Understanding the Gut-Brain Connection After Traumatic Brain Injury: How Chiropractic Care Can Help Restore Balance
A woman is experiencing gut pain symptoms after sustaining a head injury in a motor vehicle crash.
Traumatic brain injury, often called TBI, happens when a sudden blow or jolt to the head disrupts normal brain function. This can range from mild concussions to severe cases that change lives forever. However, many people are unaware that TBI doesn’t just affect the head—it can also impact the entire body, particularly the gut. The gut and brain communicate with each other constantly through a network known as the gut-brain axis. When TBI occurs, this chat becomes disrupted, leading to issues such as leaky gut, imbalanced gut bacteria, and poor digestion. These issues can exacerbate the brain injury by spreading inflammation throughout the body. On the other hand, simple changes like chiropractic adjustments may help alleviate issues by calming nerves, reducing inflammation, and strengthening the gut-brain connection.
In this article, we’ll break down how TBI harms the gut, the symptoms it causes, and why the gut matters for healing the brain. We’ll also examine how integrative chiropractic therapy—think spinal adjustments to enhance nerve signals—can alleviate digestive issues and promote recovery. Drawing from recent studies and expert insights, we’ll keep it straightforward so you can grasp the science without getting lost in jargon.
What Is Traumatic Brain Injury, and Why Does It Matter for Gut Health?
TBI strikes about 69 million people worldwide each year, from car crashes to sports hits (Dhar et al., 2024). Right after the injury, the brain swells and releases signals that stress the body. This stress doesn’t stay in the head; it travels down nerves and hormones to the belly. The gut-brain axis is like a two-way street: the brain instructs the gut when to digest food, and the gut sends back signals that influence mood and focus.
When TBI blocks this street, the gut suffers. One significant change is increased gut permeability, also known as “leaky gut.” Normally, the gut wall acts like a tight filter, letting nutrients in but keeping junk out. After a TBI, that filter loosens, allowing bacteria and toxins to slip into the blood. This sparks body-wide inflammation, which in turn inflames the brain further (Nicholson et al., 2019).
Here’s a quick list of how TBI disrupts the gut-brain axis:
Nerve Signal Glitches: The vagus nerve, a key player in the autonomic nervous system, gets thrown off, slowing gut movement and causing backups.
Hormone Shifts: Stress hormones, such as cortisol, spike, weakening the gut lining.
Immune Overdrive: Brain damage triggers alarm signals that activate gut immune cells, resulting in swelling.
These changes don’t just cause tummy troubles—they can drag out brain fog, fatigue, and even raise risks for long-term issues like depression or Alzheimer’s (Nicholson et al., 2019). Restoring the gut could significantly contribute to the recovery from traumatic brain injury.
The Gut’s Hidden Role in Brain Healing
Your gut isn’t just for breaking down lunch; it’s a powerhouse for brain health. It houses trillions of bacteria—the microbiome—that make feel-good chemicals like serotonin, which boosts mood and sleep. Approximately 90% of serotonin originates from the gut, rather than the brain (Nicholson et al., 2019). After a TBI, this factory slows down, leaving you irritable or exhausted.
The gut also absorbs key nutrients essential for brain repair, such as omega-3s for nerve growth and B vitamins for energy. When gut issues arise, you miss them, stalling the healing process. Additionally, healthy gut bacteria combat inflammation, facilitating the brain’s ability to rewire itself through neuroplasticity—the brain’s capacity to form new neural pathways.
Microbiome Magic: Good bacteria produce short-chain fatty acids (SCFAs) that calm brain swelling and support new cell growth.
Barrier Buddies: A strong gut wall blocks toxins that could cross the blood-brain barrier and worsen damage.
Mood Messengers: Gut signals via the vagus nerve influence stress and focus, key for rehab.
Studies indicate that TBI patients with gut imbalances have slower recovery and more cognitive slips (Hassan et al., 2020). However, nourishing the gut with the right foods or therapies can help reverse the situation.
How TBI Leads to Leaky Gut and Bacterial Imbalance
Leaky gut starts fast after TBI—sometimes in hours. Brain trauma intensifies stress responses, flooding the body with catecholamines that disrupt the gut’s tight junctions, the “zippers” that hold cells together (Pitman et al., 2021). Proteins like occludin and ZO-1 break down, letting bacteria sneak out.
This leakage triggers a firestorm: toxins enter the bloodstream, activating immune cells to release cytokines such as TNF-α and IL-6. These chemicals not only inflame the gut but also travel to the brain, fueling secondary damage (Dhar et al., 2024). In one study, TBI mice exhibited 2.5 times more gut leaks, which was linked to higher mortality rates from infections (Nicholson et al., 2019).
Dysbiosis, or bacterial imbalance, worsens. TBI alters the microbiome, with harmful bacteria, such as Proteobacteria, proliferating while beneficial ones, like Firmicutes, decline (Wang et al., 2021). This imbalance reduces SCFA production, which normally helps soothe inflammation. Human data support this—patients post-TBI have altered gut microbiomes for years, linked to poorer cognitive skills (Hassan et al., 2020).
Key signs of this gut takeover include:
Early Warning: Within days, slower gut motility leads to bloating and irregular poops.
Long Haul: Chronic dysbiosis increases the likelihood of ongoing inflammation and nutrient deficiencies.
Feedback Loop: Leaky gut feeds brain inflammation, which in turn worsens gut leaks—a vicious cycle.
Breaking this loop is crucial; without it, TBI recovery stalls (Cognitive FX, 2023).
Common Digestive Woes After a Brain Injury
TBI’s gut punch shows up in everyday gripes that sap energy and joy. Nausea strikes hard early on, often accompanied by vomiting or dry heaves, making eating a chore (Cognitive FX, 2023). Constipation is sneaky—slowed nerves mean food lingers too long, causing hard stools and belly pain. Diarrhea flips the script, from bacterial overgrowth or stress.
Other hits:
Bloating and Gas: Trapped air from poor motility feels like a balloon in your gut.
Appetite Crash: Loss of hunger leads to weight drops and missing nutrients.
Acid Issues: Reflux or heartburn from weakened barriers irritates the throat.
These aren’t just annoyances; they link to brain symptoms. For example, gut inflammation can amp up headaches or dizziness (Flint Rehab, 2023). In severe cases, feeding intolerance affects up to 50% of patients, hiking infection risks (Dhar et al., 2024). Spotting these early lets you act fast.
Inflammation: The Bridge Between Gut Chaos and Brain Strain
Inflammation is the troublemaker tying gut woes to brain hurt. After a TBI, damaged brain cells release danger signals (DAMPs) that alert the immune system. This revs up gut cytokines, which leak through the damaged wall and reach the brain, causing swelling of neurons (Pitman et al., 2021).
The gut, which contains 70% of immune cells, amplifies this process. Dysbiosis releases pro-inflammatory signals, while low SCFAs allow swelling to run rampant (Wang et al., 2021). Result? A body-wide storm that delays healing and sparks issues like epilepsy or PTSD (Hassan et al., 2020).
Chronic Creep: Lingering inflammation is linked to diseases years later, according to long-term studies.
Taming this fire is key; therapies that cool gut swelling often ease brain fog too (Nicholson et al., 2019).
Enteric Nervous System: The Gut’s Brain Goes Haywire
The enteric nervous system (ENS), your gut’s own nerve web, acts like a mini-brain, controlling wiggles and juices. TBI zaps it via vagus glitches and hormone floods, leading to dysfunction (Nicholson et al., 2019). Serotonin levels in the colon decrease, slowing peristalsis—the wave that propels food through the digestive tract (Traumatic brain injury alters the gut-derived serotonergic system, 2022).
This means gastroparesis (stomach paralysis) or spasms, which can worsen leaks and dysbiosis. ENS glia, support cells, become reactive, adding to swelling (Dhar et al., 2024). In patients, this ties to incontinence or pain lasting months.
Quick facts on ENS fallout:
Signal Static: Vagus tone drops, cutting anti-inflammatory acetylcholine.
Peristalsis Problems: Uneven waves cause backups or rushes.
Repair Potential: Boosting vagal signals can reset the ENS, per animal tests.
Restoring ENS flow could smooth digestion and brain signals alike.
Chiropractic Therapy: A Natural Treatment for Gut-Brain Blues
Integrative chiropractic care excels in this area, utilizing spinal adjustments to optimize the nervous system. Misaligned vertebrae, common after TBI whiplash, pinch nerves and disrupt gut chats (Auburn Chiropractors, 2023). Adjustments realign the spine, easing pressure and boosting vagus tone to promote better motility and reduced swelling.
Vagal Revival: A higher tone helps combat dysbiosis and leaky gut, according to studies on autonomic shifts.
Dr. Alexander Jimenez, a chiropractor with over 20 years in functional medicine, observes this in practice. At his clinic, TBI patients report less nausea and steadier bowels after adjustments, thanks to better spine-gut links. “Spinal care isn’t just for backs—it’s key to whole-body healing, including the gut-brain tie,” Jimenez notes in his wellness posts (Jimenez, 2023). His approach combines adjustments with nutrition, aligning with research on multi-modal solutions.
Real Ways Chiropractic Eases Digestive Drama Post-TBI
Patients under chiropractic care see quick wins. Adjustments lower cortisol, easing stress that tightens gut junctions (Eugene Chiropractor, 2023). A study-linked review shows reduced gastrointestinal symptoms in brain injury cases through vagus stimulation (Northwest Florida Physicians Group, 2023).
Benefits include:
Motility Makeover: Faster transit cuts constipation by 30–50%, according to some reports.
Barrier Build: Less permeability means fewer toxins, aiding brain clarity.
Pain Peace: Fewer headaches from gut-brain loops.
When combined with probiotics, it becomes a potent combination—Jimenez frequently pairs them for microbiome resets (Jimenez, 2023).
Blending Chiropractic with Other Gut-Healing Tools
Chiropractic isn’t a solo approach; it often teams with diet and supplements. Eat anti-inflammatory foods like salmon and greens to feed beneficial bacteria (Flint Rehab, 2023). Probiotics, such as Lactobacillus, help rebuild diversity by reducing cytokines (Li et al., 2024).
Nutrient Power: Omega-3s and fibers repair leaks.
Stress Soothers: Yoga plus adjustments amp vagal calm.
Med Check: Swap gut-hurting pills for gentler options.
Jimenez emphasizes the importance of personalization: “Tailor care to the patient’s axis—test microbiome, adjust spine, track progress” (Jimenez, 2023). This holistic approach aligns with studies on enteral nutrition following TBI (Zhang et al., 2024).
Long-Term Outlook: Healing the Gut for Lasting Brain Gains
Gut fixes post-TBI pay off big. Early action reduces chronic risks, such as neurodegeneration (Wang et al., 2021). Patients with balanced microbiomes show better memory and mood years out (Hassan et al., 2020).
Future paths? More trials on chiropractic for TBI patients, according to experts (Psychology Today, 2025b). Jimenez pushes for integrated clinics: “Chiro plus gut therapy—it’s the future for TBI survivors.”
Wrapping Up: Take Charge of Your Gut-Brain Health
TBI disrupts the gut-brain axis, but knowledge and action can help rebuild it. From leaky gut to dysbiosis, these hits cause real pain—but chiropractic offers a gentle reset. Start with a check-up, tweak your plate, and align your spine. Your body thanks you.
Dhar, R., et al. (2024). Dysregulated brain-gut axis in the setting of traumatic brain injury: Review of mechanisms and anti-inflammatory pharmacotherapies. PMC, 11083845. https://pmc.ncbi.nlm.nih.gov/articles/PMC11083845/
Brain Injury Risks in Martial Arts: Understanding Dangers and Recovery Paths
Martial arts, such as mixed martial arts (MMA), combine striking, grappling, and high-energy moves. These sports draw millions of fans and fighters worldwide. But they come with real risks to the brain. Repeated hits to the head can cause short-term problems like dizziness and confusion. Over time, these can lead to bigger issues, such as memory loss or even diseases like chronic traumatic encephalopathy (CTE). This article examines these dangers and how integrative chiropractic care can aid fighters in their recovery. It draws on studies and expert views to demonstrate why early action is crucial.
The rise of MMA has made it one of the fastest-growing sports. Fighters train hard, often taking hundreds of blows in a single session. While gloves and rules help, the brain still takes a hit. Research shows that even light taps can add up, altering how the brain functions (Bernick et al., 2015). Fighters need to know the signs and seek care fast. This knowledge can save careers and lives.
Short-Term Symptoms: What Happens Right After a Hit
When a fighter lands a punch or kick to the head, the brain inside the skull shakes. This jolt can cause a concussion, a type of traumatic brain injury (TBI). Short-term symptoms can develop rapidly and persist for days or weeks.
Vertigo and Dizziness: Fighters often feel the room spin. This comes from the inner ear and brain signals getting mixed up. Balance issues make simple tasks, such as walking, difficult.
Disorientation and Confusion: Right after a blow, a fighter might not know where they are or what just happened. This “fog” can last minutes to hours.
Headaches and Nausea: Sharp pain in the head pairs with an upset stomach. Lights and sounds feel too loud, adding to the stress.
Fatigue and Sleep Changes: Even after rest, fighters often feel exhausted. They might sleep too much or struggle to fall asleep.
These signs show the brain needs time to reset. In MMA, knockouts (KOs) or technical knockouts (TKOs) are common. A study of over 800 UFC fights found 13% ended in KOs and 21% in TKOs, mostly from head strikes (Babić et al., 2014). During a TKO, a fighter takes about 18 head hits in the last 30 seconds. That’s a lot for the brain to handle at once.
Dr. Alexander Jimenez, a chiropractor with over 30 years of experience in sports medicine, frequently sees these symptoms in his clinic. He notes that many fighters push through the pain, thinking it’s just part of training. However, ignoring early signs can exacerbate the situation (Jimenez, 2024a). His patients report quick relief from gentle adjustments that ease neck tension tied to these issues.
Medical teams at fights check pupils and ask basic questions to spot problems. If a fighter blacks out for more than 30 seconds, it’s a red flag. They might need scans to rule out bleeding (Fagan, 2020). Rest is key here—no sparring until cleared.
Long-Term Repercussions: The Hidden Cost of Repeated Hits
The real worry starts after many fights. Each hit, even if it doesn’t knock you out, chips away at brain health. Over the years, this has led to cognitive slowdown and diseases like CTE.
Cognitive Impairment: Memory slips and trouble focusing become normal. Fighters might forget training moves or struggle with decisions in the ring.
Slower Processing Speed: The brain takes longer to react. This shows up in tests where fighters with more bouts score lower (Bernick et al., 2015).
Neurodegenerative Disorders like CTE: CTE builds up from repeated trauma. It causes protein clumps in the brain, leading to mood swings, aggression, and dementia later in life (Meehan et al., 2019).
Studies link exposure to fighting to smaller brain parts, such as the thalamus, which is involved in thinking and movement. One review found 58% to 78% of MMA injuries involve the head, raising CTE odds (Stern et al., 2021). Women might face extra risks due to longer fights and more head strikes per minute (Kavanagh et al., 2022).
Psychological effects grow, too. Anxiety and depression hit hard, with 33% of TBI patients facing major mood issues in the first year (Reis, 2023). Behavioral changes, such as snapping at loved ones, can strain relationships. Physically, tremors and poor balance make daily life tough.
A survey of MMA fighters showed over 60% worry about brain damage. One vet in his 30s noticed stuttering and word loss after years of sparring (Rogers, 2020). CTE cases, like Gary Goodridge’s in 2012, highlight the stakes—no cure exists, only prevention.
Dr. Jimenez observes similar patterns among martial artists. In his practice, he uses functional assessments to spot early decline. He stresses that starting care soon can slow progression (Jimenez, 2024b).
Psychological, Behavioral, and Physiological Effects Over Time
Brain injuries don’t stay in one spot—they spread. Psychological strain increases when fighters begin to doubt their skills. Behavioral shifts, such as increased aggression, can end careers outside the ring.
Psychological Toll: Depression and panic attacks are common. Fighters feel isolated, hiding symptoms to stay competitive.
Behavioral Changes: Impulse control fades, leading to risky choices. Irritability spikes, affecting team dynamics.
Physiological Shifts: Sleep disruption, hormone imbalance, and the body heals more slowly. This cycle feeds more injuries.
These effects worsen with time. A video on concussions notes that most gym coaches miss signs, letting issues grow (Concussions in Combat Sports, 2023). The National Institute of Neurological Disorders and Stroke lists long-term risks like post-traumatic dementia from even mild hits (National Institute of Neurological Disorders and Stroke, 2023).
Fighters report feeling “off” after sessions, with speech changes that fade only after breaks (Rogers, 2020). Physiological changes include less blood flow to the brain, starving cells of oxygen.
Dr. Jimenez incorporates mental health assessments into his treatment plans. His holistic approach, which combines nutrition and therapy, helps patients rebuild their confidence (Jimenez, 2024a).
How Integrative Chiropractic Care Steps In
Integrative chiropractic care provides a comprehensive approach to addressing brain injuries. It goes beyond pain meds, targeting the spine-brain link. Chiropractors, such as Dr. Jimenez, use hands-on methods to realign the body and enhance healing.
This care mixes adjustments, therapy, and lifestyle tips. It’s safe, drug-free, and works in conjunction with doctors for optimal results (Carr Chiropractic Clinic, n.d.). For martial artists, it means a faster return to training without the risk of re-injury.
Symptom Relief: Manipulation cuts headaches and dizziness. Soft tissue work relaxes tight muscles.
Studies back this. Adjustments improve blood flow, key for brain repair (Apex Chiropractic, n.d.). Patients see gains in weeks, not months.
Key Benefits of Chiropractic for Brain Recovery
Chiropractic shines in recovery. It tackles root causes, not just signs. For TBIs, this translates to better long-term outcomes.
Here’s how it helps:
Improved Balance: Neck exercises strengthen stabilizers, reducing the risk of falls. Fighters regain ring control faster.
Increased Cerebrospinal Fluid Circulation: Adjustments clear blockages, flush toxins, and deliver nutrients to the brain.
Stimulation of Brain Neuroplasticity: The brain rewires itself. Gentle pressure sparks new connections, aiding memory and speed.
One clinic reports that patients with concussions experience improved vision and coordination after sessions (Calibration Mansfield, n.d.). Dr. Jimenez utilizes tools such as digital X-rays to track progress, noting quicker healing in athletes (Jimenez, 2024b).
For MMA injuries, care focuses on managing pain and accelerating tissue repair (Turnersville Chiropractic, 2023). It’s holistic—adding diet and exercise for full strength.
Real-World Examples and Expert Insights
Take Paula, a TBI survivor treated at a chiropractic center. After accidents, she battled depression and pain. With adjustments, laser therapy, and balance training, she was able to run half-marathons again (Reis, 2023). Stories like hers show hope.
Dr. Jimenez shares cases of martial artists regaining their agility after injury. His LinkedIn posts highlight non-invasive wins over surgery (Jimenez, 2024b). He teams with therapists for team-based care.
A YouTube doc on fighting concussions stresses protocols. Coaches must identify issues early, and chiropractic care can serve as a first step (Concussions in Combat Sports, 2023).
Prevention Tips for Fighters
Staying safe starts in the gym. Cut heavy sparring and focus on drills. Use better gear and track hits.
Train Smart: Limit head contact. Add brain games, such as puzzles, for protection.
Monitor Symptoms: Log headaches or fog. Rest at the first sign.
Seek Pros Early: Chiropractors identify issues before they become a problem.
Rule changes, such as longer counts after knockdowns, could help (Babić et al., 2014). Fighters own their health—listen to your body.
Why Choose Integrative Care for Lasting Health
Brain risks in martial arts are serious, but recovery is possible. Short-term issues like vertigo typically subside with rest. Long-term threats like CTE require immediate action. Integrative chiropractic bridges the gap, addressing spinal issues and promoting brain repair.
Benefits stack up: better flow, rewiring, and balance. Experts like Dr. Jimenez prove it works for athletes. Don’t wait—start care to fight smarter, not harder.
Bernick, C., Banks, S., Shin, K., & Rao, V. (2015). Repeated head trauma is associated with smaller thalamic volumes and slower processing speed. British Journal of Sports Medicine, 49(15), 1007. https://bjsm.bmj.com/content/49/15/1007
Stern, R. A., et al. (2021). Head injury in mixed martial arts: A review of epidemiology, affected brain structures and risks of cognitive decline. PubMed. https://pubmed.ncbi.nlm.nih.gov/33538222/
What Happens to Your Spine After a Crash, Work Injury, Sports Hit, or Head-First Fall?
The doctor explains to a patient, who may have a head injury from an accident, what happens to the spine after a high-impact collision using a vertebral column model.
Overview: Why high-impact events strain the spine (and sometimes the brain)
When you are involved in a car accident, get hurt at work, collide in sports, or fall and hit your head, your spine absorbs fast, complex forces. These include flexion and extension (bending forward and back), rotation (twisting), lateral bending, and compression (axial loading). Sudden acceleration or deceleration—especially with rotation—can cause joints to move beyond their normal range, resulting in the stretching or tearing of soft tissues. In higher-energy trauma, vertebrae and discs can fail, and the spinal cord can be injured. The result ranges from temporary pain and stiffness to lasting changes in strength, sensation, and autonomic function if the cord is involved (Mayo Clinic, 2024; NINDS, 2025). Mayo Clinic+1
These same rapid movements can also cause brain injury. When the head moves quickly and stops suddenly, the brain can strike the inside of the skull, stretching delicate nerve fibers and triggering a concussion or a more serious traumatic brain injury (TBI). Because the brain and spine share protective bones, connective tissues, cerebrospinal fluid (CSF), and vascular pathways, injury to one often affects the other. Imaging—typically CT for bones and MRI for soft tissues and the spinal cord—helps map what happened, allowing your team to guide safe care (UT Southwestern; Utz et al., 2014). UT Southwestern Medical Center+1
The forces that damage the spine
Hyperextension and hyperflexion: Whipping motions (for example, rear-end collisions) can over-stretch ligaments and joint capsules, irritate facet joints, and provoke muscle spasm—commonly called “whiplash.” In severe cases, hyperextension can fracture the posterior elements of the C2 vertebra (a “hangman’s fracture”) (Torlincasi, 2022). NCBI
Axial compression: A head-first impact loads the spine in a vertical direction. If the neck is slightly flexed, axial compression can cause vertebrae to collapse or a vertebral body to burst. In sports, this mechanism is strongly linked to catastrophic cervical injuries (Boden, 2008). PubMed
Torsion and lateral bending: Twisting and side-bending add shear forces that can tear annular fibers in discs and sprain supporting ligaments.
Deceleration with rotation: High-speed stops—common in crashes—can combine rotation with hyperflexion or extension, increasing the risk of disc herniation, ligament failure, and even vascular injury to the carotid or vertebral arteries (van den Hauwe et al., 2020). NCBI
Common spinal injuries after high-impact events
1) Soft-tissue injuries (strains, sprains, and whiplash)
What happens: Muscles and tendons strain; ligaments sprain. The facet joints can become inflamed; posture and movement patterns change to guard the area.
How it feels: Neck or back pain, stiffness, headaches, limited range of motion, and sometimes dizziness or visual strain.
Why it matters: Even when X-rays are normal, these injuries can disturb joint mechanics and load discs and nerves abnormally, delaying recovery and sometimes causing chronic pain.
2) Disc injuries (bulges and herniations)
What happens: The inner gel of the disc pushes through weakened outer fibers (annulus). A herniation can compress nearby nerves, causing radiating pain, numbness, or weakness.
Symptoms: Sharp neck or back pain accompanied by arm or leg symptoms (radiculopathy). Coughing or sneezing can worsen it.
Evidence Suggests That Disc herniation and nerve irritation are common after rapid flexion-extension and axial loading; severe cases may contribute to cord compression syndromes that require urgent attention (Mayo Clinic, 2024). Mayo Clinic
What happens: Sudden load exceeds bone strength. In the neck, a C2 “hangman’s fracture” is a classic hyperextension injury; other levels can fracture from compression or flexion-distraction.
How it feels: Severe focal pain, limited motion, neurologic changes if nerves are involved.
Evidence: Hangman’s fractures involve bilateral C2 pars/pedicle fractures from extreme hyperextension and deceleration—often diving or motor-vehicle collisions (Torlincasi, 2022). CT rapidly detects fractures; MRI checks ligaments and cord (Utz et al., 2014). NCBI+1
4) Spinal cord injury (SCI)
What happens: The cord, or cauda equina, is damaged by compression, contusion, or transection. Secondary cascades—such as edema, ischemia, and inflammation—can worsen deficits over time.
How it feels: Loss of strength or sensation below the injury, reflex changes, spasticity, balance problems, and bowel/bladder or autonomic dysfunction. Some effects can be permanent (Mayo Clinic, 2024; NINDS, 2025). Mayo Clinic+1
What happens: The carotid or vertebral arteries tear or dissect during high-energy neck trauma, risking delayed stroke.
Why it matters: Complications often occur hours to days after injury. Early identification and timely antithrombotic therapy lower the risk of ischemic events (van den Hauwe et al., 2020). NCBI
Sports, work, and falls: settings that raise risk
Sports: Football, ice hockey, wrestling, diving, skiing/snowboarding, rugby, and cheerleading have the highest risk for catastrophic spinal injuries. Axial loading to the crown of the head with slight neck flexion can cause cervical fracture and quadriplegia in any sport (Boden, 2008). PubMed
Work: Heavy lifting, falls from height, and high-energy impacts around vehicles and machinery threaten the spine.
Falls with head impact: Head-first falls concentrate force into the upper cervical spine and brain, raising the risk of combined neck injury and concussion/TBI (Weill Cornell Medicine Neurosurgery, n.d.; NINDS, 2025). NINDS
The brain–spine connection: why TBIs and spine injuries overlap
Fast acceleration-deceleration events that injure the neck also cause the brain to shake. The brain can bump the skull, causing stretch and shear of axons (diffuse axonal injury). Secondary biochemical cascades—excitotoxicity, oxidative stress, and neuroinflammation—can prolong symptoms such as headaches, dizziness, cognitive impairment, sleep disturbances, and mood changes (Mayo Clinic, 2024; NINDS, 2025). Clinically, many people present with a combined pattern, including neck pain and limited motion, vestibular symptoms, visual strain, and cognitive complaints, all of which occur after the same incident. A coordinated plan that screens for red flags, protects the spine, and addresses vestibular/ocular issues tends to help. Mayo Clinic+1
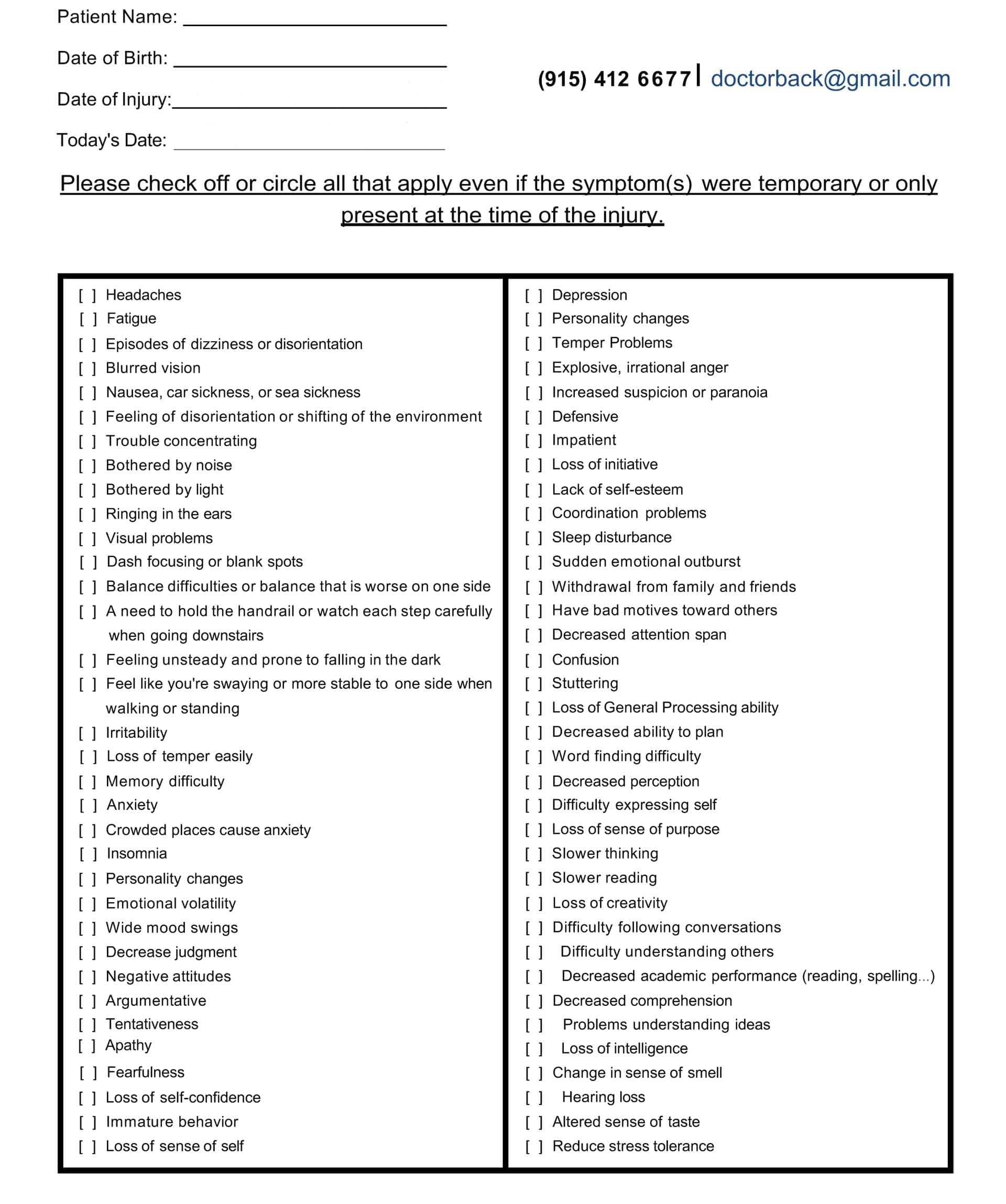
Head Injury/TBI Symptom Questionnaire:
Head Injury/TBI Symptom Questionnaire
How clinicians figure out what’s wrong
History and red-flag screen Loss of consciousness, severe or worsening headache, focal weakness/numbness, gait problems, bowel/bladder changes, saddle anesthesia, midline tenderness, or high-risk mechanism triggers urgent imaging and referral.
Physical and neurological exam Range of motion, palpation, motor/sensory/reflex testing, gait and balance, and provocative maneuvers help localize likely pain generators and nerve involvement.
Imaging strategy
CT quickly detects fractures and acute instability.
MRI is superior for ligaments, discs, cord edema/contusion, and nerve root compression.
Vascular imaging (CTA/MRA) is considered when signs or fracture patterns raise suspicion for BCVI (Utz et al., 2014; van den Hauwe et al., 2020). PubMed+1
Sports and work considerations Return-to-play or return-to-work decisions require symptom-guided progression and objective measures (strength, balance, vestibulo-ocular function, and safe lifting mechanics).
What recovery looks like: evidence-informed options
Acute protection and symptom control: Relative rest from provocative motions, pain-modulating strategies, and careful mobilization as tolerated.
Rehabilitation: A graded plan to restore mobility, strength, coordination, and endurance while protecting healing tissues.
Medication and interventional options: Based on the diagnosis and response, primary care, PM&R, neurology, pain management, or spine surgery may add targeted medications, injections, or consider operative care for unstable injuries or progressive neurological deficits.
Education and pacing: Clear timelines, ergonomic coaching, sleep support, and gradual exposure reduce flare-ups and promote consistent gains.
For moderate-to-severe SCI, long-term rehabilitation focuses on function, adaptive strategies, spasticity management, and prevention of complications; research continues on neuroregeneration and advanced technologies (NINDS, 2025; Mayo Clinic, 2024). NINDS+1
Where integrative chiropractic care fits
Important note: Chiropractic does not treat or reverse spinal cord injury. In an integrative model, chiropractic focuses on the mechanical and neuromusculoskeletal contributors to pain and movement limits, and works alongside medical specialists to co-manage complex cases.
What integrative chiropractic care emphasizes:
Thorough medical screening and referral when needed Chiropractors trained in trauma-informed assessment screen for red flags (neurological deficits, cord compression signs, suspected fracture or BCVI). Concerning findings prompt immediate imaging and referral to emergency, neurology, or spine surgery (UT Southwestern; Utz et al., 2014). UT Southwestern Medical Center+1
Gentle, graded manual care For appropriate cases (after imaging or when clinical decision rules indicate safety), joint mobilization or carefully selected adjustments may reduce painful joint restriction, improve movement, and support posture. Soft-tissue therapy helps calm protective spasm and restore glide.
Sensorimotor retraining Cervical stabilization, scapular control, proprioceptive drills, and graded vestibular/oculomotor exercises can help reduce dizziness, improve gaze stability, and normalize head–neck control patterns that often persist after crashes and sports impacts (UT Southwestern; Dr. Jimenez, 2025). UT Southwestern Medical Center+1
Posture, breathing, and load-management Rib-cage mechanics, diaphragmatic breathing, and dynamic posture training lower strain on the neck and lower back during daily tasks and lifting (Dr. Jimenez, 2025). El Paso, TX Doctor Of Chiropractic
Circulation and CSF considerations (clinical observation) Some integrative chiropractic programs incorporate strategies to optimize cervical mobility and thoracic outlet mechanics as part of a comprehensive plan that supports fluid dynamics and symptom relief. This is a developing area; clinicians should avoid over-promising benefits in serious neurological disease. In Dr. Jimenez’s clinic, CSF flow is considered within a broader framework of posture and movement for symptom-driven care (Jimenez, 2025). El Paso, TX Doctor Of Chiropractic
Whole-person coordination Chiropractors and nurse practitioners (NPs) can coordinate with PM&R, neurology, radiology, physical therapy, and behavioral health to align goals, including restoring motion, quieting pain, normalizing movement patterns, and supporting a return to activity. Dr. Alexander Jimenez, DC, APRN, FNP-BC, documents these collaborative pathways in his clinical articles and patient education resources (Jimenez, 2025). El Paso, TX Doctor Of Chiropractic+2 El Paso, TX Doctor Of Chiropractic+2
Step-by-step recovery roadmap (what a typical plan may include)
Day 0–7: Protect and clarify
Red-flag screen; order imaging when indicated.
Calm pain and inflammation; protect the neck/back from high loads.
Begin gentle motion (as tolerated) to avoid stiffness.
If a concussion/TBI is suspected, initiate a symptom-paced, relative rest plan with light activity and screen time limits; add vestibular/ocular drills as appropriate.
Weeks 2–6: Restore motion and control
Progress manual care (mobilization/adjustment as appropriate).
Sports safety insight: Catastrophic neck injuries often occur with axial loading to the crown in slight neck flexion. Coaching “heads-up” posture and avoiding head-first contact reduces risk (Boden, 2008). PubMed
Special situations that need immediate care
Progressive weakness, numbness, or trouble walking
Bowel or bladder changes; saddle anesthesia
Severe midline spine tenderness after high-risk trauma
Suspected fracture or dislocation
Stroke symptoms after neck trauma (possible BCVI): sudden one-sided weakness, facial droop, vision/language changes, or severe new headache—call emergency services (van den Hauwe et al., 2020). NCBI
Dr. Alexander Jimenez’s clinical observations (El Paso, TX)
Drawing from a dual-scope practice as a Doctor of Chiropractic and Board-Certified Family Nurse Practitioner, Dr. Jimenez highlights:
Early triage matters: identify red flags and co-manage quickly with imaging and specialty referrals when indicated.
Gentle first, then graded: start with low-load mobility and stabilization; add manual care and progressive loading as tissues tolerate.
Sensorimotor work is a staple: vestibular/ocular drills, as well as balance training, help patients with combined neck pain and concussion symptoms move forward.
High-impact events stress the spine through flexion/extension, rotation, and compression—causing soft-tissue injury, disc herniation, fractures, and, in severe cases, spinal cord injury.
The same forces often injure the brain; combined neck and concussion symptoms are common after crashes and sports impacts.
CT and MRI complement each other: CT for bone, MRI for ligaments, discs, cord, and nerves; screen for BCVI when red flags or fracture patterns suggest vascular risk.
Integrative chiropractic care involves a team-based approach, which includes carefully screening patients, using gentle manual methods when appropriate, retraining movement and balance, and collaborating with medical specialists.
With a clear roadmap and coordinated care, most people improve and return to their normal activities. For severe SCI, long-term rehabilitation and assistive strategies remain essential.
How Head Trauma Can Trigger Sciatica: The Hidden Link and Ways to Heal
A doctor of chiropractic explains to an automobile accident patient how a head injury can cause sciatica and lower back problems.
Head injuries can occur in car crashes, sports-related falls, or everyday slips. They shake the brain and body in ways you might not expect. One surprising outcome? Sciatica. That’s the sharp pain shooting down your leg from a pinched sciatic nerve. Many people don’t connect a bump on the head to that nagging leg ache. However, science reveals a clear connection between the two. This article breaks it down simply. We’ll explore how head trauma messes with your spine and nerves. We’ll also cover how gentle chiropractic care can help ease pain and speed up recovery. If you’ve had a head injury and now feel leg pain, this could explain why—and what to do next.
What Is Head Trauma and How Does It Relate to Sciatica?
Head trauma means any blow to the skull that jars the brain. It ranges from mild concussions to severe traumatic brain injuries (TBI). A concussion might leave you dizzy for days. A serious TBI could mean hospital stays and long-term changes. These injuries don’t just affect thinking. They ripple through the whole body.
Sciatica is a type of pain caused by the sciatic nerve. This nerve starts in your lower back and runs down each leg. It’s the longest nerve in your body. When irritated, it causes burning, tingling, or shooting pain from the butt to the foot. Common causes include herniated discs or tight muscles. But head trauma adds a twist. It can trigger changes deep within your nervous system that lead to nerve trouble.
Studies show that up to 78% of TBI survivors deal with ongoing pain. That includes back and leg aches, such as sciatica. Why? The brain controls everything, including how your spine moves. A head hit disrupts that control.
Dr. Alexander Jimenez, a chiropractor in El Paso, Texas, frequently observes this phenomenon in his clinic. As a Doctor of Chiropractic and Nurse Practitioner, he treats patients after accidents. He notes that head trauma often hides as simple bumps but leads to widespread pain. In his observations, many patients come in with leg pain that they attribute to old falls or crashes. His team uses functional medicine to trace the issue back to the brain-spine connection.
How Head Trauma Alters Brain Control Over Spinal Muscles
Your brain is like a boss for your muscles. It sends signals down the spinal cord to maintain balance. Head trauma throws that off. A TBI damages brain areas that regulate movement. This leads to spasticity—tight, jerky muscles in the legs and back.
Think of it this way: Normally, your brain tells spinal muscles to relax and stretch smoothly. After a head injury, those signals glitch. Muscles in the lower back get out of sync. They pull unevenly on the spine. Over time, this puts strain on the sciatic nerve roots as they exit the lower back.
One study found that mild TBIs cause extra sensitivity in the legs. It’s as if the brain amplifies pain signals through chemicals called chemokines. These build up in the spinal cord, making nerves fire too easily. For sciatica, this means even small movements cause more pain.
Dr. Jimenez observes this in athletes after concussions. “Patients tell me their legs feel heavy, like they’re fighting their own body,” he shares in his wellness podcasts. His clinic uses nerve tests to spot these glitches early. By addressing them, they prevent the pain from becoming chronic.
This muscle chaos doesn’t stop at the back. It can weaken core support, leading to poor posture. Slouching adds pressure on the sciatic nerve. It’s a slow build, but real.
Head Injury/TBI Symptom Questionnaire:
Head Injury/TBI Symptom Questionnaire
Misalignment and Muscle Impairment: Irritating the Sciatic Nerve
Head trauma often hits the neck hard. The force whips the head forward and back—like in a car crash. This misaligns the upper spine, particularly the top vertebrae, known as the atlas and axis. That misalignment travels down like a domino fall.
Impaired muscles from brain signals exacerbate the condition. Tight neck muscles pull the spine off-kilter. In the lower back, this squeezes discs and nerves. The sciatic nerve can become pinched between bones or become inflamed. Result? That classic leg zap.
Research backs this. Up to 8% of severe TBI cases come with spine injuries. Even mild ones raise the risk. A study on 180 patients showed that older folks or those with low consciousness scores face higher odds. The neck shift stresses the whole chain, irritating the sciatic nerve.
Concussions alone can spark lower back pain. The brain’s balance center gets knocked. Muscles overwork to compensate, tiring the back. Dr. Jimenez refers to this as the “cascade effect” in his LinkedIn posts. He treats it with targeted adjustments to reset muscle tone.
Raising the Risk of Further Spinal Damage
Head trauma doesn’t just irritate—it invites more trouble. A damaged brain means slower reflexes. You might stumble more easily, leading to falls that jar the spine again. Plus, inflammation from TBI spreads. It swells the tissues around the spine, causing the discs to bulge and the nerves to become vulnerable.
One key risk: Concomitant injuries. That’s when head and spine hits happen together. In motor vehicle crashes—the top TBI cause—neck strains often tag along. This doubles the chance of disc slips that pinch the sciatic nerve.
Dr. Jimenez observes this in patients involved in car accidents. “A rear-end collision jars the brain and twists the lumbar spine,” he explains in his functional medicine series. His observations show early chiropractic checks cut re-injury risks by improving stability.
The Role of Swelling and Heterotopic Ossification in Nerve Crushing
TBI triggers swelling fast. Brain tissue bruises, and fluids build up. This chaos can spread to the body. In rare but serious cases, it leads to heterotopic ossification (HO). That’s when bone grows in soft tissues—like muscles or around nerves.
Around the sciatic nerve, HO is sneaky. It starts after hip or pelvic trauma, tied to the head hit. Scar tissue hardens into bone, encasing the nerve. Over months, this crushes it. Symptoms creep in: Numbness, weakness, foot drop.
A case report described a young man following traumatic brain injury (TBI). Seventeen months later, bilateral sciatic entrapment from hip HO caused severe pain. Surgery freed the nerve, but prevention is key. Anti-inflammatory drugs or radiation cut HO risks.
Dr. Jimenez warns of this in his injury recovery blogs. He uses imaging to identify early signs of HO in TBI patients with leg pain. His integrative plans include nutrition to fight inflammation and slow bone overgrowth.
Upper Neck Misalignment: Starting a Pain Cascade to the Sciatic Nerve
The upper neck is ground zero for many head traumas. Whiplash from falls or sports bends it unnaturally. This throws off the atlas—the top bone. It shifts pressure down the spine.
The cascade? Misaligned neck pinches nerves there. Signals to the lower back get scrambled. Muscles tighten unevenly, pulling on the lumbar joints. This stresses the sciatic nerve roots, causing inflammation and pain.
Inflammation plays a big role. Concussion swelling in the neck disrupts blood flow and nerve signals, causing significant complications. It causes the brain to misread pain, amplifying the sensation of hurt in the leg.
Dr. Jimenez’s clinical notes highlight this in veterans with whiplash-TBI. “Neck shifts create a domino pain chain,” he says. His team uses precise X-rays to map it, then adjusts to break the cycle.
Integrative Chiropractic: A Path to Relief and Recovery
Integrative chiropractic blends hands-on care with wellness tools. It’s perfect for post-head injury sciatica. No drugs or surgery—just realignment and support.
First, it realigns the spine. Gentle adjustments fix neck and back shifts. This eases nerve pressure fast. For sciatica, lumbar tweaks reduce the disc bulge on the nerve.
Second, it boosts nervous system function. Adjustments reduce interference, allowing brain signals to flow more smoothly. This calms spastic muscles and dials down pain sensitivity.
Third, it fights inflammation. Soft tissue work, like massage, releases tight spots. Add nutrition advice, including anti-inflammatory foods, and use swelling drops.
Finally, it restores cerebrospinal fluid (CSF) flow. CSF cushions the brain and spine. Trauma clogs it, raising pressure. Craniosacral therapy—light touches on the skull and sacrum—clears the path. Patients report clearer heads and less pain.
Dr. Jimenez integrates all this. His clinic mixes adjustments with functional tests. “We trace sciatica back to the head hit, then rebuild from there,” he observes. Patients who have been in accidents often experience mobility gains within weeks. One testimonial: A crash survivor ditched leg braces after targeted care.
Studies agree. Chiropractic reduces TBI pain by 50% in some individuals. For post-concussion, it eases dizziness and back aches.
Real-Life Stories and Expert Tips
Take Sarah, a soccer player Dr. Jimenez treated. A header caused a concussion and later sciatica. Adjustments realigned her neck, easing leg pain. Now she plays pain-free.
Tips from experts: Start care early. Get imaging if pain lingers post-injury. Pair chiropractic care with rest and omega-3 fatty acids for managing inflammation.
Wrapping It Up: Take Control of Your Recovery
Head trauma to sciatica seems far-fetched, but the links are strong. From brain glitches to bone growth, it stresses the sciatic nerve. Integrative chiropractic offers hope—realigning, calming, and healing.
Don’t ignore the signs. See a pro like Dr. Jimenez for a check. Your body can bounce back stronger.
How Head Injuries Affect Movement—and How Chiropractic Care Gives It Back
A physiotherapist is conducting a consultation on a possible traumatic brain injury; the patient complains of back pain and mobility problems.
Head injuries and traumatic brain injuries (TBIs) can turn simple steps into big challenges. A fall, a car crash, or a sports hit can damage the brain and the nerves that tell your body how to walk, reach, or stand tall. This guide explains exactly how these injuries cause muscle fatigue, shaky balance, stiff joints, and even paralysis. You will also learn how gentle chiropractic adjustments, soft-tissue work, and targeted exercises help people move better, feel less pain, and live fuller lives.
What Happens Inside the Body After a Head Injury
When the skull jolts, the brain bounces inside. That sudden movement can tear tiny nerve wires and swell delicate tissues. The messages that once zipped from brain to legs now arrive late, weak, or not at all (Model Systems Knowledge Translation Center, 2023).
Muscle Fatigue Hits Fast
Even mild TBIs make muscles tire in minutes instead of hours. A short walk to the mailbox can feel like a marathon. Dr. Alexander Jimenez, a chiropractor and nurse practitioner in El Paso, Texas, sees this every week. “Patients tell me their legs feel like wet sandbags after five minutes of standing,” he says in his clinic videos (Jimenez, 2025).
Balance Becomes a Wobbly Game
The brain’s balance center sits deep inside the cerebellum. When it gets bruised, the ground seems to tilt. People sway, stumble, or freeze in place. One study found that even “mild” head injuries change walking patterns enough to raise fall risk by 50% (Brain Injury Association of America, 2024).
Coordination Turns Clumsy
Reaching for a coffee cup can knock over the whole table. Fine finger skills vanish. Buttons stay undone, handwriting turns shaky, and stairs feel like mountains. Physiopedia refers to this as “loss of motor dexterity” (Physiopedia, 2024).
Pain and Tiredness Make Everything Worse
Chronic headaches, neck pain, and shoulder aches are common after TBIs. When pain flares, muscles guard and stiffen. Add normal daily fatigue, and movement shuts down completely (Irvine, 2023).
Symptom Questionnaire:
From Stiffness to Locked Joints: The Contracture Trap
If a person rests too much to avoid pain, muscles shorten like dried rubber bands. Joints freeze. Doctors call these locked positions contractures. Elbows, knees, and ankles can bend only a few degrees. Contractures typically develop within weeks and become permanent within months if left untreated (Physiopedia, 2024).
Headway, a UK brain-injury charity, warns: “Lack of movement is the biggest enemy of recovery” (Headway, 2023).
How Chiropractic and Integrative Care Unlock the Body
Chiropractors do more than crack backs. They use gentle moves, hands-on muscle work, and brain-retraining exercises to restart motion and calm pain.
1. Spinal Adjustments Re-Open Nerve Highways
Misaligned neck bones pinch nerves that control arms and legs. A precise chiropractic adjustment lifts that pressure. Blood and cerebrospinal fluid flow better. Patients often feel looser the same day (Northwest Florida Physicians Group, 2023).
Dr. Jimenez films before-and-after videos: one patient who dragged her foot for two years took ten smooth steps after three visits (Jimenez, 2025).
2. Soft-Tissue Therapy Melts Tight Muscles
Fascia—the thin sleeve around every muscle—can knot after injury. Chiropractors use tools and fingers to smooth these knots. Shoulders drop, necks turn, and hips swing again (Function First, 2024).
3. Balance Boards and Eye-Tracking Drills Rewire the Brain
Simple wobble boards teach the brain to steady the body. Following a finger with the eyes rebuilds coordination pathways. These “neuro-drills” are fun and fast. Most patients notice steadier steps in four weeks (HML Functional Care, 2024).
4. Stretching Plans Stop Contractures Before They Start
Daily 10-minute routines keep joints supple. A chiropractor demonstrates the exact angle and hold time to ensure muscles lengthen safely (NR Times, 2024).
5. Posture Fixes End Headache Cycles
Slumped shoulders strain the neck and starve the brain of oxygen. One posture taping session plus two adjustments can cut headache days in half (Cognitive FX, 2024).
Real Stories That Prove It Works
Mark, age 34, car crash survivor “I couldn’t lift my toddler. After six weeks of chiropractic care, I carried her across the park.” (Patient testimonial, Apex Chiropractic, 2024)
Sarah, age 19, soccer concussion “Balance boards felt silly—until I walked the graduation stage without my cane.” (Crumley House, 2024)
Midday 10-minute walk with trekking poles, Soft-tissue massage on tight calves
Evening Wobble-board “surfing” while brushing teeth, Gentle foam-roll under guidance
Follow this for 90 days, and most people regain 70–80% of normal motion (Impact Medical Group, 2024).
When to See a Chiropractic Neurologist
Look for these red-flag signs:
Your legs drag or cross when you walk
Arms stay glued to your sides
You fall more than once a month
Painkillers no longer help
A chiropractic neurologist assesses your gait on video, tests eye reflexes, and develops a customized plan (NeuroChiro, 2024).
Science Backs the Gentle Touch
A 2022 review of 14 studies found that spinal adjustments, combined with exercise, reduced TBI pain by 41% more than exercise alone (Jimenez, 2025). Another trial showed that balance scores increased by 28 points in eight weeks with integrative care (PMC, 2022).
Safe, Drug-Free, and Covered by Many Insurances
Chiropractic care for head injuries is a non-invasive approach. No needles, no scalpels, no opioids. Most auto-insurance PIP plans and major health plans pay for 12–20 visits (Sam’s Chiropractic, 2024).
Your Next Step Today
Call a local chiropractor who lists “TBI” or “concussion” on their website.
Bring a 1-page list: “I trip, my left knee locks, headaches every afternoon.”
Traumatic Brain Injury Recovery: Effective Exercises and Chiropractic Care for Head Injuries
Rehabilitation exercises after an auto accident with head injuries.
Traumatic brain injury, or TBI, happens when a strong hit to the head harms the brain. This can come from falls, car crashes, sports, or other accidents. Head injuries are much like TBIs because they often involve the same kinds of damage to the brain and body. Recovery from these injuries requires time and effort. It focuses on getting back physical strength, mental sharpness, and balance. Rehabilitation utilizes a combination of exercises to aid recovery. These include activities that get the heart pumping, build muscle, improve steadiness, and sharpen the mind. Chiropractic care can also play a significant role, particularly in addressing issues such as headaches and dizziness. This article examines ways to recover, with a strong focus on training and improving step by step.
People with TBI or head injuries often face problems like pain, trouble moving, forgetfulness, or feeling off-balance. Starting recovery early is crucial, but it must be done slowly and safely. Doctors and therapists guide the process. Exercises help the brain rewire itself through something called neuroplasticity. This means the brain can create new pathways to repair damaged ones. Training helps build these paths. Recovery is not limited to a single type of exercise. It combines various types to cater to all needs. Let’s dive into the details.
Physical Exercises for Strength and Aerobic Health
Physical exercises are a big part of getting better from TBI or head injuries. They help rebuild muscle, boost energy, and enhance overall bodily function. Start slow because rushing can cause more harm. Always check with a doctor first.
Aerobic activities get the heart rate up without too much strain. Walking is a simple start. It can be done inside or outside, and it helps blood flow to the brain. This brings oxygen and nutrients for the healing process. Jogging on a treadmill or using a stationary bike are other options. Swimming is great too because the water supports the body, making movement easier. Aim for 150 minutes a week of moderate aerobic work, spread out over days. This could be 20 to 40 minutes per session, three to four times a week. These activities lower the risk of other health issues like heart problems or diabetes, which can slow recovery. They also lift mood and reduce tiredness.
Strength training builds muscle power. This is important because injuries can weaken muscles. Squats are a good exercise. Stand with your feet apart, as if your shoulders are wide, bend your knees as if sitting back in a chair, then stand up. Do this 10 times. Rows work the back and arms. Sit or stand, pull your elbows back like squeezing something between your shoulder blades. Use light weights or resistance bands if possible. Bicep curls are simple: Hold a water bottle, bend your elbow to bring it to your shoulder, then lower it. Repeat 10 times per arm. For legs, try seated marching. Sit in a chair and lift one knee up, then the other, like walking in place. These exercises help with daily tasks, such as getting up from a chair or carrying objects.
Other strength moves include push-ups against a wall or chair for the chest and arms. Shoulder presses: Lift arms overhead with light weights. Do these in sets, with rests in between. Strength training should be done two to three times a week, focusing on the larger muscle groups. It helps with posture and stops falls. As you become stronger, add more reps or increase the weight. But listen to your body. If it hurts, stop and rest.
Seated exercises are beneficial for individuals who are unable to stand or walk. Seated hip rotations: Sit and turn your hips side to side. This builds core strength. Alternating heel-toe raises: Lift your heels, then your toes, while sitting. These improve lower-body control and blood flow. Arm push: Push a bottle across a table with your wrist. This strengthens arms without much effort. Mixing aerobic and strength training keeps the workout fun and covers more ground for recovery.
Balance Exercises to Regain Stability
Balance problems are common after TBI or head injuries. They can cause falls and make walking hard. Balance training helps the brain and body work together better. It uses neuroplasticity to fix these issues.
Tandem stance is a basic exercise. Stand with one foot right in front of the other, like on a tightrope. Hold for 30 seconds, then switch feet. If it’s too hard, spread feet wider. Close your eyes to make it tougher once you’re ready. Weight shifts: Stand with your feet apart, shift your weight to one side, and lift the other foot slightly. Hold 30 seconds per side. This builds steadiness.
Romberg stance: Stand with feet together, eyes closed. Hold as long as you can, up to two minutes. It trains the body to use senses apart from sight for balance. Alternating heel-to-toe raises: Stand and rise on your toes, then rock back onto your heels. Do it 10 times. This strengthens legs and improves coordination.
For more challenge, use tools. A gym ball: Sit on it and reach for objects. This makes the surface unstable, forcing better control. Balance boards: Stand on a wobbly board and try not to lose your balance. Start with help. Walking on various surfaces, such as grass or sand, trains the body to adapt.
Vestibular exercises help with dizziness. These include head turns while focusing on a point, as well as eye movements such as following a finger. They retrain the inner ear and brain. Do balance work daily, but in short sessions to avoid fatigue. Progress slowly from a seated to a standing position. Good balance means safer movement and less fear of falling.
Mix balance with other training. For example, do squats while on one leg. Or walk while turning your head. This makes exercises more realistic. Recovery improves when training mimics daily activities.
Cognitive Exercises for Mental Sharpness
Mental skills can be affected after TBI or head injuries. Aspects such as memory, focus, and problem-solving require improvement. Cognitive exercises challenge the brain to build new connections.
Try new things: Walk a different path or try a new food. This sparks neuron growth. Use your non-dominant hand for tasks such as brushing your teeth. It activates the other side of the brain and strengthens thinking. Brain-training games: Play chess, Sudoku, or apps like Lumosity. These improve logic and memory.
Memorization: Recall a grocery list or song lyrics. Start small and build up. Draw maps from memory, like your route to the store. This boosts spatial thinking. Read out loud: It works reading, speaking, and listening parts of the brain.
Puzzles and games: Jigsaw puzzles or board games like Connect Four help develop planning and hand-eye coordination skills. Mental math: Add numbers in your head or count backwards by sevens. Keep a journal of senses: Note what you see, hear, and smell each day. This mixes memory and senses.
Start slow with easy tasks. Increase difficulty as you improve. Do 15-20 minutes a day. Combine with physical exercises for a complete recovery. Cognitive training helps with daily life, like remembering names or following recipes.
Integrative Chiropractic Therapy for Support
Chiropractic care helps with TBI and head injury recovery. It focuses on the spine and nervous system. This can help alleviate headaches and dizziness caused by injuries.
Adjustments align the spine, reducing nerve pressure. This improves blood flow to the brain and cuts inflammation. Craniosacral therapy: Light touch on the head and spine boosts fluid flow around the brain. It helps with headaches and brain function.
Chiropractors offer lifestyle tips, such as healthy eating and adequate sleep. They also suggest exercises, such as those for strength and balance. Combining chiropractic care with physical therapy can accelerate recovery. It addresses both body and mind.
For long-term care, regular visits prevent chronic pain. Chiropractic supports neuroplasticity by stimulating the nervous system. It’s non-invasive and can be used in conjunction with other treatments.
Insights from Dr. Alexander Jimenez
Dr. Alexander Jimenez, a chiropractor with over 30 years of experience, shares observations on TBI and head injuries. He uses integrative care for recovery. His work includes functional medicine to fix root causes. For injuries, he emphasizes the importance of prompt action with rehabilitation programs. These include exercises for mobility and nerve health. He helps with symptoms like pain and weakness through adjustments and nutrition. His clinic focuses on achieving full healing without the use of drugs or surgery.
Jimenez notes that personalized plans are most effective. He combines chiropractic with exercises to boost recovery. His insights demonstrate how training can rebuild strength and function after head injuries.
Putting It All Together for Recovery
Recovery from TBI or head injuries needs a mix of exercises and care. Focus on training: Do aerobic exercises for heart health, strength training for muscles, balance training for stability, and cognitive exercises for the mind. Add chiropractic for extra support. Start slow, be consistent, and track progress. With time, these steps lead to a better quality of life.
Always work with pros. Recovery is a journey, but training makes it possible.
Healing After a Head Injury: How Your Body Can Recover with the Right Team
Your son sustained a severe blow during Friday-night football. Your wife walked away from a three-car pile-up. Your husband fell 12 feet off a scaffold. All three left the hospital with the same three letters: TBI – traumatic brain injury. The doctor said, “Go home and rest.” But two weeks later, the headaches, foggy thinking, and stomach troubles are worse. You feel lost. This article is written for you – the person healing, the family member searching at 2 a.m., and the nurse, coach, or therapist who wants to help.
We will walk through:
What really happens inside the skull in the first minutes, hours, and weeks?
Why does the damage keep spreading if no one stops the “second wave”
How a whole-body team – including chiropractic nurse practitioners (CNPs) – can turn the tide.
Simple daily steps you can start tomorrow.
Let’s begin where the injury begins.
The Two Waves That Steal Recovery
Wave 1: The First Hit (Primary Injury)
A helmet-to-helmet tackle, a steering wheel to the forehead, or a beam to the hard hat cracks open brain cells in an instant. Blood vessels tear. The skull may stay whole, but the soft brain bounces like gelatin in a jar. This is the damage everyone sees on the CT scan (Missouri University of Science and Technology, 2025).
Wave 2: The Hidden Fire (Secondary Injury)
The real thief shows up later. Four chemical storms start inside the brain and body:
Excitotoxicity – Too much glutamate (brain messenger chemical) pours out. Neurons fire relentlessly until they burn out (Waters, 2023).
Oxidative stress – Tiny sparks called reactive oxygen species (ROS) act like rust on brain wires (Gharavi et al., 2023).
Neuroinflammation – Immune cells rush in to help, but stay too long and attack healthy tissue (Simon et al., 2017).
Gut-brain meltdown – The gut lining leaks, bad bacteria cross into the blood, and the brain swells even more (Heuer Fischer, 2024).
These four storms can last weeks, not hours. One mouse study showed that brain toxins still remained elevated 7 days after the crash (Missouri University of Science and Technology, 2025). That is why “I feel worse at week three” is so common.
Real People, Real Storms
Jake, 17, linebacker – Cleared to play after 10 days. By week four, he had forgotten his homework, snapped at his mom, and thrown up every morning. Gut-brain tests showed that no good bacteria remained.
Maria, 34, Uber driver – Whiplash plus airbag to the temple. Doctors only checked her neck X-ray. Six months later, she still can’t balance her checkbook. Blood tests revealed extremely high levels of inflammation markers.
Carlos, 42, roofer – The hard hat saved his life, but it could not protect him from the diffuse twist inside his body. His wife noticed he cried at commercials and slept 14 hours a day. His oxidative stress score was triple the norm.
All three were told, “It’s just a concussion. Wait it out.” Waiting lets the second wave win.
Symptom Questionnaire:
The Blood-Brain Barrier: Your Skull’s Broken Gate
Think of the blood-brain barrier (BBB) as a velvet rope around a VIP club. After TBI, it rips. Proteins and water leak in, causing brain swelling (edema). Two kinds matter:
Cytotoxic edema – Cells drink too much water and burst.
Vasogenic edema – The rope is cut; everything floods the dance floor (Kuriakose & Uzunova, 2023).
Swelling squeezes healthy areas. Memory, mood, and movement shut down. MRI may still look “normal” because standard scans miss these tiny leaks.
The Gut-Brain Highway No One Talks About
Your gut has more nerve endings than your spinal cord. After TBI:
Stress hormones crash.
Good bacteria die.
The gut wall gets holes.
Toxins ride the vagus nerve straight to the brain.
Result? Anxiety, constipation, and brain fog that no pill fixes (Heuer Fischer, 2024). Heal the gut, calm the brain.
Meet the Team That Sees the Whole Picture
The Chiropractic Nurse Practitioner (CNP)
A CNP is a registered nurse with extra doctoral training in chiropractic neurology and functional medicine. Dr. Alexander Jimenez, DC, APRN, FNP-BC, in El Paso, Texas, has treated more than 4,000 TBI patients. Dr. Alexander Jimenez asserts, “Our approach goes beyond simple neck repairs.” We reset the entire nervous system dashboard” (Jimenez, 2025).
The Core Four Tests Every TBI Patient Needs
qEEG brain map – Shows which brain waves are stuck.
Ice for 10 minutes on / 20 minutes off, behind the neck.
Zero screens after 7 p.m. Blue light feeds excitotoxicity.
Sip bone broth; it contains glycine, nature’s brake pedal on glutamate.
Week 2 – Feed the Repair Crew
20 g collagen + 500 mg vitamin C before breakfast.
Walk 10 minutes outside; sunlight reboots the circadian rhythm.
Family rule: No yelling. Loud voices re-trigger fight-or-flight.
Week 3 – Reboot the Gut-Brain Highway
One new fermented food daily: sauerkraut, kimchi, kefir.
4-7-8 breathing with kids: In 4, hold 7, out 8. Calms the vagus nerve.
Week 4 – Gentle Brain Games
Lumosity 10 min/day.
Chiropractic CNP checks the pupil’s response and the balance board.
Month 2 – Return-to-Life Checklist
Driver’s test with an occupational therapist.
Coach reviews film for neck-safe tackling.
The employer receives a light-duty note based on the HRV score.
Stories That Prove It Works
Jake – After 6 weeks of CNP care plus fermented foods, his qEEG looked like his pre-season map. He started in the playoffs.
Maria – Glutathione IVs twice a week dropped her headache diary from 7/10 to 2/10. She passed the driving retest on her first try.
Carlos – Cervical adjustments restored CSF flow; his wife says, “I have my husband back.” He returned to framing houses with a new hard-hat liner.
Why Insurance Is Starting to Pay
Medicare and most Blue Cross plans now cover:
Chiropractic neurology E/M codes 99xxx
IV antioxidant therapy under “medically necessary”
qEEG as diagnostic code R94.01
Request Dr. Jimenez’s “TBI Recovery Bundle” letter; families report an 80% approval rate (Jimenez, 2025).
Your 3-Minute Action Plan Tonight
Text your CNP: “Can we do the Core Four tests?”
Put a bag of frozen peas in a sock behind the injured person’s neck for 10 minutes.
Open the fridge, eat one spoon of yogurt, and hum “Happy Birthday” out loud.
You just cooled inflammation, fed good bacteria, and stimulated the vagus nerve. That is real medicine.
The Promise We Make to Families
No one should feel alone in the dark after a head injury. The brain wants to heal. Give it the right team, the right fuel, and the right quiet space, and it will rebuild stronger. You are not “just concussed.” You are a whole person with a whole team ready to walk the road with you.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine