What Happens to Your Spine After a Crash, Work Injury, Sports Hit, or Head-First Fall?
The doctor explains to a patient, who may have a head injury from an accident, what happens to the spine after a high-impact collision using a vertebral column model.
Overview: Why high-impact events strain the spine (and sometimes the brain)
When you are involved in a car accident, get hurt at work, collide in sports, or fall and hit your head, your spine absorbs fast, complex forces. These include flexion and extension (bending forward and back), rotation (twisting), lateral bending, and compression (axial loading). Sudden acceleration or deceleration—especially with rotation—can cause joints to move beyond their normal range, resulting in the stretching or tearing of soft tissues. In higher-energy trauma, vertebrae and discs can fail, and the spinal cord can be injured. The result ranges from temporary pain and stiffness to lasting changes in strength, sensation, and autonomic function if the cord is involved (Mayo Clinic, 2024; NINDS, 2025). Mayo Clinic+1
These same rapid movements can also cause brain injury. When the head moves quickly and stops suddenly, the brain can strike the inside of the skull, stretching delicate nerve fibers and triggering a concussion or a more serious traumatic brain injury (TBI). Because the brain and spine share protective bones, connective tissues, cerebrospinal fluid (CSF), and vascular pathways, injury to one often affects the other. Imaging—typically CT for bones and MRI for soft tissues and the spinal cord—helps map what happened, allowing your team to guide safe care (UT Southwestern; Utz et al., 2014). UT Southwestern Medical Center+1
The forces that damage the spine
Hyperextension and hyperflexion: Whipping motions (for example, rear-end collisions) can over-stretch ligaments and joint capsules, irritate facet joints, and provoke muscle spasm—commonly called “whiplash.” In severe cases, hyperextension can fracture the posterior elements of the C2 vertebra (a “hangman’s fracture”) (Torlincasi, 2022). NCBI
Axial compression: A head-first impact loads the spine in a vertical direction. If the neck is slightly flexed, axial compression can cause vertebrae to collapse or a vertebral body to burst. In sports, this mechanism is strongly linked to catastrophic cervical injuries (Boden, 2008). PubMed
Torsion and lateral bending: Twisting and side-bending add shear forces that can tear annular fibers in discs and sprain supporting ligaments.
Deceleration with rotation: High-speed stops—common in crashes—can combine rotation with hyperflexion or extension, increasing the risk of disc herniation, ligament failure, and even vascular injury to the carotid or vertebral arteries (van den Hauwe et al., 2020). NCBI
Common spinal injuries after high-impact events
1) Soft-tissue injuries (strains, sprains, and whiplash)
What happens: Muscles and tendons strain; ligaments sprain. The facet joints can become inflamed; posture and movement patterns change to guard the area.
How it feels: Neck or back pain, stiffness, headaches, limited range of motion, and sometimes dizziness or visual strain.
Why it matters: Even when X-rays are normal, these injuries can disturb joint mechanics and load discs and nerves abnormally, delaying recovery and sometimes causing chronic pain.
2) Disc injuries (bulges and herniations)
What happens: The inner gel of the disc pushes through weakened outer fibers (annulus). A herniation can compress nearby nerves, causing radiating pain, numbness, or weakness.
Symptoms: Sharp neck or back pain accompanied by arm or leg symptoms (radiculopathy). Coughing or sneezing can worsen it.
Evidence Suggests That Disc herniation and nerve irritation are common after rapid flexion-extension and axial loading; severe cases may contribute to cord compression syndromes that require urgent attention (Mayo Clinic, 2024). Mayo Clinic
What happens: Sudden load exceeds bone strength. In the neck, a C2 “hangman’s fracture” is a classic hyperextension injury; other levels can fracture from compression or flexion-distraction.
How it feels: Severe focal pain, limited motion, neurologic changes if nerves are involved.
Evidence: Hangman’s fractures involve bilateral C2 pars/pedicle fractures from extreme hyperextension and deceleration—often diving or motor-vehicle collisions (Torlincasi, 2022). CT rapidly detects fractures; MRI checks ligaments and cord (Utz et al., 2014). NCBI+1
4) Spinal cord injury (SCI)
What happens: The cord, or cauda equina, is damaged by compression, contusion, or transection. Secondary cascades—such as edema, ischemia, and inflammation—can worsen deficits over time.
How it feels: Loss of strength or sensation below the injury, reflex changes, spasticity, balance problems, and bowel/bladder or autonomic dysfunction. Some effects can be permanent (Mayo Clinic, 2024; NINDS, 2025). Mayo Clinic+1
What happens: The carotid or vertebral arteries tear or dissect during high-energy neck trauma, risking delayed stroke.
Why it matters: Complications often occur hours to days after injury. Early identification and timely antithrombotic therapy lower the risk of ischemic events (van den Hauwe et al., 2020). NCBI
Sports, work, and falls: settings that raise risk
Sports: Football, ice hockey, wrestling, diving, skiing/snowboarding, rugby, and cheerleading have the highest risk for catastrophic spinal injuries. Axial loading to the crown of the head with slight neck flexion can cause cervical fracture and quadriplegia in any sport (Boden, 2008). PubMed
Work: Heavy lifting, falls from height, and high-energy impacts around vehicles and machinery threaten the spine.
Falls with head impact: Head-first falls concentrate force into the upper cervical spine and brain, raising the risk of combined neck injury and concussion/TBI (Weill Cornell Medicine Neurosurgery, n.d.; NINDS, 2025). NINDS
The brain–spine connection: why TBIs and spine injuries overlap
Fast acceleration-deceleration events that injure the neck also cause the brain to shake. The brain can bump the skull, causing stretch and shear of axons (diffuse axonal injury). Secondary biochemical cascades—excitotoxicity, oxidative stress, and neuroinflammation—can prolong symptoms such as headaches, dizziness, cognitive impairment, sleep disturbances, and mood changes (Mayo Clinic, 2024; NINDS, 2025). Clinically, many people present with a combined pattern, including neck pain and limited motion, vestibular symptoms, visual strain, and cognitive complaints, all of which occur after the same incident. A coordinated plan that screens for red flags, protects the spine, and addresses vestibular/ocular issues tends to help. Mayo Clinic+1
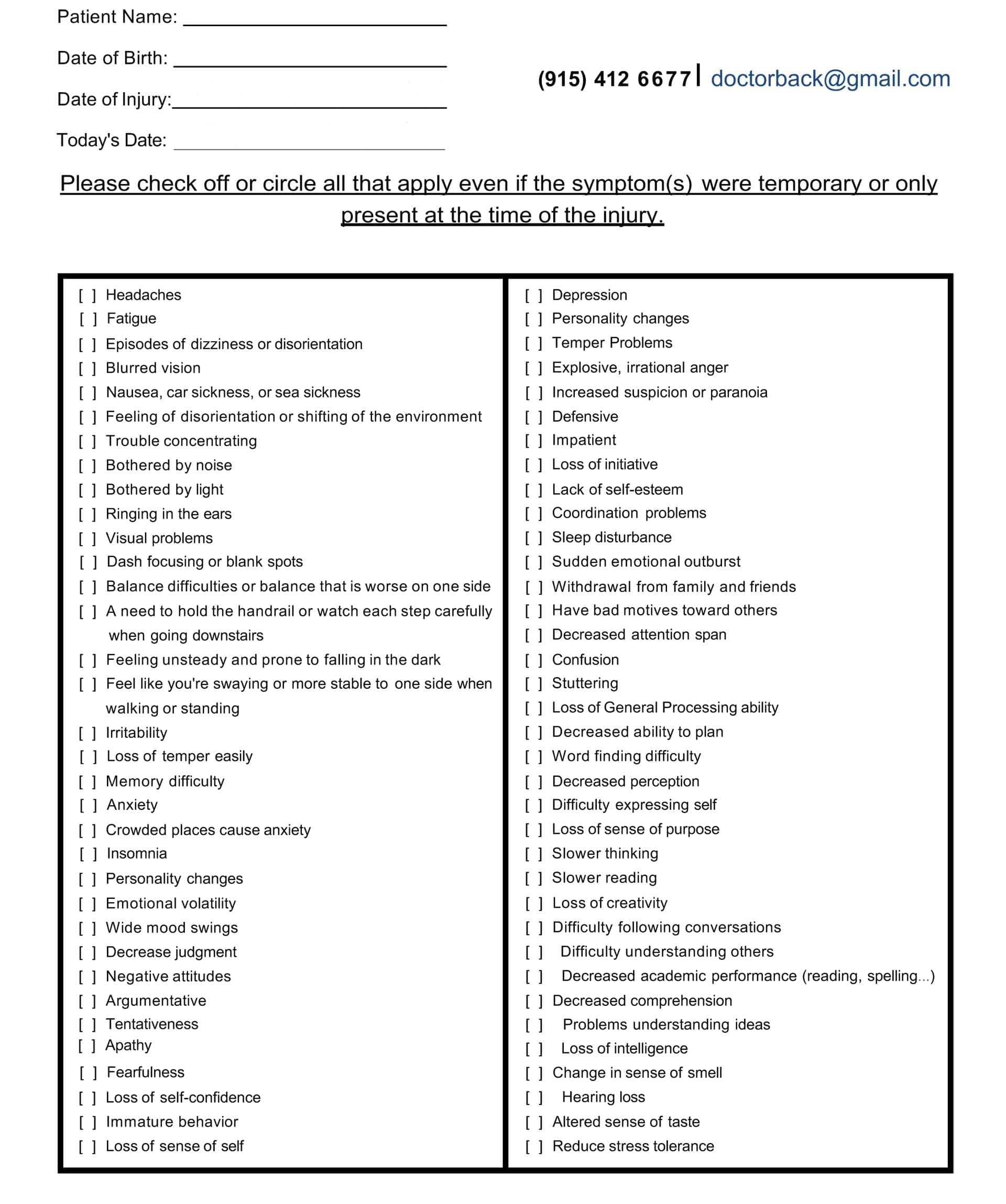
Head Injury/TBI Symptom Questionnaire:
Head Injury/TBI Symptom Questionnaire
How clinicians figure out what’s wrong
History and red-flag screen Loss of consciousness, severe or worsening headache, focal weakness/numbness, gait problems, bowel/bladder changes, saddle anesthesia, midline tenderness, or high-risk mechanism triggers urgent imaging and referral.
Physical and neurological exam Range of motion, palpation, motor/sensory/reflex testing, gait and balance, and provocative maneuvers help localize likely pain generators and nerve involvement.
Imaging strategy
CT quickly detects fractures and acute instability.
MRI is superior for ligaments, discs, cord edema/contusion, and nerve root compression.
Vascular imaging (CTA/MRA) is considered when signs or fracture patterns raise suspicion for BCVI (Utz et al., 2014; van den Hauwe et al., 2020). PubMed+1
Sports and work considerations Return-to-play or return-to-work decisions require symptom-guided progression and objective measures (strength, balance, vestibulo-ocular function, and safe lifting mechanics).
What recovery looks like: evidence-informed options
Acute protection and symptom control: Relative rest from provocative motions, pain-modulating strategies, and careful mobilization as tolerated.
Rehabilitation: A graded plan to restore mobility, strength, coordination, and endurance while protecting healing tissues.
Medication and interventional options: Based on the diagnosis and response, primary care, PM&R, neurology, pain management, or spine surgery may add targeted medications, injections, or consider operative care for unstable injuries or progressive neurological deficits.
Education and pacing: Clear timelines, ergonomic coaching, sleep support, and gradual exposure reduce flare-ups and promote consistent gains.
For moderate-to-severe SCI, long-term rehabilitation focuses on function, adaptive strategies, spasticity management, and prevention of complications; research continues on neuroregeneration and advanced technologies (NINDS, 2025; Mayo Clinic, 2024). NINDS+1
Where integrative chiropractic care fits
Important note: Chiropractic does not treat or reverse spinal cord injury. In an integrative model, chiropractic focuses on the mechanical and neuromusculoskeletal contributors to pain and movement limits, and works alongside medical specialists to co-manage complex cases.
What integrative chiropractic care emphasizes:
Thorough medical screening and referral when needed Chiropractors trained in trauma-informed assessment screen for red flags (neurological deficits, cord compression signs, suspected fracture or BCVI). Concerning findings prompt immediate imaging and referral to emergency, neurology, or spine surgery (UT Southwestern; Utz et al., 2014). UT Southwestern Medical Center+1
Gentle, graded manual care For appropriate cases (after imaging or when clinical decision rules indicate safety), joint mobilization or carefully selected adjustments may reduce painful joint restriction, improve movement, and support posture. Soft-tissue therapy helps calm protective spasm and restore glide.
Sensorimotor retraining Cervical stabilization, scapular control, proprioceptive drills, and graded vestibular/oculomotor exercises can help reduce dizziness, improve gaze stability, and normalize head–neck control patterns that often persist after crashes and sports impacts (UT Southwestern; Dr. Jimenez, 2025). UT Southwestern Medical Center+1
Posture, breathing, and load-management Rib-cage mechanics, diaphragmatic breathing, and dynamic posture training lower strain on the neck and lower back during daily tasks and lifting (Dr. Jimenez, 2025). El Paso, TX Doctor Of Chiropractic
Circulation and CSF considerations (clinical observation) Some integrative chiropractic programs incorporate strategies to optimize cervical mobility and thoracic outlet mechanics as part of a comprehensive plan that supports fluid dynamics and symptom relief. This is a developing area; clinicians should avoid over-promising benefits in serious neurological disease. In Dr. Jimenez’s clinic, CSF flow is considered within a broader framework of posture and movement for symptom-driven care (Jimenez, 2025). El Paso, TX Doctor Of Chiropractic
Whole-person coordination Chiropractors and nurse practitioners (NPs) can coordinate with PM&R, neurology, radiology, physical therapy, and behavioral health to align goals, including restoring motion, quieting pain, normalizing movement patterns, and supporting a return to activity. Dr. Alexander Jimenez, DC, APRN, FNP-BC, documents these collaborative pathways in his clinical articles and patient education resources (Jimenez, 2025). El Paso, TX Doctor Of Chiropractic+2 El Paso, TX Doctor Of Chiropractic+2
Step-by-step recovery roadmap (what a typical plan may include)
Day 0–7: Protect and clarify
Red-flag screen; order imaging when indicated.
Calm pain and inflammation; protect the neck/back from high loads.
Begin gentle motion (as tolerated) to avoid stiffness.
If a concussion/TBI is suspected, initiate a symptom-paced, relative rest plan with light activity and screen time limits; add vestibular/ocular drills as appropriate.
Weeks 2–6: Restore motion and control
Progress manual care (mobilization/adjustment as appropriate).
Sports safety insight: Catastrophic neck injuries often occur with axial loading to the crown in slight neck flexion. Coaching “heads-up” posture and avoiding head-first contact reduces risk (Boden, 2008). PubMed
Special situations that need immediate care
Progressive weakness, numbness, or trouble walking
Bowel or bladder changes; saddle anesthesia
Severe midline spine tenderness after high-risk trauma
Suspected fracture or dislocation
Stroke symptoms after neck trauma (possible BCVI): sudden one-sided weakness, facial droop, vision/language changes, or severe new headache—call emergency services (van den Hauwe et al., 2020). NCBI
Dr. Alexander Jimenez’s clinical observations (El Paso, TX)
Drawing from a dual-scope practice as a Doctor of Chiropractic and Board-Certified Family Nurse Practitioner, Dr. Jimenez highlights:
Early triage matters: identify red flags and co-manage quickly with imaging and specialty referrals when indicated.
Gentle first, then graded: start with low-load mobility and stabilization; add manual care and progressive loading as tissues tolerate.
Sensorimotor work is a staple: vestibular/ocular drills, as well as balance training, help patients with combined neck pain and concussion symptoms move forward.
High-impact events stress the spine through flexion/extension, rotation, and compression—causing soft-tissue injury, disc herniation, fractures, and, in severe cases, spinal cord injury.
The same forces often injure the brain; combined neck and concussion symptoms are common after crashes and sports impacts.
CT and MRI complement each other: CT for bone, MRI for ligaments, discs, cord, and nerves; screen for BCVI when red flags or fracture patterns suggest vascular risk.
Integrative chiropractic care involves a team-based approach, which includes carefully screening patients, using gentle manual methods when appropriate, retraining movement and balance, and collaborating with medical specialists.
With a clear roadmap and coordinated care, most people improve and return to their normal activities. For severe SCI, long-term rehabilitation and assistive strategies remain essential.
Discover how chiropractic care can help alleviate migraines and head injuries for enhanced wellness and pain relief.
Understanding Traumatic Brain Injury: How Head Injuries Cause Headaches, Migraines, and Cognitive Problems
Traumatic brain injury represents one of the most serious health conditions affecting millions of people each year. When someone experiences a blow to the head or a sudden jolt that shakes the brain inside the skull, the resulting damage can create a wide range of symptoms that affect daily life. Understanding how these injuries work and what symptoms they cause helps people recognize when they need medical attention and what treatment options are available.
What Is Traumatic Brain Injury?
Traumatic brain injury, commonly called TBI, occurs when an external force damages the brain. This injury happens when the head receives a sudden impact, causing the brain to move rapidly inside the skull. The Centers for Disease Control and Prevention reports that TBI represents a major cause of death and disability in the United States. These injuries range from mild concussions to severe brain damage that can permanently change a person’s life. mayoclinic+2
The brain sits protected inside the skull, surrounded by cerebrospinal fluid that acts like a cushion. When someone experiences a violent blow to the head, the brain can strike the inside of the skull, causing bruising, torn tissues, bleeding, and other physical damage. Sometimes the injury happens even without the head hitting anything directly—rapid acceleration or deceleration can shake the brain violently enough to cause damage. clevelandclinic+1
TBI occurs through several different mechanisms. Direct impact injuries happen when something strikes the head with force, such as during a fall, a sports collision, or an assault. Penetrating injuries occur when an object breaks through the skull and enters the brain tissue. Blast injuries, common in military settings, create pressure waves that damage brain structures. Motor vehicle accidents represent one of the leading causes of traumatic brain injury, often combining multiple injury mechanisms including impact, acceleration, and deceleration forces. americanbrainfoundation+2
Medical professionals classify TBI into three severity levels based on symptoms and diagnostic findings. Mild TBI, also known as a concussion, represents the most common form and may cause temporary confusion, headache, and other symptoms that typically resolve within weeks. Moderate TBI involves loss of consciousness lasting from several minutes to hours and confusion that can persist for days or weeks. Severe TBI results from crushing blows or penetrating injuries that cause extended unconsciousness, significant brain damage, and potentially permanent disability. mayoclinic+1
The immediate effects of TBI depend on which parts of the brain sustained damage and how severe that damage was. The frontal lobes, which control thinking, planning, and emotional regulation, are often affected by injury in TBI. Damage to the temporal lobes can affect memory and language. The brainstem, which controls basic life functions like breathing and heart rate, can be injured in severe TBI, creating life-threatening emergencies. alz+1
How TBI Causes Headaches and Migraines
Headaches represent one of the most common and persistent symptoms following traumatic brain injury. Research shows that between 30% and 90% of people who experience TBI develop headaches afterward. These post-traumatic headaches can begin immediately after the injury or develop days or even weeks later. Understanding why TBI causes headaches requires looking at the complex changes happening inside the brain and surrounding structures after injury. connectivity+3
When the brain experiences trauma, several physical and chemical changes occur that trigger headache pain. The initial impact can damage blood vessels in the brain, causing bleeding and inflammation. This inflammation triggers the release of pain-causing chemicals that activate nerve endings throughout the head and neck region. The meninges, the protective membranes that cover the brain, contain numerous pain-sensitive nerve fibers that respond to inflammation by sending pain signals. pmc.ncbi.nlm.nih+2
Brain tissue itself does not contain pain receptors, but the structures surrounding the brain are highly sensitive to pain. The blood vessels, meninges, and cranial nerves all possess pain receptors that can generate headache sensations. After a TBI, these structures may become more sensitive, a condition known as central sensitization, where the nervous system becomes hyperresponsive to pain signals. ncbi.nlm.nih+1
The connection between TBI and headaches also involves disruption of normal brain chemistry. The brain relies on neurotransmitters—chemical messengers that allow nerve cells to communicate—to function properly. Traumatic injury can disturb the balance of these neurotransmitters, particularly serotonin, which plays a crucial role in pain regulation. When serotonin levels drop or become imbalanced, the brain’s pain-filtering systems may not work correctly, allowing pain signals to reach consciousness more easily. migrainedisorders+2
Migraines represent a specific type of severe headache that many people develop after experiencing TBI. Research published in scientific journals demonstrates that people who have had a traumatic brain injury face a significantly increased risk of developing migraines compared to those who have never experienced head trauma. One study found that TBI approximately doubles the risk of developing new migraine headaches. pmc.ncbi.nlm.nih
The mechanisms linking TBI to migraines involve complex changes in brain function. The trigeminal nerve, which provides sensation to much of the face and head, becomes activated during migraines. This activation releases inflammatory substances called neuropeptides that cause blood vessel dilation and further inflammation. After TBI, the trigeminal nerve system may become more easily triggered, lowering the threshold for migraine attacks. emedicine.medscape+2
Brain imaging studies reveal that inflammation and altered connectivity between different brain regions persist long after the initial injury. These changes in how different parts of the brain communicate with each other can make the brain more susceptible to migraine triggers. The brain regions involved in pain processing, sensory filtering, and stress response show altered function in people with post-traumatic migraines. sciencedirect
Clinical Insights from Dr. Alexander Jimenez on Head Injury Assessment
Dr. Alexander Jimenez, a dual-credentialed chiropractor and nurse practitioner practicing in El Paso, brings a unique perspective to evaluating and treating patients with traumatic brain injury and post-traumatic headaches. His clinic specializes in treating injuries from various sources, including workplace accidents, sports injuries, personal injuries, and motor vehicle accidents. The dual-scope approach allows for a comprehensive assessment that combines chiropractic evaluation of neuromusculoskeletal function with advanced medical diagnostic capabilities. advantagehcs
When patients present with head injuries, Dr. Jimenez’s clinical approach emphasizes thorough neurological examination to identify the full extent of injury. This assessment includes evaluating cranial nerve function, testing reflexes, assessing balance and coordination, and screening for cognitive changes. The clinic utilizes advanced neuromusculoskeletal imaging to visualize structural damage that may contribute to ongoing symptoms. These imaging techniques include computed tomography (CT) scans, which excel at detecting skull fractures, bleeding, and swelling in the acute phase after injury. Magnetic resonance imaging (MRI) provides superior detail of soft tissue damage, including subtle brain injuries that may not appear on CT scans. pmc.ncbi.nlm.nih+4
Dr. Jimenez emphasizes that proper documentation of injuries plays a critical role, particularly in cases involving motor vehicle accidents or workplace injuries where legal and insurance considerations arise. Detailed medical records, which document the mechanism of injury, initial symptoms, physical examination findings, diagnostic test results, and treatment plans, serve essential functions in both patient care and legal proceedings. These records establish the connection between the traumatic event and the patient’s symptoms, which becomes crucial when seeking compensation for injuries. njadvocates+3
Cognitive Function Changes After TBI
The brain serves as the central control center for all mental processes, including thinking, learning, remembering, and decision-making. When traumatic injury damages brain tissue, these cognitive functions often become impaired. Understanding how TBI affects cognitive function helps patients and families recognize symptoms and seek appropriate treatment. pubmed.ncbi.nlm.nih+1
Cognitive impairment represents one of the most challenging consequences of traumatic brain injury because it affects so many aspects of daily life. The severity and pattern of cognitive problems depend on which brain regions sustained damage and how extensive that damage was. Research involving thousands of patients shows that cognitive impairment occurs across all severity levels of TBI, though more severe injuries generally produce more pronounced deficits. jamanetwork+1
Memory problems rank among the most common cognitive complaints after TBI. Short-term memory, which involves holding information in mind for brief periods, often becomes impaired. People may struggle to remember conversations, appointments, or where they placed items. Long-term memory, particularly the formation of new memories, can also be disrupted. The hippocampus, a brain structure critical for memory formation, is particularly vulnerable to injury during trauma. headway+1
Attention and concentration difficulties create significant challenges for people recovering from TBI. The ability to focus on tasks, filter out distractions, and shift attention between different activities may be compromised. These problems make it difficult to perform work duties, follow conversations, or engage in activities that require sustained mental effort. Divided attention—the ability to manage multiple tasks simultaneously—becomes especially problematic. uwmsktc.washington+1
Processing speed, which refers to how quickly the brain can take in information, understand it, and respond, typically slows after TBI. This slowing affects many aspects of functioning, from reading comprehension to reaction times while driving. Simple tasks that once seemed automatic may now require conscious effort and extra time. jamanetwork
Executive functions encompass higher-level cognitive abilities, including planning, organizing, problem-solving, and self-monitoring. The frontal lobes, which control these functions, are often damaged in TBI. Impairment of executive functions can make it difficult to manage daily responsibilities, make appropriate decisions, or adapt to changing situations. People may struggle with initiating tasks, following multi-step instructions, or recognizing and correcting errors. alz+1
Language and communication abilities can be affected by TBI, although the specific deficits vary depending on the location of the injury. Some people struggle to find the right words, form sentences, or comprehend complex language. Others may struggle with the social aspects of communication, such as interpreting social cues, taking turns in conversation, or adapting their communication style to different situations. uwmsktc.washington+1
Head Symptoms Associated with Cognitive Impairment
The cognitive changes that occur after TBI often coincide with physical symptoms affecting the head. These symptoms interconnect in ways that compound difficulties and interfere with recovery. Headaches themselves can worsen cognitive function by creating pain that distracts from mental tasks and disrupts concentration. The constant presence of head pain makes it harder to think clearly, remember information, or engage in problem-solving. pmc.ncbi.nlm.nih+2
Mental fog or clouded thinking represents a common complaint among people with TBI. This sensation of thinking through a haze makes mental tasks feel effortful and exhausting. The brain appears to operate more slowly, and thoughts may feel disorganized or disjointed. This mental fog often accompanies headaches and worsens with mental exertion. concussionalliance+1
Dizziness and balance problems frequently occur after TBI, creating a sense of instability or spinning that originates from dysfunction in the vestibular system. The inner ear structures that control balance can be damaged during head trauma, or the brain regions that process balance information may become impaired. These balance problems affect the ability to walk steadily, drive safely, or perform activities requiring coordination. mentalhealth.va+2
Pressure sensations inside the head trouble many people with TBI. This feeling of tightness, fullness, or pressure can be localized to specific areas or felt throughout the entire head. Sometimes, this pressure sensation accompanies actual changes in intracranial pressure due to swelling or fluid accumulation; however, it often represents altered sensory processing rather than true pressure changes. connectivity
Facial pain and jaw discomfort can develop after head trauma, particularly when the temporomandibular joint (TMJ) sustains injury during the trauma. The TMJ connects the jawbone to the skull, allowing for chewing and speaking. Injury to this joint or the surrounding muscles can create pain that radiates throughout the face, head, and neck. elizabethsandelmd+1
Types of Headaches Following Traumatic Brain Injury
Post-traumatic headaches can take several different forms, each with distinct characteristics and mechanisms. Recognizing the type of headache helps guide the development of appropriate treatment strategies. The International Classification of Headache Disorders provides standardized criteria for diagnosing different headache types, which healthcare providers use to categorize post-traumatic headaches. nature+2
Acute Post-Traumatic Headache
Acute post-traumatic headache develops within seven days of the injury or within seven days of regaining consciousness after the injury. These headaches typically resolve within three months of their onset. The pain may feel dull and constant or sharp and intermittent, depending on the underlying cause. Acute post-traumatic headaches often accompany other symptoms such as nausea, dizziness, sensitivity to light and sound, and cognitive difficulties. ncbi.nlm.nih+1
Persistent Post-Traumatic Headache
When headaches continue beyond three months after the traumatic injury, they are classified as persistent or chronic post-traumatic headaches. Research indicates that approximately 20% to 50% of people who develop headaches after TBI continue experiencing them long-term. These persistent headaches can last for months or even years after the initial injury. The chronic nature of these headaches has a significant impact on quality of life, interfering with work, relationships, and daily activities.ichd-3+3
Persistent post-traumatic headaches can evolve over time, changing in frequency, intensity, or character. Some people experience daily headaches, while others have episodic attacks separated by pain-free periods. The unpredictability of these headaches creates additional stress and anxiety, which can further worsen the headache pattern. pmc.ncbi.nlm.nih+1
Migraine-Type Post-Traumatic Headaches
Many post-traumatic headaches display characteristics typical of migraines. These headaches involve moderate to severe throbbing or pulsating pain, usually affecting one side of the head. The pain intensifies with physical activity such as walking or climbing stairs. Nausea and vomiting commonly accompany migraine-type headaches. Sensitivity to light (photophobia) and sound (phonophobia) makes it difficult to tolerate normal environmental stimuli. neurology+3
Migraine headaches can include an aura phase, which involves temporary neurological symptoms that typically develop before the headache pain begins. Visual auras are most common and may include seeing flashing lights, zigzag lines, or temporary blind spots. Some people experience sensory auras characterized by tingling or numbness, typically affecting one side of the body. Language disturbances or difficulty speaking can occur during the aura phase. mayoclinic+1
The relationship between TBI and migraines extends beyond the immediate post-injury period. People who experience migraines after TBI often develop chronic migraine disorder, defined as having headache on 15 or more days per month, with at least eight days meeting migraine criteria. This chronic pattern significantly disrupts functioning and requires comprehensive management strategies. pmc.ncbi.nlm.nih
Tension-Type Headaches After TBI
Tension-type headaches represent another common pattern of post-traumatic headache. These headaches create a sensation of pressure or tightness, often described as feeling like a tight band around the head. The pain is typically mild to moderate in intensity and affects both sides of the head. Unlike migraines, tension-type headaches usually do not cause nausea or vomiting and do not worsen significantly with routine physical activity. americanmigrainefoundation+3
Muscle tension in the head, neck, and shoulder regions contributes to tension-type headaches. After TBI, muscle tightness often increases due to several factors, including pain, altered posture, stress, and direct muscle injury during the trauma. This muscle tension creates sustained contraction that generates pain signals and reduces blood flow to affected tissues. physio-pedia+3
The psychological stress associated with recovering from TBI can trigger or worsen tension-type headaches. Anxiety about symptoms, worry about returning to normal activities, and frustration with ongoing limitations create emotional tension that manifests as physical muscle tightness. Sleep disturbances, common after TBI, also contribute to tension-type headaches by preventing adequate rest and recovery. aafp+1
Cervicogenic Headaches
Cervicogenic headaches originate from problems in the neck (cervical spine) but are experienced as headaches in the head. These headaches are particularly common after motor vehicle accidents and other traumas that create whiplash-type injuries to the neck. The sudden acceleration-deceleration forces during these injuries can damage the joints, ligaments, muscles, and nerves of the cervical spine. pmc.ncbi.nlm.nih+3
Cervicogenic headaches typically affect one side of the head and may be accompanied by neck pain and stiffness. The pain often starts at the base of the skull and radiates forward toward the forehead, temple, or area around the eye. Certain neck movements or sustained neck positions can trigger or worsen these headaches. Pressing on specific tender points in the neck may reproduce the headache pain, helping healthcare providers identify cervicogenic headaches. clevelandclinic+1
The upper cervical spine, particularly the C1-C3 vertebrae and their associated nerves, plays a crucial role in cervicogenic headaches. These upper cervical nerves share connections with the trigeminal nerve, which provides sensation to much of the head and face. When injury or dysfunction affects the upper cervical spine, pain signals can be referred along these nerve connections, creating headache sensations. physio-pedia
Dr. Jimenez’s clinic places particular emphasis on evaluating cervical spine involvement in patients presenting with post-traumatic headaches. The dual chiropractic and medical training allows for comprehensive assessment of both spinal mechanics and neurological function. This evaluation includes examining neck range of motion, palpating for areas of tenderness or restriction, testing nerve function, and reviewing imaging studies to identify structural problems. pubmed.ncbi.nlm.nih+3
Cluster Headaches and Trigeminal Autonomic Cephalalgias
Though less common than other headache types, cluster headaches and related conditions can occasionally develop after traumatic brain injury. Cluster headaches create severe, excruciating pain localized around one eye or on one side of the head. The pain reaches maximum intensity quickly and typically lasts 15 minutes to three hours. During attacks, people often feel restless and agitated rather than still, which distinguishes cluster headaches from migraines. pmc.ncbi.nlm.nih+2
Cluster headaches earn their name because they occur in clusters or cycles, with multiple attacks happening daily for weeks or months, followed by periods of remission. The attacks often occur at the same time each day and may wake people from sleep. Autonomic symptoms accompany the pain, including tearing, redness of the eye, nasal congestion or runny nose, eyelid drooping, and sweating on the affected side of the face. practicalneurology+2
The trigeminal autonomic reflex pathway, which connects the trigeminal nerve with autonomic nerve centers in the brainstem, becomes activated during these headaches. This activation causes autonomic symptoms, such as tearing and nasal congestion. Head trauma can potentially damage or alter the function of these neural pathways, though the exact mechanisms linking TBI to cluster headaches require further research. pmc.ncbi.nlm.nih
Sensory Dysfunction and Associated Head and Neck Symptoms
Traumatic brain injury often damages the sensory systems that allow people to perceive and interpret information from their environment. These sensory problems create significant challenges and often contribute to headaches and other symptoms affecting the head and neck region. Understanding these sensory changes helps explain why people with TBI experience such complex and varied symptoms. tbi.vcu+2
Light Sensitivity (Photophobia)
Sensitivity to light represents one of the most common and distressing sensory problems after TBI. Research indicates that between 40% and 80% of people with traumatic brain injury develop photophobia. This heightened sensitivity makes normal lighting levels feel uncomfortably bright or even painful. Indoor lighting, computer screens, and especially sunlight can trigger discomfort, eye pain, squinting, and worsening of headaches. connectivity+1
The mechanisms underlying photophobia after TBI involve several interconnected systems. The visual pathways that transmit light information from the eyes to the brain can become hypersensitive after injury. The trigeminal nerve, which provides sensation to the eyes and face, becomes more reactive to light stimulation. This nerve connects directly to pain-processing regions in the brain, explaining why bright light can trigger or worsen headaches. theraspecs+1
Brain regions involved in processing visual information and filtering sensory input may function abnormally after TBI. The brain normally filters out irrelevant sensory information, allowing people to focus on important stimuli while ignoring background noise or changes in lighting. After traumatic injury, this filtering system may malfunction, causing the brain to become overwhelmed by sensory input that would normally be manageable. connectivity+1
Photophobia significantly impacts daily functioning. Many people need to wear sunglasses even indoors, avoid bright environments, and limit screen time. These restrictions can interfere with work, social activities, and leisure pursuits. The constant need to manage light exposure can create additional stress and contribute to social isolation. theraspecs+1
Sound Sensitivity (Phonophobia)
Increased sensitivity to sound, called phonophobia or hyperacusis, commonly occurs alongside light sensitivity after TBI. Everyday sounds such as traffic noise, conversations, music, or household appliances may seem unbearably loud. This heightened sensitivity can trigger headaches, increase stress, and make it difficult to concentrate. mindeye+1
The auditory system processes sound through complex pathways that involve the inner ear, the auditory nerve, and multiple brain regions. After TBI, any component of this system may become damaged or dysfunctional. The cochlea in the inner ear can be injured by traumatic forces, resulting in hearing loss or tinnitus. The auditory nerve pathways may be stretched or damaged, which can alter how sound signals are transmitted to the brain. tbi.vcu
Central auditory processing, which involves how the brain interprets and makes sense of sounds, often becomes impaired after TBI. People may have difficulty distinguishing speech from background noise, determining the direction of sounds, or processing rapid sequences of auditory information. These processing problems make noisy environments particularly challenging and exhausting. tbi.vcu+1
The brain regions that regulate sensory gating—the ability to filter out unimportant sounds—may not function normally after TBI. This filtering failure means that all sounds reach consciousness with similar intensity, creating a sense of being bombarded by noise. The constant sensory overload contributes to mental fatigue, stress, and headaches. mindeye+1
Visual Disturbances
Visual problems affect approximately 40% to 50% of people with traumatic brain injury. These problems range from difficulty focusing to double vision, blurred vision, and loss of visual field. The visual system relies on precise coordination between the eyes, the muscles that move them, and the brain regions that process visual information. Trauma can disrupt any part of this complex system. salusuhealth+1
Eye movement problems create particular difficulties after TBI. The cranial nerves that control the muscles of the eye may be damaged, causing weakness or incoordination of eye movements. This can result in double vision (diplopia), where the two eyes do not align properly, creating separate images. Reading becomes exhausting because the eyes struggle to track smoothly across lines of text. frontiersin+2
Visual processing deficits affect how the brain interprets visual information, even when the eyes themselves function normally. People may experience difficulty with depth perception, making it challenging to judge distances or navigate stairs. Visual memory problems can make it hard to recognize faces or remember visual information. Visual attention deficits affect the ability to scan the environment effectively and notice important visual details. salusuhealth+1
The connection between vision and balance becomes apparent when visual problems contribute to dizziness and instability. The brain relies on visual information to maintain balance and orient the body in space. When visual input becomes distorted or unreliable after TBI, balance systems struggle to compensate, creating feelings of unsteadiness. frontiersin
Balance and Vestibular Dysfunction
The vestibular system, located in the inner ear, detects head movements and helps maintain balance and spatial orientation. This system can be damaged during head trauma, creating persistent dizziness, vertigo, and balance problems. Vestibular dysfunction affects approximately 30% to 65% of people with TBI. pmc.ncbi.nlm.nih+2
Vertigo, the sensation that the environment is spinning or moving when it is actually still, creates significant distress and disability. This spinning sensation can be constant or triggered by specific head movements. Benign paroxysmal positional vertigo (BPPV), which occurs when calcium crystals in the inner ear become displaced, commonly develops after head trauma. pmc.ncbi.nlm.nih
Balance problems make it difficult to walk steadily, especially on uneven surfaces or in low-light conditions when visual cues are limited. The brain normally integrates information from the vestibular system, vision, and sensors in muscles and joints to maintain balance. When one of these systems becomes impaired after TBI, the brain struggles to compensate, creating unsteadiness and increasing fall risk. frontiersin
Post-traumatic dizziness often worsens with head movements, busy visual environments, and cognitive demands. This dizziness can trigger or worsen headaches, creating a cycle where headache and dizziness reinforce each other. The constant sense of imbalance creates anxiety and limits activities, contributing to deconditioning and further functional decline. pmc.ncbi.nlm.nih+1
Altered Sensation in the Head and Neck
Changes in sensation throughout the head and neck region are commonly experienced following a TBI. These changes can include numbness, tingling, burning sensations, or areas of increased sensitivity. The cranial nerves, which provide sensation to the face, scalp, and neck, may be damaged during trauma. matrixneurological+1
The trigeminal nerve, the largest cranial nerve, supplies sensation to most of the face and head. This nerve has three main branches that provide feeling to the forehead and eyes, the cheeks and nose, and the jaw and chin. Injury to any branch of the trigeminal nerve can create altered sensation in the corresponding region. pmc.ncbi.nlm.nih
The occipital nerves, which emerge from the upper cervical spine and travel up the back of the head to the scalp, often become irritated or compressed after neck injuries. This creates pain, numbness, or tingling in the back of the head and sometimes radiates over the top of the head toward the forehead. Occipital neuralgia, inflammation or injury to these nerves, causes sharp, shooting, electric-shock-like pains in the distribution of the nerve. physio-pedia
Neck pain and stiffness frequently accompany head symptoms after TBI, particularly when cervical spine injury occurred during the trauma. The neck muscles may go into spasm as a protective response to injury, creating sustained tension that contributes to both neck pain and headaches. Ligament injuries in the cervical spine can lead to instability and persistent pain. Intervertebral disc injuries, including herniation or bulging, may compress nerve roots and create radiating pain into the arms along with headaches. elizabethsandelmd+1
Dr. Jimenez’s integrative approach emphasizes thorough evaluation of these sensory symptoms and their relationship to neuromusculoskeletal dysfunction. His clinical observations note that addressing cervical spine dysfunction through targeted chiropractic care often improves not only neck pain but also associated headaches and sensory symptoms. The neck and head share extensive neural connections, meaning that problems in one region frequently affect the other. wilbeckchiro+4
Understanding Migraines: Causes, Symptoms, and Connection to TBI
Migraines represent more than just severe headaches—they are complex neurological events involving multiple brain systems. Understanding what happens during a migraine helps explain why they become more common after traumatic brain injury and how to manage them effectively. ncbi.nlm.nih+1
What Happens in the Brain During a Migraine
Migraines involve a cascade of neurological changes that unfold over hours or even days. The process typically begins in the brainstem and hypothalamus, brain regions that regulate pain, arousal, and autonomic functions. These areas show altered activity even before headache pain begins. migrainedisorders+1
The cortical spreading depression represents a key mechanism in migraine pathogenesis. This phenomenon involves a wave of electrical silence that spreads across the brain’s surface at a rate of 2 to 3 millimeters per minute. As this wave passes through different brain regions, it temporarily suppresses normal brain activity. When the wave affects visual areas, it creates the visual aura symptoms that some people experience. The spreading depression also triggers inflammatory responses that contribute to headache pain. migrainedisorders
The trigeminal vascular system plays a central role in generating migraine pain. The trigeminal nerve sends branches to blood vessels surrounding the brain and in the meninges. When these nerve endings become activated, they release inflammatory substances, including calcitonin gene-related peptide (CGRP), substance P, and neurokinin A. These neuropeptides cause blood vessels to dilate, increase blood flow, and trigger inflammatory responses. The combination of vascular changes and inflammation activates pain receptors, creating the throbbing headache pain characteristic of migraines. emedicine.medscape+1
Neurotransmitter imbalances contribute significantly to migraine development. Serotonin, a neurotransmitter involved in pain regulation, mood, and blood vessel control, shows abnormal levels during migraines. Serotonin levels typically drop during migraine attacks, and this decrease may trigger the cascade of events that produce headache pain. Other neurotransmitters, including dopamine, norepinephrine, and glutamate, also show altered function during migraines. emedicine.medscape+1
Migraine Triggers and Risk Factors
Migraines can be triggered by numerous factors that vary from individual to individual. Common triggers include hormonal changes, particularly fluctuations in estrogen levels that occur during menstrual cycles. Many women experience migraines specifically related to their menstrual periods. Stress and emotional tension represent frequent migraine triggers, as does the relief after stress ends. Sleep disturbances, whether too little sleep, too much sleep, or irregular sleep patterns, often precipitate migraine attacks. clevelandclinic+1
Dietary factors can trigger migraines in individuals who are susceptible to them. Common food triggers include aged cheeses, processed meats containing nitrates, chocolate, alcohol (especially red wine), and foods containing monosodium glutamate (MSG). Skipping meals or fasting can also trigger migraines in some people. Caffeine presents a paradox—regular consumption followed by sudden withdrawal can trigger migraines, but caffeine can also help treat migraine pain when taken appropriately. mayoclinic
Environmental factors, including bright lights, loud sounds, strong smells, and changes in weather or barometric pressure, trigger migraines in many people. These sensory triggers become particularly problematic for people with TBI, who already experience heightened sensory sensitivity. The combination of post-TBI sensory dysfunction and migraine susceptibility creates a situation where many everyday environmental factors can trigger debilitating headaches. nature+4
Phases of a Migraine Attack
Migraines typically progress through distinct phases, though not every person experiences all phases or experiences them in the same order. The prodrome phase occurs hours or days before the onset of headache pain. During this phase, people may notice subtle changes, including mood alterations, food cravings, increased thirst, frequent urination, or neck stiffness. These prodrome symptoms result from changes in the hypothalamus and other brain regions that precede the headache. mayoclinic+1
The aura phase, which occurs in approximately 25% to 30% of people with migraines, involves temporary neurological symptoms that typically last between 5 and 60 minutes. Visual auras are the most common and may include seeing bright spots, flashing lights, zigzag lines, or the development of blind spots in the visual field. Sensory auras cause tingling or numbness that typically starts in the hand and spreads up the arm to the face. Speech and language disturbances can occur, making it difficult to find words or speak clearly. emedicine.medscape+1
The headache phase brings the characteristic migraine pain—moderate to severe, typically pulsating or throbbing, usually affecting one side of the head. The pain often intensifies with physical activity. Nausea and vomiting commonly accompany the headache. Photophobia and phonophobia make it difficult to tolerate light and sound. Many people need to lie down in a dark, quiet room during this phase. The headache phase typically lasts 4 to 72 hours if untreated. mayoclinic
The postdrome phase follows the resolution of headache pain. People often describe feeling drained, exhausted, or as if they are “hungover” during this phase. Some experience lingering head discomfort or unusual sensations. Mood changes, difficulty concentrating, and fatigue can persist for a day or more after the headache resolves. mayoclinic
How TBI Changes Migraine Patterns
Traumatic brain injury can transform migraine patterns in several ways. People who never experienced migraines before their injury may develop new-onset migraines afterward. Those who had occasional migraines before TBI often find that their migraines become more frequent, severe, or difficult to treat after injury. The study of TBI patients shows that injury severity correlates with increased migraine risk—more severe injuries create a higher likelihood of developing post-traumatic migraines. neurology+1
The mechanisms linking TBI to altered migraine patterns involve lasting changes in brain structure and function. Inflammation in the brain can persist for months or years after the initial injury. This ongoing inflammation lowers the threshold for migraine attacks, making them easier to trigger. Damage to brain regions involved in pain processing and sensory filtering creates hypersensitivity that contributes to both more frequent migraines and heightened sensitivity to migraine triggers. nature+1
Post-traumatic migraines often prove more difficult to treat than migraines unrelated to injury. Standard migraine medications may be less effective, and patients may require combination approaches involving multiple treatment modalities. The presence of other post-TBI symptoms, including cognitive impairment, mood changes, sleep disturbances, and neck pain, complicates treatment and may interfere with recovery from migraines. pmc.ncbi.nlm.nih+1
Diagnostic Assessment and Imaging for TBI and Headaches
Proper diagnosis of traumatic brain injury and post-traumatic headaches requires a comprehensive evaluation combining clinical assessment with appropriate imaging studies. Dr. Jimenez’s dual-scope practice enables thorough diagnostic workups that address both neurological and neuromusculoskeletal aspects of patient injuries. ncbi.nlm.nih+2
Clinical Evaluation
The diagnostic process begins with a detailed history-taking. Healthcare providers need to understand the mechanism of injury—how the trauma occurred, what forces were involved, whether loss of consciousness occurred, and what symptoms developed immediately afterward. Information about symptom progression helps distinguish between the effects of acute injury and complications that develop over time.advantagehcs+1
Neurological examination assesses multiple domains of function. Mental status testing evaluates the level of consciousness, orientation, memory, and cognitive abilities. Cranial nerve examination tests the function of the twelve nerve pairs that emerge from the brain and control functions including vision, eye movements, facial sensation and movement, hearing, and swallowing. Motor examination assesses muscle strength, tone, and coordination. Sensory testing evaluates the ability to perceive touch, temperature, pain, and position sense. Reflex testing provides information about the integrity of nerve pathways. ncbi.nlm.nih
Specialized testing may include vestibular evaluation for balance problems, vision testing for visual disturbances, and cognitive screening tools to identify specific areas of impairment. Headache characteristics are carefully documented, including location, quality, intensity, duration, frequency, triggers, and associated symptoms. This information helps classify the type of headache and guide treatment selection. ncbi.nlm.nih+1
A Questionnaire Example for TBI Symptoms
Imaging Studies
Computed tomography (CT) scans represent the first-line imaging study for acute traumatic brain injury. CT excels at detecting skull fractures, bleeding inside or around the brain, brain swelling, and other acute complications requiring immediate intervention. The speed of CT scanning makes it ideal for the emergency evaluation of head-injured patients. CT provides excellent visualization of bone structures, helping identify fractures that may contribute to ongoing symptoms. elementimaging+1
Magnetic resonance imaging (MRI) provides superior detail of brain tissue and detects injuries that may not appear on CT scans. MRI is particularly valuable for evaluating mild to moderate TBI, where CT may appear normal despite ongoing symptoms. Different MRI sequences highlight distinct tissue characteristics, enabling a comprehensive assessment of structural damage. Diffusion tensor imaging (DTI), an advanced MRI technique, can detect damage to white matter tracts—the nerve fiber bundles that connect different brain regions. This technique helps explain persistent symptoms when conventional imaging appears normal. pubmed.ncbi.nlm.nih+1
Cervical spine imaging plays an important role when neck injury accompanies head trauma. X-rays provide a basic evaluation of cervical vertebral alignment and identify obvious fractures or dislocations. CT offers more detailed bone visualization and can detect subtle fractures that are often missed on X-rays. MRI excels at showing soft tissue injuries, including ligament tears, disc herniations, and spinal cord damage. These cervical spine imaging studies help identify structural problems contributing to neck pain and cervicogenic headaches. pmc.ncbi.nlm.nih+2
Dr. Jimenez’s clinic utilizes advanced neuromusculoskeletal imaging as part of a comprehensive patient evaluation. This imaging approach examines not only the brain and skull but also the cervical spine, surrounding soft tissues, and musculoskeletal structures that may contribute to symptoms. The integration of imaging findings with clinical examination results enables an accurate diagnosis that informs treatment planning. advantagehcs+1
Functional Assessment
Beyond structural imaging, functional assessments evaluate how injuries affect daily activities and quality of life. Standardized questionnaires assess the impact of headaches, cognitive function, emotional well-being, and the ability to perform work, social, and recreational activities. These assessments provide objective measures of symptom severity, helping to track recovery progress over time. ncbi.nlm.nih
Neuropsychological testing provides a comprehensive evaluation of cognitive abilities, encompassing attention, memory, language, visual-spatial skills, and executive functions. These tests identify specific areas of impairment and help develop targeted rehabilitation strategies to address them. Serial testing over time documents cognitive recovery and helps determine readiness to return to work or other demanding activities. pubmed.ncbi.nlm.nih+2
Treatment Approaches: Integrative Medicine for TBI and Headaches
Managing traumatic brain injury and post-traumatic headaches requires comprehensive approaches that address multiple aspects of the condition. Dr. Jimenez’s integrative medicine practice in El Paso combines chiropractic care, medical management, physical rehabilitation, and complementary therapies to promote natural healing and optimal recovery. northwestfloridaphysiciansgroup+3
Chiropractic Care for Post-Traumatic Headaches and Neck Pain
Chiropractic treatment focuses on addressing neuromusculoskeletal dysfunction that contributes to pain and other symptoms. Following TBI, particularly when accompanied by whiplash or neck injury, the cervical spine often develops misalignments, restricted motion, and muscle tension that contribute to headaches. Chiropractic evaluation identifies these mechanical problems through a physical examination and a review of imaging. pubmed.ncbi.nlm.nih+3
Spinal manipulation, the hallmark of chiropractic treatment, involves applying controlled forces to joints to restore normal motion and alignment. For post-traumatic headaches, chiropractors typically focus on the cervical spine, particularly the upper cervical region, where dysfunction commonly contributes to head pain. Research supports the effectiveness of spinal manipulation for certain types of headaches, particularly tension-type and cervicogenic headaches. Evidence-based guidelines recommend chiropractic manipulation as a treatment option for adults with cervicogenic headaches. oakbrookmedicalgroup+4
Soft tissue techniques address muscle tension, trigger points, and fascial restrictions that contribute to pain and discomfort. These techniques may include massage, myofascial release, and instrument-assisted soft tissue mobilization. Releasing tight muscles and improving tissue quality helps reduce pain, improve range of motion, and support healing. drjeffreystinson+2
Dr. Jimenez’s chiropractic approach emphasizes gentle, specific adjustments tailored to each patient’s condition and tolerance. Following TBI, care must be taken to avoid aggressive treatment that could worsen symptoms. The dual medical training allows Dr. Jimenez to recognize situations where chiropractic care should be modified or delayed pending further medical evaluation. northwestfloridaphysiciansgroup+1
Exercise Therapy and Physical Rehabilitation
Exercise therapy plays a crucial role in the recovery from TBI. Research demonstrates that appropriate exercise can enhance neuroplasticity—the brain’s ability to reorganize and form new neural connections. This neuroplasticity represents the foundation for recovery, allowing undamaged brain regions to compensate for injured areas. pmc.ncbi.nlm.nih+3
Aerobic exercise provides multiple benefits for people recovering from TBI. Cardiovascular activity increases blood flow to the brain, delivering oxygen and nutrients needed for healing. Exercise stimulates the release of brain-derived neurotrophic factor (BDNF), a protein that supports neuron survival and growth. Regular aerobic exercise can help reduce headache frequency and intensity, while also improving mood, sleep, and cognitive function. flintrehab+2
Strength training helps restore muscle function that may have declined during the acute injury phase. Building strength in the neck and shoulder muscles provides better support for the cervical spine, reducing mechanical stress that contributes to cervicogenic headaches. Core strengthening improves posture and reduces compensatory muscle tension. rehabpartners+1
Balance and coordination exercises help address vestibular dysfunction and reduce the risk of falls. These exercises typically begin with simple activities and progress to more challenging tasks as abilities improve. Vestibular rehabilitation specifically targets the balance system through exercises that retrain the brain to process vestibular information correctly. physio-pedia+2
Cognitive exercises help restore mental functions affected by TBI. These activities challenge attention, memory, processing speed, and executive functions in a progressive and structured manner. The principle of neuroplasticity applies to cognitive recovery—repeatedly practicing specific mental tasks strengthens the neural pathways supporting those abilities. psychiatrictimes+3
Dr. Jimenez’s clinic incorporates targeted exercise programs as a central component of rehabilitation. Exercise prescriptions are tailored to each patient’s specific impairments, functional goals, and symptom tolerance. The programs typically start conservatively and progress gradually, respecting the principle that excessive exertion can worsen post-traumatic symptoms, particularly headaches.flintrehab+2
Massage Therapy for Pain Relief and Healing
Massage therapy offers multiple benefits for people recovering from traumatic injuries. Therapeutic massage reduces muscle tension, improves circulation, decreases pain, and promotes relaxation. These effects make massage particularly valuable for managing post-traumatic headaches, especially tension-type and cervicogenic headaches linked to muscle dysfunction.excelsiainjurycare+2
The mechanisms through which massage therapy provides benefits involve both local and systemic effects. Locally, massage increases blood flow to treated tissues, delivering oxygen and nutrients while removing metabolic waste products. Massage helps release trigger points—hyperirritable spots in muscle tissue that create local and referred pain. Breaking up fascial adhesions and scar tissue improves tissue mobility and reduces pain.news.harvard+2
Systemically, massage therapy influences the nervous system in ways that reduce pain perception and promote healing. Massage activates sensory receptors that send signals to the spinal cord, where they can inhibit pain signals from reaching the brain. This mechanism, sometimes referred to as “closing the gate,” helps explain how massage therapy provides pain relief. Massage also triggers the release of endorphins, the body’s natural pain-relieving chemicals. multicaremedicalcenters+1
Research demonstrates that massage therapy accelerates muscle healing after injury. Studies show that massage reduces inflammation in injured muscles while promoting the development of new mitochondria—the cellular structures responsible for producing energy. These effects translate to faster recovery and stronger healed tissue. news.harvard
For TBI patients, massage therapy addresses both direct head and neck injuries and secondary muscle tension that develops as the body compensates for pain and dysfunction. The relaxation effects of massage help reduce stress and anxiety, which commonly worsen after TBI and can trigger or intensify headaches. Many patients report improved sleep quality after massage therapy, and better sleep supports overall healing. lhphysicaltherapy+3
Dr. Jimenez’s integrative approach includes massage therapy as part of comprehensive treatment plans. Licensed massage therapists work in coordination with other healthcare providers to address soft tissue dysfunction that contributes to patient symptoms. Treatment frequency and techniques are adjusted according to the patient’s response and treatment goals. dominguezinjurycenters+2
Chiropractic Care for Healing After Trauma- Video
Acupuncture for Neurological Recovery
Acupuncture, a component of traditional Chinese medicine, involves inserting thin needles into specific points on the body to influence health and healing. Growing research evidence supports acupuncture’s effectiveness for treating various conditions related to TBI, including headaches, pain, cognitive impairment, and emotional disturbances.iamdesignedtoheal+1
Multiple mechanisms appear to mediate the effects of acupuncture on the nervous system. Acupuncture stimulation influences neurotransmitter levels, including the increase of serotonin and endorphins that help regulate pain and mood. Functional brain imaging studies demonstrate that acupuncture modulates activity in brain regions associated with pain processing, emotional regulation, and sensory integration. These changes help explain how acupuncture can reduce pain, improve mood, and enhance cognitive function. pmc.ncbi.nlm.nih+1
For TBI specifically, research suggests that acupuncture may promote neurological recovery through several pathways. Acupuncture appears to reduce neuroinflammation, a type of brain inflammation that persists after injury and contributes to ongoing symptoms. Studies in animal models demonstrate that acupuncture can enhance neuroplasticity, supporting the brain’s natural healing processes. Acupuncture also improves cerebral blood flow, ensuring adequate oxygen and nutrient delivery to healing brain tissue.pmc.ncbi.nlm.nih
Clinical studies report positive outcomes when acupuncture is incorporated into TBI rehabilitation programs. Patients receiving acupuncture show improvements in consciousness levels, cognitive function, motor abilities, and quality of life compared to those receiving standard care alone. For post-traumatic headaches, acupuncture demonstrates effectiveness comparable to or exceeding conventional treatments, often with fewer side effects.iamdesignedtoheal+1
Acupuncture treatment for TBI typically involves multiple sessions over weeks or months. Specific acupuncture points are selected based on the patient’s symptoms and treatment goals. The treatment is generally safe when performed by qualified practitioners, with minimal risk of adverse effects. iamdesignedtoheal+1
Dr. Jimenez’s clinic offers acupuncture as part of integrated treatment protocols for TBI and post-traumatic headaches. The combination of acupuncture with chiropractic care, exercise therapy, and massage therapy provides comprehensive support for healing and symptom management. This multimodal approach addresses injury causes through multiple pathways, enhancing overall treatment effectiveness. dominguezinjurycenters+1
Managing Injury Cases: Documentation and Coordinated Care
Traumatic brain injuries often occur in contexts requiring careful documentation and coordination between healthcare providers, employers, insurance companies, and legal professionals. Dr. Jimenez’s practice handles injuries from multiple sources and provides comprehensive medical and legal documentation needed for these cases. gbw+4
Work-Related Injuries
Workplace injuries, including those causing TBI, require specific procedures and documentation. Employers must provide workers’ compensation coverage that pays for medical treatment and lost wages resulting from work-related injuries. Proper documentation establishes that the injury occurred at work and defines the scope of medical treatment needed. koszdin+2
Immediate documentation begins at the time of injury. Employees should report injuries to their supervisor as soon as possible, providing details about how the injury occurred. Employers must complete incident reports that document the circumstances of the injury. Seeking prompt medical evaluation creates an official record of injuries and symptoms. jobsitecare+1
Healthcare providers treating work injuries must document the mechanism of injury, examination findings, diagnoses, treatment plans, work restrictions, and prognosis. This documentation guides workers’ compensation case management and determines which treatments receive coverage. Detailed records establish causation—the connection between workplace activities and resulting injuries. aafp+1
Dr. Jimenez’s clinic has extensive experience managing work-related injuries, including TBI from falls, struck-by accidents, and other workplace incidents. The practice provides thorough documentation meeting workers’ compensation requirements while ensuring patients receive comprehensive, evidence-based care. Clear communication with employers and case managers facilitates the appropriate authorization of treatment and planning for return to work. axiomllc+2
Sports Injuries
Athletic activities create a significant risk for traumatic brain injury, particularly in contact sports. Proper management of sports-related TBI requires expertise in both acute injury assessment and rehabilitation planning. Return-to-play decisions must strike a balance between the athlete’s desire to compete and safety considerations aimed at preventing reinjury. austinoi+2
Sports injury assessment begins with determining the severity of the injury and identifying factors that require immediate intervention. Athletes showing signs of serious TBI, including prolonged loss of consciousness, worsening symptoms, seizures, or neurological deficits, require emergency medical evaluation. For mild concussions, initial management emphasizes rest and gradual return to activities. physio-pedia+2
Rehabilitation for sports injuries follows a structured progression that gradually increases physical and cognitive demands. Athletes typically begin with gentle aerobic exercise that does not provoke symptoms, then progress through sport-specific drills, non-contact practice, and finally full-contact practice before returning to competition. Each stage should be completed without symptom recurrence before proceeding to the next stage. aspenridgephysicaltherapy+3
Documentation of sports injuries supports the provision of appropriate care and protects against premature return to play. Medical clearance from qualified healthcare providers is essential before athletes resume full participation. Some jurisdictions have laws requiring medical clearance for athletes who have sustained concussions. rehabpartners+1
Dr. Jimenez’s practice specializes in treating athletes from various sports, offering comprehensive evaluation and rehabilitation services. The clinic’s integrative approach combines medical assessment, imaging when needed, chiropractic care for associated musculoskeletal injuries, and targeted rehabilitation programs. This coordinated care supports a safe and effective return to athletic activities while minimizing the risk of reinjury. austinoi+3
Motor Vehicle Accident Injuries
Motor vehicle accidents represent a leading cause of traumatic brain injury. These incidents often combine multiple injury mechanisms, including direct head impact, rapid acceleration-deceleration forces, and whiplash-type neck injuries. The complex nature of MVA injuries requires comprehensive evaluation and treatment. cdc+3
TBI from motor vehicle accidents may not be immediately apparent. People can sustain concussions even without hitting their heads, as the rapid motion alone can injure the brain. Delayed symptom onset is common—some symptoms may not appear until hours or days after the accident. This delayed presentation highlights the importance of a thorough medical evaluation, even when initial symptoms appear minor. clevelandclinic+2
Legal and insurance considerations add complexity to MVA injury cases. Establishing the connection between the accident and resulting injuries requires detailed documentation. Medical records must describe the accident mechanism, the timing of symptom onset, examination findings, diagnostic test results, treatment provided, and any resulting functional limitations. This documentation supports insurance claims and potential legal actions. baumgartnerlawyers+3
Dr. Jimenez’s clinic regularly treats patients injured in motor vehicle accidents, providing both medical care and necessary documentation to support their claims. The practice recognizes the importance of a thorough initial evaluation to identify all injuries, including those that may not manifest immediately. Detailed records document the full scope of injuries and their impact on function. The clinic coordinates care with other specialists when needed and communicates with insurance companies and legal representatives as appropriate. njadvocates+2
Personal Injury Cases
Personal injuries from falls, assaults, or other incidents may result in TBI requiring medical treatment and potentially legal action. These cases require careful documentation linking injuries to the incident in question. Medical records provide crucial evidence establishing injury severity, necessary treatment, and prognosis. halemonico+3
A timely medical evaluation after an injury strengthens personal injury claims. Delays between injury and medical care can create questions about whether symptoms truly resulted from the incident or developed from other causes. Comprehensive initial evaluation documents all injuries and establishes the baseline from which recovery will be measured. baumgartnerlawyers+1
Ongoing documentation tracks recovery progress, treatment effectiveness, and remaining limitations. This information establishes damages—the losses and expenses resulting from the injury. Medical records that describe pain, functional limitations, treatment requirements, and the impact on daily activities support compensation claims.gbw+2
Dr. Jimenez provides a thorough medical and chiropractic evaluation for patients with personal injuries. The practice creates detailed records suitable for legal proceedings while maintaining focus on optimal patient care. Expert testimony may be provided when cases proceed to litigation, explaining injuries, treatment, and prognosis to judges and juries. njadvocates+2
Preventing Long-Term Problems Through Comprehensive Care
The integrated, patient-centered approach to TBI and post-traumatic headache management aims to prevent chronic problems that can persist for years. Early, comprehensive intervention provides the best opportunity for complete recovery. Understanding the principles that guide effective rehabilitation enables patients and their families to engage actively in the healing process. frontiersin+4
Addressing Root Causes
Effective treatment must address the underlying causes of symptoms rather than simply masking pain or other manifestations. For post-traumatic headaches, this means identifying and treating all contributing factors, including cervical spine dysfunction, muscle tension, neurological impairments, and sensory processing problems. Symptom management alone, without addressing root causes, often leads to persistent, treatment-resistant problems.traditionhealth+3
Dr. Jimenez’s diagnostic approach aims to identify all factors contributing to a patient’s symptoms. This comprehensive evaluation considers not only the direct effects of head trauma but also associated injuries to the neck, effects on posture and movement patterns, nutritional status, sleep quality, stress levels, and other factors influencing healing. Treatment plans target identified problems through appropriate interventions. traditionhealth+2
The functional medicine perspective emphasizes that optimal healing requires addressing the body’s overall health status. Nutrition provides building blocks for tissue repair and neurotransmitter production. Sleep allows the brain to clear metabolic waste products and consolidate memories. Stress management prevents the chronic activation of stress response systems, which can worsen symptoms and impair healing. Physical activity promotes neuroplasticity and cardiovascular health. This holistic view acknowledges that seemingly unrelated factors can have a significant impact on recovery from TBI. elevatewellnesschiro+2
Promoting Natural Healing
The body possesses a remarkable capacity for healing when provided with appropriate support. Neuroplasticity allows the brain to reorganize after injury, with undamaged regions developing new capabilities to compensate for lost functions. This recovery process is most effective when patients receive proper treatment and actively engage in rehabilitation. pmc.ncbi.nlm.nih+2
Chiropractic care supports natural healing by restoring normal biomechanics, reducing pain, and eliminating interference with the nervous system’s function. Manual therapy enhances joint mobility, alleviates muscle tension, and promotes healing responses. These treatments work in conjunction with the body’s inherent healing mechanisms, rather than suppressing symptoms artificially. jacksonhealingarts+3
Integrative medicine combines the best of conventional medical care with evidence-based complementary therapies. This approach recognizes that different treatment modalities offer unique benefits, and combining them often produces superior results compared to any single intervention. For TBI, this may involve using medications to manage severe symptoms while also employing chiropractic care, exercise therapy, acupuncture, and massage to address the root causes and promote healing. drestner+3
Patient Education and Empowerment
Education empowers patients to actively participate in their own recovery. Understanding their condition, what to expect during recovery, and how different treatments work helps patients make informed decisions and maintain motivation. Dr. Jimenez’s practice emphasizes patient education, ensuring people understand their diagnoses, treatment options, and self-care strategies. newmedicalchoices+2
Self-management skills are essential for long-term success. Patients learn to identify and avoid triggers that exacerbate symptoms, recognize warning signs that require medical attention, and implement strategies for managing symptoms when they occur. Activity pacing—balancing activity with rest to avoid symptom exacerbation—helps people gradually expand their functional capacity without creating setbacks. physio-pedia+2
Lifestyle modifications support healing and prevent future problems. This may include adjusting work or school schedules to accommodate cognitive limitations, modifying physical activities to reduce the risk of injury, implementing stress management techniques, improving sleep hygiene, and optimizing nutrition. These changes create an environment conducive to healing and help prevent chronic disability. elevatewellnesschiro+1
Long-Term Follow-Up and Monitoring
Recovery from TBI often takes months or years, requiring ongoing monitoring and treatment adjustment. Some symptoms resolve quickly while others persist or develop later. Regular follow-up visits enable healthcare providers to monitor progress, identify emerging issues, adjust treatments as necessary, and offer ongoing support. krwlawyers+3
Functional outcome assessment measures recovery in terms of real-world abilities, rather than relying solely on symptom checklists. Can the person return to work or school? Can they drive safely? Can they manage household responsibilities? Can they participate in social and recreational activities? These functional measures provide meaningful indicators of recovery and help identify areas needing continued intervention. krwlawyers
Preventing secondary complications represents an important aspect of long-term care. Depression, anxiety, social isolation, physical deconditioning, and chronic pain syndromes can develop after TBI, creating additional barriers to recovery. Early identification and treatment of these complications prevents them from becoming entrenched problems. mayoclinic+3
Dr. Jimenez’s practice provides continued support throughout the recovery process. The clinic’s comprehensive approach addresses not only physical symptoms but also the cognitive, emotional, and social challenges that accompany TBI. Coordination with other specialists ensures patients receive all needed services. The goal is complete recovery, allowing people to return to their previous level of function or achieve the best possible outcome given the severity of their injuries. advantagehcs
Conclusion
Traumatic brain injury creates complex challenges affecting physical, cognitive, and emotional functioning. Headaches and migraines represent some of the most common and disabling symptoms following TBI, resulting from inflammation, altered brain chemistry, sensory processing dysfunction, and associated neck injuries. Understanding how these symptoms develop and interconnect provides the foundation for effective treatment. Post-traumatic headaches take various forms, including migraine-type headaches, tension-type headaches, cervicogenic headaches, and others. Each headache type involves distinct mechanisms and responds best to targeted interventions. A comprehensive diagnostic evaluation identifies the specific factors contributing to an individual’s symptoms, enabling personalized treatment planning. The integrative medicine approach employed by Dr. Alexander Jimenez in El Paso combines chiropractic care, medical management, physical rehabilitation, massage therapy, and acupuncture to address the multifaceted aspects of TBI and its associated consequences. This coordinated, multimodal treatment strategy targets root causes rather than simply masking symptoms, promoting natural healing and preventing chronic disability.
Proper management of TBI requires not only skilled clinical care but also careful documentation, particularly for injuries occurring in work, sports, or motor vehicle accident contexts. Comprehensive medical records establish the connection between traumatic events and resulting symptoms, support insurance claims, and provide evidence in legal proceedings when necessary. Early, aggressive intervention provides the best opportunity for complete recovery from TBI. The brain’s neuroplasticity—its ability to reorganize and form new connections—represents the foundation for healing. Appropriate exercise, manual therapies, cognitive rehabilitation, and other interventions enhance neuroplasticity and support functional recovery. Patient education and empowerment facilitate active participation in the healing process, leading to improved outcomes and reduced long-term complications. Recovery from traumatic brain injury and post-traumatic headaches often requires patience and persistence. While some symptoms resolve quickly, others may persist for months or years. Comprehensive, patient-centered care addresses the full range of physical, cognitive, and emotional challenges, helping people achieve the best possible outcomes and return to meaningful, productive lives.
I Am Designed to Heal. (2024, December 11). How acupuncture supports recovery from traumatic brain injury (TBI). https://iamdesignedtoheal.com/
International Classification of Headache Disorders. (2018, February 5). 5.2 Persistent headache attributed to traumatic injury to the head. https://ichd-3.org/
JAMA Network. (2023, November 30). Profiles of cognitive functioning at 6 months after traumatic brain injury. https://jamanetwork.com/
How Head Trauma Can Trigger Sciatica: The Hidden Link and Ways to Heal
A doctor of chiropractic explains to an automobile accident patient how a head injury can cause sciatica and lower back problems.
Head injuries can occur in car crashes, sports-related falls, or everyday slips. They shake the brain and body in ways you might not expect. One surprising outcome? Sciatica. That’s the sharp pain shooting down your leg from a pinched sciatic nerve. Many people don’t connect a bump on the head to that nagging leg ache. However, science reveals a clear connection between the two. This article breaks it down simply. We’ll explore how head trauma messes with your spine and nerves. We’ll also cover how gentle chiropractic care can help ease pain and speed up recovery. If you’ve had a head injury and now feel leg pain, this could explain why—and what to do next.
What Is Head Trauma and How Does It Relate to Sciatica?
Head trauma means any blow to the skull that jars the brain. It ranges from mild concussions to severe traumatic brain injuries (TBI). A concussion might leave you dizzy for days. A serious TBI could mean hospital stays and long-term changes. These injuries don’t just affect thinking. They ripple through the whole body.
Sciatica is a type of pain caused by the sciatic nerve. This nerve starts in your lower back and runs down each leg. It’s the longest nerve in your body. When irritated, it causes burning, tingling, or shooting pain from the butt to the foot. Common causes include herniated discs or tight muscles. But head trauma adds a twist. It can trigger changes deep within your nervous system that lead to nerve trouble.
Studies show that up to 78% of TBI survivors deal with ongoing pain. That includes back and leg aches, such as sciatica. Why? The brain controls everything, including how your spine moves. A head hit disrupts that control.
Dr. Alexander Jimenez, a chiropractor in El Paso, Texas, frequently observes this phenomenon in his clinic. As a Doctor of Chiropractic and Nurse Practitioner, he treats patients after accidents. He notes that head trauma often hides as simple bumps but leads to widespread pain. In his observations, many patients come in with leg pain that they attribute to old falls or crashes. His team uses functional medicine to trace the issue back to the brain-spine connection.
How Head Trauma Alters Brain Control Over Spinal Muscles
Your brain is like a boss for your muscles. It sends signals down the spinal cord to maintain balance. Head trauma throws that off. A TBI damages brain areas that regulate movement. This leads to spasticity—tight, jerky muscles in the legs and back.
Think of it this way: Normally, your brain tells spinal muscles to relax and stretch smoothly. After a head injury, those signals glitch. Muscles in the lower back get out of sync. They pull unevenly on the spine. Over time, this puts strain on the sciatic nerve roots as they exit the lower back.
One study found that mild TBIs cause extra sensitivity in the legs. It’s as if the brain amplifies pain signals through chemicals called chemokines. These build up in the spinal cord, making nerves fire too easily. For sciatica, this means even small movements cause more pain.
Dr. Jimenez observes this in athletes after concussions. “Patients tell me their legs feel heavy, like they’re fighting their own body,” he shares in his wellness podcasts. His clinic uses nerve tests to spot these glitches early. By addressing them, they prevent the pain from becoming chronic.
This muscle chaos doesn’t stop at the back. It can weaken core support, leading to poor posture. Slouching adds pressure on the sciatic nerve. It’s a slow build, but real.
Head Injury/TBI Symptom Questionnaire:
Head Injury/TBI Symptom Questionnaire
Misalignment and Muscle Impairment: Irritating the Sciatic Nerve
Head trauma often hits the neck hard. The force whips the head forward and back—like in a car crash. This misaligns the upper spine, particularly the top vertebrae, known as the atlas and axis. That misalignment travels down like a domino fall.
Impaired muscles from brain signals exacerbate the condition. Tight neck muscles pull the spine off-kilter. In the lower back, this squeezes discs and nerves. The sciatic nerve can become pinched between bones or become inflamed. Result? That classic leg zap.
Research backs this. Up to 8% of severe TBI cases come with spine injuries. Even mild ones raise the risk. A study on 180 patients showed that older folks or those with low consciousness scores face higher odds. The neck shift stresses the whole chain, irritating the sciatic nerve.
Concussions alone can spark lower back pain. The brain’s balance center gets knocked. Muscles overwork to compensate, tiring the back. Dr. Jimenez refers to this as the “cascade effect” in his LinkedIn posts. He treats it with targeted adjustments to reset muscle tone.
Raising the Risk of Further Spinal Damage
Head trauma doesn’t just irritate—it invites more trouble. A damaged brain means slower reflexes. You might stumble more easily, leading to falls that jar the spine again. Plus, inflammation from TBI spreads. It swells the tissues around the spine, causing the discs to bulge and the nerves to become vulnerable.
One key risk: Concomitant injuries. That’s when head and spine hits happen together. In motor vehicle crashes—the top TBI cause—neck strains often tag along. This doubles the chance of disc slips that pinch the sciatic nerve.
Dr. Jimenez observes this in patients involved in car accidents. “A rear-end collision jars the brain and twists the lumbar spine,” he explains in his functional medicine series. His observations show early chiropractic checks cut re-injury risks by improving stability.
The Role of Swelling and Heterotopic Ossification in Nerve Crushing
TBI triggers swelling fast. Brain tissue bruises, and fluids build up. This chaos can spread to the body. In rare but serious cases, it leads to heterotopic ossification (HO). That’s when bone grows in soft tissues—like muscles or around nerves.
Around the sciatic nerve, HO is sneaky. It starts after hip or pelvic trauma, tied to the head hit. Scar tissue hardens into bone, encasing the nerve. Over months, this crushes it. Symptoms creep in: Numbness, weakness, foot drop.
A case report described a young man following traumatic brain injury (TBI). Seventeen months later, bilateral sciatic entrapment from hip HO caused severe pain. Surgery freed the nerve, but prevention is key. Anti-inflammatory drugs or radiation cut HO risks.
Dr. Jimenez warns of this in his injury recovery blogs. He uses imaging to identify early signs of HO in TBI patients with leg pain. His integrative plans include nutrition to fight inflammation and slow bone overgrowth.
Upper Neck Misalignment: Starting a Pain Cascade to the Sciatic Nerve
The upper neck is ground zero for many head traumas. Whiplash from falls or sports bends it unnaturally. This throws off the atlas—the top bone. It shifts pressure down the spine.
The cascade? Misaligned neck pinches nerves there. Signals to the lower back get scrambled. Muscles tighten unevenly, pulling on the lumbar joints. This stresses the sciatic nerve roots, causing inflammation and pain.
Inflammation plays a big role. Concussion swelling in the neck disrupts blood flow and nerve signals, causing significant complications. It causes the brain to misread pain, amplifying the sensation of hurt in the leg.
Dr. Jimenez’s clinical notes highlight this in veterans with whiplash-TBI. “Neck shifts create a domino pain chain,” he says. His team uses precise X-rays to map it, then adjusts to break the cycle.
Integrative Chiropractic: A Path to Relief and Recovery
Integrative chiropractic blends hands-on care with wellness tools. It’s perfect for post-head injury sciatica. No drugs or surgery—just realignment and support.
First, it realigns the spine. Gentle adjustments fix neck and back shifts. This eases nerve pressure fast. For sciatica, lumbar tweaks reduce the disc bulge on the nerve.
Second, it boosts nervous system function. Adjustments reduce interference, allowing brain signals to flow more smoothly. This calms spastic muscles and dials down pain sensitivity.
Third, it fights inflammation. Soft tissue work, like massage, releases tight spots. Add nutrition advice, including anti-inflammatory foods, and use swelling drops.
Finally, it restores cerebrospinal fluid (CSF) flow. CSF cushions the brain and spine. Trauma clogs it, raising pressure. Craniosacral therapy—light touches on the skull and sacrum—clears the path. Patients report clearer heads and less pain.
Dr. Jimenez integrates all this. His clinic mixes adjustments with functional tests. “We trace sciatica back to the head hit, then rebuild from there,” he observes. Patients who have been in accidents often experience mobility gains within weeks. One testimonial: A crash survivor ditched leg braces after targeted care.
Studies agree. Chiropractic reduces TBI pain by 50% in some individuals. For post-concussion, it eases dizziness and back aches.
Real-Life Stories and Expert Tips
Take Sarah, a soccer player Dr. Jimenez treated. A header caused a concussion and later sciatica. Adjustments realigned her neck, easing leg pain. Now she plays pain-free.
Tips from experts: Start care early. Get imaging if pain lingers post-injury. Pair chiropractic care with rest and omega-3 fatty acids for managing inflammation.
Wrapping It Up: Take Control of Your Recovery
Head trauma to sciatica seems far-fetched, but the links are strong. From brain glitches to bone growth, it stresses the sciatic nerve. Integrative chiropractic offers hope—realigning, calming, and healing.
Don’t ignore the signs. See a pro like Dr. Jimenez for a check. Your body can bounce back stronger.
Common Sports Head Injuries: From Concussions to Severe Trauma
Sports bring excitement, fitness, and teamwork, but they also come with risks. One of the biggest dangers is head injuries. These can happen in any sport, from a quick bump in soccer to a hard tackle in football. The most common sports head injury is a concussion, which is a mild traumatic brain injury. But more serious ones, like brain contusions, intracranial hematomas, and skull fractures, can also occur. Understanding these injuries helps athletes, coaches, and families stay safe. This article examines the causes, signs, and treatment options, including the role of chiropractic and integrative care.
What Are Sports Head Injuries?
Head injuries in sports happen when there’s a strong force to the head or body that makes the brain move inside the skull. This can damage brain cells and change how the brain works. Common types include concussions, which are mild, and more severe ones like fractures or bleeds. According to experts, concussions make up most of these injuries, often from a blow to the head or violent shaking (Cleveland Clinic, 2024). These shakes or hits stretch nerves and blood vessels, leading to problems.
Sports head injuries are a big issue because they can affect thinking, balance, and even emotions. In the U.S., about 300,000 concussions happen each year from sports (Bailes & Cantu, 2001). While many people recover quickly, ignoring them can lead to long-term troubles like memory loss or mood changes.
The Most Common Injury: Concussions
A concussion is the top head injury in sports. It’s a mild traumatic brain injury that changes how the brain functions for a short time. It occurs when the brain bounces against the skull due to a hit or jolt. You don’t always pass out; many people stay awake but feel off.
Causes of Concussions
Concussions come from direct hits, like a helmet clash in football, or indirect ones, like a body check that shakes the head. In soccer, heading the ball can cause one to suffer a concussion (Arsenian Law Offices, n.d.). Rotational forces, where the head twists, are especially bad because they shear brain tissues (Bailes & Cantu, 2001). Sports like football, soccer, and hockey are the most prone to collisions.
Data shows that in high school sports, football has the highest rate, with tackling causing 63% of concussions (CDC, n.d.). Girls’ soccer follows, with heading the ball linked to one in three cases. Even non-contact sports like basketball can lead to them from falls or player bumps.
Symptoms of Concussions
Symptoms can appear immediately or develop later. Common ones include headache, dizziness, nausea, confusion, and sensitivity to light or noise (Mayo Clinic, 2024a). You might feel foggy, have trouble focusing, or forget things. Emotional signs, such as irritability or sadness, can also appear (Cleveland Clinic, 2024).
In some cases, people look dazed, slur their speech, or have seizures (Mayo Clinic, 2024a). Drowsiness is another sign (American Academy of Orthopaedic Surgeons, n.d.). If symptoms worsen, such as repeated vomiting or unequal pupils, it’s an emergency.
Headaches are a big part of concussions. They can come from a brain injury or related neck strain. In sports, post-traumatic headaches happen after impacts, and things like dehydration or poor posture make them worse (Studio Athletica, n.d.).
Diagnosis of Concussions
Doctors evaluate for concussions with a physical exam, asking about symptoms and testing balance, memory, and reflexes. Tools like the Sport Concussion Assessment Tool (SCAT) help evaluate (Kazl & Giraldo, 2013). Imaging, like CT scans, isn’t always needed unless symptoms are severe, as concussions don’t usually show on scans (American Academy of Orthopaedic Surgeons, n.d.).
Head Injury/TBI Symptom Questionnaire
More Severe Sports Head Injuries
While concussions are common, sports can cause worse injuries. These need immediate medical help to avoid lasting damage or death.
Skull Fractures
A skull fracture is a break in the bone around the brain. In sports, it often results from hard falls or hits, such as in cycling or hockey (Children’s Minnesota, n.d.). Symptoms include headaches, swelling, bruising around the eyes or ears, and fluid from the nose or ears. It often comes with a concussion.
Treatment is rest and pain meds. Surgery is typically only required when the fracture is depressed or open. Follow-up checks ensure healing, and activity limits help recovery (Children’s Minnesota, n.d.).
Brain Contusions and Bleeds
Brain contusions are bruises on the brain from impacts. They cause swelling and can lead to bleeding. Symptoms depend on location but include confusion, weakness, or coma (Bailes & Cantu, 2001).
Intracranial hematomas are blood clots inside the skull. Types include:
Epidural Hematoma: From artery tears, often with skull fractures. It begins with a lucid period, followed by headache and confusion (Bailes & Cantu, 2001).
Subdural Hematoma: From vein tears, common in sports. It’s the top cause of severe head injury deaths in athletes. Symptoms range from alert to coma (Bailes & Cantu, 2001; Slobounov et al., 2020).
These need CT scans for diagnosis. Treatment may include surgery to remove blood and reduce pressure (WebMD, n.d.).
Sports with the Highest Risk
Some sports have more head injuries due to contact. Football tops the list, with 38.9% of concussions (Neural Effects, n.d.). Soccer, lacrosse, hockey, and wrestling follow (CDC, n.d.). In wrestling, takedowns cause 59% of concussions. Even basketball sees them from collisions.
Other risky sports include boxing, where repeated head blows lead to chronic issues, and cycling from crashes (Arsenian Law Offices, n.d.). Knowing these helps with prevention.
When to Seek Help
Any head hit needs watching. Go to a doctor if you have headaches, confusion, vomiting, or seizures (Cleveland Clinic, n.d.). Emergency signs include loss of consciousness, fluid from the ears, or worsening symptoms.
For athletes, stop playing right away. Second impacts can cause swelling or death (Cleveland Clinic, 2024).
Treatment and Recovery
Most concussions heal with rest. Avoid screens, exercise, and thinking tasks at first. Gradually add activities (Mayo Clinic, 2024b). Pain meds like acetaminophen help headaches.
For severe injuries, hospital stays, scans, and surgery may be needed (WebMD, n.d.). Recovery follows a 6-stage plan: rest, light exercise, sport drills, non-contact practice, full-contact practice, and then play (Kazl & Giraldo, 2013).
Chiropractic and Integrative Care
Chiropractic care helps with concussion symptoms by fixing spine misalignments from the injury. These can cause neck pain, headaches, and nerve issues. Adjustments improve alignment, reduce inflammation, and boost blood flow to the brain (Aurora Chiropractic, n.d.).
It targets musculoskeletal symptoms, such as stiffness, and neurological ones, including dizziness and focus problems. Techniques include spinal manipulation, soft tissue work, and exercises for balance (Mountain Movement Center, n.d.). This supports the body’s natural healing process.
Chiropractors work in teams with doctors, therapists, and nutritionists. Integrative care includes diet changes for anti-inflammation and gradual activity (Think Vida, n.d.). It helps athletes return stronger (Grant Chiropractic, n.d.).
Dr. Alexander Jimenez, a chiropractor with over 30 years of experience, notes that head injuries are frequently associated with spinal issues. He employs integrative methods, such as adjustments and functional medicine, to address root causes, thereby helping patients alleviate pain, improve balance, and promote recovery without surgery (Jimenez, n.d.; LinkedIn, n.d.). His work demonstrates that chiropractic care reduces chronic symptoms and enhances performance.
Prevention Tips
Wear helmets and gear. Learn safe techniques, like proper tackling. Coaches should educate themselves on concussion signs (CDC, n.d.). Rules against head-first contact help too.
Conclusion
Sports head injuries, especially concussions, are serious but manageable with knowledge and care. From causes like blows to treatments including chiropractic, staying informed keeps everyone safe. Always seek help for hits, and use team approaches for the best recovery.
Bailes, J. E., & Cantu, R. C. (2001). Classification of sport-related head trauma: A spectrum of mild to severe injury. Journal of Athletic Training, 36(3), 236–243. https://pmc.ncbi.nlm.nih.gov/articles/PMC155412/
Kazl, C., & Giraldo, C. (2013). Sports chiropractic management of concussions using the Sport Concussion Assessment Tool 2 symptom scoring, serial examinations, and graded return to play protocol: A retrospective case series. Journal of Chiropractic Medicine, 12(4), 252–259. https://pmc.ncbi.nlm.nih.gov/articles/PMC3838718/
Marshall, S., Bayley, M., McCullagh, S., Velikonja, D., & Berrigan, L. (2012). Clinical practice guidelines for mild traumatic brain injury and persistent symptoms. Canadian Family Physician, 58(3), 257–267. https://pmc.ncbi.nlm.nih.gov/articles/PMC3959977/
Slobounov, S. M., Haibach, P., & Newell, K. M. (2020). A foundational “survival guide” overview of sports-related head injuries. Frontiers in Neurology, 11, 571125. https://pmc.ncbi.nlm.nih.gov/articles/PMC7755598/
Find out how chiropractic care for TBI can reduce your tinnitus symptoms and support your health journey effectively.
Understanding Traumatic Brain Injury (TBI): How It Impacts Hearing, Auditory Function, and Sensory Health
Introduction
Traumatic brain injury (TBI) is a significant public health concern that affects millions of people around the world every year. TBIs can range from mild concussions to severe injuries that permanently affect how a person thinks, feels, and interacts with the world. One less-discussed yet important aspect of TBI is its impact on the way we hear and process sound, including issues such as ringing in the ears (tinnitus), hearing loss, and difficulty tolerating everyday noise. These symptoms can significantly impact a person’s quality of life, making it more challenging to communicate, work, or simply enjoy daily activities.
This article will explain what a TBI is, explore how it affects the ears and brain, and examine symptoms such as tinnitus. Additionally, the article features insights from Dr. Alexander Jimenez, a nurse practitioner and chiropractor from El Paso, who specializes in treating injuries resulting from accidents, sports, and workplace incidents. Drawing on scientific research and Dr. Jimenez’s clinical practice, this blog aims to help patients, families, and interested readers gain a deeper understanding of TBI and its impact on sensory health.
What Is Traumatic Brain Injury (TBI)?
Traumatic brain injury (TBI) occurs when a sudden blow or jolt to the head disrupts the brain’s normal functioning. This kind of injury can happen during falls, car crashes, sports accidents, or even violent assaults. TBIs are often classified as mild, moderate, or severe, depending on the force of impact and how long a person loses consciousness or experiences confusion (National Institute of Neurological Disorders and Stroke, 2023).
Common symptoms of TBI include headaches, confusion, dizziness, memory problems, and changes in mood. However, TBIs can also have specific effects on the sensory systems, especially hearing and balance.
How TBI Causes Symptoms Like Ringing in the Ears, Hearing Loss, and Noise Disturbances
The Connection Between TBI and the Auditory System
The auditory system includes the ears, auditory nerves, and the parts of the brain that process sound. When the head receives a blow, the impact can damage any of these parts. For example, the force may injure the delicate inner ear structures or the nerves that transmit sound signals to the brain. Even if there is no direct injury to the ear, the brain’s processing centers can be affected, leading to hearing problems and abnormal sound perception.
How TBI Leads to Ringing in the Ears (Tinnitus)
A common problem after a TBI is tinnitus, which is the sensation of hearing sounds (such as ringing, buzzing, or hissing) that are not caused by an external source. Tinnitus can be either temporary or long-lasting, and it often accompanies hearing difficulties or sensitivity to certain noises. Researchers have found that up to 53% of TBI patients experience some form of tinnitus, particularly after concussions or blast injuries (Moleirinho-Alves et al., 2023).
TBI may trigger tinnitus in several ways:
Damage to the inner ear or cochlea
Injury to the auditory nerve
Disruption in the brain’s sound-processing areas
Changes in blood flow around the ear and brain
These changes confuse the nervous system, leading it to interpret random signals as sound, which the brain perceives as tinnitus.
Hearing Loss and Noise Sensitivity After TBI
Hearing loss is another common symptom of TBI. It can range from mild difficulty understanding words to complete deafness in one or both ears. After a TBI, people may also notice:
Sounds seem much louder than before (hyperacusis)
Difficulty focusing on conversations in noisy environments
Sensitivity to sudden or loud noises
Some patients develop misophonia, a strong negative reaction to specific sounds, which can occur or worsen after TBI. These noise issues stem from damage to the auditory nerves, the cochlea, or disruptions in the brain’s auditory pathways.
Personal Injury Rehabilitation- Video
How TBI Symptoms Affect Sensory and Cognitive Function
TBIs can disrupt more than just hearing. Because the brain is the body’s control center, damage can interfere with how we process all types of sensory information—including sight, touch, balance, and sound. Some ways TBI disrupts sensory function include:
Difficulty filtering out background noise: This makes it harder to focus and can lead to feeling overwhelmed in crowds or busy environments.
Auditory processing issues: Even if hearing is normal, the brain may misinterpret sounds, making it difficult to understand words, remember instructions, or follow conversations in complex situations.
Cognitive challenges: Memory loss, poor attention, and slower thinking are also common after TBI, especially when sensory symptoms like tinnitus become distracting or distressing.
Associated Symptoms Affecting the Head, Neck, and Ears
Patients with TBI may also experience:
Headaches or migraines
Pain or pressure in the ears
Vertigo (a sensation of spinning or dizziness)
Jaw pain or tightness in the neck muscles
These symptoms often occur together, making it challenging for patients to pinpoint which one is most troubling. The interconnected nerves in the head, neck, and ears mean that an injury to one area can trigger symptoms in the others.
What Is Tinnitus? Causes, Symptoms, and Their Association with TBI
Tinnitus is the medical term for hearing sounds that originate from within the body, not from an external source. It is not a disease, but rather a symptom of an underlying condition, such as hearing loss, ear injury, or a problem in the circulatory system. It can sound like:
Ringing
Buzzing
Hissing
Roaring
Clicking or pulsing
For many people, tinnitus is a temporary condition, but in some cases, it becomes persistent and distressing.
Causes of Tinnitus
Common causes of tinnitus include:
Exposure to loud noises
Age-related hearing loss
Ear infections or injuries
Medications (especially some antibiotics and cancer drugs)
Head or neck injuries (including TBI)
When a TBI is involved, the causes are often:
Damage to hair cells in the cochlea (inner ear)
Injury to the nerves carrying sound signals
Problems in the brain’s auditory centers that interpret these signals
TBIs are uniquely associated with cases where tinnitus begins suddenly after trauma, often alongside headaches, dizziness, or other symptoms.
Symptoms That Often Happen with Tinnitus After TBI
Ringing in the ears can come with other issues, including:
Hearing loss
Difficulty concentrating
Trouble sleeping
Irritability, anxiety, or depression
When these symptoms cluster together, they can significantly disrupt daily life. For people with TBI, tinnitus is not just a simple annoyance—it can be a constant reminder of their injury and complicate recovery.
How TBI-Related Auditory Symptoms Are Diagnosed and Treated
Clinical Insights From Dr. Alexander Jimenez, DC, APRN, FNP-BC
Dr. Alexander Jimenez is a nurse practitioner and chiropractor practicing in El Paso with a unique dual-scope practice. He frequently encounters patients with various head, neck, and spine injuries from:
Work incidents
Sports accidents
Personal or home injuries
Motor vehicle accidents (MVAs)
His approach combines medical diagnosis with chiropractic care, focusing on the whole body’s recovery—not just a single symptom or injury.
A TBI Symptom Questionnaire Example:
Dual-Scope Diagnosis and Advanced Imaging
Dr. Jimenez’s clinic starts with a comprehensive evaluation, which may include:
Physical and neurological exams
Advanced imaging such as MRI or CT, to assess brain, spine, and ear structures
Specialized auditory and vestibular function tests to pinpoint hearing and balance problems associated with TBI
This thorough assessment helps distinguish between injuries that directly affect the ear (such as a ruptured eardrum) and those that impact the brain’s processing of sound.
Integrative Treatment Strategies
After diagnosis, Dr. Jimenez uses a combination of evidence-based care options, such as:
Targeted chiropractic adjustments to support neck and spine alignment, which may alleviate headaches and ear pressure
Physical therapy and custom exercise programs to improve balance, coordination, and general brain function
Massage therapy to reduce muscle tension in the neck and jaw, which can worsen auditory symptoms
Integrative medicine, including acupuncture, nutritional counseling, and stress management, supports the natural healing of injured nerve tissues and reduces chronic pain
Medical management, coordinated with other providers, for severe or persistent symptoms
Dr. Jimenez’s team works closely with patients to address not only the physical symptoms but also the cognitive and emotional challenges that accompany TBI. Legal documentation and communication with attorneys or employers are provided as needed for those dealing with workplace or accident-related injuries.
Real-Life Impact: How TBI Symptoms Can Disrupt Daily Living
Living with a TBI is challenging, especially when auditory problems like tinnitus or hearing loss develop. Everyday situations, such as talking with friends in a crowded restaurant or watching TV at a comfortable volume, can become stressful. For some, the persistent ringing of tinnitus makes it difficult to concentrate or relax enough to fall asleep. These issues, combined with headaches, neck pain, or vertigo, can affect a person’s mood and relationships, sometimes leading to anxiety or depression.
Promoting Recovery and Preventing Long-Term Problems
While not every TBI symptom can be cured, early intervention and comprehensive care can make a huge difference. Steps that help include:
Early and accurate diagnosis, including detailed assessment of hearing and sensory function
Personalized treatment plans that integrate medical, rehabilitative, and holistic approaches
Ongoing support for both physical and emotional needs, as recovery can be a long process
Safe return-to-activity programs, especially for those injured during sports or work
Prevention is also crucial. Wearing helmets, using seatbelts, and practicing safety in sports and workplaces can reduce the risk of TBIs and the sensory problems that may follow.
Conclusion
Traumatic brain injury is a serious health condition that affects far more than just the brain. When a person suffers a TBI, the damage can ripple through multiple sensory systems, particularly the auditory system responsible for hearing and sound processing. Ringing in the ears, hearing loss, noise sensitivity, and difficulty understanding speech are not uncommon side effects that many TBI survivors face during their recovery journey. The connection between TBI and hearing problems like tinnitus is scientifically well-established. Research indicates that the mechanisms underlying these symptoms—whether resulting from direct damage to the inner ear, injury to the auditory nerves, or disruption in the brain’s sound-processing centers—are complex and highly individual. This means that two people with similar TBIs may experience completely different hearing-related symptoms, requiring personalized diagnostic approaches and treatment plans.
What makes TBI-related auditory symptoms particularly challenging is that they often occur alongside other complications such as headaches, dizziness, cognitive problems, and emotional difficulties. This combination can significantly impact a person’s ability to work, socialize, and enjoy activities that once brought them joy. For many TBI survivors, managing these interconnected symptoms becomes a central focus of their recovery. The good news is that advances in medical care, integrative treatment approaches, and specialized rehabilitation have created new pathways for healing. Healthcare professionals, such as Dr. Alexander Jimenez, who combine medical expertise with comprehensive chiropractic and integrative medicine, demonstrate how a whole-body approach can address the root causes of injury rather than just treating symptoms in isolation. Through targeted exercise, manual therapy, advanced diagnostic imaging, and personalized care plans, patients can work toward regaining function and improving their overall quality of life.
If you or someone you know has experienced a head injury or is dealing with sudden hearing problems, ringing in the ears, or other sensory disturbances, seeking professional evaluation is an important first step. Early diagnosis and comprehensive treatment can significantly impact recovery outcomes and long-term health. With proper medical support, integrative care, and time, many TBI survivors find ways to adapt, heal, and move forward with their lives.
References
Moleirinho-Alves, P. et al. (2023). “Traumatic brain injury and tinnitus: prevalence, risk factors, pathophysiology, and treatment.” https://pubmed.ncbi.nlm.nih.gov/38775672/
Discover key nutritional guidelines for head injuries. Support your healing process with the right dietary choices today.
Healing the Brain After Injury: How Nutrition Supports Recovery from Traumatic Brain Injury
Understanding Traumatic Brain Injury
Traumatic brain injury (TBI) is a serious medical condition that affects millions of people worldwide. A TBI happens when an outside force injures the brain, often from a blow to the head, a fall, a car accident, or a sports collision (Maas et al., 2022). These injuries range from mild concussions to severe trauma that can change someone’s life forever. In the United States alone, TBI is a leading cause of death and disability, affecting approximately 5.3 million Americans who live with long-term challenges from their injuries (Conti et al., 2024). When the brain experiences trauma, the damage goes far beyond the initial impact. The injury triggers a cascade of biological events within the brain that can persist for days, weeks, or even months afterward. These processes include inflammation, oxidative stress (damage from unstable molecules called free radicals), changes in how brain cells communicate, and disruptions to the brain’s energy systems (Wu et al., 2007). Understanding these mechanisms is crucial because it enables us to identify effective ways to support recovery, particularly through targeted nutrition and lifestyle adjustments.
Dr. Alexander Jimenez, DC, APRN, FNP-BC, a dual-licensed chiropractor and board-certified Family Practice Nurse Practitioner in El Paso, Texas, brings over 25 years of expertise to treating patients with traumatic brain injuries and other complex injuries (A4M, n.d.). His unique clinical approach combines the biomechanical focus of chiropractic care with the diagnostic and therapeutic capabilities of a nurse practitioner, allowing him to address both the structural and systemic aspects of brain injury recovery. Dr. Jimenez’s practice emphasizes non-invasive treatment protocols, functional medicine assessments, and personalized care plans that incorporate nutrition, targeted supplementation, and rehabilitative therapies to support natural healing processes.
Common Symptoms of TBI: Focus on Nausea
The symptoms of traumatic brain injury vary depending on the severity of the injury, but several common signs appear across different types of TBI. These symptoms can be grouped into physical, sensory, and cognitive categories (Mayo Clinic, 2021). Physical symptoms often include headaches, which are the most frequently reported complaint after a brain injury. Nausea and vomiting are also extremely common, affecting many people immediately after the injury and sometimes persisting for weeks or months (Brain Injury Law of Seattle, 2025). Other physical symptoms include fatigue, drowsiness, speech difficulties, and dizziness or loss of balance. Sensory symptoms can involve blurred vision, double vision, ringing in the ears, sensitivity to light or sound, and changes in the ability to smell or taste. Cognitive symptoms may include confusion, memory problems, difficulty concentrating, and mood changes such as anxiety or depression.
Why Nausea Occurs After TBI
Nausea is particularly troubling for people recovering from TBI because it can interfere with eating, taking medications, and participating in rehabilitation activities. Understanding why nausea happens after a brain injury helps us develop better strategies to manage it.
Several mechanisms contribute to nausea following TBI (Brain Injury Law of Seattle, 2025; Complete Concussions, 2024):
Brainstem involvement: The brainstem controls many automatic bodily functions, including the vomiting reflex. When trauma affects this area, it can cause persistent nausea that continues long after the initial injury. If nausea lasts for weeks or gets worse over time, it may signal serious brainstem dysfunction that requires immediate medical evaluation.
Vestibular dysfunction: The vestibular system, located in the inner ear, helps control balance and spatial orientation. TBI can disrupt this system, leading to dizziness, motion sensitivity, and nausea. People with vestibular problems after TBI often feel worse when they move their heads or bodies in certain ways.
Increased intracranial pressure (ICP): After a head injury, swelling or bleeding inside the skull can increase pressure on the brain. This elevated pressure triggers persistent nausea, vomiting, and severe headaches. Increased ICP is a medical emergency that requires immediate treatment.
Neurochemical imbalance: TBI disrupts the brain’s natural balance of chemical messengers called neurotransmitters. These imbalances can lead to nausea, dizziness, mood changes, and other symptoms. When these chemical imbalances persist, nausea can become chronic and difficult to treat.
Vomiting after a head injury deserves special attention. While a single episode of vomiting may not indicate serious problems, persistent or repeated vomiting can signal a brain bleed, dangerous pressure buildup, or other serious complications (Complete Concussions, 2024). Anyone experiencing persistent vomiting after a head injury should seek medical care immediately. At Dr. Jimenez’s Injury Medical & Chiropractic Clinic in El Paso, patients with TBI receive comprehensive assessments that evaluate the underlying causes of symptoms, including nausea, such as vestibular dysfunction, cervical spine misalignments, and neurological imbalances. Through targeted chiropractic adjustments, acupuncture, and electro-acupuncture techniques, Dr. Jimenez addresses the physical manifestations of brain injury while supporting the body’s natural healing mechanisms (dralexjimenez.com, 2025).
How TBI Affects Nutritional Habits
Beyond the immediate symptoms, traumatic brain injury creates significant challenges for maintaining proper nutrition. These challenges can make recovery more difficult and slow the healing process.
Disrupted Communication Between Brain and Gut
Some TBI injuries affect appetite because the brain may not properly communicate with the digestive system (UCLA Health, 2022). The gut-brain axis—a bidirectional communication system between the central nervous system and the gastrointestinal tract—can be severely disrupted after brain trauma. This makes it difficult for people to recognize when they are hungry or full, leading to either inadequate food intake or excessive eating.
Research shows that digestive system disorders after TBI are closely related to cognitive function, depression, and other neurological conditions (PMC, 2024). The gut microbiome—the community of bacteria and other microorganisms living in the digestive tract—plays a crucial role in this relationship. After TBI, changes in the gut microbiome can worsen brain injury outcomes and even contribute to chronic neurological damage.
Swallowing Difficulties
After TBI, damage to the brainstem, cerebellum, or thalamus, or increased pressure inside the skull, can make swallowing difficult (PMC, 2024). Loss of consciousness and cognitive decline can also affect swallowing function. These swallowing disorders, called dysphagia, create serious risks because they can lead to choking, aspiration (food or liquid entering the lungs), and pneumonia.
People with dysphagia often need specialized diets with modified food textures to eat safely. The International Dysphagia Diet Standardization Initiative (IDDSI) provides guidelines for thickening liquids and modifying solid foods to help individuals with swallowing difficulties eat safely during rehabilitation (PMC, 2024).
Weight Changes and Eating Disorders
Weight management becomes a major concern after TBI. Patients hospitalized with severe TBI often lose significant amounts of weight, even when they receive nutrition through feeding tubes (Consultant360, 2021). However, after discharge, many people gain excessive weight. Research shows that eating disorders are common after TBI, largely due to hyperphagia (excessive hunger or food intake) and dysexecutive syndrome (loss of brain function that impairs judgment, planning, and insight).
Dr. Jimenez’s functional medicine approach includes detailed nutritional assessments that evaluate how TBI has affected eating patterns, metabolism, and nutrient absorption. His clinic uses the Living Matrix Functional Medicine Assessment to identify nutritional deficiencies, metabolic imbalances, and digestive dysfunction that may be hindering recovery. By addressing these root causes, Dr. Jimenez helps patients restore healthy eating habits and support their brain’s healing process (dralexjimenez.com, 2025).
Impact on Cognitive Function
The relationship between TBI and cognitive function is complex and far-reaching. Cognitive impairments can persist long after the physical symptoms of injury have resolved, affecting memory, attention, processing speed, executive function, and emotional regulation.
Memory and Learning Difficulties
TBI damages the hippocampus and other brain regions critical for forming and storing memories. Research demonstrates that omega-3 fatty acids, particularly docosahexaenoic acid (DHA), can improve cognitive function after traumatic brain injury by supporting synaptic membrane fluidity and function (Wu et al., 2004). DHA is a major component of neuronal membranes at sites where brain cells communicate, making it vital for learning and memory.
Brain-derived neurotrophic factor (BDNF) plays a crucial role in cognitive recovery after TBI. BDNF acts like a fertilizer for the brain, promoting the growth and survival of neurons, supporting the connections between brain cells, and facilitating learning and memory (Gomez-Pinilla & Kostenkova, 2008). Dietary interventions can influence BDNF levels, offering a non-invasive approach to support cognitive recovery.
Attention and Processing Speed
People recovering from TBI often struggle with attention and mental processing speed. They may struggle to focus on tasks, filter out distractions, or process information efficiently. These difficulties can persist even after mild TBI (concussion) and can significantly impact work, school, and daily activities.
Executive Function Challenges
Executive functions are the high-level cognitive skills we use to plan, organize, make decisions, and control our behavior. TBI frequently impairs these abilities, resulting in difficulties with judgment, impulse control, planning, and problem-solving. These impairments can contribute to poor nutritional choices and difficulty adhering to healthy eating plans.
Emotional and Psychiatric Symptoms
Anxiety and depressive disorders are extremely common among people who have sustained a TBI, with as many as 70% of patients experiencing anxiety and up to 50% experiencing depression (Consultant360, 2021). These mood disorders can have a profound impact on eating patterns and food choices, often leading to weight gain and obesity. Depression symptoms can be intensified by a poor diet, creating a vicious cycle where inadequate nutrition worsens mental health, which in turn leads to poorer food choices.
Dr. Jimenez’s integrative treatment approach addresses the cognitive and emotional aspects of TBI recovery through a combination of chiropractic care, functional medicine, and stress management techniques. His clinic offers personalized wellness programs that include cognitive rehabilitation exercises, nutritional counseling, and natural therapies to support mental clarity, emotional balance, and overall brain health (dralexjimenez.com, 2025).
The Non-Surgical Approach to Wellness with Chiropractic Care- Video
The Brain-Gut Connection in TBI Recovery
Understanding the brain-gut connection is key to optimizing nutrition after TBI. The gut and brain communicate constantly through multiple pathways, including the vagus nerve, immune system molecules, gut hormones, and the gut microbiome.
The Gut Microbiome’s Role
The gut microbiome comprises trillions of microorganisms that play crucial roles in metabolism, immune function, and neuronal function (Clark & Mach, 2016). Recent research shows that physical and emotional stress during recovery can change the composition of gut bacteria. These changes can impact brain function, intestinal barrier integrity, and immune responses—all of which are crucial for TBI recovery.
Studies in animal models demonstrate that exercise-induced stress decreased certain beneficial bacteria while increasing bacteria that degrade the intestinal mucus layer and affect immune function (Clark & Mach, 2016). In the context of TBI, maintaining a healthy gut microbiome through proper nutrition becomes even more crucial because gut health has a direct impact on brain recovery.
Gut Hormones and Cognitive Function
Several gut hormones influence emotions and cognitive processes (Gomez-Pinilla, 2008). Leptin, produced by fat tissue, helps regulate appetite and also supports synaptic plasticity—the brain’s ability to form and reorganize connections between neurons. Ghrelin, secreted by an empty stomach, not only stimulates appetite but also promotes the formation of new connections between brain cells, thereby enhancing learning and memory. Glucagon-like peptide 1 (GLP1), produced by intestinal cells, regulates energy metabolism and has been shown to improve memory in animal studies.
Fermented Foods for Gut-Brain Health
Research increasingly shows that fermented foods support both gut health and brain health (UCLA Health, 2022). Fermented foods, such as sauerkraut, pickles, yogurt, and kefir, contain beneficial probiotics that help maintain a diverse and healthy gut microbiome. Prebiotic foods—such as onions, bananas, and whole grains—provide the fuel that good bacteria need to thrive.
Dr. Jimenez’s nutritional protocols emphasize the importance of gut health in neurological recovery. His functional medicine assessments often include evaluation of digestive function, gut microbiome diversity, and food sensitivities that may be contributing to inflammation and hindering brain healing (dralexjimenez.com, 2025).
Nutritional Foods That Support Brain Function
Certain foods have been identified as particularly beneficial for brain health and recovery from TBI. Understanding which foods to emphasize can help people recovering from brain injuries make informed choices that support healing.
Omega-3 Fatty Acids
Omega-3 fatty acids, particularly DHA and eicosapentaenoic acid (EPA), are among the most important nutrients for brain health (Gomez-Pinilla, 2008). These healthy fats are abundant in fatty fish like salmon, sardines, mackerel, and trout. They serve multiple functions in brain recovery:
Membrane structure: DHA is a major component of neuronal membranes, making up a significant portion of the brain’s structure.
Anti-inflammatory effects: Omega-3s reduce inflammation in the brain, which is critical because inflammation contributes to ongoing damage after TBI.
Oxidative stress reduction: Research indicates that omega-3 supplementation can reduce oxidative damage resulting from trauma (Wu et al., 2004).
BDNF support: Omega-3 fatty acids elevate levels of BDNF, supporting cognitive function and neural recovery.
For people who don’t eat fish, alternative sources include walnuts, flaxseeds, chia seeds, and microalgae supplements. However, the omega-3s found in plant sources (alpha-linolenic acid, or ALA) are not as readily used by the brain as the EPA and DHA found in fish (UCLA Health, 2022).
Berries and Antioxidants
Berries—particularly blueberries, strawberries, and blackberries—contain powerful antioxidants called flavonoids that give them their vibrant colors (Harvard Health, 2021). Research shows that women who consumed two or more servings of strawberries and blueberries per week experienced a delay in memory decline of up to two and a half years.
Flavonoids work through several mechanisms:
They increase blood flow to the brain
They improve neuronal function
They promote neuroplasticity—the brain’s ability to reorganize and form new connections
They reduce oxidative stress and inflammation
Leafy Green Vegetables
Green, leafy vegetables such as kale, spinach, collards, and broccoli are rich in brain-healthy nutrients like vitamin K, lutein, folate, and beta-carotene (Harvard Health, 2021). Research suggests these plant-based foods may help slow cognitive decline. Vitamin K plays a role in forming certain fats that are concentrated in brain cells, while lutein and folate support cognitive function in older adults.
Nuts and Seeds
Nuts are excellent sources of protein, healthy fats, and vitamin E—all important for brain health (Harvard Health, 2021). Walnuts deserve special attention because they contain high levels of alpha-linolenic acid (ALA), a plant-based omega-3 fatty acid. Research from UCLA linked higher walnut consumption to improved cognitive test scores. Walnuts, along with other nuts like almonds and hazelnuts, are also rich in vitamin E, a powerful antioxidant that protects brain cells from oxidative damage. Pumpkin seeds provide zinc, magnesium, iron, and tryptophan—an amino acid that helps produce serotonin, a neurotransmitter involved in mood regulation (Salmon Health, 2023).
Whole Grains
Complex carbohydrates from whole grains, such as brown rice, quinoa, oats, and whole wheat bread, provide steady energy for the brain (Headway UK, n.d.). Unlike refined grains and sugars that cause rapid spikes and crashes in blood sugar, whole grains release energy slowly, helping to maintain stable energy levels throughout the day. This is especially helpful for people experiencing fatigue after TBI.
Healthy Fats: Olive Oil and Avocados
Olive oil, a cornerstone of the Mediterranean diet, has been shown to have a range of health benefits, including protective effects on memory function (Headway UK, n.d.). Avocados provide healthy monounsaturated fats, along with potassium and lutein, which support brain health (Rezilir Health, 2025).
Eggs and Choline
Eggs are one of the best dietary sources of choline, a vital nutrient essential for producing acetylcholine, a neurotransmitter involved in memory, mood regulation, and muscle control (UCI Health, 2025). Adequate choline intake has been linked to enhanced cognitive performance and may help protect against age-related memory decline. Eggs also contain B vitamins like B12, which help reduce homocysteine levels—an amino acid that, when elevated, can damage blood vessels and increase risk for stroke and dementia.
Turmeric and Curcumin
Turmeric, a yellow curry spice, contains curcumin, which has been shown to enhance recovery after brain trauma (Gomez-Pinilla & Kostenkova, 2008). Curcumin displays particular effectiveness in preserving cognitive function through several mechanisms:
Reducing oxidative stress
Protecting against lipid peroxidation (damage to cell membranes)
Neutralizing harmful free radicals
Reducing inflammation in the brain
Studies have shown that curcumin supplementation reduced the effects of experimental concussive injury on cognitive function in animal models (Wu et al., 2006).
Dark Chocolate
Dark chocolate contains flavonoids, caffeine, and theobromine—compounds that can improve cognitive function (Senior Lifestyle, 2025). Flavonoids increase blood flow to the brain, improve neuronal function, and promote neuroplasticity. Moderate consumption of dark chocolate has been linked to improved memory, attention, and overall cognitive function.
The Mediterranean Diet for Brain Health
Among various dietary patterns studied for brain health, the Mediterranean diet has emerged as particularly beneficial for people recovering from TBI (UCLA Health, 2022). This eating pattern, traditionally followed in countries bordering the Mediterranean Sea, emphasizes:
High portions of fruits and vegetables
Whole grains
Legumes (beans, lentils, chickpeas)
Nuts and seeds
Fish and seafood (at least twice per week)
Olive oil is the primary source of added fat
Moderate consumption of poultry
Limited intake of red meat and dairy products
Herbs and spices for flavoring instead of salt
Research suggests that the Mediterranean diet is associated with fewer signs of Alzheimer’s disease in the brains of older adults (NIA, 2023). Green leafy vegetables, in particular, were associated with less brain pathology. The MIND diet—a hybrid of the Mediterranean and DASH (Dietary Approaches to Stop Hypertension) diets specifically designed to support brain health—builds on these principles with additional emphasis on berries and green leafy vegetables (Mass General Hospital, 2025).
Dr. Jimenez often recommends a Mediterranean dietary pattern to his TBI patients, recognizing that this style of eating provides comprehensive support for brain health while reducing inflammation throughout the body (dralexjimenez.com, 2025).
Essential Vitamins and Supplements
Beyond whole foods, certain vitamins and supplements have shown promise in supporting brain function and recovery after TBI.
B Vitamins
B vitamins play crucial roles in brain health (Gomez-Pinilla, 2008):
Vitamin B6: Supports neurotransmitter production and has positive effects on memory performance
Vitamin B12: Essential for neurological health; deficiency has been linked to cognitive decline
Folate (B9): Critical for neurotransmitter function and DNA repair; deficiency can lead to depression and cognitive impairment
Supplementation with B vitamins has been shown to prevent cognitive decline and dementia during aging and can enhance the effects of antidepressants (Gomez-Pinilla, 2008). Foods rich in B vitamins include leafy greens (folate), fish, poultry, eggs (B12), and fortified grains.
Vitamin D
Vitamin D is crucial for maintaining cognitive function in older adults and appears to play a significant role in brain health (Gomez-Pinilla, 2008). Sources include fatty fish, mushrooms exposed to sunlight, and fortified products like milk and cereals. Many people, especially those recovering from TBI who may spend more time indoors, need vitamin D supplementation.
Vitamin E
Vitamin E functions as an antioxidant, reducing free radicals in the brain that would otherwise impede optimal neuronal function (Gomez-Pinilla & Kostenkova, 2008). Studies show that vitamin E ameliorates cognitive impairment after brain trauma in animal models and reduces cognitive decline in older adults. Food sources include nuts, seeds, spinach, avocado, and vegetable oils.
Magnesium
Magnesium plays a crucial role in nerve transmission and neuroplasticity—the brain’s ability to adapt and reorganize (UCI Health, 2025). Magnesium deficiency is common and can contribute to anxiety, depression, and cognitive problems. Good sources include leafy greens, nuts, seeds, legumes, and whole grains.
Creatine
Creatine supplementation shows promise for improving brain health, particularly in conditions characterized by brain creatine deficits (Roschel et al., 2021). These deficits can be induced by acute stressors like sleep deprivation or chronic conditions like mild traumatic brain injury. Creatine supports cognitive processing and may help with recovery from brain trauma, though the optimal protocol for increasing brain creatine levels is still being determined (Conti et al., 2024).
Omega-3 Supplements
For individuals who don’t consume adequate amounts of fatty fish, omega-3 supplements (such as fish oil or microalgae-based DHA/EPA) can help ensure an adequate intake of these critical fatty acids (Conti et al., 2024). Research indicates that omega-3 supplementation can help decrease inflammation, mitigate neural damage, and maintain a sufficient energy supply to the brain following injury.
Melatonin
Melatonin supplementation may help alleviate sleep disturbances commonly experienced after TBI (Conti et al., 2024). Since quality sleep is essential for brain recovery and the consolidation of memories, addressing sleep problems through melatonin or other interventions is a crucial part of comprehensive TBI treatment.
Other Promising Supplements
Additional supplements being investigated for TBI recovery include (Conti et al., 2024):
N-Acetylcysteine (NAC): An antioxidant that may reduce oxidative stress
Branched-chain amino acids (BCAAs): May influence mental performance, though evidence is mixed
Riboflavin (Vitamin B2): May help with migraine headaches common after TBI
Choline: Supports production of acetylcholine, a neurotransmitter critical for memory
Berry anthocyanins: Powerful antioxidants found in berries
Boswellia serrata: An anti-inflammatory botanical
Enzogenol: A pine bark extract with antioxidant properties
It’s essential to note that while supplements may be necessary for some individuals, it is crucial to consult your doctor or dietitian before taking them, as they could interact with medications or have other unintended effects (Headway UK, n.d.).
Dr. Jimenez’s functional medicine approach includes comprehensive nutritional testing to identify specific deficiencies and imbalances that may be hindering recovery. His personalized supplementation protocols are based on individual patient needs, genetics, and the severity of injury, ensuring that each patient receives targeted nutritional support for optimal healing (dralexjimenez.com, 2025).
Foods to Limit or Avoid
Just as certain foods support brain health, others can hinder recovery from TBI. While it’s important not to create overly restrictive diets that may be difficult to follow, being mindful of these foods can support better outcomes.
Saturated Fats and Trans Fats
Diets high in saturated fats have been shown to have an adverse effect on cognition (Gomez-Pinilla, 2008). Studies show that “junk food” diets—characterized by high contents of saturated fat and refined sugars—lead to a decline in cognitive performance and reduced levels of BDNF-related synaptic plasticity after just three weeks. Even more concerning, these diets elevated the neurological burden associated with experimental brain injury, resulting in worse performance in learning tasks.
Foods high in saturated fats include butter, cream, cheese, fatty meats, coconut oil, and palm kernel oil. Trans fats, found in many processed and fried foods, are particularly harmful and should be avoided.
Refined Sugars and Processed Foods
Sugar can cause weight gain and other health problems, and can cause “sugar crashes” where energy levels drop rapidly—a particular problem for people experiencing fatigue after TBI (Headway UK, n.d.). Highly processed foods often contain high amounts of salt and sugar, tend to have lower nutritional content, and may lead to weight gain.
Excessive Sodium
Salt is known to raise blood pressure and increase the risk of stroke (Headway UK, n.d.). Many people with taste and smell problems after TBI add more salt than they should. Using alternatives such as lemon juice, herbs, and spices can enhance flavor without the negative health effects associated with excess sodium.
Alcohol
Alcohol should be avoided or consumed very minimally during TBI recovery. Alcohol can interfere with healing processes, interact with medications, worsen cognitive symptoms, and increase fall risk.
Excessive Caffeine
While moderate caffeine consumption may offer cognitive benefits, excessive intake can have negative effects, particularly for people who experience urinary symptoms or sleep disturbances after brain injury (Headway UK, n.d.). Caffeine can also increase anxiety in some individuals.
Easy Brain-Boosting Recipes
Incorporating brain-healthy foods into daily meals doesn’t have to be complicated. Here are some simple, nutritious recipes designed to support neurological recovery:
Blueberry Walnut Overnight Oats
This make-ahead breakfast is perfect for busy mornings and is packed with brain-boosting nutrients.
Ingredients:
1/2 cup rolled oats
1/2 cup milk (dairy or plant-based)
1/4 cup plain Greek yogurt
1/2 cup fresh blueberries
2 tablespoons chopped walnuts
1 teaspoon honey (optional)
1/2 teaspoon vanilla extract
Instructions:
In a mason jar or bowl, mix the oats, milk, yogurt, honey, and vanilla
Top with blueberries and walnuts
Cover and refrigerate overnight
Enjoy it cold in the morning
Why it’s good for your brain: Blueberries provide antioxidants that promote brain health, while walnuts contain omega-3 fatty acids that support memory and focus. Oats provide steady energy, and Greek yogurt offers protein and probiotics for gut health.
Wild Salmon and Greens Power Bowl
This nutrient-dense bowl combines multiple brain-healthy ingredients in one satisfying meal.
Ingredients:
4 oz wild-caught salmon
2 cups mixed greens (arugula, spinach, romaine)
1/2 cup steamed broccoli
1/4 avocado, sliced
1/4 cup blueberries
1 tablespoon walnuts, chopped
2 teaspoons ground flaxseed
For the Turmeric-Tahini Dressing:
1 tablespoon tahini
1 teaspoon turmeric
Pinch of black pepper
1 teaspoon fresh lemon juice
1 teaspoon extra-virgin olive oil
Water to thin
Instructions:
Season salmon with salt and pepper; heat 1 teaspoon olive oil in a skillet over medium heat
Place salmon skin-side down; cook 4-5 minutes, flip and cook 3-4 minutes more until flaky
Steam broccoli florets for 4-5 minutes until bright green and tender
Whisk together dressing ingredients, adding water to reach the desired consistency
Layer greens in a bowl; top with broccoli, avocado, blueberries, walnuts, and flaxseed
Add salmon and drizzle with dressing
Why it’s good for your brain: Salmon provides EPA and DHA omega-3s that build neuronal membranes and reduce inflammation. Leafy greens offer folate, vitamin K, and natural nitrates that boost blood flow to the brain. Broccoli contains sulforaphane, which triggers antioxidant defenses. Turmeric’s curcumin helps reduce inflammation, while blueberries offer powerful antioxidants.
Spinach and White Bean Frittata
This protein-rich breakfast or lunch option is loaded with brain-healthy nutrients.
Ingredients:
6 eggs
1/4 cup milk
2 cups fresh spinach, chopped
1 cup cooked white beans (cannellini)
1/2 cup cherry tomatoes, halved
1/2 teaspoon turmeric
1/4 cup feta cheese (optional)
2 tablespoons olive oil
Salt and pepper to taste
Instructions:
Preheat oven to 375°F
In a bowl, whisk eggs, milk, turmeric, salt, and pepper
Heat olive oil in an oven-safe skillet over medium heat
Add spinach and cook until wilted
Add white beans and tomatoes; cook for 2 minutes
Pour the egg mixture over the vegetables
Cook without stirring for 4-5 minutes until edges begin to set
Sprinkle with feta if using
Transfer to oven and bake 12-15 minutes until center is set
Why it’s good for your brain: Eggs provide choline for memory and acetylcholine production, plus B vitamins to reduce homocysteine. Spinach offers folate, vitamin K, and lutein to slow cognitive decline. White beans provide magnesium for nerve transmission and plant-based protein to support stable blood sugar levels.
Mediterranean Chickpea and Vegetable Stew
This hearty, flavorful stew is perfect for meal prep and freezes well.
Ingredients:
2 tablespoons olive oil
1 onion, diced
3 cloves garlic, minced
2 sweet potatoes, cubed
2 cans (15 oz each) chickpeas, drained
1 can (14 oz) diced tomatoes
4 cups vegetable broth
2 cups fresh spinach
1 teaspoon cumin
1 teaspoon paprika
1/2 teaspoon turmeric
1/2 teaspoon cinnamon
Juice of 1 lemon
Salt and pepper to taste
Instructions:
Heat olive oil in a large pot over medium heat
Add onion and cook until softened, about 5 minutes
Add garlic and spices; cook 1 minute until fragrant
Add sweet potatoes, chickpeas, tomatoes, and broth
Bring to a boil, then reduce the heat and simmer 20-25 minutes until the sweet potatoes are tender
Stir in spinach until wilted
Add lemon juice and adjust seasonings
Serve warm
Why it’s good for your brain: Chickpeas provide fiber, folate, iron, and magnesium. Sweet potatoes offer antioxidants, B vitamins, and vitamin C. Spinach adds more folate and antioxidants. The spices (cumin, turmeric) provide anti-inflammatory compounds.
Brain-Boosting Berry Smoothie
A quick, easy option for breakfast or snacks.
Ingredients:
1 cup mixed berries (blueberries, strawberries, blackberries)
1/2 banana
1 cup spinach
1 tablespoon almond butter
1 tablespoon ground flaxseed
1 cup unsweetened almond milk
1/2 cup plain Greek yogurt
1/2 teaspoon cinnamon
Ice cubes
Instructions:
Add all ingredients to a blender
Blend until smooth
Add more liquid if needed for the desired consistency
Pour into a glass and enjoy immediately
Why it’s good for your brain: Berries provide flavonoids and antioxidants for brain health. Spinach adds folate and vitamin K without affecting taste. Almond butter and flaxseed provide healthy fats and omega-3s. Greek yogurt offers protein and probiotics.
Walnut-Crusted Baked Salmon
An elegant but simple preparation that maximizes brain-healthy nutrients.
Ingredients:
1 lb skinless salmon fillet
2 teaspoons Dijon mustard
1 clove garlic, minced
1/4 teaspoon lemon zest
1 teaspoon lemon juice
1 teaspoon chopped fresh rosemary
1/2 teaspoon honey
1/4 teaspoon crushed red pepper
3 tablespoons panko breadcrumbs
3 tablespoons finely chopped walnuts
1 teaspoon extra-virgin olive oil
Olive oil cooking spray
Instructions:
Preheat oven to 425°F
Line a baking sheet with parchment paper
Mix mustard, garlic, lemon zest, lemon juice, rosemary, honey, and red pepper in a small bowl
In another bowl, combine breadcrumbs, walnuts, and olive oil
Place salmon on the prepared baking sheet
Spread mustard mixture over salmon
Top with the breadcrumb-walnut mixture
Spray lightly with cooking spray
Bake 8-12 minutes until salmon is cooked through
Why it’s good for your brain: Salmon provides omega-3 fatty acids DHA and EPA. Walnuts provide more omega-3s, as well as vitamin E. Garlic offers antioxidants and anti-inflammatory compounds.
Pumpkin Seed and Berry Trail Mix
A convenient brain-boosting snack for on-the-go.
Ingredients:
1 cup raw pumpkin seeds
1/2 cup walnuts
1/2 cup almonds
1/2 cup dried blueberries (unsweetened if possible)
1/4 cup dark chocolate chips (70% cacao or higher)
1/4 cup unsweetened coconut flakes
1 teaspoon cinnamon
1/4 teaspoon nutmeg
1 tablespoon maple syrup
Instructions:
Preheat oven to 325°F
Toss pumpkin seeds, walnuts, and almonds with maple syrup and spices
Spread on a baking sheet
Bake 10-12 minutes, stirring halfway through
Cool completely
Mix with dried blueberries, chocolate chips, and coconut
Store in an airtight container
Why it’s good for your brain: Pumpkin seeds provide zinc, magnesium, and iron. Nuts offer healthy fats and vitamin E. Blueberries add antioxidants. Dark chocolate contains flavonoids that support improved brain function.
Practical Tips for Eating Well After TBI
Making healthy food choices can be challenging when dealing with the effects of brain injury. These practical strategies can help:
Meal Planning and Preparation
Find and save simple recipes that you can return to regularly (Headway UK, n.d.)
Create a weekly meal plan so you know what to prepare each day
Make a shopping list or use online grocery ordering to avoid forgetting items
Batch cook and freeze meals when you have good energy; label containers with contents and date
Shop during optimal times when you feel most alert and when stores are less crowded
Managing Symptoms While Eating
Eat at regular intervals to avoid under-eating or over-eating; don’t skip breakfast (Headway UK, n.d.)
Set alarms as reminders to eat if you experience a loss of appetite
Pay attention to use-by dates if you have problems with taste and smell
Modify food textures if swallowing is difficult; work with a speech therapist or occupational therapist
Stay hydrated by drinking plenty of water throughout the day
Making Healthy Choices Easier
Keep healthy snacks visible and accessible: nuts, cut vegetables, fruit
Use herbs and spices instead of salt for flavor
Choose whole-grain versions of bread, pasta, and rice
Read nutrition labels to understand what’s in packaged foods
Ask for help when needed; use a Brain Injury Identity Card to start conversations about your needs
Dining Out Strategies
When eating at restaurants (Taste of Home, 2023):
Review menus online beforehand to plan your choices
Ask questions about ingredients and preparation methods
Request modifications: grilled instead of fried, dressing on the side, extra vegetables
Control portions by sharing an entrée or taking half home
Choose Mediterranean-style restaurants that emphasize vegetables, fish, and olive oil
Dr. Jimenez’s Clinical Approach to TBI and Injury Recovery
Dr. Alexander Jimenez’s Injury Medical & Chiropractic Clinic in El Paso, Texas, offers a comprehensive, integrative approach to treating patients recovering from traumatic brain injuries and other complex injuries. His dual licensure as both a chiropractor and board-certified Family Practice Nurse Practitioner provides a unique perspective that addresses both the structural and systemic aspects of injury recovery.
Dual-Scope Diagnostic and Treatment Approach
Dr. Jimenez’s practice stands out due to his ability to integrate the biomechanical focus of chiropractic care with the diagnostic and therapeutic scope of a nurse practitioner (A4M, n.d.). As a chiropractor, he specializes in restoring musculoskeletal function, particularly after trauma affecting the neck, back, spine, and soft tissues. His chiropractic interventions emphasize non-invasive techniques such as spinal decompression, manual adjustments, and functional rehabilitation to alleviate pain and enhance mobility.
As a board-certified nurse practitioner, Dr. Jimenez employs evidence-based medicine to address systemic and metabolic dysfunctions. His expertise extends to managing chronic pain syndromes, hormonal imbalances, and metabolic disorders that often accompany brain injuries. This dual perspective enables him to identify the underlying causes of symptoms, ranging from biomechanical misalignments to physiological imbalances, and design treatment regimens that address both symptoms and their root causes.
Treatment of Various Injury Types
Dr. Jimenez’s clinic specializes in treating injuries from multiple sources (dralexjimenez.com, 2025):
Motor vehicle accidents (MVAs): Whiplash, soft tissue injuries, and traumatic brain injuries from car crashes require comprehensive assessment and treatment. Dr. Jimenez provides both immediate injury care and long-term rehabilitation.
Work injuries: Occupational injuries affecting the back, neck, and other body systems receive targeted treatment plans that support return to work while promoting complete healing.
Sports injuries: Athletes recovering from concussions, sprains, strains, and other sports-related trauma benefit from protocols designed to restore function and prevent re-injury.
Personal injuries, including falls, slip-and-fall accidents, and other types of personal injury cases, receive thorough evaluation and individualized treatment approaches.
Functional Medicine Assessments
Dr. Jimenez’s practice embraces Functional Integrative Medicine, a patient-focused approach that treats the whole person, not just symptoms (dralexjimenez.com, 2025). His comprehensive assessments evaluate:
Genetics: Understanding genetic predispositions to certain conditions
Lifestyle factors: Sleep, stress, exercise, and daily habits
Environmental exposures: Toxins and other environmental factors affecting health
Psychological factors: Mood, anxiety, depression, and stress responses
Nutritional status: Deficiencies, imbalances, and dietary patterns
The clinic utilizes the Living Matrix Functional Medicine Assessment and the Institute for Functional Medicine’s Collaborative Assessment Programs to create comprehensive health profiles for each patient.
Advanced Neuromusculoskeletal Imaging
Dr. Jimenez’s clinic utilizes advanced diagnostic imaging to assess the extent of injuries and track healing progress. This includes specialized neuromusculoskeletal imaging that can identify subtle changes in the spine, soft tissues, and nervous system that may not be apparent on standard imaging studies.
An Example of A TBI Symptom Questionnaire:
Integrated Treatment Modalities
The clinic offers multiple therapeutic approaches that work synergistically (dralexjimenez.com, 2025):
Chiropractic adjustments: Manual adjustments to restore proper spinal alignment and nervous system function
Acupuncture and Electro-Acupuncture: Traditional Chinese medicine techniques to reduce pain, decrease inflammation, and promote healing
Functional rehabilitation: Targeted exercises and therapies to restore strength, flexibility, and function
Nutritional counseling: Personalized dietary recommendations and supplementation protocols
Stress management: Techniques to address the emotional and psychological impacts of injury
Massage therapy: Soft tissue work to reduce muscle tension, improve circulation, and support relaxation
Medical-Legal Documentation
For patients whose injuries resulted from accidents or the negligence of others, Dr. Jimenez provides comprehensive medical-legal documentation (dralexjimenez.com, 2025). His dual training allows him to prepare thorough medical reports that detail:
Mechanism of injury
Initial presentation and symptoms
Diagnostic findings
Treatment provided
Prognosis and long-term implications
Functional limitations and disabilities
This documentation supports patients in legal proceedings and insurance claims related to their injuries.
Collaborative Care Model
Dr. Jimenez recognizes that complex injuries often require input from multiple specialists. He has partnered with top surgeons, medical specialists, and rehabilitation providers in the El Paso area to ensure patients receive the highest standard of care (dralexjimenez.com, 2025). If he believes another specialist is better suited for a patient’s condition, he provides appropriate referrals while coordinating ongoing care.
Prevention and Long-Term Wellness
Beyond treating acute injuries, Dr. Jimenez’s practice emphasizes prevention and long-term wellness. Through education, lifestyle coaching, and ongoing support, patients learn how to:
Prevent re-injury
Maintain healthy spinal alignment
Support optimal brain and body function through nutrition
Manage stress effectively
Incorporate regular exercise and movement
Maintain a healthy body weight
Optimize sleep and recovery
Dr. Jimenez’s mission is to help patients not only recover from injuries but also thrive in El Paso’s beautiful community, achieving improved health, vitality, and quality of life (dralexjimenez.com, 2025).
The Role of Exercise in Brain Recovery
While nutrition is crucial for brain health, combining dietary interventions with regular exercise can further enhance recovery. Research shows that diet and exercise work together synergistically, producing greater effects on brain plasticity and cognitive function than either intervention alone (Gomez-Pinilla & Kostenkova, 2008).
Exercise Benefits for the Brain
Physical activity influences brain health through multiple mechanisms:
The timing of exercise after TBI is important. Research indicates that exercise applied immediately following experimental traumatic brain injury can actually worsen outcomes (Gomez-Pinilla & Kostenkova, 2008). However, exercise started at appropriate times during recovery facilitates healing and improves cognitive function. Patients should work with healthcare providers, such as Dr. Jimenez, to determine when and how to safely reintroduce physical activity after a brain injury. The rehabilitation programs at Dr. Jimenez’s clinic include carefully designed flexibility, mobility, and agility programs tailored to individual recovery stages (dralexjimenez.com, 2025).
Types of Exercise
Cardiovascular exercise appears most beneficial for brain recovery. Studies comparing different exercise types found treadmill running (walking or running) to be most effective for recovery (Gomez-Pinilla & Kostenkova, 2008). Other beneficial activities include:
Walking
Swimming
Cycling
Dancing
Gentle yoga and tai chi (for balance and flexibility)
Combined Effects of Diet and Exercise
The combination of a healthy diet and exercise produces enhanced effects on brain recovery. Studies show that:
Omega-3 fatty acid supplementation combined with exercise (DHA+Exercise) had greater effects on BDNF-mediated synaptic plasticity and cognition than either intervention alone (Gomez-Pinilla & Kostenkova, 2008)
Flavonoid-enriched diets combined with exercise increased the expression of genes supporting neuronal plasticity while decreasing genes involved in inflammation and cell death
Exercise can counteract some deleterious effects of high saturated fat diets on synaptic plasticity and cognitive function
Dr. Jimenez’s integrated approach acknowledges the synergistic relationship between nutrition and physical rehabilitation, resulting in treatment plans that optimize both components for optimal recovery (dralexjimenez.com, 2025).
Sleep and Recovery
Quality sleep is essential for brain recovery after TBI. During sleep, the brain consolidates memories, clears metabolic waste products, and repairs cellular damage. Many people experience sleep disturbances after brain injury, including:
Difficulty falling asleep
Frequent awakening during the night
Early morning awakening
Excessive daytime sleepiness
Altered sleep-wake cycles
Nutritional Support for Sleep
Certain dietary strategies can support better sleep:
Avoid caffeine in the afternoon and evening
Limit alcohol, which disrupts sleep architecture
Eat tryptophan-rich foods like turkey, eggs, cheese, nuts, and seeds
Consider magnesium-rich foods like leafy greens, nuts, and whole grains
Try tart cherry juice, a natural source of melatonin
Avoid heavy, spicy, or large meals close to bedtime
Sleep Hygiene
In addition to nutritional support, good sleep hygiene practices include:
Maintaining a consistent sleep schedule
Creating a dark, cool, quiet sleep environment
Limiting screen time before bed
Engaging in relaxing activities in the evening
Getting regular exercise (but not too close to bedtime)
Dr. Jimenez’s comprehensive approach to TBI recovery includes assessment and management of sleep disturbances, recognizing that quality rest is essential for healing (dralexjimenez.com, 2025).
Conclusion
Traumatic brain injury presents complex challenges that extend far beyond the initial impact. The symptoms—including nausea, cognitive impairments, nutritional difficulties, and emotional changes—can persist for months or years, significantly affecting quality of life. However, emerging research demonstrates that nutrition plays a powerful role in supporting brain recovery and cognitive function. The evidence is clear: what we eat matters for brain health. Omega-3 fatty acids, antioxidant-rich berries, leafy greens, nuts, whole grains, and other nutrient-dense foods provide the building blocks and protective compounds the brain needs to heal. The Mediterranean dietary pattern, emphasizing these foods while limiting saturated fats and processed ingredients, offers a comprehensive nutritional approach supported by extensive research. Beyond whole foods, targeted supplementation with B vitamins, vitamin D, vitamin E, magnesium, and omega-3 fatty acids can address specific deficiencies and support recovery processes. The gut-brain connection underscores the significance of maintaining a healthy digestive system through the consumption of probiotics, prebiotics, and fermented foods. Dr. Alexander Jimenez’s integrative approach in El Paso exemplifies how comprehensive care can support TBI recovery. By combining his expertise as both a chiropractor and nurse practitioner, Dr. Jimenez addresses the structural, metabolic, and nutritional aspects of brain injury. His functional medicine assessments identify root causes of symptoms, while his treatment protocols—including chiropractic adjustments, acupuncture, targeted nutrition, and rehabilitative therapies—support the body’s natural healing processes.
For anyone recovering from TBI, whether from a motor vehicle accident, sports injury, fall, or other trauma, the path to recovery involves multiple components: proper medical care, appropriate rehabilitation, adequate rest, stress management, and—critically—optimal nutrition. By incorporating brain-healthy foods into daily meals, staying hydrated, managing symptoms that interfere with eating, and working with knowledgeable healthcare providers, individuals can support their brain’s remarkable capacity for healing and adaptation. The recipes and strategies outlined in this article offer practical and accessible ways to nourish the brain during recovery. These nutritional interventions, combined with appropriate medical care, physical rehabilitation, and lifestyle modifications, offer hope for improved outcomes and enhanced quality of life after traumatic brain injury. Remember, recovery is a journey that requires patience, persistence, and comprehensive support. With the right nutritional foundation, expert medical care from practitioners like Dr. Jimenez, and a commitment to healing, individuals recovering from TBI can work toward restoring brain function, preventing long-term complications, and living vibrant, fulfilling lives.
Clark, A., & Mach, N. (2016). Exercise-induced stress behavior, gut-microbiota-brain axis, and diet: A systematic review for athletes. Journal of the International Society of Sports Nutrition, 13, 43. https://doi.org/10.1186/s12970-016-0155-6
Conti, F., McCue, J. J., DiTuro, P., Galpin, A. J., & Wood, T. R. (2024). Mitigating traumatic brain injury: A narrative review of supplementation and dietary protocols. Nutrients, 16(15), 2430. https://doi.org/10.3390/nu16152430
dralexjimenez.com. (2025). El Paso, TX, family practice nurse practitioner and chiropractor. Retrieved from https://dralexjimenez.com/
Gómez-Pinilla, F. (2008). Brain foods: The effects of nutrients on brain function. Nature Reviews Neuroscience, 9(7), 568-578. https://doi.org/10.1038/nrn2421
Gomez-Pinilla, F., & Kostenkova, K. (2008). The influence of diet and physical activity on brain repair and neurosurgical outcome. Surgical Neurology, 70(4), 333-336. https://doi.org/10.1016/j.surneu.2008.05.023
Maas, A. I. R., Menon, D. K., Manley, G. T., et al. (2022). Traumatic brain injury: Progress and challenges in prevention, clinical care, and research. The Lancet Neurology, 21(11), 1004-1060. https://doi.org/10.1016/S1474-4422(22)00309-X
Meeusen, R., & Decroix, L. (2018). Nutritional supplements and the brain. International Journal of Sport Nutrition and Exercise Metabolism, 28(2), 200-211. https://doi.org/10.1123/ijsnem.2017-0314
Roschel, H., Gualano, B., Ostojic, S. M., & Rawson, E. S. (2021). Creatine supplementation and brain health. Nutrients, 13(2), 586. https://doi.org/10.3390/nu13020586
Toader, C., Dobrin, N., Costea, D., et al. (2024). Mind, Mood, and Microbiota-Gut-Brain Axis in Psychiatric Disorders. International Journal of Molecular Sciences, 25(6), 3340. https://doi.org/10.3390/ijms25063340
Wu, A., Ying, Z., & Gomez-Pinilla, F. (2004). Dietary omega-3 fatty acids normalize BDNF levels, reduce oxidative damage, and counteract learning disability after traumatic brain injury in rats. Journal of Neurotrauma, 21(10), 1457-1467. https://doi.org/10.1089/neu.2004.21.1457
Wu, A., Ying, Z., & Gomez-Pinilla, F. (2006). Dietary curcumin counteracts the outcome of traumatic brain injury on oxidative stress, synaptic plasticity, and cognition. Experimental Neurology, 197(2), 309-317. https://doi.org/10.1016/j.expneurol.2005.09.004
Wu, A., Ying, Z., & Gomez-Pinilla, F. (2007). Omega-3 fatty acids supplementation restores mechanisms that maintain brain homeostasis in traumatic brain injury. Journal of Neurotrauma, 24(10), 1587-1595. https://doi.org/10.1089/neu.2007.0313
Cerdó, T., Ruiz, A., Suárez, A., & Campoy, C. (2017). Probiotic, prebiotic, and brain development. Nutrients, 9(11), 1247. https://doi.org/10.3390/nu9111247
How Head Injuries Affect Movement—and How Chiropractic Care Gives It Back
A physiotherapist is conducting a consultation on a possible traumatic brain injury; the patient complains of back pain and mobility problems.
Head injuries and traumatic brain injuries (TBIs) can turn simple steps into big challenges. A fall, a car crash, or a sports hit can damage the brain and the nerves that tell your body how to walk, reach, or stand tall. This guide explains exactly how these injuries cause muscle fatigue, shaky balance, stiff joints, and even paralysis. You will also learn how gentle chiropractic adjustments, soft-tissue work, and targeted exercises help people move better, feel less pain, and live fuller lives.
What Happens Inside the Body After a Head Injury
When the skull jolts, the brain bounces inside. That sudden movement can tear tiny nerve wires and swell delicate tissues. The messages that once zipped from brain to legs now arrive late, weak, or not at all (Model Systems Knowledge Translation Center, 2023).
Muscle Fatigue Hits Fast
Even mild TBIs make muscles tire in minutes instead of hours. A short walk to the mailbox can feel like a marathon. Dr. Alexander Jimenez, a chiropractor and nurse practitioner in El Paso, Texas, sees this every week. “Patients tell me their legs feel like wet sandbags after five minutes of standing,” he says in his clinic videos (Jimenez, 2025).
Balance Becomes a Wobbly Game
The brain’s balance center sits deep inside the cerebellum. When it gets bruised, the ground seems to tilt. People sway, stumble, or freeze in place. One study found that even “mild” head injuries change walking patterns enough to raise fall risk by 50% (Brain Injury Association of America, 2024).
Coordination Turns Clumsy
Reaching for a coffee cup can knock over the whole table. Fine finger skills vanish. Buttons stay undone, handwriting turns shaky, and stairs feel like mountains. Physiopedia refers to this as “loss of motor dexterity” (Physiopedia, 2024).
Pain and Tiredness Make Everything Worse
Chronic headaches, neck pain, and shoulder aches are common after TBIs. When pain flares, muscles guard and stiffen. Add normal daily fatigue, and movement shuts down completely (Irvine, 2023).
Symptom Questionnaire:
From Stiffness to Locked Joints: The Contracture Trap
If a person rests too much to avoid pain, muscles shorten like dried rubber bands. Joints freeze. Doctors call these locked positions contractures. Elbows, knees, and ankles can bend only a few degrees. Contractures typically develop within weeks and become permanent within months if left untreated (Physiopedia, 2024).
Headway, a UK brain-injury charity, warns: “Lack of movement is the biggest enemy of recovery” (Headway, 2023).
How Chiropractic and Integrative Care Unlock the Body
Chiropractors do more than crack backs. They use gentle moves, hands-on muscle work, and brain-retraining exercises to restart motion and calm pain.
1. Spinal Adjustments Re-Open Nerve Highways
Misaligned neck bones pinch nerves that control arms and legs. A precise chiropractic adjustment lifts that pressure. Blood and cerebrospinal fluid flow better. Patients often feel looser the same day (Northwest Florida Physicians Group, 2023).
Dr. Jimenez films before-and-after videos: one patient who dragged her foot for two years took ten smooth steps after three visits (Jimenez, 2025).
2. Soft-Tissue Therapy Melts Tight Muscles
Fascia—the thin sleeve around every muscle—can knot after injury. Chiropractors use tools and fingers to smooth these knots. Shoulders drop, necks turn, and hips swing again (Function First, 2024).
3. Balance Boards and Eye-Tracking Drills Rewire the Brain
Simple wobble boards teach the brain to steady the body. Following a finger with the eyes rebuilds coordination pathways. These “neuro-drills” are fun and fast. Most patients notice steadier steps in four weeks (HML Functional Care, 2024).
4. Stretching Plans Stop Contractures Before They Start
Daily 10-minute routines keep joints supple. A chiropractor demonstrates the exact angle and hold time to ensure muscles lengthen safely (NR Times, 2024).
5. Posture Fixes End Headache Cycles
Slumped shoulders strain the neck and starve the brain of oxygen. One posture taping session plus two adjustments can cut headache days in half (Cognitive FX, 2024).
Real Stories That Prove It Works
Mark, age 34, car crash survivor “I couldn’t lift my toddler. After six weeks of chiropractic care, I carried her across the park.” (Patient testimonial, Apex Chiropractic, 2024)
Sarah, age 19, soccer concussion “Balance boards felt silly—until I walked the graduation stage without my cane.” (Crumley House, 2024)
Midday 10-minute walk with trekking poles, Soft-tissue massage on tight calves
Evening Wobble-board “surfing” while brushing teeth, Gentle foam-roll under guidance
Follow this for 90 days, and most people regain 70–80% of normal motion (Impact Medical Group, 2024).
When to See a Chiropractic Neurologist
Look for these red-flag signs:
Your legs drag or cross when you walk
Arms stay glued to your sides
You fall more than once a month
Painkillers no longer help
A chiropractic neurologist assesses your gait on video, tests eye reflexes, and develops a customized plan (NeuroChiro, 2024).
Science Backs the Gentle Touch
A 2022 review of 14 studies found that spinal adjustments, combined with exercise, reduced TBI pain by 41% more than exercise alone (Jimenez, 2025). Another trial showed that balance scores increased by 28 points in eight weeks with integrative care (PMC, 2022).
Safe, Drug-Free, and Covered by Many Insurances
Chiropractic care for head injuries is a non-invasive approach. No needles, no scalpels, no opioids. Most auto-insurance PIP plans and major health plans pay for 12–20 visits (Sam’s Chiropractic, 2024).
Your Next Step Today
Call a local chiropractor who lists “TBI” or “concussion” on their website.
Bring a 1-page list: “I trip, my left knee locks, headaches every afternoon.”
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine