The most common causes of TBI which result in ER visits include slip-and-fall accidents, blows to the head, and automobile accidents. Abrupt forces which jolt the brain violently within the skull, such as shock waves from explosions, which can also cause TBI. Traumatic brain injury can also result from bullet wounds or other injuries which penetrate the skull and brain. �
Doctors characterize traumatic brain injury as mild, moderate, or severe depending on whether the injury causes unconsciousness, how long it lasts, and other symptoms. Although most traumatic brain injuries are characterized as mild because they’re not considered life-threatening, even a mild TBI can have serious and long-lasting effects if left untreated. � Resulting from an impact to the head which interrupts brain function, TBI is a threat to cognitive health in two ways: �
The effects of traumatic brain injury, which may be long-lasting or even permanent, can include unconsciousness, inability to recall the event, confusion, difficulty learning new information, trouble speaking, unsteadiness, lack of coordination, and health issues associated with vision or hearing, among other common symptoms.
TBI may increase the risk of developing Alzheimer’s disease or dementia, years after the injury takes place.
According to the Centers for Disease Control and Prevention (CDC), approximately 2.8 million TBI-associated ER visits, hospitalizations, and deaths occurred in 2013, the latest year for which information is available. The purpose of the following article is to discuss traumatic brain injury (TBI) and its connection with Alzheimer’s disease and other health issues. �
Traumatic Brain Injury Causes
Slip-and-fall accidents are the most common cause of traumatic brain injury, where falls pose a potentially serious risk factor for older adults. According to a CDC special report evaluating data from several federal agencies, approximately 56,000 seniors are hospitalized every year as a result of head injuries sustained in falls. A serious TBI from a slip-and-fall accident may ultimately result in long-term cognitive changes and reduced ability to function as well as overall mood changes. �
About 775,000 older adults have traumatic brain injury-related disability. Measures to reduce the risk of falls include: �
Using a walker or other assistive device to compensate for mobility problems, muscle weakness or poor balance.
Having your vision checked regularly and using glasses or contact lenses that correct for changes.
Working with your doctor to watch for medication side effects or interactions among drugs you�re taking.
Avoiding household hazards, such as clutter, loose rugs or poor lighting.
Automobile accidents are another common cause of traumatic brain injury (TBI). People can reduce the risk of being involved in an auto accident by keeping their vehicle in good condition, following the rules of the road, and buckling their seat belt. Wearing a helmet and when biking, inline skating, or playing contact sports can also help protect the head from TBI. �
TBI Symptoms
The severity of symptoms for traumatic brain injuries largely depends on whether the injury is mild, moderate, or severe. Mild traumatic brain injury (TBI), also known as a concussion, can either not cause unconsciousness or can cause unconsciousness which lasts for 30 minutes or less. Mild traumatic brain injury (TBI) symptoms may include: �
Inability to remember the traumatic event immediately before or up to 24 hours after
Confusion and disorientation
Difficulty learning new information
Headache
Dizziness
Blurry vision
Nausea and vomiting
Ringing in the ears
Trouble speaking coherently
Mood changes or changes in sleeping patterns
These symptoms will commonly manifest at the time of the TBI or soon after, however, these may sometimes not develop till several days or even weeks following the traumatic event. Mild TBI symptoms are generally temporary and these will clear up within hours, days, or weeks following the traumatic even, however, they can occasionally last several months or longer. �
Moderate traumatic brain injury can cause unconsciousness which lasts more than 30 minutes but less than 24 hours and severe traumatic brain injury can cause unconsciousness for more than 24 hours. Symptoms of moderate and severe traumatic brain injury are similar to those of mild traumatic brain injury but these are more serious and longer-lasting. �
In all types of TBI, cognitive changes are the most common symptoms. The ability to learn and remember new information is also frequently affected. Other commonly affected cognitive skills include the ability to pay attention, organize thoughts, plan effective strategies for completing tasks and activities, and/or make sound judgments. More severe changes in cognitive skills may develop years after the traumatic event where the person may appear to have recovered from the previous TBI. �
TBI Diagnosis
Evaluations performed by healthcare professionals to help diagnose traumatic brain injury (TBI) generally include: �
Questions about the traumatic event
Analysis of the person’s level of consciousness and confusion
Neurological tests to analyze memory and thinking, vision, hearing, touch, balance, and reflexes
Let your doctor know if you are taking any drugs and/or medications, especially blood thinners, because they can increase the chance of complications. Also, inform your healthcare professional if you drink alcohol or take illicit drugs. �
Depending on the cause of the TBI and the severity of symptoms, brain imaging with computed tomography (CT) may be necessary to determine if there�s swelling or bleeding in the brain. If you experience a traumatic brain injury, it should be noted in your permanent medical record and mentioned whenever familiarizing a new doctor with your medical history. �
Traumatic Brain Injury Treatment
The most serious traumatic brain injuries commonly require specialized hospital care and can also need several months of rehabilitation. Most traumatic brain injuries are mild and can be treated with either a short hospital stay for observation or at-home monitoring followed by outpatient rehabilitation, if necessary. Treatment of dementia in a person with a history of traumatic brain injuries varies depending on the type of dementia diagnosed. Treatment strategies for Alzheimer’s disease or another type of dementia are ultimately the same for people with and without a history of traumatic brain injury. �
Alzheimer’s disease and other types of dementia which may occur as a long-term result of traumatic brain injury (TBI) are progressive health issues which worsen over time. As with all types of dementia, they can affect a person’s quality of life, shorten lifespan, and complicate the effort to manage other health issues effectively. However, because other types of dementia, such as CTE, are considerably new for researchers and healthcare professionals, clinical guidelines for diagnosis and treatment do not exist. Several research studies are underway to gain further insight into the patterns of TBI and Alzheimer’s disease which may be implicated in CTE and to develop strategies for prevention, diagnosis, and treatment. �
As previously mentioned in the article above, Alzheimer�s disease and other types of dementia which may occur as a long-term result of traumatic brain injury (TBI) are progressive health issues which may ultimately worsen over time. As with all types of dementia, these can affect quality of life, shorten life span, and complicate the effort to manage other health issues effectively. It’s essential for patients and healthcare professionals to diagnose and treat a traumatic brain injury to prevent further health issues in the future, including Alzheimer’s disease and dementia. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
According to research studies, TBI is ultimately associated with Alzheimer�s disease and other types of dementia. Doctors commonly characterize traumatic brain injury as mild, moderate, or severe depending on whether the previous traumatic event causes unconsciousness, how long it lasts, and other well-known symptoms. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Neural Zoomer Plus for Neurological Disease
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention. �
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force.
Traumatic brain injury (TBI) is one of the most common causes of disability and death among the general population, especially in young adults. Additionally, TBI is associated with a variety of neurodegenerative diseases, such as Alzheimer�s disease (AD) and Parkinson�s disease (PD). It is essential for patients and healthcare professionals to understand the pathophysiological mechanisms of traumatic brain injury and neurodegenerative diseases to diagnose factors which may ultimately cause neurodegeneration associated with TBI as well as determine possible treatment approaches. �
Oxidative stress, neuroinflammation, and glutamatergic excitotoxicity have previously been associated with TBI and neurodegenerative diseases. As a matter of fact, oxidative stress is believed to be an essential pathological mechanism which connects TBI to neurodegenerative diseases. Research studies have demonstrated that reactive oxygen species and their subsequent byproducts may play a role as novel fluid markers for the identification and monitoring of cellular damage. These reactive oxygen species can also serve as a suitable treatment approach to ultimately help reduce the risk of neurodegenerative diseases and promote quality of life for people suffering from TBI and other health issues. �
Pathogenesis of TBI and Neurodegenerative Diseases
Several research studies have demonstrated the development of neurodegenerative diseases following TBI. Previous research studies have also shown a three times higher prevalence of PD following TBI. Likewise, the prevalence of AD has also been shown to be higher following TBI. Moreover, traumatic brain injury has been demonstrated to be a risk factor for ALS with several research studies demonstrating an increased risk of neurological diseases in professional Italian soccer players. A case-control research study of ALS patients in the United States also found an increased risk of ALS with repeated TBI. However, it currently appears unlikely that a single occurrence of TBI could considerably affect the risk of ALS. Additionally, chronic traumatic encephalitis (CTE), a tau pathology, has been demonstrated in NFL players and professional athletes which suffer from repeated TBI. Because of the prevalence of neurodegenerative diseases and other health issues appears to increase after TBI, it is relevant to discuss the pathogenesis of TBI and neurodegenerative diseases. �
In several research studies, TBI patients and TBI animal models have been shown to demonstrate characteristic pathological mechanisms in key proteins, indicating the disruption of axonal transport due to axonal injury. The accumulated proteins which result in protein neuropathy include A?, ?-synuclein, and tau protein. These abnormal proteins are specifically interesting because it is well-known that A? protein aggregation is an essential pathological factor of AD, ?-synuclein protein aggregation is an important characteristic of PD, and tau protein aggregation is fundamental in the pathogenesis of CTE and AD. Surprisingly, these protein neuropathological changes occur in all three proteins through oxidative stress-associated free radicals and reactive aldehydes which are commonly increased following TBI. Additionally, the reactive aldehyde byproducts of lipid peroxidation have been demonstrated to result in further lipid peroxidation. Provided that these pathological proteins can also cause the development of free radicals through excitotoxicity or changes in mitochondrial ion balance. Because reactive aldehydes can cause further lipid peroxidation and protein carbonylation, it is possible that oxidative stress also plays a key role in a self-propagating cycle of lipid peroxidation, protein carbonylation, and neurodegenerative protein aggregation. Further research studies are still necessary to determine these outcome measures. �
TBI patients and TBI animal models have also demonstrated behavioral signs and symptoms, such as post-TBI dementia which resembles AD, post-TBI motor deficits which offer evidence of post-TBI brain tissue damage in the region of the hippocampus thus, resembling brain tissue damage in AD, and damage in the basal ganglia thus, resembling the brain tissue damage which occurs in PD. Functional magnetic resonance imaging (fMRI) research studies have also shown transient and persistent neuropathological functional changes in the brain of TBI patients which may contribute to the development of chronic neurodegenerative diseases. These changes observed in post-injury patients suggest that TBI could cause the initial tissue damage which resembles or results in processes in the pathophysiology of neurodegenerative diseases. �
Based on the essential role which oxidative stress plays in post-TBI secondary injury and in the pathophysiology of neurodegenerative diseases, it is possible that oxidative stress is a key process in connecting TBI to the increased prevalence of neurodegenerative diseases. Furthermore, oxidative stress may serve as a therapeutic, diagnostic, or prognostic marker in evaluating the risks of long term neurological diseases following TBI which can help determine a proper treatment approach. �
Treatment of TBI and Neurological Diseases
Considering the considerable risks caused by TBI, it is clear that there is a need for effective methods and techniques for early diagnosis and treatment of TBI patients to ultimately reduce the prevalence of post-TBI neurological sequelae. Currently, the diagnosis of TBI is primarily based on the patient’s provided history and clinical observations. Several clinical systems have been developed for the evaluation of mTBI, which is the most common type of clinical TBI, including the Sports Concussion Assessment Tool and Military Acute Concussion Evaluation. However, these assessments are made to be utilized immediately after injury and, as such, quickly decreasing in sensitivity with delayed evaluation. Moreover, the Glasgow Coma Scale has been utilized for decades and allows for both quick and constant communication of the patient’s condition nevertheless, the currently accepted threshold score of 13 may not be adequate to exclude visible abnormalities on computed tomography imaging which require neurosurgical intervention. Due to these outcome measures in current diagnostic methods and techniques, civilian and military work-groups have recommended the development of fluid or imaging-based biomarkers for the diagnosis of mTBI to ultimately determine the most appropriate treatment approach. �
Several substances and proteins have been suggested to play an essential role as fluid biomarkers, including glial fibrillary acidic protein (GFAP), calcium-binding protein S100B, and tau protein. In most cases, the presence of these biomarkers demonstrates a blood-brain barrier disruption within the central nervous system. These proteins have been demonstrated to be acutely increased following TBI in human participants, however, these currently face challenges of low specificity, poor correlation with the development of post-concussive symptoms, and poor correlation with imaging abnormalities. �
Provided the key role of oxidative stress and neuroinflammation in secondary neuronal injury and neurodegeneration, it is possible that the results of these processes may also serve as suitable biomarkers. As previously mentioned, plasma levels of several oxidative stress and inflammation-associated markers have been demonstrated to be increased in serum up to 42 days following multiple blast injuries and as early as one day following a single injury. Furthermore, lipid peroxidation products, such as acrolein and 4-hydroxynonenal, have also been demonstrated to be associated not only in TBI secondary injury but also in other types of neuronal health issues, such as spinal cord injury and ischemia-reperfusion injury. Provided that these peroxidation products are not only a cause of damage but also able to cause the modification of biomacromolecules where it is possible that measured increases may be able to demonstrate not only present damage but also continued secondary injury. Treatment of oxidative stress could help as a possible prophylactic treatment to decrease the risk of post-TBI neurodegeneration. Direct supplementation with endogenous antioxidants, such as glutathione and superoxide dismutase, has not demonstrated considerable benefits because these do not easily cross the blood-brain barrier. However, the glutathione precursor N-acetylcysteine has demonstrated several acute benefits in both animal and human research studies. Additionally, focusing on substances of the oxidative cascade, such as reactive aldehydes, has been demonstrated as a possible treatment due to the more lengthened half-lives of these substances when compared to ROS. However, despite the lengthened increase of inflammatory and oxidative byproducts, trials of antioxidant therapies have generally favored acute treatment, often within hours of the TBI, suggesting that acute treatment is appropriate. �
Considering the essential role of post-TBI oxidative stress in the development and progression of chronic neurodegenerative diseases, diagnosis and treatment of this process seem to be promising for the management and regulation of neurodegenerative diseases following TBI. Provided their connection to oxidative stress, inflammatory markers, and lipid peroxidation byproducts could serve as surrogate biofluid markers. Finally, antioxidant treatment strategies can help neutralize perpetuation of cellular and molecular damage and decrease risks of long-term neurological sequelae. �
As previously mentioned in the article above, oxidative stress seems to be the key pathological mechanism connecting neuroinflammation and glutamatergic excitotoxicity in both TBI and neurodegenerative diseases. Due to the increased prevalence of TBI and neurodegenerative diseases, the development of new safe and effective, early diagnosis and treatment approaches is fundamental for overall health and wellness. Many healthcare professionals can improve symptoms and health issues associated with TBI and neurodegenerative diseases. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
TBI is associated with a variety of neurodegenerative diseases, such as Alzheimer�s disease (AD) and Parkinson�s disease (PD). It is essential for patients and healthcare professionals to understand the pathophysiological mechanisms of traumatic brain injury and neurodegenerative diseases to diagnose factors which may ultimately cause neurodegeneration associated with TBI as well as determine possible treatment approaches. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Neural Zoomer Plus for Neurological Disease
�
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention. �
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download
* All of the above XYMOGEN policies remain strictly in force.
