All fats, including saturated fatty acids, have very important roles in the body. The most important fats are the ones that the body can�t make and must be coming from the foods that a person eats. �Essential fatty acids are lipids that are involved in various biological processes and produce many compounds when they are metabolized in the body. The two primary EFAs (essential fatty acids) are linoleic acid (Omega-6) and alpha-linolenic acid (Omega-3). These two omegas are essential for the body since they are consumed from dietary sources because the body does not have the ability to synthesize them and EFAs are synthesized into prostaglandins, which are necessary for proper hormone signaling in the body.
Contents
Omega-6
Omega-6 fatty acids or linoleic acid are polyunsaturated fatty acids that are primarily used for energy and can be converted into longer omega-6 fats called ARA (arachidonic acid). ARA are used to produce eicosanoids, but they are prone to be more pro-inflammatory. Studies have shown that pro-inflammatory eicosanoids are important chemicals in the immune systems, however, when there are too many to produce, they can increase inflammation and inflammatory diseases in the body.
Researchers state that even though omega-6 fats are essential for a healthy body, the modern Western diet is making individuals consume more omega-6 fatty acids than the recommended amount. In a regular healthy diet, the ratio of omega-6 to omega-3s is 4:1 or less. In a Western diet however, the ratio is between 10:1 and 50:1.
Even though, an individual should consume the recommended amount of omega-6 fatty acids, research has shown that omega-6 fatty acids can lower the risk of cardiovascular diseases and treat symptoms that cause chronic diseases. In certain oils that contains omega-6 fatty acids, GLA (gamma-linolenic acid), which is an anti-inflammatory component and when consumed it converts to DGLA (dihomo-gamma-linolenic acids), which has anti-inflammatory and anti-proliferative properties against cancer.
A study has shown that when an individual takes a high dose of GLA in their diet, it can significantly reduce a number of symptoms caused by rheumatoid arthritis, and another study found that taking GLA supplements with a breast cancer drug is more effective in lowering breast cancer.
Omega-3
Just like omega-6 fatty acids, omega-3 fatty acids are polyunsaturated fats that play important roles in providing a number of health benefits for a functional body. Omega-3 fatty acids contain three important compounds that are found in foods, they are ALA (alpha-linolenic acid); which converts into energy for the body, DHA (docosahexaenoic acid); which is the key component for a functional brain and retina, and lastly, EPA (eicosapentaenoic acid); which has cardiovascular benefits including lowering serum triglyceride and non-HDL-C (non-high-density lipoprotein cholesterol) in the body.
When it comes to those three important components in omega-3s, ALA is mainly found in plants, while DHA and EPA are found in mostly animal products and algae. What makes these three components work well in the omega-3 supplements is that they are a crucial part of the human cell membrane and improve heart health, support mental health, decrease liver fats and fight inflammation.
With omega-3 fatty acids, lots of people don�t consume it as much as omega-6, due to not eating a lot of fatty fish as often and consuming omega-6 through fried food being cooked in refined vegetable oils. To balance a healthy diet, individuals can take an omega-3 supplement to balance out the omega-6 consumption to make sure the body is receiving these fatty health benefits.
Prostaglandins
Prostaglandins are a component of this regulatory system, they affect multiple hormone synthesis and secretion pathways in the hypothalamus-pituitary axis. They are a group of endogenously occurring acidic lipids that appear to play a role in the reproductive physiology.
Since prostaglandins are bioactive lipids, they exert an autocrine or paracrine function by binding to specific GPCRs (G-protein-coupled receptors) to activate intracellular signaling and gene transcription. As key regulators of reproductive processes, prostaglandins has many functions like having a role in the hypothalamic and pituitary control of gonadotropin secretion, ovulation, in luteinization and in the corpus luteum regression.
Prostaglandins also play a key role in the inflammatory response in the body. Their biosynthesis is significantly increased in inflamed tissues and can contribute to the development of the cardinal signs of acute inflammation in the body.
Researchers stated that prostaglandins have a plethora of actions in the central nervous system that can affect the progress of inflammation in the body differently, however, further studies are being tested to inhibit the role of these lipid mediators.
Conclusion
All fats play a very important role in the body. Essential fatty acids produce many compounds in the body when they are being metabolized in the body. Since the body can not produce essential fatty acids, they have to be consumed through food. The two important essential fatty acids are omega-6 and omega-3. These two fatty supplements help the body gain the nutrients the body needs to synthesize. Prostaglandins are also a key role in the body since they affect the pathways in the hypothalamus-pituitary axis and plays the role of regulating the reproductive physiology. Some products are formulated to target the immune support by creating micronized structure to increase the surface-to-volume ratio of particles to be more available to enzymatic actions.
October is Chiropractic Health Month. To learn more about it, check out Governor Abbott�s proclamation on our website to get full details on this declaration.
The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or chronic disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
References:
Bardin, T P. �The Role of Prostaglandins in Reproductive Physiology.� The Ohio State Medical Journal, U.S. National Library of Medicine, Oct. 1970, www.ncbi.nlm.nih.gov/pubmed/4918753.
Behrman, H R. �Prostaglandins in Hypothalamo-Pituitary and Ovarian Function.� Annual Review of Physiology, U.S. National Library of Medicine, 1979, www.ncbi.nlm.nih.gov/pubmed/373605.
Brinton, Eliot A, and R Preston Mason. �Prescription Omega-3 Fatty Acid Products Containing Highly Purified Eicosapentaenoic Acid (EPA).� Lipids in Health and Disease, BioMed Central, 31 Jan. 2017, www.ncbi.nlm.nih.gov/pubmed/28137294.
Calder, Philip C. �n-3 Polyunsaturated Fatty Acids, Inflammation, and Inflammatory Diseases.� The American Journal of Clinical Nutrition, U.S. National Library of Medicine, June 2006, www.ncbi.nlm.nih.gov/pubmed/16841861.
Di Pasquale, Mauro G. �The Essentials of Essential Fatty Acids.� Journal of Dietary Supplements, U.S. National Library of Medicine, 2009, www.ncbi.nlm.nih.gov/pubmed/22435414.
Dinan, Timothy, et al. �Investigating the Inflammatory Phenotype of Major Depression: Focus on Cytokines and Polyunsaturated Fatty Acids.� Journal of Psychiatric Research, U.S. National Library of Medicine, Jan. 2009, www.ncbi.nlm.nih.gov/pubmed/18640689.
Gibson, Robert A, et al. �Conversion of Linoleic Acid and Alpha-Linolenic Acid to Long-Chain Polyunsaturated Fatty Acids (LCPUFAs), with a Focus on Pregnancy, Lactation and the First 2 Years of Life.� Maternal & Child Nutrition, U.S. National Library of Medicine, Apr. 2011, www.ncbi.nlm.nih.gov/pubmed/21366864.
Guesnet, Philippe, and Jean-Marc Alessandri. �Docosahexaenoic Acid (DHA) and the Developing Central Nervous System (CNS) – Implications for Dietary Recommendations.� Biochimie, U.S. National Library of Medicine, Jan. 2011, www.ncbi.nlm.nih.gov/pubmed/20478353.
Gunnars, Kris. �What Are Omega-3 Fatty Acids? Explained in Simple Terms.� Healthline, 23 May 2019, www.healthline.com/nutrition/what-are-omega-3-fatty-acids.
Innes, Jacqueline K, and Philip C Calder. �Omega-6 Fatty Acids and Inflammation.� Prostaglandins, Leukotrienes, and Essential Fatty Acids, U.S. National Library of Medicine, May 2018, www.ncbi.nlm.nih.gov/pubmed/29610056.
Jabbour, H N, and K J Sales. �Prostaglandin Receptor Signalling and Function in Human Endometrial Pathology.� Trends in Endocrinology and Metabolism: TEM, U.S. National Library of Medicine, Oct. 2004, www.ncbi.nlm.nih.gov/pubmed/15380812.
Kapoor, Rakesh, and Yung-Sheng Huang. �Gamma Linolenic Acid: an Antiinflammatory Omega-6 Fatty Acid.� Current Pharmaceutical Biotechnology, U.S. National Library of Medicine, Dec. 2006, www.ncbi.nlm.nih.gov/pubmed/17168669.
Kenny, F S, et al. �Gamma Linolenic Acid with Tamoxifen as Primary Therapy in Breast Cancer.� International Journal of Cancer, U.S. National Library of Medicine, 1 Mar. 2000, www.ncbi.nlm.nih.gov/pubmed/10699943.
Khanapure, Subhash P, et al. �Eicosanoids in Inflammation: Biosynthesis, Pharmacology, and Therapeutic Frontiers.� Current Topics in Medicinal Chemistry, U.S. National Library of Medicine, 2007, www.ncbi.nlm.nih.gov/pubmed/17305573.
Kim, Kyu-Bong, et al. �?-Linolenic Acid: Nutraceutical, Pharmacological and Toxicological Evaluation.� Food and Chemical Toxicology : an International Journal Published for the British Industrial Biological Research Association, U.S. National Library of Medicine, Aug. 2014, www.ncbi.nlm.nih.gov/pubmed/24859185.
M.Shewchuk, Brian. �Prostaglandins and n-3 Polyunsaturated Fatty Acids in the Regulation of the Hypothalamic�Pituitary Axis.� Prostaglandins, Leukotrienes and Essential Fatty Acids, Churchill Livingstone, 28 Sept. 2014, www.sciencedirect.com/science/article/abs/pii/S0952327814001495.
Parker, Helen M, et al. �Omega-3 Supplementation and Non-Alcoholic Fatty Liver Disease: a Systematic Review and Meta-Analysis.� Journal of Hepatology, Centre for Reviews and Dissemination (UK), Apr. 2012, www.ncbi.nlm.nih.gov/pubmed/22023985.
Petersen, Martin, et al. �Effect of Fish Oil versus Corn Oil Supplementation on LDL and HDL Subclasses in Type 2 Diabetic Patients.� Diabetes Care, U.S. National Library of Medicine, Oct. 2002, www.ncbi.nlm.nih.gov/pubmed/12351465.
Ph.D., Catharine Paddock. �Could Omega-6 Fatty Acids Help Us Live Longer?� Medical News Today, MediLexicon International, 20 Mar. 2018, www.medicalnewstoday.com/articles/321266.php.
Simopoulos, Artemis P. �The Importance of the Omega-6/Omega-3 Fatty Acid Ratio in Cardiovascular Disease and Other Chronic Diseases.� Experimental Biology and Medicine (Maywood, N.J.), U.S. National Library of Medicine, June 2008, www.ncbi.nlm.nih.gov/pubmed/18408140.
Wang, Xiaoping, et al. �Multiple Roles of Dihomo-?-Linolenic Acid against Proliferation Diseases.� Lipids in Health and Disease, BioMed Central, 14 Feb. 2012, www.ncbi.nlm.nih.gov/pmc/articles/PMC3295719/.
Weylandt, Karsten H, et al. �Omega-3 Polyunsaturated Fatty Acids: The Way Forward in Times of Mixed Evidence.� BioMed Research International, Hindawi Publishing Corporation, 2015, www.ncbi.nlm.nih.gov/pmc/articles/PMC4537707/.
Zurier, R B, et al. �Gamma-Linolenic Acid Treatment of Rheumatoid Arthritis. A Randomized, Placebo-Controlled Trial.� Arthritis and Rheumatism, U.S. National Library of Medicine, Nov. 1996, www.ncbi.nlm.nih.gov/pubmed/8912502.
Inflammatory reactions in the central nervous system (CNS) are currently known to be associated with many neurological disorders. In neurodegenerative diseases, such as Alzheimer’s disease (AD) and Parkinson’s disease (PD), there is considerable penetration of different leukocyte subsets into the CNS or there is severe activation of microglial cells which increases many inflammatory mediators in the CNS. In acute CNS disorders, including delayed corrosion associated with vasospasm after subarachnoid hemorrhage (SAH), ischemic stroke, spontaneous intracerebral hemorrhage (ICH), and traumatic brain injury (TBI), current evidence from a variety of research studies reveal that inflammation may be a possible target for treatment. Inflammation is becoming a promising region of research study for new treatments. �
To speed up the process of translating this information to clinical applications, a number of significant problems have to be addressed as their capacity to continuously identify characteristic cerebral deficits in people with neurodegenerative diseases, the connections of brain injuries to clinical symptoms and genetic diagnosis as well as the level to which the harm respond to various treatment approaches. In this article, findings that address some of these problems are reported by several researchers. �
Contents
Inflammation and Neurological Disorders
In neurodegenerative diseases, a research study reviewed the function of chronic neuroinflammation in the pathogenesis of Alzheimer’s disease (AD). With the glial fibrillary acidic protein-interleukin 6 (GFAP-IL6) transgenic mice model, the researchers demonstrated that this animal model, in which chronic neuroinflammation triggered the expression of the cytokine interleukin-6 (IL-6) in astrocytes, could serve as a great tool for drug and/or medicine discovery and validation in vivo. �
Another research study assessed the role of inflammation in the neuropathology of Parkinson’s disease (PD). They supplied a synopsis of current knowledge on the temporal profile of immune reactions in PD and discussed the potential effects of central and peripheral inflammation. The research study utilized TRODAT-1 SPECT to rate leukocyte apoptosis from PD patients and its association with central dopamine neuron loss. The leukocyte apoptosis and striatal dopamine transporter uptake ratios were associated with the duration of the disease and increased severity. The interaction between brain and systemic inflammation may be liable for the neurodegenerative disease progression. Another research study utilized the Longitudinal Health Insurance Database 2000 (LHID2000) to analyze and evaluate the probability of dementia between patients clinically diagnosed with autoimmune rheumatic diseases (ARD) and non-ARD patients during a 5-year follow-up interval. Their findings indicate that patients with and without ARD had comparable risks of developing dementia. �
In severe critical CNS diseases, the research study utilized traumatic brain injury (TBI) models to determine whether simvastatin, together with an antioxidant, could cause cerebral vascular endothelial inflammatory responses after traumatic brain injury in rat models. Their findings support that simvastatin combined with an antioxidant could offer neuroprotection and it could possibly be attributed to cerebral vascular inflammatory reactions. The analysis utilized a structural equation modeling to evaluate the predictive value of admission Glasgow Coma Scale (GCS) scores, duration of unconsciousness, neurosurgical intervention, and countercoup lesion associated with the impairment of memory and processing rate functions six months after a TBI. The analysis also revealed that admission GCS score is a tremendous predictor of memory/processing speed dysfunctions after TBI. �
One research study investigated serum thiobarbituric acid-reactive substances (TBARS) and free thiol levels in a variety of subtypes of acute ischemic stroke (AIS) where they evaluated their association with clinical results. They discovered that patients with the disease have greater oxidative stress but reduced antioxidant defense compared to those with disease following AIS. Serum TBARS level at the acute phase of a stroke is a predictor for the outcome. Along with other research studies, these aimed to ascertain whether serum adhesion molecules are associated with septic encephalopathy (SE). Their findings reveal that SE suggests higher mortality in nontraumatic patients with sepsis. Serum vascular cell adhesion molecule-1 (VCAM-1) degree on presentation is a much more effective predictor of SE in these patients than lactate concentration and other adhesion molecules on admission, according to research studies. �
From the CNS health issues, research studies investigated the relationship between protein expressions of two autophagy markers, LC3B and Beclin-1, with clinical trials in astrocytoma patients. Their results suggest that targeting the cancer stem-like cell in astrocytoma can offer an approach that astrocytoma cancer stem-like cells together with improved autophagy may lead to resistance. Along with another research study, researchers researched DAPK protein expression and promoter hypermethylation in central neurocytoma and oligodendroglioma. Their results demonstrated that repressed expression and DAPK promoter hypermethylation of DAPK protein were prevalent in central neurocytoma than in oligodendroglioma. DAPK promoter hypermethylation can be useful for differential diagnosis between these two types of tumors. �
In conclusion, the article above emphasizes several essential research strategies that are making it more evident that neuroinflammation or inflammatory reactions are of translational significance for different types of neurological disorders. The results from these research studies not only enable us to understand the pathogenesis of these disorders but these also show great potential to provide desperately objective biomarkers for analysis and clinical investigation. Knowledge and comprehension of those conditions have contributed to the development of effective treatments, animal models, and innovative tools to characterize these medical conditions and provide better treatment options to patients. �
Neuroinflammation is ultimately characterized as the inflammation of the nervous tissue. It can commonly occur due to a variety of factors, including toxins, infections, autoimmune diseases, and even traumatic brain injury (TBI). In the central nervous system (CNS), the microglial cells are in charge of activating inflammatory reactions associated with these factors. However, excess microglia activation can ultimately cause a variety of health issues, including neurological diseases, among others. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
Metabolic Assessment Form
The following Metabolic Assessment Form can be filled out and presented to Dr. Alex Jimenez. Symptom groups listed on this form are not intended to be utilized as a diagnosis of any type of disease, condition, or any other type of health issue. �
In honor of Governor Abbott’s proclamation, October is Chiropractic Health Month. Learn more about the proposal. �
Inflammatory reactions in the central nervous system (CNS) are currently known to be associated with many neurodegenerative diseases, such as Alzheimer’s disease (AD) and Parkinson’s disease (PD). The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or chronic disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Neural Zoomer Plus for Neurological Disease
� �
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention. �
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force.
The body secretes and circulates 50 different hormones to different organs in the body. Hormones are the chemical substances that coordinate the activities of living organism growth. They are secreted through the endocrine glands and travel through the bloodstream to different organs in the body to function properly. When there is an excessive quantity or an reduced quantity of hormones being produced, it can cause the body to malfunction and develop chronic illnesses.
Contents
The Pituitary Gland Functions
In neuroendocrinology, an endocrine gland can�t make a hormone without activation from a pituitary-stimulating hormone. The pituitary-stimulating hormone helps regulate hormones by secreting them to the endocrine glands. The pituitary gland is known as the �master gland� since it controls the activity of the other endocrine glands and it consists of 3 parts known as the anterior, intermediate and posterior lobes.
Anterior Lobe
The anterior pituitary gland is located in the sella turcica and is controlled by the hypothalamus in the brain. It secretes a quantity of peptides and glycoprotein hormones that help regulate the growth, metabolism, reproduction and stress response. The anterior pituitary gland produces 6 hormones that circulate to their respective targets in the body.
ACTH (Adrenocorticotropic hormone): This hormone is a tropic hormone as it regulates cortisol and androgen production to the adrenal cortex. Cortisol or stress hormones stimulates the release of ACTH, while the adrenal cortex secretes glucocorticoids to the body�s metabolism.
GH (Growth hormone): This hormone helps regulate the body�s growth, metabolism, and composition. GH is secreted by the somatotroph cells located primarily in the lateral wings of the anterior lobe. GH can also secrete in al pulsatile fashion and can have a maximal release during a circadian rhythm at night.
TSH (Thyroid stimulating hormone): This hormone is involved by coordinating the signal regulation of the hypothalamus, the pituitary, and the thyroid. It requires the oxidation of dietary iodine, since iodine is absorbed through the small intestine and transported to the thyroid. After the iodine is transported it can be concentrated, oxidized and then incorporated into thyroglobulin to be formed to T4 and T3 later on.
LH (Luteinizing hormone): This hormone is highly important to both men and women, since it affects the sex organs and plays a role in puberty, menstruation and fertility. For women, it creates progesterone, which help regulate menstruation and supports pregnancy in the female body. For men, it creates testosterone, which helps regulates fertility, muscle mass, fat distribution, and red blood production in the male body.
FSH (Follicle stimulating hormone): This hormone plays an important part in the reproductive system and is responsible for ovarian follicles. For females, FSH helps produce estrogen, which is a group of sex hormones that help promote the development and maintenance of female characteristics in the human body, For males, FSH helps produce spermatogenesis and regulates sperm function in the male body.
Prolactin: This is a protein hormone in the anterior lobe. It has the ability to promote lactation to nursing mothers. It synthesizes within the pituitary gland, the central nervous system, the immune system, and the uterus.
Intermediate lobe
The intermediate lobe is composed of a homogeneous population of the endocrine cells, the melanotrophs and secretes several bioactive peptides. It contains very few blood vessels and can be virtually avascular. The melanotrophs are richly supplied by nerve fibers that originate from the hypothalamus.
Melanocyte-stimulating hormone: This hormone has many functions in a diverse physiological role. It affects skin pigmentation and studies have shown that it has antiapoptotic and anti-inflammatory effects that help decrease in nephrotoxin exposure to the body.
Posterior lobe
The posterior lobe is similar to the anterior lobe since they both control endocrine function and the body�s hormonal response to the environment. The hypothalamus receives neural signals from the brain and secretes polypeptide and neuropeptide hormones for storage in the posterior lobe until they are ready to be released. The hormones in the posterior lobe are in charge of regulating water retention and inducing uterine contractions.
ADH (Antidiuretic hormone): Also known as vasopressin, this hormone is a nonapeptide that is synthesized in the hypothalamus. It plays a bunch of important roles in controlling the body�s osmotic balance, regulates blood pressure, and makes sure that the kidneys are working. ADH is mainly responsible for tonicity homeostasis as they act primarily in kidneys to increase water reabsorption.
Oxytocin: Also known as the �love hormone�, oxytocin is also a neurotransmitter that is involved in childbirth and breast-feeding. It has benefits as a treatment for a number of conditions like depression, anxiety and intestinal problems and is produced in the hypothalamus. Studies show that females have a higher level of oxytocin than males, especially to nursing mothers with their babies.
Free-fraction Hormones
When an endocrine gland synthesizes a hormone, it is released into circulation and bound to as a protein. Hormones attach themselves to proteins but they can�t bind to hormone receptors. So what a hormone needs to do is to lose its binding protein to become a �free-fraction� hormone. Studies have stated that a fraction of a hormone that is free is called in vitro and it is equivalent to the fraction of a hormone that is free and available to be transported into tissues are called in vivo. Free-fraction hormones make up less than 1% of all circulating hormones since they don�t impact the hypothalamus-pituitary feedback loop.
