The human body is an intricate machine; everything is connected in one way or another. This means that when one part is not functioning as it should, it can throw everything out of balance. The relationship between the feet, back, and hips is significant, so when there is a problem with feet, it can cause pain in those areas. Fallen arches are�a foot problem that is a prevalent cause of lower back pain. However, many people who have fallen arches don�t even realize that they have an issue.
What are Fallen Arches?
There are more than 100 ligaments and muscles in the foot that stabilize the bones and keep everything in the proper position. Ligaments prevent joints from extending beyond their intended limits. They contain elastin which allows them to act much like a rubber band, stretching with movement or flexion then returning to their regular length when the joint returns to its resting position.
There are a�variety of things that can happen that cause those ligaments to stretch, causing them to lose their ability to support the foot as they should. This can lead to pes planus (flat feet), also known as fallen arches.
Most people don�t realize that there are three arches in the foot, not just one: lateral, medial, and anterior. They act as shock absorbers for the body. When they don�t function as they should, don�t absorb the shock of movement and activity, it puts added wear and tear on the body. While foot, knee, hip, and back pain is common with fallen arches, it also is a major cause of impaired functioning of the lower extremities. It can also lead to balance problems.
Causes of Fallen Arches
The primary cause of fallen arches is improper footwear. Shoes that do not adequately support your foot and arch can lead to structural problems.
Other causes of fallen arches include:
Tendons in the foot that are torn or stretched
Certain health conditions including
Rheumatoid arthritis
Pregnancy
Diabetes
Obesity
Aging
Structural abnormalities that are present from birth
Inflammation, deformity, or damage of the posterior tibial tendon that runs from the middle of the arch to the lower leg, running along the ankle
Nerve issues
Bones that are dislocated or broken
Recognizing the symptoms of fallen arches and knowing that you have a problem can help to prevent the pain but can also arrest further damage to the foot.
Do you have Fallen Arches?
While many people with fallen arches experience no symptoms or problems, others do. If you experience any of these symptoms of flat feet, it should prompt a visit to your doctor.
Pain in the foot, knee, leg, hip, or lower back
Feet that easily get tired
Difficulty with balance
Swelling on the bottom of the foot
Pain or achiness in the foot, particularly in the heel or arch
Certain movements. such as standing on tiptoe, are difficult
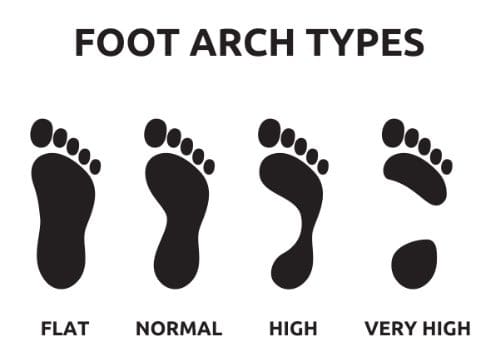
There is a quick, simple test that you can do at home to see if you have fallen arches:
Wet your feet
Stand on a flat, hard surface, such as a floor or concrete pad (you need to be able to see your footprint) or walk in soft soil or sand
Look at your footprints. If you see a print that shows the heel and ball of your foot with a thin, curved imprint running along the outside, then your foot structure is normal. If you can see the print of your entire foot, then you probably have fallen arches.
The problem with fallen arches is that the damage cannot be reversed once it begins. However, the progression can be stopped with proper treatment.
What are the Treatments for Fallen Arches?
The treatment for fallen arches depends on the cause and severity of the condition. If it isn�t causing pain or other problems, the doctor may elect to do nothing.
However, if there are pain or mobility issues present, treatments may include bracing, prescribing NSAIDs for pain and inflammation, and even surgery in some cases of torn tendons or broken bones. An increasingly popular treatment for fallen arches is chiropractic care. This natural, non-invasive therapy treats the whole body so that it addresses the cause of the condition as well as associated risk factors and helps patients manage the pain, significantly improving their quality of life.
The Texas Board of Chiropractic Examiners (Board) adopts new �78.14 concerning acupuncture.New �78.14 is adopted with changes to the proposed text as published in the July 20, 2018, issue�of the�Texas Register�(43 TexReg 4817).
This new rule with changes is adopted under Texas Occupations Code �201.152, which authorizes the Board to adopt rules necessary to perform the Board’s duties and to regulate the practice of chiropractic.
No other statute, article, or rule is affected by this rule.
Background and Justification
The Board adopts the new �78.14 (with non-substantive changes made to the proposed version)to replace the Board’s previous acupuncture rule in order to promote a clearer understanding of the requirements for the practice of acupuncture as performed by doctors of chiropractic. The rule also delineates the differences between the way chiropractors practice acupuncture and the way that of other Texas health professions do. The new rule clarifies the degree of regulatory oversight the Board exercises over the practice of acupuncture to safeguard the public while not imposing unnecessary economic burdens on either chiropractors who offer the acupuncture modality or on consumers.
Comments
The thirty-day comment period ended on August 20, 2018.
The Board received numerous comments regarding the proposed new rule, including from theTexas Chiropractic Association (TCA), the Texas Medical Association (TMA), the Texas Association of Acupuncture and Oriental Medicine (TAAOM), and eighty-seven individuals.
Comment: TCA urged the adoption of the proposed rule in its current form, but recommended the Board not adopt the proposed 200 hours of training in the use and administration of acupuncture in order for a chiropractor to receive a permit. TCA reiterated its position that increasing the training requirement from the current 100 hours is unnecessary to protect the public. Numerous other commenters also pointedly raised this issue. TCA further noted that it is inconsistent and arbitrary to impose this heightened regulatory burden on chiropractors when medical doctors, dentists, and physical therapists perform acupuncture with far less training.
Response: The Board agrees with TCA and the other commenters that the proposed increase in required training from 100 to 200 hours would impose an unnecessary economic and regulatory burden on chiropractors and students currently enrolled at chiropractic colleges without increasing public safety in any significant way. The Board notes that no evidence has been produced that the currently required 100 hours of training in acupuncture is inadequate to protect the public. The Board acknowledges that the increase in required hours could be seen as an economic barrier to market entry for newly licensed chiropractors, especially in light of the fact that other licensed health professionals are permitted to practice acupuncture with far fewer hours of training. The Board, therefore, has reduced the number of required hours from 200 to the existing 100.
Comment: Two commenters raised concerns about the proposed rule’s permission to use the terms “Board Certified,” “Board Certified in Chiropractic Acupuncture,” and “Board Certified in Acupuncture as an adjunctive modality by the Texas Board of Chiropractic Examiners” in advertising by chiropractors. The concerns were the terms were confusing and too lengthy.
Response: The Board agrees in part and has modified the rule’s language. The Board has kept the language allowing a chiropractor to use the terms “Board Certified” and “Board Certified in Chiropractic Acupuncture” if used in conjunction with the name of the nationally recognized certifying board and the specific credentials granted. The Board concurs that the advertising term “Board Certified in Acupuncture as an adjunctive modality by the Texas Board of Chiropractic Examiners” is too lengthy and may give the impression that the Board is acting as an accredited certifying board. Therefore, the Board has changed the term “certificate” to”permit” throughout the rule to make it clear that the Board is acknowledging a chiropractor’s qualifications.
The Board has also eliminated the provision in the proposed rule that required the Board to issue a separate document to permit a chiropractor to practice acupuncture; the Board will instead include the permitting language on each renewal license issued to chiropractors who meet the rule’s requirements.
Comment: Several individuals submitted comments urging the Board to include the practice of dry needling in this rule.
Response: The Board appreciates the comments but declines to address this issue as it is outside the bounds of this rule.
Comment: The Board received several comments from chiropractors who found the proposed rule’s language confusing regarding the requirements for obtaining a permit to practice acupuncture, especially for those who have been successfully practicing acupuncture in Texas under the Board’s current rule for several years.
Response: The Board agrees with the commenters that the language regarding the requirements for obtaining a permit in the proposed rule was unclear. The Board has changed what is now subsection (e) to be more precise.
The Board removed the requirement to provide patient records as proof of having practiced for at least ten years and substituted it with providing a written statement of having practiced acupuncture in a clinical setting, with the statement subject to Board verification. The Board believes the original requirement of providing redacted patient records, which could go back several years, was too onerous on chiropractors.
Comment: Several individuals said the continuing education provision in the proposed rule that required eight hours of acupuncture education for each two years of licensure was not clear.
Response: The Board agrees and has modified the language in what is now subsection (f) to state that a chiropractor permitted to practice acupuncture must complete a minimum of eight hours in Board-approved acupuncture courses every biennium.
Comment: One individual questioned why the rule’s training requirements for acupuncture only allow for didactic, clinical, and practical training, but exclude online and distance learning options.
Response: The Board appreciates the comment, but declines to include those training methods at this time.
Comment: TMA expressed its strong opposition to the proposed rule on the grounds the Board lacks the legal authority to regulate the practice of acupuncture by chiropractors. TMA made no direct comments on the language of the proposed rule itself.
Response: The Board disagrees with TMA’s position. Acupuncture or filiform needles used in the practice of acupuncture are non-incisive, meaning those needles do not cut or leave a wound when properly used. Texas courts have found that the Board’s position is not unreasonable or inconsistent with Texas Occupations Code Chapter 201. Because the use of acupuncture or filiform needles is non-incisive, their use falls within the chiropractic scope of practice, and thus the Board has statutory authority to enact rules regulating that use.
Comment: Numerous licensed acupuncturists wrote to object to the proposed rule on nearly identical grounds, including objections that the Board lacks the legal authority to promulgate the rule, that the rule potentially endangers the public, and that the rule has the potential to cause economic harm to licensed acupuncturists. These individuals made no direct comments on the language of the proposed rule itself.
Response: Regarding the objections concerning the Board’s legal authority to promulgate the proposed rule, the Board disagrees and notes its response to similar comments by TMA above.
The Board disagrees that the public would somehow be at risk from the continued practice of acupuncture by chiropractors because of a lack of training. The Board again notes there is no empirical evidence that any person in Texas has been harmed by a chiropractor practicing acupuncture under either the Board’s current rule, which requires 100 hours of training in acupuncture beyond the extensive training in physiology and anatomy all chiropractors receive in their four-year chiropractic college degree programs, or in the several decades before the current rule’s adoption. This argument is further undercut by the fact that other Texas health professionals are permitted to practice acupuncture with far fewer hours of additional training or experience.
