In individuals with lumbar back pain, can pain specialists utilize distraction techniques to reduce muscle spasms?
Introduction
Many individuals dealing with specific or nonspecific back pain can agree that it can dampen their moods as they try to find the relief they seek to get back to their routine. More often than not, back pain is a common multifactorial musculoskeletal disorder that can affect the entire body, and it all starts with how people do simple movements incorrectly, causing compression to the spine. Since the spine is the main backbone of the body, it is responsible for training, stability, and flexibility. The surrounding muscles that encompass the spine act like a barrier to protect the skeletal joints and the spinal cord from injuries that are either traumatic or normal wear and tear. Lumbar back pain is also an economic burden that can cause unnecessary stress to the body, which leads to muscle spasms and causes even more stress to the individual. With lumbar back pain being a common nuisance to everyone worldwide, many will opt for treatment to reduce the pain and continue their daily activities. In today’s article, we will explore the issues of lumbar back pain and how treatments with distraction techniques alleviate the effects of lumbar back pain and reduce muscle spasms. We speak with certified medical providers who incorporate our patients’ information to provide numerous treatment plans to mitigate lumbar back pain associated with environmental factors. We also inform our patients that there are non-surgical options to reduce the pain-like symptoms related to lumbar back pain and reduce the effects of muscle spasms. We encourage our patients to ask astounding educational questions to our associated medical providers about the pain-like symptoms they are experiencing correlating with the lumbar spine. Dr. Alex Jimenez, D.C., utilizes this information as an academic service. Disclaimer
The Issues Of Lumbar Back Pain
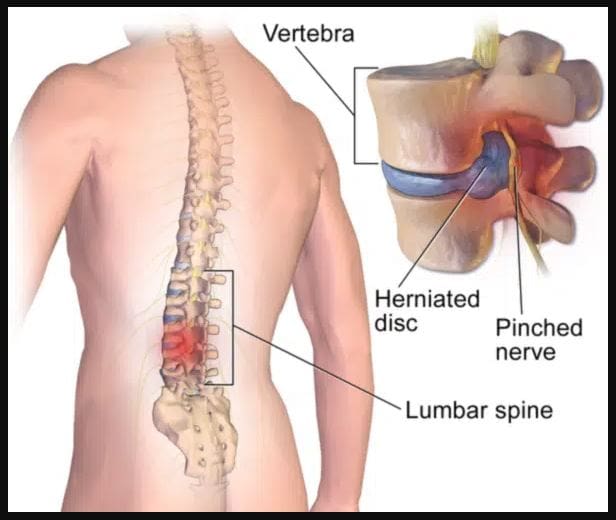
Do you often feel pain radiating from your lower back to your legs after work? Did you lift something heavy that caused your back muscles to strain and be in pain? Or do you and your loved ones feel muscle spasms in your lower back after stretching in the morning? When many individuals are dealing with these musculoskeletal issues, it often correlates with lumbar back pain. As stated earlier, the spine is the body’s backbone, and its main job is to support the body’s weight, provide stability to the upper and lower quadrants, and allow the host to move without pain or discomfort. When normal or traumatic factors start to affect many individuals over time, it can lead to the development of lumbar back pain, and it can become an issue for many young and older adults. Since lumbar back pain can be mechanical or nonspecific, it can arise intrinsically from the spine and the spinal components through repetitive muscle trauma that can be overused while being one of the common causes many people experience pain in their lumbar spine. (Will et al., 2018) When many individuals are dealing with lumbar back pain, it can become a reoccurring issue, and many go to medical clinics to get treatment for their lumbar back pain.
Another issue that lumbar back pain causes is affecting the spinal structure and the surrounding muscles, tissues, and ligaments that protect the spine. Since the body is remarkable for sensing when pain affects the spine, the vital structures are affected and start to respond by adopting other measures to maintain the spine’s stability. (Hauser et al., 2022) This means that when the body starts to develop muscle spasms in the spine, the stretched ligaments react rapidly to prevent the spine from destabilizing. This leads to individuals feeling aches and pain in their lower back, which then causes them to miss out on their activities.
The Road To Recovery: Chiropractic Care- Video
When it comes to lumbar back pain, many everyday factors can contribute to its development and cause issues for many individuals. Many individuals with lumbar back pain often experience referred pain in their lower extremity regions as the lumbar portions of the spine have compressed spinal discs, which can also correlate with nerve entrapment. To this point, many will seek out various treatments to reduce low back pain and its associated symptoms. When patients have prolonged symptoms correlating with lumbar pain, conservative management that is either non-surgical or surgical can help treat the pain-like symptoms related to lumbar back pain. (Mohd Isa et al., 2022) Lumbar back pain treatments can be customizable and cost-effective to the person’s pain severity. Non-surgical treatments can help lumbar back pain issues and reduce referred pain symptoms from different body locations in the upper or lower body quadrants. When people go to get their lumbar back pain treated, pain specialists like chiropractors, massage therapists, and physical therapists utilize various techniques and treatments to reduce pain affecting the surrounding ligaments, tissues, and muscles through stretches and traction. The video above explains how these treatments can help reduce pain caused by environmental factors and also help speed up recovery.
Distraction Techniques To Reduce Lumbar Back Pain
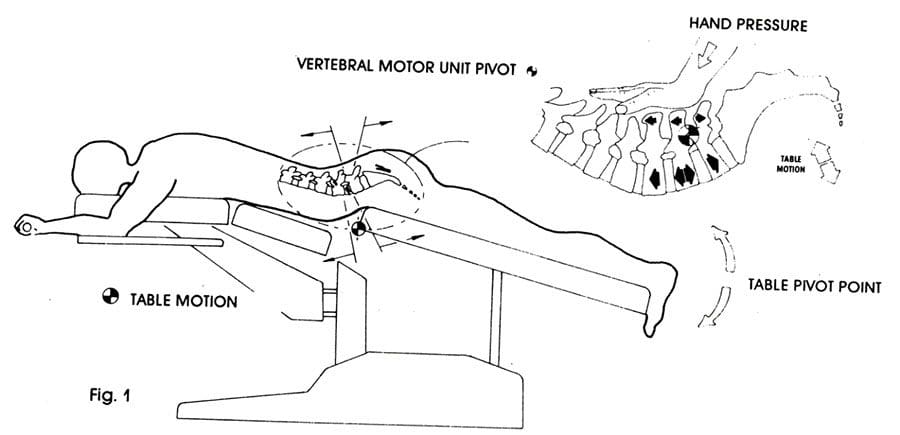
When many individuals get treated for lumbar back pain, many opt for non-surgical treatments due to being more affordable than surgical treatments. Pain specialists like chiropractors or massage therapists use distraction techniques to reduce the pain. These pain specialists also incorporate manual and mechanical therapy to be body-oriented to mobilize, manipulate, and stretch out the soft tissues and strengthen them. (Kuligowski et al., 2021) This, in turn, can help reduce lumbar back pain while allowing the individual to be more mindful about their actions to reduce the chances of back pain from returning. At the same time, the effectiveness of treating lumbar back pain through traction can effectively reduce nerve root compression and unresponsive movement symptoms. (Vanti et al., 2021) Traction therapy is a non-surgical treatment that gently stretches the spine to alleviate pain and help kick-start the natural healing process.
Distraction Techniques Reducing Muscle Spasms
Pain specialists incorporate distraction techniques to reduce lumbar back pain and muscle spasms in the lumbar region. As stated earlier, distraction techniques associated with non-surgical treatments can be an excellent way to minimize lumbar back pain. Distraction manipulation can help elevate the affected intervertebral disc by reducing the pressure off the disc and increasing its height in the spine. (Choi et al., 2015) Many individuals feel better when they incorporate distraction therapy to reduce lumbar pain. At the same time, distraction therapy can also be incorporated into a personalized plan to reduce muscle spasms and strengthen weak muscles that surround the lumbar region. The effects of lumbar traction combined with distraction therapy can improve pain and reduce functional disability within the lumbar spine. (Masood et al., 2022) When many people start to think more about their health and wellness, they can make small changes in their routine to prevent low back pain from progressing into something chronic and strengthen their weak muscles to control the pain-like symptoms from returning.
References
Choi, J., Lee, S., & Jeon, C. (2015). Effects of flexion-distraction manipulation therapy on pain and disability in patients with lumbar spinal stenosis. Journal of Physical Therapy Science, 27(6), 1937-1939. doi.org/10.1589/jpts.27.1937
Hauser, R. A., Matias, D., Woznica, D., Rawlings, B., & Woldin, B. A. (2022). Lumbar instability as an etiology of low back pain and its treatment by prolotherapy: A review. J Back Musculoskelet Rehabil, 35(4), 701-712. doi.org/10.3233/BMR-210097
Kuligowski, T., Skrzek, A., & Cieslik, B. (2021). Manual Therapy in Cervical and Lumbar Radiculopathy: A Systematic Review of the Literature. Int J Environ Res Public Health, 18(11). doi.org/10.3390/ijerph18116176
Masood, Z., Khan, A. A., Ayyub, A., & Shakeel, R. (2022). Effect of lumbar traction on discogenic low back pain using variable forces. J Pak Med Assoc, 72(3), 483-486. doi.org/10.47391/JPMA.453
Mohd Isa, I. L., Teoh, S. L., Mohd Nor, N. H., & Mokhtar, S. A. (2022). Discogenic Low Back Pain: Anatomy, Pathophysiology and Treatments of Intervertebral Disc Degeneration. Int J Mol Sci, 24(1). doi.org/10.3390/ijms24010208
Vanti, C., Turone, L., Panizzolo, A., Guccione, A. A., Bertozzi, L., & Pillastrini, P. (2021). Vertical traction for lumbar radiculopathy: a systematic review. Arch Physiother, 11(1), 7. doi.org/10.1186/s40945-021-00102-5
Will, J. S., Bury, D. C., & Miller, J. A. (2018). Mechanical Low Back Pain. American Family Physician, 98(7), 421-428. www.ncbi.nlm.nih.gov/pubmed/30252425
How does decompression alleviate sciatic nerve pain in many working individuals with lumbar disc degeneration?
Introduction
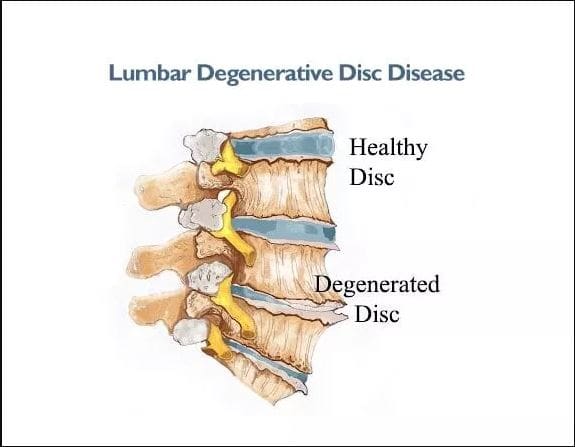
The discs between the spinal vertebrae act as a cushion when pressure is added to the body. These discs get compressed when the body is in motion. Our bodies and spines also age as we age, which causes the spinal intervertebral disc to degenerate over time. The outer part of the spinal disc may crack under pressure, causing the inner part to protrude and irritate the spinal nerve roots. This can cause sciatic nerve pain, which may result in radiating pain in the legs, buttocks, and lower back. This can cause mobility issues and disability, making it difficult for working individuals to perform their jobs. Non-surgical treatments, such as safe and gentle traction, can help alleviate sciatic nerve pain by reducing pressure on the spine and maintaining disc height. By slowing down the progression of lumbar disc degeneration, individuals can reduce the frequency of visits to their primary care doctors and avoid disability. Today’s article provides an overview of lumbar disc degeneration, its association with sciatic nerve pain, and the benefits of decompression in restoring disc height and reducing pain. As we work with certified medical providers who use our patients’ information to treat individuals experiencing sciatic nerve pain associated with lumbar disc degeneration. We inform them that non-surgical treatments like decompression can help reduce the progression of lumbar disc degeneration and reduce sciatic nerve pain. At the same time, we also explain to them how adding decompression to their routine can alleviate the pain-like symptoms. We encourage our patients to ask essential questions while seeking education from our associated medical providers about their situation. Dr. Alex Jimenez, D.C., provides this information as an educational service. Disclaimer
Lumbar Disc Degeneration Overview
Have you begun to notice how your legs, buttocks, and feet are constantly experiencing tingling sensations that it makes it difficult to do everyday actions? Do you feel excruciating pain in your legs while standing, only to find relief from resting? Or do you notice that you are getting aches and muscle strains from normal motion like bending, twisting, and turning after waking up in the morning? Many individuals, especially older working adults, are experiencing these issues due to lumbar disc degeneration. Now lumbar disc degeneration usually occurs naturally as the body ages, which then causes the intervertebral disc to wear and tear constantly under pressure, then cracks and causes the disc to herniate. Since the intervertebral disc provides structural support and shock absorption against mechanical loads to the lumbar region, when normal or traumatic factors cause changes, it can cause dysfunction and instability in the lumbar spine. (Mohd Isa et al., 2022)
When the intervertebral discs begin to crack under pressure, it can cause pain-like symptoms affecting the upper and lower extremities. Additionally, lumbar disc degeneration can cause spinal flexibility to decrease and reduce the spine’s ROM (range of motion), which causes more stress on the surrounding muscles, ligaments, and tissues. Lumbar disc degeneration can cascade events from disc bulging to nerve root irritation. (Liyew, 2020) This means that when there are advanced degenerative changes to the lumbar facet joints and the surrounding soft tissues, it can cause the spinal canal to narrow and compress the adjacent nerve root. To that point, it can lead to reduce disc height and lead to sciatic nerve pain.
Lumbar Disc Degeneration Associated With Sciatica
Now how would lumbar disc degeneration be associated with sciatic nerve pain? When the intervertebral disc is being compressed under unwanted pressure, it can crack over time and herniate out of its original position, which then can press on the nerve root causing radiating pain to travel to the affected muscle area. Since the sciatic nerve is positioned in the lumbosacral region, it runs from the top of the gluteus muscles and down to the back of the hamstrings and calves. When unwanted pressure causes the intervertebral disc to herniate and start to affect the sciatic nerve, it causes a frequent symptom known as lumbar sciatica, where the herniated disc is compressing the sciatic nerve. (Zitouna et al., 2019) To that point, it can cause radiating, shooting pain down to the leg, making it difficult for individuals with demanding jobs to find relief. Since the lumbar intervertebral discs have a corresponding relationship with the central nervous system, the nerve roots that surround the spinal discs help with providing neuron signals to the adjacent muscles, which allows the arms, hands, legs, and feet to move. (Bogduk, Tynan, & Wilson, 1981) However, when the intervertebral discs are herniated, it can disrupt the neuron signaling to the muscles and cause referred pain to the lower or upper extremities. When this happens, many individuals opt to seek treatment.
Sciatica Secrets Revealed- Video
Many individuals dealing with sciatic nerve pain associated with lumbar disc degeneration will often find temporary relief to continue their work despite constant pain. This is due to the unwanted pressure that is causing an overload on the spinal disc to cause them to degenerate and invoke pain in the lower regions. At the same time, age and degenerative structural changes have a close relationship that can cause a greater effect on stress distribution to the lower back. (Adams, McNally, & Dolan, 1996) This leads to overlapping risk profiles contributing to sciatic nerve pain associated with lumbar disc degeneration due to normal and traumatic factors. However, many individuals don’t have to suffer from pain-like symptoms related to lumbar disc degeneration as there are numerous treatments to restore disc height and reduce sciatic nerve pain. Non-surgical treatments are great for many individuals looking for cost-efficiency and can be personalized to the person’s pain. (Louis-Sidney et al., 2022) Non-surgical treatments like chiropractic care, massage and physical therapy, and spinal decompression can help many individuals with lumbar disc degeneration associated with sciatic nerve pain. These treatments incorporate mechanical and manual manipulation of the spine to realign the body out of subluxation while incorporating various techniques to stretch out the soft tissues and muscles to strengthen their length and reduce nerve entrapment. The video above explains a bit more about how these treatments can restore mobility to the body, reduce inflammation, and relieve muscle tension caused by lumbar disc degeneration associated with sciatic nerve pain.
Spinal Decompression Restores Disc Height
Now non-surgical treatments like spinal decompression can help reduce the progress of lumbar disc degeneration by restoring disc height. Spinal decompression uses gentle traction on the spine to allow the necessary nutrients, fluids, and blood to be reabsorbed back into the spine. It will enable the herniated disc to return to its original position and rehydrate it. (Yu et al., 2022) Since the spine and body age naturally, spinal decompression can restore disc height by creating negative pressure to regain mobility and stretch out the affected muscles surrounding the spine.
Spinal Decompression Reduces Sciatic Nerve Pain
Additionally, decompression can help reduce sciatic nerve pain as it can help the herniated disc alleviate the pressure on the sciatic nerve and can restore mobility to the body. Spinal decompression can become a positive outcome for many working individuals as it allows individuals to be more mindful of their habits that were the cause of the pain they were experiencing. (Brogger et al., 2018) With non-surgical treatments like spinal decompression, many individuals can become efficient with work while being more conscious about what factors contribute to the pain. This, in turn, allows them to focus on their well-being and strengthen their weak points with a personalized plan that will enable them to make small changes in their day-to-day lives and become pain-free after a few consecutive treatments.
References
Adams, M. A., McNally, D. S., & Dolan, P. (1996). ‘Stress’ distributions inside intervertebral discs. The effects of age and degeneration. J Bone Joint Surg Br, 78(6), 965-972. doi.org/10.1302/0301-620x78b6.1287
Bogduk, N., Tynan, W., & Wilson, A. S. (1981). The nerve supply to the human lumbar intervertebral discs. J Anat, 132(Pt 1), 39-56. www.ncbi.nlm.nih.gov/pubmed/7275791
Brogger, H. A., Maribo, T., Christensen, R., & Schiottz-Christensen, B. (2018). Comparative effectiveness and prognostic factors for outcome of surgical and non-surgical management of lumbar spinal stenosis in an elderly population: protocol for an observational study. BMJ Open, 8(12), e024949. doi.org/10.1136/bmjopen-2018-024949
Liyew, W. A. (2020). Clinical Presentations of Lumbar Disc Degeneration and Lumbosacral Nerve Lesions. Int J Rheumatol, 2020, 2919625. doi.org/10.1155/2020/2919625
Louis-Sidney, F., Duby, J. F., Signate, A., Arfi, S., De Bandt, M., Suzon, B., & Cabre, P. (2022). Lumbar Spinal Stenosis Treatment: Is Surgery Better than Non-Surgical Treatments in Afro-Descendant Populations? Biomedicines, 10(12). doi.org/10.3390/biomedicines10123144
Mohd Isa, I. L., Teoh, S. L., Mohd Nor, N. H., & Mokhtar, S. A. (2022). Discogenic Low Back Pain: Anatomy, Pathophysiology and Treatments of Intervertebral Disc Degeneration. Int J Mol Sci, 24(1). doi.org/10.3390/ijms24010208
Yu, P., Mao, F., Chen, J., Ma, X., Dai, Y., Liu, G., Dai, F., & Liu, J. (2022). Characteristics and mechanisms of resorption in lumbar disc herniation. Arthritis Res Ther, 24(1), 205. doi.org/10.1186/s13075-022-02894-8
Zitouna, K., Selmene, M. A., Derbel, B., Rekik, S., Drissi, G., & Barsaoui, M. (2019). An unexpected etiology of lumbosciatica. Tunis Med, 97(12), 1415-1418. www.ncbi.nlm.nih.gov/pubmed/32173813
The spine is made up of 24 bones, called vertebrae, which are stacked on top of one another. These spinal bones are ultimately connected, creating a canal to protect the spinal cord. In between each vertebra are fluid-filled intervertebral discs which act as shock absorbers for the spine. Over time, however, these flexible, jelly donut-like discs can begin to herniate, where the nucleus of the intervertebral disc pushes against its outer ring, causing low back pain. Below, we will demonstrate the various types of herniated discs and discuss their causes, symptoms and treatment options.
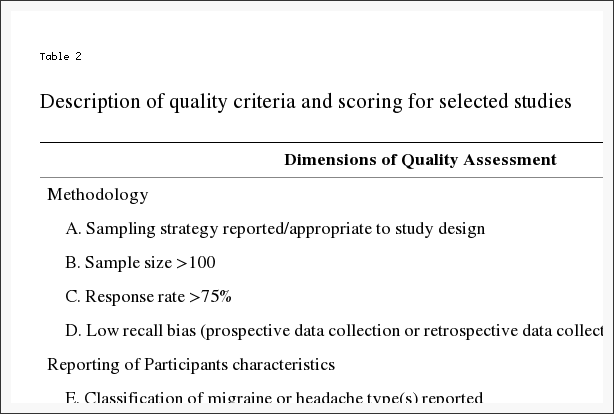
Abstract
Background Context
The paper ��Nomenclature and classification of lumbar disc pathology, recommendations of the combined task forces of the North American Spine Society, the American Society of Spine Radiology and the American Society of Neuroradiology,�� was published in 2001 in Spine (� Lippincott, Williams & Wilkins). It was authored by David Fardon, MD, and Pierre Milette, MD, and formally endorsed by the American Society of Spine Radiology (ASSR), American Society of Neuroradiology (ASNR), and North American Spine Society (NASS). Its purpose was to promote greater clarity and consistency of usage of spinal terminology, and it has served this purpose well for over a decade. Since 2001, there has been sufficient evolution in our understanding of the lumbar disc to suggest the need for revision and updating of the original document. The revised document is presented here, and it represents the consensus recommendations of contemporary combined task forces of the ASSR, ASNR, and NASS. This article reflects changes consistent with current concepts in radiologic and clinical care.
Purpose
To provide a resource that promotes a clear understanding of lumbar disc terminology amongst clinicians, radiologists, and researchers. All the concerned need standard terms for the normal and pathologic conditions of lumbar discs that can be used accurately and consistently and thus best serve patients with disc disorders.
Study Design
This article comprises a review of the literature.
Methods
A PubMed search was performed for literature pertaining to the lumbar disc. The task force members individually and collectively reviewed the literature and revised the 2001 document. The revised document was then submitted for review to the governing boards of the ASSR, ASNR, and NASS. After further revision based on the feedback from the governing boards, the article was approved for publication by the governing boards of the three societies, as representative of the consensus recommendations of the societies.
Results
The article provides a discussion of the recommended diagnostic categories pertaining to the lumbar disc: normal; congenital/developmental variation; degeneration; trauma; infection/inflammation; neoplasia; and/or morphologic variant of uncertain significance. The article provides a glossary of terms pertaining to the lumbar disc, a detailed discussion of these terms, and their recommended usage. Terms are described as preferred, nonpreferred, nonstandard, and colloquial. Updated illustrations pictorially portray certain key terms. Literature references that provided the basis for the task force recommendations are included.
Conclusions
We have revised and updated a document that, since 2001, has provided a widely acceptable nomenclature that helps maintain consistency and accuracy in the description of the anatomic and physiologic properties of the normal and abnormal lumbar disc and that serves as a system for classification and reporting built upon that nomenclature.
The nomenclature and classification of lumbar disc pathology consensus, published in 2001, by the collaborative efforts of the North American Spine Society (NASS), the American Society of Spine Radiology (ASSR) and the American Society of Neuroradiology (ASNR), has guided radiologists, clinicians, and interested public for over a decade [1]. This document has passed the test of time. Responding to an initiative from the ASSR, a task force of spine physicians from the ASSR, ASNR, and NASS has reviewed and modified the document. This revised document preserves the format and most of the language of the original, with changes consistent with current concepts in radiologic and clinical care. The modifications deal primarily with the following: updating and expansion of Text, Glossary, and References to meet contemporary needs; revision of Figures to provide greater clarity; emphasis of the term ��annular fissure�� in place of ��annular tear��; refinement of the definitions of ��acute�� and ��chronic�� disc herniations; revision of the distinction between disc herniation and asymmetrically bulging disc; elimination of the Tables in favor of greater clarity from the revised Text and Figures; and deletion of the section of Reporting and Coding because of frequent changes in those practices, which are best addressed by other publications. Several other minor amendments have been made. This revision will update a workable standard nomenclature, accepted and used universally by imaging and clinical physicians.
Introduction and History
Physicians need standard terms for normal and pathologic conditions of lumbar discs [2, 3, 4, 5]. Terms that can be interpreted accurately, consistently, and with reasonable precision are particularly important for communicating impressions gained from imaging for clinical diagnostic and therapeutic decision-making. Although clear understanding of the disc terminology between radiologists and clinicians is the focus of this work, such understanding can be critical, also to patients, families, employers, insurers, jurists, social planners, and researchers.
In 1995, a multidisciplinary task force from the NASS addressed the deficiencies in commonly used terms defining the conditions of the lumbar disc. It cited several documentations of the problem [6, 7, 8, 9, 10, 11] and made detailed recommendations for standardization. Its work was published in a copublication of the NASS and the American Academy of Orthopaedic Surgeons [9]. The work had not been otherwise endorsed by major organizations and had not been recognized as authoritative by radiology organizations. Many previous [3, 7, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19] and some subsequent [20, 21, 22, 23, 24, 25] efforts addressed the issues, but were of more limited scope and none had gained a widespread acceptance.
Although the NASS 1995 effort was the most comprehensive at the time, it remained deficient in clarifying some controversial topics, lacking in its treatment of some issues, and did not provide recommendations for standardization of classification and reporting. To address the remaining needs, and in hopes of securing endorsement sufficient to result in universal standardizations, joint task forces (Co-Chairs David Fardon, MD, and Pierre Milette, MD) were formed by the NASS, ASNR, and ASSR, resulting in the first version of the document ��Nomenclature and classification of lumbar disc pathology�� [1]. Since then, time and experience suggested the need for revisions and updating of the original document. The revised document is presented here.
The general principles that guided the original document remain unchanged in this revision. The definitions are based on the anatomy and pathology, primarily as visualized on imaging studies. Recognizing that some criteria, under some circumstances, may be unknowable to the observer, the definitions of the terms are not dependent on or imply the value of specific tests. The definitions of diagnoses are not intended to imply external etiologic events such as trauma, they do not imply relationship to symptoms, and they do not define or imply the need for specific treatment.
The task forces, both current and former, worked from a model that could be expanded from a primary purpose of providing understanding of reports of imaging studies. The result provides a simple classification of diagnostic terms, which can be expanded, without contradiction, into more precise subclassifications. When reporting pathology, degrees of uncertainty would be labeled as such rather than compromising the definitions of the terms.
All terms used in the classifications and subclassifications are defined and those definitions are adhered to throughout the model. For a practical purpose, some existing English terms are given meanings different from those found in some contemporary dictionaries. The task forces provide a list and classification of the recommended terms, but, recognizing the nature of language practices, discuss and include in the Glossary, commonly used and misused nonrecommended terms and nonstandard definitions.
Although the principles and most of the definitions of this document can be easily extrapolated to the cervical and dorsal spine, the focus is on the lumbar spine. Although clarification of terms related to posterior elements, dimensions of the spinal canal, and status of neural tissues is needed, this work is limited to the discussion of the disc. While it is not always possible to discuss fully the definition of anatomical and pathologic terms without some reference to symptoms and etiology, the definitions themselves stand the test of independence from etiology, symptoms, or treatment. Because of the focus on anatomy and pathology, this work does not define certain clinical syndromes that may be related to lumbar disc pathology [26].
Guided by those principles, we have revised and updated a document that, since 2001, has provided a widely acceptable nomenclature that is workable for all forms of observation, that addresses contour, content, integrity, organization, and spatial relationships of the lumbar disc; and that serves a system of classification and reporting built upon that nomenclature.
Diagnostic Category & Subcategory Recommendations
These recommendations present diagnostic categories and subcategories intended for classification and reporting of imaging studies. The terminology used throughout these recommended categories and subcategories remains consistent with detailed explanations given in the Discussion and with the preferred definitions presented in the Glossary.
The diagnostic categories are based on pathology. Each lumbar disc can be classified in terms of one, and occasionally more than one, of the following diagnostic categories: normal; congenital/developmental variation; degeneration; trauma; infection/inflammation; neoplasia; and/or morphologic variant of uncertain significance. Each diagnostic category can be subcategorized to various degrees of specificity according to the information available and purpose to be served. The data available for categorization may lead the reporter to characterize the interpretation as ��possible,�� ��probable,�� or ��definite.��
Note that some terms and definitions discussed below are not recommended as preferred terminology, but are included to facilitate the interpretation of vernacular and, in some cases, improper use. Terms may be defined as preferred, nonpreferred, or nonstandard. Nonstandard terms by consensus of the organizational task forces should not be used in the manner described.
Normal
Normal defines discs that are morphologically normal, without the consideration of the clinical context and not inclusive of degenerative, developmental, or adaptive changes that could, in some contexts (eg, normal aging, scoliosis, spondylolisthesis), be considered clinically normal (Fig. 1).
Figure 1: Normal lumbar disc. (Top Left) Axial, (Top Right) sagittal, and (Bottom) coronal images demonstrate that the normal disc, composed of central NP and peripheral AF, is wholly within the boundaries of the disc space, as defined, craniad and caudad by the vertebral body end plates and peripherally by the planes of the outer edges of the vertebral apophyses, exclusive of osteophytes. NP, nucleus pulposus; AF, annulus fibrosus.
Congenital/Developmental Variation
The congenital/developmental variation category includes discs that are congenitally abnormal or that have undergone changes in their morphology as an adaptation of abnormal growth of the spine, such as from scoliosis or spondylolisthesis.
