Foot problems can affect the overall well-being of the human body. Many health issues which affect the foot can result in poor posture, low back pain, and sciatica. These imbalances can ultimately result in a variety of other health issues. Custom-made foot orthotics can help promote and support overall well-being by relieving foot problems.
The following video discusses how many health issues which affect the foot can cause a variety of foot problems, including poor posture, low back pain, and sciatica. Dr. Alex Jimenez is the non-surgical choice for foot problems and other health issues. Dr. Alex Jimenez can help promote and support overall well-being with the use of custom-made foot orthotics and other treatments approaches.
Improve Whole *BODY WELLNESS* with Foot Orthotics | El Paso, TX (2019)
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
Many chiropractors encourage foot orthotics to help treat various problems ranging from back and joint pain, foot discomfort, sciatica, etc.
Custom orthotics are made by scanning and assessing your feet, that lets your doctor/chiropractor know how you distribute your body weight, and viola, a one-of-a-kind solution is created especially for you.
Reasons why orthotics can help your body:
Orthotics support all moving parts in your body
Properly stabilized feet means the rest of your body moves with ease and harmony.
If you are someone who slumps a lot or has one side more dominant over another, orthotics help correct posture and movements.
Athletes have come to favor orthotics because of the positive influence in the way the body moves.
Orthotics distribute body weight evenly
Orthotics are frequently used to treat and relieve:
If you are a person who spends a lot of time on your feet, then orthotics can make long periods on your feet more manageable.
Even distribution means you will not feel aches and pains at the end of the day.
Orthotics can help you move faster & easier
Custom orthotics are designed for each person�s unique foot to provide optimal support.
Someone who is flat-footed in one arch, may not be in another, a custom orthotic will provides specific support.
People who have jobs requiring them to spend a lot of time standing like teachers and police officers find that wearing custom orthotics helps them stay on their feet with greater ease.
Orthotics protects you from future injuries
Wearing orthotics help prevent your body from future injuries for several of the reasons mentioned above like evenly distributing your body weight, but also by supporting the various areas of your feet.
Orthotics can help relieve and prevent issues such as plantar fasciitis, heel spurs, and bursitis, as well as protecting you from injuries like twisted ankles, back strains, and unnecessary hip and knee pain.
Orthotics support your body’s foundation the feet!
It�s essential to ensure the foundation remains in tip-top shape.
As people age, our feet change.
Arthritis can present itself
Our arches can collapse
Our posture changes
Custom orthotics are designed to support your foundation to operate efficiently and without pain.
Foot Levelers is the leading custom orthotic provider in the U.S. and if you are interested in finding out more information about custom orthotics, reach out to your local chiropractor.
After a quick scan, your feet will be assessed and your custom orthotics will be designed and made especially for you.
Foot Levelers Kiosk
The Kiosk helps guide patients in selecting the best custom-made orthotics for their condition and lifestyle. It’s�
Fast:�Push the Start button and the scanner begins.
Easy to use:�User-friendly easy touch screen.
Engaging:�Videos explain the importance of healthy feet and the benefits of custom-made orthotics.
Cloud-based:�Results can be securely accessed from anywhere.
Comprehensive:�Easily retrieve previous scans to compare them to new scans and see the difference.
The Foot Levelers Kiosk saves time so you can spend more time living your life.
Orthotics
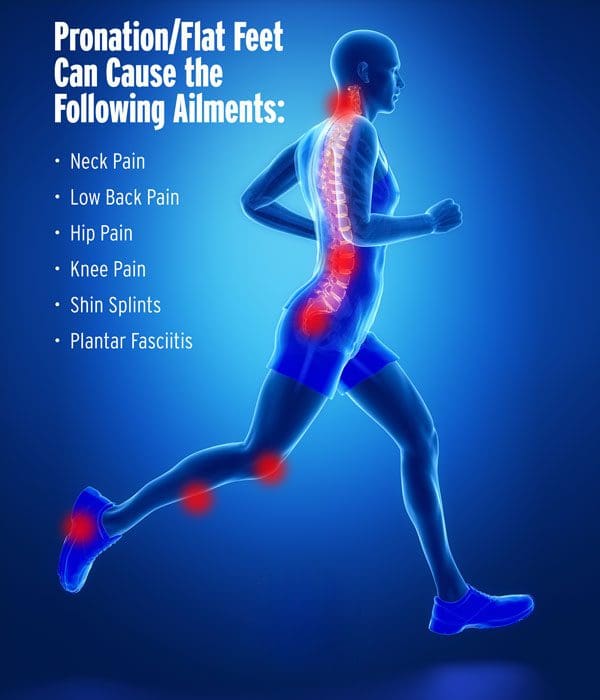
When there are problems with the feet, it can cause problems through the legs and all the way to the spine. This can cause the ankle to pronate, meaning it rolls inward. This alters the way the�bones of the foot�line up which extends through the tibia, or shin bone.
Pronation
Pronation describes the way that the foot rolls inward during its normal motion. The foot turns inward, flattening out, as the heel�s outer edge strikes the ground. For the foot to function correctly, there must be a significant degree of pronation. However, excessive pronation, or overpronation, can cause injury and damage to the foot and ankle. It creates the arch in the foot to flatten, and the ligaments, tendons, and muscles under the foot overstretch.
Experiencing foot pain, there�s no doubt you checked out your foot to make sure it�s not�injured�or hurting from�improper fitting shoes, corns, plantar fasciitis, etc. This may seem counterintuitive, but you may want to check the condition of the�lumbar spine (lower back)?� Most foot problems are caused by issues with the foot, but what if you found that pressure on the sciatic nerve can cause intense foot pain.
If you or someone you love is suffering from Crohn�s disease, you know how unpleasant it can be. A chronic inflammatory bowel disease, Crohn�s can make it difficult to lead a normal life. Even when you are able to work, play and relax the way you want, the disease can still cause painful, uncomfortable symptoms that you certainly can do without.
Fortunately, chiropractic care has been helpful for a number of patients with Crohn�s disease. You may be able to get some much-needed relief for your symptoms through regular chiropractic visits.
The Symptoms of Crohn�s Disease?
In most cases, Crohn�s disease causes parts of the small bowel and colon to become inflamed. The inflammation can result in several symptoms that are nothing you want to experience if you do not have to, including regular diarrhea, malnutrition, weight loss, abdominal pain, and fatigue.
Crohn�s Disease Is Usually Treated How?
It is an unfortunate reality that Crohn�s disease has no current cure. Standard treatments include using prescription medications and sometimes surgery to eliminate symptoms. Of course, these treatments may result in unwanted side effects which can sometimes be equal to or worse than the original symptoms. That is why chiropractors prefer to use treatments that are less invasive, like adjustments and complementary therapies.
Can Chiropractic Help with Crohn�s Disease?
There have been a variety of small studies conducted to determine the effects of chiropractic on Crohn�s disease. The results of these studies have been promising. Many have shown that chiropractic adjustments have helped those with Crohn�s to feel better than they did before the adjustments. They experienced a reduction in their symptoms, with some experiencing a significant reduction.
A young man suffering from severe belly pain, being overwhelmed by the debilitating condition of celiac disease/Crohn’s disease/strong anxiety
Why Choose Chiropractic?
The best thing about using chiropractic to treat Crohn�s symptoms is that it is so gentle and free of side effects. You can try chiropractic at very little risk to yourself or the danger of experiencing an increase in your symptoms. When you consider how likely side effects are from prescription medications�you only have to watch a commercial for pharmaceuticals to see the long list of possible side effects�and the risks of surgery, it is easy to see why so many Crohn�s sufferers look to chiropractic for relief.
What is a Chiropractic Visit like when You Have Crohn�s Disease?
Chiropractors are experienced in treating a wide variety of diseases and conditions. They also know how important it is to make you feel comfortable with your experience�from start to finish.
The first thing the chiropractor will do is conduct a thorough physical examination. He or she will also ask you a number of questions to find out exactly how you feel, and what your thoughts are on your condition.
After the examination the chiropractor will design a treatment plan that may include a variety of treatments:
Chiropractic adjustments. Adjustments focus on helping your spine and body achieve optimal alignment. The chiropractor will only apply enough pressure to achieve the desired result.
Massage therapy. Massage is an excellent complementary therapy that goes hand in hand with chiropractic care. By relaxing your muscles and releasing adhesions, massage can help your adjustments stay in place and lead to improved movement and less pain.
Spinal decompression. Using a specially designed machine, your chiropractor can increase the space between your vertebrae�space that leads to increased blood flow lowers pain levels and often results in faster healing.
Reduce *LOW BACK PAIN* with Foot Orthotics | El Paso, Tx
Approximately 80 percent of the population will experience some type of back pain sometime throughout their lifetime. Low back pain and sciatica are several of the most common complaints frequently reported in a doctor office setting. But, did you know that low back pain and sciatica can be caused due to foot problems?
Custom-made functional foot orthotics can help support and promote the natural alignment of the spine. Poor posture associated with foot problems and other health issues can be corrected through the utilization of custom-made functional foot orthotics. Because every individual has unique foot anatomy, custom-made foot orthotics can be beneficial for a variety of people with foot problems and other health issues. Dr. Alex Jimenez is the non-surgical choice for foot problems.
Foot Orthotics
Experiencing foot pain, there�s no doubt you checked out your foot to make sure it�s not�injured�or hurting from�improper fitting shoes, corns, plantar fasciitis, etc. This may seem counterintuitive, but you may want to check the condition of the�lumbar spine (lower back)?� Most foot problems are caused by issues with the foot itself, but you might be surprised to find that pressure on the sciatic nerve can cause intense foot pain.
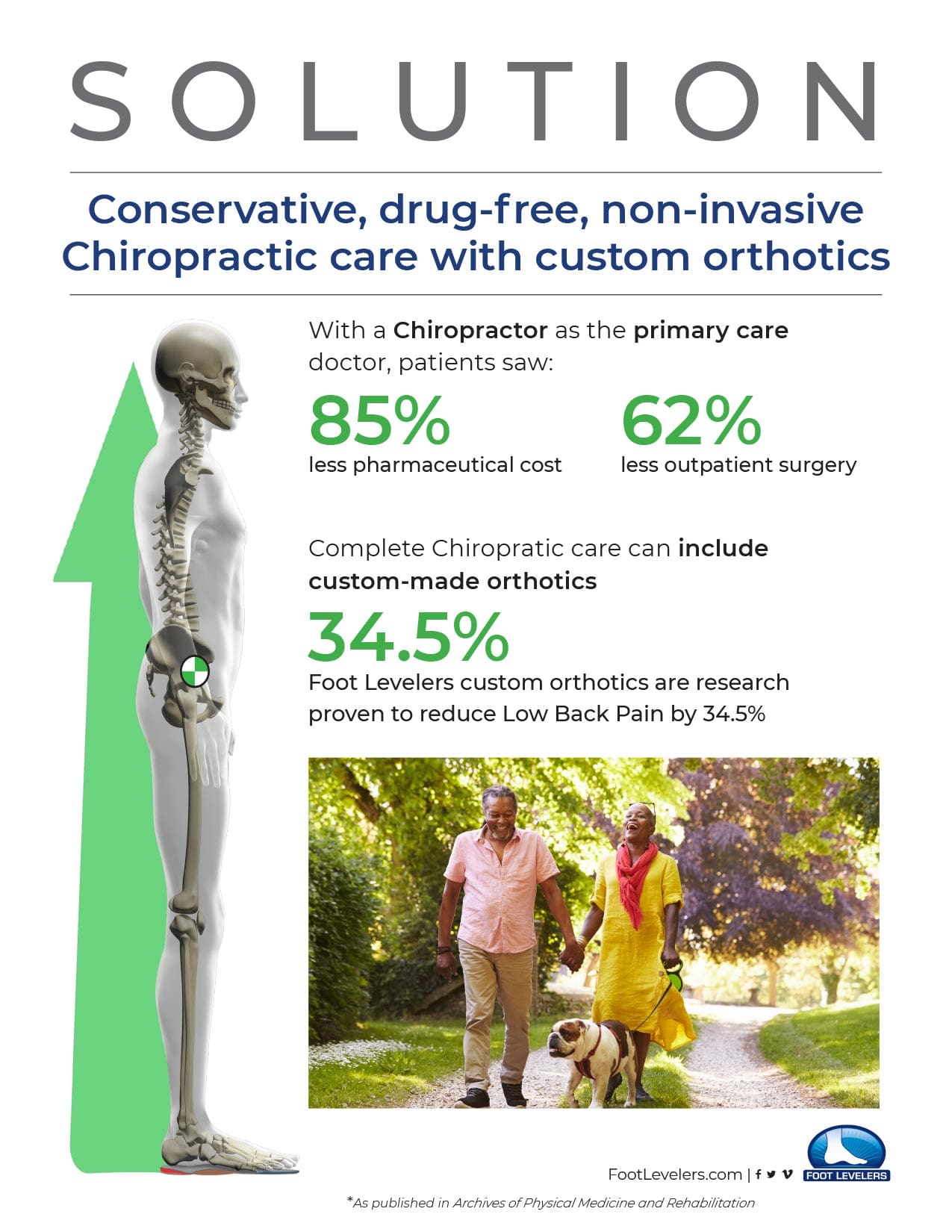
Before taking an opioid for pain control, give Chiropractic care and orthotics a try. The combination of Chiropractic and orthotics have been proven in clinical studies.
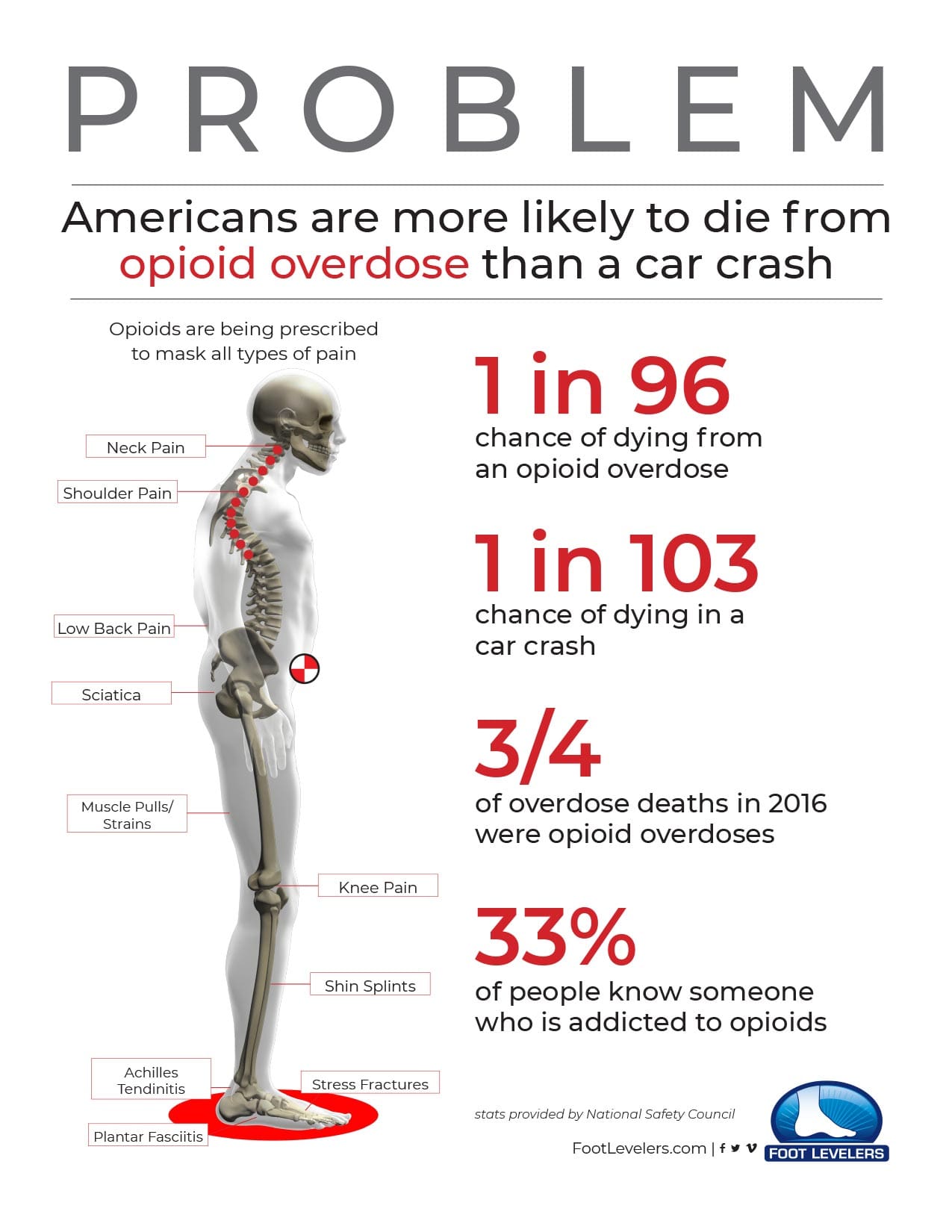
Pain & Opioid Prescription Usage
Researchers estimate that as many as 36 million people worldwide abuse opioids. Estimates in the U.S. alone reached�2.1 million people�in 2012. In 2014, six out of ten�drug overdose deaths involved an opioid � including prescription opioids for pain relief. Every day, 78 Americans die from an opioid overdose. As the Opioid drug problem continues to spiral further out of control, claiming more lives, people are looking for safer, drug-free ways to relieve their pain. Chiropractic offers such an option.
Gait Style & Chronic Postural Pain
The way a person walks, their gait, can be very telling. It can reveal problems in the feet, ankles, knees, and hips � even in�spinal alignment. A problem with gait can indicate pain in a patient as well as serious conditions like diabetes and arthritis. It, is a diagnostic tool for many conditions, injuries, and syndromes including autism.
When it comes to chiropractic care, a patient�s gait can offer critical clues regarding the root of their complaints, allowing for a more well-rounded, whole-body approach to treatment. If you think that the way you walk or moves doesn�t matter, think again. It most certainly does matter.
�NCBI Resources
Most people don�t think of chiropractic to treat conditions that do not involve the spine, but study after study shows it is effective in treating a wide variety of health issues.�Ulcerative colitis seems to have no real connection with the spine, yet patients and researches alike are touting the effectiveness of chiropractic care to treat the condition. This is due, in part to chiropractic�s approach to whole-body wellness, but�spinal alignments�are incorporated into the care as well. Bottom line, chiropractic care is extremely effective in treating uncreative colitis, and many patients are finding relief from their symptoms and discomfort.
The hip joint is the body�s largest ball-and-socket joint that allows for fluid movement during running, walking, and more.
There is a cushion of cartilage that helps prevent friction when the hip bone moves.
The hip is durable, but with age and use, this cushion can wear down or sustain an injury. So can the muscles, tendons, and bones surrounding the hip, caused by several conditions. These include:
Arthritis, Avascular necrosis (or osteonecrosis)
Certain cancers
Bursitis
Hip fractures
Hip labral tear
Muscle or tendon strain
Tendinitis
Treating your hip is successful when the focus is on restoring the balance and function of the entire body. This starts from the ground up with the feet along with a chiropractic examination that determines the root cause, which in turn helps in making an informed decision on a treatment plan. This instead of merely reducing the pain and inflammation in the irritated areas.
Symptoms of Hip Pain
Depending on the condition that’s causing your hip pain, you might feel the discomfort in:
Inside of the hip joint
Outside of the hip joint
Groin
Buttocks
Thigh
Treatment
Chiropractic and custom orthotics can help alleviate hip pain with adjustments, icing/heating and resting the affected joint.
Your chiropractor can help you set up a stretching and strengthening exercise regimen that will improve your hip�s function and reduce your pain.
Benefits of Using Custom *Foot Orthotics* | El Paso, TX (2019)
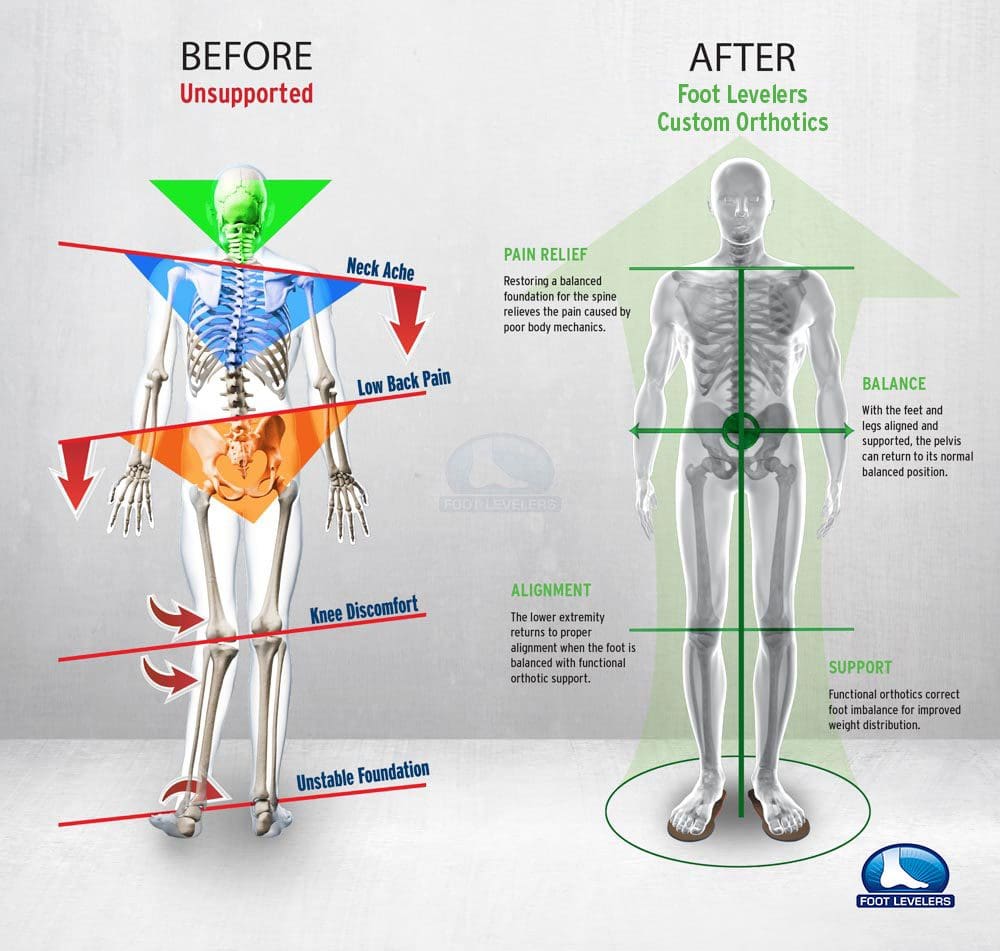
Functional custom foot orthotics understand the anatomy of the foot. By supporting the 3 arches of the foot, functional custom foot orthotics can help promote proper posture to prevent a variety of health issues, including neck pain and back pain. Over the counter, inserts may create more harm than good. Functional custom foot orthotics can also help maintain overall health and wellness. Because every person is unique, functional custom foot orthotics can help balance a person’s unique body structure and function. Dr. Alex Jimenez can help provide functional custom foot orthotics to patients who need to improve their overall health and wellness.
Custom Orthotics
When there are problems with the feet, it can cause problems through the legs and all the way to the spine. This can cause the ankle to pronate, meaning it rolls inward. This alters the way the�bones of the foot line up which extends through the tibia, or shin bone. This can cause a condition called knock knees and it can change the way the entire body is aligned. This puts the body out of balance, destabilizing the spine, and can even cause the pelvis to tilt to one side or the other.
Weak Hip Abduction
Muscle imbalances in the hip, such as tight hip flexors, can cause low back pain � or at least contribute to it. When the hip flexor muscles are too tight, it causes what is known as an anterior pelvic tilt. Hip flexors�can become too tight if the person sits for extended periods of time or engages in activities like cycling and jogging. A chiropractor can guide you through exercises that will help release the tight muscles and stop the micro spams that occur as a result.
NCBI Resources
If the health issue originates in the hip joint itself, common painful symptoms may often include groin pain on the affected side, which can occasionally radiate down the inner region of the thigh into the front of the leg. The painful symptoms can also travel to the knee, making healthcare professionals and patients believe their pain is associated with a knee problem rather than a hip problem
Plantar fasciitis is one of the most common causes of chronic heel or foot pain. According to the American Academy of Orthopedic Surgeons, approximately 2 million plantar fasciitis cases are diagnosed and treated each year. An estimated one in 10 people will develop plantar fasciitis at some point during their lifetimes. Moreover, plantar fasciitis accounts for between 11 and 15 percent of all foot symptoms, as demonstrated by research studies associated with the health issue. Most heel symptoms are caused by plantar fasciitis or the inflammation of the tissue on the bottom of the foot. �
What are the Symptoms of Plantar Fasciitis?
Plantar fasciitis is a foot health issue characterized by sharp, stabbing heel pain which generally manifests when a person gets out of bed in the morning or stands up after sitting for an extended period of time. Although the most frequent symptom of plantar fasciitis is shooting pain, the health issue may also cause swelling and inflammation in the heel. The pain from plantar fasciitis can be considerably severe after rest but it can generally improve significantly throughout the day. Additionally, the painful symptoms associated with plantar fasciitis may worsen after exercise or physical activity. �
The plantar fascia is a dense band of connective tissue found on the base of the foot which connects the heel to the front of the foot. This group of connective tissue supports the arch of the foot by functioning like a bowstring on a bow. The plantar fascia absorbs any type of stress and pressure being placed on the toes. Over time, however, a person may experience an injury or develop an underlying condition which may create inflammation of the fascia in the heel bone, resulting in plantar fasciitis, a chronic and persistent health issue. People can almost never fully rest their foot enough to heal completely. �
What Causes Plantar Fasciitis?
Plantar fasciitis occurs when the plantar fascia becomes tightened from too much stress and pressure, causing swelling and inflammation. As increasing tension builds up in the plantar fascia, tiny tears can begin to form in the dense band of connective tissue. Furthermore, more tension and ripping in the plantar fascia results in more swelling and/or inflammation. This buildup of tension and ripping ultimately causes plantar fasciitis and results in heel and foot pain. �
Men and women between the ages of 40 and 70 have a higher risk of developing plantar fasciitis. However, the health issue is slightly more prevalent among women than men. In addition, there’s a higher incidence of plantar fasciitis among athletes, especially runners, and it is sometimes referred to as “runner’s heel.” A 2002 research study demonstrated that 7.8 percent of sports injuries was plantar fasciitis. Also, the health issue ranked among the five most common sports injuries. �
What Other Health Issues Cause Heel Pain?
Plantar fasciitis is the most well-known cause of heel and foot pain. There are several less well-known causes of heel pain which should be ruled out before starting treatment for plantar fasciitis. Among these causes of heel and foot pain are: �
Bursitis: Bursas are fluid-filled sacs which cushion bones, muscles, and other soft tissues around joints in the human body. These can be found in the shoulders, elbows, and buttocks, as well as in the heel of the foot. Bursas in the feet can become irritated and inflamed due to excessive walking, running, or jumping.
Calcaneal Apophysitis: The growth plate, or epiphyseal plate, in the heel can also become irritated and inflamed. The health issue, also known as Sever’s disease, generally occurs in children during growth spurts.
Inflammatory Diseases: People with hereditary inflammatory conditions, such as rheumatoid arthritis, psoriatic arthritis, ankylosing spondylitis, Reiter’s syndrome, and gout, may experience heel pain.
Lateral Plantar Nerve Entrapment: Nerves located along the central region of the arch of the foot may become compressed or impinged between tissue and bone, leading to pain around the heel and ankle region of the foot.
Plantar Fascia Rupture: In rare cases, the plantar fascia may also rupture. This extremely debilitating injury generally occurs during high-impact exercise or physical activity, although some of the risk factors for plantar fasciitis, such as flat feet and obesity, can contribute to its occurrence. It also occurs in patients that have chronic plantar fasciitis.
Sciatica: An injury or underlying condition can compress or impinge the sciatic nerve, or the largest and longest nerve in the human body, causing low back pain and painful symptoms along the lower extremities. The pain may be felt in the foot, but it may be a tingling sensation or numbness in relation to the pain associated with plantar fasciitis.
Stress Fracture: A hairline fracture may develop in the heel bone, also referred to as the calcaneus. It’s generally caused by overuse or due to an injury where the heel is crushed under the weight of the human body, such as a fall. Calcaneal stress fractures are uncommon and account for approximately 2 percent of all fractures in adults.
Tarsal Tunnel Syndrome: The tarsal tunnel is a region within the ankle containing tendons, ligaments, arteries, and nerves. One of these soft tissues is the tibial nerve, which allows movement and provides feeling to the foot. Tarsal tunnel syndrome refers to the compression or impingement of the tibial nerve, caused by an ankle sprain, inflammatory disease, and flat or fallen arches. The common symptoms include a tingling sensation around the heel.
How Is Plantar Fasciitis Diagnosed?
Heel pain is the most common symptom associated with plantar fasciitis and it is often an unmistakable indication of the presence of the health issue. If the heel pain doesn’t improve after a few weeks, it’s recommended for you to make an appointment with a specialized healthcare professional, such as a podiatrist. A podiatrist will talk to you about your symptoms and evaluate your foot to rule out other conditions which can cause heel pain. Your podiatrist may also order an X-ray or alternative tests to make sure there’s not a fracture in your foot or anything else that’s causing your heel pain. �
Heel spurs, or small, pointed overgrowths on the heel bone or the calcaneus bone, may occasionally be seen on X-rays. However, heel spurs aren’t necessarily regarded as the cause of the pain in plantar fasciitis. As a matter of fact, they are often seen on X-rays of men and women who don’t have heel pain or plantar fasciitis and are therefore believed to be an incidental finding. One out of 10 people has heel spurs, but only 1 out of 20 individuals with heel spurs have foot pain and discomfort. �
How Is Plantar Fasciitis Treated?
Most cases of plantar fasciitis may be treated with self-care, including rest and by applying ice therapy. Stretches and exercises can also help speed up the recovery process and help prevent other health issues and complications, such as tightness or weakness of other foot muscles. However, complete recovery may take several months. �
Non-prescription and prescription drugs and/or medications can help decrease pain and swelling associated with plantar fasciitis. Orthotics, or shoe inserts which provide support and relieve stress and pressure on the foot, can also relieve pain. �
Plantar fasciitis generally requires treatment to stop it from becoming worse. When untreated, plantar fasciitis can restrict your mobility. It can also cause back problems, hip and knee problems, and other foot problems because of the way it affects the way you walk.
Chiropractic care and physical therapy can also help correct injuries and/or underlying conditions which may be causing or aggravating your plantar fasciitis.� Surgery performed to treat plantar fasciitis, called a plantar fasciotomy, can lead to complications. After surgery, some support to the foot is lost, causing temporary instability. �
Plantar fasciitis generally develops for no specific or clearly identifiable reason. However, a wide variety of risk factors can increase the chance of developing plantar fasciitis, such as excess weight and obesity, foot abnormalities, arthritis, and even wearing the improper shoes. Low back pain and sciatica can cause painful symptoms anywhere along the entire length of the sciatic nerve, however, plantar fasciitis is generally direct heel or foot pain. Low back pain and sciatica, however, can cause plantar fasciitis if the person’s posture is affected, causing stress and pressure on the heel and foot. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
Low Back Pain
The purpose of the article is to describe how plantar fasciitis can be associated with sciatica and other health issues. Sciatica is a collection of symptoms characterized by pain, tingling sensation, and numbness. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Foot Orthotics
Low back pain and sciatica are common health issues which affect many individuals worldwide. However, did you know that chronic pain may be due to foot problems? Health issues originating in the foot may ultimately cause imbalances in the spine, such as poor posture, which can cause the well-known symptoms of low back pain and sciatica. Custom foot orthotics, individually designed with 3-arch support can help promote overall health and wellness by supporting and promoting good posture and correcting foot problems. Custom foot orthotics can ultimately help improve low back pain and sciatica. �
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force. �
For many chiropractic patients, the first experience with chiropractic comes during early adulthood or middle age. Most adults seek out chiropractic care because they are in some sort of pain. If you are one of those that are new to chiropractic, its effectiveness may surprise you. Your next thought might be about how chiropractic could help others in your life�friends, family and more.
Fortunately, sharing chiropractic with your loved ones is easy because it is so well-suited to just about everyone. Whatever the age of the individual, chiropractic can be adapted to provide gentle preventative care and to improve overall health.
Smiling multi-generation family smiling down at the camera
Chiropractic for Children
Sometimes it can seem like children are invincible. They are flexible, heal quickly and tend to bounce back from situations that would floor an adult. But kids need support to be as healthy as possible, especially as they grow up. Chiropractic care is excellent for encouraging healthy growth in infants, toddlers, children, and teens.
Some of the benefits of chiropractic for children include:
Spinal alignment. The small spines of children can become misaligned much like those of adults. Regular chiropractic adjustments help to bring your child�s spine back into proper alignment, which encourages proper functioning of the nervous system, immune system and more.
Healthy movement patterns. It is normal to develop at least a few unhealthy movement patterns as we move from childhood to adulthood. These bad patterns can lead to injuries on down the line. Chiropractic care can help teach children how to move safely, which can yield benefits for a lifetime.
Gentle adjustments designed for young bodies. Chiropractors who work with children learn special techniques to ensure that adjustments heal and not hurt. Immature bodies work in much the same way as older bodies, but a delicate touch is still important for safety.
Chiropractic Care for Older Adults
Older adults can also experience numerous benefits from chiropractic care. The elderly in particular face a number of health challenges that chiropractic can assist with. Some of the benefits of chiropractic care for older adults include:
Pain relief. Chiropractic can do wonders for pain management, all without drugs or surgery. Regular adjustments and other supplemental therapies have been proven to reduce or eliminate pain, something older adults can truly appreciate.
More mobility. Just because you get older does not mean you should have to stop doing the things you love. Chiropractors know how to gently increase your mobility so that you can get back on your feet and enjoy life the way you deserve.
Improved immune response. The nervous system and immune system are linked in many ways. Adjustments help to align the spine and improve nervous system function. An adjustment can also aid in immune system function, which means your body can fight off invaders more effectively.
Contact us today to schedule an appointment with our chiropractic team. We look forward to meeting you!
Benefits of Using Custom *Foot Orthotics* | El Paso, TX (2019)
Foot Orthotics
Experiencing foot pain, there�s no doubt you checked out your foot to make sure it�s not�injured�or hurting from�improper fitting shoes, corns, plantar fasciitis, etc. This may seem counterintuitive, but you may want to check the condition of the�lumbar spine (lower back)?� Most foot problems are caused by issues with the foot itself, but you might be surprised to find that pressure on the sciatic nerve can cause intense foot pain.
What is a Pronated Foot and Can Custom Orthotics Help?
When a foot is pronated, it means the arches have fallen and the foot is flat.
Flat feet are less shock-absorbent and make for a less stable base for the rest of the body. This includes the bones, muscles, ligaments, and tendons.
Flat Feet can also:
Shift the body out of alignment
Cause pain in the feet, knees, hips, neck, and spine
Lead to injury/s like shin splints, Achilles tendinitis, and plantar fasciitis
Women with flat feet are 50% more likely to have low back pain
Up to 1/3 of people suffer from flat feet
�Pronation Causes
The connective tissue, called the plantar fascia, on the underside of the foot is what maintains the foot�s healthy arch shape.
Walking and standing, injury and health conditions can cause the fascia to stretch out and flatten.
Once the fascia stretches out, there is nothing to bring the spring back.
Treatment
Chiropractic adjusting to ensure proper positioning of bones and joints
Custom orthotics for pronation control, support, and comfort
Chronic Inversion Sprain
Foot Dysfunction can very easily cause a domino effect that extends all the way to the back. The feet are the foundation of the body and when there is a problem with the way they function it can cause the entire body to shift out of alignment. For instance, overpronation of the foot causes a series of internal changes that extend up through the leg. The femur may rotate causing hip pain and inflammation of the sacroiliac joint which leads to back pain. Other misalignments in the body that are caused by foot problems can also lead to chronic lower back pain as well.
NCBI Resources
The best way to keep your spinal joints healthy over the long-term is to make regular visits to your chiropractor while also maintaining a healthy diet and�exercise regimen. Everyone is different, which is why it is important to get customized treatment from your chiropractor.
Many individuals assume that knee pain is always associated with knee joint health issues. However, according to healthcare professionals, knee pain can also occur due to spine health issues. While pain and discomfort can be the result of a knee problem, it can also be the result of a herniated disc or a pinched nerve root, commonly the sciatic nerve, in the lower back. �
If healthcare professionals suspect that the patient’s knee pain is due to another underlying health issue, they will perform a diagnosis utilizing a variety of evaluations to determine the source of the patient’s knee pain. The purpose of the article below is to describe how low back pain and sciatica can also cause knee pain as well as other painful symptoms. �
Sciatica, Low Back Pain and Knee Pain
The sciatic nerve, the largest and longest nerve in the human body, extends from the lower back, or lumbar spine, and travels down the buttocks, hips, and thighs into the legs, knees, and feet. With age or due to an injury or underlying condition, however, the intervertebral discs may sometimes bulge out and push against or through the intervertebral disc material, pinching or irritating the sciatic nerve, causing low back pain or sciatica. Sciatica is also referred to as sciatic nerve pain. �
When the sciatic nerve becomes compressed or impinged and irritated, it can send pain signals out throughout the entire length of the sciatic nerve. �If a spinal health issue, such as a herniated disc, spinal stenosis, or arthritis is pinching the sciatic nerve, the painful symptoms may radiate into the knee and even into the feet.�If the sciatic nerve is being compressed or impinged and irritated due to an injury or underlying condition, it may cause a variety of painful symptoms, including: �
Pain and discomfort in the thigh
Knee pain
Tingling sensations and/or numbness in the leg
Weakness in the hip
In the circumstance that you are experiencing any of the painful symptoms described above, make sure to seek immediate medical attention from a qualified and experienced healthcare professional to receive an accurate diagnosis before following-up with proper treatment. Your knee pain may also be due to a hip joint health issue, therefore, a careful physical evaluation is ultimately fundamental to determine the true source of your knee pain, low back pain, and sciatica. �
Low Back Pain, Sciatica, and Knee Pain Treatment
Treating knee pain due to the compression or impingement and irritation of the sciatic nerve can ultimately be achieved through surgical interventions, however, it is generally not recommended until the patient has tried all conservative treatment options. Conservative treatment approaches are often initially preferred. Sometimes, steroid injections can be utilized to help decrease inflammation around the nerve root but these should not be the initial treatment for knee pain. �
Physical therapy and chiropractic care can help naturally restore the original integrity of the spine to treat low back pain, sciatica, and knee pain. Healthcare professionals may also recommend a variety of stretches and exercises to strengthen the surrounding structures and speed up the recovery process. Engaging or participating in a progression of stretches and exercises can help safely and effectively eliminate knee pain and improve your overall health and wellness. �
If your knee pain worsens with physical activities, the healthcare professional can also show you postural correction techniques and strategies to help decrease stress on your spine and help decrease knee pain as well as avoid future health issues. If physical activity doesn’t have any effect on your knee pain, the healthcare professional may perform a variety of tests and exams to make sure if your knee pain is due to a knee joint or hip joint health issue, among other health issues.
�
Knee pain is a well-known health issue, however, did you know that knee pain can also be caused due to low back pain and sciatica? Sciatica is a collection of painful symptoms, rather than an injury or underlying condition, characterized by pain, tingling sensations, and numbness along the entire length of the sciatic nerve. Because the sciatic nerve extends from the lower back, down the buttocks, hips, and thighs, into the legs, knees, and feet, any health issue which irritates the sciatic nerve can potentially cause knee pain. The compression or impingement of the sciatic nerve due to a variety of health issues, can ultimately cause low back pain, sciatica, and knee pain. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
Low Back Pain
The purpose of the article was to describe how knee pain can be associated with low back pain and sciatica. Sciatica is a collection of symptoms characterized by pain, tingling sensation, and numbness. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Foot Orthotics
Low back pain and sciatica are common health issues which affect many individuals worldwide. However, did you know that chronic pain may be due to foot problems? Health issues originating in the foot may ultimately cause imbalances in the spine, such as poor posture, which can cause the well-known symptoms of low back pain and sciatica. Custom foot orthotics, individually designed with 3-arch support can help promote overall health and wellness by supporting and promoting good posture and correcting foot problems. Custom foot orthotics can ultimately help improve low back pain and sciatica. �
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force. �
Healthy joints have obvious benefits, including aiding in movement, keeping you flexible and allowing you to stay active. The health of some of your joints is readily apparent�you only have to bend your knees, ankles, elbows or wrists to see how they are functioning at any given moment. But there are some joints in your body that are even more important, although you may not be as aware of them. The joints in your spine, where each vertebra connects to another, are vital to the normal, healthy function of your body. Without healthy spinal joints, you can expect pain and loss of mobility, among other unpleasant symptoms.
Fortunately, keeping your spinal joints healthy is made much easier with regular chiropractic care. Periodic visits to your chiropractor will help you keep your spine operating as well as it possibly can, year in and year out!
Ways that Chiropractic Helps In Spinal Joint Health
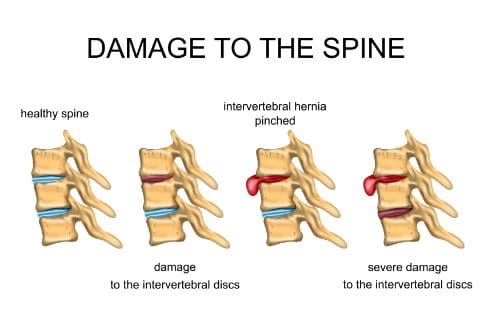
ILLUSTRATION OF A HEALTHY INTERVERTEBRAL DISC, THE DAMAGED INTERVERTEBRAL DISC, HERNIATION.
1. Circulation Increased.
Stiffness in the spine can be caused by a variety of issues, including trauma and degenerative disc disease. While chiropractic cannot prevent the wear and tear that life often brings, it can do a lot to heal that damage. One way that adjustments aid in healing is by increasing circulation to your spinal discs and surrounding tissues. Increased circulation brings in healthy nutrients and removes undesirable material, making it possible for your spine to heal more thoroughly than without good circulation.
2. Pain Is Reduced or Eliminated.
Back pain can make living a normal life difficult if not impossible. Depending on the frequency and severity of the pain, you may find yourself unable to do many of the things you once enjoyed. Even if you do not lose mobility, back pain can distract and upset you every time it shows up.
The pain in your back can most likely be alleviated through chiropractic care. By returning your spine to proper alignment, your chiropractor can ease pressure on the nerves in your back and encourage muscles and other soft tissue to release. Over time spinal adjustments can greatly reduce or even eliminate back pain, which will help you stay active and improve the health of your spinal joints.
3. Mobility Increased.
Pain in your spine and/or neck is usually accompanied by a loss of mobility. Your muscles may seize up in an effort to protect your spine, which can make it impossible to move normally. Even if you are not suffering from muscle spasms, consistent back and neck pain can make you hesitant to move in ways that will trigger pain. Over time, the lack of movement can cause the body to stiffen and weaken. The longer this goes on, the less likely you are to get the physical activity you need to keep your joints mobile and your body strong.
Chiropractic adjustments are capable of breaking up the stiffness that holds you back. By returning your spine to proper alignment, circulation is increased, pain is decreased, muscles release and mobility returns. It can take time to get back to the way you want to be, but it is time well spent.
Healthy Joint Health Requires Consistency
The best way to keep your spinal joints healthy over the long-term is to make regular visits to your chiropractor while also maintaining a healthy diet and exercise regimen. Everyone is different, which is why it is important to get customized treatment from your chiropractor. By establishing a relationship with your chiropractor, you can ensure that you are always on the right track for spinal joint health.
Contact us today to learn more about chiropractic care and to schedule an appointment with our team.
The Difference of Using *CHIROPRACTIC ORTHOTICS* | El Paso, Tx
Custom Orthotics are Worth The Cost
People who experience back, hip, and/or foot pain usually turn to orthotics for relief.
Foot Levelers is the leading custom orthotic provider in the U.S., but custom is not always cheap, as compared with the non-customized, over-the-counter orthotics.
What�s the difference and why spend money on custom orthotics?
Common Orthotics are Not The Same for Everyone
What works for one person may not work for you, which is evident by all the different insoles on the market for the same problems.
Take 10 people, all of who have different levels of activity, weight, age, types of pain and wear different shoes, go to the store for store-bought orthotics, take a quick assessment, and are all told to wear the same insole.
You need customized care, which is exactly what custom orthotics provide for your body.
Custom orthotics are created by scanning and assessing your arches, seeing how you distribute your body weight on your feet, and then a unique treatment plan is created especially for you.
The Body’s Foundation is our Feet
What if you were told that the foundation of your home was cracking and you had two options: put duct tape over the crack and hope for the best or spend a little more money and fix the problem the right way.
A scan of the feet is used to learn about each foot independently.
These scans highlight any differences between your feet like one being smaller, wider, or flatter than the other.
This information is essential to creating orthotics and helps achieve a result that over-the-counter orthotics simply cannot provide.
Although non-custom orthotics are less expensive, they are basically like putting duct tape on your foundation and may not resolve the issue\s and cause more problems and greater costs.
In the Long Run You Will Save Money
Custom orthotics are an investment that pays your body back a hundredfold.
Non-custom orthotics are cheaper and are made with unreliable and usually cheap material. These are not designed to resolve your condition, which forces you to spend more money.
Paying attention to the foundation of your body provides benefits to the rest of your body, and eliminates the cost of treating all types of discomfort.
The process of getting custom orthotics begins with a simple foot scan.
This provides us with important information to keep your body operating optimally.
Spine Pain
Overpronation and over supination can cause a variety of injuries and conditions that affect not only the feet and ankles, but also the knees, hips, and back as well. Foot Dysfunction�can very easily cause a domino effect that extends all the way to the back. The feet are the foundation of the body and when there is a problem with the way they function it can cause the entire body to shift out of alignment.
NCBI Resources
All our organs receive messages from our brain via our spinal cord. The lungs know to breathe in and out because of the messages they receive from the brain. The heart beats because of these messages as well. Every organ in our body is connected to the brain and blocking this connection�even a little�can cause serious health issues. Some health problems are easily felt like numbness in the fingers or a headache. Some troubles are not so apparent like digestive issues or kidney problems. If the spine is out of order, the organs will feel it.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine