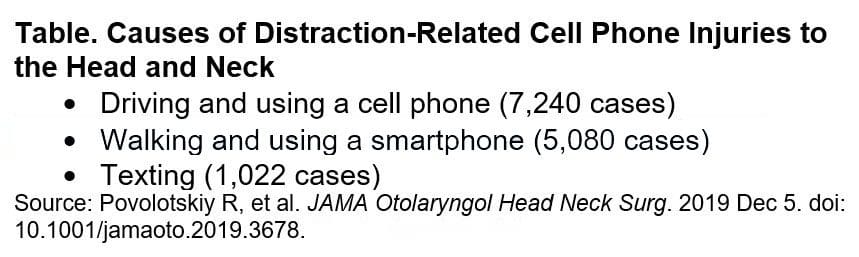
Head and neck injuries related to phone use are on the rise. Since the first iPhone was released, according to a study in JAMA Otolaryngology-Head & Neck Surgery.
Doctors are warning cell phone users to be especially careful when:
Walking around and texting
It is a distraction and one of the leading causes of head and neck injuries.
2,501 reported cases of phone-related head and neck injuries that lead to emergency room visits between January 1998 and December 2017 found in a nationwide database. Injuries in teens and young adults aged 13 to 29 years old were about 40%, in women (55%) and men (45%).
Common Phone Injuries
Common injuries include:
Cuts
Bruises
Abrasions
Internal injuries usually happen around the eyes and nose
Possible trauma to the brain
Over 41% of these injuries happened at home and were minor with little or no treatment needed. Around 50% of injuries were a result of distracted driving and 30% from distracted walking.
Any type of phone distraction in and out of the home puts you and others at risk for:
Falls
Slips
Trips
All of which can lead to injuries and other possible consequences (e.g. a busted phone).
More individuals are getting injured because of phone use while moving around and not paying attention to what’s around them.
Children
Children under the age of 13 were at higher risk to suffer a mechanical injury like parents accidentally dropping the phone on their child or children hitting themselves in the face. For example, ninety cases of injuries occurred while playing Pokemon Go.
Spending as little as two to four hours a day hunched over a smartphone is enough to make a serious impact on the body over time. And though two to four hours may not seem like a long time, it isn�t hard to arrive at two hours by adding several 15-minute or half-hour segments together.
For teenagers, specifically, two to four hours on a smartphone has changed as of now teenagers spend around seven to eight hours on their phones. Spending twice as much time on afternoons or the space between classes or lunch. Think about the impact of 1500 plus hours of bad posture throughout the year. There is no surprise that teenagers are at risk.
The lasting impact of text neck and distracted phone use on today�s young people will be costly. Therefore, the public needs to be educated about the risks of distracted phone use and reducing this distracted behavior.
*Neck* Pain Chiropractic Care El Paso, Texas
NCBI Resources
If you begin noticing pain, spasms, or irritation around the neck, shoulders, or back make an appointment with a professional chiropractor. Explain when the pain occurred, the severity, and the activity that started it. A simple adjustment may be all that is needed to get re-aligned and gain relief from pain caused by overuse. A chiropractor can also help decrease the chances of the injury worsening over time.
This is the season of the year that brings special time with loved ones, but it�s also a time when many un-merry mishaps and accidents can happen. From neck and back pain to sprains and strains to serious fractures that can put you in the emergency room. With a little care, preparation and precaution, you can be safe and enjoy the holidays to the fullest, while reducing the risk of experiencing a slip and fall injury.
The Garage
This is where holiday prep, go for tools and the like usually begin. However, the garage can be the first place where danger lurks during this season.
Most of us store the big boxes at the top on overhead storage racks etc. A wobbly step ladder, not enough upper body strength, someone opening the door where the ladder stands and tipping it, etc, is a perfect setup for a fall.
The first thing to ask is whether or not this is a job for you? If not then wait and ask for help from friends and family that can offer added strength and balance.
Plan ahead and prepare ahead so that repacking the decorations, lights, and so on will be a clean safe process.
Proper footwear that can grip a stable step ladder is a must.
Around the Tree
Anything can happen around the tree, ornaments fall and break, wire from the lights shorts out, trip and fall around it.
Just be aware of your surroundings and maybe keep a safe perimeter around the tree so nobody trips, slips and falls around it.
Focus on stability on a ladder if you have to add, adjust, the tree/ornaments, lights and what have you.
If the tree starts to lean, make sure reinforcements are there just in case when you’re ready to straighten it out.
Maybe Get Off the Floor
Wrapping gifts on the floor doesn’t pose the greatest risk for a spine injury, but it can increase chances for a�muscle�strain and sore back and neck. Hours just hunched over on the floor is a sure-fire set up for back pain.
Again plan ahead and knock out the trimmings and trappings little by little so there is plenty left in the tank when it’s time for the main event.
Maybe set up the wrapping station at a table and sit for a bit, stand for a bit,� take plenty of breaks, and move around and stretch out.
Sitting in a chair will help posture and prevent slouching.
On the House
As a spine injury specialist, I can tell you falls from the roof while hanging lights are real, and can be life-changing. From severe spine injuries to paralyzing fractures.
Safe Equipment is of the utmost importance!
Make sure the ladder you�re using is sturdy and on solid ground.
Only hang the lights from the eaves, so you can stand on a ladder.
Maybe think about using one of those projection kits that project various displays onto your house without the risk of injury.
No matter how you choose to decorate and entertain this holiday season, safety is priority one. From our team here at�Injury Medical and Chiropractic Clinic Happy Holidays!
El Paso, TX Chiropractor Personal Injury Attorney Recommended
NCBI Resources
The connective tissues in and around the spine can get:
Pulled
Strained
Sprained
Small tears in the disc can also contribute to back pain.
Basically, any number of activity and non-activity can cause damage to the spinal discs depending on the movement.
Manual tasks performed in an awkward posture
This includes:
Lifting boxes with the back and not bending the knees
Lifting something too heavy
Moderate physical activity
Vigorous physical activity
High intense strength training, long walks at the stores, handling people or animals, and picking up children can cause injury.
There are all kinds of tools for all kinds of jobs. However, using the correct tool can mean the difference between a job well done and a job that got done but also generated injuries and pain.
Examples:
Long tools are best for when you need leverage, sparing the need for massive physical force.
Vice grips and clamps can grip/stabilize objects rather than trying to hold objects with your hands.
Tilt objects to avoid overbending the wrists.
Use a cart/dolly/arm straps to carry heavy loads.
Take some time to think about how to make the job easier on yourself and look up youtube tutorials to find innovative ways to do these jobs making it less stressful both mentally and physically.
The National Institute for Occupational Safety & Health guidelines hand tool use
Keep the wrists straight &� Avoid bending/rotating the wrists.
Instead bend the tool, not the wrist and there are a variety of bent-handle tools just for this reason. Using the handshake wrist position is a good way to approach a job, as it is a neutral position for the wrist.
Don’t stand still in one place for an extended time when using a heavy tool.
Instead, reduce the size and weight of the tool which will help avoid strain, keeping the elbows low and slightly bent.
Tools that place pressure on the base of the palm stress the soft tissues of the hands and fingers interrupting circulation and nerve function.
Instead, opt for one with finger grooves that fit the hand. Short-handles help by reducing stress on the soft tissues.
Don’t use tools that need a lot of grip force to use or hold.
Instead, use one with a grip that compresses like memory foam and shapes to the hand. This is far better than hard plastic.
Don’t use tools that need the fingers to grip.
Instead, use tools that utilize a full-hand power grip.
Do not use tools that have sharp-edged handles or areas where the hands could get pinched.
Instead, use tools that keep the hands/fingers safe.
Trigger-finger operational tools should be avoided as this can easily cause repetitive finger/hand/wrist injury from the constant on-off motion.
Instead, use tools with large switches that can be operated using all four fingers.
Excessive temperatures affect manual dexterity, therefore keep hands free from extreme heat and cold.
If possible, do a different job that’s away from the extreme weather and if not wear properly insulated work gloves.
Keep excessive vibration to a minimum. Excessive vibration can affect circulation.
Use tools with control�features that limit vibration to the extremities and whole body.
Wear gloves that fit. If they are too tight they will place extreme pressure on the hands. Loose-fitting gloves reduce grip strength and the ability to grip properly.
Instead have a selection that is designed for different jobs.
Safely Operating Tools that Cause Whole-Body Vibration��
There are power tools that vibrate no matter what and transmit vibration into the operator’s arms and hands, legs, and feet. Using a tool like this can cause a condition called white finger or Raynaud’s Phenomenon to present.
The symptoms include:
Aching in the wrists and muscles of the forearm
Tingling sensations
Numbness
Whiteness in the fingers from restricted circulation
This type of vibration from riveting tools, grinders, pneumatic hammers, drills, and chain saws will affect the whole body’s well being.
Suggestions to help reduce the risk of musculoskeletal disorders
Choose power tools with anti-vibration controls and handles coated with suppressant/cushioned material to help with vibration.
Maintenance power tools by making sure they are balanced, clean, and lubricated.
Use gloves designed to absorb or reduce vibration.
Ask for help if the job requires equipment or tools that vibrate.
Whether using a hand or power tool to get a job done, the whole body is involved. Executing proper posture and body mechanics, along with proper tool choice and how it is used is vital to injury prevention.
El Paso, TX Chiropractor Recommended
Chiropractic care can help keep bodies flexible and help with range of motion. It is a very effective, non-invasive treatment for pain and can help with joint and muscular problems as well. Regular chiropractic treatments can help you better manage your body�s response to your work environment. It can also undo many of the ill effects that that type of work can cause.
NCBI Resources
Standing for extended or frequent periods of time without any breaks (such as walking or stretching) can cause the joints in the feet, knees, hips, and spine to become locked or immobilized temporarily. If the behavior continues, it can cause degenerative damage, leading to rheumatic diseases because the ligaments and tendons become damaged.
Physical therapists (PTs) are healthcare professionals that treat patients of all ages with various ailments/conditions. A spine surgeon, physiatrist, orthopedist, primary care physician, neurosurgeon, and a chiropractor may refer patients to a physical therapist as part of a non-operative treatment plan.
An organized physical therapy plan may be an integral part of after-care following surgery. Therapists practice in a variety of settings, like hospitals, outpatient clinics, rehabilitation centers, and nursing homes. Physical therapists provide:
Treatments
Exercises
Mechanics
The primary goals�of physical therapy include:
Maintain practical skills
Improvement
Building endurance and strength
Increasing flexibility
Reducing pain
Preventing impairment
Physical therapists also instruct patients on the best way to exercise to enhance overall physical fitness, move about safely (biomechanics and ergonomics), and injury prevention. Physical therapists also help patients with long-term physical incapacity (eg, spinal cord injury).
Aquatic Therapy
Patients with osteoarthritis have found�waterexercise to be beneficial. With a gravity-free environment,�patients can perform simple exercises without stressing the tender joints. Movement increases circulation to the affected joints and can relieve stiffness. Swimming is also a great exercise for anyone for loosening up stiff joints and strengthening muscles.
Electrical Stimulation
This type of therapy forces a muscle or muscle group to contract and relax. Therapists place surface patches containing electrodes on the skin over the area to be treated. The therapist programs the equipment to deliver the correct amount of stimulation for a set time.
The electrical current flows through nerve and muscle cells. The treatment is not painful. The patient feels gentle pulsating or an on/off sensation. This treatment stimulates circulation and supplies the area with oxygen and nourishment for healing. Electrical stimulation enhances healing and alleviates swelling and pain.
Electrical stimulation in physical therapy. Therapist positioning electrodes onto a patient’s knee
Heat and Ice
Heat increases circulation, decreases stiffness, pain and muscle spasms.
Patients with early arthritis symptoms find relief by taking a warm bath or hot shower.
It is best when done in the morning to help loosen up and alleviate stiffness.
Physical therapists use moist hot packs wrapped in a towel that is laid or wrapped around the affected area.
A moist hot pack transfers moist heat that penetrates deeply into soft tissues and stimulates local circulation more than heat alone.
Ice decreases pain by slowing the nerve impulses.
Inflammation subsides with forms of cold therapy:
Cold packs
Ice massage
Iced towels
They are usually the first aid following trauma.
When treating an overworked body part�ice�treatment should be supervised by a physical therapist.
Hydrotherapy
This is like a whirlpool bath. The water temperature and agitation loosen up joints, stimulate muscles and are controlled for maximum benefit.
Myofascial Release
This therapy improves circulation, decreases muscular tension and increases range of motion.
It is a type of massage that stimulates the muscles. The muscle tissue is manipulated by hand to stretch the tissue. Tight tissues become loosened using a cross friction motion with this therapy.
Movement & Conditioning
A physical therapist teaches patients how to move properly while being able to work through the pain. Therapists want patients to work as pain-free as possible. This does not mean that the exercises will be easy. More than likely they are going to be tough, but that is what you want to get back into top physical form.
Physical therapist assisting woman on an exercise ball at the clinic
Warming-Up can be accomplished by riding a stationary bike and some light stretching. The type of warm-up that goes with the therapy is determined by the individual treatment plan.
There will be muscle soreness for 24 to 48 hours following exercise therapy. This is completely normal and should be expected. As the exercises become a normal part of the day the discomfort will gradually go away. Stretching will increase flexibility. And as the treatment goes on resistive and strength exercises could be added.
Couple warming up
Home Exercise
With any treatment plan, there is usually a custom home exercise program. Exercises pretty much follow clinic exercises with variations and added stretches to keep the body from stiffening staying limber. Changes can be discussed with a physician.
Body Mechanics & Posture
Proper body mechanics helps to prevent further injury/s from occurring. Patients willing to maintain
Physical fitness
Reduce stress
Apply proper body mechanics
This reduces the risk of injury.
Proper posture is defined as keeping the natural curve of the spine. Proper posture minimizes stress to the spine. This is the first lesson a physical therapist teaches a patient.
Poor posture and poor body mechanics are leading contributors to neck and back pain.
Proper Work Habits
Do not lean over a desk for long periods.
Try not to sit without back support.
Adjust chair height so the knees are bent at a 90-degrees.
Bend the elbows at a 90-degree angle or they can rest on the work surface.
Don’t cradle the phone against the ear and shoulder as this can cause neck and shoulder issues.
Lifting and Carrying Objects
First, look at the object to be moved. If it looks too heavy find help.
Remove obstacles from the pathway where the object will be going through.
Visualize maintaining proper posture.
Get as close to the object as you can.
Place feet slightly apart and flat on the floor.
Bend at the knees to provide stable support.
Tighten the stomach muscles.
Breathe deeply.
Smoothly lift the object using arms and legs and not the back.
Hold the object at the sides and bottom.
Keep the object close to the body.
Keep back straight and carry the object with elbows slightly bent.
With shopping bags or luggage split the load in two, and try to carry the same amount of weight in each hand.
Pushing versus Pulling
Pushing is the more efficient and safer method of moving objects. Keep the back straight and use the knees to push. Keep close to the object and reposition the body every so often.
Reaching for Objects
Check the size, weight, and location of the object.
Use a proper stool or step-ladder to get the object. Stand with both feet flat.
One hand can be used for additional support.
Try not to look over too much as this can cause neck strain.
Think about storing regularly used items within easy reach.
Physical therapists may work directly for or with a physician, therapist, chiropractor and other healthcare providers to organize aspects of physical treatment plans. For example, a doctor may send physical therapist information of graphs, medications, analysis, and imaging results.
Massage Rehabilitation El Paso, Texas
NCBI Resources
During the first consultation, a physical therapist will talk about symptoms, analysis, and medical history.� Severity the location, type, and variables that decrease or increase pain are significant, and the PT will ask many questions regarding pain.
Physical therapists are healthcare professionals and members of your medical team. While physical therapy may be challenging or demanding at first, there are many benefits. It�s an opportunity to take charge of back or neck pain while building a stronger more resilient body.
One of the most recognized running injuries is runner�s knee. However, runner�s knee is not an injury but a result of different injuries. Running can hurt when improper mechanics, inadequate shoes, and cheap over the counter insoles are being used. It can lead to:
Plantar fasciitis
Achilles tendonitis
Medial tibial stress syndrome
Metatarsalgia
Runner�s knee
Runner�s knee is not an actual injury in of itself
It�s a broad description of knee pain caused by other knee injuries, which include:
Iliotibial band syndrome
Patellofemoral pain syndrome (PFPS)
Chondromalacia patella
This can keep runners sidelined, annually.
Runner�s knee is caused by usually one of two things: poor biomechanics and overuse.
Feet are the foundation of the body and if not taken care of, pain
Feet are 99% normal at birth.
Then life takes over and issues begin to arise.
8% develop foot conditions, then�by age 5 that number jumps to 41% and 80%� at twenty.
By forty pretty much everyone has a foot condition or some type of foot pain from work and activity.
These foot issues then begin to set up problems for the rest of the body, especially the generalized condition of back pain or leg/knee/hip problems.
Being able to foresee and realize a potential problem with the feet can PREVENT other injuries from beginning to present themselves and dodge any issues that can affect health and lifestyle.
Runners who are able to avoid injury are those that land the lightest, much like a cat and sustain the lowest level of impact.
Runners think about landing softly and adjust their stride so they land closer to the midfoot.
However, it’s easier said than done.
Most runners tend to be heel-strikers
Runners with excessive pronation that try to change to a forefoot strike pattern are more prone to inner foot and ankle injuries,
And runners with high arches that try to change to a forefoot strike pattern end up with sprained ankles and metatarsal fractures.
Runners try to treat the pain with stretches or exercises that target the area, but the source of the pain is actually elsewhere and they don’t realize it and are treating the wrong area.
A lot of the time the source of the imbalance comes from the feet.
An overlooked option for reducing knee injury and pain is the use of custom orthotics.
Custom orthotics align and support the foot/ankle in a more normal physiologic position for weight-bearing, which prevents dysfunction and improves the function of the body as a whole.
What they do is:
Make a symmetrical foundation that blocks pronation and supports supination
Give the heels shock absorption
Stops serial stress throughout the body
Enhances re-educating muscle-memory
Custom-made orthotics help reduce the impact of heel strikes when running or walking.
Shock absorption is a must when there is
Instability
Chronic degeneration
Inflammatory arthritis
Orthotics that are designed specifically to cushion the impact load from running can reduce pain triggers throughout the body.
Avoiding knee injuries
When orthotic care is indicated, custom-made functional orthotics can help reduce pain.
Look for orthotics that support the running gait and
Absorb shock at heel-strike
Support mid-stance
Provide propulsion at toe-off
Excessive Foot Pronation can Affect *FOOT POSTURE & MOBILITY* | El Paso, TX (2019)
The following video discusses how excessive foot pronation can ultimately have an effect on foot posture and mobility. Several things can impact foot posture and mobility, such as excessive foot pronation. Excessive foot pronation is most widespread among the overall populace, therefore, it’s regarded as one of the most frequent factors for abnormal foot posture and mobility, which can lead to a variety of health issues like overuse injuries. Excessive foot pronation and supination can ultimately impact general health and wellness.
What’s Afoot
Misalignment can be caused by many common runners� experiences including running on the same type of surface every day, running on a slanted surface such as a beach or replacing running shoes too infrequently. As a runner, you can work to vary your running surfaces and keep a better watch on your shoes, but your chiropractor will let you know if your body is in need of more balance.
NCBI Resources
If you are an active amateur or a competitive runner, using the services of a chiropractor can make a vast change in your overall health, reduce your pain from injuries and improve your alignment for a more effective run. Runners may not even realize that the tension they feel is the beginning of pain caused by being out of balance until it is adjusted. Chiropractic adjustments are often part and parcel of a runner�s training program to strengthen and improve performance. They can also help�recover from pregnancy�and postpartum bodily changes.
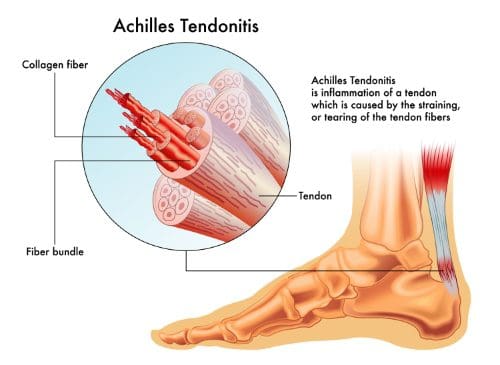
If you are suffering from Achilles tendonitis, you are definitely not alone. Plantar fasciitis and Achilles tendonitis are the two most common causes of pain in the heel. Athletes and active individuals, in particular, find themselves developing pain in the heel from Achilles tendonitis, but it is possible to develop the condition even if you are not an athlete.
Fortunately, chiropractic and associated therapies can do a lot to relieve your heel pain. With a combination of chiropractic care and Active Release therapy, you can get back on your feet and back to doing what you love as soon as possible.
Heel Pain Connected to the Achilles Tendon
Most people know how to point out the Achilles tendon. It is the large, thick tendon that travels up from the base of the heel and into the calf muscle. In fact, it connects the calf muscle and heel. It allows your body to transfer power from the calf muscle to the feet so that you can walk, run and jump. The Achilles tendon is strong and durable, but it is possible to overwork it and cause enough repetitive strain to develop tendonitis in the tendon.
Pain Causes in the Achilles Tendon
There are several stages to the process of developing pain in the Achilles tendon. These include:
Micro-tears
Heavy use of the tendon can lead to small tears. The micro-tears that develop in the Achilles tendon are known as tendinosis. They may not be noticeable at first and you may not feel much pain or any pain at all. However, over time and with increased tearing, the condition can become chronic.
Tendonitis
When you start to feel pain in your Achilles tendon that keeps occurring or lasts for a few days, you are likely experiencing tendonitis. The pain and inflammation of tendonitis need to be treated to avoid developing a chronic condition.
Tendinosis
If the pain becomes chronic�meaning it never or rarely goes away�then you have developed tendinosis. Instead of being inflamed, tendinosis is characterized by a lack of inflammation and the development of scar tissue. The scar tissue makes the tendon stiff and is usually quite painful. The stiffness of the tendon makes it more prone to tearing.
Rupture
If the tendinosis is not treated properly the tendon can eventually tear. A torn tendon is referred to as a rupture and usually requires surgery.
Symptoms
Pain and stiffness around the lower leg, right above the back of the heel
Begins as a mild ache and worsens throughout the day
Jumping,� running, stair climbing, and sprinting can spark intense pain
Tenderness or stiffness especially in the morning, but improves with movement/activity
Achilles Tendonitis Treatment
When you start to feel constant pain in your Achilles tendon it is time to go see your chiropractor. It is important to start treatment as soon as possible to avoid developing more advanced issues like tendinosis or even a ruptured tendon.
Your chiropractor will recommend several different types of treatment, including:
Active Release Therapy (ART)
ART is extremely effective for breaking up scar tissue and improving issues with soft tissues. Treatment can do a lot to improve the health of your tendon and the surrounding tissues to avoid further complications. It will also do a lot to help relieve the pain you are experiencing.
Chiropractic
Many times, the issues with your Achilles tendon are the result of misalignment in other parts of your body. When your joints are misaligned it tends to put extra stress on your feet and Achilles tendons. To minimize the stress on your joints, your chiropractor will adjust your spine and other joints to ensure proper alignment.
Get Help for Your Achilles Tendonitis
If you are experiencing heel pain, please get in touch with our chiropractic team. We can help to alleviate your pain and help you avoid experiencing further problems with your Achilles tendon.
Reduce *PLANTAR FASCIITIS PAIN* with Custom Foot Orthotics | El Paso, TX (2019)
Foot pronation is the natural movement which occurs during foot landing while walking or running. Foot pronation also occurs while standing, and in this instance, it is the amount in which the foot rolls inward toward the arch. Foot pronation is normal, however, excessive foot pronation can cause a variety of health issues, including bad posture. The following video describes the 5 red flags of excessive foot pronation, which can ultimately affect a person’s overall health and wellness. Dr. Alex Jimenez can help diagnose and treat excessive foot pronation. Patients recommend Dr. Alex Jimenez and his staff as the non-surgical choice for excessive foot pronation health issues.
Orthotics
If you are considering custom orthotics, a health care professional such as Doctor Jimenez and Injury Medical Chiropractic Clinic can perform a foot scan to show you what imbalances in the feet can lead to. The foot scan will show how the orthotics can help. Following the foot scan, a report will provide the caregiver a�Pronation/Stability Index, Foot Assessment, and Body Assessment.
What’s Afoot
Foot pain can commonly occur from various injuries. In the United States alone, about 2 million acute ankle sprains occur every year, one of the most prevalent causes of ankle pain. Chiropractic care is a popular alternative treatment option which can help treat a variety of health issues, including foot and ankle pain.
NCBI Resources
Tendonitis often recurs in many people. This is due, at least in part to improper or incomplete healing. Many people will resume normal activities as soon as the pain subsides when they should continue caring for the injury so that it can heal completely. This leads to inflammation of the area again as the original injury is aggravated, but it can also lead to re-injury in that same area. Chiropractic care can help tendonitis heal completely and help prevent re-injury to the area.
Golfer�s elbow is a condition that affects far more than those that golf regularly. According to Dynamic Chiropractic, golfer�s elbow can affect violinists, construction workers, tennis players, bikers and more. It’s more an expression similar to tennis elbow.
Anyone who overuses the elbow can find themselves with pain inside the forearm and elbow, pain that is unlikely to go away without treatment.
While medication and surgery can be options for treatment, chiropractic provides a non-invasive, effective way to relieve golfer�s elbow without the side-effects that come with surgery and medications.
What is it?
The joint and muscles on the inside of your elbow are activated during so many activities�pretty much every time you squeeze, grip or throw something, you use them. Even when you are doing less athletic activities like texting or typing at a keyboard, you are activating the muscles, tendons, and ligaments surrounding your elbow. It is not surprising that they can be overused, especially during work activities or leisure activities that you love so much you play all the time.
Golfer�s elbow is considered an overuse injury�an injury caused by using one or more parts of the body so much that they cannot recover quickly enough. Inflammation becomes constant, scar tissue can develop and pain becomes a regular problem.
How Chiropractic Helps Golfer�s Elbow
Chiropractic care is ideal for the treatment of golfer�s elbow. For some sufferers, coming to the chiropractor is the first and obvious choice. For others, going to the doctor is the first place they start.
Once they find that prescription medications are not alleviating the problem, they may be presented with the idea of surgery. Most people are hesitant to go through surgery if they do not have to, which is understandable. They reach out to a chiropractor because they are looking for an alternative that will help them heal without the pain and uncertainty that surgery brings.
At the chiropractor, you will find non-invasive, drug-free treatments that work to return your range of motion, reduce inflammation and break up the scar tissue in the soft tissues surrounding your elbow joint.
Chiropractic Treatment
Once you visit a chiropractor you will be given a careful, thorough physical examination to determine the nature of your problem and its cause. With golfer�s elbow, the problem is fairly obvious, so your chiropractor will focus on understanding exactly what your golfer�s elbow consists of�including your level of pain, your range of motion and the effects it is having on your day-to-day movement.
Some of the ways chiropractic can treat golfer�s elbow include:
Break Scar Tissue Up
Scar tissue keeps your muscles from operating correctly and causes pain. Chiropractors have methods for breaking up scar tissue to return normal muscle function, including active release.
Returns Mobility
Joint manipulation from your chiropractor is designed to make your joints move properly. The chiropractor will gently move your elbow back and forth to realign it and to ensure that it goes as far as it should go, and no further.
Reduces Inflammation
Inflammation is what causes much of the pain you are experiencing in your elbow. Joint adjustments and breaking up scar tissue are excellent ways to reduce inflammation. As the inflammation reduces the body can heal more easily and the pain will lessen.
We Can Get You the Help You Need
As you know, golfer�s elbow can be painful and make it difficult to do the things you need to do. Let us help you get some relief. Please contact our office today to schedule an appointment with our chiropractic team.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine