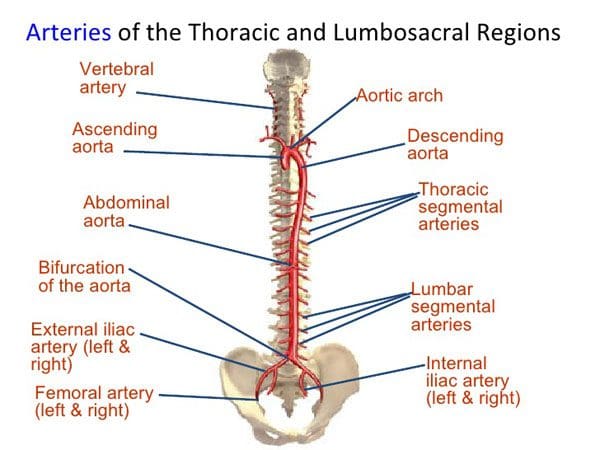
The heart never stops working. The efficiency of the heart and how it operates depends on various factors related to individual health. High blood pressure management can include chiropractic treatment for proper spinal alignment. This promotes improved nervous system function, regulation, and optimal blood flow throughout the body.
High blood pressure is also known as hypertension, often it has no symptoms, and if left untreated, it could lead to heart conditions like heart disease and stroke. Blood pressure is the force the heart exerts on the arteries each time it contracts and relaxes. It is measured with a blood pressure cuff or monitor.
Normal is around 120/80 mmHg
A blood pressure reading of 130/90 mmHg or more, is categorized as high blood pressure.
Contents
High blood pressure
Any type of heart condition can place added strain on the body and can lead to poor quality of life, disease, and be fatal. When the body’s ability to pump the proper amount of blood gets compromised the body suffers from a lack of oxygenated blood. These issues can go undiagnosed for years. Often high blood pressure does not get associated with any specific symptoms other than general poor health. When left untreated, high blood pressure can lead to issues like:
Heart attack
Stroke
Kidney disease
Dementia
Prevention and regular monitoring are crucial for staying on top of any potential heart issues.
Heart conditions
Different heart conditions can cause pain in the chest, upper back, and shoulder(s):
Angina is when the heart muscle does not get enough blood causing chest pain.
A heart attack occurs when there is reduced or complete loss of blood supply from the blockage of an artery.
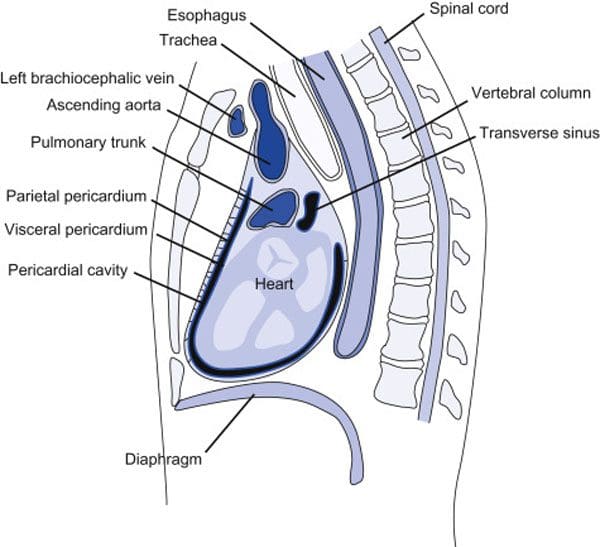
Pericarditisis the inflammation of the thin layers that surround the heart.
Heart conditions are commonly associated with chest pain but remember that chest pain is not always present or severe. Pain-related to the heart can also be felt in other areas, like the shoulder or upper back.
Risk factors
Risk factors associated with high blood pressure include:
An unhealthy diet high full of processed foods, sugar, and salt
The most common treatment for high blood pressure is medication. However, this does not address the root cause of the issue in relation to individual lifestyle and underlying imbalances of the body that include the spine.
Lifestyle
Lifestyle adjustments should be the first line of defense for managing, and reversing heart health issues. High blood pressure management includes:
Focus on nutrition
Exercise
Stress management
Chiropractic
Chiropractic is a specialized approach that focuses on identifying and addressing the root cause of musculoskeletal health issues and optimized organ function through restored impaired nerve function. Spinal misalignment can cause nerve signals to be impaired/damaged which can affect the heart and overall health.
A chiropractic physician can help reduce the strain on the body�s functions by restoring nerve function/energy/blood flow with spinal adjustments that bring the body back into proper alignment. One primary cause of high blood pressure is over-activation of the autonomic nervous system, which regulates the stress response.
When spinal alignment is achieved, there is improved regulation to prevent unnecessary spikes in stress affecting body homeostasis and organ function. Chiropractic can help an individual achieve the best possible heart health. Once the diagnosis is found, an effective customized treatment plan will be developed.
Chiropractor Near Me
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
References
Win, Ni Ni et al. �Effects of Upper and Lower Cervical Spinal Manipulative Therapy on Blood Pressure and Heart Rate Variability in Volunteers and Patients With Neck Pain: A Randomized Controlled, Cross-Over, Preliminary Study.��Journal of chiropractic medicine�vol. 14,1 (2015): 1-9. doi:10.1016/j.jcm.2014.12.005
Chronic pain and a healthy spine can require activity modification. This is so an individual can participate in activities in a way to help prevent pain from presenting. This could include:
Avoiding staying in static positions for too long
Continuous stretches throughout the day
Planning ahead when participating in physical activities that cause pain
Dietary adjustments to reduce inflammation and gain strength/flexibility
Customized exercise program
Health coaching guide
Contents
Activity Modification
Chiropractic treatment not only involves correcting spinal alignment but also continuing an individual’s health education. The objective is to treat the source, not the symptoms. The goal with activity modification is to change the habit into a positive technique. Rigorous spinal adjustments will only help to a point if the habit continues. Whether there are any underlying conditions or it is an individual’s lifestyle, variables like:
These are the primary factors when it comes to spinal health. With recurring spinal problem/s, a chiropractor needs to trace back any kinetic behavior that could have contributed to inflammation causing pain symptoms. Recognizing poor kinetic habits and teaching activity modification are core objectives of chiropractic medicine.
Identification
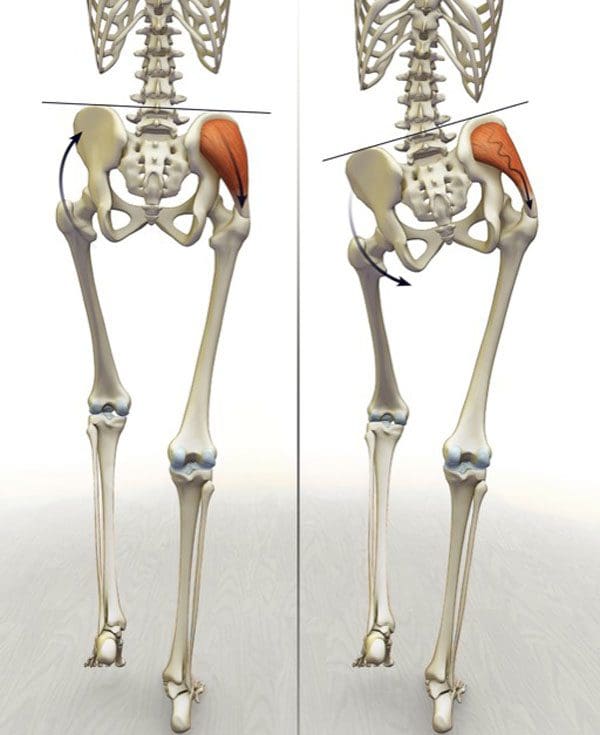
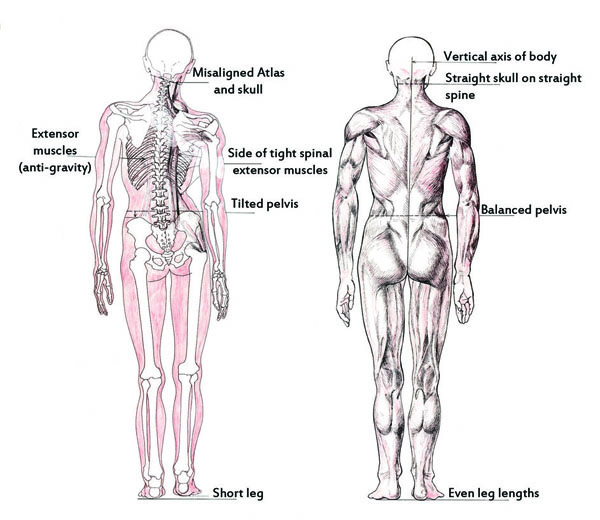
Poor habits need to be identified. Two common are forward head posture and anterior pelvic tilt. These are signs of bad habits that affect spine health. Misaligned biomechanics can be a first clue in understanding why the individual continues to experience pain.
Consistent shifting of the body to not stay in one position for too long is recommended, but when there is recurring pain this is where a chiropractor can show an individual better methods and techniques of shifting to avoid the pain. Poor posture could be traced to sitting at a disproportionate desk with no ergonomic support. And a constant forward head position on the cervical spine, nerves, shoulders, can generate enormous strain.
Modification
Precision adjustments will alleviate the effects of spinal misalignment. But modifications need to become second nature. Chiropractic modification approaches will correct poor posture and body mechanics. A chiropractor will educate an individual to be mindful of certain movements and reinforce proper positioning.
Once an individual is familiar with a healthy way of moving/shifting to restore optimal mechanics, then the individual can learn to engage in other activities with the newfound activity modification tools. This will help break the cycle of chronic spinal misalignments.
Positive Change
Corrective relief and teaching proactive wellness is the primary role of chiropractic medicine. Activity modification can be an individual’s first line of defense for changing poor habits responsible for chronic pain and recurring musculoskeletal problems. Educating individuals on how to preserve spinal adjustments and adopting long-term, healthy habits will promote overall wellness.
Chiropractic Care Crossfit Rehabilitation
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
References
Geneen, Louise J et al. �Physical activity and exercise for chronic pain in adults: an overview of Cochrane Reviews.��The Cochrane database of systematic reviews�vol. 4,4 CD011279. 24 Apr. 2017, doi:10.1002/14651858.CD011279.pub3
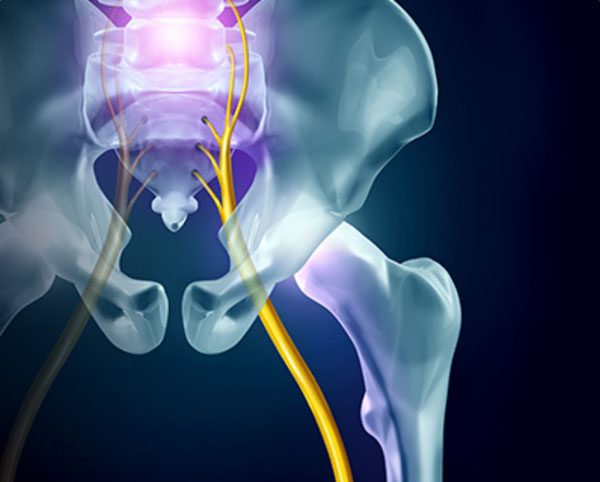
Because sciatica is an inflammatory condition, with the sciatic nerve specifically being the target, sciatica fitness and exercise is one of the first recommendations from chiropractors. Sciatica is a series of symptoms from a variety of underlying medical causes and condition/s. This could be:
Too much sitting, which most of us are doing these days
Work injuries
Automobile accident injuries
Sports injuries
Awkward movements/motions that pulled the sciatic nerve in the wrong direction
A correct diagnosis of the cause is essential to help the chiropractor formulate a customized optimal treatment plan. Individuals can experience the same symptoms across the board, however, despite the similarities, sciatica requires a careful, customized precision approach to treatment. An ideal treatment plan often requires a very specific exercise regimen and chiropractic adjustment schedule. Therefore, there is no one-size-fits-all solution.
Sciatica can be treated effectively with the right chiropractic approach with a high success rate for alleviated symptoms. Effectively treating sciatica requires direct treatment to the specific cause, rather than using techniques that only mask the pain. Example: If a herniated disc is the root cause, sciatica can be relieved by reducing the bulge of the disc, thus bringing down the irritation/inflammation and compression of the sciatic nerve.
�
Sciatica treatment/s depends on the cause
A stretching regimen for sciatica caused by a low back herniated disc will be different than stretches for treating low back spinal stenosis. Understanding how sciatica is the key to unlocking a treatment plan that will work to minimize pain and inflammation.
Exercise Can Help
Exercising and sciatica fitness will help relieve sciatic pain in various ways. These include:
Improves the range of motion, which reduces stress on the spine
Higher activity levels generate adrenaline and endorphins, to help combat the pain
Specific exercises/stretches need to be done that target the sciatic nerve and the root cause. Working with a chiropractor will bring an understanding of specifically how the body should be worked out, the intensity of the workout, and where on the body the focus should be.
For example, if the nerve is irritated from a pelvic tilt and low back compression, a chiropractor could recommend a minimal cardio workout with combined strength exercises for the hamstrings, glutes, and lower body. A strength and conditioning regimen will increase stability in the lower body, prevent pelvic tilt, and reinforce the chiropractic adjustments/alignment.
Chiropractic Benefits
However, sciatica fitness and exercise on its own is not the complete solution for dealing with chronic sciatic pain. Chiropractic adjustments along with chiropractic prevention are necessary to restore the stability and integrity of the spine. When used in combination with exercise, the re-alignment and corrections can take effect sooner and maintain optimal spinal health. When individuals condition and strengthen their body, The musculature that supports the spine gets massive reinforcement. This minimizes the chances of a reoccurring pelvic tilt from weakened core muscles. The long-term effects of sciatica fitness/exercise and chiropractic spinal/hip manipulation work together to form a perfect combination.
�
Sciatica Fitness
For truly long-term effects of pain relief and a better quality of life, a chiropractic treatment plan is highly recommended. Specific targeted adjustments and re-alignment with a sciatica fitness program will promote optimal health and wellness.
�
Whole Body Wellness Foot Orthotics
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
References
Beavers, Kristen M et al. �Effect of exercise training on chronic inflammation.��Clinica chimica acta; international journal of clinical chemistry�vol. 411,11-12 (2010): 785-93. doi:10.1016/j.cca.2010.02.069
Coulombe, Brian J et al. �Core Stability Exercise Versus General Exercise for Chronic Low Back Pain.��Journal of athletic training�vol. 52,1 (2017): 71-72. doi:10.4085/1062-6050-51.11.16
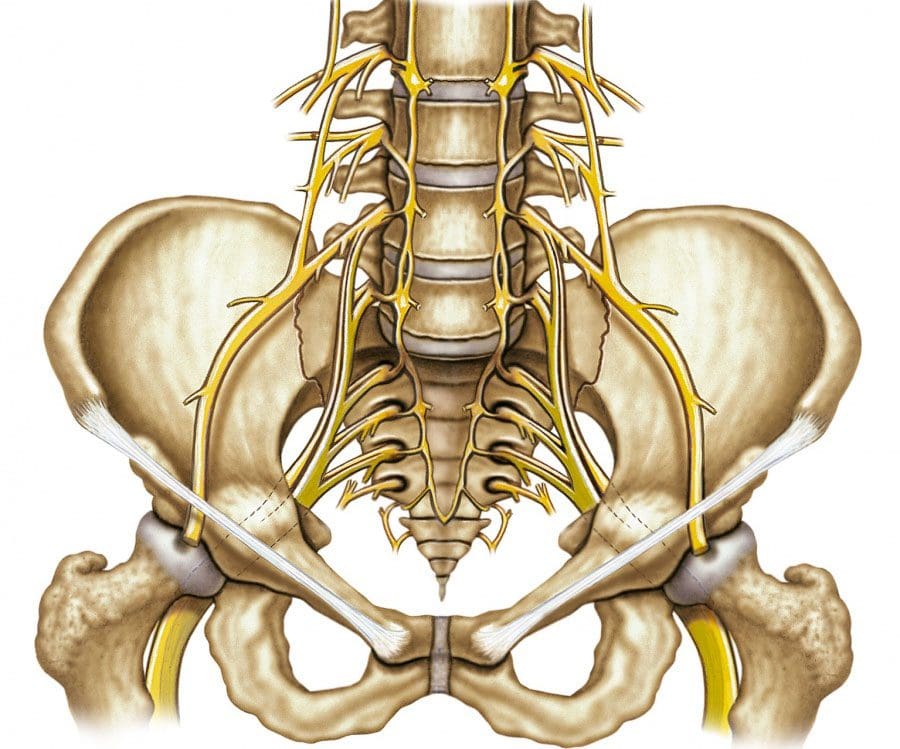
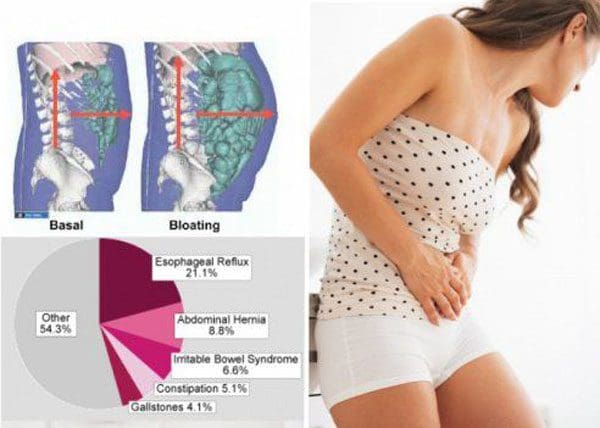
Stomach ache, acid reflux, gas, and other symptoms of gastric distress can be linked to spinal issues and misalignment. The spinal cord sends nerve signals to all parts of the body, specifically those affecting digestion functions. The lumbar spine/lower back includes the sacrum which is vital in terms of nerve function.
Various spinal cord issues could cause problems with the rest of the body. These include:
Disc compression
Herniated discs
Strained ligaments
Misalignments/problems in the lower back can result in gastric symptoms like:
Constipation
Diarrhea
Bloating
Gas
Bladder malfunction
This is because this area of the spine includes sympathetic and parasympathetic nerves that are connected to the digestive system. Any problem with these systems can result in miscommunicated signals to the rest of the body. The wide-range effects that compressed nerves can have on the body, as well as, how the spine is affected by the obstruction of these nerves, can be detrimental.
Chiropractic adjustments can help alleviate and release the gastric distress are able to correlate their spine�s role in gut health. This along with an education on the central nervous system. A chiropractic approach can help as a long-term solution to gastric distress.
Contents
The Nerves
Every organ in the body functions by sending and receiving electrical impulses, transmitted through the nerves. These impulses direct the function of organs. If blocked or the signals are improperly/partially sent/received, various health issues can begin to present. For the gut, proper nerve signal transmission at full capacity is crucial. The stomach needs to be able to properly digest food while absorbing nutrients and preparing for waste removal. This is where gastric distress conditions begin like:
Irritable bowel syndrome – IBS
Gastroesophageal reflux disease – GERD
Abdominal pain syndrome – APS
Nerve conditions worsen with time if the health and function of the affected nerves are not restored. This could mean severe chronic symptoms and the possibility of permanent nerve damage.
Nerve Blockage
Messed up nerve signals are usually pinched, blocked, or displaced. Most nerve bundles exit through the spine and are usually where a chiropractic exam will start. Through palpitation of the spine along with diagnostic imaging, a chiropractor can track down exactly where the nerve blockage/s are taking place.
The lower back and upper back are common areas to examine. This is because a majority of abdominal organ nerves branch out from these spinal segments. If spinal subluxations are present, more than likely they are affecting the function of these organs. Chiropractic will adjust the spine and reset/realign the spine to its proper form, allowing for proper blood circulation. Compressed nerves can also cause inflammation that could require more complex treatment.
Listening to the Body
If the gut is presenting with aches, and bloating after every meal, it could be indicating that something is wrong or off. Individuals cannot feel blocked nerve signals, but the gut can. Listen to it when it is alerting an issue or problem. We want to educate our patients on gut and spinal health. Chronic gastric distress can be corrected with chiropractic.
Chiropractic Pain Relief
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
References
Spiegel, Brennan M R et al. �Understanding gastrointestinal distress: a framework for clinical practice.��The American journal of gastroenterology�vol. 106,3 (2011): 380-5. doi:10.1038/ajg.2010.383
Kehl, Amy S et al. �Relationship between the gut and the spine: a pilot study of first-degree relatives of patients with ankylosing spondylitis.��RMD open�vol. 3,2 e000437. 16 Aug. 2017, doi:10.1136/rmdopen-2017-000437
The number of individuals experiencing hip along with back pain is increasing and could benefit from chiropractic hip realignment. Chiropractic treatment is the recommended first-line option for hip pain and other issues related to misaligned hips. It is non-invasive and allows the body to heal naturally.
Contents
Shifted Hips
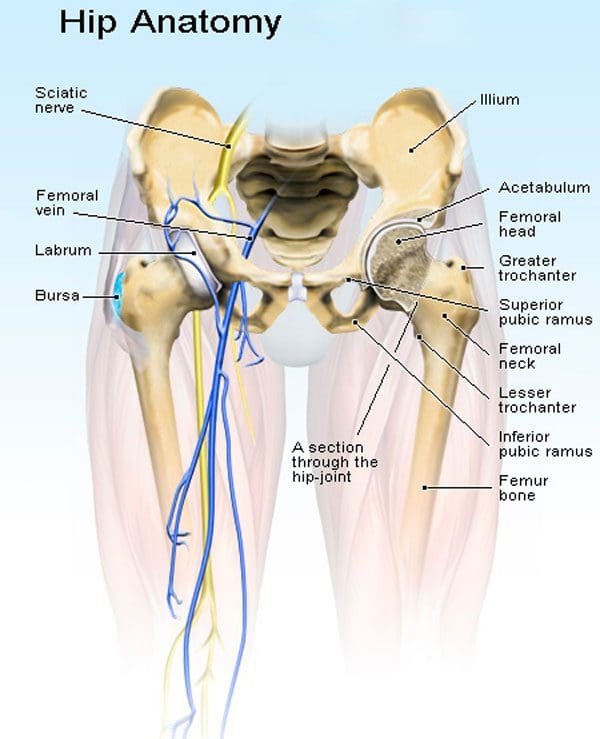
Hips that fall out of proper alignment have the potential to cause a variety of health issues in the body. The hips support a great deal of the body�s weight and facilitate substantial movement. The hips need to be properly balanced to allow for optimal mobility without compensation from the lower back and legs. A shift in the hips can occur from:
Shifted hips can cause pain in the low back, hips, and legs. This occurs from an altered gait and range of motion in this region. However, the hip joints, pelvic bones, muscles, and ligaments can all contribute to hip shifting and pain. Hip issues can also cause sciatica.
Hip Function
The hips do not receive as much attention until aches and pain start to present. Our hips are involved in nearly everything we do, providing numerous functions. It is no wonder they can cause tremendous pain when they’re out of alignment. The hips:
Keep the body upright
Bear the body’s weight
Allow for smooth:
Walking
Kicking
Running
Jumping
Sitting
Hip Adjustment
How to know if a hip adjustment is necessary? If there is any type of discomfort, soreness, and especially pain, achiropractor is the best medical professional to perform an examination and recommend if an adjustment is necessary or could just need ice/heat and rest.
However, if the source is being caused by another condition or injury the chiropractor will recommend the proper health care professional/specialist that can treat the issue. Hip pain can also be brought on from a different part of the body having its own issues. One of the most common types of hip pain is actually from a hernia or sciatica.
Chiropractic Hip Realignment
Chiropractic techniques focus on rebalancing the body, especially when realigning the hips. Manual manipulation and mobilization treatment techniques can improve flexibility, strength, and positioning to promote optimal balance and hip realignment.
A combination of adjustment techniques can be performed on the hip and spinal joints. Massage treatment can be incorporated into the treatment plan to loosen tight muscles, as the hips are realigned and are able to move freely. The holistic nature of chiropractic doesn’t just treat just the symptoms but identifies and treats the root cause. If the pain continues or worsens then the possibility for hip surgery could be recommended.
Complex Treatment
Working on imbalanced hips is not as straightforward as adjusting the low back. This is because there are a variety of arteries, nerves, joints, muscles, and other tissue structures that need to be considered during hip realignment. A chiropractor will use a careful combination of techniques when treating an imbalanced hip due to the complex nature of the area. In addition to chiropractic adjustments, chiropractors will suggest ways to improve hip mobility at home. This includes:
Stretches
Posture work
Exercises
These will help prevent the hips from shifting out of alignment. Treating pain at its source is what chiropractors do. Chiropractic hip realignment along with the realignment of the spine will allow the body to move freely, maintain balance and strength.
Hip Labral Tear Rehabilitation
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
References
Okuzu, Yaichiro et al. �Hip-Spine Syndrome: Acetabular Anteversion Angle Is Associated with Anterior Pelvic Tilt and Lumbar Hyperlordosis in Patients with Acetabular Dysplasia: A Retrospective Study.��JB & JS open access�vol. 4,1 e0025. 29 Jan. 2019, doi:10.2106/JBJS.OA.18.00025
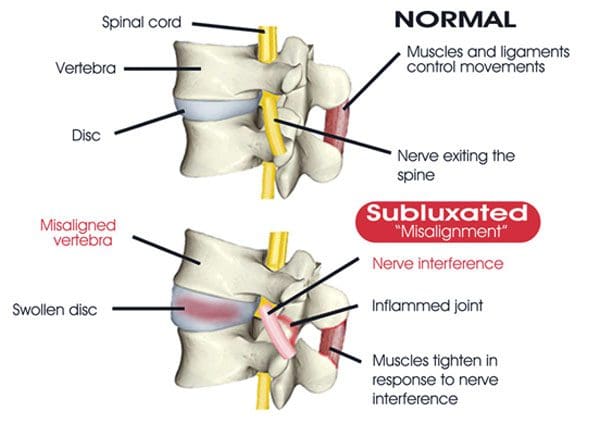
Most individuals go about their lives without thinking about poor posture and spinal misalignment, not to mention the spinal health problems/conditions that are associated with misaligned vertebrae. Most spinal misalignments come on as a result of:
Poor posture habits
Unhealthy diet
Destructive lifestyle choices
Sudden misalignments caused by accident/s or injury/s
Sudden misalignments can be associated with a direct cause that an individual can recognize increased symptoms and injury. It�s the long-term spinal misalignment that can become dangerous if left untreated and out of alignment. This is when it is time to see a chiropractor for an immediate spinal realignment.
Contents
Body Posture Mechanics
Poor posture along with poor body mechanics contributes to spinal misalignment. This creates unnecessary and consistent pressure on the:
Muscles
Ligaments
Joints
Discs
The pressure also causes a stretching of the nerves in the neck and low back. These nerves are responsible for transmitting, muscle expansion/contraction signals, vital information, and energy to the body’s organs. Any nerve interference will diminish the energy/blood flow to the limbs and organs. This can lead to disease and other major health complications like:
Chronic pain
Decreased mobility
Joint stiffness
Slouched posture
Reduced range of motion
Discomfort when sitting, standing, and lying down
Permanent joint/bone deformity/s
Broken bones, specifically in the spine
Most individuals do not recognize the gradual or long-term health problems linked to the spinal misalignment. Often the signs and symptoms are very subtle, so do not raise a cause for concern. The most direct symptoms of poor posture and spinal misalignment include:
Sore/stiff neck or back
Low energy
Tiredness/fatigue
Headaches
Back muscle spasms
Joint pain
Numbness
Tingling
Altered sensations
In addition to the symptoms, individuals should realize that underlying health conditions could also be linked to poor posture and spinal misalignment. If any of these symptoms are presenting see a chiropractor for an examination and proper diagnosis. These symptoms can be masked with pain killers, mattresses, or caffeinated drinks. However, these will not realign the spine to its proper form.
Chiropractic Lower Back Treatment
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
References
Veintemillas Ar�iz, M T et al. �Changes in spinal alignment.� �Alteraciones de la alineaci�n vertebral.��Radiologia�vol. 58 Suppl 1 (2016): 115-27. doi:10.1016/j.rx.2016.01.007
Back or disc pain is becoming increasingly common for individuals of all ages. The spinal discs are prone to injury because of the extreme amount of pressure/stress placed on the lower back and neck. Fortunately, most cases of back pain heal on their own, while others can cause long-term chronic pain that can be difficult to manage, without proper treatment.
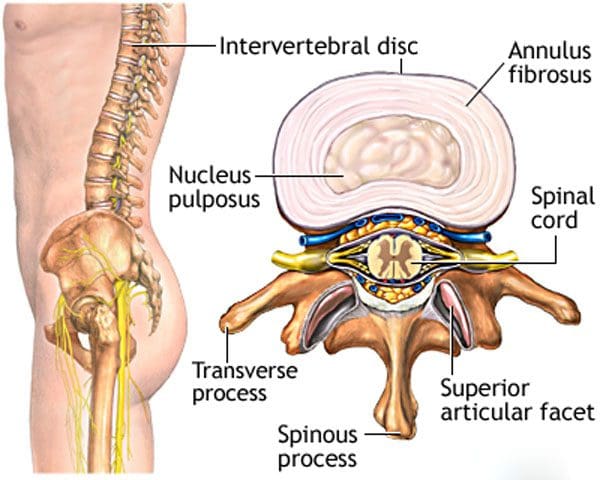
Different types of pain can be caused by problems with the spinal discs. The spinal discs are elastic sections of the spine that sit between the vertebrae. They are made up of materials called annulus fibrosus on the outside and a gel-like material called nucleus pulposus on the inside.
These discs are flexible, which allows for a range of motion to the spine and body shock absorption to increase comfort when in motion. When an individual visits a chiropractor, the practitioner will not know the exact cause of the pain, but only that it hurts around a certain area. Our spinal experts will help individuals understand the different types of ailments or conditions that could be affecting the spine. Then a customized treatment plan can be developed.
Contents
Disc problems
Spinal disc pain has two major sources of pain related to spinal discs: They are disc degeneration and nerve root pain. They are most common in the neck and the lower back. Individuals need to be informed of the difference to understand what is happening with the spine and potential treatment options to alleviate the pain and heal the problem.
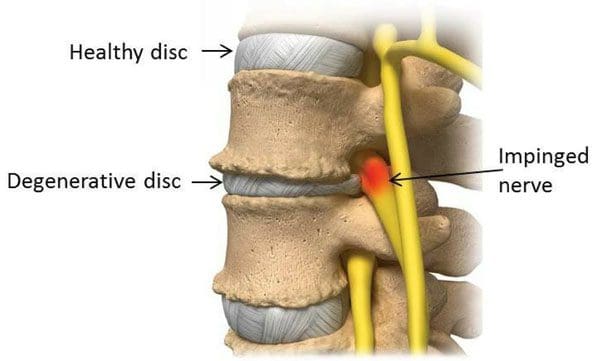
Degenerative disc disease
Degenerative disc disease is when the spinal discs begin to dry out and deteriorate. The discs start to shrink and can tear, which leaves that segment with little or no cushioning. This can cause pain, as well as inflammation of the surrounding muscles and joints. Disc degeneration usually presents with low levels of consistent pain and occasional severe flare-ups.
A chiropractor can utilize spinal manipulation to restore alignment, function, and mobility of the affected joint. Massages stretches and exercises will help alleviate the tension in the surrounding muscles along with strengthening them for better support.
Nerve root pain
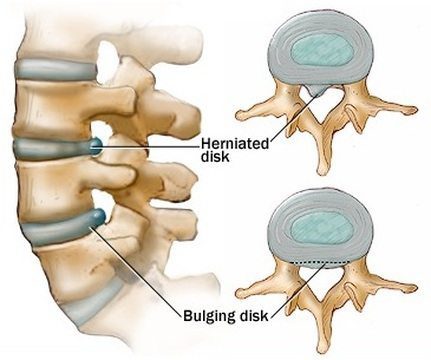
Nerve root pain does not take place within the disc but is usually caused by a bulging or herniated disc. This condition can be called a slipped disc or pinched nerve, affect the nerves that are in close proximity to the neck and lower vertebrae.
The pain can lead to numbness, tingling, and weakness along the path of the nerve, and radiate out to the arms and legs. A bulging disc is when the spinal disc progressively protrudes through a narrow opening.
This can irritate any nearby nerve roots causing inflammation and pain. If the disc herniates or breaks through then the outer protective material tears, letting the cushion/gel leak out and come in contact with the nerve root/s, which could also cause pinching and inflammation. Treatment for a bulging or herniated disc includes:
Spinal manipulation
Corrective exercises
Physical therapy
Massage
Diet adjustments
These treatments can help realign the disc/s, moving them away from any nerves, and minimizing inflammation.
Proper Identification and Diagnosis
Spinal disc problems can be similar in their pain and symptoms. For example, degenerative disc disease can weaken the spinal discs to such a degree that nerve root pain follows creating a dual combination of pain. The conditions require various approaches and treatment methods often done in combination. However, they require a proper diagnosis to create a proper and custom treatment program for every individual. This will ensure the root cause of the disc pain is properly identified and handled. Call us to learn more.
Skateboarding Injury Treatment
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
References
Browning, J E. �Chiropractic distractive decompression in the treatment of pelvic pain and organic dysfunction in patients with evidence of lower sacral nerve root compression.��Journal of manipulative and physiological therapeutics�vol. 11,5 (1988): 426-32.
Chiropractic spinal mobilization techniques involve the slow and steady movements of the spine’s joints reestablishing their range of motion. Because it is a slower treatment style the techniques are done with the hands. However, a chiropractor can use various instruments/tools as well.
Spinal mobilization treatment has the same focus as spinal manipulation. To get the body back to optimal health and allow the body to heal itself naturally. However, there can be a variety of reasons for utilizing spinal stabilization, with treatment depending on the patient’s needs, if there are underlying conditions, or previous injury/s, and individual preference.
Some prefer mobilization because it is gentler and does not generate the pops or cracking sounds. And the chiropractor’s style/specialization comes into play. Some work in the firm manipulation high-velocity style, while others utilize the softer mobilization style and others work in combination.
This adjustment re-alignment utilizes the necessary force to release the joint out of its restricted motion to improve mobility and reduce pain. There are various types of high-velocity low-amplitude manipulation approaches. These are the more common manipulation techniques:
Diversified Technique
This high-velocity low-amplitude technique is the one that is commonly associated with chiropractic manual adjustments. The chiropractor applies a short – low-amplitude, quick high-velocity thrust of the restricted joints. This is done one at a time with the objective to restore the normal range of motion. The patient is positioned in various positions to optimize the adjustment/alignment.
Gonstead Adjustment
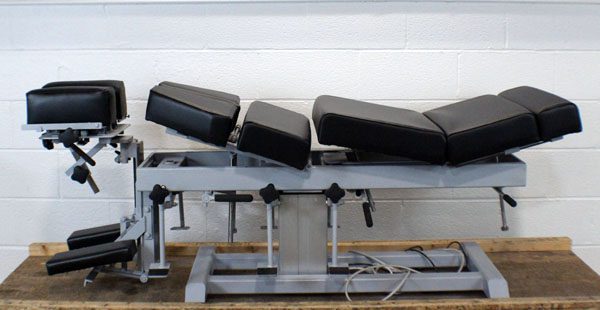
The Gonstead technique is another high-velocity low amplitude adjustment. It is similar to the diversified technique. The difference is the evaluation performed to specifically locate the painful joint and positioning of the body as the treatment is performed. Chiropractic or physical therapy chairs and tables can be used to position the patient for optimal treatment, like a cervical chair or a chest-knee table.
Thompson Terminal Point Drop Technique
Here specialized treatment tables with sections that drop down during a high-velocity low-amplitude thrust. The idea is that as the table drops the piece dropped allows for easier movement of the joint. A cracking sound can sometimes be heard. It depends on the patient and their condition. This type of manipulation can also be done in a gentle fashion making it a form of spinal mobilization.
Spinal mobilization
Slow steady motion/movements are performed to mobilize the joint. Spinal mobilization can be recommended for certain individuals for different reasons like:
Individual preference for spinal mobilization over spinal manipulation
Individuals with a sensitive nervous system can benefit from the gentle technique. This can keep the body from experiencing a negative reaction that can cause muscle spasms or other issues.
Individuals with certain conditions could be given a recommendation for spinal mobilization. This could be:
Individuals in the acute stage of their condition and experiencing severe pain
Obesity can be a factor as the positioning and the manipulation procedures can be a challenge for the provider and the patient requiring a low force approach.
Mobilization Approaches
The more common spinal mobilization approaches include:
Activator Technique
The Activator is a hand-held, spring-loaded tool that generates a low-force impulse. A patient lies face down on the adjustment table, while the chiropractor:
Examines leg length
Performs muscle testing
Adjusts the spine and/or extremity joints
Cox Flexion-Distraction Technique
Here a gentle adjustment is designed to adjust the vertebrae by gently stretching the lower spine. This is usually performed in a series of repetitive slow movements like a steady rocking motion.
Toggle Drop
Here gravity is utilized to apply the adjustment. The chiropractors’ hands are crossed and on top of each other. Then the chiropractor presses down quickly and firmly on the area of the spine while a section of the table drops. The table sections can be raised and dropped according to the localization of the spinal adjustment.
McKenzie Technique
This technique incorporates active patient involvement, empowerment, and self-care as part of the treatment.
Spinal Release
The chiropractor separates the misaligned vertebrae by applying gentle pressure using the fingertips, with the objective to restore the spine back to a natural position.
Sacro-Occipital Technique – SOT
This technique utilizes wedges/blocks under the pelvis. This allows gravity with added low-force to assist the chiropractor to realign the pelvis.
Sciatica Alleviation
All of these techniques can be utilized by a chiropractor for sciatic nerve pain alleviation or can discover other conditions that could be mimicking sciatica.
Nerve mobilization techniques have been recently used as a method to adjust radiating pain related to disc disease, and in particular, mobilization techniques for the sciatic nerves improve mobility of the sciatic nerves, decrease mechanosensitivity of the nervous system, and heighten compliance of nerve tissues, relieving low back pain. Jeong, Ui-Cheol et al. �The effects of self-mobilization techniques for the sciatic nerves on physical functions and health of low back pain patients with lower limb radiating pain.��Journal of physical therapy science�vol. 28,1 (2016): 46-50. doi:10.1589/jpts.28.46
Sciatica Rehabilitation Causes and Symptoms
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
Shoulder and arm pain can be debilitating, especially when there is no obvious cause or injury that needs to be treated. A rare condition known as brachial neuritiscan cause spasms along with pain down the arm, followed by numbness, tingling, and weakness. If not diagnosed and treated early, the symptoms can worsen with time. The pain experienced can be described as sharp, searing, and shooting. Brachial neuritis can be intense and disabling when it presents for hours and even days.
Utilizing a chiropractic approach, shoulder and spinal adjustments can provide relief and a faster healing/recovery from the inflammatory condition. Individuals experiencing shoulder, arm, and possible hand pain should consult with a chiropractor about a potential home and clinic treatment plan to improve their condition.
Contents
Medical History and Examination
The process of diagnosing brachial neuritis involves an individual’s medical history and physical exam. More complicated cases could require imaging studies and electrodiagnostic tests. The first steps in diagnosing the cause of shoulder and/or arm pain include:
Medical history
Information will be collected on an individual’s:
Medical history
Family history
Underlying conditions
Recent illnesses or injuries
Lifestyle habits
How and when symptoms began
Current symptoms
Physical examination
A chiropractor will palpate or inspect by feeling the neck, shoulder, and arm for irregularities. Then they will examine the range of motion, strength, and reflexes. If the individual’s history and physical exam suggest that the cause could be brachial neuritis or other condition involving the nerves, imaging studies, and diagnostic tests could be required to evaluate further.
Symptoms of Brachial Neuritis
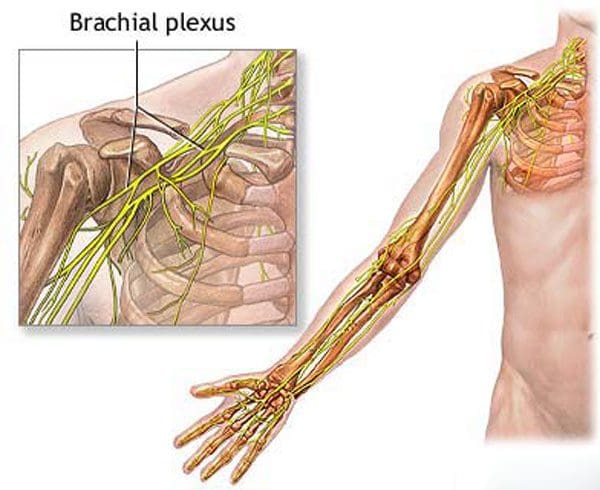
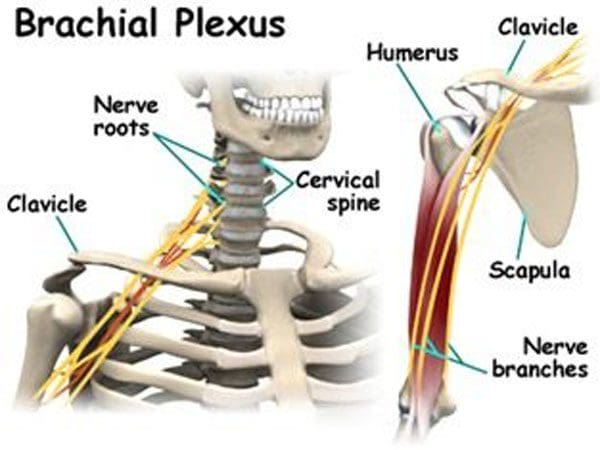
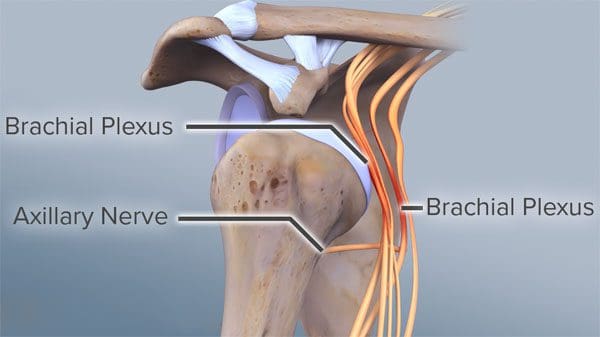
The condition is also known as Parsonage-Turner Syndrome. It affects the brachial plexus, a set of nerves that run from the neck and upper back to the shoulders. The condition usually affects only one side of the body and presents randomly.
What happens is the nerves become inflamed.
Inflammation can be triggered through an autoimmune response. This is often the result of an infection, surgical procedure, or other internal stressors. The inflammation can lead to severe debilitating shoulder pain over a few days.
This also leads to long-term numbness, weakness in the shoulder and arm.
The pain becomes worse with movement.
Typically, the pain goes away on its own within a few days.
Numbness, weakness, or tingling in the shoulder or arm continues.
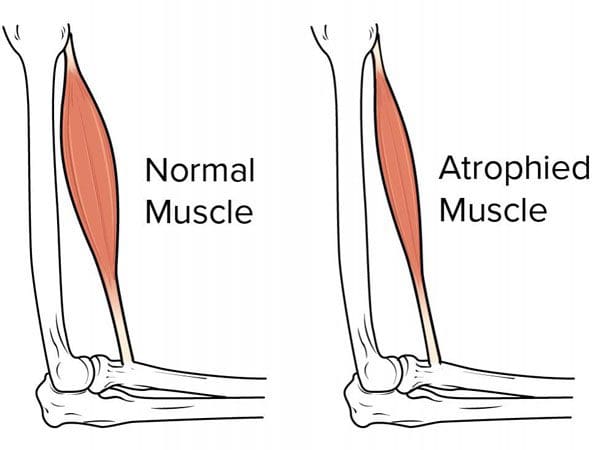
Over time the symptoms begin to worsen and, if left untreated, could lead to muscular atrophy of the arm.
The pain and weakness can make it difficult to move the arm, leading to decreased strength.
Symptoms can last up to a year or more.
This is why individuals have to find ways to strengthen their shoulder/arm despite the condition.
Chiropractic Relief
Treatment requires a pain management program until the pain subsides. Once the pain is manageable, chiropractic, physical therapy, exercises, and stretches could improve mobility and strength. Chiropractic can provide relief and tools necessary to prevent the worsening of symptoms. Chiropractic helps to:
Reduces pain
Improves mobility
Restores strength
Chiropractic manipulation will ensure that the nerves near the brachial plexus do not become compressed, but if they are, then chiropractic can be utilized to decompress/release them. In addition, trigger point release and massage can help alleviate the tension in the surrounding tissues of the arm and shoulder.
A chiropractor will educate the individuals on effective pain management techniques for home, including ice/heat therapy and stretching exercises. These techniques will help restore the proper alignment and flow of the spinal vertebrae, nerves, and muscle tissues, allowing the body to heal quickly, naturally, and more effectively.
Chiropractic Shoulder Pain Treatment
References
Feinberg, Joseph H, and Jeffrey Radecki. Parsonage-turner syndrome. HSS journal: the musculoskeletal journal of Hospital for Special Surgery vol. 6,2 (2010): 199-205. doi:10.1007/s11420-010-9176-x
Seasonal Affective Disorder is a form of depression that has to do with the changing of the seasons, specifically when fall begins. It affects around 10 million Americans during the fall and winter seasons. Back pain can be a symptom of the disorder. For most individuals, the condition follows a pattern:
These are typical symptoms for many dealing with the condition. The individual can experience aches and pains throughout the body, but especially the back. Recent studies have shown how various forms of depression, like Seasonal Affective Disorder, can present with pain, specifically back/spinal pain. Many individuals play it off as the blues, but research has found, depression can have a much more significant impact on an individual’s quality of life. The exact cause is still unknown. But research is finding a connection related to the level of sunlight an individual receives throughout the day.
Research has shown there could be a biochemical imbalance in the brain when there is less daylight during fall and winter. As the seasons change from summer to fall individuals can experience a shift in circadian rhythms that can cause them to disrupt their regular daily routine. However, Seasonal Affective Disorder is more common for individuals living where the daylight lessens and has been shown to affect women more than men and young adults.
Contents
Depression and Back Pain Connection
Depression can present with pain symptoms and the pain can enhance the depression. Headaches, Body aches, and especially backaches are common symptoms of depression. Research has shown that individuals with severe depression can actually feel a more intense level of pain.
Physical symptomslike back pain or headaches can be the only or the beginning symptom/s of seasonal affective depression. As research continues to grow as to how the nervous system interacts with the body, pain symptoms have been found to be connected to biological mechanisms connected with stress, anxiety, and depression.
Living a sedentary lifestyle, with little or no physical activity and regular exercise can be another cause for Seasonal Affective Disorder. Depression itself can cause fatigue that restrains individuals from exercising and working the core muscles for optimal spinal strength and health.
This added stress on the spine’s discs, joints, and ligaments, makes the body more susceptible to low back pain, muscle strains, illness, and injuries. Pain can wear an individual down impacting mood and overall health.
Symptoms
The difference between Seasonal Affective Disorder and chronic depression is that Seasonal Affective Disorder is limited to the same time of the year during the time of less light, and winter months. Symptoms of Seasonal Affective Disorder can be the same as those associated with depression. They are:
Feeling Low/Depressed
Weight gain
Increased appetite
Craving sugar and carbohydrates
Sleeping all-day
Consistent drowsiness
Hopelessness
Loss of interest in enjoyed activities
Symptoms can also be related to low levels of Vitamin D, which is associated with anxiety and depression for individuals with fibromyalgia. Seasonal Affective Disorder can be related to chronic pain conditions the way depression can. Some individuals with chronic fatigue syndrome can also present with symptoms of Seasonal Affective Disorder.
Treatment
Diagnosis for Seasonal Affective Disorder requires an individual to experience at least two years of symptoms that become worse at a specific time of the year. And the depressive episodes have to significantly be worse than the non-seasonal episodes of depression. There are four types of treatments, that can be used individually or in combination. They are:
Cognitive-behavioral therapy/CBT is a form of psychotherapy that is effective for the disorder, as well as other conditions. It relies on techniques that identify negative thoughts and work on ways to not dwell on the negative and focus more on positive things and thoughts.
Lightbox Therapy
Diminished sunlight when fall and winter arrive can be replaced with regular exposure to a bright, artificial lightbox. Individuals sit or stand in front of the lightbox when they get up on a daily basis. This is done when fall begins and goes on until spring. The lightbox filters out ultraviolet rays and requires around 20 to 60 minutes of exposure to 10,000 lux of cool-white fluorescent light.
Vitamin D
Low levels of vitamin D were found in individuals with Seasonal Affective Disorder. Talk to a doctor about the proper level of vitamin D that should be taken through supplements.
The Pain and Backaches
Understanding how pain and depression are interconnected treating both conditions as part of an integrative treatment plan can include:
A light aerobic exercise program that stimulates serotonin levels and releases endorphins to relieve depression and pain.
Low-dose antidepressants can reduce depression symptoms and back pain. They work to inhibit the reuptake of neurotransmitters like serotonin and norepinephrine that is associated with a person�s mood and the way they perceive pain.
What Works
Everyone is unique, which means that different treatment plans and combinations of treatment plans may have to be tried out before finding the optimal one. A significant factor is not settling with the pain and just accepting it. Healing can be a unique and complex experience. The objective is for the individual and doctor to work collaboratively.
Depression and Chronic Pain
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
References
Robertson, David et al. �Associations between low back pain and depression and somatization in a Canadian emerging adult population.��The Journal of the Canadian Chiropractic Association�vol. 61,2 (2017): 96-105.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine