Chiropractic and Massage: Duos often create more exciting outcomes. Lewis and Clark, the Lone Ranger and Tonto, and even Batman and Robin functioned more efficiently together than apart. Complementary pairings propel results and enhance efforts.
This is decidedly true with massage therapy and chiropractic care. While each offer considerable benefits on their own, they often mesh well with each other to create a comprehensive treatment plan for many conditions or injuries.
So, sit back and let us show you how massage therapy and chiropractic care are a pain-fighting, mobility-enhancing dynamic duo.
A Combination Of Both: Chiropractic And Massage
Massage Enables A More Effective Chiropractic Visit
Therapeutic massage warms up muscles and relaxes the individual’s entire body, enabling the chiropractor to maximize his or her chiropractic adjustment for optimal results.
Massage brings about a more stable adjustment.
When a chiropractor performs an adjustment to alleviate pain or increase mobility, pre or post massage couples with it to increase the body’s acceptance of the adjustment.
Chiropractic Takes Massage Therapy Further: Includes Joints & Bones
Each treatment offers strong relief and recovery to certain areas of the body. Massage produces relaxation in muscles, relieving tension and toxins. Chiropractic care picks up where massage leaves off and extends the treatment efforts to the body’s tendons, joints, bones and, ultimately, the nervous system.
Works On The Body As A Whole
Both treatments focus on broad rejuvenation and healing techniques for full body health. In a variety of instances, chiropractic care shows significant increases in treating the overall root of the problem when used in combination with massage therapy.
Gets In The Head
Whoever said “it’s all in your head” wasn’t entirely wrong. Individuals sometimes feel stress, dread, or worry over health procedures in general, and chiropractic treatment is no different. Massage therapy serves to relax and de-stress a person, preparing them to go into chiropractic treatments less stressed or tightly wound. A relaxed person’s body tends to respond better to treatment.
Offers Shorter Recovery Times
Blending both treatments into one builds an all-encompassing regimen that works on the condition or injury from multiple points. Tackling health issues this way reduces the time is takes to heal and regain the body’s full mobility.
Decreases Discomfort
Massage therapy aids in warming up muscles, readying them for chiropractic adjustments. This experience is similar to stretching thoroughly before exercising. Pliant muscles offer less resistance to a chiropractor’s regimen, resulting in greater patient comfort. This benefits the entire process, as a painless, comfortable visit increases a person’s openness and commitment to future therapeutic endeavors.
Provides Longer Lasting Results
A relaxed body is more open to treatment. Both massage therapy and chiropractic care serve to attain the goal of healing and recovery, and pain minimization or management. Achieving a synergistic effect is possible when both treatments are employed simultaneously. Chiropractic care is known to work deeper and last longer when paired with massage therapy, especially with chronic, painful health issues.
Patients who seek help with bodily conditions or injuries benefit and see results from chiropractic and�massage therapy separately. Both forms of therapeutic relief used together may create an even more significant, longer last result. Chiropractic care and massage therapy complement each other and offer positive benefits to a variety of painful health issues.
Embark on a treatment plan with this healing, effective dynamic duo! Ask your chiropractor if your specific condition would benefit from both principles of care. Give us a call today!
Low back pain is a common complaint that generally goes away on its own, however, what should a person do if their LBP becomes chronic and/or persistent? How is an individual’s quality of life affected and how does their pain intensity impact their physical capacity? Is there any type of treatment which can help improve low back pain? Many different types of treatment options can be used to safely and effectively treat low back pain. The purpose of the following research study is to determine the influence of the McKenzie method and endurance exercises on low back pain. The article demonstrates evidence-based information on the improvement of the quality of life of patients with LBP after receiving the treatment protocol mentioned below.
Influence of Mckenzie Protocol and Two Modes of Endurance Exercises on Health-Related Quality of Life of Patients with Long-Term Mechanical Low Back Pain
Abstract
Introduction
Long-term Mechanical Low-Back Pain (LMLBP) negatively impacts on patients� physical capacity and quality of life. This study investigated the relationship between Health-Related Quality of Life (HRQoL) and pain intensity, and the influence of static and dynamic back extensors� endurance exercises on HRQoL in Nigerian patients with LMLBP treated with the McKenzie Protocol (MP).
Methods
A single-blind controlled trial involving 84 patients who received treatment thrice weekly for eight weeks was conducted. Participants were assigned to the MP Group (MPG), MP plus Static Back Endurance Exercise Group (MPSBEEG) or MP plus Dynamic Endurance Exercise Group (MPDBEEG) using permuted randomization. HRQoL and pain was assessed using the Short-Form (SF-36) questionnaire and Quadruple Visual Analogue Scale respectively.
Results
Sixty seven participants aged 51.8 � 7.35 years completed the study. A total drop-out rate of 20.2% was observed in the study. Within-group comparison across weeks 0-4, 4-8 and 0-8 of the study revealed significant differences in HRQoL scores (p < 0.05). Treatment Effect Scores (TES) across the groups were significantly different (p = 0.001). MPSBEEG and MPDBEEG were comparable in TES on General Health Perception (GHP) at week 4; and GHP and Physical Functioning at week 8 respectively (p > 0.05). However, MPDEEG had significantly higher TES in the other domains of the SF-36 (p = 0.001).
Conclusion
HRQoL in patients with LMLBP decreases with pain severity. Each of MP, static and dynamic back extensors endurance exercises significantly improved HRQoL in LMLBP. However, the addition of dynamic back extensors endurance exercise to MP led to greater improvement in HRQoL.
Keywords:Mckenzie protocol, endurance exercises, quality of life, back pain
Background
Low-Back Pain (LBP) is described as the constellation of symptoms of pain or discomfort originating from impairments in the structures in the low back [1�2]. LBP is one of the most common ailments afflicting mankind [3]. It is a complicated condition which affects the physiological and psychosocial aspects of the patient [4, 5]. Epidemiological reports indicate that 70 to 85% of all people have LBP at some time in their life [1, 6]. The World Health Organization predicted that the greatest increases in LBP prevalence in the next decade will be in developing nations [7]. In line with this, a systematic review by Louw et al [8] concluded that the global burden and prevalence of LBP among Africans is rising.
It is estimated that 80-90% of patients with LBP will recover within six weeks, regardless of treatment [9]. However, 5-15% of all people that have LBP will develop long-term LBP (i.e. LBP of 12 weeks and longer) [10, 11]. The patient subgroup with long-term LBP accounts for 75-90% of the socioeconomic cost of LBP [12] and over 30% of these patients with long-term LBP seek healthcare for their back complaints. Long-term LBP significantly impacts on patients� physical [13], psychological and social functioning [14] and can affect well-being and quality of life [15]. Reduced quality of life in patients with long-term LBP is associated with poor prognosis [16], intermittent or recurrent episodes of LBP [17], disability [18] and psychosocial dysfunction [19, 20].
Assessment of Health-Related Quality of Life (HRQoL) in relation to LBP has been recommended in LBP management [21, 22]. Several HRQoL instruments have been developed to assess self-perceived general health status [21, 22]. The SF-36 Health Status Questionnaire, though a generic instrument, has been recommended in the assessment of HRQoL of patients with long-term LBP [22] and it assesses eight domains such as physical functioning, role limitations due to physical problems, bodily pain, general health perceptions, vitality, social functioning, role limitation due to emotional problems and general mental health [23, 24].
Consequent to the foregoing, treatment intervention that may help improve the HRQoL of patients with long-term LBP has been advocated. Although, physiotherapy plays an important role in the management of patients with LBP, the traditional approach based on biomedical model, which is centered on the treatment of impairments and patho-physiological variables, may not fully addressed the wider range of factors including psychosocial impairments associated with long-term LBP [25, 26]. However, long-term LBP is considered to be a multi-factorial bio-psychosocial problem which has an impact on both social life [27, 28] and quality of life [29] and thus requires a multi-dimensional approach based on a bio-psychosocial model (a model that includes physical, psychological and social elements) in its assessment and treatment [30, 31].
Based on empirical recommendations from research, recent decades have witnessed tremendous advances in preventive, pharmacological and physiotherapy management for a limited number of patients with LBP especially in developed countries. However, the improvement in health outcomes observed in most Western countries over the past few decades has not been achieved in Africa [32] and therefore, the health of Africans is of global concern [8]. Compared with Australians [33], Europeans [34] and North Americans [35], the use of exercise as medicine in Africans is poor. Exercise is the central element in the physical therapy management of patients with long-term LBP [9, 36]. Exercise often does not require expensive instruments and probably the cheapest intervention and one in which the patient has some measure of direct control [37]. Nonetheless, it remains inconclusive which exercise regimen will significantly influence the quality of life of patients with long-term LBP. The McKenzie Protocol (MP) is one of the most commonly used physical therapy interventions in long-term mechanical LBP with documented effectiveness [38�41]. However, there is a dearth of studies that have investigated the influence of the MP on HRQoL in patients with long-term mechanical LBP. Therefore, this study was intended to answer the following questions: (1). Will pain intensity significantly influence HRQoL? (2) Will static and dynamic back extensors� endurance exercises significantly influence HRQoL in Nigerian patients with long-term mechanical LBP (LMLBP) treated with the MP?
Methods
Eighty four patients with LMLBP participated in this single-blind randomized trial. The participants were consecutively recruited from the physiotherapy department, Obafemi Awolowo University (OAU) Teaching Hospitals Complex and the OAU Health Centre, Ile-Ife, Nigeria. The McKenzie Institute’s Lumbar Spine Assessment Format (MILSAF) [3] was used to determine eligibility to participate in the study. Based on the MILSAF, patients who demonstrated Directional Preference (DP) for extension only were recruited to ensure homogeneity of samples. DP is described as the posture or movement that reduces or centralizes radiating pain that emanates from the spine. Exclusion criteria were red flags indicative of serious spinal pathology with signs and symptoms of nerve root compromise (with at least two of dermatomal sensory loss, myotomal muscle weakness and reduced lower limb reflexes), individuals with any obvious spinal deformity or neurological disease; pregnancy; previous spinal surgery; previous experience of static and dynamic endurance exercise and having DP for flexion, lateral or no DP. Long-term low-back pain was defined as a history of LBP of not less than 3 months [42].
Based on the sample size table by Cohen [43] with alpha level set at 0.05, degree of freedom at 2, effect size at 0.25, and power at 80, the study found a minimum sample size of 52. However, in order to accommodate for possible attrition or loss during the study, a total of 75 patients (25 per group) was included. The participants were randomly assigned to one of three treatment groups using permuted block randomization; the McKenzie Protocol (MP) Group (MPG) (n = 29), MP plus Static Back Endurance Exercise Group (MPSBEEG) (n = 27) and MP plus Dynamic Back Endurance Exercise Group (MPDBEEG) (n = 28). Sixty seven (32 males (47.8%) and 35 females (52.2%) participants completed the eight week study. Twenty five participants completed the study in MPG, 22 in MPSBEEG and 20 in MPDBEEG. A total drop-out rate of 20.2% was observed in the study. Fourteen percent of participants in MPG were lost to follow-up. Nineteen percent of the participants in MPSBEEG dropped out (out of these, 40% were lost to follow-up while 60% absconded due to improvement in their health condition). In the MPDBEEG, 28.6% of the participants dropped out (37.5% were lost to follow-up while 62.5% absconded due to improvement in their health condition).
Treatment was given thrice weekly for eight weeks and outcomes were assessed at the end of the fourth and eighth week of study. Ethics and Research Committee of the Obafemi Awolowo University Teaching Hospitals Complex and the joint University of Ibadan /University College Hospital Institutional Review Committee respectively gave approval for the study.
Instruments
A height meter calibrated from 0-200cm was used to measure the height of each participant to the nearest 0.1cm. A weighing scale was used to measure the body weight of participants in kilograms to the nearest 1.0Kg. It is calibrated from 0 – 120kg. A metronome (Wittner Metronom system Maelzel, Made in Germany) was used to set a uniform tempo for dynamic back endurance muscles endurance test, which involves repeated contraction or movements over a period of time performed synchronously to the metronome beat. Patients lay on a plinth for the MP, static and dynamic back endurance exercise respectively.
General Health Status Questionnaire – Short Form -36 (SF-36) was used to assess the quality of life of the participants. The SF-36 has been recommended in the assessment of patients with long-term LBP [24, 44, 45]. A Yoruba translated version of the Health Status Questionnaire (SF-36) was used for participants who were literate in the Yoruba language and preferred the Yoruba version. The translation was done at the department of linguistics and African languages of Obafemi Awolowo University, Ile Ife. Pearson product moment correlation coefficient (r) of 0.84 was obtained for the criterion validity of the back translation of the Yoruba version. Quadruple Visual Analogue Scale (QVAS) was used to assess pain intensity of participants. QVAS is a reliable and valid method for pain measurement [46, 47]. A Yoruba translated version of the QVAS was used for participants who were literate in the Yoruba language and prefers the Yoruba version. The translation was done at the department of linguistics and African languages of Obafemi Awolowo University, Ile Ife. Pearson product moment correlation coefficient (r) of 0.88 was obtained for the criterion validity of the back translation of the Yoruba version.
Treatment
Treatment for the different groups (MPG, MPSBEEG and MPDBEEG) comprised three phases including warm up, main exercise and cool down. Prior to treatment, the participants were instructed in details on the study procedures. This was followed by a low intensity warm-up phase of five minutes duration comprising active stretching of the upper extremities and low back and strolling at self-determined pace around the research venue. Treatment also ended with a cool-down phase comprising of the same low intensity exercise as the warm-up for about five minutes.
The McKenzie Protocol (MP) involved a course of specific lumbosacral repeated movements in extension that cause the symptoms to centralize, decrease or abolish. The determination of the direction preference for extension was followed by the main MP activities including �Extension lying prone�, �Extension In Prone� and �Extension in standing�. The MP also included a set of back care education instructions which comprised a 9 item instructional guide on standing, sitting, lifting and other activities of daily living for home exercise for all the participants (Appendix).
In addition to completing the MP (i.e., back extension exercises plus the back care education), static back extensors endurance exercise which included five different static exercises differentiated by the alteration of the positions of the upper and lower limbs with the patient in prone lying on a plinth was carried out [48]. The participants began the exercise training programme with the first exercise position, but progressed to the next exercises at their own pace when they could hold a given position for 10 seconds. On reaching the fifth progression, they continued with the fifth progression until the end of the exercise programme [48, 49]. The following were the five exercise progressions:
Participant lay in prone position with both arms by the sides of the body and lifting the head and trunk off the plinth from neutral to extension;
Participant lay in prone position with the hands interlocked at the occiput so that shoulders were abducted to 90� and the elbows flexed, and lifting the head and trunk off the plinth from neutral to extension;
Participant lay in prone position with both arms elevated forwards, and lifting the head, trunk and elevated arms off the plinth from neutral to extension;
Participant lay in prone position and lifting the head, trunk and contralateral arm and leg off the plinth from neutral to extension; and
Participant lay in prone position with both shoulders abducted and elbows flexed to 90�, and lifting the head, trunk and both legs (with knees extended) off the plinth.
If pain was aggravated during the exercise, the participant was asked to stop. If the pain diminished within 5 minutes after the exercise, he/she was asked to continue the exercise but to hold the exercise position for only 5 seconds. The participant was asked to progress to 10 seconds if there was no adverse response. Each exercise was repeated 9 times. After 10 repetitions, the participant was instructed to rest for between 30 seconds to 1 minute. Static holding time in the exercise position was gradually increased to 20 seconds to provide a greater training stimulus [50, 51]. The dosage of series of 10 repetitions was adopted from a previous protocol for participants with sub-acute LBP [52].
In addition to completing the MP, dynamic back extensors endurance exercise which included five different isokinetic exercises differentiated by the alteration of the positions of the upper and lower limbs with the patient in prone lying on a plinth was carried out. The dynamic back endurance exercise was an exact replica of the static back extensors endurance exercise protocol in terms of exercise positions, progressions and duration. However, instead of static posturing of the trunk in the prone lying position and holding the positions of the upper and lower limbs suspended in the air during all the five exercise progressions for the 10 seconds, the participant was asked to move the trunk and the suspended limbs 10 times.
If pain was aggravated during the exercise, participant was asked to stop. If the pain diminished within 5 minutes after the exercise, the participant was asked to continue the exercise but to carry out only 5 movements in the exercise position. The participant was asked to progress to 10 movements if there is no adverse response. Each exercise was repeated 9 times. After 10 repetitions, the participants were instructed to rest for between 30 seconds to 1 minute. The number of movements of the trunk in the exercise position was gradually increased to 20 seconds to provide a greater training stimulus.
In order to achieve adequate training effect based on recommendation of previous studies, a 30 to 45 minute exercise duration, thrice weekly and eight weeks exercise; and training load of 10 seconds static hold or 10 repetitions per exercise position was adopted [53, 54].
The researchers (CEM and OA) were credentialed in the McKenzie method and supervised the exercises. The researchers were blinded to the recruitment, randomization and assessment procedures which were carried out by an assistant who was blinded to the treatment protocols of the different groups. The research assistant was also credentialed in McKenzie method. The questionnaires used in this study were self- administered.
Data Analysis
Data were analyzed using descriptive of mean and standard deviation; and inferential statistics. One-way ANOVA was used to compare the participants� general characteristics and pain intensity by treatment groups. Pearson’s Product Moment Correlation Analysis was used to test the relationship between HRQoL and intensity of pain. The Kruskal Wallis test was used to compare the treatment outcomes (mean change) on HRQoL across group at week four and eight of the study respectively. Friedman’s ANOVA and Wilcoxon signed ranked tests for multiple comparisons were used to compare within group changes in across the three study time points Alpha level was set at p = 0.05. The data analyses were carried out using SPSS 13.0 version software (SPSS Inc., Chicago, Illinois, USA).
Dr. Alex Jimenez’s Insight
How can the McKenzie method improve an individual’s quality of life? With years of experience working alongside patients to help them recover from a variety of spinal health issues, I’ve seen how debilitating low back pain can be if left untreated for an increased amount of time. Although spinal adjustments and manual manipulations can efficiently help improve symptoms of low back pain, other alternative treatment options may help patients recover faster. The McKenzie method and endurance exercises are used by many healthcare professionals to safely and effectively rehabilitate patients with LBP. The results of the research study ultimately demonstrate how the treatment protocol can help improve an individual’s quality of life.
Results
The mean age, height, weight and BMI of all the participants was 51.8 � 7.35 years, 1.66 � 0.04m, 76.2�11.2 Kg and 27.2 � 4.43 kg/m2 respectively. Comparison of the participants� general characteristics by treatment groups revealed that the participants in the different groups were comparable in their general characteristics (p > 0.05) (Table 1).
Table 1: One-way ANOVA comparison of the participants� general characteristics and pain intensity by treatment groups
The mean pain intensity score (VAS) reported by the participants was 6.55 � 1.75. The relationship between each of the eight domains of HRQoL and intensity of pain (VAS score) is presented in Table 2.
Table 2: Relationship between Health-Related Quality of Life and intensity of pain (VAS score) (n = 67)
From the result, correlation co-efficient (r) ranged between-0.603 to-0.878 at p = 0.001. Table 3 shows the comparison of the participants� baseline measure of HRQoL.
Table 3: Kruskal Wallis comparison of the participants� baseline assessment of HRQoL
The results indicate that the participants in the different treatment groups were comparable in all the domains of HRQoL (p > 0.05). Within-group comparison of HRQoL in MPG, MPSBEEG and MPDBEEG across the 3 time points (weeks 0-4, 4-8 and 0-8) of the study showed that there were significant improvements (p < 0.05) (Table 4). Comparison of treatment outcomes (mean change score (MCS)) at week four and eight of the study are presented in Table 5. There were significant differences in SF-36 scores across the group (p > 0.05) at the end of the 4th and 8th week of the study respectively. The Tukey multiple comparisons post-hoc analysis was used to elucidate where the differences within between groups lie. The result indicated that MPSBEEG and MPDBEEG had significantly higher MCS on all domains of SF-36 compared with MPG at week four and eight respectively (p < 0.05). There was no significant difference between the MPSBEEG and MPDBEEG in the MCS of General Health Perception domain of SF-36 at week four; and on General Health Perception and Physical Functioning Domains of SF-36 at week eight respectively. However, MPDBEE had significantly higher treatment effects on other domains of HRQoL (p = 0.001).
Table 4: Friedman’s ANOVA and Wilcoxon signed ranked test multiple comparisons of HRQoL among MPG, MPSBEEG and MPDBEEG across the 3 time points of the study.
Table 5: Kruskal Wallis comparison of the participants� treatment outcomes (mean change) at week four of the study.
Discussion
This study evaluated the relationship between HRQoL and pain intensity, and the influence of static and dynamic back extensors� endurance exercises on HRQoL in Nigerian patients with LMLBP treated with the MP. The mean age of the patients in this study was 51.8 � 7.35 years. This age falls within the age bracket during which LBP is reported to be a more common problem [55]. From the result of this study, no significant difference in physical characteristics and pain intensity was found in the different treatment groups at baseline. Baseline characteristics are believed to be predictors of response to treatment in clinical trials for LBP [56]. Comparability in baseline measure in clinical trials is reported to reduce the chances of co-founders other than the intervention in predicting outcomes. Therefore, it is implied that the results obtained at different point in the course of this study could have been largely due to the effects of the various treatment regimens.
This study investigated the relationship between HRQoL and the intensity of pain. From the result, significant moderate to high inverse relationships were found between pain intensity and the different domains of HRQoL. General health perception showed the least correlation (r = -0.603; p = 0.001) while social functioning had the highest correlation with pain intensity (r = -0.878; p = 0.001). It is inferred from the study’s result that HRQoL of patients with long-term LBP decreases with severity of pain. Previous studies have reported an association between LBP and psychosocial factors [26, 57]. Specifically, significant inverse correlation has been reported between severity of pain and quality of life in patients with chronic LBP [57�59]. Pain is believed to have a profound effect on HRQoL [59] and the degree, to which the patients believe that they are disabled by it, is a powerful factor in the extent of their quality of life impairments [60]. Therefore, quality of life is an indicator of the level of endurance of people to pain [61].
Within-group comparison of each of MP, MP plus Static Back Endurance Exercise (MPSBEE) and MP plus Dynamic Back Endurance Exercise (MPDBEE) across the 3 time-points (weeks 0-4, 4-8 and 0-8) of the study revealed that each treatment regimen led to significant improvement in HRQoL. Patients in this study displayed baseline values of the SF-36 comparable to those described in other studies on chronic LBP [62]. The baseline values of all domains of the SF-36 observed in this study were lower than those of adult normative data reported by Jenkinson et al [63] leaving room for any improvement accruable to treatment regimens to be assessed. From this study, all the eight domains of the SF-36 significantly improved at the 4th and 8th week assessment. However, on the final assessment, social functioning, general health perception and bodily pain improved more than the other domains of SF-36 in the MPG. General health perception, physical functioning, social functioning, bodily pain and energy vitality improved more than the other domains of SF-36 in the MPSBEEG while general health perception, physical functioning, social functioning, bodily pain and energy vitality improved more than the other domains of SF-36 in the MPDBEEG. Role physical, role emotional and mental health were the least improved domains of the SF-36 among the treatment groups. Though significant improvements were observed in the different domains by treatment groups on final assessment, the values were still lower than the adult normative data for general health status assessed using the SF-36 questionnaire [63]. A previous study by Smeets and colleagues [64] found that active physical therapy regimen primarily designed to improve physiological aspects of LBP such as aerobic fitness level, low back muscle strength and endurance can also reduce the impact of psychosocial factors that it did not deliberately target. In view of current evidence, Hill and Fritz [57] suggest that it may not necessarily follow that a psychologist is better placed to improve treatment outcomes than a physical therapist, even when a goal of treatment is the mediation of a psychosocial factor. Hill and Fritz [57] also argue that psychosocial factors including fear of movement, anxiety, a faulty coping strategy and quality of life have a strong influence on the success of treatment for patients with back pain at a group level. Literature suggests that exercise generally has a potential benefit on psychosocial aspect of patient with long-term LBP. Long-term LBP leads to deconditioning [65] and many problems associated with deconditioning are believed to be reversible through general and specific exercise regimens [66]. Harding and Watson [66] note that improvement in overall physical function is linked with improvement in psychosocial function. Unfortunately, there is a dearth of studies on the effect of the MP and back extensors endurance exercises on HRQoL in patients with long-term mechanical LBP.
From the result of this study, comparison of the different treatment regimens indicate that MPSBEE and MPDBEE had significantly higher treatment effect on all domains of HRQoL compared with MP at week four and eight respectively. MPSBEE and MPDBEE were comparable in their effect on general health perception domain at week four; and on health perception and physical functioning domains of the HRQoL at week eight. However, MPDBEE had significantly higher treatment effects on other domains of HRQoL. Generally, exercise seems to leads to improved wellness and quality of life. Still, there does not appear to be a consensus of opinion on the most effective programme designed to maintain exercise benefits. The McKenzie method is a popular and promising classification-based treatment for LBP among physical therapists [3] in addition to delivering theoretical information in order to educate patients about their condition, so that patients are better able to understand their condition and how to change their behaviour towards an episode of LBP [67]. However, few studies have investigated the effect of the MP on HRQoL in patients with LMLBP. Udermann et al [68] found significant improvements in HRQoL measures in chronic LBP patients treated with MP but reported that the addition of resistance training for the lumbar extensors provided no additional benefit. In recent times, endurance training of the low-back extensors aimed at improving physical performance and psychosocial health in patients with LBP has increased in popularity [69, 48, 52, 70], yet their effectiveness in enhancing quality of life remains unclear [71].
The observed efficacy of the MP, MPSBEE and MPDBEE in this study could be as a result of the fact that each of the regimen contained active exercise carried out in extension positions. Active exercise can be described as functional exercise performed by the patient or client. Previous studies have shown that active exercise, irrespective of the type is more effective in the management of patients with long-term LBP than passive therapy [72, 73]. The MP utilizes a system of patient self generated force to mobilize or manipulate the spine through a series of active repeated movements or static positioning and it is based on the patient’s pain response to certain movements and postures during assessment [3]. Similarly, endurance exercises are active exercises that require static posturing or repeated movements in order to initiate overload stimuli on the musculature. The different treatment regimen in this study had movement components, either from the MP which is the baseline treatment for all the groups or from the back extensors endurance exercise protocols. It is postulated from the results of this study that the significant higher treatment outcome of MPDBEE might be due to the combined effects of movements and overload stimulus on the back extensor muscles. MPDBEE seems to contain movement ingredients, firstly, from the MP which is the baseline treatment for this group and it involved a series of active repeated movements. Secondly, the dynamic back extensors endurance exercise also involved repeated movements of the trunk and limbs in the sagittal plane. It seems that extension exercise with movement elements carried out in patterns similar to the daily tasks motions might help to improve psychosocial aspects of long-term LBP as observed in this study.
Limitations of the Study
The generalizability of the findings of this study is limited by the fact that a generic quality of life tool was employed because of the scarcity of standard HRQoL tools with documented psychometric properties specific for patients with LBP. Theoretically, specific HRQoL measures are opined to be more responsive than generic HRQL measures [74]. Like all other self-reported assessment, it is possible that the patients in this study might have given exaggerated responses or overestimated the effect of exercise on their HRQoL. Furthermore, individuals� perception of psychosocial construct such as HRQoL is believed to be influenced by subjective interpretation and cultural bias [75, 76]. The high drop-out rate observed in this study is also a potential limitation and source of bias which may limit the interpretation and generalizability of study results. Finally, the treatment outcomes of the different regimens were only measured over such a short period of time of eight weeks.
Conclusion
Health-related quality of life of patients with long-term LBP decreases with severity of pain. The McKenzie Protocol, static and dynamic back extensors endurance exercises had significant therapeutic effect on HRQoL in patients with LMLBP. However, the addition of dynamic back extensors endurance exercise to MP led to higher improvement on HRQoL. It is recommended that static or dynamic endurance exercise be combined with MP in patients with LMLBP to derive maximum improvement in general health status.
Acknowledgements
This research was funded by an African Doctoral Dissertation Research Fellowship award offered by the African Population and Health Research Center (APHRC) in partnership with the International Development Research Centre (IDRC). We would like to thank the management and clinicians of the department of physiotherapy OAUTHC, Ile-Ife, Nigeria for their support in carrying out the study. We will also like to thank all the patients who participated in this study.
Competing Interests
The authors declare no competing interests.
Authors� Contributions
All the authors have contributed in this study in ways that comply to the ICMJE authorship criteria. All the authors have read and approved the final version of the manuscript.
In conclusion,�the quality of life of patients with chronic and/or persistent low back pain improved and the pain intensity of the symptoms of LBP appeared to decrease with the use of McKenzie therapy and endurance exercises, according to the study. Furthermore, under the McKenzie treatment protocol, static and dynamic back extensor endurance exercises were recorded to significantly improve symptoms as compared to endurance exercises alone. Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Sciatica
Sciatica is referred to as a collection of symptoms rather than a single type of injury or condition. The symptoms are characterized as radiating pain, numbness and tingling sensations from the sciatic nerve in the lower back, down the buttocks and thighs and through one or both legs and into the feet. Sciatica is commonly the result of irritation, inflammation or compression of the largest nerve in the human body, generally due to a herniated disc or bone spur.
1. Waddell G. London: Churchill Livingstone; 1998. The back pain revolution.
2. Burton AK, Balague F, Cardon G, Eriksen HR, Henrotin Y, Lahad A, et al. On behalf of the COST B13 Working Group on Guidelines for Prevention in Low Back Pain. European guidelines for prevention in low back pain – November 2004. Eur Spine J. 2006;15:s136�168. [PMC free article][PubMed]
3. Mckenzie RA. Waikanae, New Zealand: Spinal Publication Limited; 1990. Treat Your Own Back. Spinal Publication. Pu.
4. Sikorski JM, Stampfer HG, Cole RM, Wheatley AE. Psychological aspects of chronic low back pain. Aust N Zeal J Surg. 1996;66(5):294�7. [PubMed]
5. Filho IT, Simmonds MJ, Protas EJ, Jones S. Back pain, physical function, and estimates of aerobic capacity: what are the relationships among methods and measures? Am J Phys Med Rehabil. 2002;81(12):913�20. [PubMed]
6. Anderson GBJ. Epidemiologic features of chronic low-back pain. Lancet. 1999;354(9178):581�585. [PubMed]
7. World Health Organization (WHO) Scientific Group on the Burden of Musculoskeletal Conditions of the Start of the New Millennium. Geneva: WHO; 2003. The burden of musculoskeletal conditions at the start of the new millennium. [PubMed]
8. Louw QA, Morris LD, Grimmer-Somers K. The prevalence of low back pain in Africa: a systematic review. BMC Musculoskelet Disord. 2007;8:105. [PMC free article][PubMed]
9. van Tulder MW, Koes BW, Bouter LM. Conservative treatment of acute and chronic nonspecific low back pain. A systematic review of randomized controlled trials of the most common interventions. Spine. 1997;22(18):2128�56. [PubMed]
10. Quittan M. Management of Back Pain. Disabil Rehabil. 2002;24(8):423�34. [PubMed]
11. Bigos SJ, McKee J, Holland JP, Holland CL, Hildebrandt J. Back pain; the uncomfortable truth-assurance and activity paradigm. Der Schmertz. 2001;15(6):430�434. [PubMed]
12. Deyo RA, Tsui-Wu YJ. Functional disability due to low-back pain: a population-based study indicating the importance of socioeconomic factors. Arthritis Rheum. 1987;30(11):1247�1253. [PubMed]
13. Coste J, Delecoeuillerie G, Cohen de Lara A, Le Parc JM, Paolaggi JB. Clinical course and prognostic factors of acute low-back pain: an inception cohort study in primary care practice. BMJ. 1994;308(6928):577�80. [PMC free article][PubMed]
14. Picavet HS, Schouten JS. Musculoskeletal pain in the Netherlands: prevalences; consequences and risk groups; the DMC 3-study. Pain. 2003;102(1-2):167�78. [PubMed]
15. Tuzun EH. Quality of life in chronic musculoskeletal pain. Best Pract Res Clin Rheumatol. 2007;21(3):567�579. [PubMed]
17. Linton SJ. A review of psychological risk factors in back and neck pain. Spine. 2000;25(9):1148�56. [PubMed]
18. Scholich SL, Hallner D, Wittenberg RH, Hasenbring MI, Rusu AC. The relationship between pain, disability, quality of life and cognitive-behavioural factors in chronic back pain. Disabil Rehabil. 2012;34(23):1993�2000. [PubMed]
19. Geisser ME, Robinson ME, Miller QL, Bade SM. Psychosocial factors and functional capacity evaluation among persons with chronic pain. J Occup Rehabil. 2003;13(4):259�76. [PubMed]
20. Lam� IE, Peters ML, Vlaeyen JW, Kleef M, Patijn J. Quality of life in chronic pain is more associated with beliefs about pain, than with pain intensity. Eur J Pain. 2005;9(1):15�24. [PubMed]
21. Deyo RA, Andersson G, Bombardier C, Cherkin DC, Keller RB, Lee CK, et al. Outcome measures for studying patients with low back pain. Spine. 1994;19(Suppl 18):2032S�6. [PubMed]
22. Bombardier C. Outcome assessments in the evaluation of treatment of spinal disorders. Spine. 2000;25(24):3100�3. [PubMed]
23. Ware JE, Snow KK, Kosinski M, Gandek B. SF-36 Health Survey – Manual and Interpretation Guide. Boston: The Health Institute; New England Medical Center. 1993;4:3.
24. Ware JE, Jr, Sherbourne CD. The MOS 36-item shortform health survey (SF-36) I. Conceptual framework and item selection. Med Care. 1992;30(6):473�483. [PubMed]
25. Main CJ, George SZ. Psychosocial Influences on Low Back Pain: Why Should You Care? Phys Ther. 2011;91(5):609�13. [PubMed]
26. Vlaeyenm JWS, Kole-Snijders AM, Boeren RG, van Eek H. Fear of movement/(re)injury in chronic low back pain and its relation to behavioral performance. Pain. 1995;62:363�372. [PubMed]
27. Gatchel RJ, Polatin PB, Mayer TG. The dominant role of psychosocial risk factors in the development of chronic low back pain disability. Spine. 1995;20(24):2702�2709. [PubMed]
28. George SZ, Joel E Bialosky, Julie M Fritz. Beliefs Acute Low Back Pain and Elevated Fear-Avoidance Physical Therapist Management of a Patient With. Phys Ther. 2004;84(6):538�549. [PubMed]
29. H�gg O, Burckhardt C, Fritzell C, Nordwall A. Quality of Life in Chronic Low Back Pain: A Comparison with Fibromyalgia and the General Population. J Muscoskel Pain. 2003;11(1):31�38.
30. Woby SR, Watson PJ, Roach NK, Urmston M. Are changes in fear-avoidance beliefs, catastrophizing, and appraisals of control, predictive of changes in chronic low back pain and disability? Eur J Pain. 2004;8(3):201�210. [PubMed]
31. Weiner BK. Spine Update – The Biopsychosocial Model and Spine Care. Spine. 2008;33(2):219�223. [PubMed]
32. Lopez A, Mathers C, Ezzati M, Jamison D, Murray J. Global and regional burden of disease and risk factors, : Systematic analysis of population health data 2001. Lancet. 2006;367(9524):1747�57. [PubMed]
33. Australian Bureau of Statistics (ABS) Canberra: ABS; 2006. Physical activity in Australia: a snapshot, 2004-05. ABS cat. no. 4835.0.55.001.
36. Hayden JA, van Tulder MW, Tomlinson G. Systematic Review: Strategies for using exercise therapy to improve outcomes in chronic low-back pain. Ann Int Med. 2005;142(9):776�785. [PubMed]
38. Cherkin DC, Deyo RA, Battla MC, Street JH, Hund M, Barlow W. A comparison of Physical therapy chiropractice manipulation or an educational booklet for the treatment of low back pain. New Eng J Med. 1998;339(15):1021�1029. [PubMed]
39. McKenzie R, May S. Mechanical diagnosis & therapy. 2nd edition. Vol. 1. Waikanae, New Zealand: Spinal Publications New Zealand Ltd.; 2003. The lumbar spine.
40. Machado LA, de Souza MS, Ferreira PH, Ferreira ML. The McKenzie method for low back pain: a systematic review of the literature with a meta-analysis approach. Spine. 2006;31:254�262. [PubMed]
41. Ayanniyi O, Lasisi OT, Adegoke BOA, Oni-Orisan MO. Management of low back pain: Attitudes and treatment preferences of physiotherapists in Nigeria. Afr J Biomed Res. 2007;10(1):41�49.
42. Mbada CE, Ayanniyi O, Ogunlade SO. Effect of static and dynamic back extensor muscles endurance exercise on pain intensity, activity limitation and participation restriction in patients with long-term mechanical low-back pain. Med Rehabil. 2011;15(3):11�20.
43. Cohen J. In Statistical Power Analyses for Behavioural Sceinces 2nd Ed Chapter 8. New Jersey: Lawrence Erlbaum Associates; 1988. The analysis of variance and covariance: Sample size tables.
44. Bronfort G, Bouter LM. Responsiveness of general health status in chronic low back pain: a comparison of the COOP charts and the SF-36. Pain. 1999;83(2):201�9. [PubMed]
45. Taylor SJ, Taylor AE, Foy MA, Fogg AJB. Responsiveness of common outcome measures for patients with low back pain. Spine. 2001;24(17):1805�1812. [PubMed]
46. Jensen MP, McFarland CA. Increasing the reliability and validity of pain intensity measurement in chronic pain patients. Pain. 1993;55(2):195�203. [PubMed]
47. Von Korff M, Deyo RA, Cherkin D, Barlow SF. Back pain in primary care: Outcomes at 1 year. Spine. 1993:55�862. [PubMed]
48. Moffroid MT, Haugh LD, Haig AJ, Henry SM, Pope MH. Endurance training of trunk extensor muscles. Phys Ther. 1993;73:10�17. [PubMed]
49. Adegoke BOA, Babatunde FO. Effect of an exercise protocol on the endurance of trunk extensor muscles: a RCT. Hong Kong Physiother J. 2007;25:2�9.
50. Petrofsky JS, Lind AR. Aging, isometric strength and endurance; and cardiovascular responses to static effort. J Appl Physiol. 1975;38(1):91�95. [PubMed]
51. Bonde-Petersen F, Mork AL, Nielsen E. Local muscle blood flow and sustained contractions of human arm and back muscles. Eur J Appl Physiol Occup Physiol. 1975;34(1):43�50. [PubMed]
52. Chok B, Lee R, Latimer J, Beng Tan S. Endurance training of the trunk extensor muscles in people with sub acute low back pain. Phys Ther. 1999;79(11):1032�1042. [PubMed]
53. Fox EL, Bowers RW, Foss ML. 4th Ed. Philadelphia: Saunders College; 1988. The physiological basis of physical education and athletics.
54. Liddle SD, Baxter GD, Gracey JH. Exercise and chronic low back pain – what works? Pain. 2004;107(1-2):176�190. [PubMed]
55. Leboeuf-Yde C, Kyvik KO. At what age does low back pain become a common problem? A study of 29;4 24 individuals aged 12-41 years. Spine. 1998;23(2):228�34. [PubMed]
56. Underwood MR, Morton V, Farrin A, UK BEAM trial team Do baseline characteristics predict response to treatment for low back pain? Secondary analysis of the UK BEAM dataset. Rheumatology. 2007;46(8):1297�1302. [PubMed]
57. Hill JC, Fritz JM. Psychosocial influences on low back pain; disability; and response to treatment. Phys Ther. 2011;91(5):712�21. [PubMed]
58. Sengul Y, Kara B, Arda MN. The relationship between health locus of control and quality of life in patients with chronic low back pain. Turk Neurosurg. 2010;20(2):180�185. [PubMed]
59. Tavafian SS, Eftekhar H, Mohammad K, Jamshidi AR, Montazeri A, Shojaeezadeh D, Ghofranipour F. Quality of Life in Women with Different Intensity of Low Back Pain. Iran J Public Health. 2005;34(2):36�39.
60. Turner JA, Jensen MP, Romano JM. Do beliefs, coping, and catastrophizing independently predict functioning in patients with chronic pain. Pain. 2000;85(1-2):115�25. [PubMed]
61. Lyons RA, Lo SV, Littlepage BNC. Comparative health status of patients with 11 common illnesses in Wales. J Epidemiol Community Health. 1994;48(4):388�390. [PMC free article][PubMed]
62. Lurie J. A review of generic health status measures in patients with low back pain. Spine. 2000;25(24):3125�9. [PubMed]
63. Jenkinson C, Coulter A, Wright L. Short form 36 (SF 36) health survey questionnaire: normative data for adults ofworking age. BMJ. 1993;306(6890):143740. [PMC free article][PubMed]
64. Smeets RJ, Vlaeyen JW, Kester AD, Knottnerus JA. Reduction of pain catastrophizing mediates the outcome of both physical and cognitive-behavioral treatment in chronic low back pain. J Pain. 2006;7:261�271. [PubMed]
65. Verbunt JA, Seelen HA, Vlaeyen JW, van de Heijden GJ, Heuts PH, Pons K, Knottnerus JA. Disuse and deconditioning in chronic low back pain: concepts and hypotheses on contributing mechanisms. Eur J Pain. 2003;7(1):9�21. [PubMed]
66. Harding VR, Watson PJ. Increasing Activity & Improving Function In Chronic Pain Management. Physiotherapy. 2000;86(12):619�630.
67. Garcia AN, Gondo FLB, Costa RA, Cyrillo FN, Silva TM, Costa LCM, Costa LOP. Effectiveness of the back school and McKenzie techniques in patients with chronic non-specific low back pain: a protocol of a randomised controlled trial. BMC Musculoskelet Disord. 2011;12:179. [PMC free article][PubMed]
68. Udermann BE, Mayer JM, Donelson RG, Graves JE, Murray SR. Combining lumbar extension training with McKenzie therapy: Effects on pain; disability; and psychosocial functioning in chronic low back pain patients. GLMJ. 2004;3(2):7�12.
69. Kovascs FM, Abraira V, Zamora J, Fernandez C. The transition from acute to subacute and chronic low back pain: A study based on determinants of quality of life and prediction of chronic disability. Spine. 2005;30:1786�1792. [PubMed]
70. Johnson OE, Adegoke BOA, Ogunlade SO. Comparison of four physiotherapy regimens in the treatment of long-term mechanical low back pain. JJPTA. 2010;13(1):9�16. [PMC free article][PubMed]
71. Shaughnessy M, Caulfield B. A pilot study to investigate the effect of lumbar stabilisation exercise training on functional ability and quality of life in patients with chronic low back pain. Int J Rehabil Res. 2004;27(4):297�301. [PubMed]
72. Kank��np�� M, Taimela S, Airaksien OJ, Hannnien O. The efficacy of active rehabilitation in chronic low back pain. Effect on pain intensity; self-experienced disability and lumbar fatigability. Spine. 1999;24(10):1034�42. [PubMed]
73. Rainville J, Hartigan C, Martinez E, Limke J, Jouve C, Finno M. Exercise as a treatment for chronic low back pain. Spine J. 2004;4(1):106�115. [PubMed]
74. Guyatt Gordon. Insights and Limitations from Health-Related Quality-of-Life Research. Gen Intern Med. 1997;12(11):720�721. [PMC free article][PubMed]
75. Kleinman A, Eisenberg L, Good B. Culture, illness and care: clinical lessons from anthropologic and cross-cultural research. Ann Intern Med. 1978;88:251�258. [PubMed]
76. Carr AJ, Higginson IJ. Are quality of life measures patient centred? BMJ. 2001;322(7298):1357�1360. [PMC free article][PubMed]
Muscular energy techniques, or METs, are considered to be some of the most valuable tools any healthcare professional can have and there are several reasons for it. METs have a wide application range and essential modifications can be made for each of them for a variety of injuries and/or conditions. Muscular energy techniques also represent an important aspect of rehabilitation. Furthermore, METs are both gentle and effective. But most importantly, METs actively involve the patient in the recovery process. Unlike other types of treatment therapies, the patient is involved in every step, contracting at the appropriate time, relaxing at the appropriate time, engaging in eye movement, and even breathing when instructed by the healthcare professional.
Muscular energy techniques have been used with other treatment modalities, such as the McKenzie method, to improve the outcome measures of injuries or conditions. The following research study demonstrates clinical and experimental evidence on the impact of the McKenzie method with METs for low back pain, one of the most common complaints affecting spine health. The purpose of the article is to educate and advice patients with low back pain on the use of METs with the McKenzie method.
Impact of McKenzie Method Therapy Enriched by Muscular Energy Techniques on Subjective and Objective Parameters Related to Spine Function in Patients with Chronic Low Back Pain
Abstract
Background: The high incidence and inconsistencies in diagnostic and therapeutic process of low back pain (LBP) stimulate the continuing search for more efficient treatment modalities. Integration of the information obtained with various therapeutic methods and a holistic approach to the patient seem to be associated with positive outcomes.The aim of this study was to analyze the efficacy of combined treatment with McKenzie method and Muscle Energy Technique (MET), and to compare it with the outcomes of treatment with McKenzie method or standard physiotherapy in specific chronic lumbar pain.
Material/Methods: The study included 60 men and women with LBP (mean age 44 years). The patients were randomly assigned to 1 of 3 therapeutic groups, which were further treated with: 1) McKenzie method and MET, 2) McKenzie method alone, or 3) standard physiotherapy for 10 days. The extent of spinal movements (electrogoniometry), level of experienced pain (Visual Analogue Scale and Revised Oswestry Pain Questionnaire), and structure of the spinal discs (MRI) were examined prior to the intervention, immediately thereafter, and 3 months after the intervention.
Results: McKenzie method enriched with MET had the best therapeutic outcomes. The mobility of cervical, thoracic, and lumbar spine normalized at levels corresponding to 87.1%, 66.7%, and 95% of respective average normative values. Implementation of McKenzie method, both alone and combined with MET, was associated with a significant decrease in Oswestry Disability Index, significant alleviation of pain (VAS), and significantly reduced size of spinal disc herniation.
Conclusions: The combined method can be effectively used in the treatment of chronic LBP.
MeSH Keywords:Low Back Pain, Manipulation, Chiropractic, Manipulation, Spinal
Background
Low back pain (LBP) is the most prevalent form of musculoskeletal disorder. According to published statistical data, 70�85% of people experience LBP at some stage of their lives [1�7]. Only 39�76% of the patients recover completely after an acute episode of pain, suggesting that a considerable fraction of them develop a chronic condition [8].
The goals of physiotherapy in patients with chronic LBP include elimination of pain, restoration of the lost extent of movements, functional improvement, and improvement of the quality of life. These objectives are achieved by various protocols of exercise, manipulation, massage, relaxation techniques, and counselling. Although numerous previously published studies have dealt with various therapeutic modalities of LBP, the evidence of their efficacy is highly inconclusive [9�12]. At present the management of chronic LBP still raises many controversies. Inconsistency of established diagnoses and implemented protocols of management points to the importance of the problem in question. Despite extensive research, the issue of spinal pain management still constitutes a challenge for physicians, physiotherapists, and researchers [8,13].
McKenzie method is 1 of many treatment modalities of LBP. It is a system of mechanical diagnosis and management of spinal pain syndromes, based on comprehensive and reproducible evaluation, knowledge of symptoms patterns, directional preference, and centralization phenomenon. This method is focused on the spinal disc disorders [14]. McKenzie method is based on the phenomenon of movement of the nucleus pulposus inside the intervertebral disc, depending on the adopted position and the direction of the movements of the spine. The nucleus pulposus that is exposed to the pressure from both surfaces of the vertebral bodies takes the shape of a spherical joint. This means that it has the ability to perform 3 rotary movements in all directions and has 6 degrees of freedom of movement. The nucleus pulposus performs the movements of flexion, extension, lateral bend (left and right), rotation (right and left), linear displacement (slip) along the sagittal axis, linear displacement along the transverse axis and the separation or approximation along the vertical axis [15].Numerous studies have shown that during forward bend of the spine it is possible to observe extension of the rear surface of the fibrous ring, compressing of the front part of the intervertebral disc and the shift of nucleus pulposus to the dorsal side. When stretching, the mechanism is the opposite [16].
The musculoskeletal system is vital for the maintenance of the balanced tension of the body. Musculofascial disorders can be associated with various problems, pain, or even loss of some motor function. Muscle Energy Techniques (MET) are among the most popular therapeutic modalities aimed at the improvement of elasticity in contractile and non-contractile tissues [17].
High incidence, inconsistencies in diagnostic and therapeutic process, and huge costs associated with the management of chronic spinal disorders stimulate the continuing search for more efficient treatment modalities. This requires the knowledge of neurophysiological processes, proper interpretation of pain, identification of unfavorable motor and postural patterns, holistic approach to the patient, and integration of the information obtained with various therapeutic methods [18].
The aim of this study was to analyze the efficacy of combined treatment with McKenzie method and MET, and to compare it with the outcomes of treatment with McKenzie method or standard physiotherapy in chronic lumbar pain. We evaluated the effect exerted by each of the interventions on the extent of movements, level of experienced pain, and structure of the spinal discs as assessed by means of magnetic resonance imaging.
Material and Methods
Patients
The randomized study included 60 men and women with mean age of 44 years. All individuals were diagnosed by a specialist physician and referred for rehabilitation. The protocol of the study was approved by the Local Bioethical Committee of the Poznan University of Medical Sciences (decision no. 368/0). All patients were diagnosed with chronic spinal pain persisting for longer than 1 year. The inclusion criteria of the study were: 1) documented magnetic resonance imaging (MRI) of the spine, 2) confirmed protrusion or bulging in the lumbosacral spine, 3) intermittent lumbosacral pain, 4) projection of pain to the buttock or thigh, 5) unilateral character of the symptoms. The exclusion criteria were: 1) confirmed extrusion or sequestration of nucleus pulposus of the spinal disc, 2) symptoms manifesting below the knee, 3) history of spinal surgery, 4) structural disorders of spinal discs in more than 2 spinal segments, 5) evident stenosis of the spinal canal, 6) focal lesions of the spinal cord, and 7) spondylolisthesis.
Patients showed great interest and all completed the study.
Protocol
The following tests were used to determine the baseline (i.e. pre-intervention) parameters of the studied patients: 1) electrogoniometric determination of the extent of movement in all spinal segments and angular values of physiological curvatures, 2) Oswestry questionnaire, and 3) Visual Analogue Scale (VAS). Subsequently, the patients were randomly assigned to 1 of 3 therapeutic groups (20 persons each), which were further treated with: 1) McKenzie method and MET, 2) McKenzie method alone, 3) standard physiotherapy. Each of the 3 therapeutic protocols included 10 daily sessions, performed during 5 consecutive weekdays. 24 hours following the last therapeutic session, the same parameters as at the baseline were determined by the investigator blinded to the treatment assignment. Moreover, all patients were subjected to repeated magnetic resonance.
Therapeutic Intervention
McKenzie group One session lasted 30 minutes. On the basis of the McKenzie spinal pain classification, the derangement syndrome was diagnosed in all patients [14]. The therapy included hyperextension techniques, hyperextension with self-pressure or pressure by the therapist, and hyperextensive mobilization. These techniques were applied in the sagittal plane, following the rule of force progression [14]. Moreover, the patients were asked to self-perform the therapeutic procedure at home (5 cycles per day with 2-hour intervals, 15 repetitions each).
McKenzie + MET group The classic McKenzie method enriched with Muscle Energy Technique was implemented. McKenzie protocol in both groups (McKenzie McKenzie + MET) was the same. All patients in this therapeutic group were also diagnosed with the derangement syndrome. A technique of post-isometric relaxation was used at the end of each therapeutic session. It was characterized by the following parameters: 1) time of contraction equal to 7�10 seconds, 2) intensity of contraction corresponding to 20�35%, 3) beginning in the intermediate extent of movement for a given patient, 4) 3 seconds of interval between consecutive contraction phases, 5) 3 repetitions, 6) contraction of antagonist muscle at the terminal phase of the procedure, 7) passive return to the baseline position. The procedure involved relaxation of the erector spinae muscle group and was performed in a sitting position. The exercise was performed in an anterior and lateral flexion, and in rotation. The therapy involved bilateral parts of the erector spinae so as to balance the muscular tension [17]. The duration of 1 combined session was 40 minutes. Patients treated with the combined method were also asked to exercise at home (5 cycles per day with 2-hour intervals, 15 repetitions each).
Standard treatment group Individuals randomized to this therapeutic group were treated with classical massage, laser therapy, and transcutaneous electrical nerve stimulation (TENS) applied to the lumbosacral region. Additionally, the patients were asked to perform general exercises strengthening spinal and abdominal muscles (once a day at home). The exercises were to be performed for 15 minutes, in a prone, supine, and lateral position. The aim of the training was to strengthen the muscles stabilizing the pelvic girdle, i.e. the erector spinae, quadratus lumborum, rectus abdominis, oblique abdominal, gluteal, and iliopsoas muscles. The classical massage lasted 20 minutes. The laser therapy was conducted with a contact technique with Lasertronic LT-2S device. The duration of laser therapy was 80 seconds (2�40 s). The treatment was applied on both sides of the spinous processes of the lumbar spine. The parameters of the procedure were as follows: energy 32 J, power of radiation 400 mW, wavelength 810 nm, continuous mode. TENS electrotherapy was performed with Diatronic DT-10B device. The electrodes were placed on both sides of the lumbosacral spine. The parameters of the TENS procedure were as follows: duration 15 minutes, frequency 50 Hz, current 20�30 mA (subjectively adjusted), duration of a single impulse 50 microseconds. The total time per session=36 min 20 sec + 15 min as home exercises once a day.
Evaluation of Therapeutic Effect
Electrogoniometry The extent of movements and the angles of spinal curvatures were determined with tensiometric Penny & Giles electrogoniometer in Boocok�s modification [19], which prevents potential measurement bias associated with shifting skin and soft tissues in relation to bones. The electrogoniometer enables linear measurement with a bias no greater than 1�. The measurements were taken according to Lewandowski�s methodology [20]. The reliability of these measurements was previously verified by Szulc et al.21 The reference values used in our study were calculated on the basis of Lewandowski�s measurements taken in a group of about 20 000 individuals [20].
Revised Oswestry pain questionnaire The degree to which the dysfunction of the lumbar spine limited the performance of the activities of daily living was determined with the Revised Oswestry Pain Questionnaire [22,23]. We used the revised version of the questionnaire as it is the only variant of this instrument which examines the changes in the level of lumbar pain. The survey was conducted twice, prior to and after the therapy.
Visual analogue scale (VAS) To verify the efficacy of the therapy, the participants were examined with the visual analogue scale (VAS) at the baseline (prior to the intervention) and 24 hours after completing the treatment [24].
