIA, 2015
�Pain processing and its modulation: Activation of peripheral pain receptors (also called nociceptors) by noxious stimuli generates signals that travel to the dorsal horn of the spinal cord via the dorsal root ganglion. From the dorsal horn, the signals are carried along the ascending pain pathway or the spinothalamic tract to the thalamus and the cortex. Pain can be controlled by nociception- inhibiting and nociception-facilitating neurons. Descending signals originating in the supraspinal centers can modulate activity in the dorsal horn by controlling spinal pain transmission. CNS, central nervous system.�
SPINAL INFORMATION REACHES THE CEREBELLUM BOTH DIRECTLY AND INDIRECTLY
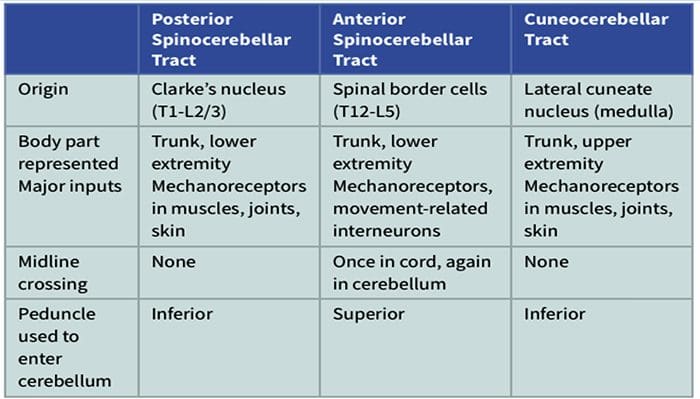
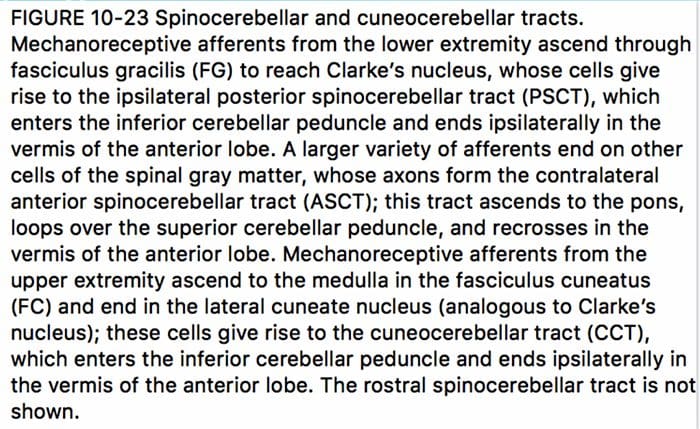
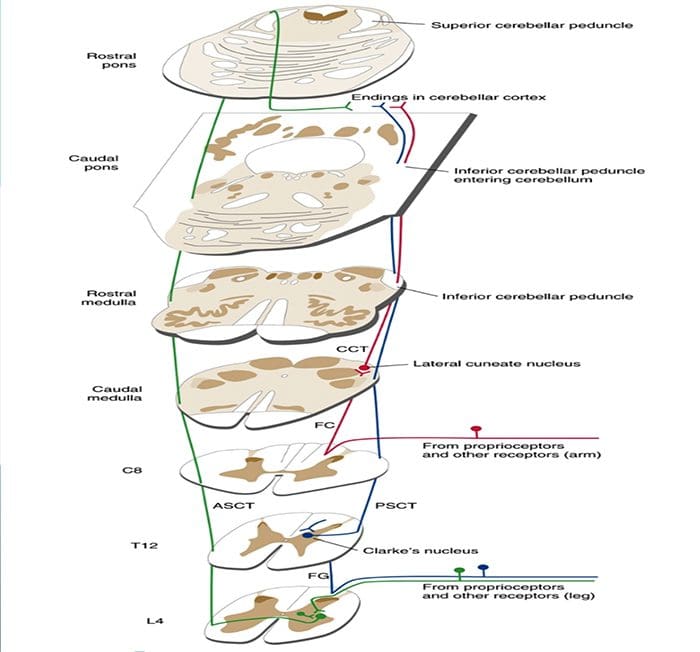
The spinal cord is an important source of information used by the cerebellum in the coordination of movement. This information reaches the cerebellar cortex and nuclei both directly, by way of spinocerebellar tracts, and indirectly, by way of relays in brainstem nuclei. A number of spinocerebellar tracts have been described, some representing the upper extremity and others the lower extremity. Only three have been well characterized.
Ascending Tracts | Spinocerebellar Tract
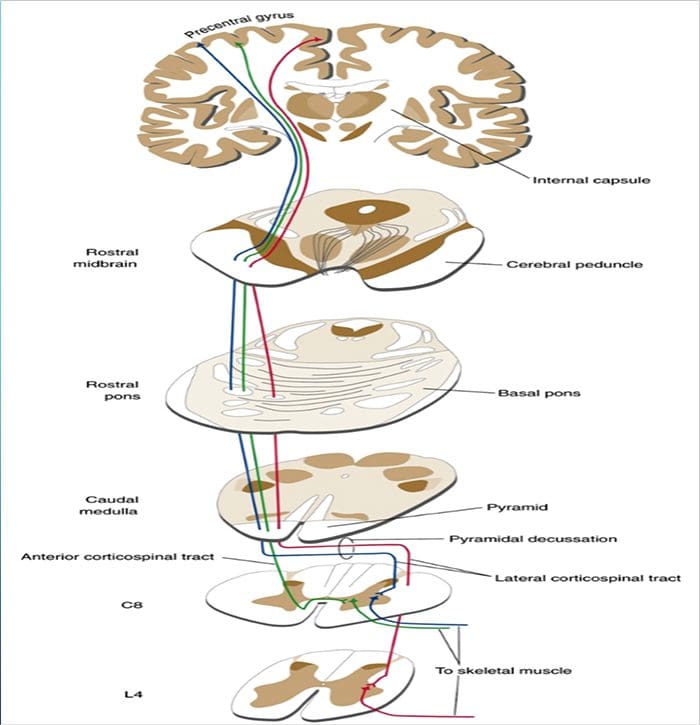
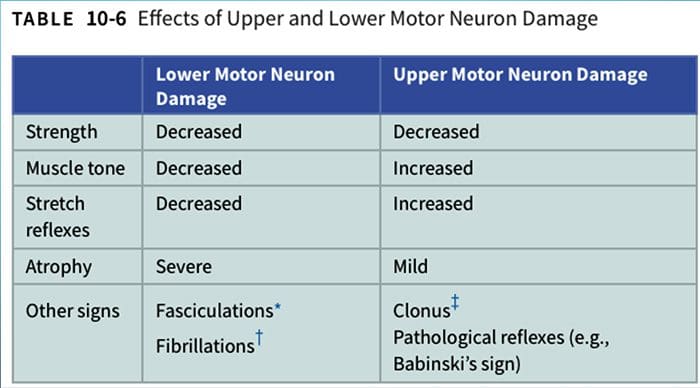
DESCENDING PATHWAYS INFLUENCE THE ACTIVITY OF LOWER MOTOR NEURONS
The vast array of symptoms caused by neuropathy, also known as peripheral neuropathy, reflect the fact that it may be caused by an equally broad range of ailments involving disease and damage to peripheral nerves.
Signs and Symptoms of Neuropathy
Depending on the reason and unique to each patient, signs and symptoms of neuropathy can include:�pain; tingling, burning or prickling sensations; increased sensitivity to touch; muscle weakness or wasting;�temporary or permanent numbness; paralysis; dysfunction in glands or organs; or impairment in urination and sexual functioning.
Such signs and symptoms are dependent on whether autonomic, sensory, or motor nerves, as well as a combination of them, are ultimately affected. Autonomic nerve damage can influence physiological functions like blood pressure or create gastrointestinal problems and issues. Damage or dysfunction in the sensory nerves may impact sensations and sense of equilibrium or balance, while harm to motor nerves may affect movement and reflexes. When both sensory and motor nerves are involved, the condition is known as sensorimotor polyneuropathy.
Diabetic Neuropathy Symptoms
Diabetic peripheral neuropathy, which affects between 12 and 50 percent of individuals with diabetes, is one of the most common types of neuropathy. Many times, symptoms include a gradual change in sensation, as well as pain and weakness in the feet and, although less commonly, the hands. As the neuropathy develops further, it can lead to a loss of sensation in the affected regions.
This lack of feeling raises the odds of harm to the affected areas, explains Matthew Villani, doctor of podiatric medicine at Central Florida Regional Hospital at Lake Mary. Without the pain to signal when there’s an issue, individuals with diabetic neuropathy may allow modest abrasions or blisters on their feet, for instance, to fester as sores or ulcers. “The ulcers can become infected since they are open wounds, which can also progress to bone infection. Unfortunately, it frequently requires amputations if it does progress to that point”, states Dr. Matthew Villani.
Chemotherapy-Associated Neuropathy Symptoms
Cancer patients may suffer with neuropathy induced by chemotherapy as well as by other drugs and/or medications used to treat the disease. Symptoms can include intense pain, impaired movement, changes in heart rate and blood pressure, issues with balance, difficulty breathing, paralysis, and even organ failure. After chemotherapy is done, the symptoms frequently abate swiftly, but occasionally they last more, or these may not go away at all.
HIV- and AIDS-Associated Neuropathy Symptoms
Individuals being treated for HIV or AIDS can develop neuropathy from effects of the virus and the drugs and/or medications used to treat it as well. Common symptoms include stiffness, burning, prickling, tingling, and loss of feeling in the toes and soles of their feet. Sometimes the nerves in the fingers, hands, and wrists are also affected. The drugs Videx (didanosine), Hivid (zalcitabine), and Zerit (stavudine) have been most commonly associated with neuropathic symptoms.