Hormone Metabolites
Hormones are metabolized by hepatic and microbiome biotransformation pathways into various hormone metabolites. Hormone metabolites have their own impact on cell receptors, studies have shown that this impact is not fully understood yet but hormone metabolites are not a reflection of direct endocrine gland production but it can be metabolized in the liver as well. Hormone metabolites can bind to hormone receptors or can be eliminated by renal or fecal clearance pathways.
Conclusion
All in all, the body secretes and circulates 50 different hormones to different organs in the body. These hormones are chemically produced in the body and keep an eye on what each of the different organs is doing. It is important that the hormone receptors are functioning properly so that an individual is feeling good both inside and out. If there is a hormonal imbalance in the body, it can cause dysfunction and chronic illnesses to a person.
October is Chiropractic Health Month. To learn more about it, check out Governor Abbott�s proclamation on our website to get full details on this declaration.
The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or chronic disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
References:
Allen, Mary J. �Physiology, Adrenocorticotropic Hormone (ACTH).� StatPearls [Internet]., U.S. National Library of Medicine, 3 Mar. 2019, www.ncbi.nlm.nih.gov/books/NBK500031/.
Clinic, Cleveland. �Overactive Pituitary Gland & Hyperpituitarism.� Cleveland Clinic, 22 Mar. 2017, my.clevelandclinic.org/health/diseases/15173-pituitary-gland–hyperpituitarism-overactive-pituitary-gland.
Cuzzo, Brian. �Vasopressin (Antidiuretic Hormone, ADH).� StatPearls [Internet]., U.S. National Library of Medicine, 2 Feb. 2019, www.ncbi.nlm.nih.gov/books/NBK526069/.
Ellis, Mary Ellen, and Rachel Nall. �Luteinizing Hormone (LH) Test: What It Is and Why It’s Important.� Healthline, 29 Aug. 2017, www.healthline.com/health/lh-blood-test.
Ellis, Ronald E, and Gillian M Stanfield. �The Regulation of Spermatogenesis and Sperm Function in Nematodes.� Seminars in Cell & Developmental Biology, U.S. National Library of Medicine, May 2014, www.ncbi.nlm.nih.gov/pmc/articles/PMC4082717/.
Freeman, M E, et al. �Prolactin: Structure, Function, and Regulation of Secretion.� Physiological Reviews, U.S. National Library of Medicine, Oct. 2000, www.ncbi.nlm.nih.gov/pubmed/11015620.
Genes, S G. �Role of the Liver in Hormone Metabolism and in the Regulation of Their Content in the Blood.� Arkhiv Patologii, U.S. National Library of Medicine, 1977, www.ncbi.nlm.nih.gov/pubmed/334126.
Goyal, Shikha. �List of Important Hormones and Their Functions.� Jagranjosh.com, 12 Mar. 2019, www.jagranjosh.com/general-knowledge/list-of-important-hormones-and-their-functions-1516176713-1.
Gunawardane, Kavinga. �Normal Physiology of Growth Hormone in Adults.� Endotext [Internet]., U.S. National Library of Medicine, 12 Nov. 2015, www.ncbi.nlm.nih.gov/books/NBK279056/.
Hadley, M E, et al. �Biological Actions of Melanocyte-Stimulating Hormone.� Ciba Foundation Symposium, U.S. National Library of Medicine, 1981, www.ncbi.nlm.nih.gov/pubmed/6268380.
Lamacz, M, et al. �The Intermediate Lobe of the Pituitary, Model of Neuroendocrine Communication.� Archives Internationales De Physiologie, De Biochimie Et De Biophysique, U.S. National Library of Medicine, June 1991, www.ncbi.nlm.nih.gov/pubmed/1717055.
Lee, Heon-Jin, et al. �Oxytocin: the Great Facilitator of Life.� Progress in Neurobiology, U.S. National Library of Medicine, June 2009, www.ncbi.nlm.nih.gov/pmc/articles/PMC2689929/.
M., William. �Transport of Protein-Bound Hormones into Tissues in Vivo *.� OUP Academic, Oxford University Press, 1 Jan. 1981, academic.oup.com/edrv/article-abstract/2/1/103/2548700?redirectedFrom=fulltext.
MacGill, Markus. �Oxytocin: The Love Hormone?� Medical News Today, MediLexicon International, 4 Sept. 2017, www.medicalnewstoday.com/articles/275795.php.
MacGill, Markus. �Testosterone: Functions, Deficiencies, and Supplements.� Medical News Today, MediLexicon International, 6 Feb. 2019, www.medicalnewstoday.com/articles/276013.php.
Nichols, Hannah. �Estrogen: Functions, Uses, and Imbalances.� Medical News Today, MediLexicon International, 2 Jan. 2018, www.medicalnewstoday.com/articles/277177.php.
Patel, Hiran. �Physiology, Posterior Pituitary.� StatPearls [Internet]., U.S. National Library of Medicine, 27 Oct. 2018, www.ncbi.nlm.nih.gov/books/NBK526130/.
Rawindraraj, Antony D. �Physiology, Anterior Pituitary.� StatPearls [Internet]., U.S. National Library of Medicine, 25 Apr. 2019, www.ncbi.nlm.nih.gov/books/NBK499898/.
Researchers, Various. �Thyroid Hormone Synthesis.� Thyroid Hormone Synthesis – an Overview | ScienceDirect Topics, 2019, www.sciencedirect.com/topics/medicine-and-dentistry/thyroid-hormone-synthesis.
Rousset, Bernard. �Chapter 2 Thyroid Hormone Synthesis And Secretion.� Endotext [Internet]., U.S. National Library of Medicine, 2 Sept. 2015, www.ncbi.nlm.nih.gov/books/NBK285550/.
Seladi-Schulman, Jill. �Everything You Need to Know About Progesterone.� Healthline, 29 Apr. 2019, www.healthline.com/health/progesterone-function.
The discs that cushion the vertebrae are made up of a tough outer layer and a softer inner layer. When the outer layer is damaged and the inner layer comes out into the spine, it is referred to as�disc herniation.
Often the symptoms of a herniated disc include back pain, as the inner layer of the disc puts pressure on nerves in the spine. A herniated disc can impact the sciatic nerve, leading to sciatica.
If you know that your sciatica was caused by a herniated disc then try these exercises and stretches to help reduce back and leg pain.
Contents
Exercises that help relieve sciatica from a herniated disc
If your spine specialist or chiropractor informed you that a herniated disc is what caused the pain also known as lumbar radiculopathy they may recommend� three sciatica exercises:
Prone on elbows into Press-up
Upper back extension
Opposite arm and leg extension
These stretches can help provide relief when the root cause of sciatica from herniated or bulging disc.
Prone Elbows/Press-Up
This exercise is to ease sciatica from herniated disc pain and pressure in the lumbar spine/low back.
How to:
Lay on stomach
Slowly push up until rested on forearms
Beginners hold for 30 seconds
Once strength is gained and you feel comfortable then hold for 3 to 5 minutes
Gently lower to the floor
Repeat 10 times
Once comfortable holding for 5 minutes then perform an extended arms version, which is like push-ups raising your arms to the point where your elbows lock
Upper Back Extension
This exercise is to strengthen and stabilize the low back muscles.
How to:
Lay on your stomach with a small pillow or rolled towel under your hips
Rest your arms at your sides
Slowly lift your upper body up off the floor, contracting your low back muscles as you rise
Hold the lifted position for 3 seconds
Slowly lower your body to the ground
Repeat 10 times
Throughout this exercise, keep movements fluid and controlled.
Opposite Arm and Leg Extension
This exercise is to stabilize your spine and strengthen your low back, hamstring and gluteus muscles.
How to:
Lay on your stomach with a small pillow or rolled towel under your abdomen
Extend both arms in front of you
Contract your abdominal muscles as you slowly lift both your right arm and left leg
Hold for 3 seconds. Lower your leg and arm down
Repeat with your left arm and right leg
Hold for 3 seconds
Repeat the exercise 5 to 10 times on each side
As you alternate the lifts, make sure to keep abdominal muscles contracted to get the full benefit.
How do these exercises relieve sciatica from herniated disc
These exercises and stretches are designed to move the pain from the leg and into the low back.
This is centralization/localization.
This is a good thing, as the goal is to get the pain centralized and back at the source.
When the leg pain goes away, it means the pressure on the sciatic nerve and related nerves has been removed.
If sciatic pain stretches down to the foot, you will feel these exercises, meaning that the pain and electrical sensations will move through the ankle and knee. Which means you’re doing it correctly.
This does not mean that the pain is immediately going to centralize to the low back, it does take time because you are trying to stretch and straighten out this long nerve.
But you will notice sciatica pain does not go as far down the leg.
Therefore�these exercises need to be done consistently and be made a part of your routine.
What to know before exercising
Before starting these stretches, consider three recommendations:
Get a doctor�s approval
A spine specialist should clear you to perform these stretches and exercises before you start.
While these exercises are safe, get a doctor�s permission before starting physical activity.
Know the cause so your exercise program helps and not makes the condition worse
Sciatica from herniated disc means a different type of exercise than sciatica caused by piriformis syndrome.
Knowing this information will help you choose an exercise plan that provides maximum relief.
Don�t push too hard
Don’t aggravate sciatica, listen to your body and go slow.
Experience any pain or symptoms:
Weakness
Tingling
Numbness
Contact a spine specialist immediately!
Sciatic nerve pain caused by a herniated or bulging disc is a common problem.
But incorporating these exercises and stretches can provide sustained relief.
The sciatic nerve is a large nerve that travels from the lower back down both of the legs and into the feet. When pressure is placed on the nerve, such as from a herniated disc, it can lead to the symptoms commonly referred to as sciatica.
The sciatic nerve can be impacted by a number of different things, including injury and degenerative diseases.
Difference Foot Orthotics Make to *REDUCE FOOT PAIN* & Correct Posture | El Paso, TX (2019)
Custom made foot orthotics can help control foot motion and posture. Healthcare professionals prescribe custom foot orthotics to help patients focus on their foot posture and mobility control. Research studies have ascertained that using custom foot orthotics for posture and mobility control can help fix excessive foot pronation and supination to prevent a variety of foot health problems. The subsequent video describes how custom foot orthotics will help control foot posture and mobility to improve health and wellness.
NCBI Resources
Sciatica is a common back ailment that affects approximately 1 in 10 adults in the United States. It is most prevalent in people between the ages of 25 and 45. Sciatica is characterized by a shooting pain that originates in the lower back and travels down through the hip, buttock, and back of the leg.
The pain can be so severe that it inhibits mobility and can prevent people from working, taking care of their homes, or just enjoying their life. Traditionally, doctors have treated the condition with medications and some invasive therapies, but chiropractic treatments have been found to be extremely effective in alleviating the pain and curing the condition.
There is plenty of controversies associated with MSG. Researchers believe that the excess consumption of monosodium glutamate can cause asthma, headaches, and even brain health issues. On the other hand, the majority of official sources, including the FDA, claim that MSG is a safe food ingredient. The following article discusses what is monosodium glutamate, or MSG, and its effects on overall health and wellness, exploring both sides of the argument on the food ingredient. �
Contents
What is Monosodium Glutamate (MSG)?
MSG is known as monosodium glutamate. It is a common food ingredient that is utilized to enhance flavor in foods. MSG comes from the amino acid, glutamate or glutamic acid, which is one of the most common amino acids found in nature. Glutamate is a non-essential amino acid, which ultimately means that the human body can naturally produce it. Monosodium glutamate also serves a variety of functions in the human body and it is commonly found in almost all types of foods. �
MSG is a white crystalline powder that looks similar to sugar or table salt. It is also made up of a combination of sodium and glutamic acid, known as sodium salt. The glutamic acid in MSG is created by fermenting starches, however, there is no chemical difference between the glutamic acid in monosodium glutamate and that found in natural foods. The glutamic acid in MSG can be easier to absorb because it isn’t bound inside big protein molecules which the body breaks down. �
Glutamate in the Human Body
Our stomach and gut lining have many glutamate receptors. MSG and other types of glutamate are absorbed through these receptors. Once in the gastrointestinal, or GI, tract, glutamate is broken down as energy or incorporated into other molecules. Glutamate is also an essential neurotransmitter in the brain. However, researchers believe that dietary glutamate is unable to cross the blood-brain barrier, which ultimately suggests that all glutamate from the brain is created there. �
Evidence from research studies in mice showed that the blood-brain barrier in newborns is immature and that glutamate can pass into the brain. Increased levels of glutamate injected into newborn mice caused considerable brain damage. A research study showed that increased levels of MSG also cause severe effects in fruit flies, causing premature death. While the levels utilized in these research studies exceeded average daily consumption reported among humans, it is essential to mention that restaurants and food manufacturers are not required to declare the levels of MSG added to their foods. �
Is MSG Good or Bad for You?
Glutamate, or glutamic acid, functions as a neurotransmitter in the human brain. It is also considered an excitatory neurotransmitter, which means that it stimulates nerve cells to transmit signals. Several people believe that MSG causes excess glutamate in the brain and excess stimulation of the nerve cells. Therefore, MSG has been labeled as an excitotoxin. �
Concerns associated with the effects of MSG date as far back as 1969, when a research study found that injecting large doses of MSG into newborn mice caused harmful neurological effects. Since then, a variety of other sources have continued to have this concern with MSG. Another research study showed that increased glutamate activity in the brain can cause harm and large doses of MSG can raise blood levels of glutamate. Aa megadose of MSG increased blood levels by 556%. �
However, dietary glutamate should have little to no effect on the human brain because it can’t cross the blood-brain barrier in large amounts. There is not enough evidence to show that MSG acts as an excitotoxin when consumed in normal amounts. �
Monosodium Glutamate (MSG) Sensitivity
Several people may also experience adverse effects from consuming MSG. This health issue is known as Chinese restaurant syndrome or MSG symptom complex. In one research study, people with self-reported MSG sensitivity consumed either 5 grams of MSG or a placebo where 36.1% reported reactions with MSG compared to 24.6% with placebo. Common symptoms included headaches, flushing, muscle tightness, tingling sensations, numbness, and weakness, among other symptoms. �
The threshold dose that causes symptoms seems to be around 3 grams per meal. However, keep in mind that 3 grams is a very high dose, approximately six times the average daily intake of MSG in the United States. It is still unclear why this happens, however, some researchers hypothesize that such large doses of MSG allow trace amounts of glutamic acid to cross the blood-brain barrier and interact with neurons which can cause brain damage, swelling, and injury. Several believe that MSG also causes asthma in susceptible people. In one 32-person research study, 40% of participants experienced an asthma attack with MSG. However, other research studies did not find any relationship between MSG intake and asthma. �
Conclusion
Depending on who you ask, MSG is either perfectly safe or a dangerous neurotoxin. The truth lies somewhere in between. Evidence indicates that MSG is safe in moderate amounts. However, megadoses may cause harm. If you react adversely to MSG, you shouldn�t eat it. That said, if you don�t experience side effects, there�s no compelling reason to avoid it. Keep in mind that MSG is generally found in processed, low-quality foods � which you should avoid or limit anyway. If you already eat a balanced diet with plenty of whole foods, you shouldn�t have to worry about high MSG intake. �
The controversy between MSG and brain health has been determined by a variety of research studies. Monosodium glutamate, or MSG, has been utilized as a food ingredient and it is largely consumed by many people in the US on a regular basis today. Although the FDA, or the Food and Drug Administration, categorizes MSG as a safe food ingredient, many research studies have determined that it can cause a variety of brain health issues, including neurological diseases, among other well-known health issues. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
Metabolic Assessment Form
The following Metabolic Assessment Form can be filled out and presented to Dr. Alex Jimenez. Symptom groups listed on this form are not intended to be utilized as a diagnosis of any type of disease, condition, or any other type of health issue. �
In honor of Governor Abbott’s proclamation, October is Chiropractic Health Month. Learn more about the proposal. � There is plenty of controversies associated with MSG. Researchers believe that the excess consumption of monosodium glutamate can cause asthma, headaches, and even brain health issues. On the other hand, the majority of official sources, including the FDA, claim that MSG is a safe food ingredient. The article discusses what is monosodium glutamate, or MSG, and its effects on overall health and wellness, exploring both sides of the argument on the food ingredient. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or chronic disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Neural Zoomer Plus for Neurological Disease
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention. �
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force.
When the weather begins to change and that cold feeling starts to creep into the bones, especially down the back. That’s when sciatica symptoms can flare-up in the worst way.
Contents
Cold weather really make sciatica worse
Of the many patients that I’ve treated, those with sciatica firmly state that cold weather makes it worse.
There are bonafide reasons why sciatica acts up when the temperature goes down.
Sciatica
It is a type of radiculopathy, caused by pressure on one or more of the five nerve roots in the lower back;
This is known as the lumbar region of the spine.
The nerves run from the lower spine under buttocks and down each hip into the legs.
Several conditions can compress these nerves at one or more spots along the way:
Numbness
Weakness in the
Lower back
Buttock
Legs on one or both sides
Research Study
Cold weather affects sciatica because it affects different types of pain.
A study surveyed around 135,000 construction workers.Researchers found that the men who worked in low temperatures reported higher cases of neck and low back pain.
This was compared with those working in warmer temperatures.
Cold Weather & the Spine
Pain and discomfort can increase because the muscles stiffen up in cold weather.
The spine’s muscles also become tight and tense.
Tension and stress, can make the pain worse and increase the risk of muscle strains/sprains.
Barometric Pressure
Air pressure drops before a storm or when the temperature changes.
These changes seep into the sensitive nerves of the lower back and cause swelling/inflammation and pain.
Physical Stress
Any type of movement can wreak havoc on a healthy spine.
This is due to the cold weather causing individuals not to:
Use correct posture
Use correct movement when performing tasks/chores
Hurrying tasks/chores
There is also the chance of a slip and fall accident or twisting your back.
All of this is the perfect set-up for spine and sciatic injury/s.
So How to reduce sciatic pain?
Keep Warm
Wear warm clothing and in layers.
A few thin layers can keep the body warmer than a single thick layer.
Keep the lower back warm
Tuck your shirt into your pants to make sure that your back doesn’t get a cold draft when you reach for something and then put a sweater on over that.
A couple of blankets or an electric blanket on your bed can help keep your muscles from tightening.
Keep home as warm as possible.
Run the car a few minutes to preheat it before heading out.
Wear Proper Shoes or Boots
Proper footwear should have enough tread to prevent slips and falls.
Proper shoes for walking in cold weather. Don’t do the flip-flop thing, that’s just asking for foot/back problems.
Orthotics can help with posture, pronation, and gait.
Warm-Up Before Starting Outdoor Activity
Stretch and loosen the muscles and joints before you go out to:
Trim the lawn/bushes
Take a walk
Play with the kids
Take a few minutes to stretch and warm up inside before going outside.
Do It Right
As previously mentioned use correct form, meaning, lift with your legs, not the back.
Move smaller amounts if landscaping etc., Do it in small increments instead of one or two heavy loads.
Don’t twist your back while lifting.
Face the direction you are going in.
Ask for Help
If sciatica is affecting the task at hand, do not be too proud or afraid to ask for help. Stubbornness can lead to severe injury/s that could have been avoided.
Stay Active
When cold weather starts to make itself known, most of us want to get on the couch, binge watch our favorite movies, sleep, get snuggly, etc.
Exercising and staying in shape is a top remedy for sciatica symptoms.
Consult with a chiropractor, physical therapist/trainer that can offer exercises that won’t present/exacerbate symptoms
Watch your weight when the cold weather kicks in and keep up with your exercise.
El Paso, TX Chiropractor Sciatica Symptoms
Sandra Rubio discusses sciatica, its causes, and its symptoms. Sciatica is the collection of symptoms caused by the compression of the sciatic nerve, the longest nerve in the human body which extends from the lower back to the feet. Sandra Rubio describes how she’s witnessed many patients come into Dr. Alex Jimenez’s office feeling painful and often severe symptoms of sciatica caused by a variety of spinal health issues. Fortunately, Dr. Jimenez is the non-surgical choice for the safe and effective treatment of sciatica symptoms.
Based upon how it’s defined, approximately 2 percent to 40 percent of individuals will experience sciatica symptoms at some point in their lifetime. It is most frequent during people’s ’40s and ’50s, and men are more frequently affected than women. About 90 percent of the time, sciatica symptoms are because of a disc herniation. Other issues that may bring about sciatica comprise of spondylolisthesis, spinal stenosis, piriformis syndrome, pelvic tumors, and compression by a baby’s head during pregnancy, among other spinal health issues.
NCBI Resources
Chiropractic care is a popular, alternative treatment option commonly utilized to help treat symptoms of sciatica. Sciatica is characterized as a collection of symptoms, rather than a single injury or condition. A chiropractor can help diagnose the source of a patient�s sciatic nerve pain, or sciatica, in order to properly determine the best treatment for their specific health issue.
Spinal adjustments and manual manipulations can be utilized to help carefully correct the alignment of the spine, restoring the natural integrity of the spine and allowing the body to heal itself, without the need for drugs and medications or surgery. In certain individuals, sciatica may fix itself, possibly happening just once or a few times throughout their lifetime. But, it�s important to remember that if an injury and/or aggravated condition is not treated effectively, symptoms may worsen.
The endocrine system is a network of glands and organs surrounding the body. While it is similar to the nervous system, it plays a vital role in controlling and regulating many body functions, as well as using chemical messengers called hormones. Since hormones circulate throughout the entire body, each type of hormone targets specific organs and tissues. The whole system is made up of glands and organs that release hormones into the body. Each has a different function to make sure that the human body is working correctly. If there is a disruption in one of the organs, it can cause problems and possibly lead to chronic illnesses later on.
Contents
Functioning The Endocrine System
In the endocrine system, it is responsible for regulating the body through the release of hormones. These hormones are secreted by the glands that travel through the bloodstream to various organs and tissues, telling them what to do or how to function in the body properly. Some of the bodily functions are controlled by the endocrine system. This includes the body�s metabolism, growth and development, heart rate, blood pressure, body temperature, appetite, and sleeping and waking cycles.
Studies have shown that the endocrine and the nervous system work closely together since the brain continuously sends instructions to the endocrine system while returning the favor, the endocrine glands receive feedback to the brain. With an intimate relationship, both methods are referred to as the neuroendocrine system. The neuroendocrine system is a mechanism where the hypothalamus maintains homeostasis, regulates reproduction, metabolism, and blood pressure. The neuroendocrine system works together with the immune system as they play an essential role in maintaining and restoring homeostasis in the body to function correctly.
The Organs of the Endocrine System
The endocrine system has a complex network of glands that secrete substances. The glands produce, store, and release throughout the body, targeting specific organs and tissues. Here are what each gland does in the endocrine system and what their functions are in the body.
Hypothalamus
The hypothalamus gland is known as the master switchboard located in the center of the brain. Its role is significant because it controls and creates many hormones in the body. It also makes sure that it has to keep the body in a homeostasis state as much as possible. If the hypothalamus is not working correctly, it can cause problems for the body, and it can lead to a wide range of rare disorders.
Pituitary
The pituitary gland is known as the master gland due to regulating the other endocrine glands activities. It plays an essential role by balancing hormone levels in the body, and together with the hypothalamus gland, they control the involuntary nervous system. This system helps manage the balance of the energy, heat, and water in the body. The pituitary gland also produces several hormones that can either regulate most of the other hormone glands or a direct effect on specific organs. When the endocrine glands produce too little or an excessive quantity of hormones, it can cause the body to be imbalanced.
Pineal
The pineal gland is a small, pea-shaped gland that is in the brain and is sometimes called �the third eye.� It plays a role in producing and regulates hormones in females that may affect fertility and the menstrual cycle, including producing and excreting melatonin in the body. A 2016 study suggests that melatonin can help protect against cardiovascular diseases; however, there is still more research being done about the potential function of melatonin in the body.
When the pineal gland is not producing the correct amount of melatonin, it can cause an individual to have sleep disorders and accumulate an excessive quantity of calcium in the body. One of the most prominent symptoms that can cause pineal gland dysfunction is a change in circadian rhythms. A person can disrupt their circadian rhythm either sleeping too much or too little, having restless nights, and feeling sleepy at unusual times.
Thyroid
The thyroid gland a butterfly wing-shaped gland that is located in the anterior neck. It plays a huge vital role in the metabolism, growth, and development of the human body. It regulates many body functions by constantly releasing a steady amount of hormones in the bloodstream. When the thyroid produces too much or too little hormones, it can cause hyperthyroidism and hypothyroidism in the body, causing many chronic illnesses in the body.
Parathyroid
The parathyroid gland is located behind the thyroid and plays a vital role in maintaining bone health, making sure the nervous system is running smoothly, and that muscles are pumping regularly. Parathyroid glands release PTH (parathyroid hormone), which regulates calcium in the bloodstream. Research shows that calcium is the only mineral in the body that has its very own dedicated regulatory gland. Calcium not only helps with bone strength, but it conducts electrical impulses in the nervous system and its energy in muscle cells. The PTH can also signal the kidneys and small intestines to save calcium from being digested.
When the parathyroid gland produces an excessive amount or a decreased amount of PTH, it can cause hyperparathyroidism and hypoparathyroidism leading the body to have many malfunctions, including weak bones in the body.
Thymus
The thymus gland is known as �the forgotten, but very important organ.� �It produces progenitor cells, which matures into T-cells and helps the organs in the immune system to grow properly. According to an article published by the NLM (U.S. National Library of Medicine), it stated that the thymus is the primary cell donor for the lymphatic system.
The adrenal glands are located on the top of the kidneys and help produce sex hormones and cortisol, they even work together with the pituitary glands. When cortisol is released from the adrenal glands, it can help with the response to stress and many essential functions in the body. When abnormal signals are disrupting the number of hormones that the pituitary glands telling the adrenal glands to produce. It can cause vitamin D to unbalance and many chronic illnesses.
Pancreas
The pancreas is located in the abdomen and is part of the digestive system. It produces insulin, essential enzymes, and hormones that help break down food and sends it to the small intestine. When the pancreas produces the insulin hormone, it secretes it into the bloodstream, regulating the body�s glucose levels. There are many problems if the pancreas is not functioning correctly, causing the entire body to malfunction. If the pancreas is not producing enough insulin in the body, an individual is at risk for diabetes. Another factor is the development of pancreatic cancer caused by smoking or heavy drinking. The best way to keep a healthy pancreas is to maintain a healthy balanced diet.
Conclusion
The endocrine system is a network of glands and organs that surrounds the body. Each gland sends out hormones throughout the body and transfers to the specific organs that need these hormones to function correctly. If there is a disruption in the endocrine system, it can cause the body to malfunction and develop chronic illnesses.
October is Chiropractic Health Month. To learn more about it, check out Governor Abbott�s declaration on our website to get full details on this proclamation.
So the mechanisms of an autoimmune disease can be either by genetics or by environmental factors that can cause an individual to have problems in their body. There are many autoimmune diseases, both common and rare, that can affect the body. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or chronic disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
References:
Bradford, Alina. �Parathyroid Glands: Facts, Function & Disease.� LiveScience, Purch, 5 May 2017, www.livescience.com/58980-parathyroid-glands.html.
Cherney, Kristeen. �Adrenal Glands.� Healthline, 26 July 2016, www.healthline.com/health/adrenal-glands.
Chu, Linda C, et al. �Diagnosis and Detection of Pancreatic Cancer.� Cancer Journal (Sudbury, Mass.), U.S. National Library of Medicine, 2017, www.ncbi.nlm.nih.gov/pubmed/29189329.
Crosta, Peter. �Pancreas: Functions and Disorders.� Medical News Today, MediLexicon International, 26 May 2017, www.medicalnewstoday.com/articles/10011.php.
Duggal, Neel. �5 Functions of the Pineal Gland.� Healthline, 7 Apr. 2017, www.healthline.com/health/pineal-gland-function.
Imrich, Richard. �The Role of Neuroendocrine System in the Pathogenesis of Rheumatic Diseases (Minireview).� Endocrine Regulations, U.S. National Library of Medicine, June 2002, www.ncbi.nlm.nih.gov/pubmed/12207559.
Johnson, Jon. �Hypothalamus: Function, Hormones, and Disorders.� Medical News Today, MediLexicon International, 22 Aug. 2018, www.medicalnewstoday.com/articles/312628.php.
Mannstadt, Michael, et al. �Hypoparathyroidism.� Nature Reviews. Disease Primers, U.S. National Library of Medicine, 31 Aug. 2017, www.ncbi.nlm.nih.gov/pubmed/28857066.
N/A, Uknown. �Circadian Rhythms.� National Institute of General Medical Sciences, U.S. Department of Health and Human Services, Aug. 2017, www.nigms.nih.gov/education/pages/factsheet_circadianrhythms.aspx.
Rosenow, E C, and B T Hurley. �Disorders of the Thymus. A Review.� Archives of Internal Medicine, U.S. National Library of Medicine, Apr. 1984, www.ncbi.nlm.nih.gov/pubmed/6608930.
Seladi-Schulman, Jill. �Endocrine System Overview.� Healthline, 22 Apr. 2019, www.healthline.com/health/the-endocrine-system.
Sun, Hang, et al. �Effects of Melatonin on Cardiovascular Diseases: Progress in the Past Year.� Current Opinion in Lipidology, Lippincott Williams & Wilkins, Aug. 2016, www.ncbi.nlm.nih.gov/pmc/articles/PMC4947538/.
Tirabassi, Giacomo, et al. �Adrenal Disorders: Is There Any Role for Vitamin D?� Reviews in Endocrine & Metabolic Disorders, U.S. National Library of Medicine, Sept. 2017, www.ncbi.nlm.nih.gov/pubmed/27761790.
Unknown, Unknown. �How Does the Pituitary Gland Work?� InformedHealth.org [Internet]., U.S. National Library of Medicine, 19 Apr. 2018, www.ncbi.nlm.nih.gov/books/NBK279389/.
Unknown, Unknown. �How Does the Thyroid Gland Work?� InformedHealth.org [Internet]., U.S. National Library of Medicine, 19 Apr. 2018, www.ncbi.nlm.nih.gov/books/NBK279388/.
Villines, Zawn. �Pineal Gland Function: Definition and Circadian Rhythm.� Medical News Today, MediLexicon International, 1 Nov. 2017, www.medicalnewstoday.com/articles/319882.php.
Vorvick, Linda J., et al. �Endocrine Glands – Health Video: MedlinePlus Medical Encyclopedia.� MedlinePlus, U.S. National Library of Medicine, 10 May 2019, medlineplus.gov/ency/anatomyvideos/000048.htm.
Yuen, Noah K, et al. �Hyperparathyroidism of Renal Disease.� The Permanente Journal, The Permanente Journal, 2016, www.ncbi.nlm.nih.gov/pubmed/27479950.
Zdrojewicz, Zygmunt, et al. �The Thymus: A Forgotten, But Very Important Organ.� Advances in Clinical and Experimental Medicine : Official Organ Wroclaw Medical University, U.S. National Library of Medicine, 2016, www.ncbi.nlm.nih.gov/pubmed/27627572.
MSG is a food additive which is found in the majority of the industrial foods. It boosts the taste of the food hence attracting customers. There is no value in terms of nutrition and it really does nothing to the eater, however, it can have many effects on foods. MSG is known as an “excitotoxin” or neurotoxin. Research studies have found that it has devastating and degenerative effects on the brain and the nervous system. The neurons or brain cells overstimulate and fatigue to their death. MSG enters the brain through the membranes in the mouth and the throat. It also enters the blood-stream through the digestion of food in the gastrointestinal (GI) tract. MSG “tricks” the human body into believing that it is getting value from these foods. �
MSG is not a natural substance found in nature. It’s a man-made chemical from glutamic acid, an amino acid found in proteins. Amino acids do happen naturally in animal cells and in several plant cells. The kinds of amino acids have been processed through the change of this pure form of glutamate. Some of the materials used for this purpose include starches, molasses, and corn. The manipulation procedure generates this type of glutamate. The d-glutamate is not found naturally. The free glutamates can enter the body about eight to ten times faster compared to natural glutamates. Natural glutamate is found in foods such as tomatoes, mushrooms, and milk. Techniques used to manufacture glutamate were not in use before the 1960s. The MSG in use now is not natural. In the article, we will discuss how MSG is associated with neurological diseases. �
Contents
Research Studies on MSG and Neurological Diseases
Research studies indicate that MSG is the reason for neurological diseases like Alzheimer’s disease, Huntington’s disease, Parkinson’s disease, and Amyotrophic lateral sclerosis. Neuroscientists have explained that MSG attacks the blood-brain barrier of the neurons which is responsible for the regulation of the fragile chemical exchange inside the brain cells. The chemical exchange process is well balanced and its performance is unquestionable. Under normal conditions, the brain and the entire immune system manage all sorts of toxins, health issues, and stress. A very small amount of poisonous substances can actually make the brain overreact, ultimately resulting in excessive exhaustion and death, according to research studies. �
MSG is a leading “excitotoxin” and it is widely known to cause harm to the brain region which governs or controls additional systems from the human body. The damage will seem like a disease in the endocrine system and the immune system. This can be shown in the cases of food cravings, persistent hunger, and unusual sleeping patterns. This normally leads to obesity. MSG is also known to cause migraine headaches, behavioral disorders, depression, asthma attacks, heart problems, arthritis, sinus issues, and digestive issues. �
MSG is a neurotoxin which requires an extremely brief time to create a broadly diverse and dramatic effect on the human body. An individual may have a mild dose of a prescription drug and also have favorable effects. However, another individual might take the prescription drug and get sad, have a swollen tongue, stomach disorders, and joint problems. The different parts of the brain affected do govern various body functions. The part which is attacked will depend on the individual. If by way of instance, an individual has had a headache, a genetic pinch in a given portion of the brain, has had a fever that’s attacking regions of the brain, or has had a stroke, then it’s certain that the component of the brain that has been affected will be due to the toxins. �
A number of the foods sold are ultimately sold as weight loss promotions to the people. MSG, along with aspartame, is added when food substances, such as fat and sugar, are eliminated from the meals. These excitotoxins have been known to cause obesity and irregular heartbeats. FDA generally allows the labeling of MSG’S as natural flavors, hydrolyzed proteins, and autolyzed yeast, when used as just a partial ingredient in an additive rather than only MSG. Americans now are consuming 160 million lbs of MSG per year. Author and toxicologist Dr, George Schwartz asserts that two tablespoons of MSG on bread could kill a medium-sized dog within a moment. The FDA in 1995 claimed that no one can respond to less than 3 grams of MSG per meal. In spite of their confirmation, they’ve warned that children, pregnant or lactating women, and the elderly should avoid MSG. An extremely sensitive individual can also ultimately react even to under a gram of MSG. �
Effects of MSG and Neurological Diseases
Research studies have shown that from the late 1950s, an estimated amount of 12 grams per person of MSG was utilized by most Americans each year. These days, taking a look at precisely the same health issue, the quote is between 400 and 500 g per person each year. This is an amount which requires evaluation. The wide usage of MSG arrived in the mid-1970s. It gained much popularity throughout the 1980s with manufacturers of food. Two powerful excitotoxic food additives which took the food sector by storm have been the use of MSG and aspartame. MSG has been broadly associated with a wide assortment of symptoms and health issues. As previously stated, it affects the human body’s neurological system. The same ailments are being reported to be on their rise. The ailments are absolutely unexpected and difficult to describe. �
Neurological diseases associated with MSG and numbers of interest released by federal organizations have been recorded in fibromyalgia, which is a growing epidemic. Its patients eliminated aspartame and MSG during the research study conducted by the Florida University which reported complete relief of symptoms. On the other hand, the most cognitive research study was conducted to prove the connection between fibromyalgia and MSG along with several different additives as a common rheumatologic disorder. In this case, 4 patients had been diagnosed for 2 to 17 years with fibromyalgia syndrome. They had undergone various methods of therapy whilst failing to consider MSG as the causative agent. After eliminating aspartame and MSG in their diets, complete or near complete resolution of symptoms diagnosed was listed within months. The subjects were women who had recurring symptoms and multiple comorbidities. It’s therefore indicative that the excitotoxins, present in compounds, such as aspartate and MSG, become excitatory neurotransmitters once ingested and when consumed in excess may lead to neurotoxicity. These 4 patients may, therefore, signify this fibromyalgia syndrome and act as a link to conclusively establish a link to MSG. Therefore, persistent research studies, if carried out on a larger sample, might serve to connect the fibromyalgia syndrome into MSG and aspartame more concretely. Further research studies are required. �
Moreover, a research study connected MSG to adrenal adenomas. The hypothalamus which leads damage on the nerves is overstimulated by MSG. The hypothalamus is responsible for directing the pituitary gland’s actions, which can be known as the endocrine gland since it in turn directs the rest of the glands in the human body and their activities such as metabolism, development of reproductive and sex organs and other essential development functions. Statistics have demonstrated that 25 percent of Kenyans have a pituitary adenoma. However, research studies linking pituitary adenomas to MSG have ultimately been inconclusive. Some research studies had depicted this as a disease but have been proven wrong. �
About half of the pituitary adenomas secrete prolactin. These can become large over time in the optic nerve, thus, affecting vision. It also prevents ovulation and menses. This prevents pregnancy or conception generally. Furthermore, since prolactin is responsible for lactation, lactation can be caused by secretion in the individual even if they’re male or even when they were not pregnant. Men with these adenomas grow breasts. Since the tumor can only be discovered when it’s big and dangerous unlike in women that are forewarned by the effects on vision or related headaches, this problem is deadly in men. There’s a further need to sponsor more research studies so as to ultimately associate MSG and brain tumors, among others. �
Other effects which were attributed to MSG and neurological diseases are headaches and migraines, asthma, and obesity amongst others. In headaches and migraines, an approximate amount of $2.2 billion each year are being spent on drugs and/or medicines that treat head pain. This chronic condition has received a 74 percent increase. Second, asthma associated with the brain was connected to MSG. According to data, there was a decrease of asthma before the mid-eighties. Since then, however, there’s been a 100 percent gain in the rate of death among children and seniors. This prevalence has increased by 600 percent in the last 10 years. FDA has identified that uncontrollable asthma can be caused by MSG, sadly, no measures are taken to take care of the situation. In defects of birth and disorders of production, MSG was identified as a mutagen i.e. mutates fetuses. It’s reputed to cause damage to the development, reproduction, and growth patterns as well as the functions. Such research studies have not been concrete. Other consequences include emotional or neurological disorders. Laboratory research studies demonstrate devastating effects on brain development, including dyslexia, attention deficit, autism, hyperactivity, violent episodes or rage, panic attacks, depression, paranoia, seizures and cerebral palsy. Rats were utilized with this research study. However, human beings are five times more sensitive to MSG than rats. �
This topic of ailments in behavior for children is becoming a frequent discussion amongst professionals. These have associated attention deficits, behaviour, and instability to chemical imbalances occurring in the brain. It is now becoming an intense possibility that there’ll be damage caused by excitotoxins in the blood-brain barrier of young brains. �
In April 1994, a magazine article confirmed the rising problem of behavioral disorders. The magazine stated that the attention deficit hyperactivity disorder wasn’t in existence. It’s however said that it is currently affecting 3.3 million American kids. This magazine article estimates prominent research studies which 10 years ago stated that symptoms of ADHD and ADD vanished with maturity. Nowadays, however, ADD is the fastest growing diagnostic category for adults. The combination of both excitotoxins i.e. MSG and aspartame came into wide utilization in the 1980s. �
In the medical field, a controversy as to whether MSG is associated with neurological diseases has been determined. Monosodium glutamate, or MSG, has been utilized as a flavorant in the food industry for approximately 100 years and it is consumed by the masses on a regular basis today. Although the FDA, or the Food and Drug Administration, categorizes MSG as a safe food ingredient, many research studies have determined that it can cause a variety of health issues, including neurodegenerative diseases, among others. – Dr. Alex Jimenez D.C., C.C.S.T. Insight – Dr. Alex Jimenez D.C., C.C.S.T. Insight
Metabolic Assessment Form
The following Metabolic Assessment Form can be filled out and presented to Dr. Alex Jimenez. Symptom groups listed on this form are not intended to be utilized as a diagnosis of any type of disease, condition, or any other type of health issue. �
In honor of Governor Abbott’s proclamation, October is Chiropractic Health Month. Learn more about the proposal. � MSG is a food additive. It boosts the taste of food, attracting customers. There is no nutrition and it really does nothing to the eater, however, it can have many effects on foods. MSG is known as an “excitotoxin” or neurotoxin. Research studies have found that it has devastating and degenerative effects on the brain and the nervous system. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or chronic disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Neural Zoomer Plus for Neurological Disease
� �
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention. �
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force.
There are those that can predict approaching storms, and weather change based on the way, their joints behave.
Similarly, individuals with chronic back pain can at times sense a change in how they feel when the weather shifts.
The connection between weather and back pain is not fully understood but here are a few beliefs on why people feel pain based on the season/weather.
There is not a great deal of research on weather’s effects on spinal conditions. said Dr. Alexander Jimenez, D.C. in El Paso, Texas.
Some spinal conditions have been shown to have a clear link to cold weather. An example is sciatica patients that would experience worsened pain when the weather would shift.
Chiropractor Alexander Jimenez breaks down how weather can affect back pain and explains six ways to help weather-related back pain.
Contents
Weather and Osteoarthritis
Dr. Jimenez talks of a study that examined joint pain differencesbetween older people with osteoarthritis that were weather-sensitive versus those who also had osteoarthritis but were not weather-sensitive.
More than two-thirds said weather affected their osteoarthritis pain
Researchers found that weather sensitivity and pain:
More prevalent among women
People with anxiety conditions
Weather and season change alters how we feel mentally and emotionally.
That link is definitely true between depression and back pain.Dr. Jimenez sees the shift in spine health from the hot summer months into the cold ones and that is when the health problems peak.
Winter brings cloudier weather, and that increasesmelatonin from the brain, which causes drowsiness and less energy.
Sunlight increases serotonin, which causes feelings of happiness.
Cold, dark, winter weather can deplete energy and makes people stay indoors. This is not good because being outside, involved in activity and exercise definitely helps with joint pain.
Staying inside and not moving will worsen pain and possibly lead to severe conditions.
When the seasons begin to change, it also brings to realization the holiday season, which can cause all kinds of:
Anxiety
Stress
Tension
The holiday season can cause major stress, and the changes in weather are a reminder of that upcoming stress.
Theories
A common theory suggests that when the temperature drops it affects the viscosity of the synovial fluid in the joints.
This could be one of the reasons why people with spinal joint pain experience flare-ups during the cold shift.
Dr. Jimenez says that the structures within your:
Joints
Tendons
Ligaments
Muscles
Connective tissues
All have different densities and react differently to temperature changes.
In the cold, some connective tissues are looser than others.
So those that are tighter take longer to warm up, and if not then there is a perfect set-up for joint dysfunction.Another theory is that barometric pressure is what causes the pain. This theory supports people with joint pain that can tell when it�s about to rain.
Some rheumatologists believe the joint capsule and tissues around the joint are like a balloon.
The barometric pressure squeezes this balloon, causing the balloon to expand/inflammation that causes pain.
Moving to Warmer Climate
Mental
Emotional
Physical
Factors play into how pain affects the individual and moving to a sunny place is not necessarily the answer.
Dr. Jimenez says that warmer climates have been thought to be healthier for various conditions.
In a sunny climate, one is likely to be in the sun, being active physically/mentally,� getting plenty of vitamin D, which is good for bones and joints and makes for a good mood all around.
But moving to a warm climate isn�t always an option, so lifestyle changes can do the trick.
Clinical treatments, like infrared sauna, can bring�the sun’s benefits during dark winter days.
People with chronic pain have said they feel pain-free and relaxed after sitting in an infrared sauna.
An infrared sauna does not give off ultraviolet rays, but healthy light.
The light penetrates into the tissues, warms the body, and makes the connective tissue stretchier and looser, which moves easier and doesn’t hurt.
6 Tips
There is no need to move to a sunny climate.
Dr. Jimenez says you can minimize the weather�s effects with these tips:
Diet
Dr. Jimenez recommends reducing consumption of inflammation-inducing foods like:
Red meats
Fried foods
Sugars
Processed starches
Quitting smoking tobacco is essential for finding pain relief.
Proper Hydration
Alcoholic beverages dehydrate and can worsen depression and anxiety.
Dr. Jimenez says drinking plenty of water is important for the spine, and is often overlooked by the senior community.
Older adults don’t have an active thirst like a young person, and can, therefore, dehydrate rapidly.�
Stay Warm
Layer clothing or keep the house warm.
Keep a humidifier running with the heater to prevent respiratory problems caused by the dry heat.
Get Into The Sun Regularly
Natural light helps wards off depression, and it improves productivity in the workplace
Exercise
Physical activity plays a huge part in particularly with low back conditions, walking, which he said engages the postural muscles in the spine.
Dr. Jimenez personally sees the benefits of this: When I�m working out, I don�t feel my hip pain. And I continue because I know that I’m strengthening my body for the better, especially since I help others with their pain.
Hobbies Can Help
A hobby creates a diversion from the pain and releases endorphins, the body’s natural painkillers.
A hobby allows you to focus on something else besides the pain.
Depression & Chronic pain | El Paso, Tx
Chronic pain caused by accidents and/or aggravated conditions can often be one of the primary reasons for depression in patients. When painful symptoms induce patients to struggle with their everyday physical activities, their mental health can be tremendously influenced. Chiropractic care utilizes spinal adjustments and manual manipulations which could help restore the initial integrity of the backbone. Patients describe how chiropractic care has helped them recover their well-being and they highly recommend Dr. Alex Jimenez, doctor of chiropractic, as the non-surgical choice for chronic pain and depression, one of a variety of other common health issues.
NCBI Resources
Back pain can be debilitating, causing immobility, inflexibility, and have a significant impact on a person�s quality of life. It can make even the most mundane daily activities extremely difficult � and even excruciating. Building the muscles that make up your core (abdominals and back) can help support your spine and reduce back pain. In many cases, strengthening these muscles can assist a patient to avoid medication with its unpleasant side effects and even avoid surgery. With just a few smart moves you can significantly decrease your�back pain, increase your mobility, and take back your life.
The cold and flu season can cause havoc on a person�s body during the colder seasons. An individual can feel overly tired, congested, the body has aches and shivers, and lastly, the immune system will work overtime to help fight off the germs. When this happens, many remedies can help these symptoms when a person feels a little bit under the weather. They help the body give that extra boost to recover from cold and flu symptoms and can provide the body a chance to rest.
When anyone is starting to feel sick, an important note is to try and get as much rest as they possibly can. It can be anything like getting more sleep, scaling down on exercising, or take some time off of work to heal more quickly. In this article, here are some of the top 5 foods to help the body improve and recover from the cold and flu season, with some additional remedies to boost the immune system as well.
Contents
Soups
Soups are one of the most excellent sources of feeling better during cold and flu season. They are easily digestible and helps soothe the body by containing ample waters to keep it hydrated. Water-based soups like chicken noodle, Hippocrates soup, and vegetable soup incorporates all the essential nutrients that the body needs when it is the colder season, helping to combat the flu.
Garlic
Garlic has a wide variety of health benefits that can help the body during the cold and flu season. It can help reduce the risk of heart diseases, improve mental health, and enhance the immune system. Studies have shown that whole garlic contains a compound called alliin. When garlic is chopped, chewed, or crushed, it will help boost the disease-fighting response of white blood cells in the body when they are encountering viruses that cause the common cold or flu.
Studies also stated that garlic helps support neurodegenerative health, cardiovascular health, and compromised liver functioning from excessive alcohol use. Researchers at the Toxicology, School of Public Health, Shandong University in China, have isolated the garlic compound, DADS (diallyl disulfide), as the main compound that helps protects the body from ethanol-induced oxidative stress.
Foods That Are Rich in Vitamin C
Foods that contain vitamin C is highly essential when it comes to battling the cold or flu. Vitamin C is a powerful, potent supplement that has antioxidants and immune system boosters that protects the body from environmental factors like reducing oxidative stress, prevent and treat respiratory and systemic infections. With vitamin C-rich foods, they contain essential minerals, vitamins, and high in flavonoids that help individuals who don�t feel like eating or preferring bland foods to consume when they are sick. Initially, they can eat vitamin C rich food by either juice or soup. Here are some delicious fruits and juices that contain a high amount of vitamin C to combat the cold and flu.
Guava
Strawberries
Tomato juice
Oranges and Orange juice
Apple Cider Vinegar
Apple Cider Vinegar can provide many minerals and enzymes that can fight off pathogens that can be caused by the common cold or flu. A 2011 study has shown that the probiotics in apple cider vinegar have an immune-boosting effect that can shorten the duration of a cold when an individual drinks apple cider vinegar. Taking apple cider vinegar with a glass of water can also help the body when it is not cold and flu season. Apple cider vinegar helps inhibits bacterial growth, can support healthy blood pressure levels in the body, as well as an excellent addition to the medicine cabinet during cold and flu season.
Ginger
Ginger is a medicinal root plant that has been used for thousands of years. This root has been known to relieve motion sickness and nausea in the digestive system. Studies have shown that 70% of the immune system is found in the gut, and so it is highly essential that the digestive system in the body is working efficiently. Since ginger is made up of hundreds of compounds, some of them have potent antioxidants and can help support healthy inflammatory pathways in the body. Ginger can be found as a fresh root, dried, as an extract or oil, tinctures, capsules, and lozenges. Here are some of the foods that contain ginger to help the body fight the common cold or flu.
Ginger tea
Curry
Gingerbread
Cookies
Gingersnaps
Ginger ale
“It is highly essential to stay hydrated during the cold and flu season. Ample fluids like water, coconut water, and herbal teas are the first line of defense.
Additionally, getting a good night’s sleep helps the immune system in the body recover faster. It is also essential to avoid eating foods like processed foods, alcohol, soda, fried foods, and dairy when it is cold and flu season. Since it can cause inflammation and aggravate the immune system when the body is trying to recover from being sick.”- Dr. Alex Jimenez D.C., C.C.S.T. Insight – Dr. Alex Jimenez D.C., C.C.S.T. Insight
Conclusion
All in all, when it is cold and flu season, people can start stocking up on these five remedies and taking antibiotics to get a head start on not getting sick. When the body does get sick, taking these remedies, getting lots and lots of rest, staying hydrated, and relaxing can ensure that the body will recover faster. Since food matters to people�s health, it�s vital to give the body the nourishment it needs for the cold and flu season.
October is Chiropractic Health Month. To learn more about it, check out Governor Abbott�s proclamation on our website to get full details on this declaration.
So the mechanisms of an autoimmune disease can be either by genetics or by environmental factors that can cause an individual to have problems in their body. There are many autoimmune diseases, both common and rare, that can affect the body. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or chronic disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
References:
Biotics Education Team, Unknown. �5 Foods to Eat During the Cold & Flu Season.� Biotics Research Blog, 16 Sept. 2019, blog.bioticsresearch.com/5-foods-to-eat-during-the-cold-flu-season.
Borlinghaus, Jan, et al. �Allicin: Chemistry and Biological Properties.� Molecules (Basel, Switzerland), MDPI, 19 Aug. 2014, www.ncbi.nlm.nih.gov/pubmed/25153873.
Carr, Anitra C, and Silvia Maggini. �Vitamin C and Immune Function.� Nutrients, MDPI, 3 Nov. 2017, www.ncbi.nlm.nih.gov/pmc/articles/PMC5707683/.
Das, Arabinda, et al. �Garlic Compounds Generate Reactive Oxygen Species Leading to Activation of Stress Kinases and Cysteine Proteases for Apoptosis in Human Glioblastoma T98G and U87MG Cells.� Wiley Online Library, John Wiley & Sons, Ltd, 23 July 2007, onlinelibrary.wiley.com/doi/full/10.1002/cncr.22888.
Felman, Adam. �Antibiotics: Uses, Resistance, and Side Effects.� Medical News Today, MediLexicon International, 18 Jan. 2019, www.medicalnewstoday.com/articles/10278.php.
Newman, Tim. �Congestive Heart Failure: Causes, Symptoms, and Treatments.� Medical News Today, MediLexicon International, 3 Jan. 2018, www.medicalnewstoday.com/articles/156849.php.
Song, Fu-Young, et al. �The Activation of HO-1/Nrf-2 Contributes to the Protective Effects of Diallyl Disulfide (DADS) against Ethanol-Induced Oxidative Stress.� Biochimica Et Biophysica Acta (BBA) – General Subjects, Elsevier, 28 June 2013, www.sciencedirect.com/science/article/pii/S0304416513002882.
Surh, Y J, et al. �Chemoprotective Properties of Some Pungent Ingredients Present in Red Pepper and Ginger.� Mutation Research, U.S. National Library of Medicine, 18 June 1998, www.ncbi.nlm.nih.gov/pubmed/9675305.
Vighi, G, et al. �Allergy and the Gastrointestinal System.� Clinical and Experimental Immunology, Blackwell Science Inc, Sept. 2008, www.ncbi.nlm.nih.gov/pmc/articles/PMC2515351/.
West, Helen. �How Garlic Fights Colds and The Flu.� Healthline, 17 Mar. 2016, www.healthline.com/nutrition/garlic-fights-colds-and-flu.
Yagnik, Darshna, et al. �Antimicrobial Activity of Apple Cider Vinegar against Escherichia Coli, Staphylococcus Aureus and Candida Albicans; Downregulating Cytokine and Microbial Protein Expression.� Scientific Reports, Nature Publishing Group UK, 29 Jan. 2018, www.ncbi.nlm.nih.gov/pmc/articles/PMC5788933/.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine



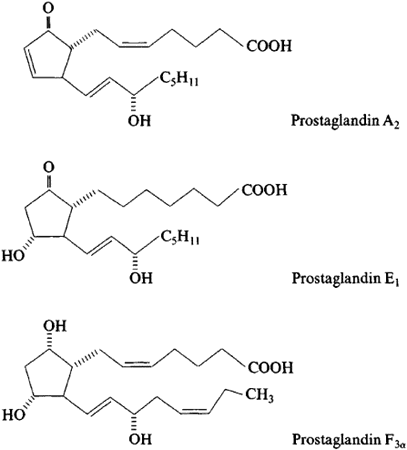




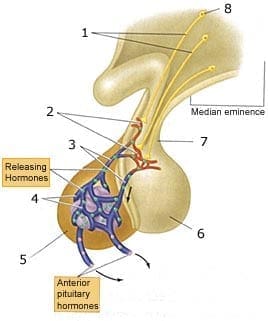
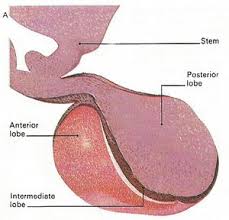
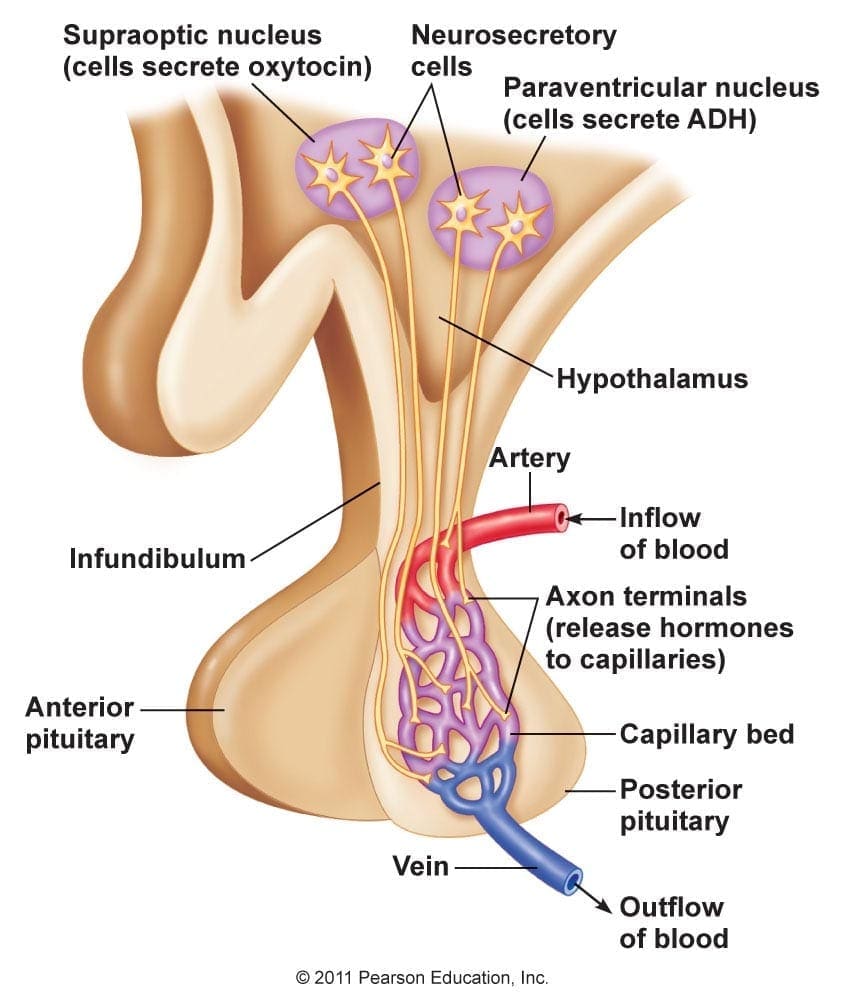

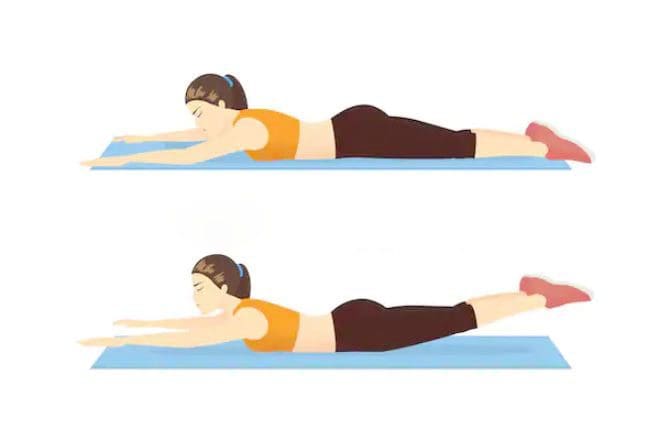




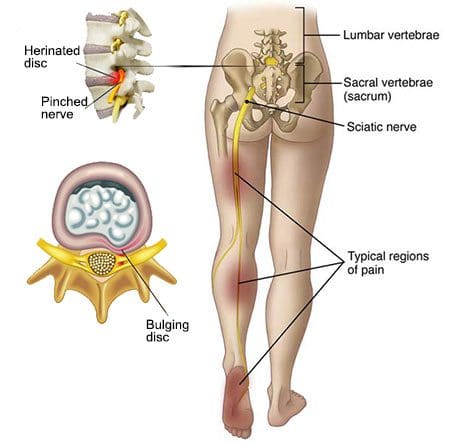 The nerves run from the lower spine under buttocks and down each hip into the legs.
Several conditions can compress these nerves at one or more spots along the way:
The nerves run from the lower spine under buttocks and down each hip into the legs.
Several conditions can compress these nerves at one or more spots along the way:


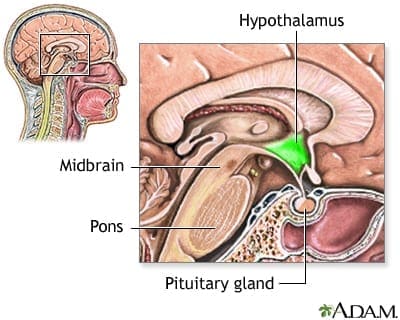
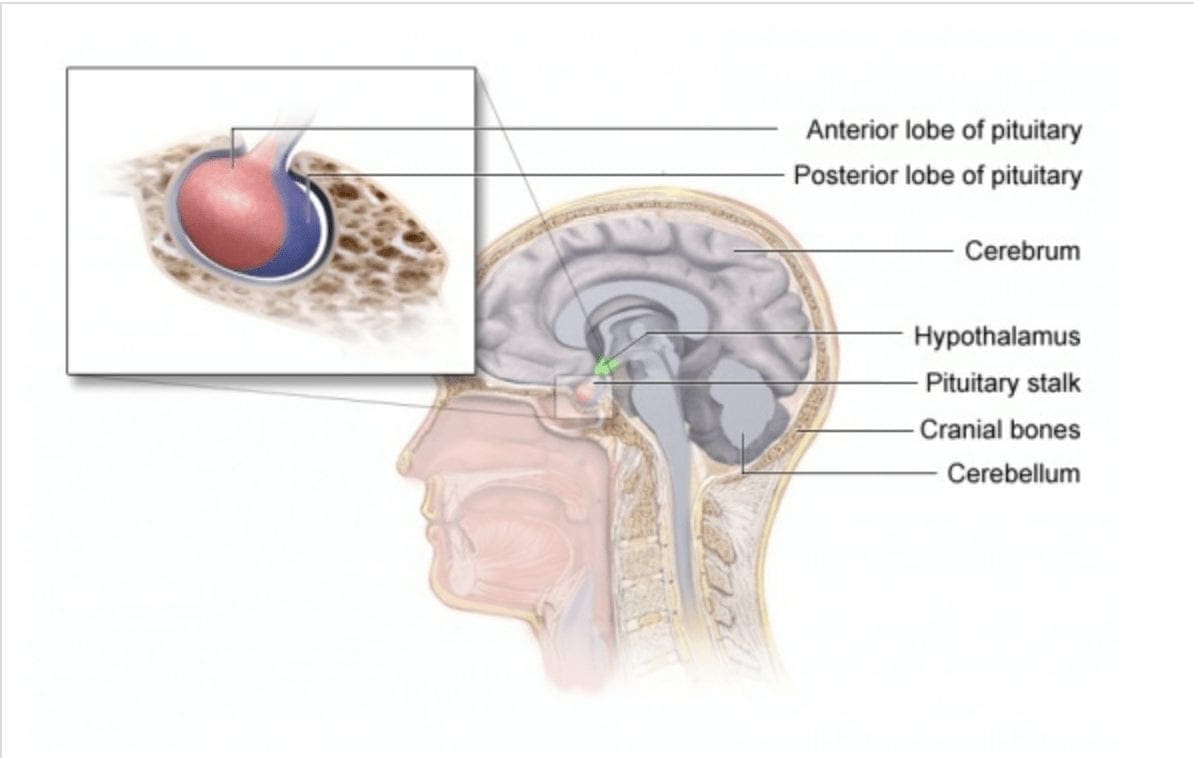
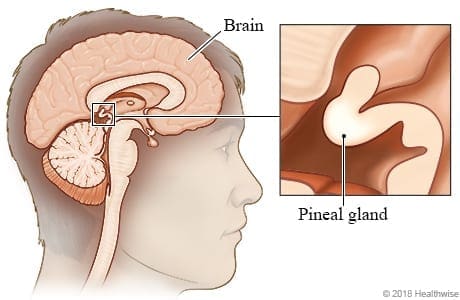
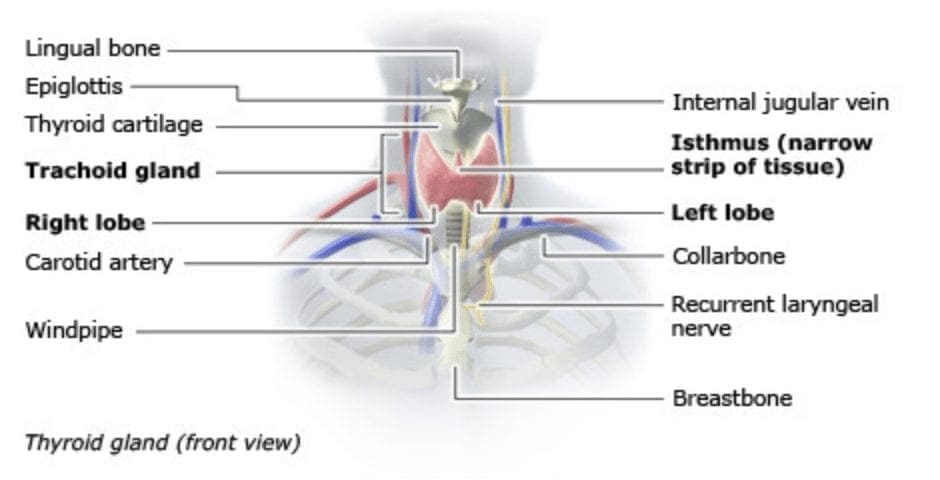
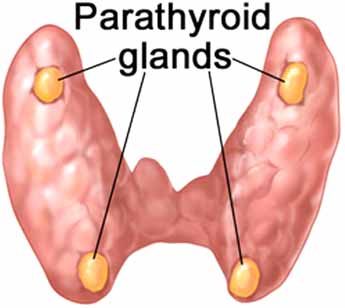
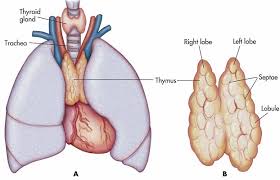
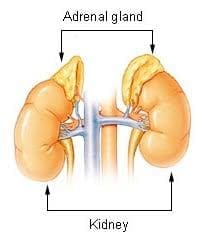
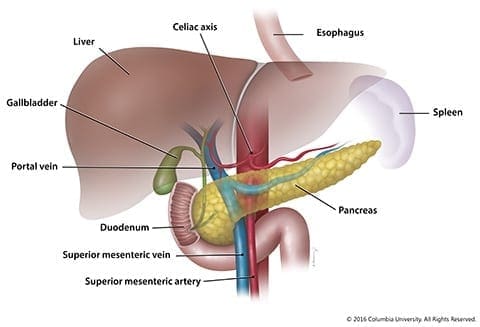








 “It is highly essential to stay hydrated during the cold and flu season. Ample fluids like water, coconut water, and herbal teas are the first line of defense.
“It is highly essential to stay hydrated during the cold and flu season. Ample fluids like water, coconut water, and herbal teas are the first line of defense.