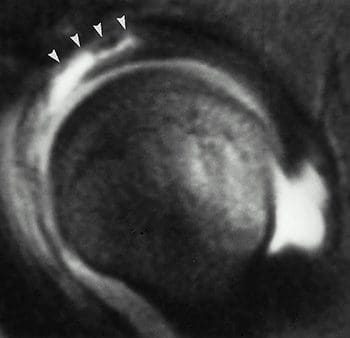
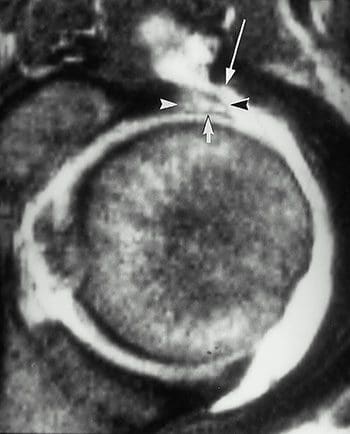
Magnetic resonance imaging The degree of degeneration of the spinal discs and the therapeutic outcome were verified on magnetic resonance imaging performed prior to and after the intervention, at the same time of the day. The examination was conducted in sagittal and axial planes, and used T1- and T2-weighted images. The displacement of the nucleus pulposus was expressed in mm. The methodology of examination was described previously by Fazey et al. [25].
Statistical Analysis
Statistical analysis was conducted with Statistica 10.0 software. Bivariate analysis of variance (AVOVA) with 1 intergroup factor (type of intervention) and 1 intragroup factor (measurement prior to intervention, 24 hours and 3 months after the intervention) was used to analyze the differences in studied parameters resulting from the type of the implemented therapy, and to verify the efficacy of various therapeutic protocols. The significance of differences in multiple comparisons was verified with the Scheff�s post-hoc test.
Dr. Alex Jimenez’s Insight
Low back pain is a common symptom that can be treated in a number of ways. Chiropractic care is one of the most common alternative treatment options for LBP, however, healthcare professionals have started using other treatment modalities to help improve symptoms of low back pain. Physical therapy and exercise have commonly been used together, alongside well-known treatment modalities, to help speed up the patient’s recovery process. The research study aims to determine how the McKenzie method and muscular energy techniques can improve low back pain and promote overall health and wellness. As a doctor of chiropractic, the positive effects of physical therapy and exercise is reflected on the recovery of patients.
Results
The significant effects of bivariate interaction (method � time) suggest that the implemented therapeutic methods exerted variable time-dependent effect on the functional parameters of the spine, Oswestry questionnaire scores, values of visual analog scale, and the results of magnetic resonance imaging in patients with chronic low back pain.
Data on the mobility of various spinal segments prior to the intervention, and 24 hours and 3 months after the intervention suggests that the implementation of McKenzie method enriched with MET was reflected by better therapeutic outcome compared to classical McKenzie method and standard physiotherapy. Mobility of various spinal segments in all axes and planes improved significantly as a result of the therapy with McKenzie method enriched in MET. In contrast, the least pronounced improvement of spinal mobility was documented in the case of standard physiotherapy (Tables 1?�3).
Table 1: Basic statistical characteristics and significance of differences between the angular values of the cervical spine mobility depending on the phase of the study and type of implemented therapeutic method.
Table 2: Basic statistical characteristics and significance of differences between the angular values of the thoracic spine mobility depending on the phase of the study and type of implemented therapeutic method.
Table 3: Basic statistical characteristics and significance of differences between the angular values of the lumbar spine mobility depending on the phase of the study and type of implemented therapeutic method.
The analysis of the anterior flexion of the cervical spine revealed that the improvement of mobility was most pronounced in McKenzie + MET group (?%=42.02). The lack of significant difference between the measurement taken immediately after the intervention and 3 months thereafter suggests that the therapeutic effect was persistent. Less pronounced, albeit significant, improvement of the mobility was also documented in the case of McKenzie method alone (?%=14.79); also this effect persisted after 3 months. In contrast, no significant changes in the extent of anterior flexion of the cervical spine were documented in the group subjected to standard physiotherapy (Figure 1).
Figure 1: Mean angular values of the anterior flexion of the cervical spine determined at various phases of the study in patients treated with three different therapeutic methods (McKenzie method + MET, McKenzie method alone, standard physiotherapy).
Also, the analysis of changes in the degree of thoracic and lumbar spine anterior flexion revealed variability in the outcomes of the studied methods (Figures 2, ?3).
Figure 2: Mean angular values of the anterior flexion of the thoracic spine determined at various phases of the study in patients treated with three different therapeutic methods (McKenzie method + MET, McKenzie method alone, standard physiotherapy).
Figure 3: Mean angular values of the anterior flexion of the lumbar spine determined at various phases of the study in patients treated with three different therapeutic methods (McKenzie method + MET, McKenzie method alone, standard physiotherapy).
The greatest improvement of the mobility, equal to ?%=80.34 and ?%=40.43 in the thoracic and lumbar segment, respectively, was documented in the McKenzie + MET group. The lack of significant difference between the measurements of both the segments taken immediately after the intervention and 3 months thereafter suggests that the therapeutic effect was persistent (Tables 2, ?3). The changes in the remaining functional spinal parameters followed a similar pattern and are summarized in Tables 1?�3.
The degree of mobility in various spinal segments observed after implementation of studied therapeutic methods was compared with respective average normative values published by Lewandowski [20[ (Figures 4?�6). Implementation of McKenzie method enriched with MET was reflected by the most pronounced improvement in the spinal mobility, which fit within the respective normative ranges. The functional parameters of cervical, thoracic, and lumbar spine normalized at levels corresponding to 87.1%, 66.7%, and 95% of respective average normative values.
Figure 4: Functional parameters of the cervical spine (CL � cervical lordosis; CAF � cervical anterior flexion; CPF � cervical posterior flexion; CRF � cervical right flexion; CLF � cervical left flexion; CRR � cervical right rotation; CLR � cervical left rotation) � comparison between values determined in patients treated with three different therapeutic methods and respective normative values published by Lewandowski.
Figure 5: Functional parameters of the thoracic spine (ThK � thoracic kyphosis; ThAF � thoracic anterior flexion; ThPF � thoracic posterior flexion; ThRF � thoracic right flexion; ThLF � thoracic left flexion; ThRR � thoracic right rotation; ThLR � thoracic left rotation) � comparison between values determined in patients treated with three different therapeutic methods and respective normative values published by Lewandowski.
Figure 6: Functional parameters of the lumbar spine (LL � lumbar lordosis; LAF � lumbar anterior flexion; LPF � lumbar posterior flexion; LRF � lumbar right flexion; LLF � lumbar left flexion; LRR � lumbar right rotation; LLR � lumbar left rotation) � comparison between values determined in patients treated with three different therapeutic methods and respective normative values published by Lewandowski.
Irrespective of the therapeutic method and timing of measurement, the angular values of all spinal curvatures fit within the respective normative values and no significant inter- and intragroup differences were documented (Table 4).
Table 4: Basic statistical characteristics and significance of differences between the angular values of the physiological spinal curvatures depending on the phase of the study and type of implemented therapeutic method.
The scores of Oswestry questionnaire also differed depending on the type of implemented intervention. Implementation of McKenzie method, both alone and combined with MET, was reflected by a significant decrease in Oswestry Disability Index. No significant differences were documented between the outcomes of these 2 methods. In contrast, standard physiotherapy had the least pronounced effect on the Oswestry Disability Index (Table 5).
Table 5: Basic statistical characteristics and significance of differences between the Oswestry questionnaire scores, values of visual analogue scale, and magnetic resonance imaging findings depending on the phase of the study and type of implemented therapeutic method.
The analysis of visual analogue scale values suggests that both McKenzie method enriched with MET and classical McKenzie method produced the strongest therapeutic effects, i.e. alleviation of pain. Implementation of both these methods was reflected by marked augmentation of experienced pain, without any significant intergroup differences. In contrast, standard physiotherapy reduced pain to a minimal extent, and no significant differences were observed between VAS scores obtained prior to and after this intervention (Table 5).
Magnetic resonance imaging performed prior to and after the intervention confirmed that McKenzie method enriched with MET produced the best therapeutic outcome manifested by a reduced size of spinal disc herniation. Smaller, albeit significant, improvement of this parameter was also documented in the case of classical McKenzie method. These 2 therapeutic methods did not differ significantly in terms of the post-intervention size of the spinal disc herniation. In contrast, no reduction in the size of the spinal disc herniation was documented after implementation of standard physiotherapy (Table 5).
Discussion
The number of studies validating the efficacy of combined therapeutic methods and techniques is sparse [3,21,26,27]. Wilson et al. [26] concluded that MET is an optimal adjunct technique for other therapeutic modalities [26].
Many studies confirmed the positive effects of McKenzie method [28�36]. Similarly, a body of evidence confirms the therapeutic value of MET [37�44]. Moreover, positive outcomes of both these techniques were documented in patients with spinal pain, including LBP [45,46]. However, to the best of our knowledge, none of the previous studies verified whether the combination of these methods improves the therapeutic outcome.
Noticeably, both the therapies are based on different concepts and involve different therapeutic techniques. The McKenzie method is oriented at the management of all structural abnormalities of the spinal discs. The aim of this therapy is to eliminate pain and normalize function of the affected spinal segment [14]. Therefore, McKenzie method focuses on the treatment of spinal disc pathologies as the principal cause of pain. Takasaki et al. [35] documented positive changes in the spinal disc, i.e. the resolution of herniation, in patient treated with McKenzie method.
However, various injuries and other medical conditions, as well as repetitive negative motor pattern, are also reflected by the disorders of the musculofascial system. This can be reflected by the development of certain compensatory mechanisms, accumulation of muscular tension, motor limitation, and functional disorders [17,40,42]. In contrast, the treatment of the musculofascial system is not included in the concept of McKenzie method. Therefore, the aim of including the muscle energy techniques in the proposed protocol of combined therapy was to potentiate its therapeutic effect through the relaxation and stretching of contracted musculature, strengthening of weakened muscles, reduction of passive muscular tension, improvement of joint mobility, and normalization of motor function [26,43].
The differences observed with regards to the mobility of various spinal segments prior to and after the intervention point to better therapeutic outcome of the combined methods. Noticeably, improved mobility was documented not only in the lumbar spine but also in the cervical and thoracic segment. Therefore, the implementation of MET improved the scope of the combined method (McKenzie + MET) as compared to the classical McKenzie method. Our findings suggest that musculofascial disorders may to a large extent be responsible for limited spinal mobility in patients with chronic LBP. In their papers on the therapeutic effects of manual therapy, Pool et al. [12] and Zaproudina et al. [47] emphasize the importance of limitations in spinal mobility as a sensitive marker of pathological changes.
The magnetic resonance findings documented in patients treated with combined McKenzie method and MET suggest that this combination has no negative effect on the size of spinal disc herniation (Figure 7). This confirms the safety of MET and plausibility of its application in patients with spinal disc pathologies [26]. Of note, relatively large subjective and objective improvements were achieved despite the short duration of the treatment, which included only 10 sessions throughout a 2-week period.
Figure 7: Magnetic resonance images of the structural changes of the L5�S1 spinal disc: (A) prior to, and (B) after the combined therapy (McKenzie method + MET).
Furthermore, control electrogoniometry conducted 3 months after the intervention confirmed the persistent effect of the combined treatment. Moreover, a slight improvement was documented in the case of some functional parameters examined immediately after the intervention and 3 months thereafter. Perhaps, this phenomenon reflected proper education of our patients and further prophylactic self-exercising according to McKenzie method.
Chronic low back pain (CLBP) has a multifactorial etiology [18], and as such requires multimodal treatment. The evidence of therapeutic effects should not be limited to the diagnostic imaging, but mostly be reflected by functionality of a patient, level of experienced pain, extent of movements, and normalization of motor function.
Conclusions
The following conclusions can be formulated on the basis of our findings:
Comparison of the subjective and objective outcomes of 3 therapeutic methods � standard physiotherapy, McKenzie method alone, and McKenzie method combined with MET � in patients with chronic low back pain suggests that the combined method is the most effective.
The use of the combined method (McKenzie + MET) exerts a positive effect on structural (resolution of spinal disc herniation documented on MRI) and functional parameters (improved mobility of various spinal segments), improves the quality of life, and reduces the level of experienced pain.
Acknowledgements
The study was conducted under the auspices of the University School of Physical Education in Poznan. The authors express their gratitude to the owners of the Private Rehabilitation Practice �Antidotum� for consent to perform the study in their facility.
Footnotes
Source of support: The study was supported by the resources from the Ministry of Science and Higher Education for the statutory activity of the Department of Anatomy of the University School of Physical Education in Poznan
Conflict of interest: None declared.
In conclusion, the research study demonstrating clinical and experimental evidence on the impact of the McKenzie method with METs for low back pain, one of the most common complaints affecting spine health, concluded that the combined treatment modalities were effectively used in the improvement of chronic low back pain. The purpose of the article was to educate and advice patients with low back pain on the use of METs with the McKenzie method. Furthermore, the use of the combined treatment modalities demonstrated a positive effect on structural and functional parameters, improving the patient’s quality of life and reducing the level of pain they experienced. Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
[accordions title=”References”]
[accordion title=”References” load=”hide”]1. Drozda K, Lewandowski J, G�rski P. Back pain in lower and upper secondary school pupils living in urban areas of Poland. The case of Poznan. Ortopedia, Traumatologia, Rehabilitacja. 2011;13(5(6)):489�503. [PubMed]
2. Drozda K, Lewandowski J. Epidemiology of back pain among secondary school pupils in Poznan. Fizjoterapia Polska. 2011;4(1):31�40.
3. Dunsford A, Kumar S, Clarke S. Integrating evidence into practice: use of McKenzie-based treatment for mechanical low back pain. J Multidiscip Healthc. 2011;4:393�402. [PMC free article] [PubMed]
4. Joud A, Petersson IF, Englund M. Low back pain: epidemiology of consultations. Arthritis Care Res (Hoboken) 2012;64:b1084�88. [PubMed]
5. Lewandowski J, Szulc P, Boch-Kmieciak J, et al. Epidemiology of low back pain in students of physical education and physiotherapy. Studies in Physical Culture and Tourism. 2011;18(3):265�69.
6. Pereira LM, Obara K, Dias JM, et al. Comparing the Pilates method with no exercise or lumbar stabilization for pain and functionality in patients with chronic low back pain: systematic review and meta-analysis. Clin Rehabil. 2012;26:10�20. [PubMed]
7. Werneke MW, Hart D, Oliver D, et al. Prevalence of classification methods for patients with lumbar impairments using the McKenzie syndromes, pain pattern, manipulation, and stabilization clinical prediction rules. J Man Manip Ther. 2010;18:197�204. [PMC free article] [PubMed]
8. da C Menezes Costa L, Maher CG, Hancock MJ, et al. The prognosis of acute and persistent low-back pain: a meta-analysis. CMAJ. 2012;184:E613�24. [PMC free article] [PubMed]
9. Borges TP, Greve JM, Monteiro AP, et al. Massage application for occupational low back pain in nursing staff. Rev Lat Am Enfermagem. 2012;20:511�19. [PubMed]
10. Cherkin DC, Sherman KJ, Kahn J, et al. A comparison of the effects of 2 types of massage and usual care on chronic low back pain: a randomized, controlled trial. Ann Intern Med. 2011;155:1�9. [PMC free article] [PubMed]
11. Kilpikoski S, Al�n M, Paatelma M, et al. Outcome comparison among working adults with centralizing low back pain: Secondary analysis of a randomized controlled trial with 1-year follow-up. Adv Physiother. 2009;11:210�17.
12. Pool JJ, Ostelo RW, Knol DL, et al. Is a behavioral graded activity program more effective than manual therapy in patients with subacute neck pain? Results of a randomized clinical trial. Spine. 2010;35:1017�24. [PubMed]
13. Frankel BS, Moffett JK, Keen S, et al. Guidelines for low back pain: changes in GP management. Fam Pract. 1999;16:216�22. [PubMed]
14. McKenzie R, May S. The lumbar spine: mechanical diagnosis and therapy. 2nd ed. Waikanae: Spinal Publications; 2003.
15. Kanpandji AI. Anatomia funkcjonalna staw�w. Tom 3.6 ed. Wroc?aw: Elsevier Urban & Partners; 2010. [in Polish]
16. Alexander LA, Hancock E, Agouris I, et al. The response of the nucleus pulposus of the lumbar intervertebral discs to functionally loaded positions. Spine. 2007;32(14):1508�12. [PubMed]
17. Chaitow L. Muscle energy techniques. 3rd ed. Edinburgh: Churchill Livingstone; 2006.
18. O�Sullivan P. It�s time for change with the management of non-specific chronic low back pain. Br J Sports Med. 2012;46:224�27. [PubMed]
19. Boocock MG, Jackson JA, Burton AK, et al. Continuous measurement of lumbar posture using flexible electrogoniometers. Ergonomics. 1994;37:175�85. [PubMed]
20. Lewandowski J. Formation of physiological curvatures and segmental mobility of the human spine aged from 3 to 25 years in electrogoniometric studies. 1st ed. Poznan: AWF Poznan; 2006.
21. Szulc P, Lewandowski J, Marecki B. Verification of selected anatomic landmarks used as reference points for universal goniometer positioning during knee joints mobility range measurements. Med Sci Monit. 2001;7:312�15. [PubMed]
22. Fairbank JC, Pynsent PB. The Oswestry disability index. Spine. 2000;25:2940�52. [PubMed]
23. Hicks GE, Manal TJ. Psychometric properties of commonly used low back disability questionnaires: are they useful for older adults with low back pain? Pain Med. 2009;10:85�94. [PMC free article] [PubMed]
24. Mudgalkar N, Bele SD, Valsangkar S, et al. Utility of numerical and visual analog scales for evaluating the post-operative pain in rural patients. Indian J Anaesth. 2012;56:553�57. [PMC free article] [PubMed]
25. Fazey PJ, Takasaki H, Singer KP. Nucleus pulposus deformation in response to lumbar spine lateral flexion: an in vivo MRI investigation. Eur Spine J. 2010;19(11):1115�20. [PMC free article] [PubMed]
26. Wilson E, Payton O, Donegan-Shoaf L, et al. Muscle energy technique in patients with acute low back pain: a pilot clinical trial. J Orthop Sports Phys Ther. 2003;33:502�12. [PubMed]
27. Bronfort G, Goldsmith CH, Nelson CF, et al. Trunk exercise combined with spinal manipulative or NSAID therapy for chronic low back pain: a randomized, observer-blinded clinical trial. J Manipulative Physiol Ther. 1996;19:570�82. [PubMed]
28. Bybee RF, Olsen DL, Cantu-Boncser G, et al. Centralization of symptoms and lumbar range of motion in patients with low back pain. Physiother Theory Pract. 2009;25:257�67. [PubMed]
29. Chen J, Phillips A, Ramsey M, et al. A case study examining the effectiveness of mechanical diagnosis and therapy in a patient who met the clinical prediction rule for spinal manipulation. J Man Manip Ther. 2009;17:216�20. [PMC free article] [PubMed]
30. Garcia AN, Gondo FL, Costa RA, et al. Effects of two physical therapy interventions in patients with chronic non-specific low back pain: feasibility of a randomized controlled trial. Rev Bras Fisioter. 2011;15:420�27. [PubMed]
31. Hosseinifar M, Akbari M, Behtash H, et al. The effects of stabilization and Mckenzie exerciseson transverse abdominis and multifidus muscle thickness, pain, and disability: A randomized controlled trial in nonspecific chronic low back pain. J Phys Ther Sci. 2012;25:1541�45. [PMC free article] [PubMed]
32. Mbada CE, Ayanniyi O, Ogunlade SO, et al. Influence of Mckenzie protocol and two modes of endurance exercises on health-related quality of life of patients with long-term mechanical low-back pain. Pan Afr Med J. 2014;17(Supp 1):5. [PMC free article] [PubMed]
33. Garcia AN, da Cunha Menezes Costa L, Hancock MJ, et al. Efficacy of the McKenzie method in patients with chronic nonspecific low back pain: a protocol of randomized placebo-controlled trial. Phys Ther. 2015;95:267�73. [PubMed]
34. Schenk RJ, Jozefczyk C, Kopf A. A randomized trial comparing interventions in patients with lumbar posterior derangement. J Man Manip Ther. 2003;11:95�102.
35. Takasaki H, May S, Fazey PJ, et al. Nucleus pulposus deformation following application of mechanical diagnosis and therapy: a single case report with magnetic resonance imaging. J Man Manip Ther. 2010;18:153�58. [PMC free article] [PubMed]
36. Williams B, Vaughn D, Holwerda T. A mechanical diagnosis and treatment (MDT) approach for a patient with discogenic low back pain and a relevant lateral component: a case report. J Man Manip Ther. 2011;19:113�18. [PMC free article] [PubMed]
37. Chugh R, Kalra S, Sharma N, et al. Effects of muscle energy techniques and its comparison to self stretch of bilateral ankle plantarflexors on performance of balance scores in healthy elderly subjects. Physiother Occup Ther J. 2011;4:61�71.
38. Fryer G, Ruszkowski W. The influence of contraction duration in muscle energy technique applied to the atlanto-axial joint. J Osteopath Med. 2004;7:79�84.
39. Fryer G, Pearce AJ. The effect of muscle energy technique on corticospinal and spinal reflex excitability in asymptomatic participants. J Bodyw Mov Ther. 2013;17(4):440�47. [PubMed]
40. Gugliotti M. The use of mobilization, muscle energy technique, and soft tissue mobilization following a modified radical neck dissection of a patient with head and neck cancer. Rehabil Oncol. 2011;29:3�8.
41. K???k?en S, Yilmaz H, Sall? A, U?urlu H. Muscle energy technique versus corticosteroid injection for management of chronic lateral epicondylitis: Randomized controlled trial with 1-year follow-up. Arch Phys Med Rehabil. 2013;94:2068�74. [PubMed]
42. Moore SD, Laudner KG, McLoda TA, et al. The immediate effects of muscle energy technique on posterior shoulder tightness: a randomized controlled trial. J Orthop Sports Phys Ther. 2011;41:400�7. [PubMed]
43. Rajadurai V. The effect of muscle energy technique on temporomandibular joint dysfunction: a randomized clinical trail. Asian J Sci Res. 2011;4:71�77.
44. Shadmehr A, Hadian MR, Naiemi SS, et al. Hamstring flexibility in young women following passive stretch and muscle energy technique. J Back Musculoskelet Rehabil. 2009;22:143�48. [PubMed]
45. Day JM, McKeon P, Nitz A. The efficacy of cervical/thoracic active range of motion for detecting changes associated with individuals receiving muscle energy techniques. Phys Ther Rev. 2010;15:453�61.
46. Day JM, Nitz AJ. The effect of muscle energy techniques on disability and pain scores in individuals with low back pain. J Sport Rehabil. 2012;21:194�98. [PubMed]
47. Zaproudina N, Hietikko T, Hanninen OO, et al. Effectiveness of traditional bone setting in treating chronic low back pain: a randomised pilot trial. Complement Ther Med. 2009;17:23�28. [PubMed][/accordion]
[/accordions]
Additional Topics: Sciatica
Sciatica is referred to as a collection of symptoms rather than a single type of injury or condition. The symptoms are characterized as radiating pain, numbness and tingling sensations from the sciatic nerve in the lower back, down the buttocks and thighs and through one or both legs and into the feet. Sciatica is commonly the result of irritation, inflammation or compression of the largest nerve in the human body, generally due to a herniated disc or bone spur.
These assessment and treatment recommendations represent a synthesis of information derived from personal clinical experience and from the numerous sources which are cited, or are based on the work of researchers, clinicians and therapists who are named (Basmajian 1974, Cailliet 1962, Dvorak & Dvorak 1984, Fryette 1954, Greenman 1989, 1996, Janda 1983, Lewit 1992, 1999, Mennell 1964, Rolf 1977, Williams 1965).
Clinical Application of Neuromuscular Techniques: Scalenes
Box 4.9 Notes on Scalenes
The scalenes are a controversial muscle since they seem to be both postural and phasic (Lin et al 1994), their status being modified by the type(s) of stress to which they are exposed (see Ch. 3 for discussion of this topic).
Janda (1988) reports that �spasm and/or trigger points are commonly present in the scalenes as also are weakness and/or inhibition�.
The attachment sites of the scalene muscles vary, as does their presence. The scalene posterior is sometimes absent, and sometimes blends with the fibres of medius.
Scalene medius is noted to frequently attach to the atlas (Gray 1995) and sometimes extend to the 2nd rib (Simons et al 1998).
The scalene minimus (pleuralis), which attaches to the pleural dome, is present in onethird (Platzer 1992) to three-quarters (Simons et al 1998) of people, on at least one side and, when absent, is replaced by a transverse cupular ligament (Platzer 1992).
The brachial plexus exits the cervical column between the scalenus anterior and medius. These two muscles, together with the 1st rib, form the scalene hiatus (also called the �scalene opening� or �posterior scalene aperture�) (Platzer 1992). It is through this opening�that the brachial plexus and vascular structures for the upper extremity pass. When scalene fibres are taut, they may entrap the nerves (scalene anticus syndrome) or may elevate the 1st rib against the clavicle and indirectly crowd the vascular, or neurologic, structures (simultaneous compromising of both neural and vascular structures is rare) (Stedman 1998). Any of these conditions may be diagnosed as �thoracic outlet syndrome�, which is �a collective title for a number of conditions attributed to compromise of blood vessels or nerve fibers (brachial plexus) at any point between the base of the neck and the axilla� (Stedman 1998).
Assessment of Shortness in Scalenes (14)
Assessment of cervical sidebending (lateral flexion) strength. This involves the scalenes and levator scapulae (and to a secondary degree the rectus capitis lateralis and the transversospinalis group).
The practitioner places a stabilising hand on the top of the shoulder to prevent movement and the other on the head above the ear, as the seated patient attempts to flex the head laterally against this resistance. Both sides are assessed.
Observation assessment (a) There is no easy test for shortness of the scalenes apart from observation, palpation and assessment of trigger point activity/tautness and a functional observation as follows:
In most people who have marked scalene shortness there is a tendency to overuse these (and other upper fixators of the shoulder and neck) as accessory breathing muscles.
There may also be a tendency to hyperventilation (and hence for there to possibly be a history of anxiety, phobic behaviour, panic attacks and/or fatigue symptoms).
These muscles seem to be excessively tense in many people with chronic fatigue symptoms.
The observation assessment consists of the practitioner placing his relaxed hands over the patient�s shoulders so that the fingertips rest on the clav-icles, at which time the seated patient is asked to inhale deeply. If the practitioner�s hands noticeably rise towards the patient�s ears during inhalation then there exists inappropriate use of scalenes, which indicates that they are stressed, which also means that, by definition, they will have become shortened and require stretching treatment.
Observation assessment (b) (Fig. 4.33) Alternatively, during the history taking interview, the patient can be asked to place one hand on the abdomen just above the umbilicus and the other flat against the upper chest.
Figure 4.33 Observation assessment of respiratory function. Any tendency for the upper hand to move cephalad, or earlier than the caudad hand, suggests scalene overactivity.
On inhalation, the hands are observed: if the upper hand initiates the breathing process and rises significantly towards the chin, rather than moving forwards, a pattern of upper chest breathing can be assumed, and therefore stress, and therefore shortness of the scalenes (and other accessory breathing muscles, notably sternomastoid).
MET Treatment of Short Scalenes (Fig. 4.34A, B, C)
Patient lies supine with a cushion or folded towel under the upper thoracic area so that, unless supported by the practitioner�s contralateral hand, the head would fall into extension. The head is rotated contralaterally (away from the side to be treated). There are three positions of rotation required:
Full contralateral rotation of the head/neck produces involvement of the more posterior fibres of the scalenes
A contralateral 45� rotation of the head/neck involves the middle fibres
A position of only slight contralateral rotation involves the more anterior fibres.
The practitioner�s free hand is placed on the side of the patient�s head to restrain the isometric contraction which will be used to release the scalenes. The patient�s head is in one of the above degrees of rotation, supported by the practitioner�s contralateral hand.
Figure 4.34A MET for scalenus posticus. On stretching, following the isometric contraction, the neck is allowed to move into slight extension while a mild stretch is introduced by the contact hand which rests on the second rib, below the lateral aspect of the clavicle.
Figure 4.34B MET treatment for the middle fibres of scalenes. The hand placement (thenar or hypothenar eminence of relaxed hand) is on the 2nd rib below the centre of the clavicle.
Figure 4.34C MET treatment of the anterior fibres of the scalenes; hand placement is on the sternum
The patient is instructed to try to lift the forehead a fraction and to attempt to turn the head towards the affected side, with appropriate breathing cooperation, while resistance is applied by the practitioner�s hand to prevent both movements (�breathe in and hold your breath as you �lift and turn�, and hold this for 7�10 seconds�). Both the effort and, the counter-pressure should be modest and painless at all times.
After a 7�10 second contraction, the head is placed into extension and one hand remains on it to prevent movement during the scalene stretch.
The patient�s contralateral hand is placed (palm down) just inferior to the lateral end of the clavicle on the affected side (for full rotation of the head, posterior scalenes). The practitioner�s hand which was acting to produce resistance to the isometric contraction is now placed onto the dorsum of the patient�s �cushion� hand.
As the patient slowly exhales, the practitioner�s contact hand, resting on the patient�s hand, which is itself resting on the 2nd rib and upper thorax, pushes obliquely away and towards the foot on that same side, following the rib movement into its exhalation position, so stretching the attached musculature and fascia. This stretch is held for at least 20 seconds after each isometric contraction. The process is then repeated at least once more.
The head is rotated 45� contralaterally and the �cushion� hand contact, which applies the stretch of the middle scalenes, is placed just inferior to the middle aspect of the clavicle. When the head is in the almost upright facing position for the anterior scalene stretch, the �cushion� hand contact is on the upper sternum itself.
In all other ways the methodology is as described for the first position above.
NOTE: It is important not to allow heroic degrees of neck extension during any phase of this treatment. There should be some extension, but it should be appropriate to the age and condition of the individual.
A degree of eye movement can assist scalene treatment and may be used as an alternative to the �lift and turn� muscular effort described above. If the patient makes the eyes look caudally (towards the feet) and towards the affected side during the isometric contraction, she will increase the degree of contraction in the muscles. If during the resting phase, when stretch is being introduced, she looks away from the treated side, with eyes looking towards the top of the head, this will enhance the stretch of the muscle.
This whole procedure should be performed bilaterally several times in each of the three head positions. Scalene stretches, with all their variable positions, clearly also influence many of the anterior neck structures.
Dr. Alex Jimenez offers an additional assessment and treatment of the hip flexors as a part of a referenced clinical application of neuromuscular techniques by Leon Chaitow and Judith Walker DeLany. The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
By Dr. Alex Jimenez
Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.
The hips joints join the legs to the trunk of the body, and are formed by the femurs and pelvic bones. The hips are ball-and-socket type joints, where the femoral head (ball) fits into the cup-shaped acetabulum (socket) of the pelvis (Figure 1). When compared to the shoulder, which is also a ball-and-socket joint, the acetabulum is a deeper socket, and encompasses a greater area of the ball, or femoral head. This accommodation is necessary to provide stability for the hip, as it is a major weight-bearing joint, and one of the largest joints in the body. When not weight-bearing, the ball and socket of the hip joint are not perfectly fitted. However, as the hip joint bears more weight, the surface area contact increases, and the joint becomes more stable. When in a standing position, the body�s center of gravity passes through the center of the acetabula. While walking, weight-bearing stresses on the hips can be five times a person�s body weight. Healthy hips can support your weight and allow for pain-free movement. Hip injuries or disease can cause changes that affect your gait, as well as changes that affect the ability of the hips to distribute weight bearing. Abnormal stress is then placed on the joints that are above and below the hips.
The three fused hips or innominate bones that form the acetabulum include the ilium, pubis, and ischium. The ilium forms the superior aspect, the pubis forms the inferior and anterior aspect, and the ischium forms the inferior and posterior aspect. The depth of the acetabulum socket is further increased by the attached fibrocartilaginous labrum (Figure 2). In addition to providing stability to the hip joint, the labrum allows flexibility and motion. Hip joint stability can be hampered by injuries resulting from playing sports, running, overuse, or falling, as well as by disease or tumor. MRI of the hips may be ordered to assess the joint(s) for internal derangement, fracture, or degenerative joint disease. A blow to the hip joint or a fall can result in dislocation of the hip, or a hip fracture. Osteoporosis or low bone density can also lead to hip fractures. Successful prevention and/or treatment of osteoporosis may be achieved through nutrition (adequate amounts of calcium, vitamin D and phosphorus), exercise, safety measures, and medications.
Articular cartilage covers the femoral head and the acetabulum (Figure 3). This cartilage is thin but tough, flexible, smooth and slippery, with a rubbery consistency. It absorbs shock, and allows the bones to move against each other easily and without pain. It is kept lubricated by synovial fluid, which is made in the synovial membrane (joint lining). Synovial fluid is both viscous and sticky. This fluid is what allows us to flex our joints under great pressure without wear. The articular cartilage of the hip is typically about � inch thick, except in the posterior aspect of the hip socket (Figure 4). Here, the cartilage is thicker, as this area absorbs most of the force during walking, running, and jumping. MRI of the hip joint can detect problems involving both the articular cartilage and the fibrocartilaginous ring, or labrum. Cartilage has minimal blood vessels, so it is not good at repairing itself. Fraying, fissuring, and other abnormalities or defects of the cartilage can lead to arthritis in the hip joint. Contrast can be directly injected in the hip joint for a detailed look at the cartilage and labrum.
The femurs are the longest bones in the body, with large round heads that rotate and glide within the acetabula of the pelvis. The femoral head is particularly subject to pathologic changes if there is any significant alteration of blood supply (avascular necrosis). The femoral neck connects the head of the femur to the shaft. The neck ends at the greater and lesser trochanters, which are sites of muscle and tendon attachments. A disease characterized by an inadequate blood supply to the femoral head is Legg-Calve-Perthes disease, also known as LCP or simply Perthes disease. This is a degenerative disease of the hip joint that affects children, most commonly seen in boys ages two through twelve. One of the growth plates of the femoral head, the capital femoral epiphysis, is inside the joint capsule of the hip. Blood vessels that feed this epiphysis run along the side of the femoral neck, and are in danger of being torn or �pinched off� if the growth plate is damaged. This can result in a loss of blood supply to the epiphysis, leading to a deformity of the femoral head (Figure 5). The femoral head may become unstable and break easily, which can lead to incorrect healing and deformities of the entire hip joint (Figure 6). Treatment of Perthes disease is centered on the goal of returning the femoral head to a normal shape. Surgical and non-surgical treatments are used, based on the idea of �containment�- holding the femoral head in the acetabulum as much as possible, while still allowing motion of the hip joint for cartilage nutrition and healthy growth of the joint.
High level athletes and active individuals may be susceptible to a hip condition known as Femoro-Acetabular Impingement, or FAI. FAI is characterized by excessive friction in the hip joint. The femoral head and acetabulum rub abnormally, and can create damage to the articular or labral cartilage. FAI is also associated with labral tears, early hip arthritis, hyperlaxity and low back pain. FAI generally occurs in two forms: Cam and Pincer. The Cam form results in abnormal contact between the femoral head and the socket of the hip because the femoral head and neck relationship is aspherical (Figure 7). Males and those involved in significant contact sports typically display Cam impingement. Pincer impingement occurs when the acetabulum covers too much of the femoral head, resulting in the labral cartilage being pinched between the rim of the socket and the anterior femoral head-neck junction (Figure 8). Pincer impingement may be more common in women. Typically, these two forms exist together, and are labeled as �mixed impingement� (Figure 9).
Ewing�s sarcoma is a malignant bone tumor that may affect the pelvis and/or femur, thereby also affecting the stability of the hips. Like Perthes disease, Ewing�s sarcoma is more common in males, typically presenting in childhood or early adulthood. MRI is routinely used in the work-up of these malignant tumors to show bony and soft tissue extent of the tumor, and its relation to nearby anatomic structures (Figure 10). Contrast may be used to help determine the amount of necrosis within the tumor, which aids in determining the response to treatment before surgery.
Figure 10. MRI demonstrating Ewing�s sarcoma.
Ligaments Of The Hips
Hip stability is further increased by three strong ligaments that encompass the hip joint and form the joint capsule. These ligaments connect the femoral head to the acetabulum, with names suggestive of the bones they connect. They include the pubofemoral and iliofemoral ligaments anteriorly, and the ischiofemoral ligament posteriorly (Figure 11). The iliofemoral ligament is the strongest ligament in the body. However, sports and overuse can still result in sprains of these sturdy ligaments of the joint capsules of the hips. A smaller ligament, the ligamentum teres, is an intracapsular ligament that connects the tip of the femoral head to the acetabulum (Figure 12). A small artery within this ligament brings some of the blood supply to the femoral head. Damage to the ligamentum teres, and its enclosed artery, can result in avascular necrosis.
Muscles & Tendons Of The Hips
The muscles of the thigh and lower back work together to keep the hip stable, in alignment, and able to move. The hip gains stability because the hip muscles do not attach right at the joint. Hip muscles allow the movements of flexion, extension, abduction, adduction, and medial and lateral rotation. To better understand the functions of the muscles surrounding the hip, they can be divided into groups based on their locations- anterior, posterior, and medial.
The anterior thigh muscles are the main hip flexors, and are located anterior to the hip joint. Seventy percent of the thigh�s muscle mass is made up of the quadriceps femoris muscle, so named because it arises from four muscle heads- the rectus femoris, vastus medialis, vastus intermedius, and vastus lateralis (Figures 13, 14). The rectus femoris is the only one of the �quad� muscles to cross the hip joint. The sartorius muscle is found anterior to the quadriceps, and also serves as an abductor and lateral rotator of the hip. The most powerful of the anterior thigh hip flexors is the iliopsoas, which originates in the low back and pelvis and attaches at the lesser trochanter.
Posterior hip muscles include those of both the thigh and gluteal regions. The posterior thigh muscles are also known as the hamstrings- semimembranosus, semitendinosus, and biceps femoris (Figure 15). These muscles originate at the inferior pelvis, and are the extensors for the hip. They are active in normal walking motions. When the hamstrings are �tight�, they limit hip flexion when the knee joint is extended (bending forward from the waist with knees straight), and can limit lumbar movement, leading to back pain. The gluteal muscles include the gluteus maximus, medius, and minimus, six deep muscles that serve as lateral rotators, and the tensor fasciae latae. The three gluteals and the anterior sartorius muscle are all involved in abduction. The gluteus maximus is the main hip extensor, and is the most superficial of the gluteal muscles. It is involved in running and walking uphill, and assists with normal tone of the iliotibial band, which lies lateral to it. The gluteus medius and minimus both insert at the greater trochanter of the femur. The minimus is the deepest of the three gluteal muscles. Anterior to the gluteus minimus is the tensor fasciae latae muscle. It is a flexor and medial rotator of the hip, originating from the anterior superior iliac spine (ASIS) and inserting on the iliotibial band. The term �tensor fasciae latae� defines this muscle�s job- �muscle that stretches the band on the side�. This muscle helps the iliopsoas, gluteus medius, and gluteus minimus muscles during flexion, abduction and medial rotation of the thigh by making the iliotibial band taut, thereby steadying the trunk and stabilizing the hip (Figure 16). The iliotibial band or tract is not a muscle, but a thickened, fibrous band of deep fascia, or connective tissue. It is found at the lateral aspect of the thigh, and runs from the ilium to the tibia. It encloses the muscles and helps with lateral stabilization of the knee joint, as well as helping to maintain both hip and knee extension. Tightening of the iliotibial (IT) band typically causes more problems at the knee as opposed to the hip, but hip pain can result from the IT band rubbing as it passes over the greater trochanter.
The medial thigh (groin) muscles include five muscles of adduction, and one lateral rotator (Figures 17, 18). The lone lateral rotator is the obturator externus, which covers the external surface of the obturator foramen in the deep upper medial thigh. The adductors include the gracilis, the pectineus, and the adductor brevis, longus and magnus. The gracilis is the longest adductor, extending from the medial inferior aspect of the pubic bone, to the medial aspect of the tibia. The adductor magnus is the most massive of the medial muscles of the thigh.
The tendons and muscles of the hips are very powerful and create great forces, making them prone to inflammation and irritation. Tendonitis of the hip can result from repetitive movements involving the soft tissues surrounding the hip joint. Overuse of the hip joint in fitness workouts can lead to tendonitis. Tendons lose their elasticity as we age, resulting in swelling and irritation when the tendons are no longer �gliding� on their normal paths. Iliopsoas tendonitis plays a major role in snapping hip syndrome, or dancer�s hip. A snapping sensation when the hip is flexed and extended may be accompanied by an audible snapping or popping noise, as well as pain. This can be both an extra-articular and an intra-articular occurrence. Extra-articular snapping is often found in those patients with a leg length difference (the longer leg is symptomatic), those with tightness of the iliotibial band on the involved side, and those with weak hip abductors and external rotators. Lateral extra-articular snapping can be caused by the iliotibial band, tensor fascia latae or gluteus medius tendon as they slide back and forth across the greater trochanter (Figure 19). If any of these connective tissue bands thickens, they can �catch� on the greater trochanter during the motion of hip extension, thereby creating the �snapping� sensation and sound. Medial extra-articular snapping, which is less common, can occur when the iliopsoas tendon catches on the anterior inferior iliac spine, lesser trochanter, or iliopectineal ridge during hip extension. Intra-articular snapping hip syndrome is similar in many ways to the extra-articular type, but often involves an underlying mechanical problem in the lower extremity, and more intense pain. Intra-articular snapping may be indicative of a torn acetabular labrum, recurrent hip subluxation, a tear of the ligamentum teres, loose bodies, articular cartilage damage, or synovial chondromatosis (cartilage formations in the synovial membrane of the joint). Snapping hip syndrome is usually found in those ages 15-40, often in those in training for the military. It can also affect athletes, especially those involved in dance, gymnastics, soccer, and track and field. These athletes will all be performing repeated hip flexions, which can lead to tendonitis in the hip area. The repetitive motions of those involved in weightlifting and running generally lead to a thickening of the tendons in the hip region, rather than snapping hip syndrome. Prevention, or at least a lessening, of this syndrome may be found with increased stretching of the iliopsosas muscle or the iliotibial band. Surgery is usually not required, unless intra-articular pathology is present.
Figure 19. Hip muscles.
Tendon or muscle strains can occur suddenly, as in sports injuries, or they can develop over time, with symptoms including pain, swelling, muscle spasms, and difficulty moving certain muscles. MRI can be used to detect tendon and muscle tears and strains, as well as bone tumors and infection. MRI has shown good accuracy for the diagnosis of tears of the gluteus medius and gluteus minimus tendons, which are both abductor tendons of the hip. An association was found between these tears and areas of high signal intensity superior or lateral to the greater trochanter on T2-weighted images, tendon elongation in the gluteus medius, and tendon discontinuity (Figure 20). STIR and fat-suppressed T2-weighted coronal images are very sensitive for detection of areas of high signal intensity superior to the greater trochanter. Coronal T1-weighted images demonstrate tendon elongation in the gluteus medius (Figure 21). Axial images may prove superior for localizing involvement to individual abductor tendons and confirming tendon discontinuity (Figure 22). Tears of the abductor tendons may be the leading cause of greater trochanteric pain syndrome.
Figure 20. Sag. T2 shows high signal intensity superior to greater trochanter (gt) corresponding to swollen bursa (*).
Figure 21. Coronal STIR shows high signal intensity superior to greater trochanter in bursa (*) between gluteus medius (me) and gluteus minimus (mi) tendons.
Figure 22. Axial T2 shows high signal intensity corresponding to fluid replacing distal rt. gluteus medius tendon (black arrow); normal left tendon (white arrow).
Nerves Of The Hips
The nerves of the hip supply the various muscles in the hip area. The major nerves include the femoral, obturator, and lateral femoral cutaneous nerves anteriorly, and the large sciatic nerve posteriorly (Figure 23). The femoral nerve innervates the quadriceps femoris and sartorius, and is the sensory nerve to the anterior thigh. Trauma to this nerve usually occurs in the pelvis, as it passes through or near the psoas muscle. The obturator nerve passes along the lateral pelvic wall and through the obturator foramen, then splits into branches that supply the adductor muscle group. This nerve can also be subject to trauma in the pelvis due to its passage through the obturator foramen. The lateral femoral cutaneous nerve is a sensory nerve that travels along the anterolateral aspect of the thigh. It supplies sensation to the skin surface of the thigh. This is the single nerve involved in a painful condition called meralgia paresthetica, which is characterized by tingling, numbness, and burning pain in the outer part of the thigh. Meralgia paresthetica results from focal entrapment of the lateral femoral cutaneous nerve as it passes through the tunnel formed by the lateral attachment of the inguinal ligament and the ASIS. The posterior sciatic nerve passes deep to the gluteus maximus into the posterior thigh, where it innervates the hamstring muscles, on its way down to the lower leg and foot. The sciatic nerve is approximately as big around as the thumb, and is the largest single nerve in the human body. It can be injured in cases of posterior hip dislocation. Pressure on this nerve can cause nerve pain, numbness, tingling and weakness (sciatica symptoms) in the buttocks, leg, or foot, depending on the site of origin of the sciatic nerve compression.
Figure 23. Anterior and posterior views of the nerves of the hip.
Arteries & Veins Of The Hips
The arterial blood vessels that supply the hips are branches of the internal and external iliacs. The internal iliac artery gives off the superior and inferior gluteals, and the obturator artery. The inferior gluteal flows to the posterior aspect of the hip joint and proximal femur, where it joins a branch of the femoral artery. The obturator artery runs through the obturator foramen, and sends its acetabular branch to the ligamentum teres as part of the blood supply to the femoral head. The external iliac becomes the femoral artery, which has numerous branches that supply the hip and proximal femur. The largest femoral branch is the profunda femoris, which branches superiorly into the medial and lateral circumflex femorals (Figure 24). The circumflex femorals and the inferior gluteal artery contribute to the anastomoses to supply the femoral head, femoral neck, and the hip joint. The medial circumflex also has an acetabular branch to the ligamentum teres. Congenital anomalies in the hip anastomoses, degenerative processes, and trauma can all compromise the blood supply to the hip joint area.
Figure 24. Anterior and posterior views of the arteries of the hip.
Venous flow in the hip and proximal femur typically follows the arterial flow, including the same names for the vessels. The deep veins of the hip and thigh can be the origination of a deep vein thrombosis, which can result in a pulmonary embolus. This can be caused by immobility after hip surgery, sitting in cars or airplanes for extended trips, being overweight, or slow or low blood flow. These blood clots can break off, travel through the larger veins of the thigh and hip, continue through the heart, and become lodged in the smaller vessels of the lung. MRI is being used more frequently to diagnose this very serious condition.
Bursae Of The Hips
The hip joint is surrounded by bursae, similar to the shoulder. These fluid-filled sacs are lined with a synovial membrane, which produces synovial fluid. Their function is to lessen the friction between tendon and bone, ligament and bone, tendons and ligaments, and between muscles. There may be as many as 20 bursae around the hip. If they become infected or inflamed, the result is a painful condition called bursitis. Common hip bursae that may become inflamed include the greater trochanteric bursa, the iliopsoas bursa, and the ischial bursa (Figure 25). The greater trochanteric bursa is sandwiched between the greater trochanter of the femur, and the muscles and tendons that cross over it. If this bursal sac becomes inflamed, patients experience pain with every step they take, as each step requires the tendon to move over the femur at the hip joint. A tight iliotibial band can also cause irritation of the greater trochanteric bursa. Iliopsoas bursitis can result from irritation of the bursa found between the hip joint and the iliopsoas muscle that passes in front of it. Another common site for bursitis is the ischial bursa, which acts as a lubricating pad between tendons and the ischial tuberosity, which is the bony prominence of the pelvis that you sit on. The ischial bursa acts to prevent destruction of the tendons as they move over the ischial tuberosity. Prolonged sitting can cause ischial bursitis. Inflammation around the ischial tuberosity can irritate the sciatic nerve, and trigger symptoms similar to sciatica. Hip bursitis is seen in runners and athletes in sports that involve excessive running (soccer, football, etc.). It can also be caused by an injury (traumatic bursitis), and is seen in post-op hip replacement and hip surgery patients. Treatment for hip bursitis typically includes rest, anti-inflammatory medications, and ice. It may become necessary to aspirate the bursa, which can be combined with a cortisone injection. MRI may be needed if the diagnosis is unclear, or if the problem does not resolve with normal treatments.
Figure 25. Bursae of the hip.
Axial Scans
When positioning unilateral axial slices for the hip, a coronal image can be used to ensure inclusion of all pertinent anatomy. The slices should extend superiorly to include the entire femoral head and acetabulum, and inferiorly to include anatomy below the lesser trochanter. The slices should be aligned perpendicular to the shaft of the femur, as seen in the coronal image in Figure 39.
Figure 39. Axial slice setup using sagittal and coronal images.
For bilateral axial hip slice setup, parameters may have to be altered to maintain adequate resolution with the larger FOV that is required (Figure 40). The slice group may require angulation to maintain alignment of the femoral heads on the resultant images.
Figure 40. Bilateral axial slice setup using a coronal image.
Coronal Scans
Coronal slices of the hip should cover the area from the posterior margin to the anterior margin of the femoral head. The area from the proximal margin of the femoral shaft to the greater sciatic notch should be included in the image (Figure 41). Slices may be angled so that they are parallel to the femoral neck. Thinner slices may be requested for coronal scanning.
Figure 41. Coronal slice setup using axial and sagittal images.
Sagittal Scans
Sagittal slices of the hip should extend past the greater trochanter laterally, and through the acetabulum medially. The slices should be aligned along the long axis of the femur, and perpendicular to the coronal slices, as seen in the coronal image in Figure 42. Two different slice groups will be necessary when performing bilateral sagittal scans.
Figure 42. Sagittal slice setup using coronal and axial images.
Hips Arthrography
MR hip arthrography is often times referred to as the gold standard for assessment of the labrum of the hip. The most clinically significant abnormal findings that result from hip arthrography are labral detachments and tears. Detachment of the labrum, which is more common than a labral tear, can be diagnosed from the appearance of the injected contrast at the acetabular-labral interface (Figure 43). A labral tear can result in injected contrast appearing within the substance of the labrum (Figure 44). Contrast injection is necessary to differentiate torn or detached labra from other pathologic conditions, which may have separate signal intensities. The sensitivity and accuracy for the diagnosis of labral tears and detachment with MR arthrography vs. nonarthrographic MR is 90%. Hip arthrography with MR can also depict intrarticular loose bodies, osteochondral abnormalities, and abnormalities of soft-tissue structures.
Hip arthrography can be performed under fluoro in the x-ray dept., with the patient being moved to the MRI dept. for further imaging, or the entire procedure can be performed in the MRI suite, if MR compatible supplies are available for interventional techniques. The patient should be securely positioned with the hips in internal rotation.
T1-weighted imaging is performed post-contrast to visualize the high signal of the intraarticular contrast. T1 gradient echo sequences offer the benefits of thin sections, elimination of partial volume averaging, and increased detection of small tears. Fatsat sequences are helpful in increasing the contrast between the injected contrast and the adjacent soft tissue. STIR or fatsat T2 sequences performed in the coronal plane may help to detect unsuspected pathologic conditions in the soft tissue and adjacent osseous structures.
Post-contrast axial oblique images have been shown to optimize the detection of the most common sports-related acetabular labral tears, which are anterior or anterosuperior in location. Using a mid-coronal localizer, the axial oblique slices should be prescribed parallel to the long axis of the femoral neck.
Figure 43. Labral detachment as seen in a fat-suppressed T1-wtd. sag. image; arrowheads indicate involvement of anterior and anterosuperior labrum.
Figure 44. Labral tear as seen in a T1-wtd. image; arrowheads indicate enlarged labrum; short arrow indicates linear intralabral collection of contrast material; long arrow indicates communication between the joint and the iliopsoas bursa.
blank
References:
Kapit, Wynn, and Lawrence M. Elson. The Anatomy Coloring Book. New York: HarperCollins, 1993.
Hip Anatomy, Function, and Common Problems. (Last updated 28July2010). Retrieved from http://healthpages.org/anatomy-function/hip-structure-function-common-problems/
Cluett, J. M.D. (Updated 22May2012). Labral Tear of the Hip Joint. Retrieved from http://orthopedics.about.com/od/hipinjuries/qt/labrum.htm
Hughes, M. D.C. (15July2010). Diseases of the Femur Bone. Retrieved from http://www.livestrong.com/article/175599-diseases-of-the-femur-bone/
A Patient�s Guide to Perthes Disease of the hip. (n.d.). Retrieved from http://www.orthopediatrics.com/docs/Guides/perthes.html
Hip Injuries and Disorders. (Last reviewed 10February2012). Retrieved from http://nlm.nih.gov/medlineplus/hipinjuriesanddisorders.html
Ligament of head of femur. (Updated 20December2011). Retrieved from http://en.wikipedia.org/wiki/Ligament_of_head_of_femur
Ewing�s sarcoma. (Last modified 06January2012). Retrieved from http://en.wikipedia.org/wiki/Ewing%27s_sarcoma
Hip Anatomy. (n.d.). Retrieved from http://www.activemotionphysio.ca/Injuries-Conditions/Hip
Iliotibial Band Friction Syndrome. (n.d.). Retrieved from http://www.physiotherapy-treatment.com/iliotibial-band-friction-syndrome.html
Snapping hip syndrome. (Last modified 09November2011). Retrieved from http://en.wikipedia.org/wiki/Snapping_hip_syndrome
Sekul, E. (Updated 03February2012). Meralgia Paresthetica. Retrieved from http://emedicine.medscape.com/article/1141848-overview
Yeomans, S. D.C. (Updated 07July2010). Sciatic Nerve and Sciatica. Retrieved from http://www.spine-health.com/conditions/sciatica/sciatic-nerve-and-sciatica
Mayo Clinic staff. (26July2011). Meralgia paresthetica. Retrieved from http://www.mayoclinic.com/health/meralgia-paresthetica/DS00914
Deep Vein Thrombosis (DVT)-Blood Clots in the Legs. (n.d.). Retrieved from http://catalog/nucleusinc.com/displaymonograph.php?MID=148
Petersilge, C. M.D. (03May2000). Chronic Adult Hip Pain: MR Arthrography of the Hip. Retrieved from http://radiographics.rsna.org/content/20/suppl_1/S43.full
Acetabular branch of medial circumflex femoral artery. (Last modified 17November2011). Retrieved from http://en.wikipedia.org/wiki/Acetabular_branch_of_medial_circumflex_femoral_artery
Cluett, J. M.D. (Updated 26March2011). Hip Bursitis. Retrieved from http://orthopedics.about.com/cs/hipsurgery/a/hipbursitis.htm
Steinbach, L. M.D., Palmer, W. M.D., Schweitzer, M. M.D. (10June2002). Special Focus Session MR Arthrography. Retrieved from http://radiographics.rsna.org/content/22/5/1223.full
Schueler, S. M.D., Beckett, J.M.D., Gettings, S.M.D. (Last updated 05August2010). Ischial Bursitis/Overview. Retrieved from http://www.freemd.com/ischial-bursitis/overview.htm
Hwang, B., Fredericson, M., Chung, C., Beaulieu, C., Gold, G. (29October2004). MRI Findings of Femoral Diaphyseal Stress Injuries in Athletes. Retrieved from http://www.ajronline.org/content/185/1/166.full.pdf
The Femur (Thigh Bone). (n.d.). Retrieved from http://education.yahoo.com/reference/gray/subjects/subject/59
Norman, W. PhD, DSc. (n.d.). Joints of the Lower Limb. Retrieved from http://home.comcast.net/~wnor/lljoints.htm
Femur. (Last modified 24September2012). Retrieved from http://en.wikipedia.org/wiki/Femur
Wheeless, C. III, M.D. (Last updated 25April2012). Ligaments of Humphrey and Wrisberg. Retrieved from http://wheelessonline.com/ortho/ligaments_of_humphrey_and_wrisberg
Muscle Strains in the Thigh. (Last reviewed August2007). Retrieved from http://orthoinfo.aaos.org/topic.cfm?topic=A00366
Shiel, W. Jr., M.D. (Last reviewed 23July2012). Hamstring Injuries. Retrieved from http://www.medicinenet.com/hamstring_injury/article.htm
Hamstring Muscle Injuries. (Last reviewed July 2009). Retrieved from http://orthoinfo.aaos.org/topic.cfm?topic=a00408
Knee. (Last modified 19September2012). Retrieved from http://en.wikipedia.org/wiki/Knee
DeBerardino, T. M.D. (Updated 30March2012). Quadriceps Injury. Retrieved from http://emedicine.medscape.com/article/91473-overview
Kan, J.H. (n.d.). Osteochondral Abnormalities: Pitfalls, Injuries, and Osteochondritis Dissecans. Retrieved from http://www.arrs.org/shopARRS/products/s11p_sample.pdf
Nerves of the Lower Limb. (Last updated 30March2006). Retrieved from http://download.videohelp.com/vitualis/med/lowrnn.htm
The Adductor Canal. (Last updated 30March2006). Retrieved from http://download.videohelp.com/vitualis/med/addcanal.htm
Nabili, S. M.D. (n.d.). Varicose Veins & Spider Veins. Retrieved from http://www.medicinenet.com/varicose_veins/article.htm
Basic Venous Anatomy. (n.d.). Retrieved from http://vascular-web.com/asp/samples/sample104.asp
Femoral nerve. (Last modified 23September2012). Retrieved from http://en.wikipedia.org/wiki/Femoral_nerve
Peron, S. RDCS. (Last modified 16October2010). Anatomy � Lower Extremity Veins. Retrieved from http://www.vascularultrasound.net/vascular-anatomy/veins/lower-extremity-veins
Medical Multimedia Group, L.L.C. (n.d.). Knee Anatomy. Retrieved from http://www.eorthopod.com/content/knee-anatomy
Knee Joint Anatomy, Function and Problems. (Last updated 06July2010). Retrieved from http://healthpages.org/anatomy-function/knee-joint-structure-function-problems/
Coronary ligament of the knee. (Last modified 09May2010). Retrieved from http://en.wikipedia.org/wiki/Coronary_ligament_of_the_knee
Walker, B. (n.d.). Patellar Tendonitis Treatment � Jumper�s Knee. Retrieved from http://www.thestretchinghandbook.com/archives/patellar-tendonitis.php
Osgood-Schlatter disease. (Last reviewed 12November2010). Retrieved from http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0002238/
Grelsamer, R. M.D. (n.d.). The Anatomy of the Patella and the Extensor Mechanism. Retrieved from http://kneehippain.com/patient_pain_anatomy.php
Oblique popliteal ligament. (Last modified 24March2012). Retrieved from http://en.wikipedia.org/wiki/Oblique_popliteal_ligament
Shiel, W. Jr., M.D. (Last reviewed 27July2012). Chondromalacia Patella (Patellofemoral Syndrome). Retrieved from http://www.medicinenet.com/patellofemoral_syndrome/article.htm
Knee. (Last modified 19September2012). Retrieved from http://en.wikipedia.org/wiki/Knee
Mosher, T. M.D. (Last updated 11April2011). MRI of Knee Extensor Mechanism Injuries Overview of the Knee Extensor Mechanism. Retrieved from http://emedicine.medscape.com/article/401001-overview
Carroll, J. M.D. (December 2007). Oblique Menisco-meniscal Ligament. Retrieved from http://radsource.us/clinic/0712
DeBerardino, T. M.D. (Last updated 30March2012). Medial Collateral Knee Ligament Injury. Retrieved from http://emedicine.medscape.com/article/89890-overview#a0106
Farr, G. (Last updated 31December2007). Joints and Ligaments of the Lower Limb. Retrieved from http://becomehealthynow.com/article/bodyskeleton/951/
Knee anatomy overview. (02March2008). Retrieved from http://www.kneeguru.co.uk/KNEEnotes/node/741
Dixit, S. M.D., Difiori, J. M.D., Burton, M. M.D., Mines, B. M.D. (15January2007). Management of Patellofemoral Pain Syndrome. Retrieved from http://www.aafp.org/afp/2007/0115/p194.html
Knee Muscles. (Last updated 05September2012). Retrieved from http://www.knee-pain-explained.com/kneemuscles.html
Popliteus muscle. (Last updated 20February2012). Retrieved from http://en.wikipedia.org/wiki/Popliteus_muscle
Kneedoc. (10February2011). Nerves. Retrieved from http://thekneedoc.co.uk/neurovascular/nerves
Wheeless, C. III, M.D. (Last updated 15December2011). Popliteal Artery. Retrieved from http://wheelessonline.com/ortho/popliteal_artery
The Popliteal Artery. (n.d.) Retrieved from http://education.yahoo.com/reference/gray/subjects/subject/159
Knee bursae. (Last updated 09May2012). Retrieved from http://en.wikipedia.org/wiki/Bursae_of_the_knee_joint
Hirji, Z., Hunjun, J., Choudur, H. (02May2011). Imaging of the Bursae. Retrieved from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3177464/
Kimaya Wellness Limited. (n.d.). Organ>Popliteal Artery. Retrieved from http://kimayahealthcare.com/OrganDetail.aspx?OrganID=103&AboutID=1
Total Vein Care. (Last updated 24February2012). Varicose Vein Anatomy and Function for Patients. Retrieved from http://www.veincare.com/education/
Tibia. (Last updated 01April2012). Retrieved from http://en.wikipedia.org/wiki/Tibia
Norkus,S., Floyd, R. (Published 2001). The Anatomy and Mechanisms of Syndesmotic Ankle Sprains. Retrieved from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC155405/
Soleus muscle. (Last updated 10April2012). Retrieved from http://en.wikipedia.org/wiki/Soleus_muscle
Achilles Tendinitis. (Last reviewed June2010). Retrieved from http://orthoinfo.aaos.org/topic.cfm?topic=A00147
Wheeless, C. III,M.D. (Last updated 11April2012). Sural Nerve. Retrieved from http://wheelessonline.com/ortho/sural_nerve
Medical Multimedia Group, L.L.C. (Last updated 26July2006). Ankle Syndesmosis Injuries. Retrieved from http://www.orthogate.org/patient-education/ankle/ankle-syndesmosis-injuries.html
Cluett, J. M.D. (Last updated 16September2008). Exertional Compartment Syndrome. Retrieved from http://orthopedics.about.com/od/overuseinjuries/a/compartment.htm
Leg Veins (Thigh, Lower Leg) Anatomy, Pictures and Names. (Last updated 21November2010). Retrieved from http://www.healthype.com/leg-veins-thigh-lower-leg-anatomy-pictures-and-names.html
Cluett, J.M.D. (Last updated 6October2009). Stress Fracture. Retrieved from http://orthopedics.about.com/cs/otherfractures/a/stressfracture.htm
Ostlere, S. (1December2004). Imaging the ankle and foot. Retrieved from http://imaging.birjournals.org/content/15/4/242.full
Inverarity, L. D.O. (Last updated 23January2008). Ligaments of the Ankle Joint. Retrieved from http://physicaltherapy.about.com/od/humananatomy/p/ankleligaments.htm
Golano, P., Vega, J., DeLeeuw, P., Malagelada, F.,Manzanares, M., Gotzens, V., van Dijk, C. (Published online 23March2010). Anatomy of the ankle ligaments:a pictorial essay. Retrieved from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2855022/
Numkarunarunrote, N., Malik, A., Aguiar, R.,Trudell, D., Resnick, D. (11October2006). Retinacula of the Foot and Ankle: MRI with Anatomic Correlation in Cadavers. Retrieved from http://www.ajronline.org/content/188/4/W348.full
Medical Multimedia Group, L.L.C. (n.d.). A Patient�s Guide to Ankle Anatomy. Retrieved from http://www.eorthopod.com/content/ankle-anatomy
The Anterior Tibial Artery. (n.d.). Retrieved from http://education.yahoo.com/reference/gray/subjects/subject/160
Foot and Ankle Anatomy. (Last updated 28July2011). Retrieved from http://northcoastfootcare.com/pages/Foot-and-Ankle-Anatomy.html
Donnelly, L., Betts, J., Fricke, B. (1July2009). Skimboarder�s Toe: Findings on High-Field MRI. Retrieved from http://www.ajronline.org/content/184/5/1481.full
Foot. (Last updated 28August2012). Retrieved from http://en.wikipedia.org/wiki/Foot
Wiley, C. (n.d.). Major Ligaments in the Foot. Retrieved from http://www.ehow.com/list_6601926_major-ligaments-foot.html
Turf Toe: Symptoms, Causes, and Treatments. (Last reviewed 9August2012). Retrieved from http://www.webmd.com/fitness-exercise/turf-toe-symptoms-causes-and-treatments
Cluett, J. M.D. (Last updated 02April2012). Turf Toe. Retrieved from http://orthopedics.about.com/od/toeproblems/p/turftoe.htm
Neurology and the Feet. (n.d.) Retrieved from http://footdoc.ca/www.FootDoc.ca/Website%20Nerves%20Of%20The%20Feet.htm
The Veins of the Lower Extremity, Abdomen, and Pelvis. (n.d.). Retrieved from http://education.yahoo.com/reference/gray/subjects/subject/173
Corley, G., Broderick, B., Nestor, S., Breen, P., Grace, P., Quondamatteo, F., O�Laighin, G. (n.d.). The Anatomy and Physiology of the Venous Foot Pump. Retrieved from http://www.eee.nuigalway.ie/documents/go_anatomy_of_the_plantar_venous_plexus_manuscript.pdf
Morton�s neuroma. (Last modified 8August2012). Retrieved from http://en.wikipedia.org/wiki/Morton%27s_metatarsalgia
Acknowledging statistical data, low back pain can be the result of a variety of injuries and/or conditions affecting the lumbar spine and its surrounding structures. Most cases of low back pain, however, will resolve on their own in a matter of weeks. But when symptoms of low back pain become chronic, its essential for the affected individual to seek treatment from the most appropriate healthcare professional. The McKenzie method has been used by many healthcare specialists in the treatment of low back pain and its effects have been recorded widely throughout various research studies. The following two articles are being presented to evaluate the McKenzie method in the treatment of LBP in comparison to other types of treatment options.
Efficacy of the McKenzie Method in Patients With Chronic Nonspecific Low Back Pain: A Protocol of Randomized Placebo-Controlled Trial
Presented Abstract
Background: The McKenzie method is widely used as an active intervention in the treatment of patients with nonspecific low back pain. Although the McKenzie method has been compared with several other interventions, it is not yet known whether this method is superior to placebo in patients with chronic low back pain.
Objective: The purpose of this trial is to assess the efficacy of the McKenzie method in patients with chronic nonspecific low back pain.
Design: An assessor-blinded, 2-arm, randomized placebo-controlled trial will be conducted.
Setting: This study will be conducted in physical therapy clinics in S�o Paulo, Brazil.
Participants: The participants will be 148 patients seeking care for chronic nonspecific low back pain.
Intervention: Participants will be randomly allocated to 1 of 2 treatment groups: (1) McKenzie method or (2) placebo therapy (detuned ultrasound and shortwave therapy). Each group will receive 10 sessions of 30 minutes each (2 sessions per week over 5 weeks).
Measurements: The clinical outcomes will be obtained at the completion of treatment (5 weeks) and at 3, 6, and 12 months after randomization. The primary outcomes will be pain intensity (measured with the Pain Numerical Rating Scale) and disability (measured with the Roland-Morris Disability Questionnaire) at the completion of treatment. The secondary outcomes will be pain intensity; disability and function; kinesiophobia and global perceived effect at 3, 6, and 12 months after randomization; and kinesiophobia and global perceived effect at completion of treatment. The data will be collected by a blinded assessor.
Limitations: Therapists will not be blinded.
Conclusions: This will be the first trial to compare the McKenzie method with placebo therapy in patients with chronic nonspecific low back pain. The results of this study will contribute to better management of this population.
Subject:Therapeutic Exercise, Injuries and Conditions: Low Back, Protocols
Issue Section:Protocol
Low back pain is a major health condition associated with a high rate of absenteeism from work and a more frequent use of health services and work leave entitlements.[1] Low back pain recently was rated by the Global Burden of Disease Study as one of the 7 health conditions that most affect the world’s population,[2] and it is considered a debilitating health condition that affects the population for the greatest number of years over a lifetime.[2] The point prevalence of low back pain in the general population is reported to be up to 18%, increasing to 31% in the last 30 days, 38% in the last 12 months, and 39% at any point in life.[3] Low back pain also is associated with high treatment costs.[4] It is estimated that in European countries, the direct and indirect costs vary from �2 to �4 billion a year.[4] The prognosis of low back pain is directly related to the duration of the symptoms.[5,6] Patients with chronic low back pain have a less favorable prognosis compared with patients with acute low back pain[5,7] and are responsible for most of the costs for management of back pain, generating the need for research aimed at finding better treatments for these patients.
There is a great variety of interventions for the treatment of patients with chronic low back pain, including the McKenzie method developed by Robin McKenzie in New Zealand in 1981.[8] The McKenzie method (also known as Mechanical Diagnosis and Therapy [MDT]) is an active therapy that involves repeated movements or sustained positions and has an educational component with the purpose of minimizing pain and disability and improving spinal mobility.[8] The McKenzie method involves the assessment of symptomatic and mechanical responses to repeated movements and sustained positions. Patients’ responses to this assessment are used to classify them into subgroups or syndromes called derangement, dysfunction, and posture.[8�10] Classification according to one of these groups guides the treatment principles.
Derangement syndrome is the largest group and characterized by patients who demonstrate centralization (transition of pain from distal to proximal) or disappearance of pain[11] with repeated movement testing in one direction. These patients are treated with repeated movements or sustained positions that could reduce pain. Patients classified as having dysfunction syndrome are characterized by pain that occurs only at the end of the range of motion of only one movement.[8] The pain does not change or centralize with repeated movement testing. The treatment principle for patients with dysfunction is repeated movements in the direction that generated the pain. Finally, patients classified as having postural syndrome experience intermittent pain only during sustained positioning at the end of the range of motion (eg, sustained slumped sitting).[8] The treatment principle for this syndrome consists of posture correction.[11]
The McKenzie method also includes a strong educational component based on the books titled The Lumbar Spine: Mechanical Diagnosis & Therapy: Volume Two[11] and Treat Your Own Back.[12] This method, unlike other therapeutic methods, aims to make the patients as independent of the therapist as possible and thus capable of controlling their pain through postural care and the practice of specific exercises for their problem.[11] It encourages patients to move the spine in the direction that is not harmful to their problem, thus avoiding movement restriction due to kinesiophobia or pain.[11]
Two previous systematic reviews have analyzed the effects of the McKenzie method[9,10] in patients with acute, subacute, and chronic low back pain. The review by Clare et al[9] demonstrated that the McKenzie method showed better results in short-term pain relief and improvement of disability compared with active interventions such as physical exercise. The review by Machado et al[10] showed that the McKenzie method reduced pain and disability in the short term when compared with passive therapy for acute low back pain. For chronic low back pain, the 2 reviews were unable to draw conclusions about the effectiveness of the McKenzie method due to the lack of appropriate trials. The randomized controlled trials that have investigated the McKenzie method in patients with chronic low back pain[13�17] compared the method with other interventions such as resistance training,[17] the Williams method,[14] unsupervised exercises,[16] trunk strengthening,[15] and stabilization exercises.[13] Better results in reducing pain intensity were obtained with the McKenzie method compared with resistance training,[17] the Williams method,[14] and supervised exercise.[16] However, the methodological quality of these trials[13�17] is suboptimal.
It is known from the literature that the McKenzie method yields beneficial results when compared with some clinical interventions in patients with chronic low back pain; however, to date, no studies have compared the McKenzie method against a placebo treatment in order to identify its actual efficacy. Clare et al[9] highlighted the need to compare the McKenzie method with placebo therapy and to study the effects of the method in the long term. In other words, it is not known whether the positive effects of the McKenzie method are due to its real efficacy or simply to a placebo effect.
The objective of this study will be to assess the efficacy of the McKenzie method in patients with chronic nonspecific low back pain using a high-quality randomized placebo-controlled trial.
Method
Study Design
This will be an assessor-blinded, 2-arm, randomized placebo-controlled trial.
Study Setting
This study will be conducted in physical therapy clinics in S�o Paulo, Brazil.
Eligibility Criteria
The study will include patients seeking care for chronic nonspecific low back pain (defined as pain or discomfort between the costal margins and the inferior gluteal folds, with or without referred symptoms in the lower limbs, for at least 3 months[18]), with a pain intensity of at least 3 points as measured with the 0- to 10-point Pain Numerical Rating Scale, aged between 18 and 80 years, and able to read Portuguese. Patients will be excluded if they have any contraindication to physical exercise[19] or ultrasound or shortwave therapy, evidence of nerve root compromise (ie, one or more motor, reflex, or sensation deficits), serious spinal pathology (eg, fracture, tumor, inflammatory and infectious diseases), serious cardiovascular and metabolic diseases, previous back surgery, or pregnancy.
Procedure
First, the patients will be interviewed by the study’s blinded assessor, who will determine eligibility. Eligible patients will be informed about the objectives of the study and asked to sign a consent form. Next, the patient’s sociodemographic data and medical history will be recorded. The assessor will then collect the data related to the study outcomes at the baseline assessment, after completion of 5 weeks of treatment, and 3, 6, and 12 months after randomization. With the exception of baseline measurements, all other assessments will be collected over the telephone. All data entry will be coded, entered into an Excel (Microsoft Corporation, Redmond, Washington) spreadsheet, and double-checked prior to the analysis.
Outcome Measures
The clinical outcomes will be measured at the baseline assessment, after treatment, and 3, 6, and 12 months after random allocation. The primary outcomes will be pain intensity (measured with the Pain Numerical Rating Scale)[20] and disability (measured with the Roland-Morris Disability Questionnaire)[21,22] after completion of 5 weeks of treatment. The secondary outcomes will be pain intensity and disability 3, 6, and 12 months after randomization and disability and function (measured by the Patient-Specific Functional Scale),[20] kinesiophobia (measured with the Tampa Scale of Kinesiophobia),[23] and global perceived effect (measured with the Global Perceived Effect Scale)[20] after treatment and 3, 6, and 12 months after randomization. On the day of the baseline assessment, each patient’s expectancy for improvement also will be assessed using the Expectancy of Improvement Numerical Scale,[24] followed by assessment using the McKenzie method.[8] Patients may experience an exacerbation of symptoms after the baseline assessment due to the MDT physical examination. All measurements were previously cross-culturally adapted into Portuguese and clinimetrically tested and are described below.
Pain Numerical Rating Scale
The Pain Numerical Rating Scale is a scale that assesses the levels of pain intensity perceived by the patient using an 11-point scale (varying from 0 to 10), in which 0 represents �no pain� and 10 represents the �worst possible pain.�[20] The participants will be instructed to select the average of pain intensity based on the last 7 days.
Roland-Morris Disability Questionnaire
This questionnaire consists of 24 items that describe daily activities that patients have difficulty performing due to low back pain.[21,22] The higher the number of affirmative answers, the higher the level of disability associated with low back pain.[21,22] The participants will be instructed to complete the questionnaire based on the last 24 hours.
Patient-Specific Functional Scale
The Patient-Specific Functional Scale is a global scale; therefore, it can be used for any part of the body.[25,26] The patients will be asked to identify up to 3 activities that they feel unable to perform or that they have difficulty performing due to their low back pain.[25,26] Measurement will be taken using Likert-type, 11-point scales for each activity, with higher average scores (ranging from 0 to 10 points) representing better ability to perform the tasks.[25,26] We will calculate the average of these activities based on the last 24 hours, with a final score ranging from 0 to 10.
Global Perceived Effect Scale
The Global Perceived Effect Scale is a Likert-type, 11-point scale (ranging from ?5 to +5) that compares the patient’s current condition with his or her condition at the onset of symptoms.[20] Positive scores apply to patients who are better and negative scores apply to patients who are worse in relation to the onset of symptoms.[20]
Tampa Scale of Kinesiophobia
This scale assesses the level of kinesiophobia (fear of moving) by means of 17 questions that deal with pain and intensity of symptoms.[23] The scores from each item vary from 1 to 4 points (eg, 1 point for �strongly disagree,� 2 points for �partially disagree,� 3 points for �agree,� and 4 points for �strongly agree�).[23] For the total score, it is necessary to invert the scores of questions 4, 8, 12, and 16.[23] The final score can vary from 17 to 68 points, with higher scores representing a higher degree of kinesiophobia.[23]
Expectancy of Improvement Numerical Scale
This scale assesses the patient’s expectancy for improvement after treatment in relationship to a specific treatment.[24] It consists of an 11-point scale varying from 0 to 10, in which 0 represents �no expectancy for improvement� and 10 represents �expectancy for the greatest possible improvement.�[24] This scale will be administered only on the first day of assessment (baseline) before the randomization. The reason for including this scale is to analyze whether the expectation of improvement will influence the outcomes.
Random Allocation
Before the treatment begins, the patients will be randomly allocated to their respective intervention groups. The random allocation sequence will be implemented by one of the researchers not involved with recruiting and assessing the patients and will be generated on Microsoft Excel 2010 software. This random allocation sequence will be inserted into sequentially numbered, opaque, sealed envelopes (to ensure that allocation is concealed from the assessor). The envelopes will be opened by the physical therapist who will treat the patients.
Blinding
Given the nature of the study, it is not possible to blind the therapists to the conditions of treatment; however, the assessor and the patients will be blinded to the treatment groups. At the end of the study, the assessor will be asked whether the patients were allocated to the real treatment group or to the placebo group in order to measure assessor blinding. A visual representation of the study design is presented in the Figure.
Figure 1: Flow Diagram of the Study.
Interventions
The participants will be allocated to groups receiving 1 of 2 interventions: (1) placebo therapy or (2) MDT. Participants in each group will receive 10 sessions of 30 minutes each (2 sessions per week over 5 weeks). The studies on the McKenzie method do not have a standard number of sessions given that some studies propose low doses of treatment,[16,17,27] and others recommend higher doses.[13,15]
For ethical reasons, on the first day of treatment, patients from both groups will receive an information booklet called The Back Book,[28] based on the same recommendations as the existing guidelines.[29,30] This booklet will be translated into Portuguese so that it can be completely understood by the study’s participants, who will receive additional explanations regarding the content of the booklet, if needed. Patients will be asked in each session if they have felt any different symptom. The chief investigator of the study will periodically audit the interventions.
Placebo Group
The patients allocated to the placebo group will be treated with detuned pulsed ultrasound for 5 minutes and detuned shortwave diathermy in pulsed mode for 25 minutes. The devices will be used with the internal cables disconnected to obtain the placebo effect; however, it will be possible to handle them and adjust doses and alarms as if they were connected to simulate the pragmatism of clinical practice as well as to increase credibility of use of these devices on the patients. This technique has been used successfully in previous trials with patients with low back pain.[31�35]
McKenzie Group
The patients of the McKenzie group will be treated according to the principles of the McKenzie method,[8] and the choice of therapeutic intervention will be guided by the physical examination findings and classification. Patients also will receive written instructions from the Treat Your Own Back[12] book and will be asked to perform home exercises based on the principles of McKenzie method.[11] The descriptions of the exercises that will be prescribed in this study are published elsewhere.[27] Adherence to home exercises will be monitored by means of a daily log that the patient will fill in at home and bring to the therapist at each subsequent session.
Statistical Methods
Sample Size Calculation
The study was designed to detect a difference of 1 point in pain intensity measured with the Pain Numerical Rating Scale[20 ](estimate for standard deviation=1.84 points)[31] and a difference of 4 points in disability associated with low back pain measured with the Roland-Morris Disability Questionnaire[21,22] (estimate for standard deviation=4.9 points).[31] The following specifications were considered: statistical power of 80%, alpha level of 5%, and follow-up loss of 15%. Therefore, the study will require a sample of 74 patients per group (148 in total).
Analysis of the Effects of Treatment
The statistical analysis of our study will follow intention-to-treat principles.[36] The normality of the data will be tested by visual inspection of histograms, and the characterization of the participants will be calculated using descriptive statistical tests. The between-group differences (effects of treatment) and their respective 95% confidence intervals will be calculated by constructing mixed linear models[37] using interaction terms of treatment groups versus time. We will conduct a secondary exploratory analysis to assess whether patients classified as having derangement syndrome have a better response to the McKenzie method (compared with placebo) than those with other classifications. For this assessment, we will use a 3-way interaction for group, time, and classification. For all of these analyses, we will use the IBM SPSS software package, version 19 (IBM Corp, Armonk, New York).
Ethics
This study was approved by the Research Ethics Committee of the Universidade Cidade de S�o Paulo (#480.754) and prospectively registered at ClinicalTrials.gov (NCT02123394). Any protocol modifications will be reported to the Research Ethics Committee as well as to the trial registry.
Dr. Alex Jimenez’s Insight
Low back pain is one of the most common reasons people seek immediate medical attention for every year. Although many healthcare professionals are qualified and experienced in the diagnosis of the source of the patient’s low back pain, finding the right healthcare specialist who can provide the proper treatment for the individual’s LBP can be the real challenge. A variety of treatments can be used to treat low back pain, however, a wide array of healthcare professionals have started utilizing the McKenzie method in the treatment of patients with nonspecific low back pain. The purpose of the following article is to evaluate the effectiveness of the McKenzie method for low back pain, carefully analyzing the data of the research study.
Discussion
Potential Impact and Significance of the Study
The existing randomized controlled trials investigating the McKenzie method in patients with chronic low back pain have all used an alternative intervention as the comparison group.[14�17] To date, no study has compared the McKenzie method with a placebo treatment in patients with low back pain in order to identify its real efficacy, which is an important gap in the literature.[9] Interpretation of the previous comparative effectiveness studies is limited by the lack of knowledge of the efficacy of the McKenzie method for people with chronic low back pain. This study will be the first to compare McKenzie method with placebo therapy in patients with chronic nonspecific low back pain. A proper comparison against a placebo group will provide more unbiased estimates of the effects of this intervention. This type of comparison has already been done in trials aiming to assess the efficacy of motor control exercises for patients with chronic low back pain,[31] spinal manipulative therapy and diclofenac for patients with acute low back pain,[38] and exercise and advice for patients with subacute low back pain.[39]
Contribution to the Physical Therapy Profession and for Patients
The McKenzie method is one of the few methods used in physical therapy that advocates for the independence of patients.[8,12] This method also provides patients with tools to promote their autonomy in managing the current pain and even future recurrences.[12] We expect that patients treated with the McKenzie method will benefit more than the patients treated with the placebo treatment. If this hypothesis is confirmed in our study, the results will contribute to better clinical decision making of physical therapists. Moreover, the approach has the potential to reduce the burden associated with the recurrent nature of low back pain if patients can better self-manage future episodes.
Strengths and Weaknesses of the Study
This trial contemplates a substantial number of patients to minimize bias, and it was prospectively registered. We will use true randomization, concealed allocation, blinded assessment, and an intention-to-treat analysis. The treatments will be conducted by 2 therapists who were extensively trained to perform the interventions. We will monitor the home exercise program. Unfortunately, due to the interventions, we will not be able to blind the therapists to the treatment allocation. It is known from the literature that the McKenzie method yields beneficial results when compared with some clinical interventions in patients with chronic low back pain.[14�17] To date, however, no studies have compared the McKenzie method with a placebo treatment in order to identify its actual efficacy.
Future Research
The intention of this study group is to submit the results of this study to a top-level, international peer-reviewed journal. These published results may provide a basis for future trials that investigate the effectiveness of the McKenzie method when delivered at different doses (different numbers of sets, repetitions, and sessions), which is still unclear in the literature. Our secondary exploratory analysis aims to assess whether patients classified as having derangement syndrome have a better response to the McKenzie method (compared with placebo treatment) than those with other classifications. This assessment will contribute to a better understanding of possible subgroups of patients with chronic low back pain who respond best to specific interventions. This is an important issue, as exploring subgroups is currently considered the most important research priority in the field of low back pain.[40]
This study was fully funded by S�o Paulo Research Foundation (FAPESP) (grant number 2013/20075-5). Ms Garcia is funded by a scholarship from the Coordination for the Improvement of Higher Education Personnel/Brazilian Government (CAPES/Brazil).
The study was prospectively registered at ClinicalTrials.gov (trial registration: NCT02123394).
Predicting a Clinically Important Outcome in Patients with Low Back Pain Following McKenzie Therapy or Spinal Manipulation: A Stratified Analysis in a Randomized Controlled Trial
Presented Abstract
Background: Reports vary considerably concerning characteristics of patients who will respond to mobilizing exercises or manipulation. The objective of this prospective cohort study was to identify characteristics of patients with a changeable lumbar condition, i.e. presenting with centralization or peripheralization, that were likely to benefit the most from either the McKenzie method or spinal manipulation.
Methods: 350 patients with chronic low back pain were randomized to either the McKenzie method or manipulation. The possible effect modifiers were age, severity of leg pain, pain-distribution, nerve root involvement, duration of symptoms, and centralization of symptoms. The primary outcome was the number of patients reporting success at two months follow-up. The values of the dichotomized predictors were tested according to the prespecified analysis plan.
Results: No predictors were found to produce a statistically significant interaction effect. The McKenzie method was superior to manipulation across all subgroups, thus the probability of success was consistently in favor of this treatment independent of predictor observed. When the two strongest predictors, nerve root involvement and peripheralization, were combined, the chance of success was relative risk 10.5 (95% CI 0.71-155.43) for the McKenzie method and 1.23 (95% CI 1.03-1.46) for manipulation (P?=?0.11 for interaction effect).
Conclusions: We did not find any baseline variables which were statistically significant effect modifiers in predicting different response to either McKenzie treatment or spinal manipulation when compared to each other. However, we did identify nerve root involvement and peripheralization to produce differences in response to McKenzie treatment compared to manipulation that appear to be clinically important. These findings need testing in larger studies.
Electronic supplementary material: The online version of this article (doi:10.1186/s12891-015-0526-1) contains supplementary material, which is available to authorized users.
Keywords:Low back pain, McKenzie, Spinal manipulation, Predictive value, Effect modification
Background
The most recent published guidelines for the treatment of patients with persistent non-specific low back pain (NSLBP) recommend a program focusing on self-management after initial advice and information. These patients should also be offered structured exercises tailored to the individual patient and other modalities such as spinal manipulation [1,2].
Previous studies have compared the effect of the McKenzie-method, also known as Mechanical Diagnosis and Therapy (MDT), with that of spinal manipulation (SM) in heterogeneous populations of patients with acute and subacute NSLBP and found no difference in outcome [3,4].
Recently, the need for studies testing the effect of treatment strategies for subgroups of patients with NSLBP in primary care has been emphasized in consensus-papers [5,6] as well as the current European guidelines [7], based on the hypothesis that subgroup analyses, preferably complying with the recommendations of �Prognostic Factor Research�[8], will improve decision making towards the most effective management strategies. Although initial data show promising results, there is presently insufficient evidence to recommend specific methods of subgrouping in primary care [1,9].
Three randomized studies, comprising patients with predominantly acute or subacute low back pain (LBP), have tested the effects of MDT versus SM in a subgroup of patients that presented with centralization of symptoms or directional preference (favorable response to end range motions) during physical examination [10-12]. The conclusions drawn from these studies were not in concurrence and the usefulness was limited by a low methodological quality.
Our recent randomized study, comprising patients with predominantly chronic LBP (CLBP), found a marginally better overall effect of MDT versus SM in an equivalent group [13]. In order to pursue the idea of subgrouping further, it was part of the study plan to explore predictors based on patient characteristics that could assist the clinician in targeting the most favorable treatment to the individual patient.
The objective of this study was to identify subgroups of patients with predominantly CLBP, presenting with centralization or peripheralization, which were likely to benefit from either MDT or SM two months after the completion of treatment.
Methods
Data Collection
The present study is a secondary analysis of a previously published randomized controlled trial [13]. We recruited 350 patients from September 2003 through May 2007 at an outpatient back care centre in Copenhagen, Denmark.
Patients
Patients were referred from primary care physicians for treatment of persistent LBP. Eligible patients were between 18 and 60 years of age, suffering from LBP with or without leg pain for a period of more than 6 weeks, able to speak and understand the Danish language, and fulfilled the clinical criteria for centralization or peripheralization of symptoms during initial screening. Centralization was defined as the abolition of symptoms in the most distal body region (such as the foot, lower leg, upper leg, buttocks, or lateral low back) and peripheralization was defined as the production of symptoms in a more distal body region. These findings have previously been found to have acceptable degree of inter-tester reliability (Kappa value 0.64) [14]. The initial screening was performed prior to randomization by a physical therapist with a diploma in the MDT examination system. Patients were excluded if they were free of symptoms at the day of inclusion, demonstrated positive non-organic signs [15], or if serious pathology, i.e. severe nerve root involvement (disabling back or leg pain in combination with progressive disturbances in sensibility, muscle strength, or reflexes), osteoporosis, severe spondylolisthesis, fracture, inflammatory arthritis, cancer, or referred pain from the viscera, was suspected based on physical examination and/or magnetic resonance imaging. Other exclusion criteria were application for disability pension, pending litigation, pregnancy, co-morbidity, recent back surgery, language problems, or problems with communication including abuse of drugs or alcohol.
The trial population had predominantly CLBP lasting on average 95 weeks (SD 207), mean age was 37 years (SD10), mean level of back and leg pain was 30 (SD 11.9) on a Numeric Rating Scale ranging from 0 to 60, and mean level of disability was 13 (SD 4.8) on Roland Morris Disability Questionnaire (0-23). Our method of pain measurement reflects that back pain is often a fluctuating condition where pain location and severity might vary on a daily basis. Therefore, a validated comprehensive pain questionnaire [16] was used in order to guarantee that all aspects of back and leg pain intensity were recorded. The scales are outlined in the legend to Table 1.
After baseline measures were obtained, randomisation was carried out by a computer-generated list of random numbers in blocks of ten using sealed opaque envelopes.
Ethics
Ethical approval of the study was granted by Copenhagen Research Ethics Committee, file no 01-057/03. All patients received written information about the study and gave their written consent prior to participation.
Treatments
The practitioners performing the treatments had no knowledge of the results of the initial screening. The treatment programs were designed to reflect daily practice as much as possible. Detailed information on these programs have been published earlier [13].
The MDT treatment was planned individually following the therapist�s pre-treatment physical assessment. Specific manual vertebral mobilization techniques including high velocity thrust were not allowed. An educational booklet describing self care [17] or a �lumbar roll� for correction of the seated position was sometimes provided to the patient at the discretion of the therapist. In the SM treatment, high velocity thrust was used in combination with other types of manual techniques. The choice of combination of techniques was at the discretion of the chiropractor. General mobilizing exercises, i.e. self-manipulation, alternating lumbar flexion/extension movements, and stretching, were allowed but not specific exercises in the directional preference. An inclined wedged pillow for correction of the seated position was available to the patients if the chiropractor believed this to be indicated.
In both treatment groups, patients were informed thoroughly of the results of the physical assessment, the benign course of back pain, and the importance of remaining physically active. Guidance on proper back care was also given. In addition, all patients were provided with a Danish version of �The Back Book� which previously has been shown to have beneficial effect on patients� beliefs about back pain [18]. A maximum of 15 treatments for a period of 12 weeks were given. If considered necessary by the treating clinician, patients were educated in an individual program of self-administered mobilizing, stretching, stabilizing, and/or strengthening exercises at the end of the treatment period. Treatments were performed by clinicians with several years of experience. Patients were instructed to continue their individual exercises at home or at a gym for a minimum of two months after completion of the treatment at the back center. Because the patients suffered predominantly from CLBP we expected this period of self administered exercises to be necessary for the patients to experience the full effect of the intervention. Patients were encouraged not to seek any other kind of treatment during this two months period of self-administered exercises.
Outcome Measures
The primary outcome was the proportion of patients reporting success at follow-up two months after end of treatment. Treatment success was defined as a reduction of at least 5 points or a final score below 5 points on the 23-item modified Roland Morris Disability Questionnaire (RMDQ) [19]. A validated Danish version of RMDQ was used [20]. The definition of treatment success was based on the recommendations by others [21,22]. A sensitivity analysis using 30% relative improvement on RMDQ as definition of success was also performed. In accordance with the protocol [13], we considered a relative between-group difference of 15% in the number of patients with successful outcome to be minimal clinically important in our analysis of interaction.
Prespecified Predictor Variables
In order to reduce the likelihood of spurious findings [23], we restricted the number of candidate effect modifiers in the dataset to six. To increase the validity of our findings, a directional hypothesis was established for each variable according to the recommendations of Sun et al. [24] Four baseline variables have previously been suggested in randomized studies to be predictive of long term good outcome in patients with persistent LBP following MDT in comparison with strengthening training: centralization [25,26], or following SM in comparison to physiotherapy or treatment chosen by a general practitioner: age below 40 years [27,28], duration of symptoms more than 1 year [27], and pain below the knee [29]. As recommended by others [30], another two variables were added based on the participating experienced clinicians� judgments of which characteristics they would expect to predict good outcome from their treatment compared to the other. The additional variables prioritized by the physiotherapists in the MDT group were signs of nerve root involvement and substantial leg pain. The additional variables prioritized by the chiropractors in the SM group were no signs of nerve root involvement and not substantial leg pain.
In a supplementary analysis, we took the opportunity to explore whether the inclusion of further six baseline variables, assumed to have prognostic value for good outcome in either of the treatment groups, would appear to have an effect modifying effect as well. To our knowledge, no further variables from previous one arm studies have been reported to have prognostic value of long term good outcome in patients with persistent LBP following MDT, whereas three variables have been reported to have prognostic value following SM: male gender [28], mild disability [28], and mild back pain [28]. Another three variables were agreed upon by the clinicians to be included in the supplementary analysis as they were assumed by experience from clinical practice to have prognostic value for good outcome regardless of treatment with MDT or SM: low number of days on sick leave past year, high patient expectations to recovery, and high patient expectations about coping with work tasks six weeks after initiation of treatment.
Dichotomization of possible predictor variables were made to allow for comparisons to be made with those of earlier studies. In cases where no cut off values could be found in the literature, dichotomization was performed above/below the median found in the sample. Definitions of variables are presented in the legend to Table 1.
Statistics
The entire intention-to-treat (ITT) population was used in all the analyses. The last score was carried forward for subjects with missing two months RMDQ scores (7 patients in the MDT group and 14 patients in the SM group). In addition, a post hoc per protocol analysis was carried out comprising only those 259 patients that completed the full treatment. The analysis plan was agreed in advance by the trial management group.
The possible predictors were dichotomized and the chance of success was investigated by estimating the relative risk (RR) of success in each of the two strata. The impact of the investigated predictors was estimated by comparing the chance of success between the treatment groups when divided into the two strata. To test for treatment effect modification of the predictors we performed chi-squared tests for interaction between intervention and the two different strata for each of the predictors. This is basically the same as an interaction from a regression model. Confidence intervals were also inspected for potential clinically important effects.
Following the univariate analysis, a multivariate analysis was planned including effect modifiers with a p-value below 0.1.
Dr. Alex Jimenez’s Insight
Low back pain can occur due to several types of injuries and/or conditions and its symptoms may be acute and/or chronic. Patients with low back pain can benefit from a variety of treatments, including chiropractic care. Chiropractic treatment is one of the most common alternative treatment options utilized to treat low back pain. According to the article, the results of the improvement of LBP with spinal adjustments and manual manipulations, along with the use of exercise, vary considerably among the participants. The focus of the following research study is to determine which patients are most likely to benefit from the McKenzie method as compared to spinal adjustments and manual manipulations.
Results
Participants were similar with respect to socio-demographic and clinical characteristics at baseline in the treatment groups. An overview of the distribution of the included dichotomized variables at baseline is provided in Table 1. No differences were found between the treatment groups.
Overall, the post hoc per protocol analysis did not produce outcome results that were different from the results of the ITT analysis and therefore only the results of the ITT analysis will be reported.
Figure 1 presents the distribution of predictors with regards to effect modification in the MDT group versus SM. In all subgroups, the probability of success with MDT was superior to that of SM. Because of low sample size, confidence intervals were wide and none of the predictors had a statistically significant treatment modifying effect. The predictors with a clinically important potential effect in favor of MDT compared to SM were nerve root involvement (28% higher proportion of patients with success when nerve root involvement was present than when absent) and peripheralization of symptoms (17% higher proportion of patients with success in case of peripheralization than in case of centralization). If present, nerve root involvement increased the chance of success following MDT 2.31 times compared to that of SM and 1.22 times if not present. This means that for the subgroup of patients with nerve root involvement receiving MDT, compared to those receiving SM, the relative effect appeared to be 1.89 times (2.31/1.22, P?= 0.118) higher than for the subgroup with no nerve root involvement.
Figure 1: Treatment effect modified by predictors. The top point estimate and confidence intervals indicate overall effect without subgrouping. Subsequent pairs of point estimates and confidence intervals show the chances of treatment success.
Figure 2 presents the modifying effect of a composite of the two predictors with a clinically important potential effect. If signs of nerve root involvement and peripheralization were present at baseline, the chance of success with MDT compared to SM appeared 8.5 times higher than for the subgroup with no centralization and nerve root involvement. The number of patients was very small and the differences were not statistically significant (P?=?0.11).
Figure 2: Impact of the two clinically important predictors combined on treatment effect. RR?=?Relative Risk with Yates correction.
None of the prognostic candidate variables explored in the supplementary analysis appeared to have any clinically important modifying effect (Additional file 1: Table S1).
The results from the sensitivity analysis using 30% relative improvement on RMDQ as definition of success were not markedly different from those presented above (Additional file 2: Table S2).
Discussion
To our knowledge, this is the first study trying to identify effect modifiers when two mobilizing strategies, i.e. MDT and SM, are compared in a sample of patients with as changeable condition characterized by centralization or peripheralization.
Our study found that none of the potential effect modifiers were able to statistically significantly increase the overall effect of MDT compared to that of SM. However, the between-group difference for two of the variables exceeded our clinically important success-rate of 15% in number of patients with successful outcome, so our study is likely to have missed a true effect and, in that sense, did not have a large enough sample size.
The most apparent finding is that in our small subgroup of patients with signs of nerve root involvement, the relative chance of success appeared 1.89 times (2.31/1.22) higher than in patients with no nerve root involvement when treated with MDT, compared to those treated with SM. The difference was in the expected direction.
Although not statistically significant in our small sample, the variable peripheralization exceeded our clinically important success-rate of 15%, but was found not to be in the expected direction. No previous studies have assessed the effect modification of centralization or peripheralization in patients with CLBP. The RCT by Long et al. [25,26] concluded that patients with directional preference, including centralization, fared better 2 weeks after baseline than patients with no directional preference when treated with MDT in comparison with strengthening training. However, the outcome among peripheralizers was not reported, so the poor outcome reported in patients with no directional preference might be related to the subgroup of patients who responded with no change in symptoms during initial examination and not to those that responded with peripheralization. An alternative explanation might be that the effect modifying impact of centralization or peripheralization on MDT is dependent on the control treatment. Our findings suggest that future studies in this area need to involve predictive value of peripheralization as well as centralization.
When a composite of the two most promising predictors, peripheralization and signs of nerve root involvement, were present at baseline, the relative chance of success with MDT compared to SM appeared 8.5 times higher than for the subgroup with no centralization and nerve root involvement. The number of patients was very small and the confidence interval was wide. Therefore only a preliminary conclusion about interaction can be drawn and it calls for a validation in future studies.
In our study, there appeared to be no characteristic by which SM had better results compared to MDT. Thus, we could not support the results of two studies with a similar design as ours (two arms, sample of patients with persistent LBP, and outcome reported in terms of reduction of disability at long term follow up) [27,29]. In those studies, Nyiendo et al. [29] found a modifying effect of leg pain below knee on treatment by SM compared to that of the general practitioner six months after baseline, and Koes et al. [27] found a modifying effect of age below 40 years and symptom duration more than a year on treatment by SM compared to that of physiotherapy 12 months after baseline. However, results from those, as well as other previous RCTs comprising patients with persistent LBP, have supported our findings regarding the lack of effect modification of age [27,29,31], sex [29,31], baseline disability [27,29,31], and duration of symptoms [31], on SM when measured on reduction of disability 6-12 months after randomization. So, although evidence is emerging in patients with acute LBP regarding subgroup characteristics predictive of better results from SM compared to other types of treatment [32], we are still in the dark with respect to patients with persistent LBP.
The usefulness of choosing a criterion for success by combining an improvement of at least 5 points or an absolute score below 5 points on RMDQ is debatable. A total of 22 patients were considered successful based on score below 5 at follow up without having an improvement of at least 5 points. We therefore performed a sensitivity analysis using a relative improvement of at least 30% as criterion of success as recommended by others [22] (see Additional file 2: Table S2). As a result, the percentage of patients with successful outcome in the MDT group remained the same whereas 4 more patients were defined as successes in the SM group. Overall the sensitivity analysis did not produce outcome results that were markedly different from those of the primary analysis and therefore only those have been discussed above.
Strengths and Limitations
This study used data from a RCT, whereas many others have used single arm designs not suitable for the purpose of evaluating treatment effect modification [33]. In accordance with the recommendations by the PROGRESS group [8] we prespecified the possible predictors and also the direction of the effect. Furthermore, we limited the number of predictors included in order to minimize the chance of spurious findings.
The main limitation in secondary studies to previously conducted RCTs is that they are powered to detect overall treatment effect rather that effect modification. In recognition of the post hoc nature of our analysis, reflected in wide confidence intervals, we must emphasize that our findings are exploratory and require formal testing in a larger sample size.
Conclusions
In all subgroups, the probability of success with MDT was superior to that of SM. Although not statistically significant, the presence of nerve root involvement and peripheralization appear promising effect modifiers in favour of MDT. These findings need testing in larger studies.
Acknowledgements
The authors thank Jan Nordsteen and Steen Olsen for clinical expert advice, and Mark Laslett for comments and language correction.
This study was in part supported by grants from The Danish Rheumatism Association, The Danish Physiotherapy Organization, The Danish Foundation for Chiropractic Research and Continuous Education, and The Danish Institute for Mechanical Diagnosis and Therapy. RC/The Parker Institute acknowledge the funding support from the Oak Foundation. The funds were independent of the management, analyses, and interpretation of the study.
Footnotes
Competing interests: The authors declare that they have no competing interests.
Authors� contributions: All authors were involved in the data analysis and the writing process, and the requirements for authorship have been met. All analyses were conducted by TP, RC, and CJ. TP conceived and led the study and was responsible for writing the first draft of the paper, but the other authors have participated throughout the writing process and have read and approved the final version.
In conclusion,�the above two articles were presented in order to evaluate the McKenzie method in the treatment of LBP in comparison to other types of treatment options. The first research study compared the McKenzie method with placebo therapy in patients with low back pain, however, the results of the study still need additional evaluations. In the second research study, no significant results could predict a different response in the use of the McKenzie method. Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
[accordions title=”References”]
[accordion title=”References” load=”hide”]1
Waddell
G
. The Back Pain Revolution
. 2nd ed
. New York, NY
: Churchill Livingstone
; 2004
.
2
Murray
CJ
, Lopez
AD
. Measuring the global burden of disease
. N Engl J Med
. 2013
;369
:448
�457
.
Google Scholar
CrossRef
PubMed
3
Hoy
D
, Bain
C
, Williams
G
, et al.
. A systematic review of the global prevalence of low back pain
. Arthritis Rheum
. 2012
;64
:2028
�2037
.
Google Scholar
CrossRef
PubMed
4
van Tulder
MW
. Chapter 1: European guidelines
. Eur Spine J
. 2006
;15
:134
�135
.
Google Scholar
CrossRef
5
Costa Lda
C
, Maher
CG
, McAuley
JH
, et al.
. Prognosis for patients with chronic low back pain: inception cohort study
. BMJ
. 2009
;339
:b3829
.
Google Scholar
CrossRef
PubMed
6
da C Menezes Costa
, Maher
CG
, Hancock
MJ
, et al.
. The prognosis of acute and persistent low-back pain: a meta-analysis
. CMAJ
. 2012
;184
:E613
�E624
.
Google Scholar
CrossRef
PubMed
7
Henschke
N
, Maher
CG
, Refshauge
KM
, et al.
. Prognosis in patients with recent onset low back pain in Australian primary care: inception cohort study
. BMJ
. 2008
;337
:154
�157
.
Google Scholar
CrossRef
8
McKenzie
R
, May
S
. The Lumbar Spine: Mechanical Diagnosis & Therapy: Volume One
. 2nd ed
. Waikanae, New Zealand
: Spinal Publications
; 2003
.
9
Clare
HA
, Adams
R
, Maher
CG
. A systematic review of efficacy of McKenzie therapy for spinal pain
. Aust J Physiother
. 2004
;50
:209
�216
.
Google Scholar
CrossRef
PubMed
10
Machado
LA
, de Souza
MS
, Ferreira
PH
, Ferreira
ML
. The McKenzie method for low back pain: a systematic review of the literature with a meta-analysis approach
. Spine (Phila Pa 1976)
. 2006
;31
:254
�262
.
Google Scholar
CrossRef
PubMed
11
McKenzie
R
, May
S
. The Lumbar Spine: Mechanical Diagnosis & Therapy: Volume Two
. 2nd ed
. Waikanae, New Zealand
: Spinal Publications
; 2003
.
12
McKenzie
R
. Trate Noc� Mesmo a sua Coluna [Treat Your Own Back]
. Crichton, New Zealand
: Spinal Publications New Zealand Ltd
; 1998
.
13
Miller
ER
, Schenk
RJ
, Karnes
JL
, Rousselle
JG
. A comparison of the McKenzie approach to a specific spine stabilization program for chronic low back pain
. J Man Manip Ther
. 2005
;13
:103
�112
.
Google Scholar
CrossRef
14
Nwuga
G
, Nwuga
V
. Relative therapeutic efficacy of the Williams and McKenzie protocols in back pain management
. Physiother Theory Pract
. 1985
;1
:99
�105
.
Google Scholar
CrossRef
15
Petersen
T
, Larsen
K
, Jacobsen
S
. One-year follow-up comparison of the effectiveness of McKenzie treatment and strengthening training for patients with chronic low back pain: outcome and prognostic factors
. Spine (Phila Pa 1976)
. 2007
;32
:2948
�2956
.
Google Scholar
CrossRef
PubMed
16
Sakai
Y
, Matsuyama
Y
, Nakamura
H
, et al.
. The effect of muscle relaxant on the paraspinal muscle blood flow: a randomized controlled trial in patients with chronic low back pain
. Spine (Phila Pa 1976)
. 2008
;33
:581
�587
.
Google Scholar
CrossRef
PubMed
17
Udermann
BE
, Mayer
JM
, Donelson
RG
, et al.
. Combining lumbar extension training with McKenzie therapy: effects on pain, disability, and psychosocial functioning in chronic low back pain patients
. Gunders Lutheran Medical Journal
. 2004
;3
:7
�12
.
18
Airaksinen
O
, Brox
JI
, Cedraschi
C
, et al.
. Chapter 4: European guidelines for the management of chronic nonspecific low back pain
. Eur Spine J
. 2006
;15
:192
�300
.
Google Scholar
CrossRef
19
Kenney
LW
, Humphrey
RH
, Mahler
DA
. ACSM’s Guidelines for Exercise Testing and Prescription
. Baltimore, MD
: Williams & Wilkins
; 1995
.
20
Costa
LO
, Maher
CG
, Latimer
J
, et al.
. Clinimetric testing of three self-report outcome measures for low back pain patients in Brazil: which one is the best?
Spine (Phila Pa 1976)
. 2008
;33
:2459
�2463
.
Google Scholar
CrossRef
PubMed
21
Costa
LO
, Maher
CG
, Latimer
J
, et al.
. Psychometric characteristics of the Brazilian-Portuguese versions of the Functional Rating Index and the Roland-Morris Disability Questionnaire
. Spine (Phila Pa 1976)
. 2007
;32
:1902
�1907
.
Google Scholar
CrossRef
PubMed
22
Nusbaum
L
, Natour
J
, Ferraz
MB
, Goldenberg
J
. Translation, adaptation and validation of the Roland-Morris questionnaire: Brazil Roland-Morris
. Braz J Med Biol Res
. 2001
;34
:203
�210
.
Google Scholar
CrossRef
PubMed
23
de Souza
FS
, Marinho Cda
S
, Siqueira
FB
, et al.
. Psychometric testing confirms that the Brazilian-Portuguese adaptations, the original versions of the Fear-Avoidance Beliefs Questionnaire, and the Tampa Scale of Kinesiophobia have similar measurement properties
. Spine (Phila Pa 1976)
. 2008
;33
:1028
�1033
.
Google Scholar
CrossRef
PubMed
24
Devilly
GJ
, Borkovec
TD
. Psychometric properties of the credibility/expectancy questionnaire
. J Behav Ther Exp Psychiatry
. 2000
;31
:73
�86
.
Google Scholar
CrossRef
PubMed
25
Chatman
AB
, Hyams
SP
, Neel
JM
, et al.
. The Patient-Specific Functional Scale: measurement properties in patients with knee dysfunction
. Phys Ther
. 1997
;77
:820
�829
.
Google Scholar
PubMed
26
Pengel
LH
, Refshauge
KM
, Maher
CG
. Responsiveness of pain, disability, and physical impairment outcomes in patients with low back pain
. Spine (Phila Pa 1976)
. 2004
;29
:879
�883
.
Google Scholar
CrossRef
PubMed
27
Garcia
AN
, Costa
LCM
, da Silva
TM
, et al.
. Effectiveness of Back School versus McKenzie exercises in patients with chronic nonspecific low back pain: a randomized controlled trial
. Phys Ther
. 2013
;93
:729
�747
.
Google Scholar
CrossRef
PubMed
28
Manchester
MR
, Glasgow
GW
, York
JKM
, et al.
. The Back Book: Clinical Guidelines for the Management of Acute Low Back Pain
. London, United Kingdom
: Stationery Office Books
; 2002
:1
�28
.
29
Delitto
A
, George
SZ
, Van Dillen
LR
, et al.
. Low back pain
. J Orthop Sports Phys Ther
. 2012
;42
:A1
�A57
.
Google Scholar
CrossRef
PubMed
30
van Tulder
M
, Becker
A
, Bekkering
T
, et al.
. Chapter 3: European guidelines for the management of acute nonspecific low back pain in primary care
. Eur Spine J
. 2006
;15
:169
�191
.
Google Scholar
CrossRef
31
Costa
LO
, Maher
CG
, Latimer
J
, et al.
. Motor control exercise for chronic low back pain: a randomized placebo-controlled trial
. Phys Ther
. 2009
;89
:1275
�1286
.
Google Scholar
CrossRef
PubMed
32
Balthazard
P
, de Goumoens
P
, Rivier
G
, et al.
. Manual therapy followed by specific active exercises versus a placebo followed by specific active exercises on the improvement of functional disability in patients with chronic non specific low back pain: a randomized controlled trial
. BMC Musculoskelet Disord
. 2012
;13
:162
.
Google Scholar
CrossRef
PubMed
33
Kumar
SP
. Efficacy of segmental stabilization exercise for lumbar segmental instability in patients with mechanical low back pain: a randomized placebo controlled crossover study
. N Am J Med Sci
. 2012
;3
:456
�461
.
34
Ebadi
S
, Ansari
NN
, Naghdi
S
, et al.
. The effect of continuous ultrasound on chronic non-specific low back pain: a single blind placebo-controlled randomized trial
. BMC Musculoskelet Disord
. 2012
;13
:192
.
Google Scholar
CrossRef
PubMed
35
Williams
CM
, Latimer
J
, Maher
CG
, et al.
. PACE�the first placebo controlled trial of paracetamol for acute low back pain: design of a randomised controlled trial
. BMC Musculoskelet Disord
. 2010
;11
:169
.
Google Scholar
CrossRef
PubMed
36
Hollis
S
, Campbell
F
. What is meant by intention to treat analysis? Survey of published randomised controlled trials
. BMJ
. 1999
;319
:670
�674
.
Google Scholar
CrossRef
PubMed
37
Twisk
JWR
. Applied Longitudinal Data Analysis for Epidemiology: A Practical Guide
. New York, NY
: Cambridge University Press
; 2003
.
38
Hancock
MJ
, Maher
CG
, Latimer
J
, et al.
. Assessment of diclofenac or spinal manipulative therapy, or both, in addition to recommended first-line treatment for acute low back pain: a randomised controlled trial
. Lancet
. 2007
;370
:1638
�1643
.
Google Scholar
CrossRef
PubMed
39
Pengel
LH
, Refshauge
KM
, Maher
CG
, et al.
. Physiotherapist-directed exercise, advice, or both for subacute low back pain: a randomized trial
. Ann Intern Med
. 2007
;146
:787
�796
.
Google Scholar
CrossRef
PubMed
40
Costa Lda
C
, Koes
BW
, Pransky
G
, et al.
. Primary care research priorities in low back pain: an update
. Spine (Phila Pa 1976)
. 2013
;38
:148
�156
.
Google Scholar
CrossRef
PubMed[/accordion]
[accordion title=”References” load=”hide”]1. Chou R, Qaseem A, Snow V, Casey D, Cross JT, Jr, Shekelle P, et al. Diagnosis and treatment of low back pain: a joint clinical practice guideline from the American College of Physicians and the American Pain Society. Ann Intern Med. 2007;147(7):478�91. doi: 10.7326/0003-4819-147-7-200710020-00006. [PubMed] [Cross Ref]
2. NHS Early management of persistent non-specific low back pain. NICE Clinical Guideline. 2009;88:1�30.
3. Cherkin DC, Battie MC, Deyo RA, Street JH, Barlow W. A comparison of physical therapy, chiropractic manipulation, and provision of an educational booklet for the treatment of patients with low back pain. N Engl J Med. 1998;339(15):1021�9. doi: 10.1056/NEJM199810083391502. [PubMed] [Cross Ref]
4. Paatelma M, Kilpikoski S, Simonen R, Heinonen A, Alen M, Videman T. Orthopaedic manual therapy, McKenzie method or advice only for low back pain in working adults. A randomized controlled trial with 1 year follow-up. J Rehabil Med. 2008;40(10):858�63. doi: 10.2340/16501977-0262. [PubMed] [Cross Ref]
5. Foster NE, Dziedzic KS, van Der Windt DA, Fritz JM, Hay EM. Research priorities for non-pharmacological therapies for common musculoskeletal problems: nationally and internationally agreed recommendations. BMC Musculoskelet Disord. 2009;10:3. doi: 10.1186/1471-2474-10-3. [PMC free article] [PubMed] [Cross Ref]
6. Kamper SJ, Maher CG, Hancock MJ, Koes BW, Croft PR, Hay E. Treatment-based subgroups of low back pain: a guide to appraisal of research studies and a summary of current evidence. Best Pract Res Clin Rheumatol. 2010;24(2):181�91. doi: 10.1016/j.berh.2009.11.003. [PubMed] [Cross Ref]
7. Airaksinen O, Brox JI, Cedraschi C, Hildebrandt J, Klaber-Moffett J, Kovacs F, et al. Chapter 4. European guidelines for the management of chronic nonspecific low back pain. Eur Spine J. 2006;15(Suppl 2):S192�300. doi: 10.1007/s00586-006-1072-1. [PMC free article] [PubMed] [Cross Ref]
8. Hingorani AD, Windt DA, Riley RD, Abrams K, Moons KG, Steyerberg EW, et al. Prognosis research strategy (PROGRESS) 4: Stratified medicine research. BMJ. 2013;346:e5793. doi: 10.1136/bmj.e5793. [PMC free article] [PubMed] [Cross Ref]
9. Fersum KV, Dankaerts W, O�Sullivan PB, Maes J, Skouen JS, Bjordal JM, et al. Integration of sub-classification strategies in RCTs evaluating manual therapy treatment and exercise therapy for non-specific chronic low back pain (NSCLBP): a systematic review. Br J Sports Med. 2010;44(14):1054�62. doi: 10.1136/bjsm.2009.063289. [PubMed] [Cross Ref]
10. Erhard RE, Delitto A, Cibulka MT. Relative effectiveness of an extension program and a combined program of manipulation and flexion and extension exercises in patients with acute low back syndrome. Phys Ther. 1994;74(12):1093�100. [PubMed]
11. Schenk RJ, Josefczyk C, Kopf A. A randomized trial comparing interventions in patients with lumbar posterior derangement. J Man Manipul Ther. 2003;11(2):95�102. doi: 10.1179/106698103790826455. [Cross Ref]
12. Kilpikoski S, Alen M, Paatelma M, Simonen R, Heinonen A, Videman T. Outcome comparison among working adults with centralizing low back pain: Secondary analysis of a randomized controlled trial with 1-year follow-up. Adv Physiol Educ. 2009;11:210�7. doi: 10.3109/14038190902963087. [Cross Ref]
13. Petersen T, Larsen K, Nordsteen J, Olsen S, Fournier G, Jacobsen S. The McKenzie method compared with manipulation when used adjunctive to information and advice in low back pain patients presenting with centralization or peripheralization. A randomized controlled trial. Spine (Phila Pa 1976) 2011;36(24):1999�2010. doi: 10.1097/BRS.0b013e318201ee8e. [PubMed] [Cross Ref]
14. Petersen T, Olsen S, Laslett M, Thorsen H, Manniche C, Ekdahl C, et al. Inter-tester reliability of a new diagnostic classification system for patients with non-specific low back pain. Aust J Physiother. 2004;50:85�94. doi: 10.1016/S0004-9514(14)60100-8. [PubMed] [Cross Ref]
15. Waddell G, McCulloch JA, Kummel E, Venner RM. Nonorganic physical signs in low-back pain. Spine. 1980;5(2):117�25. doi: 10.1097/00007632-198003000-00005. [PubMed] [Cross Ref]
16. Manniche C, Asmussen K, Lauritsen B, Vinterberg H, Kreiner S, Jordan A. Low Back Pain Rating scale: validation of a tool for assessment of low back pain. Pain. 1994;57(3):317�26. doi: 10.1016/0304-3959(94)90007-8. [PubMed] [Cross Ref]
17. McKenzie RA. Treat your own back. Waikanae: Spinal Publications New Zealand Ltd; 1997.
18. Burton AK, Waddell G, Tillotson KM, Summerton N. Information and advice to patients with back pain can have a positive effect. A randomized controlled trial of a novel educational booklet in primary care. Spine. 1999;24(23):2484�91. doi: 10.1097/00007632-199912010-00010. [PubMed] [Cross Ref]
19. Patrick DL, Deyo RA, Atlas SJ, Singer DE, Chapin A, Keller RB. Assessing health-related quality of life in patients with sciatica. Spine. 1995;20(17):1899�908. doi: 10.1097/00007632-199509000-00011. [PubMed] [Cross Ref]
20. Albert H, Jensen AM, Dahl D, Rasmussen MN. Criteria validation of the Roland Morris questionnaire. A Danish translation of the international scale for the assessment of functional level in patients with low back pain and sciatica [Kriterievalidering af Roland Morris Sp�rgeskemaet – Et oversat internationalt skema til vurdering af �ndringer i funktionsniveau hos patienter med l�ndesmerter og ischias] Ugeskr Laeger. 2003;165(18):1875�80. [PubMed]
21. Bombardier C, Hayden J, Beaton DE. Minimal clinically important difference. Low back pain: outcome measures. J Rheumatol. 2001;28(2):431�8. [PubMed]
22. Ostelo RW, Deyo RA, Stratford P, Waddell G, Croft P, Von KM, et al. Interpreting change scores for pain and functional status in low back pain: towards international consensus regarding minimal important change. Spine. 2008;33(1):90�4. doi: 10.1097/BRS.0b013e31815e3a10. [PubMed] [Cross Ref]
23. Moons KG, Royston P, Vergouwe Y, Grobbee DE, Altman DG. Prognosis and prognostic research: what, why, and how? BMJ. 2009;338:1317�20. doi: 10.1136/bmj.b1317. [PubMed] [Cross Ref]
24. Sun X, Briel M, Walter SD, Guyatt GH. Is a subgroup effect believable? Updating criteria to evaluate the credibility of subgroup analyses. BMJ. 2010;340:c117. doi: 10.1136/bmj.c117. [PubMed] [Cross Ref]
25. Long A, Donelson R, Fung T. Does it matter which exercise? A randomized control trial of exercise for low back pain. Spine. 2004;29(23):2593�602. doi: 10.1097/01.brs.0000146464.23007.2a. [PubMed] [Cross Ref]
26. Long A, May S, Fung T. The comparative prognostic value of directional preference and centralization: a useful tool for front-line clinicians? J Man Manip Ther. 2008;16(4):248�54. doi: 10.1179/106698108790818332. [PMC free article] [PubMed] [Cross Ref]
27. Koes BW, Bouter LM, van Mameren H, Essers AH, Verstegen GJ, Hofhuizen DM, et al. A randomized clinical trial of manual therapy and physiotherapy for persistent back and neck complaints: subgroup analysis and relationship between outcome measures. J Manipulative Physiol Ther. 1993;16(4):211�9. [PubMed]
28. Leboeuf-Yde C, Gronstvedt A, Borge JA, Lothe J, Magnesen E, Nilsson O, et al. The nordic back pain subpopulation program: demographic and clinical predictors for outcome in patients receiving chiropractic treatment for persistent low�back pain. J Manipulative Physiol Ther. 2004;27(8):493�502. doi: 10.1016/j.jmpt.2004.08.001. [PubMed] [Cross Ref]
29. Nyiendo J, Haas M, Goldberg B, Sexton G. Pain, disability, and satisfaction outcomes and predictors of outcomes: a practice-based study of chronic low back pain patients attending primary care and chiropractic physicians. J Manipulative Physiol Ther. 2001;24(7):433�9. doi: 10.1016/S0161-4754(01)77689-0. [PubMed] [Cross Ref]
30. Foster NE, Hill JC, Hay EM. Subgrouping patients with low back pain in primary care: are we getting any better at it? Man Ther. 2011;16(1):3�8. doi: 10.1016/j.math.2010.05.013. [PubMed] [Cross Ref]
31. Underwood MR, Morton V, Farrin A. Do baseline characteristics predict response to treatment for low back pain? Secondary analysis of the UK BEAM dataset. Rheumatology (Oxford) 2007;46(8):1297�302. doi: 10.1093/rheumatology/kem113. [PubMed] [Cross Ref]
32. Slater SL, Ford JJ, Richards MC, Taylor NF, Surkitt LD, Hahne AJ. The effectiveness of sub-group specific manual therapy for low back pain: a systematic review. Man Ther. 2012;17(3):201�12. doi: 10.1016/j.math.2012.01.006. [PubMed] [Cross Ref]
33. Stanton TR, Hancock MJ, Maher CG, Koes BW. Critical appraisal of clinical prediction rules that aim to optimize treatment selection for musculoskeletal conditions. Phys Ther. 2010;90(6):843�54. doi: 10.2522/ptj.20090233. [PubMed] [Cross Ref][/accordion]
[/accordions]
Additional Topics: Sciatica
Sciatica is referred to as a collection of symptoms rather than a single type of injury or condition. The symptoms are characterized as radiating pain, numbness and tingling sensations from the sciatic nerve in the lower back, down the buttocks and thighs and through one or both legs and into the feet. Sciatica is commonly the result of irritation, inflammation or compression of the largest nerve in the human body, generally due to a herniated disc or bone spur.
Low back pain, or LBP, is a very common condition which affects the lumbar spine, or the lower section of the spine. Approximately more than 3 million cases of LBP are diagnosed in the United States aline every year and about 80 percent of adults worldwide experience low back pain at some point during their lifetime. Low back pain is generally caused by injury to a muscle (strain) or ligament (sprain) or due to damage from a disease. Common causes of LBP include poor posture, lack of regular exercise,�improper lifting, fracture, herniated discs and/or arthritis. Most cases of low back pain may often go away on their own, however, when LBP becomes chronic, it may be important to seek immediate medical attention. Two therapeutic methods have been utilized to improve LBP. The following article compares the effects of Pilates and McKenzie training on LBP.
A Comparison of the Effects of Pilates and McKenzie Training on Pain and General Health in Men with Chronic Low Back Pain: A Randomized Trial
Abstract
Background: Today, chronic low back pain is one of the special challenges in healthcare. There is no unique approach to treat chronic low back pain. A variety of methods are used for the treatment of low back pain, but the effects of these methods have not yet been investigated adequately.
Aim: The aim of this study was to compare the effects of Pilates and McKenzie training on pain and general health of men with chronic low back pain.
Materials and Methods: Thirty-six patients with chronic low back pain were chosen voluntarily and assigned to three groups of 12 each: McKenzie group, Pilates group, and control group. The Pilates group participated in 1-h exercise sessions, three sessions a week for 6 weeks. McKenzie group performed workouts 1 h a day for 20 days. The control group underwent no treatment. The general health of all participants was measured by the General Health Questionnaire 28 and pain by the McGill Pain Questionnaire.
Results: After therapeutic exercises, there was no significant difference between Pilates and McKenzie groups in pain relief (P = 0.327). Neither of the two methods was superior over the other for pain relief. However, there was a significant difference in general health indexes between Pilates and McKenzie groups.
Conclusion: Pilates and McKenzie training reduced pain in patients with chronic low back pain, but the Pilates training was more effective to improve general health.
Keywords:Chronic back pain, general health, Mckenzie training, pain, Pilates training
Introduction
Low back pain with a history of more than 3 months and without any pathological symptom is called chronic low back pain. For patient with chronic low back pain, the physician should take into consideration the likelihood of muscle pain development with spinal origin, in addition to low back pain with unknown origin. This type of pain may be mechanical (increase in pain with movement or physical pressure) or nonmechanical (increase in pain at the rest time).[1] Low back pain or spine pain is the most common musculoskeletal complication.[2] About 50%�80% of healthy people may experience low back pain during their lifetime, and about 80% of the problems are related to the spine and occur in the lumbar area.[3] Low back pain may be caused by trauma, infection, tumors, etc.[4] Mechanical injuries which are caused by overuse of a natural structure, deformity of an anatomical structure, or the injury in the soft tissue are the most common reasons for back pain. From occupational health perspective, back pain is among the most important reasons for the absence from work and occupational disability;[5] in fact, the longer the period of disease,[6] the less likely it is to improve and return to work.[1] Disability due to low back pain in addition to disturbance in doing daily and social activities has a very negative effect, from social and economic perspectives, on the patient and the community, which makes chronic low back pain highly important.[3] Today, chronic low back pain is one of the critical challenges in medicine. Patients with chronic low back pain are responsible for 80% of the costs paid for the treatment of low back pain that is also the reason for mobility restrictions in most people under 45 years.[7] In the developed countries, the overall cost paid for low back pain per year is 7.1 of total share of the gross national product. Clearly, most of the cost is related to counseling and treatment of patients with chronic low back pain rather than with intermittent and recursive low back pain.[8] The existence of various methods of treatment is because of no single cause of low back pain.[9] A variety of methods such as pharmacotherapy, acupuncture, infusions, and physical methods are the most common interventions for treatment of low back pain. However, the effects of these methods remain to be fully known.[6] An exercise program, developed based on the physical conditions of patients, can promote the quality of life in patients with chronic disease.[10,11,12,13,14]
Literature shows that the effect of exercise in controlling chronic low back pain is under study and there is strong evidence about the fact that movement therapy is effective to treat low back pain.[15] However, no specific recommendations exist about the type of exercise, and the effects of certain types of movement therapies have been determined in few studies.[9] Pilates training consists of the exercises that focus on improving flexibility and strength in all the body organs, without increasing the mass of muscles or destroying them. This training method consists of controlled movements that form a physical harmony between the body and brain, and can raise the ability of the body of people at any age.[16] In addition, people who do Pilates exercise would have better sleep and less fatigue, stress, and nervousness. This training method is based on standing, sitting, and lying positions, without intervals, jumping, and leaping; thus, it may reduce injuries resulting from the joint damage because the exercise movements in the ranges of motion in the above three positions are performed with deep breathing and muscle contraction.[17] McKenzie method, also called mechanical diagnosis and therapy and based on the patient’s active participation, is used and trusted by patients and the people who use this method worldwide. This method is based on physical therapy which has been frequently studied. The distinctive characteristic of this method is the principle of initial assessment.[18] This principle is a reliable and safe method to make a diagnosis that makes the correct treatment planning possible. In this way, the time and energy are not spent for costly tests, rather McKenzie therapists, using a valid indicator, quickly recognize that how much and how this method is fruitful for the patient. More appropriately, McKenzie method is a comprehensive approach based on the correct principles whose full understanding and following is very fruitful.[19] In the recent years, non-pharmacological approaches have attracted the attention of physicians and patients with low back pain.[20] Complementary therapies[21] and treatments with holistic nature (to increase physical and mental well-being) are appropriate to manage physical illness.[13] Complementary therapies can slow down disease progression and improve capacity and physical performance. The aim of the present study is to compare the effect of the Pilates and McKenzie training on pain and general health in men with chronic low back pain.
Materials and Methods
This randomized clinical trial was conducted in Shahrekord, Iran. The total study population screened was 144. We decided to enroll at least 25% of the population, 36 individuals, using a systematic random sampling. First, the participants were numbered and a list was developed. The first case was selected using random number table and then one out of four patients was randomly enrolled. This process continued till a desired number of participants were enrolled. Then, the participants were randomly assigned to experimental (Pilates and McKenzie training) groups and control group. After explaining the research purposes to the participants, they were asked to complete the consent form for participation in the study. Furthermore, the patients were ensured that the research data are kept confidential and used only for research purposes.
Inclusion Criteria
The study population included men aged 40�55 years in Shahrekord, South-West Iran, with chronic back pain, that is, history of more than 3 months of low back pain and no specific disease or other surgery.
Exclusion Criteria
The exclusion criteria were low back arch or so-called army back, serious spinal pathology such as tumors, fractures, inflammatory diseases, previous spinal surgery, nerve root compromise in the lumbar region, spondylolysis or spondylolisthesis, spinal stenosis, neurological disorders, systemic diseases, cardiovascular diseases, and receiving other therapies simultaneously. The examiner who assessed the outcomes was blinded to group assignment. Twenty-four hours before the training, a pretest was administered to all three groups to determine pain and general health; and then, the training began after completion of the McGill Pain Questionnaire (MPQ) and the General Health Questionnaire-28 (GHQ-28). The MPQ can be used to evaluate a person experiencing significant pain. It can be used to monitor the pain over time and to determine the effectiveness of any intervention. Minimum pain score: 0 (would not be seen in a person with true pain), maximum pain score: 78, and the higher the pain score the more severe the pain. Investigators reported that the construct validity and the reliability of the MPQ were reported as a test-retest reliability of 0.70.[22] The GHQ is a self-administered screening questionnaire. Test-retest reliability has been reported to be high (0.78�0 0.9) and inter- and intra-rater reliability have both been shown to be excellent (Cronbach’s ? 0.9�0.95). High internal consistency has also been reported. The lower the score is, the better the general health is.[23]
The participants in the experimental groups started training program under supervision of a sports medicine specialist. The training program consisted of 18 sessions of supervised individual training for both groups, with the sessions held three times per week for 6 weeks. Each training session lasted for an hour and was performed at the Physiotherapy Clinic in the School of Rehabilitation of the Shahrekord University of Medical Sciences in 2014�2015. The first experimental group performed Pilates training for 6 weeks, three times a week about an hour per session. In each session, first, a 5-min warm-up and preparation procedures were run; and at the end, stretching and walking were done to return to the baseline condition. In the McKenzie group, six exercises were used: Four extension-type exercises and two flexion-types. The extension-type exercises were performed in prone and standing positions, and the flexion-type exercises in the supine and sitting positions. Each exercise was run ten times. In addition, the participants conducted twenty daily individual training sessions for an hour.[18] After training of both groups, the participants filled out the questionnaires and then the collected data were presented in both descriptive and inferential statistics. Furthermore, the control group without any training, at the end of a period when other groups have completed, filled the questionnaire. Descriptive statistics were used for central tendency indicators such as mean (� standard deviation) and relevant diagrams were used to describe the data. Inferential statistics, one-way ANOVA and post hoc Tukey’s test, were used to analyze the data. Data analysis was done by SPSS Statistics for Windows, Version 21.0 (IBM Corp. Released 2012. IBM Armonk, NY: IBM Corp). P < 0.05 was considered statistically significant.
Dr. Alex Jimenez’s Insight
Alongside the use of spinal adjustments and manual manipulations for low back pain, chiropractic care commonly utilizes therapeutic exercise methods to improve LBP symptoms, restoring the affected individual’s strength, flexibility and mobility as well as promoting a faster recovery. The Pilates and McKenzie method of training, as mentioned in the article, are compared to determine which therapeutic exercise is best for treating low back pain. As�a Level I Certified Pilates Instructor, Pilates training is implemented with chiropractic treatment to improve LBP more effectively. Patients participating in a therapeutic exercise method alongside a primary form of treatment for low back pain can experience additional benefits. McKenzie training can also be implemented with chiropractic treatment to further improve LBP symptoms. The purpose of this research study is to demonstrate evidence-based information on the benefits of Pilates and McKenzie methods for low back pain as well as to educate patients on which of the two therapeutic exercises should be considered to help treat their symptoms and achieve overall health and wellness.
Level I Certified Pilates Instructors at Our Location
Dr. Alex Jimenez D.C., C.C.S.T | Chief Clinical Director and Level I Certified Pilates Instructor
Truide Torres | Director of Patient Relations Advocate Dept. and Level I Certified Pilates Instructor
Results
The results showed no significant difference between the case and control groups regarding the gender, marital status, job, educational level, and income. The results showed changes in pain index and general health in the participants before and after Pilates and McKenzie training in the two experimental and even control groups [Table 1].
A significant difference was seen in pain and general health between the control and the two experimental groups at the pre- and post-test, so that the exercise training (both Pilates and McKenzie) resulted in reduced pain and promoted general health; while in the control group, pain increased and general health declined.
Discussion
The results of this study indicate that back pain reduced and general health enhanced after exercise therapy with both Pilates and McKenzie training, but in the control group, pain was intensified. Petersen et al. study on 360 patients with chronic low back pain concluded that at the end of 8 weeks of McKenzie training and high-intensity endurance training and 2 months training at home, pain and disability decreased in McKenzie group at the end of 2 months, but at the end of 8 months, no differences were seen among the treatments.[24]
The results of another study show that McKenzie training is a beneficial method for reducing pain and increasing the movements of the spine in patients with chronic low back pain.[18] Pilates training can be an effective method for improving general health, athletic performance, proprioception, and reduction of pain in patients with chronic low back pain.[25] The improvements in strength seen in the participants in the present study were more likely to be due to decrease in pain inhibition than to neurological changes in muscle firing/recruitment patterns or to morphological (hypertrophic) changes in the muscle. In addition, neither of the treatments was superior over the other in view of reducing the intensity of pain. In the present study, 6 weeks of McKenzie training led to significant reduction in pain levels in men with chronic low back pain. The rehabilitation of patients with chronic low back pain is aimed to restore strength, endurance, and flexibility of soft tissues.
Udermann et al. showed that McKenzie training improved pain, disability, and psychosocial variables in patients with chronic low back pain, and back stretching training did not have any additional effect on pain, disability, and psychosocial variables.[26] The results of another study show that there is a reduction in pain and disability due to McKenzie method for at least 1 week in comparison with the passive treatment in patients with low back pain, but reduction in pain and disability due to McKenzie method in comparison with the active treatment methods is desirable within 12 weeks after treatment. Overall, McKenzie treatment is more effective than passive methods to treat low back pain.[27] One of the popular exercise therapies for patients with low back pain is McKenzie training program. McKenzie method leads to improvement of low back pain symptoms such as pain in the short-term. Moreover, McKenzie therapy is more effective in comparison with passive treatments. This training is designed to mobilize the spine and to strengthen the lumbar muscles. Previous studies have shown that weakness and atrophy in the body central muscles, particularly the transverse abdominal muscle in patients with low back pain.[28] The results of this research also showed that there was a significant difference in the general health indexes between Pilates and McKenzie groups. In the present study, 6 weeks of Pilates and McKenzie training led to a significant reduction in the level of general health (physical symptoms, anxiety, social dysfunction, and depression) in men with chronic low back pain and the general health in Pilates training group improved. The results of most studies show that exercise therapy reduces pain and improves general health in patients with chronic low back pain. Importantly, the agreement about the duration, type, and intensity of the training remains to be achieved and there is no definite training program that can have the best effect on patients with chronic low back pain. Therefore, more research is needed to determine the best duration and treatment method to reduce and improve general health in patients with low back pain. In the Al-Obaidi et al. study, pain, fear, and functional disability improved after 10 weeks of treatment in patients.[5]
Besides that McKenzie training increases the range of motion of lumbar flexion. Overall, neither of the two methods of treatment was superior over the other.[18]
Borges et al. concluded that after 6 weeks of treatment, the average index of pain in experimental group was lower than the control group. Furthermore, the general health of the experimental group exhibited greater improvement than the control group. The results of this research support recommending Pilates training to patients with chronic low back pain.[29] Caldwell et al. on the university students concluded that Pilates training and Tai chi guan improved mental parameters such as self-sufficiency, quality of sleep, and morality of students but had no effect on physical performance.[30] Garcia et al. study on 148 patients with nonspecific chronic low back pain concluded that treating patients with nonspecific chronic low back pain by McKenzie training and back school caused disability to improve after treatment, but quality of life, pain, and the range of motor flexibility did not change. McKenzie treatment is typically more effective on disability than back school program.[19]
The overall findings of this study are supported by the literature, demonstrating that a Pilates program may offer a low-cost, safe alternative to the treatment of low back pain in this specific group of patients. Similar effects have been found in patients with unspecific chronic low back pain.[31]
Our study had good levels of internal and external validity and thus can guide therapists and patients considering therapies of choice for back pain. The trial included a number of features to minimize bias such as prospectively registering and following a published protocol.
Study Limitation
Small sample size enrolled in this study limits the generalization of the study findings.
Conclusion
The results of this study showed that 6-week Pilates and McKenzie training reduced pain in patients with chronic low back pain, but there was no significant difference between the effect of two therapeutic methods on pain and both exercise protocols had the same effect. In addition, Pilates and McKenzie training improved general health; however, according to the mean general health changes after the exercise therapy, it can be argued that the Pilates training has a greater effect in improving general health.
Financial Support and Sponsorship
Nil.
Conflicts of Interest
There are no conflicts of interest.
In conclusion,�when comparing the effects of Pilates and McKenzie training on general health as well as on painful symptoms in men with chronic low back pain, the evidence-based research study determined that both the Pilates and the McKenzie method of training effectively reduced pain in patients with chronic LBP. There was no significant difference between the two therapeutic methods altogether, however, the mean results of the research study demonstrated that Pilates training was more effective towards improving general health in men with chronic low back pain than McKenzie training.� Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Sciatica
Sciatica is referred to as a collection of symptoms rather than a single type of injury or condition. The symptoms are characterized as radiating pain, numbness and tingling sensations from the sciatic nerve in the lower back, down the buttocks and thighs and through one or both legs and into the feet. Sciatica is commonly the result of irritation, inflammation or compression of the largest nerve in the human body, generally due to a herniated disc or bone spur.
1. Bergstr�m C, Jensen I, Hagberg J, Busch H, Bergstr�m G. Effectiveness of different interventions using a psychosocial subgroup assignment in chronic neck and back pain patients: A 10-year follow-up. Disabil Rehabil. 2012;34:110�8. [PubMed]
2. Hoy DG, Protani M, De R, Buchbinder R. The epidemiology of neck pain. Best Pract Res Clin Rheumatol. 2010;24:783�92. [PubMed]
3. Balagu� F, Mannion AF, Pellis� F, Cedraschi C. Non-specific low back pain. Lancet. 2012;379:482�91. [PubMed]
4. Sadock BJ, Sadock VA. Kaplan and Sadock’s Synopsis of Psychiatry: Behavioral Sciences/Clinical Psychiatry. New York: Lippincott Williams & Wilkins; 2011.
5. Al-Obaidi SM, Al-Sayegh NA, Ben Nakhi H, Al-Mandeel M. Evaluation of the McKenzie intervention for chronic low back pain by using selected physical and bio-behavioral outcome measures. PM R. 2011;3:637�46. [PubMed]
6. Dehkordi AH, Heydarnejad MS. Effect of booklet and combined method on parents’ awareness of children with beta-thalassemia major disorder. J Pak Med Assoc. 2008;58:485�7. [PubMed]
7. van der Wees PJ, Jamtvedt G, Rebbeck T, de Bie RA, Dekker J, Hendriks EJ. Multifaceted strategies may increase implementation of physiotherapy clinical guidelines: A systematic review. Aust J Physiother. 2008;54:233�41. [PubMed]
8. Maas ET, Juch JN, Groeneweg JG, Ostelo RW, Koes BW, Verhagen AP, et al. Cost-effectiveness of minimal interventional procedures for chronic mechanical low back pain: Design of four randomised controlled trials with an economic evaluation. BMC Musculoskelet Disord. 2012;13:260. [PMC free article][PubMed]
9. Hernandez AM, Peterson AL. Handbook of Occupational Health and Wellness. Springer: 2012. Work-related musculoskeletal disorders and pain; pp. 63�85.
10. Hassanpour Dehkordi A, Khaledi Far A. Effect of exercise training on the quality of life and echocardiography parameter of systolic function in patients with chronic heart failure: A randomized trial. Asian J Sports Med. 2015;6:e22643. [PMC free article][PubMed]
11. Hasanpour-Dehkordi A, Khaledi-Far A, Khaledi-Far B, Salehi-Tali S. The effect of family training and support on the quality of life and cost of hospital readmissions in congestive heart failure patients in Iran. Appl Nurs Res. 2016;31:165�9. [PubMed]
12. Hassanpour Dehkordi A. Influence of yoga and aerobics exercise on fatigue, pain and psychosocial status in patients with multiple sclerosis: A Randomized Trial. J Sports Med Phys Fitness. 2015 [Epub ahead of print] [PubMed]
13. Hassanpour-Dehkordi A, Jivad N. Comparison of regular aerobic and yoga on the quality of life in patients with multiple sclerosis. Med J Islam Repub Iran. 2014;28:141. [PMC free article][PubMed]
14. Heydarnejad S, Dehkordi AH. The effect of an exercise program on the health-quality of life in older adults. A randomized controlled trial. Dan Med Bull. 2010;57:A4113. [PubMed]
15. van Middelkoop M, Rubinstein SM, Verhagen AP, Ostelo RW, Koes BW, van Tulder MW. Exercise therapy for chronic nonspecific low-back pain. Best Pract Res Clin Rheumatol. 2010;24:193�204. [PubMed]
16. Critchley DJ, Pierson Z, Battersby G. Effect of pilates mat exercises and conventional exercise programmes on transversus abdominis and obliquus internus abdominis activity: Pilot randomised trial. Man Ther. 2011;16:183�9. [PubMed]
17. Kloubec JA. Pilates for improvement of muscle endurance, flexibility, balance, and posture. J Strength Cond Res. 2010;24:661�7. [PubMed]
18. Hosseinifar M, Akbari A, Shahrakinasab A. The effects of McKenzie and lumbar stabilization exercises on the improvement of function and pain in patients with chronic low back pain: A randomized controlled trial. J Shahrekord Univ Med Sci. 2009;11:1�9.
19. Garcia AN, Costa Lda C, da Silva TM, Gondo FL, Cyrillo FN, Costa RA, et al. Effectiveness of back school versus McKenzie exercises in patients with chronic nonspecific low back pain: A randomized controlled trial. Phys Ther. 2013;93:729�47. [PubMed]
20. Hassanpour-Dehkordi A, Safavi P, Parvin N. Effect of methadone maintenance treatment of opioid dependent fathers on mental health and perceived family functioning of their children. Heroin Addict Relat Clin. 2016;18(3):9�14.
21. Shahbazi K, Solati K, Hasanpour-Dehkordi A. Comparison of hypnotherapy and standard medical treatment alone on quality of life in patients with irritable bowel syndrome: A Randomized Control Trial. J Clin Diagn Res. 2016;10:OC01�4. [PMC free article][PubMed]
22. Ngamkham S, Vincent C, Finnegan L, Holden JE, Wang ZJ, Wilkie DJ. The McGill Pain Questionnaire as a multidimensional measure in people with cancer: An integrative review. Pain Manag Nurs. 2012;13:27�51. [PMC free article][PubMed]
23. Sterling M. General health questionnaire-28 (GHQ-28) J Physiother. 2011;57:259. [PubMed]
24. Petersen T, Kryger P, Ekdahl C, Olsen S, Jacobsen S. The effect of McKenzie therapy as compared with that of intensive strengthening training for the treatment of patients with subacute or chronic low back pain: A randomized controlled trial. Spine (Phila Pa 1976) 2002;27:1702�9. [PubMed]
25. Gladwell V, Head S, Haggar M, Beneke R. Does a program of pilates improve chronic non-specific low back pain? J Sport Rehabil. 2006;15:338�50.
26. Udermann BE, Mayer JM, Donelson RG, Graves JE, Murray SR. Combining lumbar extension training with McKenzie therapy: Effects on pain, disability, and psychosocial functioning in chronic low back pain patients. Gundersen Lutheran Med J. 2004;3:7�12.
27. Machado LA, Maher CG, Herbert RD, Clare H, McAuley JH. The effectiveness of the McKenzie method in addition to first-line care for acute low back pain: A randomized controlled trial. BMC Med. 2010;8:10. [PMC free article][PubMed]
28. Kilpikoski S. The McKenzie Method in Assessing, Classifying and Treating Non-Specific Low Back Pain in Adults with Special Reference to the Centralization Phenomenon. Jyv�skyl� University of Jyv�skyl� 2010
29. Borges J, Baptista AF, Santana N, Souza I, Kruschewsky RA, Galv�o-Castro B, et al. Pilates exercises improve low back pain and quality of life in patients with HTLV-1 virus: A randomized crossover clinical trial. J Bodyw Mov Ther. 2014;18:68�74. [PubMed]
30. Caldwell K, Harrison M, Adams M, Triplett NT. Effect of pilates and taiji quan training on self-efficacy, sleep quality, mood, and physical performance of college students. J Bodyw Mov Ther. 2009;13:155�63. [PubMed]
31. Altan L, Korkmaz N, Bingol U, Gunay B. Effect of pilates training on people with fibromyalgia syndrome: A pilot study. Arch Phys Med Rehabil. 2009;90:1983�8. [PubMed]
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine








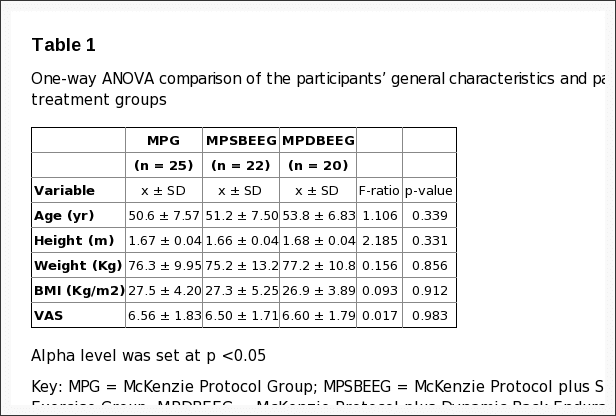
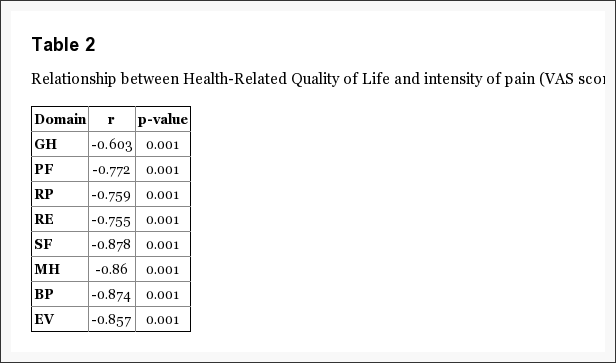
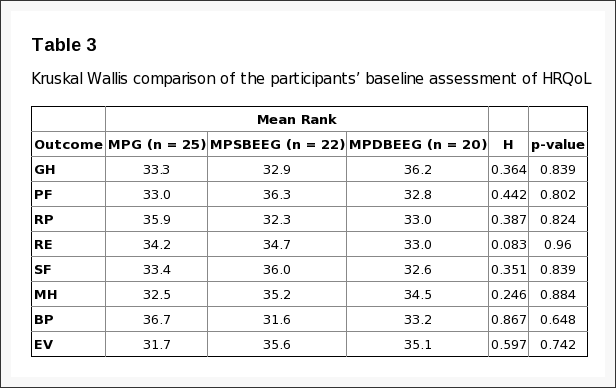
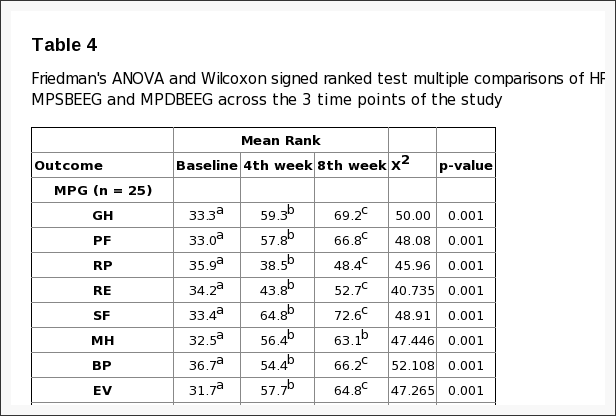
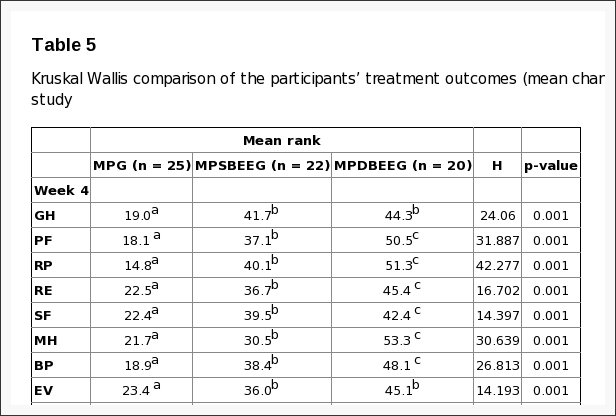





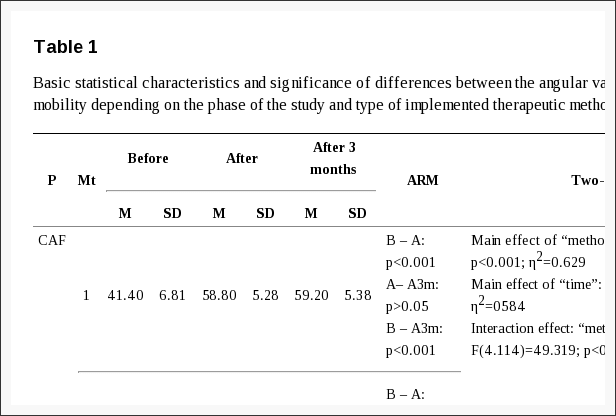
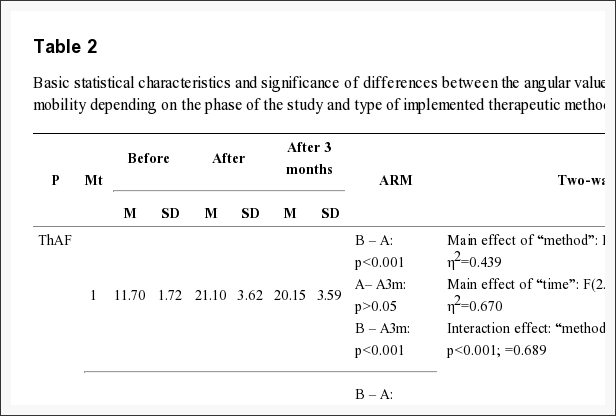
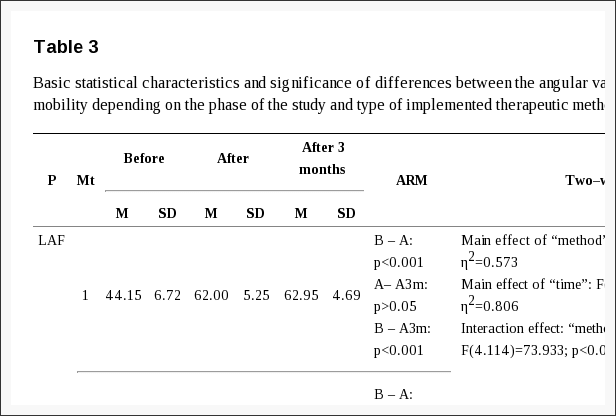
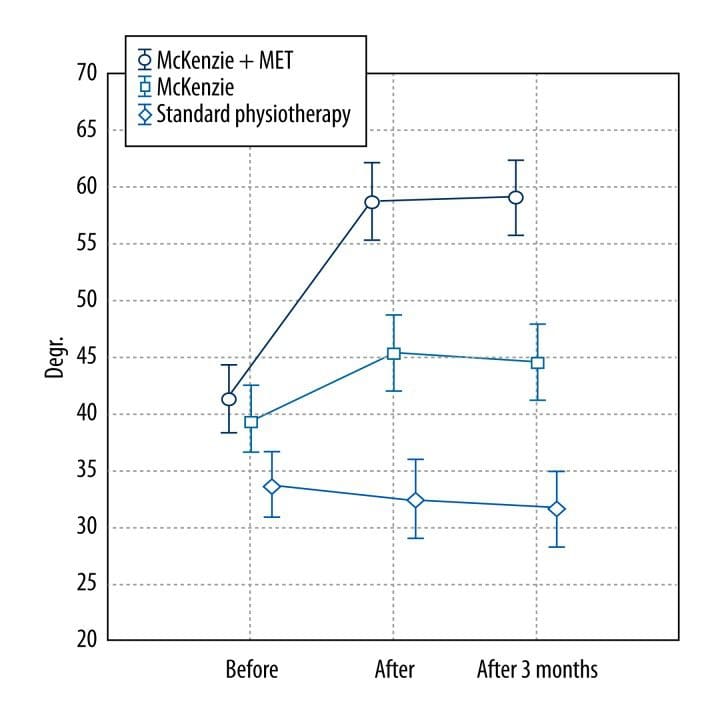
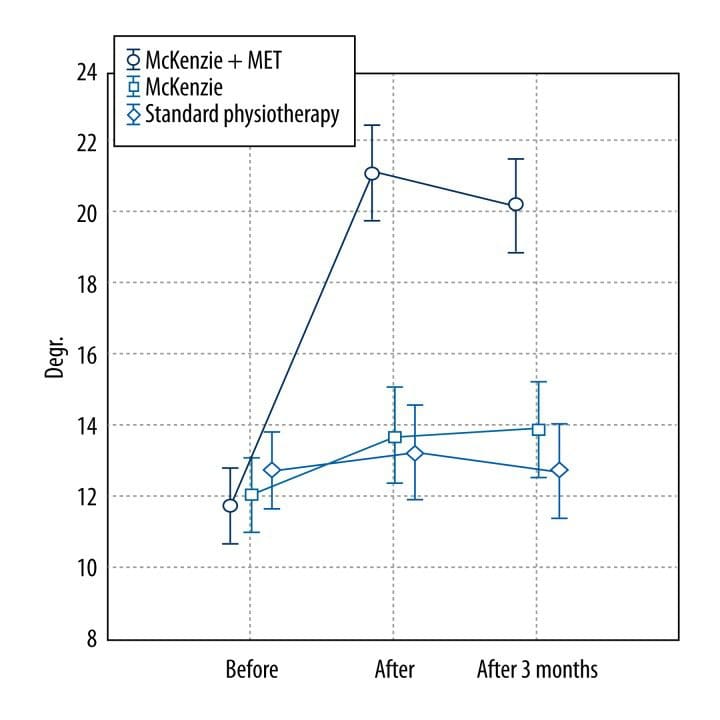
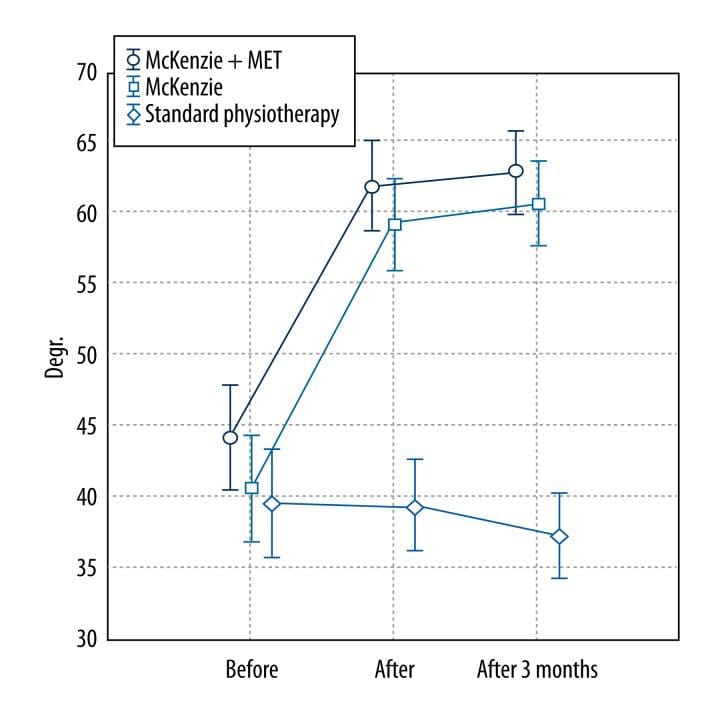
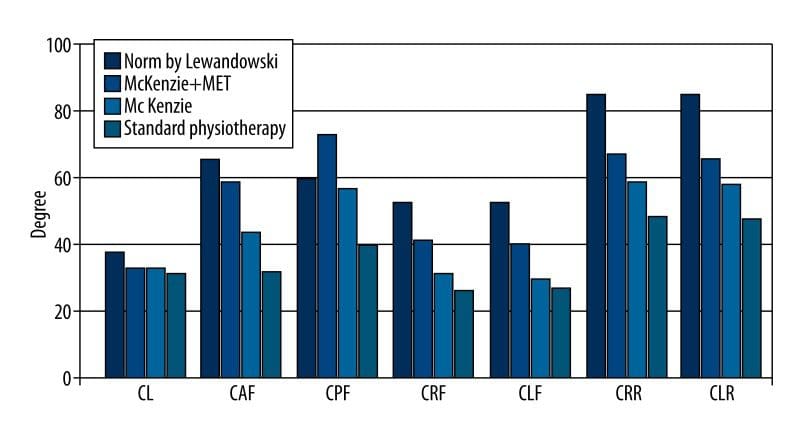
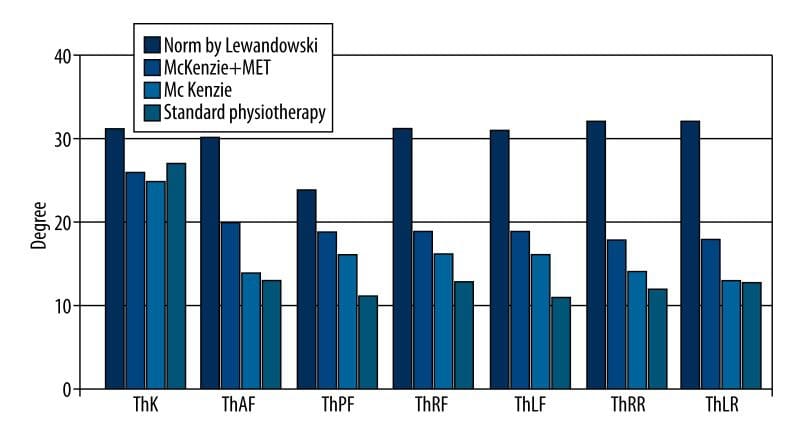
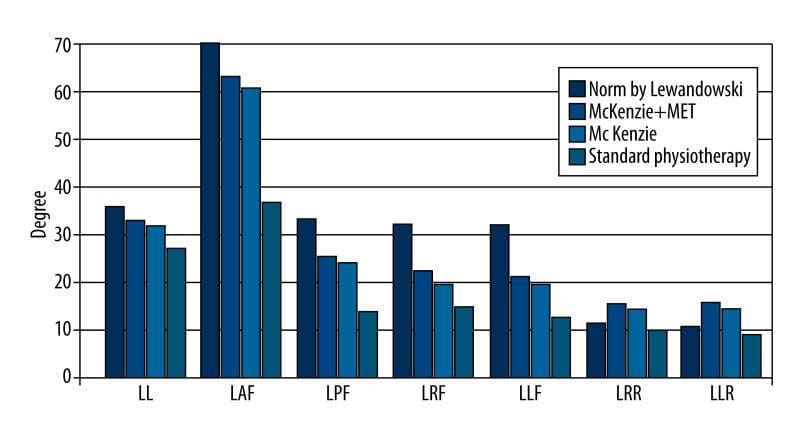
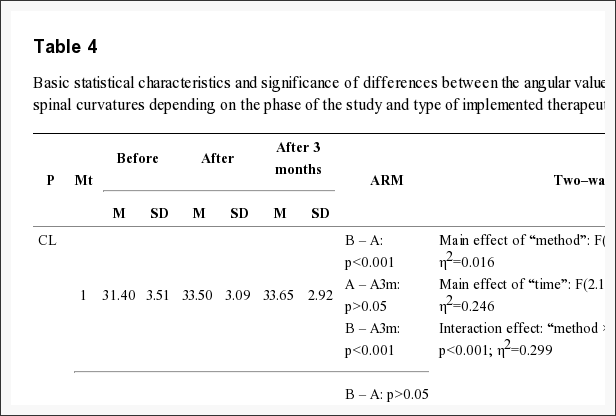
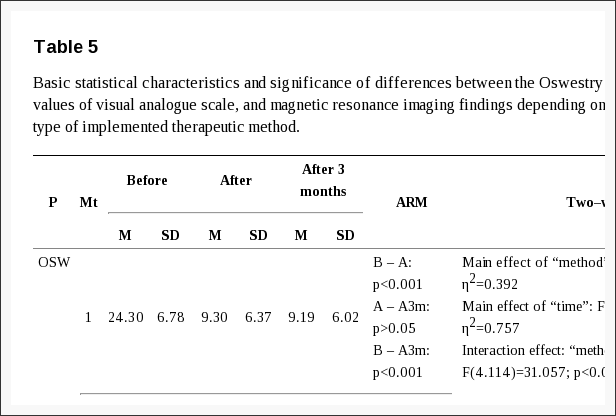
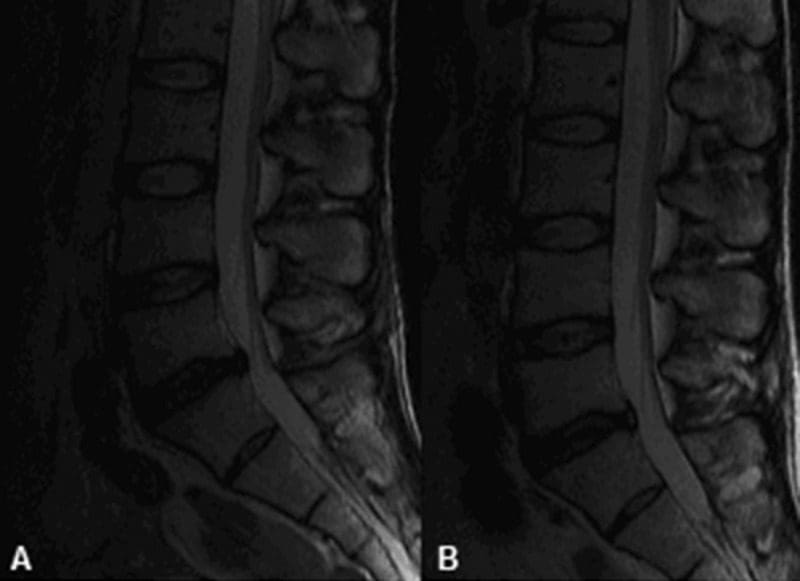





 MRI may be requested for:
MRI may be requested for: