Ataxia is a degenerative disease of the nervous system. Symptoms can mimic those of being inebriated/intoxicated, with� slurred speech, stumbling, falling, and unable to maintain coordination. This comes from degeneration of the cerebellum, which is the part of the brain responsible for coordinating movement. It is a disease that affects people of all ages. However, age of symptom onset can vary, from childhood to late adulthood. Complications from the disease can be serious, even debilitating and life shortening.
Symptoms can vary from person to person, as well as, the type of Ataxia. Symptom onset and progression can vary as well. Symptoms can worsen slowly, over decades or quickly, over a few months. The common symptoms are lack of coordination, slurred speech, trouble eating, swallowing, eye movement abnormalities, motor skill deterioration, difficulty walking, gait abnormalities, tremors, and heart problems. People with Ataxia usually require wheelchairs, walkers, and/or scooters to aid in mobility.
Contents
Ataxia
The Loss Of Full Control Of Bodily Movements, Especially Gait
History Of Ataxia
- How long has it been present?
- Slow onset ? Degenerative disease?
- Acute onset ? Stroke?
- When does it occur?
- If worsened by walking on uneven surfaces, or with limited vision ? Sensory ataxia?
- Are there any coexisting symptoms?
- Vertigo, weakness, stiffness, cognitive changes, etc.
- Have others noticed this gait disturbance?
- If no, consider psychogenic cause
- Is the gait change explainable by physical problems such as pain or weakness?
- Antalgic gait, limp, etc.
-
Weakness
- Proximal muscle weakness�? Myopathy?
- Distal muscle weakness ? Neuropathy?
- UMN signs?
- LMN signs?
- Has the patient fallen? Or at risk for fall?
- Is ataxia limiting ADLs?
Balance
- Utilizes
- Vestibular system
- Cerebellar system
- Conscious proprioceptive information (joint position sense)
- Visual information
- Motor strength and coordination
Vestibular System
- Generally, if the problem lies in the vestibular system the patient will experience dizziness, possibly having vertigo or nystagmus
- Unable to walk a straight line
- When walking, will tend to veer to one side
Testing The Vestibular System
-
Fukuda Stepping Test
- Patient marches in place with eyes closed and arms raised to 90 degrees in front of them
- If they rotate more than 30 degrees = positive
- Patient will rotate toward the side of vestibular dysfunction
-
Rhomberg Test
- If patient sways a different direction every time their eyes are closed, this may indicate vestibular dysfunction
Cerebellar System
- Cerebellar gaits present with a wide-base and generally involve staggering and titubation
- Patient will have difficulty doing Rhomberg�s test with eyes open or closed, because they cannot stand with their feet together
- Afferent information helps make assessments about where the body is in space
- Ventral spinocerebellar tract
- Dorsal spinocerebellar tract
- Cuneocerebellar tract
- Olivocerebellar tract
- Efferent tracts carry responsive information to make adjustments to muscle tone and position to maintain balance
Testing The Cerebellar System
-
Piano-playing test & hand-patting test
- Both assess for dysdiadochokinesia
- Both tests, patient will have more difficulty moving the limb on the side of cerebellar dysfunction
-
Finger-to-nose test
- Patient may be hyper/hypo metric in movement
- Intention tremor may be reveled
Joint Position Sense
- Conscious proprioception may be diminished, especially in elderly patients and patients with neuropathy
Visual Information
- Patients with joint position sense losses often rely on visual information to help compensate.
- When visual input is removed or diminished these patient�s have exaggerated ataxia.
Motor Strength & Coordination
- If patient has reduced frontal lobe control they may end up with an apraxia of gait, where they have difficult with the volitional control of movement
- Extrapyramidal disorders such as Parkinson disease result in inability to control motor coordination
- Pelvic girdle muscle weakness due to a myopathy will produce an abnormal gait pattern
Commonly Seen Abnormal Gait Patterns
-
Circumduction gait
- Hemiplegia
- Often due to stroke
- Bilaterally (Diplegic gait), causes toe walking
- Typical gait of cerebral palsy patients
-
Festinating gait
- Small steps due to spasticity
- Often seen in Parkinson Disease
-
Myopathicgait(waddling)
- Seen in disorders of proximal muscle weakness
-
Steppage gait/Neuropathic gait
- Leg is lifted from the hip, without dorsiflexion at the ankle
- Often seen in patients with foot-drop due to a LMN lesion
- Wide-BasedCerebellargait
Gait Deviations
Dizziness
The Sensation Of Loss Of Balance
-
4 Main Types
- Vertigo
- Peripheral
- Central
- Pre-Syncope/Light-headedness
- Disequilibrium
- Other/Floating type
Peripheral Vertigo
- More common than central vertigo
- Due to damage to the inner ear or CN VIII
- Usually produces abnormal eye movements
- Nystagmus � May be horizontal or rotary
- Usually jerky in nature, with a fast and slow phase
- Named for the direction of the fast phase
- Vertigo usually worsens when patient looks to the side of the fast phase of nystagmus
- Severity of nystagmus usually correlates with severity of vertigo
- No other symptoms/signs of CNS dysfunction
- Patient may have nausea or difficulty walking, but only because of vestibular dysfunction
- Patient may also have hearing loss or tinnitus due if CN VIII or auditory mechanism function is damaged
- Typically the causes are benign, including
- Benign paroxysmal positional vertigo (BPPV)
- Cervicogenic vertigo
- Acute labyrinthitis/Vestibular neuronitis
- Meniere�s Disease
- Perilymph fistula
- Acoustic Neuroma
Narrowing It Down
- If movement, particularly of the head/neck exacerbate vertigo, consider:
- BPPV
- Vertebrobasilar artery insufficiency
- Cervicogenic vertigo
- If noise brings on episodes, consider:
- Meniere�s disease
- Perilymph fistula
Vertigo Hx Questions
- Does your dizziness feel like you�re on an amusement park ride?
- Do you get nauseous when you�re dizzy?
- Are you spinning?
- Or is the world spinning?
Benign Paroxysmal Positional Vertigo (BPPV/BPV)
 May develop spontaneously, especially in the elderly
May develop spontaneously, especially in the elderly- May arise due to head trauma
- Vertiginous episodes associated with specific movements:
- Looking at a high shelf (�top-shelf vertigo�)
- Bending over
- Rolling over in bed
- Onset of vertigo begins a few seconds after the movement, and resolves within about a minute
- Diagnostic test
- Dix-Hallpike Maneuver
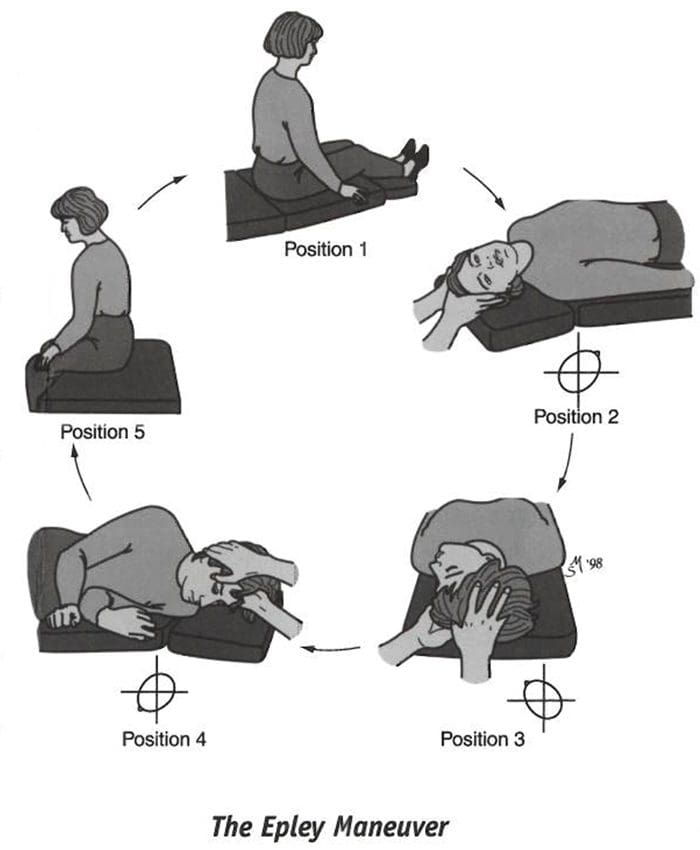
- Treatment procedure
- Epley Maneuver
- Brandt-Daroff Exercises
- Can self resolve as crystals dissolve, but it may take months and new otoliths can become displaced
Cervicogenic Vertigo
- Occurs after head/neck injuries, but is not very common
- Usually accompanied by pain and/or joint restriction
- Usually vertigo and nystagmus will be less severe than in BPPV
- Vertigo begins with change in head position but does not subside as quickly as it does in BPPV
Vertebrobasilar Artery Insufficiency
- Occurs if the vertebral artery is compressed during head rotation/extension
- Onset of vertigo is delayed more than in BPPV or cervigogenic vertigo, because ischemia will take up to 15 seconds to occur
- Orthopedic test may help in evaluation
- Barre?-Lie?ou Sign
- DeKlyn Test/Hallpike Maneuver
- Hautant test
- Underberg Test
- Vertebrobasilar After Functional Maneuver
Acute Labyrinthitis/ Vestibular Neuronitis
- Not well understood, but believed to be inflammatory in origin
- Follows viral infection or arise seemingly without cause
- Single, monophasic attack of vertigo
- Resolves in days to a few weeks and generally does not reoccur
Meniere�s Disease
- Increased pressure in the endolymph causes membrane ruptures and sudden mixture of endolymph and perilymph
- Episodes last 30 minutes to several hours, until equilibrium between the fluids is reached
- Over time, episodes damage vestibular and cochlear hair cells
- Low-pitch buzzing tinnitus
- Loss of hearing of low tones
Meniere�s Disease vs. Syndrome
- Meniere�s syndrome is when then symptoms of Meniere�s disease are found to be secondary to another condition, such as:
- Hypothyroidism
- Acoustic neuroma
- Superior semicircular canal dehiscence (SCDS)
- Perilymph fistula
- True Meniere�s disease is idiopathic
Perilymph Fistula
- Small leak due to trauma, especially barotrauma
- Can look very similar symptomatically to Meniere�s disease/syndrome
- Exacerbated by changes in pressure
- Airplane rides
- Driving uphill
- Hennebert�s sign
- Vertigo or nystagmus episode brought on by sealing pressure of the ear (such as by inserting an otoscope)
Central Vertigo
- Less common than peripheral vertigo
- Caused by damage to the processing centers of vestibular information in the brain stem and the cerebral cortex
- Typically �dizziness� is less severe than with peripheral vertigo
- Nystagmus
- Usually more severe than the description/patient�s complaint
- May go in multiple directions, including vertical
- May or may not have other CNS findings on examination
- No change in hearing expected
Causes Include:
- Cerebrovascular disease (such as transient ischemic attacks)
- Multiple Sclerosis
- Arnold-Chiari Malformation
- Damage to caudal brainstem or vestibulocerebellum
- Migraine condition
Pre-Syncope Hx Qustions
- Does it feel like you�re going to pass out?
- Does the dizziness feel similar to when you stand up too fast?
Pre-Syncope
- �Light-headedness�
- CardiacOrigin
- Output disorders
- Arrhythmias
- Holter monitor testing
- Postural/Orthostatic hypotension
- May be secondary to other problems (diabetic neuropathy, adrenal hypofunction, Parkinsons, certain medications, etc.)
- Vasovagal episodes
- Slow heart rate with low blood pressure
- Often brought on by stress, anxiety or hyperventilation
- Migraine
- Due to cerebrovascular instability
- Blood sugar dysregulation
Disequilibrium Hx Questions
- Does the dizziness only occur when you�re on your feet?
- Does it get better if you touch/hold onto something?
Disequilibrium
- Common in the elderly
- Due to sensory deficits
- Gradual onset
- Worsened by reduced vision
- Dark
- Eyes closed
- Visual acuity losses
- Improved by touching a stationary object
- Subjective of dizziness often improves with a gait assistive device (cane, walker, etc.)
Other Causes
- Psychological stress
- Often patient will describe dizziness as �floating�
- Rule out hyperventilation and other types of dizziness
Sources
Blumenfeld, Hal. Neuroanatomy through Clinical Cases. Sinauer, 2002.
Alexander G. Reeves, A. & Swenson, R. Disorders of the Nervous System. Dartmouth, 2004.
General Disclaimer, Licenses and Board Certifications *
Professional Scope of Practice *
The information herein on "Ataxia And Dizziness | El Paso, TX." is not intended to replace a one-on-one relationship with a qualified health care professional or licensed physician and is not medical advice. We encourage you to make healthcare decisions based on your research and partnership with a qualified healthcare professional.
Blog Information & Scope Discussions
Welcome to El Paso's Premier Wellness and Injury Care Clinic & Wellness Blog, where Dr. Alex Jimenez, DC, FNP-C, a Multi-State board-certified Family Practice Nurse Practitioner (FNP-BC) and Chiropractor (DC), presents insights on how our multidisciplinary team is dedicated to holistic healing and personalized care. Our practice aligns with evidence-based treatment protocols inspired by integrative medicine principles, similar to those on this site and on our family practice-based chiromed.com site, focusing on naturally restoring health for patients of all ages.
Our areas of multidisciplinary practice include Wellness & Nutrition, Chronic Pain, Personal Injury, Auto Accident Care, Work Injuries, Back Injury, Low Back Pain, Neck Pain, Migraine Headaches, Sports Injuries, Severe Sciatica, Scoliosis, Complex Herniated Discs, Fibromyalgia, Complex Injuries, Stress Management, Functional Medicine Treatments, and in-scope care protocols.
Our information scope is multidisciplinary, focusing on musculoskeletal and physical medicine, wellness, contributing etiological viscerosomatic disturbances within clinical presentations, associated somato-visceral reflex clinical dynamics, subluxation complexes, sensitive health issues, and functional medicine articles, topics, and discussions.
We provide and present clinical collaboration with specialists from various disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for musculoskeletal injuries or disorders.
Our videos, posts, topics, and insights address clinical matters and issues that are directly or indirectly related to our clinical scope of practice.
Our office has made a reasonable effort to provide supportive citations and has identified relevant research studies that support our posts. We provide copies of supporting research studies upon request to regulatory boards and the public.
We understand that we cover matters that require an additional explanation of how they may assist in a particular care plan or treatment protocol; therefore, to discuss the subject matter above further, please feel free to ask Dr. Alex Jimenez, DC, APRN, FNP-BC, or contact us at 915-850-0900.
We are here to help you and your family.
Blessings
Dr. Alex Jimenez, DC, MSACP, APRN, FNP-BC*, CCST, IFMCP, CFMP, ATN
email: [email protected]
Multidisciplinary Licensing & Board Certifications:
Licensed as a Doctor of Chiropractic (DC) in Texas & New Mexico*
Texas DC License #: TX5807, Verified: TX5807
New Mexico DC License #: NM-DC2182, Verified: NM-DC2182
Multi-State Advanced Practice Registered Nurse (APRN*) in Texas & Multi-States
Multi-state Compact APRN License by Endorsement (42 States)
Texas APRN License #: 1191402, Verified: 1191402 *
Florida APRN License #: 11043890, Verified: APRN11043890 *
Colorado License #: C-APN.0105610-C-NP, Verified: C-APN.0105610-C-NP
New York License #: N25929, Verified N25929
License Verification Link: Nursys License Verifier
* Prescriptive Authority Authorized
ANCC FNP-BC: Board Certified Nurse Practitioner*
Compact Status: Multi-State License: Authorized to Practice in 40 States*
Graduate with Honors: ICHS: MSN-FNP (Family Nurse Practitioner Program)
Degree Granted. Master's in Family Practice MSN Diploma (Cum Laude)
Dr. Alex Jimenez, DC, APRN, FNP-BC*, CFMP, IFMCP, ATN, CCST
My Digital Business Card
Licenses and Board Certifications:
DC: Doctor of Chiropractic
APRNP: Advanced Practice Registered Nurse
FNP-BC: Family Practice Specialization (Multi-State Board Certified)
RN: Registered Nurse (Multi-State Compact License)
CFMP: Certified Functional Medicine Provider
MSN-FNP: Master of Science in Family Practice Medicine
MSACP: Master of Science in Advanced Clinical Practice
IFMCP: Institute of Functional Medicine
CCST: Certified Chiropractic Spinal Trauma
ATN: Advanced Translational Neutrogenomics
Memberships & Associations:
TCA: Texas Chiropractic Association: Member ID: 104311
AANP: American Association of Nurse Practitioners: Member ID: 2198960
ANA: American Nurse Association: Member ID: 06458222 (District TX01)
TNA: Texas Nurse Association: Member ID: 06458222
NPI: 1205907805
| Primary Taxonomy | Selected Taxonomy | State | License Number |
|---|---|---|---|
| No | 111N00000X - Chiropractor | NM | DC2182 |
| Yes | 111N00000X - Chiropractor | TX | DC5807 |
| Yes | 363LF0000X - Nurse Practitioner - Family | TX | 1191402 |
| Yes | 363LF0000X - Nurse Practitioner - Family | FL | 11043890 |
| Yes | 363LF0000X - Nurse Practitioner - Family | CO | C-APN.0105610-C-NP |
| Yes | 363LF0000X - Nurse Practitioner - Family | NY | N25929 |
Dr. Alex Jimenez, DC, APRN, FNP-BC*, CFMP, IFMCP, ATN, CCST
My Digital Business Card






