Chiropractic care focuses not only on the skeletal system and joints but also on the treatment of muscle pain. The muscles are interwoven with fascia, a type of tissue that allows muscles to glide smoothly over one another. Both muscles and fascia can develop painful adhesions, often recognized by their hard or knot like texture under the skin.
Muscle pain can be quite uncomfortable and even debilitating in certain cases. When you are suffering from muscle pain, your chiropractor can provide some much-needed relief using a variety of effective treatment options.
Contents
What is it?
The word �myofascial� is a mouthful, but there is a reason it is used by chiropractors. The first part of the word, �myo�, generally refers to your muscles. The second part of the word, �fascia�, refers to the connective tissue that is found all throughout your body. Myofascial pain syndrome is used to indicate muscle pain in its various forms. This may include issues with your fascia, muscle tissue, or both.
Myofascial pain can vary considerably, ranging from mild and frustrating to completely debilitating. Fortunately, whatever the intensity of the discomfort, chiropractic treatment can provide a solution that lessens and often eliminates the pain.
Trigger Points
The knots you have probably felt in your muscles or had others identify are also known as trigger points. These tight spots are often sensitive to the touch and can be found in any muscle in your body. As they develop, they may produce symptoms like numbness, burning, weakness, pain, and tingling.
Trigger points are caused by trauma to the body, such as an accident in a car or during athletics. They can also be caused by more mild, long-term trauma, such as working at a desk without proper ergonomics or making a repetitive motion over a long period of time.
Trigger points are challenging to identify sometimes because they occur at different spots in different people. They also produce something called �referred pain�, a pain that is felt somewhere else besides where the actual trigger point is. Chiropractors are trained to track down trigger points, though, so even if they are somewhat hidden by referred pain, they can be found eventually.
How Chiropractic Helps with Myofascial Pain Syndrome
Chiropractors are not only good at finding trigger points, but they are also good at treating them. They accomplish this using a variety of techniques. Some of the benefits of chiropractic for myofascial pain include:
Adhesion Break Up
Trauma in the muscles can cause adhesions to form. Adhesions are when muscle fibers and/or fascia bond together into a form of scar tissue. The adhesions cause the muscles to catch instead of slide smoothly, which can have a cascading effect on the body. Not only does the adhesion hurt, but it also causes joints to become misaligned and further problems to develop.
Trigger Point Pressure
Sometimes the most effective way to treat a trigger point is to apply pressure to smooth out the muscle and fascia. Chiropractors can do this with their hands or specific tools.
Alignment Improved
The cause of trigger points and muscle pain is often trauma, but sometimes the trauma is not as obvious as an accident or a trauma directly to the affected area. Misalignment in the spine or the extremities can cause the body to move incorrectly. Over time, the incorrect movement patterns can put extra strain on the muscles. Chiropractic focuses on helping your whole body become aligned, which can ease muscle pain and prevent further issues from developing.
Muscle Pain
Please contact our office to schedule an appointment with a chiropractor. Let us help alleviate your muscle pain and get you back on your feet again!
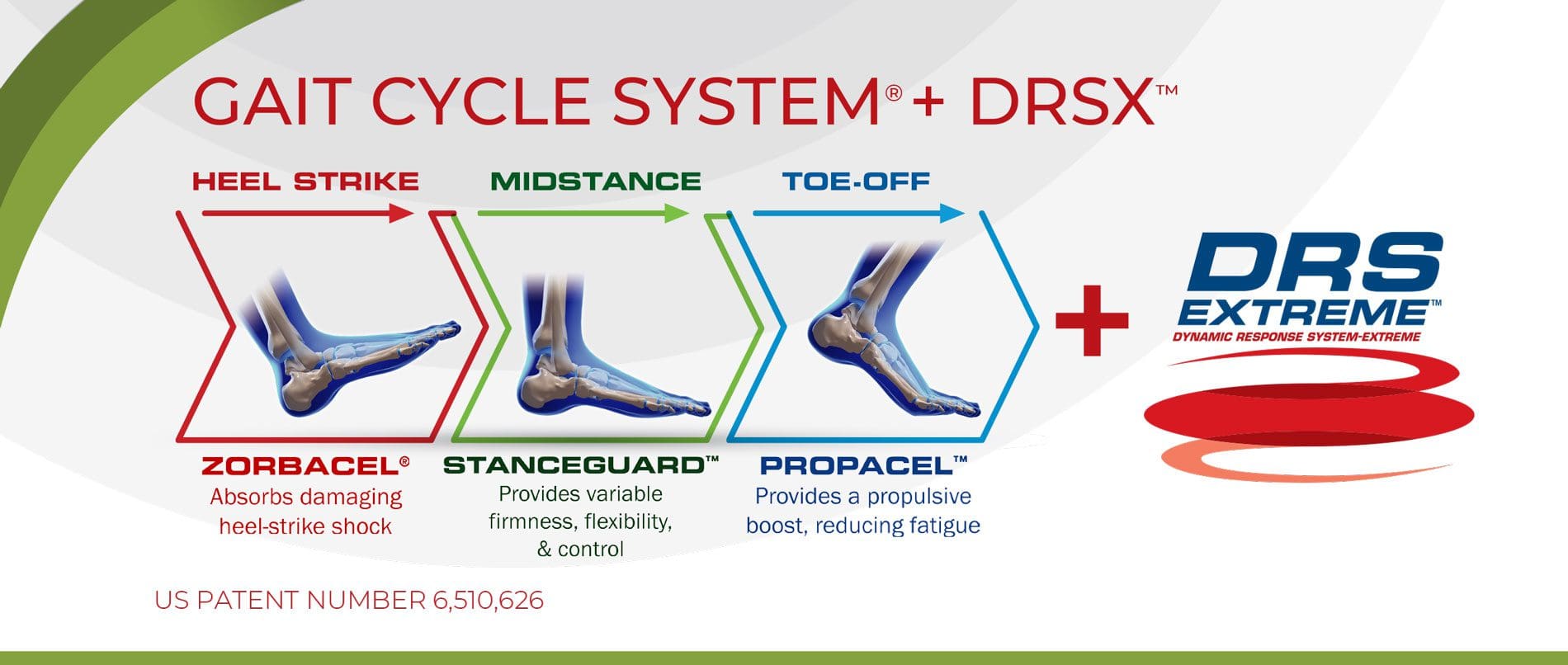
The Difference of Using *CHIROPRACTIC ORTHOTICS* | El Paso, Tx
Support for the 3 Arches
The feet are the foundation of the body. They provide the stability to perform activities by supporting the weight of the entire body using the 3-arched bond called the plantar vault.
The plantar vault provides numerous benefits:
Balances the body
Propels us forward
Absorbs heel-strike shock
Walking and running stresses adaptation
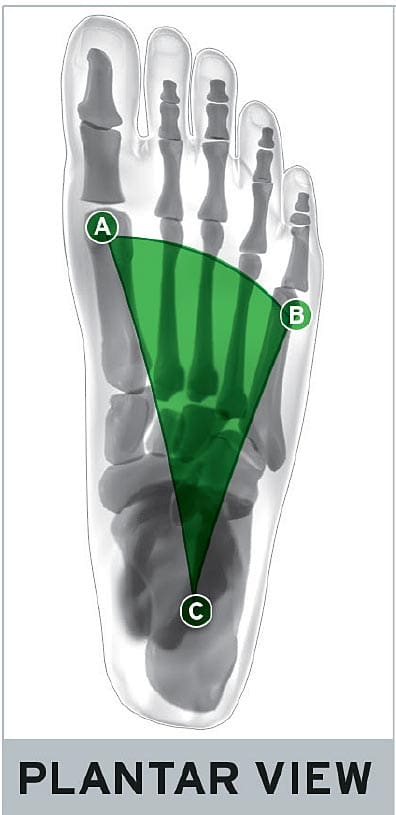
The Plantar Vault
The foot is made up of 3 arches. These arches are what keep the body balanced:
Medial longitudinal arch (A�C)
Lateral longitudinal arch (B�C)
Anterior transverse (metatarsal) arch (A�B)
Together, these 3 arches form an extremely strong, supportive �plantar vault� that distributes weight evenly throughout the entire body.
Arch Collapse
Over time, one or more of the arches will weaken due to pressure and wear and tear. This process is completely natural but injuries, a short leg, improper posture, and naturally weak ligaments and tendons can cause the collapse.
Custom-made orthotics are designed to provide the best possible support for all 3 arches:
Individually crafted from 3D scans to bolster the arches in your feet
Prescribed through Chiropractors to ensure you get the best possible orthotic
Available in a variety of styles and builds to suit your lifestyle and needs
Custom orthotics are designed to provide both the instant �ah� factor that over-the-counter orthotics like to market, and the actual needed support for your arches that will relieve pain now and prevent pain later by compensating for any and all of your weakened arches to correct your posture.
Orthotics For All Occasions
Typically, overpronation and oversupination, are caused by muscle imbalances in the foot, ankle, and lower leg. Improper shoes, misalignment in the body, and other issues can cause these muscle imbalances. The chiropractor will work with the patient to find the cause of the foot problem so that can be corrected, then work to the damage or injury done.
Overpronation and oversupination can cause a variety of injuries and conditions that affect not only the feet and ankles, but also the knees,�hips, and back as well.
NCBI Resources
The human body is an intricate machine, and everything is connected so when something goes wrong in one area, it can cause problems in other areas. The back carries a lot of the stress in the body so when there is a problem with the hips, knees, or a foot dysfunction, the spine can bear at least some of the brunt of the pain and other effects.
As people grow into adults, maintaining normal flexibility gets to be much more challenging and losing flexibility can result in a lot of pain to the musculoskeletal system.
Unfortunately, many of us do not retain flexibility throughout the day, even when attempting to be active. Many jobs are largely sedentary, and even leisure activities keep us stuck in one place. In order to remain functional, joints and muscles need to be used, which means they need to be properly stretched without being overworked. The balance is often very delicate, fortunately, chiropractic adjustments increase flexibility.
Contents
Chiropractic’s Role in Flexibility
Most adults are not concerned with being able to twist like a pretzel, however, they do want to be able to maneuver through daily life without a lot of pain. One of the main things accomplished in most chiropractic visits is that the chiropractor will look for misalignments in the spine and seek to correct them with a combination of chiropractic adjustments and exercises.
Adjustments
When the spine is misaligned it can affect many different areas of the body including flexibility. Someone who is not flexible will have a limited range of motion (ROM) and treatments are designed to improve this and restore natural posture.
But being flexible is about more than moving better. When the body is stiff, even simple movement results in pain because it is blocked by the misalignment. When this is adjusted/corrected, blood flow improves and the process of improving flexibility becomes less taxing.
Nutrition
There is more to a chiropractor’s day than correcting misalignments in the spine. Chiropractic is holistic in nature and in order to be truly successful, it relies on the patient to be a cooperative participant in treatment. Giving nutritional advice is a big part of this.
While advice can vary from patient to patient, generally, when a person struggling with flexibility adds protein and fatty acids into their diet it can help joints and muscles to be properly nourished. People should also monitor their intake of processed and pre-packaged foods as these can contribute to inflammation.
Training Exercises
Because of many factors in our lives, as well as the effects of aging, people’s range of motion inevitably decreases as time goes by, especially if nothing is purposefully done to maintain it. Flexibility exercises are commonly strongly suggested by chiropractors as they strive to help their patients with range of motion (ROM) and flexibility issues.
In many cases, such as those where someone is suffering from tendinitis or bursitis, the truly therapeutic exercises are resistive exercises. These, however, are limited, unless a higher level of flexibility is achieved.
Flexibility programs are implemented in order to make a given joint have a wider level of extensibility, which may be achieved by either traditional static stretching or Proprioceptive Neuromuscular Facilitation (PNF) techniques, which incorporates a slow reversal hold.
Working with a chiropractor on a regular basis for help in gaining flexibility can help assure that a patient moves forward at an appropriate pace that is in line with their age and fitness level. This will help them achieve a higher level of success in their chosen sport or similar activity, and/or become more productive in their daily lives while experiencing less pain.
*FIX BAD POSTURE* with Custom Orthotics | El Paso, TX (2019)
Proper Posture
Your spine does more than keep your body upright: it�s the brain that communicates to the rest of the body. Posture even affects your emotional well-being, including self-confidence!
Poor posture takes a serious toll on health. Here are a few of the negative results:
Muscle soreness
Subluxations
Blood vessel constriction
Nerve constriction
As the years go by the problems worsen, which results
Maintaining proper posture involves sitting, standing, and lying down properly. Here is an excerpt from the American Chiropractic Association website on how to:
Sit the right way
Keep your feet on the floor or on a footrest, if they can’t reach the floor
Don’t cross your legs. Your ankles should be in front of your knees
Keep a small gap between the back of your knees and the front of your seat.
Your knees should be at or below the level of your hips.
Bear your weight primarily on the balls of your feet.
Keep your knees slightly bent.
Keep your feet about shoulder-width apart.
Let your arms hang naturally down the sides of the body.
Lie down the right way
Find the mattress that is right for you. While a firm mattress is generally recommended, some people find that softer mattresses reduce their back pain. Go with your comfort
Sleep with a pillow. Special pillows can help with postural problems resulting from a poor sleeping position
Avoid sleeping on your stomach
Healthy Feet Equals A Healthy Spine
The feet are complex structures which function�to provide protection and support to the body in relation to the spine and head posture. The feet are essential towards balancing the body�s entire weight, allowing it to walk, run, stand, and, jump. Consequently, foot complications may cause severe issues throughout the spine, hips, knees, and ankles if left untreated.
Gait & Chronic Postural Pain
Chiropractic care can be effective for treating injuries or conditions such as plantar fasciitis, Achilles tendonitis, and ankle sprains, among others. Foot health is essential towards establishing the body�s proper support and balance, together with a proper spinal posture. In the presence of foot complications, chiropractic treatment can be used to achieve long-lasting health.
NCBI Resources
Flexibility is a critical component of keeping your body fit and healthy. Research shows that people who are more flexible are better able to reach their�optimum fitness level. It can also help to prevent injury and reduce your risk of conditions like arthritis and other�chronic diseases.�They also have a better range of motion and mobility as they age.
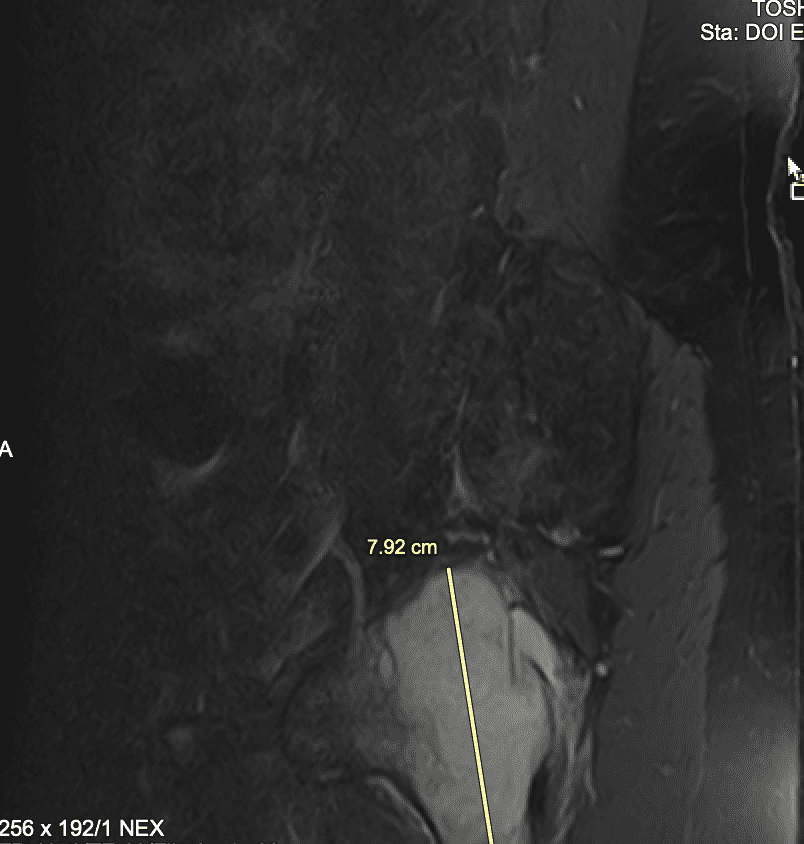
It’s natural for people to wonder whether an underlying health issue may be due to a tumor or another serious health issue, especially when you’ve got severe pain and discomfort. Tumors in the spine can cause back pain when the growth weakens the bone, which can ultimately result in spinal fractures, compression or impingement of the nerves, and spinal distress. �
Contents
Spinal Tumor Symptoms
Spinal tumor symptoms may ultimately be similar to those of other well-known health issues, including sciatica, especially if the spinal tumor irritates the sciatic nerve. The symptoms below may be commonly associated with a spinal tumor, including: �
Neck pain or back pain followed by neurological health issues, such as tingling sensations, weakness, and numbness in the upper and lower extremities as well as abnormal bladder and bowel habits.
Painful symptoms, particularly in the morning
Severe pain with manipulation of the affected region of the spine
Painful symptoms which do not decrease with rest
Back pain and other associated symptoms, such as loss of appetite, nausea, vomiting, weight loss, fever, or chills.
Other Symptoms of Spinal Tumors
Spinal tumors themselves may present a variety of other symptoms. Characteristics associated with spinal tumors include: �
Tumors which develop in the spine (primary tumors) are very rare
Spinal tumors grow slowly and are benign, frequently occurring in younger adults
Most spinal tumors have spread (metastasized) from another region of the human body
For individuals who have cancer, an evaluation is required to determine if cancer has spread to the spine
Types of Spinal Tumors
Most back pain is caused by other health issues. However, when painful symptoms are caused by spinal tumors, it’s essential for a healthcare professional to perform an accurate diagnosis to follow-up with proper treatment. There are three types of tumors which can cause back pain; vertebral column tumors, intradural-extramedullary tumors, and intramedullary tumors. �
Vertebral Column Tumors
Primary tumors: These type of tumors develop from the vertebrae or intervertebral discs in the spine. These commonly occur in younger adults. Osteogenic sarcoma, or osteosarcoma, is the most common type of malignant bone tumor. Many primary spinal tumors are generally considered to be rare and they will frequently grow slowly. � Metastatic tumors: These type of tumors frequently spread, or metastasize, from cancer in a different region of the human body. These spinal tumors will generally cause pain which doesn’t decrease with rest, can worsen at night and is commonly accompanied by other symptoms of spinal tumors, such as nausea or vomiting, weight loss, and fever or chills. In women, spinal tumors can spread from breast or lung cancer. In men, spinal tumors can spread from lung or prostate cancer. �
Intradural-Extramedullary Tumors
Intradural-Extramedullary tumors develop inside the spinal canal below the membrane which protects the spinal cord but outside of the nerves. These spinal tumors grow slowly and are benign. However, they can cause pain and fatigue. � Meningiomas: These type of tumors commonly take place in the membranes surrounding the spinal cord and are often benign, however, they can be cancerous. These tumors are more frequent in middle-aged and elderly women. � Nerve sheath tumors (schwannomas and neurofibromas): These type of tumors originate in the nerve roots which exit from the spinal cord. This type of tumor grows slowly and is benign. It can take years before any health issues occur. �
Intramedullary Tumors
Intramedullary tumors develop from within the spinal cord or within the nerves and frequently occur in the cells that promote physical support and insulating material for the nervous system or glial cells. These type of spinal tumors occur most commonly in the neck or cervical spine. Although these spinal tumors are considered to be benign, surgery to remove intramedullary tumors may be challenging. The two varieties of intramedullary tumors are ependymomas and astrocytomas. �
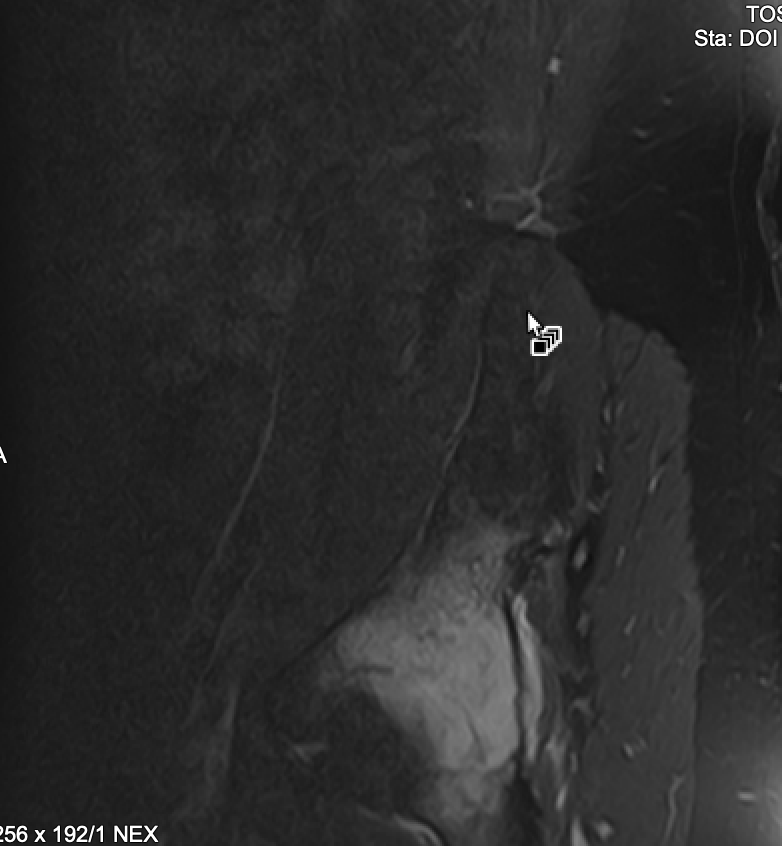
Pelvic tumor demonstrated in the hip of the patient.
� � � � �
Spinal Tumor Treatments
If any tumor is located in the spine and if there’s no other known cancer, a healthcare professional may perform a comprehensive evaluation of all common organs in which cancer can develop. A comprehensive evaluation may include: �
Complete medical history
Complete physical evaluation
Complete neurological evaluation
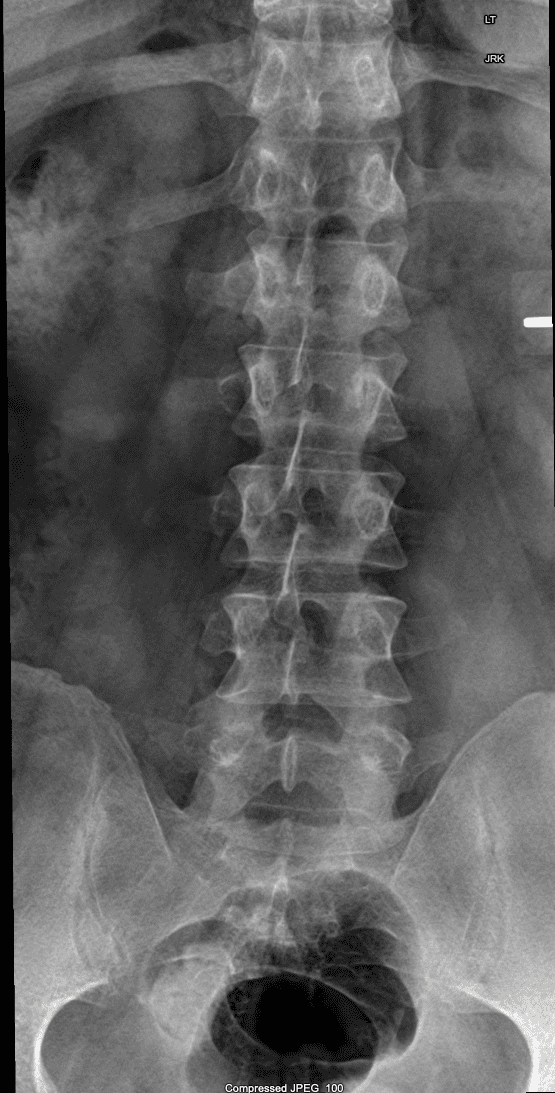
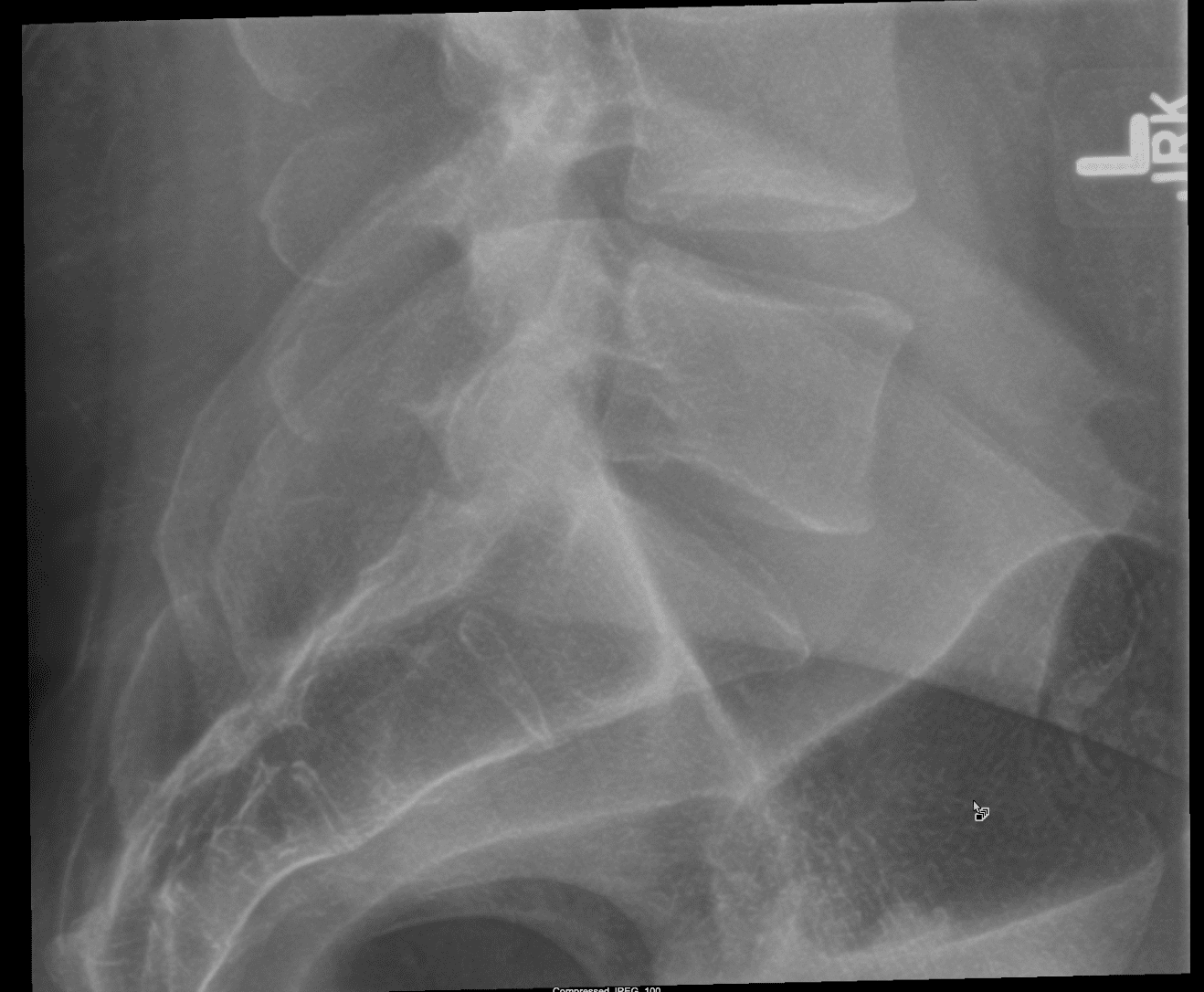
Radiographic study of the spine, chest, and GI tract
MRI and CAT scan to evaluate the spine
Vertebral Column Tumor Treatment
Because many vertebral column tumors originate from cancer in another organ, the goal of spinal tumor treatment is to:
Regulate severe painful symptoms which occur with these spinal tumors by removing pressure on the nerve roots
Maintain neurological structure and function by removing pressure on the spinal cord
Correct structural and functional instability in the spine by correcting the unstable spine with a spinal fusion
Intradural-Extramedullary and Intramedullary Tumor Treatment
These type of spinal tumors are generally surgically removed. The goal of spinal tumor treatment is to: �
Completely remove the spinal tumor
Preserve neurological structure and function
The spinal cord and nerves are extremely sensitive and preventing damage to their structure and function is an essential portion of surgical intervention. Monitoring methods and techniques can be utilized throughout the surgery to make sure the structure and function of the spinal cord are preserved since the spinal tumors are ultimately being removed. � If the spinal tumor cannot be fully removed, by way of instance, if it adheres to many nerve roots, post-surgical radiation treatment can help improve outcome. If the spinal tumor is metastatic, chemotherapy may also be helpful. After the surgery, it could take some time for the nerves to fully recover. Rehabilitation can help enhance a patient’s neurological performance. �
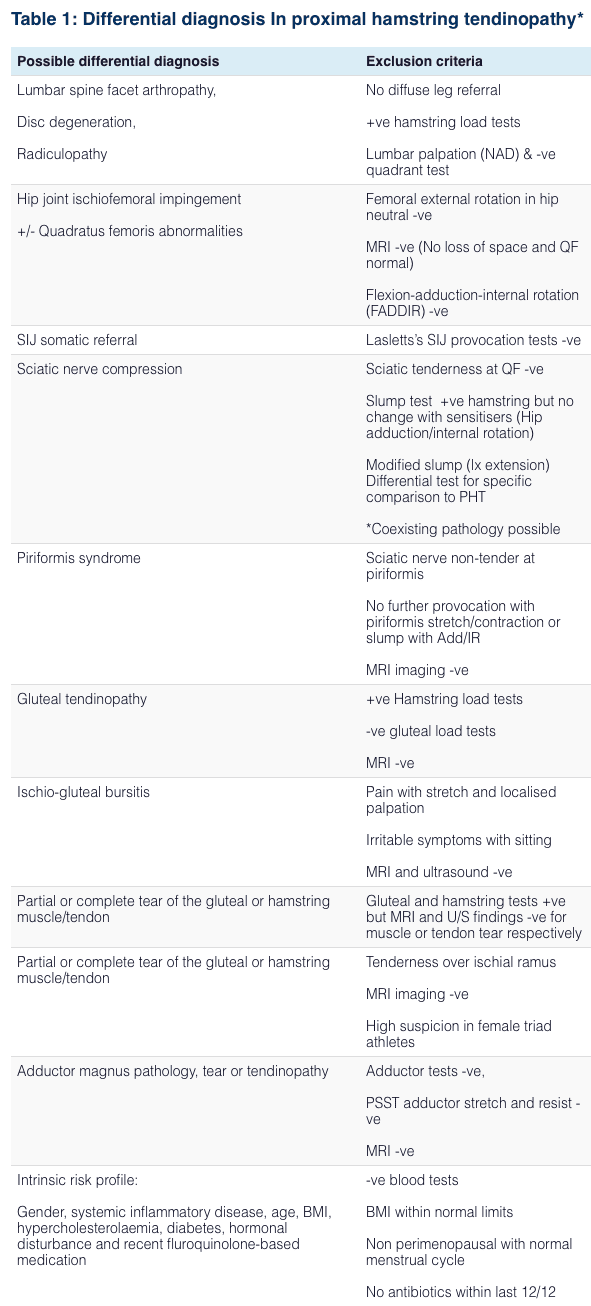
Differential Diagnosis of Hip Pain and Discomfort
�
Spinal tumors can cause back pain and sciatica. Although most cases of back pain and sciatic nerve pain are not caused by a spinal tumor, it’s essential to receive an accurate diagnosis to determine the source of the painful symptoms. As mentioned above, common symptoms of spinal tumors include pain and discomfort as well as numbness. Spinal tumors are health issues which should be evaluated immediately by a healthcare professional to follow-up with proper treatment. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
Fibromyalgia Magazine
The purpose of the article was to discuss spinal tumors and sciatica. Spinal tumors may often present symptoms of sciatica. Accurate diagnosis and proper treatment are important for this health issue. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Severe Sciatica
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. Your spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of sciatica, or sciatic nerve pain. Sports injuries or automobile accident injuries are often the most frequent cause of painful symptoms, however, sometimes the simplest of movements can have these results. Fortunately, alternative treatment options, such as chiropractic care, can help ease sciatic nerve pain, or sciatica, through the utilization of spinal adjustments and manual manipulations, ultimately improving pain relief. �
�
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force. �
If you are an active amateur or a competitive runner, using the services of a chiropractor can make a vast change in your overall health, reduce your pain from injuries and improve your alignment for a more effective run.
Chiropractors are excellent when it comes to rehabilitation, and they can help you keep your body in top condition as an athlete. All sports is an area that chiropractors can specialize in, focusing their training and experience on targeted treatments for runners.
Contents
Recovering from Sports Injury/s
Most athletes get injured at one point or another in their career, whether it is while participating in their sport or an accident in their daily lives. Recovery from an injury can be difficult at times, and even after hours of physical therapy, you may feel that you aren’t ready to start training again.
Physical therapy is a great help in recovering strength in soft tissue and muscle after an injury or surgery. However, sports-medicine trained chiropractors can improve the mobility of your joints after an injury. Sports chiropractors work with the soft tissue in conjunction with the joints in a coordinated fashion. An examination will take a look at:
After the examination, the sports chiropractor will assess the runner to recommend treatment.
People running fast in a city marathon on street
Sports Chiropractic
According to U.S. News and World Report, there are four primary chiropractic treatments for running injuries.
Active Release Technique (ART) – combines massage and stretching by applying deep tension while moving a joint through its range of motion. This treatment is used primarily for adhesions in the muscle.
Graston Technique – used to break down surface-level scar tissue with hand-held stainless steel tools.
Functional Dry Needling – releases tension in trigger points through deep muscle stimulation with needles. This treatment can help the psoas muscle, a hip flexor muscle.
Electrical Muscle Stimulation (EMS) – releases tension through the stimulation of surface muscles.
General Adjustments
Chiropractors are trained to look at the whole body and align it for optimum balance. Many runners find it beneficial to have regular periodic adjustments to regain their body’s balance from daily stress and the impact of running. Aligning the body can relieve tension or pain that is caused by misalignment before it becomes more than a minor impediment.
Runners may not even realize that the tension they feel is the beginning of pain caused by being out of balance until it is adjusted. Chiropractic adjustments are often part and parcel of a runner’s training program to strengthen and improve performance. They can also help recover from pregnancy and postpartum bodily changes.
Prevents Injury and Promotes Optimal Performance
With regular care of a sports-trained chiropractor, runners can actually prevent injury and promote optimal performance by keeping their bodies fine-tuned, working at maximum capacity. A trained chiropractor can find imbalances that may lead to injury and correct them before they become a problem. With your body in perfect balance, muscles and joints work more efficiently, powering up your performance as a runner and making the most of your body’s resources.
Misalignment can be caused by many common runners� experiences including running on the same type of surface every day, running on a slanted surface such as a beach or replacing running shoes too infrequently. As a runner, you can work to vary your running surfaces and keep a better watch on your shoes, but your chiropractor will let you know if your body is in need of more balance.
To learn more or to schedule an appointment, please give us a call at the number provided at the top of this website. We’re here to help!
Red Flags of foot *PRONATION* | El Paso, Tx
Feet: A foundation for pain
99% of feet are normal at birth. But after the first year, 8% develop foot problems, 41% by age 5 and 80% by age 20. By age 40, almost everyone has a foot condition of some sort. Many foot conditions eventually contribute to health concerns, especially the generalized condition of �back pain� or runner�s knee. Spotting a potential problem originating in the feet can prevent other injuries from affecting your health and lifestyle.
Runners who are able to avoid injury are those who land the lightest on their feet, which sustains the lowest levels of impact. Researchers suggest that runners think about landing more softly and adjust their stride so that they land closer to the midfoot.
But that is easier said than done, as most runners tend to be heel-strikers.
Runners with excessive pronation that try to transition to a forefoot strike pattern could be more susceptible to inner foot and ankle injuries.Runners with high arches who attempt to transition to a forefoot strike pattern are prone to suffer sprained ankles and metatarsal stress fractures.
Running can lead to a number of different injuries
Sudden trauma
Developed over time from microtrauma
Biomechanical errors
Structural asymmetries
Tissue weaknesses
Excessive external loads
Runners do their best to treat pain through stretching or exercises that target the area that hurts, but sometimes the source of the pain might actually be elsewhere. That source is foot imbalance.
Custom orthotics improve biomechanics
Custom orthotics are used to align and support the foot/ankle complex in a more near-normal physiologic position for a weight-bearing foot to prevent dysfunction and/or improve the function of movable body parts.[3] They are indicated to:
Creates a symmetrical foundation by blocking pronation or support supination
Provides heel strike shock absorption
Inhibits serial biomechanical stress
Enhances neuromuscular re-education
Custom-made orthotics that use viscoelastic materials can help to reduce the musculoskeletal impact from heel strikes when running.
This shock absorption can be of help particularly when there is instability, chronic degeneration, or inflammatory arthritis in the joints.
Orthotics are designed specifically to cushion foot impact and reduce pain triggers.
Everyone is misaligned
Patellofemoral pain care
Understanding the exact mechanical contributions of the knee is critical for the therapist to effectively manage injuries or conditions.
NCBI Resources
These injuries and conditions affect runners, cross fitters, group exercise enthusiasts (PUMP classes) and simple recreational walkers who spend a lot of time on hills and stairs.
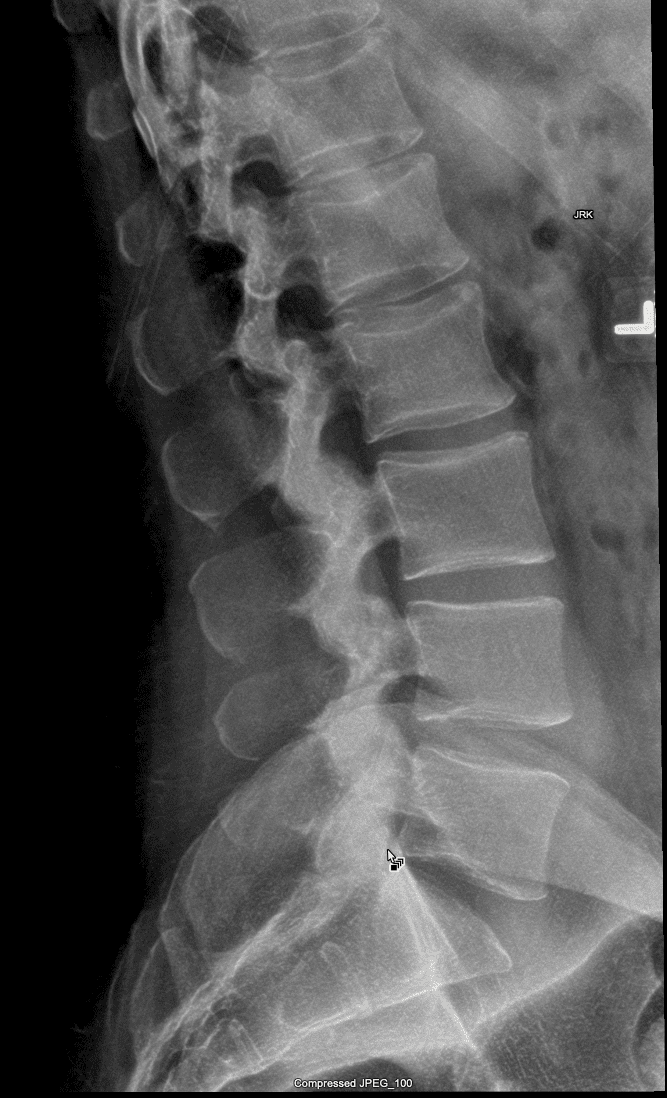
Sacroiliac joint dysfunction is characterized as a sharp, stabbing pain which radiates from the pelvis and hips, down into the lower back or lumbar spine and throughout the legs. Patients might experience tingling sensations or numbness. The sacroiliac joint is generally attributed to causing between 15 to 30 percent of chronic low back pain cases. Approximately 80 percent of adults will experience some type of low back pain throughout their lifetimes. Low back pain is also ultimately considered to be one of the most general causes of disability as well as the most common cause of missed workdays. �
Contents
What are the Sacroiliac Joints?
The sacroiliac joints are situated where the sacrum and ilium come together. The sacrum is the triangle-shaped bone close to the base of the spine, just over the coccyx or the tailbone. Among the three bones that make up the hip structure, the ilium is at the top of the pelvis. The sacroiliac joints support the weight of the human body, maintaining it around the pelvis. This reduces pressure and functions as a shock absorber. The bones of the sacroiliac joints are all jagged to remain in alignment. �
Gaps between the bones of the sacroiliac joints are filled with fluid for lubrication. These gaps are also filled with free nerve endings which are in charge of transmitting pain signals. It may be debilitating when the sacroiliac joints come out of alignment. All the bones at the sacroiliac joints are connected by muscles and ligaments which promote stability and permit for limited motion. This motion is essential for women to give birth and for people to stay standing vertically. �
What Causes Sacroiliac Joint Dysfunction?
Irritation, swelling, or inflammation of one or more sacroiliac joints is commonly referred to as sacroiliac joint dysfunction, sacroiliac joint disease, or sacroiliitis. Moreover, sacroiliac joint dysfunction or disease may cause sacroiliitis. This can be a health issue which encompasses a variety of other injuries and/or underlying conditions. These include: �
Walking patterns
Injury
Gout
Ankylosing spondylitis
Osteoarthritis
Pregnancy
What are the Symptoms of SI Joint Dysfunction?
Every person experiences symptoms of SI joint dysfunction differently and the signs can vary from person to person, depending on the source of the sacroiliac joint dysfunction. Common signs and symptoms of SI joint dysfunction include: �
low back pain
pain in the buttocks, hips, and pelvis
pain in the groin
painful symptoms in the SI joints
pain when standing from a sitting position
stiffness
burning sensations
weakness
numbness
pain radiating down into the thighs and legs
feeling like the legs may buckle and not support the weight of the body
How is Sacroiliac Joint Dysfunction Diagnosed?
SI joint dysfunction can be hard to diagnose. Because the joints are situated deep within the human body, it often makes it difficult for healthcare professionals to properly diagnose the health issue. Moreover, damage due to trauma or injury to the sacroiliac joints doesn’t appear on imaging tests like CT scans, MRIs, or X-rays. And the signs and symptoms are much like other health issues, such as sciatica, bulging or herniated discs and arthritis of the hip. The healthcare professional may perform a variety of tests so as to diagnose SI joint dysfunction and determine other health issues, including: �
Provocative tests are frequently utilized by healthcare professionals to determine whether the painful symptoms are originating from the SI joint. The maneuvers are utilized to isolate the SI joint as the source of pain.
Injecting a numbing drug and/or medication, such as lidocaine, to the sacroiliac joint. This can ultimately help determine if the patient has an SI joint health issue if the painful symptoms are reduced after a brief period of time.
Imaging tests, including X-rays, MRIs, and CT scans.
Diagnosing SI Joint Disorders – Provocative Testing
How is Sacroiliac Joint Dysfunction Treated?
Physical therapy, chiropractic care, stretches and exercises, such as yoga, and massage can help stabilize and strengthen the SI joints and alleviate painful symptoms. Another treatment suggestion involves the utilization of cold packs for pain relief. Utilize heat with a heating pad or heat wrapping, or a soak in a warm bath after the painful symptoms are more manageable. It is also possible to put on a sacroiliac belt to help support the sacroiliac joint which might help alleviate painful symptoms. �
Medicine and Non-surgical Treatment
If sacroiliac joint dysfunction signs and symptoms can’t be managed with physical therapy, chiropractic care, stretches and exercises, and/or massage, or whether it is brought on by an underlying health issue, your healthcare professional may recommend the utilization of medicine and non-surgical treatment. These treatment approaches can include: �
anti-inflammatory medications, including nonsteroidal, anti-inflammatory drugs (NSAIDs)
muscle relaxants
oral steroids, but only for short-term utilization
tumor necrosis factor inhibitors (TNF inhibitors)
corticosteroid injections
radiofrequency ablation, which utilizes energy to deactivate the nerves which are causing pain and discomfort
Healthcare professionals consider surgery to be the last resort for sacroiliac joint dysfunction if none of the other treatment approaches mentioned above helped reduce painful symptoms. With sacroiliac joint surgery, small plates and screws are utilized to hold the SI joint together so the bones fuse or grow together. The healthcare professional may suggest this surgery if the pain and discomfort become constant and other treatment approaches haven’t been effective. Furthermore, it’s fundamental for patients to receive a diagnosis for them to follow-up with treatment for their SI joint dysfunction. �
Differential Diagnosis of Hip Pain and Discomfort
� �
Sacroiliac, or SI, joint dysfunction is believed to be a common cause of low back pain and hip/thigh/leg pain. Because of the painful symptoms along the lower extremities, SI joint dysfunction may feel similar to sciatica. However, sciatica is caused by the compression or impingement of the sciatic nerve. Accurately diagnosing sacroiliac joint dysfunction can be difficult. A positive diagnosis for SI joint dysfunction is generally determined through the utilization of provocative testing and/or an injection. Proper diagnosis is important for proper treatment. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
Fibromyalgia Magazine
The purpose of the article was to discuss SI joint dysfunction and sciatica. SI joint dysfunction is often confused with the symptoms of sciatica, however, diagnosis and treatment differ for this health issue. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez
Additional Topic Discussion: Severe Sciatica
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. Your spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of sciatica, or sciatic nerve pain. Sports injuries or automobile accident injuries are often the most frequent cause of painful symptoms, however, sometimes the simplest of movements can have these results. Fortunately, alternative treatment options, such as chiropractic care, can help ease sciatic nerve pain, or sciatica, through the utilization of spinal adjustments and manual manipulations, ultimately improving pain relief. �
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force. �
Athletes participate in a variety of exercises and physical activities on a regular basis, however, this can increase the risk of injury. Proper sports injury therapy depends on the correct diagnosis in order for them to be able to return-to-play quickly. Dr. Alexander Jimenez, a chiropractor, helps many athletes recover to optimal performance through the use of chiropractic treatment.
Chiropractic utilizes adjustments and manual manipulations to restore the integrity of the spine. And this is to decrease injury symptoms and promote healing. Patients describe how Dr. Jimenez and his team helped them recover their life, health, and wellness. These patients highly recommend Dr. Jimenez as yoursports injury chiropractor.
Contents
El Paso Back Clinic
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
Our services are specialized and focused on injuries and the complete recovery process.�Our areas of practice include�Wellness & Nutrition, Chronic Pain,�Personal Injury,�Auto Accident Care, Work Injuries, Back Injury, Low�Back Pain, Neck Pain,�Migraine�Treatment, Sports Injuries,�Severe Sciatica, Scoliosis, Complex Herniated Discs,�Fibromyalgia, Chronic Pain, Stress Management, and Complex Injuries.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused on treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
We want you to live a life filled with more energy, positive attitude, better sleep, less pain, proper body weight and educated on how to maintain this way of life.
We Are Ready To Help Get You Back To Optimal Performance!
The Foot Levelers Kiosk
The Kiosk helps guide patients in selecting the best custom-made orthotics for their condition and lifestyle. It’s�
Fast: Push the Start button and the scanner begins.
Easy to use: User-friendly easy touch screen.
Engaging: Videos explain the importance of healthy feet and the benefits of custom-made orthotics.
Cloud-based: Results can be securely accessed from anywhere.
Comprehensive: Easily retrieve previous scans to compare them to new scans and see the difference.
The Foot Levelers Kiosk helps you. It saves time so you can spend more time living your life.
Workouts & Working
Our uplifting southwest community surrounded by it infinite beauty is a fantastic place to live and enjoy our families; it is, therefore, our mission to help each of our patients to�live,�to�love,�to�matter�and�to�thrive�pain-free�in this beautiful special place.
When your body is truly healthy, you will arrive at your optimal fitness level proper physiological fitness state. �We want to help you live a new and improved lifestyle. Over the last two decades, while researching and testing methods with thousands of patients, we have learned what works effectively at decreasing pain while increasing human vitality.
The facet joints are the joints which are found behind the spine to counterbalance the intervertebral discs found between the vertebrae of the spine. These are ultimately essential for restricting the movements of the spine for the vertebrae to maintain proper alignment. Over time, the natural aging process can cause the facet joints to deteriorate or wear down. Facet joint arthritis can also gradually develop over time, as it may in any other joint. This is referred to as arthropathy. �
What are the Symptoms of Facet Arthropathy?
Individuals with facet arthropathy will generally experience low back pain which can often worsen with standing, twisting, or bending backward. The painful symptoms associated with facet joint arthropathy occur in one specific region of the spine. The pain and discomfort are commonly described as a dull ache on one or both sides of the lower back or lumbar spine.� �However, unlike the well-known signs and symptoms of sciatica, caused by the compression or impingement of the sciatic nerve in the lower back, facet arthropathy signs and symptoms generally don’t radiate down the buttocks or into the legs. �
However, the facet joint, in the same way as any other joint which has arthritis, can become enlarged and add pressure on nerve roots, causing pain and discomfort to radiate down the lower extremities. Facet arthropathy symptoms are generally relieved by bending forward. Bending your body forward into a spinal flexion position can help reduce painful symptoms. �
What Causes Facet Arthropathy?
The natural aging process is frequently considered to be one of the most common indirect sources of facet arthropathy. Other health issues which can affect the facet joints and ultimately cause facet arthropathy include: �
Osteoarthritis: Degeneration of joint cartilage and underlying bone, generally during middle age
Facet joint degeneration: Wear and tear on the facet joint brought on over time due to aging
Facet joint injury: Trauma to the facet joints caused by an impact, such as a fall or automobile accident
Synovial cyst: A fluid-filled sac which develops in the spine, generally as a result of aging
How is Facet Arthropathy Diagnosed?
If you’re experiencing chronic low back pain, make an appointment with a healthcare professional to determine a diagnosis and follow-up with the proper treatment. By performing a physical evaluation, your healthcare professional will then be able to analyze the source of your painful symptoms. The doctor will also ask you questions regarding your medical history and your symptoms as well as order several of the following tests to help diagnose facet arthropathy, including: �
CT scan or MRI scan: These imaging tests can show evidence of facet joint degeneration, even mild to moderate cases.
Bone scan: This test shows bone density to demonstrate any source of inflammation on the spine.
Anti-inflammatory steroid injection: An injection into your facet joint can determine facet arthropathy.
X-rays: These will help the healthcare professional evaluate the overall health and wellness of your spine.
Can Facet Arthropathy Cause Other Health Issues?
Facet arthropathy may cause bone spurs, tiny bone outgrowths. Bone spurs can decrease the distance available between nerve roots, causing a health issue known as spinal stenosis. Spinal stenosis may cause pain, weakness, and numbness on the buttocks, hips, and thighs. It’s frequently associated with other health issues which could lead to facet arthropathy. �
Arthritis caused by a variety of other health issues, such as degenerative disc disease, can occur due to the human body’s natural aging process, causing the discs between the vertebrae of the spine to lose their flexibility, elasticity, and capacity to absorb shock from walking and other physical activities. This may ultimately cause painful symptoms to develop. �
How is Facet Arthropathy Treated?
There are numerous treatment approaches to help treat facet arthropathy symptoms. Treatments include: �
Anti-inflammatory drugs and/or medications
Avoidance of movements which cause pain and discomfort, such as repetitive twisting or lifting
Physical therapy
Chiropractic care
Epidural steroid injections
Facet joint ablation or the destruction of the facet nerves with electrical shocks
Spinal surgery when there is nerve-root compression
Differential Diagnosis of Hip Pain and Discomfort
� �
Facet joint arthropathy is a well-known health issue which can commonly occur due to the human body’s natural aging process, however, injury or underlying conditions may also cause facet joint arthropathy. Although facet joint arthropathy may cause pain, discomfort, and numbness in the lower back, the symptoms are different from sciatica in which these don’t radiate down the buttocks, legs, and/or feet. Diagnosis is essential for facet joint arthropathy to follow-up with treatment. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
Fibromyalgia Magazine
The purpose of the article was to discuss degenerative disc disease and sciatica. Degenerative disc disease is often associated with pain, tingling sensations, and numbness, similar to the symptoms of sciatica. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Severe Sciatica
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. Your spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of sciatica, or sciatic nerve pain. Sports injuries or automobile accident injuries are often the most frequent cause of painful symptoms, however, sometimes the simplest of movements can have these results. Fortunately, alternative treatment options, such as chiropractic care, can help ease sciatic nerve pain, or sciatica, through the utilization of spinal adjustments and manual manipulations, ultimately improving pain relief. �
�
�
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force. �
Rheumatoid arthritis (RA) is a condition that causes considerable discomfort if diagnosed with this autoimmune disease. This is when your immune system starts attacking your joints, instead of foreign invaders, which then causes inflammation.
The worse the RA, the more severe the symptoms become. If things get bad enough you can lose mobility altogether, which is why it is so important to get treatment. Fortunately, chiropractic is excellent for reducing inflammation and improving mobility. Chiropractic treatment can do a lot to ease your pain and get you back to moving the way you are supposed to.
Contents
RA and Chiropractic
Chiropractic is an effective RA treatment for a number of reasons. Chiropractic treatment:
Individual Treatment
The image many people have of a chiropractic adjustment is one of popping backs and hard, jerking motions. While adjustments can certainly include these things, they do not have to. According to the Arthritis Foundation, chiropractors have more than 150 techniques they can use to adjust your body.
They strive to give treatments specific to the needs of each patient, which means adjusting the body as gently as necessary to produce the desired result. If your joints are swollen and painful the chiropractor will carefully work to realign the joint�which reduces inflammation and improves movement�while minimizing any pain or discomfort you feel from the adjustment.
Reduced Inflammation
With RA typically the worst symptoms are the result of inflammation. Chiropractic treatment may not be able to change the way your immune system is malfunctioning, but it can do a lot to help the painful areas become less inflamed.
The treatment you get from your chiropractor will ensure that your joints are moving as properly as possible given your condition. By putting the body back in alignment, chiropractic improves the way the nervous system operates and lessens inflammation.
Improved Mobility
One of the most difficult things for many with RA is the loss of mobility that comes when their joints swell. When the pain becomes more substantial it is normal for RA sufferers to avoid movement because it hurts.
But it is important to remember that movement, even when it hurts, is necessary to maintain joint mobility. The longer you avoid moving a joint the more likely it is that you will lose function.
A useful aspect of chiropractic is that you can get help with moving, so you are not all alone with the daunting prospect of moving your joints so they start working better. Your chiropractor is your partner in movement, helping to guide your body so that it moves as well as possible. Results are different for everyone based on their unique situations, but you can be sure that chiropractic will serve as a powerful tool to keep your body working as well as possible.
Hand Deformed From Rheumatoid Arthritis
Drug-Free and Non-invasive
In chiropractic, the focus is to help the body heal itself, which means avoiding surgery and prescription medications as much as possible. Surgery and medication often have unwanted side-effects�sometimes worse than the problem they were intended to solve. With chiropractic negative side-effects are unlikely. You can get a lot of relief from gentle, effective treatments that will not make you feel worse than when you started.
Your Chiropractic Source
Our chiropractic team has experience helping patients with RA, and we are interested in doing the same for you. We understand how hard it can be to have RA. Let us help you get the relief you deserve.
Please contact our office to schedule an appointment. We look forward to speaking with you!
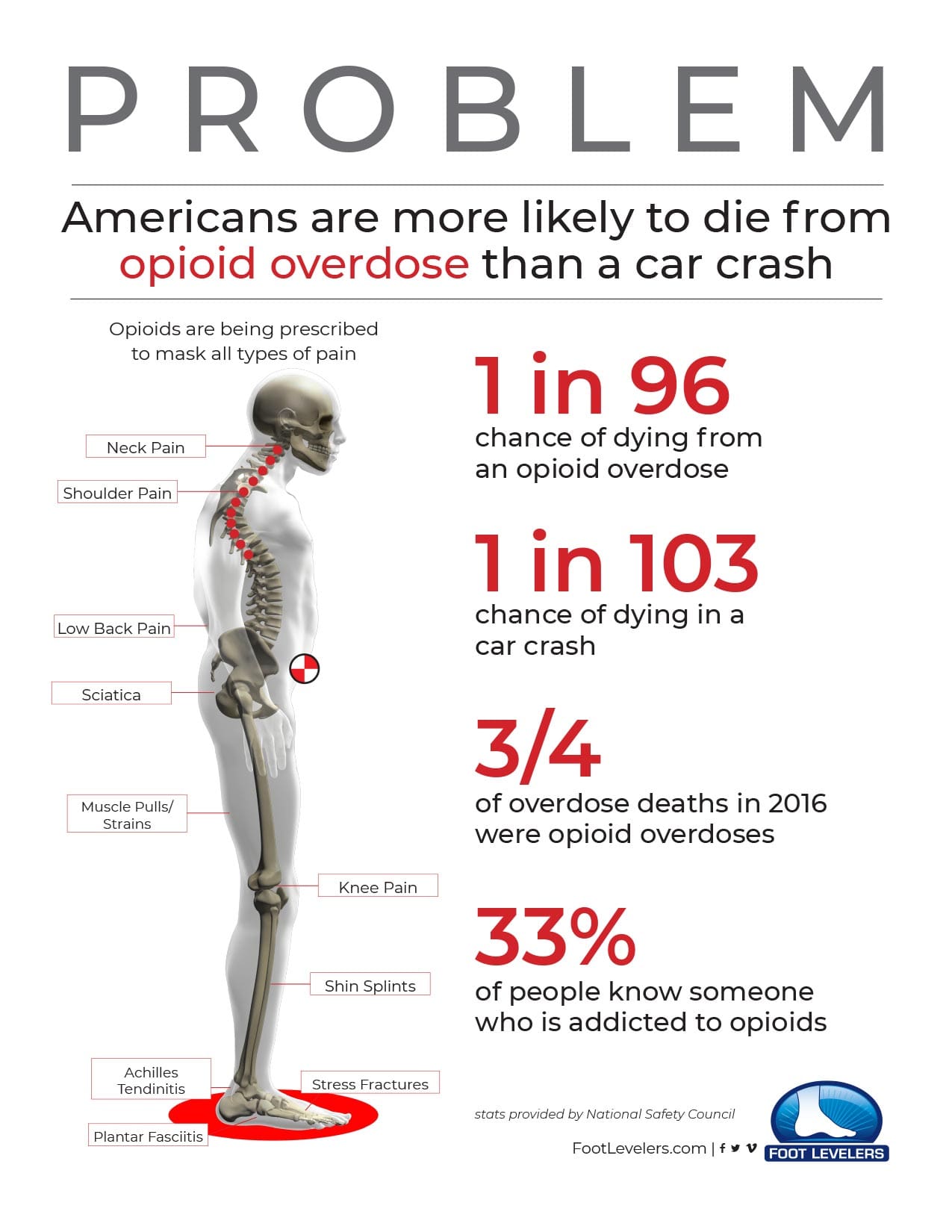
Opioid Addiction Alternative
Opioids (such as hydrocodone, oxycodone, codeine, and morphine) mask symptoms and do nothing to address the cause of pain.
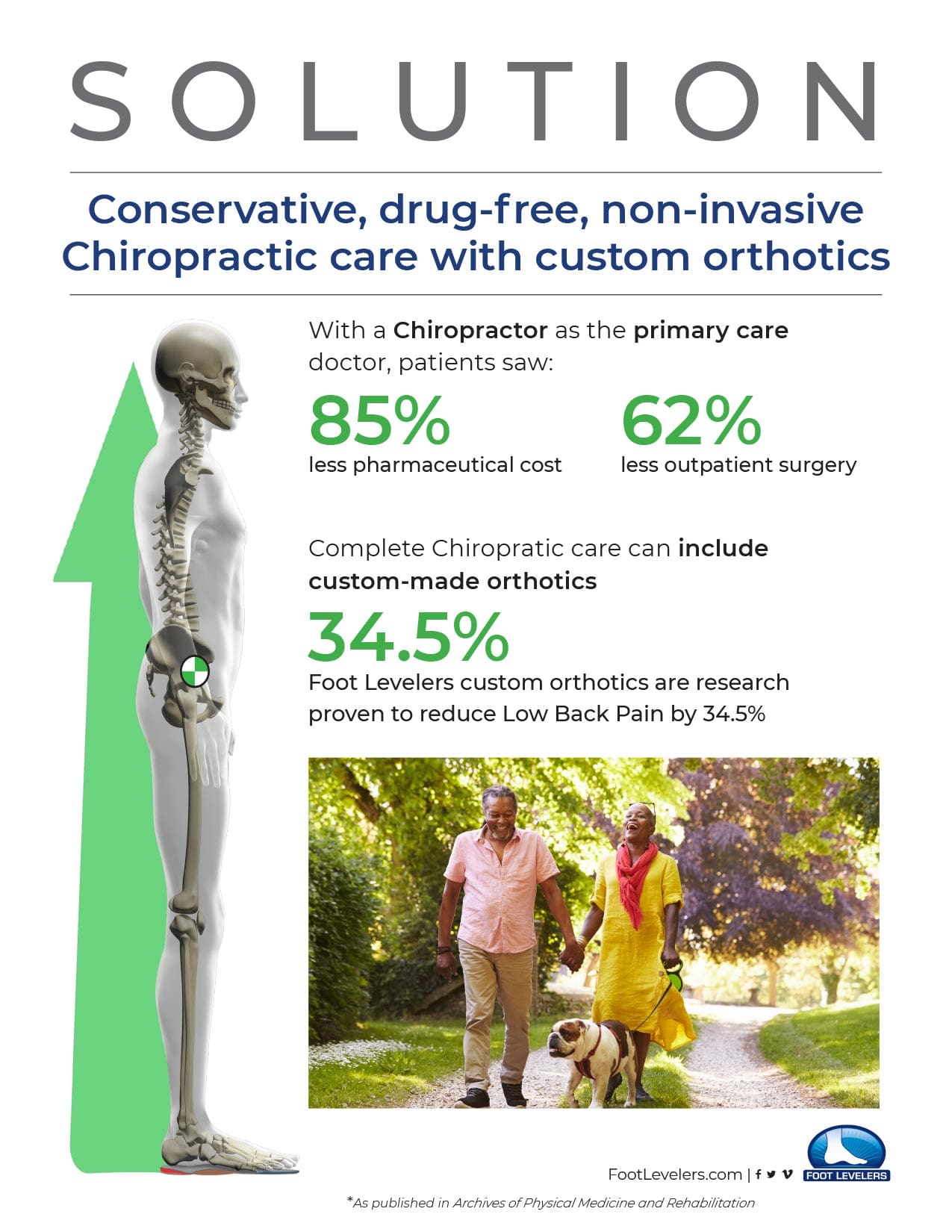
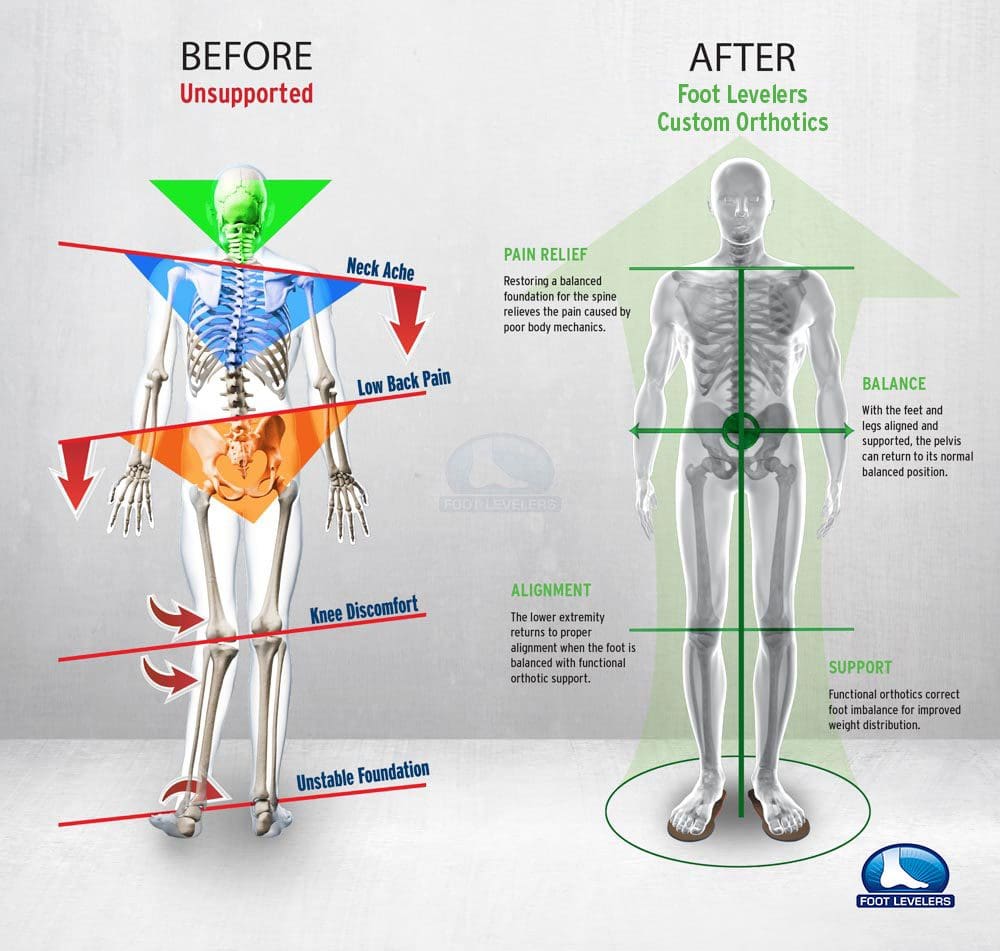
There is an opioid crisis raging.� A sensible and safe alternative to opioids: Custom-made orthotics help relieve low back pain as well as hip and neck pain by removing imbalances in the musculoskeletal system, which originate in the feet.
Before considering taking an opioid for pain control, give Chiropractic care and foot orthotics a try. The combination of Chiropractic and orthotics is proven in clinical studies.
In 2015, about 2 million Americans had substance abuse disorders related to opioid medications.
In 2012, 80 out of 100 Americans were prescribed opioids. That’s about 259 million prescriptions � more than enough to give every American adult their own bottle of pills.
Less Pain & More Comfort
Custom orthotics help more than your feet! Stabilizing orthotics bring health and healing to the whole body by balancing the musculoskeletal system.
El Paso Back Clinic
Here are some videos that discuss how chiropractic care can help with arthritis, fibromyalgia, seniors and whole body wellness.
NCBI Resources
Here are some articles to check out for extended information on arthropathies.
You need to understand your feet! Flat feet, foot pronation, and foot imbalances can lead to all kinds of pain:
Knee pain
Hip pain
Back pain
Yes even Shoulder pain
If you are considering custom orthotics, a health care professional such as Doctor Jimenez and Injury Medical Chiropractic Clinic can perform a foot scan to show you what imbalances in the feet can lead to. The foot scan will show how the orthotics can help. Following the foot scan, a report will provide the caregiver a Pronation/Stability Index, Foot Assessment, and Body Assessment.
Contents
Pronation & Stability
The Pronation/Stability Index� score appears on the clinical report that is produced when your feet are scanned by our 3D machine.
The Pronation/Stability Index� is an algorithm based on 16 different measurements. Taken from a laser scan of the feet, the index indicates the amount of arch collapse. The higher the number, the more collapse.
The index reveals the severity of pronation/stability of your feet, which can be anywhere from optimal to severe. An index of 102, for example, is a moderate pronation/instability. Untreated imbalances at any level can lead to chronic problems.
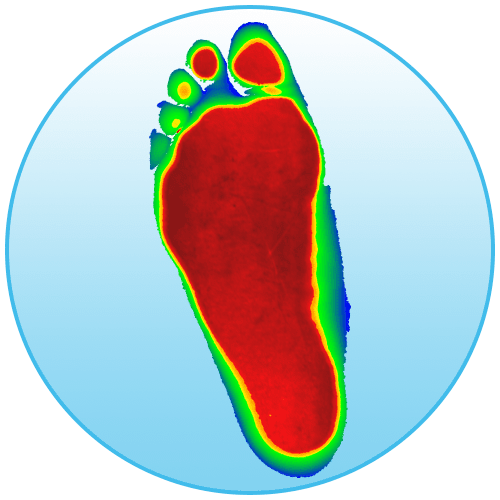
Optimal Feet
This image shows what the optimal foot looks like.
The red areas represent where pressure on your foot should be:
The toes
The balls of the foot
The heel
Unfortunately, 99% of feet do not look like this.
Flat Feet
This image shows what flat feet look like. Here, all three arches of the foot have collapsed. Once the arches collapse it throws the rest of the body off. So when you move there is a higher risk for pain. This includes pain in the feet, knees, hips, back, and neck.
The Body
The body image shows imbalances in the feet and how they can lead to knee rotation, pelvic tilt and shoulder drop.
Throughout our lives, we need some type of support for our feet. After all, they take all of our weight, so let’s treat them right and understand your feet.
El Paso Back Clinic
NCBI Resources
Effective footwear can make a huge difference. Especially when it comes to being able to stand and walk in a comfortable manner.
Degenerative disc disease is a health issue which occurs when one or more of the discs found between the vertebrae of the spine break down, causing painful symptoms and other problems. Common symptoms may include pain, tingling sensations, weakness, and numbness. Despite its name, degenerative disc disease is actually not a disease, but rather, a natural process which occurs with aging. The rubbery discs found between the vertebrae function like shock absorbers, allowing the back to flex and bend accordingly.� When they wear out, however, they no longer provide as much protection as before. �
Contents
Causes
The intervertebral discs also referred to as spinal discs or intervertebral fibrocartilage, provide the padding required between the vertebrae of the spine. The intervertebral discs are an elastic structure made from fibrocartilage tissue. The outer part of the disc is referred to as the annulus fibrosus. The annulus fibrosus is tough and it’s made up of many overlapping layers. The inner part of the disc is referred to as the nucleus pulposus. The nucleus pulposus is soft and gelatinous. The intervertebral discs cushion the stress of the spine, bears weight, and also helps the spine bend and flex. �
As people age, repeated daily stresses on the backbone and occasional trauma and/or injuries, including minor, undetected health issues, may ultimately damage the intervertebral discs in the back. Changes caused by damage may include: �
Decreased fluid: The intervertebral disks of a healthy young adult are made up of around 90 percent fluid. With age, the fluid material decreases, causing the disc to become thinner. The distance between each vertebra, in turn, becomes smaller and it makes them even less effective to function as a cushion or shock-absorber.
Disc structure: Small tears or cracks can become larger in the outer layer of the disc. The soft and gelatinous material from the inner part may push through the disc, causing a bulging or ruptured disc. The disc may break into fragments.
If the vertebrae have less padding between them, the backbone also becomes less stable. To compensate, the human body builds osteophytes, or bone spurs, small bony structures which develop along the edge of bones. These structures can compress or impinge the spinal cord or nerve roots. Other health issues caused by degenerative disc disease includes the breakdown of cartilage or the tissue which cushions the joints, a bulging disc, known as a herniated disc, and a narrowing of the spinal cord, also referred to as spinal stenosis. These changes can cause painful symptoms and lead to fatigue. �
Symptoms
Degenerative disc disease can either cause no symptoms or the pain and discomfort may be so severe, it can tremendously affect an individual’s quality of life. This health issue generally aggravates due to injury or trauma to the backbone, however, symptoms can also affect other parts of the human body, depending on the direct location of the degenerative disc disease. The pain and discomfort can range from mild to severe and it may often be debilitating. It may ultimately result in osteoarthritis, with pain and discomfort along with stiffness in the back. Fatigue can generally accompany other symptoms. �
If degenerative disc disease affects the low back or the lumbar spine, the pain and discomfort may radiate down the buttocks, hips, and thighs, into the knees and feet. There might also be tingling sensations and numbness, a collection of symptoms known as sciatica, caused due to the compression or impingement of the sciatic nerve. If degenerative disc disease affects the neck or the cervical spine, the pain and discomfort may radiate into the shoulders, arms, and hands. The painful symptoms may worsen when sitting, bending, twisting or lifting. Rest may help provide some pain relief. �
Diagnosis
A healthcare professional will ask the patient about their symptoms, including where and when the pain developed as well as whether there are tingling sensations or numbness. The doctor may also need to know which circumstances cause the most painful symptoms and if the patient suffered any injuries and/or aggravated conditions. A physical evaluation may examine pain and discomfort in response to touch or movement, muscle strength, flexibility, and performance, as well as nerve structure and function. The healthcare professional may also order diagnostic tests, such as MRI or CT scans. �
Treatment
Treatment for degenerative disc disease might include occupational therapy, physical therapy, chiropractic care, exercise or physical activity, drugs and/or medications, weight loss, and surgery. Medical options include injecting the joints next to the broken disc with steroids and a local anesthetic. Medicines include pain relief medicine, such as Tylenol, and non-steroidal anti-inflammatory medications, or NSAIDs, including ibuprofen. Muscle relaxers and steroids may also be prescribed. �
A corset or brace may also offer back support. Patients who don’t respond well to conservative treatment options might require surgery. Furthermore, a patient who develops osteoarthritis, a herniated disc, or spinal stenosis may require a combination of different types of treatment approaches to achieve pain relief. It’s fundamental for a healthcare professional to provide a patient with the proper diagnosis of their symptoms to follow-up with the most appropriate treatment. �
Differential Diagnosis of Hip Pain and Discomfort
�
Degenerative disc disease is characterized as the normal, gradual deterioration of the intervertebral discs with age, which may occasionally cause a variety of painful symptoms. Common symptoms associated with degenerative disc disease can include pain and discomfort, tingling sensations, and numbness, similar to sciatica. Painful symptoms may also cause fatigue and other health issues. Nearly everyone’s intervertebral discs will break down over time, however, not everyone will develop painful symptoms. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
Fibromyalgia Magazine
The purpose of the article was to discuss degenerative disc disease and sciatica. Degenerative disc disease is often associated with pain, tingling sensations, and numbness, similar to the symptoms of sciatica. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Severe Sciatica
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. Your spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of sciatica, or sciatic nerve pain. Sports injuries or automobile accident injuries are often the most frequent cause of painful symptoms, however, sometimes the simplest of movements can have these results. Fortunately, alternative treatment options, such as chiropractic care, can help ease sciatic nerve pain, or sciatica, through the utilization of spinal adjustments and manual manipulations, ultimately improving pain relief. �
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force. �
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine






 �
�  �
�  �
�  �
� 
 �
�









 In 2015, about 2 million Americans had substance abuse disorders related to opioid medications.
In 2015, about 2 million Americans had substance abuse disorders related to opioid medications.
 In 2012, 80 out of 100 Americans were prescribed opioids. That’s about 259 million prescriptions � more than enough to give every American adult their own bottle of pills.
In 2012, 80 out of 100 Americans were prescribed opioids. That’s about 259 million prescriptions � more than enough to give every American adult their own bottle of pills.