Degeneration
Degenerative changes in the discs are included in a broad category that includes the subcategories annular fissure, degeneration, and herniation.
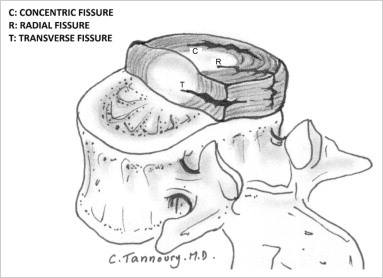
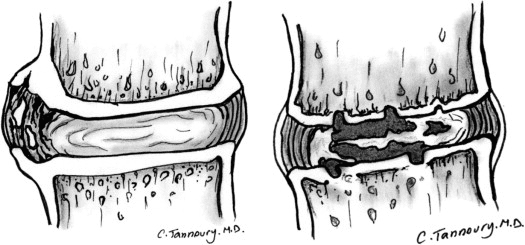
Annular fissures are separations between the annular fibers or separations of annular fibers from their attachments to the vertebral bone. Fissures are sometimes classified by their orientation. A ��concentric fissure�� is a separation or delamination of annular fibers parallel to the peripheral contour of the disc (Fig. 2). A ��radial fissure�� is a vertically, horizontally, or obliquely oriented separation of (or rent in) annular fibers that extends from the nucleus peripherally to or through the annulus. A ��transverse fissure�� is a horizontally oriented radial fissure, but the term is sometimes used in a narrower sense to refer to a horizontally oriented fissure limited to the peripheral annulus that may include separation of annular fibers from the apophyseal bone. Relatively wide annular fissures, with stretch of the residual annular margin, at times including avulsion of an annular fragment, have sometimes been called ��annular gaps,�� a term that is relatively new and not accepted as standard [27]. The term ��fissures�� describes the spectrum of these lesions and does not imply that the lesion is a consequence of injury.
Figure 2: Fissures of the annulus fibrosus. Fissures of the annulus fibrosus occur as radial (R), transverse (T), and/or concentric (C) separations of fibers of the annulus. The transverse fissure depicted is a fully developed, horizontally oriented radial fissure; the term ��transverse fissure�� is often applied to a less extensive separation limited to the peripheral annulus and its bony attachments.
Use of the term ��tear�� can be misunderstood because the analogy to other tears has a connotation of injury, which is inappropriate in this context. The term ��fissure�� is the correct term. Use of the term ��tear�� should be discouraged and, when it appears, should be recognized that it is usually meant to be synonymous with ��fissure�� and not reflective of the result of injury. The original version of this document stated preference for the term ��fissure�� but regarded the two terms as almost synonymous. However, in this revision, we regard the term ��tear�� as nonstandard usage.
Degeneration may include any or all of the following: desiccation, fibrosis, narrowing of the disc space, diffuse bulging of the annulus beyond the disc space, fissuring (ie, annular fissures), mucinous degeneration of the annulus, intradiscal gas [28], osteophytes of the vertebral apophyses, defects, inflammatory changes, and sclerosis of the end plates [15, 29, 30, 31, 32, 33, 34].
Herniation is broadly defined as a localized or focal displacement of disc material beyond the limits of the intervertebral disc space. The disc material may be nucleus, cartilage, fragmented apophyseal bone, annular tissue, or any combination thereof. The disc space is defined craniad and caudad by the vertebral body end plates and, peripherally, by the outer edges of the vertebral ring apophyses, exclusive of osteophytes. The term ��localized�� or ��focal�� refers to the extension of the disc material less than 25% (90�) of the periphery of the disc as viewed in the axial plane.
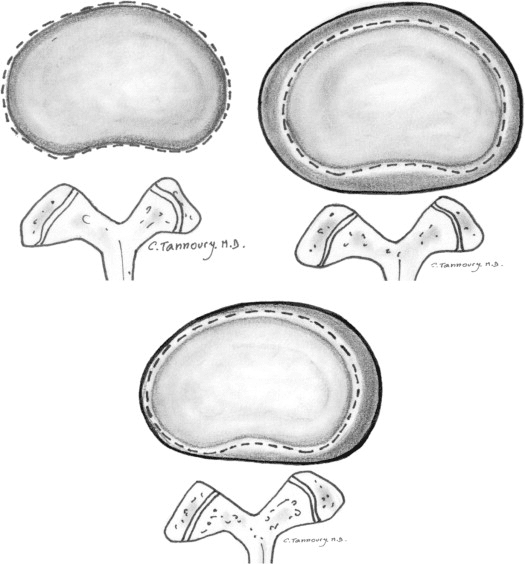
The presence of disc tissue extending beyond the edges of the ring apophyses, throughout the circumference of the disc, is called ��bulging�� and is not considered a form of herniation (Fig. 3, Top Right). Asymmetric bulging of disc tissue greater than 25% of the disc circumference (Fig. 3, Bottom), often seen as an adaptation to adjacent deformity, is, also, not a form of herniation. In evaluating the shape of the disc for a herniation in an axial plane, the shape of the two adjacent vertebrae must be considered [15, 35].
Figure 3: Bulging disc. (Top Left) Normal disc (for comparison); no disc material extends beyond the periphery of the disc space, depicted here by the broken line. (Top Right) Symmetric bulging disc; annular tissue extends, usually by less than 3 mm, beyond the edges of the vertebral apophyses symmetrically throughout the circumference of the disc. (Bottom) Asymmetric bulging disc; annular tissue extends beyond the edges of the vertebral apophysis, asymmetrically greater than 25% of the circumference of the disc.
Herniated discs may be classified as protrusion or extrusion, based on the shape of the displaced material.
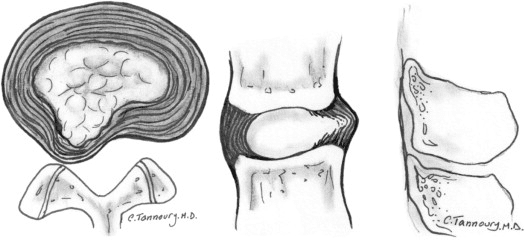
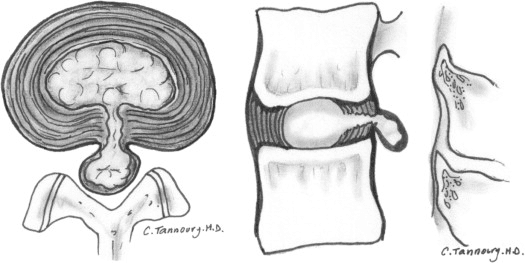
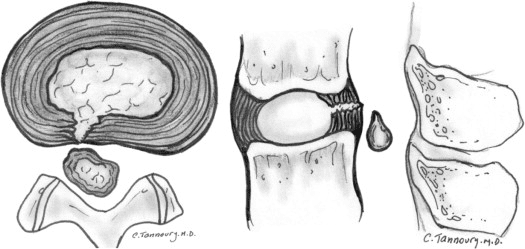
Protrusion is present if the greatest distance between the edges of the disc material presenting outside the disc space is less than the distance between the edges of the base of that disc material extending outside the disc space. The base is defined as the width of disc material at the outer margin of the disc space of origin, where disc material displaced beyond the disc space is continuous with the disc material within the disc space (Fig. 4). Extrusion is present when, in at least one plane, any one distance between the edges of the disc material beyond the disc space is greater than the distance between the edges of the base of the disc material beyond the disc space or when no continuity exists between the disc material beyond the disc space and that within the disc space (Fig. 5). The latter form of extrusion is best further specified or subclassified as sequestration if the displaced disc material has lost continuity completely with the parent disc (Fig. 6). The term migration may be used to signify displacement of disc material away from the site of extrusion. Herniated discs in the craniocaudad (vertical) direction through a gap in the vertebral body end plate are referred to as intravertebral herniations (Schmorl nodes) (Fig. 7).
Figure 4: Herniated disc: protrusion. (Left) Axial and (Right) sagittal images demonstrate displaced disc material extending beyond less than 25% of the disc space, with the greatest measure, in any plane, of the displaced disc material being less than the measure of the base of displaced disc material at the disc space of origin, measured in the same plane.
Figure 5: Herniated disc: extrusion. (Left) Axial and (Right) sagittal images demonstrate that the greatest measure of the displaced disc material is greater than the base of the displaced disc material at the disc space of origin, when measured in the same plane.
Figure 6: Herniated disc: sequestration. (Left) Axial and (Right) sagittal images show that a sequestrated disc is an extruded disc in which the displaced disc material has lost all connection with the disc of origin.
Figure 7:�Intravertebral herniation (Schmorl node). Disc material is displaced beyond the disc space through the vertebral end plate into the vertebral body, as shown here in sagittal projection
Disc herniations may be further specifically categorized as contained, if the displaced portion is covered by outer annulus fibers and/or the posterior longitudinal ligament, or uncontained when absent of any such covering. If the margins of the disc protrusion are smooth on axial computed tomography (CT) or magnetic resonance imaging (MRI), then the displaced disc material is likely contained by the posterior longitudinal ligament and perhaps a few superficial posterior annular fibers [21, 35, 36, 37]. If the posterior margin of the disc protrusion is irregular, the herniation is likely uncontained. Displaced disc tissue is typically described by location, volume, and content, as discussed later in this document.
An alternative scheme of distinguishing protrusion from extrusion is discussed in the Discussion section.
Trauma
The category of trauma includes disruption of the disc associated with physical and/or imaging evidence of violent fracture and/or dislocation and does not include repetitive injury, contribution of less than violent trauma to the degenerative process, fragmentation of the ring apophysis in conjunction with disc herniation, or disc abnormalities in association with degenerative subluxations. Whether or not a ��less than violent�� injury has contributed to or been superimposed on a degenerative change is a clinical judgment that cannot be made based on images alone; therefore, from the standpoint of description of images, such discs, in the absence of significant imaging evidence of associated violent injury, should be classified as degeneration rather than trauma.
Inflammation/Infection
The category of inflammation/infection includes infection, infection-like inflammatory discitis, and inflammatory response to spondyloarthropathy. It also includes inflammatory spondylitis of the subchondral end plate and bone marrow manifested by Modic Type I MRI changes [29, 30, 38] and usually associated with degenerative pathologic changes in the disc. To simplify the classification scheme, the category is inclusive of disparate conditions; therefore, when data permit, the diagnosis should be subcategorized for appropriate specificity.
Neoplasia
Primary or metastatic morphologic changes of disc tissues caused by malignancy are categorized as neoplasia, with subcategorization for appropriate specificity.
Miscellaneous Paradiscal Masses of Uncertain Origin
Although most intraspinal cysts are of meningeal or synovial origin, a minority arise from the disc and create a paradiscal mass that does not contain nuclear material. Epidural bleeding and/or edema, unrelated to trauma or other known origin may create a paradiscal mass or may increase the size of herniated disc material. Such cysts and hematomas may be seen acutely and unaccompanied by other pathology or may be a component of chronic disc pathology.
Morphologic�Variant of Unknown Significance
Instances in which data suggest abnormal morphology of the disc, but in which data are not complete enough to support a diagnostic categorization can be categorized as a morphologic variant of unknown significance.
Discussion of Nomenclature in Detail
This document provides a nomenclature that facilitates the description of surgical, endoscopic, or cadaveric findings as well as imaging findings; and also, with the caveat that it addresses only the morphology of the disc, it facilitates communication for patients, families, employers, insurers, and legal and social authorities and permits accumulation of more reliable data for research.
Normal Disc
Categorization of a disc as ��normal�� means the disc is fully and normally developed and free of any changes of disease, trauma, or aging. Only the morphology, and not the clinical context, is considered. Clinically ��normal�� (asymptomatic) people may have a variety of harmless imaging findings, including congenital or developmental variations of discs, minor bulging of the annuli, age-related desiccation, anterior and lateral marginal vertebral body osteophytes, prominence of disc material beyond one end plate as a result of luxation of one vertebral body relative to the adjacent vertebral body (especially common at L5�S1), and so on [39]. By this article�s morphology-based nomenclature and classification, however, such individual discs are not considered ��normal,�� but rather are described by their morphologic characteristics, independent of their clinical import unless otherwise specified.
Disc with Fissures of the Annulus
There is a general agreement about the various forms of loss of integrity of the annulus, such as radial, transverse, and concentric fissures. Yu et al. [40] have shown that annular fissures, including radial, concentric, and transverse types, are present in nearly all degenerated discs [41]. If the disc is dehydrated on an MRI scan, it is likely that there is at least one or more small fissures in the annulus. Relatively wide, radially directed annular fissures, with stretch of the residual annular margin, at times involving avulsion of an annular fragment, have sometimes been called ��annular gaps,�� although the term is relatively new and not accepted as a standard [27].
The terms ��annular fissure�� and ��annular tear�� have been applied to the findings on T2-weighted MRI scans of localized high intensity zones (HIZ) within the annulus [30, 42, 43, 44]. High intensity zones represent fluid and/or granulation tissue and may enhance with gadolinium. Fissures occur in all degenerative discs but are not all visualized as HIZs. Discography reveals some fissures not seen by the MRI, but not all fissures are visualized by discography. Description of the imaging findings is most accurate when limited to the observation of an HIZ or discographically demonstrated fissure, with the understood caveat that there is an incomplete concordance with the HIZs, discogram images, and anatomically observed fissures.
As far back as the 1995 NASS document, authors have recommended that such lesions be termed ��fissures�� rather than ��tears,�� primarily out of concern that the word ��tear�� could be misconstrued as implying a traumatic etiology [9, 30, 45, 46]. Because of potential misunderstanding of the term ��annular tear,�� and consequent presumption that the finding of an annular fissure indicates that there has been an injury, the term ��annular tear�� should be considered nonstandard and ��annular fissure�� be the preferred term. Imaging observation of an annular fissure does not imply an injury or related symptoms, but simply defines the morphologic change in the annulus.
Degenerated Disc
Because there is a confusion in the differentiation of changes of pathologic degenerative processes in the disc from those of normal aging [17, 31, 47, 48, 49], the classification ��degenerated disc�� includes all such changes, thus does not compel the observer to differentiate the pathologic from the normal consequence of aging.
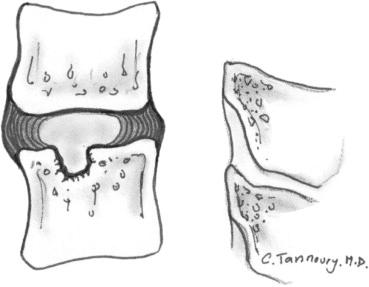
Perceptions of what constitutes the normal aging process of the spine have been greatly influenced by postmortem anatomic studies involving a limited number of specimens, harvested from cadavers from different age groups, with unknown past medical histories and the presumption of absence of lumbar symptoms [23, 50, 51, 52, 53, 54, 55, 56, 57]. With such methods, pathologic change is easily confused with consequences of normal aging. Resnick and Niwayama [31] emphasized the differentiating features of two degenerative processes involving the intervertebral disc that had been previously described by Schmorl and Junghanns [58]; ��spondylosis deformans,�� which affects essentially the annulus fibrosus and adjacent apophyses (Fig. 8, Left) and ��intervertebral osteochondrosis,�� which affects mainly the nucleus pulposus and the vertebral body end plates and may include extensive fissuring of the annulus fibrosus that may be followed by atrophy (Fig. 8, Right). Although Resnick and Niwayama stated that the cause of the two entities was unknown, other studies suggest that spondylosis deformans is the consequence of normal aging, whereas intervertebral osteochondrosis, sometimes also called ��deteriorated disc,�� results from a clearly pathologic, although not necessarily symptomatic, process [29, 31, 42, 59, 60].
Figure 8:�Types of disc degeneration by radiographic criteria. (Left) Spondylosis deformans is manifested by apophyseal osteophytes, with relative preservation of the disc space. (Right) Intervertebral osteochondrosis is typified by disc space narrowing, severe fissuring, and end plate cartilage erosion.
Degrees of disc degeneration have been graded based on gross morphology of midsagittal sections of the lumbar spine (Thompson scheme) [19]; postdiscography CT observations of integrity of the interior of the disc (Dallas classification) (Fig. 9) [42]; MRI observations of vertebral body marrow changes adjacent to the disc (Modic classification) [30], (Fig. 10); and MRI-revealed changes in the nucleus (Pfirrmann classification) [61]. Various modifications of these schemes have been proposed to suit specific clinical and research needs [17, 35, 62, 63].
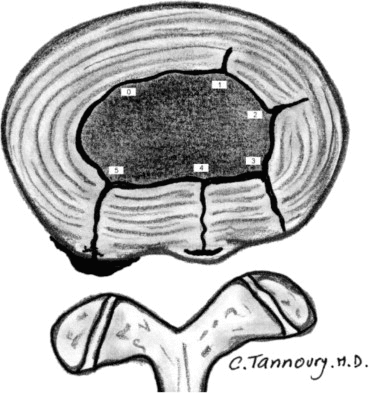
Figure 9:�Internal disc integrity. The extent of radial fissuring, as visualized on postdiscography CT, graded 0 to 5 by the Modified Dallas Discogram classification, as depicted.
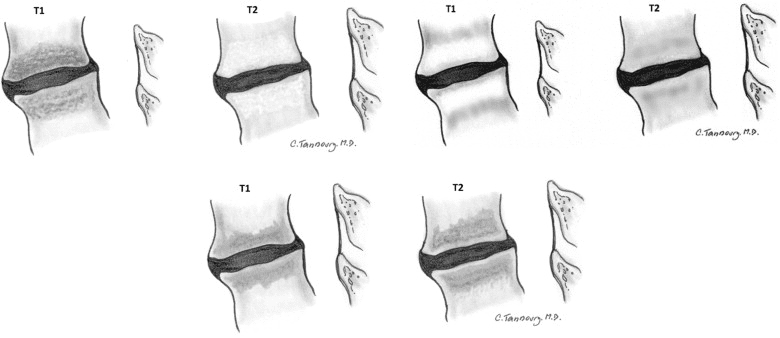
Figure 10:�Reactive vertebral body marrow changes. These bone marrow signal changes adjacent to a degenerated disc on magnetic resonance imaging. T1- and T2-weighted sequences are frequently classified as (Top Left) Modic I, (Top Right) Modic II, or (Bottom) Modic III.
Herniated Disc
The needs of common practices make necessary a diagnostic term that describes disc material beyond the intervertebral disc space. Herniated disc, herniated nucleus pulposus (HNP), ruptured disc, prolapsed disc (used nonspecifically), protruded disc (used nonspecifically), and bulging disc (used nonspecifically) have all been used in the literature in various ways to denote imprecisely defined displacement of disc material beyond the interspace. The absence of clear understanding of the meaning of these terms and the lack of definition of limits that should be placed on an ideal general term have created a great deal of confusion in clinical practice and in attempts to make meaningful comparisons of research studies.
For the general diagnosis of displacement of disc material, the single term that is most commonly used and creates least confusion is ��herniated disc.�� ��Herniated nucleus pulposus�� is inaccurate because materials other than nucleus (cartilage, fragmented apophyseal bone, and fragmented annulus) are common components of displaced disc material [64]. ��Rupture�� casts an image of tearing apart and therefore carries more implication of traumatic etiology than ��herniation,�� which conveys an image of displacement rather than disruption.
Though ��protrusion�� has been used by some authors in a nonspecific general sense to signify any displacement, the term has a more commonly used specific meaning for which it is best reserved. ��Prolapse,�� which has been used as a general term, as synonymous with the specific meaning of protrusion, or to denote inferior migration of extruded disc material, is not frequently used in a way to provide specific meaning and is best regarded as nonstandard, in deference to the more specific terms ��protrusion�� and ��extrusion.��
By exclusion of other terms, and by reasons of simplicity and common usage, ��herniated disc�� is the best general term to denote displacement of disc material. The term is appropriate to denote the general diagnostic category when referring to a specific disc and to be inclusive of various types of displacements when speaking of groups of discs. The term includes discs that may properly be characterized by more specific terms, such as ��protruded disc�� or ��extruded disc.�� The term ��herniated disc,�� as defined in this work, refers to localized displacement of nucleus, cartilage, fragmented apophyseal bone, or fragmented annular tissue beyond the intervertebral disc space. ��Localized�� is defined as less than 25% of the disc circumference. The disc space is defined, craniad and caudad, by the vertebral body end plates and, peripherally, by the edges of the vertebral ring apophyses, exclusive of the osteophyte formation. This definition was deemed more practical, especially for the interpretation of imaging studies, than a pathologic definition requiring identification of disc material forced out of normal position through an annular defect. Displacement of disc material, either through a fracture or defect in the bony end plate or in conjunction with displaced fragments of fractured walls of the vertebral body, may be described as ��herniated�� disc, although such description should accompany description of the fracture so as to avoid confusion with primary herniation of disc material. Displacement of disc materials from one location to another within the interspace, as with intraannular migration of nucleus without displacement beyond the interspace, is not considered herniation.
To be considered ��herniated,�� disc material must be displaced from its normal location and not simply represent an acquired growth beyond the edges of the apophyses, as is the case when connective tissues develop in gaps between osteophytes or when annular tissue is displaced behind one vertebra as an adaptation to subluxation. Herniation, therefore, can only occur in association with disruption of the normal annulus or, as in the case of intravertebral herniation (Schmorl node), a defect in the vertebral body end plate.
Details of the internal architecture of the annulus are most often not visualized by even the best quality MRIs [21]. The distinction of herniation is made by the observation of displacement of disc material beyond the edges of the ring apophysis that is ��focal�� or ��localized,�� meaning less than 25% of the circumference of the disc. The 25% cutoff line is established by way of convention to lend precision to terminology and does not designate etiology, relation to symptoms, or treatment indications.
The terms ��bulge�� or ��bulging�� refer to a generalized extension of disc tissue beyond the edges of the apophyses [65]. Such bulging involves greater than 25% of the circumference of the disc and typically extends a relatively short distance, usually less than 3 mm, beyond the edges of the apophyses (Fig. 3). ��Bulge�� or ��bulging�� describes a morphologic characteristic of various possible causes. Bulging is sometimes a normal variant (usually at L5�S1), can result from an advanced disc degeneration or from a vertebral body remodeling (as consequent to osteoporosis, trauma, or adjacent structure deformity), can occur with ligamentous laxity in response to loading or angular motion, can be an illusion caused by posterior central subligamentous disc protrusion, or can be an illusion from volume averaging (particularly with CT axial images).
Bulging, by definition, is not a herniation. Application of the term ��bulging�� to a disc does not imply any knowledge of etiology, prognosis, or need for treatment or imply the presence of symptoms.
A disc may have, simultaneously, more than one herniation. A disc herniation may be present along with other degenerative changes, fractures, or abnormalities of the disc. The term ��herniated disc�� does not imply any knowledge of etiology, relation to symptoms, prognosis, or need for treatment.
When data are sufficient to make the distinction, a herniated disc may be more specifically characterized as ��protruded�� or ��extruded.�� These distinctions are based on the shape of the displaced material. They do not imply knowledge of the mechanism by which the changes occurred.
Protruded Discs
Disc protrusions are focal or localized abnormalities of the disc margin that involve less than 25% of the disc circumference. A disc is ��protruded�� if the greatest dimension between the edges of the disc material presenting beyond the disc space is less than the distance between the edges of the base of that disc material that extends outside the disc space. The base is defined as the width of the disc material at the outer margin of the disc space of origin, where disc material displaced beyond the disc space is continuous with the disc material within the disc space (Fig. 4). The term ��protrusion�� is only appropriate in describing herniated disc material, as discussed previously.
Extruded Discs
The term ��extruded�� is consistent with the lay language meaning of material forced from one domain to another through an aperture [37, 64]. With reference to a disc, the test of extrusion is the judgment that, in at least one plane, any one distance between the edges of the disc material beyond the disc space is greater than the distance between the edges of the base measured in the same plane or when no continuity exists between the disc material beyond the disc space and that within the disc space (Fig. 5). Extruded disc material that has no continuity with the disc of origin may be characterized as ��sequestrated�� [53, 66] (Fig. 6). A sequestrated disc is a subtype of ��extruded disc�� but, by definition, can never be a ��protruded disc.�� Extruded disc material that is displaced away from the site of extrusion, regardless of continuity with the disc, may be called ��migrated,�� a term that is useful for the interpretation of imaging studies because it is often impossible from images to know if continuity exists.
The aforementioned distinctions between protrusion and extrusion and between contained and uncontained are based on common practice and wide acceptance of the definitions in the original version of this document. Another set of criteria, espoused by some respected practitioners, defines extrusion as uncontained and protrusion as a persistence of containment, regardless of the relative dimensions of the base to displaced portion of disc material. Per these criteria, a disc extrusion can be identified by the presence of a continuous line of low signal intensity surrounding the disc herniation. They state that current advanced imaging permits this basis of distinction and that the presence or absence of containment has more clinical relevance than the morphology of the displaced material [35].
Whether their method will prove superior to the currently recommended method will be determined by future study. The use of the distinction between ��protrusion�� and ��extrusion�� is optional and some observers may prefer to use, in all cases, the more general term ��herniation.�� Further distinctions can often be made regarding containment, continuity, volume, composition, and location of the displaced disc material.
Containment, Continuity, and Migration
Herniated disc material can be ��contained�� or ��uncontained.�� The test of containment is whether the displaced disc tissues are wholly held within intact outer annulus and/or posterior longitudinal ligament fibers. Fluid or any contrast that has been injected into a disc with a ��contained�� herniation would not be expected to leak into the vertebral canal. Although the posterior longitudinal ligament and/or peridural membrane may partially cover the extruded disc tissues, such discs are not considered ��contained�� unless the posterior longitudinal ligament is intact. The technical limitations of currently available noninvasive imaging modalities (CT and MRI) often preclude the distinction of a contained from an uncontained disc herniation. CT-discography does not always allow one to distinguish whether the herniated components of a disc are contained, but only whether there is a communication between the disc space and the vertebral canal.
Displaced disc fragments are sometimes characterized as ��free.�� A ��free fragment�� is synonymous with a ��sequestrated fragment,�� but not synonymous with ��uncontained.�� A disc fragment should be considered ��free�� or ��sequestrated�� only if there is no remaining continuity of the disc material between it and the disc of origin. A disc can be ��uncontained,�� with the loss of integrity of the posterior longitudinal ligament and the outer annulus, but still have continuity between the herniated/displaced disc material and the disc of origin.
The term ��migrated�� disc or fragment refers to the displacement of most of the displaced disc material away from the opening in the annulus through which the material has extruded. Some migrated fragments will be sequestrated, but the term ��migrated�� refers only to position and not to continuity.
The terms ��capsule�� and ��subcapsular�� have been used to refer to containment by an unspecified combination of annulus and ligament. These terms are nonpreferred.
Referring specifically to the posterior longitudinal ligament, some authors have distinguished displaced disc material as ��subligamentous,�� ��extraligamentous,�� ��transligamentous,�� or ��perforated.�� The term ��subligamentous�� is favored as an equivalent to ��contained.��
Volume and Composition of Displaced Material
A scheme to define the degree of canal compromise produced by disc displacement should be practical, objective, reasonably precise, and clinically relevant. A simple scheme that fulfills the criteria uses two-dimensional measurements taken from an axial section at the site of the most severe compromise. Canal compromise of less than one third of the canal at that section is ��mild,�� between one and two-thirds is ��moderate,�� and greater than two-thirds is ��severe.�� The same grading can be applied for foraminal involvement.
Such characterizations of volume describe only the cross-sectional area at one section and do not account for the total volume of displaced material; proximity to, compression, and distortion of neural structures; or other potentially significant features, which the observer may further detail by narrative description.
Composition of the displaced material may be characterized by terms such as nuclear, cartilaginous, bony, calcified, ossified, collagenous, scarred, desiccated, gaseous, or liquefied.
Clinical significance related to the observation of volume and composition depends on the correlation with clinical data and cannot be inferred from morphologic data alone.
Location
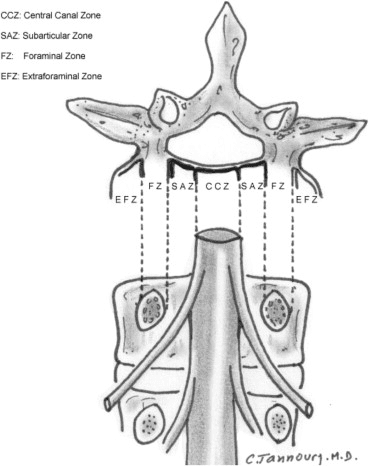
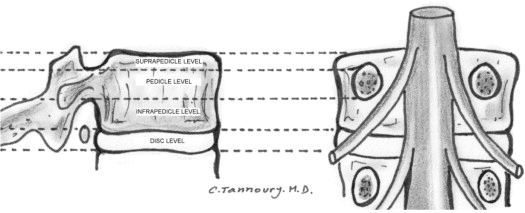
Bonneville proposed a useful and simple alphanumeric system to classify, according to location, the position of disc fragments that have migrated in the horizontal or sagittal plane [6, 13]. Using anatomic boundaries familiar to surgeons, Wiltse proposed another system [14, 67]. Anatomic ��zones�� and ��levels�� are defined using the following landmarks: medial edge of the articular facets; medial, lateral, upper, and lower borders of the pedicles; and coronal and sagittal planes at the center of the disc. On the horizontal (axial) plane, these landmarks determine the boundaries of the central zone, the subarticular zone (lateral recess), the foraminal zone, the extraforaminal zone, and the anterior zone, respectively (Fig. 11). On the sagittal (craniocaudal) plane, they determine the boundaries of the disc level, the infrapedicular level, the pedicular level, and the suprapedicular level, respectively (Fig. 12). The method is not as precise as the drawings depict because borderlines such as the medial edges of facets and the walls of the pedicles are curved, but the method is simple, practical, and in common usage.
Figure 11:�Anatomic zones depicted in axial and coronal projections.
Figure 12: Anatomic levels depicted in sagittal and coronal projections.
Moving from the central to right lateral in the axial (horizontal) plane, location may be defined as central, right central, right subarticular, right foraminal, or right extraforaminal. The term ��paracentral�� is less precise than defining ��right central�� or ��left central,�� but is useful in describing groups of discs that include both, or when speaking informally, when the side is not significant. For reporting of image observations of a specific disc, ��right central�� or ��left central�� should supersede the use of the term ��paracentral.�� The term ��far lateral�� is sometimes used synonymously with ��extraforaminal.��
In the sagittal plane, location may be defined as discal, infrapedicular, suprapedicular, or pedicular. In the coronal plane, anterior, in relationship to the disc, means ventral to the midcoronal plane of the centrum.
Glossary
Note:�some terms and definitions included in this Glossary are not recommended as preferred terminology but are included to facilitate the interpretation of vernacular and, in some cases, improper use. Preferred definitions are listed first. Nonstandard definitions are placed in brackets, and by consensus of the organizational task forces, should not be used in the manner described. Some terms are also labeled as colloquial, with further designation as to whether they are considered nonpreferred or nonstandard.
Acute disc herniation:�disc herniation of a relatively recent occurrence. Note: paradiscal inflammatory reaction and relatively bright signal of the disc material on T2-weighted images suggest relative acuteness. Such changes may persist for months, however. Thus, absent clinical correlation and/or serial studies, it is not possible to date precisely by imaging when a herniation occurred. An acutely herniated disc material may have brighter signal on T2-weighted MRI sequences than the disc from which the disc material originates [46,�59,�64,�68]. Note that a relatively acute herniation can be superimposed on a previously existing herniation. An acute disc herniation may regress spontaneously without specific treatment. See: chronic disc herniation.
Aging disc:�disc demonstrating any of the various effects of aging on the disc. Loss of water content from the nucleus occurs before MRI changes, followed by the progression of MRI manifested changes consistent with the progressive loss of water content and increase in collagen and aggregating proteoglycans. See Pfirrmann classification.
Annular fissure:�separations between annular fibers, separations of fibers from their vertebral body insertions, or separations of fibers that extend radially, transversely, or concentrically, involving one or many layers of the annular lamellae. Note that the terms ��fissure�� and ��tear�� have often been used synonymously in the past. The term ��tear�� is inappropriate for use in describing imaging findings and should not be used (tear: nonstandard). Neither term suggests injury or implies any knowledge of etiology, neither term implies any relationship to symptoms or that the disc is a likely pain generator, and neither term implies any need for treatment. See also: annular gap, annular rupture, annular tear, concentric fissure, HIZ, radial fissure, transverse fissure.
Annular gap�(nonstandard): focal attenuation (CT) or signal (MRI) abnormality, often triangular in shape, in the posterior aspect of the disc, likely representing widening of a radially directed annular fissure, bilateral annular fissures with an avulsion of the intermediate annular fragment, or an avulsion of a focal zone of macerated annulus.
Annular rupture:�disruption of fibers of the annulus by sudden violent injury. This is a clinical diagnosis; use of the term is inappropriate for a pure imaging description, which instead should focus on a detailed description of the findings. Ruptured annulus is�not�synonymous with ��annular fissure,�� or ��ruptured disc.��
Annular tear,�torn annulus�(nonstandard): see fissure of the annulus and rupture of annulus.
Anterior displacement:�displacement of disc tissues beyond the disc space into the anterior zone.
Anterior zone:�peridiscal zone that is anterior to the midcoronal plane of the vertebral body.
Anulus, annulus (abbreviated form of annulus fibrosus):�multilaminated fibrous tissue forming the periphery of each disc space, attaching, craniad and caudad, to end plate cartilage and a ring apophyseal bone and blending centrally with the nucleus pulposus. Note: either anulus or annulus is correct spelling. Nomina Anatomica uses both forms, whereas Terminologia Anatomica states �� anulus fibrosus�� [22]. Fibrosus has no correct alternative spelling; fibrosis has a different meaning and is incorrect in this context.
Asymmetric bulge:�presence of more than 25% of the outer annulus beyond the perimeter of the adjacent vertebrae, more evident in one section of the periphery of the disc than another, but not sufficiently focal to be characterized as a protrusion. Note: asymmetric disc bulging is a morphologic observation that may have various causes and does not imply etiology or association with symptoms. See bulge.
Balloon disc (colloquial, nonstandard):�diffuse apparent enlargement of the disc in superior-inferior extent because of bowing of the vertebral end plates due to weakening of the bone as in severe osteoporosis.
Base (of displaced disc):�the cross-sectional area of the disc material at the outer margin of the disc space of origin, where disc material beyond the disc space is continuous with disc material within the disc space. In the craniocaudal direction, the length of the base cannot exceed, by definition, the height of the intervertebral space. On axial imaging, base refers to the width at the outer margin of the disc space, of the origin of any disc material extending beyond the disc space.
Black disc�(colloquial, nonstandard): see dark disc.
Bulging disc, bulge (noun [n]), bulge (verb [v])
A disc in which the contour of the outer annulus extends, or appears to extend, in the horizontal (axial) plane beyond the edges of the disc space, usually greater than 25% (90�) of the circumference of the disc and usually less than 3 mm beyond the edges of the vertebral body apophysis.
(Nonstandard) A disc in which the outer margin extends over a broad base beyond the edges of the disc space.
(Nonstandard) Mild, diffuse, smooth displacement of disc.
(Nonstandard) Any disc displacement at the discal level.
Note:�bulging is an observation of the contour of the outer disc and is not a specific diagnosis. Bulging has been variously ascribed to redundancy of the annulus, secondary to the loss of disc space height, ligamentous laxity, response to loading or angular motion, remodeling in response to adjacent pathology, unrecognized and atypical herniation, and illusion from volume averaging on CT axial images. Mild symmetric posterior disc bulging may be a normal finding at L5�S1. Bulging may or may not represent pathologic change, physiologic variant, or normalcy. Bulging is not a form of herniation; discs known to be herniated should be diagnosed as herniation or, when appropriate, as specific types of herniation. See: herniated disc, protruded disc, extruded disc.
Calcified disc:�calcification within the disc space, not inclusive of osteophytes at the periphery of the disc space.
Cavitation:�spaces, cysts, clefts, or cavities formed within the nucleus and inner annulus from disc degeneration.
See vacuum disc.
Central zone:�zone within the vertebral canal between sagittal planes through the medial edges of each facet. Note: the center of the central zone is a sagittal plane through the center of the vertebral body. The zones to either side of the center plane are�right central�and�left central, which are preferred terms when the side is known, as when reporting imaging results of a specific disc. When the side is unspecified, or grouped with both right and left represented, the term�paracentral�is appropriate.
Chronic disc herniation:�a clinical distinction that a disc herniation is of long duration. There are no universally accepted definitions of the intervals that distinguish between acute, subacute, and chronic disc herniations. Serial MRIs revealing disc herniations that are unchanged in appearance over time may be characterized as chronic. Disc herniations associated with calcification or gas on CT may be suggested as being chronic. Even so, the presence of calcification or gas does not rule out an acutely herniated disc. Note that an acute disc herniation may be superimposed on a chronic disc herniation. Magnetic resonance imaging signal characteristics may, on rare occasion, allow differentiation of acute and chronic disc herniations [16,�59,�64]. In such cases, acutely herniated disc material may appear brighter than the disc of origin on T2-weighted sequences [46,�59,�61]. Also, see disc-osteophyte complex.
Claw osteophyte:�bony outgrowth arising very close to the disc margin, from the vertebral body apophysis, directed, with a sweeping configuration, toward the corresponding part of the vertebral body opposite the disc.
Collagenized disc or nucleus:�a disc in which the mucopolysaccharide of the nucleus has been replaced by fibrous tissue.
Communicating disc, communication (n), communicate (v)�(nonstandard): communication refers to interruption in the periphery of the disc annulus, permitting free passage of fluid injected within the disc to the exterior of the disc, as may be observed during discography. Not synonymous with ��uncontained.�� See ��contained disc�� and ��uncontained disc.��
Concentric fissure:�fissure of the annulus characterized by separation of annular fibers in a plane roughly parallel to the curve of the periphery of the disc, creating fluid-filled spaces between adjacent annular lamellae. See: radial fissures, transverse fissures, HIZ.
Displaced disc tissue existing wholly within an outer perimeter of uninterrupted outer annulus or posterior longitudinal ligament.
(Nonstandard) A disc with its contents mostly, but not wholly, within annulus or capsule.
(Nonstandard) A disc with displaced elements contained within any investiture of the vertebral canal.
A disc that is less than wholly contained by annulus, but under a distinct posterior longitudinal ligament, is contained. Designation as ��contained�� or ��uncontained�� defines the integrity of the ligamentous structures surrounding the disc, a distinction that is often but not always possible by advanced imaging. On CT and MRI scans, contained herniations typically have a smooth margin, whereas uncontained herniations most often have irregular margins because the outer annulus and the posterior longitudinal ligament have been penetrated by the disc material [35,�37]. CT-discography also does not always allow one to distinguish whether the herniated components of a disc are contained, but only whether there is communication between the disc space and the vertebral canal.
Continuity:�connection of displaced disc tissue by a bridge of disc tissue, however thin, to tissue within the disc of origin.
Dallas classification�(of postdiscography imaging): commonly used grading system for the degree of annular fissuring seen on CT imaging of discs after discography. Dallas Grade 0 is normal; Grade 1: leakage of contrast into the inner one-third of the annulus; Grade 2: leakage of contrast into the inner two-thirds of the annulus; Grade 3: leakage through the entire thickness of the annulus; Grade 4: contrast extends circumferentially; Grade 5: contrast extravasates into the epidural space (See discogram, discography).
Dark disc�(colloquial, nonstandard): disc with nucleus showing decreased signal intensity on T2-weighted images (dark), usually because of desiccation of the nucleus secondary to degeneration. Also: black disc (colloquial, nonstandard). See: disc degeneration, Pfirrmann classification.
Changes in a disc characterized to varying degrees by one or more of the following: desiccation, cleft formation, fibrosis, and gaseous degradation of the nucleus; mucinous degradation, fissuring, and loss of integrity of the annulus; defects in and/or sclerosis of the end plates; and osteophytes at the vertebral apophyses.
Imaging manifestation of such changes, including [35]�standard roentgenographic findings, such as disc space narrowing and peridiscal osteophytes, MRI disc findings (see Pfirrmann classification [61]), CT disc findings (see discogram/discography and Dallas classification [42]), and/or MRI findings of vertebral end plate and marrow reactive changes adjacent to a disc (see Modic classification [38]).
Degenerative disc disease�(nonstandard term when used as an imaging description): a condition characterized by manifestations of disc degeneration and symptoms thought to be related to those of degenerative changes. Note: causal connections between degenerative changes and symptoms are often difficult clinical distinctions. The term ��degenerative disc disease�� carries implications of illness that may not be appropriate if the only or primary indicators of illness are from imaging studies, and thus this term should not be used when describing imaging findings. The preferred term for description of imaging manifestations is ��degenerated disc�� or ��disc degeneration,�� rather than ��degenerative disc disease.��
Delamination:�separation of circumferential annular fibers along the planes parallel to the periphery of the disc, characterizing a concentric fissure of the annulus.
Desiccated disc
Disc with reduced water content, usually primarily of nuclear tissues.
Imaging manifestations of reduced water content of the disc, such as decreased (dark) signal intensity on T2-weighted images, or of apparent reduced water content, as from alterations in the concentration of hydrophilic glycosaminoglycans. See also: dark disc (colloquial, nonstandard).
Disc (disk):�complex structure composed of nucleus pulposus, annulus fibrosus, cartilaginous end plates, and vertebral body ring apophyseal attachments of annulus. Note: most English language publications use the spelling ��disc�� more often than ��disk�� [1,�20,�22,�69,�70]. Nomina Anatomica designates the structures as ��disci intervertebrales�� and Terminologia Anatomica as ��discus intervertebralis/intervertebral disc�� [22,�70]. (See ��disc level�� for naming and numbering of a particular disc).
Disc height:�The distance between the planes of the end plates of the vertebral bodies craniad and caudad to the disc. Disc height should be measured at the center of the disc, not at the periphery. If measured at the posterior or anterior margin of the disc on a sagittal image of the spine, this should be clearly specified as such.
Disc level:�Level of the disc and vertebral canal between axial planes through the bony end plates of the vertebrae craniad and caudad to the disc being described.
A particular disc is best named by naming the region of the spine and the vertebra above and below it; for example, the disc between the fourth and fifth lumbar vertebral bodies is named ��lumbar 4�5,�� commonly abbreviated as L4�L5, and the disc between the fifth lumbar vertebral body and the first sacral vertebral body is called ��lumbosacral disc�� or ��L5�S1.�� Common anomalies include patients with six lumbar vertebrae or transitional vertebrae at the lumbosacral junction that require, for clarity, narrative explanation of the naming of the discs.
(Nonstandard) A disc is sometimes labeled by the vertebral body above it; for example, the disc between L4 and L5 may be labeled ��the L4 disc��.
Note: ��a motion segment,�� numbered in the same way, is a functional unit of the spine, comprising the vertebral body above and below, the disc, the facet joints, and the connecting soft tissues and is most often referenced with regard to the stability of the spine.
Disc of origin:�disc from which a displaced fragment originated. Synonym: parent disc. Note: since displaced fragments often contain tissues other than nucleus, disc of origin is preferred to nucleus of origin. Parent disc is synonymous, but more colloquial and nonpreferred.
Disc space:�space limited, craniad and caudad, by the end plates of the vertebrae and peripherally by the edges of the vertebral body ring apophyses, exclusive of osteophytes. Synonym: intervertebral disc space. See ��disc�� level for naming and numbering of discs.
Discogenic vertebral sclerosis:�increased bone density and calcification adjacent to the end plates of the vertebrae, craniad and caudad, to a degenerated disc, sometimes associated with intervertebral osteochondrosis. Manifested on MRI as Modic Type�III.
Discogram, discography:�a diagnostic procedure in which contrast material is injected into the nucleus of the disc with radiographic guidance and observation, often followed by CT/discogram. The procedure is often accompanied by pressure measurements and assessment of pain response (provocative discography). The degree of annular fissuring identified by discography may be defined by the Dallas classification and its modifications (See Dallas classification).
Disc-osteophyte complex:�intervertebral disc displacement, whether bulge, protrusion, or extrusion, associated with calcific ridges or ossification. Sometimes called a hard disc or chronic disc herniation (nonpreferred). Distinction should be made between ��spondylotic disc herniation,�� or ��calcified disc herniation�� (nonpreferred), the remnants of an old disc herniation; and ��spondylotic bulging disc,�� a broad-based bony ridge presumably related to chronic bulging disc.
Displaced disc�(nonstandard): a disc in which disc material is beyond the outer edges of the vertebral body ring apophyses (exclusive of osteophytes) of the craniad and caudad vertebrae, or, as in the case of intravertebral herniation, has penetrated through the vertebral body end plate.
Note: displaced disc is a general term that does not imply knowledge of the underlying pathology, cause, relationship to symptoms, or need for treatment. The term includes, but is not limited to, disc herniation and disc migration. See: herniated disc, migrated disc.
Epidural membrane:�See peridural membrane.
Extraforaminal zone:�the peridiscal zone beyond the sagittal plane of the lateral edges of the pedicles, having no well-defined lateral border, but definitely posterior to the anterior zone. Synonym: ��far lateral zone,�� also ��far-out zone�� (nonstandard).
Extraligamentous:�posterior or lateral to the posterior longitudinal ligament. Note: extraligamentous disc refers to displaced disc tissue that is located posterior or lateral to the posterior longitudinal ligament. If the disc has extruded through the posterior longitudinal ligament, it is sometimes called ��transligamentous�� or ��perforated�� and if through the peridural membrane, it is sometimes refined to ��transmembranous.��
Extruded disc, extrusion (n), extrude (v):�a herniated disc in which, in at least one plane, any one distance between the edges of the disc material beyond the disc space is greater than the distance between the edges of the base of the disc material beyond the disc space in the same plane or when no continuity exists between the disc material beyond the disc space and that within the disc space. Note: the preferred definition is consistent with the common image of extrusion, as an expulsion of material from a container through and beyond an aperture. Displacement beyond the outer annulus of the disc material with any distance between its edges greater than the distance between the edges of the base distinguishes extrusion from protrusion. Distinguishing extrusion from protrusion by imaging is best done by measuring the edges of the displaced material and the remaining continuity with the disc of origin, whereas relationship of the displaced portion to the aperture through which it has passed is more readily observed surgically. Characteristics of protrusion and extrusion may coexist, in which case the disc should be subcategorized as extruded. Extruded discs in which all continuity with the disc of origin is lost may be further characterized as ��sequestrated.�� Disc material displaced away from the site of extrusion may be characterized as ��migrated.�� See: herniated disc, migrated disc, protruded disc.
Note: An alternative scheme is espoused by some respected radiologists who believe it has better clinical application. This scheme defines extruded disc as synonymous with �uncontained disc� and does not use comparative measurements of the base versus the displaced material. Per this definition, a disc extrusion can be identified by the presence of a continuous line of low signal intensity surrounding the disc herniation. Future study will further determine the validity of this alternative definition. See: contained disc.
Far lateral zone:�the peridiscal zone beyond the sagittal plane of the lateral edge of the pedicle, having no well defined lateral border, but definitely posterior to the anterior zone. Synonym: ��extraforaminal zone.��
Fissure of annulus:�see annular fissure.
Foraminal zone:�the zone between planes passing through the medial and lateral edges of the pedicles. Note: the foraminal zone is sometimes called the ��pedicle zone�� (nonstandard), which can be confusing because pedicle zone might also refer to measurements in the sagittal plane between the upper and lower surfaces of a given pedicle that is properly called the ��pedicle level.�� The foraminal zone is also sometimes called the ��lateral zone�� (nonstandard), which can be confusing because the ��lateral zone�� can be confused with ��lateral recess�� (subarticular zone) and can also mean extraforaminal zone or an area including both the foraminal and extraforaminal zones.
Free fragment
A fragment of disc that has separated from the disc of origin and has no continuous bridge of disc tissue with disc tissue within the disc of origin. Synonym: sequestrated disc.
(Nonstandard) A fragment that is not contained within the outer perimeter of the annulus.
(Nonstandard) A fragment that is not contained within the annulus, posterior longitudinal ligament, or peridural membrane.
Note: ��sequestrated disc�� and ��free fragment�� are virtually synonymous. When referring to the condition of the disc, categorization as extruded with subcategorization as sequestrated is preferred, whereas when referring specifically to the fragment, free fragment is preferred.
Gap of annulus:�see annular gap.
Hard disc (colloquial):�disc displacement in which the displaced portion has undergone calcification or ossification and may be intimately associated with apophyseal osteophytes. Note: the term ��hard disc�� is most often used in reference to the cervical spine to distinguish chronic hypertrophic and reactive changes at the periphery of the disc from the more acute extrusion of soft, predominantly nuclear tissue. See: chronic disc herniation, disc-osteophyte complex.
Herniated disc, herniation (n), herniated (v):�localized or focal displacement of disc material beyond the normal margin of the intervertebral disc space. Note: ��localized�� or ��focal�� means, by way of convention, less than 25% (90�) of the circumference of the disc.
Herniated disc material may include nucleus pulposus, cartilage, fragmented apophyseal bone, or annulus fibrosus tissue. The normal margins of the intervertebral disc space are defined, craniad and caudad, by the vertebral body end plates and peripherally by the edges of the vertebral body ring apophyses, exclusive of osteophytic formations. Herniated disc generally refers to displacement of disc tissues through a disruption in the annulus, the exception being intravertebral herniations (Schmorl nodes) in which the displacement is through the vertebral end plate. Herniated discs may be further subcategorized as protruded or extruded. Herniated disc is sometimes referred to as HNP, but the term ��herniated disc�� is preferred because displaced disc tissues often include cartilage, bone fragments, or annular tissues. The terms ��prolapse�� and ��rupture�� when referring to disc herniations are nonstandard and their use should be discontinued. Note: ��herniated disc�� is a term that does not imply knowledge of the underlying pathology, cause, relationship to symptoms, or need for treatment.
Herniated nucleus pulposus�(HNP, nonpreferred): see herniated disc.
High intensity zone (HIZ):�area of high intensity on T2-weighted MRIs of the disc, located commonly in the outer annulus. Note: HIZs within the posterior annular substance may indicate the presence of an annular fissure within the annulus, but these terms are not synonymous. An HIZ itself may represent the actual annular fissure or alternatively, may represent vascularized fibrous tissue (granulation tissue) within the substance of the disc in an area adjacent to a fissure. The visualization of an HIZ does not imply a traumatic etiology or that the disc is a source of pain.
Infrapedicular level:�the level between the axial planes of the inferior edges of the pedicles craniad to the disc in question and the inferior end plate of the vertebral body above the disc in question. Synonym: superior vertebral notch.
Internal disc disruption:�disorganization of structures within the disc. See intraannular displacement
Intervertebral osteochondrosis:�degenerative process of the disc and vertebral body end plates that is characterized by disc space narrowing, vacuum phenomenon, and vertebral body reactive changes. Synonym: osteochondrosis (nonstandard).
Intraannular displacement:�displacement of central, predominantly nuclear, tissue to a more peripheral site within the disc space, usually into a fissure in the annulus. Synonym: (nonstandard) intraannular herniation, intradiscal herniation. Note: intraannular displacement is distinguished from disc herniation, that is, herniation of disc refers to displacement of disc tissues beyond the disc space. Intraannular displacement is a form of internal disruption. When referring to intraannular displacement, it is best not to use the term ��herniation�� to avoid confusion with disc herniation.
Intradural herniation:�disc material that has penetrated the dura so that it lies in an intradural extramedullary location.
Intravertebral herniation:�a disc displacement in which a portion of the disc projects through the vertebral end plate into the centrum of the vertebral body. Synonym: Schmorl node.
Lateral recess:�that portion of the subarticular zone that is medial to the medial border of the pedicle. It refers to the entire cephalad-caudad region that exists medial to the pedicle, where the same numbered thoracic or lumbar nerve root travels caudally before exiting the nerve root foramen under the caudal margin of the pedicle. It does not refer to the nerve root foramen itself. See also subarticular zone.
Lateral zone�(nonstandard): see foraminal zone.
Leaking disc�(nonstandard): see communicating disc.
Limbus vertebra:�separation of a segment of vertebral ring apophysis. Note: limbus vertebra may be a developmental abnormality caused by failure of integration of the ossifying apophysis to the vertebral body; a chronic herniation (extrusion) of the disc into the vertebral body at the junction of the fusing apophyseal ring, with separation of a portion of the ring with bony displacement; or a fracture through the apophyseal ring associated with intrabody disc herniation. This occurs in children before the apophyseal ring fuses to the vertebral body. In adults, a limbus vertebra should not be confused with an acute fracture. A limbus vertebra does not imply that there has been an injury to the disc or the adjacent apophyseal end plate.
Marginal osteophyte:�osteophyte that protrudes from and beyond the outer perimeter of the vertebral end plate apophysis.
1.Herniated disc in which a portion of the extruded disc material is displaced away from the fissure in the outer annulus through which it has extruded in either sagittal or axial plane.
2.(Nonstandard) A herniated disc with a free fragment or sequestrum beyond the disc level.
Note: migration refers to the position of the displaced disc material, rather than to its continuity with disc tissue within the disc of origin; therefore, it is not synonymous with sequestration.
Modic classification (Type I, II, and III)�[30]: a classification of degenerative changes involving the vertebral end plates and adjacent vertebral bodies associated with disc inflammation and degenerative disc disease, as seen on MRIs. Type I refers to decreased signal intensity on T1-weighted spin echo images and increased signal intensity on T2-weighted images, representing penetration of the end plate by fibrovascular tissue, inflammatory changes, and perhaps edema. Type I changes may be chronic or acute. Type II refers to increased signal intensity on T1-weighted images and isointense or increased signal intensity on T2-weighted images, indicating replacement of normal bone marrow by fat. Type III refers to decreased signal intensity on both T1-and T2-weighted images, indicating reactive osteosclerosis (See: discogenic vertebral sclerosis).
Motion segment:�the functional unit of the spine. See disc level.
Nonmarginal osteophyte:�an osteophyte that occurs at sites other than the vertebral end plate apophysis. See: marginal osteophyte.
Normal disc:�a fully and normally developed disc with no changes attributable to trauma, disease, degeneration, or aging. Note: many congenital and developmental variations may be clinically normal; that is, they are not associated with symptoms, and certain adaptive changes in the disc may be normal considering adjacent pathology; however, classification and reporting for medical purposes is best served if such discs are not considered normal. Note, however, that a disc finding considered not normal does not necessarily imply a cause for clinical signs or symtomatology; the description of any variation of the disc is independent of clinical judgment regarding what is normal for a given patient.
Nucleus of origin (nonpreferred):�the central, nuclear portion of the disc of reference, usually used to reference the disc from which the tissue has been displaced. Note: since displaced fragments often contain tissues other than the nucleus, disc of origin is preferred to nucleus of origin. Synonym: disc of origin (preferred), parent nucleus (nonpreferred).
Osteophyte:�focal hypertrophy of the bone surface and/or ossification of the soft tissue attachment to the bone.
Paracentral:�in the right or left central zone of the vertebral canal. See central zone. Note: the terms ��right central�� or ��left central�� are preferable when speaking of a single site when the side can be specified, as when reporting the findings of imaging procedures. ��Paracentral�� is appropriate if the side is not significant or when speaking of mixed sites.
Parent disc�(nonpreferred): see disc of origin.
Parent nucleus�(nonpreferred): see nucleus of origin, disc of origin.
Pedicular level:�the space between the axial planes through the upper and lower edges of the pedicle. Note: the pedicular level may be further designated with reference to the disc in question as ��pedicular level above�� or ��pedicular level below�� the disc in question.
Perforated (nonstandard):�see transligamentous.
Peridural membrane:�a delicate, translucent membrane that attaches to the undersurface of the deep layer of the posterior longitudinal ligament, and extends laterally and posteriorly, encircling the bony spinal canal outside the dura. The veins of Batson plexus lie on the dorsal surface of the peridural membrane and pierce it ventrally. Synonym: lateral membrane, epidural membrane.
Pfirrmann classification:�a grading system for the severity of degenerative changes within the nucleus of the intervertebral disc. A Pfirrmann Grade I disc has a uniform high signal in the nucleus on T2-weighted MRI; Grade II shows a central horizontal line of low signal intensity on sagittal images; Grade III shows high intensity in the central part of the nucleus with lower intensity in the peripheral regions of the nucleus; Grade IV shows low signal intensity centrally and blurring of the distinction between nucleus and annulus; and Grade V shows homogeneous low signal with no distinction between nucleus and annulus.[61]
Prolapsed disc, prolapse (n, v)�(nonstandard): the term is variously used to refer to herniated discs. Its use is not standardized and the term does not add to the precision of disc description, so is regarded as nonstandard in deference to ��protrusion�� or ��extrusion.��
Protruded disc, protrusion (n), protrude (v):�1. One of the two subcategories of a ��herniated disc�� (the other being an ��extruded disc��) in which disc tissue extends beyond the margin of the disc space, involving less than 25% of the circumference of the disc margin as viewed in the axial plane. The test of protrusion is that there must be localized (less than 25% of the circumference of the disc) displacement of disc tissue and the distance between the corresponding edges of the displaced portion must not be greater than the distance between the edges of the base of the displaced disc material at the disc space of origin (See base of displaced disc). While sometimes used as a general term in the way herniation is defined, the use of the term ��protrusion�� is best reserved for subcategorization of herniation meeting the above criteria. 2. (nonstandard) Any or unspecified type of disc herniation.
Radial fissure:�disruption of annular fibers extending from the nucleus outward toward the periphery of the annulus, usually in the craniad-caudad (vertical) plane, although, at times, with axial horizontal (transverse) components. ��Fissure�� is the preferred term to the nonstandard term ��tear.�� Neither term implies knowledge of injury or other etiology. Note: Occasionally, a radial fissure extends in the transverse plane to include an avulsion of the outer layers of annulus from the apophyseal ring. See concentric fissures, transverse fissures.
Rim lesion (nonstandard): See limbus vertebra.
Rupture of annulus, ruptured annulus:�see annular rupture.
Ruptured disc, rupture�(nonstandard): a herniated disc. The term ��ruptured disc�� is an improper synonym for herniated disc, not to be confused with violent disruption of the annulus related to injury. Its use should be discontinued.
Schmorl node:�see intravertebral herniation.
Sequestrated disc, sequestration (n), sequestrate (v); (variant: sequestered disc):�an extruded disc in which a portion of the disc tissue is displaced beyond the outer annulus and maintains no connection by disc tissue with the disc of origin. Note: an extruded disc may be subcategorized as ��sequestrated�� if no disc tissue bridges the displaced portion and the tissues of the disc of origin. If even a tenuous connection by disc tissue remains between a displaced fragment and disc of origin, the disc is not sequestrated. If a displaced fragment has no connection with the disc of origin, but is contained within peridural membrane or under a portion of posterior longitudinal ligament that is not intimately bound with the annulus of origin, the disc is considered sequestrated. Sequestrated and sequestered are used interchangeably. Note: ��sequestrated disc�� and ��free fragment�� are virtually synonymous. See: free fragment. When referring to the condition of the disc, categorization as extruded with subcategorization as sequestered is preferred, whereas when referring specifically to the fragment, free fragment is preferred. See sequestrum.
Sequestrum (nonpreferred):�refers to disc tissue that has displaced from the disc space of origin and lacks any continuity with disc material within the disc space of origin. Synonym: free fragment (preferred). See sequestrated disc. Note: ��sequestrum�� (nonpreferred) refers to the isolated free fragment itself, whereas sequestrated disc defines the condition of the disc.
Spondylitis:�inflammatory disease of the spine, other than degenerative disease. Note: spondylitis usually refers to noninfectious inflammatory spondyloarthropathies.
Spondylosis:�1. Common nonspecific term used to describe effects generally ascribed to degenerative changes in the spine, particularly those involving hypertrophic changes to the apophyseal end plates and zygapophyseal joints. 2. (nonstandard) Spondylosis deformans, for which spondylosis is a shortened form.
Spondylosis deformans:�degenerative process of the spine involving the annulus fibrosus and vertebral body apophysis, characterized by anterior and lateral marginal osteophytes arising from the vertebral body apophyses, while the intervertebral disc height is normal or only slightly decreased. See degeneration, spondylosis.
Subarticular zone:�the zone, within the vertebral canal, sagittally between the plane of the medial edges of the pedicles and the plane of the medial edges of the facets and coronally between the planes of the posterior surfaces of the vertebral bodies and the anterior surfaces of the superior facets. Note: the subarticular zone cannot be precisely delineated in two-dimensional depictions because the structures that define the planes of the zone are irregular. The lateral recess is that portion of the subarticular zone defined by the medial wall of the pedicle, where the same numbered nerve root traverses before turning under the inferior wall of the pedicle into the foramen.
Subligamentous:�beneath the posterior longitudinal ligament. Note: although the distinction between outer annulus and posterior longitudinal ligament may not always be identifiable, subligamentous has meaning distinct from subannular when the distinction can be made. When the distinction cannot be made, subligamentous is appropriate. Subligamentous contrasts to extraligamentous, transligamentous, or perforated. See extraligamentous, transligamentous.
Submembranous:�enclosed within the peridural membrane. Note: with reference to the displaced disc material, characterization of a herniation as submembranous usually infers that the displaced portion is extruded beyond annulus and posterior longitudinal ligament so that only the peridural membrane invests it.
Suprapedicular level:�the level within the vertebral canal between the axial planes of the superior end plate of the vertebra caudad to the disc space in question and the superior margin of the pedicle of that vertebra. Synonym: inferior vertebral notch.
Syndesmophytes:�thin and vertically oriented bony outgrowths extending from one vertebral body to the next and representing ossification within the outer portion of the annulus fibrosus.
Tear of annulus, torn annulus�(nonstandard): see annular tear.
Thompson classification:�a five-point grading scale of degenerative changes in the human intervertebral disc, from 0 (normal) to 5 (severe degeneration), based on gross pathologic morphology of midsagittal sections of the lumbar spine.
Traction osteophytes:�bony outgrowth arising from the vertebral body apophysis, 2 to 3 mm above or below the edge of the intervertebral disc, projecting in a horizontal direction.
Transligamentous:�displacement, usually extrusion, of disc material through the posterior longitudinal ligament. Synonym: (nonstandard) (perforated). See also extraligamentous, transmembranous.
Transmembranous:�displacement of extruded disc material through the peridural membrane.
Transverse fissure:�fissure of the annulus in the axial (horizontal) plane. When referring to a large fissure in the axial plane, the term is synonymous with a horizontally oriented radial fissure. Often ��transverse fissure�� refers to a more limited, peripheral separation of annular fibers including attachments to the apophysis. These more narrowly defined peripheral fissures may contain gas visible on radiographs or CT images and may represent early manifestations of spondylosis deformans. See annular fissure, concentric fissure, radial fissure.
Uncontained disc:�displaced disc material that is not contained by the outer annulus and/or posterior longitudinal ligament. See discussion under contained disc.
Vacuum disc:�a disc with imaging findings characteristic of gas (predominantly nitrogen) in the disc space, usually a manifestation of disc degeneration.
Vertebral body marrow changes:�reactive vertebral body signal changes associated with disc inflammation and disc degeneration, as seen on MRIs. See Modic classification.
Vertebral notch (inferior):�incisura of the upper surface of the pedicle corresponding to the lower part of the foramen (suprapedicular level).
Vertebral notch (superior):�incisura of the under surface of the pedicle corresponding to the upper part of the foramen (infrapedicular level).
A herniated disc most commonly develops as a result of age-related wear and tear or degeneration on the spine. In children and young adults, the intervertebral discs have a much higher water content. As we age, however, the water content of the intervertebral discs decreases and these begin to shrink while the spaces between the vertebra gets narrower, ultimately turning less flexible and becoming more prone to disc herniation. Proper diagnosis and treatment are essential to avoid further symptoms of low back pain. The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
References
Fardon, D.F. and Milette, P.C.�Nomenclature and classification of lumbar disc pathology: recommendations of the combined task forces of the North American Spine Society, the American Society of Spine Radiology and the American Society of Neuroradiology.�Spine.�2001;�26:�E93�E113
Stadnik, T.W., Lee, R.R., Coen, H.L. et al.�Annular tear and disk herniation: prevalence and contrast enhancement on MR images in the absence of low back pain or sciatica.�Radiology.�1998;�206:�49�55
Mink, J.H.�Terminology of lumbar spine disorders, the problem… and a solution.�California Managed Imaging Medical Group Publication,�Burlingame, CA;�1993
Brant-Zawadzki, M.N. and Jensen, M.C.�Imaging corner: spinal nomenclature. Inter- and intra-observer variability in interpretation of lumbar disc abnormalities: a comparison of two nomenclatures.�Spine.�1995;�20:�388�390
Fardon DF, White AH, Wiesel S. Diagnostic terms and conservative treatments favored for lumbar disorders by spine surgeons in North America. Presented at the first annual meeting, North American Spine Society, Lake George, New York,�1986.
Arana, E., Royuela, A., Kovacs, F.M. et al.�Lumbar spine: agreement in�the interpretation of 1.5T MR images by using the Nordic Modic�consensus group classification form.�Radiology.�2010;�254:�809�817
Farfan, H.F., Huberdeau, R.M., and Dubow, H.I.�Lumbar intervertebral disc degeneration: the influence of geometrical features on the pattern of disc degeneration: a post-mortem study.�J Bone Joint Surg [Am].�1972;�54:�492�510
Milette, P.C., Fontaine, S., Lepanto, L. et al.�Differentiating lumbar disc protrusions, disc bulges, and discs with normal contour but abnormal signal intensity.�Spine.�1999;�24:�44�53
Thompson, J.P., Pearce, R.H., Schechter, M.T. et al.�Preliminary evaluation of a scheme for grading the gross morphology of the human intervertebral disc.�Spine.�1990;�15:�411�415
Fardon, D.F., Balderston, R.A., Garfin, S.R. et al.�Disorders of the spine, a coding system for diagnoses.�Hanley and Belfus,�Philadelphia;�1991:�20�22
International anatomical nomenclature committee approved by Eleventh International Congress of anatomists. Nomina anatomica.�5th ed.�Waverly Press,�Baltimore, MD;�1983:�A23
Jarvik, J.G., Haynor, D.R., Koepsell, T.D. et al.�Interreader reliability for a new classification of lumbar disc abnormalities.�Acad Radiol.�1996;�3:�537�544
Ketler, A. and Wilke, H.J.�Review of existing grading systems for cervical or lumbar disc and facet joint degeneration.�(with Erratum note in Eur Spine J 15(6); 729)Eur Spine J.�2006;�15:�705�718
Kieffer, S.A., Stadlan, E.M., Mohandas, A., and Peterson, H.O.�Discographic-anatomical correlation of developmental changes with age in the intervertebral disc.�Acta Radiol [Diagn] (Stockholm).�1969;�9:�733�739
Bartynski, W.S., Rothfus, W.E., and Kurs-Lasky, M.�Post-diskogram CT features of lidocaine-sensitive and lidocaine-insensitive severely painful disks at provocation lumbar diskography.�AJNR.�2008;�29:�1455�1460
Resnick, D. and Niwayama, G.�Degenerative disease of the spine.�in:�D. Resnick (Ed.)�Diagnosis of bone and joint disorders.�3rd ed.�WB Saunders,�Philadelphia;�1995:�1372�1462
Marinelli, N.L., Haughton, V.M., and Anderson, P.A.�T2 relaxation times correlated with stage of lumbar disc degeneration and patient age.�AJNR.�2010;�31:�1278�1282
Oh, K.-J., Lee, J.W., Kwon, E.T. et al.�Comparison of MR imaging findings between extraligamentous and subligamentous disk herniations in the lumbar spine.�AJNR.�2013;�34:�683�687
United States Department of Health and Human Services. Publication no (PHS) 91-1260, International Classification of Diseases Ninth Revision, clinical modification fifth edition, Washington, DC, 1998; Adapted and published by Practice Management Information Corporation, Los Angeles, and by St. Anthony�s Publishing Company, Alexandria, Virginia,�1999.
Williams, A.L., Haughton, V.M., Daniels, D.L., and Grogan, J.P.�Differential CT diagnosis of extruded nucleus pulposus.�Radiology.�1983;�148:�141�148
Boden, S.D., Davis, D.O., Dina, T.S. et al.�Abnormal magnetic-resonance scans of the lumbar spine in asymptomatic subjects. A prospective investigation.�J Bone Joint Surg.�1990;�72:�403�408
Sachs, B.L., Vanharanta, H., Spivey, M.A. et al.�Dallas discogram description. A new classification of CT/discography in low-back disorders.�Spine.�1987;�12:�287�294
Carragee, E.J., Paragioudakis, S.J., and Khurana, S.�Lumbar high-intensity zone and discography in subject without low back problems.�Spine.�2000;�25:�2987�2992
Schellhas, K.P., Pollei, S.R., Gundry, C.R. et al.�Lumbar disc high intensity zone. Correlation of magnetic resonance imaging and discography.�Spine.�1996;�21:�79�86
Rothman, S.L.G. and Chafetz, N.I.�An anatomic explanation for overreading disc herniations on MRI imaging studies of the lumbar spine: poster presentation.�American Society of Neuroradiology,Chicago, Illinois;�1995
Coventry, M.B., Ghormley, R.K., and Kernohan, J.W.�The intervertebral disc: its microscopic anatomy and pathology.�(233�7)J Bone Joint Surg.�1945;�27:�105�112
Nathan, H.�Osteophytes of the vertebral column. An anatomical study of their development according to age, race, and sex, with consideration as to their etiology and significance.�J Bone Joint Surg Am.�1962;�44:�243�268
Sether, L.A., Yu, S., Haughton, V.M., and Fischer, M.E.�Intervertebral disk: normal age-related changes in MR signal intensity.�Radiology.�1990;�177:�385�388
Schmorl, G. and Junghanns, H.�(American Ed, 1971. Transl. by EF Besemann) (186�98)in:�The human spine in health and disease.�2nd.�Grune and Stratton,�New York;�1971:�141�148
Pfirrmann, C.W., Metzdorf, A., Zanetti, M. et al.�Magnetic resonance classification of lumbar intervertebral disc degeneration.�Spine.�2001;�26:�1873�1878
Griffith, J.F., Wang, W.X., and Antonio, G.E.�Modified Pfirrmann grading system for lumbar intervertebral disc degeneration.�Spine.�2007;�32:�E708�E712
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
Herniated discs are a debilitating condition characterized by pain, numbness and weakness in one or more limbs. While some people may experience no pain at all, those that do may often wish for fast pain relief to avoid long periods of sick leave from their jobs. Many healthcare professionals recommend surgery for patients with persistent and/or worsening herniated disc symptoms but other non-operative treatment options can help treat disc herniations. The purpose of the following article is to demonstrate how a�structured physiotherapy treatment model can provide rapid relief to patients who qualify for lumbar disc surgery.
A Structured Physiotherapy Treatment Model Can Provide Rapid Relief to Patients Who Qualify for Lumbar Disc Surgery: A Prospective Cohort Study
Abstract
Objective: To evaluate a structured physiotherapy treatment model in patients who qualify for lumbar disc surgery.
Design: A prospective cohort study.
Patients: Forty-one patients with lumbar disc herniation, diagnosed by clinical assessments and magnetic resonance imaging.
Methods: Patients followed a structured physiotherapy treatment model, including Mechanical Diagnosis and Therapy (MDT), together with graded trunk stabilization training. Study outcome measures were the Oswestry Disability Index, a visual analogue scale for leg and back pain, the Tampa Scale for Kinesiophobia, the European Quality of Life in 5 Dimensions Questionnaires, the Zung Self-Rating Depression Scale, the Self-Efficacy Scale, work status, and patient satisfaction with treatment. Questionnaires were distributed before treatment and at 3-, 12- and 24-month follow-ups.
Results: The patients had already improved significantly (p<0.001) 3 months after the structured physiotherapy treatment model in all assessments: disability, leg and back pain, kinesiophobia, health-related quality of life, depression and self-efficacy. The improvement could still be seen at the 2-year follow-up.
Conclusion: This study recommends adopting the structured physiotherapy treatment model before considering surgery for patients with symptoms such as pain and disability due to lumbar disc herniation.
Symptoms of lumbar disc herniation are relatively common in the general population, although the prevalence rates vary widely between different studies (1). Symptom severity also varies and, in many patients, pain and loss of function may lead to disability and long periods of sick leave (2). Spontaneous resolution of symptoms after a lumbar disc herniation is regarded as common, which makes it difficult to evaluate the effects of treatment. Furthermore, in studies evaluating spontaneous healing, different physiotherapy treatments are often included, together with pain medication (3�5), which makes it difficult to determine the extent of natural healing. On the other hand, in patients with sciatica, but without confirmed disc herniation on magnetic resonance imaging (MRI), approximately one-third of subjects recover 2 weeks after the onset of sciatica and approximately three-quarters recover after 3 months (6).
In contrast to evaluating spontaneous healing, surgery for lumbar disc herniation has been investigated in numerous studies. Surgery has been compared with a variety of treatments, such as education, chiropractic, unspecified physiotherapy, acupuncture, injections and medication (7�10). The non-surgical treatments have, however, been described only in vague terms, and variations in treatments have been used. Previous studies have reported favourable short-term (after 1 year) outcomes for surgery, but no major differences between surgical and other treatments have been demonstrated in the long term (over 2 years) (7, 10, 11). The conclusions that are drawn from the comparison between surgery and non-systematic non-surgical treatments may thus be misleading. This has been confirmed in a systematic review, which concluded that there is conflicting evidence as to whether surgery is more beneficial than nonsurgical care for both short- and long-term follow-up (12).
Kinesiophobia has been evaluated in patients after lumbar disc surgery, and almost 50% of patients were classified as having kinesiophobia (13). To our knowledge kinesiophobia has not been evaluated in patients with lumbar disc herniation treated with a structured physiotherapy treatment.
There are many different non-surgical treatment methods for patients with low-back pain and sciatica. One common management method is Mechanical Diagnosis and Therapy (MDT), also known as the McKenzie method, which aims to eliminate or minimize pain (14). A systematic review from 2004 of the efficacy of MDT showed that patients with low-back pain treated�with MDT reported a greater, more rapid reduction in pain and disability compared with non-steroidal anti-inflammatory drugs (NSAIDs), educational booklets, back massage and back care advice, strength training, spinal mobilization and general exercises (15). In a randomized controlled trial with a 1-year follow-up from 2008, Paatelma and co-workers (16) found that the McKenzie method was only marginally more effective compared with only giving advice to patients with low-back pain. For patients with low-back pain, sciatica and a verified lumbar disc herniation, it has, however, been shown that a selected group of patients who responded to MDT after 5 days of treatment also reported that they were satisfied after 55 weeks (17). The patients started treatment just 12 days after the onset of symptoms and the effects of spontaneous healing cannot therefore be excluded. Taken together, the treatment effects of MDT for patients with a verified lumbar disc herniation appear to require further evaluation.
Trunk stabilization exercises, which aim to restore deep trunk muscle control, have been used for the prevention and rehabilitation of low-back pain (18). A randomized controlled trial revealed a reduction in the recurrence of low-back pain episodes after specific trunk stabilization exercises compared with a control group receiving advice and the use of medication (19). Dynamic lumbar stabilization exercises have been found to relieve pain and improve function in patients who have undergone microdiscectomy (20). The effects of trunk stabilization exercises combined with MDT have, however, not been studied in patients with non-operated lumbar disc herniation. MDT is seldom recommended for patients with MRI verified lumbar disc herniation with a broken outer annulus. At our hospital, however, we have several years of good clinical experience of a combination of MDT and trunk stabilization exercises for this category of patients. To our knowledge, no previous study has investigated whether patients with a lumbar disc herniation verified by MRI, symptoms for at least 6 weeks (minimizing effects of spontaneous healing) and who qualified for disc surgery could improve with a structured physiotherapy treatment model including MDT and gradually progressive trunk stabilization exercises. The aim of this study was therefore to�evaluate a structured physiotherapy treatment model in patients who qualified for lumbar disc surgery.
Material and Methods
During the study inclusion period, 150 patients, who were referred to the orthopaedic clinic at Sahlgrenska University Hospital, Gothenburg, from November 2003 to January 2008, were identified as potential participants since disc herniation was confirmed with MRI. Inclusion criteria were: 18�65 years of age; MRI confirming disc herniation explaining the clinical findings; symptoms for at least 6 weeks (minimizing the effects of spontaneous healing) and pain distribution with concomitant neurological disturbances correlated to the affected nerve root. Exclusion criteria were: cauda equina syndrome, previous spinal surgery, other spinal diseases, such as spinal stenosis and spondylolisthesis, and inadequate command of Swedish. However, 70 patients were excluded because of spontaneous resolution of pain and symptoms. The remaining 80 patients met the inclusion criteria and qualified for surgery. Orthopaedic surgeons determined whether the patients qualified for lumbar disc surgery after MRI and physical examination according to the recommendations of the American Academy of Orthopaedic Surgeons for patients with lumbar disc herniation (21).
Initially, the study was planned as a randomized controlled trial (RCT) between a structured physiotherapy treatment model and surgery, but the number of patients was not sufficient to obtain acceptable power. Eighteen of the 80 patients were initially randomized to physiotherapy, 17 patients were randomized to surgery and 45 patients did not agree to undergo randomization. Twenty-seven of the 45 patients who did not agree to randomization agreed to take part in the structured physiotherapy treatment and 18 patients agreed to undergo surgery. A decision was therefore made solely to present a cohort of 45 patients treated according to the structured physiotherapytreatment protocol (Fig. 1). Patients were given verbal and written information and informed consent was obtained. The study was approved by the Regional Ethical Review Board.
Before structured physiotherapy treatment began, 4 patients recovered to the extent that they could no longer be accepted as surgical candidates and they were therefore excluded from the study. The remaining 41 patients treated according to the structured physiotherapy model are presented in this paper.
A Structured Physiotherapy Treatment Model
Six physiotherapists with credentialed examinations in MDT, which is an examination within the MDT concept after completing 4 courses of 4 days each for evaluating and treating patients with spinal problems. Following completion of these courses, an extensive literature study and practice in evaluating and treating patients is required before the examination can be completed. The physiotherapists involved in the study had 5�20 years of clinical experience of treating patients with back problems and herniated lumbar disc. The inter-examiner reliability of the MDT assessment has been shown to be good if the examiner is trained in the MDT method (22). The physiotherapists examined and treated the patients during a 9-week period (Table I). For the first 2 weeks of treatment, an MDT protocol was followed, based on clinical examinations of individual mechanical and symptomatic responses to positions and movements, with the aim of minimizing pain and with the emphasis on self-management (14). During the third week of treatment, graded trunk stabilization exercises were added to the MDT protocol. The purpose of graded trunk stabilization exercises was to improve muscle control (23). The low-load muscular endurance exercises were gradually increased in intensity on an individual�basis with respect to the patients� reported leg pain and the observed movement control and quality. During treatment, the patients were encouraged to continue exercising on their own at a gym, or to perform some other type of physical training of their own choice after the structured physiotherapy treatment was concluded. Four weeks after the completion of the 9-week physiotherapy treatment period, the patients attended a follow-up visit with the physiotherapist who had treated them. The aim of this visit was to encourage a high level of compliance with respect to continued trunk stabilization exercises and MDT practice (Table I).
Study Outcome Measures
The patients were given a battery of questionnaires to complete. Independent examiners, who were not involved in the treatment, distributed the questionnaires before treatment (baseline) and at the 3-, 12- and 24-month follow-ups.
The primary outcome measures were pain intensity in the leg, rated using a visual analogue scale (VAS) 0�100 mm (24) and the Oswestry Disability Index (ODI) 0�100 % (25). A score of 0�10 mm on the VAS was defined as no pain according to �berg et al. (26). An ODI score of 0�20% was defined as minimal or no disability, and a score of over 40% was defined as severe disability (25). These primary outcome measures are commonly used in evaluations after surgery for lowback pain and for assessing patients with lumbar disc herniation (27).
Secondary outcome measures included pain intensity in the back rated using a VAS and the degree of kinesiophobia using the Tampa Scale for Kinesiophobia (TSK). The TSK score varies between 17 and 68 and a cut-off more than 37 was defined as a high degree of kinesiophobia (28). Health-Related Quality of Life (HRQoL) in the European Quality of Life in 5 Dimensions Questionnaires (EQ-5D) was used. The EQ-5D includes 2 parts, EQ-5Dindex ranges from 0 to 1.0, where 1.0 is optimal health and EQ-5DVAS is a vertical visual analogue scale ranging from 0 (worst possible health state) to 100 (best possible health state) (29). The Zung Self-Rating Depression Scale (ZDS) ranges from 20�80 and the more depressed the patient is, the higher score (30). The Self-Efficacy Scale (SES) ranges from 8 to 64, with higher scores indicating more positive beliefs (31) was also used. Work status was measured using a 3-grade Likert scale: working full time, full-time sick leave and part-time sick leave. Likewise, patient�satisfaction with treatment was measured on a 3-grade Likert scale; satisfied, less satisfied and dissatisfied (32). These secondary outcome measures evaluate bio-psychosocial factors described as important in connection with lumbar disc surgery (33).
Statistical Analyses
The results are presented as median values and interquartile range (IQR), except for age, which is presented as the mean and standard deviation (SD). Changes over time within the group were analysed with the Wilcoxon signed-rank test. Statistical significance was set at an alpha level of 0.05.
Results
The baseline characteristics are shown in Table II. No patient had undergone surgery at the 3-month follow-up. At the 12-month follow-up, 3 patients had undergone surgery and, at the 24-month follow-up, 1 additional patient had been operated on. After surgery, these 4 patients were excluded from further follow-ups (Fig. 1).
Change Over Time in Primary Outcome Measures
Disability. The patients showed significant improvements (p < 0.001) in ODI at the 3-month follow-up compared with baseline. The median (IQR) score decreased from 42 (27�53) to 14 (8�33). This improvement could still be seen at 12 and 24 months (Table III and Fig. 2). At baseline, 22 patients reported�severe disability (54%) and 3 patients reported no disability. The degree of disability decreased at the 3-month follow-up, as only 9 patients (22%) reported severe disability and 26 (64%) reported no disability. At 12- and 24-month follow-ups only 2 patients (5%) reported severe disability. At 12-month followup 26 patients still reported no disability, and at 24-month follow-up 27 patients reported no disability.
Leg pain. A significant reduction in patients� leg pain was found at the 3-month follow-up (p < 0.001) on the VAS compared with baseline. The median (IQR) on the VAS decreased from 60 (40�75) to 9 (2�27). This improvement could still be seen at the 12- and 24-month follow-ups (Table III and Fig. 2). Before treatment, all patients reported leg pain. Three months after treatment, the median on the VAS was 9 mm, i.e. classified as no leg pain (26). Twenty-three patients (56%) reported no leg pain at the 3-month follow-up. At the 12-month follow-up 22 patients reported no leg pain, and after 24 months 24 patients reported no leg pain.
Change in Secondary Outcome Measures Over Time
Back pain. A significant improvement in back pain was found at the 3-month follow-up (p < 0.001) on the VAS compared with baseline. This improvement could still be seen at 12 and 24 months (Table III). At baseline, 6 patients (15%) reported no back pain. Three months after treatment began, 20 patients (49%) reported no back pain.
Kinesiophobia. The degree of kinesiophobia showed a significant improvement at the 3-month follow-up (p < 0.001) and the improvement could be seen throughout the follow-up period (Table III). Before treatment, 25 patients (61%) were classified as having kinesiophobia and 15 patients (37%) had no kinesiophobia, while data for 1 patient was missing. After 3 months, 15 patients (37%) had kinesiophobia and 26 (63%) had no kinesiophobia. At the 12-month follow-up, the number of patients with kinesiophobia had reduced to 4 (11%) (Fig. 3).
Health-related quality of life, depression and self-efficacy. All 4 assessments (EQ-5Dindex, EQ-5DVAS, ZDS and SES) showed significant improvements at the 3-month follow-up (p < 0.001). This improvement could still be seen at 12 and 24 months (Table III).
Sick leave. At baseline, 22 patients (54%) were on full-time sick leave (Table IV), compared with 9 (22%) patients at�the 3-month follow-up. At baseline, 14 patients (34%) were working full time, compared with 22 (54%) at the 3-month follow-up.
Satisfaction with Treatment
At the 3-month follow-up, 32 (78%) of 41 patients were satisfied with the structured physiotherapy treatment. Seven patients were less satisfied and 2 patients were dissatisfied. Both of the dissatisfied patients were later operated. At the 2-year follow-up, the number of satisfied patients was 29 (80%) of 36. Seven patients were less satisfied, but none dissatisfied after structured physiotherapy treatment.
Dr. Alex Jimenez’s Insight
A disc herniation in the lumbar spine can cause pain, numbness and weakness in the lower back. Because of the severity of the symptoms, many patients seeking fast pain relief consider surgery. However, many non-operative treatment options can help improve as well as manage lumbar herniated disc symptoms.�A structured physiotherapy treatment model can provide rapid pain relief to patients who would otherwise qualify for lumbar disc surgery, according to the following article. Patients looking to avoid taking long periods of sick leave from work due to their symptoms may benefit from a structured physiotherapy treatment model. As with any type of injury and/or condition, the use of other treatment options should be properly considered before turning to surgical interventions for fast pain relief.
Discussion
The principal finding of this study was that patients who qualified for lumbar disc surgery improved to a statistically significant and clinically substantial degree just 3 months after the start of the structured physiotherapy treatment in all assessments: disability, leg and back pain, kinesiophobia, health-related quality of life, depression and self-efficacy. The improvements could still be seen at the 2-year follow-up.
The natural course of healing must be considered carefully, especially when evaluating treatment effects in patients with disc herniation. The symptoms often vary over time and many discs heal spontaneously and the symptoms cease. Approximately 75% of patients with sciatica, without an MRI-verified disc herniation, recover within 3 months, and approximately one-third of patients recover within 2 weeks after the onset of sciatica (6). The natural course of sciatica was evaluated in a randomized controlled trial (34), which compared NSAIDs with placebo. The patients were, however, examined within 14 days after the onset of radiating leg pain. After 3 months, 60% of the patients had recovered and, after 12 months, 70% had recovered. In order to minimize the influence of spontaneous healing in the present study, the patients were therefore included only if they had had persistent pain and disability for more than 6 weeks. In fact, the majority of the patients had had pain and disability for more than 3 months. It is therefore most likely that the effects of treatment seen in the present study are, in the majority of patients, an effect of the structured physiotherapy treatment model and not a result of spontaneous healing.
In the study by Weber et al. (34), the VAS leg pain mean score was reduced from 54 mm at baseline to 19 mm within 4 weeks for all 183 patients, regardless of treatment. After 1 year, the VAS leg pain mean score was 17 mm. The patients in the present study who were a little worse at baseline (60 mm) reported 9 mm on the VAS leg pain just 3 months after treatment. Consequently, in the present study, the median VAS level had already been reduced to under the no-pain score, defined as 0�10 on the VAS (26), at the 3-month follow-up and this was maintained to the 12- and 24-month follow-ups.
Physiotherapy treatment for patients with lumbar disc herniation can lead to improvements. Br�tz et al. (17) included a selected group of patients who responded with the centralization of pain after the first 5 daily sessions of treatment according to the MDT method. Centralization of pain is defined as a clinically induced change in the location of pain referred from the spine, that moves from the most distal position toward the lumbar midline (35). However, the patients� medium duration of symptoms before treatment was only 12 days and the possibility that patients recovered naturally cannot therefore be excluded (17).
In a retrospective study, 95 patients were treated with a functional restoration programme (36). The patients achieved significant improvements after a mean treatment period of 8.7 months. The evaluation was performed at discharge only. With a treatment period of this length, it is, however, difficult to differentiate between the effects of treatment and the natural healing process. In the present study, a shorter treatment period was adopted, and large and significant improvements were found after just 3 months and were still present at the 24-month follow-up. It is therefore not likely that the natural healing process was responsible for the positive results in the present study.
In a prospective study of 82 consecutive patients with acute severe sciatica, included for conservative management, only a minority of the patients had made a full recovery after 12 months (37). Twenty-five percent of the patients underwent surgery within 4 months and one-third had surgery within 1 year. In spite of the fact that the inclusion criteria in the present study followed the recommendations for surgery (21, 38), no patient required surgery at the 3-month follow-up and, after 12 months, only 3 patients (7%) had undergone surgery. The interpretation of the divergence could be that the structured physiotherapy treatment model used in the present study appeared to influence patients with lumbar disc herniation in a very positive direction. One recommendation is therefore to follow the structured physiotherapy treatment model before considering surgery.
In this study, MRI verification of disc herniation was an inclusion criterion. In clinical practice, MRI verification is not mandatory, as it is in surgical treatment, before introducing structured physiotherapy treatment to patients with symptoms from a disc herniation. Consequently, treatment according to the structured physiotherapy treatment model can start early after the commencement of symptoms, as it is not necessary to wait for an MRI. It is possible to speculate that, if treatment with a structured physiotherapy model starts earlier than in the present study, the improvements would be even better, further reducing the risk of persistent pain and accompanying problems. Moreover, the need for MRI is likely to diminish; this, however, should be further evaluated in future studies.
One explanation for the good results of this study could be that the patients followed a structured physiotherapy treatment model, comprising MDT and trunk stabilization exercises, allowing for an individual design and progression of the treatment. Similar results were described in a retrospective cohort study (39) using several treatment methods for pain control as well as for exercise training for patients with lumbar disc herniation. The evaluation was not carried out until approximately 31 months after treatment. The results of Saal et al. (39) and of the present study are in agreement, in that structured physiotherapy treatment can reduce symptoms, but symptoms were relieved much more rapidly in the present study.
In a multicentre study comprising 501 patients, randomized to surgery or non-operative care, 18% of the patients assigned to non-operative treatment underwent surgery within 6 weeks and 30% had surgery at approximately 3 months (7). The nonoperative treatment group received non-specified �usual care�, which could include a variety of different treatment methods. In contrast, the patients in the present study were offered a structured physiotherapy treatment model that included both bio-psychological and social components, as described in the International Classification of Functioning, Disability and Health (40).
There are many possible explanations for the positive effects seen in this present study, and 5 of these will now be discussed. Firstly, the patients were well informed about the design of the structured physiotherapy treatment model, including the timetable for different phases of the treatment and when the treatment was planned to end. This information enhanced the patients� opportunity for self-management and gave them an active role in treatment decision-making.
Secondly, the patients acquired strategies to deal with their pain by using the different activities and movements in order to reduce pain according to the MDT method (14). The MDT method aims to enhance the patients� ability to cope with the symptoms, motivate the patient to comply with the treatment and empower them to achieve independence. Leijon et al. (41) have shown that low levels of motivation plus pain are important factors that enhance non-adherence to physical activity. It therefore appears important to reduce pain and increase motivation as early as possible. It is reasonable to believe that, when the patients participated in the evaluation of different activities and exercises, this augmented their opportunity to discover the connection between activities and the following reduction or increase in symptoms. This could have led to the increased self-efficacy and empowerment of the patients. The use of empowerment in physiotherapy has been recommended in a review by Perrault (42), who argues that empowerment improves the intervention.
Thirdly, the intensity of exercises was gradually increased on an individual basis with respect to the patients� reported pain. The objective was to strengthen the patients� self-efficacy, which also improved significantly in the present study. Fourthly, the trunk stabilization exercises were conducted with the aim of increasing deep trunk muscle control (23). It can be speculated that the physiological effects of training may also have led to reduced pain through increased blood circulation, muscle relaxation and the release of pain-reducing substances, such as endorphins.
Finally, one reason for the improvements could be that the physiotherapists were experienced and well educated in the MDT method. Subsequently, the physiotherapists were able to guide the patients during the rehabilitation process. It is, however, not possible to determine whether and how much each of the reasons discussed above contributed to the improvements. It seems reasonable to assume that all 5 factors were operating.
In this study, the majority of patients experienced kinesiophobia before treatment started. As early as 3 months after the structured physiotherapy treatment started, the number of patients with kinesiophobia fell dramatically and the majority of patients no longer experienced kinesiophobia. These results are in agreement with those of a study of patients with chronic pain and high kinesiophobia who increased their physical activity level after a pain management programme designed to enable the patients to regain overall function (43).
There are some limitations to this study. It is not possible to exclude the possibility that some patients may have improved spontaneously without treatment. Measures were taken to limit this risk by using symptoms for at least 6 weeks as an inclusion criterion. Again, the majority of patients had symptoms for more than 3 months. Another limitation might relate to whether the patients were selected accurately for the study. Clinically experienced orthopaedic surgeons evaluated the clinical findings and the MRI scans and classified the patients as surgical candidates based on recommendations from the American Academy of Orthopaedic Surgeons for intervention for disc herniation published in 1993 (21). The patients included in the present study also fulfilled the recommendations as presented by Bono and co-workers in 2006 (38). The patients can therefore be regarded as serving as their own controls, and comparisons can be made with baseline symptoms and with patients from other studies. An RCT would have been the best way to explore different treatment options; however, we did not reach the number of patients required for an RCT. As the treatment model used in the present study has not been evaluated previously in a group of patients with long-standing pain, with the majority of the patients having pain for more than 3 months due to disc herniation, and, as the results are clinically interesting, it was decided to present the results as a cohort study.
In conclusion, this study shows that patients eligible for lumbar disc surgery improved significantly after treatment with the structured physiotherapy model, as early as 3 months after treatment, and the results could still be seen at the 24-month follow-up. Consequently, these patients did not qualify for lumbar disc surgery 3 months after the physiotherapy treatment started. Moreover, the majority of patients had symptoms for more than 3 months at the start of treatment and, for this reason, most of the spontaneous healing ought to have occurred before this study started. This study therefore recommends adoption of the structured physiotherapy treatment model before considering surgery when patients report symptoms such as pain and disability due to lumbar disc herniation.
Acknowledgements
The authors would like to thank physiotherapists Patrik Drevander, Christina Grund�n, Sofia Frid�n and Eva Fahlgren for treating the patients and Valter Sundh for statistical support. This study was supported by grants from the Health & Medical Care Committee of the V�stra G�taland Region, Ren�e Eander�s Foundation and Wilhelm & Martina Lundgren�s Foundation of Science.
Herniated discs can cause pain, numbness and weakness, a variety of symptoms which may often become so severe, that surgery might seem like the only option for fast relief. However, a�structured physiotherapy treatment model can provide rapid relief to patients who qualify for lumbar disc surgery, according to the results of the research study. Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Neck Pain
Neck pain is a common complaint which can result due to a variety of injuries and/or conditions. According to statistics, automobile accident injuries and whiplash injuries are some of the most prevalent causes for neck pain among the general population. During an auto accident, the sudden impact from the incident can cause the head and neck to jolt abruptly back-and-forth in any direction, damaging the complex structures surrounding the cervical spine. Trauma to the tendons and ligaments, as well as that of other tissues in the neck, can cause neck pain and radiating symptoms throughout the human body.
1. Konstantinou K, Dunn KM. Sciatica: review of epidemiological
studies and prevalence estimates. Spine (Phila Pa 1976) 2008;
33: 2464�2472.
2. Nygaard OP, Kloster R, Solberg T. Duration of leg pain as a
predictor of outcome after surgery for lumbar disc herniation:
a prospective cohort study with 1-year follow up. J Neurosurg
2000; 92: 131�134.
3. Orief T, Orz Y, Attia W, Almusrea K. Spontaneous resorption
of sequestrated intervertebral disc herniation. World Neurosurg
2012; 77: 146�152.
4. Maigne JY, Rime B, Deligne B. Computed tomographic follow-up
study of forty-eight cases of nonoperatively treated lumbar intervertebral
disc herniation. Spine (Phila Pa 1976) 1992; 17: 1071�1074.
5. Takada E, Takahashi M, Shimada K. Natural history of lumbar disc
hernia with radicular leg pain: spontaneous MRI changes of the
herniated mass and correlation with clinical outcome. J Orthopaed
Surg (Hong Kong) 2001; 9: 1�7.
6. Vroomen PC, de Krom MC, Knottnerus JA. Predicting the outcome
of sciatica at short-term follow-up. Br J Gen Pract 2002;
52: 119�123.
7. Weinstein JN, Tosteson TD, Lurie JD, Tosteson AN, Hanscom
B, Skinner JS, et al. Surgical vs nonoperative treatment for lumbar
disk herniation: the Spine Patient Outcomes Research Trial
(SPORT): a randomized trial. JAMA 2006; 296: 2441�2450.
8. Peul WC, van den Hout WB, Brand R, Thomeer RT, Koes BW.
Prolonged conservative care versus early surgery in patients with
sciatica caused by lumbar disc herniation: two year results of a
randomised controlled trial. BMJ 2008; 336: 1355�1358.
9. Atlas SJ, Keller RB, Wu YA, Deyo RA, Singer DE. Long-term
outcomes of surgical and nonsurgical management of sciatica secondary
to a lumbar disc herniation: 10 year results from the maine
lumbar spine study. Spine (Phila Pa 1976) 2005; 30: 927�935.
10. Weber H. Lumbar disc herniation. A controlled, prospective
study with ten years of observation. Spine (Phila Pa 1976) 1983;
8: 131�140.
11. Osterman H, Seitsalo S, Karppinen J, Malmivaara A. Effectiveness of microdiscectomy for lumbar disc herniation: a randomized
controlled trial with 2 years of follow-up. Spine (Phila Pa 1976)
2006; 31: 2409�2414.
12. Jacobs WC , van Tulder M, Arts M, Rubinstein SM, van Middelkoop
M, Ostelo R, et al. Surgery versus conservative management of
sciatica due to a lumbar herniated disc: a systematic review. Eur
Spine J 2011; 20: 513�522.
13. Svensson GL, Lundberg M, �stgaard HC, Wendt GK. High degree
of kinesiophobia after lumbar disc herniation surgery: a crosssectional
study of 84 patients. Acta Orthop 2011; 82: 732�736.
14. McKenzie R, May S. The lumbar spine: mechanical diagnosis
& therapy. 2nd ed. Spinal Publications New Zealand Limited:
Wellington; 2003.
15. Clare HA, Adams R, Maher CG. A systematic review of efficacy
of McKenzie therapy for spinal pain. Aust J Physiother 2004;
50: 209�216.
16. Paatelma M, Kilpikoski S, Simonen R, Heinonen A, Alen M, Videman
T. Orthopaedic manual therapy, McKenzie method or advice
only for low back pain in working adults: a randomized controlled
trial with one year follow-up. J Rehabil Med 2008; 40: 858�863.
17. Br�tz D, Kuker W, Maschke E, Wick W, Dichgans J, Weller M.
A prospective trial of mechanical physiotherapy for lumbar disk
prolapse. J Neurol 2003; 250: 746�749.
18. Hodges PW, Moseley GL. Pain and motor control of the lumbopelvic
region: effect and possible mechanisms. J Electromyogr
Kinesiol 2003; 13: 361�370.
19. Hides JA, Jull GA, Richardson CA. Long-term effects of specific
stabilizing exercises for first-episode low back pain. Spine (Phila
Pa 1976) 2001; 26: E243�E248.
20. Yilmaz F, Yilmaz A, Merdol F, Parlar D, Sahin F, Kuran B. Efficacy
of dynamic lumbar stabilization exercise in lumbar microdiscectomy.
J Rehabil Med 2003; 35: 163�167.
21. Nachemson AL. Lumbar disc herniation � conclusions. Acta Orthop
Scand Suppl 1993; 251: 49�50.
22. Kilpikoski S, Airaksinen O, Kankaanpaa M, Leminen P, Videman
T, Alen M. Interexaminer reliability of low back pain assessment
using the McKenzie method. Spine (Phila Pa 1976) 2002; 27:
E207�E214.
23. Richardson CA, Jull GA. Muscle control-pain control. What exercises
would you prescribe? Man Ther 1995; 1: 2�10.
24. Scott J, Huskisson EC. Graphic representation of pain. Pain 1976;
2: 175�184.
25. Fairbank JC, Couper J, Davies JB, O�Brien JP. The Oswestry
low back pain disability questionnaire. Physiotherapy 1980; 66:
271�273.
26. �berg B, Enthoven P, Kjellman G, Skargren E. Back pain in
primary care: a prospective cohort study of clinical outcome and
healthcare consumption. Adv Physiother 2003; 5: 98.
27. Bombardier C. Outcome assessments in the evaluation of treatment
of spinal disorders: summary and general recommendations. Spine
2000; 25: 3100�3103.
28. Vlaeyen JW, Kole-Snijders AM, Boeren RG, van Eek H. Fear of
movement/(re)injury in chronic low back pain and its relation to
behavioral performance. Pain 1995; 62: 363�372.
29. EuroQol � a new facility for the measurement of health-related quality
of life. The EuroQol Group. Health Policy 1990; 16: 199�208.
30. Zung WW. A self-rating depression scale. Arch Gen Psychiatry
1965; 12: 63�70.
31. Estlander AM, Vanharanta H, Moneta GB, Kaivanto K. Anthropometric
variables, self-efficacy beliefs, and pain and disability
ratings on the isokinetic performance of low back pain patients.
Spine 1994; 19: 941�947.
32. Str�mqvist B, J�nsson B, Fritzell P, H�gg O, Larsson BE, Lind B.
The Swedish National Register for lumbar spine surgery: Swedish
Society for Spinal Surgery. Acta Orthop Scand 2001; 72: 99�106.
33. den Boer JJ, Oostendorp RA, Beems T, Munneke M, Oerlemans
M, Evers AW. A systematic review of bio-psychosocial risk factors
for an unfavourable outcome after lumbar disc surgery. Eur Spine
J 2006; 15: 527�536.
34. Weber H, Holme I, Amlie E. The natural course of acute sciatica
with nerve root symptoms in a double-blind placebo-controlled
trial evaluating the effect of piroxicam. Spine (Phila Pa 1976)
1993; 18: 1433�1438.
35. Werneke M, Hart DL, Cook D. A descriptive study of the centralization
phenomenon. A prospective analysis. Spine (Phila Pa
1976) 1999; 24: 676�683.
36. Hahne AJ, Ford JJ, Hinman RS, Taylor NF, Surkitt LD, Walters
AG, et al. Outcomes and adverse events from physiotherapy
functional restoration for lumbar disc herniation with associated
radiculopathy. Disabil Rehabil 2011; 33: 1537�1547.
37. Balague F, Nordin M, Sheikhzadeh A, Echegoyen AC, Brisby H,
Hoogewoud HM, et al. Recovery of severe sciatica. Spine (Phila
Pa 1976) 1999; 24: 2516�2524.
38. Bono CM, Wisneski R, Garfin SR. Lumbar disc herniations. In:
Herkowitz HN, Garfin SR, Eismont FJ, Bell GR, Balderston RA,
editors. Rothman-Simeone the spine. 5th ed. Saunders Elsevier:
Philadelphia; 2006: p. 979�980.
39. Saal JA, Saal JS. Nonoperative treatment of herniated lumbar
intervertebral disc with radiculopathy. An outcome study. Spine
(Phila Pa 1976) 1989; 14: 431�437.
40. World Health Organisation. International Classification of Functioning,
Disability and Health (ICF). 2001 [cited 2012 Oct 9].
Available from: www.who.int/classifications/icf/en/.
41. Leijon ME, Faskunger J, Bendtsen P, Festin K, Nilsen P. Who is
not adhering to physical activity referrals, and why? Scand J Prim
Health Care 2011; 29: 234�240.
42. Perreault K. Linking health promotion with physiotherapy for low
back pain: a review. J Rehabil Med 2008; 40: 401�409.
43. Koho P, Orenius T, Kautiainen H, Haanpaa M, Pohjolainen T, Hurri
H. Association of fear of movement and leisure-time physical
activity among patients with chronic pain. J Rehabil Med 2011;
43: 794�799.
A herniated disc is typically a very painful condition, especially if the inner gel-like substance of the intervertebral disc, known as the nucleus pulposus, pushes through the thick, outer ring of cartilage and puts pressure on the sensitive nerves of the spine. Discs are soft, rubbery pads found between each vertebrae of the spine that act as shock-absorbers, allowing the spine to bend and/or flex. An intervertebral disc may begin to rupture as a result of wear-and-tear or due to a sudden injury. Fortunately, most individuals who’ve suffered a herniated disc can find relief from a variety of non-operative treatments before considering surgery. The following article highlights the impact of early treatment for herniated discs in the lumbar spine, or low back.
The Impact of Early Recovery on Long-Term Outcomes in a Cohort of Patients Undergoing Prolonged Non-Operative Treatment for Lumbar Disc Herniation: Clinical Article
Abstract
Object
The authors comprehensively studied the recovery of individual patients undergoing treatment for lumbar disc herniation. The primary goal was to gain insight into the variability of individual patient utility scores within a treatment cohort. The secondary goal was to determine how the rates and variability of patient recovery over time, represented by improvement in utility scores, affected long-term patient outcomes.
Methods
EuroQol Group�5 Dimension (EQ-5D) scores were obtained at baseline and at 2, 4, 8, 12, 26, 38, and 52 weeks for 93 patients treated under a prolonged conservative care protocol for lumbar disc herniation. Gaussian kernel densities were used to estimate the distribution of utility scores at each time point. Logistic regression and multistate Markov models were used to characterize individual patient improvement over time. Fisher exact tests were used to compare the distribution of EQ-5D domain scores.
Results
The distribution of utility scores was bimodal at 1 year and effectively sorted patients into a �higher� utility group (EQ-5D = 1; 43% of cohort) and a �lower� utility group (EQ-5D ? 0.86; 57% of cohort). Fisher exact tests revealed that pain/discomfort, mobility, and usual activities significantly differed between the 2 utility groups (p ? 0.001). The utility groups emerged at 8 weeks and were stable for the remainder of the treatment period. Using utility scores from 8 weeks, regression models predicted 1-year outcomes with 62% accuracy.
Conclusions
This study is the first to comprehensively consider the utility recovery of individual patients within a treatment cohort for lumbar disc herniation. The results suggest that most utility is recovered during the early treatment period. Moreover, the findings suggest that initial improvement is critical to a patient’s long-term outcome: patients who do not experience significant initial recovery appear unlikely to do so at a later time under the same treatment protocol.
Abbreviations used in this paper: AUC = area under a receiver-operating curve; EQ-5D = EuroQol Group�5 Dimension. Address correspondence to: Matthew C. Cowperthwaite, Ph.D., The University of Texas at Austin, Texas Advanced Computing Center, J.J. Pickle Research Campus, ROC 1.101, 10100 Burnet Rd., Austin, TX 78758. email: mattccowp@mac.com.
Plublished online June 28, 2013; DOI: 10.3171/2013.5.SPINE12992.
Introduction
Lumbar disc herniation is one of the most common causes of low-back pain and radiculopathy.[4] Treatment for patients with a herniated lumbar disc usually begins with conservative care such as analgesics, epidural steroid injections, and physical therapy,[1,5] with surgery reserved for patients with severe nerve root or cauda equina dysfunction or if conservative therapy is unsuccessful in controlling the symptoms.
Several recent studies have compared the effectiveness of conservative care and surgical treatment protocols for treating herniated lumbar discs, and have arrived at varying conclusions.[2,3,9,10,15�18] However, these studies have generally considered outcomes over a period of years, which is a significant length of time for patients who are waiting for their quality of life to improve. In clinical practice, this often leads to the following dilemma: most patients, particularly those with moderate symptoms, would prefer to avoid surgery, but are unwilling to wait an indefinite period of time for their symptoms to resolve. Unsurprisingly, lumbar discectomy is the most frequently performed surgical procedure in the US.[17,18]
Moreover, the above-mentioned studies have typically compared the average difference between treatment groups, without regard for individual recovery within the cohort. Additionally, this approach assumes that recovery in the protocols being compared proceeded similarly between observation intervals. To better understand the treatment responses of individual patients and the time frames of their responses, we comprehensively analyzed a cohort of patients undergoing a prolonged conservative care treatment protocol to gain insight into the dynamics of individual patient recovery over time, and whether these recovery dynamics influence long-term outcomes.
Methods
Study Data Set
The data set contained 142 patients randomized to a protocol of prolonged conservative care as part of the Leiden�The Hague Spine Intervention Prognostic Study.[10,15] The Sciatica Trial was reviewed and approved by the Medical Ethics Committee of Leiden University Medical Center.[11] Patients were enrolled into the Sciatica Trial entirely in the Netherlands.
In the Sciatica Trial, all patients aged 18 to 65 years, with persistent radicular pain in the L-4, L-5, or S-1 dermatome (with or without mild neurological deficit), severe disabling leg pain (lumbosacral radicular syndrome) lasting 6�12 weeks, and radiologically (MRI) confirmed disc herniation were considered eligible to enroll in the trial. Cauda equina syndrome or severe paresis, prior complaints of lumbosacral radicular syndrome in the previous 12 months, history of same-level unilateral disc surgery, spinal canal stenosis, and degenerative or lytic spondylolisthesis were all exclusion criteria. Cohort demographics and baseline characteristics were previously described; all patients reported both back and leg pain, but leg pain was generally more severe (mean leg pain 67.2 � 27.7 vs back pain 33.8 � 29.6, measured on a 100-point, horizontal visual analog scale).[15]
The Sciatica Trial used a pragmatic study design: conservative-care management was influenced as little as possible and was supervised by each patient’s general practitioner. Use of analgesics and physical therapy was determined by the treating physician. In this cohort, 46 patients (32%) elected to have surgery before the end of the 1st year; the mean timing of surgery was 12.6 weeks after the start of treatment. The surgical patients and 3 additional subjects with more than 2 missing utility measures were removed from the sample, resulting in a cohort of 93 patients considered in the present study; the crossover patients will be discussed in a separate study (manuscript in preparation). Our results were qualitatively unchanged when the excluded patients were retained in the analyses (data not shown).
In the Leiden�The Hague Spine Intervention Prognostic Study the EQ-5D instrument was used to measure patient utility at baseline and at 2, 4, 8, 12, 26, 38, and 52 weeks after enrollment into the study. The average duration of sciatica prior to enrollment was 9.5 weeks.[10,15] Utility is a valuation of a patient’s quality of life on a scale between 0 (as bad as dead) and 1 (perfect health). To estimate utility, the EQ-5D assesses a patient’s functional impairment in 5 domains: mobility, self-care, usual activities, pain, and anxiety.[6] For each domain, patients self-report the scores of 1 (no problems), 2 (some problems), or 3 (extreme problems). Utility scores were computed using the US valuation model,[12] which clearly distinguishes patients reporting no health problems (EQ-5D = 1) from those reporting at least some health problems (EQ-5D ? 0.86). Our results are independent of the particular valuation model (not shown). Completeness of the EQ-5D measures during follow-up ranged from 98% at 2 weeks to 90% at 38 weeks.
Statistical Analysis
All statistical analyses were conducted using the R statistical environment (version 2.9.2; www.rproject.org/) with the additional �msm,�[8] �ROCR,�[14] and �rms�[7] packages (all freely available from cran.rproject.org). Continuous variables are presented as means (� SEM) and were compared using 2-tailed Student t-tests. Significance was assessed at an ? ? 0.05 significance level, unless otherwise indicated. Missing EQ-5D measures were imputed using the mean of the measures at adjacent time points; our results are qualitatively similar under forward or backward imputation schemes (not shown).
Gaussian kernel density estimates were computed to estimate the distribution of utility scores. The kernel density estimates were estimated using a Silverman’s �rule-of-thumb� bandwidth and a Gaussian smoothing kernel.[13] The left- and right-most points were set to the theoretical minimum and maximum EQ-5D values, respectively, so that the area under the density curve summed to 1.
To determine whether specific EQ-5D domains differed between utility groups, Fisher-exact tests were conducted on contingency tables of the number of patients in each utility group that reported scores of 1, 2, or 3. Significance was assessed using a Bonferroni-corrected p value of 0.01.
Two-state, continuous-time Markov models were used to study the patterns and probabilities of patients transitioning between a �lower� utility (EQ-5D ? 0.86) and a �higher� utility group (EQ-5D = 1). The threshold utility value defining the groups remained fixed over time and was used to assign each patient to a utility group at each observation time. The models were fitted using the �msm� package[14] with piecewise-constant transition intensity matrices (Qt) estimated for each time interval between the points t = 0, 4, 8, 12, 26, 38, 52 (t = 2 was omitted because there were insufficient transitions to yield a robust model). Transition intensities were permitted to change between subsequent observation intervals, but remained homogeneous within each observation interval. The starting transition intensities were based on the observed frequencies of transitions in the data set and were calculated using the formula
in which nij is the observed number of transitions from Group i to Group j over the duration of the study period (T), and nj is the initial number of patients in Group j. The fitted models were robust to the choice of starting transition intensities and yielded qualitatively similar parameter estimates over a range of starting parameters (not shown). The likelihood function was maximized using a Nelder-Mead algorithm, and convergence was visually verified and typically occurred well short of the maximum number of iterations.
Logistic regression models were used to test whether utility measurements from earlier time points could predict long-term outcomes. These models only included utility values up to a particular time point as predictors, with the response variable being the patient’s 1-year outcome (higher or lower utility group) modeled as a dichotomous variable; no additional clinical or demographic covariates were included in the models. The models were fitted using the �rms� package[7] and the fit was assessed using chi-square tests (? ? 0.05). Separate regression models were created for all utility measurements up to and including those for 2, 4, 8, 12, and 26 weeks; for example, the 8-week model would include utility measurements at 0, 2, 4, and 8 weeks. The AUC statistic was used to assess the performance of the models and was calculated using the ROCR package.[14]
Results
Delineation of Higher and Lower Utility Groups
The distributions of patient utility scores markedly changed over the course of 1 year of conservative care (Fig. 1). At baseline, the majority of patients reported a relatively poor quality of life; the mean EQ-5D score was 0.55 (median 0.60). Two distinct utility groups were found to be present at baseline: a �lower� utility group (EQ-5D ? 0.86) and a �higher� utility group (EQ-5D = 1). At 6 months, the lower utility group (n = 62, 67%) was larger than the higher utility group (n = 31, 33%); at 1 year, the lower utility group (n = 53, 57%) had declined, but remained larger than the higher utility group (n = 40, 43%).
Figure 1: Distribution of EQ-5D patient utilities at baseline, 6 months, and 1 year. The solid lines depict Gaussian kernel density estimates (right axis) of each distribution. The gray lines outline the histogram with the height of each bar representing the frequency of patients (left axis) in the equal-width bins (0.05) with utility greater than the lower bound and less than or equal to the upper bound. The bounds of both distributions are set to the theoretical minimum and maximum of the EQ-5D utility instrument.
EQ-5D Domain Scores Between Groups
The average scores in each domain of the EQ-5D (Table 1) suggested that the pain/discomfort (low score = 1.9, high score = 1.0), mobility (low score = 1.4, high score = 1.0), and usual activities (low score = 1.5, high score = 1.0) domains differed most significantly between the high and low utility groups (p ? 0.001). The anxiety (low score = 1.2, high score = 1.0) and self-care (low score = 1.1, high score = 1.0) domains differed much less between the 2 utility groups, although they were also significant (p < 0.01).
Trajectory of Patient Utility Over Time
The series of patient utility scores measured over the study period are referred to as utility �trajectories,� which were studied to understand how patients recovered over the study period. In the study cohort, all patients experienced improvement during at least 1 observation period; only 19.3% (n = 18) never experienced a decline during their recovery. Recovery was variable: 49.5% of the patients (n = 46) experienced at least 2 reversals, which were defined as improvements (declines) immediately followed by declines (improvements) at the next observation. Furthermore, only 29% of patients (n = 27) had stable trajectories with no reversals. Overall, increases in utility were 4 times more common than decreases in utility.
The utility of the entire cohort increased by 0.296 (51.8% above baseline; p ? 0.001, Wilcoxon Mann-Whitney test) over the year (Fig. 2), but was markedly faster during the first 2 months (0.022/week) than the final 3 months (0.005/week). Over the same time frames, utility scores improved by 0.178 (35.2% above the baseline average) over the first 2 months and by 0.063 (1.3% above the 9-month average) during the final 3 months. The mean utility scores significantly differed between the 2 final utility groups at 8 weeks and remained significant for the rest of the year (p < 0.01, Student t-test; Fig. 2).
Figure 2: Graph of mean patient utilities at each measurement time point. Error bars represent 95% CIs about the mean. High and low utility group refers to the final group in which the patient belongs at the 1-year time point.
Modeling Patient Recovery
Given that 2 utility groups were present over the study period, Markov models were used to study the robustness of these groups by estimating the likelihood of patients switching between the groups. The models suggested that the average probability of a patient remaining within their utility group was 97.9% and 97.6% for patients currently in the low and high utility groups, respectively (Fig. 3). The probability of a patient transitioning from the low to the high utility group was 2.1%; the corresponding probability for transitions from the high to the low utility group was 2.3%.
Figure 3: Graphs of the Markov transition probabilities (per week) for transitions within (lower) and between (upper) utility groups. Each point is centered at the middle of each time interval and represents the maximum-likelihood estimate of the per-week transition probability during the entire interval. Error bars (mean width of the 95% CI was 1.8) were omitted for clarity because the differences were not significant.
The models also suggested that the likelihood of a patient transitioning to another utility group declined over the study period. During the first 8 weeks, 2.8% and 3.5% of patients experienced low-to-high and high-to-low transitions, respectively; over the last 3 months, 1.6% and 1.3% of patients experienced low-to-high and high-to-low group transitions, respectively.
Predicting Individual Patient Outcome
At 8 weeks, logistic regression models could predict a patient’s outcome (final utility group) with modest accuracy (AUC = 0.62, or 62%). The accuracy of the models steadily increased as data from later time points were included; the 26-week model performance was good with an AUC of 0.78 (Fig. 4). The amount of improvement in utility scores from baseline to 8 weeks was also investigated as a predictor of good outcome (higher utility group). Patients with EQ-5D scores that improved by at least 0.30 during the first 8 weeks of treatment were 60% more likely to have a good outcome.
Figure 4: Graph showing the accuracy of classifiers based on patient utilities. The horizontal line is drawn at 0.50, above which models would perform better than randomly assigning patients to utility groups.
Dr. Alex Jimenez’s Insight
Herniated disc commonly develop in the lumbar spine, or lower back. Also referred to as a slipped disc or a ruptured disc, a herniated disc occurs when the soft, gel-like center of an intervertebral disc pushes through a tear in its surrounding outer ring, known as the annulus fibrosus. The symptoms of a herniated disc are generally specific to the exact level of the spine where the disc herniation occurs and whether or not the nerve tissue has been irritated by the intervertebral disc material leaking out of the inside of the disc. The most common symptoms of a disc herniation include pain, numbness, weakness and tingling sensations as well as causing radiating symptoms along the upper or lower extremities. Depending on the severity of the symptoms, herniated disc treatment can include, drugs and/or medications, epidural injections, physical therapy, chiropractic, and surgery, among others. According to the following article, early treatment can help promote and manage a faster herniated disc recovery from prolonged non-operative treatment methods.
Discussion
Several studies have sought to compare the relative effectiveness of surgery and conservative care for treatment of a lumbar disc herniation.[4�9,11] Generally, these studies have compared �average� differences between the study cohorts, while the individual trajectories by which patient utility changes over time have received less attention. To our knowledge, this study provides the first comprehensive statistical analysis of individual patient-level utility data from a large cohort of patients randomized to a prolonged conservative-care treatment protocol for lumbar disc herniation.[9]
The decision to proceed with surgery is straightforward in patients with severe, disabling symptoms or neurological deficits. Likewise, the decision to continue conservative care is simple for patients with mild symptoms or those who are content to live with their symptoms indefinitely. However, patients with moderate symptoms often present a greater challenge because most patients would prefer to avoid surgery if possible, but are also not content to wait indefinitely for their pain to resolve. These patients often ask for more than just the overall probability they will improve eventually; they usually want to know when they will recover. Moreover, they are usually interested in whether their current symptoms and progress affect the probability and extent of their future improvement.
For patients with moderate symptoms, the following observations from our study may be useful. First, the utility scores for individual patients diverged sharply at 8 weeks and were thereafter easily classified as either those reporting no health problems (higher utility, EQ-5D = 1) or those reporting at least some health problems (lower utility, EQ-5D ? 0.86). Among the lower utility group, the �pain/discomfort,� �mobility,� and �usual activities� domains of the EQ-5D differed most significantly from the higher utility group, which could potentially represent incompletely treated radiculopathy. Second, most improvement occurred early: almost one-third of the overall improvement in utility came in the first 2 months, while only 1% occurred in the last 3 months. Third, recovery is variable, with most patients (80%) experiencing at least 1 interval of deterioration and only 19% continuously improving without any setbacks. This may provide some reassurance to patients with generally good recovery to �stay the course� without resorting to more invasive measures such as surgery simply because of what may be a brief transient decrease in quality of life. Lastly, the probability of moving into another group was quite low (2%), which may be considered when counseling a patient who is not improving with his or her current treatment regimen.
We note the following limitations inherent in this cohort study. First, this is an observational study, and therefore we cannot infer causality for the emergence of the 2 utility groups, and because the individual treatment plans were unknown to us, we cannot comment on any specific type of conservative therapy. However, even if one considers the patients in the low utility group as nonresponders to conservative therapy (which is likely at least partly incorrect), the study does not imply that surgery would necessarily be beneficial in these patients. Second, the EQ-5D scores a patient’s overall health, and therefore unknown comorbid conditions likely account for at least some of the patients residing in the lower utility group and for part of the utility fluctuations. However, in the clinical setting, it should be obvious as to whether a patient’s symptoms are resulting from unresolved radiculopathy or from preexisting comorbidities. Lastly, we excluded crossover patients from our analysis. Crossover patients are likely those with the most severe symptoms and thus our results may be limited to patients with mild to moderate symptoms. However, we believe this exclusion is appropriate because, as mentioned above, the decision to operate is fairly straightforward when a patient has severe symptoms. From a clinical standpoint, patients with moderate symptoms and without neurological deficits after 8 weeks need the most information about the potential time course and extent of their nonoperative recovery to make an informed treatment decision.
The focus of the present study is individual utility recovery within a patient cohort rather than comparing average response to different treatment protocols. The goal was to gain insight into the dynamics of utility recovery among individual patients treated conservatively, but our approach could be applied to almost any treatment protocol. Studies of the changes (improvements or declines) in individual utility over time are useful because they may provide insights into a patient’s perception of their current treatment protocol (for example, patients in the low utility group would likely report a poor response to treatment), and also to identify a point at which continuing the same treatment is unlikely to improve a patient’s quality of life. Patients entering a conservative-care treatment protocol are likely to experience an initial period of rapid recovery, followed by a longer phase of more modest recovery. Our results suggest that, once the long-term recovery phase begins, patients are unlikely to spontaneously change their recovery for better or worse under the same treatment protocol. Lastly, patient utility scores early in the treatment process were reasonable predictors of long-term outcomes. This study is a comprehensive characterization of individual patients’ recovery of health utility from a lumbar disc herniation, and provides a unique picture for clinicians taking care of these patients. Our findings suggest that most recovery occurs early during treatment, and this early recovery period is important to long-term outcomes.
Conclusions
In a cohort of patients undergoing prolonged conservative care for treatment of lumbar disc herniation, 57% of the patients had lingering health problems at 1 year. Utility was recovered most rapidly early in the treatment process, and the majority of utility was also recovered in the initial treatment period. After the initial recovery period, we could identify with reasonable accuracy those patients who would fully recover and those who would not. Over the course of the year, recovery was observed to be highly variable, although most fluctuations were relatively small and only transient. These findings suggest that patients not initially responding to their treatment protocol should consider other options because they are unlikely to respond at a later time. However, patients and clinicians should also be mindful of transient decreases in quality of life, and carefully consider any changes in their treatment plan.
Disclosure
This work was partially supported by a charitable grant from the St. David’s Foundation Impact Fund to Dr. Cowperthwaite, and does not necessarily represent the views of the Impact Fund or the St. David’s Foundation.
Author contributions to the study and manuscript preparation include the following. Conception and design: all authors. Acquisition of data: Cowperthwaite, van den Hout. Analysis and interpretation of data: all authors. Drafting the article: Cowperthwaite. Critically revising the article: all authors. Reviewed submitted version of manuscript: all authors. Approved the final version of the manuscript on behalf of all authors: Cowperthwaite. Statistical analysis: Cowperthwaite, van den Hout. Administrative/technical/material support: Cowperthwaite. Study supervision: Cowperthwaite.
In conclusion, early non-operative treatment of lumbar herniated disc can effectively improve as well as manage recovery outcomes in patients with the condition. It’s important for patients with disc herniations in the lumbar spine to comprehend the source of their issue before receiving appropriate treatment for their symptoms. Furthermore, non-operative treatment is effective in most patients, surgical interventions may be considered according to the individual’s recovery outcome. Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Neck Pain
Neck pain is a common complaint which can result due to a variety of injuries and/or conditions. According to statistics, automobile accident injuries and whiplash injuries are some of the most prevalent causes for neck pain among the general population. During an auto accident, the sudden impact from the incident can cause the head and neck to jolt abruptly back-and-forth in any direction, damaging the complex structures surrounding the cervical spine. Trauma to the tendons and ligaments, as well as that of other tissues in the neck, can cause neck pain and radiating symptoms throughout the human body.
1. Andersson GB, Brown MD, Dvorak J, Herzog RJ, Kambin P, Malter A, et al.: Consensus summary of the diagnosis and treatment of lumbar disc herniation. Spine (Phila Pa 1976) 21:24 Suppl75S�78S, 1996 Medline
2. Atlas SJ, Deyo RA, Keller RB, Chapin AM, Patrick DL, Long JM, et al.: The Maine Lumbar Spine Study, Part II. 1-year outcomes of surgical and nonsurgical management of sciatica. Spine (Phila Pa 1976) 21:1777�1786, 1996 Crossref, Medline
3. Atlas SJ, Deyo RA, Keller RB, Chapin AM, Patrick DL, Long JM, et al.: The Maine Lumbar Spine Study, Part III. 1-year outcomes of surgical and nonsurgical management of lumbar spinal stenosis. Spine (Phila Pa 1976) 21:1787�1795, 1996 Crossref, Medline
4. Baldwin NG: Lumbar disc disease: the natural history. Neurosurg Focus 13:2E2, 2002
5. Dawson E, Bernbeck J: The surgical treatment of low back pain. Phys Med Rehabil Clin N Am 9:489�495, x, 1998
6. EuroQol Group: EuroQol�a new facility for the measurement of health-related quality of life. The EuroQol Group Health Policy 16:199�208, 1990 Crossref, Medline
7. Harrell FE: Regression Modeling Strategies: With Applications to Linear Models, Logistic Regression and Survival Analysis New York, Springer, 2001
8. Jackson CH, Sharples LD, Thompson SG, Duffy SW, Couto E: Multistate Markov models for disease progression with classification error. The Statistician 52:193�209, 2003
9. Keller RB, Atlas SJ, Singer DE, Chapin AM, Mooney NA, Patrick DL, et al.: The Maine Lumbar Spine Study, Part I. Background and concepts. Spine (Phila Pa 1976) 21:1769�1776, 1996 Crossref, Medline
10. Peul WC, van den Hout WB, Brand R, Thomeer RTWM, Koes BW: Prolonged conservative care versus early surgery in patients with sciatica caused by lumbar disc herniation: two year results of a randomised controlled trial. BMJ 336:1355�1358, 2008 Crossref, Medline
11. Peul WC, van Houwelingen HC, van der Hout WB, Brand R, Eekhof JA, Tans JT, et al.: Prolonged conservative treatment or �early� surgery in sciatica caused by a lumbar disc herniation: rationale and design of a randomized trial [ISRCT 26872154]. BMC Musculoskelet Disord 6:8, 2005 Crossref, Medline
12. Shaw JW, Johnson JA, Coons SJ: US valuation of the EQ-5D health states: development and testing of the D1 valuation model. Med Care 43:203�220, 2005 Crossref, Medline
13. Silverman BW: Density Estimation for Statistics and Data Analysis London, Chapman & Hall, 1986
14. Sing T, Sander O, Beerenwinkel N, Lengauer T: ROCR: visualizing classifier performance in R. Bioinformatics 21:3940�3941, 2005
15. van den Hout WB, Peul WC, Koes BW, Brand R, Kievit J, Thomeer RTWM, et al.: Prolonged conservative care versus early surgery in patients with sciatica from lumbar disc herniation: cost utility analysis alongside a randomised controlled trial. BMJ 336:1351�1354, 2008 Crossref, Medline
16. Weber H: Lumbar disc herniation. A controlled, prospective study with ten years of observation. Spine (Phila Pa 1976) 8:131�140, 1983 Crossref, Medline
17. Weinstein JN, Lurie JD, Tosteson TD, Skinner JS, Hanscom B, Tosteson ANA, et al.: Surgical vs nonoperative treatment for lumbar disk herniation: the Spine Patient Outcomes Research Trial (SPORT) observational cohort. JAMA 296:2451�2459, 2006 Crossref, Medline
18. Weinstein JN, Tosteson TD, Lurie JD, Tosteson ANA, Hanscom B, Skinner JS, et al.: Surgical vs nonoperative treatment for lumbar disk herniation: the Spine Patient Outcomes Research Trial (SPORT): a randomized trial. JAMA 296:2441�2450, 2006 Crossref, Medline
Close Accordion
Blank
Cited By
1. Anurekha Ramakrishnan, MS, K. Michael Webb, MD, and Matthew C. Cowperthwaite, PhD. (2017) One-year outcomes of early-crossover patients in a cohort receiving nonoperative care for lumbar disc herniation. Journal of Neurosurgery: Spine 27:4, 391-396. . Online publication date: 1-Oct-2017. Abstract | Full Text | PDF (2037 KB)
2. Kimberly A Plomp, Una Strand Vi�arsd�ttir, Darlene A Weston, Keith Dobney, Mark Collard. (2015) The ancestral shape hypothesis: an evolutionary explanation for the occurrence of intervertebral disc herniation in humans. BMC Evolutionary Biology 15:1. . Online publication date: 1-Dec-2015. [Crossref]
One of the most prevalent causes of lower back pain and sciatica may be due to the compression of the nerve roots in the low back from a lumbar herniated disc, or a ruptured disc in the lumbar spine. Common symptoms of lumbar herniated discs include varying intensities of pain, muscle spasms or cramping, sciatica and leg weakness as well as loss of proper leg function. While these may not appear to be closely associated with each other, a lumbar herniated disc may also affect the cervical spine, manifesting symptoms of migraine and headache. The purpose of the following articles is to educate patients and demonstrate the relation between migraine pain and lumbar herniated disc, further discussing the treatment of these two common conditions.
A Critical Review of Manual Therapy Use for Headache Disorders: Prevalence, Profiles, Motivations, Communication and Self-Reported Effectiveness
Abstract
Background
Despite the expansion of conventional medical treatments for headache, many sufferers of common recurrent headache disorders seek help outside of medical settings. The aim of this paper is to evaluate research studies on the prevalence of patient use of manual therapies for the treatment of headache and the key factors associated with this patient population.
Methods
This critical review of the peer-reviewed literature identified 35 papers reporting findings from new empirical research regarding the prevalence, profiles, motivations, communication and self-reported effectiveness of manual therapy use amongst those with headache disorders.
Results
While available data was limited and studies had considerable methodological limitations, the use of manual therapy appears to be the most common non-medical treatment utilized for the management of common recurrent headaches. The most common reason for choosing this type of treatment was seeking pain relief. While a high percentage of these patients likely continue with concurrent medical care, around half may not be disclosing the use of this treatment to their medical doctor.
Conclusions
There is a need for more rigorous public health and health services research in order to assess the role, safety, utilization and financial costs associated with manual therapy treatment for headache. Primary healthcare providers should be mindful of the use of this highly popular approach to headache management in order to help facilitate safe, effective and coordinated care.
The co-occurrence of tension headache and migraine is very high [1]. Respectively, they are the second and third most common disorders worldwide with migraine ranking as the seventh highest specific cause of disability globally [2] and the sixteenth most commonly diagnosed condition in the US [3]. These common recurrent headache disorders place a considerable burden upon the personal health, finances and work productivity of sufferers [3�5] with migraine further complicated by an association with cardiovascular and psychiatric co-morbidities [6, 7].
Preventative migraine drug treatments include analgesics, anticonvulsants, antidepressants and beta-blockers. Preventative drug treatments for tension-type headaches can include analgesics, NSAIDs, muscle relaxants and botulinum toxin as well as anticonvulsants and antidepressants. While preventative drug treatments are successful for a significant proportion of sufferers, headache disorders are still reported as under-diagnosed and under-treated within medical settings [8�16] with other studies reporting sufferers can cease continuing with preventative headache medications long-term [9, 17].
There is a number of non-drug approaches also utilized for the prevention of headaches. These include psychological therapies such as cognitive behavioral therapy, relaxation training and EMG (electromyography) biofeedback. In addition, there is acupuncture, nutritional supplementation (including magnesium, B12, B6, and Coenzyme Q10) and physical therapies. The use of physical therapies is significant, with one recent global survey reporting physical therapy as the most frequently used �alternative or complementary treatment� for headache disorders across many countries [18]. One of the most common physical therapy interventions for headache management is manual therapy (MT), [19�21] which we define here as treatments including �spinal manipulation (as commonly performed by chiropractors, osteopaths, and physical therapists), joint and spinal mobilization, therapeutic massage, and other manipulative and body-based therapies� [22].
Positive results have been reported in many clinical trials comparing MT to controls [23�27], other physical therapies [28�30] and aspects of medical care [31�34]. More high quality research is needed however to assess the efficacy of MT as a treatment for common recurrent headaches. Recent systematic reviews of randomized clinical trials of MT for the prevention of migraine report a number of significant methodological short-comings and the need for more high quality research before any firm conclusions can be made [35, 36]. Recent reviews of MT trials for tension-type headache and cervicogenic headache are cautious in reporting positive outcomes and the strong need for further robust research [37�41]. Despite the limited clinical evidence there has been no critical review of the significant use of MT by headache populations.
Methods
The aim of this study is to report from the peer-reviewed literature; 1) the prevalence of MT use for the treatment of common recurrent headaches and 2) factors associated with this use across several key themes. The review further identifies key areas worthy of further research in order to better inform clinical practice, educators and healthcare policy within this area.
Design
A comprehensive search of peer-reviewed articles published in English between 2000 and 2015 reporting new empirical research findings of key aspects of MT use among patients with migraine and non-migraine headache disorders was undertaken. Databases searched were MEDLINE, AMED, CINAHL, EMBASE and EBSCO. The key words and phrases used were: �headache�, �migraine�, �primary headache�, �cephalgia�, �chronic headache� AND �manual therapy�, �spinal manipulation�, �manipulative therapy�, �spinal mobilization�, �chiropractic�, �osteopathy�, �massage�, �physical therapy� or �physiotherapy� AND then �prevalence�, �utilization� or �profile� was used for additional searches against the previous terms. The database search was accompanied by a hand search of prominent peer-reviewed journals. All authors accessed the reviewed literature (data) and provided input to analysis.
Due to the focus of the review, literature reporting randomized control trials and similar clinical research designs were excluded as were articles identified as letters, correspondence, editorials, case reports and commentaries. Further searches were undertaken of the bibliographies in the identified publications. All identified articles were screened and only those reporting new empirical findings on MT use for headache in adults were included in the review. Articles identified and selected for the review were research manuscripts mostly within epidemiological and health economics studies. The review includes papers reporting MT use pooled with the use of other therapies, but only where MT patients comprised a large proportion (as stated) of the included study population. Results were imported into Endnote X7 and duplicates removed.
Search Outcomes, Analyses and Quality Appraisal
Figure 1 outlines the literature search process. The initial search identified 3286 articles, 35 of which met the inclusion criteria. Information from each article was organized into a review table (Table 1) to summarise the findings of the included papers. Information is reported under two selected headache groups and within each individual MT profession – chiropractic, physiotherapy, osteopathy and massage therapy � where sufficient detail was available.
Figure 1: Flow Chart of Study Selection.
Table 1: Research-based studies of manual therapy use for headache disorders.
An appraisal of the quality of the articles identified for review was conducted using a quality scoring system (Table 2) developed for the critical appraisal of health literature used for prevalence and incidence of health problems [42] adapted from similar studies [43�45]. This scoring system was applicable to the majority of study designs involving surveys and survey-based structured interviews (29 of the 35 papers) but was not applicable to a small number of included studies based upon clinical records, secondary analysis or practitioner characteristics.
Two separate authors (CM and JA) independently searched and scored the articles. Score results were compared and any differences were further discussed and resolved by all the authors. The quality score of each relevant article is reported in Table 3.
Results
The key findings of the 35 articles were grouped and evaluated using a critical review approach adapted from previous research [46, 47]. Based on the limited information available for other headache types, prevalence findings are reported within one of two categories – either as �migraine� for papers reporting studies where the population was predominately or entirely made up of migraine patients or as �headache� for papers where the study population was predominately other headache types (including tension-type headaches, cluster headaches, cervicogenic headache) and/or where the headache type was not clearly stated. Ten papers reported findings examining prevalence rates for the �migraine� category alone, 18 papers reported findings examining prevalence for the �headache� category alone and 3 papers reported findings for both categories. Based on the nature of the information available, prevalence use was categorised by manual therapy providers. The extracted data was then analysed and synthesized into four thematic categories: prevalence; profile and motivations for MT use; concurrent use and order of use of headache providers; and self-reported evaluation of MT treatment outcomes.
Prevalence of MT Use
Thirty-one of the reviewed articles with a minimum sample size (>100) reported findings regarding prevalence of MT use. The prevalence of chiropractic use for those with migraine ranged from 1.0 to 36.2% (mean: 14.4%) within the general population [19�21, 48�52] and from 8.9 to 27.1% (mean: 18.0%) within headache-clinic patient populations [53, 54]. The prevalence of chiropractic use for those reported as headache ranged from 4 to 28.0% (mean: 12.9%) within the general population [20, 48, 51, 55�57]; ranged from 12.0 to 22.0% (mean: 18.6%) within headache/pain clinic patient populations [58�60] and from 1.9 to 45.5% (mean: 9.8%) within chiropractic patient populations [61�69].
The prevalence use of physiotherapy for those with migraine ranged from 9.0 to 57.0% (mean: 24.7%) within the general population [19, 20, 48, 52] and from 4.9 to 18.7% (mean: 11.8%) within headache-clinic patient populations [54, 70]. The prevalence use of physiotherapy for those reported as headache ranged from 12.2 to 52.0% (mean: 32.1%) within the general population [20, 48] and from 27.8 to 35.0%% (mean: 31.4%) within headache/pain clinic populations [60, 70].
Massage therapy use for those with migraine ranged from 2.0 to 29.7% (mean: 15.6%) within the general population [49, 50, 71] and from 10.1 to 56.4% (mean: 33.9%) within headache-clinic populations [53, 54, 72, 73]. Massage/acupressure use for those reported as headache within headache/pain clinic patient populations ranged from 12.0 to 54.0% (mean: 32.5%) [58�60, 70].
Osteopathy use for those with migraine was reported as 1% within the general population [49]; as 2.7% within a headache-clinic patient population [53] and as 1.7% within an osteopathy patient population [74]. For headache the prevalence was 9% within a headache/pain clinic population [60] and ranged from 2.7 to 10.0% (mean: 6.4%) within osteopathy patient populations [74, 75].
The combined prevalence rate of MT use across all MT professions for those with migraine ranged from 1.0 to 57.0% (mean: 15.9%) within the general population; ranged from 2.7 to 56.4% (mean: 18.4%) within headache-clinic patient populations and was reported as 1.7% in one MT patient population. The combined prevalence rate of MT use across all MT professions for those reported as headache ranged from 4.0 to 52.0% (mean: 17.7%) within the general population; ranged from 9.0 to 54.0% (mean: 32.3%) within headache-clinic patient populations and from 1.9 to 45.5% (mean: 9.25%) within MT patient populations.
Profile and Motivations for MT Use
While patient socio-demographic profiles were not reported within headache populations that were exclusively using MT, several studies report these findings where MT users made up a significant percentage of the non-medical headache treatments utilized by the study population (range 40% � 86%: mean 63%). While findings varied for level of income [58, 70] and level of education, [70, 72, 73] this patient group were more likely to be older [70, 72], female [20], have a higher rate of comorbid conditions [58, 70, 76] and a higher rate of previous medical visits [20, 58, 70] when compared to the non-user group. Overall, this group were reported to have a higher level of headache chronicity or headache disability than non-users [20, 54, 58, 70, 72, 77].
Several studies within headache-clinic populations report patient motivations for the use of complementary and alternative headache treatments where MT users made up a significant proportion of the study population (range 40% � 86%: mean 63%) [58, 70, 72, 78]. From these studies the most common motivation reported by study patients was �seeking pain relief� for headache which accounted for 45.4% � 84.0% (mean: 60.5%) of responses. The second most common motivation was patient concerns regarding the �safety or side effects� of medical headache treatment, accounting for 27.2% � 53.0% (mean: 43.8%) of responses [58, 70, 72]. �Dissatisfaction with medical care� accounted for 9.2% � 35.0% (mean: 26.1%) of responses [58, 70, 72].
A limited number of reviewed papers (all from Italy) report on the source of either the referral or recommendation to MT for headache treatment [53, 58, 59]. From these studies, referral from a GP to a chiropractor ranged from 50.0 to 60.8% (mean: 55.7%), while referral from friends/relatives ranged from 33.0 to 43.8% (mean: 38.7%) and self-recommendation ranged from 0 to 16.7% (mean: 5.6%). For massage therapy, referral from a GP ranged from 23.2 to 50.0% (mean: 36.6%), while referral from friends/relatives ranged from 38.4 to 42.3% (mean: 40.4%) and self-recommendation ranged from 7.7 to 38.4% (mean: 23.1%). For acupressure, referral from a GP ranged from 33.0 to 50.0% (mean: 41.5%), while referral from friends/relatives was reported as 50% and self-recommendation ranged from 0 to 16.6% (mean: 8.3%). One study reported findings for osteopathy where referral from both GP�s and friends/relatives was reported as 42.8% and self-recommendation was reported as 14.4%. Overall, the highest proportion of referrals within these studies was from GPs to chiropractors for chronic tension-type headache (56.2%), cluster headache (50%) and migraine (60.8%).
Concurrent Use and Order of Use of Headache Providers and Related Communication of MT Users
Several studies report on the concurrent use of medical headache management with complementary and alternative therapies. In those studies where the largest percentage of the patient population were users of MT�s (range 57.0% � 86.4%: mean 62.8%), [58, 70, 78] concurrent use of medical care ranged between 29.5% and 79.0% (mean: 60.0%) of the headache patient population.
These studies further report on the level of patient non-disclosure to medical providers regarding the use of MT for headache. Non-disclosure ranged between 25.5 and 72.0% (mean: 52.6%) of the patient population, with the most common reason for non-disclosure reported as the doctor �never asking�, ranging from 37.0 to 80.0% (mean: 58.5%). This was followed by a patient belief that �it was not important for the doctor to know� or �none of the doctor�s business�, ranging from 10.0 to 49.8% (mean: 30.0%). This was followed by a belief that either �the doctor would not understand� or �would discourage� these treatments, ranging from 10.0 to 13.0% (mean: 11.5%) [53, 77].
One large international study reported the ordering of the typical provider of headache care by comparing findings between several countries for migraine patients [21]. Primary care providers followed by neurologists were reported as the first and second providers for migraine treatment for nearly all countries examined. The only exception was Australia, where those with chronic migraine selected chiropractors as typical providers at equal frequency to neurologists (14% for both) while those with episodic migraine selected chiropractors at a greater frequency to neurologists (13% versus 5%). Comparatively, chiropractors were selected as the typical provider for those with chronic migraine by 10% in USA and Canada, 1% in Germany and 0% for UK and France. Chiropractors were selected as the typical provider for those with episodic migraine by 7% in USA, 6% in Germany, 4% in Canada and by 1% in both the UK and France.
Self-Reported Effectiveness of MT Treatment Outcomes
Several headache and pain-clinic population studies provide findings for the self-reported effectiveness of MT headache treatment. For chiropractic, patient self-reporting of partially effective or fully effective headache relief ranged from 27.0 to 82.0% (mean: 45.0%) [53, 58�60, 78]. For massage therapy, patient self-reporting of partially effective or fully effective headache relief ranged from 33.0 to 64.5% (mean: 45.2%)[53, 58, 60, 73, 78], and for acupressure this ranged from 33.4 to 50.0% (mean: 44.5%) [53, 58, 59]. For osteopathy and physiotherapy, one study reported effectiveness as 17 and 36% respectively [60].
When results are combined across all MT professions the reporting of MT as either partially or fully effective ranged from 17.0 to 82.0% (mean 42.5%) [53, 58�60, 73, 78]. In addition, one general population study provides findings for the self-reported effectiveness for chiropractic and physiotherapy at 25.6 and 25.1% respectively for those with primary chronic headache and 38 and 38% respectively for those with secondary chronic headache [79].
Discussion
This paper provides the first critical integrative review on the prevalence and key factors associated with the use of MT treatment for headaches within the peer-reviewed literature. While study methodological limitations and lack of data prevent making strong conclusions, these findings raise awareness of issues of importance to policy-makers, educators, headache providers and future research.
Our review found that MT use was generally higher within medical headache-clinic populations when compared to general populations. However, the use of individual MT providers does vary between different regions and this is likely due to a number of factors including variation in public access, healthcare funding and availability of MT providers. For example, the use of physiotherapy for some headache types may be relatively higher in parts of Europe [20, 60] while the use of chiropractors for some headache types may be relatively higher in Australia and the USA [19, 21]. Overall, the prevalence use of MT for headache appears to be substantial and likely to be the most common type of physical therapy utilized for headache in many countries [19�21, 49]. More high quality epidemiological studies are needed to measure the prevalence of MT use across different headache types and sub-types, both within the general population and clinical populations.
Beyond prevalence, data is more limited regarding who, how and why headache patients seek MT. From the information available however, the healthcare needs of MT headache patients may be more complex and multi-disciplinary in nature compared to those under usual medical care alone. Socio-demographic findings suggest that users of MT and other complementary and alternative therapies have a higher level of headache disability and chronicity compared to non-users. This finding may correlate with the higher prevalence of MT users within headache-clinic populations and a history of more medical appointments. This may also have implications for future MT trial designs both in terms of the selection of trial subjects from inside versus outside MT clinical settings and the decision to test singular MT interventions versus MT in combination with other interventions.
Limited information suggests that a pluralistic approach toward the use of medical and non-medical headache treatments such as MT is common. While findings suggest MT is sought most often for reasons of seeking headache relief, the evidence to support the efficacy of MT for headache relief is still limited. MT providers must remain mindful of the quality of the evidence for a given intervention for a given headache disorder and to inform patients where more effective or safer treatment interventions are available. More research is needed to assess these therapies individually and through multimodal approaches and for studies to include long-term follow-up.
Information limited to Italy, suggests referral from GPs for MT headache treatment can be common in some regions, while this is less likely to widespread given the issue of patient non-disclosure to medical doctors regarding the use of this treatment in other studies. High quality healthcare requires open and transparent communication between patients and providers and between the providers themselves. Non-disclosure may adversely influence medical management should unresponsive patients require further diagnostic investigations [80] or the implementation of more effective approaches to headache management [81] or prevents discussion in circumstances where MT may be contraindicated [82]. Primary headache providers may benefit from paying particular attention to the possibility of non-disclosure of non-medical headache treatments. Open discussion between providers and patients about the use of MT for headache and the associated outcomes may improve overall patient care.
Future Research
Despite the strong need for more high quality research to assess the efficacy of MT as a treatment for headache, the substantial use of MT brings attention to the need for more public health and health services research within this area of headache management. The need for this type of research was identified in a recent global report on the use of headache-related healthcare resources [18]. Furthering this information can lead to improvements in healthcare policy and the delivery of healthcare services.
The substantial use of physical therapies such as MT has been under-reported within many of the national surveys reporting headache-related healthcare utilization [3, 5, 83�85]. Regardless, the role of physical therapies in headache management continues to be assessed, often within mainstream and integrated headache management settings [86�89]. Continuing this research may further our understanding of the efficacy and outcomes associated with a more multidisciplinary approach to headache management.
Further to this is the need for more research to understand the healthcare utilization pathways associated with those patients who use MT in their headache management. Little is known about the sociodemographic background, types of headaches, level of headache disability and comorbidities more common to this patient population. In turn, such information can provide insights that may be valuable to provider clinical decision-making and provider education.
Limitations
The design and findings of our review has a number of limitations. The design of the review was limited by a search within English language journals only. As a result, some research on this topic may have been missed. While the quality scoring system adopted for this review requires further validation, the data we collected was limited by the low to moderate quality of available papers which averaged 6.4 out of 10 points (Table 3). The low scoring was largely due to significant methodological issues and the small sample size associated with much of the collected papers. Much of the data on this topic was heterogeneous in nature (telephone, postal surveys and face-to-face interviews). There was a lack of validated practitioner and patient questionnaires to report findings, such as for questions on prevalence, where the time frames utilized varied between �currently�, �last 12 months� and �ever�.
Data on the prevalence of MT use for headache was limited particularly within individual MT provider populations when compared to data found within the general population and headache-clinic populations. Many studies assessed the use of MT for headache without identifying headache types. Only one study inside an MT population had reported the percentage of patients attending for reasons of migraine alone (osteopathy). The prevalence of MT use for headache was reported most within chiropractic patient population studies, however information was limited on the types of headache. We found no studies reporting the prevalence of headache patients within physiotherapy or massage therapy patient populations using our search terms.
A lack of data for some themes necessitated providing findings pooled with users of other non-medical headache providers. Data within many geographical regions was very limited with the most limited data was on the source of referral to MT headache providers (three papers from Italy only). These limitations support the call for more research to be focused exclusively within MT populations and different regional areas before stronger conclusions can be drawn.
Conclusion
The needs of those with headache disorders can be complex and multi-disciplinary in nature. Beyond clinical research, more high quality public health and health services research is needed to measure and examine a number of issues of significance to the delivery and use of MT�s within headache management. With unmet needs still remaining for many who suffer recurrent headaches, clinicians should remain cognizant of the use of MT�s and remain open to discussing this approach to headache management in order to ensure greater safety, effectiveness and coordination of headache care.
Acknowledgements
Not applicable.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors while the first author on this paper receives a PhD scholarship made available by the Australian Chiropractors� Association.
Availability of Data and Materials
Not applicable (all data is reported in article).
Authors’ Contributions
CM, JA and DS designed the paper. CM carried out the literature search, data collection and selection. CM and DS provided the analysis and interpretation. CM and JA wrote the drafts. All authors contributed to the critical review and intellectual content. All authors read and approved the final manuscript.
Competing Interests
The authors declare that they have no competing interests.
Consent for Publication
Not applicable.
Ethics Approval and Consent to Participate
Not applicable.
Publisher�s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
A staggering 15% of the population suffers from migraines, a debilitating condition which affects an individual’s ability to engage in everyday activities. Although widely misunderstood by researches today, I believe that migraine pain can be a symptom of a much bigger underlying health issue. Lumbar herniated discs, or ruptured discs in the lumbar spine, are a common cause of lower back pain and sciatica. When the soft, gel-like center of a lumbar herniated disc compresses the nerve roots of the low back, it can result in symptoms of pain and discomfort, numbness and weakness in the lower extremities. What’s more, a lumbar herniated disc can unbalance the structure and function of the entire spine, eliciting symptoms along the cervical spine that could ultimately trigger migraines. People who constantly experience migraine pain often have to carefully go about their day in hopes of avoiding the blaze of another painful episode. Fortunately, many migraine pain and lumbar herniated disc treatment methods are available to help improve as well as manage the symptoms. Other treatment options can also be considered before surgical interventions.
Surgical versus Non-Operative Treatment for Lumbar Disc Herniation: Eight-Year Results for the Spine Patient Outcomes Research Trial (SPORT)
Abstract
Study Design
Concurrent prospective randomized and observational cohort studies.
Objective
To assess the 8-year outcomes of surgery vs. non-operative care.
Summary of Background Data
Although randomized trials have demonstrated small short-term differences in favor of surgery, long-term outcomes comparing surgical to non-operative treatment remain controversial.
Methods
Surgical candidates with imaging-confirmed lumbar intervertebral disc herniation meeting SPORT eligibility criteria enrolled into prospective randomized (501 participants) and observational cohorts (743 participants) at 13 spine clinics in 11 US states. Interventions were standard open discectomy versus usual non-operative care. Main outcome measures were changes from baseline in the SF-36 Bodily Pain (BP) and Physical Function (PF) scales and the modified Oswestry Disability Index (ODI – AAOS/Modems version) assessed at 6 weeks, 3 and 6 months, and annually thereafter.
Results
Advantages were seen for surgery in intent-to-treat analyses for the randomized cohort for all primary and secondary outcomes other than work status; however, with extensive non-adherence to treatment assignment (49% patients assigned to non-operative therapy receiving surgery versus 60% of patients assigned to surgery) these observed effects were relatively small and not statistically significant for primary outcomes (BP, PF, ODI). Importantly, the overall comparison of secondary outcomes was significantly greater with surgery in the intent-to-treat analysis (sciatica bothersomeness [p > 0.005], satisfaction with symptoms [p > 0.013], and self-rated improvement [p > 0.013]) in long-term follow-up. An as-treated analysis showed clinically meaningful surgical treatment effects for primary outcome measures (mean change Surgery vs. Non-operative; treatment effect; 95% CI): BP (45.3 vs. 34.4; 10.9; 7.7 to 14); PF (42.2 vs. 31.5; 10.6; 7.7 to 13.5) and ODI (?36.2 vs. ?24.8; ?11.2; ?13.6 to ?9.1).
Conclusion
Carefully selected patients who underwent surgery for a lumbar disc herniation achieved greater improvement than non-operatively treated patients; there was little to no degradation of outcomes in either group (operative and non-operative) from 4 to 8 years.
Keywords:SPORT, intervertebral disc herniation, surgery, non-operative care, outcomes
Introduction
Lumbar discectomy for relief of sciatica in patients with intervertebral disc herniation (IDH) is a well-researched and common indication for spine surgery, yet rates of this surgery exhibit considerable geographic variation.[1] Several randomized trials and large prospective cohorts have demonstrated that surgery provides faster pain relief and perceived recovery in patients with herniated disc.[2�6] The effect of surgery on longer term outcomes remains less clear.
In a classic RCT evaluating surgery versus non-operative treatment for lumbar IDH, Weber et al. showed a greater improvement in the surgery group at 1 year that was statistically significant; there was also greater improvement for surgery at 4 years, although not statistically significant, but no apparent difference in outcomes at 10 years.[2] However, a number of patients in the non-operative group eventually underwent surgery over that time, complicating the interpretation of the long-term results. The Maine Lumbar Spine Study, a prospective observational cohort, found greater improvement at one year in the surgery group that narrowed over time, but remained significantly greater in the surgical group for sciatica bothersomeness, physical function, and satisfaction, but no different for work or disability outcomes.[3] This paper reports 8-year results from the Spine Patient Outcomes Research Trial (SPORT) based on the continued follow-up of the herniated disc randomized and observational cohorts.
Methods
Study Design
SPORT is a randomized trial with a concurrent observation cohort conducted in 11 US states at 13 medical centers with multidisciplinary spine practices. The human subjects committees at each participating institution approved a standardized protocol for both the observational and the randomized cohorts. Patient inclusion and exclusion criteria, study interventions, outcome measures, and follow-up procedures have been reported previously.[5�8]
Patient Population
Men and women were eligible if they had symptoms and confirmatory signs of lumbar radiculopathy persisting for at least six weeks, disc herniation at a corresponding level and side on imaging, and were considered surgical candidates. The content of pre-enrollment non-operative care was not pre-specified in the protocol.[5�7] Specific enrollment and exclusion criteria are reported elsewhere.[6,7]
A research nurse at each site identified potential participants, verified eligibility and used a shared decision making video for uniformity of enrollment. Participants were offered enrollment in either the randomized trial or the observational cohort. Enrollment began in March of 2000 and ended in November of 2004.
Study Interventions
The surgery was a standard open discectomy with examination of the involved nerve root.[7,9] The non-operative protocol was �usual care� recommended to include at least: active physical therapy, education/counseling with home exercise instruction, and non-steroidal anti-inflammatory drugs if tolerated. Non-operative treatments were individualized for each patient and tracked prospectively.[5�8]
Study Measures
Primary endpoints were the Bodily Pain (BP) and Physical Function (PF) scales of the SF-36 Health Survey[10] and the AAOS/Modems version of the Oswestry Disability Index (ODI)[11] as measured at 6 weeks, 3 and 6 months, and annually thereafter. If surgery was delayed beyond six weeks, additional follow-up data was obtained 6 weeks and 3 months post-operatively. Secondary outcomes included patient self-reported improvement; work status; satisfaction with current symptoms and care;[12] and sciatica severity as measured by the sciatica bothersomeness index.[13,14] Treatment effect was defined as the difference in the mean changes from baseline between the surgical and non-operative groups.
Statistical Considerations
Initial analyses compared means and proportions for baseline patient characteristics between the randomized and observational cohorts and between the initial treatment arms of the individual and combined cohorts. The extent of missing data and the percentage of patients undergoing surgery were calculated by treatment arm for each scheduled follow-up. Baseline predictors of time until surgical treatment (including treatment crossovers) in both cohorts were determined via a stepwise proportional hazards regression model with an inclusion criterion of p < 0.1 to enter and p > 0.05 to exit. Predictors of missing follow-up visits at yearly intervals up to 8 years were separately determined via stepwise logistic regression. Baseline characteristics that predicted surgery or a missed visit at any time-point were then entered into longitudinal models of primary outcomes. Those that remained significant in the longitudinal models of outcome were included as adjusting covariates in all subsequent longitudinal regression models to adjust for potential confounding due to treatment selection bias and missing data patterns.[15] In addition, baseline outcome, center, age and gender were included in all longitudinal outcome models.
Primary analyses compared surgical and non-operative treatments using changes from baseline at each follow-up, with a mixed effects longitudinal regression model including a random individual effect to account for correlation between repeated measurements within individuals. The randomized cohort was initially analyzed on an intent-to-treat basis.[6] Because of cross-over, additional analyses were performed based on treatments actually received. In these as-treated analyses, the treatment indicator was a time-varying covariate, allowing for variable times of surgery. Follow-up times were measured from enrollment for the intent-to-treat analyses, whereas for the as-treated analysis the follow-up times were measured from the beginning of treatment (i.e. the time of surgery for the surgical group and the time of enrollment for the non-operative group), and baseline covariates were updated to the follow-up immediately preceding the time of surgery. This procedure has the effect of including all changes from baseline prior to surgery in the estimates of the non-operative treatment effect and all changes after surgery in the estimates of the surgical effect. The six-point sciatica scales and binary outcomes were analyzed via longitudinal models based on generalized estimating equations[16] with linear and logit link functions respectively, using the same intent-to-treat and adjusted as-treated analysis definitions as the primary outcomes. The randomized and observational cohorts were each analyzed to produce separate as-treated estimates of treatment effect. These results were compared using a Wald test to simultaneously test all follow-up visit times for differences in estimated treatment effects between the two cohorts.[15] Final analyses combined the cohorts.
To evaluate the two treatment arms across all time-periods, the time-weighted average of the outcomes (area under the curve) for each treatment group was computed using the estimates at each time period from the longitudinal regression models and compared using a Wald test.[15]
Kaplan-Meier estimates of re-operation rates at 8 years were computed for the randomized and observational cohorts and compared via the log-rank test.[17,18]
Computations were done using SAS procedures PROC MIXED for continuous data and PROC GENMOD for binary and non-normal secondary outcomes (SAS version 9.1 Windows XP Pro, Cary, NC). Statistical significance was defined as p < 0.05 based on a two-sided hypothesis test with no adjustments made for multiple comparisons. Data for these analyses were collected through February 4, 2013.
Results
Overall, 1,244 SPORT participants with lumbar intervertebral disc herniation were enrolled (501 in the randomized cohort, and 743 in the observational cohort) (Figure 1). In the randomized cohort, 245 were assigned to surgical treatment and 256 to non-operative treatment. Of those randomized to surgery, 57% had surgery by 1 year and 60% by 8 years. In the group randomized to non-operative care, 41% of patients had surgery by 1 year and 48% by 8 years. In the observational cohort, 521 patients initially chose surgery and 222 patients initially chose non-operative care. Of those initially choosing surgery, 95% received surgery by 1 year; at 8 years 12 additional patients had undergone primary surgery. Of those choosing non-operative treatment, 20% had surgery by 1 year and 25% by 8 years. In both cohorts combined, 820 patients received surgery at some point during the first 8 years; 424 (34%) remained non-operative. Over the 8 years, 1,192 (96%) of the original enrollees completed at least 1 follow-up visit and were included in the analysis (randomized cohort: 94% and observational cohort 97%); 63% of initial enrollees supplied data at 8 years with losses due to dropouts, missed visits, or deaths (Figure 1).
Figure 1: Exclusion, enrollment, randomization and follow-up of trial participants.
Patient Characteristics
Baseline characteristics have been previously reported and are summarized in Table 1.[5,6,8] The combined cohorts had an overall mean age of 41.7 with slightly more men than women. Overall, the randomized and observational cohorts were similar. However, patients in the observational cohort had more baseline disability (higher ODI scores), were more likely to prefer surgery, more often rated their problem as worsening, and were slightly more likely to have a sensory deficit. Subjects receiving surgery over the course of the study were: younger; less likely to be working; more likely to report being on worker�s compensation; had more severe baseline pain and functional limitations; fewer joint and other co-morbidities; greater dissatisfaction with their symptoms; more often rated their condition as getting worse at enrollment; and were more likely to prefer surgery. Subjects receiving surgery were also more likely to have a positive straight leg test, as well as more frequent neurologic, sensory, and motor deficits. Radiographically, their herniations were more likely to be at the L4�5 and L5-S1 levels and to be posterolateral in location.
Table 1: Patient baseline demographic characteristics, comorbidities and health status measures according to study cohort and treatment received.
Surgical Treatment and Complications
Overall surgical treatment and complications were similar between the two cohorts (Table 2). The average surgical time was slightly longer in the randomized cohort (80.5 minutes randomized vs. 74.9 minutes observational, p=0.049). The average blood loss was 75.3cc in the randomized cohort vs. 63.2cc in the observational, p=0.13. Only 6 patients total required intra-operative transfusions. There were no perioperative mortalities. The most common surgical complication was dural tear (combined 3% of cases). Re-operation occurred in a combined 11% of cases by 5 years, 12% by 6 years, 14% by 7 years, and 15% by 8 years post-surgery. The rates of reoperation were not significantly different between the randomized and observational cohorts. Eighty-seven of the 119 re-operations noted the type of re-operation; approximately 85% of these (74/87) were listed as recurrent herniations at the same level. One death occurred within 90 days post-surgery related to heart surgery at another institution; the death was judged to be unrelated and was reported to the Institutional Review Board and the Data and Safety Monitoring Board.
Cross-Over
Non-adherence to treatment assignment affected both treatment arms: patients chose to delay or decline surgery in the surgical arm and crossed over to surgery in the non-operative arm. (Figure 1) Statistically significant differences of patients crossing over to non-operative care within 8 years of enrollment were that they were older, had higher incomes, less dissatisfaction with their symptoms, more likely to have a disc herniation at an upper lumbar level, more likely to express a baseline preference for non-operative care, less likely to perceive their symptoms as getting worse at baseline, and had less baseline pain and disability (Table 3). Patients crossing over to surgery within 8 years were more dissatisfied with their symptoms at baseline; were more likely to perceive they were getting worse at baseline; more likely to express a baseline preference for surgery; and had worse baseline physical function and more self-rated disability.
Table 3: Statistically significant predictors of adherence to treatment among RCT patients.
Main Treatment Effects
Intent-to-Treat Analysis In the intention-to-treat analysis of the randomized cohort, all measures over 8 years favored surgery but there were no statistically significant treatment effects in the primary outcome measures (Table 4 and Figure 2). In the overall intention-to-treat comparison between the two treatment groups over time (area-under the curve), secondary outcomes were significantly greater with surgery in the intention-to-treat analysis (sciatica bothersomeness (p=0.005), satisfaction with symptoms (p=0.013), and self-rated improvement (p=0.013)) (Figure 3) Improvement in sciatica bothersomeness index was also statistically significant in favor of surgery at most individual time point comparisons (although non-significant in years 6 and 7) (Table 4).
Figure 2: Primary outcomes (SF-36 Bodily Pain and Physical Function, and Oswestry Disability Index) in the randomized and observational cohorts during 8 years of follow-up.
Figure 3: secondary outcomes (Sciatica Bothersomeness, Satisfaction with Symptoms, and Self-rated Global Improvement) in the randomized and observational cohorts during 8 years of follow-up.
Table 4: Primary analysis results for years 1 to 8. Intent-to-treat for the randomized cohort and adjusted* analyses according to treatment received for the randomized and observational cohorts combined.
As-Treated Analysis The adjusted as-treated effects seen in the randomized and observational were similar. Accordingly, the cohorts were combined for the final analyses. Treatment effects for the primary outcomes in the combined as-treated analysis were clinically meaningful and statistically significant out to 8 years: SF-36 BP 10.9 p < 0.001 (95% CI 7.7 to 14); SF-36 PF 10.6 p<0.001 (95% CI 7.7 to 13.5); ODI ?11.3 p<0.001 (95% CI ?13.6 to ?9.1) (Table 4). The footnote for Table 4 describes the adjusting covariates selected for the final model.
Results from the intent-to-treat and as-treated analyses of the two cohorts are compared in Figure 2. In the combined analysis, treatment effects were statistically significant in favor of surgery for all primary and secondary outcome measures (with the exception of work status which did not differ between treatment groups) at each time point (Table 4 and Figure 3).
Loss-to-Follow-Up
At the 8-year follow-up, 63% of initial enrollees supplied data, with losses due to dropouts, missed visits, or deaths. Table 5 summarized the baseline characteristics of those lost to follow-up compared to those retained in the study at 8-years. Those who remained in the study at 8 years were – somewhat older; more likely to be female, white, college educated, and working at baseline; less likely to be disabled, receiving compensation, or a smoker; less symptomatic at baseline with somewhat less bodily pain, better physical function, less disability on the ODI, better mental health, and less sciatica bothersomeness. These differences were small but statistically significant. Table 6 summarizes the short-term outcomes during the first 2 years for those retained in the study at 8 years compared to those lost to follow-up. Those lost to follow-up had worse outcomes on average; however this was true in both the surgical and non-operative groups with non-significant differences in treatment effects. The long-term outcomes are therefore likely to be somewhat over-optimistic on average in both groups, but the comparison between surgical and non-operative outcomes appear likely to be un-biased despite the long-term loss to follow-up.
Table 5: Patient baseline demographic characteristics, comorbidities, and health status measures according to patient follow-up status as of 02/01/2013 when the IDH8yr data were pulled.
Table 6: Time-weighted average of treatment effects at 2 years (AUC) from adjusted* as-treated randomized and observational cohorts combined primary outcome analysis, according to treatment received and patient follow-up status.
Discussion
In patients with a herniated disc confirmed by imaging and leg symptoms persisting for at least 6 weeks, surgery was superior to non-operative treatment in relieving symptoms and improving function. In the as-treated analysis, the treatment effect for surgery was seen as early as 6 weeks, appeared to reach a maximum by 6 months and persisted over 8 years; it is notable that the non-operative group also improved significantly and this improvement persisted with little to no degradation of outcomes in either group (operative and non-operative) between 4 and 8 years. In the longitudinal intention-to-treat analysis, all the outcomes showed small advantages for surgery, but only the secondary outcomes of sciatica bothersomeness, satisfaction with symptoms, and self-rated improvement were statistically significant. The persistent small benefit in the surgery group over time has made the overall intention-to-treat comparison more statistically significant over time despite high levels of cross-over. The large effects seen in the as-treated analysis after adjustments for characteristics of the crossover patients suggest that the intent-to-treat analysis may underestimate the true effect of surgery since the mixing of treatments due to crossover can be expected to create a bias toward the null in the intent-to-treat analyses.[4,19] Loss to follow-up among patients who were somewhat worse at baseline and with worse short-term outcomes probably leads to overly-optimistic estimated long-term outcomes in both surgery and non-operative groups but unbiased estimates of surgical treatment effects.
Comparisons to Other Studies
There are no other long-term randomized studies reporting the same primary outcome measures as SPORT. The results of SPORT primary outcomes at 2 years were quite similar to those of Peul et al but longer follow up for the Peul study is necessary for further comparison.[4,20] In contrast to the Weber study, the differences in the outcomes in SPORT between treatment groups remained relatively constant between 1 and 8 years of follow-up. One of the factors in this difference may be the sensitivity of the outcome measures � for example, sciatica bothersomeness, which was significantly different out to 8 years in the intention-to-treat, may be a more sensitive marker of treatment success than the general outcome measure used by Weber et al.[2]
The long-term results of SPORT are similar to the Maine Lumbar Spine Study (MLSS).[21] The MLSS reported statistically significantly greater improvements at 10 years in sciatica bothersomeness for the surgery group (?11.9) compared to the nonsurgical groups (?5.8) with a treatment effect of ?6.1 p=0.004; in SPORT the improvement in sciatica bothersomeness in the surgical group at 8 years was similar to the 10 year result in MLSS (?11) though the non-operative cohort in SPORT did better than their MLSS counterparts (?9.1) however the treatment effect in SPORT, while smaller, remained statistically significant (?1.5; p<0.001) due to the much larger sample size. Greater improvements in the non-operative cohorts between SPORT and MLSS may be related to differences in non-operative treatments over time, differences between the two cohorts since the MLSS and did not require imaging confirmation of IDH.
Over the 8 years there was little evidence of harm from either treatment. The 8-year rate of re-operation was 14.7%, which is lower than the 25% reported by MLSS at 10 years.[22]
Limitations
Although our results are adjusted for characteristics of cross over patients and control for important baseline covariates, the as-treated analyses presented do not share the strong protection from confounding that exists for an intent-to-treat analysis.[4�6] However, However, intent-to-treat analyses are known to be biased in the presence of noncompliance at the level observed in SPORT, and our adjusted as-treated analyses have been shown to produce accurate results under reasonable assumptions about the dependence of compliance on longitudinal outcomes.[23] Another potential limitation is the heterogeneity, of the non-operative treatment interventions, as discussed in our prior papers.[5,6,8] Finally, attrition in this long-term follow-up study meant that only 63% of initial enrollees supplied data at 8 years with losses due to dropouts, missed visits, or deaths; based on analyses at baseline and at short-term follow-up, this likely leads to somewhat overly-optimistic estimated long-term outcomes in both treatment groups but an unbiased estimation of surgical treatment effect.
Conclusions
In the intention-to-treat analysis, small, statistically insignificant surgical treatment effects were seen for the primary outcomes but statistically significant advantages for sciatica bothersomeness, satisfaction with symptoms, and self-rated improvement were seen out to 8 years despite high levels of treatment cross-over. The as-treated analysis combining the randomized and observational cohorts, which carefully controlled for potentially confounding baseline factors, showed significantly greater improvement in pain, function, satisfaction, and self-rated progress over 8 years compared to patients treated non-operatively. The non-operative group, however, also showed substantial improvements over time, with 54% reporting being satisfied with their symptoms and 73% satisfied with their care after 8 years.
Acknowledgments
The National Institute of Arthritis and Musculoskeletal and Skin Diseases (U01-AR45444; P60-AR062799) and the Office of Research on Women�s Health, the National Institutes of Health, and the National Institute of Occupational Safety and Health, the Centers for Disease Control and Prevention grant funds were received in support of this work. Relevant financial activities outside the submitted work: consultancy, grants, stocks.
This study is dedicated to the memories of Brieanna Weinstein and Harry Herkowitz, leaders in their own rights, who simply made the world a better place.
In conclusion, individuals who suffer from migraine pain require the most effective type of treatment in order to help improve as well as manage their symptoms, particularly if their migraines were elicited from a lumbar herniated disc. The purpose of the following articles was to associate the two conditions with each other and demonstrate the results of the research above. Various treatment options can be considered before surgery for migraine pain and lumbar herniated disc treatment. Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Neck Pain
Neck pain is a common complaint which can result due to a variety of injuries and/or conditions. According to statistics, automobile accident injuries and whiplash injuries are some of the most prevalent causes for neck pain among the general population. During an auto accident, the sudden impact from the incident can cause the head and neck to jolt abruptly back-and-forth in any direction, damaging the complex structures surrounding the cervical spine. Trauma to the tendons and ligaments, as well as that of other tissues in the neck, can cause neck pain and radiating symptoms throughout the human body.
1. Lyngberg AC, Rasmussen BK, J�rgensen T, Jensen R. Has the prevalence of migraine and tension-type headache changed over a 12-year period? a Danish population survey. Eur J Epidemiol. 2005;20:243�9. doi: 10.1007/s10654-004-6519-2. [PubMed][Cross Ref]
2. Vos T, Flaxman A, Naghavi M. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990�2010: a systematic analysis for the global burden of disease study 2010. Lancet. 2012;380:2163�96. doi: 10.1016/S0140-6736(12)61729-2. [PubMed][Cross Ref]
3. Burch RC, Loder S, Loder E, Smitherman TA. The prevalence and burden of migraine and severe headache in the united states: updated statistics from government health surveillance studies. Headache. 2015;55:21�34. doi: 10.1111/head.12482. [PubMed][Cross Ref]
4. Lanteri-Minet M. Economic burden and costs of chronic migraine. Curr Pain Headache Rep. 2014;18:385. doi: 10.1007/s11916-013-0385-0. [PubMed][Cross Ref]
5. Bloudek L, Stokes M, Buse D, Wilcox T, Lipton R, Goadsby P, Varon S, Blumenfeld A, Katsarava Z, Pascual J, et al. Cost of healthcare for patients with migraine in five European countries: results from the international burden of migraine study (IBMS) J Headache Pain. 2012;13:361�78. doi: 10.1007/s10194-012-0460-7. [PMC free article][PubMed][Cross Ref]
6. Antonaci F, Nappi G, Galli F, Manzoni GC, Calabresi P, Costa A. Migraine and psychiatric comorbidity: a review of clinical findings. J Headache Pain. 2011;12:115�25. doi: 10.1007/s10194-010-0282-4. [PMC free article][PubMed][Cross Ref]
7. Kurth T, Chabriat H, Bousser M-G. Migraine and stroke: a complex association with clinical implications. Lancet Neurol. 2012;11:92�100. doi: 10.1016/S1474-4422(11)70266-6. [PubMed][Cross Ref]
8. Lipton R, Goadsby P, Sawyer J, Blakeborough P, Stewart W. Migraine: diagnosis and assessment of disability. Rev Contemp Pharmaco. 2000;11:63�73.
9. Diamond S, Bigal ME, Silberstein S, Loder E, Reed M, Lipton RB. Patterns of diagnosis and acute and preventive treatment for migraine in the united states: results from the American migraine prevalence and prevention study. Headache. 2007;47:355�63. [PubMed]
10. Lipton RB, Bigal ME, Diamond M, Freitag F, Reed M, Stewart WF. Migraine prevalence, disease burden, and the need for preventive therapy. Neurology. 2007;68:343�9. doi: 10.1212/01.wnl.0000252808.97649.21. [PubMed][Cross Ref]
11. Berger A, Bloudek LM, Varon SF, Oster G. Adherence with migraine prophylaxis in clinical practice. Pain Pract. 2012;12:541�9. doi: 10.1111/j.1533-2500.2012.00530.x. [PubMed][Cross Ref]
12. Peres MFP, Silberstein S, Moreira F, Corchs F, Vieira DS, Abraham N, Gebeline-Myers C. Patients’ preference for migraine preventive therapy. Headache. 2007;47:540�5. doi: 10.1111/j.1526-4610.2007.00757.x. [PubMed][Cross Ref]
13. Nicholson RA, Rooney M, Vo K, O’Laughlin E, Gordon M. Migraine care among different ethnicities: Do disparities exist? Headache. 2006;46:754�65. doi: 10.1111/j.1526-4610.2006.00453.x. [PMC free article][PubMed][Cross Ref]
14. Lafata JE, Tunceli O, Cerghet M, Sharma KP, Lipton RB. The use of migraine preventive medications among patients with and without migraine headaches. Cephalalgia. 2010;30:97�104. doi: 10.1111/j.1468-2982.2009.01909.x. [PubMed][Cross Ref]
15. Cevoli S, D’Amico D, Martelletti P, Valguarnera F, Del Bene E, De Simone R, Sarchielli P, Narbone MC, Testa L, Genco S, et al. Underdiagnosis and undertreatment of migraine in Italy: a survey of patients attending for the first time 10 headache centres. Cephalalgia. 2009;29:1285�93. doi: 10.1111/j.1468-2982.2009.01874.x. [PubMed][Cross Ref]
16. Stark RJ, Valenti L, Miller GC. Management of migraine in Australian general practice. Med J Aust. 2007;187:142. [PubMed]
17. Lipton RB, Buse DC, Serrano D, Holland S, Reed ML. Examination of unmet treatment needs among persons with episodic migraine: results of the American migraine prevalence and prevention (AMPP) study. Headache. 2013;53:1300�11. doi: 10.1111/head.12154. [PubMed][Cross Ref]
19. Bigal ME, Serrano D, Reed M, Lipton RB. Chronic migraine in the population Burden, diagnosis, and satisfaction with treatment. Neurology. 2008;71:559�66. doi: 10.1212/01.wnl.0000323925.29520.e7. [PubMed][Cross Ref]
20. Kristoffersen ES, Grande RB, Aaseth K, Lundqvist C, Russell MB. Management of primary chronic headache in the general population: the Akershus study of chronic headache. J Headache Pain. 2012;13:113�20. doi: 10.1007/s10194-011-0391-8. [PMC free article][PubMed][Cross Ref]
21. Sanderson JC, Devine EB, Lipton RB, Bloudek LM, Varon SF, Blumenfeld AM, Goadsby PJ, Buse DC, Sullivan SD. Headache-related health resource utilisation in chronic and episodic migraine across six countries. J Neurol Neurosurg Psychiatry. 2013;84:1309�17. doi: 10.1136/jnnp-2013-305197. [PMC free article][PubMed][Cross Ref]
23. Marcus D, Scharff L, Mercer S, Turk D. Nonpharmacological treatment for migraine: incremental utility of physical therapy with relaxation and thermal biofeedback. Cephalalgia. 1998;18:266�72. doi: 10.1046/j.1468-2982.1998.1805266.x. [PubMed][Cross Ref]
24. Lawler SP, Cameron LD. A randomized, controlled trial of massage therapy as a treatment for migraine. Ann Behav Med. 2006;32:50�9. doi: 10.1207/s15324796abm3201_6. [PubMed][Cross Ref]
25. Tuchin PJ, Pollard H, Bonello R. A randomized controlled trial of chiropractic spinal manipulative therapy for migraine. J Manipulative Physiol Ther. 2000;23:91�5. doi: 10.1016/S0161-4754(00)90073-3. [PubMed][Cross Ref]
26. Hoyt W, Shaffer F, Bard D, Benesler J, Blankenhorn G, Gray J, Hartman W, Hughes L. Osteopathic manipulation in the treatment of muscle-contraction headache. J Am Osteopath Assoc. 1979;78:322�5. [PubMed]
27. Jull G, Trott P, Potter H, Zito G, Niere K, Shirley D, Emberson J, Marschner I, Richardson C. A randomized controlled trial of exercise and manipulative therapy for cervicogenic headache. Spine (Phila Pa 1976) 2002;27:1835�43. doi: 10.1097/00007632-200209010-00004. [PubMed][Cross Ref]
28. Haas M, Spegman A, Peterson D, Aickin M, Vavrek D. Dose-Response and Efficacy of Spinal Manipulation for Chronic Cervicogenic Headache: A Pilot Randomized Controlled Trial. Spine J. 2010;10:117�28. [PMC free article][PubMed]
29. Bove G, Nilsson N. Spinal manipulation in the treatment of episodic tension-type headache: a randomized controlled trial. JAMA. 1998;280:1576�9. doi: 10.1001/jama.280.18.1576. [PubMed][Cross Ref]
30. Parker GB, Pryor DS, Tupling H. Why does migraine improve during a clinical trial? Further results from a trial of cervical manipulation for migraine. Aust N Z J Med. 1980;10:192�8. doi: 10.1111/j.1445-5994.1980.tb03712.x. [PubMed][Cross Ref]
31. Hsieh LL-C, Liou H-H, Lee L-H, Chen TH-H, Yen AM-F. Effect of acupressure and trigger points in treating headache: a randomized controlled trial. Am J Chin Med. 2010;38:1�14. doi: 10.1142/S0192415X10007634. [PubMed][Cross Ref]
32. Boline P, Kassack K, Bronfort G, Nelson C, Anderson A. Spinal manipulation vs. amitriptyline for the treatment of chronic tension-type headaches: a randomized clinical trial. J Manipulative Physiol Ther. 1995;18:148�54. [PubMed]
33. Nelson CF, Bronfort G, Evans R, Boline P, Goldsmith C, Anderson AV. The efficacy of spinal manipulation, amitriptyline and the combination of both therapies for the prophylaxis of migraine headache. J Manipulative Physiol Ther. 1998;21:511�9. [PubMed]
34. Castien RF, Windt DA, Grooten A, Dekker J. Effectiveness of manual therapy for chronic tension-type headache: a pragmatic, randomised, clinical trial. Cephalalgia. 2011;31:133�43. doi: 10.1177/0333102410377362. [PubMed][Cross Ref]
35. Chaibi A, Tuchin P, Russell M. Manual therapies for migraine: a systematic review. J Headache Pain. 2011;12:127�33. doi: 10.1007/s10194-011-0296-6. [PMC free article][PubMed][Cross Ref]
36. Posadzki P, Ernst E. Spinal manipulations for the treatment of migraine: a systematic review of randomized clinical trials. Cephalalgia. 2011;31:964�70. doi: 10.1177/0333102411405226. [PubMed][Cross Ref]
37. Posadzki P, Ernst E. Spinal manipulations for tension-type headaches: a systematic review of randomized controlled trials. Complement Ther Med. 2012;20:232�9. doi: 10.1016/j.ctim.2011.12.001. [PubMed][Cross Ref]
38. Racicki S, Gerwin S, DiClaudio S, Reinmann S, Donaldson M. Conservative physical therapy management for the treatment of cervicogenic headache: a systematic review. J Man Manip Ther. 2013;21:113�24. doi: 10.1179/2042618612Y.0000000025. [PMC free article][PubMed][Cross Ref]
39. Chaibi A, Russell MB. Manual therapies for cervicogenic headache: a systematic review. J Headache Pain. 2012;13:351�9. doi: 10.1007/s10194-012-0436-7. [PMC free article][PubMed][Cross Ref]
40. Chaibi A, Russell MB. Manual therapies for primary chronic headaches: a systematic review of randomized controlled trials. J Headache Pain. 2014;15:67. doi: 10.1186/1129-2377-15-67. [PMC free article][PubMed][Cross Ref]
41. Mesa-Jim�nez JA, Lozano-L�pez C, Angulo-D�az-Parre�o S, Rodr�guez-Fern�ndez �L, De-la-Hoz-Aizpurua JL, Fern�ndez-de-las-Pe�as C. Multimodal manual therapy vs. pharmacological care for management of tension type headache: A meta-analysis of randomized trials. Cephalalgia. 2015;35:1323�32. doi: 10.1177/0333102415576226. [PubMed][Cross Ref]
42. Loney PL, Chambers LW, Bennett KJ, Roberts JG, Stratford PW. Critical appraisal of the health research literature prevalence or incidence of a health problem. Chronic Dis Inj Can. 1998;19:170. [PubMed]
43. Fejer R, Kyvik KO, Hartvigsen J. The Prevalence of neck pain in the world population: a systematic critical review of the literature. Eur Spine. 2006;15:834�48. doi: 10.1007/s00586-004-0864-4. [PMC free article][PubMed][Cross Ref]
44. Bishop F, Prescott P, Chan Y, Saville J, von Elm E, Lewith G. Complementary medicine use by men with prostate cancer: a systematic review of prevalence studies. Prostate Cancer Prostatic Dis. 2011;14:1�13. doi: 10.1038/pcan.2010.38. [PubMed][Cross Ref]
45. Adams J, Barbery G, Lui C-W. Complementary and alternative medicine use for headache and migraine: a critical review of the literature. Headache. 2013;53:459�73. doi: 10.1111/j.1526-4610.2012.02271.x. [PubMed][Cross Ref]
46. Adams J, Chi-Wai L, Sibbritt D, Broom A, Wardle J, Homer C. Attitudes and referral practices of maternity care professionals with regard to complementary and alternative medicine: an integrative review. J Adv Nurs. 2011;67:472�83. doi: 10.1111/j.1365-2648.2010.05510.x. [PubMed][Cross Ref]
47. Solomon D, Adams J. The use of complementary and alternative medicine in adults with depressive disorders. A critical integrative review. J Affect Disord. 2015;179:101�13. doi: 10.1016/j.jad.2015.03.031. [PubMed][Cross Ref]
48. Vukovi? V, Plavec D, Lovrenci? Huzjan A, Budisi? M, Demarin V. Treatment of migraine and tension-type headache in Croatia. J Headache Pain. 2010;11:227�34. doi: 10.1007/s10194-010-0200-9. [PMC free article][PubMed][Cross Ref]
49. Cooke LJ, Becker WJ. Migraine prevalence, treatment and impact: the canadian women and migraine study. Can J Neurol Sci. 2010;37:580�7. doi: 10.1017/S0317167100010738. [PubMed][Cross Ref]
50. Wells RE, Bertisch SM, Buettner C, Phillips RS, McCarthy EP. Complementary and alternative medicine use among adults with migraines/severe headaches. Headache. 2011;51:1087�97. doi: 10.1111/j.1526-4610.2011.01917.x. [PMC free article][PubMed][Cross Ref]
51. Wells RE, Phillips RS, Schachter SC, McCarthy EP. Complementary and alternative medicine use among US adults with common neurological conditions. J Neurol. 2010;257:1822�31. doi: 10.1007/s00415-010-5616-2. [PMC free article][PubMed][Cross Ref]
52. Lyngberg AC, Rasmussen BK, J�rgensen T, Jensen R. Secular changes in health care utilization and work absence for migraine and tension-type headache: a population based study. Eur J Epidemiol. 2005;20:1007�14. doi: 10.1007/s10654-005-3778-5. [PubMed][Cross Ref]
53. Rossi P, Di Lorenzo G, Malpezzi MG, Faroni J, Cesarino F, Di Lorenzo C, Nappi G. Prevalence, pattern and predictors of use of complementary and alternative medicine (CAM) in migraine patients attending a headache clinic in Italy. Cephalalgia. 2005;25:493�506. doi: 10.1111/j.1468-2982.2005.00898.x. [PubMed][Cross Ref]
54. Minen MT, Seng EK, Holroyd KA. Influence of family psychiatric and headache history on migraine-related health care utilization. Headache. 2014;54:485�92. doi: 10.1111/head.12300. [PubMed][Cross Ref]
55. Xue C, Zhang A, Lin V, Myers R, Polus B, Story D. Acupuncture, chiropractic and osteopathy use in Australia: a national population survey. BMC Public Health. 2008;8:105. doi: 10.1186/1471-2458-8-105. [PMC free article][PubMed][Cross Ref]
56. Gaumer G. Factors associated with patient satisfaction with chiropractic care: survey and review of the literature. J Manipulative Physiol Ther. 2006;29:455�62. doi: 10.1016/j.jmpt.2006.06.013. [PubMed][Cross Ref]
57. Ndetan HT, Bae S, Evans MW, Jr, Rupert RL, Singh KP. Characterization of health status and modifiable risk behavior among United States adults using chiropractic care as compared with general medical care. J Manipulative Physiol Ther. 2009;32:414�22. doi: 10.1016/j.jmpt.2009.06.012. [PubMed][Cross Ref]
58. Rossi P, Di Lorenzo G, Faroni J, Malpezzi MG, Cesarino F, Nappi G. Use of complementary and alternative medicine by patients with chronic tension-type headache: results of a headache clinic survey. Headache. 2006;46:622�31. doi: 10.1111/j.1526-4610.2006.00412.x. [PubMed][Cross Ref]
59. Rossi P, Torelli P, Di Lorenzo C, Sances G, Manzoni GC, Tassorelli C, Nappi G. Use of complementary and alternative medicine by patients with cluster headache: results of a multi-centre headache clinic survey. Complement Ther Med. 2008;16:220�7. doi: 10.1016/j.ctim.2007.05.002. [PubMed][Cross Ref]
60. Ossendorf A, Schulte E, Hermann K, Hagmeister H, Schenk M, Kopf A, Schuh-Hofer S, Willich SN, Bergh�fer A. Use of complementary medicine in patients with chronic pain. Eur J Integrative Med. 2009;1:93�8. doi: 10.1016/j.eujim.2009.05.002. [Cross Ref]
61. Brown BT, Bonello R, Fernandez-Caamano R, Eaton S, Graham PL, Green H. Consumer characteristics and perceptions of chiropractic and chiropractic services in Australia: results from a cross-sectional survey. J Manipulative Physiol Ther. 2014;37:219�29. doi: 10.1016/j.jmpt.2014.01.001. [PubMed][Cross Ref]
62. Cherkin DC, Deyo RA, Sherman KJ, Hart LG, Street JH, Hrbek A, Davis RB, Cramer E, Milliman B, Booker J, et al. Characteristics of visits to licensed acupuncturists, chiropractors, massage therapists, and naturopathic physicians. J Am Board Fam Med. 2002;15:463�72. [PubMed]
63. Jackson P. Summary of the 2000 ACA professional survey on chiropractic practice. J Am Chiro Assn. 2001;38:27�30.
64. French S, Charity M, Forsdike K, Gunn J, Polus B, Walker B. Chiropractic Observation and Analysis Study (COAST): providing an understanding of current chiropractic practice. Med J Aust. 2013;10:687�91. [PubMed]
65. Ailliet L, Rubinstein SM, de Vet HCW. Characteristics of chiropractors and their patients in Belgium. J Manipulative Physiol Ther. 2010;33:618�25. doi: 10.1016/j.jmpt.2010.08.011. [PubMed][Cross Ref]
66. Coulter I, Hurwitz E, Adams A, Genovese B, Hays R, Shekelle P. Patients using chiropractors in North America: who are they, and why are they in chiropractic care? Spine (Phila Pa 1976) 2002;27:291�8. doi: 10.1097/00007632-200202010-00018. [PubMed][Cross Ref]
67. Rubinstein S, Pfeifle CE, van Tulder MW, Assendelft WJJ. Chiropractic patients in the Netherlands: A descriptive study. J Manipulative Physiol Ther. 2000;23:557�63. doi: 10.1067/mmt.2000.109675. [PubMed][Cross Ref]
68. Hartvigsen J, Bolding-Jensen O, Hviid H, Grunnet-Nilsson N. Danish chiropractic patients then and now�a comparison between 1962 and 1999. J Manipulative Physiol Ther. 2003;26:65�9. doi: 10.1067/mmt.2003.14. [PubMed][Cross Ref]
69. Brown B, Bonello R, Fernandez-Caamano R, Graham P, Eaton S, Green H. Chiropractic in Australia : a survey of the general public. Chiropractic J Aust. 2013;43:85�92.
70. Gaul C, Eismann R, Schmidt T, May A, Leinisch E, Wieser T, Evers S, Henkel K, Franz G, Zierz S. Use of complementary and alternative medicine in patients suffering from primary headache disorders. Cephalalgia. 2009;29:1069�78. doi: 10.1111/j.1468-2982.2009.01841.x. [PubMed][Cross Ref]
71. Malone CD, Bhowmick A, Wachholtz AB. Migraine: treatments, comorbidities, and quality of life, in the USA. J Pain Res. 2015;8:537�47. doi: 10.2147/JPR.S88207. [PMC free article][PubMed][Cross Ref]
72. Gaul C, Schmidt T, Czaja E, Eismann R, Zierz S. Attitudes towards complementary and alternative medicine in chronic pain syndromes: a questionnaire-based comparison between primary headache and low back pain. BMC Complement Altern Med. 2011;11:1�8. doi: 10.1186/1472-6882-11-89. [PMC free article][PubMed][Cross Ref]
73. Karakurum Goksel B, Coskun O, Ucler S, Karatas M, Ozge A, Ozkan S. Use of complementary and alternative medicine by a sample of Turkish primary headache patients. Agri Dergisi. 2014;26:1�7. [PubMed]
74. Morin C, Aubin A. Primary reasons for osteopathic consultation: a prospective survey in quebec. PLoS One. 2014;9:e106259. doi: 10.1371/journal.pone.0106259. [PMC free article][PubMed][Cross Ref]
75. Orrock PJ. Profile of members of the Australian osteopathic association: part 2 � the patients. Int J Osteopath Med. 2009;12:128�39. doi: 10.1016/j.ijosm.2009.06.001. [Cross Ref]
76. Bethell C, Kemper KJ, Gombojav N, Koch TK. Complementary and conventional medicine use among youth with recurrent headaches. Pediatrics. 2013;132:e1173�e83. doi: 10.1542/peds.2013-1816. [PMC free article][PubMed][Cross Ref]
77. Lambert TD, Morrison KE, Edwards J, Clarke CE. The use of complementary and alternative medicine by patients attending a UK headache clinic. Complement Ther Med. 2010;18:128�34. doi: 10.1016/j.ctim.2010.05.035. [PubMed][Cross Ref]
78. von Peter S, Ting W, Scrivani S, Korkin E, Okvat H, Gross M, Oz C, Balmaceda C. Survey on the use of complementary and alternative medicine among patients with headache syndromes. Cephalalgia. 2002;22:395�400. doi: 10.1046/j.1468-2982.2002.00376.x. [PubMed][Cross Ref]
79. Kristoffersen ES, Aaseth K, Grande RB, Lundqvist C, Russell MB. Self-reported efficacy of complementary and alternative medicine: the Akershus study of chronic headache. J Headache Pain. 2013;13:113�20. doi: 10.1007/s10194-011-0391-8. [PMC free article][PubMed][Cross Ref]
80. Sobri M, Lamont A, Alias N, Win M. Red flags in patients presenting with headache: clinical indications for neuroimaging. Br J Radiol. 2014;76(908):532�35. [PubMed]
81. Carville S, Padhi S, Reason T, Underwood M, Group GD. Diagnosis and management of headaches in young people and adults: summary of NICE guidance. BMJ. 2012;345:e5765. doi: 10.1136/bmj.e5765. [PubMed][Cross Ref]
82. Puentedura EJ, March J, Anders J, Perez A, Landers MR, Wallmann HW, Cleland JA. Safety of cervical spine manipulation: are adverse events preventable and are manipulations being performed appropriately? a review of 134 case reports. J Man Manip Ther. 2012;20:66�74. doi: 10.1179/2042618611Y.0000000022. [PMC free article][PubMed][Cross Ref]
83. Becker C, Brobert GP, Almqvist PM, Johansson S, Jick SS, Meier CR. Migraine incidence, comorbidity and health resource utilization in the UK. Cephalalgia (Wiley-Blackwell) 2008;28:57�64. doi: 10.1111/j.1468-2982.2007.01469.x. [PubMed][Cross Ref]
84. Brandes JL. Global trends in migraine care: results from the MAZE survey. CNS Drugs. 2002;16:13�8. doi: 10.2165/00023210-200216001-00003. [PubMed][Cross Ref]
85. Radtke A, Neuhauser H. Prevalence and burden of headache and migraine in Germany. Headache. 2009;49:79�89. doi: 10.1111/j.1526-4610.2008.01263.x. [PubMed][Cross Ref]
86. Zeeberg P, Olesen J, Jensen R. Efficacy of multidisciplinary treatment in a tertiary referral headache centre. Cephalalgia (Wiley-Blackwell) 2005;25:1159�67. doi: 10.1111/j.1468-2982.2005.00980.x. [PubMed][Cross Ref]
87. Wallasch T-M, Angeli A, Kropp P. Outcomes of a headache-specific cross-sectional multidisciplinary treatment program. Headache. 2012;52:1094�105. doi: 10.1111/j.1526-4610.2012.02189.x. [PubMed][Cross Ref]
88. Wallasch T-M, Hermann C. Validation of criterion-based patient assignment and treatment effectiveness of a multidisciplinary modularized managed care program for headache. J Headache Pain. 2012;13:379�87. doi: 10.1007/s10194-012-0453-6. [PMC free article][PubMed][Cross Ref]
89. Gaul C, Visscher CM, Bhola R, Sorbi MJ, Galli F, Rasmussen AV, Jensen R. Team players against headache: multidisciplinary treatment of primary headaches and medication overuse headache. J Headache Pain. 2011;12:511�9. doi: 10.1007/s10194-011-0364-y. [PMC free article][PubMed][Cross Ref]
Close Accordion
Blank
References
1. Dartmouth Atlas Working Group. Dartmouth Atlas of Musculoskeletal Health Care. Chicago, IL: American Hospital Association Press; 2000.
2. Weber H. Lumbar disc herniation. A controlled, prospective study with ten years of observation. Spine. 1983;8:131�40. [PubMed]
3. Atlas SJ, Deyo RA, Keller RB, et al. The Maine Lumbar Spine Study, Part II. 1-year outcomes of surgical and nonsurgical management of sciatica. Spine. 1996;21:1777�86. [PubMed]
4. Peul WC, van Houwelingen HC, van den Hout WB, et al. Surgery versus prolonged conservative treatment for sciatica. N Engl J Med. 2007;356:2245�56. [PubMed]
5. Weinstein JN, Lurie JD, Tosteson TD, et al. Surgical vs nonoperative treatment for lumbar disk herniation: the Spine Patient Outcomes Research Trial (SPORT) observational cohort. Jama. 2006;296:2451�9. [PMC free article][PubMed]
6. Weinstein JN, Tosteson TD, Lurie JD, et al. Surgical vs nonoperative treatment for lumbar disk herniation: the Spine Patient Outcomes Research Trial (SPORT): a randomized trial. Jama. 2006;296:2441�50. [PMC free article][PubMed]
7. Birkmeyer NJ, Weinstein JN, Tosteson AN, et al. Design of the Spine Patient outcomes Research Trial (SPORT) Spine. 2002;27:1361�72. [PMC free article][PubMed]
8. Weinstein JN, Lurie JD, Tosteson TD, et al. Surgical versus nonoperative treatment for lumbar disc herniation: four-year results for the Spine Patient Outcomes Research Trial (SPORT) Spine (Phila Pa 1976) 2008;33:2789�800. [PMC free article][PubMed]
9. Delamarter R, McCullough J. Microdiscectomy & Microsurgical Laminotomies. In: Frymoyer J, editor. The Adult Spine: Principles and Practice. 2. Philadelphia: Lippincott-Raven Publishers; 1996.
10. McHorney CA, Ware JE, Jr, Lu JF, et al. The MOS 36-item Short-Form Health Survey (SF-36): III. Tests of data quality, scaling assumptions, and reliability across diverse patient groups. Med Care. 1994;32:40�66. [PubMed]
11. Daltroy LH, Cats-Baril WL, Katz JN, et al. The North American Spine Society lumbar spine outcome assessment Instrument: reliability and validity tests. Spine. 1996;21:741�9. [PubMed]
12. Deyo RA, Diehl AK. Patient satisfaction with medical care for low-back pain. Spine. 1986;11:28�30. [PubMed]
13. Atlas SJ, Deyo RA, Patrick DL, et al. The Quebec Task Force classification for Spinal Disorders and the severity, treatment, and outcomes of sciatica and lumbar spinal stenosis. Spine. 1996;21:2885�92. [PubMed]
14. Patrick DL, Deyo RA, Atlas SJ, et al. Assessing health-related quality of life in patients with sciatica. Spine. 1995;20:1899�908. discussion 909. [PubMed]
15. Fitzmaurice G, Laird N, Ware J. Applied Longitudinal Analysis. Philadelphia, PA: John Wiley & Sons; 2004.
16. Diggle PJ, Liang K-Y, Zeger SL. Analysis of Longitudinal Data. Oxford, England, UK: Oxford University Press; 1994.
17. Kaplan EL, Meier P. Nonparametric estimation from incomplete observations. Journal of the American Statistical Association. 1958;53:457�81.
18. Peto R, Peto J. Asymptotically Efficient Rank Invariant Test Procedures. Journal of the Royal Statistical Society Series a-General. 1972;135:185.
19. Meinert CL. Clinical Trials: Design, Conduct, and Analysis. New York, NY: Oxford University Press, Inc; 1986.
20. Peul WC, van den Hout WB, Brand R, et al. Prolonged conservative care versus early surgery in patients with sciatica caused by lumbar disc herniation: two year results of a randomised controlled trial. Bmj. 2008;336:1355�8. [PMC free article][PubMed]
21. Atlas SJ, Keller RB, Chang Y, et al. Surgical and nonsurgical management of sciatica secondary to a lumbar disc herniation: five-year outcomes from the Maine Lumbar Spine Study. Spine. 2001;26:1179�87. [PubMed]
22. Atlas SJ, Keller RB, Wu YA, et al. Long-term outcomes of surgical and nonsurgical management of sciatica secondary to a lumbar disc herniation: 10 year results from the maine lumbar spine study. Spine. 2005;30:927�35. [PubMed]
23. Sitlani CM, Heagerty PJ, Blood EA, et al. Longitudinal structural mixed models for the analysis of surgical trials with noncompliance. Statistics in medicine. 2012;31:1738�60. [PMC free article][PubMed]
A herniated disc can lead to pain as well as disrupt your daily activities, as you likely know. That is probably what brings you to the office of the doctor: You have back pain or neck pain, and you’d love to understand why.
Your doctor will ask you questions and execute a few exams. This is to try to find the origin of your pain and also to find out which intervertebral disks are herniated. An accurate diagnosis will help your doctor develop a treatment plan method to help you recover and to handle your herniated disc pain and other spine symptoms.
Physical Exam: Herniated Disc Diagnosis
As part of the physical exam, your doctor will ask about your current symptoms and remedies you have already tried for your pain. Some average herniated disc diagnostic questions include:
When did the pain begin? Where’s the pain (cervical, thoracic or mid-back, or lumbar or lower back)?
What activities did you lately do?
What do you do for your herniated disc pain?
Can the disc herniation pain radiate or travel to other parts of your body?
Does anything reduce the disk pain or make it even worse?
Your doctor may also observe your position, range of movement, and physical condition both lying down and standing up. Movement that causes pain will be noticed. A Las�gue evaluation, also referred to as the Straight-Leg Raising evaluation, may be accomplished. You’ll be asked to lie down and extend your knee with your hip bent. If it produces pain or makes your pain worse, this may indicate a herniated disc.
With a herniated disc (or a bulging or ruptured disc), you might feel stiff and may have lost your normal spinal curvature because of muscle strain. Your physician may also feel for tightness and note the spine’s curvature and alignment.
Neurological Exam: Herniated Disc Diagnosis
Your spine specialist will also run a neurological exam, which tests your reflexes, muscle strength, other nerve changes, and pain disperse. Radicular pain (pain that travels away from the source of the pain) can increase when stress is applied directly to the affected area. You might, for instance, have sciatica; this is radicular pain that might be caused by the herniated disk. Since the disc is compressing a nerve, you might experience pain and symptoms in other areas of the body, although the origin of the pain is on your spine.
Imaging Tests for Herniated Discs
Your spine specialist may order imaging tests to help diagnose your injury or condition; you might have to see an imaging facility for those evaluations.
An X-ray may demonstrate a secondhand disk space, fracture, bone spur, or arthritis, which might rule out disk herniation. A computerized axial tomography scan (a CT or CAT scan) or a magnetic resonance imaging test (an MRI) equally can show soft tissue of a bulging disk or herniateddisc. So that you may get treatment these tests will demonstrate location and the stage of the herniated discs.
Other Tests to Diagnose�a Herniated Disc
To obtain the most accurate identification, your spine specialist may order additional tests, for example:
Electromyography (EMG): He or she may order an examination known as an electromyography to measure your nerves respond, if your spine pro suspects you’ve got nerve damage.
Discogram or discography: A sterile procedure where dye is injected into one of your vertebral disc and seen under special conditions (fluoroscopy). The goal is to pinpoint which disk(s) might be causing your pain.
Bone scan: This technique generates film or computer images of bones. A very small number of radioactive substance is injected into a blood vessel throughout the blood flow. It collects on your bones and can be detected by a scanner. This procedure helps doctors detect spinal problems such as disease, a fracture, tumor, or arthritis.
Laboratory evaluations: Typically blood is attracted (venipuncture) and tested to determine if the blood cells are normal or abnormal. A metabolic disease which might be contributing to a back pain may be indicated by Chemical changes in the blood.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
By Dr. Alex Jimenez
Additional Topics: Sciatica
Lower back pain is one of the most commonly reported symptoms among the general population. Sciatica, is well-known group of symptoms, including lower back pain, numbness and tingling sensations, which often describe the source of an individual’s lumbar spine issues. Sciatica can be due to a variety of injuries and/or conditions, such as spinal misalignment, or subluxation, disc herniation and even spinal degeneration.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine