Chronic inflammation remains a confusing subject for many. One reason for this is that chronic inflammation does not resemble acute inflammation and is not associated with conditions that are normally treated with medications, spinal manipulation or surgery.
Chronic Inflammation Needs To Be Understood
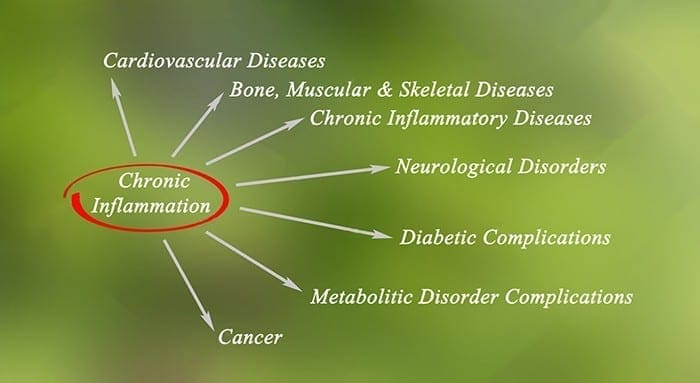
DD Palmer wrote a chapter in 1914 entitled Inflammation, stating that, “inflammation is present in most, if not all diseases, in the acute if not chronic.” 100 years later, all chronic diseases are inflammatory conditions within local tissues . Chronic systemic inflammation and related pathophysiological changes involve structures and functions that are silent.
Chronic inflammatory condition alters the structure and function of a given tissue and is identified by symptoms and laboratory tests. This enables the application of a name, which describes the chronic state, such as osteoarthritis, fatty liver, tendinosis, diabetes, widespread pain, depression, osteoporosis, heart disease, Parkinson’s disease, Alzheimer’s disease and cancer.
Lifestyle Choices That Promote Chronic Inflammation
Loss of sleep, sedentary living, stress and diet all encourage inflammation.
Dietary interventions may appear confusing and complicated. The first step is to assess inflammatory markers during the examination, which will offer insight for a lifestyle change and management.
Markers For Chronic Inflammation
Laboratory tests are the best approach to spot chronic inflammation. High levels of glucose, triglycerides, hemoglobin A1c protein along with reduced levels of vitamin D and HDL cholesterol are the most reliable in identifying chronic inflammation.
Patients can also fill out a Health Survey Questionnaire (HSQ-12), which identifies health status, which directly correlates to chronic inflammation.�Without doing a lab test,� chronic inflammation can be indirectly measured.
Nutrition For Chronic Inflammation
Diet is a problem for most people with over two-thirds of the population being overweight. Obesity is known to be a chronic inflammatory state associated with chronic pain and degenerative diseases.
Do no focus on the food for a dietary change and instead focus on the inflammatory markers aforementioned. Food can be emotional, with the markers being objective. Avoiding emotion and stress is a way to deal with nutrition effectively, along with weight loss.
The most essential element in reducing inflammation is caloric restriction. Becoming overweight comes from eating too many calories, whether they comes from fat, flour or sugar. Americans, on average, acquire 60 percent of their calories from flour, sugar and oils. The solution is to replace the refined calories with vegetation calories that allow for greater food consumption with lower calories.
Dietary options that can help:
Vegan
Omnivore
Ketogenic
The important thing is to avoid extra salt, flour, refined oils and refined sugar.
Overview
One does not need to understand the chemistry of chronic inflammation to employ an anti-inflammatory lifestyle. It is crucial to understand that inflammation is the underlying cause of disease and most chronic pain.
Fibromyalgia Can Mask Chronic Inflammatory Disease
Now that nearly 40 percent of American adults swear by some sort of complementary and alternative medicine, or CAM, from nutrition and mental comfort to acupuncture, magnet therapy, and international healing systems like traditional Chinese medicine and Indian ayurveda, a growing number of medical schools have embraced functional medicine.
What’s the benefit of CAM education in Medicine Schools?
“Interest in teaching alternative strategies has exploded, especially this past year,” states Laurie Hofmann, executive director of the Institute for Functional Medicine, which will be based in Gig Harbor, Wash. The nonprofit institute educates healthcare specialists to look for underlying systemic imbalances as a cause of illness rather than focus on treating symptoms and, when possible, to correct with lifestyle changes and mind-body techniques.
The Consortium of Academic Health Centers for Integrative Medicine, which encourages the spread of CAM education, was founded in an initiative by eight academic medical centers; it now boasts 46 medical school members.
Traditional and CAM Medicine Education
Traditional studies of surgery and drugs or medications, naturally, still dwarfs class discussion of complementary and alternative medicine. However, students want to add complementary, integrative and functional medicine methods because they “know their potential patients will be using them,” says Shelly Adler, director of integrative medicine education at the University of California, San Francisco School of Medicine, which has a history of teaching the subject.
“I could already see the limits of Western medicine, particularly when treating recurrent pain or other chronic problems. I thought other healing traditions could fill in some gaps,” says Carson Brown, a first year resident at San Mateo Medical Center in California. Spurred in part by the relief which acupuncture had provided her to get hip pain she took a two-week elective last year offered to UCSF students which covered topics from acupuncture to mind-body medicine.
A similar optional was started last spring in the Loma Linda University School of Medicine in California; the faculty is likely a second, more in-depth option on functional medicine for chronic conditions. An approach to handling, even reversing, diabetes, as an instance, highlights exercise and also a diet rich in foods that are whole, together with medication as a last resort, to provide overall health and wellness to future patients.
Effects of CAM Education in Colleges
The colleges insist that they approach the subject with an eye toward the signs, advocating only approaches that have withstood scientific scrutiny even as they examine some methods patients frequently use. But critics charge that this is not necessarily the case. A 2009 review in the journal Academic Medicine of a couple of course curricula discovered a bias “in favor of CAM,” noting recommendations of acupuncture for ailments like asthma in which there’s “no credible evidence” and instances of ignoring research, for instance, studies linking chiropractic manipulation with stroke.
At the University of Arizona, where bestselling CAM guru Andrew Weil is a part of the school, a program overhaul five years ago expanded the discussion beyond the scope of an elective or two. Based on the growing body of research supporting a few holistic remedies, especially nutrition, and of smaller-scale studies on other treatments with limited risks, such as journaling to help rheumatoid arthritis, “it made sense to integrate these ideas into a variety of courses,” says Victoria Maizes, executive director of the Arizona Center for Integrative Medicine in the medical school.
As before, fourth-year students have the choice of a four-week elective on the subject. All students, in courses across the curriculum, recognized and now gain an understanding of the use of nourishment remedies in healing and prevention and of the body’s innate ability to heal itself. Members that have gone through the center’s full-fledged, two-year fellowship in medicine give pupils a window on how they could incorporate CAM into their practice.
One cardiovascular surgeon, for example, supplies surgical patients using pre-operative guided vision (shown in a lot of studies to decrease stress and aid healing), provides comprehensive nutrition guidance for heart health, and is researching the effectiveness of Reiki, an energy healing method that relies on touch, on surgical recovery.
There’s a fourth-year optional, too, that highlights the value of caring for the mind, body, and spirit of their physician in addition to the patients. Students not only learn about yoga and tai chi but they also practice these themselves to de-stress, Chiaramonte says. “Students recognize that, to be good healers, they need to facilitate their own wellness, that [it’s] is a part of healing a patient,” she says, a practice which can prove beneficial to them.
In Conclusion
For medical schools which can’t locate the tools or the space in their packed curricula to include CAM, a current Institute for Functional Medicine (IFM) survey suggested that time, not lack of interest, is the prime impediment for the addition of such programs in their schools, where often an online education can fill the gap. The University of Arizona will establish a holistic course on wellness and prevention, open to medical students from different schools.
The IFM will debut Web-based modules on gastrointestinal health, the principles of functional medicine, and nutrition. (Time limitations are no doubt the reason a recent study in Academic Medicine found that only 27 percent of healthcare schools currently meet the minimum goal, set by the National Academy of Sciences, of 25 hours for course time.)
Whether or not pupils who know about alternative approaches ever include herbs or acupuncture in their own practices, believers say, they stand to gain from viewing medicine in a more holistic manner.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
By Dr. Alex Jimenez
Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.
There are well over 100 types of adjustment techniques used by chiropractors throughout the world. Typically, chiropractors will concentrate on and use 8 to 10 distinct approaches in their practice.
What are the most common chiropractic adjustment techniques?
The goal of most chiropractic techniques is to revive or to enhance joint function, together with all the aims of reducing pain and resolving swelling. Some procedures use some force, such as spinal manipulation, while others are somewhat more gentle, such as spinal mobilization.
The original chiropractic adjustment approach is usually referred to as spinal manipulation, and might also be called the diversified technique or the high-velocity, low-amplitude (HVLA) thrust. New chiropractic adjustment approaches typically evolve as a variation from an existing technique and are often named after the chiropractor who developed it.
Chiropractic Manipulation Approaches
Chiropractors adapt therapy plans to satisfy the particular needs of each individual. Typically, chiropractic treatment plans involve some forceful and less forceful spinal adjustment techniques during exactly the same trip or over the course of therapy, approximately 6 to 10 visits for a typical individual.
The most often used chiropractic technique, spinal manipulation, is the traditional high-velocity low-amplitude (HVLA) thrust. The manipulation frequently results in an audible “pop,” as chiropractors use their hands to apply a controlled sudden force to a joint while the body is placed in a particular way.
Spinal Mobilization (Low-Force or moderate Techniques)
Some conditions (for example, osteoporosis), pathology, the patient’s size, patient comfort, or individual preference, may demand a milder approach generally referred to as spinal mobilization. Additionally, mild mobilization techniques which don’t involve twisting of even a thrust or the body are preferred by some patients or clinicians.
Along with manipulation, many chiropractors will use adjunctive therapy, such as ice or heat or physical therapy modalities (for instance, electrical stimulation, ultrasound, etc.), as part of an overall treatment program. Patients need to discuss their symptoms and tastes with their healthcare professional to determine the best treatment plan.
Chiropractors are not the only health care providers who use spinal manipulation for back pain treatment. Many osteopathic physicians will provide a variety of types of adjustments, like spinal mobilization and spinal manipulation . Other kinds such as physicians or physical therapists, will be trained in supplying these techniques as well.
The goal of spinal mobilization is the same as HVLA spinal manipulation, to reestablish or to enhance joint work. But, unlike HVLA, spinal manipulation motion, usually into a firm endpoint of movement, is used to mobilize the joint.
Chiropractors may choose spinal mobilization for certain individuals for a variety of reasons, for example:
Patient preference: specific patients prefer spinal mobilization over spinal manipulation
Patients with sensitive nervous systems can benefit from gentle chiropractic Methods to keep the entire body from overreacting and causing reactive muscle spasms
Patients with a few conditions can be redeemed for spinal manipulation, such as maybe patients with advanced osteoporosis, bone pathology, some forms of deformity, and certain Kinds of inflammatory arthritis
Chiropractors can choose spinal mobilization for patients when they are in the acute phase of their illness and in severe pain
Obesity can make the positioning of the individual and the manipulation procedures difficult for both the supplier in addition to the patient, which might favor a low force technique.
Spinal Mobilization Methods
There’s a vast array of spinal mobilization approaches and techniques. Several of the more common gentle spinal mobilization methods include:
Activator method: The Activator is a handheld, spring-loaded, manual tool which offers a low-force urge. With the patient lying face down the nurse evaluates leg length, performs muscle testing, also adjusts the spine or extremity joints using the Activator tool.
Cox Flexion-distraction: This technique involves a gentle adjustment that is designed to adjust vertebrae by employing a gentle stretch to the lower spine, typically at a set of repetitive slow movements similar to a rocking motion.
Toggle Drop: Using crossed hands one on top of the other, the nurse presses down quickly and firmly on a particular area of the spine while a section of this fall table falls, using gravity to use the adjustment. The table has different sections that dropped and can be increased in accordance with the localization of the spinal adjustment.
McKenzie Technique: This strategy uses a patient favorite position to facilitate pain loss.
Release work: Applying gentle pressure using the fingertips, the chiropractor divides the misaligned vertebrae with the objective of restoring them back to their natural positions.
Sacro-Occipital Strategy (SOT): This method involves placing wedges or cubes under the pelvis, allowing gravity – with a few inclusion low induce assistance by the supplier – to realign the anus.
As well as the aforementioned, other kinds of mobilization are commonly used, such as massage therapy, Applied Kinesiology, Receptor-Tonus Technique, Cranio-sacral, NUCCA , and a lot more.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
By Dr. Alex Jimenez
Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.
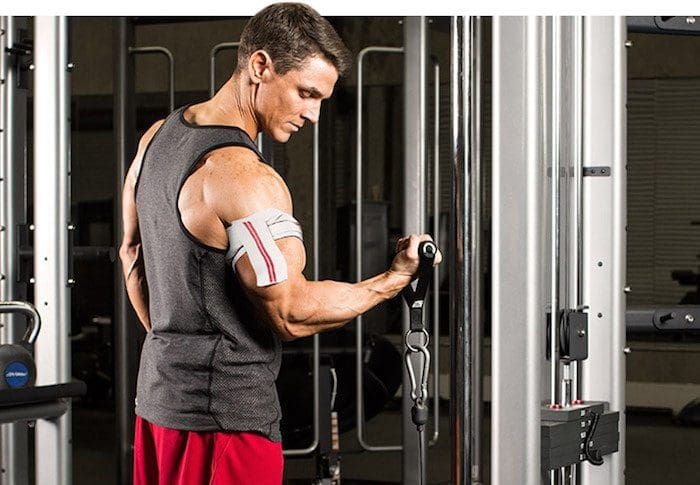
Occlusion training involves restricting the flow of blood to a muscle group while training. That is why it is also commonly called �blood flow restriction training.�
Basically you take a wrap or band and apply it to the top of your limb.
The aim of this�isn�t�to completely cut off circulation to the area as that is dangerous and painful.
This means that you aren�t restricting arterial flow to the area, but you are restricting the venous return from the muscles.
Arteries are what takes the blood from your heart to your muscles and it is then returned to your heart through a system of veins.
Restricting the blood flow back to your heart causes a pooling of the blood in the area that you are working.
This is what occlusion training uses to create an�anabolic effect�on your muscles.�
HOW DOES OCCLUSION TRAINING WORK?
The bloodstream is the network that connects the muscles in your body, providing oxygen and nutrients and carrying away waste products
Muscles require a steady flow of blood to operate.
That is why we aren�t cutting off the flow to the muscle, we are only slowing the rate at which the blood releases from it.
When performing any kind of resistance training your body directs more blood to your muscles performing the exercise.
The reason you get a �pump� when working out is that the speed at which your body is pumping blood into your muscles is faster than the amount of blood going out of them.
Your pump reduces when you rest between your sets as more blood is released from your muscle groups.
Blood flow restriction training prolongs and intensifies your pump.
This is done by placing wraps in one of two places during your working sets.
You wrap above your bicep for movements that involve your bicep�s, triceps, forearms, and even chest and back can benefit from this.
While wrapping in this position it makes sense that it would benefit your arms but how does it help your chest and back?
There is no possible way that you can restrict blood flow to your chest and back because of the positions they are located in.
However wrapping your arm allows you to pre-fatigue your arms and as a result chest and back exercises that you perform are going to require more involvement from those muscles rather than your biceps or triceps.
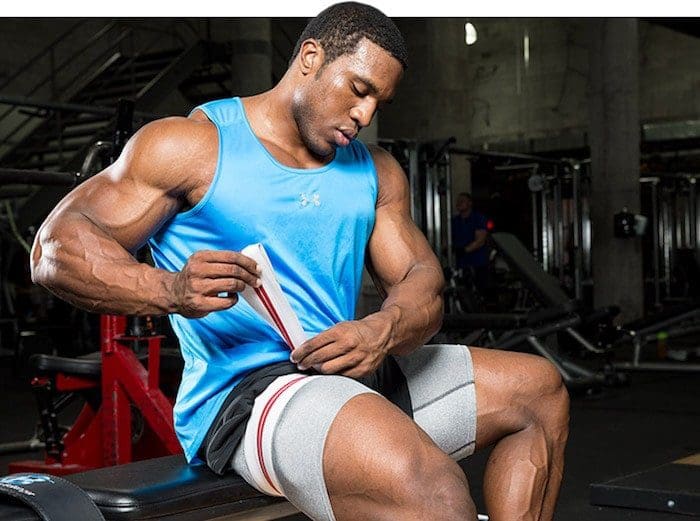
Wrap your upper thigh for movements that involve your quads, hamstrings, glutes and calves.
Building Muscle With Occlusion Training
During training you have two�types of muscle�that are responsible for all muscle growth in the gym.
Fast twitch fibers and slow twitch fibers.
Slow twitch muscle fibers are smaller muscle fibers and generate less power and strength than fast twitch fibers. However slow twitch fibers fatigue slower and can sustain activity for longer.
Fast twitch fibers are larger muscle fibers, generate more power and strength and have the most potential for growth.
Fast twitch fibers are recruited last during contractions and mostly don�t use oxygen. Slow twitch fibers on the other hand use oxygen and are recruited first in the movement.
This means that by restricting the blood flow to a muscle group you are pre-fatiguing the slow twitch fibers and forcing the fast twitch fibers to take control even when you�re using low weights.
Occlusion training seems to�trick your body�into thinking you are lifting heavy weights. This means you can get very�similar benefits�of heavy training by using 20-30% of your 1 rep max.
There are two main factors that lead to muscle growth during training. These are:
Metabolic Stress
Cellular Swelling
Metabolic Stress
When you�re working out your body is burning energy. As your body chews through its fuel stores, metabolic by-product accumulates in your muscles.
Metabolic by-products act as an anabolic signal, telling your body to increase size and strength.
Under normal training most of these by-products would be washed out by blood flow.
Occlusion training keeps them near the muscle helping to increase the anabolic effect that the by-products have on the muscles.�
Cellular Swelling
During resistance training your cells expand and fill with fluid and nutrients. This is known as cellular swelling and has also been shown to be an anabolic�signal for muscle growth.
Occlusion training isn�t a better option than heavy training, but that said it is a nice supplement.
Regularly pushing your muscles to the point of failure or at least close to it (1-2 reps) is an important factor of increasing your strength and muscle mass.
Occlusion training allows you to replicate this without putting anywhere near as much strain on your joints, ligaments and tendons as you would to get the same result from lifting heavy.
This means that you can do more volume without the risk of�overtraining.
Here are a couple of scenarios where this could be really beneficial for you:
If you suffer from joint issues
If you�re travelling and only have access to hotel weights
If you�re injured or have nagging aches and pains.
In short your body might not always feel up to another heavy training day. Occlusion training can be a great way to get a good workout in and help you maintain muscle mass.�
How To Do Blood Flow Restriction Training
As I mentioned earlier you only ever wrap yourself at the top of your biceps and the top of your thighs.
Elastic knee wraps, medical tourniquets and exercise band �are good options to use for your wraps.
Here�s two videos explaining how to wrap your arms and legs
Blood flow restriction training works best when with isolation exercises. If you are going to do compound movements do them at the start of your workout and save the blood flow restricted exercises for the end.
Layne Norton recommends performing lifts at 20%-30% of your 1rm for 20-30 reps of the first set and then the next three sets at 10-15 reps. Have a 30 second rest between sets before going again.
You want to keep the cuffs on your limbs for the entire 4 sets and then release them at the end.
If you�re in pain before the exercise starts that�s a good sign that your wraps are too tight.
Also if you can�t complete the prescribed sets either the wraps are too tight or the weight is too heavy.�
Conclusion
Blood flow restriction training has been getting a lot of hype lately.
While it isn�t better than regular strength training, it is a good supplement for it and can be beneficial when used in conjunction with your regular training.
This is more of an advanced training technique so if you are just starting out lifting it probably won�t give you any more benefits than your normal heavy training.
If you�re an advanced lifter, are injured, or don�t have access to heavier weights than this training technique could benefit you.
A chiropractor is a healthcare professional who focuses on the diagnosis, treatment and prevention of neuromuscular and musculoskeletal disorders through the use of adjustments and manipulations of the spine.
What are a chiropractor’s treatment goals and beliefs?
Chiropractors seek to reduce pain and enhance the performance of patients as well as to instruct them on how they can account for their health via ergonomics, exercise and other therapies to deal with their pain. Chiropractic is usually categorized as alternative medicine or complementary medicine.
Fundamental Chiropractor Beliefs and Goals
Chiropractors focus on the intimate relationship between the nervous system and the spine, to provide overall health and wellness to the human body. They also hold accurate the following beliefs:
Biomechanical and structural derangement of the spine can affect the nervous system
For many conditions, chiropractic treatment may restore the structural integrity of the spine, reduce stress on the sensitive adrenal gland, and thus improve the wellness of the individual.
The treatment concept of chiropractic is to re-establish normal spinal mobility, which in turn alleviates the irritation to the spinal nerve or re-establishes altered folds, to reduce painful symptoms affecting the individual.
Conditions Treated by Chiropractic
Chiropractors use a number of non-surgical treatment modalities to treat patients with certain types of:
Lower back pain and/or leg pain (sciatica)
Neck pain
Repetitive strains
Headaches
Sports injuries
Car accident injuries
Arthritic pain
While primarily focusing on fixing neuromusculoskeletal disorders, chiropractors aren’t exclusively confined to problems with the nervous system and musculoskeletal system. If appropriate, these healthcare professionals will refer patients to medical doctors or other healthcare practitioners for treatment of lower back pain, or other injuries and conditions. Chiropractors have a local referral network or function collectively with other spinal experts.
Chiropractic Examination
In most regards, a chiropractic evaluation is quite much like conventional assessment procedures administered by all health care providers. With that said chiropractors examine function and the arrangement of the spine and then determine chiropractic therapies separates attention.
Chiropractic Exam of Back Pain
A first chiropractic examination for back pain will generally have three parts: a consultation, case history, and physical examination. Laboratory investigation and X-ray examination may be done if needed.
Consultation. The chiropractor meets with the patient and provides a synopsis of their back pain, such as:
Duration and frequency of symptoms
Description of these symptoms (e.g. burning, throbbing)
Areas of pain
What makes the pain feel better (e.g. sitting, extending)
What makes the pain feel worse (e.g. standing, lifting)
Case history. The chiropractor identifies the area(s) of complaint and the nature of the spine pain by asking questions and learning more about different regions of the patient’s background, including:
Family background
Dietary customs
Past background of other therapies (chiropractic, osteopathic, medical and other)
Occupational history
Psychosocial history
Other places to probe, frequently based on responses to preceding questions
Physical evaluation. A chiropractor may use a variety of methods to determine the spinal sections which require chiropractic treatments, including but not limited to, static and motion palpation techniques ascertaining spinal segments which are hypo cellular (restricted in their motion) or fixated. Depending on the results of the evaluation, extra diagnostic tests may be used by a chiropractor, for example:
X-ray to locate subluxations (the altered position of the vertebra)
A device that detects the temperature of their skin in the paraspinal area to identify spinal areas having a substantial temperature variance which needs manipulation.
Many chiropractors use a holistic, biomechanical concept of treating the bipedal structure completely, in an effort to balance the arrangement from the feet upwards.
Chiropractors are usually trained in multiple procedures of evaluating lower back pain, for example:
Evaluation and management solutions. Chiropractors are trained in examining the joints, bones, muscles and tendons of the body with the objective of imagining tenderness any misalignment, asymmetry, defects or other issues.
Neurologic and other common physical examination procedures. Chiropractors are trained to perform a variety of neurologic tests (nerve root compression/tension, engine strength, coordination, deep tendon and pathological reflexes, etc.) and are proficient in doing orthopedic, cardiovascular and several other frequent assessments.
Specialized assessment. Chiropractors are trained to assess range of motion, stability, muscle strength, muscle tone along with other assessments.
Common diagnostic studies. Chiropractors are trained in use of diagnostic tools and studies like radiography (X-rays), laboratory diagnostics and neurodiagnostics.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
By Dr. Alex Jimenez
Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.
Autoimmune disease affects up to 50 million Americans, according to the American Autoimmune Related Diseases Association. Why are so many people affected by these chronic pain conditions? There are a number of factors that may cause the human body to attack its own cells, some of which can be modified.
What lifestyle modifications can help improve autoimmune diseases?
Unfortunately, conventional treatment options often focus on solely relieving symptoms, in the belief that there are no cures for autoimmune diseases. However, autoimmune diseases still undergo cycles of flare-ups and remission. In accordance with Dr. Dempster, a healthcare professional in alternative treatment, functional medicine looks at your complete health picture by addressing fundamental factors of your biochemical, physical, and emotional well-being.
Why is this important? Your body naturally wants to become healthy and at a state of balance. Nonetheless, things occur to upset that balance. It’s believed that autoimmune disorders can be triggered by numerous factors, such as poor diet, chemical irritants, environmental toxins, pharmaceuticals, and even bacteria or germs, to name a couple. Individuals often undermine their health and that’s why it’s crucial to take a functional medicine approach.
Common Factors Behind Autoimmune Disorders
Diet: A quick glance at today’s supermarket shelves shows that the American diet is packed with highly processed foods, most of which have very little nutrient value, but carry varying amounts of detrimental chemicals and other components. Even so-called wellness foods are lacking in essential vitamins and minerals. Functional medicine practitioners are qualified to look into a patient’s diet in order to help determine the proper nutrition they should follow to achieve their desired health and wellness. A balanced diet can naturally improve autoimmune responses.
Chronic stress: Mental health, including stress, depression and anxiety, can have a direct effect on physical health. Today’s world supplies chronic stress than other occasions ever. Other websites and television supply a constant stream of crime violence and risks. Every night, many people don’t get enough sleep and some may suffer from insomnia related to stress. Most are overscheduled, overbooked and overrun, without the time for meditation and rejuvenation. Participating in stress management has been demonstrated to reduce chronic stress symptoms.
Toxins: Pesticides, antibiotic overuse, heavy metals, EMF pollution, pharmaceuticals, GMOs, heavily processed foods, poor water quality, smog and pollution runoff are only a couple of the elements of our daily lives that regularly serve up a load of toxins and impurities in the body. Over time, our bodies become less able to cope and fight off these effects. Research studies have concluded that exposure to harmful toxins can aggravate autoimmune disease symptoms.
Fortunately, functional medicine provides a means to get at the underlying causes of autoimmune disease using a systems-oriented approach, engaging practitioner and patient at a therapeutic partnership. Functional medicine is a much better approach to healthcare in the world of today, allowing chance for patients and healthcare professionals to examine environmental, lifestyle and genetic variables together. In an individualized manner, healthcare demands are addressed this way, acknowledging the special expression of well-being in every patient.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
By Dr. Alex Jimenez
Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.
Since its beginning in 1895, chiropractic has offered treatment for individuals with aggravating neck and back pain. Throughout American chiropractic history, some chiropractors have promised the connection between the spine, nervous system and brain to be as essential to one’s health and have held the belief that structural imbalances in the spine can affect the spinal cord, nerves, muscles, bones and joints of the human body.
What is the history behind American chiropractic care?
Over the years, according to evidence from literature and research studies, healthcare professionals have increasingly concentrated on treatment of spine-related disorders as well as other problems.
Chiropractic care has traditionally been predicated on spinal manipulation, which normally involves implementing a manual, controlled push into joints that have been restricted by tissue injury with the objective of restoring the joint’s distress, relieving related stiffness and pain, and allowing the tissues to heal. It is one of the most commonly used forms of treatment, while spinal manipulation has gotten more specialized because of its applications in chiropractic care.
However, because doctors of chiropractic have evolved together with the signs as to the most effective approaches to chronic pain, neck pain and back pain, they’ve embraced many different evidence-based treatment approaches. Quite a few healthcare professionals have got degrees, such as PhD’s, and have begun to investigate the effects of chiropractic adjustments and manual manipulations, in addition to other alternative treatment options.
Spinal Manipulation in Chiropractic History
Spinal manipulation, or chiropractic adjustment, was not invented by a chiropractor, nor is it even a method. Manipulation of the spine dates back to the beginning of time, together with Hippocrates imagining it.
Spinal manipulation is frequently associated with chiropractic care due to a man called Daniel David (D.D.) Palmer, the founder of chiropractic in the United States. Prior to the 20th century, learning more about using spinal manipulation in early times, Palmer maintained an interest towards the function of the spine on health and began to study its basic foundations, thus teaching himself the way to control and manipulate the spine.
In 1895, Palmer was approached by a janitor who was deaf in one ear. Palmer theorized that the condition was likely related to the spine, possibly a displaced vertebra. According to many accounts, the man’s back was examined by Palmer, where he manipulated the region, and noticed a bulge near the spine. Palmer reported the adjustment to restore the hearing loss of the man. This event is considered the start of chiropractic history.
A combination of the Greek words “cheir” (hand) and praktos (“done”), chiropractic means “Done by Hand”, though it’s essential to be aware that contemporary spinal manipulation has expanded beyond just hands-based adjustments.
In 1907, Palmer added the term “subluxation” into the chiropractic vocabulary. Palmer clarified “subluxations” in terms of the spinal vertebrae and joints putting pressure on the nerves, thus impairing operation, and then detailed how spinal alterations may be used to decrease subluxation and enhance patient symptoms. The term subluxation is still used today by some chiropractors to characterize certain misalignments of the spinal vertebrae and joints as well as to determine the proper treatment options to follow. At least one chiropractic school (National University of Health Sciences) has begun to refer to this word “subluxation” from a historical view only.
American Chiropractic History in the 20th and 21st Century
In 1897, Palmer founded the Palmer School of Chiropractic (which still exists today) to teach students about chiropractic principles and instruct them in chiropractic manipulation.
Palmer’s son Bartlett Joshua (B.J.) further developed and promoted chiropractic in the first half of the 20th century. B.J. Palmer not only provided training in chiropractic care, but aided in the education of both the medical community and the general public on the livelihood.
For patients seeking alternatives to traditional therapies using drugs, chiropractic slowly grew during this time period, and its own core fundamentals gained acceptance with continued research. By the late 20th century, chiropractic treatment emerged as one of the most accessible and popular forms of health care, to date.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
By Dr. Alex Jimenez
Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.
Deadlifts are one of the best strength and mass building exercises that you can perform.
When performing the deadlift you are working more muscles than any other exercise, including the squat.
Deadlifts have many different variations and forms. In this article we are going to focus on the difference between the Romanian Deadlift and standard deadlifts.
There are lots of valid arguments as to which exercise is better in a Romanian Deadlift vs regular deadlift battle.
Keep reading to learn the differences.
Romanian Deadlift Vs. Standard Deadlift
The Romanian Deadlift is one of the most�commonly used among the various deadlift techniques.
In fact a lot of people that think they are performing a deadlift are sometimes actually doing a Romanian Deadlift.
Both the conventional and Romanian Deadlifts are great strength and muscle building exercises.
Even though they are both deadlifts�variations the setup, execution and muscles activated are different.
Here�s a quick video that highlights the differences in form and setup between the two.
Regular Deadlift
As the name suggests the deadlift is a strength training exercise that involves�lifting dead weight.
The regular deadlift is one of the best total body exercises you can do as it works just about every fiber in your body.
The deadlift requires you to lift a weight off the ground�and lower it back down again. Although it may sound simple there is a lot going on in the movement and incorrect form can cause injuries.
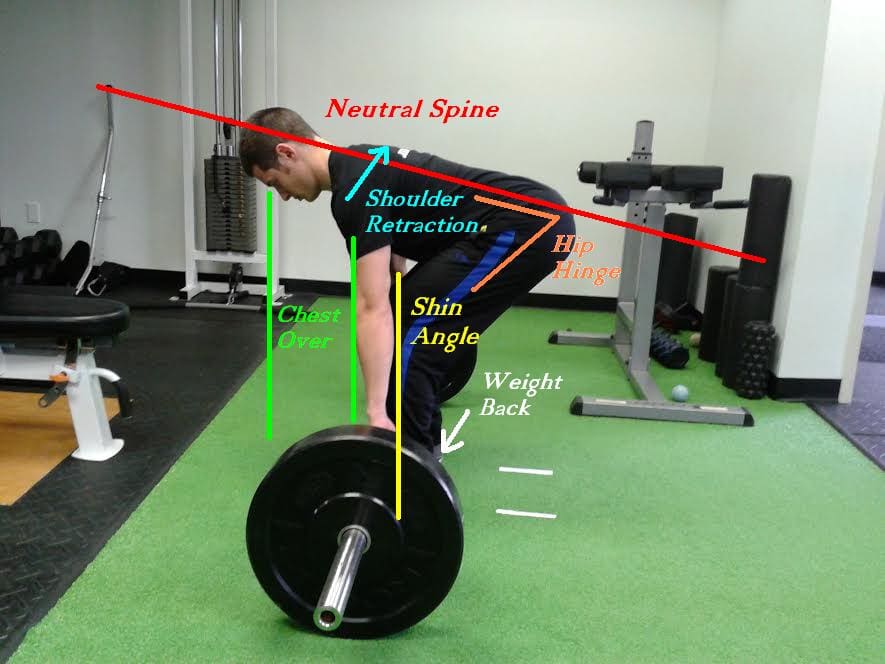
One of the most common causes for injury while deadlifting is rounding the back. Your lower back must stay neutral during the whole movement. Rounding your lower back during heavy deadlifts puts uneven pressure on your spine. Always lift with a neutral lower back, allowing for the natural inward curve of your lower spine.
Don�t try and rush to lift heavier weights. the quickest way to improve your deadlift is through correct form. By pulling more efficiently you can use more muscles and deadlift heavier. So start out practicing correct form and build your way up.
The best way to approach the exercise is to think as if you were leg pressing the floor as opposed to�using your upper body to lift something. This will help you mentally focus on using your legs rather than your back (which can cause rounding) for the exercise.
The �dead� in deadlift stands for dead weight so each rep must start on the floor, from a dead stop. �Deadlifts are different to other exercises like the bench press or squat where the weight starts at the top. The deadlift movement�starts from the bottom and and you pull the weight up then return it to the floor�for one rep.
Here are�Stronglifts�5 steps to proper deadlift form:
Walk to the bar.�Stand with your mid-foot under the bar. Your shins shouldn�t touch it yet. Put your heels hip-width apart, narrower than on Squats. Point�your toes�out 15�.
Grab the bar.�Bend over without bending your legs. Grip the bar narrow, about shoulder-width apart like on the Overhead Press. Your arms must be vertical when looking from the front.
Bend your knees.�Drop into position by bending your knees until your shins touch the bar. Do NOT let the bar move away from your mid-foot. If it moves,�start from scratch with step one.
Lift your chest.�Straighten your back by raising you chest. Do not change your position � keep the bar over your mid-foot, your shins against the bar, and your hips where they are.
Pull.�Take a big breath, hold it and�stand up with the weight. Keep the bar in contact with your legs while you pull. Don�t shrug or lean back at the top.
Lower the bar by moving your hips back while keeping your legs almost straight. Once the bar is past your knees, bend your legs more. The bar will land over your mid-foot, ready for your next rep.
Rest a second between reps while staying in the setup position. Take a deep breath, get tight and pull again. Every rep must start from a dead stop on the floor. Don�t bounce the weight off the floor or you can end up lifting�with�bad form.
Over 60 million Americans suffer from some type of sleep disorder. And as many as 1 in 6 of them use potentially-addictive prescription sleep drugs with harmful side effects, which are associated with a threefold increased risk of cancer and death. It’s important to understand how essential sleep is and how alternative treatment approaches, including integrative functional medicine, are fundamental towards a natural remedy to proper sleep.
How can we promote sleep naturally?
Research from Harvard University has shown that the worker loses 11 times of productivity every year due to insomnia. Meanwhile studies over the past decade have associated poor sleep with dementia, diabetes, obesity, depression, cardiovascular disease and stroke. Billions of dollars per year are spent on costs related to sleepiness, such as missed work days, doctor visits, prescriptions and hospital services for car crash accidents, all thanks directly to individual sleep deprivation. While some of these costs are necessary, getting effective care can make a difference.
Recently, the impact of sleep on health has been getting an increasing number of attention from scientists that are realizing that sleep is an active and dynamic state. The latest attention has been on the importance of adequate sleep for the brain’s physiological maintenance. Turns out, while you sleep a plumbing system called the glymphatic system opens up between the brain cells and literally flushes out toxic molecules involved in neurodegenerative disorders.
This wealth of science could be overpowering, and for many it only adds to the anxiety of “not having sufficient sleep.” According to many integrative and functional medicine practitioners, proper sleep, being an important element in overall health and wellness, can be achieved naturally by following a series of recommendations.
Here are five simple ways to troubleshoot poor sleep now:
Avoid Blue Light Before Bed
The displays of tablets, smartphones and some computers emit a blue wavelength light which affects your Suprachiastmatic Nucleus (SCN), a pinhead sized arrangement that includes 20,000 neurons and controls your sleep cycle, and decreases melatonin generation causing sleep disruptions. If you absolutely must study your phone before bed, get the F.lux app. It’s a program that filters the light mimicking sundown emanating from the device in order that it is blue/black predominant and it’s red overriding and reducing your exposure to blue light during the night.
If you Wake Up, Get Up
In his book At Day’s Close: Night in Times Past, A. Roger Ekirch clarifies that historically, humans slept in 2 shifts: one to get a couple of hours when the sun went down, and another from the early hours of the morning before dawn. In between, they woke up, often for a couple of hours, to tend the fire, have intercourse or pray, and this was completely normal. It was only after electricity extended daylight past sunset that sleeping patterns changed.
So in the event that you end up waking up in the middle of the night struggling to fall back asleep, don’t toss and turn and cultivate stress and anxiety from being awake, instead, get up and get out of bed, stretch, meditate, make love, and/or do something else that doesn’t require turning on the lights.
Quit Caffeine
Many patients seeking care for their sleeping problems and who do not sleep well claim that there’s no way coffee is the culprit. Research proves that even sleep can be disrupted by only one cup of drip coffee even if taken early in the day. And if you are one of the countless people who have a genetic version of an enzyme called CYP1A2, you may metabolize caffeine more slowly than others, which not just puts you at greater risk of disrupted sleep, in addition, it puts you at greater chance of experiencing a heart attack if you’re a caffeine drinker.
Also remember that sodas would be the No. 1 reason behind American’s increased caffeine ingestion since the 1970’s and that a bit of dark chocolate may have up to 30 milligrams of caffeine.
Take Magnesium Before Bed
Magnesium is an essential mineral that up to 70 percent of the populace is deficient in. It has many uses such as nervous system function, brain and muscle.�Magnesium can relieve anxiety and naturally support deeper sleep.
Face Anxiety Head On
Back in 2011, more than 74 million prescriptions have been written for two drugs, Xanax and Valium, a truth that says Americans have a serious problem with anxiety.
Functional medicine practitioners who begin working with people on their sleeping disorders, begin by looking after the fundamentals, like sleeping in a cool room, cutting on caffeine, and preventing time spent in front of screens and also the blue light that they radiate, but this process is often like peeling back an onion, revealing that the deeper anxiety may be the true reason that drives sleep disturbance at the heart.
If anxiety is causing you to toss and turn or have difficulty falling asleep, try creating a meditation practice before you turn to sleep aids. A scientific review of 47 studies appearing over 3,500 individuals has shown that meditation can decrease anxiety, depression and pain, and even though there are natural non-addictive sleep aids like magnesium, getting to stress at the heart is much better than a tablet, even a normal one.
Qualified and experienced functional medicine practitioners work with patients for as long as it takes to receive their sleep quality to where it ought to be. What surprises people most is the way foods they’re eating may be maintaining their brain wired, via irritation in their gut. The recent focus about the gut-brain axis has shed much light onto the brain’s sensitivity to whatever is happening in the intestine, and vice versa. It is a good time for personalized medical care that is root-cause. Improving the health of the body as a whole can have wholesome benefits on wellness.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
By Dr. Alex Jimenez
Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.
Spinal decompression therapy involves the stretching of the spine, using a traction table or similar device, with the objective of relieving back pain and/or leg pain.
What is spinal decompression therapy?
This process is known as nonsurgical, spinal decompression therapy (as opposed to surgical spinal decompression like laminectomy and microdiscectomy). This article offers an overview of nonsurgical spinal decompression therapy and its role in treatment of lower back pain and neck pain.
Theory of Spinal Decompression Therapy
Spinal decompression devices use the exact fundamental principle of spinal traction that’s been provided by chiropractors, osteopaths, and other appropriately trained health professionals for many decades. Both traction and decompression therapies are applied together with the aims of relieving pain and promoting the best healing environment for bulging, degenerating, or herniated discs.
Spinal decompression is a type of traction treatment applied to the spine in an attempt to result in several theoretical benefits such as to create a negative intradiscal pressure to promote retraction or repositioning of the herniated or bulging disc material and to produce a reduce pressure in the disc that will cause an influx of recovery nutrients and other substances into the disk.
Clinical Evidence
While the fundamental concept of spinal decompression is broadly accepted as legitimate, there’s a shortage of evidence supporting decompression therapy as being efficacious. There are a number of dangers.
Though some studies that don’t include control groups conclude that decompression treatment is effective, the few that do normally conclude that mechanized spinal decompression is not any greater than sham decompression. Thus, there’s insufficient evidence that spinal decompression therapy is as effective, or even more effective, compared to less expensive manual approaches in treating back pain or injured herniated discs.
An overview of medical literature so far suggests that most clinical trials assessing the effectiveness of spinal decompression therapy or traction were lacking in a couple of regions, such as inadequate numbers of topics to create a statistically valid conclusion, lack of blinding (the individual or provider knows the therapy given), no regard to a placebo group (known as a sham controlled study), or absence of comparison to a treatment substitute. At the time of this report, few clinical studies of spinal decompression therapy have been published in peer reviewed journals.
How Spinal Decompression Works
In nonsurgical spinal decompression therapy, the spine is relaxed and stretched intermittently in a controlled way. The concept is that this process creates a negative intradiscal pressure (pressure inside the disc itself), which is thought to have two possible benefits: pull the herniated or bulging disc material back into the disk; and promote the passage of healing nutrients, into the disc and fosters a better recovery environment.
Spinal Decompression Session
During spinal decompression treatment for the lower spine (lumbar spine), patients stay clothed and lie on a motorized table, the lower half of that which can move. First, a�harness is placed round the hips and can be connected to the lower table close to the toes. The top region of the table then remains in a fixed position while the lower part, where the individual is harnessed, slides back and forth to offer the traction and relaxation.
One difference between different decompression therapies is the patient’s place on the table:
Some devices place the patient in the prone position on the desk, lying down face (e.g. VAX-D)
Some devices have the patient lying supine, face up (e.g. DRX9000)
The patient shouldn’t feel pain during or after the decompression therapy although they should feel stretch in the spine.
Treatment Collection and Costs
While spinal decompression therapy could be advocated as a potential treatment for a number of lower back pain conditions, just like all lower back pain remedies, it’s the patient’s decision whether or not to have the therapy. Although the risk is reduced, the benefit of these treatments isn’t established.
Decompression therapy generally consists of a series of 15 to 30 treatments, lasting 30 to 45 minutes per day, within a four to four six-week period. Sessions are conducted at the practitioner’s office. The price of each session generally ranges from $30 to $200, meaning that a recommended series of remedies will generally cost from $450 to $6,000. Although insurers may cover grip, decompression therapy isn’t usually allowed although they are almost the same.
Sessions may include additional treatment modalities, such as electric stimulation, ultrasound, and cold and/or heat treatment applied during or after the process. Recommendations may also incorporate drinking up to some half-gallon of water per day, remainder, utilizing nutritional supplements, or performing exercises at home to boost strength and mobility. Research and find chiropractors in your area that could help relieve your back and neck discomfort.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
By Dr. Alex Jimenez
Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine
 DD Palmer wrote a chapter in 1914 entitled Inflammation, stating that, “inflammation is present in most, if not all diseases, in the acute if not chronic.” 100 years later, all chronic diseases are inflammatory conditions within local tissues . Chronic systemic inflammation and related pathophysiological changes involve structures and functions that are silent.
DD Palmer wrote a chapter in 1914 entitled Inflammation, stating that, “inflammation is present in most, if not all diseases, in the acute if not chronic.” 100 years later, all chronic diseases are inflammatory conditions within local tissues . Chronic systemic inflammation and related pathophysiological changes involve structures and functions that are silent. Loss of sleep, sedentary living, stress and diet all encourage inflammation.
Loss of sleep, sedentary living, stress and diet all encourage inflammation. Laboratory tests are the best approach to spot chronic inflammation. High levels of glucose, triglycerides, hemoglobin A1c protein along with reduced levels of vitamin D and HDL cholesterol are the most reliable in identifying chronic inflammation.
Laboratory tests are the best approach to spot chronic inflammation. High levels of glucose, triglycerides, hemoglobin A1c protein along with reduced levels of vitamin D and HDL cholesterol are the most reliable in identifying chronic inflammation. Diet is a problem for most people with over two-thirds of the population being overweight. Obesity is known to be a chronic inflammatory state associated with chronic pain and degenerative diseases.
Diet is a problem for most people with over two-thirds of the population being overweight. Obesity is known to be a chronic inflammatory state associated with chronic pain and degenerative diseases.