Kinesio taping is common for injuries, but can also be effective for non-sports related injuries/ailments. Kinesio taping is a rehabilitative therapeutic taping method that facilitates the body�s ability to heal naturally. The tape provides support, and stability for muscles, and joints without restricting motion. Plus there is added soft tissue support prolonging the tape’s effectiveness. The technique can have added benefits when combined with chiropractic. This technique is the norm among athletes nowadays but can benefit everybody. As a chiropractic physician, I use the technique for:
Sports injuries
Sprains
Strains
Injury Prevention
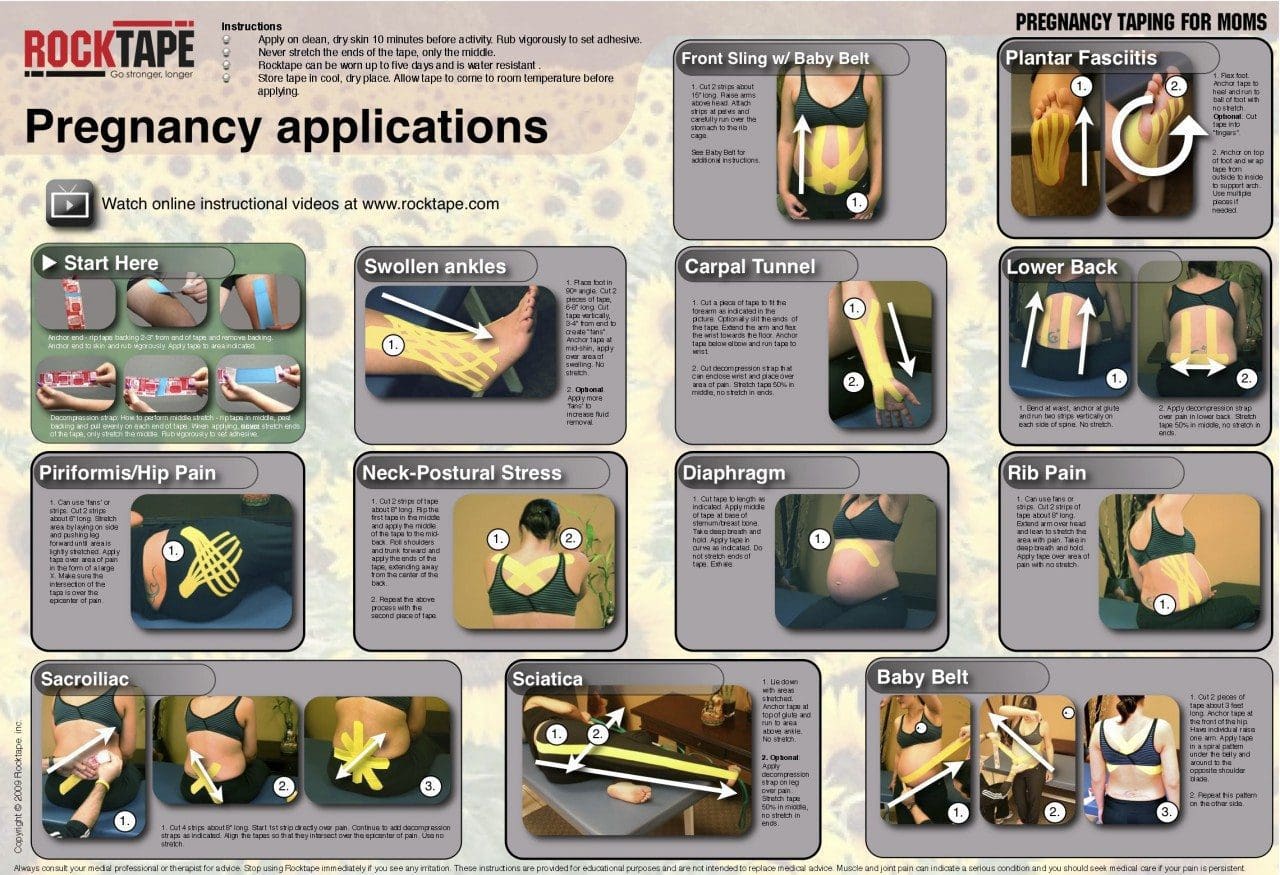
Pregnancy
The taping involves applying the tape over and around muscles stimulating them to send neuromuscular signals that optimize performance and helps injuries heal naturally. This is a versatile treatment that can benefit everyone.
Pain Relief
We all get strained, overused muscles that can cause tension and soreness. Millions suffer from neck, upper, mid, and low back pain from poor posture or sitting all day. It reduces pain by relieving the pressure on the strained or injured area. According to a study, stroke patients with shoulder pain experienced relief and reduction in shoulder pain after three weeks of Kinesio Taping intervention. Another study published in the Journal of Back and Musculoskeletal Rehabilitation had similar results for reduced pain in patients with tennis elbow. Kinesio tape therapy can improve pain symptoms while continuing to heal the specific muscle/s.
Reduce Inflammation
It also reduces pressure on the lymphatic system, which removes fluid from the tissues. Reduced pressure allows the body to drain fluids like lactic acid that can build up in an injured area. This benefit goes beyond just healing injuries. It helps reduce inflammation and swelling after surgery and with inflammatory conditions like lymphedema. Kinesio could be beneficial for individuals with chronic inflammatory conditions.
Overused Muscle Recovery
Taping improves blood flow, the delivery of oxygen, and nutrients to the affected area, which helps overused muscles heal quickly. This added benefit is one of the reasons taping is now used in everyday practice to treat:
Taping helps improve overall function. This is a key factor for optimal healing. A study found elderly patients with degenerative knee arthritis tried the therapy and experienced reduced pain, stiffness, improved knee joint function, and increased overall motion. For improved function Kinesio is commonly used on the:
Ankles
Back
Feet
Knees
Shoulders
Overall Benefits
One of the most important benefits, it comes without side effects from prescription meds.
It provides support without restricting the muscle�s range of motion
Individuals can continue to be active and not worry about overstretching the injured muscle/s, as the tape will let them know.
The tape can be worn 24-hours a day for several days per application.
This Kinesio taping technique is currently used by thousands of:
Physical therapists
Occupational therapists
Chiropractors
Medical doctors
Certified athletic trainers
Massage therapists
Correct Bad Posture with Functional Foot Orthotics
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
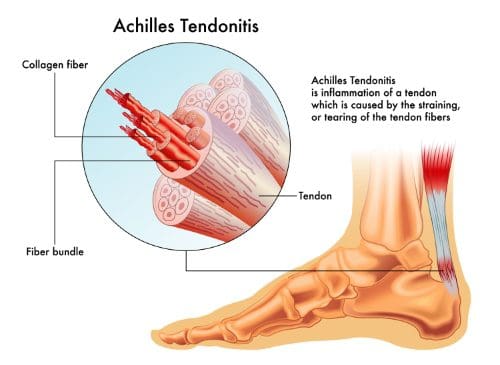
Tendonitis can be a painful condition that occurs when tendon/s that connect bone/s to muscle/s become damaged/injured. This can be from overuse of the particular tendon/s or using them in an improper fashion. Whatever the case, the result is inflammation, pain, and swelling. With injury/s where the tendon is stressed/strained to the point of injury, the soft tissue around the area can also be affected. More than 4 million�people�a year in the U.S. seek some form of medical treatment for�tendonitis symptoms.
Common types include:
Achilles tendonitis
Runner�s knee
Golfer’s elbow
Jumper’s knee
Pitcher�s shoulder
Swimmers shoulder
Tennis elbow
Other tendons in the body can also experience symptoms. Symptoms usually occur at the point where the tendon attaches to the bone and include:
Pain as a dull ache, especially when moving the limb or joint
Tenderness
Moderate swelling
The�wrist,�fingers, Achilles tendon, and ankle can all become inflamed from the condition. Primary care physicians are the ones to usually diagnose the injury. Once there is a definitive diagnosis, a non-surgical non-invasive treatment plan is the first recommended option. If these do not work then surgical procedures could be discussed. Chiropractic care is a first-line option that many physicians recommend.
Proper Rehabilitation Makes a Difference
This is usually from improper or incomplete healing.�Many individuals resume normal activities/chores as soon as the pain goes away. This is a mistake, as this is the time when continued care for the injury needs to be observed to heal completely. For this reason, tendonitis tends to recur. This inflames the area of the original injury which can then become aggravated, causing more pain. But more importantly, this aggravation can lead to a re-injury in the same area, which can be more severe the second time around. Chiropractic can help the tendon heal completely and help prevent re-injury to the area.
Chiropractic
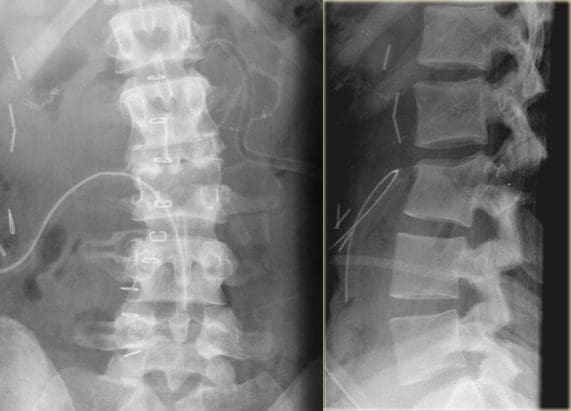
Tendonitis symptoms can resemble other conditions, therefore the first step is confirmation. A doctor may use X-rays, MRIs, or CAT scans to make a positive diagnosis. A chiropractor will work with the patient in developing a treatment plan that is effective, and customized to the patient�s needs. The core of the treatment is focused on the root cause of the problem, and not just alleviating the symptoms.
With severe inflammation, a chiropractor will utilize inflammation reducing techniques like bracing, rest, ice, electrical muscle stimulation, ultrasound, low-level laser therapy, massage, and physical therapy. The focus is to loosen the tendon/s to reduce inflammation so that the treatment can continue to the next phase. Once the inflammation is under control, a chiropractor might start:
Massage
Physical therapy
Joint manipulation
Strength exercises
If the individual has limited joint mobility then joint manipulation and adjustments could be the best option.
Treatment Plan
Initial pain often subsides or even disappears after the first two to three weeks. This does not mean that the injury is fully healed. Many patients mistakenly believe that once the pain is gone the condition is gone. This is not true. Inflammation could decrease over the first three weeks, however, complete healing takes around six weeks and longer.� Scar tissue forms during this time which is how the body repairs the injury.
Once the injury is repaired the scar tissue has to be broken down so the area can regain mobility and flexibility. A chiropractor will use specialized techniques to break down the scar tissue. This could also�include massage and ultrasound to help in the process.�Mild stretching exercises could also be incorporated into the plan. As the tissues heal fully then a therapeutic exercise regiment can continue in the aid in breaking down the scar tissue further. These exercises will work the muscles but do not involve the tendons.
Better Health
Tendon inflammation can be healed completely and chiropractic care can help in achieving this. Chiropractic medicine takes the entire body approach, which means that everything is connected in some way. So if there is a form of pain in one place, it does not mean that that spot is where the source of the pain is coming from. It could be somewhere completely different, and so the chiropractor is going to work both areas and possibly others to alleviate the cause and not just alleviate the symptoms. Chiropractic medicine also includes diet, supplemental help, and lifestyle choicesthat can help the healing process and overall health. Once treatment is complete the individual can typically return to normal activities without the risk of re-injury and re-inflammation.
Kinesio taping method is a therapeutic technique that offers an approach of supporting the individual and rehabilitating the condition or affected area. Kinesio tape can stimulate or relax muscles, depending on the technique and type of tension that is put on the body. It raises the skin in microscopic increments that aid in lymphatic drainage.
It decreases inflammation and swelling reducing pressure in the area, allowing the blood and lymphatic fluid to flow naturally and more effectively in and out of the affected area.
This helps the body return to homeostasis. It can be applied in a variety of different configurations, but usually, applications are single:
I
Y
X
Kinesio Taping
There are unique taping shapes specialized to address certain areas of the body and conditions.�Providing stability and support for the body�s joints and muscles, it does not restrict the body’s range of motion. The techniques are designed to address soft tissue injury/s by manipulating the area and promoting natural healing, alleviating pain, reducing swelling, and providing all-around relief.
Kinesio Taping can Treat
A variety of conditions benefit from Kinesio taping. Chiropractors and physical therapists use it for:
Athletes use it for additional support and injury prevention.
Taping and Chiropractic
The tape uses the body�s own natural healing process with many individuals finding it, as the preferred treatment for many conditions. When combined with chiropractic care, Kinesio Taping is highly effective. A chiropractor may use a variety of techniques, depending on the condition or injury.
They can use spinal manipulation, physical therapy, massage, electrical stimulation, ultrasound, heat, and ice, combining them with recommendations for lifestyle and diet modifications. As aforementioned it encourages the body to heal itself, thus eliminating the need for medication/s� their undesired and invasive surgery. Kinesio Taping is safe, natural, and a perfect complement to chiropractic treatment.
Foot Levelers Custom Orthotics Reduce Low Back Pain
It’s the weekend in the backyard doing some chores, grilling, etc, while several kids play and jump on a� nearby trampoline. The joviality from all this fun is filled with laughter, screams of joy, and other sounds or game instructions from one child to another. Then there is silence. The kids are huddled around their friend. One of the children fell off flat on their back.
The paramedics arrive and immobilize the head, neck, and spine strapping the child to a backboard and off to the hospital where there is no severe damage, just some mild bruising but everything turned out ok. This was a made-up scenario but unfortunately, emergency room doctors are seeing and treating this type of injury more and more.
Statistics
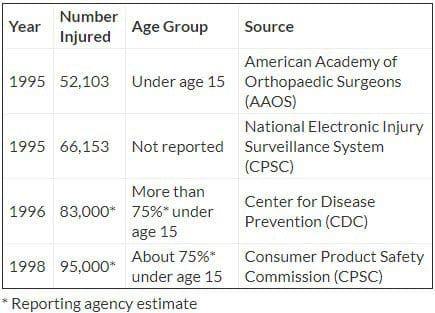
The statistics of the number of trampoline-related injuries treated in emergency rooms.
A simple analysis of the above stats is shocking. This means that since 1995, the number of injuries has increased between 30 and 45 percent. The CDC states that around 10 percent of trampoline injuries affect the head and neck. Many injuries are minor like bruising, scrapes and whatnot but some can be serious like broken bones, blunt-force trauma, and even paralysis.
For Home
Most of us see trampolines as a toy but are not aware of the dangers that come with it. Most injuries take place on trampolines purchased for home use. The American Academy of Pediatrics recommends that parents never let their children use a friend’s trampoline. While the American Medical Association recommends children should not be allowed to play/jump on a trampoline, even with adult supervision.
Trampoline Safety
Equipment Tips
A full-size trampoline consists of flexible fabric attached to a metal frame with springs, hooks, and a safety mesh/net. Most are around three feet off the ground. Consider the following safety tips:
Read the information and instructions provided by the trampoline manufacturer. Give this information to anyone who will be using the trampoline.
The proper placement of the trampoline is very important. Look at the location and surrounding area. Don’t place the trampoline close to a house/building, playground equipment, a swimming pool, the street, electrical lines, outdoor appliances, and plants/trees.
Remember a child can bounce 10 feet or higher in the air from a trampoline.
Make sure the springs, hooks, and frame are secured and covered with sturdy shock-absorbing pads.
There should be shock-absorbing material all-around and under the trampoline.�Use the owner�s manual for recommended materials.
Stores where trampolines are sold often sell special padding.
Check the trampoline for wear and tear often. Which include the frame’s structure like the screws, bolts springs, hooks, and fabric.
Using the Trampoline
Step-ladders, boxes, and chairs to climb on the trampoline should be kept out of reach to prevent children from using the equipment without permission. And they should be moved out of the way once the individuals are on.
Do not use the trampoline when darkness begins to take over like sunset. Individuals cannot see and when up in the air judging distance and where the trampoline is can be difficult/impossible.
Before use, warm-up with a few exercises. To make sure muscles are loose and ready to react.
Children need adult supervision at all times. Judging distances, foreseeing danger and quick reaction in situations that can become dangerous require an adult.
At least two adults are needed to spot the individuals and help prevent anyone from falling off.
Most want to jump together but too many people on a trampoline can be dangerous. Limit the number of people to where they can bounce safely without bumping into someone else, or falling off from lack of space.
CDC reports that half of all injuries happen when more than two people use a trampoline. Usually, this happens with children that are lightweight, still not fully coordinated, and can’t control how they move, especially in the air.
Learn how to land properly.
Unless a professional or expertly trained do not try somersaults, backflips, stunts, or crazy acrobatics.
Don’t jump or bounce off the trampoline.
Professional Help
There are professional gymnastic centers that have trampolines with padding all around and also give lessons/classes on proper usage. This could help a great deal, as it could be a safe alternative instead of home use. But if not then take the classes which could save a trip to an emergency room!
As El Paso�s Chiropractic Rehabilitation & Integrated Medicine Center, we are focused on treating patients after debilitating injuries and chronic pain conditions. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
The Best Sports Injury Rehabilitation Chiropractor El Paso, TX.
NCBI Resources
Spinal cord injuries occur more in the neck or cervical spine. Around 60% of cases involve the neck, followed by the mid-back or thoracic spine that averages to around 32% of injuries. Although most people experience low-back pain,�only 9% of spinal injuries occur in the low back and tailbone or lumbosacral spine.
Damage to the spinal cord not only affects the area where the point of impact occurred. The primary injury can also�damage cells, dislocate the vertebrae and cause spinal compression.�It can also trigger secondary injuries, that cause a series of biological changes. This can happen within weeks or months after the injury.
Ultrasound is a passive therapy, which means this is a treatment that a physical therapist administers. It creates gentle pulsating, penetrating heat that soothes, and relaxes spinal and any other muscles that may be tight, knotted and sore.
It is an added supplemental therapy of the primary treatment like chiropractic, therapeutic stretching, and exercise. Ultrasound releases and warms the muscles and soft tissues thus increasing circulation that speeds recovery/healing.
How does ultrasound work?
The equipment creates high-frequency sound waves that flow through to the tight, knotted area with a round-headed probe. The sound waves flow deep into the muscle tissue and ligaments all the while creating a soothing heat that loosens up the tissues.
Treatment application
The therapist will apply a hypoallergenic gel to the skin, that makes for a smooth moveable surface. Then the therapist goes in gentle, circular motions with the probe, and performs the treatment, that can last several minutes.
Ultrasound can also be utilized when performing phonophoresis. This is a treatment that involves the application of topical anti-inflammatory medications that are mixed with ultrasound gel�then applied to the area with the probe. The sound waves force the medicine into the tissues to help reduce inflammation.
Does it hurt?
Absolutely not, the patient will only feel a tingling sensation around the area being treated. There will also be a warming sensation from the sound waves.
Ultrasound results
The ultrasound probe is glided over the surface, all the while sound waves are penetrating through the skin’s surface, which causes the soft tissues to vibrate, creates muscle tightness soothing/releasing heat. The heat induces vasodilation that draws blood into the tissues that are hurting. The increased blood flow delivers much needed:
Oxygen
Nutrients
Removes the cell’s waste
The heat relieves pain and inflammation, reduces muscle spasms, and accelerates healing. Depending on thearea being treated, the range of motion will be increased.
Shoulder Pain Rehabilitation
NCBI Resources
Physical therapists also�instruct patients on the best way to exercise to enhance overall physical fitness, move about safely (biomechanics and ergonomics), and injury prevention. Physical therapists also help patients with�long-term physical incapacity�(eg, spinal cord injury).
In today’s workforce, many jobs place workers at a higher risk for a back injury. The list is pretty extensive and may surprise you! Individuals that have suffered a� neck or back injury at work know the cost goes beyond lost wages. The impact of these injuries on employees, employers, and the economy is staggering.
In a report published by the Bureau of Labor Statistics, there were 2.8 million cases of non-fatal occupational injuries and in 2018.� Of these cases, more than 50% lost time from work, transferred to a different job, or restricted work activity. Not all of these cases were spine-related injuries. However, 880,000 cases were back pain-related injuries.
The World Health Organization’s International Labour Office says that the problem is global.
Musculoskeletal diseases are a very common part of 270 million non-fatal work/job accidents where employees missed at least 3 workdays.
Risky Jobs
Occupational safety experts gather all kinds of information that they factor. This includes job requirements, work environment, and work station set up. In compiling the list of risky occupations, here are some of the criteria:
Heavy physical work
Forceful lifting movements
Bending
Twisting
Awkward work postures
Whole-body vibration
Static work postures like standing/sitting but never changing position compounds the risks to workers.
Two occupations that lead the list of jobs placing workers at the highest risk are construction and nurses/nursing home workers. Workers in both of these jobs tend to share the under-reporting of work-related injuries. This happens as the employees fear they will lose their job and cannot afford to take any time off.
Construction Workers
Employees at a construction site are repeatedly lifting, bending, carrying, pulling, and tugging. These repetitive movements lead to overuse injuries and back strain/sprains are a common part of this. More than 30% of workers have to miss job time. Those that must climb ladders or work on scaffolds have a greater risk of falling. This is where some serious spinal injuries can occur, causing disability and sometimes being fatal.
Nurses/Nursing Workers
Nursing homes and employment opportunities are growing from elderly population growth. These workers are at high risk for back pain and spine injury. This comes from transferring patients’ from their beds, bathtub, and bathroom facilities. All these actions require lifting, carrying, holding, pulling, pushing, and turning. The Bureau of Labor Statistics reports nearly all back and shoulder injuries are the result of moving patients.
Warehouse Workers
This is another job that requires lifting, along with using forceful movements, bending, twisting, carrying, and placing the body in awkward positions. Sometimes these workers have to drive a truck or an industrial vehicle that creates whole-body vibration. Continual exposure to vibration can cause backache and soreness that can lead to lost work time.
Dentists and Surgeons
Both of these professions involve prolonged standing, stooping, bending, and awkward body positioning. Not to mention the mental strain that diverts the doctor’s attention to proper posture and body mechanics that results in injury and pain.
Landscapers
The American Chiropractic Association puts landscapers in the top 10 list of jobs that cause back pain. This job puts these workers at a greater risk for cumulative trauma disorders. All the tasks that a landscaper has to do that include hedge trimming, tree pruning, and planting. These actions/movements involve lifting, reaching, bending, and stooping. This is a perfect set up for an overuse back injury.
Hand tools that get used over and over can cause painful conditions like carpal tunnel syndrome and thoracic outlet syndrome. Thoracic outlet syndrome is when the nerves and blood vessels become compressed between the neck and shoulder.
Store Cashier
Grocery and retail store cashiers require workers to stand in one place for a long time. This along with the repetitive motions of scanning, typing, opening, closing combined with bagging and lifting bags over and over can cause neck, shoulder, back, leg and foot pain. Over half of checkout workers complain of back pain.
We may not be able to instantly change our occupation, but there are steps to help prevent neck and back injuries. The key is workplace ergonomics and safety. Be proactive to help reduce workplace risk for neck and back injury and share what you learn with co-workers.
*BEST* Heel Spurs Treatment | El Paso, Tx (2020)
NCBI Resources
Injuries that are caused by repetitive movements often develop gradually.�This is the time when the symptoms are mild and come and go, so the individual just works through it and doesn�t think about it. It�s�not until the symptoms get very painful and debilitating that the individual realizes that something is wrong, and then they seek medical attention. Don�t wait, as soon as you feel a tingle, slight pinch, or a little soreness�and you feel that it stems from your work�s repetitive movements, get in touch with a doctor or chiropractor before it becomes excruciating.
Spinal Cord Injuries Are Not Only Caused by Trauma
When people think of spinal cord injury/s or SCI’s, traumatic events like a major auto accident, hard fall, severe sports injury or intense work injury come to mind. It is true that auto accidents are the leading cause, however, non-traumatic accidents and diseases like a spinal tumor can also cause spinal cord injuries.
These types of injuries involve damage to the spinal cord that can temporarily or permanently affect its functionality. Spinal cord injuries are divided into 2 categories: traumatic and non-traumatic. Even with non-traumatic injuries the impact or severity is not lessened and the aftermath can have a devastating effect on a person�s life.
Spinal Cord Injury Trauma
Vehicle crashes: Motor vehicle accidents are the leading cause of traumatic spinal cord injuries, and they account for 40% of all SCI’s.
Falls: Falls are the second cause of traumatic spinal cord injuries, and they account for 32% of injuries.
Violence: Violent acts, like gunshot wounds or a stabbing cause around 14% of spinal cord injuries.
Spinal cord injuries occur more in men than women with 80% of cases affecting men.
Although people of all ages can experience SCI, there are activities/events that increase the risk that affects different age groups more than others. An example is high-impact actions like motor vehicle accidents and sports injuries occur more in young adults. Conversely, spinal cord injuries caused by a fall happens more in adults over age 60.
Regardless, SCI occurs more in the neck or cervical spine. Around 60% of cases involve the neck, followed by the mid-back or thoracic spine that averages to around 32% of injuries. Although most people experience low-back pain, only 9% of spinal injuries occur in the low back and tailbone or lumbosacral spine.
Understanding SCI Trauma
Damage to the spinal cord not only affects the area where the point of impact occurred. The primary injury can also damage cells, dislocate the vertebrae and cause spinal compression. It can also trigger secondary injuries, that cause a series of biological changes. This can happen within weeks or months after the injury.
The secondary injury cascade processes:
Glial cells along with the nerve cells in the spinal cord begin to die. These cells provide nutrients and other support to the nerve cells in the central nervous system. This consists of the brain and spinal cord.
The blood vessels in the spinal cord lose their ability to function, and this reduces the blood supply to the cord. When the blood supply becomes inadequate it is called ischemia. Blood vessel injuries expose the cord to inflammatory cells that in turn cause swelling. When the spinal cord becomes inflamed the spinal cord gets more and more compressed. If this happens�the initial injury progressively worsens.
This changes the cord�s structure and its normal operation. The secondary injury cascade can interfere with the cord�s ability to heal itself. This means an individual could experience permanent nerve pain and dysfunction.
Non-traumatic SCI
Spinal cord damage does not only happen with traumatic events. An SCI can also be caused by non-traumatic diseases in the spine. Tumors are the leading cause, but infections and degenerative disc disease can also cause serious damage.
Non-traumatic SCI’s happen more than traumatic based ones. �The incidence of traumatic SCI in North America comes to around 54 cases per one million people. With the incidence of non-traumatic SCI is around 1,227 cases per million people.
Healthy Spinal Cord Injury Outcomes
Spine researchers are making great strides in developing optimal protective and regenerative treatments to improve spinal cord health after these injuries occur.
Currently, innovative medical, surgical, cell-based and alternative treatments are furthering the medical community�s understanding of SCI’s. This is dramatically improving the quality of life and creating positive futures for individuals who experience these injuries.
Car Accident Injury Rehabilitation | El Paso, Tx (2020)
NCBI Resources
The muscles in the back keep the spine moving and functioning properly.�When the spine or�abdominal muscles are�weak this creates a higher probability of a back strain or injury. Having strong, healthy spine muscles are important because they function in maintaining correct posture, which in some cases, causes chronic back pain because of poor posture.
If�only one part of the body is�strengthened like the back is not enough. Therefore strengthening the rest of the body is a must. These include the body�s core and leg muscles. Total body strength will reduce back pain and can help perform regular activities, like�lifting heavy objects much easier, with more confidence and with a lesser probability of injury.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine