Sandra Rubio discusses the symptoms, causes and treatments of neck pain. Headaches, migraines, dizziness, confusion and weakness in the upper extremities are some of the most common symptoms associated with neck pain. Trauma from an injury, such as that from an automobile accident or a sports injury, or an aggravated condition due to improper posture can commonly cause neck pain and other symptoms. Dr. Alex Jimenez utilizes spinal adjustments and manual manipulations, among other chiropractic treatment methods like deep-tissue massage, to restore the alignment of the cervical spine and improve neck pain. Chiropractic care with Dr. Alex Jimenez is the non surgical choice for improving overall health and wellness.
Cervical Pain Treatment
Neck pain is a common health issue, with approximately two-thirds of the population being affected by neck pain at any time throughout their lives. Neck pain originating in the cervical spine, or upper spine, can be caused by numerous other spinal health issues. Neck pain can result due to the pinching of the nerves emanating from the vertebrae, or because of muscular tightness in both the upper spine and the neck. Joint disruption in the neck can generate a variety of other common symptoms, including headache, or head pain, and migraines, as does joint disturbance in the back. Neck pain affects about 5 percent of the global population as of 2010, according to statistics.
If you have enjoyed this video and/or we have helped you in any way please feel free to subscribe and share us.
Are you experiencing back pain right now? The impact may seem identical, although it can be characterized as a dull throb or a sharp pain. Your life may have already been negatively affected as a result of your back pain. Some estimates show that 80 percent of people may experience the distress of back pain at any point in their life. And from an employer’s perspective, more than 25 percent of those working adults missed a period at work in the previous few months following back pain. Back pain can be aggravating. The pain and discomfort might only last a few days or a couple weeks, however, it may often become a chronic health issue if left untreated for an extended period of time, impacting the lives of the average person as well as that of athletes alike.
Typically, back pain originates from a mechanical problem caused by the regular wear-and-tear of the spine and associated to the aging process of the human body. Daily usage, or the average movement during the course of the day, can take a toll on the structure and function of the spine, discs, and the joints. Sprains and strains, skeletal irregularities, or being involved in an auto accident can also cause the degeneration of the spine but the end results are exactly the same. While anyone can experience back pain, there are some factors that can raise the risk, including age, fitness level, pregnancy and weight gain, occupational risk factors with physically demanding tasks, preexisting mental health difficulties and even overloaded backpacks carried by school children.
Fortunately, relief can be achieved by chiropractic care. Experts estimate it that roughly 22 million Americans visit their chiropractor each year and 35 percent of these patients are seeing their chiropractor to get a remedy for their back pain, recurring neck pain, headaches and numbness or tingling in their arms and legs.
Contents
Chiropractic Care Helps Back Pain
Chiropractic care involves the manipulation of the spine with varying levels of pressure exerted through a treatment method intended to restore the health of the human body. The hope is the proper alignment of the spine, adjusted during a process known as a spinal adjustment, to allow the body to heal itself, without forcing the individual to switch to surgical interventions or the use of drugs and/or medication. Patients can expect a thorough evaluation with a comprehensive questionnaire, followed by a physical examination. Lab tests and diagnostic instruments might be used to diagnose the source of back pain.
Spinal manipulation or adjustments take place on densely padded treatment tables which places the patients lying down, which allow the chiropractor to apply the necessary pressure. It is during these spinal adjustments that patients can experience the benign “popping” or “crackling” sound often associated with chiropractic care. A chiropractor might also utilize ultrasound therapy electrical stimulation and massage therapy to treat patients. Chiropractors might additionally suggest nutritional advice, such as the usage of vitamins, as well as recommend a few exercises to enhance the patient’s strength, flexibility and movement in order to help speed up the recovery process.
Chiropractic care is a well-known alternative treatment option for pain back. Some patients feel immediate relief following treatment, although a couple of people may experience mild aching or soreness. Before seeking a diagnosis for your back pain pain, however, it may be important for you to first understand several of the common causes of back pain. Having an understanding of the types of injuries and/or conditions which could be the source of your symptoms could help you and the chiropractor arrange the best type of treatment for your specific cause of back pain. Below are six of the most common causes of mechanical back pain.
Causes of Mechanical Back Pain
The most common causes of back and neck pain are mechanical, meaning they may manifest due to the movements of the spine. The mechanical parts of the spine include the tendons, ligaments, muscles, intervertebral discs and the facet joints. The most frequent region for mechanical back pain is the lumbar spine, or the lower back. This area of the spine�disperse and absorb the majority of the human body’s weight during active and static movement. Static means the body is stationary (eg, standing) although not actively moving (eg, walking). Meanwhile, the neck, or the cervical spine, is the most mobile region of the spinal column. Here, the spine supports the weight of the head. The diversity of motion includes nodding, bending forward, backward, and side to side movements.
However, even if the body isn’t moving, parts of the body continue to support the spine. There are also mechanical forces, such as gravity, pressure, compression and stress, which can still affect the spine. Below are six of the most common causes of mechanical back pain.
Back or Neck Sprain and Strain
A back or neck sprain occurs when a ligament of the spine, or a complex group of strong tissues that hold the bones of the spine together, is overstretched or torn as a result of trauma from an injury. In contrast, neck or back strain involves the over-stretching or tearing of a muscle or tendon attachment due to an injury. Because a sprain or strain can affect any of the complex structures in the spine, finding the exact source of the patient’s symptoms may be challenging without the proper equipment. If you sprain or strain your back (or neck), the delicate tissues are hurt and respond by swelling, thus causing pain and discomfort. Muscles that are affected may go into spasm which can also be painful. Stiffness is another symptom that may make movement difficult.
Disc Herniation
Intervertebral discs divide the drum-shaped vertebral bodies of the spine. Each disc is carefully anchored into place by endplates; a fibrous connective tissue that makes up each intervertebral disc. Intervertebral discs are made of fibrocartilage and allow a small amount of movement at each vertebral segment (2 vertebrae and one disk). The disc’s outer ring, known as the annulus fibrosis, protects the internal workings centre of the disc, known as the nucleus pulposus. Disc herniation occurs when the gel-like substance breaks through the outer ring, often causing nerve compression, inflammation, irritation, and pain. Pain may radiate or travel down to an arm or leg, depending on the region of the spine where the herniation occurred. Weakness, numbness, and tingling sensations can accompany pain and discomfort associated with the herniation of the discs. In addition, an intervertebral disc may rupture in various directions: front (anterior), back (posterior), and/or side (lateral), causing stress against the complex structures of the spine.
Vertebral Compression Fracture (VCF)
A vertebral compression fracture occurs when force from an impact causes the vertebrae of the spine to collapse. Trauma (eg, fall) is a common cause of vertebral compression fracture, though VCF is often related to osteoporosis, a weight loss reduction of bone mineral density and strength. A VCF can also occur during bending forwards or lifting. These fractures usually result in sudden and severe back pain.
Lumbar Spinal Stenosis (LSS)
Spinal stenosis in the lower back, or lumbar spine, develops when the nerve root passageways and/or the spinal canal become narrow. As a matter of fact, the term stenosis means “narrow”. When complex structures of the spine, such as the nerve roots, are compressed as a result of the narrowing of the spinal canal, the dominating symptoms includes pain and discomfort which radiates into one or both legs, a commonly known collection of symptoms referred to as sciatica. Lumbar spinal stenosis, or LSS, prevalently affects adults and may be related to hormonal changes which cause tissue or bone to develop into neural pathways, compressing the spinal cord canal.
Spinal Osteoarthritis (Spondylosis)
Spondylosis is a medical term used to define degenerative spinal osteoarthritis; frequent in older adults. Similar to other kinds of arthritis, spondylosis can affect the facet joints, causing symptoms of swelling, stiffness, pain in the back. It might develop in the neck, known as cervical spondylosis, mid back, known as thoracic spondylosis, and in the lower back, known as lumbar spondylosis. Spondylosis can consist of other degenerative changes that can often lead to disc herniation and spinal stenosis.
Spondylolisthesis
If one vertebral body slips forward over the vertebra underneath, it is characterized as spondylolisthesis. Spondylolisthesis may occur in the neck, however, the lower back or lumbar spine is most commonly affected by this type of condition. The diagnosis and identification of the severity of a patient’s spondylolisthesis includes determining the degree of the vertebrae’s movement. Grade 1 means the vertebra has shifted forward by about 25 percent where Grade 5 refers to a complete slip of the vertebra, known as spondyloptosis. Grade 5 might be caused by a fracture of the bone that helps stabilize the placement of the vertebrae. Aside from pain and discomfort, severe muscle spasms and sciatic-type symptoms may develop.
Dr. Alex Jimenez’s Insight
Although back pain is one of the most common complaints frequently treated in the medical field today, properly treating it may often be difficult because the source of the symptoms may be due to a variety of spinal health issues, including sprains and strains as well as spinal disc herniation and spinal stenosis. Chiropractic care is a popular, alternative treatment option commonly utilized to diagnose, treat and prevent a variety of injuries and/or conditions associated with the musculoskeletal and nervous system. After a thorough medical evaluation is performed by a chiropractor, the back pain specialist may use spinal adjustments and manual manipulations to carefully restore the original alignment of the spine. By correcting spinal misalignments, or subluxations, a chiropractor can release the tension and pressure being placed agains the spine, allowing the human body to naturally heal itself without the need for surgical interventions and drugs and/or medications. Visit a chiropractic care office to discuss the treatment options for your specific type of back pain.
In conclusion,�back pain can occur as a result of a variety of injuries and/or conditions. However, mechanical back pain, caused by the movement of the spine, has been referred to as the most common cause of back pain and spine health issues. Understanding the type of injuries and/or conditions discussed above can help you and the healthcare professional determine the best type of treatment for your specific health problems. Chiropractic care is a well-known alternative treatment option commonly utilized to help treat back pain symptoms, among other types of health issues.�The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Back Pain
According to statistics, approximately 80% of people will experience symptoms of back pain at least once throughout their lifetimes. Back pain is a common complaint which can result due to a variety of injuries and/or conditions. Often times, the natural degeneration of the spine with age can cause back pain. Herniated discs occur when the soft, gel-like center of an intervertebral disc pushes through a tear in its surrounding, outer ring of cartilage, compressing and irritating the nerve roots. Disc herniations most commonly occur along the lower back, or lumbar spine, but they may also occur along the cervical spine, or neck. The impingement of the nerves found in the low back due to injury and/or an aggravated condition can lead to symptoms of sciatica.
Chiropractic treatment is a nonsurgical option that can help reduce neck pain and related symptoms. Below are some of the different types of neck (cervical) conditions that Doctors of Chiropractic (DC’s) treat:
Chiropractors also use manual therapies to treat neck pain:
Cervical intervertebral disc injuries that don�t require surgery
Cervical sprain injuries
Degenerative joint syndrome of the neck (eg, facet joints)
A chiropractor evaluates the spine as a whole because other regions of the neck (cervical), mid back (thoracic) and low back (lumbar) can be affected as well. Along with treating the spine as a whole, chiropractic medicine treats the entire person and not just a specific symptom/s. Chiropractors may educate on nutrition, stress management, and lifestyle goals in addition to treating neck pain.
A chiropractor will do a thorough examination to diagnose the specific cause of the neck pain before deciding on which approach/technique to use.
They will determine any areas of restricted movement and will look at a walking cycle along with posture and spinal alignment. Doing these things can help the chiropractor understand the body’s mechanics.
In addition to the physical exam, a chiropractor will want to go over past medical history, and they may order imaging tests (eg, an x-ray or MRI) to help them diagnose the exact cause of the neck pain.
All these steps in the diagnostic process will give a chiropractor more information about the neck pain, which will help the� chiropractor create a customized treatment plan for the individual patient.
A chiropractor will rule out neck pain conditions that require surgery. If they believe surgery is the best treatment for the neck pain, then the patient will be referred to a spine surgeon.
Chiropractic Treatment: Neck Pain
A chiropractor may use a combination of spinal manipulation, manual therapy, and other techniques as part of the treatment plan.
Spinal Manipulation Techniques Used:
Flexion-Distraction Technique:�Gentle hands-on spinal manipulation that involves a pumping action on the intervertebral disc rather than direct force.
Instrument Assisted Manipulation:�Uses hand-held instruments, which allow the chiropractor to apply force without thrusting into the spine.
Specific Spinal Manipulation:�Restores joint movement with a gentle thrusting technique.
Chiropractors also use manual therapies to treat neck pain.
Instrument Assisted Soft Tissue Therapy: uses special instruments to diagnose and treat muscle tension.
Trigger Point Therapy is used to relieve tight, painful points on a muscle.
Other therapies used to ease neck pain symptoms.
Inferential Electrical Stimulation:�Is a low frequency electrical current used to stimulate neck muscles.
Ultrasound:�Sound waves travel into the muscle tissues to help stiffness and pain in the neck.
Therapeutic Exercises:�Helps improve overall range of motion in the neck and prevent neck pain from progressing.
The treatments listed are examples of possible chiropractic treatment for neck pain; The actual treatment plan will depend on the diagnosis. A chiropractor will thoroughly explain the treatment options available along with the actual customized treatment for the individual patient.
Chiropractic Clinic Extra: Neck Pain Care & Treatments
Improve Posture: Your mother always told you to stand up straight � and she was right. Good posture is very important. It is good for your health, your mood, and even how you are perceived by others. Good posture can help you stave off age related conditions and allow your vital organs plenty of room to do their job correctly.
Contents
Improve Posture With Chiropractic
A Word About Posture
Sometimes though things can happen that impact your posture. Maybe you sustain an injury and your body compensates by listing to one side or you hunch over in an effort to relieve the pain. Other times you may slouch in an effort to make yourself �invisible� in a crowd. Then there are those who just don�t give good posture its due and slouch because they simply don�t feel like standing up straight.
Whatever the case, poor posture can lead to back pain, headaches, increased risk of injury, decreased flexibility, and diminished mobility. It can actually cause you to age much faster. The good news is, in most cases even those with very poor posture can turn it around and stand a little taller. Chiropractic care has shown to help many people regain their youthful, straight, healthy posture that they�ve lost.
Postural Conditions That Chiropractic Care Can Help
There are certain postural conditions that chiropractic care is particularly helpful is alleviating, including:
Hip or pelvis unleveling
Scoliosis
Damage to the low back, mid back, and neck that affects its normal curvature
Forward head posture (often associated with using mobile devices)
Kyphosis or hunchback
Chiropractic Treatment For Posture Problems
When you first visit your chiropractor, he or she will sit down with you and discuss the problems you are having, what your complaints are, when the problem started, and events that may have contributed to the problem. They will take a thorough medical history and observe the way you sit, walk, bend, and move.
Your chiropractor may request x-rays and will assess the alignment of your spine. You may also be asked to have neurological or orthopedic testing done to ensure that there is no underlying condition or injury that is causing your problem.
You will be asked to stand straight and the doctor will take measurements to determine if there is any visible deviation from your optimum posture. He or she will ask you to move and bend while they test your range of motion, mobility and flexibility as well as your muscle strength and length.
A Prescription For Perfect Posture
Once your assessments are complete your chiropractor will discuss treatment options with you. He or she will walk you through the adjustments that will be done and other types of therapies they recommend. You will talk about the best course of action to relieve any pain that you are experiencing as well as get your spine back into alignment and improve your posture.
Your chiropractor will also likely talk to you about stretching exercises and things you can do at home in between appointments. They may discuss sleep positions, diet, work area adjustments, exercise, and weight loss. Chiropractic is a whole body treatment, addressing lifestyle changes that affect the entire body and getting it into optimal working order as a whole.
If you have poor posture you can change it, even if you are an older adult � or a senior. Often simple chiropractic adjustments can help improve posture within just a few sessions. Once your body is in alignment you will feel more energetic, healthier, and happier. Your body is an intricate machine and when one part isn�t functioning as it should, it affects all the other parts. Chiropractic can turn that around, helping your body function more effectively so you feel better.
Suffer Migraines: If you�ve ever had a migraine you know that it�s more than just a headache. The debilitating pain can be accompanied by nausea and other symptoms � and it�s more common than you may think. Research shows that in every four American households, one person is a migraine sufferer. In fact, 12 percent of the U.S. population suffers from migraines, including children. This means migraines affect more people that asthma and diabetes combined.
It is estimated that 18 percent of women suffer from migraines while 6 percent of men are migraine sufferers. It most commonly affects people who are between the ages of 25 and 55, but even young children have been diagnosed. Migraines can stop you in your tracks, but there are treatments that can help. Chiropractic care has been shown to help ease the pain, intensity, and frequency of migraines.
Contents
Suffer From Migraines
What Is A Migraine?
Migraines are vicious headaches that can last several minutes to several hours or even days. It is characterized by intense pulsing or a throbbing sensation that is typically confined to one area of the head. It is often accompanied by vomiting, nausea, and extreme sensitivity to sound and light. The pain can be so severe that you can barely function. Many people find themselves confined to bed in a darkened room, waiting for it to pass.
Many times migraine sufferers report experiencing an aura, or sensory warning symptoms, such as strange smells, blind spots, flashes of light, or tingling in your leg or arm. They also tend to run in families. If one parent is a migraine sufferer the child has a 40 percent chance of having migraines as well. If both parents get migraines that chance jumps to 90 percent. It is the 8th most debilitating illness on a global scale.
For the most part, doctors do not know much about what causes migraines. However, there are some things that have been identified as migraine triggers:
Hormonal changes � at certain times during the month, women experience fluctuations in estrogen which can trigger migraines
Oral contraceptives � medications that change or replace hormones can make headaches worse
Certain foods � processed foods, MSG, salty foods, aged cheeses
Fasting or skipping meals
Aspartame
Alcohol
Stress
Sensory overstimulation
Dehydration
Intense physical exertion
Too much or too little sleep
Medications
How Chiropractic Care Can Help Migraine Sufferers
Many doctors believe that headaches and migraines may be caused by a spine that is out of alignment. When your spine is misaligned your entire body suffers. It can irritate the nerves that run from the brain to the spine causing a headache. Chiropractic adjustments can help relieve the pain of migraines. In fact, many people report a distinct difference after just one session.
A Doctor of Chiropractic will align your spine and work with you to create a wellness plan that includes lifestyle changes and diet. Making changes to your sleep patterns and eliminating certain foods from your diet can help prevent migraines. By creating a whole body wellness program, you and your chiropractor can not only help prevent your migraines, but other health conditions as well.
Your chiropractor may also recommend that you keep a journal to help you pinpoint your own unique migraine triggers. You will record the foods you eat, environmental factors that may affect you, stressors, and sleep patterns, as well as when you have migraines, how long they last, and their severity. By tracking these things, you can determine what may be causing your migraines and make adjustments to your lifestyle, thus preventing them. Incorporating chiropractic care as part of your whole body maintenance, as well as migraine prevention, can help you stave off these headaches so you can get on with your life.
If you or a loved one suffers from migraine headaches, make sure you give us a call. Our Doctor of Chiropractic is here to help!
Approximately 8 out of 10 people living in the United States will experience back pain at least once throughout their lifetime. Fortunately, many healthcare professionals, including chiropractors and physical therapists, are qualified and experienced in the treatment of back pain. Because symptoms of back pain may occur due to a variety of health issues, however, properly diagnosing the source of an individual’s back pain in order to treat them accordingly may often be difficult.
Chiropractic care is a well-known, alternative treatment option commonly utilized to diagnose, treat and prevent a variety of injuries and/or conditions associated with the musculoskeletal and nervous system. A chiropractor, or doctor of chiropractic, will carefully use spinal adjustments and manual manipulations, among other treatment methods, to safely and effectively correct any spinal misalignment, or subluxation, found along the length of the spine which may be causing symptoms of back pain. By restoring the original alignment of the spine, a chiropractor can improve the function of the spine, allowing the human body to naturally heal itself without the need for invasive procedures and/or the use of drugs and/or medications.
Chiropractic care can improve a patient’s ability to better manage their back pain symptoms because it can help reduce pain and discomfort, decreases inflammation, and improves strength, mobility, and flexibility. Furthermore, a chiropractor may recommend lifestyle modifications, including nutritional changes and fitness advice, to speed up the patient’s recovery process. However, before seeking any type of treatment for your specific symptoms of back pain, it’s essential to understand the different types of back pain, its symptoms and its causes as well as what you can expect from a doctor visit for back pain.
Contents
Upper, Mid Back, Low and Lower Back
Back pain is one of the most common complaints frequently reported in doctor office visits on a regular basis. As a matter of fact, back pain has been identified to affect approximately three in four adults at least once through their lifetime. When referring to “back pain” healthcare professionals utilize the term loosely to medically define it as pain which originates anywhere between the upper back, or the cervical spine, and the lower back, or the lumbar spine, regardless of the cause of the symptoms.
Other Symptoms Associated with Back Pain
Back pain can also be characterized by different types of pain. Acute back pain is identified as short-term but severe in nature. Chronic back pain is long-term and may vary in intensity. It can often be severe, but it may also be identified as mild, deep, achy, burning, or electric-like in nature. Back pain which radiates into another part of the body, including the upper and/or lower extremities, is identified as radicular pain, particularly when it radiates below the knee, into the feet. This type of back pain is commonly known as lumbar radiculopathy. Fortunately, not all types of back pain include radiating pain symptoms.
It is not uncommon for back pain to cause other symptoms, such as numbness and tingling sensations, stiffness, achiness, and weakness. Furthermore, specific activities are known to aggravate existing back pain symptoms. Everyday activities like sitting, walking, standing, bending over, and twisting at the waist are several movements which can make back pain worse. However, not every patient will experience every symptoms associated with their specific type of back pain. Symptoms of back pain generally depend on the diagnosis, level of the injury and/or condition affecting the spine, or cause of back pain.
Dr. Alex Jimenez’s Insight
Back pain is a common symptom which affects about 80 percent of the population at least once throughout their lifetime. Because a variety of injuries and/or conditions may be the cause of back pain symptoms, many healthcare professionals consider the diagnosis of back pain to be difficult, however, back pain specialists, including chiropractors and physical therapists, can safely and effectively diagnose the source of an individual’s back pain symptoms. As a chiropractor, the use of spinal adjustments and manual manipulations can help naturally restore the original structure and function of the spine, without the need for drugs and/or medications or surgical interventions.
Understanding Back Pain Doctor Terms
When you visit a doctor regarding your symptoms, they may often use terms such as thoracic, lumbar, lumbosacral, or sacrum to describe your type of back pain. Back pain can originate anywhere along the spine, therefore, a healthcare professional will use the following terms to describe the source of the patient’s symptoms. The different regions of the spine are explained below.
The cervical spine refers to your neck.
The thoracic spine is found along the upper and middle regions of the back and where your ribs attach to the spinal column.
The lumbar spine refers to your low back.
The lumbosacral is found along the low back, sacrum, and the tailbone, also referred to as the coccyx.
The sacrum�refers to the part of the spine that is at the back of your pelvis.
Back pain can be challenging to properly diagnose because the spine consists of 17 vertebral bones, from the upper back to the tailbone, many joints, the sacrum and tailbone. In addition, the spine is made up of other fibrous and muscular supporting structures, intervertebral discs, the spinal cord and nerve roots, as well as blood vessels. Trauma from an injury, such as a back sprain/strain from lifting and twisting simultaneously, can cause immediate and severe back pain which may often become debilitating if left untreated.
Not all cases of back pain are due to trauma from an injury. Many other spinal health issues are congenital, meaning they developed since birth, degenerative or associated with age, due to disease, and they may even be connected to poor posture, obesity or the result of an unhealthy lifestyle habit, such as smoking. In other cases, the back pain may be worse than the severity of the injury and/or conditions causing it, which raises the question, �When should I seek medical attention for back pain?� If you are experiencing symptoms of back pain, among others commonly associated with spine health issues, you should seek immediate medical attentions if:
You cannot stand upright;
Fever accompanies pain;
Loss of bladder or bowel function or control occurs;
Leg pain and/or weakness progressively worsens; or if
Pain is relentless or worsens.
It’s normal for patients with back pain to feel afraid and anxious about seeking medical attention for their symptoms. Most individuals who experience severe and debilitating back pain will intuitively known when it’s time to receive the proper health care they need for their spinal health issues. Many healthcare professionals, such as chiropractors and physical therapists, are qualified and experienced back pain specialists who will help safely and effectively treat your specific back pain.
What to Expect from a Back Pain Specialist
Whether your doctor office visit is due to the urgent symptoms above or if you’re simply seeking immediate medical attention to prevent worsening back pain, below is a list of what you can expect in a back pain specialist visit. In order to properly diagnose the source of the patient’s back pain symptoms, a healthcare professional will first:
Review your medical history, including that of immediate family members who also have spinal health issues. Some instances of back pain, like scoliosis and osteoporosis, have a genetic potential.
Discuss when back pain started, what you were doing when the symptoms started, current severity and characteristics of your back pain as well as how these may have changed since they began, among other questions. Your doctor wants to learn as much about your pain and discomfort before they evaluate you accordingly�while the exam may be uncomfortable at first, your doctor doesn�t want to make the process intolerable.
Physical examination�to evaluate your vital signs, including heart rate. Blood pressure levels may become elevated as a result of pain. The doctor will examine your spine, feeling for abnormalities and areas of tenderness.
Neurological examination involves assessing sensation and function. The doctor may employ the pin prick test to determine if feeling is the same on both sides of particular parts of the body. Function, strength, mobility and flexibility are assessed while you walk, bend forward and backward (if able to), and during other movements. The doctor may also test your reflexes.
After a thorough examination, a healthcare professional should then be able to come up with a proper diagnosis for the patient’s back pain. To obtain more information and to help confirm the diagnosis, the doctor may order an X-ray, CT scan, or MRI. Sometimes lab tests may be ordered as well. It’s essential to keep in mind that an accurate diagnosis is essential towards a well-developed treatment plan. Once a proper diagnosis has been established, a healthcare professional will begin treatment accordingly, utilizing the recommended treatment methods for the patient’s specific cause of their back pain. Furthermore, a doctor may also be able to advice the patient regarding the best treatment methods to prevent further back pain.
In conclusion, back pain is a�common�symptoms which affects a majority of the population in the United States on a regular basis. Understanding the different types of back pain, its symptoms and its causes is essential towards receiving the right treatment from a qualified and experienced healthcare professional. Several procedures can be expected in a doctor office visit for back pain. Chiropractic care is a popular, alternative treatment option commonly utilized to help treat back pain and other injuries and/or conditions associated with the musculoskeletal and nervous system. A chiropractor, or doctor of chiropractic, will utilize spinal adjustments and manual manipulations to carefully restore the natural integrity of the spine, reducing symptoms of back pain. The overview above can help patient’s understand the process they must undergo in order to find relief from their back pain.�The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Back Pain
According to statistics, approximately 80% of people will experience symptoms of back pain at least once throughout their lifetimes. Back pain is a common complaint which can result due to a variety of injuries and/or conditions. Often times, the natural degeneration of the spine with age can cause back pain. Herniated discs occur when the soft, gel-like center of an intervertebral disc pushes through a tear in its surrounding, outer ring of cartilage, compressing and irritating the nerve roots. Disc herniations most commonly occur along the lower back, or lumbar spine, but they may also occur along the cervical spine, or neck. The impingement of the nerves found in the low back due to injury and/or an aggravated condition can lead to symptoms of sciatica.
Sports Performance is everything! Regardless of whether you�re a pro football player or a weekend warrior, your level of performance in your chosen athletic activity is what takes you to competitive heights.
There are certain things that every athlete knows will make them stronger, faster, more flexible, and have more stamina. Chiropractic care is becoming increasingly popular as a way for the sportsman in all of us to have that competitive edge.
You may know that chiropractic is great for people with back pain or even headaches, but you may be wondering how it can help an athlete. Solid research, along with a proven track record show that chiropractic helps sports performance in several key areas.
Contents
Sports Performance & Chiropractic
Increased Flexibility
Flexibility is important for nearly every sport and chiropractic care helps to increase flexibility throughout the body. As the spine is aligned, the body is better able to perform as it should and flexibility is a big part of that.
Better Mobility
When a person has better flexibility they are able to move around better. Chiropractic loosens the joints and spine, releasing energy to flow through the body. Blood flow is increased which means that nutrients and oxygen are carries much more efficiently to the vital organs and brain. This whole body wellness encourages better mobility.
More Resistant To Injury
Because chiropractic keeps the body flexible, there is a much lower risk of injury. Tight muscles can lead to injuries, sometimes serious injury. When the body well aligned and flexible the chances of a pulled or torn muscle or torn ligament are greatly decreased.
Helps Relieve Sports Hernias
Groin pain is a component of around 20 percent of all sports injuries. The thing is, it is often not due to sudden movements that result in injury like a torn muscle. Most of the time is it due to a condition called athletic pubalgia, or sports hernia.
Sports like hockey and football are full contact sports and injuries are not uncommon. However, even milder sports like horseback riding or cycling can also result in injuries or pain from over exertion. One study showed how chiropractic helped relieve the pain of shoulder instability in hockey players.
Chiropractic aligns the spine and body while increasing blood flow, but endorphins are also released through the treatment. This helps the body combat pain in a natural, less invasive way without the use of medications.
Increases Strength
While chiropractic care is typically regarded as a method for relieving pain and alleviating skeletal and muscular issues, it has also been found to improve physical strength. A study on judo athletes who received just three chiropractic care sessions showed that their grip strength improved by 16 percent.
Helps Sports Related Injuries Heal Faster
Chiropractic care has long been a standard practice for aiding in the healing of many sports related injuries including tennis elbow, hamstring pulls, rotator cuff injuries, back strains, and neck pain. While it does help prevent these injuries, in the event that they do occur, chiropractic care helps the athlete recover faster and get back in the game quicker.
So whether you enjoy the occasional game of touch football with the guys or you are a college basketball star, chances are you too can benefit from chiropractic care. Each of these benefits are exceptional in their own right and athletes rely on their chiropractor to keep them in the game, but all these little benefits add up to one significant plus: it improves sports performance. If you want to be stronger, faster, and more agile, the research shows that chiropractic care can certainly help.
Massage Therapy: Damaris Formeman is a massage therapist at Dr. Alex Jimenez’s chiropractic care clinic. As an employee, Damaris has witnessed the recovery process and the tremendous improvement of many patients receiving chiropractic care with Dr. Alex Jimenez. Damaris Formeman understands how chiropractic treatment methods, like massage therapy, can help patients with a variety of health issues, including sciatica, low back pain, neck pain and shoulder pain, among others. Damaris describes how each patient is carefully cared for by Dr. Alex Jimenez and she adds that building a strong bond with the patient during treatment is an important part of the patient’s healing journey.�
Massage Therapy Chiropractic Care
Massage therapy is medically defined as the manipulation of the soft tissues of the body for the purpose of restoring the health of those tissues. Massage therapy consists of manual techniques that include applying fixed or movable pressure and holding, and/or causing movement of or to the body. Massage is commonly believed to affect the circulation of blood and the flow of blood and lymph, reduce muscular tension or flaccidity, affect the nervous system through stimulation or sedation, and enhance tissue healing. These effects can provide a variety of health benefits for individuals affected by musculoskeletal injuries and conditions, including those affecting the nervous system, among others.
If you have enjoyed this video and/or we have helped you in any way please feel free to subscribe and share us.
Thank You & God Bless.
Dr. Alex Jimenez DC, C.C.S.T
Whole Body Wellness: Annually, chiropractors care for more than 30 million Americans, adults and children alike. Doctors of chiropractic are licensed to practice in all 50 states and in many nations around the world.
An increasing list of research studies and reviews has established that the treatment methods and techniques provided by chiropractic physicians are both safe and effective. The evidence strongly supports the natural, whole body wellness and cost-effective approach of chiropractic care for a variety of conditions.
Share Free Ebook
Chiropractic treatment is included in most health insurance plans, including: major medical plans, worker�s compensation, Medicare, some Medicaid plans, and Blue Cross Blue Shield plans for federal employees, and many others.
Chiropractic is used widely by young and professional athletes to help prevent and treat injuries and/or aggravated conditions as well as to aid them achieve optimal health and whole body wellness. Also commonly utilized by the general population, chiropractic care can help restore an individual�s original well being, increasing their strength, flexibility and mobility as well as decreasing symptoms such as pain, inflammation and discomfort caused by spinal complications. Following up with the chiropractor�s treatment recommendations can also help speed up the individual�s recovery process, helping them return to their everyday lifestyles.
Contents
Whole Body Wellness & Chiropractic
Many new patients are unsure about what to expect during their first appointment with a chiropractor. Foremost, a doctor of chiropractic will begin the consultation by taking a patient�s history and then performing a physical examination in order to develop a working diagnosis. Imaging or lab tests, including MRI, CT scans and/or X-rays, may be used to confirm a diagnosis.
The combination of the history, exam, and diagnostic study results will ultimately allow the chiropractor to determine a proper diagnosis for the individual�s injury or condition, which will then allow the healthcare professional to follow up with the best treatment procedures according to their overall health and wellness. If your chiropractor determines you would be more appropriately managed or co-managed by another healthcare professional, he or she will make the proper referral.
Through a process of shared decision-making, you and your chiropractic physician can establish which treatment methods and techniques will be right for you. As part of this process, the chiropractor will explain your injury and/or condition, recommend an appropriate treatment plan and finally, they will review the risks and benefits of all procedures with you.
As with all forms of treatment, time and patience is required to heal an injury or condition and visiting your chiropractor regularly can ensure the process is smooth and effective. Following the healthcare professional�s treatment plan accordingly is the best, most recommended decision you can take as an individual to achieve overall health and wellness.
Choosing A Whole Body Wellness Chiropractor
Ask Family/Friends For A Recommendation
A friend or family member who knows both you and the chiropractor may be able to judge whether your health philosophies and personalities are compatible.
Meet The Doctor
Many chiropractors will agree to a no-cost consultation to determine whether you are a good match. To make this visit as productive as possible, here are a few things to consider:
Does The Practice Focus On Vertebral Subluxation & Wellness?
Physical, biochemical, and psychological stress may result in spinal subluxations that disrupt nerve function and compromise your health. If you�re looking for a wellness chiropractor, it�s essential that this be the focus.
Some chiropractors confine their practice to the mechanical treatment of back and neck pain, and this is something you need to be aware of beforehand.
Does The Doctor Walk The Talk?
If he or she is overweight, looks unhealthy, or does not live a healthy lifestyle, this speaks volumes regarding their commitment to wellness.
Do The Two Of You Click?
Do you like each other? Do you communicate well? Avoid a doctor who seems rushed, talks down to you, or seems disinterested in listening to your concerns.
Does The Doctor Use Objective Assessments Of Nerve Function?
Since your care is not based just on addressing pain, your chiropractor should be using some form of objective assessment of your nerve function, as spinal subluxations can sometimes be asymptomatic.
Non-invasive instruments that measure the electrical activity in your muscles, and/or a thermal scanner that evaluates the function of your autonomic nervous system can be used, for example.
What Treatment Techniques Are Used?
Chiropractic techniques include low-force adjustments by hand, and more forceful adjustments using instruments. Ask which technique would be used on you, and if you have a preference, make sure the doctor is willing to use it.
As mentioned earlier, many chiropractors are also trained in other complementary techniques, so ask what else your doctor may have in their tool bag.
Dr. Alex Jimenez is an El Paso Chiropractor who has been helping people recover from their specific injuries or conditions through the use of chiropractic adjustments and manipulations. With over 27 years of experience, Dr. Jimenez can provide safe and effective care to those in need.
Low back pain represents one of the most common complaints in healthcare settings. While various injuries and conditions associated with the musculoskeletal and nervous system can cause low back pain, many healthcare professionals believe that work injury may have a prevalent connection to low back pain. For instance, improper posture and repetitive movements may often cause work-related injuries. In other cases, environmental accidents at work may cause work injuries. In any case, diagnosing the source of a patient’s low back pain to correctly determine which would be the best treatment method to restore the individual’s original health and wellness is generally challenging.
First and foremost, getting the right doctors for your specific source of low back pain is essential for finding relief from your symptoms. Many healthcare professionals are qualified and experienced in treating work-related low back pain, including doctors of chiropractic or chiropractors. As a result, several work injury treatment guidelines have been established to manage low back pain in healthcare settings. Chiropractic care focuses on diagnosing, treating, and preventing various injuries and conditions, such as LBP, associated with the musculoskeletal and nervous system. By carefully correcting the misalignment of the spine, chiropractic care can help improve symptoms of low back pain, among other symptoms. The purpose of the following article is to discuss occupational health guidelines for the management of low back pain.
Contents
Occupational Health Guidelines for the Management of Low Back Pain: an International Comparison
Abstract
Background: The enormous socioeconomic burden of low back pain emphasizes the need to manage this problem, especially in an occupational context effectively. To address this, occupational guidelines have been issued in various countries.
Aims: To compare available international guidelines for managing low back pain in an occupational health care setting.
Methods: The guidelines were compared regarding generally accepted quality criteria using the AGREE instrument and also summarised regarding the guideline committee, the presentation, the target group, and assessment and management recommendations (that is, advice, return to work strategy, and treatment).
Results and Conclusions: The results show that the guidelines variously met the quality criteria. Common flaws concerned the absence of proper external reviewing in the development process, lack of attention to organizational barriers and cost implications, and lack of information on the extent to which editors and developers were independent. There was general agreement on numerous issues fundamental to occupational health management of back pain. The assessment recommendations included diagnostic triage, screening for red flags and neurological problems, and identifying potential psychosocial and workplace barriers to recovery. The guidelines also agreed on advice that low back pain is a self-limiting condition and that remaining at work or an early (gradual) return to work, if necessary with modified duties, should be encouraged and supported.
Dr. Alex Jimenez’s Insight
Low back pain is one of the most prevalent health issues treated in chiropractic offices. Although the following article describes low back pain as a self limiting condition, the cause of an individual’s LBP can also trigger debilitating and severe pain and discomfort of left untreated. It’s important for an individual with symptoms of low back pain to seek proper treatment with a chiropractor to properly diagnose and treat their health issues as well as prevent them from returning in the future. Patients who experience low back pain for more than 3 months are less than 3 percent likely to return to work. Chiropractic care is a safe and effective alternative treatment option which can help restore the original function of the spine. Furthermore, a doctor of chiropractic, or chiropractor, can provide lifestyle modifications, such as nutritional and fitness advice, to speed up the patient’s recovery process. Healing through movement is essential for LBP recovery.
Low back pain (LBP) is one of the industrial countries’ most common health problems. Despite its benign nature and sound course, LBP is commonly associated with incapacity, productivity loss due to sick leave, and high societal costs.[1]
Because of that impact, there is an obvious need for effective management strategies based on scientific evidence derived from studies of sound methodological quality. Usually, these are randomized controlled trials (RCTs) on the effectiveness of therapeutic interventions, diagnostic studies, or prospective observational studies on risk factors or side effects. The scientific evidence, summarised in systematic reviews and meta-analyses, provides a solid basis for guidelines on managing LBP. In a previous paper, Koes et al. compared various existing clinical guidelines for managing LBP targeted at primary healthcare professionals, showing a considerable commonality.[2]
The problems in occupational health care are different. Management focuses mainly on counseling the worker with LBP and addressing the issues of assisting them to continue working or return to work (RTW) after sick listing. However, LBP is also an important issue in occupational health care because of the associated incapacity for work, productivity loss, and sick leave. Several guidelines, or sections of guidelines, have now been published dealing with the specific issues of management in an occupational health care setting. Since the evidence is international, it would be expected that the recommendations of different occupational guidelines for LBP would be more or less similar. However, it is not clear whether the guidelines meet currently accepted quality criteria.
This paper critically appraises available occupational guidelines on managing LBP and compares their assessment and management recommendations.
Main Messages
In various countries, occupational health guidelines are issued to improve the management of low back pain in an occupational context.
Common flaws of these guidelines concern the absence of proper external reviewing in the development process, lack of attention to organizational barriers and cost implications, and lack of information on the independence of editors and developers.
In general, the assessment recommendations in the guidelines consisted of diagnostic triage, screening for red flags and neurological problems, and identifying potential psychosocial and workplace barriers to recovery.
There is general agreement on advice that low back pain is a self-limiting condition and that remaining at work or an early (gradual) return to work, if necessary with modified duties, should be encouraged and supported.
Methods
Guidelines on the occupational health management of LBP were retrieved from the authors’ personal files. Retrieval was checked by a Medline search using the keywords low back pain, guidelines, and occupational up to October 2001, and personal communication with experts in the field. Policies had to meet the following inclusion criteria:
Guidelines aimed at managing workers with LBP (in occupational health care settings or addressing occupational issues) or separate sections of policies that dealt with these topics.
Guidelines are available in English or Dutch (or translated into these languages).
The exclusion criteria were:
Guidelines on primary prevention (that is, prevention before the onset of the symptoms) of work-related LBP (for example, lifting instructions for workers).
Clinical guidelines for the management of LBP in primary care.[2]
The quality of the included guidelines was appraised using the AGREE instrument, a generic tool designed primarily to help guideline developers and users assess the methodological quality of clinical practice guidelines.[3]
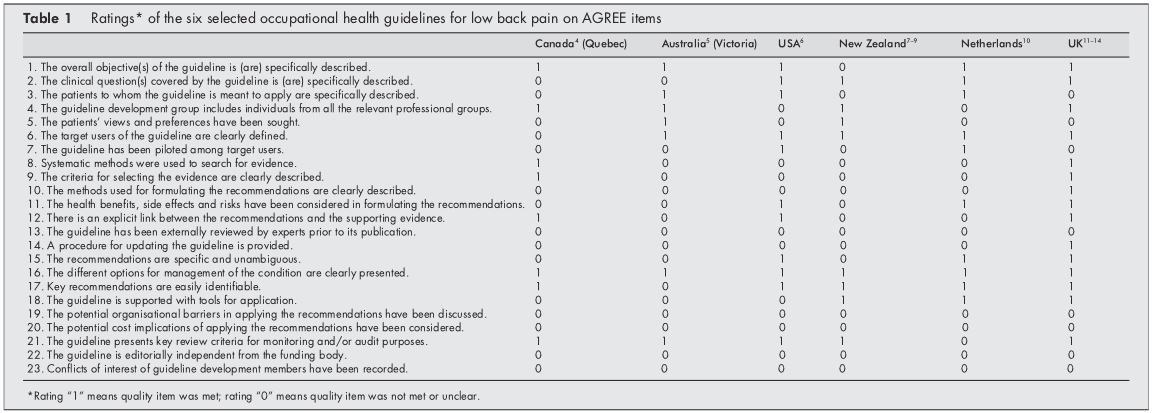
The AGREE instrument provides a framework for assessing the quality on 24 items (table 1), each rated on a four-point scale. The full operationalization is available on www.agreecollaboration.org.
Two reviewers (BS and HH) independently rated the quality of the guidelines and then met to discuss disagreements and to reach a consensus on the ratings. When they could not agree, a third reviewer (MvT) reconciled the remaining differences and decided on the ratings. To facilitate analysis in this review, ratings were transformed into dichotomous variables of whether each quality item was or was not met.
The assessment recommendations were summarised and compared to recommendations on advice, treatment, and return to work strategies. The selected guidelines were further characterized and reached regarding the guideline committee, the presentation of the procedure, the target group, and the extent to which the recommendations were based on available scientific evidence. All of this information was extracted directly from the published guidelines.
Policy Implications
The management of low back pain in occupational health care should follow evidence-based guidelines.
Future occupational guidelines for managing low back pain and updates of those guidelines should consider the criteria for proper development, implementation, and evaluation of approaches as suggested by the AGREE collaboration.
Results
Selection of Studies
Our search found ten guidelines, but four were excluded because they dealt with the management of LBP in primary care,[15] were aimed at the guidance of sick-listed employees in general (not specifically LBP),[16] were intended for the primary prevention of LBP at work,[17] or were not available in English or Dutch.[18] The final selection, therefore, consisted of the following six guidelines, listed by date of issue:
(1) Canada (Quebec). A scientific approach to the assessment and management of activity-related spinal disorders. A monograph for clinicians. Report of the Quebec Task Force on Spinal Disorders. Quebec Canada (1987).[4]
(2) Australia (Victoria). Guidelines for the management of employees with compensable low back pain. Victorian WorkCover Authority, Australia (1996).[5] (This is a revised version of guidelines developed by the South Australian WorkCover Corporation in October 1993.)
(3) the USA. Occupational Medicine Practice Guidelines. American College of Occupational and Environmental Medicine. USA (1997).[6]
(4) New Zealand
(a)Active and working! Managing acute low back pain in the workplace. Accident Compensation Corporation and National Health Committee. New Zealand (2000).[7]
(b)Patient guide to acute low back pain management. Accident Compensation Corporation and National Health Committee. New Zealand (1998).[8]
(c) Assess psychosocial yellow flags in acute low back pain. Accident Compensation Corporation and National Health Committee. New Zealand (1997).[9]
(5) the Netherlands. Dutch guideline for managing occupational physicians of employees with low back pain. Dutch Association of Occupational Medicine (NVAB). Netherlands (1999).[10]
(6) the UK
(a)Occupational health guidelines for managing low back pain at work principal recommendations. Faculty of Occupational Medicine. UK (2000).[11]
(b)Occupational health guidelines for managing low back pain at work leaflet for practitioners. Faculty of Occupational Medicine. UK (2000).[12]
(c)Occupational health guidelines for managing low back pain at work evidence review. Faculty of Occupational Medicine. UK (2000).[13]
(d)The Back Book, The Stationery Office. UK (1996).[14]
Two guidelines (4 and 6) could not be evaluated independently from additional documents to which they refer (4bc, 6bd), so these documents were also included in the review.
Appraisal of the Quality of the Guidelines
Initially, there was an agreement between the two reviewers regarding 106 (77%) of the 138 item ratings. After two meetings, the consensus was reached for all but four items, which required adjudication by the third reviewer. Table 1 presents the final ratings.
All included guidelines presented the different options for managing LBP in occupational health. In five of the six policies, the overall objectives of the procedure were explicitly described,[46, 1014] the target users of the system were clearly defined,[514] easily identifiable key recommendations were included,[4, 614] or critical review criteria were presented for monitoring and audit purposes.[49, 1114]
The results of the AGREE appraisal showed that none of the guidelines paid sufficient attention to potential organizational barriers and cost implications in implementing the recommendations. It was also unclear for all included guidelines whether or not they were editorially independent of the funding body and whether or not there were conflicts of interest for the members of the guideline development committees. Furthermore, it was unclear for all guidelines whether experts had externally reviewed the policies before publication. Only the UK guideline clearly described the method used to formulate the recommendations and provided for updating the approach.[11]
Development of the Guidelines
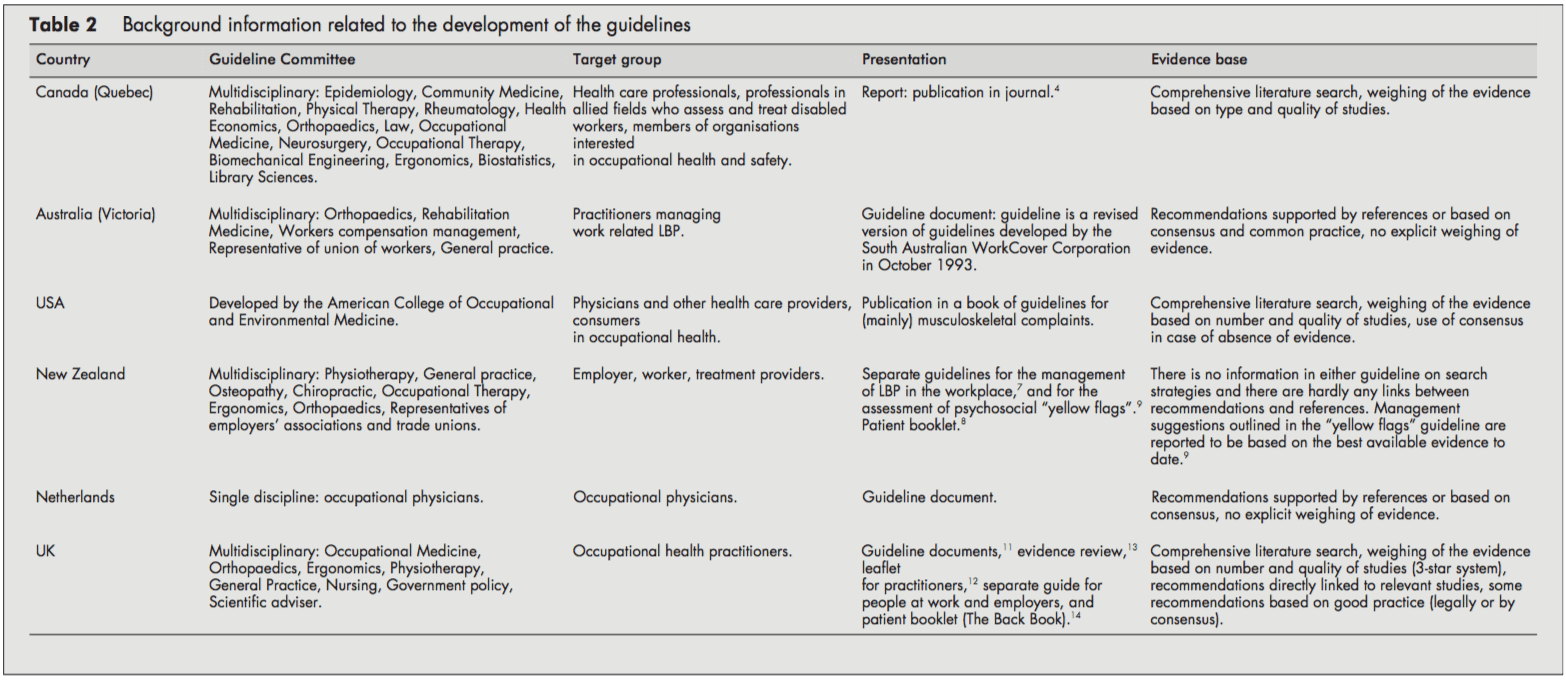
Table 2 presents background information on the development process of the guidelines.
The target users for the guidelines were physicians and other healthcare providers in the field of occupational healthcare. Several policies were also directed at informing employers, workers [68, 11, 14], or members of organizations interested in occupational health.[4] The Dutch guideline was only targeted at the occupational health physician.[10]
The guideline committees responsible for developing the guidelines were generally multidisciplinary, including disciplines like epidemiology, ergonomics, physiotherapy, general practice, occupational medicine, occupational therapy, orthopedics, and representatives of employers’ associations and trade unions. Chiropractic and osteopathic representatives were in the guideline committee of the New Zealand guidelines.[79] The Quebec task force (Canada) also included representatives of rehabilitation medicine, rheumatology, health economics, law, neurosurgery, biomechanical engineering, and library sciences. In contrast, the guideline committee of the Dutch guideline consisted only of occupational physicians.[10]
The guidelines were issued as a separate document,[4, 5, 10] as a chapter in a textbook,[6] or as several interrelated documents.[79, 1114]
The UK,[13] the USA,[6] and Canadian[4] guidelines provided information on the search strategy applied to the identification of relevant literature and the weighing of the evidence. On the other hand, the Dutch[10] and the Australian[5] guidelines supported their recommendations only by references. The New Zealand guidelines showed no direct links between suggestions and concerns [79]. The reader was referred to other literature for background information.
Patient Population and Diagnostic Recommendations
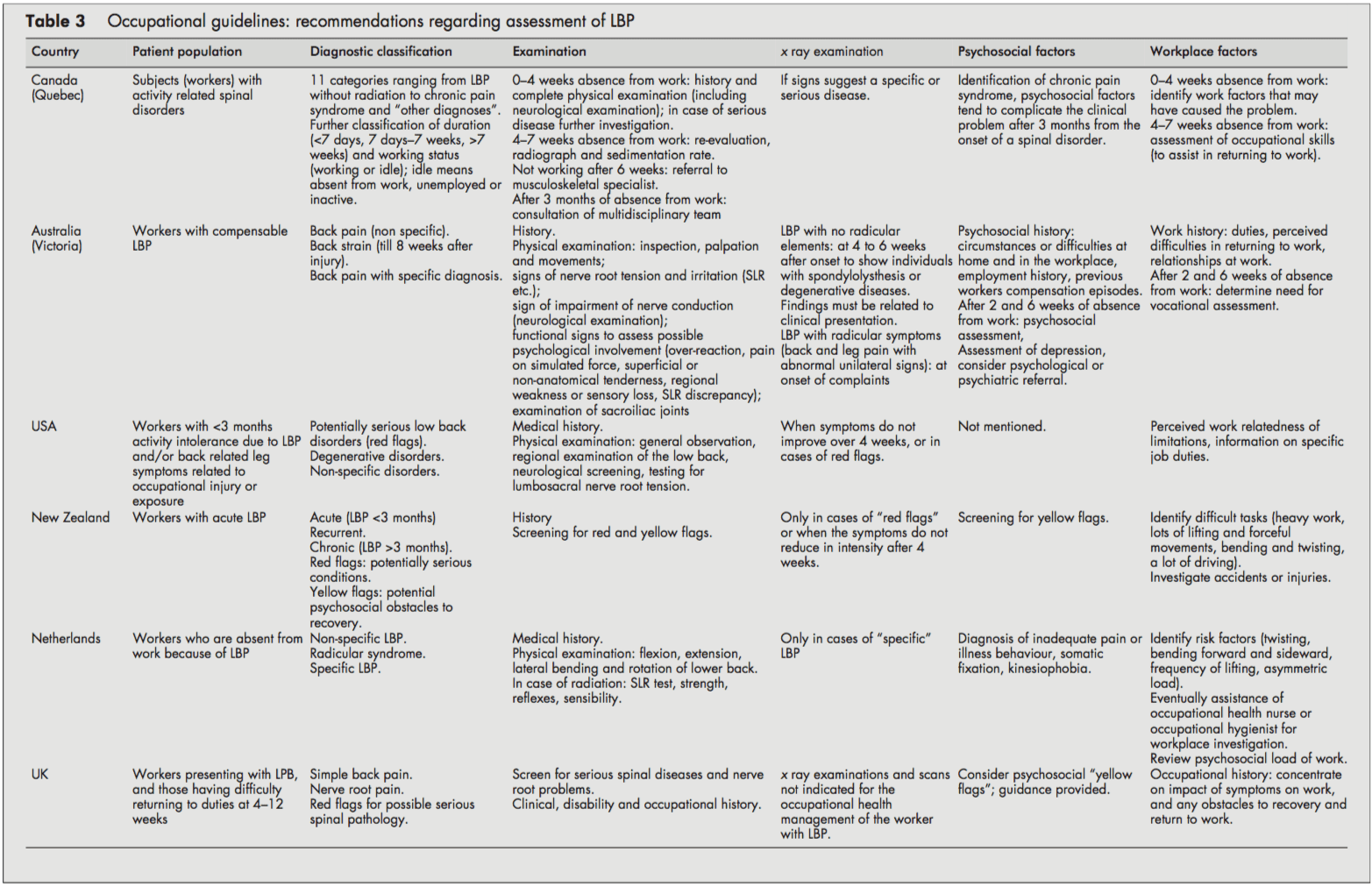
Although all guidelines focused on workers with LBP, it was often unclear whether they dealt with acute or chronic LBP or both. Acute and chronic LBP were often not defined, and cut-off points were given (for example, <3 months). It was usually unclear whether these referred to the onset of symptoms or absence from work. However, the Canadian guideline introduced a classification system (acute/subacute/ chronic) based on the distribution of claims of spinal disorders by time since absence from work.[4]
All guidelines distinguished specific and non-specific LBP. Specific LBP concerns the potentially serious red flag conditions like fractures, tumors, or infections, and the Dutch and UK guidelines also distinguish the radicular syndrome or nerve root pain.[1013] All procedures were consistent in their recommendations to take a clinical history and to carry out a physical examination, including neurological screening. In cases of suspected specific pathology (red flags), x-ray examinations were recommended by most guidelines. In addition, New Zealand and the US guideline also recommended an x-ray examination when symptoms did not improve after four weeks.[6, 9] The UK guideline stated that x-ray examinations are not indicated and do not assist occupational health management of the patient with LBP (distinct from any clinical indications).[1113]
Most guidelines considered psychosocial factors as yellow flags as obstacles to recovery that healthcare providers should address. The New Zealand[9] and UK guidelines [11, 12] explicitly listed factors and suggested questions to identify those psychosocial yellow flags.
All guidelines addressed the importance of the clinical history identifying physical and psychosocial workplace factors relevant to LBP, including physical demands of work (manual handling, lifting, bending, twisting, and exposure to whole-body vibration), accidents or injuries, and perceived difficulties in returning to work or relationships at work. The Dutch and the Canadian guidelines contained recommendations to carry out a workplace investigation[10] or an assessment of occupational skills when necessary.[4]
Summary of Recommendations for the Assessment of LBP
Diagnostic triage (non-specific LBP, radicular syndrome, specific LBP).
Exclude red flags and neurological screening.
Identify psychosocial factors and potential obstacles to recovery.
Identify workplace factors (physical and psychosocial) that may be related to the LBP problem and return to work.
X-Ray examinations are restricted to suspected cases of specific pathology.
Recommendations Regarding Information and Advice, Treatment, and Return to Work Strategies
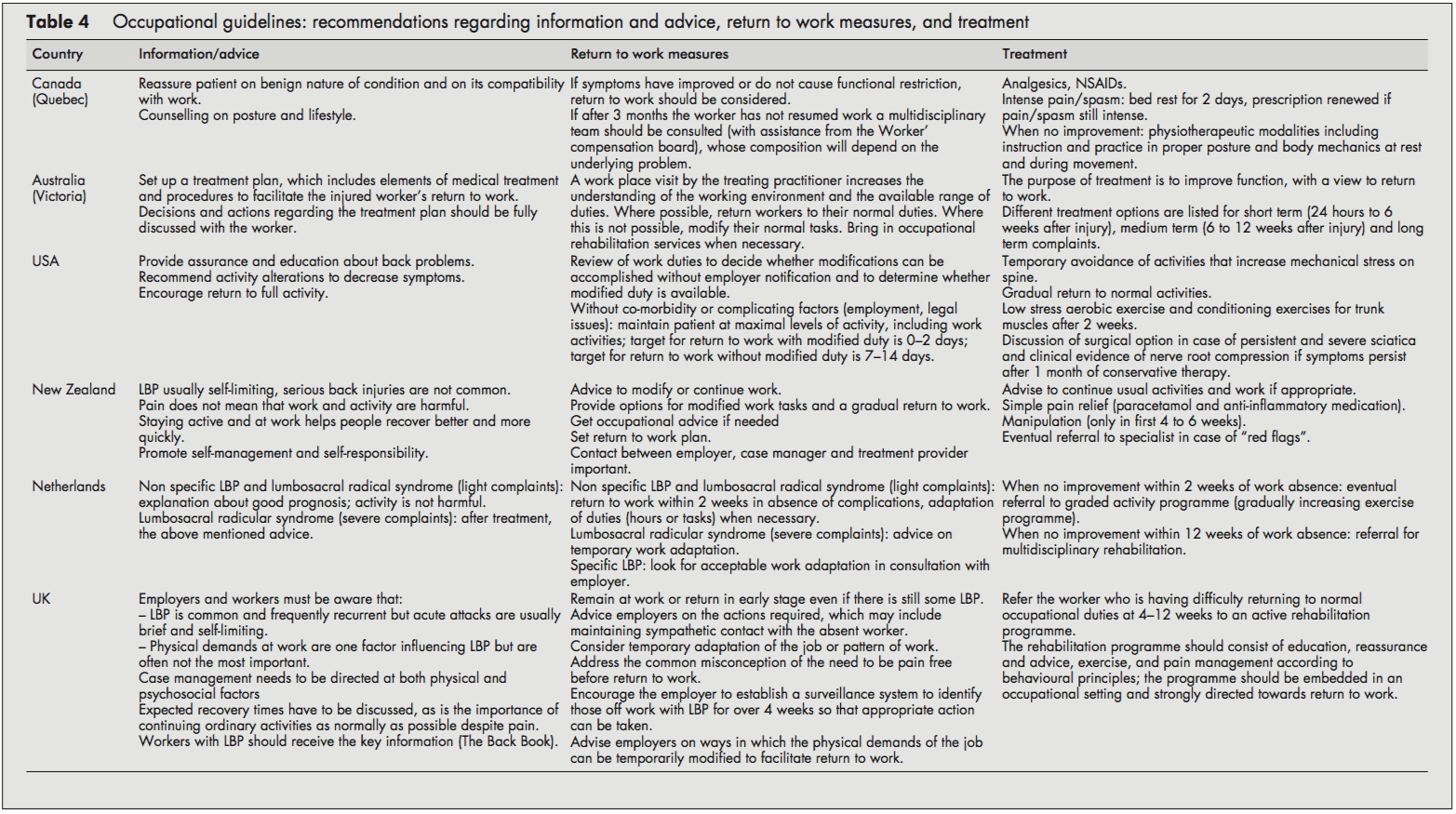
Most guidelines recommended reassuring the employee and providing information about LBP’s self-limiting nature and good prognosis. Encouragement of return to ordinary activity as generally as possible was frequently advised.
In line with the recommendation to return to regular activity, all guidelines also stressed the importance of returning to work as rapidly as possible, even if there is still some LBP and, if necessary, starting with modified duties in more severe cases. Work duties could then be increased gradually (hours and tasks) until total return to work was reached. The US and Dutch guidelines provided detailed time schedules for return to work. The Dutch approach proposed a return to work within two weeks with an adaptation of duties when necessary.[10] The Dutch system also stressed the importance of time-contingent management about a return to work.[10] The US guideline proposed every attempt to maintain the patient at maximal levels of activity, including work activities; targets for disability duration in terms of return to work were given as 02 days with modified duties and 714 days if modified duties are not used/available.[6] In contrast to the others, the Canadian guideline advised return to work only when symptoms and functional restrictions had improved.[4]
The most frequently recommended treatment options in all the included guidelines were: medication for pain relief,[5, 7, 8] gradually progressive exercise programs,[6, 10] and multidisciplinary rehabilitation.[1013] The US guideline recommended referral within two weeks to an exercise program consisting of aerobic exercises, conditioning exercises for trunk muscles, and exercise quota.[6] The Dutch guideline recommended that if there is no progress within two weeks of work absence, workers should be referred to a graded activity program (gradually increasing exercises) and, if there is no improvement by four weeks, to a multidisciplinary rehabilitation program.[10] The UK guideline recommended that workers who have difficulty returning to regular occupational duties by 412 weeks should be referred to an active rehabilitation program. This rehabilitation program should include education, reassurance and advice, a progressive vigorous exercise and fitness program, and pain management according to behavioral principles; it should be embedded in an occupational setting and directed firmly toward a return to work.[11-13] Extensive lists of possible treatment options were presented in the guidelines of Canada and Australia [4, 5], although most of these were not based on scientific evidence.
Summary of Recommendations Regarding Information, Advice, Return to Work Measures, and Treatment in Workers with LBP
Reassure the worker and provide adequate information about LBP’s self-limiting nature and good prognosis.
Advise the worker to continue ordinary activities or to return to regular exercise and work as soon as possible, even if there is still some pain.
Most workers with LBP return to more or less regular duties quite rapidly. Consider temporary adaptations of work duties (hours/tasks) only when necessary.
When a worker fails to return to work within 212 weeks (there is considerable variation in the time scale in different guidelines), refer them to a gradually increasing exercise program, or multidisciplinary rehabilitation (exercises, education, reassurance, and pain management following behavioral principles). These rehabilitation programs should be embedded in an occupational setting.
Discussion
The management of LBP in an occupational health setting must address the relation between low back complaints and work and develop strategies aimed at a safe return to work. This review compared available occupational health guidelines from various countries. Policies are rarely indexed in Medline, so when searching for guidelines, we had to rely primarily on personal files and personal communication.
Quality Aspects and Development Process of the Guidelines
The assessment by the AGREE instrument[3] showed some differences in the quality of the guidelines reviewed, which may partly reflect the variation in the dates of development and publication of the guidelines. The Canadian guideline, for example, was published in 1987 and the Australian guideline in 1996.[4, 5] The other guidelines were more recent and incorporated a more extensive evidence base and more up to date guideline methodology.
Several common flaws related to the development process of the guidelines were shown by the assessment by the AGREE instrument. Firstly, it is important to make clear whether a guideline is editorially independent from the funding body, and whether there are conflicts of interest for the members of the guideline committee. None of the included guidelines clearly reported these issues. Further, reported external review of the guideline by clinical and methodological experts prior to publication was also lacking in all guidelines included in this review.
Several guidelines provided comprehensive information on the way relevant literature was searched and translated into recommendations.[4, 6, 11, 13] Other guidelines supported their recommendations by references,[5, 7, 9, 10] but this does not permit assessment of the robustness of the guidelines or their recommendations.
Guidelines depend on the scientific evidence, which changes over time, and it is striking that only one guideline provided for future update.[11, 12] Possibly there are updates planned for the other guidelines but they are not explicitly stated (and conversely stating there will be future update does not mean it will actually occur). This lack of reporting may also hold true for other AGREE criteria that we rated negatively. The use of the AGREE framework as a guide for both the development and the reporting of guidelines should help to improve the quality of future guidelines.
Assessment and Management of LBP
The diagnostic procedures recommended in the occupational health guidelines were largely similar to the recommendations of clinical guidelines,[2] and, logically, the main difference was the emphasis on addressing occupational issues. The reported methods for addressing workplace factors in the assessment of LBP of the individual worker concerned the identification of difficult tasks, risk factors, and obstacles for return to work by occupational histories. Obviously, these obstacles for return to work not only concern physical load factors, but also work related psychosocial problems regarding responsibilities, cooperation with co-workers, and the social atmosphere at the workplace.[10] Screening for work related psychosocial yellow flags may help to identify those workers who are at risk for chronic pain and disability.[1113]
A potentially important feature of the guidelines is that they were consistent regarding their recommendations to reassure the employee with LBP, and to encourage and support return to work even with some persisting symptoms. There is general consensus that most workers do not have to wait until they are completely free of pain before returning to work. The lists of treatment options provided by the Canadian and Australian guidelines may reflect the lack of evidence at that time,[4, 5] leaving users of the guidelines to choose for themselves. It is, however, questionable whether such lists really contribute to improved care, and in our view guideline recommendations should be based on sound scientific evidence.
The US, Dutch, and UK occupational guidelines[6, 1013] recommend that active multidisciplinary treatment is the most promising intervention for return to work, and this is supported by strong evidence from RCTs.[19, 20] However, more research is still needed to identify the optimum content and intensity of those treatment packages.[13, 21]
Despite some evidence for a contribution of workplace factors in the aetiology of LBP,[22] systematic approaches for workplace adaptations are lacking, and are not offered as recommendations in the guidelines. Perhaps this represents a lack of confidence in the evidence on the overall impact of workplace factors, a difficulty of translation into practical guidance, or because these issues are confounded with local legislation (which was hinted at in the UK guideline[11]). It may be that the participatory ergonomics intervention, which proposes consultations with the worker, the employer, and an ergonomist, will turn out to be a useful return to work intervention.[23, 24] The potential value of getting all the players onside[25] was stressed in the Dutch and the UK guidelines,[1113] but further evaluation of this approach and its implementation is required.
Development of Future Guidelines in Occupational Health Care
The purpose of this review was to give both an overview and a critical appraisal of occupational guidelines for the management of LBP. The critical appraisal of the guidelines is meant to help direct future development and planned updates of guide- lines. In the still emerging field of guideline methodology we consider all past initiatives as laudable; we recognise the need for clinical guidance, and appreciate that guidelines developers cannot wait for research to provide all the methodology and evidence required. However, there is room for improvement and future guidelines and updates should consider the criteria for proper development, implementation, and evaluation of guidelines as suggested by the AGREE collaboration.
The implementation of the guidelines is beyond the scope of this review, but it was noted that none of the guideline documents specifically described implementation strategies, so it is uncertain to what extent the target groups may have been reached, and what effects that may have had. This may be a fruitful area for further research.
The very existence of these occupational health guidelines shows that existing primary care clinical guidelines for LBP2 are considered inappropriate or insufficient for occupational health care. There is a clear perception internationally that the needs of the worker experiencing back pain are intrinsically linked to a variety of occupational issues not covered by usual primary care guidance and, consequently, practice. What emerges is that, despite the methodological flaws, considerable agreement is evident on a range of fundamental occupational health strategies for managing the worker with back pain, some of which are innovative and challenge previously held views. There is agreement on the fundamental message that prolonged work loss is detrimental, and that early work return should be encouraged and facilitated; there is no need to wait for complete symptom resolution. Although the recommended strategies vary somewhat, there is considerable agreement on the value of positive reassurance and advice, availability of (temporary) modified work, addressing workplace factors (getting all the players onside), and rehabilitation for workers having difficulty returning to work.
Acknowledgements
This study was supported by the Dutch Health Care Insurance Council (CVZ), grant DPZ no. 169/0, Amstelveen, Netherlands. J B Staal is currently working at the Department of Epidemiology, Maastricht University, PO Box 616 6200 MD Maastricht, Netherlands. W van Mechelen is also part of the Research Centre on Physical Activity, Work and Health, Body@work TNO-VUmc.
In conclusion, symptoms of low back pain are one of the most common health issues associated with work injuries. Because of it, several occupational health guidelines have been established for the management of low back pain. Chiropractic care, among other treatment methods, may be utilized in order to help the patient find relief from their LBP. Furthermore, the article above demonstrated the safety and effectiveness of a variety of traditional as well as alternative treatment options in the diagnosis, treatment and prevention of a variety of low back pain cases. However, further research studies are required in order to properly determine the efficiency of each individual treatment method. Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Back Pain
According to statistics, approximately 80% of people will experience symptoms of back pain at least once throughout their lifetimes. Back pain is a common complaint which can result due to a variety of injuries and/or conditions. Often times, the natural degeneration of the spine with age can cause back pain. Herniated discs occur when the soft, gel-like center of an intervertebral disc pushes through a tear in its surrounding, outer ring of cartilage, compressing and irritating the nerve roots. Disc herniations most commonly occur along the lower back, or lumbar spine, but they may also occur along the cervical spine, or neck. The impingement of the nerves found in the low back due to injury and/or an aggravated condition can lead to symptoms of sciatica.
1. Van Tulder MW, Koes BW, Bouter LM. A cost-of-illness study of back pain in the Netherlands. Pain 1995;62:233�40.
2. Koes BW, van Tulder MW, Ostelo R, et al. Clinical guidelines for the management of low back pain in primary care: an international
comparison. Spine 2001;26:2504�14.
3. The AGREE Collaboration. Appraisal of Guidelines Research &
Evaluation Instrument, www.agreecollaboration.org.
4. Spitzer WO, Leblanc FE, Dupuis M. Scientific approach to the
assessment and management of activity-related spinal disorders. A monograph for clinicians. Report of the Quebec Task Force on Spinal Disorders. Spine 1987;12(suppl 7S):1�59.
5. Victorian WorkCover Authority. Guidelines for the management of employees with compensable low back pain. Melbourne: Victorian WorkCover Authority, 1996.
6. Harris JS. Occupational medicine practice guidelines. Beverly, MA: OEM Press, 1997.
7. Accident Compensation Corporation and National Health Committee. Active and working! Managing acute low back pain in the workplace. Wellington, New Zealand, 2000.
8. Accident Compensation Corporation and National Health Committee, Ministry of Health. Patient guide to acute low back pain management. Wellington, New Zealand, 1998.
9. Kendall, Linton SJ, Main CJ. Guide to assessing psychosocial yellow flags in acute low back pain. Risk factors for long-term disability and work loss. Wellington, New Zealand, Accident Rehabilitation & Compensation Insurance Corporation of New Zealand and the National Health Committee, 1997.
10. Nederlandse Vereniging voor Arbeids- en Bedrijfsgeneeskunde (Dutch Association of Occupational Medicine, NVAB). Handelen van de bedrijfsarts bij werknemers met lage-rugklachten. Richtlijnen voor Bedrijfsartsen. [Dutch guideline for the management of occupational physicians of employees with low back pain]. April 1999.
11. Carter JT, Birell LN. Occupational health guidelines for the management of low back pain at work�principal recommendations. London: Faculty of Occupational Medicine, 2000 (www.facoccmed.ac.uk).
12. Occupational health guidelines for the management of low back pain at work�leaflet for practitioners. London: Faculty of Occupational Medicine, 2000 (www.facoccmed.ac.uk).
13. Waddell G, Burton AK. Occupational health guidelines for the management of low back pain at work�evidence review. Occup Med 2001;51:124�35.
14. Roland M, et al. The back book. Norwich: The Stationery Office, 1996.
15. ICSI. Health care guideline. Adult low back pain. Institute for Clinical Systems Integration, 1998 (www.icsi.org/guide/).
16. Kazimirski JC. CMA policy summary: The physician�s role in helping patients return to work after an illness or injury. CMAJ 1997;156:680A�680C.
17. Yamamoto S. Guidelines on worksite prevention of low back pain. Labour standards bureau notification, No. 57. Industrial Health 1997;35:143�72.
18. INSERM. Les Lombalgies en milieu professionel: quel facteurs de risque et quelle prevention? [Low back pain at the workplace: risk factors and prevention]. Paris: les editions INSERM, Synthese bibliographique realise a la demande de la CANAM, 2000.
19. Lindstro?m I, Ohlund C, Eek C, et al. The effect of graded activity on patients with subacute low back pain: a randomised prospective clinical study with an operant-conditioning behavioural approach. Physical Therapy 1992;72:279�93.
20. Karjalainen K, Malmivaara A, van Tulder M, et al. Multidisciplinary biopsychosocial rehabilitation for subacute low back pain in working-age adults: a systematic review within the framework of the Cochrane Collaboration Back Review Group. Spine 2001;26:262�9.
21. Staal JB, Hlobil H, van Tulder MW, et al. Return-to-work interventions for low back pain: a descriptive review of contents and concepts of working mechanisms. Sports Med 2002;32:251�67.
22. Hoogendoorn WE, van Poppel MN, Bongers PM, et al. Physical load during work and leisure time as risk factors for back pain. Scand J Work Environ Health 1999;25:387�403.
23. Loisel P, Gosselin L, Durand P, et al. A population-based, randomised clinical trial on back pain management. Spine 1997;22:2911�18.
24. Loisel P, Gosselin L, Durand P, et al. Implementation of a participatory ergonomics program in the rehabilitation of workers suffering from subacute back pain. Appl Ergon 2001;32:53�60.
25. Frank J, Sinclair S, Hogg-Johnson S, et al. Preventing disability from work-related low-back pain. New evidence gives new hope�if we can just get all the players onside. CMAJ 1998;158:1625�31.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine

 If you have enjoyed this video and/or we have helped you in any way please feel free to subscribe and share us.
If you have enjoyed this video and/or we have helped you in any way please feel free to subscribe and share us.
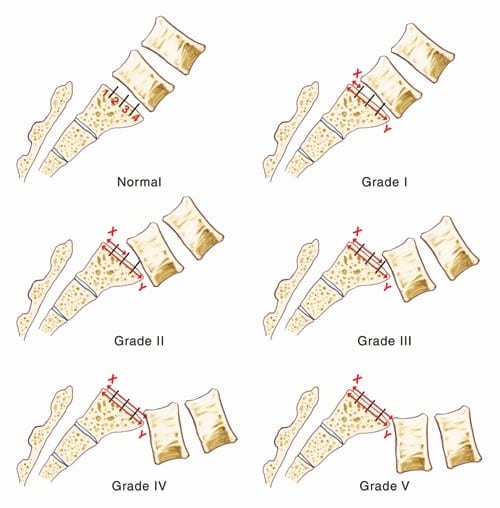




 A chiropractor may use a combination of spinal manipulation, manual therapy, and other techniques as part of the treatment plan.
A chiropractor may use a combination of spinal manipulation, manual therapy, and other techniques as part of the treatment plan.








 Choosing A Whole Body Wellness Chiropractor
Choosing A Whole Body Wellness Chiropractor