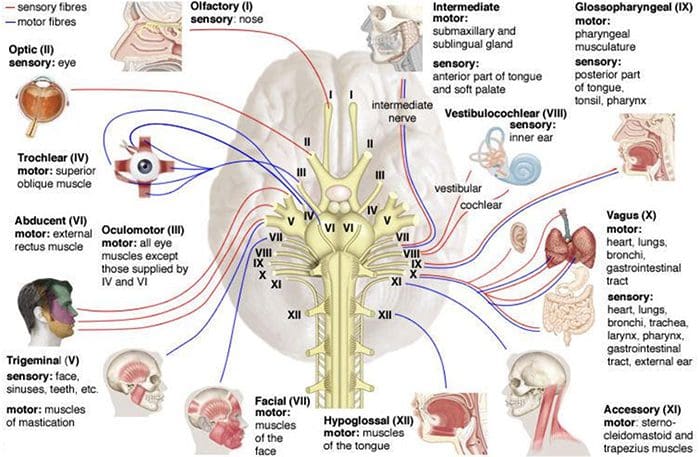
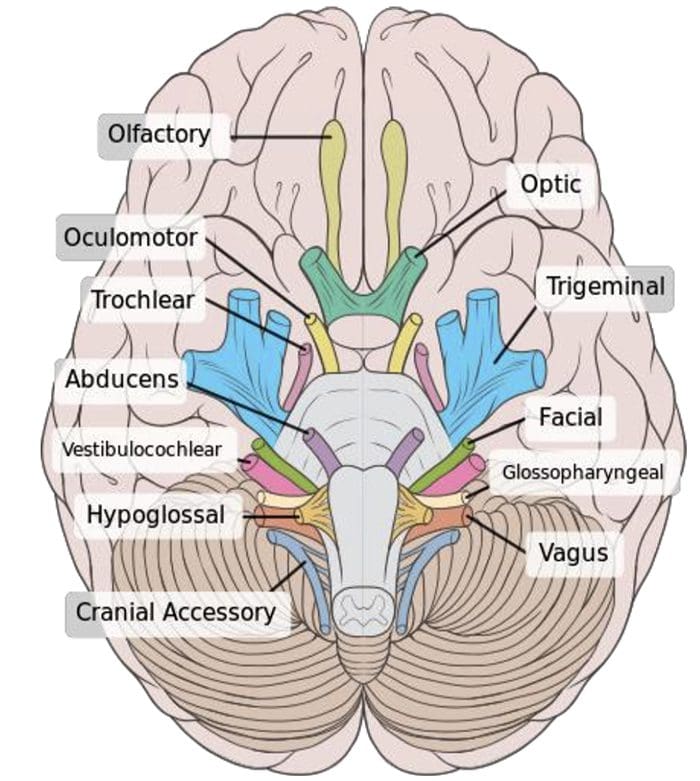
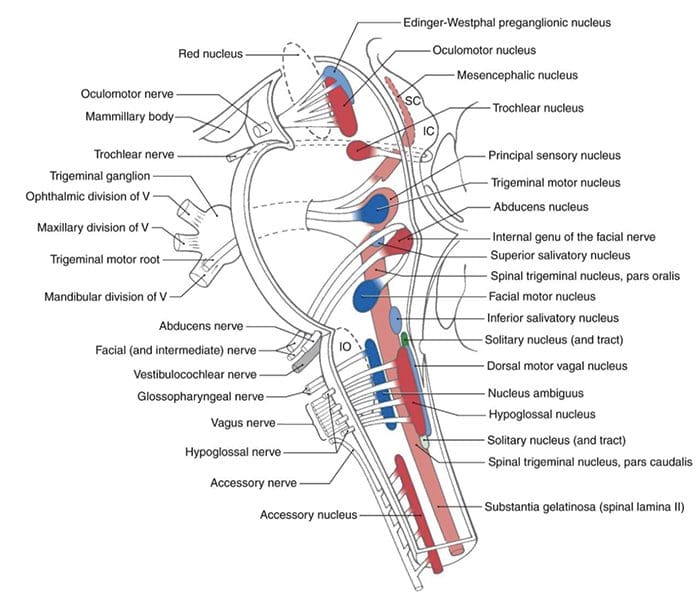
Human Cranial nerves are a set of 12 paired nerves that come directly from the brain. The first two (olfactory and optic) come from the cerebrum, with the remaining ten come from the brain stem. The names of the these nerves relate to what function they perform and are also numerically identified in roman numerals (I-XII).�The�nerves serve in functions of smell, sight, eye movement, and feeling in the face. These�nerves also control balance, hearing, and swallowing.
As with all nerves, symptoms describe the location of the lesion
Lesion in the lingual nerve will result in loss of taste, general sensation in tongue & salivary secretion
Lesion proximal to the branching of the chorda tympani such as in the facial canal will result in the same symptoms without the loss of general sensation of the tongue (because V3 has not yet joined the CN VII)
Corticobulbar innervation is asymmetric to the upper and lower parts of the Facial Motor Nucleus
If there is an UMN lesion (lesion to the corticobulbar fibers) the patient will have paralysis of the muscles of facial expression in the contralateral lower quadrant
If there is a LMN lesion (lesion to the facial nerve itself) the patient will have paralysis of the muscles of facial expression in the ipsilateral half of the face
Bell�s Palsy
Testing Cranial Nerve CN VII
Ask the patient to mimic you or follow instructions to make certain facial expressions
Be sure to assess all four quadrants of the face
Raise eyebrows
Puff cheeks
Smile
Close eyes tightly
Check for strength of the buccinator muscle against resistance
Ask patient to hold air in their cheeks as you press gently from the outside
Patient should be able to hold air in against resistance
Cranial Nerve VIII – Vestibulocochlear
Cranial Nerve VIII Clinically
Changes in hearing alone are most often due to
Infections (otitis media)
Skull fracture
The most common lesion to this nerve is caused by an acoustic neuroma
This affects CN VII and CNVIII (cochlear AND vestibular divisions) due to proximity in the internal auditory meatus
Symptoms include nausea, vomiting, dizziness, hearing loss, tinnitus, and bell�s palsy etc.
Testing Cranial Nerve CN VIII
Otoscopic Exam
Scratch Test
Can the patient hear equally on both sides?
Weber Test
Tests for lateralization
256 Hz tuning fork placed on top of the patient�s head in the center, is it louder on one side than the other?
Rinne Test
Compares air conduction to bone conduction
Normally, air conduction should last 1.5-2 as long as bone conduction
Almost everyone can say that they’ve experienced a feeling of unsteadiness or a spinning/whirling sensation in their heads at one point in their lifetimes. Usually it’s narrowed down to dizziness, however, dizziness is a broad term that can mean different things to different individuals. It is a prevalent complaint which can also be serious. Dizziness has no specific medical definition, but there are four common conditions which can be considered types of dizziness:
Vertigo. The feeling of motion where there is no movement, as if you were spinning or your environment is whirling. Spinning/whirling yourself around and around, then abruptly stopping, can produce temporary vertigo. However, when it occurs throughout an individual’s regular course of living, it could mean that there’s an underlying health issue in the vestibular system of the inner ear, the body’s equilibrium system which tells you which way is up or down and senses the position of your head. About half of all dizziness complaints are diagnosed as vertigo.
Lightheadedness. Also referred to as near syncope or pre-syncope, lightheadedness is the feeling that you’re about to faint. It is commonly believed to occur from standing up too fast or by breathing deeply enough times to generate the sensation.
Disequilibrium. A problem with walking. People with disequilibrium feel unsteady on their feet or feel as if they will fall.
Anxiety. Individuals who are scared, worried, depressed, or fearful of open spaces can use the term “dizzy” to imply feeling frightened, depressed, or anxious.
Individuals who frequently suffer from dizziness may also ultimately complain of more than one type of dizziness. For instance, people with vertigo may also feel anxious. Dizziness may be a one-time event, or it can be a chronic, long-lasting issue. Nearly everyone who experiences some form of dizziness will recover over time. This is because an individual’s sense of balance is an intricate interaction between the brain, each ear’s different vestibular system, sensors in the muscles, and sense of vision. When one component experiences dysfunction, others can generally learn how to compensate. Below, we will be narrowing down the four common types of dizziness.
Vertigo, the sensation of spinning or whirling, can be divided into two different categories: peripheral vertigo and central vertigo. Peripheral vertigo is more common than central vertigo and it typically develops due to damage to the inner ear or CN VIII. This type of vertigo produces abnormal eye movements, referred to as nystagmus, which may be horizontal or rotary.
Nystagmus is usually jerky in nature with a fast and slow phase, however it is often named for the direction of the fast phase. Peripheral vertigo may worsen when the patient looks to the side of the fast phase of nystagmus. Furthermore, the severity of nystagmus can correlate with the severity of the patient’s vertigo. Peripheral vertigo is also characterized as having no other signs and/or symptoms of CNS dysfunction. Patient may describe having symptoms of nausea or may present difficulty when walking, but only due to vestibular dysfunction. The patient may also have hearing loss or tinnitus if the CN VIII or auditory mechanism function is damaged.
The causes of peripheral vertigo are typically benign, including: benign paroxysmal positional vertigo, or BPPV, cervicogenic vertigo, acute labyrinthitis/vestibular neuronitis, Meniere’s disease, perilymph fistula, and acoustic neuroma. Identifying a patient’s cause of vertigo can be determined by narrowing down the symptoms through proper diagnosis from a healthcare professional. If movements, especially of the neck and head, aggravate vertigo, it may be attributed to BPPV, vertebrobasilar artery insufficiency or cervicogenic vertigo. If noise manifests episodes of vertigo, it may be attributed to Meniere’s disease or perilymph fistula.
Common Causes of Dizziness
Vertigo can be Brought on by many things:
Infections, such as the ones which cause the frequent cold or diarrhea, can lead to temporary vertigo through an ear infection. This inner ear disease is generally viral, benign, and usually goes away in one to six weeks, however, drugs and/or medications are readily available if these become too severe.
Benign paroxysmal positional vertigo, or BPPV, is caused by the motion of a misplaced otolith, a tiny calcium particle the size of a grain of sand, from the component of the inner ear which senses gravity into the part that senses head position. The individual feels as if their head is turning when it isn’t. After diagnosis of BPPV using a special methods known as the Dix-Hallpike test, treatment done right in the doctor’s office can help move the otolith back where it belongs and fix the health issue. This therapy, known as the Epley maneuver, has been accounted to cure vertigo 80 percent of the time.
Meniere’s disease is a disorder characterized by long-lasting episodes of severe vertigo. Other symptoms of Meniere’s disease are tinnitus, or ringing in the ears, hearing loss, and fullness or pressure in the ear.
Dandy’s syndrome is a feeling of everything bouncing up and down. It may occur to individuals who take an antibiotic that is toxic to the ear. However, it usually improves over time.
Less frequent, deadly diseases may also result in vertigo, like tumors or stroke.
Below, we will be narrowing down some of the common causes of vertigo, described above, in further detail.
Benign Paroxysmal Positional Vertigo (BPPV)
Benign paroxysmal positional vertigo, or BPPV, may develop spontaneously, particularly in the elderly. It may also commonly develop as a result of head trauma or head injury, such as that resulting from an automobile accident. Vertiginous episodes associated with BPPV may manifest through specific movements, including, looking at a high shelf, referred to as top-shelf vertigo, bending over, and rolling over in bed at night. The onset of vertigo with BPPV can begin a few seconds after movement and often resolves within a minute. As mentioned above, the diagnostic test commonly utilized to diagnose BPPV is the Dix-Hallpike maneuver. Treatment procedures to treat BPPV include the Epley maneuver and Brandt-Daroff Exercises. Furthermore, benign paroxysmal positional vertigo may also resolve on its own as the loose crystals in the inner ear dissolve, however, it may take months and new otoliths can also become displaced.
Cervicogenic vertigo occurs after a neck or head injury, however, it is not very common. It’s generally accompanied by pain and/or joint restriction where vertigo and nystagmus are less severe than that in BPPV. Cervicogenic vertigo manifests with changes in head position but does not subside as quickly as it does with benign paroxysmal positional vertigo.
Vertebrobasilar Artery Insufficiency
Vertebrobasilar artery insufficiency occurs if the vertebral artery is compressed during head rotation or extension. In this instance, the onset of vertigo is delayed more than in BPPV or cervicogenic vertigo due to the fact that ischemia often takes up to 15 seconds to occur. Orthopedic tests for vertebrobasilar artery insufficiency may help in its diagnosis. Diagnostic tests include the�Barre?-Lie?ou sign, DeKlyn Test or Dix-Hallpike Maneuver, Hautant test, Underberg test and the vertebrobasilar after functional maneuver.
Acute Labyrinthitis and Vestibular Neuronitis
Acute labyrinthitis and vestibular neuronitis are not well understood, however, they’re believed to develop as a result of inflammation. These conditions generally follow after a viral infection or may occur seemingly without a cause.�Acute labyrinthitis and vestibular neuronitis are characterized by a single, monophasic attack of vertigo which typically resolves in days to a few weeks and generally does not reoccur.
Meniere’s Disease
Meniere’s disease is characterized by increased pressure in the endolymph which causes membrane ruptures and a sudden mixture of endolymph and perilymph. With Meniere’s disease, episodes of vertigo can last from 30 minutes to several hours, or until equilibrium between the fluids in the inner ears to be reached. Over time, these episodes can damage vestibular and cochlear hair cells, resulting in low-pitch buzzing tinnitus and the loss of hearing of low tones. In comparison to Meniere’s disease, Meniere’s syndrome is when the symptoms of Meniere’s disease are found to be secondary to another condition, such as: hypothyroidism, acoustic neuroma, superior semicircular canal dehiscence or SCDS, or perilymph fistula. True Meniere’s disease is idiopathic.
Perilymph Fistula
Perilymph fistula is an abnormal connection, or tear, which causes a small leak within the inner ear due to trauma or injury, especially barotrauma. Perilymph fistula can look very similar symptomatically to Meniere’s disease/syndrome and it’s often aggravated by changes in pressure causes by airplane rides or driving uphill. Another symptom of perilymph fistula includes Hennebert’s sign, where a vertigo or nystagmus episode is brought on by sealing pressure of the ear, such as by inserting an otoscope.
Central vertigo, another category of vertigo, is less common than peripheral vertigo, as described above. It is caused by damage to the processing center of vestibular information in the brain stem and the cerebral cortex. However, episodes of dizziness are considered to be less severe than with peripheral vertigo while episodes of nystagmus are more severe than the patient’s complaint or description. This specific nystagmus associated with central vertigo may go in multiple directions, including vertical. Central vertigo may or may not have other CNS findings upon diagnosis or examination and no changes in hearing can be expected with this form of vertigo. The most common causes of central vertigo include: cerebrovascular disease, such as transient ischemic attacks, multiple sclerosis, Arnold-Chiari malformation, damage to caudal brainstem or vestibulocerebellum and/or migraine condition.
Lightheadedness, or pre-syncope dizziness, is generally caused by some surrounding circumstance impairing blood flow into the brain when an individual is standing up. Blame this problem on our ancestors who learned to walk upright, placing our brain above our heart. It is a challenge for your heart to keep the brain supplied with blood and it is easy for this system to break down. When blood vessels in the brain become dilated, or enlarged, as a result of elevated fever, excitement or hyperventilation, alcohol ingestion, or prescription drugs and/or medications, such as antidepressants, it’s no wonder someone may commonly get lightheaded. There can also be serious causes, however, such as a stroke and cardiovascular disease.
Pre-syncope dizziness is specifically from cardiac origin, such as output disorders, arrhythmias, Holter monitor testing. It may also be caused by postural/orthostatic hypotension, which may be secondary to other health issues like diabetic neuropathy, adrenal hypofunction, Parkinsons, certain drugs and/or medications, etc. Light-headedness can involve vasovagal episodes accompanied by slow heart rate with low blood pressure often caused by stress, anxiety or hyperventilation. Finally, pre-syncope dizziness can be caused by migraine headaches due to cerebrovascular instability and blood sugar dysregulation.
Disequlibrium, can be caused by:
A type of arthritis in the neck called cervical spondylosis, which puts stress on the spinal cord.
Parkinson’s disease or related disorders that cause an individual to stoop forward.
Disorders involving part of the brain known as the cerebellum. The cerebellum is the part of the brain responsible for coordination and balance.
Diseases like diabetes that can lead to lack of sensation in the legs.
Disequilibrium is most common in the elderly and it generally occurs due to sensory deficits. In addition, disequilibrium has a gradual onset which worsens with reduced vision, darkness, eyes closed and visual acuity losses. However, it is improved by touching a stationary object which is often subjective as dizziness improves with a gait assistive device like a cane, walker, etc.
Dr. Alex Jimenez’s Insights
If you’ve ever experienced a sudden spinning or whirling sensation or even felt faint, woozy or unsteady, you’re not alone. Dizziness is a term used to describe a range of sensations and it is one of the most common reasons why many adults visit their healthcare professionals. While these false sensations can rarely signal a life-threatening condition, frequent episodes can significantly affect an individual’s quality of life. Diagnosis and treatment of dizziness can depend largely on the cause of the symptoms. Fortunately, many treatment methods used to treat dizziness are considered safe and effective.
Other causes of dizziness can be attributed to psychological stress. In this instance, the patient will describe their dizziness as a “floating” sensation.�Dizziness in the kind of anxiety is frequently, but not always, caused by depression. In addition, it can be attributed to an anxiety disorder or anxiety. Various medications can also cause dizziness as a side effect. It’s essential for a healthcare professional to rule out this type of dizziness caused by hyperventilation as well as other types of dizziness. The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Sciatica
Sciatica is medically referred to as a collection of symptoms, rather than a single injury and/or condition. Symptoms of sciatic nerve pain, or sciatica, can vary in frequency and intensity, however, it is most commonly described as a sudden, sharp (knife-like) or electrical pain that radiates from the low back down the buttocks, hips, thighs and legs into the foot. Other symptoms of sciatica may include, tingling or burning sensations, numbness and weakness along the length of the sciatic nerve. Sciatica most frequently affects individuals between the ages of 30 and 50 years. It may often develop as a result of the degeneration of the spine due to age, however, the compression and irritation of the sciatic nerve caused by a bulging or herniated disc, among other spinal health issues, may also cause sciatic nerve pain.
Ataxia is a medical term used to describe a lack of muscle control or coordination of voluntary movements, including everyday physical activities like walking or picking up objects. Often referred to as a symptoms of an underlying health issue, ataxia can affect various movements, causing difficulties with speech patterns and language, eye movement and even swallowing.
Persistent ataxia generally results from damage to the part of the brain which controls muscle coordination, known as the cerebellum. Many causes and conditions can lead to ataxia, such as alcohol abuse, certain drugs and/or medications, stroke, tumors, cerebral palsy, brain degeneration and multiple sclerosis. Inherited faulty genes have also been associated to lead to ataxia.
Diagnosis and treatment for ataxia depends largely on the cause and/or condition. Adaptive devices, including walkers or canes, can help patients with ataxia maintain their independence. Chiropractic care, physical therapy, occupational therapy, speech therapy and regular aerobic stretches and exercises can also help improve the symptoms associated with this health issue.
Symptoms of Ataxia
Ataxia is a health issue which can develop gradually over time or it can come on unexpectedly. As a symptom of a number of neurological disorders, ataxia may ultimately lead to:
Poor coordination
Unsteady walk along with a tendency to stumble
Difficulty with fine motor tasks, such as eating, writing or buttoning a shirt
Changes in speech
Involuntary back-and-forth eye movements, known as nystagmus
Difficulty swallowing
When to Visit a Doctor
In the instance that a patient is not aware of whether they may have an underlying health issue that causes ataxia, such as multiple sclerosis, it’s essential to visit a doctor immediately if the patient:
Loses equilibrium
Loses muscle coordination at a hand, leg or arm
Has difficulty walking
Slurs their speech
Has trouble swallowing
Causes of Ataxia
Damage, degeneration or loss of neural cells in the section of the brain which controls muscle coordination, or the cerebellum, often results in ataxia. The cerebellum is made up of two pingpong-ball-sized parts of folded tissue located at the base of the brain close to the brainstem. The right side of the cerebellum controls coordination over the right side of the body; the left side of the cerebellum controls coordination on the left side of the body. Diseases that damage the spinal cord and peripheral nerves which connect the cerebellum to the muscles can also lead to ataxia. Ataxia causes include:
Head trauma. Damage to the brain or spinal cord due to a blow to the head, such as in the case of an automobile accident, can cause acute cerebellar ataxia, which comes on unexpectedly.
Stroke. After the blood supply to part of the brain is interrupted or severely reduced, depriving brain tissue of nutrients and oxygen, brain cells die.
Cerebral palsy. This can be a general term for a group of disorders brought on by damage to a child’s brain during early development, before, during or shortly after birth, which affects the child’s ability to coordinate body movements.
Autoimmune diseases. Multiple sclerosis, sarcoidosis, celiac disease and other autoimmune conditions can cause ataxia.
Infections. Ataxia may be an uncommon complication of chickenpox and other viral ailments. It may manifest in the healing phases of the infection and can last for days or weeks. Generally, the ataxia resolves over time.
Paraneoplastic syndromes. These are rare, degenerative health issues triggered by the body’s own immune system’s reaction to a cancerous tumor, referred to as neoplasm, most frequently from lung, ovarian, breast or lymphatic cancer. Ataxia can appear months or years before the cancer is even diagnosed.
Tumors. A growth on the brain, cancerous, or malignant, or noncancerous, or benign, can also harm the cerebellum, leading to ataxia.
Toxic reaction. Ataxia is a possible side effect of certain drugs and/or medications, particularly barbiturates, like phenobarbital; sedatives, like benzodiazepines; as well as some kinds of chemotherapy. These are important to diagnose because the effects are usually reversible. Also, some drugs and/or medications can cause problems with age, which means a person may need to reduce their dose or discontinue its use. Alcohol and drug intoxication; heavy metal poisoning, such as from mercury or lead; and solvent poisoning, like from paint thinner, can also cause ataxia.
Vitamin E, vitamin B-12 or thiamine deficiency. Not getting enough of these nutrients, due to the inability to absorb them enough, alcohol misuse or other reasons, may also ultimately lead to ataxia.
For a number of adults that develop sporadic ataxia, no particular cause is found. Sporadic ataxia can take lots of forms, including multiple system atrophy, a progressive and degenerative disease.
Dr. Alex Jimenez’s Insights
The cerebellum is the region of the brain which is in charge of controlling movement in the body. Electrical signals are transmitted from the brain through the spinal cord and into the peripheral nerves to stimulate a muscle to contract and initiate movement. Sensory nerves also gather data from the environment regarding position and proprioception. When one or more of these pathway components experiences a problem, it can subsequently lead to ataxia. Ataxia is a medical term utilized to describe the lack of muscle coordination when a voluntary movement is attempted. It can make any motion which requires muscles to function a challenge, from walking to picking up an object, even swallowing. Diagnosis and treatment can help manage and improve the symptoms associated with ataxia.
Diagnosis of Ataxia
If an individual has developed symptoms of ataxia, a healthcare professional may perform a diagnosis in order to look for a treatable cause. Besides running a physical examination and a neurological examination, including assessing a patient’s memory and concentration, vision, hearing, balance, coordination, and reflexes, your doctor might request lab tests, including:
Imaging studies. A CT scan or MRI of a patient’s brain might help determine possible causes of ataxia. An MRI can sometimes reveal shrinkage of the cerebellum and other brain structures in people with ataxia. It might also demonstrate other findings that are treatable, such as a blood clot or benign tumor, which may be pressing on the cerebellum.
Lumbar puncture (spinal tap). A needle is inserted into the lower spine, or the lumbar spine, between two lumbar bones, or vertebrae, to remove a sample of cerebrospinal fluid. The fluid, which surrounds and protects the brain and spinal cord, is transported to a laboratory for testing.
Genetic testing. A healthcare professional might recommend genetic testing to determine whether a child has the gene mutation which causes hereditary ataxia. Gene tests are available for many but not all of the hereditary ataxias.
Furthermore, diagnosing ataxia may depend on which system is affected. For instance,�if the health issue lies in the vestibular system, the patient will experience dizziness, possibly having vertigo or nystagmus. They may also be unable to walk in a straight line and when walking, they will tend to veer to one side. If the health issue lies in the cerebellar system, cerebellar gaits present with a wide-base and generally involves staggering and titubation. Patient will also have difficulty doing the Rhomberg�s test with their eyes open or closed, because they cannot stand with their feet together, as described below.
Testing the Vestibular System
Testing the vestibular system to determine the diagnosis of ataxia can include the Fakuda Stepping Test and the Rhomberg Test. The�Fakuda Stepping Test is performed by having the patient march in place with their eyes closed and their arms raised to 90 degrees in front of them. If they rotate more than 30 degrees, the test is considered to be positive. It’s important to note that the patient will rotate toward the side of the vestibular dysfunction. The Rhomberg Test will confirm a diagnosis of ataxia if the patient sways a different direction every time their eyes are closed, as this may indicate vestibular dysfunction.
Testing the Cerebellar System
Testing the cerebellar system to determine the diagnosis of ataxia can include the piano-playing test and the hand-patting test as well as the finger-to-nose test. The piano-playing test and hand-patting test both assess for dysdiadochokinesia. Also in both tests, the patient will have more difficulty moving the limb on the side of cerebellar dysfunction. With the finger-to-nose test, the patient may be hyper/hypo metric in movement and intention tremor may be reveled.
Joint Position Sense
In patients with changes to their joint position sense, conscious proprioception may be diminished, especially in elderly patients and patients with neuropathy. Patients with joint position sense losses often rely on visual information to help compensate. When visual input is removed or diminished, these patient�s have exaggerated ataxia.
Motor Strength and Coordination
If the patient has reduced frontal lobe control, they may end up with an apraxia of gait, where they have difficult with the volitional control of movement. Extrapyramidal disorders, such as Parkinson disease, result in the inability to control motor coordination. Pelvic girdle muscle weakness due to a myopathy in this instance will produce an abnormal gait pattern.
There’s no specific treatment for ataxia. In some cases, treating the underlying health issue often resolves the ataxia, such as quitting the use of drugs and/or medications that cause it. In other cases, such as ataxia that results from chickenpox or other viral infection, it’s likely to resolve on its own. A healthcare professional might recommend treatment to manage symptoms, such as pain, fatigue or nausea, or they may recommend the use of adaptive devices or therapies to help with ataxia. Chiropractic care is a safe and effective, alternative treatment option which focuses on the treatment of a variety of injuries and/or conditions associated with the musculoskeletal and nervous system. A chiropractor commonly uses spinal adjustments and manual manipulations to correct any spinal misalignment, or subluxation, which may be causing a patient’s symptoms. In addition, a doctor of chiropractic, or chiropractor, may also recommend a series of appropriate lifestyle modifications, including nutritional advice and exercise plans, in order to restore a patient’s strength, mobility and flexibility. Chiropractic care together with the proper fitness routine can help speed up the patient’s recovery process.
Adaptive Devices
Ataxia brought on by conditions like multiple sclerosis or cerebral palsy might not be curable. In that circumstance, a healthcare professional might have the ability to recommend adaptive devices. These can include:
Hiking sticks or walkers for walking
Modified utensils for eating
Communication aids for speaking
Other therapies
A patient with ataxia might benefit from particular therapies, including: physical therapy to help improve coordination and enhance mobility; occupational treatment to help with daily living activities, such as eating on their own; and speech therapy to improve speech as well as aid with swallowing.
Coping and Support
The challenges a person face when living with ataxia or with a child with the condition might make the patient feel lonely or it may contribute to depression and anxiety. Talking to a counselor or therapist may help. Or perhaps the patient may find encouragement and understanding in a support group, possibly for ataxia or for their specific underlying condition, such as cancer or multiple sclerosis.
Although support groups aren’t for everyone, they may be good sources of advice. Group members often know about the newest treatments and tend to share their own experiences. If you’re interested, your healthcare professional may be able to recommend a group in your area. The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Sciatica
Sciatica is medically referred to as a collection of symptoms, rather than a single injury and/or condition. Symptoms of sciatic nerve pain, or sciatica, can vary in frequency and intensity, however, it is most commonly described as a sudden, sharp (knife-like) or electrical pain that radiates from the low back down the buttocks, hips, thighs and legs into the foot. Other symptoms of sciatica may include, tingling or burning sensations, numbness and weakness along the length of the sciatic nerve. Sciatica most frequently affects individuals between the ages of 30 and 50 years. It may often develop as a result of the degeneration of the spine due to age, however, the compression and irritation of the sciatic nerve caused by a bulging or herniated disc, among other spinal health issues, may also cause sciatic nerve pain.
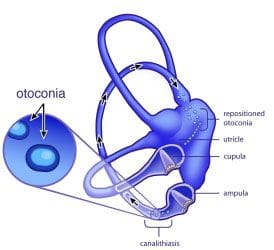
Benign paroxysmal positional vertigo, or BPPV, is a mechanical issue in the inner ear. It occurs when some of the calcium carbonate crystals (otoconia) that are normally embedded in gel at the utricle become dislodged and migrate to at least one of those 3 fluid-filled semicircular canals, where they are not supposed to be. When enough of these particles accumulate in one of the canals they interfere with the normal fluid motion that these canals utilize to sense head motion, causing the inner ear to send false signals to the mind.
Fluid in the semi-circular canals doesn’t normally react to gravity. However, the crystals do proceed with gravity, thereby shifting the fluid when it normally would be still. When the fluid moves, nerve endings in the canal are eager and send a message to the brain the mind is moving, even though it is not. This false information doesn’t match what another ear is sensing, together with what the eyes are seeing, or with what the joints and muscles are doing, and also this mismatched information is perceived by the brain as a turning sensation, or vertigo, which generally lasts less than one minute. Between vertigo spells some people today feel symptom-free, while some feel a mild sense of imbalance or disequilibrium.
A healthcare professional will execute a collection of tests and evaluations in order to properly diagnose the individual’s BPPV. Regular medical imaging (e.g. an MRI) is not helpful in diagnosing BPPV, because it doesn’t show the crystals which have moved to the semi-circular canals. But when someone with BPPV has their own head moved into a position that produces the dislodged crystals move within a tube, the error signals cause the eyes to move in a very specific pattern, called”nystagmus”.
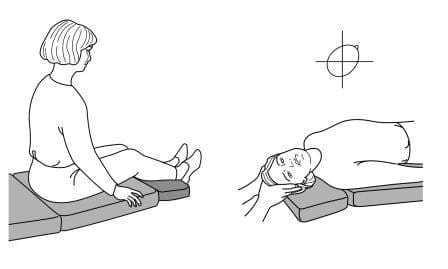
The nystagmus will possess distinct characteristics that let a trained practitioner to identify which ear the crystals that are displaced are in, and then canal(s) they have moved into. Tests such as the Dix-Hallpike or Roll Tests involve moving the head into specific orientations, allowing gravity to move the dislodged crystals and activate the vertigo while the professional watches for the tell-tale eye movements, or nystagmus.�To execute the Dix-Hallpike test, a healthcare professional will ask the patient to sit on the test table with their legs stretched out. They will then turn the head 45 degrees to one side, which contrasts the right posterior semicircular canal with the sagittal plane of the body, then they are going to allow the patient to lie back quickly, while the eyes are open, so that their head hangs slightly over the edge of the desk.
When the health care provider has finished the diagnosis, then they can perform the appropriate treatment maneuver. The maneuvers make use of gravity to guide the crystals back to the room where they are supposed to be via a very specific series of head movements, commonly referred to as Repositioning Maneuvers. Repositioning maneuvers are highly effective in treating BPPV, inexpensive, and easy to apply.
Dr. Alex Jimenez’s Insights
While the use of surgical interventions as well as that of drugs and/or medications are occasionally recommended to relieve the symptoms associated with benign paroxysmal positional vertigo, or BPPV, they do not treat the underlying health issue. Repositioning maneuvers, like the ones demonstrated below, are considered to be safe yet effective treatment options for BPPV. There is good evidence to support the treatment of BPPV with the Epley maneuver. Although less amounts of research studies have been conducted on other repositioning maneuvers, outcome measures of a variety of patients with BPPV have benefitted from the other treatment options for benign paroxysmal positional vertigo.
Considering that the therapeutic efficacy among maneuvers for every canal is comparable, the option of treatment is generally predicated on clinician preference, complexity of their maneuvers themselves, therapy response to certain maneuvers, as well as musculoskeletal considerations, such as arthritic changes and range of motion of the cervical spine. Below, many repositioning maneuvers are demonstrated, for instance, deep mind hanging maneuver, the Lempert (BBQ) maneuver and the Epley maneuver.
The deep head hanging maneuver is a repositioning maneuver which is used for one of the least common places where BPPV occurs, the superior semi-circular canal, amounting to only about 2 percent of most benign paroxysmal positional vertigo instances. However, the advantage of deep head hanging maneuvers is that they may be effectively performed without knowledge of the side involved. It consists of three steps with four position changes at intervals of approximately 30 seconds.
The deep head hanging maneuver is performed with the patient at the long-sitting position, while the head is brought to a minimum of 30� below the horizontal with the head straight up. When the nystagmus induced by this measure is finished, the head is brought up rapidly to touch the chest while the patient remains supine, and after 30 seconds, the individual has been brought back to a seated position with head flexion maintained. Finally, the patient will be brought back to a neutral head position.
The Lempert maneuver, also referred to as the Barbeque maneuver or the Roll maneuver, is a repositioning maneuver commonly utilized to help treat canilithiasis of the horizontal and lateral canal. It might occur as a complication of posterior canal BPPV treatment repositioning maneuvers. The side with the most notable horizontal nystagmus is assumed to be the affected side.
To perform the Lempert maneuver, the patient should lie supine on the exam table, using the affected ear facing down. Afterward, the healthcare professional will quickly turn the head 90� towards the unaffected side, facing up, waiting 15-20 minutes between each head turn. The medical professional will subsequently turn the head 90� so the affected ear is currently facing up. The next step includes having the individual tuck their arms to their torso, in order to allow the doctor to roll the patient to a more moderate position with their head down. The individual must be turned on their side since the physician rolls their head 90� (returning them to their original position, with the affected ear facing down ). At length, the medical professional should place the patient so that they are face up and bring them into a sitting posture.
Treatment with the Lempert maneuver is efficient approximately 75% of the moment, however, the effectiveness can vary from individual to individual. It is important to keep in mind that longer periods of time between head turns may provoke nausea. This sort of repositioning maneuver shouldn’t be done on patients in which it isn’t safe to move their mind, including in the case of cervical spine injuries.
Epley Maneuver for BPPV
The most common repositioning maneuver for the treatment of benign paroxysmal positional vertigo, or BPPV, is known as the Epley maneuver. The Epley maneuver, occasionally referred to as the canalith repositioning maneuver, is a process which involves a series of head movements, normally performed by a healthcare professional who’s experienced and qualified in the treatment of vestibular disorders, so as to relieve the symptoms associated with BPPV, including dizziness.
The Epley maneuver is performed by placing the patient’s mind at an angle in where gravity can help alleviate the symptoms. Tilting the mind can move the crystals out of the semicircular canals of the inner ear. This means that they will quit displacing the fluid, relieving the dizziness and nausea they may have been causing. In this manner, the Epley maneuver alleviates the symptoms of BPPV. But, it may have to be repeated more than once, as occasionally, some head movements can once again displace the small crystals of the internal ear, once they had been repositions after the first treatment.
Research studies have shown that the Epley maneuver is a safe and effective treatment for the specific vertigo disorder, offering both long-term and immediate relief. The Epley maneuver, named after Dr. John Epley, has been named the canalith repositioning maneuver because it helps to reposition the small crystals at a person’s inner ear, which might be causing the sensation of dizziness.
Repositioning these tiny crystals called otoconia helps to ease BPPV symptoms.�There are two types of BPPV: one where the loose crystals can move freely in the fluid of the canal (canalithiasis), and, more rarely, one where the crystals are thought to be �hung up� on the bundle of nerves that sense the fluid movement (cupulolithiasis).�It is important to make this distinction, as each repositioning maneuver may affect each variant differently. The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Sciatica
Sciatica is medically referred to as a collection of symptoms, rather than a single injury and/or condition. Symptoms of sciatic nerve pain, or sciatica, can vary in frequency and intensity, however, it is most commonly described as a sudden, sharp (knife-like) or electrical pain that radiates from the low back down the buttocks, hips, thighs and legs into the foot. Other symptoms of sciatica may include, tingling or burning sensations, numbness and weakness along the length of the sciatic nerve. Sciatica most frequently affects individuals between the ages of 30 and 50 years. It may often develop as a result of the degeneration of the spine due to age, however, the compression and irritation of the sciatic nerve caused by a bulging or herniated disc, among other spinal health issues, may also cause sciatic nerve pain.
Benign paroxysmal positional vertigo is a common type of vertigo, a sensation of spinning or whirling and loss of balance, which has been reported to account for as many as 17 percent of all cases of dizziness. Benign paroxysmal positional vertigo, or BPPV, is believed to be caused by a health issue in the inner ear. While it is typically associated with aging, head injuries have also been found to cause BPPV.
BPPV occurs when several of the small crystals found in the inner ear, known as otoconia, become loose and wind up in one or more of the three fluid-filled semicircular canals of the ear. Whenever these crystals move around the inner ear, they can cause the fluid in the semicircular canals to become displaced. This ultimately results in a spinning or whirling sensation, otherwise referred to as vertigo. The symptoms of BPPV can often come on suddenly when an individual with benign paroxysmal positional vertigo moves their head in a certain position. By way of instance, symptoms may trigger when turning over in bed during night time. Symptoms of BPPV can last anywhere from several seconds to several minutes, and may include:
Dizziness;
A feeling that surroundings are spinning or moving (vertigo);
A loss of equilibrium or balance;
Nausea; and
Vomiting.
BPPV Treatment
Although many healthcare professionals often prescribe drugs and/or medications for BPPV, there is not enough evidence to support their use as treatment for this condition. In other, very rare cases, surgical interventions are considered. However, in the majority of instances, BPPV can safely and effectively be adjusted mechanically.
Once a healthcare professional specializing in vestibular disorders, such as a vestibular rehabilitation therapist, a chiropractor, a specially trained physical therapist, an occupational therapist or audiologist, or an ENT (ear, nose & throat specialist who specializes on vestibular disorders), has properly diagnosed the individual’s type of benign paroxysmal positional vertigo by performing tests like the Dix-Hallpike Test, then they’ll have the ability to understand which of the semicircular canal(s) the crystals are in, and whether it is canalithiasis, where the loose crystals can move freely in the fluid of the tube, or cupulolithiasis, where the crystals are believed to be ‘hung up’ on the bundle of nerves that feel the fluid motion, then they can recommend you the appropriate therapy maneuver.
Other Auditory & Vestibular Function Tests
The Dix-Hallpike Test is commonly used to diagnose BPPV, however, if the diagnosis is negative, healthcare professionals may utilize a variety of other auditory and vestibular function tests in order to properly diagnose the patient’s source of their symptoms.
The most common treatment for benign paroxysmal positional vertigo, or BPPV, is called the Epley maneuver. The Epley maneuver, sometimes referred to as canalith repositioning, is a procedure which involves a succession of head movements, normally performed by a healthcare professional who is qualified and experienced in the treatment of vestibular disorders, in order to relieve the symptoms associated with BPPV.
Research studies have demonstrated that the Epley maneuver is a safe and effective treatment for the condition, offering both immediate and long-term relief. The Epley maneuver, named after Dr. John Epley, has been named the canalith repositioning maneuver because it�helps reposition the small crystals in a individual’s ear, which may be causing the sensation of dizziness. Repositioning these small crystals, also known as otoconia, ultimately helps to relieve BPPV symptoms.
The Epley maneuver is performed by placing the patient’s head at an angle from where gravity can help alleviate the symptoms. Tilting the head can move the crystals from the semicircular canals of the inner ear. This means that they will stop displacing the fluid, relieving the dizziness and nausea they may have been causing. In this way, the Epley maneuver alleviates the symptoms of BPPV. But, it may need to be repeated more than once, as occasionally, some head movements can once again displace the small crystals of the inner ear, once they had already been repositions after the initial treatment.
When a healthcare professional carries out the Epley maneuver, they’ll perform the following measures:
Ask the patient to sit upright in an examination table, completely extending their legs out in front of them.
Rotate the patient’s head in a 45-degree angle to the side they’re experiencing the worst vertigo.
Instantly push the patient back, so they are lying with their shoulders touching the table. The patient’s head is retained facing the side most negatively affected by vertigo but at a 30-degree angle, so that it is lifted slightly off the table. The healthcare professional holds the patient in this position for between 30 seconds and two minutes, until their symptoms stop.
Rotate the patient’s head 90 degrees from the opposite direction, stopping when the other ear is 30 degrees away from the table. Again, the doctor holds the patient in this position for between 30 minutes and two minutes, until their symptoms cease.
Next, the healthcare professional will roll the patient in precisely the same direction that they are facing, onto their side. The moment they encounter the worst vertigo on will be facing upward. The physician holds the patient in this position for between 30 minutes and 2 minutes, until their symptoms stop.
Eventually, the healthcare professional will bring the patient back up into a sitting position.
The whole process is repeated up to three times, until the patients’s symptoms have been completely relieved.
A healthcare professional specializing in vestibular disorders, such as a chiropractor or physical therapist, will utilize the Epley maneuver to help alleviate an individual’s dizziness and nausea, among other symptoms, when they have decided that BPPV is the cause. As mentioned before, the Epley maneuver isn’t suitable to treat vertigo brought on by another health issue aside from BPPV. If the individual is unsure of what is causing their vertigo, they ought to talk to a doctor and ask to be properly diagnosed. Other causes of vertigo may include:
Migraine headaches
Ear infections
Anemia
Cerebellar stroke
After performing the Epley maneuver, a doctor will advise the patient who has BPPV to prevent specific movements that may dislodge the crystals. These movements include:
Bending quickly
Lying down fast
Leaning the head
Moving the head back and forth
Many research studies have been done on the safety and effectiveness of therapy maneuvers for BPPV, such as the Epley maneuver, together with results and outcome measures demonstrating that the rates of recovery are well into the 90 percent range by 1 to 3 treatments. The more infrequent cupulolithiasis, or ‘hung-up’ version of BPPV, can be a little more stubborn to resolve, as this type of BPPV is generally the consequence of trauma or injury.
Dr. Alex Jimenez’s Insight
If you’ve ever experienced a sudden spinning or whirling sensation, dizziness and nausea when you make certain head movements, especially while rolling over in bed at night or when getting out of bed in the morning, you may be suffering from a common condition called benign paroxysmal positional vertigo, or BPPV. This type of vertigo can be frustrating to deal with and it can tremendously affect an individual’s quality of life. A healthcare professional who specializes in vestibular disorders, including chiropractors and physical therapists, frequently diagnose BPPV using the Dix-Hallpike Test before following up treatment for benign paroxysmal positional vertigo using the Epley maneuver.
Benign Paroxysmal Positional Vertigo, or BPPV, is a frequent health issue, and will be encountered more and more as our population ages. The effect can vary from a mild annoyance to a highly debilitating condition, and can affect function and safety as well as increase the risk of falls. Fortunately, symptoms tend to decrease in intensity over time as the brain gradually adjusts to the strange signals it is receiving, or as the condition resolves on its own. However, with a healthcare professional who’s suitably qualified and experienced in the diagnosis and treatment of BPPV, most patients will find overall relief of their problem once it readily corrected and their world stops spinning or whirling. The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Sciatica
Sciatica is medically referred to as a collection of symptoms, rather than a single injury and/or condition. Symptoms of sciatic nerve pain, or sciatica, can vary in frequency and intensity, however, it is most commonly described as a sudden, sharp (knife-like) or electrical pain that radiates from the low back down the buttocks, hips, thighs and legs into the foot. Other symptoms of sciatica may include, tingling or burning sensations, numbness and weakness along the length of the sciatic nerve. Sciatica most frequently affects individuals between the ages of 30 and 50 years. It may often develop as a result of the degeneration of the spine due to age, however, the compression and irritation of the sciatic nerve caused by a bulging or herniated disc, among other spinal health issues, may also cause sciatic nerve pain.
Benign Paroxysmal Positional Vertigo, or BPPV, is the most common vestibular disorder and it is by far the most common cause of vertigo, a false sensation of rotational movement or spinning. BPPV isn’t life-threatening, it can come in unexpectedly in brief spells and it can trigger with certain head positions or motions. This might frequently occur when you tip your head down or up, when you lie down, or when you flip over or sit up in bed.
BPPV is a mechanical problem in the inner ear. It occurs when some of the calcium carbonate crystals, known as otoconia, that are typically embedded in gel at the utricle, become dislodged and migrate into at least one of the 3 fluid-filled semicircular canals, in which they are not supposed to be. When enough of these particles collect among the canals, they interfere with the fluid movement that these canals use to sense head motion, causing the internal ear to send false signals to the brain.
Fluid from the canals does not normally respond to gravity. On the other hand, the crystals do interact with gravity, thereby shifting the fluid when it normally would remain still. After the fluid moves, nerve endings in the canal are triggered and send a message to the brain that the head is moving, even though it is not. This false information does not match what the other ear may be sensing, together with what the eyes are seeing, or using what the muscles and joints do, and this mismatched information is sensed by the brain as a spinning sensation, or vertigo, which normally lasts less than one minute. Between vertigo spells some people may feel symptom-free, while others feel a mild sense of imbalance or disequilibrium.
Symptoms of BPPV
The signs and symptoms of benign paroxysmal positional vertigo, or BPPV, may include:
Dizziness
A feeling that you or your surroundings are spinning or moving (vertigo)
A loss of equilibrium or balance
Nausea
Vomiting
The signs and symptoms of BPPV can come and go, with these generally lasting less than one minute. Episodes of benign paroxysmal positional vertigo can disappear for a while and then return. Activities that cause the signs and symptoms of BPPV may vary from person to person, but are nearly always brought on by a change in the placement of the head. Some people also feel out of balance when standing or walking. Abnormal rhythmic eye movements, known as nystagmus, usually follow the outward signs of benign paroxysmal positional vertigo, or BPPV.
It’s essential, however, to understand that BPPV will not give you continuous dizziness that is unaffected by motion or even a change in position. Also, it will not affect your hearing or produce fainting, headache or neurological signs, such as numbness, a sensation of “pins and needles,” difficulty speaking or difficulty coordinating your movements. If you have one or more of these additional symptoms, tell a healthcare professional immediately. Other disorders could be originally misdiagnosed as BPPV. By alerting a healthcare professional about any signs and symptoms you may be experiencing along with vertigo, they could reevaluate your illness and think about whether you might have another kind of disorder, instead of or in addition to BPPV.
BPPV is rather common, with an estimated prevalence of 107 per 100,000 annually plus a lifetime prevalence of 2.4 percent. It is thought to be quite rare in children but can affect adults of any age, particularly seniors. The wide majority of cases happen for no apparent reason, with many individuals describing how they simply went to get out of bed and the room began to spin. Nevertheless, associations have been made with injury, migraine headaches, inner ear infection or disease, diabetes, osteoporosis, intubation, presumably due to protracted time lying in bed, and reduced blood flow. There might also be a correlation with a person’s favorite sleeping side.
Diagnosis for BPPV
General practitioners normally refer patients to a healthcare professional specifically trained to take care of vestibular disorders, most commonly a vestibular rehabilitation therapist, such as a chiropractor, a specially trained physical therapist, or sometimes an occupational therapist or audiologist. An ENT (ear, nose & throat specialist) who specializes on vestibular disorders can also diagnose BPPV.
Normal medical imaging (e.g. an MRI) isn’t effective in diagnosing BPPV, because it doesn’t show the crystals that have moved to the semi-circular canals. However, when someone with BPPV has their own head moved into a position that makes the dislodged crystals go within a canal, the error signals have been known to cause the eyes to move in a very specific pattern, known as “nystagmus”.
The association between the internal ears and the eye muscles are what generally permit us to remain focused on our environment while the head is moving. Since the dislodged crystals make the brain think a person is moving when they are not, it causes the eyes to move, making it seem like the room is spinning. The eye movement is the indication that something is happening automatically in order to move the fluid in the inner ear canals when it shouldn’t be.
The nystagmus will have different characteristics that allow a healthcare professional to recognize which ear the displaced crystals are inside, as well as which canal(s) they have moved into. Evaluations like the Dix-Hallpike test involves moving the head into specific orientations, allowing gravity to move the dislodged crystals and activate the vertigo while the healthcare professional watches for the recognizable eye movements, or nystagmus.
Dix-Hallpike Test for BPPV
Healthcare professionals, such as chiropractors specializing in vestibular diseases, typically utilize the Dix-Hallpike test, sometimes called the Dix-Hallpike maneuver, to test for benign paroxysmal positional vertigo, or BPPV. To execute the Dix-Hallpike test, your doctor will ask you to sit on the test table with your legs stretched out. He’ll turn your head 45 degrees to one side, which contrasts the right posterior semicircular canal with the sagittal plane of the body, then they are going to allow you to lie back quickly, while the eyes are open, so that your head hangs slightly over the edge of the desk.
This motion may cause the loose crystals to move inside your semicircular canals. The healthcare professional will ask if you are feeling symptoms of vertigo and observe your eyes to find out how they move. As soon as you’ve got a few minutes to recover, your doctor may do the test on the opposite side of your head.
The latency, length and direction of nystagmus, if present, along with the latency and duration of vertigo, if present, should be noted. If the test is negative, it will demonstrate that�benign paroxysmal positional vertigo is a less probable diagnosis and central nervous system involvement ought to be considered. There are two sorts of BPPV: One at which loose crystals can move freely in the fluid of the canal (canalithiasis), and, more infrequently, one where the crystals are believed to be ‘wrapped up’ on the bundle of nerves that feel the fluid motion, or cupulolithiasis.
With canalithiasis, it requires less than a moment for those crystals to stop moving after a particular change in head position has triggered a twist. Once the crystals quit shifting, the fluid motion settles and the nystagmus and vertigo cease. With cupulolithiasis, the crystals trapped on the package of sensory nerves will make the nystagmus and vertigo last longer, until the head is moved out of the offending position. It is necessary to make the proper diagnosis, since the treatment is different for every variant. BPPV can be treated using various treatment methods, one of the most common being the Epley Maneuver.
Dr. Alex Jimenez’s Insight
Chiropractic care is an alternative treatment option commonly utilized to help treat a variety of injuries and conditions associated with the proper alignment of the spine. Occasionally, a spinal misalignment, or subluxation, can develop into numerous health issues, causing a wide array of symptoms if left untreated for an extended period of time. However, many chiropractors can treat many other ailments not closely associated with the spine. In a clinical setting, chiropractic care has been used for the management of benign paroxysmal positional vertigo, or BPPV. Chiropractors will utilize the Dix-Hallpike test to diagnose a patient followed by the Epley maneuver to help treat patients with BPPV. Many patients have reported a reduction in symptoms.
The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Sciatica
Sciatica is medically referred to as a collection of symptoms, rather than a single injury and/or condition. Symptoms of sciatic nerve pain, or sciatica, can vary in frequency and intensity, however, it is most commonly described as a sudden, sharp (knife-like) or electrical pain that radiates from the low back down the buttocks, hips, thighs and legs into the foot. Other symptoms of sciatica may include, tingling or burning sensations, numbness and weakness along the length of the sciatic nerve. Sciatica most frequently affects individuals between the ages of 30 and 50 years. It may often develop as a result of the degeneration of the spine due to age, however, the compression and irritation of the sciatic nerve caused by a bulging or herniated disc, among other spinal health issues, may also cause sciatic nerve pain.
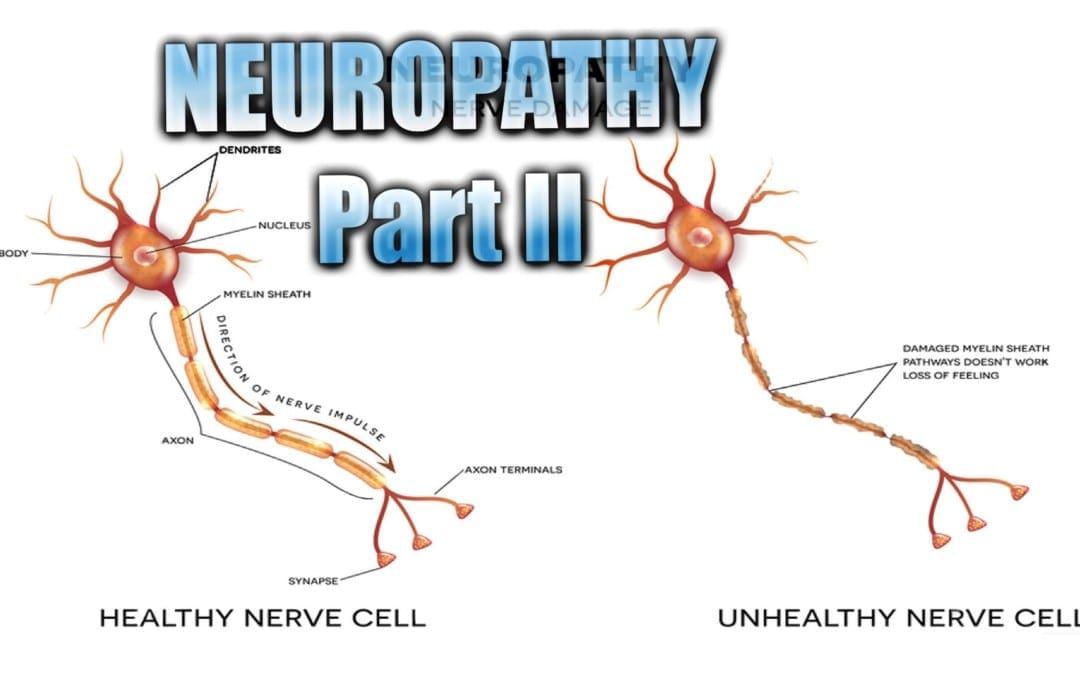
Neuropathy Presentation II:�El Paso, TX. Chiropractor, Dr. Alexander Jimenez�continues the overview with neuropathy part II. Continued are the most common neuropathies to be seen in practice. Because the human body is composed of many different kinds of nerves which perform different functions, nerve damage is classified into several types. Neuropathy can also be classified according to the location of the nerves being affected and according to the disease causing it. For instance, neuropathy caused by diabetes is called diabetic neuropathy. Furthermore, depending on which nerves are affected will depend on the symptoms that will manifest. The complications which follow neuropathy depends on the type of nerves that are damaged. According to Dr. Jimenez, different neuropathies can cause numbness and/or tingling sensations, increased pain or the loss of ability to feel pain, muscle weakness along with twitching and cramps, even dizziness and/or loss of bladder control function.
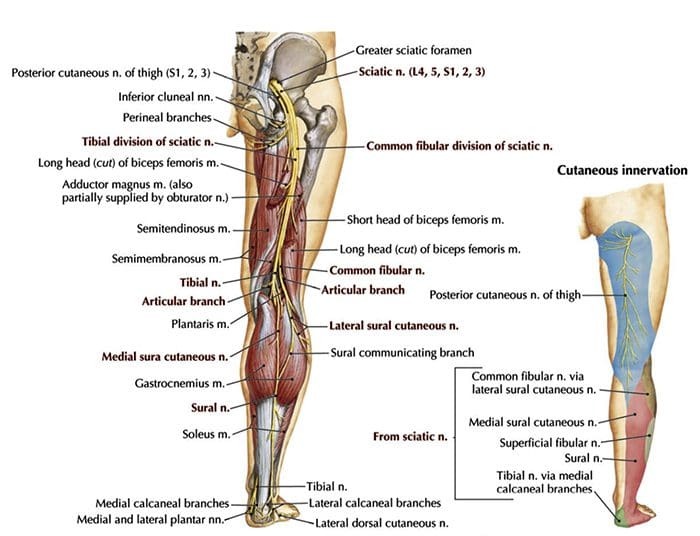
Sciatic Nerve Entrapment
Piriformis Syndrome
Peroneal Nerve Entrapment
Tarsal Tunnel Syndrome
Sciatic N. Piriformis Syndrome
Causes
Anatomic variation
Piriformis overuse/tension
Exam
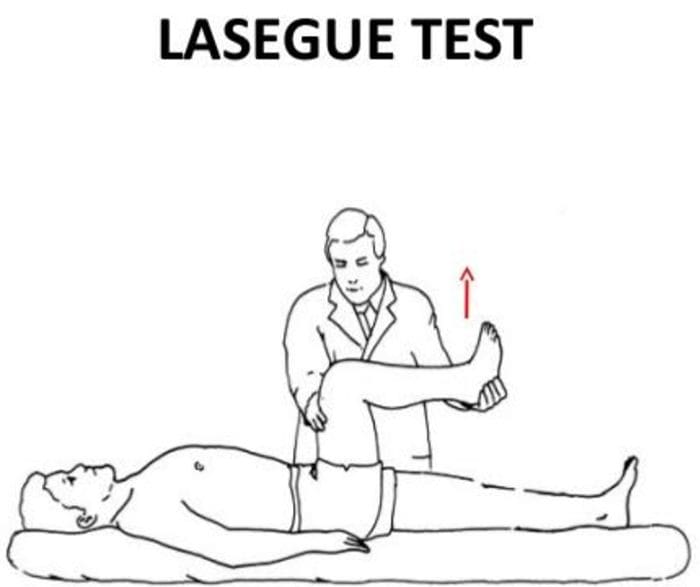
Positive Lase?gue test possible
Doctor extends patient�s leg passively, while patient is lying supine positive test if maneuver is limited by pain
Tenderness and palpable tension in piriformis muscle which elicits symptoms
Sciatic N. Peroneal Nerve Entrapment
Peroneal or Fibular branch of Sciatic nerve entrapped at the fibular head
Tinel�s sign may be present at fibular head/neck
Usually affects common peroneal nerve, therefore motor and sensory symptoms can be seen
Weakness of ankle dorsiflexion and eversion (tibialis anterior m.)
Sensory disruption on the dorsum of the foot and lateral aspect of the calf
Sciatic N. Tarsal Tunnel Syndrome
Tibial nerve impinged in the tarsal tunnel
Sensory changes in the sole of the foot
Tinel�s sign may be present with percussion posterior to the medial malleolus
Radiculopathy
A mononeuropathy � located in one specific area
Neuropathy involving spinal nerve roots
Presents as changes in sensory and/or motor function affecting a single or a few nerve root level(s)
Nerve sheath tumors (schwannomas and neurofibromas)
Guillain-Barre? syndrome
Herpes Zoster (shingles)
Lyme disease
Cytomegalovirus
Myxedema/Thyroid disorder
Idiopathic neuritis
Narrowing Down Common Causes Of Radiculopathy
Disc Herniation
Most commonly affected nerve roots are C6, C7, L5 & S1
Spinal Stenosis
Lumbar stenosis may produce neurogenic claudication
Pain & weakness with ambulation
Cervical stenosis may present with mixed picture of radiculopathy and myelopathy due to long tract involvement
Trauma
May cause compression, trauma or avulsion of the nerve roots
Diabetes
More likely to cause a polyneuropathy, but mononeuropathy is possible
Herpes Zoster (Shingles)
Most often on the trunk, accompanied by vesicular lesions in a single dermatome
If pain persits past vesicular regression = post-herpetic neuralgia
Patient History Of Radiculopathy
The patient will often complain of burning pain or tingling that radiates or shoots down an affected area in a dermatomal pattern.
Sometimes patient will complain of motor weakness, however if onset is recent, there is often no motor involvement
Exam Of Radiculopathy
Most often hypoesthesia in the affected dermatome level
Best to evaluate for pain, as light touch can be difficult for these patient�s to distinguish
Fasciculations and/or atrophy may be seen if radiculopathy is chronic, due to lower motor neuron being impinged
Motor weakness may be seen in muscles innervated by the same root level
Orthopedic tests:
Straight-leg raise test (SLR)
Pain between 10-60 degrees likely indicates nerve root compression
Well-leg raise/Crossed straight-leg raise test (WLR)
If positive, 90% specificity for L/S nerve root compression
Valsalva Maneuver
Positive if increase in radicular symptoms
Spinal Percussion
Pain may indicate metastatic disease, abscess or osteomyelitis
Examinations: Merck Manual Professional
How To Test Reflexes
How To Do A Sensory Exam
How To Do A Motor Examination
Dermatomes
Testing Cervical Nerve Roots
Testing Lumbosacral Nerve Roots
Specific Radiculopathy Patterns
T1 radiculopathy can cause Horner�s syndrome
This is due to affect on cervical sympathetic ganglia
Ptosis, miosis, anhidrosis
Below L1, radiculopathies can cause Cauda Equina syndrome
Saddle anesthesia (sensory loss in S2-S5 distribution)
Urinary retention or overflow incontinence
Constipation, decreased rectal tone or fecal incontinence
Loss of erectile function
Must be referred for emergency care immediately to prevent permanent dysfunction
Other Patterns Of Neuropathy
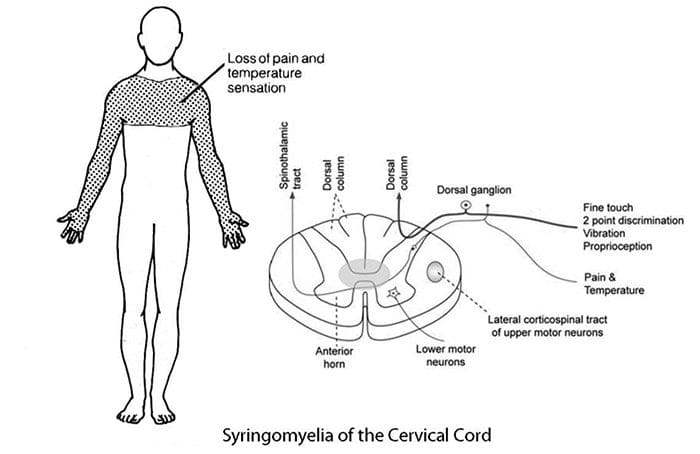
Cape/Shawl distribution of symptoms
Intramedullary lesion
Syringomyelia
Intramedullary tumor
Central cord damage
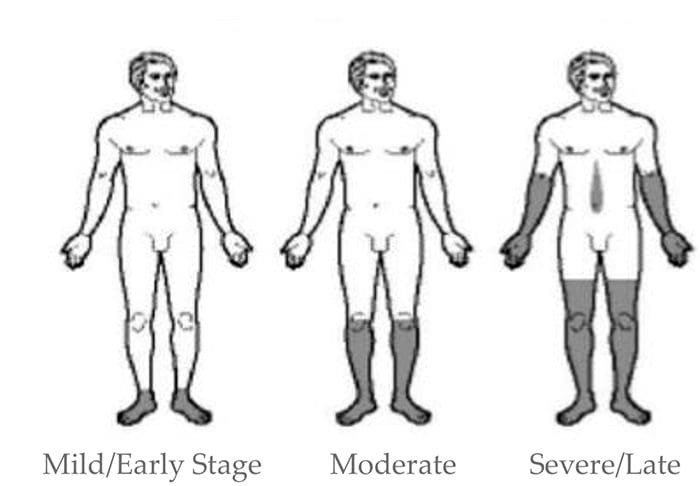
Stocking and Glove Distribution of Symptoms
Diabetes mellitus
B12 deficiency
Alcoholism/hepatitis
HIV
Thyroid dysfunction/myxedema
Cape/Shawl Pattern
Intramedullary lesion such as tumor, syringomyelia or hyperextension injury in patient with C/S spondylosis
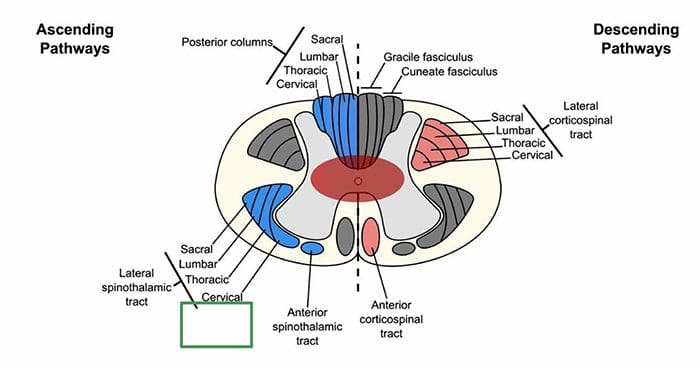
Loss of pain and temp sensation in C/T dermatomes because of arrangement of lateral spinothalamic tract
Stocking & Glove Pattern
Symmetrical polyneuropathy
Feet/legs usually affected first, followed by hands/arms
Vibration sensation in the smallest toes is usually the first thing lost and neuropathy progresses across foot to great toe and then upward through the ankle and leg, then hands, arms and finally trunk if sever
Most likely cause of this distribution is diabetes mellitus, but other possible causes include B12 deficiency, alcoholism, HIV, chemotherapy treatment, thyroid dysfunction and multiple other causes
Diabetic Neuropathy
Diabetic neuropathy often presents as a polyneuropathy but can also present as a mononeuropathy, usually with acute onset
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine
 CN I Clinically
CN I Clinically Cranial Nerve II Clinically
Cranial Nerve II Clinically
 Cranial Nerve III Clinically
Cranial Nerve III Clinically Testing Cranial Nerve CN II & III
Testing Cranial Nerve CN II & III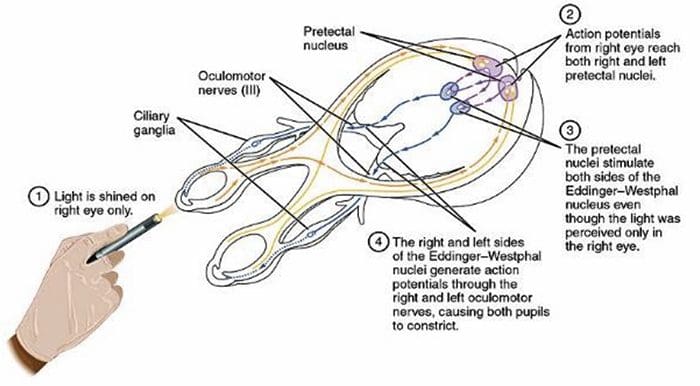
 Cranial Nerve IV Clinically
Cranial Nerve IV Clinically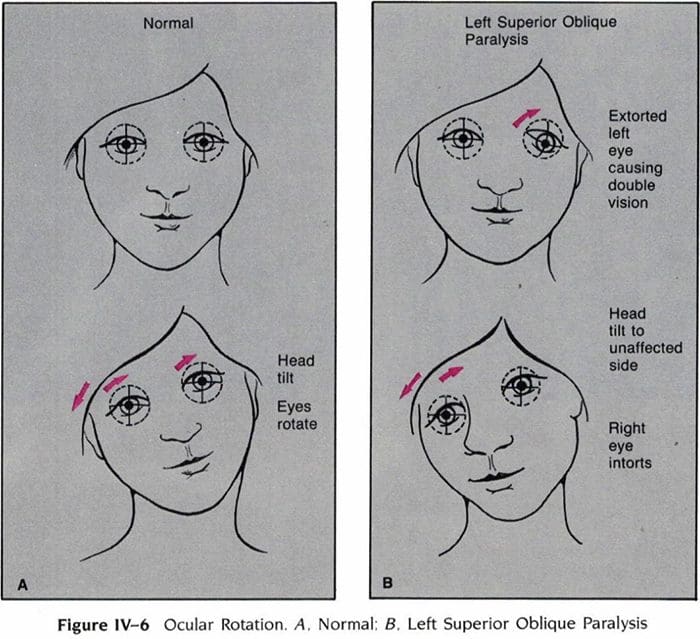
 Cranial Nerve VI Clinically
Cranial Nerve VI Clinically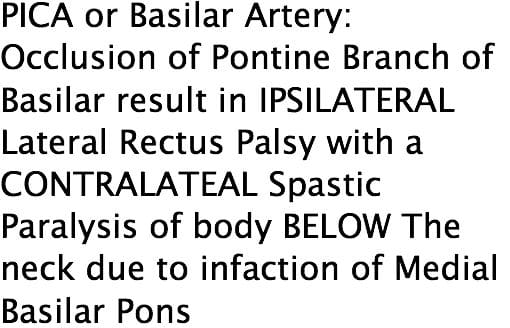
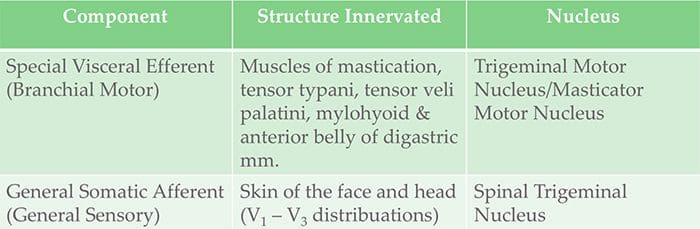 Cranial Nerve V Clinically
Cranial Nerve V Clinically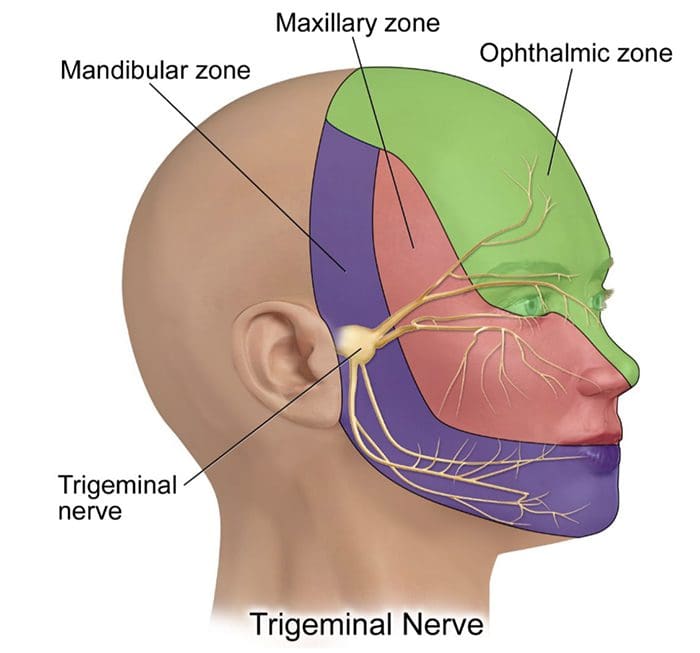
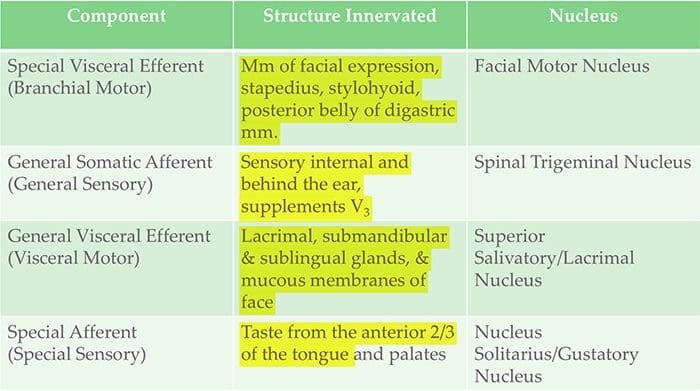 Cranial Nerve VII Clinically
Cranial Nerve VII Clinically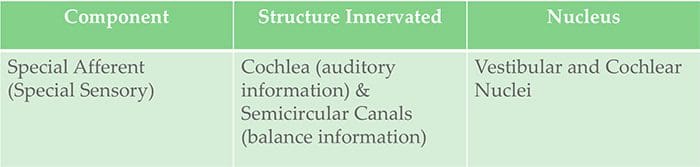 Cranial Nerve VIII Clinically
Cranial Nerve VIII Clinically
 Cranial Nerve IX Clinically
Cranial Nerve IX Clinically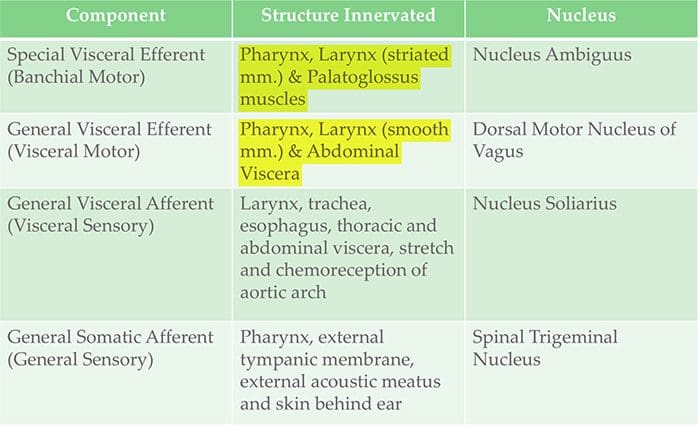 Cranial Nerve X Clinically
Cranial Nerve X Clinically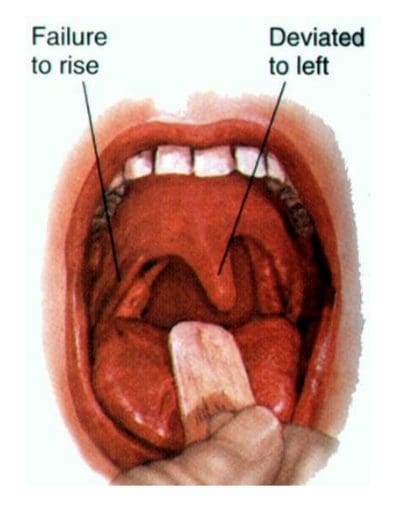
 Cranial Nerve XI Clinically
Cranial Nerve XI Clinically Cranial Nerve XII Clinically
Cranial Nerve XII Clinically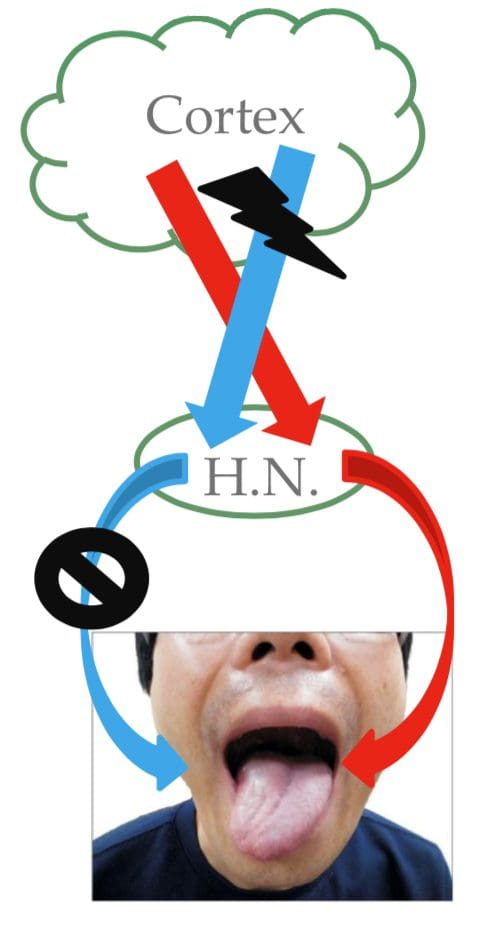








 Causes
Causes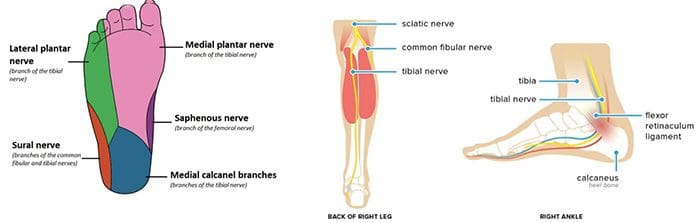 Radiculopathy
Radiculopathy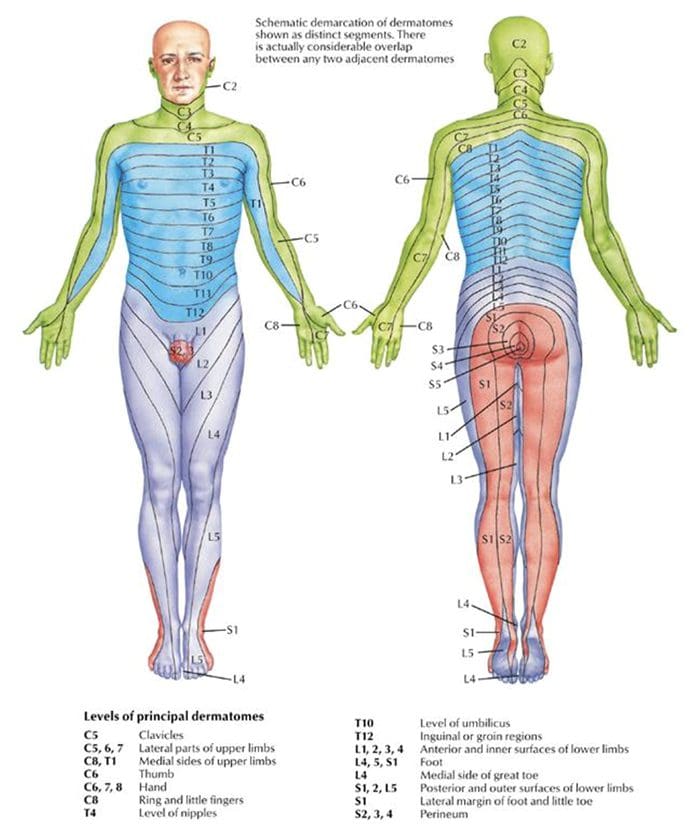 Testing Cervical Nerve Roots
Testing Cervical Nerve Roots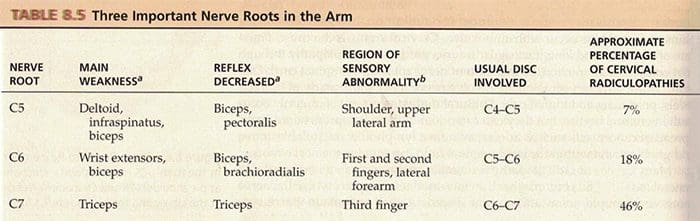 Testing Lumbosacral Nerve Roots
Testing Lumbosacral Nerve Roots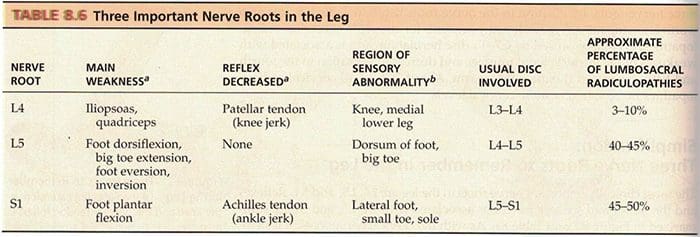
 Stocking & Glove Pattern
Stocking & Glove Pattern