Inflammation-Associated Neuropathy Symptoms
Inflammation caused by infections, like herpes zoster (also known as shingles), Lyme disease, or hepatitis B and hepatitis C, may lead to neuropathy, as may inflammation caused by autoimmune disorders, such as vasculitis, sarcoidosis, or autoimmune disease. In such situations, the signs and symptoms generally include burning and tingling sensations or numbness.
Other Causes of Neuropathy Symptoms
Additional causes of neuropathy and associated signs and symptoms include metabolic disorders, such as hypoglycemia or kidney failure; autoimmune disorders, such as rheumatoid arthritis, lupus, Sjogren’s syndrome, and Guillain-Barr� syndrome; toxicity; hereditary disorders, such as Charcot-Marie-Tooth disorder; hormonal disorders; alcoholism; vitamin deficiencies; physical trauma or injury; compression; and repetitive stress. In addition, many individuals may experience idiopathic neuropathy signs and symptoms, meaning that healthcare professionals may not know the reason for their neuropathy.
Dr. Alex Jimenez’s Insight
Neuropathy can be caused by a variety of injuries and/or aggravated conditions, often manifesting into a plethora of associated signs and symptoms. While every type of neuropathy, such as diabetic neuropathy or autoimmune disease-associated neuropathy, develops its own unique group of signs and symptoms, many patients will often report common complaints. Individuals with neuropathy generally describe their pain as stabbing, burning or tingling in character. If you experience unusual or abnormal tingling or burning sensations, weakness and/or pain in your hands and feet, it’s essential to seek immediate medical attention in order to receive a proper diagnosis of the cause of your specific signs and symptoms. Early diagnosis may help prevent further nerve injury.
What are the Common Signs and Symptoms of Neuropathy?
“Although there’s a wide array of signs and symptoms associated with neuropathy, the type of pain that people encounter may be common in many aspects of the disorder”, notes Vernon Williams, MD, a sports neurologist and director of the Center for Sports Neurology and Pain Medicine at Cedars-Sini Kerlan-Jobe Institute in Los Angeles. “The character and quality of neuropathic pain will often be pain that is burning or electric in character.” Furthermore, he describes that the pain will frequently be associated with different symptoms, like paresthesia, or a lack of normal sensation associated with pain; allodynia, or a painful reaction to a stimulus that wouldn’t normally trigger pain signals; and hyperalgesia, or a striking or severe pain in response to a stimulus that normally causes moderate pain.
How is Neuropathy Diagnosed?
If you think you’re having any of the above neuropathy signs and symptoms, consult a healthcare professional. A number of tests can be done to diagnose neuropathy. “There are certain patterns of complaints that indicate neuropathy,” stated Dr. Williams, “so taking down a patient’s history which includes a description of these complaints is an important first step.”
“After that, your healthcare professional can perform a physical evaluation, including checking motor and sensory function, assessing deep tendon reflexes, as well as looking for signs and symptoms like allodynia and hyperalgesia,” Williams says. “Then we can even perform electrodiagnostic testing; the most common being electromyography and nerve conduction testing, where we can stimulate nerves and document responses, calculate the rate at which signals are being transmitted and see whether there are some areas where nerves are not transmitting signals normally,” Williams continues.
With needle tests, Williams states, “We can put modest needles into human muscles, and, according to what we see and listen together with all the needle in the muscle, we get details about the way the nerves supplying those muscle tissues are functioning. There are a number of unique tests that could be handy to identifying neuropathy, in addition to localizing where the abnormality is the most likely to be coming from”, concluded Dr.�Vernon Williams.
Often, blood tests may test for elevated blood glucose to see whether your neuropathy signs and symptoms could possibly be associated to type 2 diabetes, nutritional deficiencies, toxic elements, hereditary disorders, and evidence of an abnormal immune response. Your healthcare professional may also do a nerve biopsy, which normally involves removing a small segment of a sensory nerve to search for abnormalities, or even a skin biopsy to see if there’s a reduction in nerve endings.
To give yourself the best chance of an accurate diagnosis as well as relief from your neuropathy signs and symptoms, be prepared to describe everything you are experiencing in detail, even when you experience them, how long an episode persists, and the amount of pain, discomfort or loss of sensation or movement you experience. The more specific you are on the signs and symptoms you’re experiencing, the easier it’ll be for your doctor to understand what’s happening. The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Sciatica
Sciatica is medically referred to as a collection of symptoms, rather than a single injury and/or condition. Symptoms of sciatic nerve pain, or sciatica, can vary in frequency and intensity, however, it is most commonly described as a sudden, sharp (knife-like) or electrical pain that radiates from the low back down the buttocks, hips, thighs and legs into the foot. Other symptoms of sciatica may include, tingling or burning sensations, numbness and weakness along the length of the sciatic nerve. Sciatica most frequently affects individuals between the ages of 30 and 50 years. It may often develop as a result of the degeneration of the spine due to age, however, the compression and irritation of the sciatic nerve caused by a bulging or herniated disc, among other spinal health issues, may also cause sciatic nerve pain.
El Paso, TX. Chiropractor, Dr. Alexander Jimenez discusses the anatomy of nerve fibers, receptors, spinal tracts and brain pathways. Regions of the Central Nervous System (CNS) coordinate various somatic processes using sensory inputs and motor outputs of peripheral nerves. Important areas of the CNS that play a role in somatic processes are separated in the spinal cord brain stem. Sensory pathways that carry peripheral sensations to the brain are referred to an ascending pathway, or tract. Various sensory modalities follow specific pathways through the CNS. Somatosensory stimuli activate receptors in the skin, muscles, tendons, and joints throughout the entire body. The somatosensory pathways are divided into two separate systems based on the location of the receptor neurons. Somatosensory stimuli from below the neck run along the sensory pathways of the spinal cord, and the somatosensory stimuli from the head and neck travel through cranial nerves.
ANATOMY OF RECEPTORS, NERVE FIBERS, SPINAL CORD TRACTS AND BRAINSTEM PATHWAYS
RECEPTORS AND RECEPTOR BASED THERAPY
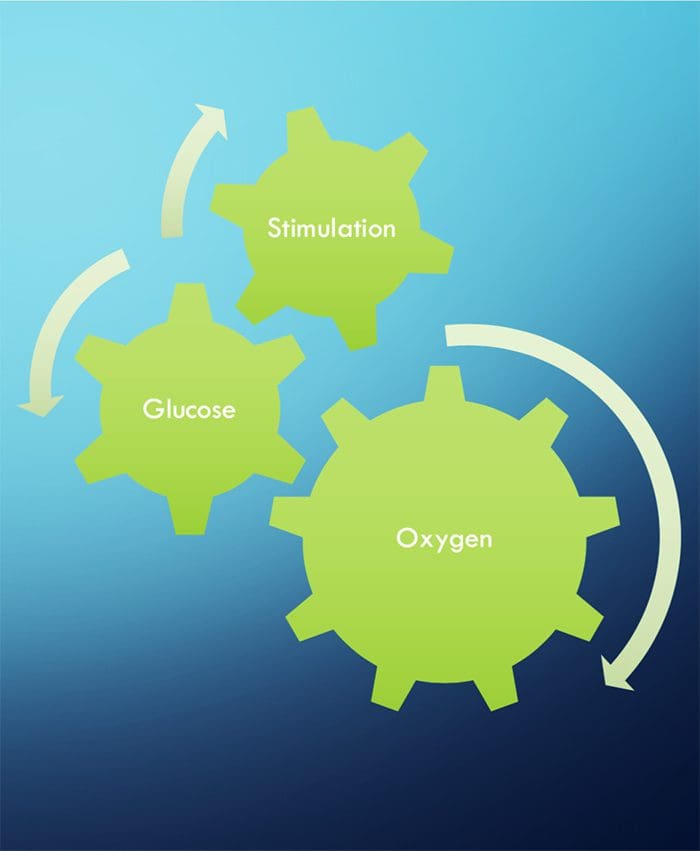
NEURONS NEED THREE THINGS TO SURVIVE!
FUNCTIONAL NEUROLOGY KEY CONCEPTS
The cell needs three things to survive.
Oxygen, glucose and stimulation.
Stimulation = Chiropractic, exercise, etc.
Stimulation leads to neuronal growth
Neuronal growth leads to plasticity
Subluxations alter the frequency of firing of neurons
Activation of one side will stimulate ipsilateral cerebellum and contralateral cortex (usually)
Proper stimulation CAN reduce pain.
CHIROPRACTIC IS RECEPTOR-BASED THERAPY
INTRODUCTION
The ongoing activity and output of the CNS are greatly influenced, and sometimes more or less determined, by incoming sensory information.
The basis of this incoming sensory information is an array of sensory receptors, cells that detect various stimuli and produce receptor potentials in response, often with astonishing effectiveness.
The health of the neuron, however, plays a huge role in how neurons can produce receptor potentials, the endurance of the neuron and the ability to create plasticity.
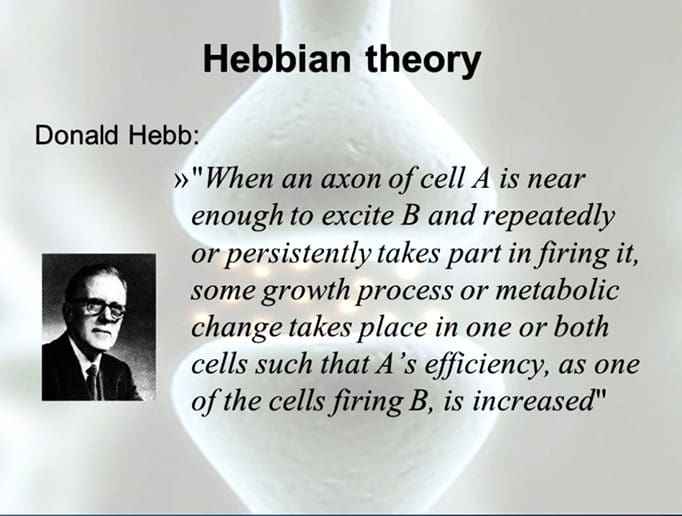
�Neurons that fire together, wire together.� Hebbian Theory
TYPES OF RECEPTORS
Chemoreceptors
Smell, taste, interoceptors
Thermoreceptors
Temperature
Mechanoreceptors
Cutaneous receptors for touch, auditory, vestibular, proprioceptors
Nociceptors
Pain
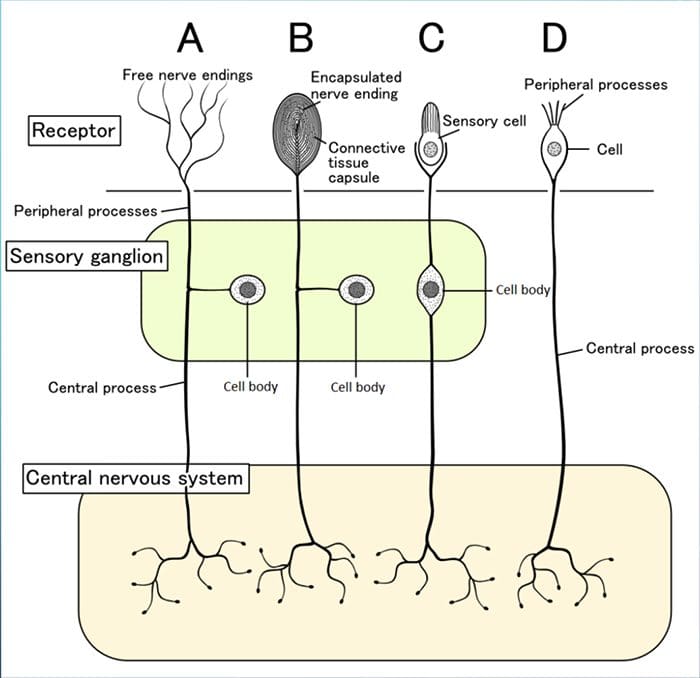
PARTS OF RECEPTORS
Although their morphologies vary widely, all receptors have three general parts:
1. Receptive Area 2. Area Rich In Mitochondria
Health of the neurons within the receptors will determine its response to stimulation
3. Synaptic Area To Pass Messages To The CNS
RECEPTIVE FIELDS
These are particular areas in the periphery where application of an adequate stimulus causes the receptors to respond.
Neurons in successive levels of sensory pathways (second- order neurons, thalamic and cortical neurons-also have receptive fields, although they may be considerably more elaborate than those of the receptors.
TRANSDUCTION
Sensory receptors use ionotropic and metabotropic mechanisms to produce receptor potentials
Sensory receptors transduce some physical stimulus into an electrical signal � a receptor potential � that the nervous system can understand.
Sensory receptors are similar to postsynaptic membranes as their adequate stimuli are analogous to neurotransmitters.
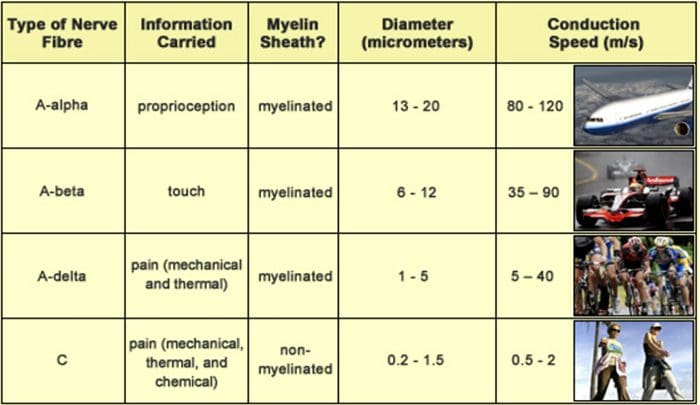
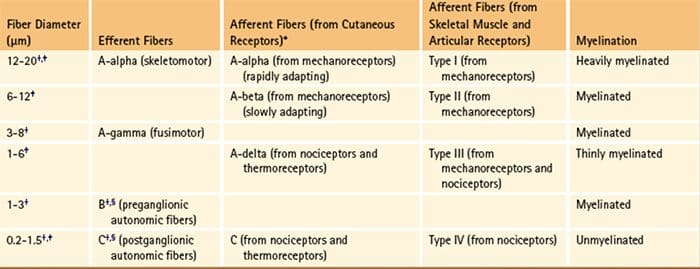
THE DIAMETER OF A NERVE FIBER IS CORRELATED WITH ITS FUNCTION
BIGGER = FASTER
Larger fibers conduct action potentials faster than do smaller fibers.
A? fibers are the largest and most rapidly conducting myelinated fibers.
The slowest conducting fibers of the body are the C fibers
RECEPTORS IN MUSCLES AND JOINTS DETECT MUSCLE STATUS AND LIMB POSITION
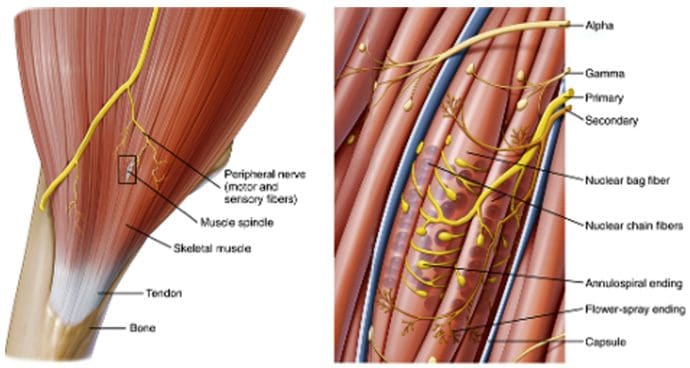
MUSCLE SPINDLES
Muscle spindles (Fig. 9-14) are long, thin stretch receptors scattered throughout virtually every striated muscle in the body.
These muscle spindles sense muscle length and proprioception (�one�s own� perception).
They are quite simple in principle, consisting of a few small muscle fibers with a capsule surrounding the middle third of the fibers.
These fibers are called intrafusal muscle fibers (fusus is Latin for �spindle,� so intrafusal means �inside the spindle�), incontrast to the ordinary extrafusal muscle fibers (�outside the spindle�).
The ends of the intrafusal fibers are attached to extrafusal fibers, so whenever the muscle is stretched, the intrafusal fibers are also stretched.
The central region of each intrafusal fiber has few myofilaments and is noncontractile, but it does have one or more sensory endings applied to it.
When the muscle is stretched, the central part of the intrafusal fiber is stretched, mechanically sensitive channels are distorted, the resulting receptor potential spreads to a nearby trigger zone, and a train of impulses ensues at each sensory ending.
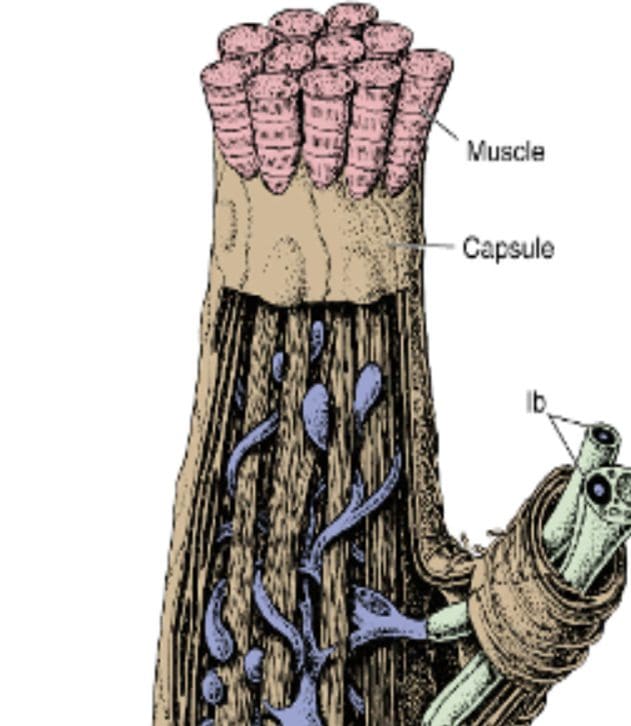
GOLGI TENDON ORGANS
Golgi tendon organs are spindle-shaped receptors found at the�junctions between muscles and tendons. They are similar to Ruffini endings in their basic organization, consisting of interwoven collagen bundles surrounded by a thin capsule (Fig. 9-16).
Large sensory fibers enter the capsule and branch into fine processes that are inserted among the collagen bundles. Tension on the capsule along its long axis squeezes these fine processes, and the resulting distortion stimulates them.
If tension is generated in a tendon by making its attached muscle contract, tendon organs are found to be much more�sensitive and can actually respond to the contraction of just a few muscle fibers.
Thus Golgi tendon organs very specifically monitor the tension generated by muscle contraction and come into play whe
n fine adjustments in muscle tension need to be made (e.g., when handling a raw egg).
�
Thus the mode of action of Golgi tendon organs is quite different from that of muscle spindles (Fig. 9-17). If a muscle�contracts isometrically, tension is generated across its tendons, and the tendon organs signal this; however, the muscle spindles signal nothing because muscle length has not changed (assuming that the activity of the gamma motor neurons remains unchanged).
In contrast, a relaxed muscle can be stretched easily, and the muscle spindles fire; the tendon organs, however, experience little tension and remain silent. A muscle, by virtue of these two types of receptors, can have its length and tension monitored simultaneously.
Neuropathy affects about 8 percent of individuals over the age of 55. Your nervous system is composed of 2 parts: the central nervous system and the peripheral nervous system. The nerves of your peripheral nervous system transmit messages between your central nervous system, that is your brain and spinal cord, along with the rest of the body.
These nerves regulate a massive range of functions throughout the body, such as voluntary muscle movement, involving the motor nerves, involuntary organ action, through the autonomic nerves, and also the perception of stimuli, involving the sensory nerves. Peripheral neuropathy, which is often simply referred to as “neuropathy,” is a state that happens when your nerves become damaged or injured, often times simply disrupted. It’s estimated that neuropathy affects roughly 2.4 percent of the general populace and approximately 8 percent of people older than age 55. However, this quote doesn’t include people affected by neuropathy caused by physical trauma to the nerves.
Types of Neuropathy
Neuropathy can affect any of the three types of peripheral nerves:
Sensory nerves, which transmit messages from the sensory organs, such as the eyes, nose, etc., to your brain;
Motor nerves, which track the conscious movement of your muscles; and
Autonomic nerves, which regulate the involuntary functions of your own body.
Sometimes, neuropathy will only impact one nerve. This is medically referred to as mononeuropathy and instances of it include:
Ulnar neuropathy, which affects the elbow;
Radial neuropathy, which affects the arms;
Peroneal neuropathy, which affects the knees;
Femoral neuropathy, which affects the thighs; and
Cervical neuropathy, which affects the neck.
Sometimes, two or more isolated nerves in separate regions of the body can become damaged, injured or disrupted, resulting in mononeuritis multiplex neuropathy. Most often, however, multiple peripheral nerves malfunction at the same time, a condition called polyneuropathy. According to the National Institute for Neurological Disorders and Stroke, or the NINDS, there are over 100 kinds of peripheral neuropathies.
Dr. Alex Jimenez’s Insight
Neuropathy is medically defined as a disease or dysfunction of one or more peripheral nerves, accompanied by common symptoms of pain, weakness and numbness. The peripheral nerves are in charge of transmitting messages from the central nervous system, the brain and the spinal cord, to the rest of the body. Neuropathy can affect a wide array of nerves. It is also associated with numerous underlying medical conditions and it has been reported to affect approximately 20 million individuals in the United States alone. While physical trauma, infection or exposure to toxins can cause neuropathy, diabetes has been considered to be the most common cause for neuropathy.
Causes of Neuropathy
Neuropathies are often inherited from birth or they develop later in life. The most frequent inherited neuropathy is the neurological disease Charcot-Marie-Tooth disease, which affects 1 in 2,500 people in the USA. Although�healthcare professionals are sometimes not able to pinpoint the exact reason for an acquired neuropathy, medically referred to as idiopathic neuropathy, there are many known causes for them, including: systemic diseases, physical trauma, infectious diseases and autoimmune disorders.
A systemic disease is one which affects the whole body. The most frequent systemic cause behind peripheral neuropathy is diabetes, which can lead to chronically high blood glucose levels that harm nerves.
A number of other systemic issues can cause neuropathy, including:
Kidney disorders, which permit high levels of nerve-damaging toxic chemicals to flow in the blood;
Toxins from exposure to heavy metals, including arsenic, lead, mercury, and thallium;
Certain drugs and/or medications, including anti-cancer medications, anticonvulsants, antivirals, and antibiotics;
Chemical imbalances because of liver ailments;
Hormonal diseases, including hyperthyroidism, which disturbs metabolic processes, potentially inducing cells and body parts to exert pressure on the nerves;
Deficiencies in vitamins, such as E, B1 (thiamine), B6 (pyridoxine), B12, and niacin, that can be vital for healthy nerves;
Alcohol abuse, which induces vitamin deficiencies and might also directly harm nerves;
Cancers and tumors that exert damaging pressure on nerve fibers and pathways;
Chronic inflammation, which can damage protective tissues around nerves, which makes them more vulnerable to compression or vulnerable to getting inflamed and swollen; and
Blood diseases and blood vessel damage, which may damage or injure nerve tissue by decreasing the available oxygen supply.
Additionally, if a nerve suffers from isolated bodily injury, it can become damaged, resulting in neuropathy. Nerves may suffer a direct blow that severs, crushes, compresses, or stretching them, even to the point of detaching them from the spinal cord. Common causes for these injuries are automobile accidents, falls, and sports injuries.
Nerve damage can also arise from powerful pressure on a nerve, like from broken bones and poorly fitted casts. Prolonged pressure on a nerve can also cause neuropathy, as in carpal tunnel syndrome, which occurs when the median nerve at the wrist becomes pinched. Also, persistent physical stress could inflame muscles, tendons, and ligaments, placing substantial pressure on the nerves.
Numerous infections from bacteria and viruses can lead to neuropathy by attacking nerve tissues directly or indirectly, for instance:
HIV
Shingles
Epstein-Barr virus
Lyme disease
Diphtheria
Leprosy
In addition, various autoimmune disorders, in which the body’s immune system attacks and destroys body tissue that is healthy, may result in nerve damage, including:
Peripheral neuropathy may result in several complications, as a result of disease or its symptoms. Numbness from the ailment can allow you to be less vulnerable to temperatures and pain, making you more likely to suffer from burns and serious wounds. The lack of sensations in the feet, for instance, can make you more prone to developing infections from minor traumatic accidents, particularly for diabetics, who heal more slowly than other people, including foot ulcers and gangrene.
Furthermore, muscle atrophy may cause you to develop particular physical disfigurements, such as pes cavus, a condition marked by an abnormally high foot arch, and claw-like deformities in the feet and palms. The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Sciatica
Sciatica is medically referred to as a collection of symptoms, rather than a single injury and/or condition. Symptoms of sciatic nerve pain, or sciatica, can vary in frequency and intensity, however, it is most commonly described as a sudden, sharp (knife-like) or electrical pain that radiates from the low back down the buttocks, hips, thighs and legs into the foot. Other symptoms of sciatica may include, tingling or burning sensations, numbness and weakness along the length of the sciatic nerve. Sciatica most frequently affects individuals between the ages of 30 and 50 years. It may often develop as a result of the degeneration of the spine due to age, however, the compression and irritation of the sciatic nerve caused by a bulging or herniated disc, among other spinal health issues, may also cause sciatic nerve pain.
Hip Labral Tear: Andrew Hutchinson turned to chiropractic care and crossfit rehabilitation after suffering a high ankle sprain and a hip labrum tear for which he went through with surgery to repair it. After being bedridden for months in order to properly recover, Andrew Hutchinson transitioned to chiropractic care and crossfit rehabilitation to regain his strength, mobility and flexibility before returning to play. Although he has suffered other sports injuries, Andrew Hutchinson continues to trust in chiropractic care and crossfit rehabilitation to keep his spine properly aligned and maintain overall health and wellness.
Hip Labral Tear Treatment
Labrum tears in athletes can occur from a single event or recurring trauma. Running may cause labrum tears due to the labrum being utilized more for weight bearing and taking excess forces while at the end-range motion of the leg. Sporting activities are probable causes, specifically those that require frequent hip rotation or pivoting to a loaded femur as in ballet or hockey. Constant hip rotation places increased strain on the capsular tissue and harm to the iliofemoral ligament. This subsequently causes hip instability putting increased stress on the labrum and causing a hip labrum tear.
We focus on what works for you. We also strive to create fitness and better the body through researched methods and total wellness programs. These programs are natural, and use the body�s own ability to achieve goals of improvement, rather than introducing harmful chemicals, controversial hormone replacement, surgery, or addictive drugs.
We want you to live a life that is fulfilled with more energy, positive attitude, better sleep, less pain, proper body weight and educated on how to maintain this way of life. I have made a life of taking care of each and every one of my patients.
I assure you, I will only accept the best for you�
God Bless You & Your Health�?
If you have enjoyed this video and/or we have helped you in any way please feel free to subscribe and share us.
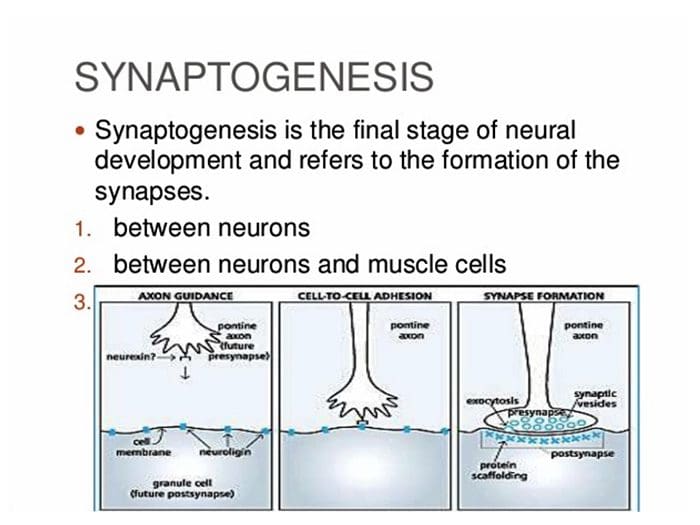
Neurons are believed to establish neuronal connections through innate predetermined programs during the developmental process of the brain. It’s also believed that neurons gravitate to areas of attraction and move away from areas of repulsion in a theory known as the chemoaffinity hypothesis. The Chemoaffinity hypothesis claims that neurons first make connections with their targets based on interactions with specific molecular markers and, therefore, that the first wiring diagram of an organism is indirectly determined by its genotype.
These markers are created during cellular differentiation and aid not just with synaptogenesis, but also act as guidance cues for their individual axon. The development of the mature nervous system formations demands axons to navigate to their correct targets in order to establish neuronal connections or synaptic connections. Growing axons create highly motile structures, known as growth cones, which direct the axon to its goal. They do it by responding to specific guidance molecules that either attract or repel the growth cone.
The Theory of Neuronal Connections
The concept that axons are directed principally by molecular determinants, rather than mechanical determinants, such as cells, extracellular material and other neurons, was established by Roger Wolcott Sperry, a neuropsychologist and neurobiologist, in 1963. However, it was not until the discovery of guidance molecules including netrins, semaphorins, ephrins and Slits, that Sperry’s chemoaffinity hypothesis became widely recognized as a prevalent mechanism for guidance of not only axons, but of all cells.
In 1981, Roger Sperry received the Nobel Prize for Physiology or Medicine for his discoveries concerning the functional specialization of the cerebral hemispheres. He performed studies on patients with epilepsy in whom the corpus callosum, or the bundle of axons fibers which connects the two brain hemispheres, was severed to stop seizures. A number of tests and evaluations revealed the way both brain hemispheres hold independent streams of conscious awareness, perceptions, thoughts and memories, and most fundamentally, that neuronal connections are formed and preserved with a high degree of precision.
Having demonstrated that the institution of specific neuronal connections is fundamental to the overall function of the brain, Sperry turned to look at how these connections are created, and used his chemoaffinity theory to describe how axons find the right target during the development of the brain. Others had raised the possibility that compound determinants might function in axon guidance, but it was Sperry that supplied the direct histological evidence and proposed the chemoaffinity hypothesis for axon guidance.
Roger Sperry and his Chemoaffinity Hypothesis
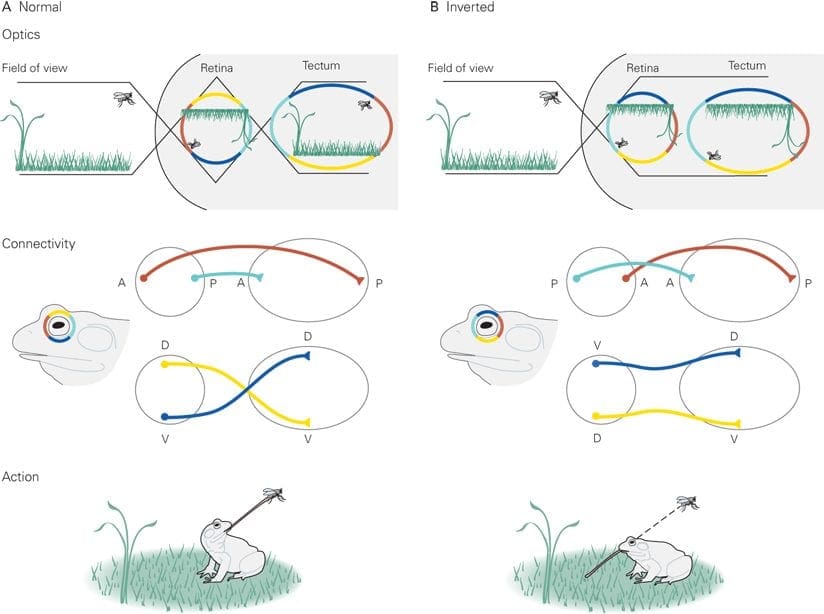
Roger Wolcott Sperry pioneered the inception of the Chemoaffinity Hypothesis after the 1960’s in a series of elegant experiments employing the retinotectal system of the African Clawed Frog, he sectioned the optic nerves and steered the eyes 180 degrees. He wished to know whether vision would be ordinary following regeneration or if the animal would eternally see the world ‘upside down’. If the latter held true, this could reveal that the nerves were somehow guided back to their original sites of termination; however, restoration of normal eyesight would mean that the nerves had resumed at new sites. Sperry showed that these creatures did indeed view the world ‘upside down’.
According to the experiment, initial�eye orientation gives that the top of the eye is Dorsal, and the underside is Ventral. Post-operation, the “top” of the eye is now Ventral, and the base is Dorsal. After a food source was supplied, the frog extended its tongue, meaning that the Dorsal-Ventral orientation of the eye still remained. In follow up experiments, the eye was dispersed and rotated 180� and the optic nerve was also cut to determine if this could affect the Dorsal-Ventral orientation. The results were identical. It was those studies which directed Sperry to suggest that complicated chemical codes, under genetic control, direct axons to their targets, his chemoaffinity hypothesis.
In his first theory, Sperry proposed that distinct cells bear different cell-surface proteins that serve as markers, a notion that demanded an unsatisfactorily high variety of proteins. He revised his model suggesting that double gradients of guidance cues in the afferent and target areas would enable proper axon targeting. There is now extensive experimental data to support the chemoaffinity hypothesis, as well as the requirement for gradients of receptor and/or ligand, such as ephrins and Eph receptors, in the projection and target regions is well established.
Roger Wolcott Sperry concluded that every individual optic nerve and tectal neuron used some kind of chemical markers that dictated their connectivity through development. He concluded that if the eye had been rotated, each optic fiber and every tectal neuron possessed cytochemical labels that uniquely denoted their neuronal kind and place and that optic fibers may use these labels to navigate to their own matching target cell, hence the visuomotor impairment.�Although certain aspects and details about Sperry’s model are unproven or incorrect, the basic notion of this chemoaffinity hypothesis has become dogma in developmental neurobiology.
Dr. Alex Jimenez’s Insight
Over the years, the principle to understand the establishment of neuronal connections has continued throughout the field of neurophysiology as well as prenatal development of the brain. Neuronal connections are believed to be established during the migration of growth cones guided by extracellular guidance cue gradients. Although this theory has been revisited countless of times, Roger Sperry was the first to explain how axons navigate to their correct targets in his chemoaffinity hypothesis. Countless experimental and clinical data now exists to support the chemoaffinity hypothesis.
The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Sciatica
Sciatica is medically referred to as a collection of symptoms, rather than a single injury and/or condition. Symptoms of sciatic nerve pain, or sciatica, can vary in frequency and intensity, however, it is most commonly described as a sudden, sharp (knife-like) or electrical pain that radiates from the low back down the buttocks, hips, thighs and legs into the foot. Other symptoms of sciatica may include, tingling or burning sensations, numbness and weakness along the length of the sciatic nerve. Sciatica most frequently affects individuals between the ages of 30 and 50 years. It may often develop as a result of the degeneration of the spine due to age, however, the compression and irritation of the sciatic nerve caused by a bulging or herniated disc, among other spinal health issues, may also cause sciatic nerve pain.
Neuroembryology: As an embryo all of the cells in the body are identical. But as time passes, some cells develop into neurons and others develop into skin, hair, or muscle cells.
Why do some cells become neurons? How do neurons become organized in the spinal cord and brain in order to allow us to walk, talk, see, recall life events, feel pain, keep balance, and think?
The answers will help us understand how we develop from an embryo into a full-grown person and how our body and brain constantly adapts, throughout our lives to the environments changes.
El Paso, TX. Chiropractor, Dr. Alexander Jimenez discusses neuroembryology, with the intent of educating patients, past and present, and the general public about the how the spine is connected to everything and where everything begins.
INTRODUCTION
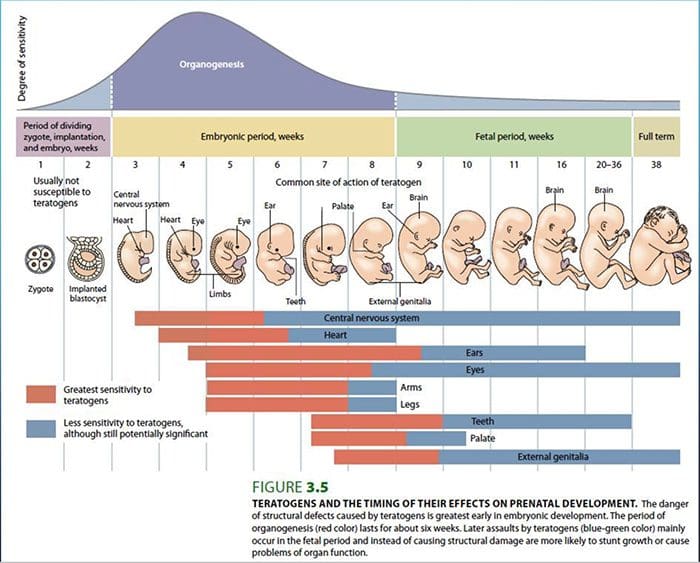
Focusing attention on the development of the nervous system can increase a clinician’s insight into brain functionality and treatment possibilities.
Dysfunctions that may be associated with developmental abnormalities of the brain may range from a mild reduction in cortical function to conditions such as autism and schizophrenia.
The development of the nervous system is influenced by both endogenous and exogenous mechanisms.
Endogenous referring to genetics, exogenous referring to the embryo�s environment.
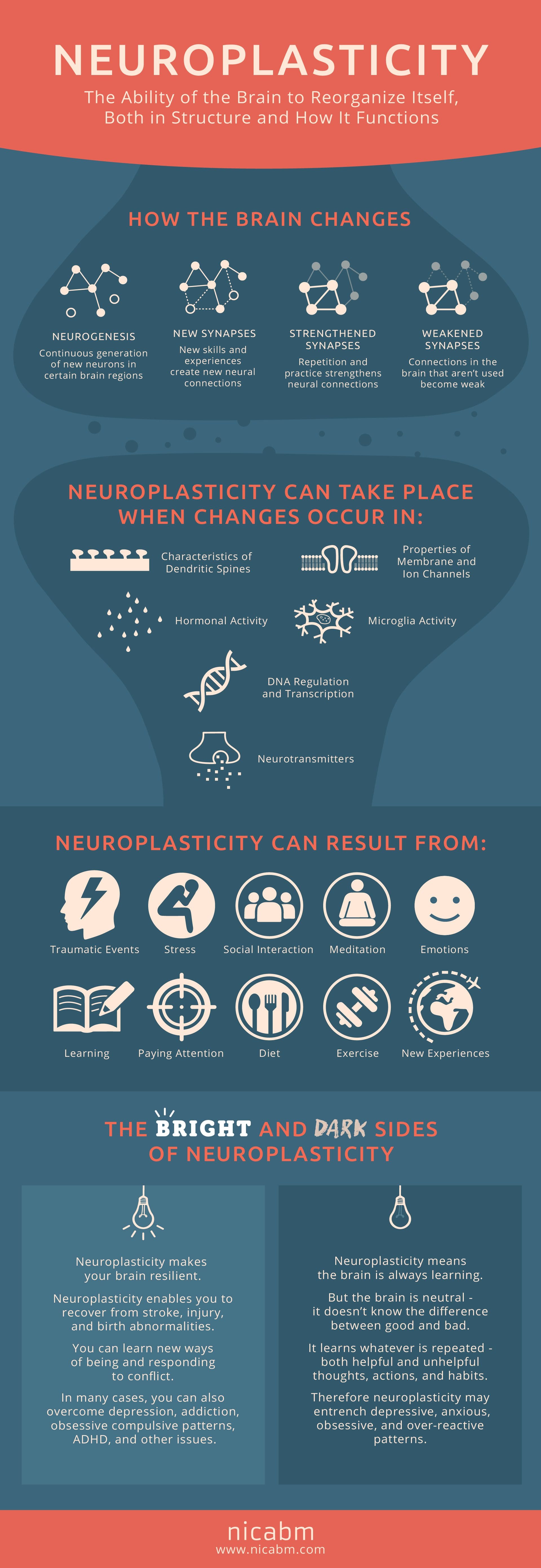
Development is an ongoing process….NEUROPLASTICITY
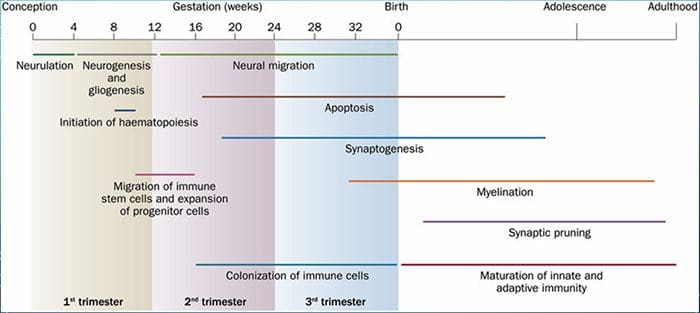
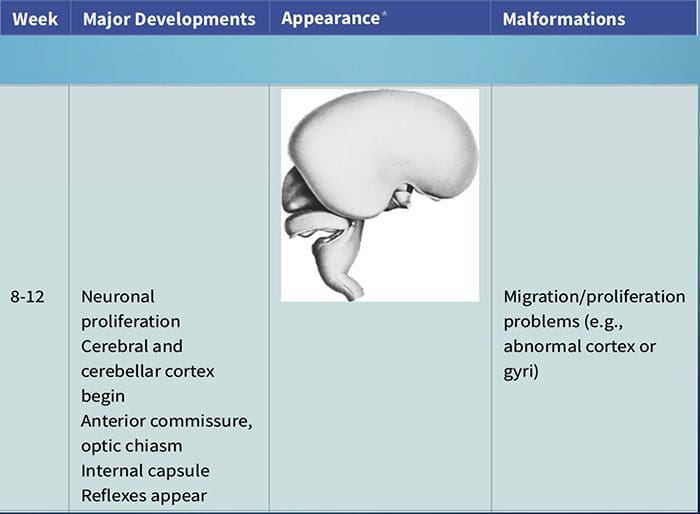
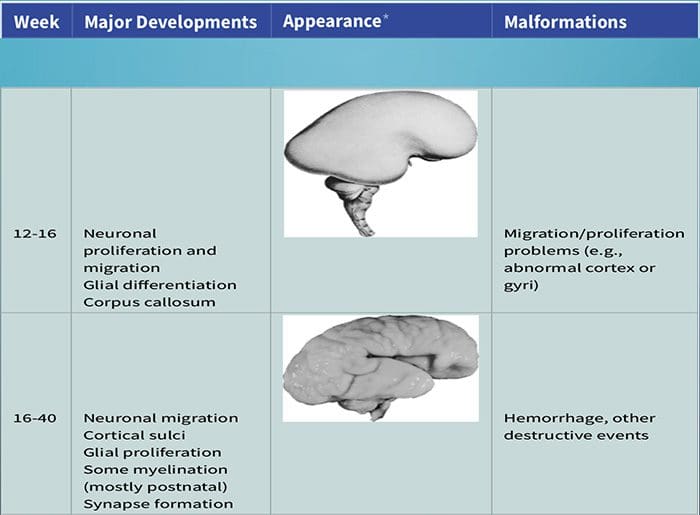
Neuroembryology: DEVELOPMENT
Development of the nervous system can first be identified at about 3 weeks after conception.
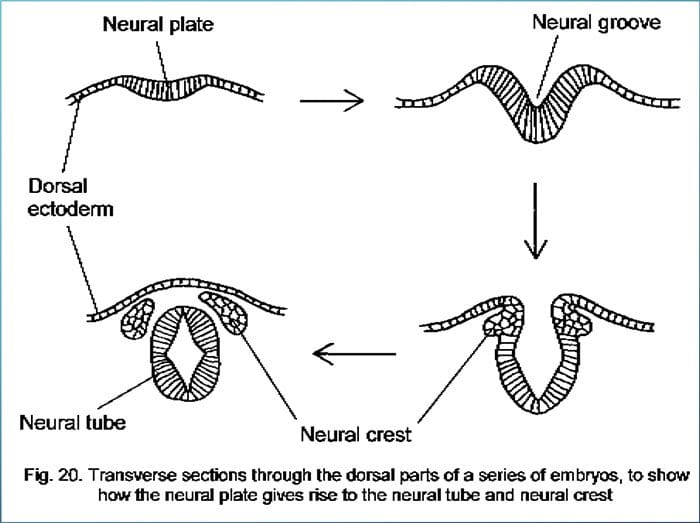
At 3 weeks, in response to underlying chemical signaling from the mesoderm, the neural plate forms, which quickly transitions into the neural groove.
At the beginning of the 4th week, the two folds forming the neural groove begin to fuse starting the formation of the neural tube
Fusion proceeds cranially and caudally and the entire neural tube is closed by the end of the 4th week.
This process is known as primary neurulation.
As the neural tube closes, it progressively separates from the ectodermal surface�and leaves behind neural crest cells.
Neural crest cells develop into the PNS.
The neural tube develops into virtually the entire CNS.
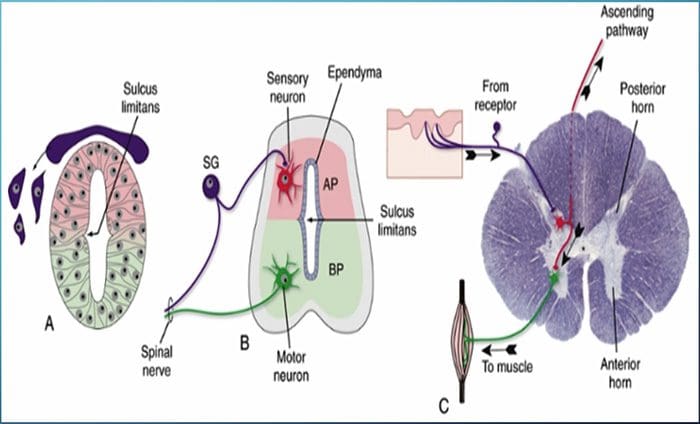
A longitudinal groove forms on the lateral wall of the neural tube�during the fourth week of development
This is known as the sulcus limitans, which separates the tube into dorsal and ventral halves.
The gray matter of the dorsal half forms an alar plate and the ventral half forms a basal plate.
This distinction is of great functional importance because the alar plate plays a role in sensory processing and the basal plate plays a role in motor output.
This similarity is seen in the adult spinal cord with the posterior gray matter receiving sensory input and the anterior gray matter producing motor output.
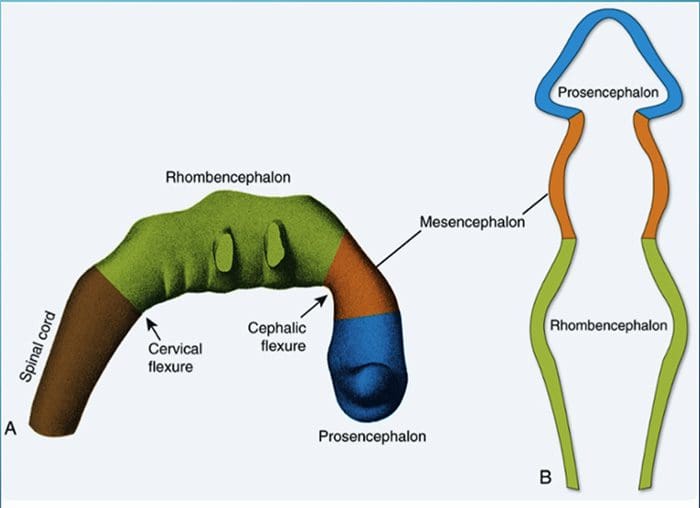
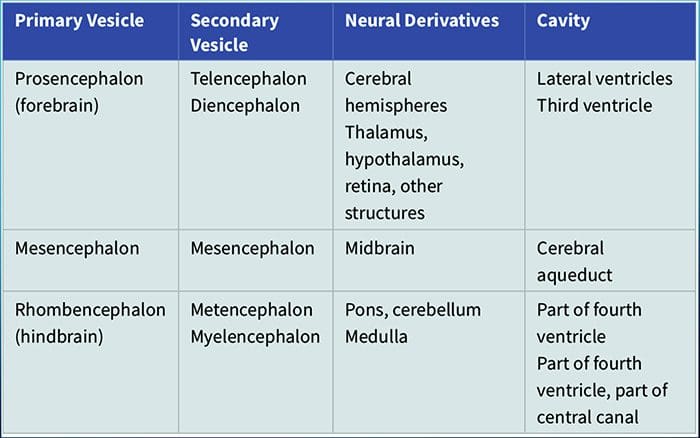
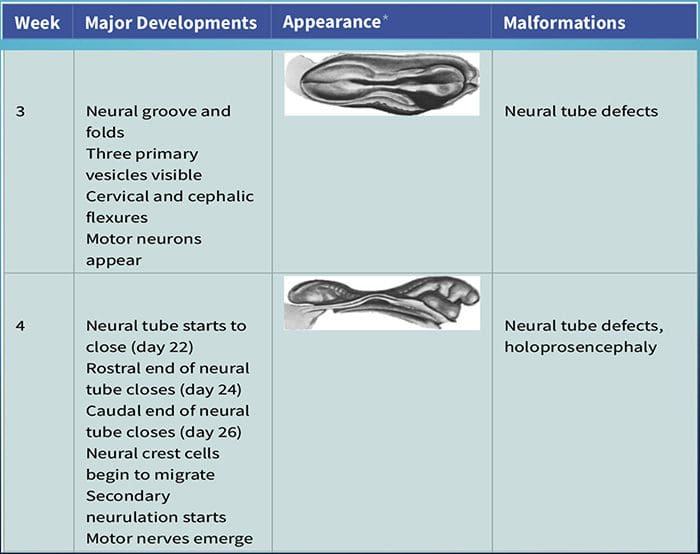
THREE PRIMARY VESICLES
Prosencephalon
Mesencephalon
Rhombencephalon
FIVE SECONDARY VESICLES
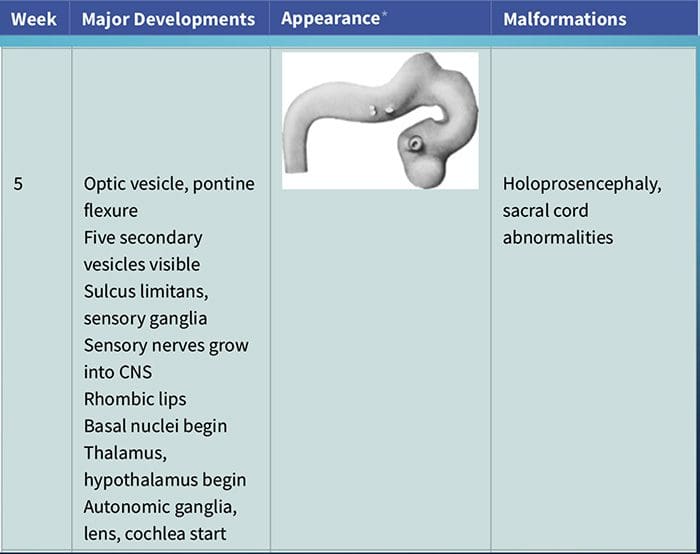
Telencephalon
Diencephalon
Mesencephalon (remains unchanged)
Metencephalon
Myelencephalon
ESTABLISHMENT OF NEURONAL CONNECTIONS
Neurons may have innate predetermined programs that lay out the basic patterns of connections to be formed initially in their development.
Theoretically, neurons gravitate to areas of attraction and move away from areas of repulsion � Chemoaffinity hypothesis
Several mechanisms allow axons to accurately find their way to their target destinations:
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine
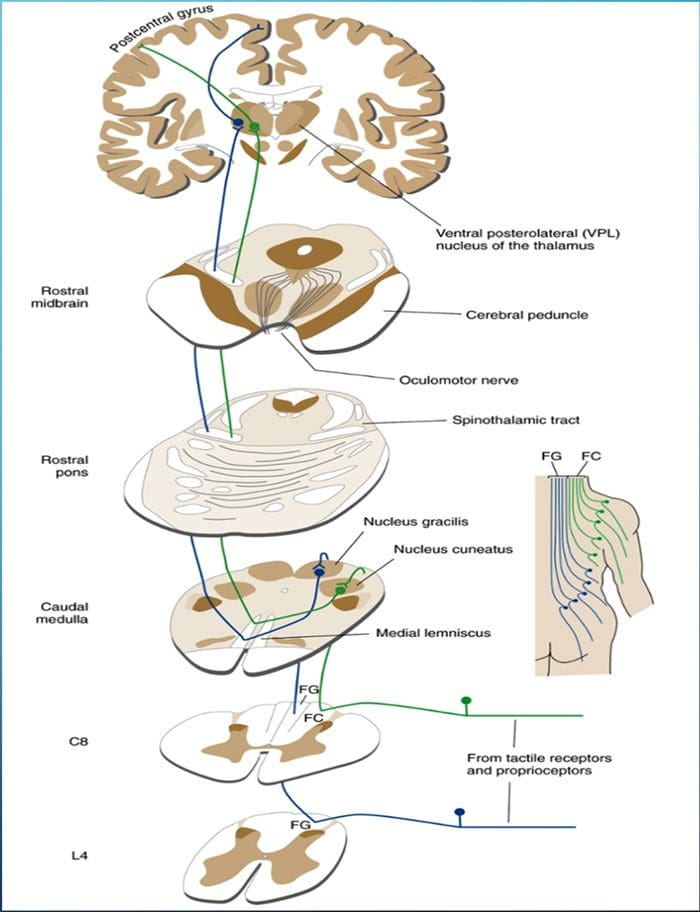 The term posterior column refers to the entire contents of a posterior funiculus, exclusive of its share of the propriospinal tract. The posterior columns consist mainly of ascending collaterals of large myelinated primary afferents carrying impulses from various kinds of mechanoreceptors (although substantial numbers of second-order fibers and unmyelinated fibers are also included). This has traditionally been considered the major pathway by which information from low-threshold cutaneous, joint, and muscle receptors reaches the cerebral cortex.
The term posterior column refers to the entire contents of a posterior funiculus, exclusive of its share of the propriospinal tract. The posterior columns consist mainly of ascending collaterals of large myelinated primary afferents carrying impulses from various kinds of mechanoreceptors (although substantial numbers of second-order fibers and unmyelinated fibers are also included). This has traditionally been considered the major pathway by which information from low-threshold cutaneous, joint, and muscle receptors reaches the cerebral cortex.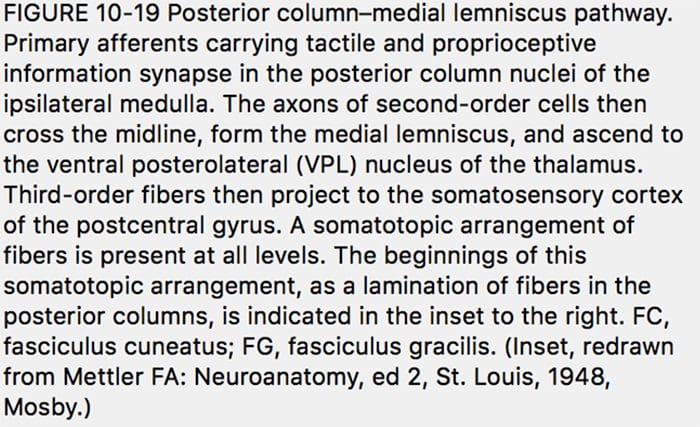
 Pain is a complex sensation, in that a noxious stimulus leads not only to the perception of where it occurred but also to things such as a rapid increase in level of attention, emotional reactions, autonomic responses, and a greater likelihood that the event and its circumstances will be remembered. Corresponding to this complexity, multiple pathways convey nociceptive information rostrally from the spinal cord. One of them (the spinothalamic tract) is analogous to the posterior column�medial lemniscus pathway.
Pain is a complex sensation, in that a noxious stimulus leads not only to the perception of where it occurred but also to things such as a rapid increase in level of attention, emotional reactions, autonomic responses, and a greater likelihood that the event and its circumstances will be remembered. Corresponding to this complexity, multiple pathways convey nociceptive information rostrally from the spinal cord. One of them (the spinothalamic tract) is analogous to the posterior column�medial lemniscus pathway.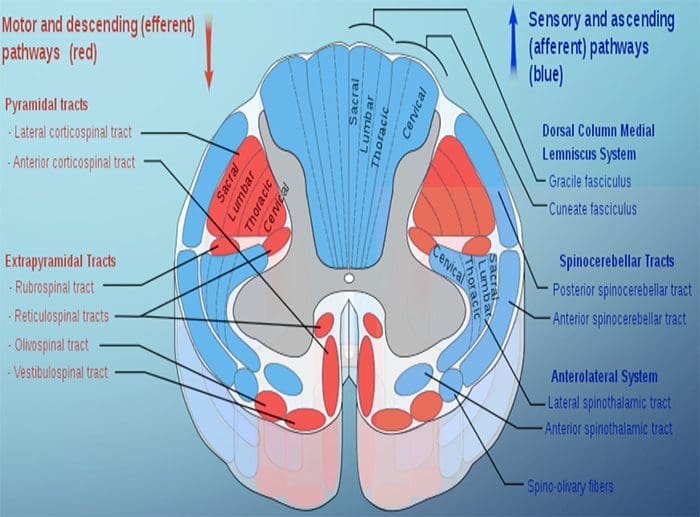




 The cell needs three things to survive.
The cell needs three things to survive.
 The health of the neuron, however, plays a huge role in how neurons can produce receptor potentials, the endurance of the neuron and the ability to create plasticity.
The health of the neuron, however, plays a huge role in how neurons can produce receptor potentials, the endurance of the neuron and the ability to create plasticity.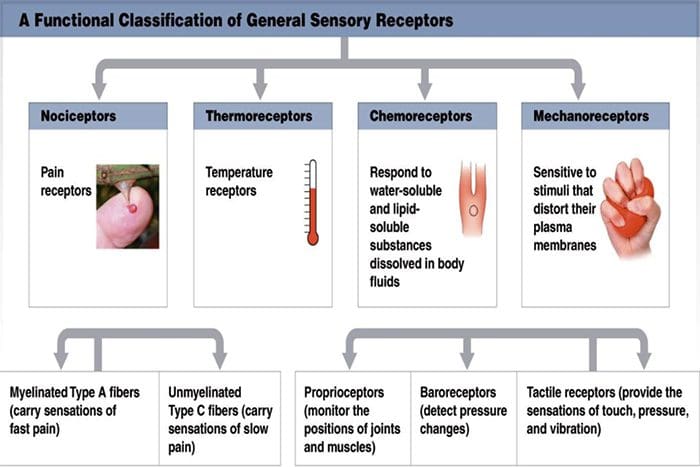 Chemoreceptors
Chemoreceptors Although their morphologies vary widely, all receptors have three general parts:
Although their morphologies vary widely, all receptors have three general parts: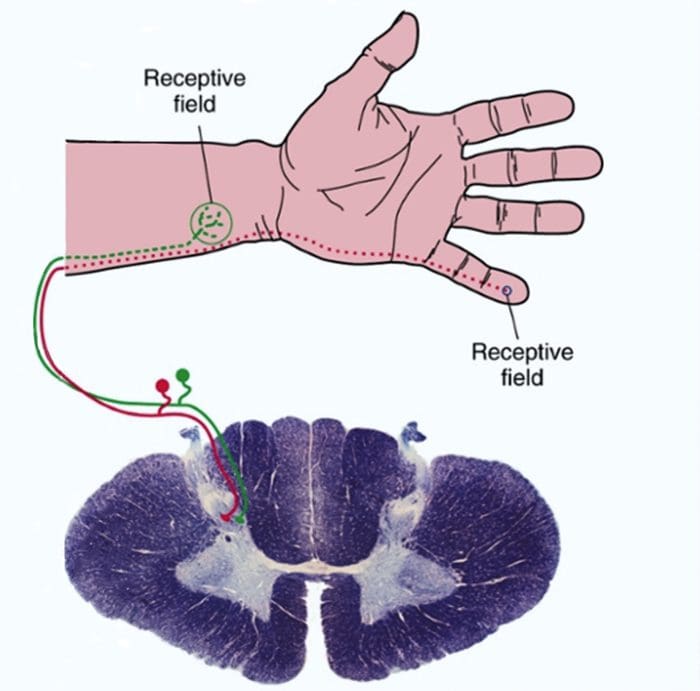
 Sensory receptors use ionotropic and metabotropic mechanisms to produce receptor potentials
Sensory receptors use ionotropic and metabotropic mechanisms to produce receptor potentials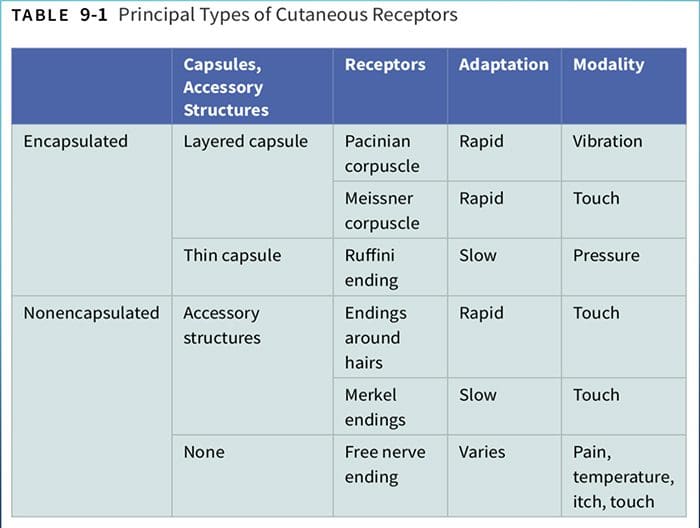
 Larger fibers conduct action potentials faster than do smaller fibers.
Larger fibers conduct action potentials faster than do smaller fibers.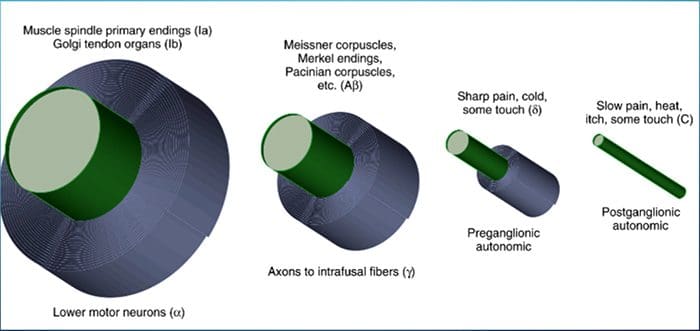

 junctions between muscles and tendons. They are similar to Ruffini endings in their basic organization, consisting of interwoven collagen bundles surrounded by a thin capsule (Fig. 9-16).
junctions between muscles and tendons. They are similar to Ruffini endings in their basic organization, consisting of interwoven collagen bundles surrounded by a thin capsule (Fig. 9-16).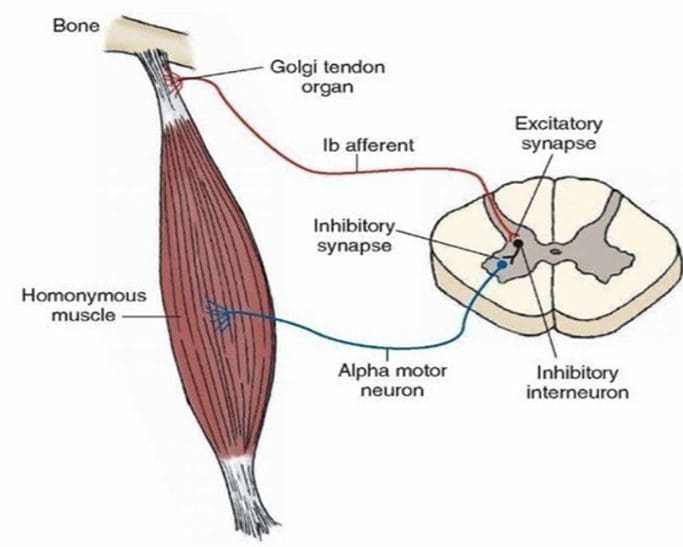 sensitive and can actually respond to the contraction of just a few muscle fibers.
sensitive and can actually respond to the contraction of just a few muscle fibers.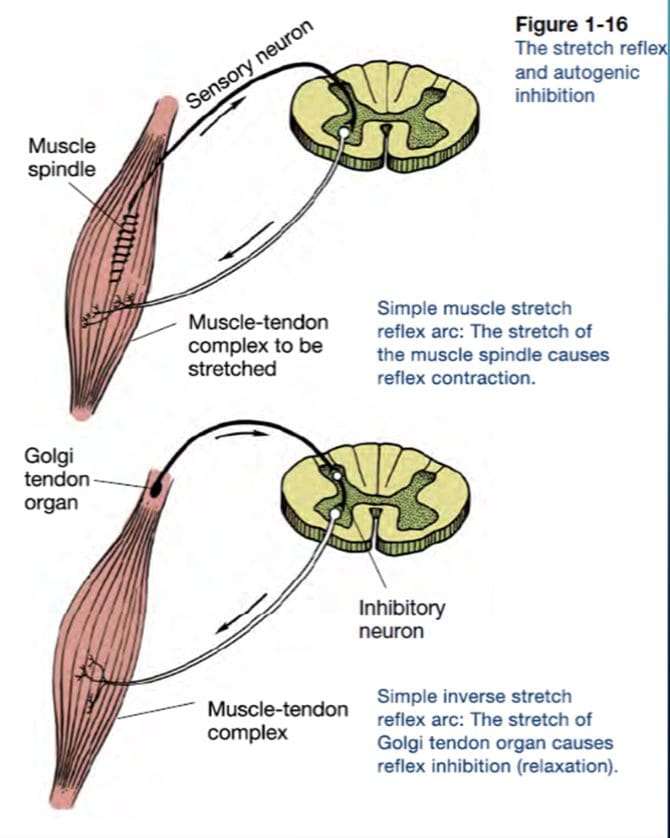





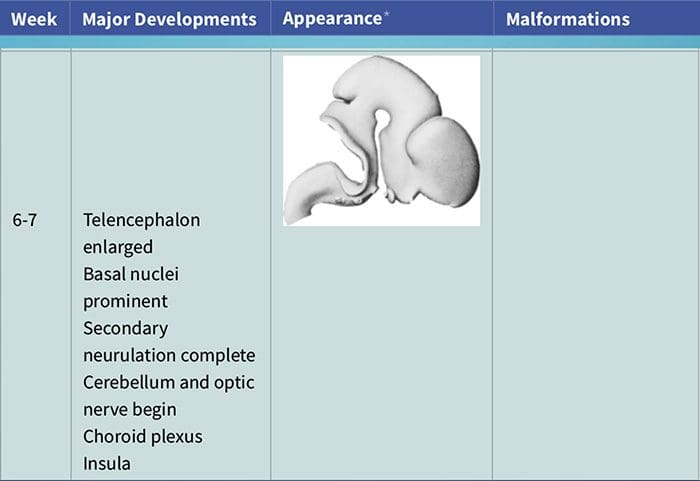
 CLINICAL SIGNIFICANCE OF NEURODEVELOPMENT
CLINICAL SIGNIFICANCE OF NEURODEVELOPMENT