Traumatic brain injury (TBI) is one of the most common causes of disability and death in people. About 1.6 million individuals suffer traumatic brain injuries in the United States every year. TBI can cause a process of injury which may ultimately cause a variety of neurodegenerative diseases and other health issues. Many of the neurodegenerative diseases following TBI include health issues such as Alzheimer’s disease (AD), Parkinson’s disease (PD), and amyotrophic lateral sclerosis (ALS). �
The mechanisms underlying the pathogenesis which result in these type of neurodegenerative diseases, however, are still completely misunderstood. Where many of the health issues following TBI have a high incidence, there are currently only several treatment approaches which can help prevent the pathological development of chronic neurological diseases. �
An understanding of the mechanisms underlying TBI and neurodegenerative diseases is fundamental to determine the possible connection between these health issues, to allow the safe and effective diagnosis and treatment. In the following article, we discuss the pathological mechanisms of neurodegenerative diseases and how they’re associated with traumatic brain injury (TBI), including Alzheimer’s disease (AD), Parkinson’s disease (PD), and amyotrophic lateral sclerosis (ALS). �
Pathological Mechanisms of Neurodegenerative Diseases
Although many neurological diseases may have different symptoms, AD, PD, and ALS have several common characteristics. Each neurodegenerative disease is caused by genetic risk factors, however, most cases are idiopathic or unknown. The pathological mechanisms of these health issues are ultimately characterized by the degeneration of brain cells or neurons together with several common symptoms. Moreover, abnormal clusters or dysfunction of the substances amyloid-? (A?), ?-synuclein, and superoxide dismutase (SOD1) are generally found in AD, PD. Although the exact pathological mechanisms of neurodegenerative diseases have not been fully determined, it has been suggested that oxidative stress, glutamatergic excitotoxicity, and neuroinflammation play fundamental roles in neurological diseases such as AD, PD, and ALS. �
AD has a tremendous prevalence among older adults which can greatly decrease their rate of survival and their overall quality of life. In 2008, as many as 24 million people worldwide had dementia, where most had AD, a number which is expected to double every 20 years as the population ages. The pathological mechanisms of AD include the presence of neuritic plaques and the loss of cholinergic neurons or brain cells in the human brain, however, the underlying risk factors leading to these events are still unclear. Neurodegeneration in AD is believed to happen due to the accumulation of amyloid ?-peptide (A?) in plaques in the brain tissue however its aggregation and toxicity are still completely misunderstood. �
Research studies have demonstrated that oxidative stress may play a fundamental role in the pathogenesis of AD because of increased neurotoxic markers of lipid peroxidation, such as 4-hydroxynonenal, in human participants, increased brain protein oxidation in AD, increased nuclear DNA oxidation in the brain of AD patients, 30 percent increased activity of the free radical scavenging enzyme SOD-1 in cell lines of AD patients, and considerable evidence that beta amyloid creates free radical peptides. In addition, it has been demonstrated that free radicals and lipid peroxidation caused by A? can ultimately result in neuronal death in AD. In vitro and animal research studies have demonstrated that the antioxidant effect of cannabinoids was able to prevent neurodegeneration in the neurological disease, suggesting the role of oxidative stress in AD. �
Neuroinflammation has also been associated wit A? toxicity which has likewise been connected to oxidative stress by inflammatory cytokine activity. The purpose of inflammation is to restore cellular homeostasis and balance redox equilibrium, however, inflammation changes with co-localized A? deposits, inflammatory-related proteins, and activated microglial cells in AD. Microglia and astroglia recognize misfolded proteins which can trigger an immune response that may be responsible for the progression and severity of the neurodegenerative disease. The microglial cells promote A? clearance and support neuroprotective properties in early stages of AD, but as the health issue progresses, inflammatory cytokines downregulate A? clearance genes and promote A? accumulation, ultimately causing neurodegeneration. Moreover, cytokines can trigger the creation of arachidonic acid which aggravates neurodegeneration by increasing extracellular levels of glutamate, known to cause excitotoxicity in AD as well as causing the creation of superoxide free radicals which are responsible for cellular death. Furthermore, research studies suggest that non-enzymatically glycated tau causes oxidative stress which results in cytokine gene expression and release of A?-peptide in AD, demonstrating pathological mechanisms between cytokines and oxidative stress which causes the progression and severity of AD. In addition, oxidative damage from reactive oxygen species and lipid peroxidation products, such as 4-hydroxy-2-nonenal (HNE), can restrict glutamate transporters, causing a decreased glutamate uptake that is fundamental for neuronal survival, an increased glutamate concentration in the synaptic cleft, and subsequent excitotoxicity which ultimately causes neurodegeneration in AD. �
Neurodegenerative Diseases in Functional Neurology
Chronic traumatic encephalopathy (CTE) is a neurodegenerative disease associated with repeated blunt force impacts to the head with the transfer of acceleration and deceleration forces to the brain or repetitive mild traumatic brain injuries, although the central pathological mechanisms for the development of neurodegeneration in CTE has not been discovered. CTE has been associated with behavioral and personality changes, parkinsonism, and dementia. Research studies demonstrated similarities between CTE and Alzheimer�s disease but these were different in the predominance of tau protein deposition over amyloid. The tau protein deposition in CTE has been previously demonstrated to restrict kinesin-dependent transport of peroxisomes and the loss of peroxisomes makes the cells vulnerable to oxidative stress, ultimately causing neurodegeneration. This tau protein deposition, which occurs in AD, also restricts the transport of amyloid precursor protein (APP) in axons or dendrites, causing its accumulation in the cell body. Along with tau proteins, portions of TDP43, a nuclear RNA/DNA binding protein which controls the transcription of thousands of genes, have been demonstrated in AD, PD, ALS, and CTE, which cause the misfolding of SOD1, affecting the surrounding cells with free-radical damage. The research studies have also demonstrated the purpose of oxidative stress in CTE neurodegeneration and in other neurological diseases. �
Chronic inflammation has also been demonstrated in CTE and AD, which is believed to aggravate neurodegeneration and, as previously mentioned, it is ultimately associated with oxidative stress though inflammatory cytokines. Moreover, it has been demonstrated that after the initial head trauma in CTE, microglia activate and release toxic levels of cytokines and excitotoxins, such as glutamate, where the excitotoxins restrict phosphatases, resulting in hyperphosphorylated tau, neurotubule dysfunction, and neurofibrillary tangle deposition, all of which are fundamental factors of CTE. Research studies have also demonstrated a synergy between proinflammatory cytokines and glutamate receptors which increase reactive oxygen species and worsens neurodegeneration in the injured brain associated with TBI and neurological diseases. �
Parkinson�s disease is the second most prevalent neurodegenerative disease with a prevalence of approximately 0.3 percent of the older adult population. PD is characterized by the development of ?-synuclein rich Lewy bodies and subsequent death of the dopaminergic neurons of the substantia nigra. Several genetic risk factors have also been demonstrated, including mutations to the ubiquitin-proteasome system. Although the pathological mechanisms which trigger dopaminergic degeneration in non-hereditary PD are still unclear, it has been suggested that oxidative modification or carbonylation of the lysine-rich N-terminus and the non-amyloid factor of ?-synuclein may ultimately cause an ?-synuclein aggregation. �
The reactive carbonyls created as secondary products in oxidative stress have been demonstrated to develop lysine adducts and promote ?-synuclein aggregation in vitro. Additionally, animal models of PD utilizing agents, such as 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine, have demonstrated the increased development of superoxide in dopaminergic cells associated with the cortex. Furthermore, mitochondrial localization of ?-synuclein has been demonstrated to promote oxidative stress in vitro. Neuroinflammation is believed to be a partial cause for the oxidative stress in PD with activated microglial cells demonstrated in the substantia nigra and striatum of deceased PD patients. Activated microglia were also demonstrated in rhesus monkeys up to 14 years after model induction. In addition, glutamatergic excitotoxicity is believed to play a fundamental role in PD. Rotigotine, an FDA approved dopamine receptor agonist, has been suggested to improve the efficiency of glutamate transporter 1 (GLT-1) and has been demonstrated to support neuroprotection against glutamatergic excitotoxicity in dopaminergic cell culture as well as a variety of other functions in the human brain in Parkinson’s disease. �
ALS is a fatal neurodegenerative disease characterized by the death of motor neurons in the central nervous system (CNS) and it is the most common motor neuron disease. Approximately 10 percent of all ALS cases have been associated with genetic causes while the majority are idiopathic or of unknown cause. Mutations affecting superoxide dismutase (SOD1) are responsible for almost 20 percent of all familial cases, however, this is responsible for only 2 percent of all overall cases. Despite the characterized mutations, the exact pathological mechanisms of ALS have yet to be fully determined. �
Research studies utilizing SOD1 mutant mouse models have demonstrated the development of SOD1 aggregates. Given the fundamental role of SOD1 in detoxification of superoxide radicals, it has been previously mentioned that loss of function could cause increased cellular exposure to reactive oxygen species, however, this hypothesis has been challenged by outcome measures in the normal development of SOD1 deficient mice in the absence of considerable traumatic injuries. Furthermore, research studies demonstrated that SOD1 mutant animals ultimately demonstrated no considerable improvement in symptomatic progression with knockout or coexpression of wild type SOD1 which suggests that the mutation results not in the loss of function but rather in the gain of toxic properties. Research studies in rats and human patients suggest that, similar to ?-synuclein and A?, SOD1 mutation cause the development of potentially cytotoxic protein aggregates even in patients without SOD1 mutations. Additionally, the catalysis changes achieved by several mutant variants causes decreased astroglial reuptake of glutamate through restriction of GLT-1. Riluzole, an FDA approved treatment for ALS, has been suggested to help improve glutamatergic excitotoxicity with increased glutamate uptake through GLT-1 and blockade of sensitive channels. Oxidative stress is also involved in neuronal death and in the progression of ALS. �
Given its fundamental role in maintaining and regulating damage from neuroinflammation and excitotoxicity, it is possible that oxidative stress also plays a fundamental role in the pathophysiology of AD, PD, and ALS in a similar fashion to TBI. As such, addressing oxidative stress in neurodegeneration could serve as an effective treatment strategy in neuroprotection. �
Conclusion
Despite the prevalence of TBI the significant neurological sequelae associated with such injuries, diagnosis, and treatment of TBI remains greatly misunderstood. In addition, the causing factors connected to TBI and neurodegenerative diseases, such as AD, PD, ALS, and CTE, have not been fully determined. Several processes, including oxidative stress and neuroinflammation, have also been found to be common between secondary TBI and several neurodegenerative diseases. In particular, oxidative stress appears to be the key mechanism connecting neuroinflammation and glutamatergic excitotoxicity in both TBI and neurological diseases. It is possible that the oxidative cascade caused by TBI ultimately causes and results in the characteristic pathologies of neurodegenerative diseases through oxidation or carbonylation of essential proteins. �
Due to the high prevalence of TBI and neurodegenerative diseases, the development of new safe and effective treatment approaches for TBI is fundamental. Given the essential role that oxidative stress plays in connecting secondary injury and neurodegeneration, detection of ROS and key byproducts could serve as a method or technique for the diagnosis and treatment of potential cellular damage. Finally, these reactive species may serve as a viable therapeutic target for reducing long-term neurodegenerative disease risk following TBI, helping to reduce the disability and death as well as improve the quality of life of individuals in the United States that suffer from traumatic brain injury (TBI) and other health issues. �
TBI is among one of the most common causes of disability and death among the general population in the United States. According to a variety of research studies, mild, moderate, and severe traumatic brain injury has been associated with neurodegenerative diseases, such as Alzheimer’s disease and Parkinson’s disease, as well as a variety of other neurodegenerative diseases. It is fundamental to understand the pathophysiological mechanisms of neurodegenerative diseases while further research studies are still required to determine the association between TBI and neurological diseases. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
Traumatic brain injury (TBI) is one of the most common causes of disability and death in people. About 1.6 million individuals suffer traumatic brain injuries in the United States every year. TBI can cause a process of injury which may cause a variety of neurodegenerative diseases and health issues, such as Alzheimer’s disease (AD). The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Neural Zoomer Plus for Neurological Disease
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention. �
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force.
When we look at our patients, we try to figure out what is causing their ailments from living their best lives. Some practitioners would prescribe medications to alleviate pain. While other practitioners will start trying to figure out what is causing the patient to have these ailments. Here at Injury Medical Clinic, we talk to our patients about the importance of functional medicine and how it can benefit them. In this article, we will be discussing Connective Tissue Disorder and how it is linked to wheat-related disorders.
What is Connective Tissue Disorder?
CTD (Connective Tissue Disorder) is an autoimmune disorder that can affect the connective tissues such as the collagen and elastin in our skins. This disease is highly inflammatory and can occur alongside with other autoimmune diseases, and it is common if families have a history of Connective Tissue Disorder.
About 3% of the population has a connective tissue disorder, and it is most likely to occur in women than men. In fact, women who are diagnosed with connective tissue disorder have a ration of 10:1, compared to men.
CTD includes (but is not limited to) the following conditions:
Systemic Lupus Erythematosus (SLE): SLE is a widespread and chronic autoimmune condition, for unknown reasons, can cause the immune system to attack the body�s own tissue and organs, including joints, kidneys, heart, lungs, brain, blood, and skin.
Sjogren�s Syndrome: This autoimmune disease causes white blood cells to attack moisture-producing glands, such as the tear ducts and salivary glands. This can make it very difficult for the body to produce tears and saliva.
Systemic sclerosis (scleroderma): This condition causes the skin and connective tissue to harden and tighten.
Rheumatoid arthritis (RA): RA is a chronic inflammatory condition and an autoimmune disorder that can generally affect the lining of the joints, but mostly in the hands and feet. Rheumatoid arthritis causes painful swelling that can eventually lead to deformity and erosion in the joints and bones.
Polymyositis: This is a persistent inflammatory muscle disease that causes weakness in the skeletal muscles, which can affect your body movement.
Dermatomyositis: This is an uncommon inflammatory disease that is marked by muscle weakness and can cause a distinctive skin rash.
These conditions can group together and can be very hard to diagnose because of the research and many tests that the patient is taking. Surprisingly, the average patient suffers from symptoms for 3.6 years before meeting diagnostic criteria. And the systems alone are difficult to classify, and often mimic or overlap other conditions. Some of the symptoms include hair loss, muscle pain, numbness or tingling, inflammation, low-grade fever, weakness and fatigue, joint pain, sensitive skin, and rashes.
Increased Need For Advanced Testing and Early Diagnosis
Sadly though, patients wait longer when they have these conditions, and it can worsen in the process as it takes years to get diagnosed for CDT. Practitioners can use treatments on their patients, but the medications act as a band-aid to mask the symptoms, but it does not adequately address the root causes of the disease. Sometimes the symptoms can progress faster than the current diagnostic test. So if you want to make sure your patients have any autoimmune diseases, run a diagnostic test on them, so you can detect early stages of the disease and start treating them so it can go away.
Antinuclear antibody (ANA) is used as an initial test that can help evaluate a person for an autoimmune disorder that can affect many tissues and organs throughout the body. It is most often used when practitioners are diagnosing patients for systemic lupus erythematosus.
Surprisingly ENA can be more predictive than ANA. However, patients were followed for 2 years, and about 20% of those patients developed positive ENA.
Vibrant Wellness Wheat Zoomer
In�a�previous article, we talked about gluten sensitivity and introduced the wheat zoomer. What the Vibrant Wheat Zoomer does is that it actually runs a test on your microbiomes to determine if you have a wheat sensitivity or a gluten sensitivity. It can actually detect IgG and IgA antibodies as well as detecting if your body has the celiac disease and intestinal permeability.� It pairs well with the Vibrant Gut Zoomer, and here at Injury Medical, we use the Wheat Zoomer on our patients to inform them about what is causing them to have gut inflammation or even leaky gut.
Celiac Disease and Wheat Allergens
Celiac Disease and Wheat Allergens is an autoimmune disorder in genetically susceptible individuals, and it affects about 1% of the population. In a previous article, we mentioned the hidden problems that gluten does to the body. And surprisingly, any wheat-related disorders can exist on a spectrum, this includes wheat allergy, gluten sensitivity, and wheat sensitivity.
When a person, has the celiac disease, having any traces of wheat can actually upset their intestinal permeability and causing them to have a leaky gut.
The Connection to CTD and Celiac Disease
But how do connective tissue disorder and celiac disease are connected? Well, surprisingly, Rheumatoid arthritis (RA) and celiac disease (CD) share multiple aspects in epidemiology and clinical manifestations. Both disorders have been proven to be influenced by comparable environmental factors and a recent incidental surge of associated antibodies. Even though they have different depositions, both of them are mediated by endogenous enzymes that target different tissues and organs.
Conclusion
However through functional medicine; local chiropractors and health coaches here at Injury Medical Clinic, strive to understand what do our patients need to make their bodies feel better. If we can use functional medicine to prevent leaky gut at the early stages and help our patients with any ailments that they may have, then we can gently push them into the right direction of exercising throughout the week (even if it is about thirty minutes) and eating nutritious, whole, organic foods; as well as, preventing their ailments coming back then their bodies can finally heal.
Traumatic brain injury (TBI) is one of the most common causes of disability and death in people. About 1.6 million individuals suffer traumatic brain injuries in the United States every year. TBI can cause a process of injury which may ultimately cause a variety of neurodegenerative diseases and other health issues. Many of the neurodegenerative diseases following TBI include health issues such as Alzheimer’s disease (AD), Parkinson’s disease (PD), and amyotrophic lateral sclerosis (ALS). �
The mechanisms underlying the pathogenesis which result in these type of neurodegenerative diseases, however, are still completely misunderstood. Where many of the health issues following TBI have a high incidence, there are currently only several treatment approaches which can help prevent the pathological development of chronic neurological diseases. �
A better understanding of the mechanisms underlying TBI and neurodegenerative diseases is ultimately fundamental to determine the possible connection between these health issues to allow safe and effective diagnosis and treatment. In part 1 of the following article, we will discuss the pathological mechanisms of traumatic brain injury (TBI) and how it’s associated with the development of a variety of neurological diseases and other health issues, including Alzheimer’s disease (AD). �
Pathological Mechanisms of Traumatic Brain Injury
In most instances, TBI is caused by a physical blow to the head during traumatic events, such as falls, automobile accidents, or sports-related accidents, although TBI may also be aggravated by exposure to explosive blasts. TBI can be characterized as mild, moderate, or severe according to the symptoms, such as the length of loss of consciousness and post-traumatic amnesia. Mild TBI (mTBI) is prevalent in the majority of cases, however, it may be difficult to diagnose. This difficulty in diagnosis can be a serious concern as a result of severe consequences like instant impact syndrome or other health issues. �
Damage to the nervous tissue can be characterized as the main injury which happens as a direct effect of a physical blow and secondary injury which happens due to pathophysiological processes subsequent to the traumatic event. The injury process occurs from the rapid acceleration-deceleration of the brain which is believed to harm the brain by causing sheer force within tissue resulting in impact and axonal injury with the cranial wall. These injuries can be contralateral or ipsilateral to the physical blow. In more severe instances, the injury may cause intracranial hypertension and intracranial hemorrhage. This increase in pressure not only damages brain tissue but it also causes potential injury and cerebral hypoperfusion. �
Secondary injury in TBI generally happens several days, weeks, and even months following the traumatic circumstance because of the biochemical changes which occur in the nervous tissue. This harm is often mediated by free radicals and reactive oxygen species (ROS) which develop from ischemia-reperfusion damage, glutamatergic excitotoxicity, or neuroinflammation. After the injury, axonal damage from the sheer force of injury can affect membrane balance. Moreover, uptake of calcium through either membrane disruption or activation of the NMDA and the AMPA receptors by glutamate could ultimately cause mitochondrial dysfunction as well as the overproduction of free radicals and the activation of apoptotic caspase signaling. Following inflammatory processes associated with TBI, such as the activation of microglial cells, can cause oxidative stress through the effects of inflammatory cytokines. These radicals can also cause cellular damage through lipid peroxidation and protein modifications which can overwhelm endogenous antioxidant systems. The secondary products of free radical-mediated lipid peroxidation, such as reactive carbonyl species, can also be electrophilic and can further propagate oxidative damage to biomacromolecules, which can be associated with various neurological diseases. �
Clinical and preclinical research studies have demonstrated the presence of oxidative stress and its byproducts following TBI with both serological and histological methods and techniques. In animal research studies, these products have been demonstrated to continue over a recurrent injury and it may increase following a single traumatic event. Spectroscopic evaluations suggest that the endogenous antioxidants glutathione and ascorbic acid may decrease for 3 to 14 days following the injury. Furthermore, the increase of F2-isoprostane, a lipid peroxidation byproduct, was demonstrated in the cerebrospinal fluid of severe TBI patients with increased levels at 1 day following the injury, however, this was primarily an assessment of alternative treatment and didn’t establish a contrast with healthy controls. Lipid peroxidation products like 4-hydroxynoneal were also found to be elevated in the serum of acute TBI patients needing treatment. Although chronic oxidative stress has not currently been detected following single mild injuries in people, it seems possible that oxidative stress and its associated processes may aggravate or prolong post-concussive symptoms. Given the involvement of oxidative stress in excitotoxicity and reperfusion injury, it’s possible that oxidative stress plays a role in cerebral injury after TBI. �
The pathological mechanisms of secondary TBI are particularly interesting due to the ability to prolong cellular injury beyond the initial traumatic event. Some of these characteristic modifications, such as oxidative stress and excitotoxicity, have also been demonstrated in the pathophysiology of neurodegenerative diseases and other health issues which also suggests a possible pathological mechanistic connection between TBI and neurological diseases. Further research studies of the pathological mechanisms in cerebral diseases and TBI may help determine the factors for neurodegenerative diseases. �
Conclusion
Despite the prevalence of TBI the significant neurological sequelae associated with such injuries, diagnosis, and treatment of TBI remains greatly misunderstood. In addition, the causing factors connected to TBI and neurodegenerative diseases, such as AD, PD, ALS, and CTE, have not been fully determined. Several processes, including oxidative stress and neuroinflammation, have also been found to be common between secondary TBI and several neurodegenerative diseases. In particular, oxidative stress appears to be the key mechanism connecting neuroinflammation and glutamatergic excitotoxicity in both TBI and neurological diseases. It is possible that the oxidative cascade caused by TBI ultimately causes and results in the characteristic pathologies of neurodegenerative diseases through oxidation or carbonylation of essential proteins. �
Due to the high prevalence of TBI and neurodegenerative diseases, the development of new safe and effective treatment approaches for TBI is fundamental. Given the essential role that oxidative stress plays in connecting secondary injury and neurodegeneration, detection of ROS and key byproducts could serve as a method or technique for the diagnosis and treatment of potential cellular damage. Finally, these reactive species may serve as a viable therapeutic target for reducing long-term neurodegenerative disease risk following TBI, helping to reduce the disability and death as well as improve the quality of life of individuals in the United States that suffer from traumatic brain injury (TBI) and other health issues. �
Traumatic brain injury is among one of the most prevalent causes of disability and death among the general population in the United States. According to a variety of research studies, mild, moderate, and severe traumatic brain injury has been associated with neurodegenerative diseases, such as Alzheimer’s disease, as well as a variety of other neurological diseases and health issues. It is fundamental to understand the pathophysiological mechanisms of traumatic brain injury while further research studies are still required to determine the association between TBI and neurodegenerative diseases. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
Traumatic brain injury (TBI) is one of the most common causes of disability and death in people. About 1.6 million individuals suffer traumatic brain injuries in the United States every year. TBI can cause a process of injury which may cause a variety of neurodegenerative diseases and health issues, such as Alzheimer’s disease (AD). The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Neural Zoomer Plus for Neurological Disease
� �
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention. �
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force.
Alzheimer�s disease (AD) is one of the most common types of dementia among older adults. Research studies have demonstrated that pathological changes in the human brain, whether directly or indirectly, can ultimately cause loss of synaptic function, mitochondrial damage, microglial cell activation, and neuronal cell death. However, the pathogenesis of AD is not yet fully understood and there is currently no definitive treatment for the neurological disease. Research studies have demonstrated that the activation and priming of microglial cells may contribute to the pathogenesis of AD. �
A proinflammatory status of the central nervous system (CNS) can also cause changes in the function of the microglial cells or microglia. Neuroinflammation is closely associated with the activation of microglia and astrocytes which are connected to a variety of neurological diseases by the synthesis and secretion of inflammatory mediators such as iNOS, ROS, and proinflammatory cytokines. According to research studies, microglial priming is also caused by the inflammation of the CNS. �
Therefore, whether microglial priming is the result or the cause of neuroinflammation is still controversial. Microglial cell activation commonly causes an increase of A? and tau proteins as well as a decrease of neurotrophic factors, ultimately leading to the loss of healthy brain cells or neurons and the development of neuritic plaques and neurofibrillary tangles which are closely associated with AD. With the progression of Alzheimer’s disease, changes from neuronal dysfunctions which may have no obvious symptoms to memory loss and cognitive impairment may become more noticeable. �
Microglial Priming, Neuroinflammation, and AD
Although the accurate and detailed, fundamental role of the microglial cells continues to be discovered and explained, there is a consensus among many researchers that primed microglia are associated with the inflammatory response of the CNS in AD. It has also been determined that neuroinflammation caused by microglial priming is mainly associated with aging, systemic inflammation, gene regulation, and blood-brain barrier impairment. The purpose of the article below is to discuss how microglial priming and neuroinflammation in Alzheimer’s disease can be caused due to a variety of risk factors. �
Aging
Aging is considered to be one of the main risk factors for AD and it is generally followed by chronic, systemic up-regulation of pro-inflammatory factors and a considerable decrease in an anti-inflammatory response. This change from homeostasis to an inflammatory state occurs through age-related elements which cause an imbalance between anti-inflammatory and pro-inflammatory systems. Microglia is primed into an activated state which can increase the consistent neuroinflammation and inflammatory reactivity in the aged human brain. Research studies have demonstrated that microglia in the brain of rodents developed an activated phenotype during aging characterized by the increased expression of CD11b, CD11c, and CD68. �
Systemic Inflammation
Recent research studies have determined that the neuroinflammation from primed microglial cells can also cause the pathogenesis of AD. Continuous activation of microglia can promote the synthesis and secretion of pro-inflammatory cytokines and trigger a pro-inflammatory response, ultimately causing neuronal damage. Neuroinflammation is an early symptom in the progression of AD. The microglia can have a tremendous effect on the inflammation of the human brain. �
The inflammation and health issues of the CNS can be associated with systemic inflammation through molecular pathways. One research study demonstrated that ROS development of primed microglia decreases the levels of intracellular glutathione and increases nitric oxide in NADPH oxidase subunit NOX2. Moreover, researchers demonstrated that these simultaneously occurring processes ultimately cause the development of more neurotoxic peroxynitrite. This is demonstrated in rodents with peripheral LPS or proinflammatory cytokines, such as TNF-?, IL-1?, and IL-6, IL-33. �
The outcome measures of numerous research studies have demonstrated that systemic inflammation can cause microglial activation. The results of the research studies emphasize the variability of the inflammatory response in the human brain associated with AD and the underlying health issues associated with systemic inflammation and neuroinflammation, as shown in Table 1. MAPK (mitogen-activated protein kinase) signaling pathways regulate mechanisms of the eukaryotic cell and microglial MAPK can also cause an inflammatory response to the aged brain with AD. Furthermore, chronic or continuous systemic inflammation causes neuroinflammation, resulting in the onset and accelerating the progression of AD. �
�
Genetic Regulation
In the aging human brain, gene regulation has ultimately been associated with an innate immune response. Recent preclinical, bioinformatics, and genetic data have demonstrated that the activation of the brain immune system is associated with the pathology of AD and causes the pathogenesis of this neurological disease. Genome-wide association studies (GWAS), functional genomics, and even proteomic evaluations of cerebrospinal fluid (CSF) and blood have demonstrated that dysfunctional immune pathways from genic mutation are risk factors in LOAD, which is the vast majority of AD. �
GWAS have become a fundamental tool in the screening of genes as well as demonstrating several new risk genes associated with AD. Apolipoprotein E (APOE) ?4allele is one of the most considerable and well-known risk genes for sporadic AD and this mutation ultimately increases the risk of neurological disease onset by 15 times in homozygous carriers and by three times in heterozygous carriers. Further research studies have demonstrated how microglial cell function can be affected through a variety of rare mutations which have demonstrated to have an increased risk factor of Alzheimer’s disease. �
An extracellular domain mutation of the TREM2 gene has also demonstrated an almost identical extent with APOE?4 in increasing the risk factor of AD. TREM2 is increasingly demonstrated on the surface of microglia and mediates phagocytosis as well as the removal of neuronal debris. Additionally, several other genes, such as PICALM, Bin1, CLU, CR1, MS4A, and CD33 have been demonstrated as risk genes for AD. Most of the risk mutation genes are expressed by microglial cells. �
Blood-Brain Barrier (BBB) Impairment
The blood-brain barrier (BBB) is a specialized barrier commonly developed between the blood and the brain by tight liner sheets consisting of specific endothelial cells and tight junctions or structures which connects a variety of cells together. The CNS is fundamental for the human body, and the BBB is fundamental for the CNS. The BBB and the blood-nerve barrier develop a defense system to control the communications of cells and soluble factors between blood and neural tissue where it plays a considerable role in maintaining and regulating the homeostasis of the CNS and peripheral nervous system. �
With development, continuous inflammation can also cause damage to the BBB. This damage can ultimately cause loss of hypersensitive neurons, neuroinflammatory regions, and focal white matter impairment following the damage. The compromised BBB also allows more leukocytes to enter into the CNS where an immune response can be aggravated by brain microglia under the condition of peripheral inflammation. These processes may ultimately be under the control of chemokine and cytokine signaling which can also have an effect on brain microglial cells as well as other health issues in AD. �
By way of instance, it has been determined that TNF-?, IL-17A, and IL-1? can reduce the tight junctions and eliminate the BBB. Loss of BBB integrity and abnormal expression of tight junctions are associated with neuroinflammation. Several research studies also demonstrated in an animal model of AD that the vulnerability of BBB to inflammation increases. Current evidence has also demonstrated that the BBB integrity is fundamental while further evidence of the BBB may demonstrate a new treatment approach for AD associated with microglial priming as shown in Figure 2 below. �
�
Conclusion
Microglia play a fundamental role in maintaining and regulating the homeostasis of the CNS’s micro-environment. If the balance of the homeostasis of the human brain is interrupted, the microglial cells can be activated to restore the balance in the CNS by defending against the stimulation and protecting the structure and function of the brain. However, chronic and continuous stimulation can trigger microglia into a state known as microglial priming, which is more sensitive to potentially minor stimulation, causing a variety of health issues, such as central sensitization, chronic pain, and fibromyalgia. �
Microglial priming mainly causes the boost of A?, tau protein as well as neuroinflammation and reduces neurotrophic factors which can cause the loss of healthy brain cells or neurons as well as the development of neuritic plaques and neurofibrillary tangles which are associated with Alzheimer’s disease. Although this �double-edged sword� plays a fundamental role, it can increase the progression of abnormal protein development and aggravate neuronal loss and dysfunction. However, research studies have ultimately demonstrated that aging can cause the progression of AD and there’s not much we can do about it. �
Microglial cells play a fundamental role as the protectors of the brain and they ultimately help maintain as well as regulate the homeostasis of the CNS microenvironment. However, continuous stimulation can cause the microglia to trigger and activate at a much stronger state which is known as microglial priming. Once the microglial cells go into protective mode, however, primed microglia can become much more sensitive to even minor stimulation and they have a much stronger possibility of reacting towards normal cells. Microglial priming has been associated with neuroinflammation and Alzheimer’s disease (AD) as well as central sensitization and fibromyalgia. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
AD is one of the most common types of dementia among older adults. However, the pathogenesis of AD is misunderstood and there is no definitive treatment for the neurological disease. Research studies have ultimately demonstrated that the activation and priming of microglial cells may contribute to the pathogenesis of AD. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Neural Zoomer Plus for Neurological Disease
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention. �
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force.
Microglial cells make up about 10 to 15 percent of all the glial cells in the human body, which can be found in the central nervous system (CNS) and play a fundamental role in the human brain. Microglial cells are responsible for maintaining and regulating changes in the physiological and pathological condition of the CNS by changing their morphology, phenotype and function. In an average physiological state, the microglial cells are continuously in charge of controlling their environment. �
However, when the homeostasis of the brain is interrupted, the microglia change into an amoeba-like shape and become a phagocyte where they can actively reveal a variety of antigens. If the homeostasis interruption in the CNS continues, the microglial cells will then trigger at a much stronger state, which is known as microglial priming. Microglia are the “Bruce Banner” of the CNS. However, once they go into protective “Hulk” mode, primed microglia become much more sensitive to stimulation and they have a much stronger possibility of reacting to stimulation, even reacting towards normal cells. �
�
Microglial priming can become a double-edged sword. As a matter of fact, primed microglia are created from different phenotypes of microglia and the phenotypes are context-dependent, which means they are associated to the sequence and duration of their exposure to different varieties of stimulation in a variety of pathologies. In the article below, we will demonstrate the effect of microglial priming on the central nervous system (CNS), especially in neurological diseases. �
Role of Microglial Cells in the CNS
Microglial cells are commonly found in the central nervous system (CNS), where they are considered to be one of the most flexible types of brain cells. Microglial cells are created from precursor cells found within mesoderm bone marrow, or more specifically found in the mesodermal yolk sac, and they are divided in different densities throughout several regions of the brain. As mentioned above, microglia will remain in a dormant state when the homeostasis of the brain remains stable. �
Microglia have a small cell body and morphological branches which extend towards all directions to help maintain and regulate the overall function of the CNS. Changes in their microenvironment can trigger microglia into an “activated� state. Research studies have demonstrated that microglia play a fundamental role in brain development and a variety of functions, including synaptic pruning and clearing out cell debris. Moreover, microglia create an immune surveillance system in the human brain and control fundamental processes associated with a variety of pathologies, including the clearance and uptake of A? and abnormal tau protein as well as the production of neurotrophic factors and neuroinflammatory factors. �
Microglial Priming Overview
Microglial priming activates when continuous interruptions in the brain’s microenvironment trigger a much stronger microglial response compared to an initial interruption which simply triggers microglial activation. Primed microglia in the CNS are also much more sensitive to possibly minor stimulation. This increased response involves microglial proliferation, morphology, physiology, and biochemical markers or phenotype. However, these changes will ultimately promote an increase in cytokines and inflammation mediator production which can have a tremendous impact on synaptic plasticity, neuronic survival, individual cognitive and behavioral function. Below is an overview of the effects of microglial priming in the CNS. �
Mechanisms of Microglial Priming in the CNS
The microenvironment of the central nervous system (CNS), by way of instance, is one of the main factors which can affect the microglial cells. Increased oxidative stress, lipid peroxidation and DNA damage associated with brain aging can all commonly trigger microglial priming. Another common factor for microglial priming includes traumatic brain injury. Research studies have shown that traumatic CNS injury activates microglia as well as the development of primed microglia. �
Many research studies have also shown that both focal and diffuse traumatic brain injury increase inflammation in the brain associated with microglia and astrocytes. CNS infections can also trigger microglial priming where viruses are the main cause of CNS infection. Both DNA and RNA viruses can trigger microglial priming including microglia and astrocytes. Recent research studies have shown that complement dysfunction can change the expression of complement receptors and trigger microglial priming after continuous activation following a variety of functions, including synapse maturation, immune product clearance, hematopoietic stem/progenitor cells (HSPC) mobilization, lipid metabolism, and tissue regeneration. �
Moreover, research studies have shown that there is increased priming of the microglia in a variety of neurological diseases. By way of instance, microglial cells with a morphological phenotype are found in large numbers in the human brain. In the last several years, research studies have suggested that neuroinflammation can continuously activate the microglia and trigger microglial priming. Furthermore, all of the previously mentioned situations are closely associated with neuroinflammation. Research studies have also demonstrated that neuroinflammation, as well as microbial debris and metabolic effects, are associated with central sensitization in neurological diseases, such as fibromyalgia, also referred to as the “brain on fire”. �
In the context of the previous situations mentioned above, microglia are primed though a series of pro-inflammatory stimulation, such as lipopolysaccharide (LPS), pathogenetic proteins (e.g., A?), ?synuclein, human immunodeficiency virus (HIV)-Tat, mutant huntingtin, mutant superoxide dismutase 1 and chromogranin A. There is also a variety of signaling pathways and it is common for different types of cells to express special pattern recognition receptors (PRRs) which can affect inflammatory signaling pathways. By way of instance, several signaling pathways, known as pathogen-associated molecular patterns (PAMPs), which can commonly increase in infected tissue, could also control microbial molecules. �
Additionally, peptides or mislocalized nucleic acids identified as misfolded proteins through a series of pathways, known as danger-associated molecular patterns (DAMPs), can also cause microglial priming. Toll-like receptors (TLRs) and carbohydrate-binding receptors commonly function in these pathways. There are also many different receptors found in microglia, including triggering receptors expressed on myeloid cells (TREM), Fc? receptors (Fc?Rs), CD200 receptor (CD200R), receptor for advanced glycation end products (RAGE), chemokine receptors (CX3CR1, CCR2, CXCR4, CCR5, and CXCR3), which can be recognized and mixed in with other signaling pathways, although some pathways are still not clear. �
Consequences of Microglial Priming in the CNS
Microglia show a low rate of mitosis in their normal state and a high rate of proliferation after microglial priming, showing that the microglia have the ability to affect cell turnover and pro-inflammation stimulation. With continued stimulation, microglia activate from their resting state, changing into amoeboid microglial cells in morphology. However, the changes in the shape of the microglia cannot differentiate the characteristics of microglial activation and the function of primed microglia depends on their phenotypes which are associated with receptors and molecules which they create and recognize. �
The different types of tissue macrophages, under microenvironmental impetus, are able to differentiate M1 and M2 phenotypes. First, M1 polarization, also known as classical activation, ultimately needs interferon-? (IFN-?) to be mixed with TLR4 signaling which then causes the production of inducible nitric oxide synthases (iNOS), reactive oxygen species (ROS), proinflammatory cytokines, and finally, ultimately reduces the release of neurotrophic factors, ultimately causing inflammation with increased markers of main histocompatibility complex II (MHC II), interleukin-1? (IL-1?) and CD68. �
Moreover, M2 polarization, also known as alternative activation, is ultimately believed to be associated with tissue-supportive in the situation of wound healing, reducing inflammation and improving tissue repair of collagen form. They trigger in response to IL-4 and IL-13 in vivo. M2 polarization is characterized by the increased expression of neurotrophic factors, proteases, enzymes arginase 1 (ARG1), IL-10 transforming growth factor-? (TGF-?), scavenger receptor CD206 and coagulation factors as well as improving phagocytic activity. As a matter of fact, there are currently no clear boundaries between the two polarizations and the M1 phenotype shares many similar characteristics with the M2 phenotype. �
Another phenotype of primed microglia, known as acquired deactivation, has been recently discovered. This new phenotype overlaps with M2 and has the ability to improve anti-inflammatory and functional recovery. Additionally, a research study conducted ultra-structural analyses and identified a brand-new phenotype, known as �dark microglia�, which is rarely seen in the microglial cell’s resting state. Systemic inflammation triggers microglia into an activated state to promote cell and tissue recovery and achieve homeostasis. Microglial priming is ultimately the second interruption in the CNS microenvironment. �
The primed microglia is a double-edged sword for brain health. Many research studies in vivo and in vitro have shown that neurological diseases are associated with microglial activation. The inflammatory phenotypes of the microglia create neurotoxic factors, mediators and ROS which can affect the CNS. Primed microglia play a fundamental and beneficial role in neuronal regeneration, repair, and neurogenesis. Primed microglia are also much more sensitive and respond much stronger to brain injury, inflammation, and aging as well as increase the activation of microglial cells by switching from an anti-inflammation, potentially protective phenotype to a pro-inflammation destructive phenotype, as shown in (Figure 1). �
�
In the early stages of microglial priming, the ability and function to phagocytize cell debris, misfolded proteins, and inflammatory medium are increased where more protective molecules, such as IL-4, IL-13, IL-1RA, and scavenging receptors, are created. The changes can affect wound healing and damage tissue repairment, neuron protection, and homeostasis recovery. Classically activated microglia (M1) make up a large proportion of all microglia and promote an increased creation of neurotoxic factors, such as IL-1?, TNF-?, NO and H2O2 (6), where more microglia are primed immediately afterward. �
This increased and extended neuroinflammation caused by primed microglia can ultimately be associated with the development and clustering of the protein tau and A?. Furthermore, it can lead to loss of neurons as well as the decrease of cognitive function and memory, such as in Alzheimer’s disease. Although the mechanisms are not clear enough, people have reached an agreement that primed microglia cause a chronic proinflammatory response and a self-perpetuating cycle of neurotoxicity. And this is believed to be the key factor in brain health issues resulting in neurological diseases. �
Microglia are known as the protectors of the brain and they play a fundamental role in maintaining as well as regulating the homeostasis of the CNS microenvironment. Constant stimulation causes the microglia to trigger at a much stronger state, which is known as microglial priming. Microglial cells are the “Bruce Banner” of the CNS. However, once they go into protective “Hulk” mode, primed microglia become much more sensitive to stimulation and they have a much stronger possibility of reacting to stimulation, even reacting towards normal cells. �- Dr. Alex Jimenez D.C., C.C.S.T. Insight
Microglial cells make up about 10 to 15 percent of all the glial cells in the human body, which can be found in the central nervous system (CNS) and play a fundamental role in the human brain. Microglial cells are responsible for maintaining and regulating changes in the physiological and pathological condition of the CNS. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Neural Zoomer Plus for Neurological Disease
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention. �
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download�
* All of the above XYMOGEN policies remain strictly in force.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine






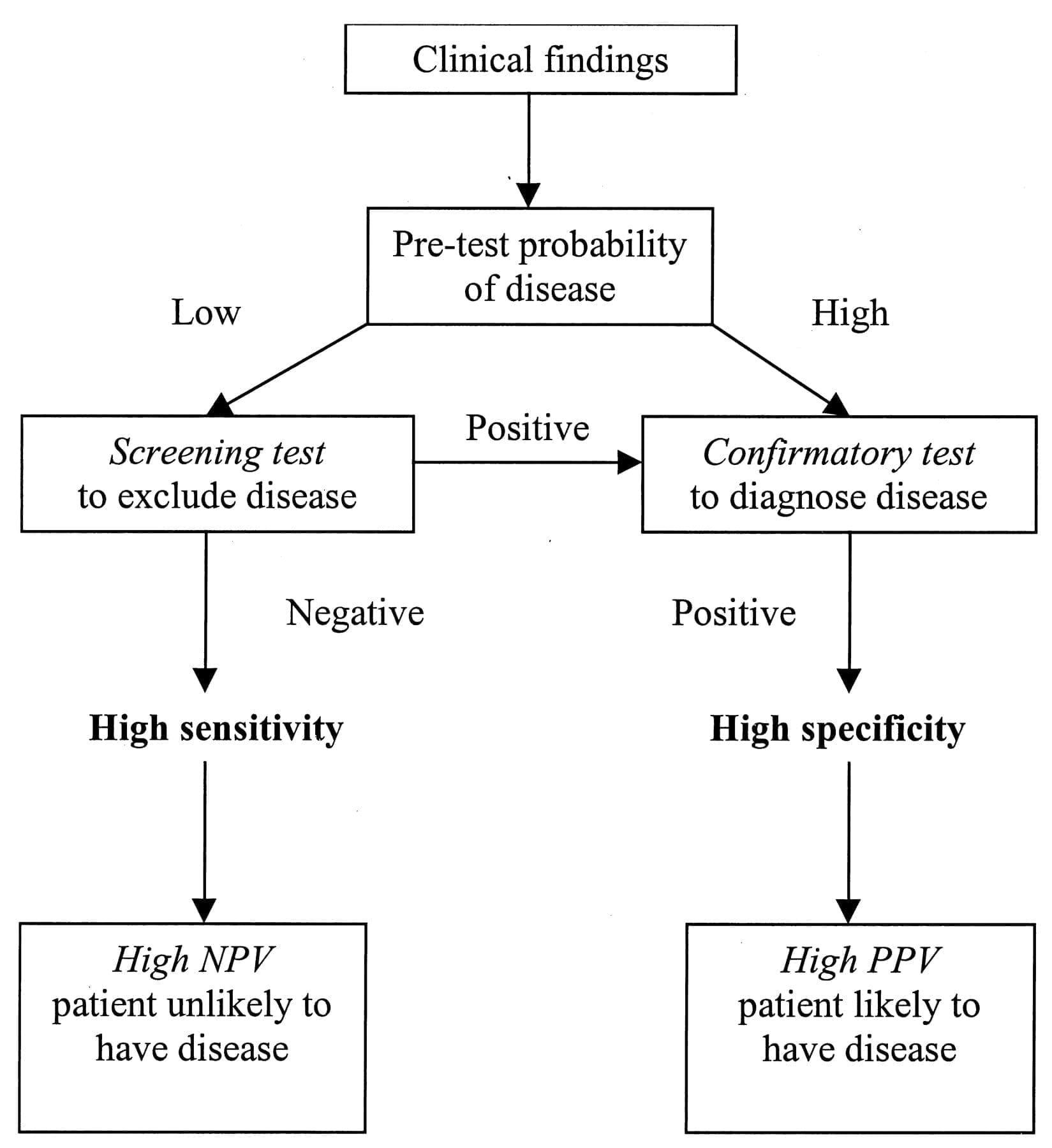

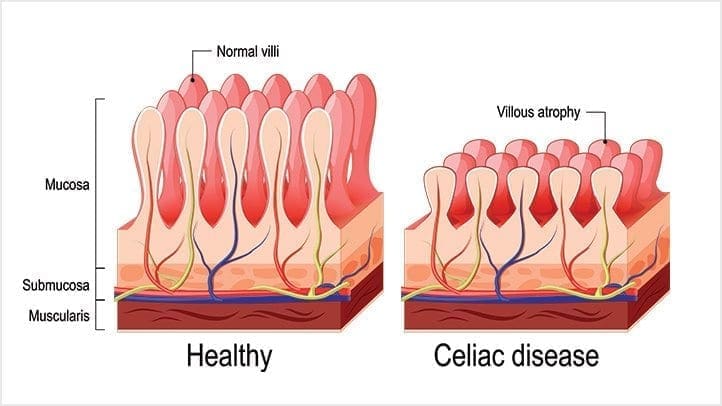

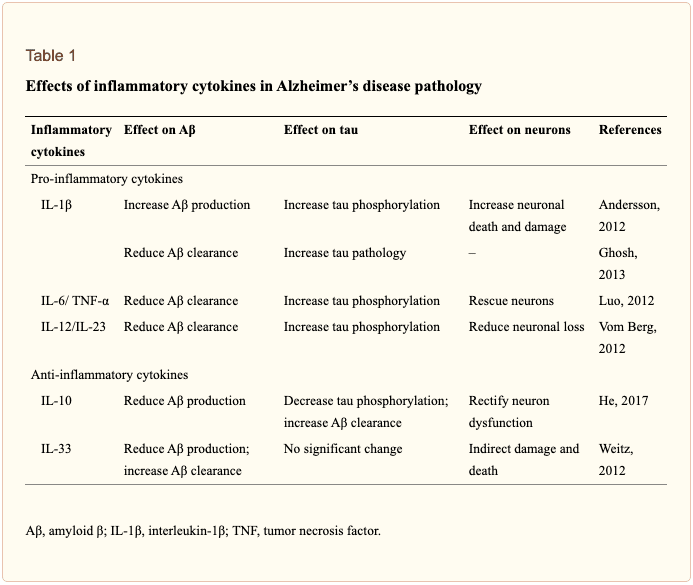 �
�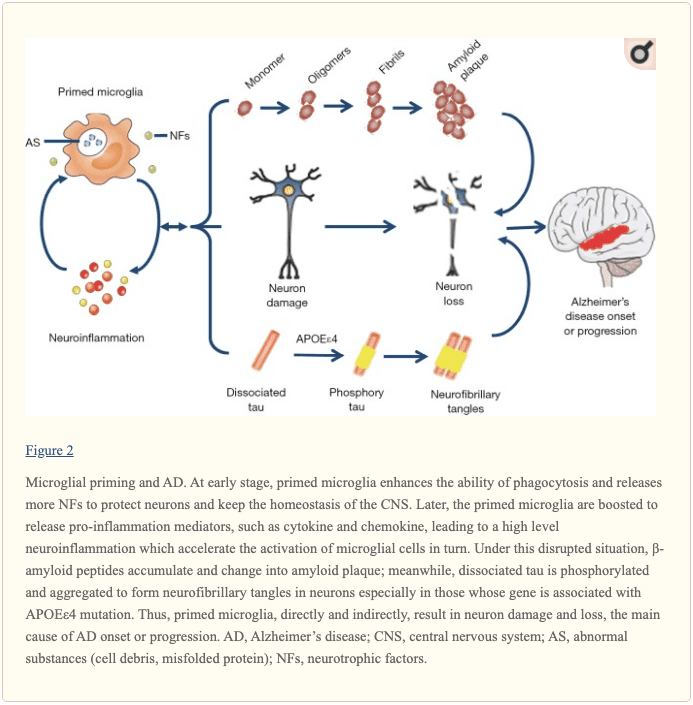 �
�
 �
�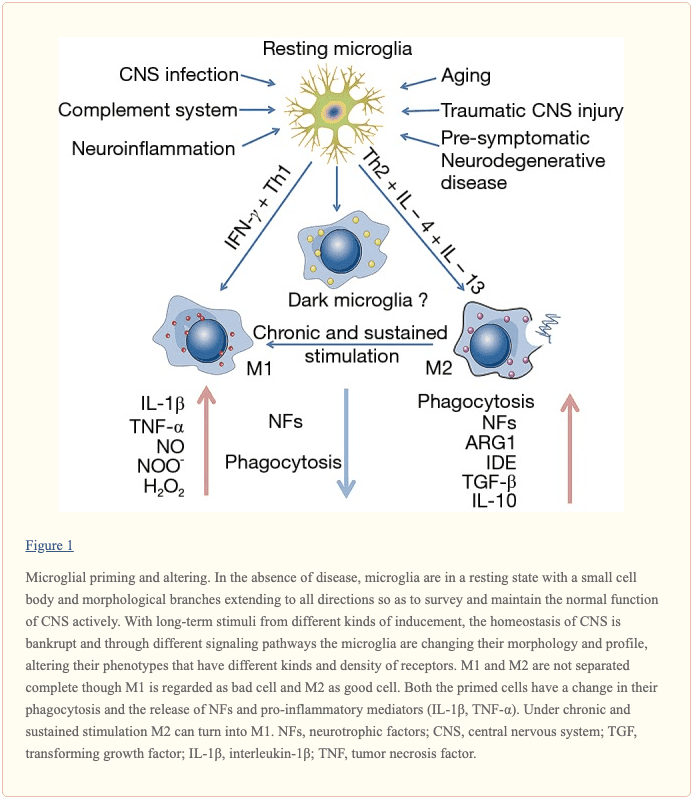 �
�






