Headaches are very common health issues, and lots of people treat themselves by using basic painkillers, drinking additional water, with rest, or by simply waiting for the headache to go away on its own. As a matter of fact, a headache is among the most common reasons for doctor office visits.
Just about everyone will experience a headache sometime during their life. Most headaches are not caused by serious or sinister conditions. However, people understandably worry if headaches feel different, whether they’re especially severe, particularly frequent or unusual in any other manner. But, the most common concern is whether the headache may be a symptom of an underlying health issue, such as a brain tumor.
The following article discusses headaches generally. It explains the various types of headaches you may experience and describes those very rare situations where a headache may be a symptom of a serious disease.
Types of Headaches
Headaches can be categorized as primary, or they can be classified as secondary, meaning they are a side-effect of another injury or condition.
A healthcare professional can usually determine the possible cause of your headaches from speaking to you and examining you. When they have found the cause then you’ll have the ability to decide the best treatment approach for your head pain symptoms. This may involve taking drugs only when you get the headaches, taking daily medication to stop them altogether, and/or even stopping medication you’re already taking. Very occasionally, headaches may need further diagnosis to rule out more serious underlying causes. Chiropractic care and physical therapy are also commonly utilized to help treat headaches. Below, we will discuss the different types of headaches.
Primary Headaches
The most common types of headaches, by far, are tension headaches and migraines.
Tension Headaches
Tension headaches are generally felt as a band around the forehead. They may last for many days. They may be tiring and uncomfortable, but they don’t normally disturb sleep. Most people can carry on working with a tension headache. These often have a tendency to worsen as the day progresses, however, they aren’t usually made worse with physical activities, though it’s not strange to be somewhat sensitive to bright light or noise.
Migraines
Migraines are also very common types of headaches. A typical migraine is described as a throbbing sensation. Headaches which are one-sided, headaches which throb and headaches that make you feel sick are more inclined to be migraines compared to anything else. Migraines are often severe enough to be disabling. Some individuals will need to go to bed to sleep off their aggravation.
Cluster Headaches
Cluster headaches are extremely severe headaches, sometimes called “suicide headaches”. They occur in clusters, often every day for a number of days or maybe weeks. Then they vanish for weeks on end. These types of headaches are rare and often occur particularly in adult male smokers. They’re intense, one-sided headaches, which are very disabling, meaning they stop routine activity. People often describe them as the worst pain they have ever felt. Cluster headaches are typically one-sided. Patients frequently have a red watery eye on the other hand, a stuffy runny nose and a droopy eyelid.
Chronic Tension Headaches
Chronic tension headaches (or chronic daily headache) is generally caused by muscle tension in the back of the neck and affects women more frequently than men. Chronic means that the problem is persistent and ongoing. These headaches can develop due to neck injuries or tiredness and may worsen with drug/medication overuse. A headache that occurs virtually every day for 3 weeks or more is known as a chronic daily headache or a chronic tension headaches.
Medication-Overuse Headaches
Medication-overuse headaches or medication-induced aggravation, is an unpleasant and long-term headache. It’s brought on by taking painkillers usually meant for headaches. Unfortunately, when painkillers are taken regularly for headaches, the body reacts by creating additional pain sensors in the brain. Finally, the pain sensors are so many that the head becomes super-sensitive and the headache won’t go away. Individuals who have these headaches often take an increasing number of painkillers to attempt and feel much better. But, the painkillers may have regularly long ceased to work. Medication-overuse headaches are the most common cause of secondary headache.
Exertional Headaches/Sexual Headaches
Exertional headaches are headaches associated with physical activity. They may get severe very quickly following a strenuous activity like coughing, running, with intercourse, and straining with bowel movements. They’re more commonly experienced by patients that also have migraines, or who have relatives with migraine.
Headaches associated with sex particularly worry patients. They can occur as sex starts, at orgasm, or following sex. Headaches at orgasm would be the most common type. They are generally acute, at the back of the head, behind the eyes or all around. They last about twenty minutes and aren’t usually an indication of any other underlying health issues or problems.
Exertional and sexual intercourse-related headaches aren’t typically an indication of serious underlying problems. Very occasionally, they can be a sign that there is a leaky blood vessel on the surface of the brain. As a result, if they are marked and repeated, it’s sensible to talk about them with your healthcare professional.
Primary Stabbing Headaches
Primary traumatic headaches are sometimes called “ice-pick headaches” or “idiopathic stabbing headache”. The term “idiopathic” is used by doctors for something that comes without a clear cause. These are brief, stabbing headaches that are extremely sudden and severe. They generally last between 5 and 30 seconds and they occur at any time of the day or night. They feel as though a sharp object, like an ice pick, is being stuck into your head. They frequently occur in or just behind the ear and they are sometimes quite frightening. Even though they aren’t migraines they’re more prevalent in those who suffer from migraines, nearly half of individuals who experience migraines have principal stabbing headaches.
They are often felt at the place on the head where the migraines have a tendency to happen. Primary stabbing headaches are too brief to take care of, even though migraine prevention medications may reduce their number.
Hemicrania Continua
Hemicrania continua is a major chronic daily headache. It typically induces a continuous but shifting pain on one side of the brain. The pain is generally continuous with episodes of severe pain, which can last between 20 minutes and several days. During those episodes of severe pain there may be other symptoms, such as watering or redness of the eye, runny or blocked nose, and drooping of the eyelid, around precisely the same side as the aggravation. Similar to a migraine, there may also be sensitivity to light, feeling sick, such as nausea, and being sick, such as vomiting. The headaches do not go away but there may be periods when you don’t have any headaches. Hemicrania continua headaches respond to medicine called indometacin.
Trigeminal Neuralgia
Trigeminal neuralgia causes facial pain. The pain consists of very short bursts of electric shock-like sensations in the face, particularly at the area of the eyes, nose, scalp, brow, lips or limbs. It’s usually one-sided and is more common in people over age 50. It may be triggered by touch or a light breeze on the surface area.
Headache Causes
Occasionally, headaches have underlying causes, and treatment of the headache involves treating the cause. Individuals often fear that headaches are caused by serious illness, or by high blood pressure. Both of these are extremely uncommon causes of headache, really increased blood pressure usually causes no symptoms in any way.
Chemicals, Drugs and Substance Withdrawal
Headaches can be because of a substance, or its withdrawal, for example:
Carbon monoxide, that is made by gas heaters which aren’t properly ventilated
Drinking alcohol, with headache often experienced the morning afterwards
Deficiency of body fluid or dehydration
Headaches Due to Referred Pain
Some headaches may be caused by pain in some other portion of the head, such as ear or tooth pain, pain in the jaw joint and pain in the neck.
Sinusitis is also a frequent cause of headaches. The sinuses are “holes” in the skull which are there to stop it from becoming too heavy for the neck to transport around. They are lined with mucous membranes, such as the lining of the nose, and this creates mucus in response to colds or allergy. The liner membranes also swell and can block the drainage of the mucus out of the space. It subsequently becomes cracked and infected, resulting in headache. The headache of sinusitis is often felt at the front of the head and also in the face or teeth.
Frequently the face feels tender to tension, particularly just below the eyes beside the nose. You might have a stuffy nose and the pain is often worse when you bend forwards. Acute sinusitis is the kind that comes on fast in conjunction with a cold or abrupt allergy. You may have a temperature and be generating a lot of mucus. Chronic sinusitis may be caused by allergy, by overusing decongestants or with the acute sinusitis that doesn’t settle. The sinuses become chronically infected and the nasal linings chronically swollen. The contents of this uterus may be thick but frequently not infected.
Acute glaucoma can cause severe headaches. In this condition, the pressure inside the eyes goes up suddenly and this causes a surprisingly, very severe headache behind the eye. Even the eyeball can feel really hard to touch, the eye is red, the front part of the eye, or cornea, can seem cloudy and the eyesight is generally blurred.
What Types of Headaches are Dangerous or Serious?
All headaches are unpleasant and some, such as headache from medication abuse, are serious in the sense that if not treated correctly they might never go away. But a few headaches are indications of serious underlying issues. These are uncommon, in many cases very rare. Dangerous headaches often occur suddenly, and also eventually become increasingly worse over time. They are more common in elderly people. They comprise of the following:
Bleeding Around the Brain (Subarachnoid Haemorrhage)
Subarachnoid haemorrhage is a really serious condition which occurs when a tiny blood vessel pops on the surface of the brain. Patients develop a serious headache and stiff neck and may become unconscious. This is a rare cause of acute headache.
Meningitis and Brain Infections
Meningitis is infection of the tissues around and on the surface of the brain and encephalitis is infection of the brain itself. Brain infections can be caused by germs called bacteria, viruses or parasites and they are thankfully rare. They cause a severe, disabling headache. Normally, patients may feel sick or vomit and can’t bear bright lights, something known as photophobia. Often they have a rigid neck, too stiff for your physician to have the ability to bend the head down so that the chin touches the chest, even in the event that you attempt to relax. Patients are generally also unwell, experiencing hot, sweaty and overall sick sensations.
Giant Cell Arteritis (Temporal Arteritis)
Giant cell arteritis (temporal arteritis) is, generally, just seen in people over the age of 50. It is due to swelling, or inflammation, of the arteries at the temples and behind the eye. It causes a headache behind the forehead, also referred to as a sinus headache. Typically the blood vessels at the forehead are tender and individuals detect pain from the scalp when they comb their own hair. Frequently the pain gets worse with chewing. Temporal arteritis is severe because if it’s not treated it can cause sudden loss of eyesight. Treatment is with a course of steroids. The need to keep these steroids is generally monitored by the GP through blood tests, and they are typically needed for several months.
Brain Tumors
Brain tumors are a very uncommon cause of headache, although most patients with long-term, severe or persistent headaches start to worry that this might be the reason. Brain tumors can lead to headaches. Usually the aggravation of brain tumors exists on waking in the morning, is worse on sitting up, and becoming steadily worse in the day to day, never easing and never disappearing. It can sometimes be worse on coughing and sneezing, as may sinus headaches and migraines.
When Should I Worry About a Headache?
Most headaches do not have a serious underlying cause. However, healthcare professionals are trained to ask you about the signs and symptoms that might suggest your headache needs further diagnosis, just to make certain it’s nothing serious.
The things which would suggest to your physician and nurse that your headache may need additional evaluation include the following. They don’t mean that your headache is severe or sinister, but they imply that the healthcare professional may wish to do some additional evaluations to make sure if:
You have had a substantial head injury in the previous three months.
Your headaches are worsening and accompanied with high temperature or fever.
Your headaches begin extremely unexpectedly.
You’ve developed problems with speech and balance as well as headache.
You’ve developed problems with your memory or changes in your behavior or personality in addition to headache.
You’re confused or muddled along with your headache.
Your headache started when you coughed, sneezed or strained.
Your headache is much worse when you sit or stand.
Your headache is associated with red or painful eyes.
Your headaches are not like anything you’ve ever experienced before.
You have unexplained nausea together with the aggravation.
You have low immunity, for instance, when you have HIV, or are about oral steroid medicine or immune suppressing drugs.
You have or have had a type of cancer that can spread throughout the body.
Dr. Alex Jimenez’s Insight
Headaches are extremely common health issues which affect a wide range of the population around the world. Although frequent, a headache which is described to be like no other ever experienced before, may often become a concern. There are several types of headaches which can be caused by a variety of injuries and/or underlying conditions. As a healthcare professional, it’s essential to be able to determine between sinister or dangerous types of headaches and benign types of headaches, in order to decide the best treatment approach. By properly diagnosing the source of a patient’s headaches, both benign and sinister types of headaches can be treated accordingly.
Overview
Many headaches, whilst unpleasant, are harmless and react to a variety of treatments, including chiropractic care. Migraine, tension headaches and medication-overuse headaches are very common. The majority of the populace will experience one or more of these. Working out exactly the underlying cause of any headaches through discussion with your doctor is often the best method to resolve them. It is possible to develop a persistent or chronic and constant headache through taking drugs and/or medications that you took to get rid of your headache. Your physician can support you through the practice of quitting painkillers when that is the case.
Headaches are, quite infrequently, an indication of a serious or sinister underlying illness, and many headaches go away on their own.
If you have a headache which is uncommon for you then you need to discuss it with your doctor. You should also speak to your doctor about headaches which are particularly severe or that affect your regular activities, those that are associated with other symptoms, such as tingling or weakness, and those which make your own scalp tender, especially if you’re over 50 years old. Finally, always speak to a healthcare professional when you have an unremitting morning headache which is present for at least three days or is becoming gradually worse.
Remember that headaches are not as likely to occur in people who:
Handle their anxiety levels well.
Eat a balanced, regular diet.
Take balanced routine exercise.
Focus on posture and core muscles.
Sleep on two pillows or fewer.
Drink loads of water.
Have plenty of sleep.
Anything that you can do to enhance one or more of these aspects of your life will improve your health and well-being and cut back the number of headaches you experience. Make sure to seek the appropriate medical attention from a qualified and experienced healthcare professional in the event of a severe headache unlike anything you’ve ever experienced before. The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Back Pain
Back pain is one of the most prevalent causes for disability and missed days at work worldwide. As a matter of fact, back pain has been attributed as the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience some type of back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
Robert “Bobby” Gomez was born with cerebral palsy. Bobby describes how he felt like an outcast, growing up with the disorder, but he explains how much he can accomplish when he’s not underestimated. While Robert Gomez describes experiencing no setbacks due to his cerebral palsy, he suffered from pain and limited mobility. That’s when he decided to seek chiropractic care with Dr. Alex Jimenez and found much more help than he expected. Through spinal adjustments, manual manipulations, and rehabilitation exercises, Robert “Bobby” Gomez has regained some mobility and has experienced decreased pain symptoms. Bobby recommends Dr. Jimenez as the non-surgical choice for back pain and encourages others to educate themselves on cerebral palsy.
Chiropractic Treatment For Cerebral Palsy
Cerebral palsy is a permanent movement disorder that appears in early youth. Signs and symptoms vary among people. Symptoms often include poor coordination, stiff muscles, weakness, and tremors. There may be problems with feeling, vision, hearing, swallowing, and talking. Usually, infants with cerebral palsy don’t roll over, sit, walk or crawl as early as other kids of their age. Other symptoms may include seizures and problems with reasoning or thinking, which happen in about one-third of individuals with cerebral palsy. While the symptoms may get more noticeable over the first few years of life, the underlying problems don’t worsen. Cerebral palsy is caused by abnormal development or damage to the areas of the brain that control movement, balance, and posture. Most often, the problems occur during pregnancy; however, they may also happen during childbirth or soon after birth.
We are blessed to present El Paso s Premier Wellness & Injury Care Clinic to you.
At El Paso’s Chiropractic Rehabilitation Clinic & Integrated Medicine Center, we are passionately focused on treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility, and agility programs tailored for all age groups and disabilities.
Please feel free to subscribe and share if you have enjoyed this video and we have helped you.
The rule of 4 of the brainstem: a simplified method for understanding brainstem anatomy and brainstem vascular
syndromes for the non-neurologist.
The Rule Of 4 & The Brainstem
The rule of 4 is a simple method developed to help �students of neurology� to remember the anatomy of the brainstem and thus the features of the various brainstem vascular syndromes. As medical students, we are taught detailed anatomy of the brainstem containing a bewildering number of structures with curious names such as superior colliculi, inferior olives, various cranial nerve nuclei and the median longitudinal fasciculus. In reality when we do a neurological examination we test for only a few of these structures. The rule of 4 recognizes this and only describes the parts of the brainstem that we actually examine when doing a neurological examination. The blood supply of the brainstem is such that there are paramedian branches and long circumferential branches (the anterior inferior cerebellar artery (AICA), the posterior inferior cerebellar artery (PICA) and the superior cerebellar artery (SCA). Occlusion of the paramedian branches results in medial (or paramedian) brainstem syndromes and occlusion of the circumferential branches results in lateral brainstem syndromes. Occasionally lateral brainstem syndromes are seen in unilateral vertebral occlusion. This paper describes a simple technique to aid in the understanding of brainstem vascular syndromes.
Any attempt to over simplify things runs the risk of upsetting those who like detail and I apologize in advance to the anatomists among us, but for more than 15 years this simple concept has helped numerous students and residents understand, often for the first time, brainstem anatomy and the associated clinical syndromes that result.
In The Rule Of 4 There Are 4 Rules:
There are 4 structures in the �midline� beginning with M.
There are 4 structures to the side beginning with S.
There are 4 cranial nerves in the medulla, 4 in the pons and 4 above the pons (2 in the midbrain).
The 4 motor nuclei that are in the midline are those that divide equally into 12 except for 1 and 2, that is 3, 4, 6 and 12 (5, 7, 9 and 11 are in the lateral brainstem).
If you can remember these rules and know how to examine the nervous system, in particular the cranial nerves, then you will be able to diagnose brainstem vascular syndromes with ease.
Figure 1 shows a cross-section of the brainstem, in this case at the level of the medulla, but the concept of 4 lateral and 4 medial structures also applies to the pons, only the 4 medial structures relate to midbrain vascular syndromes.
The 4 Medial Structures & The Associated Deficit Are:
The Motor pathway (or corticospinal tract): contra lateral weakness of the arm and leg.
The Medial Lemniscus: contra lateral loss of vibration and proprioception in the arm and leg.
The Medial longitudinal fasciculus: ipsilateral inter- nuclear ophthalmoplegia (failure of adduction of the ipsilateral eye towards the nose and nystagmus in the opposite eye as it looks laterally).
The Motor nucleus and nerve: ipsilateral loss of the cranial nerve that is affected (3, 4, 6 or 12).
The 4 Lateral Structures & The Associated Deficit Are:
The Spinocerebellar pathways: ipsilateral ataxia of the arm and leg.
The Spinothalamic pathway: contra lateral alteration of pain and temperature affecting the arm, leg and rarely the trunk.
The Sensory nucleus of the 5th: ipsilateral alteration of pain and temperature on the face in the distribution of the 5th cranial nerve (this nucleus is a long vertical structure that extends in the lateral aspect of the pons down into the medulla).
The Sympathetic pathway: ipsilateral Horner�s syndrome, that is partial ptosis and a small pupil (miosis)
These pathways pass through the entire length of the brainstem and can be likened to �meridians of longitude� whereas the various cranial nerves can be regarded as �parallels of latitude�. If you establish where the meridians of longitude and parallels of latitude intersect then you have established the site of the lesion.
Figure 2 shows the ventral aspect of the brainstem.
The 4 Cranial Nerves In The Medulla Are:
9 Glossopharyngeal: ipsilateral loss of pharyngeal sensation. 10 Vagus: ipsilateral palatal weakness. 11 Spinal accessory: ipsilateral weakness of the trapezius and sternocleidomastoid muscles. 12 Hypoglossal: ipsilateral weakness of the tongue.
The 12th cranial nerve is the motor nerve in the midline of the medulla. Although the 9th, 10th and 11th cranial nerves have motor components, they do not divide evenly into 12 (using our rule) and are thus not the medial motor nerves.
The 4 Cranial Nerves In The Pons Are:
5 Trigeminal: ipsilateral alteration of pain, temperature and light touch on the face back as far as the anterior two-thirds of the scalp and sparing the angle of the jaw. 6 Abducent: ipsilateral weakness of abduction (lateral movement) of the eye. 7 Facial: ipsilateral facial weakness. 8 Auditory: ipsilateral deafness.
The 6th cranial nerve is the motor nerve in the pons.
The 7th is a motor nerve but it also carries pathways of taste, and using the rule of 4 it does not divide equally in to 12 and thus it is not a motor nerve that is in the midline. The vestibular portion of the 8th nerve is not included in order to keep the concept simple and to avoid confusion. Nausea and vomiting and vertigo are often more common with involvement of the vestibular connections in the lateral medulla.
The 4 Cranial Nerves Above The Pons Are:
4 Olfactory: not in midbrain. 5 Optic: not in midbrain. 6 Oculomotor: impaired adduction, supraduction and infraduction of the ipsilateral eye with or without a dilated pupil. The eye is turned out and slightly down. 7 Trochlear: eye unable to look down when the eye is looking in towards the nose.
The 3rd and 4th cranial nerves are the motor nerves in the midbrain.
Thus a medial brainstem syndrome will consist of the 4 M�s and the relevant motor cranial nerve, and a lateral brainstem syndrome will consist of the 4 S�sand either the 9�11th cranial nerve if in the medulla, or the 5th, 7th and 8th cranial nerve if in the pons.
MEDIAL (PARAMEDIAN) BRAINSTEM SYNDROMES
Let us assume that the patient you are examining has a brainstem stroke. If you find upper motor neurone signs in the arm and the leg on one side then you know the patient has a medial brainstem syndrome because the motor pathways is paramedian and crosses at the level of the foramen magnum (decussation of the pyramids). The involvement of the motor pathway is the �meridian of longitude�. So far the lesion could be anywhere in the medial aspect of the brainstem, although if the face is also affected it has to be above the mid pons, the level where the 7th nerve nucleus is.
The motor cranial nerve �the parallels of latitude� indicates whether the lesion is in the medulla (12th), pons (6th) or midbrain (3rd). Remember the cranial nerve palsy will be ipsilateral to the side of the lesion and the hemiparesis will be contralateral. If the medial lemniscus is also affected then you will find a contra lateral loss of vibration and proprioception in the arm and leg (the same side affected by the hemiparesis) as the posterior columns also cross at or just above the level of the foramen magnum. The median longitudinal fasciculus (MLF) is usually not affected when there is a hemiparesis as the MLF is further back in the brainstem.
The MLF can be affected in isolation �a lacunar infarct� and this results in an ipsilateral internuclear ophthalmoplegia, with failure of adduction (movement towards the nose) of the ipsilateral eye and leading eye nystagmus on looking laterally to the opposite side of the lesion in the contra lateral eye. If the patient had involvement of the left MLF then, on being asked to look to the left, the eye movements would be normal, but on looking to the right the left eye would not go past the midline, while there would be nystagmus in the right eye as it looked to the right.
Figure 3 shows the clinical features of the medial brainstem syndromes.
LATERAL BRAINSTEM SYNDROMES
Once again we are assuming that the patient you are seeing has a brainstem problem, most likely a vascular lesion. The 4 S�s or �meridians of longitude� will indicate that you are dealing with a lateral brainstem problem and the cranial nerves or �parallels of latitude� will indicate whether the problem is in the lateral medulla or lateral pons.
A lateral brainstem infarct will result in ipsilateral ataxia of the arm and leg as a result of involvement of the Spinocerebellar pathways, contralateral alteration of pain and temperature sensation as a result of involvement of the Spinothalamic pathway, ipsilateral loss of pain and temperature sensation affecting the face within the distribution of the Sensory nucleus of the trigeminal nerve (light touch may also be affected with involvement of the spinothalamic pathway and/or sensory nucleus of the trigeminal nerve). An ipsilateral Horner�s syndrome with partial ptosis and a small pupil (miosis) is because of involvement of the Sympathetic pathway. The power tone and the reflexes should all be normal. So far all we have done is localize the problem to the lateral aspect of the brainstem; by adding the relevant 3 cranial nerves in the medulla or the pons we can localize the lesion to this region of the brain.
The lower 4 cranial nerves are in the medulla and the 12th nerve is in the midline so that 9th, 10th and 11th nerves will be in the lateral aspect of the medulla. When these are affected, the result is dysarthria and dysphagia with an ipsilateral impairment of the gag reflex and the palate will pull up to the opposite side; occasionally there may be weakness of the ipsilateral trapezius and/or sternocleidomastoid muscle. This is the lateral medullary syndrome usually resulting from occlusion of the ipsilateral vertebral or posterior inferior cerebellar arteries.
The 4 cranial nerves in the pons are: 5th, 6th, 7th and 8th. The 6th nerve is the motor nerve in the midline, the 5th, 7th and 8th are in the lateral aspect of the pons, and when these are affected there will be ipsilateral facial weakness, weakness of the ipsilateral masseter and pterygoid muscles (muscles that open and close the mouth) and occasionally ipsilateral deafness. A tumour such as an acoustic neuroma in the cerebello-pontine angle will result in ipsilateral deafness, facial weakness and impairment of facial sensation; there may also be ipsilateral limb ataxia if it compresses the ipsilateral cerebellum or brainstem. The sympathetic pathway is usually too deep to be affected.
If there are signs of both a lateral and a medial (paramedian) brainstem syndrome, then one needs to consider a basilar artery problem, possibly an occlusion.
In summary, if one can remember that there are 4 pathways in the midline commencing with the letter M, 4 pathways in the lateral aspect of the brainstem commencing with the letter S, the lower 4 cranial nerves are in the medulla, the middle 4 cranial nerves in the pons and the first 4 cranial nerves above the pons with the 3rd and 4th in the midbrain, and that the 4 motor nerves that are in the midline are the 4 that divide evenly into 12 except for 1 and 2, that is 3, 4, 6 and 12, then it will be possible to diagnose brainstem vascular syndromes with pinpoint accuracy.
P. GATES
The Geelong Hospital, Barwon Health, Geelong, Victoria, Australia
Physicians, neurologists, and other healthcare professionals may often run a cranial nerve examination as part of a neurological evaluation to analyze the operation of the cranial nerves. This involves a highly formalized series of tests that evaluate the status of each cranial nerve. A cranial nerve test begins with observation of the patient partly due to the fact that cranial nerve lesions may ultimately affect the symmetry of the face or eyes, among other signs and symptoms.
The visual fields for neural lesions or nystagmus�are tested via an evaluation of particular eye movements. The sensation of the face is tested by asking patients to execute different facial movements, like puffing out their cheeks. Hearing is tested through voice and tuning forks. The position of the individual’s uvula is also examined because asymmetry in its placement could indicate a lesion of the glossopharyngeal nerve. After the capability of the individual to use their shoulder to test the accessory nerve (XI), the patient’s tongue operation is generally assessed by detecting various tongue movements.
Damage or Injury of the Cranial Nerves
Compression
Cranial nerves may be compressed due to increased intracranial pressure, a profound effect of an intracerebral haemorrhage, or tumour which presses against the cranial nerves and interferes with the communication of impulses along the length of a nerve. In some instances, a loss of functionality of one cranial nerve may on occasion be the first symptom of an intracranial or skull base cancer.
An increase in intracranial pressure can lead to dysfunction of the optic nerves (II) because of the compression of the surrounding veins and capillaries, resulting in swelling of the eyeball, known as papilloedema. A cancer, such as an optic glioma, can also affect the optic nerve (II). A pituitary tumour can compress the optic tracts or the optic chiasm of the optic nerve (II), causing visual field loss. A pituitary tumour may also extend into the cavernous sinus, compressing the oculuomotor nerve (III), the trochlear nerve (IV) and the abducens nerve (VI), often leading to double-vision and strabismus. These cranial nerves may also be impacted by herniation of the temporal lobes of the brain via the falx cerebri.
The cause of trigeminal neuralgia, where one side of the face experiences painful signs and symptoms, is believed to be due to the compression of a cranial nerve by an artery as the nerve exits from the brain stem. An acoustic neuroma, especially at the junction between the pons and medulla, may compress the facial nerve (VII) and the vestibulocochlear nerve (VIII), resulting in hearing and sensory loss on the affected side.
Stroke
Occlusion of blood vessels which supply the cranial nerves or their nuclei, or an ischemic stroke, might cause specific signs and symptoms which could localize where the occlusion happened. A clot in a blood vessel draining the cavernous sinus, also known as the cavernous sinus thrombosis, may affect the oculomotor (III), the trochlear (IV), and the opthalamic branch of the trigeminal nerve (V1) and the abducens nerve (VI).
Inflammation
Inflammation caused by an infection may impair the operation of any of the cranial nerves. Infection of the facial nerve (VII), for instance, can result in Bell’s palsy. Multiple sclerosis, an inflammatory process which can produce a loss of the myelin sheathes that encircle the cranial nerves, may cause a variety of shifting signs and symptoms which can ultimately affect multiple cranial nerves.
Other
Trauma to the skull, bone disease like Paget’s disease, and damage or injury to the cranial nerves through neurosurgery, by way of instance, through tumor removal, are other potential causes of cranial nerve health issues.
Dr. Alex Jimenez’s Insight
There are 12 pairs of cranial nerves which exit the brain, one in each side. These cranial nerves are named and numbered (I-XII) according to their location in the brain as well as their specific function in the body. Common conditions, such as multiple sclerosis, may affect one or more of the cranial nerves, resulting in dysfunction of the specific regions innervated by them. Signs and symptoms associated with health issues affecting specific cranial nerves can help healthcare professionals determine the source of the problem. Testing the cranial nerves involves a number of steps in order to be certain which function of the human body has been ultimately affected.
Clinical Significance of the Cranial Nerves
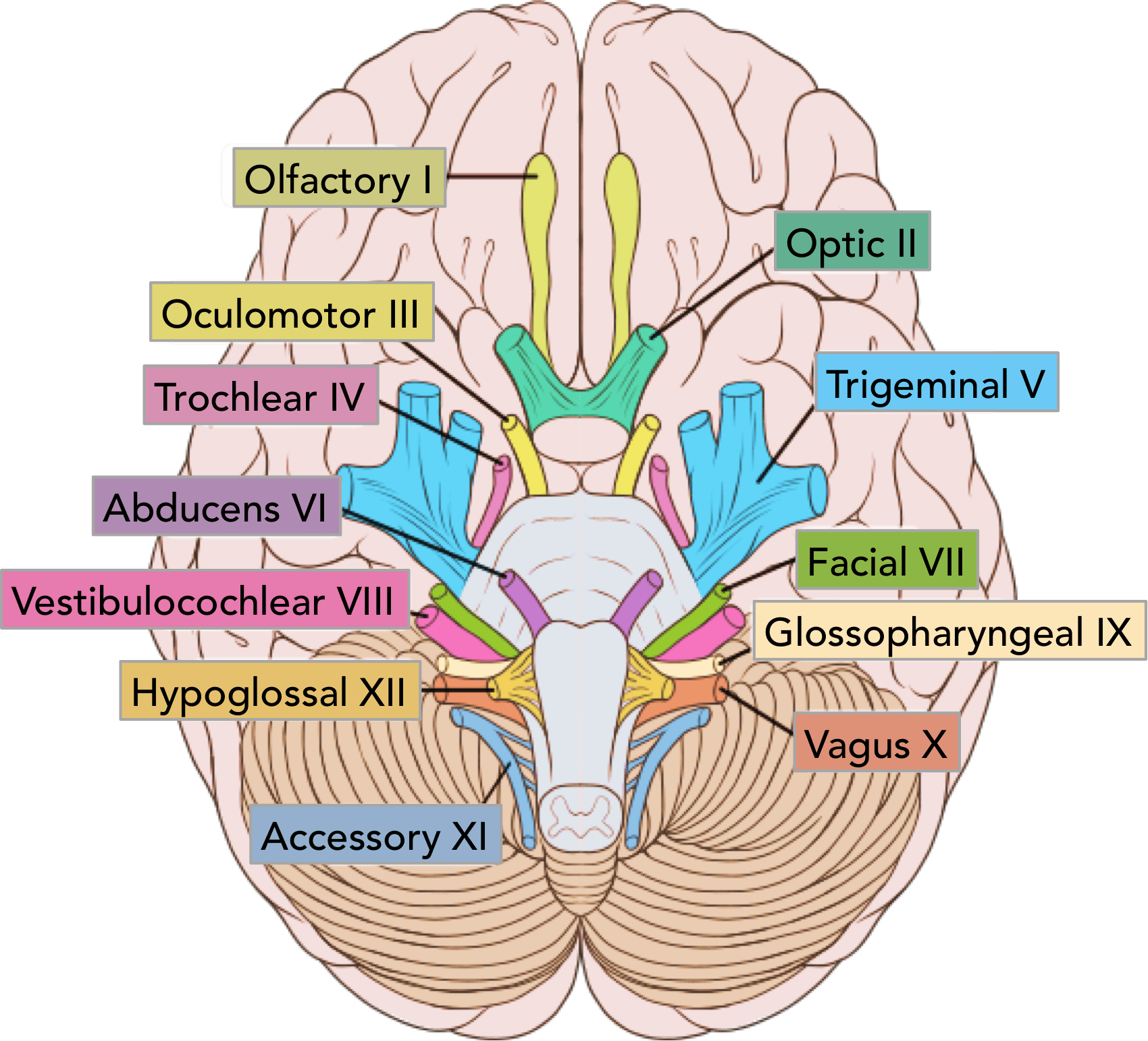
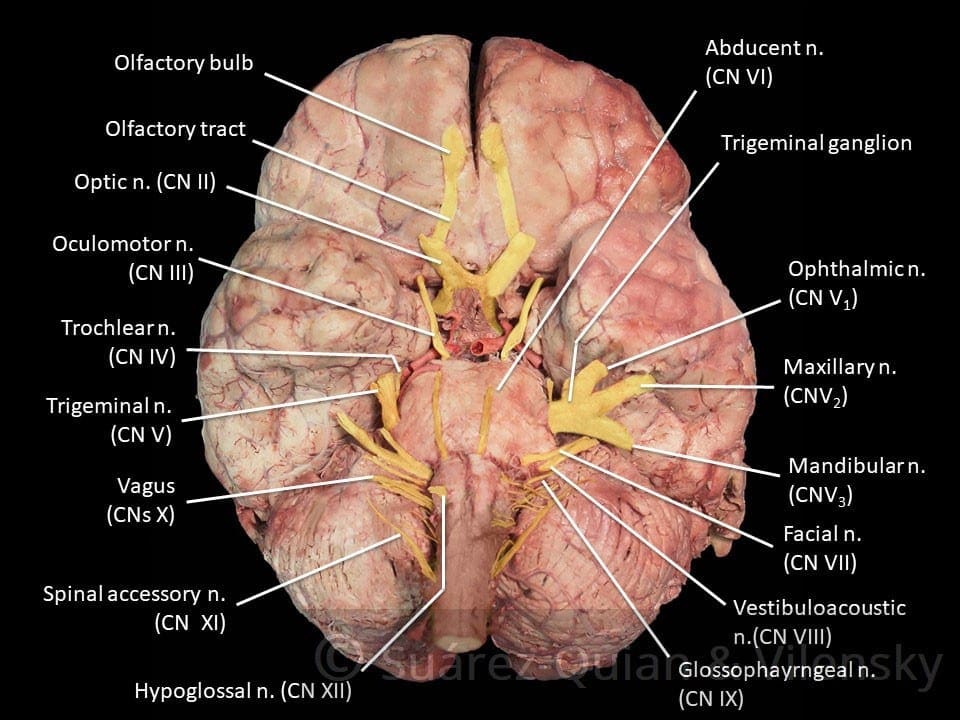
Most commonly, humans are believed to have twelve pairs of cranial nerves which have been assigned Roman numerals I-XII for identification. The numbering of the cranial nerves is based on the order in which they emerge from the brain, or from the front to the back of the brainstem. These include: the olfactory nerve (I), the optic nerve (II), the oculomotor nerve (III), the trochlear nerve (IV), the trigeminal nerve (V), the abducens nerve (VI), the facial nerve (VII), the vestibulocochlear nerve (VIII), the glossopharyngeal nerve (IX), the vagus nerve (X), the accessory nerve (XI), and the hypoglossal nerve (XII). Below we will narrow down the clinical significance of the cranial nerves.
Olfactory Nerve (I)
The olfactory nerve (I) communicates the sensation of smell to the brain. Lesions resulting in anosmia, or loss of the sense of smell, have been previously described to occur through trauma, damage or injury to the head, especially in the instance that a patient hits the back of their head. In addition, frontal lobe masses, tumors, and SOL have also been associated with the loss of the sense of smell. Healthcare professionals have previously identified that the loss of the sense of smell is one of the first symptoms seen in Alzheimer’s and early dementia patients.
Healthcare professionals may test the function of the olfactory nerve (I) by having the patient close their eyes and cover one nostril at a time in order to have them breathe out through their nose while placing a scent under the nostril and having them breathe in. The doctor will ask the patient, “do you smell anything?”, and record the findings. This tests whether the nerve is operating appropriately. If the patient says yes, the doctor will then ask the patient to identify the scent. This tests whether the processing pathway, known as the temporal lobe, is functioning accordingly.
Optic Nerve (II)
The optic nerve (I) communicates visual information to the retina. Lesions to this cranial nerve can be the result of CNS disease, such as MS, or CNS tumors and SOL. Most health issues associated with the visual system emerge from direct trauma, metabolic or vascular diseases. FOV lost in the periphery can also indicate that SOL may be affecting the optic chiasm, including a pituitary tumor.
A healthcare professional will often test the function of the optic nerve (II) by asking whether the patient can see. If the patient describes having vision in each eye, the optic nerve is functional. Doctors may also perform visual acuity testing using the Snellen chart, first one eye at a time, then the two eyes together, or they may perform distance vision testing. Near vision testing will often involve the Rosenbaum chart, first one eye at a time, then the two eyes together. Additional associated testing for the visual system can include, the ophthalmoscopic or funduscopic exam, which assess the A/V ratio and vein/artery health as well as assess cup to disc ratio of the visual system. Other testing methods include field of vision testing, intraoccular pressure testing and the iris shadow test.
Oculomotor Nerve (III), Trochlear Nerve (IV), and Abducens Nerve (VI)
The oculomotor nerve (III), the trochlear nerve (IV), the abducens nerve (VI) and the ophthalmic division of the trigeminal nerve (V1) travel through the cavernous sinus to the superior orbital fissure, passing out of the skull into the orbit. These cranial nerves control the tiny muscles that move the eye and also offer sensory innervation to the eye and orbit.
The clinical significance of the oculomotor nerve (III) includes diplopia, lateral strabismus (unopposed lateral rectus m.), head rotation away from the side of the lesion, a dilated pupil (unopposed dilator pupillae m.), and ptosis of the eyelid (loss of function of the levator palpebrae superioris m.). Lesions to the oculomotor nerve (III) can occur due to inflammatory diseases, such as syphilitic and tuberculous meningitis, aneurysms of the posterior cerebral or superior cebellar aa., and SOL in the cavernous sinus or displacing the cerebral peduncle to the opposite side. Testing this cranial nerve is performed by moving a light in front of the patient’s pupil from the lateral side and hold for 6 seconds. The doctor should watch for direct (ispilateral eye) and consensual (contralateral eye) pupillary constriction in order to distinguish dysfunction of the oculomotor nerve (III).
The clinical significance of the trochlear nerve (IV) is characterized where the patient presents diplopia and difficulty while maintaining a downward gaze, often complaining of having difficulties when walking down stairs, resulting in more frequent tripping and/or falling, followed by extortion of the affected eye (unopposed inferior oblique m.) and a head tilt to the unaffected side. Lesions to the trochlear nerve (IV) can commonly be the result of inflammatory diseases, aneurysms of the posterior cerebral or superior cerebellar aa., SOL in the cavernous sinus or superior orbital fissure and surgical damage during mesencephalon procedures. Head tilts in superior oblique palsy (CN IV failure) may also be identified.
The clinical significance of the abducens nerve (VI) includes diplopia, medial strabismus (unopposed medial rectus m.), and head rotation towards the side of the lesion. Lesions to this cranial nerve can be the result of aneurysms of the posterior inferior cerebellar or basilar aa., SOL in the cavernous sinus or 4th ventricle, such as a cerebellar tumor, fractures of the posterior cranial fossa, and increased intracranial pressure. Testing this cranial nerve is performed through the H-Pattern testing, where the healthcare professional will have the patient follow an object no bigger than 2 inches. It’s essential for the doctor to follow these specific guidelines as patient’s can have difficulties focusing on items that are too large, and it’s also important for the doctor not to hold the object too close to the patient. Convergence and accommodation testing is performed by bringing the object close to the bridge of the patient’s nose and back out at least 2 times. The physician must look for pupillary constriction response as well as convergence of the eyes.
Trigeminal Nerve (V)
The trigeminal nerve (V) is made up of three different parts: The . When put together, these nerves provide sensation to the skin of the face and also controls the muscles of mastication, or chewing. Cranial nerve dysfunction along any of the separate sections of the trigeminal nerve (V) can manifest as decreased bite strength on the ipsilateral side of the lesion, loss of sensation along the distribution of V1, V2, and V3, and loss of corneal reflex. Lesions to the trigeminal nerve (V) can be the result of aneurysms or SOL affecting the pons, particularly tumors at the cerebellopontine angle, skull fractures on the facial bones or damage to the foramen ovale, and Tic doloureux, most frequently referred to as trigeminal neuralgia, characterized by sharp pain along the distributions of the different parts of the trigeminal nerve (V). Physicians may utilize analgesic, anti-inflammatory or contralateral stimulation to control the signs and symptoms.
Testing the trigeminal nerve (V) includes pain & light touch testing along the ophthalmic (V1), the maxillary (V2), as well as the Mandibular (V3) nerves of the cranial nerve.�Testing is best done toward the more medial or proximal areas of
the face, where the V1, the V2 and the V3 are better delineated. A healthcare professional may also assess dysfunction along this cranial nerve using the blink/corneal reflex testing, performed by puffing air or doing a small tissue tap from the lateral side of the eye on the cornea. If normal, the patient blinks. The CN V provides the sensory (afferent) arc of this reflex. Bite strength may also be tested by having the patient bite down on a tongue depressor while the doctor tries to remove it. The jaw jerk/Masseter reflex may also be performed with the patient�s mouth slightly open, by placing the thumb on a patient�s chin and tapping the own thumb with a reflex hammer. Strong closure of the mouth indicates UMN lesion. CN V provides both the motor and sensory of this reflex.
Facial Nerve (VII) and Vestibulocochlear Nerve (VIII)
The facial nerve (VII) and the vestibulocochlear nerve (VIII) both input the inner auditory canal in the temporal bone. The facial nerve subsequently extends to the side of the face then distributes to control and reach all of the muscles in charge of facial expressions. The vestibulocochlear nerve reaches the organs which control equilibrium and hearing in the temporal bone.
As with all cranial nerves, signs and symptoms along the facial nerve (VII) describe the location of the lesion. Lesion in the lingual nerve will manifest as loss of taste, general sensation in the tongue and salivary secretion. Lesion proximal to the branching of the chorda tympani, such as in the facial canal, will result in the same signs and symptoms, without the loss of general sensation of the tongue, partly due because the V3 has not yet joined the facial nerve (VII). Corticobulbar innervation is asymmetric to the upper and lower parts of the facial motor nucleus. In the instance of an UMN lesion, or a lesion to the corticobulbar fibers, the patient will experience paralysis of the muscles in charge of facial expression in the contralateral lower quadrant. If there is an LMN lesion, or a lesion to the facial nerve itself, the patient will experience paralysis of the muscles of facial expression in the ipsilateral half of the face, otherwise known as Bell’s palsy.
A healthcare professional will test the facial nerve (VII) initially by asking the patient to mimic or follow specific instructions to make certain facial expressions. The doctor should make sure to evaluate all four quadrants of the face by asking the patient to raise their eyebrows, puff their cheeks, smile and then close their eyes tightly. Subsequently, the doctor will test the facial nerve (VII) by checking the strength of the buccinator muscle against resistance. The healthcare professional will achieve this by asking the patient to hold air in their cheeks as they press gently from the outside. The patient should be able to hold air in against the resistance.
Signs and symptoms of dysfunction in the vestibulocochlear nerve (VIII) often involve changes in hearing alone, most commonly as a result of infections in the otitis media and/or as a result of skull fractures. The most common lesion to this nerve is caused by an acoustic neuroma which affects the CN VII and the CN VIII, particularly the cochlear and vestibular divisions, as a result of proximity in the internal auditory meatus. Signs and symptoms of the health issue include nausea, vomiting, dizziness, hearing loss, tinnitus, and Bell’s palsy, etc.
Testing the vestibulocochlear nerve (VIII) for dysfunction commonly involves an otoscopic exam, the scratch test, which determines whether a patient can hear equally on both sides, the Weber test, tests for lateralization, a 256 Hz tuning fork placed on top of the patient�s head in the center, which can help point out whether a patient hears it louder on one side than the other, and finally the Rinne test, which compares air conduction to bone conduction. Normally, air conduction should last twice as long as bone conduction.
Glossopharyngeal Nerve (IX), Vagus Nerve (X) and Accessory Nerve (XI)
The glossopharyngeal (IX), the vagus nerve (X) and the accessory nerve (XI) all emerge from the skull to enter the neck. The glossopharyngeal nerve (IX) provides innervation to the upper throat and the back of the tongue, the vagus nerve (X) offers innervation to the muscles at the voicebox, and proceeds down to provide parasympathetic innervation to the chest and abdomen. The accessory nerve (XI) controls the trapezius and sternocleidomastoid muscles at the neck and shoulder.
The glossopharyngeal nerve (IX) is rarely damaged alone, due to it�s proximity to the CN X and XI. A healthcare professional should perform a test to look for signs of CN X & XI damage as well if CN IX involvement is suspected.
Patients with clinical signs and symptoms caused by vagus nerve (X) dysfunction may experience dysarthria, or difficulty speaking clearly, as well as dysphagia, or difficulty swallowing. These may present as food or liquid coming out of their nose or frequent chocking or coughing when eating and/or drinking. Further clinical presentations include hyperactivity of a visceral motor component, leading to the hypersecretion of gastric acid and resulting in ulcers. Hyper-stimulation of the general sensory component can cause coughing, fainting, vomiting and reflex visceral motor activity. The visceral sensory component of this nerve only provides general feelings of un-wellness but visceral pain may transfer on to the sympathetic nerves.
Testing for the glossopharyngeal nerve (IX) and the vagus nerve (X) can include the gag reflex, where the�CN IX provides the afferent (sensory) arc and the�CN X provides the efferent (motor) arc. Approximately 20 percent�of patients have a minimal or absent gag reflex. Other tests may include wwallowing, gargling, etc., as it requires CN X function. Healthcare professionals may also test palatal elevation because it requires CN X function. Furthermore, the doctor will see whether the palate elevates and uvula deviates
contralateral to damaged side. Finally, the healthcare professional will test the auscultation of the heart, since the R CN X innervates SA node (more rate regulation) and the L CN X the AV node (more rhythm regulation).
Lesions in the accessory nerve (XI)�may occur due to radical surgeries in the neck area, such as the removal of the laryngeal carcinomas. Testing for the accessory nerve (XI) may include the strength test SCM m. Patients with clinical signs and symptoms due to lesions in the accessory nerve (XI) will experience difficulties turning their head against the resistance of a healthcare professional, particularly toward the side opposite of the lesion. Testing for the accessory nerve (XI) may also include the strength test trapezius m. Patients with clinical signs and symptoms due to lesions in the accessory nerve (XI) will experience difficulties with shoulder elevation on the side of the lesion.
Hypoglossal Nerve (XII)
The hypoglossal nerve (XII) originates from the skull to reach the tongue in order to control essentially all of the muscles involved in the movements of the tongue. The clinical significance of health issues associated to the hypoglossal nerve (XII) can manifest as a deviating tongue towards the side of an inactive genioglossus m. upon tongue protrusion. This may often be contralateral to a corticobulbar, or UMN, lesion or from an ipsilateral to a hypoglossal n., or LMN, lesion.
Testing for the hypoglossal nerve (XII) involves the healthcare professional asking a patient to stick out their tongue. The doctor will look for any deviation which may signal a health issue along the length of the hypoglossal nerve (XII). Another test the doctor may perform as a part of the evaluation may include the physician asking the patient to place their tongue inside their cheek and apply light resistance, one side at a time. The patient should be able to resist moving their tongue with pressure.
The clinical significance of the signs and symptoms which manifest as a result of cranial nerve dysfunction are essential in order for the healthcare professional to properly diagnose the patient’s specific health issue. The clinical findings described above are often unique to the affected cranial nerve and the tests and evaluations for each can help confirm a diagnosis. Proper diagnosis is fundamental in order for the doctor to continue with the patient’s appropriate treatment. The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Sciatica
Sciatica is medically referred to as a collection of symptoms, rather than a single injury and/or condition. Symptoms of sciatic nerve pain, or sciatica, can vary in frequency and intensity, however, it is most commonly described as a sudden, sharp (knife-like) or electrical pain that radiates from the low back down the buttocks, hips, thighs and legs into the foot. Other symptoms of sciatica may include, tingling or burning sensations, numbness and weakness along the length of the sciatic nerve. Sciatica most frequently affects individuals between the ages of 30 and 50 years. It may often develop as a result of the degeneration of the spine due to age, however, the compression and irritation of the sciatic nerve caused by a bulging or herniated disc, among other spinal health issues, may also cause sciatic nerve pain.
Ataxia is a degenerative disease of the nervous system. Symptoms can mimic those of being inebriated/intoxicated, with� slurred speech, stumbling, falling, and unable to maintain coordination. This comes from degeneration of the cerebellum, which is the part of the brain responsible for coordinating movement. It is a disease that affects people of all ages. However, age of symptom onset can vary, from childhood to late adulthood. Complications from the disease can be serious, even debilitating and life shortening.
Symptoms can vary from person to person, as well as, the type of Ataxia. Symptom onset and progression can vary as well. Symptoms can worsen slowly, over decades or quickly, over a few months. The common symptoms are lack of coordination, slurred speech, trouble eating, swallowing, eye movement abnormalities, motor skill deterioration, difficulty walking, gait abnormalities, tremors, and heart problems. People with Ataxia usually require wheelchairs, walkers, and/or scooters to aid in mobility.
Ataxia
The Loss Of Full Control Of Bodily Movements, Especially Gait
History Of Ataxia
How long has it been present?
Slow onset ? Degenerative disease?
Acute onset ? Stroke?
When does it occur?
If worsened by walking on uneven surfaces, or with limited vision ? Sensory ataxia?
Are there any coexisting symptoms?
Vertigo, weakness, stiffness, cognitive changes, etc.
Have others noticed this gait disturbance?
If no, consider psychogenic cause
Is the gait change explainable by physical problems such as pain or weakness?
Antalgic gait, limp, etc.
Weakness
Proximal muscle weakness�? Myopathy?
Distal muscle weakness ? Neuropathy?
UMN signs?
LMN signs?
Has the patient fallen? Or at risk for fall?
Is ataxia limiting ADLs?
Balance
Utilizes
Vestibular system
Cerebellar system
Conscious proprioceptive information (joint position sense)
Visual information
Motor strength and coordination
Vestibular System
Generally, if the problem lies in the vestibular system the patient will experience dizziness, possibly having vertigo or nystagmus
Does the dizziness feel similar to when you stand up too fast?
Pre-Syncope
�Light-headedness�
CardiacOrigin
Output disorders
Arrhythmias
Holter monitor testing
Postural/Orthostatic hypotension
May be secondary to other problems (diabetic neuropathy, adrenal hypofunction, Parkinsons, certain medications, etc.)
Vasovagal episodes
Slow heart rate with low blood pressure
Often brought on by stress, anxiety or hyperventilation
Migraine
Due to cerebrovascular instability
Blood sugar dysregulation
Disequilibrium Hx Questions
Does the dizziness only occur when you�re on your feet?
Does it get better if you touch/hold onto something?
Disequilibrium
Common in the elderly
Due to sensory deficits
Gradual onset
Worsened by reduced vision
Dark
Eyes closed
Visual acuity losses
Improved by touching a stationary object
Subjective of dizziness often improves with a gait assistive device (cane, walker, etc.)
Other Causes
Psychological stress
Often patient will describe dizziness as �floating�
Rule out hyperventilation and other types of dizziness
Sources
Blumenfeld, Hal. Neuroanatomy through Clinical Cases. Sinauer, 2002.
Alexander G. Reeves, A. & Swenson, R. Disorders of the Nervous System. Dartmouth, 2004.
You have been diagnosed with Benign Paroxysmal Positional Vertigo. This brochure is designed to help increase your understanding of this disorder and its potential treatments.
Benign Paroxysmal Positional Vertigo
What Is BPPV?
Benign paroxysmal positional vertigo (BPPV) is a disorder of the inner ear. People with BPPV typically experi�ence brief episodes of vertigo (dizziness) when they change the position of their head with respect to gravity. Approximately 20 percent of all vertigo is due to BPPV.
What Causes BPPV?
Benign Paroxysmal Positional Vertigo is thought to be due to tiny crystals, called otoconia, that have collected within a sensitive part of the inner ear. Otoconia are crystals of calcium carbonate that are normally located in a structure of the ear called the utricle.
Dizziness occurs when the crystals are displaced from the utricle into the semicircular canals of the inner ear.
Otoconia may become displaced when the utricle is injured, if there is an infection or other disorder of the inner ear, or simply due to advanced age. When you change the position of your head, the otoconia move within the semicircular canals and this causes the dizziness. The dizziness subsides when the otoconia stop moving.
The most common cause of BPPV in people under age 50 is head injury. In older people, the most common cause is degeneration of the vestibular system of the inner ear. BPPV becomes much more common with advancing age. Other causes include minor strokes, Meniere’s disease, and viruses such as those causing vestibular neuritis. In approximately half of all BPPV cases, no cause can be determined.
What Are The Symptoms?
The symptoms of BPPV include dizziness or vertigo, lightheadedness, imbalance, and nausea. Activities that
bring on symptoms vary among individuals, but symptoms are usually associated with a change in the position of the head with respect to gravity. Getting out of bed, rolling over in bed, and tipping the head back to look up are common “problem” motions. The use of shampoo bowls in hair salons may bring on symptoms. An intermittent pattern is common. BPPV may be present for a few weeks, then stop, and then come back again.
How Is Benign Paroxysmal Positional Vertigo (BPPV) Diagnosed?
BPPV is diagnosed with the Dix-Hallpike test. This test involves observing the eyes with the head and body positioned in specific ways. It can be performed either by the clinician, or as part of a laboratory test called an electronystagmography, or ENG. If the Dix-Hallpike test is abnormal and the findings are “dassic” for BPPV, then additional testing is not necessary. If the results are normal or not “classic” then the diagnosis of BPPV is less certain and other tests may be suggested.
What Are The Treatments For BPPV?
There are four approaches to treating BPPV.
1. Do Nothing And Wait For It To Go Away By Itself
BPPV symptoms sometimes go away within six months of onset, therefore you might want to wait and see if your symptoms subside on their own. During this waiting period, medications to prevent motion sickness or nausea are sometimes helpful in controlling the nausea associated with BPPV.
2. Physical Maneuvers Performed In The Clinic
(The Epley and Semont Maneuvers)
The Epley and Semont maneuvers, named for their inventors, are treat�ments that are performed in the clinic. These treatments are specifi�cally intended to move the otoconia from the semicircular canals to a less sensitive location within the inner ear. Your clinician will select the treatment that is most appropriate for you.
Each of these treatments takes about 15 minutes and alleviates symptoms in about 80 percent of patients. In the remaining 20 percent, a second treatment may be necessary, or you may be instructed to perform the Brandt-Daroff exercises (see “Home Treatment”).
The Epley maneuver, also called the canalith reposi�tioning procedure (CRP) and particle repositioning, is a procedure in which the clinician moves your head into five positions, maintaining each position for ap�proximately 30 seconds. The Semont maneuver (also called the liberatory maneuver) is a procedure in which the clinician rapidly moves you from lying on one side to lying on the other side. These maneuvers may not be appropriate for patients with neck or back problems. Pa�tients who experience nausea or anxiety may wish to take medication prior to the treatment.
INSTRUCTIONS FOR PATIENTS AFTER CLINIC TREATMENTS
Follow these instructions after the Epley or Semont maneuver. B.Y doing so you will minimize the opportunity for otoconia to return to the semicircular canals of the inner ear and reduce the potential that your dizziness will recur.
Wait at least 10 minutes after the maneuver before going home.
This is to avoid “quick spins” or brief bursts of vertigo as the otoconia reposition themselves immedi�ately after the maneuver. If possible, arrange to have someone drive you home.
The following two days:
Sleep semi-recumbent for the next two nights. This means sleeping with your head halfway between flat and upright, at a 45-degree angle. This is most easily done by sleeping in a recliner chair or by sleeping with pillows appropriately arranged on a couch.
During the day, try to keep your head vertical. A soft neck brace may be helpful.
Do not go to the barber, hairdresser or dentist.
When shaving, keep your head vertical by bending forward at your hips with your neck extended.
If you need to administer eye drops, try to keep your head as vertical as possible.
Sham�poo only under the shower.
During the following week, avoid provoking head positions that might bring on BPPV.
Use two pillows when you sleep.
Avoid sleeping on the affected side.
Don’t turn your head far up or far down.
Avoid tilting your head back especially when lying on your back with your head turned toward the affected side.
If possible, postpone elective surgery and going to the beauty parlor or the dentist’s office.
Avoid far head-forward positions and exercises where the head is not kept upright, for example toe touches.
The effectiveness of the clinic treatment cannot be determined for one week.
Wait one week after treatment to test the effectiveness of treatment. Place yourself in the position that usually makes you dizzy. Be sure to position yourself cautiously and under conditions in which you can’t fall or hurt yourself.
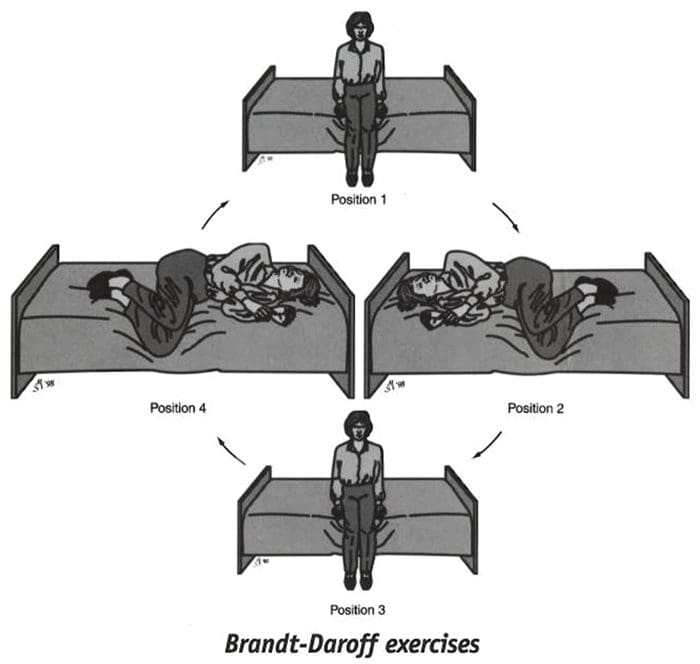
3. Home Treatment Of Benign Paroxysmal Positional Vertigo (Brandt-Daroff Exercises)
When the clinic treatment (Epley or Semont) fails, when the involved side is not determined, or when a case is mild, the Brandt-Daroff exercises may be recommended. These exercises succeed in 95 percent of cases but take longer to work than the clinic treatments. You should perform these exercises only if instructed to do so by your clinician. If your clini�cian performed the Epley or Semont maneuver, you must wait one week after that treatment before you begin the Brandt-Daroff exercises.
These exercises should be performed on a flat surface, without a pillow.
Start sitting upright on the edge of the bed or on the floor.
(Position 1)�Turn your head 45 degrees to the left and lie down on your right side.
(Position 2)�When in the right side-lying position, your head should be at a 45-degree angle turned halfway between the flat surface and the ceiling. Stay in the side-lying position for at least 30 seconds. If you are still dizzy, stay until the dizziness subsides or one minute, whichever is less.
Then sit up (Position 3} and stay in the sitting posi�tion for 30 seconds. Turn your head 45 degrees to the right and lie down on your left side.
(Position 4)�Again keeping your head turned halfway toward the ceiling for 30 seconds or until the dizziness subsides. Return to Position 1 (sit upright) for 30 seconds. This is one repetition.
One set (five repetitions) takes about 10 minutes to complete and should be performed each morning, mid-day and evening.
The Brandt-Daroff exercises should be performed for two weeks, three sets each day, or for three weeks, two sets each day (52 sets total). In most individuals, complete relief from symptoms is obtained after 30 sets, or about 10 days. In approximately 30 percent of patients, BPPV will recur within one year. If BPPV recurs you may wish to add one 10-minute exercise (one set) to your daily routine.
If the maneuvers or exercises do not control symptoms that have persisted for a year or longer and the diagnosis is very clear, surgery may be recommended. The most common surgical procedure, called posterior canal plugging, blocks most of the posterior canal’s function without affecting the functions of the other canals or parts of the ear. There is, however, a small risk of hearing loss. This surgery is effective in about 90 percent of individuals who have not responded to other treatments and when symptoms are severe and long-standing.
�?2000 Northwestern University. Authors: Timothy C. Hain, MD, Janet Odiry Helminski, PhD, PT.
This information is for educational purposes and is not intended as a substitute for examination, diagnosis, or medical care provided by a licensed and qualified health professional. This work was supported by the Center for Sensory and Communicotion Disorders at Northwestern University, a national research and training center funded by the National Institute on Deafness and Other Communication Disorders.
The cranial nerves are the nerves which come out straight from the brain, including the brainstem, in comparison to the spinal nerves, which come out from sections of the spinal cord. Of those, 10 out of 12 of these cranial nerves originate in the brainstem. Cranial nerves transfer information between the brain and parts of the human body, particularly to and from areas of the head and neck.
Spinal nerves exit from the spinal cord with the spinal nerve closest to the head (C1) exiting in the space above the first cervical vertebra. The cranial nerves, however, exit from the central nervous system above this region. Each cranial nerve is paired and is present on either side of the brain. Based on the definition in humans, there are twelve, sometimes thirteen, cranial nerve pairs, which have been assigned Roman numerals I-XII for identification, sometimes including cranial nerve zero as well. The numbering of the cranial nerves is based on the order in which they emerge from the brain, or from the front to the back of the brainstem.
The terminal nerves, olfactory nerves (I) and optic nerves (II) come out from the cerebrum, or forebrain, where the rest of the ten pairs of cranial nerves arise in the brainstem, which is the lower portion of the brain. The cranial nerves are considered components of the peripheral nervous system (PNS), though on a structural level, the olfactory, the optic and the trigeminal nerves are more accurately considered a portion of the central nervous system (CNS).
Most commonly, humans are believed to have twelve pairs of cranial nerves (I-XII). These include: the olfactory nerve (I), the optic nerve (II), the oculomotor nerve (III), the trochlear nerve (IV), the trigeminal nerve (V), the abducens nerve (VI), the facial nerve (VII), the vestibulocochlear nerve (VIII), the glossopharyngeal nerve (IX), the vagus nerve (X), the accessory nerve (XI), and the hypoglossal nerve (XII). There may be a thirteenth cranial nerve, known as the terminal nerve, or nerve N or O, which Is quite small and may or may not be functional in humans.
Anatomy of the Cranial Nerves
The cranial nerves are usually named according to their structure or function. For instance, the olfactory nerve (I) supplies smell, and the facial nerve (VII) supplies motor innervation to the face. Since Latin was the common language of the study of anatomy once the nerves were documented, recorded, and mentioned, many nerves maintain Greek or Latin names, including the trochlear nerve (IV), named based on its arrangement, as it supplies a muscle which attaches to a pulley (Greek: trochlea). The trigeminal nerve (V) is named based on its three components (Latin: trigeminus meaning triplets), and the vagus nerve (X) is known because of its wandering course (Latin: vagus).
In addition, cranial nerves are numbered according to their rostral-caudal, or front-back, position, when looking at the brain. If the brain is carefully removed from the skull, the nerves are typically visible in their numeric order, with the exception of the final nerve, the CN XII, which seems to come out from above, into the CN XI.
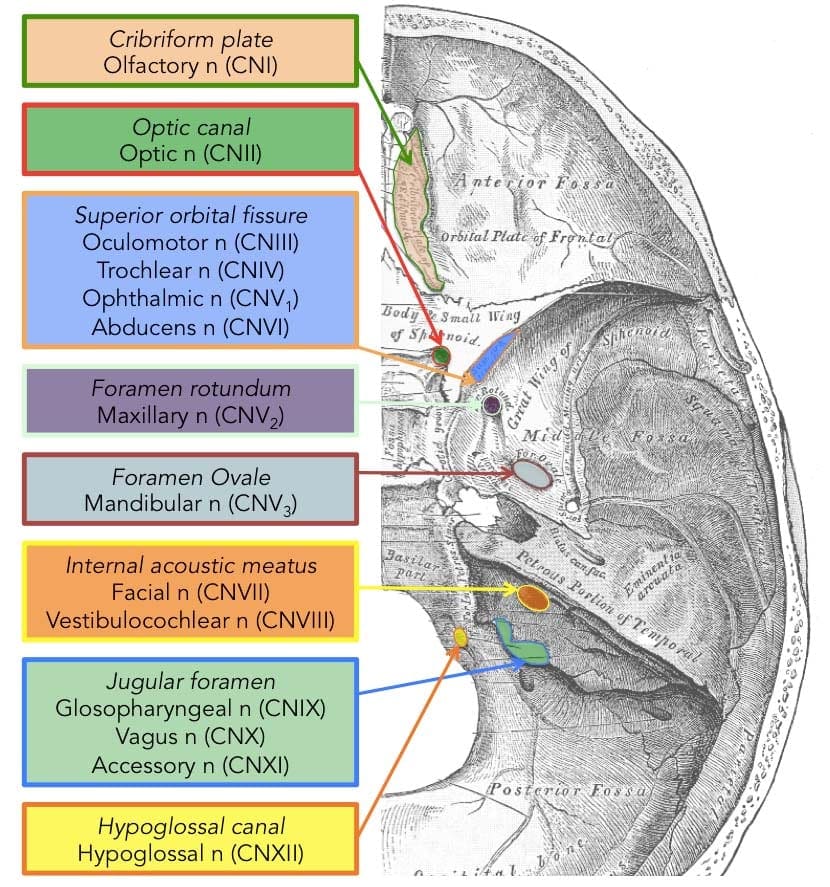
Cranial nerves have pathways within and away from the skull. The pathways inside the skull are known as “intracranial paths” and the pathways outside the skull are known as “extracranial pathways”. There are a number of holes in the skull known as “foramina”, by which the nerves may exit from the skull. All cranial nerves are paired, meaning that they can be found on both the left and right sides of the human body. The skin, muscles, or other structural function provided by a nerve on the same side of the human body as the side it originates from, is referred to as an ipsilateral function. In case the function is on the other hand from the origin of the nerve, then this is referred to as a contralateral function.
Location of the Cranial Nerves
After coming out from the brain, the cranial nerves from inside the skull must leave this bony structure in order to arrive to their destinations. Several of the cranial nerves pass through the foramina,�holes in the skull, as they journey to their destinations. Other nerves pass through bony canals, longer pathways enclosed by bone. The foramina and canals might contain more than just one cranial nerve, and may also include blood vessels. Below is a list of the twelve cranial nerves and a brief summary of their function.
The olfactory nerve (I), composed of many small separate nerve fibers, which passes through perforations from the cribiform plate component of the ethmoid bone. These fibers end in the upper part of the nasal cavity and also operate to communicate impulses containing information about scents or odors into the brain.
The optic nerve (II) passes through the optic foramen from the sphenoid bone in order to reach the eye. It communicates visual information to the brain.
The oculomotor nerve (III), the trochlear nerve (IV), the abducens nerve (VI) and the ophthalmic division of the trigeminal nerve (V1) journey through the cavernous sinus to the superior orbital fissure, passing out of the skull into the orbit. These cranial nerves control the tiny muscles that move the eye and also offer sensory innervation to the eye and orbit.
The maxillary division of the trigeminal nerve (V2) moves through the foramen rotundum from the sphenoid bone to supply the skin of the middle of the face.
The mandibular branch of the trigeminal nerve (V3) moves through the foramen ovale of the sphenoid bone to supply the lower face with sensory innervation. This nerve also extends to nearly all the muscles that control chewing.
The facial nerve (VII) and the vestibulocochlear nerve (VIII) both input the inner auditory canal in the temporal bone. The facial nerve subsequently extends to the side of the face using the stylomastoid foramen, also from the temporal bone. Its fibers then distribute to control and reach all of the muscles in charge of facial expressions. The vestibulocochlear nerve reaches the organs which control equilibrium and hearing in the temporal bone, and therefore doesn’t reach the outside surface of the skull.
The glossopharyngeal (IX), the vagus nerve (X) and the accessory nerve (XI) all emerge from the skull via the jugular foramen to enter the neck. The glossopharyngeal nerve provides innervation to the upper throat and the back of the tongue, the vagus nerve offers innervation to the muscles at the voicebox, and proceeds down to provide parasympathetic innervation to the chest and abdomen. The accessory nerve controls the trapezius and sternocleidomastoid muscles at the neck and shoulder.
The hypoglossal nerve (XII) exits the skull using the hypoglossal canal at the occipital bone and also reaches the tongue to control virtually all the muscles involved in movements of this organ.
Function of the Cranial Nerves
The cranial nerves give motor and sensory innervation particularly to the structures found inside the neck and head. The sensory innervation contains both “overall” feelings, such as temperature and touch, and “particular” innervation, such as flavor, vision, smell, balance and hearing. For instance, the vagus nerve (X) gives sensory and autonomic, or parasympathetic, motor innervation to structures in the neck and to many of the organs in the chest and abdomen. Below, we will discuss the function of each cranial nerves in further detail.
Smell (I)
The olfactory nerve (I) communicates the sense of smell. Damage to the olfactory nerve (I) may cause an inability to smell, referred to as anosmia, a distortion in the sense of odor, referred to as parosmia, or even a distortion or absence of flavor. When there’s suspicion of a change in the sense of smell, every nostril is tested with compounds of known odors, such as coffee or soap. Intensely smelling chemicals, such as ammonia, can lead to the activation of pain receptors, known as nociceptors, of the trigeminal nerve which are situated in the nasal cavity, which may ultimately confound olfactory testing.
Vision (II)
The optic nerve (II) communicates visual information. Damage to the optic nerve (II) affects specific aspects of vision which are based on the area of the lesion. An individual may not be able to observe objects in their left or right sides, known as homonymous hemianopsia, or might have difficulty seeing objects on their outer visual areas, known as bitemporal hemianopsia, if the optic chiasm is included. Vision may be analyzed by examining the visual field, or simply by analyzing the retina with an ophthalmoscope, with a procedure called funduscopy. Visual field testing can be employed to pin-point structural lesions in the optic nerve, or further along the visual pathways.
Eye Movement (III, IV, VI)
The oculomotor nerve (III), the trochlear nerve (IV) and the abducens nerve (VI) coordinate eye motion. Damage to nerves III, IV, or VI can impact the movement of the eyeball globe. One or both eyes may be influenced; in either case, double vision, referred to as diplopia, will likely occur since the movements of the eyes are no longer synchronized. Nerves III, IV and VI are tested by observing the way the eye follows an object in different directions. This object may be a finger or even a pin, and may be moved at several directions to test for pursuit velocity. If the eyes don’t work together, the most likely cause is harm to a specific cranial nerve or its nuclei.
Damage to the oculomotor nerve (III) can lead to double vision, or diplopia, and inability to coordinate the movements of both eyes, known as strabismus, as well as eyelid drooping, referred to as ptosis, and pupil dilation, or mydriasis. Lesions may also lead to theinability to open the eye due to paralysis of the levator palpebrae muscle. People suffering from a lesion in the oculomotor nerve may compensate by leaning their heads to relieve symptoms because of paralysis of one or more of the eye muscles it regulates.
Damage to the trochlear nerve (IV) may also cause diplopia with all the eye adducted and raised. The result will be an eye which can’t move downwards properly, especially downwards when within an inward position. This is a result of impairment from the superior oblique muscle, which is innervated by the trochlear nerve.
Damage to the abducens nerve (VI) can also result in diplopia This is a result of impairment in the lateral rectus muscle, which is innervated by the abducens nerve.
Trigeminal nerve (V)
The trigeminal nerve (V) is made up of three different parts: The ophthalmic (V1), the maxillary (V2), as well as the Mandibular (V3) nerves. When put together, these nerves provide sensation to the skin of the face and also controls the muscles of mastication, or chewing. Conditions affecting the trigeminal nerve (V) include, trigeminal neuralgia, cluster headaches, and trigeminal zoster. Trigeminal neuralgia may occur later in life, from middle age onwards, most often after the age of 60, and it is a condition commonly associated with a very strong pain that spreads over the region innervated by the maxillary or mandibular nerve divisions of the trigeminal nerve (V2 and V3).
Facial expression (VII)
Lesions of the facial nerve (VII) may manifest as facial palsy. This is where a individual is unable to move the muscles on one or both sides of the face. An extremely frequent and generally temporary facial palsy is called Bell’s palsy. Bell’s Palsy is the end result of an idiopathic (unknown cause), unilateral lower motor neuron lesion of the facial nerve and is characterized by an inability to move the ipsilateral muscles of facial expression, including altitude of the eyebrow and furrowing of their forehead. Patients with Bell’s palsy frequently have a drooping mouth over the affected side and often have difficulty chewing since the buccinator muscle is affected. Bell’s palsy occurs very rarely, affecting around 40,000 Americans annually. Facial paralysis may be caused by other conditions including, stroke. Related conditions to Bell’s Palsy are sometimes misdiagnosed as Bell’s Palsy. Bell’s Palsy is a temporary condition usually lasting 2-6 months, but can have life-changing results and may reoccur often. Strokes typically also impact the cranial nerve by cutting off blood flow to nerves within the brain which is a clear indication that the nerve is present with similar symptoms.
Hearing and Equilibrium (VIII)
The vestibulocochlear nerve (VIII) divides into the vestibular and cochlear nerve. The vestibular region is in charge of innervating the vestibules and semicircular canal of the inner ear; this structure communicates information regarding equilibrium, and is a significant element of the vestibuloocular reflex, which keeps the brain stable and allows the eyes to track moving objects. The cochlear nerve communicates data from the cochlea, allowing sound to be heard. If damaged, the vestibular nerve can manifest the sensation of spinning and dizziness. Function of the vestibular nerve may be analyzed by placing warm and cold water in the ears and watching eye motions caloric stimulation. Damage to the vestibulocochlear nerve may also pose as repetitive and involuntary eye movements, previously described as nystagmus, particularly when looking in a horizontal plane. Damage to the cochlear nerve may cause partial or complete deafness in the affected ear.
Oral Sensation, Taste, and Salivation (IX)
The glossopharyngeal nerve (IX) innervates the stylopharyngeus muscle and supplies sensory innervation to the oropharynx and back of the tongue. The glossopharyngeal nerve additionally supplies parasympathetic innervation to the parotid gland. Unilateral absence of a gag reflex suggests a lesion of the glossopharyngeal nerve (IX), and perhaps the vagus nerve (X).
Vagus Nerve (X)
Reduction of function of the vagus nerve (X) can lead to a reduction of parasympathetic innervation to quite a high number of structures. Important consequences of damage to the vagus nerve could include an increase in blood pressure and heart rate. Isolated dysfunction of just the vagus nerve is rare, but can be diagnosed with a hoarse voice, because of dysfunction of one of its branches, the recurrent laryngeal nerve. Damage to this nerve may result in difficulties swallowing.
Shoulder Elevation and Head-Turning (XI)
Damage to the accessory nerve (XI) can lead to ipsilateral weakness in the trapezius muscle. This can be tested by asking the patient to elevate their shoulders or shrug, where the shoulder blade, or scapula, will protrude to a winged position. Additionally, if the nerve is damaged, weakness or an inability to elevate the scapula may be present because the levator scapulae muscle is only able to provide this function. Based on the location of the lesion, there may also be weakness within the sternocleidomastoid muscle, which then acts to reverse the head so that the face points to the other side.
Tongue Movement (XII)
The hypoglossal nerve (XII) is unique in that it is innervated in the motor cortices of both hemispheres of the brain. Damage to the nerve at lower motor neuron level may cause fasciculations or atrophy of the muscles of the tongue. The fasciculations of the tongue are sometimes said to look like a”bag of worms”. Upper motor neuron damage won’t cause atrophy or fasciculations, but only weakness of the innervated muscles. Once the nerve is damaged, it will lead to weakness of tongue movement on one side. When damaged and extended, the tongue will move towards the weaker or damaged side, as shown in the image.
Dr. Alex Jimenez’s Insights
The cranial nerves are a set of 12 nerves which emerge directly from the brain. The first two nerves, known as the olfactory nerve and the optic nerve, come out from the cerebellum, where the remaining ten cranial nerves emerge from the brain stem. The names of the cranial nerves relate directly to their function and they are also numerically identified in roman numerals I-XII by their specific location of the brain and by the order in which they exit the cranium. Damage to any of the above mentioned cranial nerves can cause health issues associated to the specific structure and function of each nerve. Common signs and symptoms in these regions can help healthcare professionals identify the affected cranial nerves.
The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Sciatica
Sciatica is medically referred to as a collection of symptoms, rather than a single injury and/or condition. Symptoms of sciatic nerve pain, or sciatica, can vary in frequency and intensity, however, it is most commonly described as a sudden, sharp (knife-like) or electrical pain that radiates from the low back down the buttocks, hips, thighs and legs into the foot. Other symptoms of sciatica may include, tingling or burning sensations, numbness and weakness along the length of the sciatic nerve. Sciatica most frequently affects individuals between the ages of 30 and 50 years. It may often develop as a result of the degeneration of the spine due to age, however, the compression and irritation of the sciatic nerve caused by a bulging or herniated disc, among other spinal health issues, may also cause sciatic nerve pain.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine





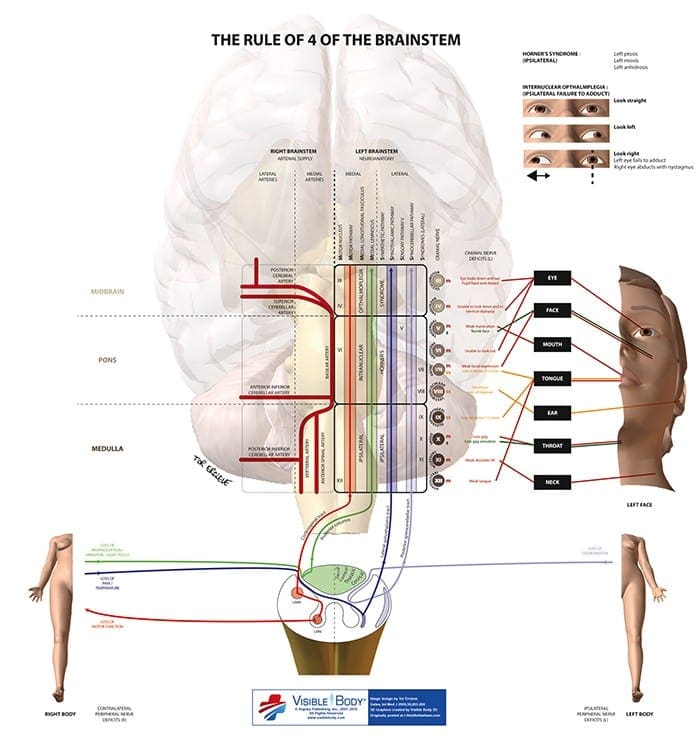
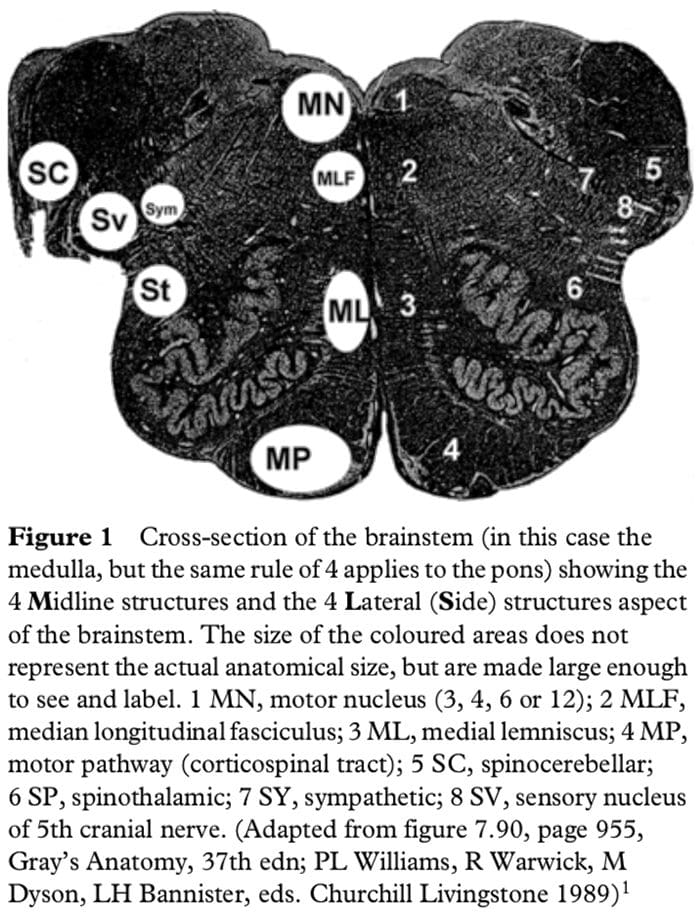
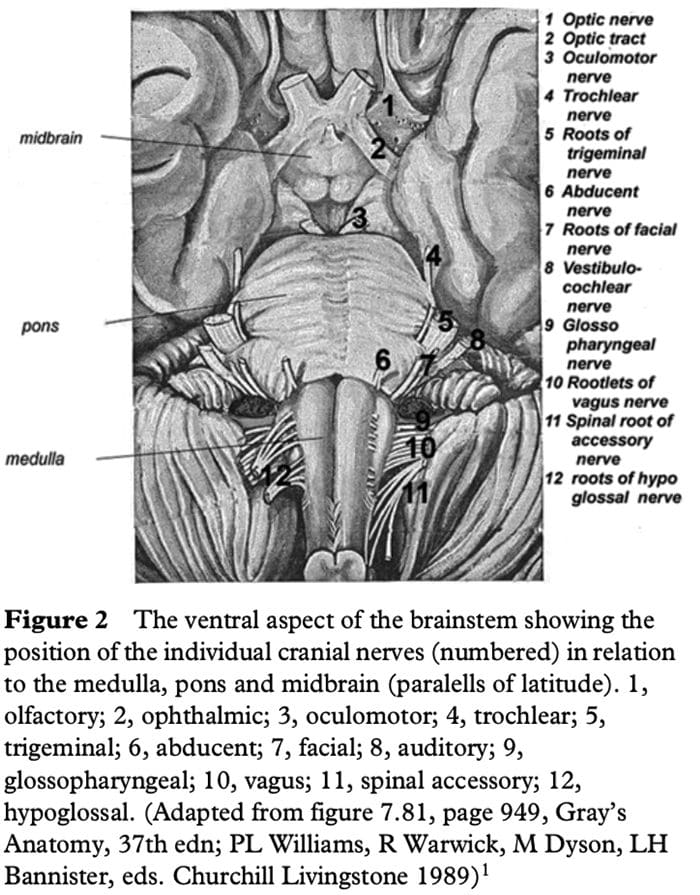
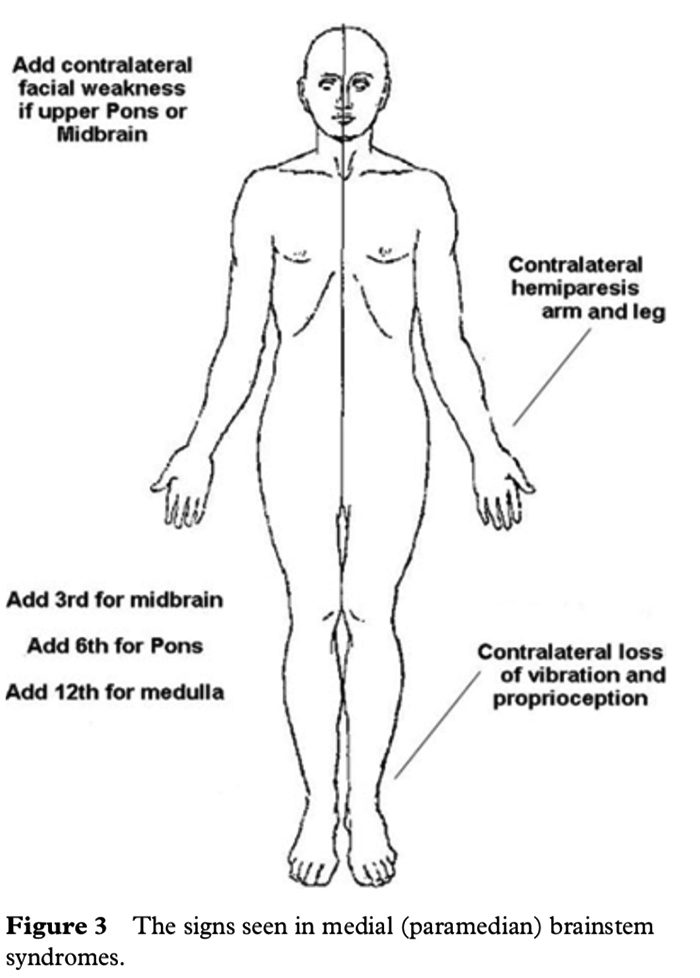 LATERAL BRAINSTEM SYNDROMES
LATERAL BRAINSTEM SYNDROMES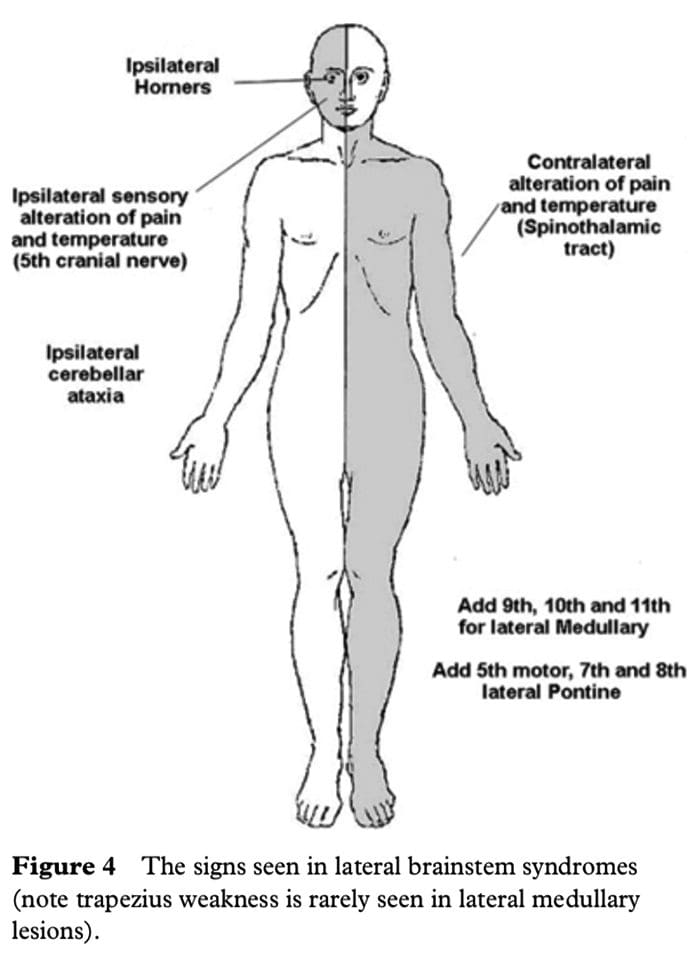 The lower 4 cranial nerves are in the medulla and the 12th nerve is in the midline so that 9th, 10th and 11th nerves will be in the lateral aspect of the medulla. When these are affected, the result is dysarthria and dysphagia with an ipsilateral impairment of the gag reflex and the palate will pull up to the opposite side; occasionally there may be weakness of the ipsilateral trapezius and/or sternocleidomastoid muscle. This is the lateral medullary syndrome usually resulting from occlusion of the ipsilateral vertebral or posterior inferior cerebellar arteries.
The lower 4 cranial nerves are in the medulla and the 12th nerve is in the midline so that 9th, 10th and 11th nerves will be in the lateral aspect of the medulla. When these are affected, the result is dysarthria and dysphagia with an ipsilateral impairment of the gag reflex and the palate will pull up to the opposite side; occasionally there may be weakness of the ipsilateral trapezius and/or sternocleidomastoid muscle. This is the lateral medullary syndrome usually resulting from occlusion of the ipsilateral vertebral or posterior inferior cerebellar arteries.
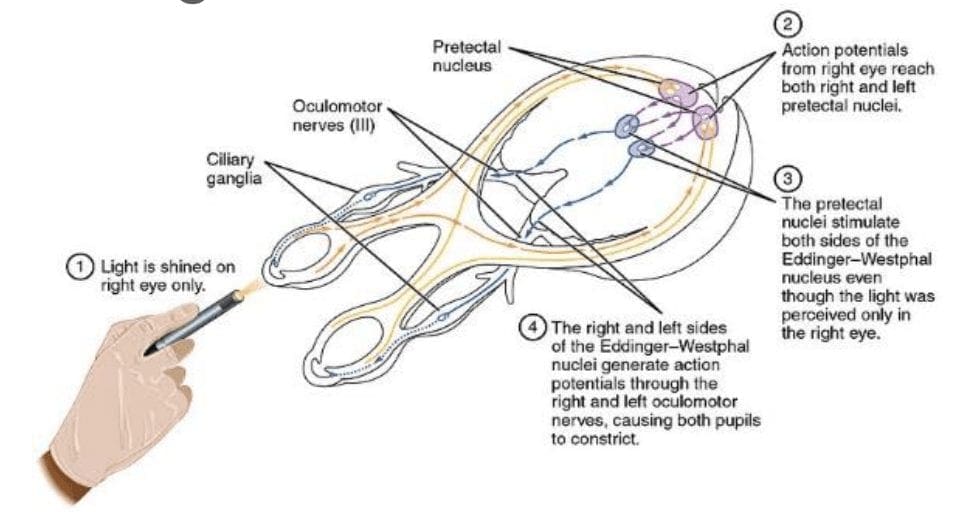
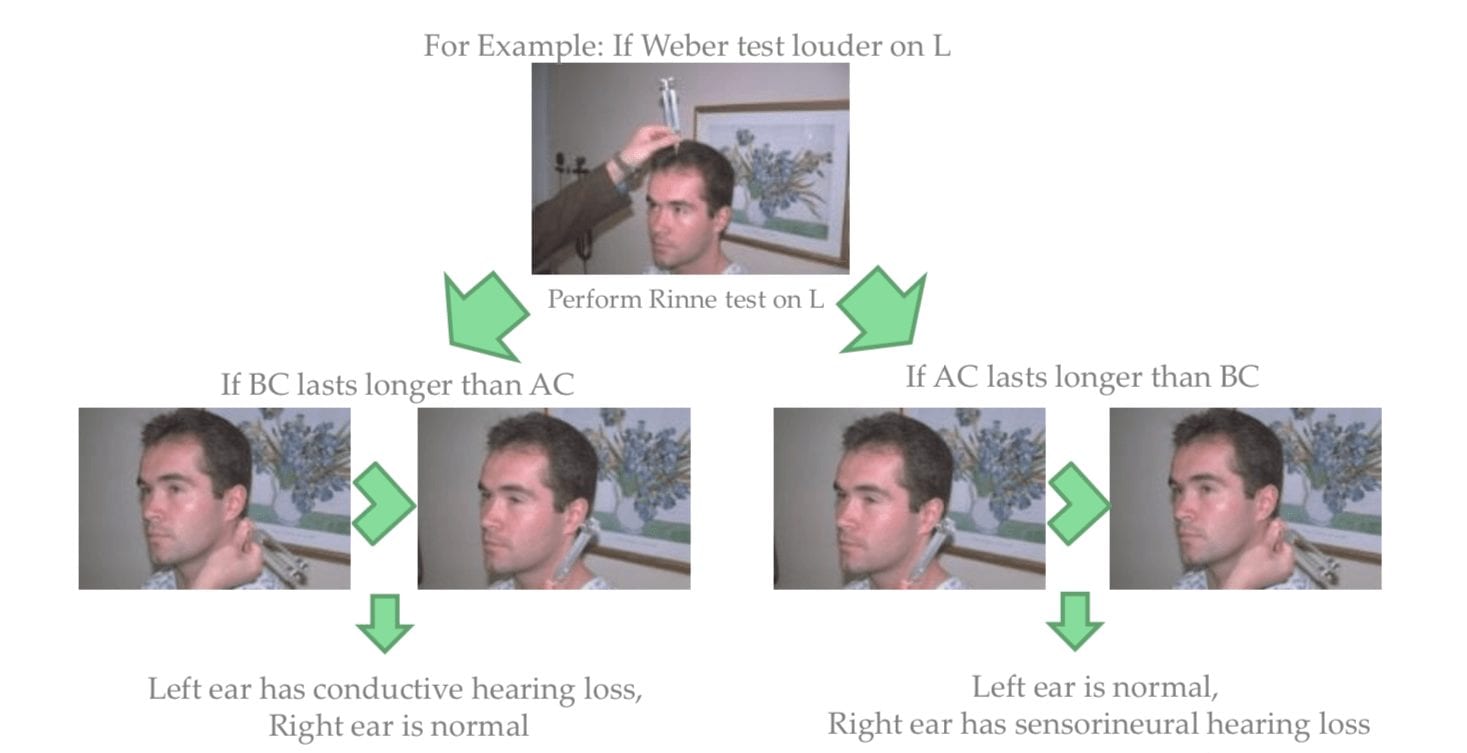
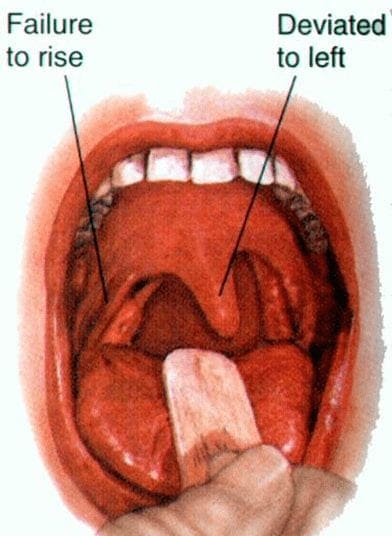
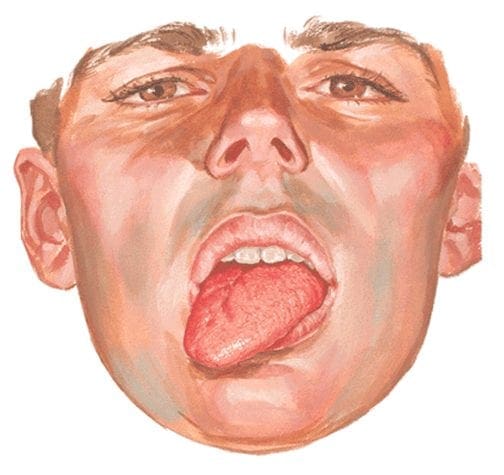
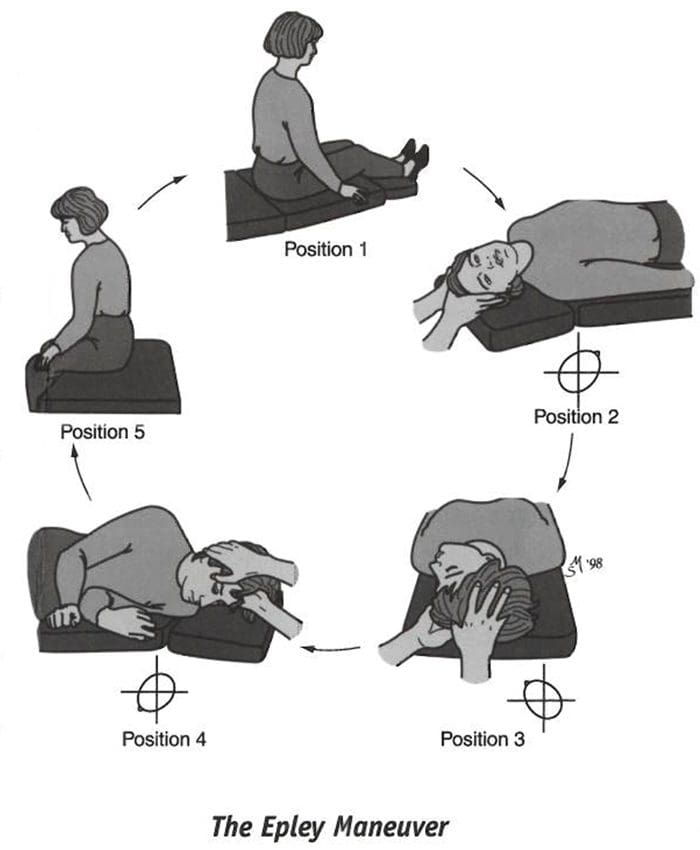 May develop spontaneously, especially in the elderly
May develop spontaneously, especially in the elderly
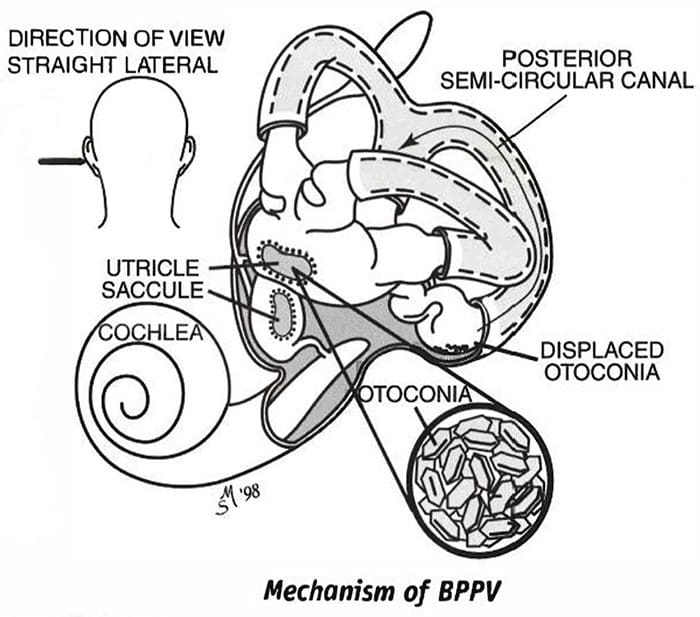
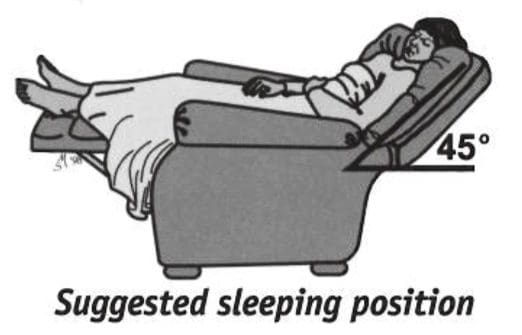 Sleep semi-recumbent for the next two nights. This means sleeping with your head halfway between flat and upright, at a 45-degree angle. This is most easily done by sleeping in a recliner chair or by sleeping with pillows appropriately arranged on a couch.
Sleep semi-recumbent for the next two nights. This means sleeping with your head halfway between flat and upright, at a 45-degree angle. This is most easily done by sleeping in a recliner chair or by sleeping with pillows appropriately arranged on a couch.