The Board also disagrees with the argument that allowing chiropractors to practice acupuncture would economically harm acupuncturists. Chiropractors and acupuncturists have both practiced acupuncture, albeit with differing philosophies, for several decades in Texas. the existing were safely practicing acupuncture in Texas long before the enactment of Texas Occupations Code Chapter 205. There is no evidence that acupuncturists have suffered been produced harm up to now, nor is there any to show there will be any future harm. The Board takes seriously its oversight mandate to protect the public health without imposing unnecessary economic costs on either chiropractors or consumers.
Comment: TAAOM submitted lengthy comments to the Board regarding the proposed rule.
Response: The Board disagrees with TAAOM’s assertion that the Board has no authority to define acupuncture or to authorize the practice of acupuncture by its licensees. The Board does have such statutory authority. As noted above in the Board’s response to TMA, acupuncture or filiform needles used in the practice of acupuncture are non-incisive, and thus within the scope of practice under Texas Occupations Code Chapter 201.
The Board declines to respond to TAAOM’s comments concerning dry needling as that is outside the bounds of this rulemaking.
The Board agrees, in part, with TAAOM that the use of the term “board certification” could cause confusion. The rule has been changed to state that a chiropractor who meets the rule’s requirements for the practice of acupuncture will be granted a permit to perform acupuncture as opposed to a certificate, so as not to give the impression that the chiropractor has been credentialed by the Board.
The Board disagrees with TAAOM’s claim that the hours of training in acupuncture chiropractors receive are inadequate to protect the public. Doctors of chiropractic on average receive over 4200 hours of doctoral-level training that focuses on anatomy and physiology, which far exceeds the training an undergraduate-level acupuncturist receives. It is, therefore, incorrect to suggest that a chiropractor trained in acupuncture has a lesser understanding of physiological mechanics than does an acupuncturist.
The Board disagrees with TAAOM’s insistence the Board increase the verification requirements for chiropractors who began practicing acupuncture before 2010 and have always done so safely before the Board may grant them permits. Because it lacks a legitimate public health rationale, TAAOM’s position would only add unnecessary and burdensome economic costs on chiropractors. The Board believes the documentation the new rule requires of chiropractors who began practicing acupuncture before 2010 is more than sufficient to protect the public health.
The Board disagrees with TAAOM’s position that a chiropractor who practices acupuncture should be prevented from advertising that fact. The practice of acupuncture is within a chiropractor’s scope of practice. To deny a chiropractor the ability to advertise without a legitimate public safety rationale, as TAAOM urges the Board to do, is nothing more than the restriction of the economic freedom and commercial free speech rights of one profession for the benefit of another. The Board declines to impose such a limit.
The Board agrees with TAAOM that unnecessary references to other Board rules should be removed. Those references have been removed.
Chiropractic care is an alternative treatment option which utilizes a variety of methods and techniques to treat injuries and/or conditions. As mentioned in the article, when it comes to the use of acupuncture in chiropractic care, the final ruling is that chiropractors, or doctors of chiropractic, are allowed to practice acupuncture. Dr. Alex Jimenez D.C., C.C.S.T. Insight
�78.14. Acupuncture.
(a) Acupuncture, and the related practices of acupressure and meridian therapy, includes methods for diagnosing and treating a patient by stimulating specific points on or within the musculoskeletal system by various means, including manipulation, heat, cold, pressure,vibration, laser, ultrasound, light electro current, and the insertion of acupuncture needles or solid filiform needles for the purpose of obtaining a bio-positive reflex response by nerve stimulation.
(b) A licensee shall practice acupuncture only after obtaining a permit from the Texas Board of Chiropractic Examiners (Board).
(c) The Board shall place on each renewal license to practice chiropractic a statement that a licensee who has met all Board requirements is permitted to practice acupuncture. A licensee whose license does not contain the statement permitting the practice of acupuncture shall not practice or advertise the practice of acupuncture.
(d) A licensee with an acupuncture permit cannot delegate the performance of acupuncture.
(e) Requirements for an acupuncture permit:
(1) On or after the effective date of this rule, a licensee may receive an acupuncture permit from the Board by completing at least one hundred (100) hours of training in acupuncture and passing the National Board of Chiropractic Examiners’ examination. The training must be provided by an accredited chiropractic college, or post-secondary university, or other educational or testing institution approved by the Board. Such training shall include didactic, clinical, and practical training in the practice of acupuncture, clean needle techniques, examination, and protocols that meet the blood-borne pathogen standard established by the Occupational Safety and Health Administration.
(2) A person who became a licensee after January 1, 2010, and before the effective date of this rule, who has been practicing acupuncture in compliance with previous Board rules, shall have until September 1, 2019, to obtain an acupuncture permit from the Board by passing the National Board of Chiropractic Examiners’ standardized certification examination in acupuncture and completing 100 hours of acupuncture training.
(3) A person who became a licensee before January 1, 2010, shall have until September 1, 2019, to obtain an acupuncture permit from the Board by having:
(A) Successfully completed and passed an examination in a one hundred (100) hour training course in acupuncture; or
(B) Successfully completed and passed either the National Board of Chiropractic Examiners’standardized certification examination in acupuncture or the examination offered by the National Certification Commission of Acupuncture before the effective date of this rule; or
(C) Successfully completed formal training along with providing a statement to the Board of having practiced acupuncture in clinical practice for at least ten years before January 1, 2010, and is in good standing with the Board and the regulatory entities of the other jurisdictions in which the licensee is licensed. The Board may audit any statement for accuracy.
(4) Documentation of acupuncture training shall be in the form of signed certificates of attendance or completion, or diplomas from course sponsors or instructors.
(f) A licensee permitted to practice acupuncture must complete a minimum of eight (8) hours in Board-approved acupuncture courses every biennium.
(g) A licensee shall not practice acupuncture until the licensee has submitted proof of compliance with subsection (e) and has received a permit from the Board.
(h) A licensee practicing acupuncture shall not advertise in a manner that suggests the licensee possesses a license to practice acupuncture issued by the Texas State Board of AcupunctureExaminers, including using any of the terms “acupuncturist,” “licensed acupuncturist,” “L.Ac.,” “Traditional Chinese Medicine,” or “degreed in acupuncture.”
(i) A licensee’s advertising may include the terms “Board Certified” or “Board Certified in Chiropractic Acupuncture” if it also clearly identifies the nationally recognized certifying board and credentials.
(j) Approved programs in clinical acupuncture or meridian therapy offered by accredited chiropractic colleges or universities are designed for doctors of chiropractic and other disciplines. These courses are not intended as a substitute for a full curriculum teaching traditional Chinese medicine; rather they focus on the principle, theory, scientific findings, and practical modern application of acupuncture as currently practiced by doctors of chiropractic.
(k) The practice of acupuncture by a licensee who has not complied with the requirements of this section constitutes unprofessional conduct and subjects the licensee to disciplinary action. A licensee who advertises acupuncture without first obtaining a permit also has engaged in unprofessional conduct.
The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Chiropractic for Athletes with Back Pain
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain is the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
Chiropractic care is an alternative treatment option which focuses on the diagnosis, treatment, and prevention of a variety of injuries and/or underlying conditions associated with the musculoskeletal and nervous system. Dr. Alex Jimenez, a chiropractor, has helped many patients find relief from their symptoms of neck pain, back pain, and sciatica, among other health issues. Recommended for his outstanding services and ability to provide care and education to his patients, Dr. Alex Jimenez, and his staff make sure to offer the best treatment option for each patient’s specific needs. The patients express how Dr. Alex Jimenez has helped them find pain relief.
Most Recommended Chiropractor
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused on treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
If you have enjoyed this video and we have helped you in any way, please feel free to subscribe and recommend�us.
About 1.5 million people in the United States have rheumatoid arthritis. Rheumatoid arthritis, or RA, is a chronic, autoimmune disease characterized by pain and inflammation of the joints. With RA, the immune system, which protects our well-being by attacking foreign substances like bacteria and viruses, mistakenly attacks the joints. Rheumatoid arthritis most commonly affects the joints of the hands, feet, wrists, elbows, knees and ankles. Many healthcare professionals recommend early diagnosis and treatment of RA.
Abstract
Rheumatoid arthritis is the most commonly diagnosed systemic inflammatory arthritis. Women, smokers, and those with a family history of the disease are most often affected. Criteria for diagnosis include having at least one joint with definite swelling that is not explained by another disease. The likelihood of a rheumatoid arthritis diagnosis increases with the number of small joints involved. In a patient with inflammatory arthritis, the presence of a rheumatoid factor or anti-citrullinated protein antibody, or elevated C-reactive protein level or erythrocyte sedimentation rate suggests a diagnosis of rheumatoid arthritis. Initial laboratory evaluation should also include complete blood count with dif- ferential and assessment of renal and hepatic function. Patients taking biologic agents should be tested for hepatitis B, hepatitis C, and tuberculosis. Earlier diagnosis of rheumatoid arthritis allows for earlier treatment with disease-modifying antirheumatic agents. Combinations of medications are often used to control the disease. Methotrexate is typically the first-line drug for rheumatoid arthritis. Biologic agents, such as tumor necrosis factor inhibitors, are generally considered second-line agents or can be added for dual therapy. The goals of treatment include minimiza- tion of joint pain and swelling, prevention of radiographic damage and visible deformity, and continuation of work and personal activities. Joint replacement is indicated for patients with severe joint damage whose symptoms are poorly controlled by medical management. (Am Fam Physician. 2011;84(11):1245-1252. Copyright � 2011 American Academy of Family Physicians.)
Rheumatoid arthritis (RA) is the most common inflammatory arthritis, with a lifetime prevalence of up to 1 percent worldwide.1 Onset can occur at any age, but peaks between 30 and 50 years.2 Disability is common and significant. In a large U.S. cohort, 35 percent of patients with RA had work disability after 10 years.3
Etiology and Pathophysiology
Like many autoimmune diseases, the etiology of RA is multifactorial. Genetic susceptibility is evident in familial clustering and monozygotic twin studies, with 50 percent of RA risk attributable to genetic factors.4 Genetic associations for RA include human leukocyte antigen-DR45 and -DRB1, and a variety of alleles called the shared epitope.6,7 Genome-wide association studies have identified additional genetic signatures that increase the risk of RA and other autoimmune diseases, including STAT4 gene and CD40 locus.5 Smoking is the major environmental trigger for RA, especially in those with a genetic predisposition.8 Although infections may unmask an autoimmune response, no particular pathogen has been proven to cause RA.9
RA is characterized by inflammatory pathways that lead to proliferation of synovial cells in joints. Subsequent pannus formation may lead to underlying cartilage destruction and bony erosions. Overproduction of pro-inflammatory cytokines, including tumor necrosis factor (TNF) and interleukin-6, drives the destructive process.10
Risk Factors
Older age, a family history of the disease, and female sex are associated with increased risk of RA, although the sex differential is less prominent in older patients.1 Both current and prior cigarette smoking increases the risk of RA (relative risk [RR] = 1.4, up to 2.2 for more than 40-pack-year smokers).11
Pregnancy often causes RA remission, likely because of immunologic tolerance.12 Parity may have long-lasting impact; RA is less likely to be diagnosed in parous women than in nulliparous women (RR = 0.61).13,14 Breastfeeding decreases the risk of RA (RR = 0.5 in women who breastfeed for at least 24 months), whereas early menarche�(RR = 1.3 for those with menarche at 10 years of age or younger) and very irregular menstrual periods (RR = 1.5) increase risk.14 Use of oral contraceptive pills or vitamin E does not affect RA risk.15
Diagnosis
Typical Presentation
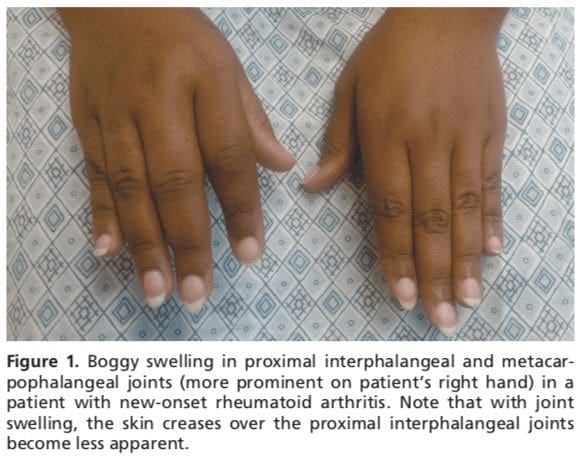
Patients with RA typically present with pain and stiffness in multiple joints. The wrists, proximal interphalangeal joints, and metacarpophalangeal joints are most commonly involved. Morning stiffness lasting more than one hour suggests an inflammatory etiology. Boggy swelling due to synovitis may be visible (Figure 1), or subtle synovial thickening may be palpable on joint examination. Patients may also present with more indolent arthralgias before the onset of clinically apparent joint swelling. Systemic symptoms of fatigue, weight loss, and low-grade fever may occur with active disease.
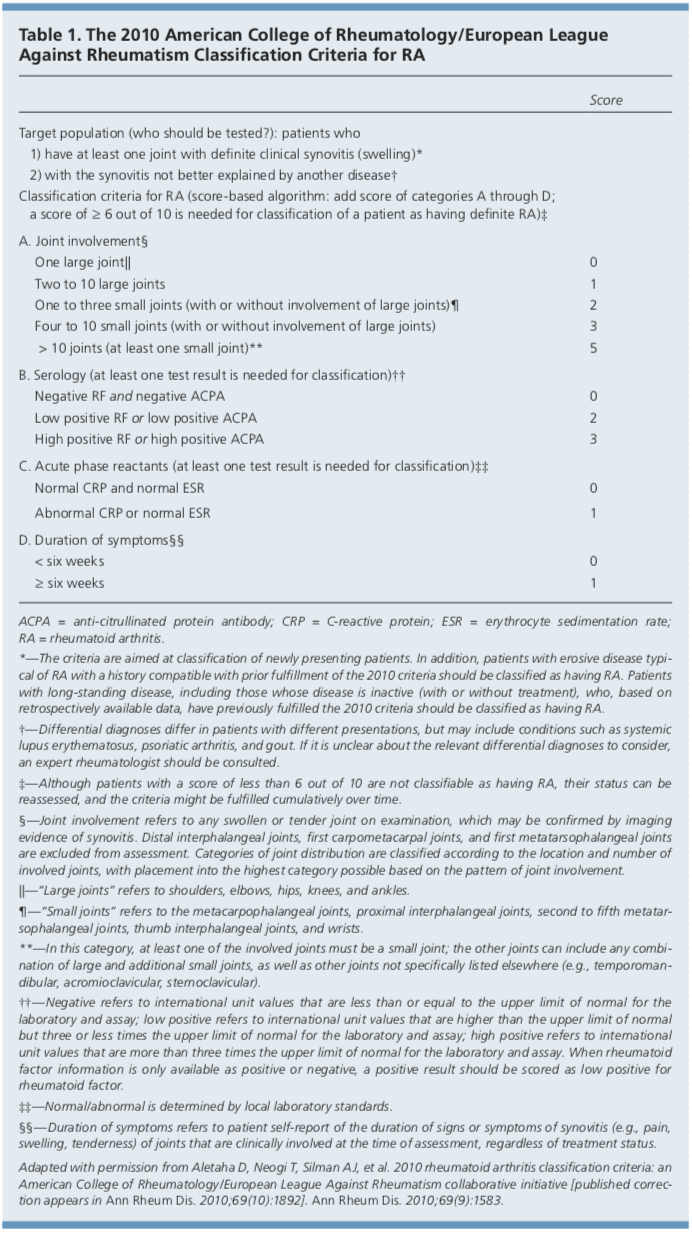
Diagnostic Criteria
In 2010, the American College of Rheumatology and European League Against Rheumatism collaborated to create new classification criteria for RA (Table 1).16 The new criteria are an effort to diagnose RA earlier in patients who may not meet the 1987 American College of Rheumatology classification criteria. The 2010 criteria do not include presence of rheumatoid nodules or radiographic erosive changes, both of which are less likely in early RA. Symmetric arthri- tis is also not required in the 2010 criteria, allowing for early asymmetric presentation.
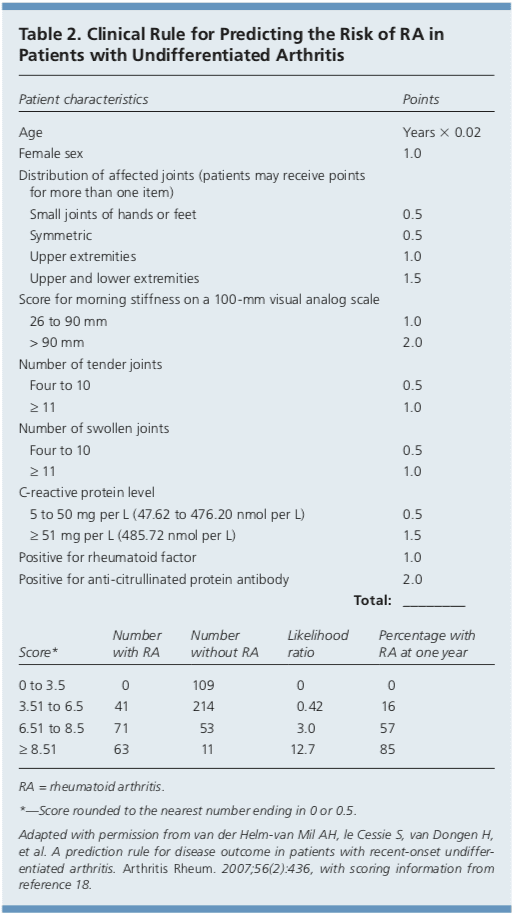
In addition, Dutch researchers have developed and validated a clinical prediction rule for RA (Table 2).17,18 The purpose of this rule is to help identify patients with undifferentiated arthritis that is most likely to progress to RA, and to guide follow-up and referral.
Diagnostic Tests
Autoimmune diseases such as RA are often characterized by the presence of autoanti- bodies. Rheumatoid factor is not specific for RA and may be present in patients with other diseases, such as hepatitis C, and in healthy older persons. Anti-citrullinated protein antibody is more specific for RA and may play a role in disease pathogenesis.6 Approxi- mately 50 to 80 percent of persons with RA have rheumatoid factor, anti-citrullinated protein antibody, or both.10 Patients with RA may have a positive antinuclear antibody test result, and the test is of prognostic impor- tance in juvenile forms of this disease.19 C-reactive protein levels and erythrocyte sedimentation rate are often increased with active RA, and these acute phase reactants are part of the new RA classification criteria.16 C-reactive protein levels and erythrocyte sedimentation rate may also be used to follow disease activity and response to medication.
Baseline complete blood count with differential and assessment of renal and hepatic function are helpful because the results may influence treatment options (e.g., a patient with renal insufficiency or significant thrombocytopenia likely would not be prescribed a nonsteroidal anti-inflammatory drug [NSAID]). Mild anemia of chronic disease occurs in 33 to 60 percent of all patients with RA,20 although gastrointestinal blood loss should also be considered in patients taking corticosteroids or NSAIDs. Methotrexate is contraindicated in patients with hepatic disease, such as hepatitis C, and in patients with significant renal impairment.21 Biologic therapy, such as a TNF inhibitor, requires a negative tuberculin test or treatment for latent tuberculosis. Hepatitis B reactivation can also occur with TNF inhibitor use.22 Radiography of hands and feet should be performed to evaluate for characteristic periarticular erosive changes,�which may be indicative of a more aggressive RA subtype.10
Differential Diagnosis
Skin findings suggest systemic lupus erythematosus, systemic sclerosis, or psoriatic arthritis. Polymyalgia rheumatica should be considered in an older patient with symptoms primarily in the shoulder and hip, and the patient should be asked questions related to associated temporal arteritis.
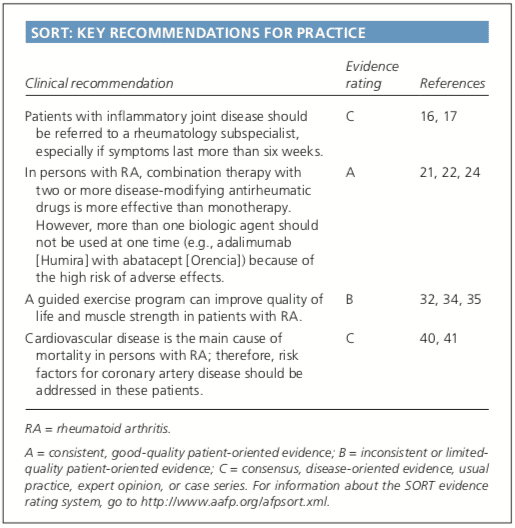
Chest radiography is helpful to evaluate for sarcoidosis as an etiology of arthritis.�Patients with inflammatory back symptoms, a history of inflammatory bowel disease, or inflammatory eye disease may have spondyloarthropathy. Persons with less than six weeks of symptoms may have a viral process, such as parvovirus. Recurrent self-limited episodes of acute joint swelling suggest crystal arthropathy, and arthrocentesis should be performed to evaluate for monosodium urate monohydrate or calcium pyrophosphate dihydrate crystals. The presence of numerous myofascial trigger points and somatic symptoms may suggest fibromyalgia, which can coexist with RA. To help guide diagnosis and determine treatment strategy, patients with inflammatory arthritis should be promptly referred to a rheumatology subspecialist.16,17
Rheumatoid arthritis, or RA, is the most common type of arthritis. RA is an autoimmune disease, caused when the immune system, the human body’s defense system, attacks its own cells and tissues, particularly the joints. Rheumatoid arthritis is frequently identified by symptoms of pain and inflammation, often affecting the small joints of the hands, wrists and feet. According to many healthcare professionals, early diagnosis and treatment of RA is essential to prevent further joint damage and decrease painful symptoms. Dr. Alex Jimenez D.C., C.C.S.T. Insight
Treatment
After RA has been diagnosed and an initial evaluation performed, treatment should begin. Recent guidelines have addressed the management of RA,21,22 but patient preference also plays an important role. There are special considerations for women of childbearing age because many medications have deleterious effects on pregnancy. Goals of therapy include minimizing joint pain and swelling, preventing deformity (such as ulnar deviation) and radiographic damage (such as erosions), maintaining quality of life (personal and work), and controlling extra-articular manifestations. Disease-modifying antirheumatic drugs (DMARDs) are the mainstay of RA therapy.
