Chiropractic and Shockwave for Injury Relief
Abstract
In this educational post, I share my personal journey from debilitating plantar fasciitis to lasting recovery, and how that experience led me to integrate true shockwave therapy into comprehensive chiropractic and physical therapy care at El Paso Back Clinic. I explain how shockwaves work at the cellular level, why electrohydraulic systems deliver stronger and more reliable therapeutic effects than radial pressure waves, and how focused and broad-focus energy can improve tissue healing, angiogenesis, and modulation of inflammation. I present outcome data from leading registries, highlight on-field recovery examples from professional athletes, and outline how integrative chiropractic care, manual therapy, and targeted rehabilitation protocols synergize with shockwave to accelerate return to sport and work. You will find clear explanations, clinical reasoning, and practical protocols for plantar fasciitis, adductor strains, bone edema, tendinopathies, and post-operative healing—prioritizing non-invasive, cash-pay, and workflow-friendly solutions that minimize reliance on injections or medications while keeping hormone and pharmacologic strategies in the background.
Introduction: Why I Brought Shockwave into Integrative Chiropractic Care
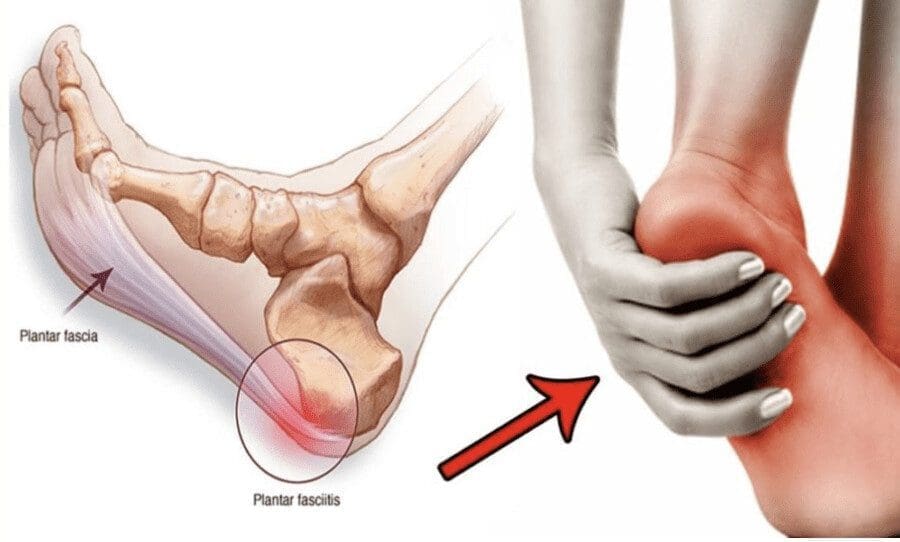
Seven years ago, a patient developed severe plantar fasciitis in both feet. They were told cortisone injections might help, but declined, hoping for a better way. A friend in the shockwave field saw them hobbling and suggested they try treatment. The first session was intense—the prevailing view back then was “push through pain”—and while they felt better that day, the pain returned within a few days. Two months later, without elaborate stretching or self-care, they woke up and realized they hadn’t felt foot pain for days. The relief lasted almost four years before they needed another round. This experience highlighted the potential of technologies that safely and effectively stimulate the body’s natural repair systems.
At El Paso Back Clinic, true shockwave therapy—specifically electrohydraulic technology—is integrated into a broader model of chiropractic care, physical therapy, and evidence-based rehabilitation. The goal is to make healing predictable, comfortable, and accessible for patients while reducing dependence on injections or medications unless truly necessary.
Shockwave Therapy Basics: What It Is and Why the Mechanism Matters
- Core concept: A shockwave is a rapidly propagating acoustic wave with steep pressure gradients that exerts a mechanical force on cells and tissues.
- Mechanotransduction: When a true shockwave hits a cell membrane, it causes a rapid pressure change that makes the membrane transiently more permeable. This mechanical stimulus triggers cellular signaling, promoting angiogenesis, modulation of inflammation, and tissue repair (Schmitz et al., 2015; Wang, 2012).
- Therapeutic outcomes: Research shows increased microvascular density, improved perfusion, and activation of pathways such as VEGF, eNOS, and BMPs, thereby supporting bone and soft tissue regeneration (Wang, 2012; Schmitz et al., 2015).
Why Electrohydraulic Shockwaves Outperform Radial Pressure Waves
Not all “shockwaves” are equal. In community advertising, the term “shockwave” often refers to radial pressure-wave devices, which are distinct from true shockwaves.
- Radial pressure waves:
- Mechanism: Generate surface-level pressure pulses that disperse broadly and do not reach the speeds or waveform required for a classic shockwave.
- Effect: More superficial stimulation, often relying on tissue irritation to induce local blood flow. It can be beneficial for short-term analgesia but is less reliable for deep tissue regeneration, especially in the plantar fascia, adductors, hip, and deep tendons (Sorg et al., 2020).
- Electrohydraulic shockwaves:
- Mechanism: A submerged electrode ignites a plasma bubble; the leading edge of the bubble forms a true shockwave inside the applicator. Energy emerges already at shockwave speed and waveform, penetrating up to ~12 cm depending on settings and tissue properties.
- Benefit: Consistent depth, strong mechanotransduction, and more uniform dosing across the therapeutic column of tissue (Schmitz et al., 2015).
Electromagnetic and Piezoelectric Alternatives: What’s Different
- Both electromagnetic and piezoelectric sources can generate shockwaves, but their sound waves may converge into shockwave form outside the applicator, leaving a gap that requires careful tip selection and positioning for precise targeting (ISMS T guidelines; Schmitz et al., 2015).
- Electrohydraulic energy begins as a shockwave, reducing sensitivity to positioning and providing a broader, more forgiving therapeutic column. This consistency matters in real-world clinics, where anatomy varies, scar tissue is present, and motion is restricted.
Focused Plus Broad-Focus Energy Delivery: Two-for-One Tissue Coverage
In electrohydraulic systems with parabolic reflectors, I utilize both:
- The focused wave: like a laser pointer, ideal for pinpointing lesions (e.g., proximal plantar fascia origin, adductor insertion, enthesopathic changes).
- The broad-focus column: distributes the reflected energy across a larger volume, covering diffuse pathology (e.g., fascial chains, kinetic-chain contributions, and regional interdependencies).
Why It Matters
- Larger therapeutic zones shorten treatment times.
- Less technician dependency: Patient biofeedback—gentle tapping in healthy tissue and heightened sensation over inflamed or damaged areas—guides us to the right spot without surgical precision.
- Greater comfort: Broad dispersion reduces peak discomfort, allowing higher energy without anesthesia.
Patient Outcomes: What Registries and Clinical Data Show
Third-party registries have reported contrasting outcomes among radial pressure waves, focused shockwaves, and electrohydraulic systems.
- Radial: Often effective for short-term pain relief; at ~6 months, many patients report a return to baseline symptoms.
- Focused shockwave: Meaningful pain reduction by ~3 months, with some drift back by ~6 months.
- Electrohydraulic with broad coverage: Sustained reduction in pain scores at 6 months, likely due to deeper, wider mechanotransduction and vascular changes supporting continued remodeling (Schmitz et al., 2015; Meta-analyses: Rompe et al., 2007; Wang, 2012).
Integrative Chiropractic Model: How We Fit Shockwave into Care
We blend shockwave therapy with chiropractic and physical therapy to support the body’s capacity to heal and move.
- Chiropractic adjustments:
- Correct regional joint restrictions contributing to overload of the plantar fascia, adductors, or hip stabilizers.
- Improve kinematic chain alignment—foot-ankle-knee-hip-pelvis-lumbar spine—to redistribute stress away from inflamed tissues.
- Soft tissue techniques:
- Myofascial release and instrument-assisted soft tissue mobilization reduce densification and restore glide between fascial layers.
- Trigger point therapy to deactivate hyperirritable points perpetuating pain.
- Physical therapy:
- Eccentric loading protocols for tendinopathies (e.g., plantar fascia, Achilles, adductors) to stimulate collagen alignment and tendon resilience.
- Neuromuscular re-education for foot intrinsics and hip abductors to improve stability and dynamic control.
- Lifestyle and load management:
- Footwear and orthotics as needed to correct pronation/supination, mechanics.
- Graded return-to-sport plans to avoid reinjury and leverage tissue remodeling windows.
Clinical Physiology: Why These Interventions Work Together
- Shockwave mechanotransduction increases angiogenesis (e.g., VEGF), improving oxygen and nutrient delivery during rehabilitation.
- Adjustments enhance segmental motion and reduce abnormal torque, decreasing repetitive microtrauma.
- Myofascial techniques address fibrosis and improve interstitial fluid flow, supporting the vascular benefits of shockwave therapy.
- Eccentric loading stimulates tenocyte activity and collagen realignment, capitalizing on shockwave’s activation of repair pathways (Wang, 2012).
Case Insight: Plantar Fasciitis Recovery and Long-Term Resilience
My personal case mirrored many patients at El Paso Back Clinic: initial plantar fascia pain responding to shockwave with subsequent delayed but sustained resolution. In the clinic, I see:
- Patients reporting immediate pain relief after the first session due to nociceptive modulation.
- Progressive improvements at 4–8 weeks consistent with vascular remodeling and matrix repair.
- Enhanced durability when combined with foot intrinsic strengthening, hip stabilizer training, and chiropractic alignment work.
Sports Medicine Perspective: Adductor Strain and Return to Play
Professional teams increasingly use shockwave therapy for adductor strains and hip and groin injuries. The immediate benefits include reduced pain and accelerated tissue recovery compared with conventional timelines. In our practice:
- We target the adductor longus origin and the fascial plane along the inner thigh while normalizing pelvic mechanics with sacroiliac and lumbar adjustments.
- We integrate isometric-to-eccentric progressions and adductor-abductor balance training to reduce reinjury risk.
- The combination improves tolerance to sport-specific loads and hastens return to competition.
Bone Edema and Post-Operative Healing: A Non-Invasive Boost
Electrohydraulic shockwave has supportive data in bone marrow edema and delayed union/slow healing states:
- Mechanism: Induction of osteogenic signals (e.g., BMPs), increased neovascularization, and modulation of inflammatory mediators help restore homeostasis in bone and periosteum (Wang, 2012).
- Clinical integration: We use shockwave alongside gentle mobilization and loading strategies, emphasizing safe progression while pain and function improve.
Radial vs. True Shockwave: Setting Patient Expectations
Many patients come in having tried “shockwave” elsewhere—usually radial pressure wave therapy—and feel wary because it was painful or ineffective long term. Education is essential:
- We explain the difference between pressure waves and true shockwaves.
- We demonstrate the biofeedback sensation: mild over healthy tissue, sharper over pathology.
- We emphasize comfort: broader energy distribution allows higher therapeutic levels with better tolerability.
How We Deliver Care: Workflow and Patient Experience
- Session length: 10–15 minutes for shockwave application, integrated into chiropractic and PT visits.
- Immediate feedback: Often, we see same-day reductions in pain, which motivates adherence.
- Training and delegation: The broad focus makes it safe for trained clinical assistants to apply my protocols, maintaining quality and efficiency.
- Billing: Primarily cash-pay, with transparent packages; we discuss any local reimbursement possibilities if applicable.
Our Protocols: Practical Steps and Reasoning
Plantar Fasciitis
- Assessment:
- Foot posture, gait analysis, palpation of proximal fascia, and medial calcaneal tubercle.
- Evaluate kinetic chain: tibial rotation, hip internal rotation, pelvic tilt, lumbar mechanics.
- Shockwave dosing:
- Begin with moderate energy over the plantar fascia origin and along fascial planes.
- Expand to the calf fascia and posterior chain for regional interdependency.
- Chiropractic:
- Midfoot/forefoot adjustments for metatarsal mobility.
- Subtalar and talocrural mobilization to correct pronation mechanics.
- Pelvic and lumbar adjustments to reduce compensatory loading.
- PT:
- Eccentric calf raises, plantar fascia-specific stretches, and foot intrinsics (short-foot exercises).
- Progressive loading; integrate balance and proprioception.
- Rationale:
- Mechanotransduction enhances vascularity and signaling; alignment reduces strain; eccentric loading re-patterns collagen.
Adductor Strains
- Assessment:
- Palpate the adductor origin/insertion, assess pelvic stability, SI joint function, and hip ROM.
- Shockwave:
- Focused pulses at tender points; broad-focus across the adductor fascia and pubic aponeurosis.
- Chiropractic:
- Pelvic alignment, symphysis pubis mobilization when indicated, and lumbosacral mechanics.
- PT:
- Isometrics transitioning to eccentrics; adductor-abductor co-contraction drills; lateral movement patterns.
- Rationale:
- Pain modulation permits earlier activation; vascular changes support remodeling; alignment reduces shear.
Achilles Tendinopathy
- Shockwave:
- Mid-substance and insertion coverage, addressing paratenon and surrounding fascia.
- Chiropractic:
- Talocrural joint mobilization, posterior chain alignment.
- PT:
- Alfredson-style eccentrics, progressive plyometrics, once pain subsides.
- Rationale:
- Shockwave stimulates tenocyte activity; eccentrics align collagen; adjustments correct dorsiflexion mechanics to reduce tendon load.
Bone Edema and Slow-Healing Fractures
- Shockwave:
- Lower frequency, targeted dosing over the affected bone segment while respecting pain thresholds.
- Chiropractic/PT:
- Gentle mobilization for adjacent joints, graded weight-bearing, and circulation-enhancing strategies.
- Rationale:
- Supports osteogenesis and neovascularization; movement aids recovery without overloading.
Integrating Orthobiologics Carefully
While we focus on chiropractic and physical therapy first, shockwave can bridge the gap for patients reluctant to injections. When orthobiologics are warranted:
- Same-day approach:
- Shockwave first to reduce pain and improve tolerance; injection follows under improved comfort.
- Staged approach:
- Shockwave 48–72 hours before injection to enhance perfusion and microenvironment.
- Evidence-building:
- Biofeedback mapping demonstrates lesion localization to the care team and patient, supporting shared decision-making.
Comfort, Tolerance, and Safety
Electrohydraulic systems with broad-focus reflectors allow higher energy dosing with less discomfort:
- Patients describe healthy tissue as gentle tapping.
- Over lesions, they feel a clear but tolerable sensation guiding us to the target.
- We avoid “torture” models—modern protocols prioritize comfort while achieving biologically meaningful dosing.
Real-World Implementation at El Paso Back Clinic
- Training:
- My team and I conduct device education, maintenance, and immediate patient trials so we can start treating day one.
- Ongoing support:
- We continue case reviews, update protocols, and refine integration with chiropractic and PT workflows.
- Marketing:
- We grow organically through patient word-of-mouth, outcome reporting, and community education.
What Patients Can Expect: Timeline and Milestones
- First session:
- Often a reduction in pain scores and improved movement due to nociceptive modulation.
- 2–4 weeks:
- Vascular changes and early remodeling translate into improved function; PT progression intensifies.
- 6–12 weeks:
- Collagen realignment and kinetic-chain improvements make gains more durable; return to sport or work accelerates.
Clinical Observations from My Practice
- Sustained relief in plantar fasciitis with fewer recurrences when we address foot mechanics, hip stability, and load management alongside shockwave.
- Faster return to play in adductor strains when pelvic corrections are included and eccentric programs are supervised.
- Improved tolerance of loading in Achilles and patellar tendinopathies when shockwave precedes progressive rehab blocks.
- Bone marrow edema cases respond well when shockwave is combined with graded load, alignment work, and patient-specific timelines.
Why This Model Works
- We harness the body’s regenerative physiology—mechanotransduction, angiogenesis, osteogenesis—while restoring biomechanical balance through chiropractic adjustments and targeted rehab.
- We keep injections and medications in the background, reserving them for cases that truly need them, and use shockwave to improve the microenvironment for all conservative strategies.
Call to Action: Experience Integrative Recovery
If you are dealing with plantar fasciitis, adductor strains, tendinopathies, or slow-healing injuries, we invite you to visit El Paso Back Clinic. We will evaluate your condition, map painful tissues using biofeedback, align your mechanics, and build a personalized plan that combines true electrohydraulic shockwave, chiropractic care, and physical therapy to help you recover efficiently and sustainably.
References
- Shock wave therapy—principles and indications (Rompe, J. D., et al., 2007). Schmerz.
- Current evidence of shockwave therapy in musculoskeletal disorders (Wang, C. J., 2012). The American Journal of Sports Medicine.
- Recommendations for the appropriate use of extracorporeal shockwave therapy (ESWT) in musculoskeletal disorders (Schmitz, C., et al., 2015). European Journal of Applied Physiology.
- Radial vs. focused ESWT clinical considerations and outcomes (Sorg, H., et al., 2020). Journal of Orthopaedic Research.
- International Society for Medical Shockwave Treatment Guidelines (ISMST, n.d.).
In-text citations
- Mechanotransduction and angiogenesis: (Wang, 2012; Schmitz et al., 2015)
- Focused vs. radial outcomes: (Sorg et al., 2020; Schmitz et al., 2015)
- ESWT indications and efficacy: (Rompe et al., 2007; Wang, 2012; ISMST)
General Disclaimer, Licenses and Board Certifications *
Professional Scope of Practice *
The information herein on "Chiropractic and Shockwave for Injury Relief Benefits" is not intended to replace a one-on-one relationship with a qualified health care professional or licensed physician and is not medical advice. We encourage you to make healthcare decisions based on your research and partnership with a qualified healthcare professional.
Blog Information & Scope Discussions
Welcome to El Paso's Premier Wellness and Injury Care Clinic & Wellness Blog, where Dr. Alex Jimenez, DC, FNP-C, a Multi-State board-certified Family Practice Nurse Practitioner (FNP-BC) and Chiropractor (DC), presents insights on how our multidisciplinary team is dedicated to holistic healing and personalized care. Our practice aligns with evidence-based treatment protocols inspired by integrative medicine principles, similar to those on this site and on our family practice-based chiromed.com site, focusing on naturally restoring health for patients of all ages.
Our areas of multidisciplinary practice include Wellness & Nutrition, Chronic Pain, Personal Injury, Auto Accident Care, Work Injuries, Back Injury, Low Back Pain, Neck Pain, Migraine Headaches, Sports Injuries, Severe Sciatica, Scoliosis, Complex Herniated Discs, Fibromyalgia, Chronic Pain, Complex Injuries, Stress Management, Functional Medicine Treatments, and in-scope care protocols.
Our information scope is multidisciplinary, focusing on musculoskeletal and physical medicine; wellness; contributing etiological viscerosomatic disturbances within clinical presentations; associated somato-visceral reflex clinical dynamics; subluxation complexes; sensitive health issues; and functional medicine articles, topics, and discussions.
We provide and present clinical collaboration with specialists from various disciplines. Each specialist is governed by their professional scope of practice and licensure jurisdiction. We use functional health & wellness protocols to treat and support care for musculoskeletal injuries or disorders.
Our videos, posts, topics, and insights address clinical matters and issues that directly or indirectly relate to our clinical scope of practice.
Our office has made a reasonable effort to provide supportive citations and has identified relevant research studies that support our posts. We provide copies of supporting research studies upon request to regulatory boards and the public.
We understand that we cover matters that require an additional explanation of how they may assist in a particular care plan or treatment protocol; therefore, to discuss the subject matter above further, please feel free to ask Dr. Alex Jimenez, DC, APRN, FNP-BC, or contact us at 915-850-0900.
We are here to help you and your family.
Blessings
Dr. Alex Jimenez, DC, MSACP, APRN, FNP-BC*, CCST, IFMCP, CFMP, ATN
email: coach@elpasofunctionalmedicine.com
Multidisciplinary Licensing & Board Certifications:
Licensed as a Doctor of Chiropractic (DC) in Texas & New Mexico*
Texas DC License #: TX5807, Verified: TX5807
New Mexico DC License #: NM-DC2182, Verified: NM-DC2182
Multi-State Advanced Practice Registered Nurse (APRN*) in Texas & Multi-States
Multi-state Compact APRN License by Endorsement (42 States)
Texas APRN License #: 1191402, Verified: 1191402 *
Florida APRN License #: 11043890, Verified: APRN11043890 *
Colorado License #: C-APN.0105610-C-NP, Verified: C-APN.0105610-C-NP
New York License #: N25929, Verified N25929
License Verification Link: Nursys License Verifier
* Prescriptive Authority Authorized
ANCC FNP-BC: Board Certified Nurse Practitioner*
Compact Status: Multi-State License: Authorized to Practice in 40 States*
Graduate with Honors: ICHS: MSN-FNP (Family Nurse Practitioner Program)
Degree Granted. Master's in Family Practice MSN Diploma (Cum Laude)
Dr. Alex Jimenez, DC, APRN, FNP-BC*, CFMP, IFMCP, ATN, CCST
(Board Certified: Family Practice Nurse Practitioner—Multistate)*
(Licensed Nurse Practitioner & Chiropractor - Multistate)*
Clinical Director
Digital Business Card
Dr. Maria Cardenas, MD
(Board Certified: Internal Medicine)
(Licensed Medical Doctor)
Medical Director, Clinical Director & Collaborative Physician
NPI # 1164426749
MD License #: J2933
Licenses and Board Certifications:
MD: Medical Doctor
DC: Doctor of Chiropractic
APRNP: Advanced Practice Registered Nurse
FNP-BC: Family Practice Specialization (Multi-State Board Certified)
RN: Registered Nurse (Multi-State Compact License)
CFMP: Certified Functional Medicine Provider
MSN-FNP: Master of Science in Family Practice Medicine
MSACP: Master of Science in Advanced Clinical Practice
IFMCP: Institute of Functional Medicine
CCST: Certified Chiropractic Spinal Trauma
ATN: Advanced Translational Neutrogenomics
Memberships & Associations:
TCA: Texas Chiropractic Association: Member ID: 104311
AANP: American Association of Nurse Practitioners: Member ID: 2198960
ANA: American Nurse Association: Member ID: 06458222 (District TX01)
TNA: Texas Nurse Association: Member ID: 06458222
NPI: 1205907805
National Provider Identifier
| Primary Taxonomy |
Selected Taxonomy |
State |
License Number |
| No |
111N00000X - Chiropractor |
NM |
DC2182 |
| Yes |
111N00000X - Chiropractor |
TX |
DC5807 |
| Yes |
363LF0000X - Nurse Practitioner - Family |
TX |
1191402 |
| Yes |
363LF0000X - Nurse Practitioner - Family |
FL |
11043890 |
| Yes |
363LF0000X - Nurse Practitioner - Family |
CO |
C-APN.0105610-C-NP |
| Yes |
363LF0000X - Nurse Practitioner - Family |
NY |
N25929 |
Dr. Alex Jimenez, DC, APRN, FNP-BC*, CFMP, IFMCP, ATN, CCST
(Board Certified: Family Practice Nurse Practitioner—Multistate)*
(Licensed Nurse Practitioner & Chiropractor - Multistate)*
Clinical Director
Digital Business Card
Dr. Maria Cardenas, MD
(Board Certified: Internal Medicine)*
(Licensed Medical Doctor)*
Medical Director, Clinical Director & Collaborative Physician
NPI # 1164426749
MD License #: J2933
{kind=link}