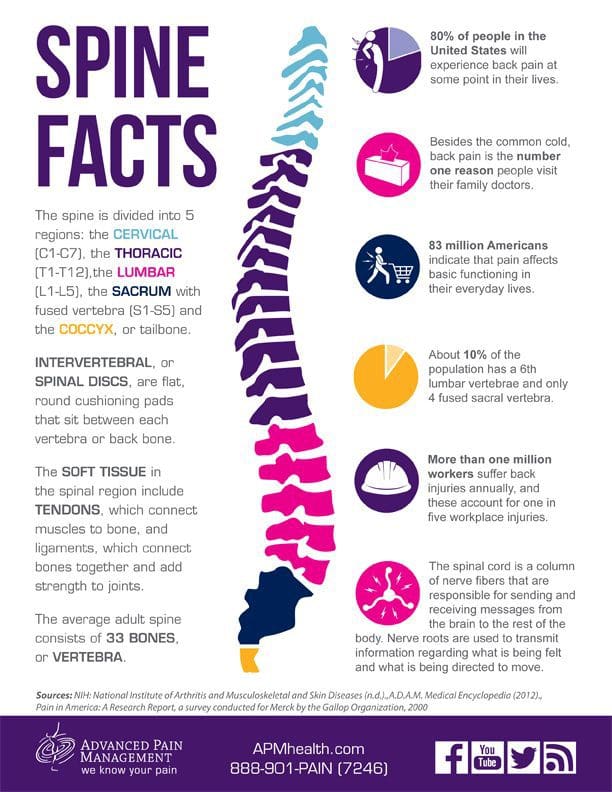
The spinal cord and brain make up the central nervous system while the spinal nerves that branch to the spinal cord and cranial nerves that branch to the brain makes up the peripheral nervous system.
There are thirty-one sets of nerves that extend out of the spinal cord and are connected to it by the nerve root. Each nerve branches out about a half inch from the spinal cord before dividing into smaller branches. The dorsal rami are on the posterior side of the branch while the larger ventral rami are on the anterior side.
The dorsal rami provide nerve function for the skin of the trunk and posterior muscles. The ventral rami from T1 to T12 provide nerve function to the skin of the trunk as well as the lateral and anterior muscles. The anterior divisions that remain for plexuses, networks that provide nerve function to the body. Each plexus has specific areas on the body for skin sensitivity as well as certain muscles. Their point where they exit the spine determines how they are numbered. The four primary plexuses are:
Cervical plexus, C1 � C4, innervates the diaphragm, shoulder, and neck
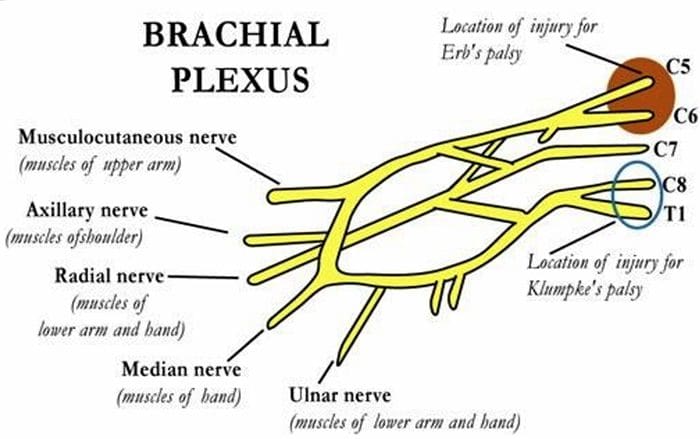
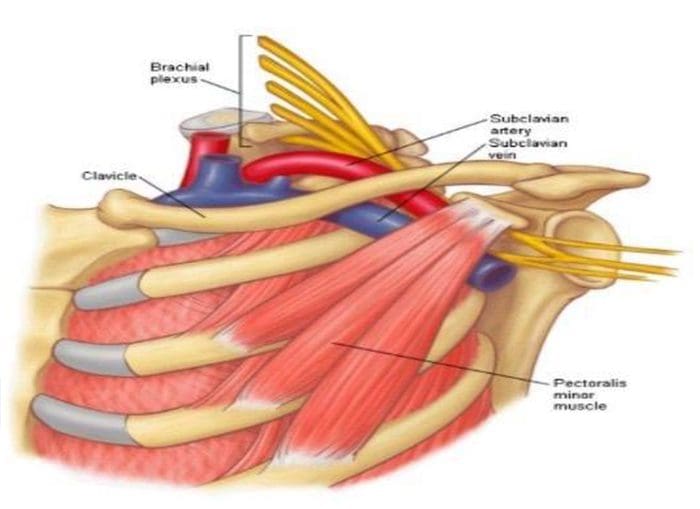
Brachial plexus, C5 � T1, innervates the upper limbs
Lumbar plexus, T12/L1 � L4, innervates the thigh
Sacral plexus, L4 � S4, innervates the leg and foot.
These spinal nerves have two sets of fibers: motor and sensory. Motor fibers facilitate movement and provide nerve function to the muscles. Sensory fibers facilitate sensitivities to touch, temperature and other stimuli. They provide nerve function to the skin.
What are Myotomes and Dermatomes?
A group of muscles that are innervated by the motor fibers that stem from a specific nerve root is called a myotome. An area of the skin that is innervated by the sensory fibers that stem from a specific nerve root is called a dermatome. These patterns of myotome and dermatome are almost always identical from person to person. There are occasionally variances, but that is rare.
This consistency allows doctors to treat nerve pain in patients. If a specific area is hurting, they know that it is attributed to a certain myotome or dermatome, whichever the case may be, and its corresponding nerve root. Problems with nerve damage are often the result of stretching the nerve or compressing it.
When the nerves are injured in specific areas like the lumbosacral or brachial plexus, it presents as sensory and motor deficits in the limbs that correspond to them. Myotomes and dermatomes are used to assess the extent of the damage.
How are Myotomes and Dermatomes used to Assess Nerve Damage?
When a doctor tests for nerve root damage in a patient, he or she will often test the myotomes or dermatomes for the nerves assigned to that location. A dermatome is examined for abnormal sensation, such as hypersensitivity or lack of sensitivity.
This is done by using stimulus inducing tools such as a pen, paper clip, pinwheel, fingernails, cotton ball, or pads of the fingers. The patient is instructed to provide feedback regarding their response. Some of the abnormal sensation responses include:
A myotome is tested for nerve damage in the muscles which presents as muscle weakness. This grading scale, which assigns a rating to the degree of muscle weakness, is often used:
5 � Normal � Complete range of motion against gravity with full resistance
4 � Good � Complete range of motion against gravity with some resistance
3 � Fair � Complete range of motion against gravity with no resistance, active ROM
2 � Poor � Complete range of motion with some assistance and gravity eliminated
1 � Trace � Evidence of slight muscular contraction, no joint motion evident
0 � Zero � No evidence of muscle contraction
During a typical chiropractic exam, your chiropractor will assess both dermatomes and myotomes for potential neurological problems. This gives them additional insight on how to treat your condition, whether it’s related to a subluxation of vertebral bodies or other, other disease processes.
Origin: The most common cause of�migraines/headaches�can relate to neck complications. From spending excessive time looking down at a laptop, desktop, iPad, and even from constant texting, an incorrect posture for extended periods of time can begin to place pressure on the neck and upper back leading to problems that can cause headaches. The majority of these type of headaches occurs as a result of tightness between the shoulder blades, which in turn causes the muscles on the top of the shoulders to also tighten and radiate pain into the head.
Arteriovenous malformations and expanding aneurysms
Lupus cerebritis
Venous sinus thrombosis
Cervical fracture or malformation
Fracture or dislocation
Occipital neuralgia
Vertebral artery dissection
Chiari malformation
Metabolic
Hypoglycemia
Hypercapnea
Carbon monoxide
Anoxia
Anemia
Vitamin A toxicity
Glaucoma
Subarachnoid Hemorrhage
Usually due to ruptured aneurysm
Sudden onset of severe pain
Often vomiting
Patient appears ill
Often nuchal rigidity
Refer for CT and possibly lumbar puncture
Meningitis
Patient appears ill
Fever
Nuchal rigidity (except in elderly and young children)
Refer for lumbar puncture – diagnostic
Neoplasms
Unlikely cause of HA in average patient population
Mild and nonspecific head pain
Worse in the morning
May be elicited by vigorous head shaking
If focal symptoms, seizures, focal neurologic signs, or evidence of increased intracranial pressure are present rule our neoplasm
Subdural Or Epidural Hemorrhage
Due to hypertension, trauma or defects in coagulation
Most often occurs in the context of acute head trauma
Onset of symptoms may be weeks or months after an injury
Differentiate from the common post-concussion headache
Post-Concussive HA may persist for weeks or months after an injury and be accompanied by dizziness or vertigo and mild mental changes, which will all subside
Exquisite tenderness and/or swelling over the temporal or occipital arteries
Evidence of arterial insufficiency in the distribution of branches of the cranial vessels
High ESR
Cervical Region HA
Neck trauma or with symptoms or signs of cervical root or cord compression
Order MR or CT cord compression due to fracture or dislocation
Cervical instability
Order cervical spine x-rays lateral flexion and extension views
Ruling Out Dangerous HA
Rule our history of serious head or neck injury, seizures or focal neurologic symptoms, and infections that may predispose to meningitis or brain abscess
Check for fever
Measure blood pressure (concern if diastolic >120)
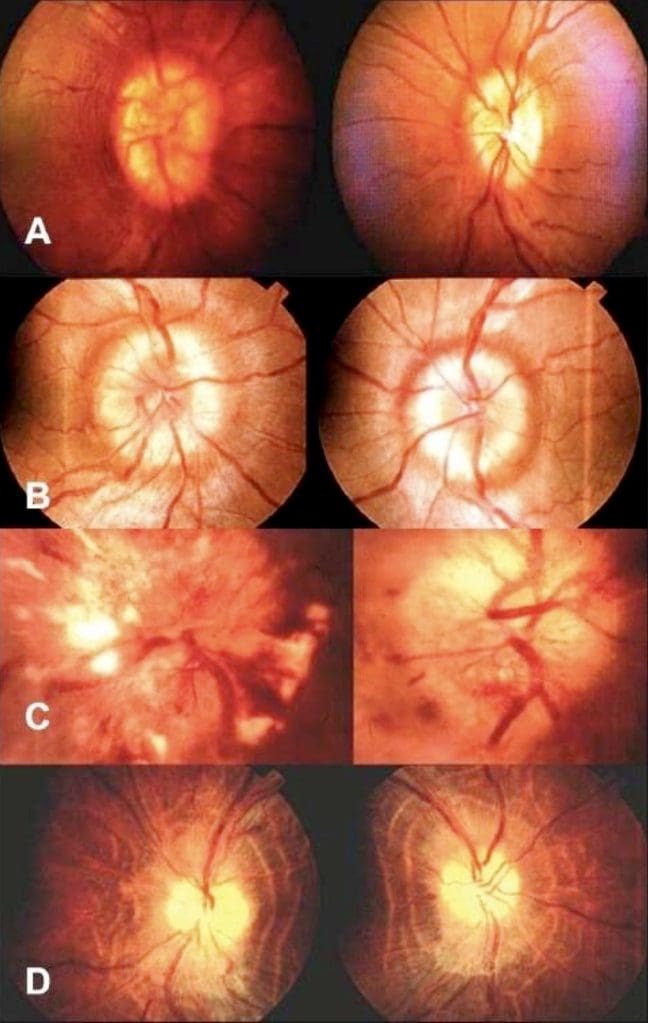
Ophthalmoscopic exam
Check neck for rigidity
Auscultate for cranial bruits.
Complete neurologic examination
If needed order complete blood cell count, ESR, cranial or cervical imaging
Episodic Or Chronic?
<15 days per month = Episodic
>15 days per month = Chronic
Migraine HA
Generally due to dilation or distension of cerebral vasculature
Serotonin In Migraine
AKA 5-hydroxytryptamine (5-HT)
Serotonin becomes depleted in migraine episodes
IV 5-HT can stop or reduce severity
Migraine With Aura
History of at least 2 attacks fulfilling the following criteria
One of the following fully reversible aura symptoms:
Visual
Somatic sensory
Speech or language difficulty
Motor
Brain stem
2 of the following 4 characteristics:
1 aura symptom spreads gradually over ?5 min, and/or 2 symptoms occur in succession
Each individual aura symptom lasts 5-60 min
1 aura symptom is unilateral
Aura accompanied or followed in <60 min by headache
Not better accounted for by another ICHD-3 diagnosis, and TIA excluded
Migraine Without Aura
History of at least 5 attacks fulfilling the following criteria:
Headache attacks lasting 4-72 h (untreated or unsuccessfully treated)
Unilateral pain
Pulsing/pounding quality
Moderate to severe pain intensity
Aggravation by or causing avoidance of routine physical activity
During headache nausea and/or sensitivity to light and sound
Not better accounted for by another ICHD-3 diagnosis
Cluster Headache
Severe unilateral orbital, supraorbital and/or temporal pain
�Like an ice pick stabbing me the eye�
Pain lasts 15-180 minutes
At least one of the following on the side of headache:
Conjunctival injection
Facial sweating
Lacrimation
Miosis
Nasal congestion
Ptosis
Rhinorrhea
Eyelid edema
History of similar headaches in the past
Tension Headache
Headache pain accompanied by two of the following:
Pressing/tightening (non-pulsing) quality
�Feels like a band around my head�
Bilateral location
Not aggravated by routine physical activity
Headache should be lacking:
Nausea or vomiting
Photophobia and phonophobia (one or the other may be present)
History of similar headaches in the past
Rebound Headache
Headache occurring on ?15 days a month in a patient with a pre-existing headache disorder
Regular overuse for >3 months of one or more drugs that can be taken for acute and/or symptomatic treatment of headache
Due to medication overuse/withdrawal
Not better accounted for by another ICHD-3 diagnosis
Sources
Alexander G. Reeves, A. & Swenson, R. Disorders of the Nervous System. Dartmouth, 2004.
The rule of 4 of the brainstem: a simplified method for understanding brainstem anatomy and brainstem vascular
syndromes for the non-neurologist.
The Rule Of 4 & The Brainstem
The rule of 4 is a simple method developed to help �students of neurology� to remember the anatomy of the brainstem and thus the features of the various brainstem vascular syndromes. As medical students, we are taught detailed anatomy of the brainstem containing a bewildering number of structures with curious names such as superior colliculi, inferior olives, various cranial nerve nuclei and the median longitudinal fasciculus. In reality when we do a neurological examination we test for only a few of these structures. The rule of 4 recognizes this and only describes the parts of the brainstem that we actually examine when doing a neurological examination. The blood supply of the brainstem is such that there are paramedian branches and long circumferential branches (the anterior inferior cerebellar artery (AICA), the posterior inferior cerebellar artery (PICA) and the superior cerebellar artery (SCA). Occlusion of the paramedian branches results in medial (or paramedian) brainstem syndromes and occlusion of the circumferential branches results in lateral brainstem syndromes. Occasionally lateral brainstem syndromes are seen in unilateral vertebral occlusion. This paper describes a simple technique to aid in the understanding of brainstem vascular syndromes.
Any attempt to over simplify things runs the risk of upsetting those who like detail and I apologize in advance to the anatomists among us, but for more than 15 years this simple concept has helped numerous students and residents understand, often for the first time, brainstem anatomy and the associated clinical syndromes that result.
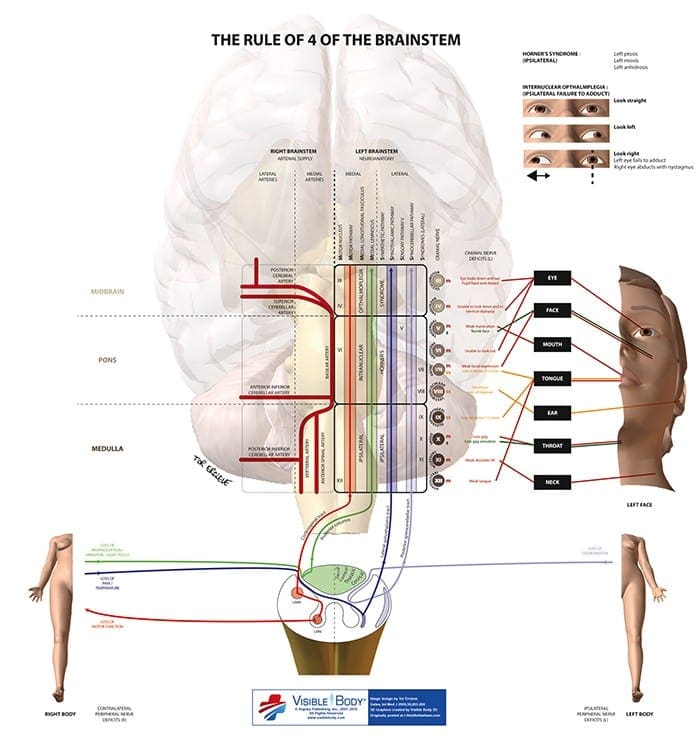
In The Rule Of 4 There Are 4 Rules:
There are 4 structures in the �midline� beginning with M.
There are 4 structures to the side beginning with S.
There are 4 cranial nerves in the medulla, 4 in the pons and 4 above the pons (2 in the midbrain).
The 4 motor nuclei that are in the midline are those that divide equally into 12 except for 1 and 2, that is 3, 4, 6 and 12 (5, 7, 9 and 11 are in the lateral brainstem).
If you can remember these rules and know how to examine the nervous system, in particular the cranial nerves, then you will be able to diagnose brainstem vascular syndromes with ease.
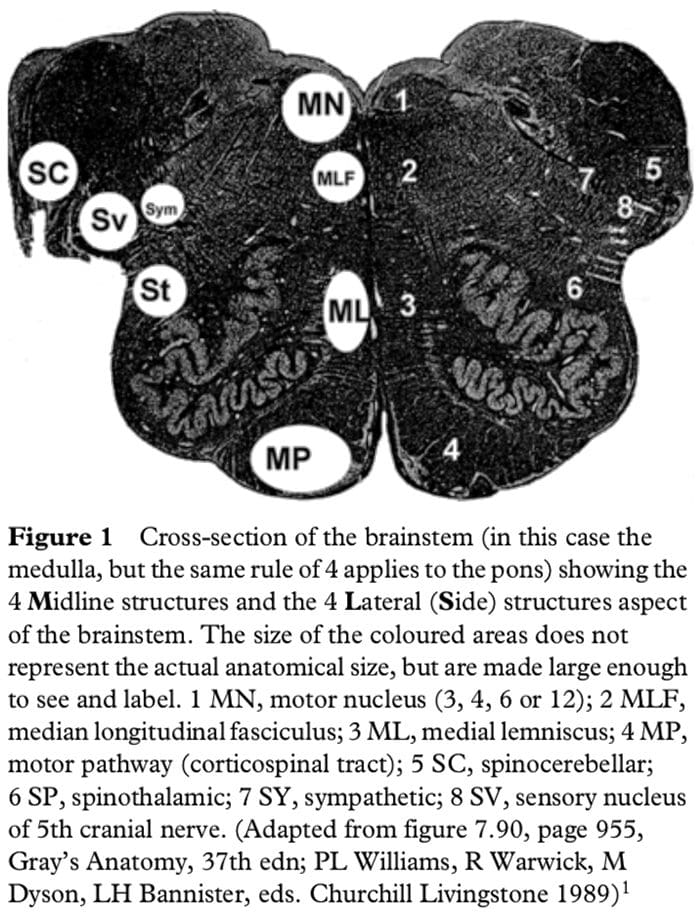
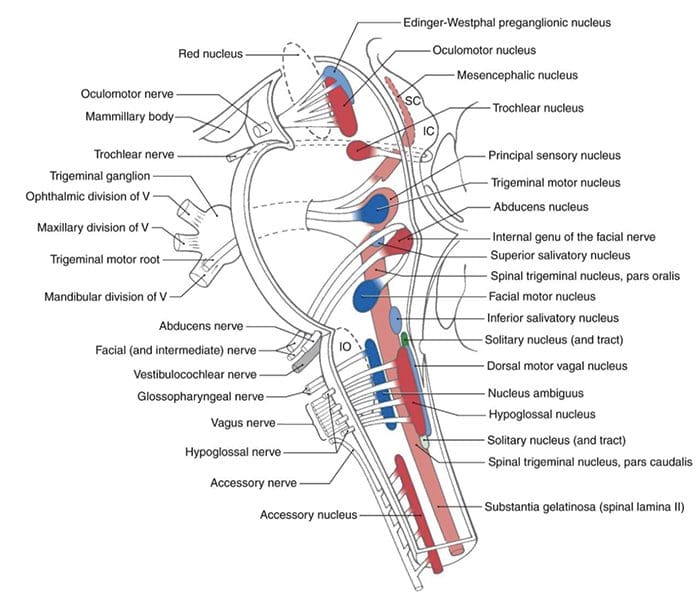
Figure 1 shows a cross-section of the brainstem, in this case at the level of the medulla, but the concept of 4 lateral and 4 medial structures also applies to the pons, only the 4 medial structures relate to midbrain vascular syndromes.
The 4 Medial Structures & The Associated Deficit Are:
The Motor pathway (or corticospinal tract): contra lateral weakness of the arm and leg.
The Medial Lemniscus: contra lateral loss of vibration and proprioception in the arm and leg.
The Medial longitudinal fasciculus: ipsilateral inter- nuclear ophthalmoplegia (failure of adduction of the ipsilateral eye towards the nose and nystagmus in the opposite eye as it looks laterally).
The Motor nucleus and nerve: ipsilateral loss of the cranial nerve that is affected (3, 4, 6 or 12).
The 4 Lateral Structures & The Associated Deficit Are:
The Spinocerebellar pathways: ipsilateral ataxia of the arm and leg.
The Spinothalamic pathway: contra lateral alteration of pain and temperature affecting the arm, leg and rarely the trunk.
The Sensory nucleus of the 5th: ipsilateral alteration of pain and temperature on the face in the distribution of the 5th cranial nerve (this nucleus is a long vertical structure that extends in the lateral aspect of the pons down into the medulla).
The Sympathetic pathway: ipsilateral Horner�s syndrome, that is partial ptosis and a small pupil (miosis)
These pathways pass through the entire length of the brainstem and can be likened to �meridians of longitude� whereas the various cranial nerves can be regarded as �parallels of latitude�. If you establish where the meridians of longitude and parallels of latitude intersect then you have established the site of the lesion.
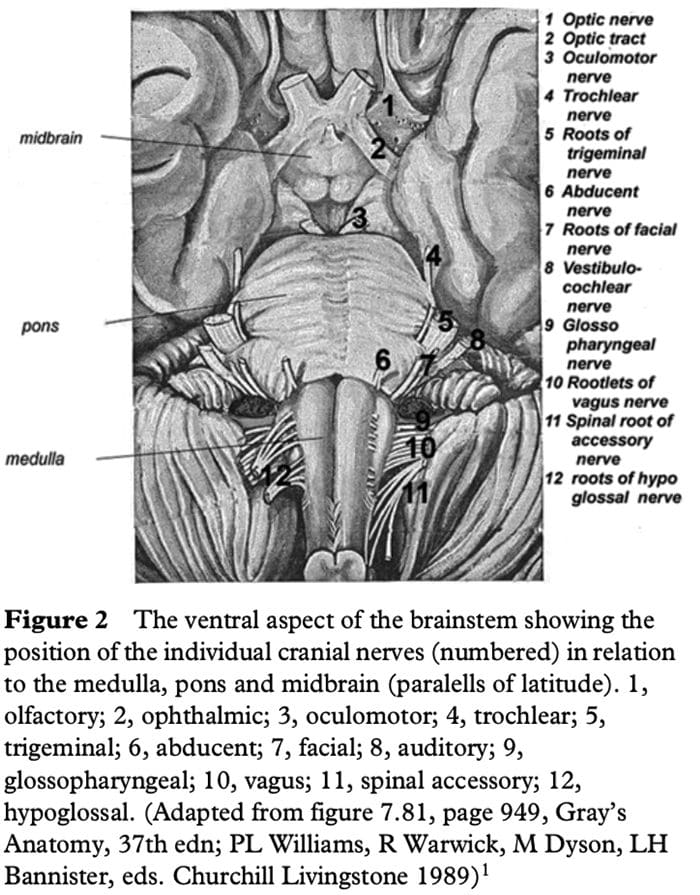
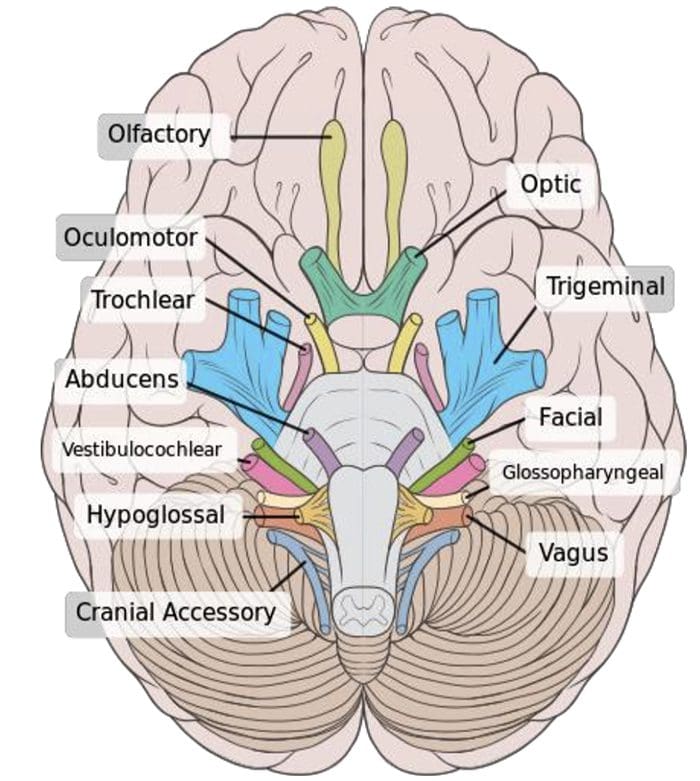
Figure 2 shows the ventral aspect of the brainstem.
The 4 Cranial Nerves In The Medulla Are:
9 Glossopharyngeal: ipsilateral loss of pharyngeal sensation. 10 Vagus: ipsilateral palatal weakness. 11 Spinal accessory: ipsilateral weakness of the trapezius and sternocleidomastoid muscles. 12 Hypoglossal: ipsilateral weakness of the tongue.
The 12th cranial nerve is the motor nerve in the midline of the medulla. Although the 9th, 10th and 11th cranial nerves have motor components, they do not divide evenly into 12 (using our rule) and are thus not the medial motor nerves.
The 4 Cranial Nerves In The Pons Are:
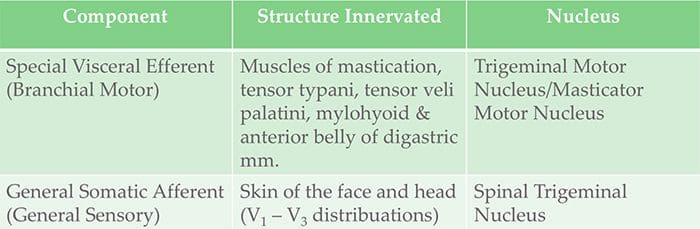
5 Trigeminal: ipsilateral alteration of pain, temperature and light touch on the face back as far as the anterior two-thirds of the scalp and sparing the angle of the jaw. 6 Abducent: ipsilateral weakness of abduction (lateral movement) of the eye. 7 Facial: ipsilateral facial weakness. 8 Auditory: ipsilateral deafness.
The 6th cranial nerve is the motor nerve in the pons.
The 7th is a motor nerve but it also carries pathways of taste, and using the rule of 4 it does not divide equally in to 12 and thus it is not a motor nerve that is in the midline. The vestibular portion of the 8th nerve is not included in order to keep the concept simple and to avoid confusion. Nausea and vomiting and vertigo are often more common with involvement of the vestibular connections in the lateral medulla.
The 4 Cranial Nerves Above The Pons Are:
4 Olfactory: not in midbrain. 5 Optic: not in midbrain. 6 Oculomotor: impaired adduction, supraduction and infraduction of the ipsilateral eye with or without a dilated pupil. The eye is turned out and slightly down. 7 Trochlear: eye unable to look down when the eye is looking in towards the nose.
The 3rd and 4th cranial nerves are the motor nerves in the midbrain.
Thus a medial brainstem syndrome will consist of the 4 M�s and the relevant motor cranial nerve, and a lateral brainstem syndrome will consist of the 4 S�sand either the 9�11th cranial nerve if in the medulla, or the 5th, 7th and 8th cranial nerve if in the pons.
MEDIAL (PARAMEDIAN) BRAINSTEM SYNDROMES
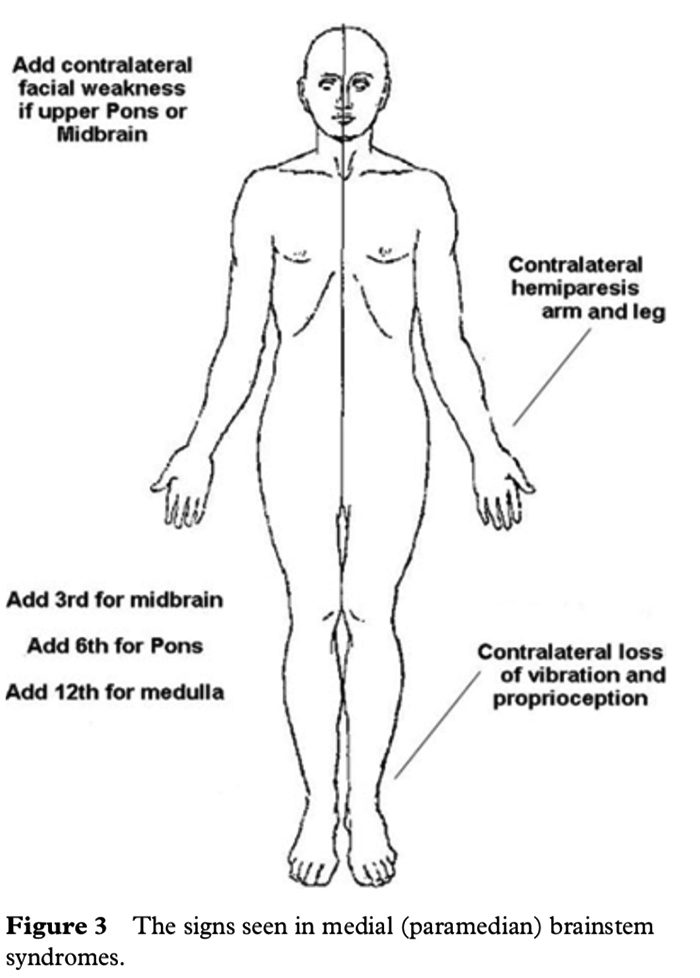
Let us assume that the patient you are examining has a brainstem stroke. If you find upper motor neurone signs in the arm and the leg on one side then you know the patient has a medial brainstem syndrome because the motor pathways is paramedian and crosses at the level of the foramen magnum (decussation of the pyramids). The involvement of the motor pathway is the �meridian of longitude�. So far the lesion could be anywhere in the medial aspect of the brainstem, although if the face is also affected it has to be above the mid pons, the level where the 7th nerve nucleus is.
The motor cranial nerve �the parallels of latitude� indicates whether the lesion is in the medulla (12th), pons (6th) or midbrain (3rd). Remember the cranial nerve palsy will be ipsilateral to the side of the lesion and the hemiparesis will be contralateral. If the medial lemniscus is also affected then you will find a contra lateral loss of vibration and proprioception in the arm and leg (the same side affected by the hemiparesis) as the posterior columns also cross at or just above the level of the foramen magnum. The median longitudinal fasciculus (MLF) is usually not affected when there is a hemiparesis as the MLF is further back in the brainstem.
The MLF can be affected in isolation �a lacunar infarct� and this results in an ipsilateral internuclear ophthalmoplegia, with failure of adduction (movement towards the nose) of the ipsilateral eye and leading eye nystagmus on looking laterally to the opposite side of the lesion in the contra lateral eye. If the patient had involvement of the left MLF then, on being asked to look to the left, the eye movements would be normal, but on looking to the right the left eye would not go past the midline, while there would be nystagmus in the right eye as it looked to the right.
Figure 3 shows the clinical features of the medial brainstem syndromes.
LATERAL BRAINSTEM SYNDROMES
Once again we are assuming that the patient you are seeing has a brainstem problem, most likely a vascular lesion. The 4 S�s or �meridians of longitude� will indicate that you are dealing with a lateral brainstem problem and the cranial nerves or �parallels of latitude� will indicate whether the problem is in the lateral medulla or lateral pons.
A lateral brainstem infarct will result in ipsilateral ataxia of the arm and leg as a result of involvement of the Spinocerebellar pathways, contralateral alteration of pain and temperature sensation as a result of involvement of the Spinothalamic pathway, ipsilateral loss of pain and temperature sensation affecting the face within the distribution of the Sensory nucleus of the trigeminal nerve (light touch may also be affected with involvement of the spinothalamic pathway and/or sensory nucleus of the trigeminal nerve). An ipsilateral Horner�s syndrome with partial ptosis and a small pupil (miosis) is because of involvement of the Sympathetic pathway. The power tone and the reflexes should all be normal. So far all we have done is localize the problem to the lateral aspect of the brainstem; by adding the relevant 3 cranial nerves in the medulla or the pons we can localize the lesion to this region of the brain.
The lower 4 cranial nerves are in the medulla and the 12th nerve is in the midline so that 9th, 10th and 11th nerves will be in the lateral aspect of the medulla. When these are affected, the result is dysarthria and dysphagia with an ipsilateral impairment of the gag reflex and the palate will pull up to the opposite side; occasionally there may be weakness of the ipsilateral trapezius and/or sternocleidomastoid muscle. This is the lateral medullary syndrome usually resulting from occlusion of the ipsilateral vertebral or posterior inferior cerebellar arteries.
The 4 cranial nerves in the pons are: 5th, 6th, 7th and 8th. The 6th nerve is the motor nerve in the midline, the 5th, 7th and 8th are in the lateral aspect of the pons, and when these are affected there will be ipsilateral facial weakness, weakness of the ipsilateral masseter and pterygoid muscles (muscles that open and close the mouth) and occasionally ipsilateral deafness. A tumour such as an acoustic neuroma in the cerebello-pontine angle will result in ipsilateral deafness, facial weakness and impairment of facial sensation; there may also be ipsilateral limb ataxia if it compresses the ipsilateral cerebellum or brainstem. The sympathetic pathway is usually too deep to be affected.
If there are signs of both a lateral and a medial (paramedian) brainstem syndrome, then one needs to consider a basilar artery problem, possibly an occlusion.
In summary, if one can remember that there are 4 pathways in the midline commencing with the letter M, 4 pathways in the lateral aspect of the brainstem commencing with the letter S, the lower 4 cranial nerves are in the medulla, the middle 4 cranial nerves in the pons and the first 4 cranial nerves above the pons with the 3rd and 4th in the midbrain, and that the 4 motor nerves that are in the midline are the 4 that divide evenly into 12 except for 1 and 2, that is 3, 4, 6 and 12, then it will be possible to diagnose brainstem vascular syndromes with pinpoint accuracy.
P. GATES
The Geelong Hospital, Barwon Health, Geelong, Victoria, Australia
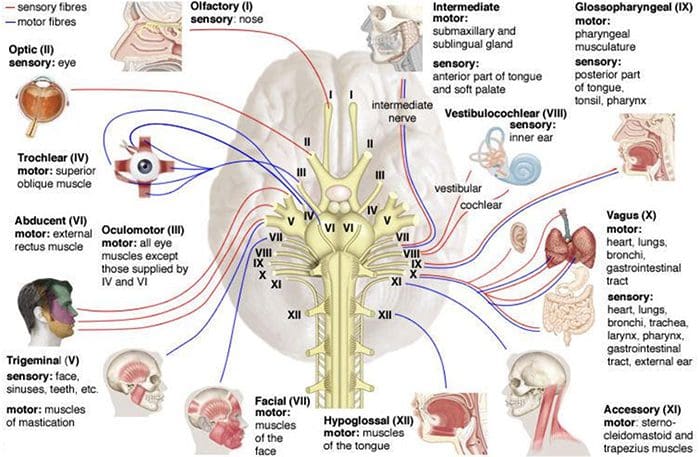
Human Cranial nerves are a set of 12 paired nerves that come directly from the brain. The first two (olfactory and optic) come from the cerebrum, with the remaining ten come from the brain stem. The names of the these nerves relate to what function they perform and are also numerically identified in roman numerals (I-XII).�The�nerves serve in functions of smell, sight, eye movement, and feeling in the face. These�nerves also control balance, hearing, and swallowing.
As with all nerves, symptoms describe the location of the lesion
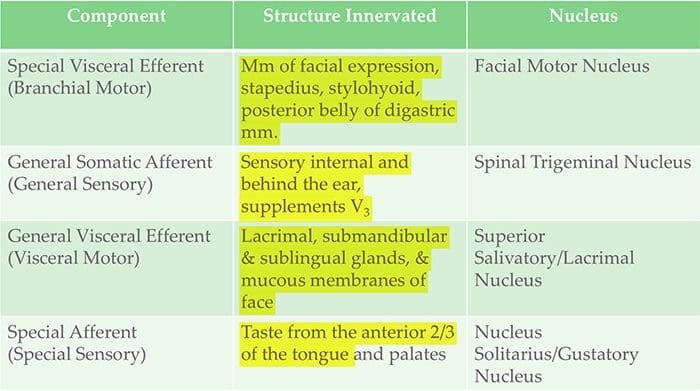
Lesion in the lingual nerve will result in loss of taste, general sensation in tongue & salivary secretion
Lesion proximal to the branching of the chorda tympani such as in the facial canal will result in the same symptoms without the loss of general sensation of the tongue (because V3 has not yet joined the CN VII)
Corticobulbar innervation is asymmetric to the upper and lower parts of the Facial Motor Nucleus
If there is an UMN lesion (lesion to the corticobulbar fibers) the patient will have paralysis of the muscles of facial expression in the contralateral lower quadrant
If there is a LMN lesion (lesion to the facial nerve itself) the patient will have paralysis of the muscles of facial expression in the ipsilateral half of the face
Bell�s Palsy
Testing Cranial Nerve CN VII
Ask the patient to mimic you or follow instructions to make certain facial expressions
Be sure to assess all four quadrants of the face
Raise eyebrows
Puff cheeks
Smile
Close eyes tightly
Check for strength of the buccinator muscle against resistance
Ask patient to hold air in their cheeks as you press gently from the outside
Patient should be able to hold air in against resistance
Cranial Nerve VIII – Vestibulocochlear
Cranial Nerve VIII Clinically
Changes in hearing alone are most often due to
Infections (otitis media)
Skull fracture
The most common lesion to this nerve is caused by an acoustic neuroma
This affects CN VII and CNVIII (cochlear AND vestibular divisions) due to proximity in the internal auditory meatus
Symptoms include nausea, vomiting, dizziness, hearing loss, tinnitus, and bell�s palsy etc.
Testing Cranial Nerve CN VIII
Otoscopic Exam
Scratch Test
Can the patient hear equally on both sides?
Weber Test
Tests for lateralization
256 Hz tuning fork placed on top of the patient�s head in the center, is it louder on one side than the other?
Rinne Test
Compares air conduction to bone conduction
Normally, air conduction should last 1.5-2 as long as bone conduction
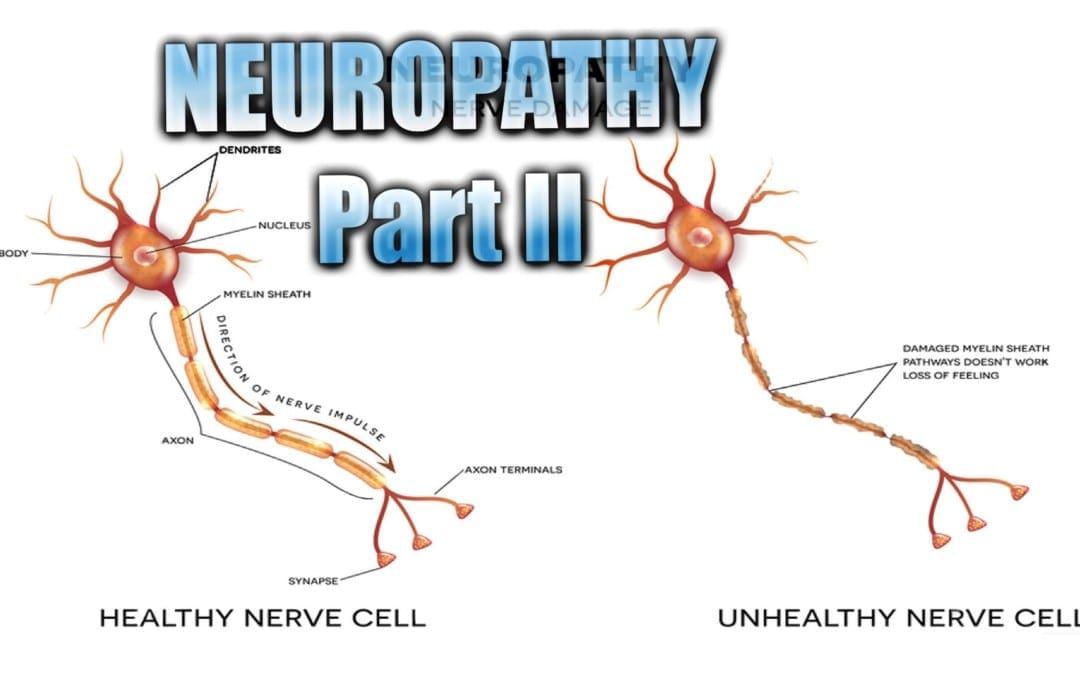
Neuropathy Presentation II:�El Paso, TX. Chiropractor, Dr. Alexander Jimenez�continues the overview with neuropathy part II. Continued are the most common neuropathies to be seen in practice. Because the human body is composed of many different kinds of nerves which perform different functions, nerve damage is classified into several types. Neuropathy can also be classified according to the location of the nerves being affected and according to the disease causing it. For instance, neuropathy caused by diabetes is called diabetic neuropathy. Furthermore, depending on which nerves are affected will depend on the symptoms that will manifest. The complications which follow neuropathy depends on the type of nerves that are damaged. According to Dr. Jimenez, different neuropathies can cause numbness and/or tingling sensations, increased pain or the loss of ability to feel pain, muscle weakness along with twitching and cramps, even dizziness and/or loss of bladder control function.
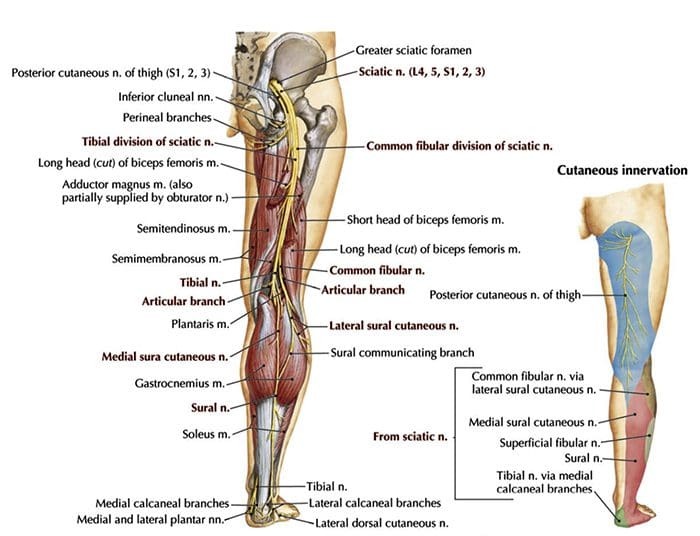
Sciatic Nerve Entrapment
Piriformis Syndrome
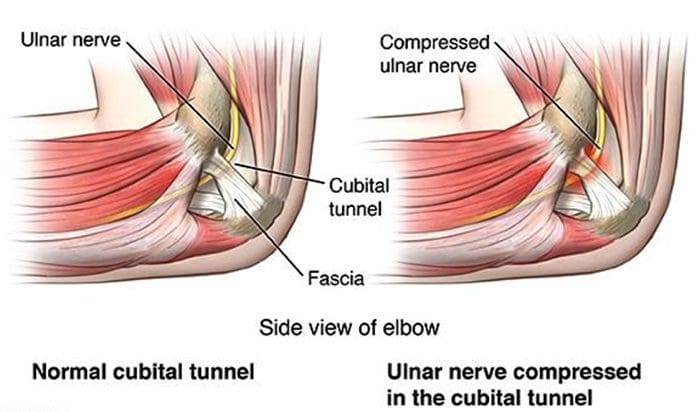
Peroneal Nerve Entrapment
Tarsal Tunnel Syndrome
Sciatic N. Piriformis Syndrome
Causes
Anatomic variation
Piriformis overuse/tension
Exam
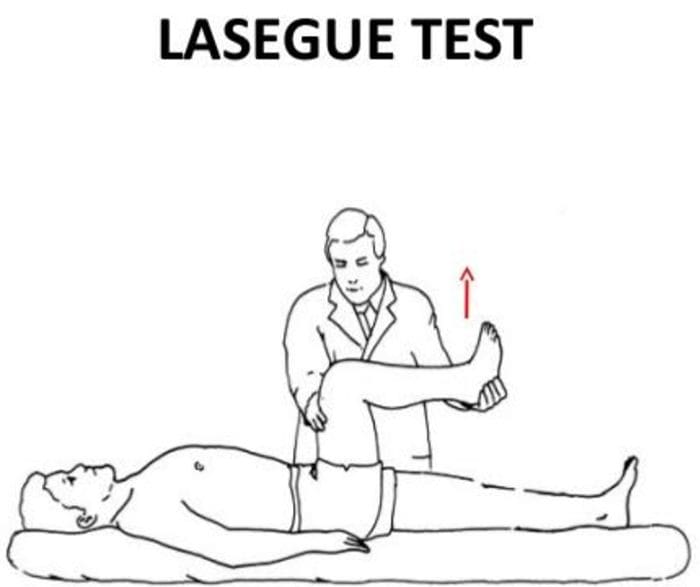
Positive Lase?gue test possible
Doctor extends patient�s leg passively, while patient is lying supine positive test if maneuver is limited by pain
Tenderness and palpable tension in piriformis muscle which elicits symptoms
Sciatic N. Peroneal Nerve Entrapment
Peroneal or Fibular branch of Sciatic nerve entrapped at the fibular head
Tinel�s sign may be present at fibular head/neck
Usually affects common peroneal nerve, therefore motor and sensory symptoms can be seen
Weakness of ankle dorsiflexion and eversion (tibialis anterior m.)
Sensory disruption on the dorsum of the foot and lateral aspect of the calf
Sciatic N. Tarsal Tunnel Syndrome
Tibial nerve impinged in the tarsal tunnel
Sensory changes in the sole of the foot
Tinel�s sign may be present with percussion posterior to the medial malleolus
Radiculopathy
A mononeuropathy � located in one specific area
Neuropathy involving spinal nerve roots
Presents as changes in sensory and/or motor function affecting a single or a few nerve root level(s)
Nerve sheath tumors (schwannomas and neurofibromas)
Guillain-Barre? syndrome
Herpes Zoster (shingles)
Lyme disease
Cytomegalovirus
Myxedema/Thyroid disorder
Idiopathic neuritis
Narrowing Down Common Causes Of Radiculopathy
Disc Herniation
Most commonly affected nerve roots are C6, C7, L5 & S1
Spinal Stenosis
Lumbar stenosis may produce neurogenic claudication
Pain & weakness with ambulation
Cervical stenosis may present with mixed picture of radiculopathy and myelopathy due to long tract involvement
Trauma
May cause compression, trauma or avulsion of the nerve roots
Diabetes
More likely to cause a polyneuropathy, but mononeuropathy is possible
Herpes Zoster (Shingles)
Most often on the trunk, accompanied by vesicular lesions in a single dermatome
If pain persits past vesicular regression = post-herpetic neuralgia
Patient History Of Radiculopathy
The patient will often complain of burning pain or tingling that radiates or shoots down an affected area in a dermatomal pattern.
Sometimes patient will complain of motor weakness, however if onset is recent, there is often no motor involvement
Exam Of Radiculopathy
Most often hypoesthesia in the affected dermatome level
Best to evaluate for pain, as light touch can be difficult for these patient�s to distinguish
Fasciculations and/or atrophy may be seen if radiculopathy is chronic, due to lower motor neuron being impinged
Motor weakness may be seen in muscles innervated by the same root level
Orthopedic tests:
Straight-leg raise test (SLR)
Pain between 10-60 degrees likely indicates nerve root compression
Well-leg raise/Crossed straight-leg raise test (WLR)
If positive, 90% specificity for L/S nerve root compression
Valsalva Maneuver
Positive if increase in radicular symptoms
Spinal Percussion
Pain may indicate metastatic disease, abscess or osteomyelitis
Examinations: Merck Manual Professional
How To Test Reflexes
How To Do A Sensory Exam
How To Do A Motor Examination
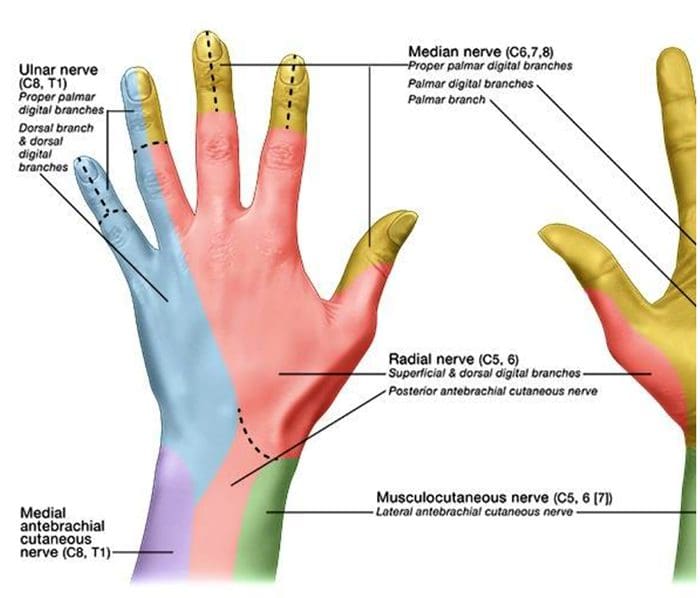
Dermatomes
Testing Cervical Nerve Roots
Testing Lumbosacral Nerve Roots
Specific Radiculopathy Patterns
T1 radiculopathy can cause Horner�s syndrome
This is due to affect on cervical sympathetic ganglia
Ptosis, miosis, anhidrosis
Below L1, radiculopathies can cause Cauda Equina syndrome
Saddle anesthesia (sensory loss in S2-S5 distribution)
Urinary retention or overflow incontinence
Constipation, decreased rectal tone or fecal incontinence
Loss of erectile function
Must be referred for emergency care immediately to prevent permanent dysfunction
Other Patterns Of Neuropathy
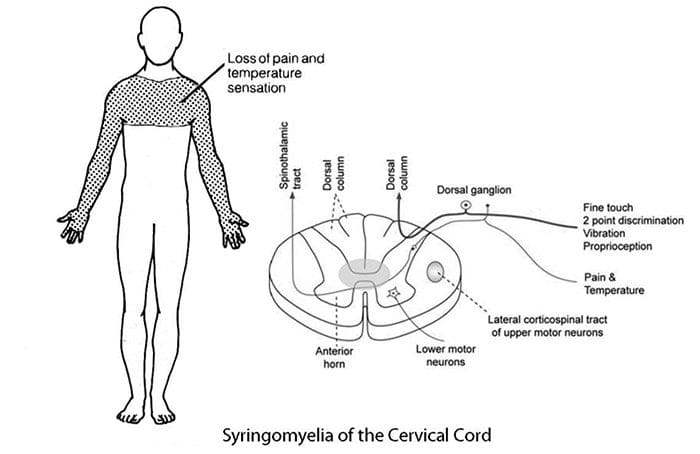
Cape/Shawl distribution of symptoms
Intramedullary lesion
Syringomyelia
Intramedullary tumor
Central cord damage
Stocking and Glove Distribution of Symptoms
Diabetes mellitus
B12 deficiency
Alcoholism/hepatitis
HIV
Thyroid dysfunction/myxedema
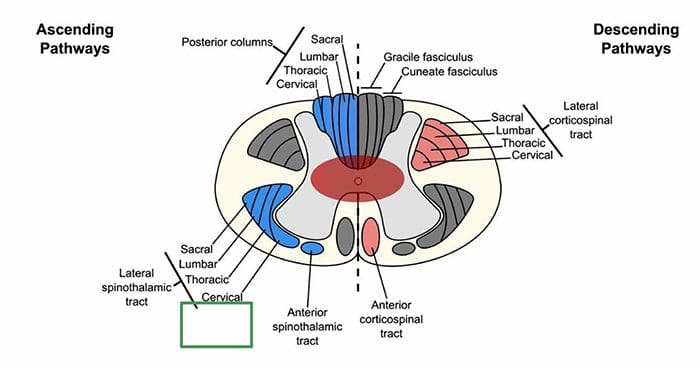
Cape/Shawl Pattern
Intramedullary lesion such as tumor, syringomyelia or hyperextension injury in patient with C/S spondylosis
Loss of pain and temp sensation in C/T dermatomes because of arrangement of lateral spinothalamic tract
Stocking & Glove Pattern
Symmetrical polyneuropathy
Feet/legs usually affected first, followed by hands/arms
Vibration sensation in the smallest toes is usually the first thing lost and neuropathy progresses across foot to great toe and then upward through the ankle and leg, then hands, arms and finally trunk if sever
Most likely cause of this distribution is diabetes mellitus, but other possible causes include B12 deficiency, alcoholism, HIV, chemotherapy treatment, thyroid dysfunction and multiple other causes
Diabetic Neuropathy
Diabetic neuropathy often presents as a polyneuropathy but can also present as a mononeuropathy, usually with acute onset
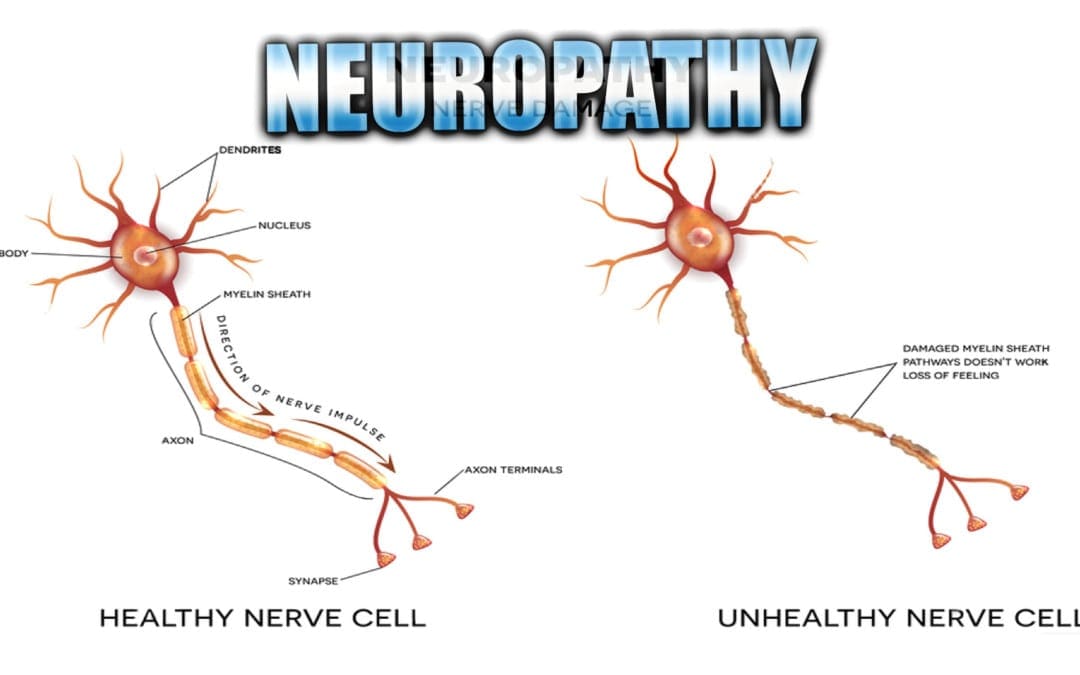
Neuropathy Presentation: El Paso, TX. Chiropractor, Dr. Alexander Jimenez�presents an overview of neuropathy. These are the most common neuropathies to be seen in practice.�Neuropathy is a medical term used to characterize damage or injury to the nerves, which refers to the peripheral nerves as opposed to the central nervous system. The complications which follow neuropathy depends largely on the type of nerves that are affected. According to Dr. Alex Jimenez, different neuropathies can cause numbness and tingling sensations, increased pain or the loss of ability to feel pain, muscle weakness along with twitching and cramps, even dizziness and/or loss of control over bladder function.
Neuropathy
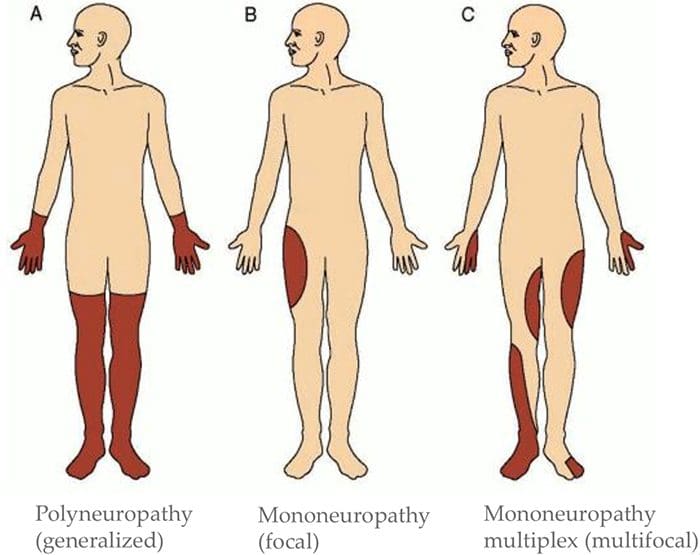
Three primary classifications based on location of symptoms:
If sensory disruption is limited to certain modalities, it implies CNS is involved
If all sensation is affected in the area, implies PNS is involved
Determine Pattern Of Symptoms
Mononeuropathy (focal)?
Mononeuropathy multiplex (multifocal)?
Polyneuropathy (generalized)?
Motor Exam
Determine if there is change to muscle strength
Determine if there is a change in muscle tone
Determine which muscles are affected
Determine if there has been a change in reflexes
This information can help determine the level(s) of involvement
Check For Autonomic�Signs
Auscultate heart
Palpate palms
Auscultate abdomen
Assess autonomic history
For example, is patient complaining about sweating more on one side than another? Complaining of stress levels?
Suggest ANS involvement
Exams: Merck Manual Professional Version
How To Test Reflexes
How To Do The Sensory Exam
How To Do The Motor Examination
Classification Of Nerve Injuries Resulting In Neuropathy
Neurapraxia – This is a transient episode of motor paralysis with little or no sensory or autonomic dysfunction; no disruption of the nerve or its sheath occurs; with removal of the compressing force, recovery should be complete
Axonotmesis – This is a more severe nerve injury, in which the axon is disrupted but the Schwann sheath is maintained; motor, sensory, and autonomic paralysis results; recovery can occur if the compressing force is removed in a timely fashion and if the axon regenerates
Neurotmesis – This is the most serious injury, in which both the nerve and its sheath are disrupted; although recovery may occur, it is always incomplete, secondary to loss of nerve continuity
Brachial Plexopathies
Erb�s Palsy
Klumke�s Palsy
Erb�s Palsy
AKA Erb�Duchenne palsy or Waiter’s tip palsy
Most common mechanism of injury in adults is a patient who fall forward while holding onto something behind them
Can also happen to an infant during childbirth ? Results from damage to C5-6 nerve roots in the brachial plexus
Dermatomal distribution of sensory disruption
Weakness or paralysis in deltoid, biceps, and brachialis muscles resulting in �waiter�s tip� position
Klumke�s Palsy
AKA Dejerine�Klumpke palsy
Happens to infants during childbirth if arm is pulled overhead
Can also happen to adults with overhead traction injuries
Results from damage to C8-T1 nerve roots in the brachial plexus
Dermatomal distribution of sensory disruption
Weakness or paralysis in wrist flexors and pronators as well as muscles of the hand
May produce Horner�s syndrome due to T1 involvement
Results in a �claw hand� appearance
Forearm supinated with wrist hyperextended, with finger flexion
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine




 LATERAL BRAINSTEM SYNDROMES
LATERAL BRAINSTEM SYNDROMES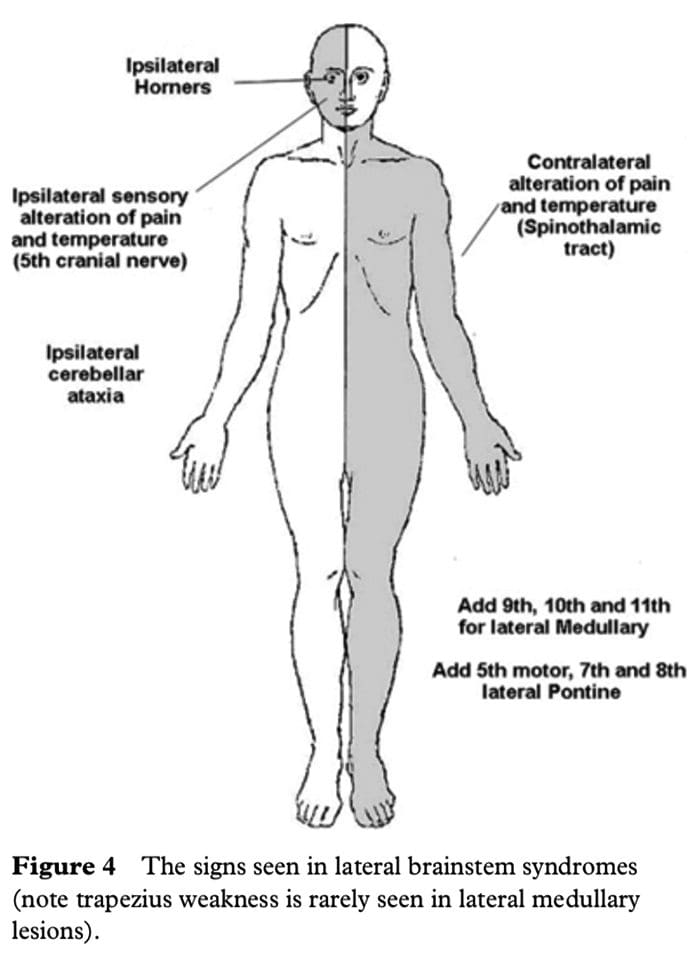 The lower 4 cranial nerves are in the medulla and the 12th nerve is in the midline so that 9th, 10th and 11th nerves will be in the lateral aspect of the medulla. When these are affected, the result is dysarthria and dysphagia with an ipsilateral impairment of the gag reflex and the palate will pull up to the opposite side; occasionally there may be weakness of the ipsilateral trapezius and/or sternocleidomastoid muscle. This is the lateral medullary syndrome usually resulting from occlusion of the ipsilateral vertebral or posterior inferior cerebellar arteries.
The lower 4 cranial nerves are in the medulla and the 12th nerve is in the midline so that 9th, 10th and 11th nerves will be in the lateral aspect of the medulla. When these are affected, the result is dysarthria and dysphagia with an ipsilateral impairment of the gag reflex and the palate will pull up to the opposite side; occasionally there may be weakness of the ipsilateral trapezius and/or sternocleidomastoid muscle. This is the lateral medullary syndrome usually resulting from occlusion of the ipsilateral vertebral or posterior inferior cerebellar arteries.
 CN I Clinically
CN I Clinically Cranial Nerve II Clinically
Cranial Nerve II Clinically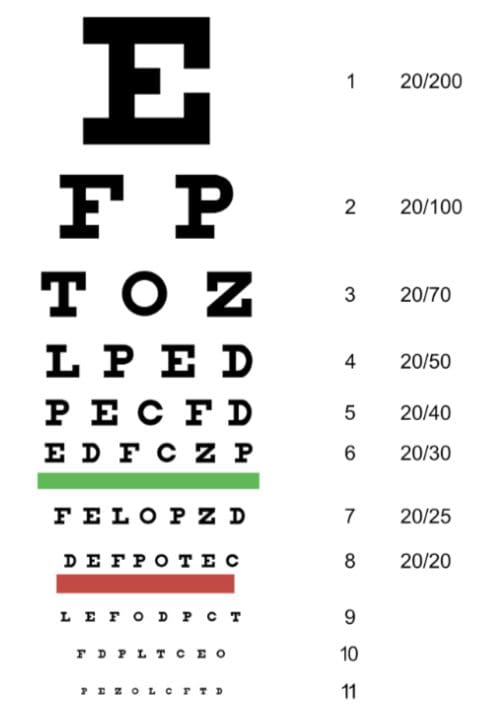
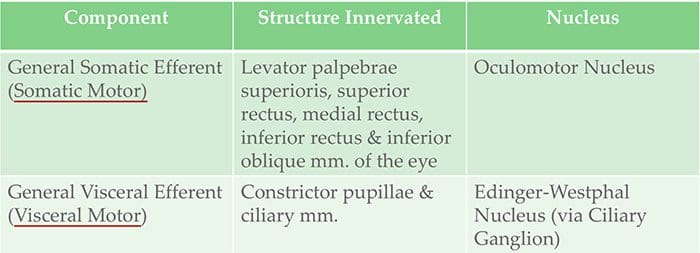 Cranial Nerve III Clinically
Cranial Nerve III Clinically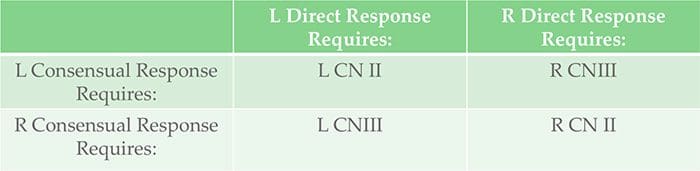 Testing Cranial Nerve CN II & III
Testing Cranial Nerve CN II & III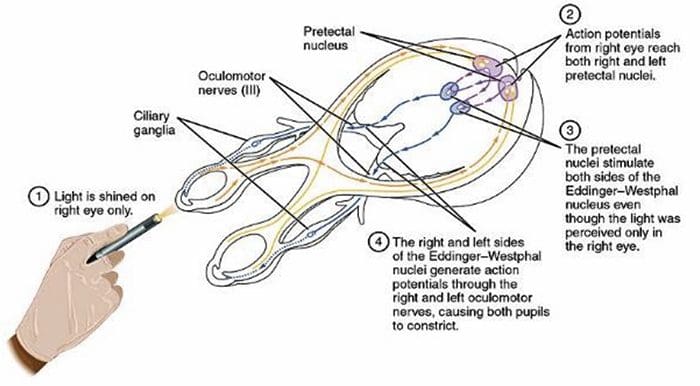
 Cranial Nerve IV Clinically
Cranial Nerve IV Clinically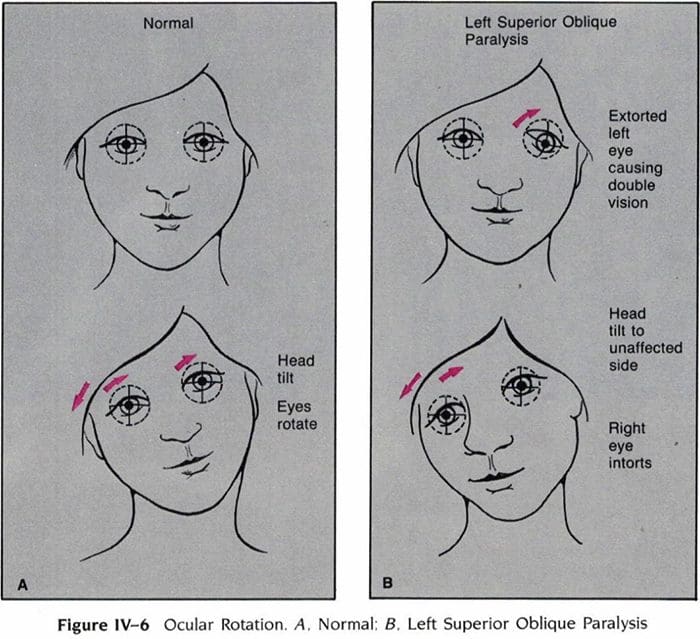 Pauwels, Linda Wilson, et al. Cranial Nerves: Anatomy and Clinical Comments. Decker, 1988.
Pauwels, Linda Wilson, et al. Cranial Nerves: Anatomy and Clinical Comments. Decker, 1988. Cranial Nerve VI Clinically
Cranial Nerve VI Clinically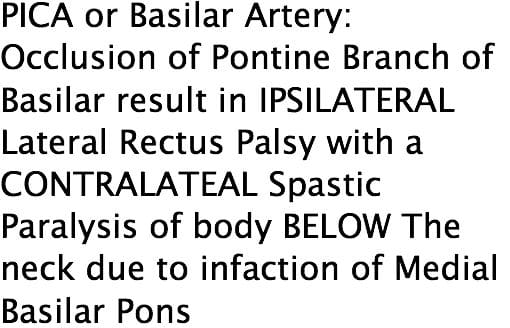
 Cranial Nerve V Clinically
Cranial Nerve V Clinically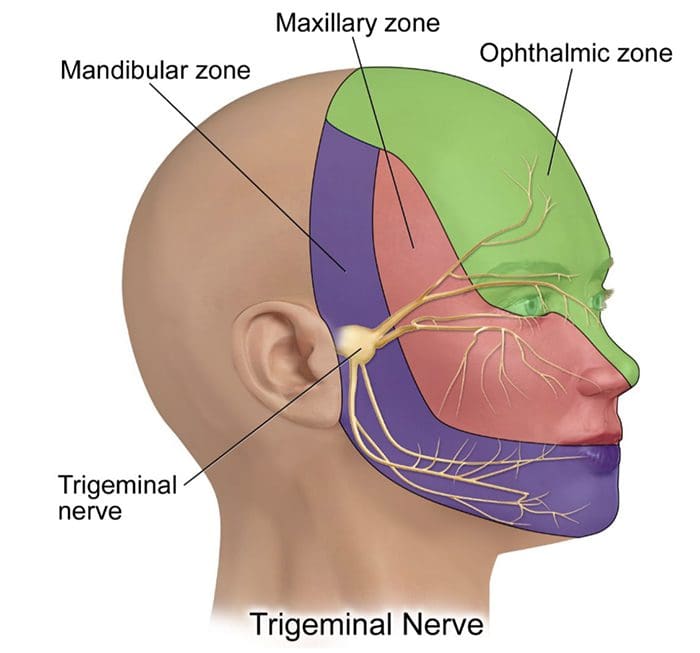
 Cranial Nerve VII Clinically
Cranial Nerve VII Clinically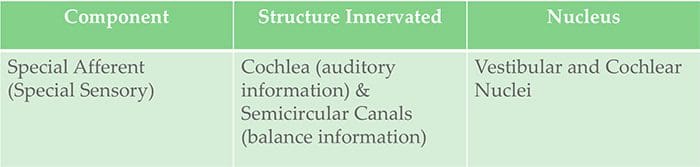 Cranial Nerve VIII Clinically
Cranial Nerve VIII Clinically
 Cranial Nerve IX Clinically
Cranial Nerve IX Clinically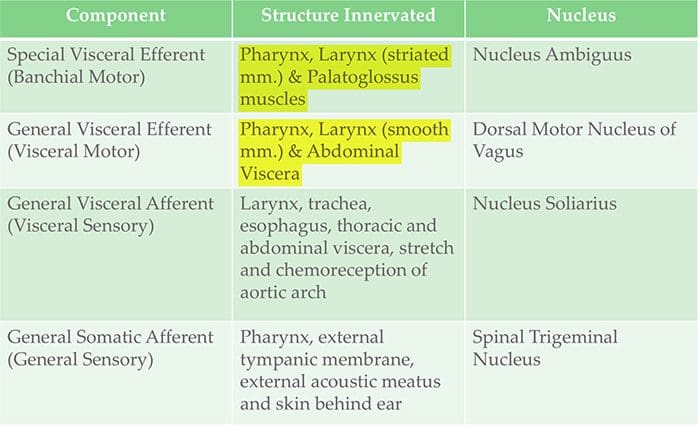 Cranial Nerve X Clinically
Cranial Nerve X Clinically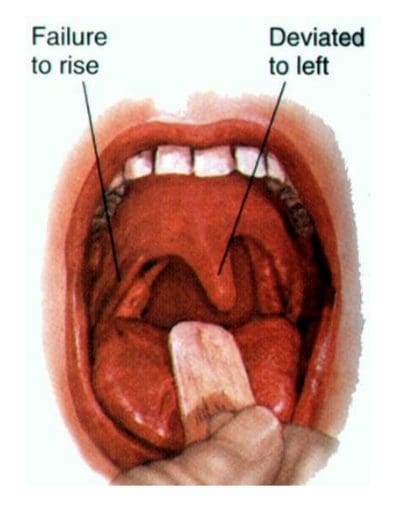
 Cranial Nerve XI Clinically
Cranial Nerve XI Clinically Cranial Nerve XII Clinically
Cranial Nerve XII Clinically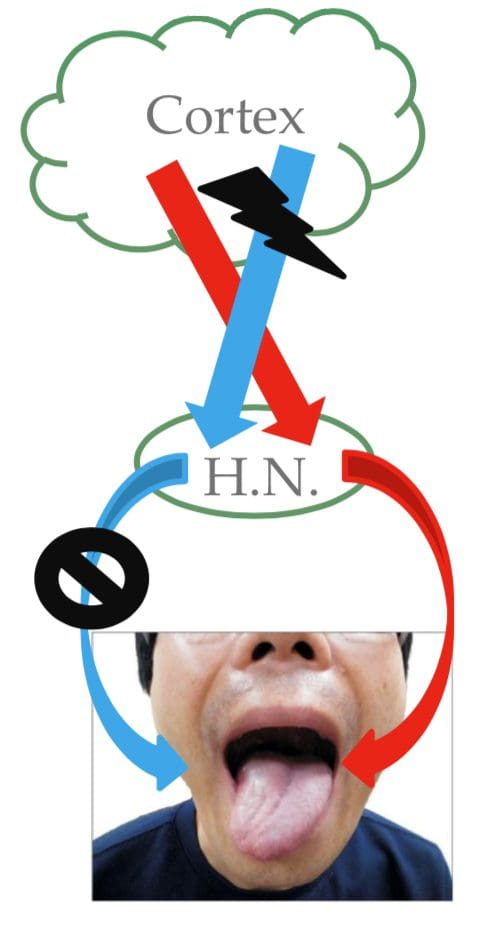
 Causes
Causes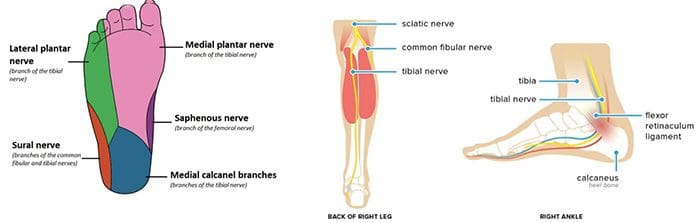 Radiculopathy
Radiculopathy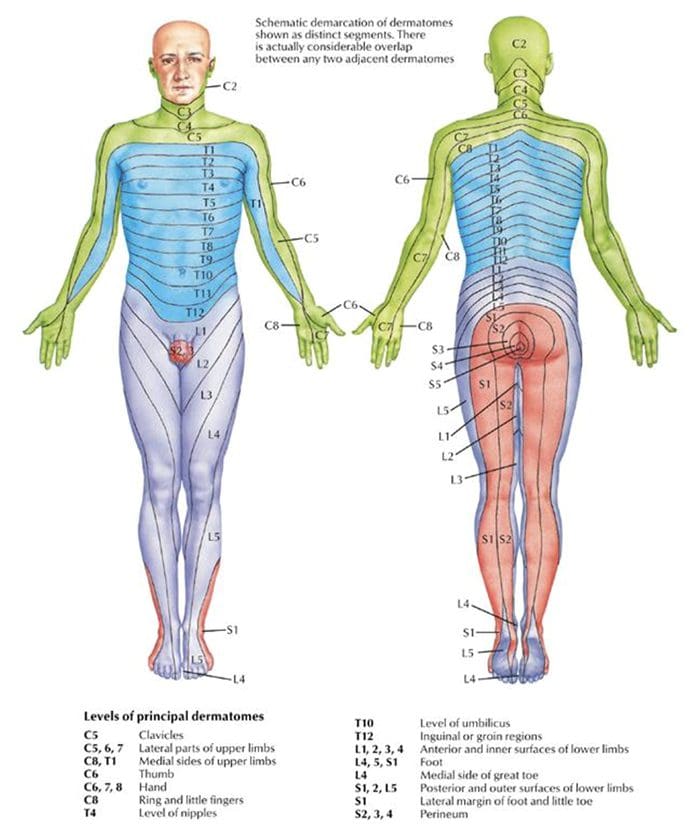 Testing Cervical Nerve Roots
Testing Cervical Nerve Roots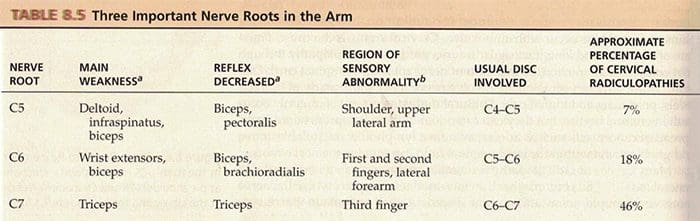 Testing Lumbosacral Nerve Roots
Testing Lumbosacral Nerve Roots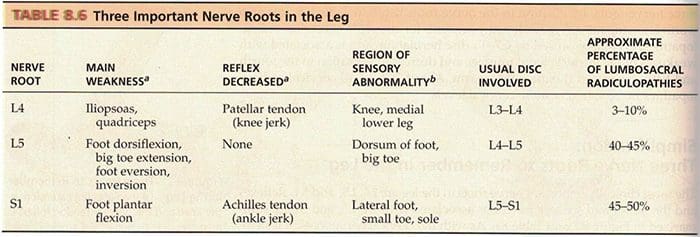
 Stocking & Glove Pattern
Stocking & Glove Pattern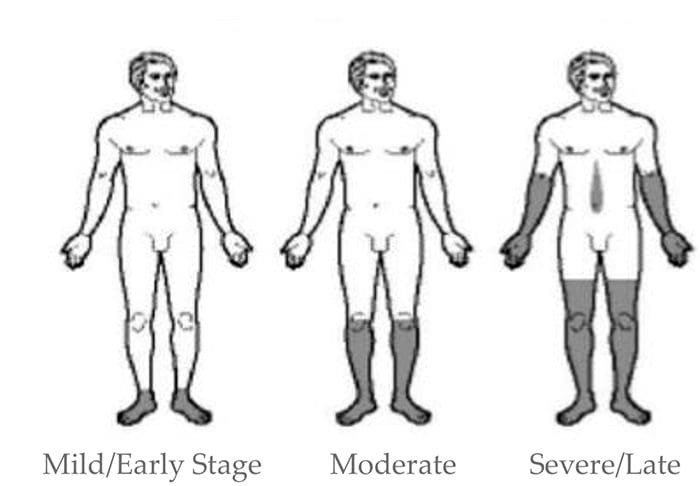
 Erb�s Palsy
Erb�s Palsy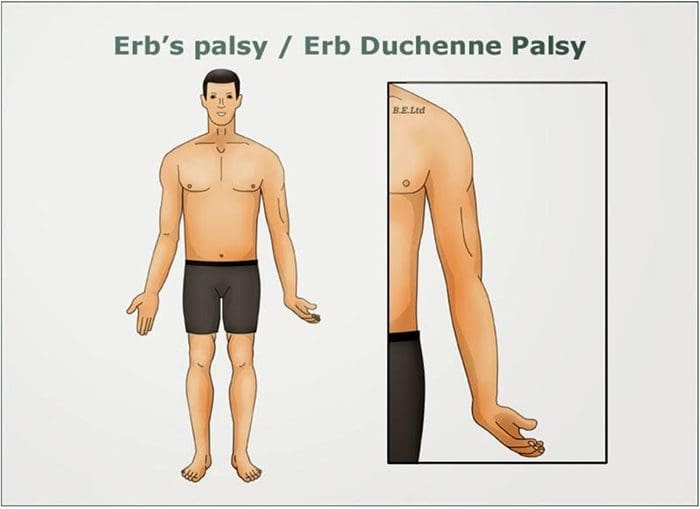 Klumke�s Palsy
Klumke�s Palsy Entrapment Neuropathies
Entrapment Neuropathies
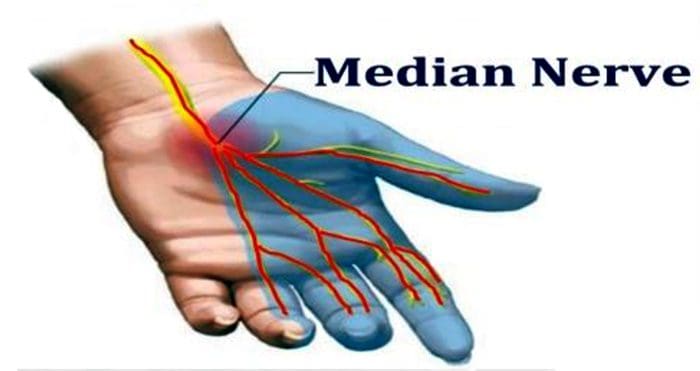 Median N. Pronator Teres Syndrome
Median N. Pronator Teres Syndrome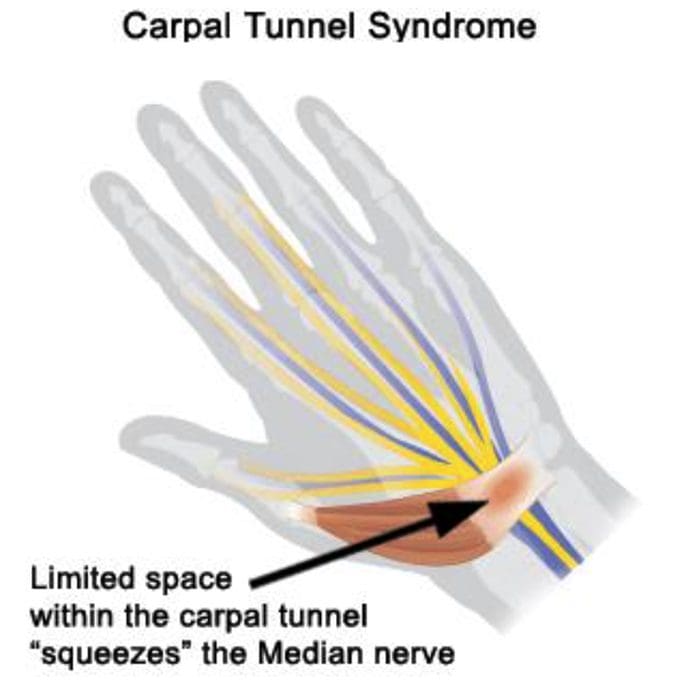
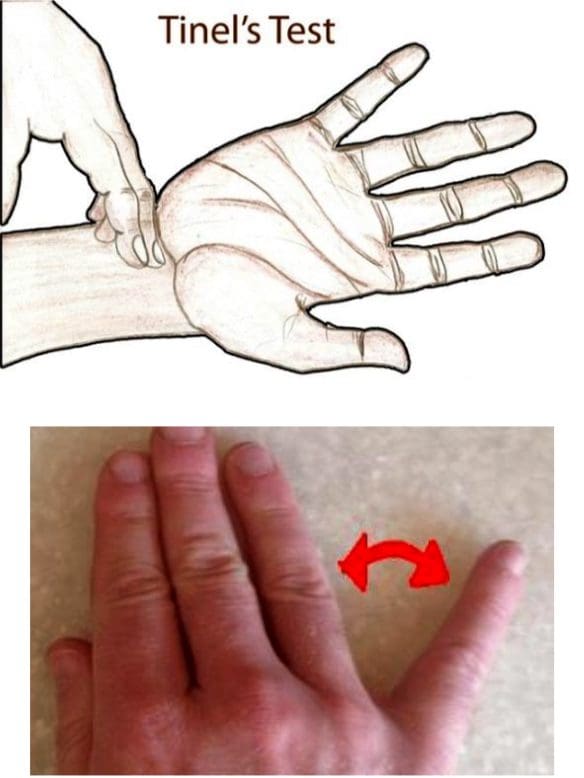
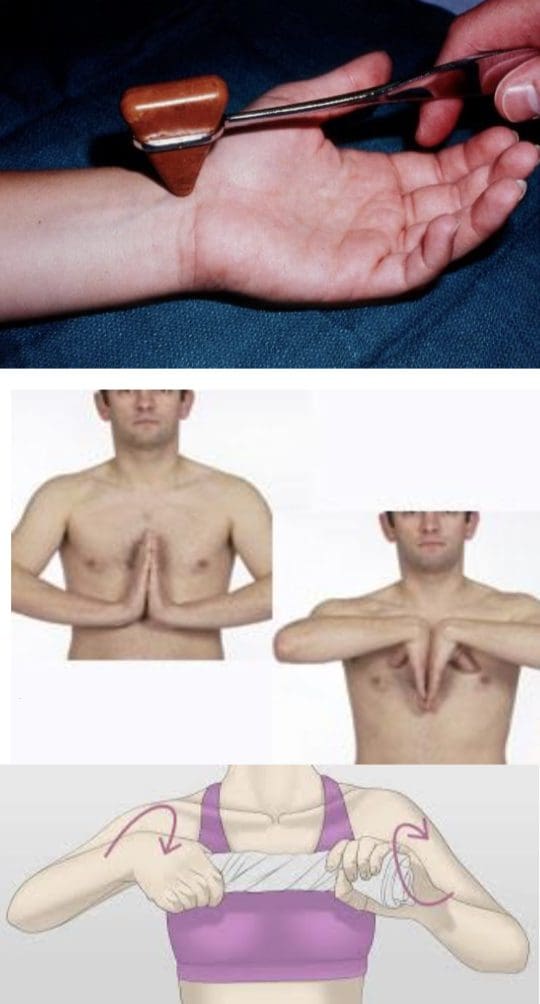 Tinel�s Sign
Tinel�s Sign
 Etiology
Etiology