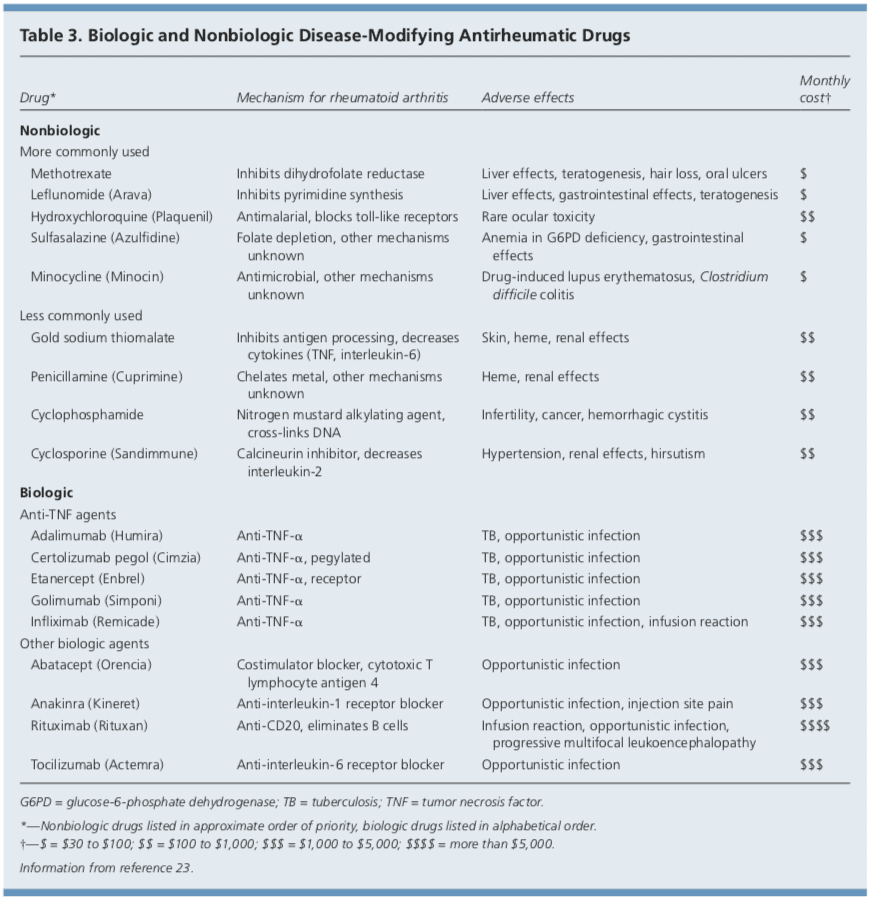
DMARDs
DMARDs can be biologic or nonbiologic (Table 3).23 Biologic agents include monoclonal antibodies and recombinant receptors to block cytokines that promote the inflammatory cascade responsible for RA symptoms. Methotrexate is recommended as the first- line treatment in patients with active RA, unless contraindicated or not tolerated.21 Leflunomide (Arava) may be used as an alternative to methotrexate, although gastrointestinal adverse effects are more common. Sulfasalazine (Azulfidine) or hydroxychloroquine (Plaquenil) pro-inflammatory as monotherapy in patients with low disease�activity or without poor prognostic features (e.g., seronegative, non-erosive RA).21,22
Combination therapy with two or more DMARDs is more effective than monotherapy; however, adverse effects may also be greater.24 If RA is not well controlled with a nonbiologic DMARD, a biologic DMARD should be initiated.21,22 TNF inhibitors are the first-line biologic therapy and are the most studied of these agents. If TNF inhibitors are ineffective, additional biologic therapies can be considered. Simultaneous use of more than one biologic therapy (e.g., adalimumab [Humira] with abatacept [Orencia]) is not�recommended because of an unacceptable rate of adverse effects.21
NSAIDs and Corticosteroids
Drug therapy for RA may involve NSAIDs and oral, intramuscular, or intra-articular corticosteroids for controlling pain and inflammation. Ideally, NSAIDs and corticosteroids are used only for short-term management. DMARDs are the preferred therapy.21,22
Complementary Therapies
Dietary interventions, including vegetarian and Mediterranean diets, have been�studied in the treatment of RA without convincing evidence of benefit.25,26 Despite some favorable outcomes, there is a lack of evidence for the effectiveness of acupuncture in placebo-controlled trials of patients with RA.27,28 In addition, thermotherapy and therapeutic ultrasound for RA have not been studied adequately.29,30 A Cochrane review of herbal treatments for RA concluded that gamma-linolenic acid (from evening primrose or black currant seed oil) and Tripterygium wilfordii (thunder god vine) have potential benefits.31 It is important to inform patients that serious adverse effects have been reported with use of herbal therapy.31
Exercise and Physical Therapy
Results of randomized controlled trials sup- port physical exercise to improve quality of life and muscle strength in patients with RA.32,33 Exercise training programs have not been shown to have deleterious effects on RA disease activity, pain scores, or radiographic joint damage.34 Tai chi has been shown to improve ankle range of motion in persons with RA, although randomized trials are limited.35 Randomized controlled trials of Iyengar yoga in young adults with RA are underway.36
Duration of Treatment
Remission is obtainable in 10 to 50 percent of patients with RA, depending on how remission is defined and the intensity of therapy.10 Remission is more likely in males, nonsmokers, persons younger than 40 years, and in those with late-onset disease (patients older than 65 years), with shorter duration of disease, with milder disease activity, without elevated acute phase reactants, and without positive rheumatoid factor or anti-citrullinated protein antibody findings.37
After the disease is controlled, medication dosages may be cautiously decreased to the minimum amount necessary. Patients will require frequent monitoring to ensure stable symptoms, and prompt increase in medication is recommended with disease flare-ups.22
Joint Replacement
Joint replacement is indicated when there is severe joint damage and unsatisfactory control of symptoms with medical management. Long-term outcomes are support, with only 4 to 13 percent of large joint replacements requiring revision within 10 years.38 The hip and knee are the most commonly replaced joints.
Long-Term Monitoring
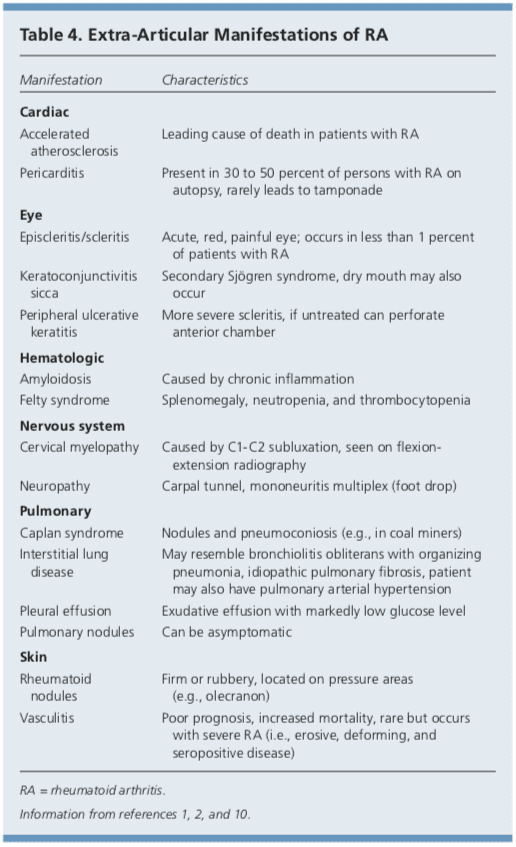
Although RA is considered a disease of the joints, it is also a systemic disease capable of involving multiple organ systems. Extra-articular manifestations of RA are included in Table 4.1,2,10
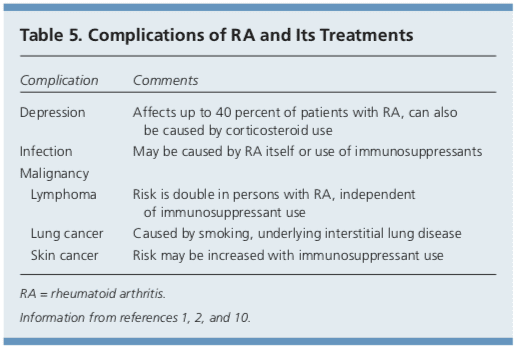
Patients with RA have a twofold increased risk of lymphoma, which is thought to be caused by the underlying inflammatory�process, and not a consequence of medical treatment.39 Patients with RA are also at an increased risk of coronary artery disease, and physicians should work with patients to modify risk factors, such as smoking, high blood pressure, and high cholesterol.40,41 Class III or IV congestive heart failure (CHF) is a contraindication for using TNF inhibitors, which can worsen CHF outcomes.21 In patients with RA and malignancy, caution is needed with continued use of DMARDs, especially TNF inhibitors. Biologic DMARDs, methotrexate, and leflunomide should not be initiated in patients with active herpes zoster, significant fungal infection, or bacterial infection requiring antibiotics.21 Complications of RA and its treatments are listed in Table 5.1,2,10
Prognosis
Patients with RA live three to 12 years less than the general population.40 Increased mortality in these patients is mainly due to accelerated cardiovascular disease, especially in those with high disease activity and chronic inflammation. The relatively new biologic therapies may reverse progression of atherosclerosis and extend life in those with RA.41
Data Sources: A PubMed search was completed in Clinical Queries using the key terms rheumatoid arthritis, extra-articular manifestations, and disease-modifying antirheumatic agents. The search included meta-analyses, randomized controlled trials, clinical trials, and reviews. Also searched were the Agency for Healthcare Research and Quality evidence reports, Clinical Evidence, the Cochrane database, Essential Evidence, and UpToDate. Search date: September 20, 2010.
Author disclosure: No relevant financial affiliations to disclose.
In conclusion, rheumatoid arthritis is a chronic, autoimmune disease which causes painful symptoms, such as pain and discomfort, inflammation and swelling of the joints, among others. The joint damage characterized as RA is symmetrical, meaning it generally affects both sides of the body. Early�diagnosis is essential for treatment of RA. The scope of our information is limited to chiropractic and spinal health issues. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topic Discussion: Relieving Knee Pain without Surgery
Knee pain is a well-known symptom which can occur due to a variety of knee injuries and/or conditions, including�sports injuries. The knee is one of the most complex joints in the human body as it is made-up of the intersection of four bones, four ligaments, various tendons, two menisci, and cartilage. According to the American Academy of Family Physicians, the most common causes of knee pain include patellar subluxation, patellar tendinitis or jumper’s knee, and Osgood-Schlatter disease. Although knee pain is most likely to occur in people over 60 years old, knee pain can also occur in children and adolescents. Knee pain can be treated at home following the RICE methods, however, severe knee injuries may require immediate medical attention, including chiropractic care.
1. Etiology and pathogenesis of rheumatoid arthritis. In: Firestein GS, Kelley WN, eds. Kelley�s Textbook of Rheu- matology. 8th ed. Philadelphia, Pa.: Saunders/Elsevier; 2009:1035-1086. 2. Bathon J, Tehlirian C. Rheumatoid arthritis clinical and laboratory manifestations. In: Klippel JH, Stone JH, Crofford LJ, et al., eds. Primer on the Rheumatic Dis- eases. 13th ed. New York, NY: Springer; 2008:114-121. 3. Allaire S, Wolfe F, Niu J, et al. Current risk factors for work disability associated with rheumatoid arthritis. Arthritis Rheum. 2009;61(3):321-328. 4. MacGregor AJ, Snieder H, Rigby AS, et al. Characteriz- ing the quantitative genetic contribution to rheumatoid arthritis using data from twins. Arthritis Rheum. 2000; 43(1):30-37. 5. Orozco G, Barton A. Update on the genetic risk fac- tors for rheumatoid arthritis. Expert Rev Clin Immunol. 2010;6(1):61-75. 6. Balsa A, Cabezo?n A, Orozco G, et al. Influence of HLA DRB1 alleles in the susceptibility of rheumatoid arthritis and the regulation of antibodies against citrullinated proteins and rheumatoid factor. Arthritis Res Ther. 2010;12(2):R62. 7. McClure A, Lunt M, Eyre S, et al. Investigating the via- bility of genetic screening/testing for RA susceptibility using combinations of five confirmed risk loci. Rheuma- tology (Oxford). 2009;48(11):1369-1374. 8. Bang SY, Lee KH, Cho SK, et al. Smoking increases rheu- matoid arthritis susceptibility in individuals carrying the HLA-DRB1 shared epitope, regardless of rheumatoid factor or anti-cyclic citrullinated peptide antibody sta- tus. Arthritis Rheum. 2010;62(2):369-377. 9. Wilder RL, Crofford LJ. Do infectious agents cause rheu- matoid arthritis? Clin Orthop Relat Res. 1991;(265): 36-41. 10. Scott DL, Wolfe F, Huizinga TW. Rheumatoid arthritis. Lancet. 2010;376(9746):1094-1108. 11. Costenbader KH, Feskanich D, Mandl LA, et al. Smoking intensity, duration, and cessation, and the risk of rheu- matoid arthritis in women. Am J Med. 2006;119(6): 503.e1-e9. 12. Kaaja RJ, Greer IA. Manifestations of chronic disease during pregnancy. JAMA. 2005;294(21):2751-2757. 13. Guthrie KA, Dugowson CE, Voigt LF, et al. Does preg- nancy provide vaccine-like protection against rheuma- toid arthritis? Arthritis Rheum. 2010;62(7):1842-1848. 14. Karlson EW, Mandl LA, Hankinson SE, et al. Do breast- feeding and other reproductive factors influence future risk of rheumatoid arthritis? Results from the Nurses� Health Study. Arthritis Rheum. 2004;50(11):3458-3467. 15. Karlson EW, Shadick NA, Cook NR, et al. Vitamin E in the primary prevention of rheumatoid arthritis: the Women�s Health Study. Arthritis Rheum. 2008;59(11): 1589-1595. 16. Aletaha D, Neogi T, Silman AJ, et al. 2010 rheumatoid arthritis classification criteria: an American College of Rheumatology/European League Against Rheumatism collaborative initiative [published correction appears in Ann Rheum Dis. 2010;69(10):1892]. Ann Rheum Dis. 2010;69(9):1580-1588. 17. van der Helm-van Mil AH, le Cessie S, van Dongen H, et al. A prediction rule for disease outcome in patients with recent-onset undifferentiated arthritis. Arthritis Rheum. 2007;56(2):433-440. 18. Mochan E, Ebell MH. Predicting rheumatoid arthritis risk in adults with undifferentiated arthritis. Am Fam Physi- cian. 2008;77(10):1451-1453. 19. Ravelli A, Felici E, Magni-Manzoni S, et al. Patients with antinuclear antibody-positive juvenile idiopathic arthri- tis constitute a homogeneous subgroup irrespective of the course of joint disease. Arthritis Rheum. 2005; 52(3):826-832. 20. Wilson A, Yu HT, Goodnough LT, et al. Prevalence and outcomes of anemia in rheumatoid arthritis. Am J Med. 2004;116(suppl 7A):50S-57S. 21. Saag KG, Teng GG, Patkar NM, et al. American College of Rheumatology 2008 recommendations for the use of nonbiologic and biologic disease-modifying antirheu- matic drugs in rheumatoid arthritis. Arthritis Rheum. 2008;59(6):762-784. 22. Deighton C, O�Mahony R, Tosh J, et al.; Guideline Devel- opment Group. Management of rheumatoid arthritis: summary of NICE guidance. BMJ. 2009;338:b702. 23. AHRQ. Choosing medications for rheumatoid arthritis. April 9, 2008. http://www.effectivehealthcare.ahrq.gov/ ehc/products/14/85/RheumArthritisClinicianGuide.pdf. Accessed June 23, 2011. 24. Choy EH, Smith C, Dore? CJ, et al. A meta-analysis of the efficacy and toxicity of combining disease-modify- ing anti-rheumatic drugs in rheumatoid arthritis based on patient withdrawal. Rheumatology (Oxford). 2005; 4 4 (11) :1414 -1421. 25. Smedslund G, Byfuglien MG, Olsen SU, et al. Effective- ness and safety of dietary interventions for rheumatoid arthritis. J Am Diet Assoc. 2010;110(5):727-735. 26. Hagen KB, Byfuglien MG, Falzon L, et al. Dietary inter- ventions for rheumatoid arthritis. Cochrane Database Syst Rev. 2009;21(1):CD006400. 27. Wang C, de Pablo P, Chen X, et al. Acupuncture for pain relief in patients with rheumatoid arthritis: a systematic review. Arthritis Rheum. 2008;59(9):1249-1256. 28. Kelly RB. Acupuncture for pain. Am Fam Physician. 2009;80(5):481-484. 29. Robinson V, Brosseau L, Casimiro L, et al. Thermother- apy for treating rheumatoid arthritis. Cochrane Data- base Syst Rev. 2002;2(2):CD002826. 30. Casimiro L, Brosseau L, Robinson V, et al. Therapeutic ultrasound for the treatment of rheumatoid arthritis. Cochrane Database Syst Rev. 2002;3(3):CD003787. 31. Cameron M, Gagnier JJ, Chrubasik S. Herbal therapy for treating rheumatoid arthritis. Cochrane Database Syst Rev. 2011;(2):CD002948. 32. Brodin N, Eurenius E, Jensen I, et al. Coaching patients with early rheumatoid arthritis to healthy physical activ- ity. Arthritis Rheum. 2008;59(3):325-331. 33. Baillet A, Payraud E, Niderprim VA, et al. A dynamic exercise programme to improve patients� disability in rheumatoid arthritis: a prospective randomized con- trolled trial. Rheumatology (Oxford). 2009;48(4): 410-415. 34. Hurkmans E, van der Giesen FJ, Vliet Vlieland TP, et al. Dynamic Exercise programs (aerobic capacity and/or mus- cle strength training) in patients with rheumatoid arthri- tis. Cochrane Database Syst Rev. 2009;(4):CD006853. 35. Han A, Robinson V, Judd M, et al. Tai chi for treat- ing rheumatoid arthritis. Cochrane Database Syst Rev. 2004;(3):CD004849. 36. Evans S, Cousins L, Tsao JC, et al. A randomized con- trolled trial examining Iyengar yoga for young adults with rheumatoid arthritis. Trials. 2011;12:19. 37. Katchamart W, Johnson S, Lin HJ, et al. Predictors for remis- sion in rheumatoid arthritis patients: a systematic review. Arthritis Care Res (Hoboken). 2010;62(8):1128-1143. 38. Wolfe F, Zwillich SH. The long-term outcomes of rheu- matoid arthritis: a 23-year prospective, longitudinal study of total joint replacement and its predictors in 1,600 patients with rheumatoid arthritis. Arthritis Rheum. 1998;41(6):1072-1082. 39. Baecklund E, Iliadou A, Askling J, et al. Association of chronic inflammation, not its treatment, with increased lymphoma risk in rheumatoid arthritis. Arthritis Rheum. 2006;54(3):692-701. 40. Friedewald VE, Ganz P, Kremer JM, et al. AJC editor�s consensus: rheumatoid arthritis and atherosclerotic cardiovascular disease. Am J Cardiol. 2010;106(3): 442-447. 41. Atzeni F, Turiel M, Caporali R, et al. The effect of phar- macological therapy on the cardiovascular system of patients with systemic rheumatic diseases. Autoimmun Rev. 2010;9(12):835-839.
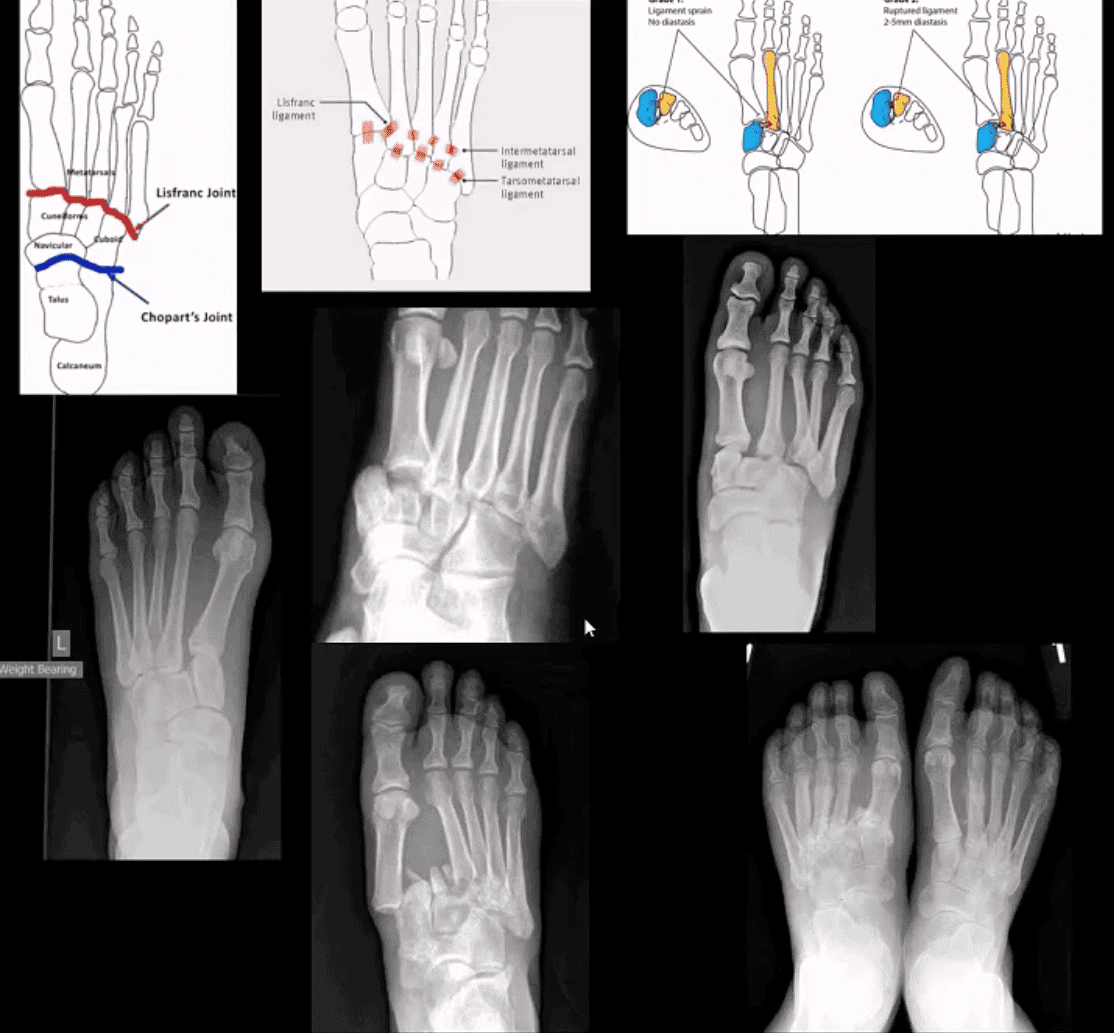
M/C dislocation of the foot at tarsal-metatarsal articulation (Lisfranc joint). Direct impact or landing and plantar or dorsal flexing the foot. Lisfranc ligament holding 2nd MT base and 1st Cu is torn. Manifests with or w/o fracture-avulsion.
Imaging: 1st step: foot radiography in most cases sufficient to Dx. MSK US may help: show disrupted Cu1-Cu2. Ligament and widened space > 2.5mm. MRI may help but not essential. Weight-bearing view aids Dx.
2-types: homolateral (1st MTP joint in contact) and divergent (2-5 MT displaced laterally and 1st MT medially)
Management: operative fixation is crucial
N.B. Atraumatic Lisfranc dislocation is a frequent complication of a diabetic Charcot foot
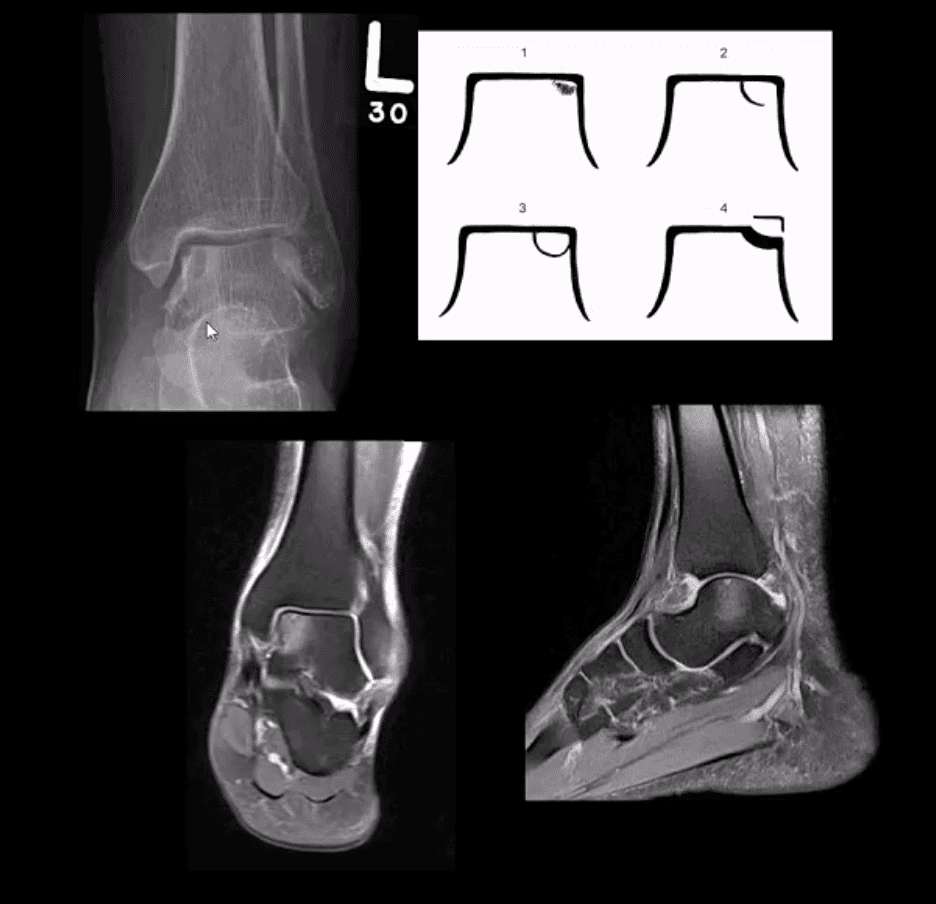
Osteochondral Injury of the Talus (OCD)
Common. Non-traumatic found in superior-medial talar dome. Traumatic may affect supero-lateral dome.
Clinically: pain/effusion/locking. Imaging is crucial.
1st step: radiography may reveal focal radiolucent concavity/halo, fragment.
MRI helpful esp. if OCD is cartilaginous and to demonstrate bone edema.
Jones Fx: extra-articular Fx of proximal metaphysis of the 5th MT. Prone to non-union. Often fixed operatively.
Pseudo-Jones: intra-articular avulsion of 5th MT styloid/base by eccentric contraction of Peroneus Brevis M. Managed conservatively: boot-cast immobilization. Both Jones & Pseudo-Jones Dx by foot series radiography.
Stress Fx. Calcaneus, 2nd, 3rd, 5th MTs. Repeated loading (running) or “March foot” 2nd/3rd MT. Clinically: pain on activity, reduced by rest. Dx: x-rays often unrewarding earlier. MRI or MSK US may help. Managed: Conservatively. Complications; progress into complete Fx
Turf toe: common athletic hyperextension of 1st MTP-sesamoid/plantar plate complex is tearing. 1st MTP unstable/loose. Managed operatively.
Arthritis of the Foot & Ankle
DJD of the ankle: uncommon a primary OA. Typically develops as 2nd to trauma/AVN, RA, CPPD, Hemophilic arthropathy, Juvenile Idiopathic Arthritis, etc. manifests as DJD: osteophytes, JSL, subchondral cysts all seen on x-rays
Inflammatory Arthritis: RA may develop in the ankle or any synovial joint. Will typically presents with symmetrical Hands/feet RA initially (2nd, 3rd MCP, wrists, MTPs in feet) usually with erosion, uniform JSL, juxta-articular osteopenia, and delayed subluxations.
HLA-B27 spondyloarthropathies: commonly affect lower extremity: heel, ankle esp in Reactive (Reiter). Erosive-productive bone proliferation is a crucial Dx.
Gouty Arthritis: common in the lower extremity. Ankle, mid-foot foot esp 1st MTPs. Initial onset: acute gouty arthritis with ST effusion and no erosions/tophi. Chronic tophaceous gout: peri-articular, intra-osseous punched-out erosions with over-hanging edges, no initial JSL/osteopenia, ST. Tophi may be seen.
Miscellaneous arthropathy: PVNS. Not common. Affects 3-4th decades of life. The result of synovial proliferation with Macrophages and multi-nucleated Giant Cells filled with hemosiderin and fatty accumulation may lead to inflammation, cartilage damage, extrinsic bone erosions. Dx: x-rays are insensity, MRI modality of choice. Synovial biopsy. Management: operative, can be difficult.
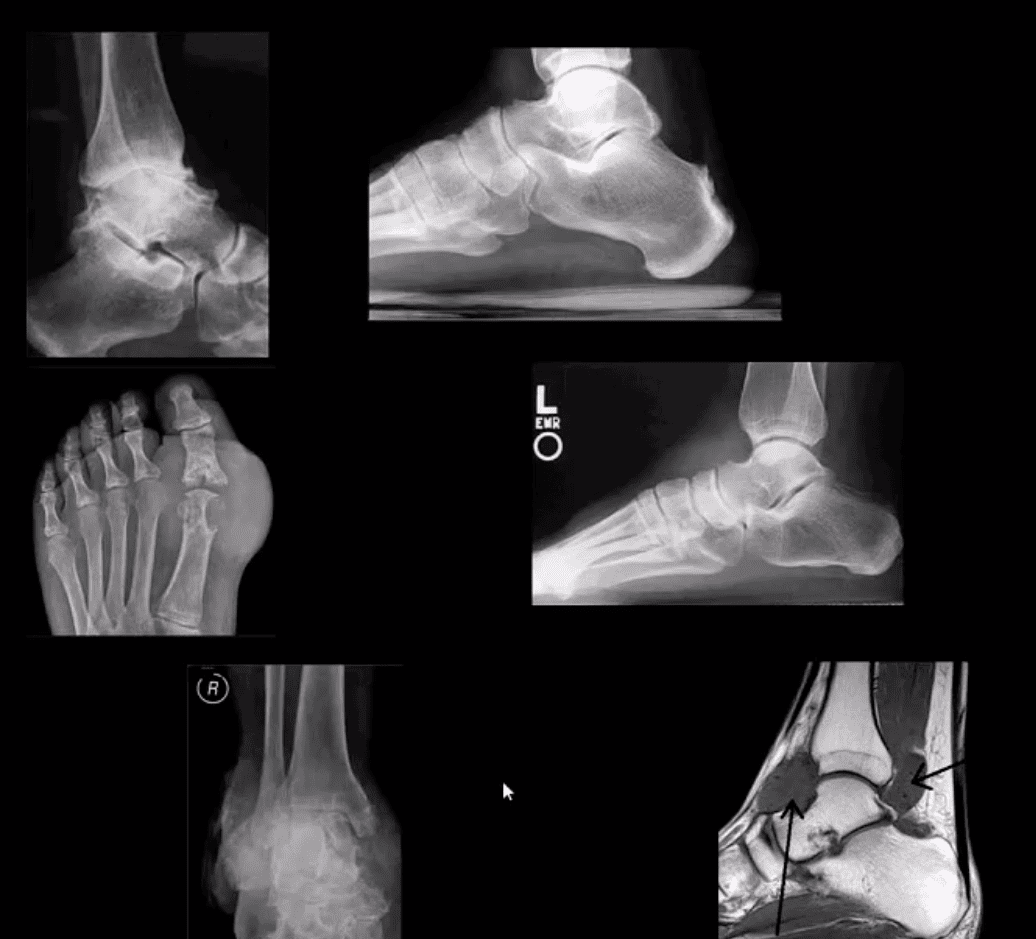
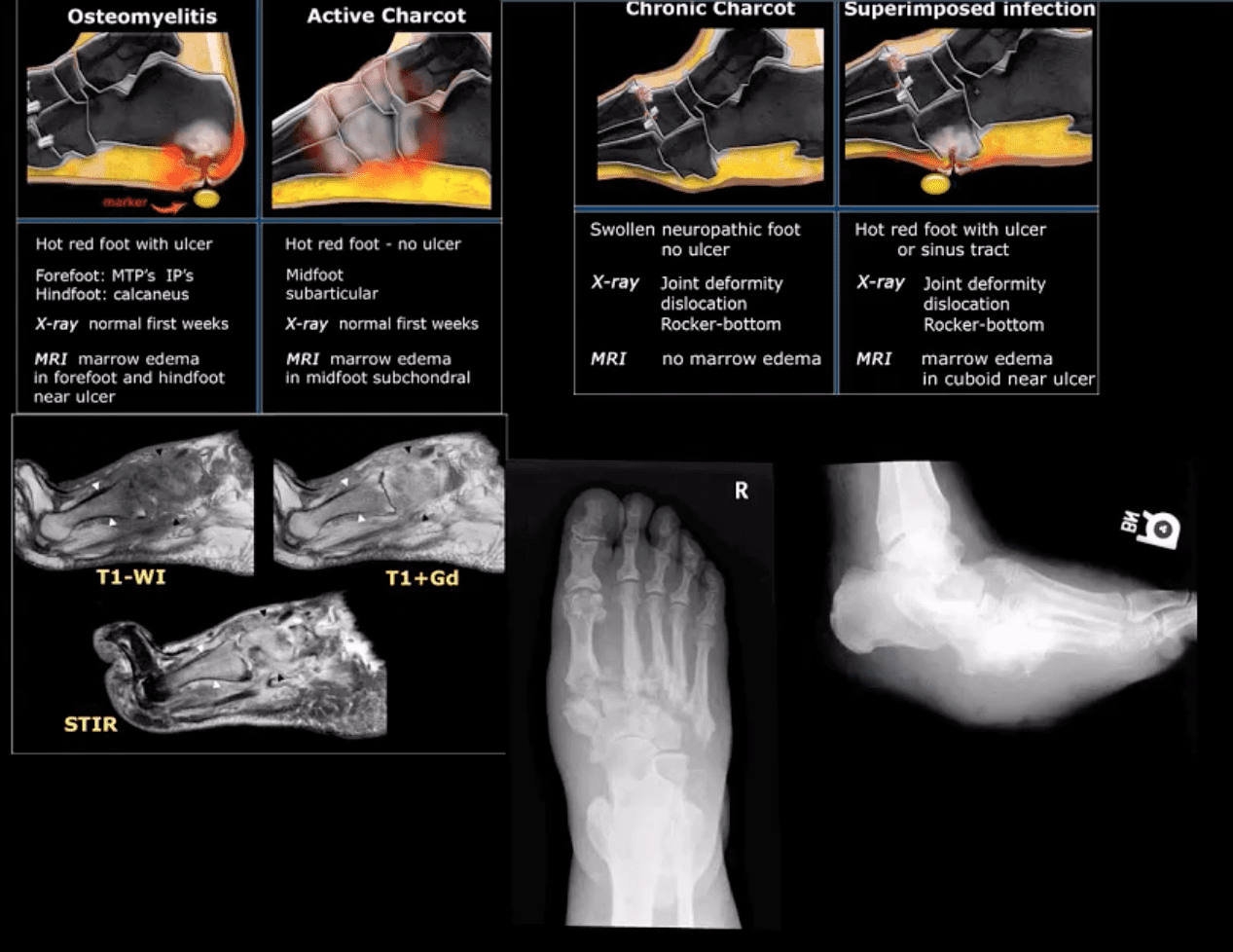
Neuropathic Osteoarthropathy
(Charcot’s joint) Common and on the rise d/t epidemic in type 2 DM. May present with pain initially (50% of cases) and painless destructive arthropathy as a late manifestation. Early Dx: delayed. Imaging is crucial: x-rays: initially unrewarding, some SF effusion is seen. MRI helps with early Dx and extremity off-loading. Late Dx: irreversible dislocations, collapse, disability. Note: Lisfrance dislocation in Charcot joint
M/C mid-foot (TM joint) in 40% of cases, ankle 15%. Progression: Rocker-bottom foot, ulcerations, infections, increased morbidity, and mortality.
Early Dx: by MRI is crucial. Suspect it in patients with type 2 DM especially if early non-traumatic foot/ankle pain reported.
Arthritis is characterized as the inflammation of one or multiple joints. The most common symptoms of arthritis include pain and discomfort, swelling, inflammation, and stiffness, among others. Arthritis may affect�any joint in the human body, however, it commonly develops in the knee. � Knee arthritis can make everyday�physical activities difficult. The most prevalent types of arthritis are osteoarthritis and rheumatoid arthritis, although there are well over 100 distinct forms of arthritis, affecting children and adults alike. While there is no cure for arthritis, many treatment approaches can help treat the symptoms of knee arthritis.
Anatomy of the Knee
� The knee is the largest and strongest joint in the human body. It is made up of the lower end of the thigh bone,�or femur, the top end of the shin bone, or tibia, and the kneecap, or patella. The ends of the three bones are covered with articular cartilage, a smooth, slippery structure which protects and cushions the bones when bending and straightening the knee.
� Two wedge-shaped parts of cartilage, known as the meniscus, function as shock absorbers between the bones of the knee to help cushion the joint and provide stability. The knee joint is also surrounded by a thin lining known as the synovial membrane. This membrane releases a fluid which lubricates the cartilage and also helps reduce friction in the knee. The significant kinds of arthritis that affect the knee�include osteoarthritis, rheumatoid arthritis, and post-traumatic arthritis.
Osteoarthritis
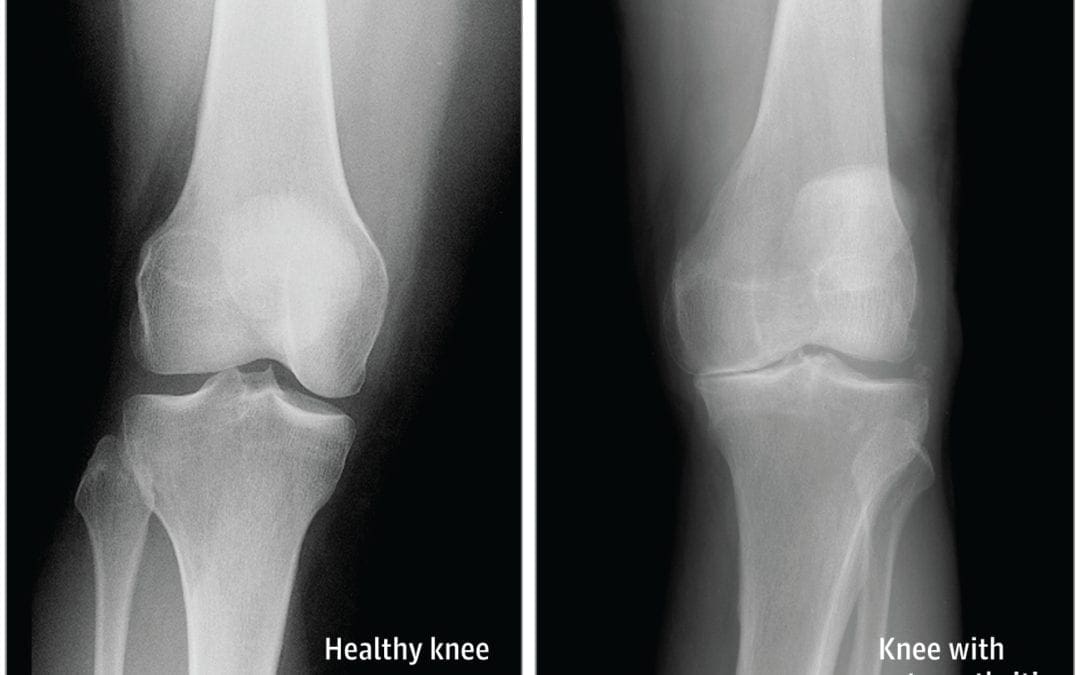
� Osteoarthritis is the most common type of arthritis which affects the knee joint. This form of arthritis is a degenerative, wear-and-tear health issue which occurs most commonly in people 50 years of age and older, however, it may also develop in younger people.
� In osteoarthritis, the cartilage in the knee joint gradually wears away. As the cartilage wears away, the distance between the bones decreases. This can result in bone rubbing and it can�create painful bone spurs. Osteoarthritis generally develops slowly but the pain may worsen over time.
Rheumatoid Arthritis
� Rheumatoid arthritis is a chronic health issue which affects multiple joints throughout the body, especially the knee joint. RA is also symmetrical, meaning it often affects the same joint on each side of the human body.
� In rheumatoid arthritis, the synovial membrane that covers the knee joint becomes inflamed and swollen, causing knee pain, discomfort, and stiffness. RA is an autoimmune disease, which means that the immune system attacks its own soft tissues. The immune system attacks healthy tissue,�including tendons, ligaments and cartilage, as well as softens the bone.
Post-traumatic Arthritis
� Posttraumatic arthritis is a form of arthritis that develops after damage or injury to the knee. By way of instance, the knee joint may be harmed by a broken bone, or fracture, and result in post-traumatic arthritis years after the initial injury. Meniscal tears and ligament injuries can cause additional wear-and-tear on the knee joint, which over time can lead to arthritis and other problems.
Symptoms of Knee Arthritis
� The most common symptoms of knee arthritis include pain and discomfort, inflammation, swelling, and stiffness. Although sudden onset is probable, the painful symptoms generally�develop gradually over time. Additional symptoms of knee arthritis can be recognized as follows:
The joint may become stiff and swollen, making it difficult to bend and straighten the knee.
Swelling and inflammation may be worse in the morning, or when sitting or resting.
Vigorous activity might cause the pain to flare up.
Loose fragments of cartilage and other soft tissue may interfere with the smooth motion of the joints, causing the knee to lock or stick through motion. It could also creak, click, snap or make a grinding sound, known as crepitus.
Pain can cause a sense of fatigue or buckling from the knee.
Many individuals with arthritis may also describe increased joint pain with rainy weather and climate changes.
Diagnosis for Knee Arthritis
� During the patient’s appointment for diagnosis of knee arthritis, the healthcare professional will talk about the symptoms and medical history, as well as conduct a physical examination. The doctor may also order imaging diagnostic tests, such as X-rays, MRI or blood tests for further diagnosis. During the physical examination, the doctor will search for:
Joint inflammation, swelling, warmth, or redness
Tenderness around the knee joint
Assortment of passive and active movement
Instability of the knee joint
Crepitus, the grating sensation inside the joint, with motion
Pain when weight is placed on the knee
Issues with gait, or manner of walking
Any signs of damage or injury to the muscles, tendons, and ligaments surrounding the knee joint
Involvement of additional joints (an indicator of rheumatoid arthritis)
Imaging Diagnostic Tests
X-rays. These imaging diagnostic tests produce images of compact structures, such as bones. They can help distinguish among various forms of arthritis. X-rays for knee arthritis may demonstrate a portion of the joint distance, changes in the bone as well as the formation of bone spurs, known as osteophytes.
Additional tests. Sometimes, magnetic resonance imaging, or MRI, scans, computed tomography, or CT,�scans, or bone scans are required to ascertain the condition of the bone and soft tissues of the knee.
Blood Tests
� Your doctor may also recommend blood tests to determine which type of arthritis you have. With some kinds of arthritis, such as rheumatoid arthritis, blood tests can help with the proper identification of the disease.
Although the knee joint is one of the strongest and largest joints in the human body, it is often prone to suffering damage or injury, resulting in a variety of conditions. In addition, however, other health issues, such as arthritis, can affect the knee joint. In network for most insurances of El Paso, TX, chiropractic care can help ease painful symptoms associated with knee arthritis, among other health issues. Dr. Alex Jimenez D.C., C.C.S.T. Insight
�
Treatment for Knee Arthritis
Non-surgical Treatment
� Non-surgical treatment approaches are often recommended before considering surgical treatment for knee arthritis. Healthcare professionals may recommend a variety of treatment options, including chiropractic care, physical therapy, and lifestyle modifications, among others.
� Lifestyle modifications. Some lifestyle modifications can help protect the knee joint and impede the progress of arthritis. Minimizing physical activities which aggravate the condition, will put less strain on the knee. Losing weight may also help lessen stress and pressure on the knee joint, resulting in less painful symptoms and increased function.
� Chiropractic care and physical therapy.�Chiropractic care utilizes full body chiropractic adjustments to carefully restore any spinal misalignments, or subluxations, which may�be causing symptoms, including arthritis. The doctor may also recommend physical therapy to create an individualized exercise and physical activity program for each patient’s needs.�Specific exercises will help increase range of motion and endurance, as well as help strengthen the muscles in the lower extremities.
� Assistive devices. Using assistive devices, such as a cane, shock-absorbing shoes or inserts, or a brace or knee sleeve, can decrease painful symptoms. A brace helps with function and stability, and may be particularly useful if the arthritis is based on one side of the knee. There are two types of braces that are often used for knee arthritis: A “unloader” brace shifts weight from the affected section of the knee, while a “support” brace helps support the entire knee load.
� Drugs and/or medications. Several types of medications are useful in treating arthritis of the knee. Since individuals respond differently to medications, your doctor will work closely with you to determine the medications and dosages which are safe and effective for you.
Surgical Treatment
� The healthcare professional may recommend surgical treatment if the patient’s knee arthritis causes severe disability and only if the problem isn’t relieved with non-surgical treatment. Like all surgeries, there are a few risks and complications with surgical treatment for knee arthritis. The�doctor will discuss the possible problems with the patient.
� Arthroscopy. During arthroscopy, physicians use instruments and small incisions to diagnose and treat knee joint problems. Arthroscopic surgery isn’t frequently used in the treatment of arthritis of the knee. In cases where osteoarthritis is accompanied with a degenerative meniscal tear, arthroscopic surgery may be wise to treat the torn meniscus.
� Cartilage grafting. Normal cartilage tissue may be taken from a tissue bank or through a different part of the knee to fill out a hole in the articular cartilage. This process is typically considered only for younger patients.
� Synovectomy. The lining damaged by rheumatoid arthritis is eliminated to reduce swelling and pain.
� Osteotomy. In a knee osteotomy, either the tibia (shinbone) or femur (thighbone) is cut then reshaped to relieve stress and pressure on the knee joint. Knee�osteotomy is utilized when early-stage osteoarthritis has damaged one facet of the knee joint. By changing the weight distribution, this can relieve and enhance the function of the knee.
� Total or partial knee replacement (arthroplasty).�The�doctor will remove the damaged bone and cartilage, then place new plastic or metal surfaces to restore the function of the knee�and its surrounding structures.
� Following any type of surgery for knee�arthritis will involve a period of recovery. Recovery time and rehabilitation will depend on the type of surgery performed. It’s essential to talk with your healthcare professional to determine the best treatment option for your�knee arthritis. The scope of our information is limited to chiropractic and spinal health issues. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
� Curated by Dr. Alex Jimenez �
�
Additional Topic Discussion: Relieving Knee Pain without Surgery
� Knee pain is a well-known symptom which can occur due to a variety of knee injuries and/or conditions, including�sports injuries. The knee is one of the most complex joints in the human body as it is made-up of the intersection of four bones, four ligaments, various tendons, two menisci, and cartilage. According to the American Academy of Family Physicians, the most common causes of knee pain include patellar subluxation, patellar tendinitis or jumper’s knee, and Osgood-Schlatter disease. Although knee pain is most likely to occur in people over 60 years old, knee pain can also occur in children and adolescents. Knee pain can be treated at home following the RICE methods, however, severe knee injuries may require immediate medical attention, including chiropractic care.
As we age, specific changes take place in the body. The spine gets a lot of wear and tear because it is the primary supportive structure that does everything from keeping the head upright to providing a pathway for neural impulses, to providing mobility. It�s no wonder that there comes the point where the body does not function like it once did. Cervical spondylosis is a broad term describing a condition that is related to the natural wear and tear on the disks in the neck.
What is Cervical Spondylosis?
Also known as neck arthritis or cervical osteoarthritis, cervical spondylosis is very common in elderly patients, particularly in those over age 60. More than 85% of people over 60 years of age have some form of it, usually with few or no symptoms present. It does get worse with age, though, so it could progress to the point where the patient does experience pain, reduced flexibility, stiffness, lack of mobility, or other symptoms.
Cervical spondylosis is a blanket term that is used to describe some conditions, and while it is usually considered an age-related condition, it can have other causes as well including heredity. This condition often begins with changes in the disk.
With age, the disks in the spine and neck will dehydrate. This causes them to shrink, leaving little or no padding between the vertebrae. As a result, the patient may develop signs of osteoarthritis and in some cases, bone spurs. Depending on how the condition progresses and presents, it can be a cause of chronic pain.
What are the Treatments for Cervical Spondylosis?
Treatment for cervical spondylosis involves relieving the symptoms. There is no way to reverse the effects that it has on the body so treating the pain, stiffness, and other issues that accompany the condition is the course that is usually taken by doctors. Depending on the exact symptoms, treatment may include using an ice pack, bed rest, warm compress, and low impact exercise as the patient can handle it.
The doctor may recommend an analgesic or nonsteroidal anti-inflammatory drug (NSAID). In cases where the pain is severe and difficult to manage, they may prescribe a narcotic painkiller, steroids, or a muscle relaxant.
They might also combine drug therapy with physical therapy. In very severe cases the doctor may recommend spinal injections or surgery. Some common operations for cervical spondylosis include intervertebral disc arthroplasty, invertebral disc annuloplasty, and spinal fusion.
In many cases, soft collars, rigid orthoses, molded cervical pillow, or a Philadelphia collar may be recommended to provide support. However, many doctors believe that these methods are not entirely effective and that any benefit the patient receives is primarily due to a placebo effect.
This is because the neck is still mobile and does not have�restrictions of movement. If used correctly, though, it can provide some support. This means that the patient needs to wear it as much as possible when they are not sleeping.
In many cases, the medications have unpleasant side effects, and some can even be harmful. This is especially true with prescription pain medications which can be addictive.
Surgery is also not a preferred treatment due to potential complications, the invasiveness of the procedure, and the length of time it takes to heal. Often patients seek other forms of treatment that are more natural and gentle on the body. Chiropractic is one of the most popular remedies for cervical spondylosis.
Chiropractic for Cervical Spondylosis
Chiropractic is a popular treatment for cervical spondylosis. Many patients gravitate toward it because it is non-invasive and does not use harmful medications. Its natural, whole body approach makes it an appealing treatment method.
In addition to spinal manipulation, the chiropractor may use massage to help relieve stiffness and pain. He or she may also recommend ice or heat, rest, stretching, lifestyle changes, and even dietary modifications.
Patients may be advised to remove foods from their diet that increase inflammation and taught special exercises that help keep the neck supple. Some chiropractors recommend special supplements to help work with the body enabling its natural ability to heal itself.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine