Hormone deficiencies and imbalances are more common than one might originally think. Research suggests that “nearly half of the women in the United States have experienced a hormone imbalance” (Grinta, 1) . However, hormone imbalance does not just affect women, “as nearly 35% of males in their seventh decade have lower testosterone levels than younger men”. (McBride, 2)��An imbalance in hormones can cause an array of symptoms and ultimately affect an individuals day to day life.�
Symptoms�
The symptoms of hormone deficiency might not be as obvious as one could imagine. Some symptoms are small and could be brushed off as stress or lack of sleep, but it is important to look at the symptoms for what they really are. “In women, low estrogen can contribute to:
mood swings
hot flashes
headaches
depression
trouble concentrating
fatigue
irregular or absent periods
increased UTI’s “
(Swns, 3)�
In men, some of the symptoms are similar to those in women, but also include:
decreased bone mass
sleep disturbances
decreased motivations
increased body fat
decreased muscle mass
hair loss
libido
(Wallace, 4)
Solutions�
If these symptoms are affecting an individual’s lifestyle, there are multiple steps that can be taken to diagnose the problem and ultimately reduce symptoms. In today’s medical world, practitioners are able to use integrative techniques towards functional medicine, focusing on the biochemical level. If a patient is seeking solutions, the first step taken is an extensive questionnaire. This allows the doctor to pinpoint the exact symptoms, issues, and gives an insider look as to what direction to head towards first.
An example of the questions asked are as follows:
Once the questionnaire is completed and reviewed, a lab test is needed in order to confirm and view the exact levels the hormones are at. D.U.T.C.H ( Dried Urine Test for Comprehensive Hormones) provides one of the most accurate results. To gain more insight on D.U.T.C.H and how it works, please see last week’s article, linked here.
Testing & Conclusions
Filling out the questionnaire�essentially allows the practitioner to score and rate the severity of the issues. Adding the D.U.T.C.H results to the questionnaire gives the practitioner a factual level and complete understanding of their patient’s sex and adrenal hormones and metabolites.
This further allows the practitioner to diagnose (if necessary) and suggest nutraceuticals to help the patient’s hormone levels return to normal and minimize symptoms. There are many factors and systems involved when it comes to treating hormones and having tests completed that reflect the numbers that need to be adjusted is necessary. A hormone imbalance can easily take charge of an individual’s life, but now is the time to get these symptoms under control and get back to feeling like you used to!
A great place to start is to find a doctor or healthcare provider who will supply you with a full questionnaire and listen to the symptoms you’re having. This condition is fairly common and can be treated! October is Chiropractor Health Month, and we would love to see you and aid in providing treatment if you are experiencing any of these symptoms. Due to the fact that hormones can be complex and affect different body systems, we take the time to really understand and check all aspects before jumping to a conclusion. – Kenna Vaughn, Senior Health Coach
The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or chronic disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
Bibliography
(1) Ginta, Daniela. �What Are the Symptoms of Low Estrogen in Women and How Are They Treated.� Healthline, 31 Jan. 2017, www.healthline.com/health/womens-health/low-estrogen-symptoms.
(2) McBride, J Abram, et al. �Testosterone Deficiency in the Aging Male.� Therapeutic Advances in Urology, SAGE Publications, Feb. 2016, www.ncbi.nlm.nih.gov/pmc/articles/PMC4707424/.
(3) Swns. �Nearly Half of Women Have Been Affected by a Hormonal Imbalance.� New York Post, New York Post, 22 Feb. 2019, nypost.com/2019/02/22/nearly-half-of-women-have-been-affected-by-a-hormonal-imbalance/.
(4) Wallace, Ryan, and Kathleen Yoder. �12 Signs of Low Testosterone .� Healthline, 25 Apr. 2019, www.healthline.com/health/low-testosterone/warning-signs.
Today, we will be talking about what does the protein compounds and the peptide compounds do when a patient is being tested for food sensitivity. And we will also discuss what the Lectin and Dairy Zoomer do when a patient has a reaction to those types of food groups. In the last article, we mentioned about immunoglobulins in the intestinal barrier. And what do IgA and IgG antibodies do to the peptide and protein level?
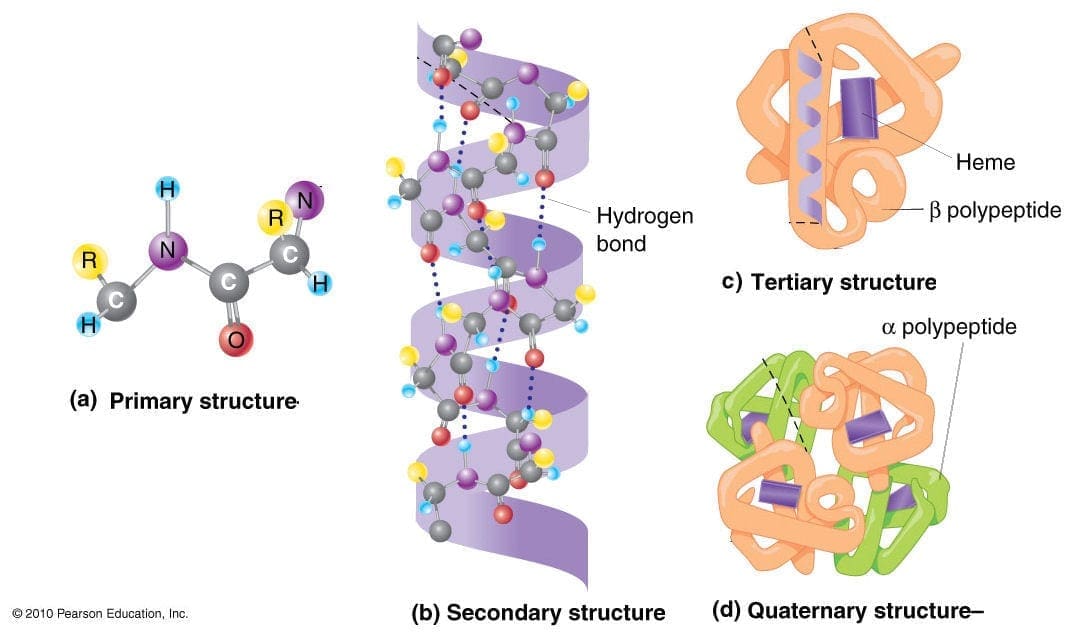
Proteins vs. Peptides
So let us take a look at proteins and peptides since this is what Vibrant Food Zoomers are actually testing on a patient. Remember that the Food Zoomers are testing the peptides in the whole protein and testing all the links to see what the patient is actually sensitive to the foods they are consuming.
Proteins
Protein is basically abundant biomolecule that is consist of one or more long chains of amino acid residues. Proteins can be found in whole foods like meats and vegetables that can help the muscles in our bodies. In the last article, we talked about how IgA and IgG antibodies are used for food sensitivity testing.
However, there is a limitation of a whole protein food sensitivity testing on a patient. Practitioners do make the assumption that the patient�s gut barrier is functional and intact since there are no signs of a leaky gut syndrome presented in the results. But, if that patient has the leaky gut syndrome, then the food sensitivity test will reflect what the patient has been eating. Another assumption is that the patient�s HCI and digestive enzymes are sufficient for tolerable proteolysis. Which means that those enzymes are breaking down whole proteins into smaller peptides.
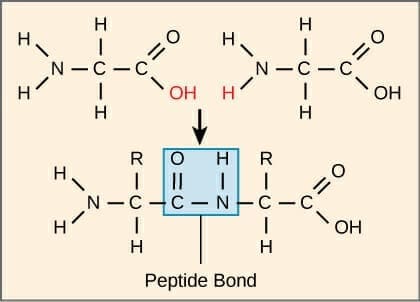
Peptides
Peptides are what in protein molecules as they are short chains of amino acids and are linked by the peptide bonds. When they are being tested by the food sensitivity tests, the reproducibility is higher. It doesn�t rely on the excess HCI (hydrochloric acid) or enzymes. What the test eliminates is the cross-reactivity because peptides in proteins are not going to have molecular mimicry to other unrelated proteins.
The antibodies are highly specific to the peptides because they are not going to be generalized or more massive antibodies of proteins since cross-reactivity is eliminated. Another thing is that the peptide test does is that it can measure thousands of peptides in one protein for a full spectrum of reactivity.
When patients are coming in with digestive problems and inflammatory condition/symptoms, practitioners take note that a lot of patients commonly have hypochlorhydria and deficiencies of enzymes and/or bile acids. Most patients sometimes have moderate to severe impairment of the intestinal barrier. When that happens, local doctors discuss with them that they may have to change their diets slowly but surely. And with integrative functional medicine that can occur.� Local practitioners look at their patient�s ailments and start detoxifying their bodies slowly. This helps their bodies heal and recommend them whole, nutritious, organic foods, and supplements to help repair the body naturally. Sometimes medicines can cause disruption to our bodies, however with whole natural foods and specific diets, it can help restore our bodies. Plus making sure that we exercise to make our bodies feel good and look good.
So now that we understand what proteins and peptides do when they are being tested. Let�s take a look at the food zoomers that can help you in case you have a sensitivity to these food groups. These are the Vibrant Lectin Zoomer and the Dairy Zoomer.
Lectin Zoomer
The Lectin Zoomer is consist of a handful of lectins and a handful of aquaporins. The most common lectins that people consume are barley, bell pepper, chickpea, corn, cucumber, potato, etc. And the most common aquaporins that people consume are spinach, soybean, tomato, tobacco, etc.
Difference between Lectins and Aquaporins
The difference between lectins and aquaporins is that lectins are sugar-binding proteins that are found in both animals and plants, which can bind to the carbohydrate structures on cells. While aquaporins are water channels that are found in cavities in both plants and humans. Some aquaporins can cross-react and can lead to primarily neurological symptoms.
How Problematic are Lectins?
Some studies show cell toxicity in humans is done by using extreme cytotoxic lectins. Ricin, for example, is a common biological warfare element that is not from the commonly consumed legumes or grains. It contains cytotoxic lectins and is being consumed by animals like mice or pigs. The assumption is being made that there are similarities with humans and animal gut glycosylation (the process of sugar-binding) in these situations.
Unfortunately, though it hasn�t been demonstrated thoroughly. But lectins have biological activity in the human body. They have been used as a cancer treatment mechanism because they can agglutinate cancer cells. Which means that they produce cytotoxicity to cancer cells and can actually carry chemotherapy across cancer cell membranes.
Even though that is a good thing, lectins can facilitate the bacterial endotoxins across the epithelial barrier and go into the peripheral tissues. And that can cause inflammation to the intestinal epithelial barrier in the small intestines. Animals studies show that raw lectin consumptions can cause hemagglutinating effects, causing inflammation.
But we as humans don�t eat raw lectins because they are cooked, not pressurized cook. Certain foods that are lectins can be eaten raw or cooked. But animal studies stated that they are using for these studies are grain and legume lectins that are raw like beans and grains. But the upside is that lectins can affect the metabolism of nutrients to increase fat loss which is a positive side effect.
Measuring the Sensitivity to Lectins
On the Food Zoomers test, lectins are really not included in each analysis, except for the Wheat Zoomer. Surprisingly, a Food Zoomer may be non-reactive, but whoever is sensitive to a lectin component in the food they eat, may be reactive. So when that happens, it is necessary to eliminate the food temporarily.
If you are sensitive to a particular food, you can have a Food Zoomer and a lectin Zoomer combine. Because if you are sensitive to the food you consume, and it doesn�t show up on the Food Zoomer, but it shows up on the Lectin Zoomer. Then you should eliminate it from your diet for a bit until you retake the test.
Conditions Associated with Lectins
If you do have a lectin sensitivity, here are some of the terms that can affect your body.
Arthritis/rheumatoid arthritis
Connective tissue disorder
Gastrointestinal inflammation
Intestinal permeability
Possible cancer in established cancer patients
Now let�s take a look at the Dairy Zoomer and its functions if you are sensitive to whole dairy products.
Dairy Zoomer
The Dairy Zoomer is a peptide level assessment of the full spectrum of immune response possible to proteins in cow�s milk dairy. What this means that the Dairy Zoomer is only specific to cow�s milk. Since some proteins in cow�s milk are similar enough in the molecular structure to have the same homology to goat or sheep�s milk.
This means that these other kinds of milk may be potential can cause inflammatory in some individuals. The oral challenge for alternative types of fluid may be warranted, but use your best clinical judgment after the intestinal barrier is healed.
What the Dairy Zoomer does is that it takes the milk protein and breaking each individual protein down to its different peptides. If you are wondering if the Dairy Zoomer is a test for lactose intolerance, it is not. Since lactose intolerance is not an immune-based reaction to dairy and does not involve any protein constituents of the food, therefore no antibodies are being generated.
What it is going to test for is the casein and whey proteins in the milk product from all animals, and the ratio of these proteins will vary by species. But all the proteins and milk will generally fall into one of these two proteins.
What to do with the results?
Once your patient comes back after taking the Food Zoomers test, here are some of the things to look for when you are retesting them.
If there are any IgA antibodies still in your patient, warrant an immediate elimination, regardless that it�s moderate or positive.
If there are any Moderate IgG antibodies in your patient, then it should be eliminated in the short term. Then rotate after a 30-60-day elimination and assessing the status of the intestinal permeability to confirm that that gut barrier is no longer �leaky.�
If there is a positive IgG result, then it should be eliminated long term and only reintroduced after 90+ days and confirm of an intact intestinal barrier.
Conclusion
So all in all, food sensitivity combine with the food zoomers test are an excellent way to help your body, especially the intestinal system. The Food Zoomers we used is functional for our patient�s wellness. Because we want to get rid of the excess antibodies and heal our patient�s body through the use of functional medicine.
The expression biocentrism encompasses all environmental integrity that extend the status of things from human beings to all living organisms. Biocentric ethics involves a rethinking of the relationship between nature and humans.
Biocentrism beliefs state that nature doesn’t exist simply to be used or consumed by people, but instead, that people are simply one species amongst many, and that since we are a part of an ecosystem, those activities that can negatively affect the living systems of which we’re a portion of can negatively influence us as well.
Much of the history regarding biocentric ethics can be understood concerning an expanding array of values. As environmental issues, such as human population growth, waste disposal, and resource depletion have begun to become a growing issue for society, several ethicists argued that value ought to be extended to include future generations of human beings. It’s been argued under biocentrism that individuals should expand moral standing to animals and plants and then to wilderness areas as well as ecosystems, species, and populations. Roots of biocentric ethics originated in several customs as well as in several historic figures.
The first of the five basic precepts of Buddhist ethics is to avoid harming or killing any living thing. The Christian saint Francis of Assisi preached to animals and proclaimed a theology that included plants and animals. Some Native American traditions hold that all things are sacred. The Romantic movement of the 18th and 19th centuries lacked the inherent value of the natural world against the propensity of the technological age to treat all nature as having value.
Biocentrism in the Medical World
While early biocentric beliefs and ideals have expanded through various aspects of society, biocentrism has also become the basis of ethics regarding its relation to human biomedical and behavioral research in the practice of human medicine, including natural, alternative care options, such as integrative medicine.
Integrative medicine is an approach to care that places the patient at the center and addresses the full array of physical, emotional, mental, social, spiritual and environmental influences that affect a person�s health. Implementing a personalized plan that considers the individual’s unique conditions, needs and circumstances, integrative medicine utilizes the most suitable interventions from an array of scientific disciplines to cure disease and illness as well as help people regain and maintain their overall health and wellness.
Integrative medicine is grounded from the definition of well-being. The World Health Organization (WHO) defines health as “a state of complete physical, psychological and social well-being and not just the absence of disease or infirmity.”
As mentioned above, integrative medicine attempts to restore and maintain health across a person’s lifespan by understanding the patient’s unique set of conditions affecting them and addressing the full selection of physical, emotional, mental, social, spiritual and environmental influences which can ultimately affect their wellness. During personalizing care, integrative medicine goes beyond the treatment of symptoms to address the causes of an illness. The patient’s immediate health needs in addition to the impacts of the complex and long-term interplay between influences are often taken into account before proceeding with the proper treatment.
Integrative medicine combines conventional medical treatments with remedies that are carefully selected and shown to be safe and effective. The goal is to combine the best that traditional medicine has to offer with therapeutic systems and therapies derived from ideas and cultures both new and old.
Integrative medicine is not the same as alternative medicine, which refers to an approach to healing that’s utilized in place of conventional treatments, or complementary medicine, which describes therapeutic modalities that are used to match allopathic approaches. Maintenance may be integrative irrespective of which modalities are used if the defining principles are implemented.
Many individuals erroneously use the term integrative medicine interchangeably with the conditions complementary medicine and other drugs, also known collectively as complementary and alternative medicine, or CAM. While medicine is not synonymous with CAM, CAM therapies do constitute an significant part the integrative medicine model.
The defining principles of integrative medicine are:
The individual and professional are partners in the healing process.
All aspects that influence health are taken into consideration, including body, mind, soul and community.
Providers utilize all healing sciences to facilitate the body’s innate healing response.
Powerful interventions which are organic and less invasive are utilized whenever possible.
Good medicine is based in good science. It is inquiry driven and open to new paradigms.
Together with the idea of treatment, the concepts of health promotion and the prevention of illness are paramount.
The maintenance is personalized to best address the individual’s unique conditions, needs and circumstances.
Practitioners of integrative medicine devote themselves into self-development and self-exploration and exemplify its fundamentals.
In addition to treating and managing the immediate health problems as well as the deeper causes of the disease or illness, integrative medicine strategies also focus on prevention and foster the growth of healthy behaviours and skills for successful treatment that patients can use throughout their lives. Much like the biocentrism ideals, professionals who practice integrative medicine ensure that the patient is surrounded by healthy, external factors, including environmental exposure as well as the proper nutrition, aside from the person’s unique human experience.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
By Dr. Alex Jimenez
Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.
Is coconut oil a metabolism-boosting superfood or an artery-clogging threat to heart health?
That question has fueled a raging debate for many years, and it was reignited in mid-June when the American Heart Association (AHA) issued an advisory reiterating its longstanding recommendation to avoid saturated fats. Attention quickly focused on coconut oil, which has become trendy in natural health circles despite its high saturated fat content.
Proponents of coconut oil say its medium-chain triglycerides are quickly burned for energy, increasing metabolism. Coconut oil fats are also said to be good for the brain, which is made mostly of fat, and help regulate blood sugar and, ironically, cholesterol levels.
But the AHA advisory contends that all saturated fats raise risk of cardiovascular disease.
“Taking into consideration the totality of the scientific evidence…we conclude strongly that lowering intake of saturated fat and replacing it with unsaturated fats, especially polyunsaturated fats, will lower the incidence of cardiovascular disease,” states the advisory.
The AHA researchers specifically advise against using coconut oil, which they note is 82 percent saturated fat and raises “bad” LDL cholesterol levels, “a cause of atherosclerosis.”
But many other scientific reviews in recent years — including one meta-analysis encompassing nearly 350,000 people followed for as long as 23 years — found no link between saturated fat and heart disease.
“Those reviews were much more limited because they didn’t take into consideration what the substitution [for saturated fats in the diet] was,” explains Dr. Alice Lichtenstein, co-author of the AHA advisory. “The better reviews that looked at replacing saturated fat with either carbohydrates or mono- or polyunsaturated fats, show clear differences.”
Many natural health practitioners take exception to the AHA conclusions, including integrative cardiologist Dr. Jack Wolfson. He contends that AHA researchers cherry-picked data from decades-old studies, and that branding all LDL as harmful is outdated science.
“Total LDL numbers are a very poor prognosticator of heart disease,” says Wolfson, a doctor of osteopathy and board-certified cardiologist based in Phoenix, Ariz. “What’s more relevant is LDL particle size and numbers. Small, dense particles are bad for the heart, but studies show that large fluffy particles, like those promoted by coconut oil, cause no harm.”
But Lichtenstein, director of the Cardiovascular Nutrition Laboratory at Tuft University’s Human Nutrition Center on Aging, dismisses the LDL particle size factor, saying, “There’s much more written on the Internet about that than data to support it.”
Wolfson further questions AHA recommendations to use “highly processed” vegetable oils, saying their omega-6 fatty acids can contribute to systematic inflammation. In an AHA newsletter, the advisory’s lead author, Dr. Frank Sacks, suggests that people forsake butter and coconut oil for cooking and use canola, corn, soybean, and extra virgin olive oil instead.
“There’s nothing wrong with deep frying as long as you deep fry in a nice unsaturated vegetable oil,” Sacks adds.
That suggestion may send shudders through natural health practitioners, who widely contend that vegetable oils break down into harmful compounds under high heat.
“Coconut oil has a high smoke point, which makes it more stable for cooking,” explains Wolfson. “Unsaturated vegetable oils oxidize through the cooking process and cause oxidative stress and inflammation in the body.”
Lichtenstein once again cites a lack of data on the adverse effect of cooking with vegetable oils, telling Newsmax Health, “It’s not a concern.”
Wolfson also points out that the evolving science of heart disease seems to be shifting away from cholesterol and more toward inflammation as the primary cause.
“The risk of a cardiovascular event – heart attack, stroke and dying — is much higher when you have inflammation,” says Wolfson, author of “The Paleo Cardiologist: The Natural Way to Heart Health” and advocate of eating diets similar to our caveman ancestors.
“Coconut oil doesn’t cause inflammation. Sugar, artificial ingredients, pesticide residue in food…these are the types of things that cause inflammation.”
He emphasizes that it’s important to eat healthy saturated fats that are organic and, if animal-based, come from grass-fed pasture-grazers. Wolfson adds that he has history on his side in the debate over whether they are healthy or harmful.
“Our ancestors ate saturated fats for millions of years,” he tells Newsmax Health. “Why would evolution make it plug up our pipes and kill us? People in the South Pacific have diets that are more than 50 percent coconut-based, and they have virtually no heart disease. If we were all on a deserted island eating coconuts, fish and vegetables, and getting plenty of sunshine and sleep, heart disease would be a non-issue.”
Eating fish at least twice a week may significantly reduce the pain and swelling associated with rheumatoid arthritis, a new study says.
Prior studies have shown a beneficial effect of fish oil supplements on rheumatoid arthritis symptoms, but less is known about the value of eating fish containing omega-3, the researchers said.
“We wanted to investigate whether eating fish as a whole food would have a similar kind of effect as the omega 3 fatty acid supplements,” said the study author, Dr. Sara Tedeschi, an associate physician of rheumatology, immunology and allergy at Brigham and Women’s Hospital in Boston.
Generally, the amount of omega 3 fatty acids in fish is lower than the doses that were given in the trials, she said.
Even so, as the 176 study participants increased the amount of fish they ate weekly, their disease activity score lowered, the observational study found.
In rheumatoid arthritis, the body’s immune system mistakenly attacks the joints, creating swelling and pain. It can also affect body systems, such as the cardiovascular or respiratory systems. The Arthritis Foundation estimates that about 1.5 million people in the United States have the disease, women far more often than men.
The new study, which was heavily female, draws attention to the link between diet and arthritic disease, a New York City specialist said.
“While this is not something that is new, per se, and it was a small trial, it does raise an interesting concept of what you eat is as important as the medications you take,” said Dr. Houman Danesh.
“A patient’s diet is something that should be addressed before medication is given,” added Danesh, director of integrative pain management at Mount Sinai Hospital.
When his patients with rheumatoid arthritis ask about diet, he said he often suggests they eat more fish for a few months to see if it will help.
“I encourage them to try it and decide for themselves,” he said, explaining that study results so far have been mixed.
In this case, the majority of study participants were taking medication to reduce inflammation, improve symptoms and prevent long-term joint damage.
Participants were enrolled in a study investigating risk factors for heart disease in rheumatoid arthritis patients. The researchers conducted a secondary study from that data, analyzing results of a food frequency questionnaire that assessed patients’ diet over the past year.
Consumption of fish was counted if it was cooked — broiled, steamed, or baked — or raw, including sashimi and sushi. Fried fish, shellfish and fish in mixed dishes, such as stir-fries, were not included.
Frequency of consumption was categorized as: never or less than once a month; once a month to less than once a week; once a week; and two or more times a week.
Almost 20 percent of participants ate fish less than once a month or never, while close to 18 percent consumed fish more than twice a week.
The most frequent fish eaters reported less pain and swelling compared to those who ate fish less than once a month, the study found.
Researchers can’t prove that the fish was responsible for the improvements. And they theorized that those who regularly consumed fish could have a healthier lifestyle overall, contributing to their lower disease activity score.
While they were unable to get specific data on information such as patients’ exercise, its benefits are proven, Tedeschi said.
She acknowledged that fish tends to be an expensive food to purchase. For those unable to afford fish several times a week, Danesh cited other options.
“In general, patients should eat whole, unprocessed foods,” he said. “If you can’t for whatever reason, an omega 3 pill is a second option.”
Because the study was not randomized, researchers were unable to make definite conclusions, but they were pleased with what they learned.
One finding that impressed Tedeschi “was that the absolute difference in the disease activity scores between the group that ate fish the most frequently and least frequently was the same percentage as what has been observed in trials of methotrexate, which is the standard of care medication for rheumatoid arthritis,” she said.
The findings were reported June 21 in Arthritis Care & Research.
Abstract objective: �To examine the diagnosis and care of a patient suffering from chronic low back pain with associated right leg pain and numbness. ���Diagnostic studies include standing plain film radiographs, lumbar MRI without contrast, chiropractic analysis, range of motion, orthopedic and neurological examination. ���Treatments include both manual and instrument assisted chiropractic adjustments, ice, heat, cold laser, Pettibon wobble chair and repetitive neck traction exercises and non-surgical spinal decompression. ��The patient’s� outcome was very good with significant reduction in pain frequency, pain intensity and abatement of numbness in foot.
Introduction: �A 58 year old, 6�0�, 270 pound male was seen for a chief complaint of lower back pain with radiation into the right leg with right foot numbness. �The pain had started 9 months prior with an insidious onset. ��The patient had first injured his back in high school lifting weights with several episodes of pain over the ensuing years. ��The patient had been treating with Advil and had tried physical therapy, acupuncture, chiropractic and ice with no relief of pain and numbness. ��Walking and standing tend to worsen the problem and lying down did provide some relief. ���A number of activities of daily living were affected at a severe level including standing, walking, bending over, climbing stairs, looking over shoulder, caring for family, grocery shopping, household chores, lifting objects staying asleep and exercising. ��The patient remarked that he �Feels like 100 years old.� �Social history includes three to four beers per week, three diet cokes per day.
The patient�s health history included high blood pressure, several significant shoulder injuries, knee injuries, apnea, hearing loss, weight gain, anxiety and low libido. ���Family history includes Alzheimer�s disease, heart disease, colon cancer and obesity.
Clinical Findings
Posture analysis revealed a high left shoulder and hip with 2 inches of anterior head projection. Bilateral weight scales revealed a +24 pound differential on the left. ��Weight bearing dysfunction and imbalance suggest that neurological compromise, ligamentous instability and or spinal distortion may be present. �Range of motion in the lumbar spine revealed a 10 degree decrease in both flexion and extension. There was a 5 degree decrease in both right and left lateral bending with sharp pain with right lateral bending.
Cervical range of motion revealed a 30 degree decrease in extension, a 42 and 40 degree decrease in right and left rotation respectively and a 25 degree decrease in both right and left lateral flexion. ��Stability analysis to assess and identify the presence of dynamic instability of the cervical and lumbar spine showed positive in the cervical and lumbar spine and negative for sacroiliac dysfunction. ��Palpatory findings include spinal restrictions at occiput, C5, T5, T10, L4,5 and the sacrum. ��Muscle palpation findings include +2 spasm in the psoas, traps, and all gluteus muscles.
Cervical radiographs reveal significant degenerative changes throughout the cervical spine. This represents phase II of spinal degeneration according the Kirkaldy-Wills degeneration classification. ���Cervical curve is 8 degrees which represents an 83% loss from normal. ��Flexion and extension stress x-rays reveal decreased flexion at occiput through C4 and decreased extension at C2, C4-C7.
Lumbar radiographs reveal significant degenerative changes throughout representing phase II of spinal degeneration according to the Kirkaldy-Willis spinal degeneration classification. ���There is a 9 degree lumbar lordosis which represents a 74% loss from normal. ��There is a 2 mm short right leg and a grade II spondylolisthesis at the L5-S1 level.
Lumbar MRI without contrast was ordered immediately with a 4 mm slice thickness and 1 mm gap in between slices on a Hitachi Oasis 1.2 Telsa machine for optimal visualization of pathology due to the clinical presentation of right L5 nerve root compression.
Lumbar MRI Imaging Results
Significant degenerative changes throughout the lumbar spine including multi-level degenerative disc changes at all levels.
Transverse Annular Fissures at L1-2 (17.3 mm), L2-3 (29.5 mm), L4-5 (14.3 mm) and L5-S1 (30.8 mm) and broad based disc bulging at all levels except L5-S1. ���The fissures at L2-3 and L5-S1 both have radial components extends through to the vertebral endplate.
Facet osteoarthritic changes and facet effusions at all levels.
Grade II spondylitic spondylolisthesis is confirmed at L5-S1 with severe narrowing of the right neural foramen compressing the right exiting L5 nerve root.
Degenerative retrolisthesis at L1-2.
Modic Type II changes at L2 inferior endplate, L3 superior endplate, L4 inferior endplate and L5 inferior endplate.2
There is a 18.9 mm wide Schmorl�s node at the superior endplate of L3.
There is a 5.7 mm wide focal protrusion type disc herniation at L4-5 which impinges on the thecal sac.
T2 sagittal Lumbar Spine MRI:� Note the Modic Type II changes and the L2-3 Schmorls node.
T1 Sagittal Annular fissures at multiple levels and spondylolisthesis at L5S1
T2 Axial L4-5:� Focal Disc Protrusion Type Herniation
Definition �Bulging Disc: A disc in which the contour of the outer annulus extends, or appears to extend, in the horizontal (axial) plane beyond the edges of the disc space, over greater than 50% (180 degrees) of the circumference of the disc and usually less than 3mm beyond the edges of the vertebral body apophyses.3
Definition: Herniation is defined as a localized or focal displacement of disc material beyond the limits of the intervertebral disc space.3
Protrusion Type Herniation: is present if the greatest distance between the edges of the disc material presenting outside the disc space is less than the distance between the edges of the base of that disc material extending outside the disc space.3
Definition: Extrusion Type Herniation: �is present when, in at least one plane, any one distance between the edges of the disc material beyond the disc space is greater than the distance between the edges of the base of the disc material beyond the disc space or when no continuity exists between the disc material beyond the disc space and that within the disc space. 3
Definition: �Annular Fissures: �separations between the annular fibers of separations of the annual fibers from their attachments to the vertebral bone. 4
Definition � Radiculopathy: Sometimes referred to as a pinched nerve, it refers to compression of the nerve root – the part of a nerve between vertebrae. This compression causes pain to be perceived in areas to which the nerve leads.
The patient underwent multimodal treatment regime consisting of 4 months of active chiropractic adjustments, non-surgical spinal decompression with pretreatment spinal warm-up exercises on the Pettibon wobble chair and neck traction and heat. Post spinal decompression with ice and cold laser. ��The patient reported long periods of symptom free activities of daily living with occasional short flare-ups of pain. ��Exacerbations are usually of short duration and much lower frequency. �The only activity of daily living noted as affected severely at the end of care is exercising.
Post care lumbar radiographs revealed a 26 degree lumbar curve a 15 degree (38%) increase
Post care cervical x-rays revealed a 10 mm decrease in anterior head projection and a 2 degree improvement in the cervical lordosis.
Range of Motion
pre
post
increase
Lumbar
flexion
60
60
0
extension
40
40
0
r. lateral flexion
20
25
5
l. lateral flexion
20
25
5
cervical
pre
Post
increase
flexion
50
50
0
extension
30
40
10
r. lateral flexion
20
35
15
l. lateral flexion
20
20
0
r. rotation
38
70
42
l. rotation
40
80
40
Discussion of Results
It is appropriate to immediately order MRI imaging with radicular pain and numbness. ��Previous health providers who did not order advanced imaging with these long term radicular symptoms are at risk of missing important clinical findings that could adversely affect the patient�s health. ��The increasing managed care induced trend to forego taking plain film radiographs is also a risk factor for patients with these problems.
This case is a typical presentation of long standing spinal injuries that over many years have gone through periods of high and low symptoms but continue to get worse functionally and eventually result in a breakdown of spinal tissues leading to neurological compromise and injury.
Chiropractic treatment resulted in a very favorable outcome aided by an accurate diagnosis. �This is also the case where the different treatment modalities all contributed to the success of the protocol. ��The different modalities all focus on different areas of pathology contributing to the patients� disabled condition.
Modality
Therapeutic Goals
Chiropractic adjustment
Manual and instrument assisted forces introduced to the osseous structures that focuses on improving motor segment mobility
Cold laser
Increases speed of tissue repair and decreases inflammation.4
Pettibon
wobble chair
Loading and unloading cycles applied to injured soft tissues and
Pettibon
neck traction
speeds up & improves remodeling of injured tissue as well as rehydrates dehydrated vertebral discs.5
Non-surgical
spinal decompression
Computer assisted, slow and controlled stretching of spine, creating vacuum effect on spinal disc, bringing it back into its proper place in the spine.6,7
Ice
Decrease inflammation through vasoconstriction
Heat
Warm up tissues for mechanical therapy through increasing blood flow.
Posture Correction Hat
Weighted hat that activates righting reflex resetting head posture.8
A major factor in the success of the care plan in this case was an integrative approach to the spine. �John Bland, M.D. in the text Disorders of the Cervical Spine writes
�We tend to divide the examination of the spine into regions: cervical, thoracic and the lumbar spine clinical studies.� This is a mistake.� The three units are closely interrelated structurally and functionally- a whole person with a whole spine.� The cervical spine may be symptomatic because of a thoracic or lumbar spine abnormality, and vice versa!� Sometimes treating a lumbar spine will relieve a cervical spine syndrome, or proper management of cervical spine will relieve low backache.�9
When addressing the spine as an integrative system, and not regionally it has a very strong benefit to the total care results. ��The focus on the restoration of the cervical spine function as well as lumbar spine function is a hallmark of a holistic spine approach that has been a tradition in the chiropractic profession.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
References:
Kirkaldy-Willis, W.H, Wedge JH, Young-Hing K.J.R. Pathology and pathogenesis of lumbar spondylosis and stenosis. �Spine 1978; 3: 319-328
David F. Fardon, MD, Alan L. Williams, MD, Edward J. Dohring, MD. Lumbar disc nomenclature: version 2.0 Recommendations of the combined task forces of the North American Spine Society, the American Society of Spine Radiology and the American Society of Neuroradiology. The Spine Journal 14 (2014) 2525�2545
Shealy CM, Decompression, Reduction and Stabilization of the Lumbar Spine: A cost effective treatment for lumbosacral pain.�� Pain management 1955, pg 263-265
Shealy, CM, New Concepts of Back Pain Management, Decompression, Reduction and Stabilization.�� Pain Management, a Practical guide for Clinicians.� Boca Raton, St. Lucie Press: 1993 pg 239-251
Bland, John MD, Disorders of the Cervical Spine WB Saunders Company, 1987 pg 84
Additional Topics: Preventing Spinal Degeneration
Spinal degeneration can occur naturally over time as a result of age and the constant wear-and-tear of the vertebrae and other complex structures of the spine, generally developing in people over the ages of 40. On occasion, spinal degeneration can also occur due to spinal damage or injury, which may result in further complications if left untreated. Chiropractic care can help strengthen the structures of the spine, helping to prevent spinal degeneration.
The sheer magnitude of America�s prescription opioid abuse epidemic has evoked visceral responses and calls-to-action from public and private sectors. As longtime advocates of drug-free management of acute, subacute and chronic back, neck and neuro-musculoskeletal pain, the chiropractic profession is aligned with these important initiatives and committed to actively participate in solving the prescription opioid addiction crisis.As professionals dedicated to health and well-being, Doctors of Chiropractic (DCs) are educated, trained and positioned�to deliver non-pharmacologic pain management and play a leading role in �America�s Opioid Exit Strategy.�
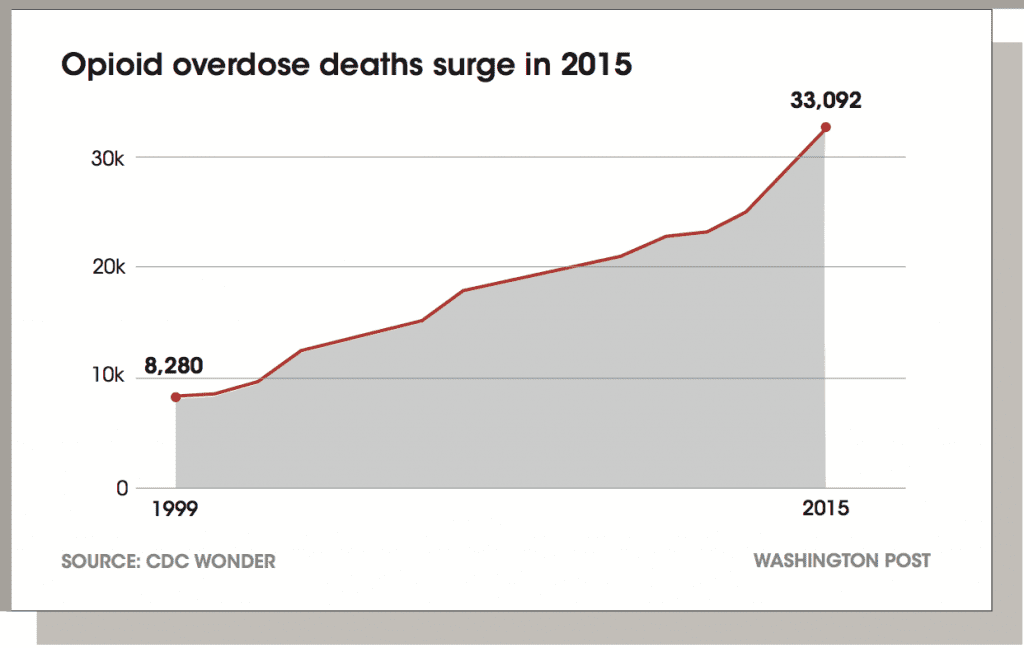
Data released by the Centers for Disease Control and Prevention (CDC) revealed that opioid deaths continued to surge in 2015, surpassing 30,000 for the first time in recent history. CDC Director Tom Frieden said,�The epidemic of deaths involving opioids continues to worsen. Prescription opioid misuse and use of heroin and illicitly manufactured fentanyl are intertwined and deeply troubling problems.�1
The human toll of prescription opioid use, abuse, dependence, overdose and poisoning have rightfully become a national public health concern. Along with the tragic loss of life, it is also creating a monumental burden on our health and related health care costs:
Health care costs for opioid abusers are eight times higher than for nonabusers.2
A new retrospective cohort study shows a 72 percent increase in hospitalizations related to opioid abuse/dependence from 2002 to 2012. Not surprisingly, inpatient charges more than quadrupled over that time. Previous estimates of the annual excess costs of opioid abuse
to payers range from approximately $10,000 to $20,000 per patient, imposing a substantial economic burden on payers.3
A recent government study puts the economic burden to the U.S. economy at $78.5 billion annually. For this study, CDC researchers analyzed the financial impact to include direct health care costs, lost productivity and costs to the criminal justice system.4
AMERICA�S COMMITMENT TO PRESCRIPTION OPIOID ABUSE: A PAINFUL REALITY CHECK
As a non-pharmacologic approach to effectively address acute, subacute and chronic non- cancer pain, integrative care management answers the needs of individuals nationwide.
With patient access to opioids becoming more restricted through more responsible clinician prescribing and government-mandated reduced production of opioids — and as those who are addicted become empowered to reduce their utilization — people experiencing pain face new, daunting challenges:
Without the use of drugs, how will they cope with pain?
How can they get referrals and access to drug-free care that will be effective for acute, subacute and chronic pain?
How can they ensure that their health care plans and insurance will cover the cost of non- pharmacologic care?
While the chiropractic profession lauds many of the noteworthy announcements and strides to overcome opioid addiction, these recommendations fall short in providing meaningful answers and solutions for those who are suffering from pain.
It is encouraging to see the July 22, 2016 enactment of the Comprehensive Addiction and Recovery Act (P.L. 114-198), the first major federal addiction legislation in 40 years, and the most comprehensive effort undertaken to address the opioid epidemic. It encompasses
all six pillars necessary for such a coordinated response � prevention, treatment, recovery, law enforcement, criminal justice reform and overdose reversal.5 The recent passage of the 21st Century Cures Act included $1 billion for states to use to fight opioid abuse.6 Unfortunately, this legislation has drawn critics who say it is simply a huge de-regulatory giveaway to the pharmaceutical and medical device industry.7
Closer examination of these legislative initiatives points to the absence of programs that address non-pharmacologic options for those fighting drug addiction, notably chiropractic care. When paired with the U.S. Surgeon General�s declaration of war on addiction,8 the government�s designation of �Prescription Opioid and Heroin Epidemic Awareness Week,� 9 and the commitment from 40 prescriber groups to ensure that 540,000 health care providers would complete training on appropriate opioid prescribing within two years,10 these �solutions� appear woefully inadequate to address the challenges of those who need effective, drug- free pain management.
This follow-up discussion to �Chiropractic: A Safer Strategy than Opioids� (June 2016), examines the positive steps as well as the shortcomings of initiatives undertaken from July 2016 – March 2017 to address the opioid crisis. It also assesses the current landscape of opportunities to offer patients, doctors and payers meaningful programs to effectively address acute, subacute and chronic neck, low back and neuro-musculoskeletal pain without the use of painkillers.
The chiropractic profession contends this should be a top priority, and it appears that a growing number of stakeholders are in agreement. In fact, the world�s second-largest pharmaceutical company has agreed to disclose in its marketing material that opioid painkillers might carry a serious risk of addiction, and promised not to promote prescription opioids for unapproved uses, such as long-term back pain.11
Based upon the evidence articulated in this document, it becomes clear that chiropractic care is a key component of �America�s Opioid Exit Strategy� on several levels:
�Perform first-line assessment and care for neck, back and neuro-musculoskeletal pain to avoid opiate prescribing from the first onset of pain.
�Provide care throughout treatment to mitigate the introduction of drugs.
�Offer an effective approach to acute, subacute and chronic pain management that helps addicts achieve a wellness focused, pain-free lifestyle as they reduce their utilization of opioids.
It�s also a compelling opportunity for our health system, commercial and government payers, employers — and most importantly patients — to resolve the issues surrounding pain at lower costs, with improved outcomes and without drugs or surgery.
Further complicating the situation: escalating prices of the opioid OD drug naloxone may threaten efforts to reduce opioid-related deaths across America, warn teams at
Yale University and the Mayo Clinic.13
Naloxone is a drug given to people who overdose on prescription opioids and heroin. If administered in time, it can reverse the toxic and potentially deadly effects of �opioid intoxication.�
The research team called attention to skyrocketing prices for the lifesaving antidote, noting:
Hospira (a Pfizer Inc. company) charges $142 for a 10-pack of naloxone — up 129 percent since 2012.
Amphastar�s 1 milligram version of naloxone is used off-label as a nasal spray. It�s priced around $40 — a 95 percent increase since September 2014.
Newer,easier-to-use formulations are even more expensive — a two-dose package of Evzio (naloxone) costs $4,500, an increase of more than 500 percent over two years.�The challenge is as the
price goes up for naloxone, it becomes less accessible for patients,� said Ravi Gupta, the study�s lead author.
Government & Regulators Restrict Access To Opioids
In the wake of this firestorm surrounding opioid abuse, and following the dissemination of prescribing guidelines introduced by the CDC, it becomes evident that certain market forces are influencing the battle against opioid addiction and the availability of drugs.
Among the most egregious stakeholders are those in the pharmaceutical sector.There are numerous instances which document their role attempting to thwart many legislative initiatives throughout the country to combat drug abuse.They impose exorbitant costs for life-saving antidotes, and aggressively develop and market the use of more drugs to fight opioid-induced side effects such as constipation. It becomes apparent that many of their answers to opioid addiction are simply more pills.14
The opioid market is worth nearly $10 billion in annual sales, and has expanded to include an unlimited universe of medications aimed at treating secondary effects rather than controlling pain.15 Given the financial incentives to produce, sell and distribute drugs, it�s no wonder that pharmaceutical companies (pharmcos) have a material interest in promoting drug utilization.
This set of behaviors has drawn extensive criticism.
�The root cause of our opiate epidemic has been the over-prescribing of prescription pain medications. Physicians get little to no training related to addiction in general, but particularly around opiate prescriptions. Over the past year, however, you hear more and more physicians admitting �we are part of the problem and can be part of the solution�.�16
—- Michael Botticelli, former White House drug policy director, commonly called the nation�s drug czar.
While physicians have been responding to calls for more responsible prescribing, the drug industry has historically been accused of providing physicians with misleading information regarding the addictive qualities of certain drugs.Appropriate education of prescribers is a key component of necessary change.
For example, when semisynthetic opioids like oxycodone and hydrocodone � found in Percocet and Vicodin respectively � were first approved in the mid�20th century, they were recommended only for managing pain during terminal illnesses such as cancer, or for acute short-term pain, like recovery from surgery, to ensure patients wouldn�t get addicted. But in the 1990s, doctors came under increasing pressure to use opioids to treat the millions of Americans suffering from chronic non-malignant conditions, like back pain and osteoarthritis.
A physician pain specialist helped lead the campaign, claiming prescription opioids were a �gift from nature,� with assurances to his fellow doctors � based on a 1986 study of only 38 patients � that fewer than one percent of long-term users became addicted.17
Today, drug makers may be getting their �wings clipped� with the introduction of new government directives slashing production of popular prescription painkillers. In 2016, the U.S. Drug Enforcement Administration (DEA) finalized a previous order on 2017 production quotas for a variety of Schedule I and II drugs, including addictive narcotics like oxycodone, hydromorphone, codeine and fentanyl. The agency has the authority to set limits on manufacturing under the Controlled Substances Act. The DEA said it is reducing �the amount of almost every Schedule II opiate and opioid medication� by at least 25 percent.18 Some, like hydrocodone, commonly known by brand names like Vicodin or Lortab, will be cut by one-third.
Despite these setbacks, the drug industry continues to launch strong initiatives that fight state- mandated opioid limits. Amid the crisis and regardless of the pressures urging a shift away from opioid use, the makers of prescription painkillers recently adopted a 50-state strategy that includes hundreds of lobbyists and millions in campaign contributions to help kill or weaken measures aimed at stemming the tide of prescription opioids.19
While the drug makers vow they�re combating the addiction problem,The Associated Press
and the Center for Public Integrity found that these manufacturers often employ a statehouse playbook of delay and defend tactics.This includes funding advocacy groups that use the veneer of independence to fight limits on the drugs, such as OxyContin, Vicodin and Fentanyl, a potent, synthetic opioid pain medication with a rapid onset and short duration of action that is estimated to be between 50 and 100 times as potent as morphine.20
In its national update released Dec. 16, 2016 in the Morbidity and Mortality Weekly Report, the CDC reported that more than 300,000 Americans have lost their lives to an opioid overdose since 2000.
As enforcement restricts the availability of prescription opioids, people addicted
to painkillers — such as oxycodone (OxyContin) and morphine — have increasingly turned to — street drugs like heroin.21
These independent sources also found that the drug makers and allied advocacy groups employed an annual average of 1,350 lobbyists in legislative hubs from 2006 through 2015, when opioids� addictive nature came under increasing scrutiny.
�The opioid lobby has been doing everything it can to preserve the status quo of aggressive prescribing.They are reaping enormous profits from aggressive prescribing.�22
Andrew Kolodny, MD, founder, Physicians for Responsible Opioid Prescribing
Undaunted by these interferences, and buoyed by a thirst for profits, pharmcos are now fueling other creative solutions to drive even greater revenues from the sale and distribution of drugs.
It now appears that pharmcos are directing their activities toward medicines known as abuse-deterrent formulations: opioids with physical and/or chemical barriers have built-in properties that make the pills difficult to crush,chew or dissolve.This aims to deter abuse through intranasal and intravenous routes of administration.These drugs ultimately are more lucrative, since they�re protected by patent and do not yet have generic competitors.They cost insurers more than generic opioids without the tamper-resistant technology.23
Skeptics warn that they carry the same risks of addiction as other opioid versions, and the U.S. FDA noted that they don�t prevent the most common form of abuse � swallowing pills whole.
�This is a way that the pharmaceutical industry can evade responsibility, get new patents and continue to pump pills into the system,� said Dr. Anna Lembke, Chief of Addiction Medicine at the Stanford University School of Medicine.24
Drug makers have discovered yet another way to profit from addicts taking high doses of prescription opioid painkillers � the new billion-dollar drug to treat opioid-induced constipation (OIC) rather than controlling pain.
Studies show that constipation afflicts 40-90 percent of opioid patients.Traditionally,doctors advised people to cut down the dosage of their pain meds, take them less often or try non-drug interventions. By promoting OIC as a condition in need of more targeted treatment, the drug industry is creating incentives to maintain painkillers at full strength and add another pill instead.25
Collectively, the subsets of new pharmaceutical submarkets to treat opioid addiction, overdoses, and side effects such as OIC are estimated to be worth at least $1 billion a year in sales.These economics, some experts say, work against efforts to end the epidemic.26
While there is continued pressure to limit the number and scope of opiates for patients, new government statistics reveal that drug overdose deaths continue to surge in the United States, now exceeding the number of deaths caused by motor vehicle accidents.27 Although it is reported that the number of opioid prescriptions has fallen across the U.S. over the past three years, with intermittent data on this decline in states such as West Virginia and Ohio, they still kill more Americans each year than any other drug.
Just over 33,000 (63 percent) of the more than 52,000 fatalities reported in 2015 are linked to the illicit use of prescription painkillers.28 States including Massachusetts, and most recently Virginia, have declared public health emergencies as the number of deaths has escalated.29
Regardless of whether these issues are viewed from the perspective of patients, clinician prescribers, or government regulators, the status quo is clearly not acceptable.
Responsible Prescribing
�My new patient didn�t mention his back pain until the very end of the visit.As he was rising to leave, he asked casually if I could refill his Percocet. I told him I am not a pain or a back specialist and that I generally prescribe muscle relaxants or anti-inflammatory medications for back pain � not opioids, which are addictive and do not really treat the underlying problem.
The patient persisted. He said his prior internist always prescribed it, and the medication also helped his mood. He promised he had its use under control and did not feel he needed to take more and more to achieve the same effect.
I didn�t relent. I offered to refer him to a back specialist instead. It was an uncomfortable end to an otherwise positive visit.
Unfortunately, we doctors are enablers.Too many of us fill those prescriptions for chronic pain. And when we don�t, too many of our patients leave us for other doctors who will. Or worse, they turn to buying heroin on the street.�30
Marc Siegel, MD, FOX NEWS
Clinical prescribers of pain medications are beginning to recognize their responsibilities for increased prescribing vigilance, and are expected to become important advocates for drug-free pain care. More than half of doctors across America are curtailing opioid prescriptions, and nearly 1 in 10 have stopped prescribing the drugs, according to a new nationwide online survey. More than one-third of the respondents said the reduction in prescribing has hurt patients with chronic pain.
The survey, conducted for The Boston Globe by the SERMO physicians social network, offers fresh evidence of the changes in prescribing practices in response to the opioid crisis that has killed thousands in New England and elsewhere around the country.The deaths awakened fears of addiction and accidental overdose, and led to state and federal regulations aimed at reining in excessive prescribing.
Doctors face myriad pressures as they struggle to treat addiction and chronic pain, two complex conditions in which most physicians receive little training.Those responding to the survey gave two main reasons for cutting back: the risks and hassles involved in prescribing opioids, and a better understanding of the drugs� hazards.31
In Wisconsin, the Medical Society says the state�s effort to fight the opioid epidemic is showing results.A new report found about eight million fewer opioids were dispensed between July and September 2016 compared to the same time during the previous year.The Medical Society says it�s doing more to help physicians monitor patients� use of opioids by supporting the release of an enhanced prescription drug monitoring program � or PDMP. Starting in April 2017, doctors will have to access the program while pharmacists will only have 24 hours to enter information instead of seven days.This gives doctors an update in case patients are going from doctor to doctor for more prescriptions.32
Prescription drug monitoring programs (PDMPs), launched in 2013, are state-run electronic databases used to track the prescribing and dispensing of controlled prescription drugs to patients.They are designed to monitor this information for suspected abuse or diversion (i.e., channeling drugs into illegal use), and can give a prescriber or pharmacist critical information regarding a patient�s controlled substance prescription history.This information can help prescribers and pharmacists identify patients at high-risk who would benefit from early interventions.
PDMPs continue to be among the most promising state-level interventions to improve opioid prescribing, inform clinical practice and protect patients at risk.33
Hospital Admissions Due To Heroin, Painkillers Rose 64% 2005-2014
Researchers found misuse of prescription painkillers and street opioids climbed nationwide, related hospital stays jumped from 137 per 100,000 people to 225 per 100,000 in that decade.
States where overdoses required at least 70 percent more hospital beds between 2009 and 2014 were North Carolina, Oregon, South Dakota and Washington.
In 2014, the District of Columbia, Maryland, Massachusetts, New York, Rhode Island and West Virginia each reported rates above 300 per 100,000 people — far above the national average.34
Health Plans Report Limited Prescribing Is Paying Off
According to IMS Health, a global health information and technology firm, the rate of opioid prescribing in the U.S. has dropped since its peak in 2012.The drop is the first that has been reported since the early 1990s, when OxyContin first hit the market and pain became �the fifth vital sign� doctors were encouraged to more aggressively treat.35
However, continued pressure on physician prescribing patterns and opportunities for therapies other than opioids may be paying off. Prescriptions for powerful painkillers dropped significantly among patients covered by Massachusetts� largest insurer after measures were introduced to reduce opioid use.36 The Blue Cross Blue Shield of Massachusetts program serves as an example of a private health insurer collaborating on a public health goal.
In 2012, the insurer � the state�s largest, with 2.8 million members � instituted a program intended to induce doctors and patients to weigh the risks of opioids and consider alternatives.As part of that initiative, first-time opioid prescriptions are limited to 15 days, with a refill allowed for 15 more days. Blue Cross must approve in advance any prescription for longer than a month or for any long-acting opioid such as OxyContin. Pharmacy mail orders for opioids are prohibited.
Doctors and others who prescribe must assess the patient�s risk of abusing drugs and develop a treatment plan that considers options other than opioids. And patients with chronic pain are referred to case managers who advise on therapies other than opioids.
By the end of 2015, the average monthly prescribing rate for opioids decreased almost 15 percent, from 34 per 1,000 members to 29. About 21 million fewer opioid doses were dispensed during the three years covered in the study.37
In another example, Highmark (Pennsylvania) shared data in December 2016 showing that the number of prescriptions for opioids it reimbursed in each of the past three months was lower than in any of the prior nine months. One leading health plan in the state reported that 16 percent of its insured population received at least one opioid prescription in 2016, down from 20 percent in 2015.38 UPMC Health Plan indicated it is using �an algorithm to identify patients who may be at risk for opioid addiction,� and training doctors to use other pain management tools.
Mounting Evidence & Support For Non-Pharmacologic Care For Acute, Subacute & Chronic Back, Neck & Neuro-Musculoskeletal Pain
The earlier sections of this white paper have focused on the continuing and growing problem of opioid use, abuse and addiction. It is essential that this information is understood and appreciated as it clearly calls for a wholesale change in the approach American health care providers and patients bring to the care and management of pain.
No matter what is done to address the use, abuse and addiction associated with opioids it is a fact of life that opioid containing products will continue to be required by individuals suffering severe, intractable and unrelenting pain.This issue is not about the cessation of all opioid use, rather it is about not turning to opioids before they are required, and not until all less onerous approaches to pain management have been exhausted.
We began this discussion with three questions in mind:
�Without the use of drugs, how will they cope with pain?
How can they get referrals and access to drug-free care that will be effective for both acute, subacute and chronic pain?
�How can they ensure that their health care plans and insurance will cover the cost of non- pharmacologic care?
According to new guidelines developed by the American College of Physicians,39 conservative non-drug treatments should be favored over drugs for most back pain. The guidelines are an update that include a review of more than 150 recent studies and conclude that,�For acute and subacute pain, the guidelines recommend non-drug therapies first, such as applying heat, massage, acupuncture, or spinal manipulation, which is often done by a chiropractor.�
The Wall Street Journal
As we have previously noted the CDC, FDA and IOM have all called for the early use of non- pharmacologic approaches to pain and pain management. Unfortunately, beyond asserting the need to move in this direction, little, if any, guidance has been offered to providers, patients and payors on how to accomplish this important transition.
It is a fact that a chasm exists between the worlds of pharmacologic based management of pain, and the non-pharmacologic based management of pain. Medical physicians are not going to suddenly attain knowledge and understanding of practices, procedures and management options that they have never been trained in or exposed to. Similarly, the non-pharmacologic providers addressing pain management do not encounter or understand the barriers that prevent prescribers from directing patients toward non-pharma approaches.These two spheres of healthcare are distinct and separate, and demonstrate little, if any, knowledge about the other.
The first step is to provide resources to prescribers that will detail the indications, effectiveness, efficiency and safety of non-pharmacologic approaches. In particular, the chiropractic profession, through its 70,000 practitioners in the United States, represents a significant and proven non- pharmacologic approach for reducing the need for opioids, opioid-related products and non- opioid pain medications.
Chiropractic, like other complementary health care approaches, suffers from a lack of awareness about its high level of education, credentialing and regulation. In addition, a substantial awareness gap exists among frontline providers in terms of referring patients to chiropractors as part of patient care.
The chiropractic profession and the health care consumer are equally supported by a robust oversight infrastructure.This infrastructure ranges from institutional and programmatic accreditation of chiropractic education by agencies recognized by the U.S. Department of Education to standardize national credentialing examinations and licensure by state agencies and ongoing professional development as a requirement for continued practice in many states.
Typically, after earning a Bachelor of Science, chiropractors follow a four-year curriculum to earn a Doctor of Chiropractic (DC) as a prerequisite to earning the right to independent practice. Chiropractic, medical, osteopathic, dental, optometric and naturopathic education share a similar foundation in the basic sciences, followed by discipline-specific content that focuses on the unique contribution of each provider type. For example, a medical student pursues the study of pharmacology and surgery, while a chiropractic student studies the intricacies of manual approaches to health care and the acquisition of the skills needed to perform spinal adjusting or manipulation.
Chiropractors also pursue specialization in specific areas, such as radiology, through structured residency programs, similar to other disciplines. DCs also pursue focus areas related to various methods of spinal adjusting and related patient management.
For over a century, DCs have studied the relationship between structure, primarily the spine, and function, primarily of the nervous system, and how this interrelationship impacts health and well- being. Due to this emphasis on the spine, chiropractors have become associated with spinal and skeletal pain syndromes, and bring their non-surgical, non-drug rationale to the management of these problems.
DCs are the quintessential example of non-pharmacologic providers of health care with particular expertise in neuro-musculoskeletal conditions.
A Look At The Evidence
While the United States is attempting to deal with its opioid epidemic, our nation is making only limited headway in providing non-pharmacologic approaches to patients with pain.
Over 100 million Americans suffer with chronic pain,40 and an estimated 75 to 85 percent of all Americans will experience some form of back pain during their lifetime. However, 50 percent of
all patients who suffer from an episode of low back pain will have a recurrent episode within one year.41 Surgery has a very limited role in the management of spinal pain, and is only considered appropriate in a handful of cases per hundred patients. Likewise, opioids have very limited utility in the spinal pain environment with the recommended use of these drugs being limited to three days.
Of special relevance, this data relates to the most commonly-reported pain conditions:42
When asked about four common types of pain, respondents of a National Institute of Health Statistics survey indicated that low back pain was the most common (27 percent), followed by severe headache or migraine pain (15 percent), neck pain (15 percent) and facial ache or pain (4 percent).
Back pain is the leading cause of disability in Americans under 45 years old. More than 26 million Americans between the ages of 20-64 experience frequent back pain.
Adults with low back pain are often in worse physical and mental health than people who do not have low back pain: 28 percent of adults with low back pain report limited activity due to a chronic condition, as compared to 10 percent of adults who do not have low back pain. Also, adults reporting low back pain were three times as likely to be in fair or poor health and more than four times as likely to experience serious psychological distress as people without low back pain.
Results of a 2010 study indicate that DCs provide approximately 94 percent of the manipulation services performed in the U.S.,43 with a number of published studies documenting manipulation, along with other drug-free interventions, as effective for the management of neck44 and back pain.45 Most high-quality guidelines target the noninvasive management of nonspecific low back pain and recommend education, staying active/exercising, manual therapy, and paracetamol or NSAIDs as first-line treatments.46
Action Needed
Care pathways and clinical guidelines need to be modified to bring greater attention to the use of non-pharmacologic approaches to pain management. Primary medical care providers must be encouraged to make recommendations or referrals to drug-free resources and appropriate providers, such as DCs, rather than turning to the prescription pad when managing patients who have pain, particularly those with spinal pain. Patients should be educated about non- pharmacologic options for dealing with pain first and foremost, and the dangers of opioids.
For these good intentions to be effective, drug-free pathways will need to be funded by payers in the private sector and government. Government leadership and policy support for introducing innovative reimbursement initiatives by the CMS is a critical step toward allowing health providers to acquire familiarity with non-pharmaceutical approaches.These could frame and stimulate use of evidence-based care options and promote referrals, access to care and reimbursement. By re- engineering these approaches to care to fit the current health care landscape, rather than simply reacting to the opioid crisis by de-emphasizing pain treatment, CMS can better serve patients.
One example: CMS should consider a chronic pain shared-savings program targeting accountable care organizations (ACOs), where success is tied explicitly to patient functional outcomes. Benchmarking against ACO performance measures to determine if care results in savings or losses would allow these organizations to work towards meeting or exceeding quality performance standards � leading to receiving a portion of the savings generated. By incorporating incentives, this type of model would be consistent for more effective integrative intervention for pain.47
Fortunately, progressive thinking is gaining traction in this area. In a January 5, 2017 posting on the CMS Blog, authors wrote that the CMS is focusing on significant programs, including increased use of evidence-based practices for acute and chronic pain management.
�We are working with Medicare and Medicaid beneficiaries, their families and caregivers, health care providers, health insurance plans and states to improve how opioids are prescribed by providers and used by beneficiaries, how opioid use disorder is identified and managed, and how alternative approaches to pain management can be promoted.�48
While we applaud CMS, we feel it is important to point out that this approach begins with a focus on how opioids are prescribed.The focus needs to shift to early applications of non-pharmacologic approaches first and not as a follow-on after the drug path has been established.
Documented Results & Cost Savings
WORKPLACE INJURIES
Back pain is the most common occupational injury in the United States and Canada,49 and represents the most common non-fatal occupational injury, according to the U.S. Bureau of Labor Statistics. Musculoskeletal disorders (MSDs), such as sprains or strains resulting from overexertion in lifting, accounted for 31 percent (356,910 cases) of the total cases for all workers.50
Most recently, Maine Department of Labor data showed injuries to a person�s lumbar region represented 14.3 percent of all injuries reported in 2014, up from 10.7 percent just five years earlier.51 Health care employees have among the highest rates of musculoskeletal injuries for workers, second only to those working in the transportation and warehousing sectors.52
Opiates are not a safe alternative especially when operating heavy machinery, transportation or caring for patients because side effects can alter performance and have tragic outcomes.
Take for example, a 56-year-old nurse at the Maine Medical Center in Portland. She relies on a comprehensive strategy to address her chronic back pain, which originates from having to wear heavy lead aprons when giving radiation treatments, and moving patients and equipment. Her regimen, which includes regularly seeing a chiropractor, exercises, stretches and building up her core muscles, has helped her to control her pain.53
In terms of the value of a �gatekeeper� health care provider for insured workers like this nurse, a study published in Journal of Occupation Rehabilitation (September 17, 2016) cites this factor as
a significant predictor of the duration of the first episode of a worker�s compensation claim. They analyzed a cohort of 5,511 workers, comparing the duration of financial compensation and the occurrence of a second episode of compensation for back pain among patients seen by three types of first health care providers: physicians, chiropractors and physical therapists in the context of workers� compensation.54
When compared with medical doctors, chiropractors were associated with shorter duration of compensation and physical therapists (PT) with longer ones.There was also greater likelihood that PT patients were more likely to seek additional types of care that incurred longer compensation duration.
Additionally, earlier research confirms that on a case adjusted basis 42.7 percent of workers who initially visited a surgeon underwent surgery compared with only 1.5 percent of those who first consulted a chiropractor.55
Medicaid
The National Academy for State Health Policy (NASHP), an independent academy of state health policymakers dedicated to helping states achieve excellence in health policy and practice, recently studied chronic pain management therapies in Medicaid, including policy considerations for non-pharmacological alternatives to opioids. A non-profit and non-partisan organization, NASHP provides a forum for constructive work across branches and agencies of state government on critical health issues.56
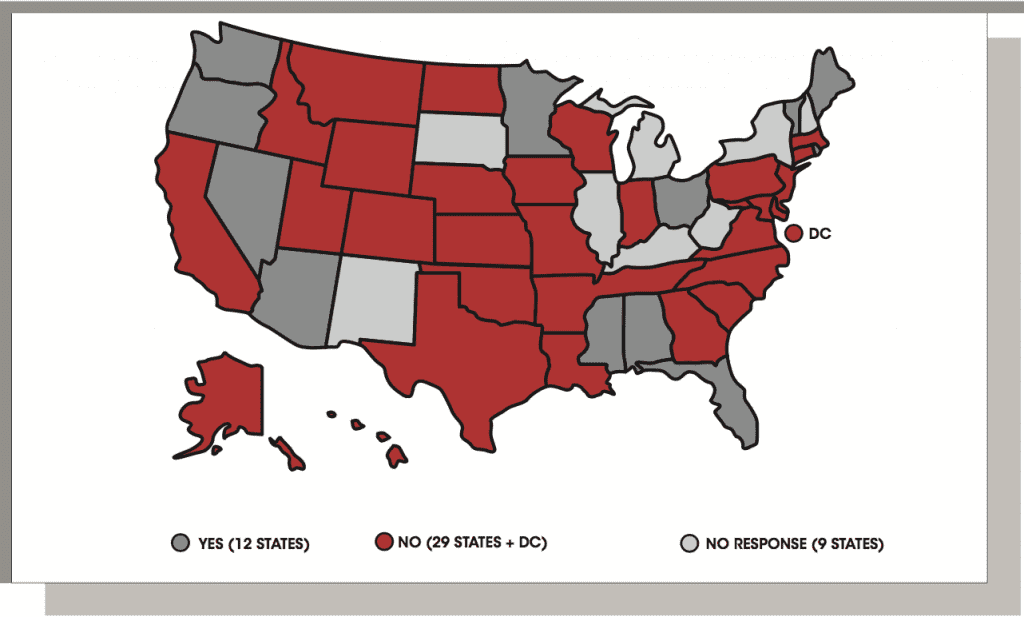
SURVEY RESULTS:
�Has your Medicaid agency implemented specific policies or programs to encourage or require alternative pain management strategies in lieu of opioids for acute or chronic non-cancer pain?�
A September 2016 NASHP report states that although most Medicaid agencies cover services that can be used as alternatives to opioids for pain management, significantly fewer states have policies or procedures in place to encourage their use.
Between March and June 2016, NASHP conducted a survey of all 51 Medicaid agencies to determine the extent to which states have implemented specific programs or policies to encourage or require non-opioid therapies for acute or chronic non-cancer pain.They contacted each Medicaid director via email and, in cases of non-response, followed up with Medicaid medical directors. Ultimately, they received responses from 41 states and the District of Columbia.
Because reimbursement is a key incentive to access alternative care, they also note the most recent results of Medicaid agency reimbursement data from The Henry J. Kaiser Family Foundation (KFF):57
Among the key findings, researchers found most Medicaid agencies cover services that can be used to treat pain in lieu of opioids, but less than half have taken steps to specifically encourage or require their use. Non-pharmacological therapies commonly used to address pain include physical therapy, cognitive behavioral therapy, and exercise, as well as other services, commonly known as Complementary and Alternative Medicine (CAM), including chiropractic manipulation, acupuncture and massage.
They point out that while the current literature on non-pharmacological alternatives is mixed, there is a growing body of evidence to support the use of alternative services to treat chronic pain. For example, a systematic review suggests lower costs for patients experiencing spine pain who received chiropractic care.58
This finding is substantiated in Rhode Island, where the state�s Section 1115 Demonstration authorizes certain individuals enrolled in Medicaid managed care delivery systems to receive CAM services for chronic pain.59 Rhode Island Medicaid has implemented this benefit through its Communities of Care program, a state initiative designed to reduce unnecessary emergency room utilization. Medicaid managed care enrollees with four or more emergency room visits within a 12-month period are eligible to receive acupuncture, chiropractic or massage therapy services.
The state�s two managed care plans, Neighborhood Health Plan of Rhode Island (NHPRI) and United HealthCare of New England, were responsible for developing participation criteria for their enrollees. For example, NPRHI published clinical practice guidelines for its Ease the Pain program, which specified when CAM services referrals were appropriate. Under NHPRI�s guidelines, qualifying individuals diagnosed with back pain, neck pain, and fibromyalgia can be referred for chiropractic services, acupuncture and massage.
Substantiating the results for CAM, Advanced Medicine Integration Group, L.P. in Rhode Island contracted with the two health plans to identify and manage their Medicaid eligible members suffering from chronic pain through its Integrated Chronic Pain Program (ICPP).The target Medicaid population for this program was the Community of Care (CoC) segment — high utilizers of ER visits and opioids/pharmaceuticals.
The objectives of the ICPP are to reduce pain levels (and opioid use), improve function and overall health outcomes, reduce emergency room costs and, through a holistic approach and behavioral change models, educate members in self-care and accountability.
The design of the program for this patient population features holistic nurse case management with directed use of patient education, community services and CAM modalities, including chiropractic care, acupuncture and massage.
Individuals with chronic pain conditions were identified using proprietary predictive modeling algorithms applied to paid claims data to determine opportunities for reducing chronic pain-related utilization and costs.
Results for enrolled CoC Medicaid members with chronic pain conditions document:
�Reduced per member per year (PMPY) total average medical costs by 27 percent
�Decreased the average number of ER visits by 61 percent
Lowered the number of average total prescriptions by 63 percent
�Reduced the average number of opioid scripts by 86 percent
These reductions exceeded by two to three times those reported for a non-enrolled control group of conventionally managed CoC chronic pain patients. Every $1 spent on CAM services and program fees resulted in $2.41 of medical expense savings.
Military
At the time of publication, a study entitled: Assessment of Chiropractic Treatment for Low Back Pain and Smoking Cessation in Military Active Duty Personnel, has completed its clinical trial activities and is currently in the analysis phase. Funded by a four-year grant from the Department of Defense, it is the largest multi-site clinical trial on chiropractic to date, with a total sample size of 750 active- duty military personnel.60
The purpose of this study is to evaluate the effectiveness of chiropractic manipulative therapy for pain management and improved function in active duty service members with low back pain that do not require surgery.The study also measures the impact of a tobacco cessation program delivered to participants allocated to the chiropractic arm.
Low back pain (LBP) is the most common cause of disability worldwide, but it is even more prevalent in active duty military personnel. More than 50 percent of all diagnoses resulting in disability discharges from the military across all branches are due to musculoskeletal conditions. LBP has been characterized as �The Silent Military Threat� because of its negative impact on mission readiness and the degree to which it compromises a fit fighting force. For these reasons, military personnel with LBP need a practical and effective treatment that relieves their pain and allows them to return to duty quickly. It must preserve function and military readiness, address the underlying causes of the episode and protect against re-injury.
This multisite Phase II Clinical Comparative Effectiveness Trial is designed to rigorously compare the outcomes of chiropractic manipulative therapy (CMT) and conventional medical care (CMC) to CMC alone. Chiropractic treatment will include CMT plus ancillary physiotherapeutic interventions. CMC will be delivered following current standards of medical practice at each site. At each of the four participating sites, active military personnel, ages 18 to 50, who present with acute, sub-acute or chronic LBP that does not require surgery will be randomized to one of the two treatment groups.
Outcome measures include the Numerical Rating Scale for pain, the Roland-Morris Low Back Pain and Disability questionnaire, the Back Pain Functional Scale for assessing function, and the Global Improvement questionnaire for patient perception regarding improvement in function. Patient Expectation and Patient Satisfaction questionnaires will be used to examine volunteer expectations toward care and perceptions of that care. Pharmaceutical use and duty status data will also be collected.The Patient Reported Outcomes Measurement Information System (PROMIS-29) will be utilized to compare the general health component and quality of life of the sample at baseline.
Also, because DCs are well positioned to provide information to support tobacco cessation, this clinical trial includes a nested study designed to measure the impact of a tobacco cessation program delivered by a DC.The results will provide critical information regarding the health and mission-support benefits of chiropractic health care delivery for active duty service members in the military.61
This current research was preceded by a pilot study on LBP, conducted at an Army Medical Center in El Paso,Texas, with 91 active-duty military personnel between the ages of 18 and
35.62 Results reported in the journal SPINE showed that 73 percent of those who received standard medical care and chiropractic care rated their improvement as pain �completely gone,��much better� or �moderately better.� In comparison, 17 percent of participants who received only standard medical care rated their improvement this way.These results, as well as other measures of pain and function between the two groups, are considered both clinically and statistically significant.
Recommendations & Next Steps
The opioid crisis has provided a wake-up call for regulators, policy experts, clinicians and payers nationwide. As the support for complementary health techniques builds, interdisciplinary and integrative approaches to chronic pain management are considered best practices.
While the Centers for Disease Control and Prevention�s Guideline validates the need for a shift away from the utilization of opioid prescription painkillers as a frontline treatment option for pain relief, the mention of chiropractic care as a safe, effective and drug-free alternative is omitted.
Instead, CDC recommendations encourage utilization of physical therapy, exercise and over- the-counter (OTC) pain medications prior to prescription opioids for chronic pain.63
�Though the guidelines are voluntary, they could be widely adopted by hospitals, insurers and state and federal health systems.�
CBS News64
The CDC rarely advises physicians on how to prescribe medication — which further adds to the significance of their pronouncements. Many payers and state legislators have already added these findings to their coverage on the use of opioids.
With the likelihood of major players in the industry adopting the well-respected guidelines, it is critical that chiropractic care receives the consideration it deserves.
Chiropractic care has earned a leading role as a pain relief option and is regarded as an important element of the nation�s Opioid Exit Strategy: a drug-free, non-invasive and cost-effective alternative for acute or chronic neck, back and musculoskeletal pain management.
For individuals who may be suddenly �cut-off� from painkillers, chiropractic offers a solution. But access to care will depend upon several important factors:
�Pharmaceutical Industry �Re-engineering�: A change toward responsible marketing and physician education.
�Physician Referrals to Ensure Access to Chiropractic Care: Physician prescribing of chiropractic care rather than opioids.
�Benefit Coverage and Reimbursement for Chiropractic Care: Government and commercial payers as well as plan sponsors have a responsibility to offer patients the option of chiropractic care � and reimburse DCs as participating providers.
�Access to Chiropractic Care for Active Military and Veteran Populations: Chiropractic care should be expanded in the Department of Defense and veterans� health care systems.
As a nation, we have all come to recognize that pain is a complex, multifaceted condition that impacts millions of Americans, their families and caregivers. Unfortunately, the lessons learned about long-term opioid therapy for non-cancer pain have been deadly and heartbreaking.We now understand that there is little to no evidence to support their effectiveness for ongoing chronic pain management.
It is now incumbent upon all stakeholders to increasingly explore the appropriateness, efficacy and cost-effectiveness of alternative pain management therapies and embrace these solutions as a realistic opportunity for America�s Opioid Exit Strategy.
accessed December 8, 2016.
15 Cha, Ariana Eunjung, 2016.
16 Shedrrofsky, Karma, 2016.
17 America�s Painkiller Epidemic, Explained; The Week, February 13, 2016; theweek.com/articles/605224/americas-painkiller-epidemic-explained
18 Wing, Nick; DEA Is Cutting Production Of Prescription Opioids By 25 Percent In 2017; Huffington Post, October 5, 2016; www.huffingtonpost.com/entry/dea-cutting-prescription-opioids_us_57f50078e4b03254526297bd
19 Mulvihill, Geoff, Whyte, Liz Essley, Wieder, Ben; Politics of pain: Drugmakers fought state opioid limits amid crisis; The Center
for Public Inegrity, December 15, 2016. www.publicintegrity.org/2016/09/18/20200/politics-pain-drugmakersfought-state-opioid-limits-amid-crisis;
accessed December 20, 2016.
20 Himani, A, Manohar S., Reddy, Gopal N., Supriya, P.; COMPARISON OF EFFICACY OF BUTORPHANOL AND FENTANYL AS INTRATHECAL
ADJUVANT TO BUPIVACAINE, Journal of Evolution of Medical and Dental Sciences; jemds.com/latest-articles.php?at_id=7552; accessed December 31, 2016.
21 CDC: 10 Most Dangerous Drugs Linked to Overdose Deaths, Health Day, December 22, 2016. www.empr.com/
news/cdc-10-most-dangerous-drugs-linked-to-overdose-deaths/article/580540/; accessed January 1, 2017.
22 Mulvihill et.al.., 2016.
23 Mulvihill et.al.., 2016.
24 Mulvihill, et. al., 2016.
25 Cha, Ariana Eunjung, 2016.
26 Cha, Ariana Eunjung, 2016.
�2017 Foundation for Chiropractic Progress PAGE 27
27 Centers for Disease Control and Prevention. Web-based Injury Statistics Query and Reporting System (WISQARS). 2014
(www.cdc.gov/injury/wisqars/fatal.html).
28 Thompson, Dennis; Drug Overdose Deaths Climb Dramatically in U.S.; HealthDay News, December 20, 2016; consumer.healthday.com/bone-and-joint-information-4/opioids-990/drug-overdose-deaths-climb-dramatically-inu-s-717988.html;
accessed December 23, 2016.
29 Bernstein, Lenny; Crites, Alice, Higham, Scott, and Rich, Steven; Drug industry hired dozens of officials from the DEA as
the agency tried to curb opioid abuse; The Washington Post, December 22, 2016; www.washingtonpost.com/
investigations/key-officials-switch-sides-from-dea-to-pharmaceutical-industry/2016/12/22/55d2e938-c07b-11e6-b527-
949c5893595e_story.html.
30 Siegel, Marc, MD; We doctors are enablers: A physician�s take on the opioid epidemic; FOXNews, December 21, 2016; www.foxnews.com/opinion/2016/12/21/doctors-are-enablers-physicians-take-on-opioid-epidemic.html;
accessed January 4, 2017.
31 Freyer, Felice J.; Doctors are cutting opioids, even if it harms patients; Boston Globe, January 3, 2017; www.bostonglobe.com/metro/2017/01/02/doctors-curtail-opioids-but-many-see-harm-pain-patients/z4Ci68TePafcD9AcORs04J/story.html.
32 Blair, Nolan; Doctors prescribing less opioids; ABC WBAY.com, November 2, 2016. wbay.com/2016/11/02/report-finds-decrease-in-opioid-prescriptions/
33 Centers for Disease Control; www.cdc.gov/drugoverdose/pdmp/; accessed January 5, 2017.
34 Lord, Rich; Attention to opioids may be curbing doctors prescriptions; Pittsburgh Post-Gazette, December 26, 2016; http://
www.post-gazette.com/news/overdosed/2016/12/26/Attention-to-opioids-may-be-curbing-doctors-prescriptions/stories/201612260013
35 Nuzum, Lydia; Opioid prescriptions in US, WV down for first time in two decades; The Charleston Gazette-Mail, June 6, 2016. www.wvha.org/Media/NewsScan/2016/June/6-6-16-Opioid-prescriptions-in-US,-WV-down-for-fir.aspx
36 Freyer, Felice J.; Opioid prescriptions drop among patients covered by state�s biggest insurer; Boston Globe, October 20,
2016; www.bostonglobe.com/metro/2016/10/20/opioid-prescriptions-drop-significantly-among-patients-covered-state-biggest-insurer/06jIYorfogaG2o8Wrhr8ZN/story.html
37 Freyer, Felice J., 2016.
38 U.S. Agency for Healthcare Research and Quality, Opioid Overdoses Burden U.S. Hospitals: Report, HealthDay News, December
15, 2016. consumer.healthday.com/public-health-information-30/heroin-news-755/opioid-overdoses-taketoll-on-u-s-hospitals-717872.html;
accessed December 16, 2016.
39 Reddy, S. (2017, February 13). No Drugs for Back Pain, New Guidelines Say. Retrieved from www.wsj.com/articles/no-drugs-for-back-pain-new-guidelines-say-1487024168
40 Institute of Medicine Report from the Committee on Advancing Pain Research, Care, and Education: Relieving Pain in
America, A Blueprint for Transforming Prevention, Care, Education and Research. The National Academies Press, 2011. books.nap.edu/openbook.php?record_id=13172&page=1.
41 American Association of Neurological Surgeons; Low Back Pain, May 2016. www.aans.org/Patientpercent20Information/Conditionspercent20andpercent20Treatments/Lowpercent20Backpercent20Pain.aspx
42 American Academy of Pain Medicine; Facts and Figures About Pain; www.painmed.org/PatientCenter/Facts_on_Pain.aspx#refer; accessed January 7, 2017.
43 Daniel C. Cherkin, Robert D. Mootz; Chiropractic in the United States: Training, Practice, and Research, 2010.
Chiropractic in the United States: Training, Practice, and Research�; accessed January 17, 2017.
44 Wong, J. J., Shearer, H. M., Mior, S., Jacobs, C., C�t�, P., Randhawa, K., . . . Taylor-Vaisey, A. (2016). Are manual therapies, passive
physical modalities, or acupuncture effective for the management of patients with whiplash-associated disorders or
neck pain and associated disorders? An update of the Bone and Joint Decade Task Force on Neck Pain and Its Associated
Disorders by the OPTIMa collaboration. The Spine Journal, 16(12), 1598-1630. doi:10.1016/j.spinee.2015.08.024.
45 Spinal Manipulation for Low-Back Pain. (2016, April 20). Retrieved January 17, 2017, from nccih.nih.gov/health/pain/spinemanipulation.htm.
46 Wong, J., C�t�, P., Sutton, D., Randhawa, K., Yu, H., Varatharajan, S., . . . Taylor-Vaisey, A. (2016). Clinical practice guidelines for
the noninvasive management of low back pain: A systematic review by the Ontario Protocol for Traffic Injury Management
(OPTIMa) Collaboration. European Journal of Pain, 21(2), 201-216. doi:10.1002/ejp.931
47 Doctor, Jason, October 4, 2016.
48 Goodrich, Kate, MD; Agrawal, Shantanu, MD; The CMS Blog; Addressing the Opioid Epidemic: Keeping Medicare and Medicaid
Beneficiaries Healthy, January 5, 2017; blog.cms.gov/2017/01/05/addressing-the-opioid-epidemic/
49 Deyo RA, Mirza SK, Martin BI. Back pain prevalence and visit rates: estimates from U.S. national surveys, 2002. Spine.
2006;31(23):2724�7. doi:10.1097/01.brs.0000244618.06877.cd
PAGE 28 �2017 Foundation for Chiropractic Progress
CHIROPRACTIC � A KEY TO AMERICA’S OPIOID EXIT STRATEGY
50 Bureau of Labor Statistics; Nonfatal Occupational Injuries and Illnesses Requiring Days Away From Work, 2015,
November 10, 2016; www.bls.gov/news.release/osh2.nr0.htm; accessed January 8, 2017.
51 Lawlor, Joe; Back injuries most common type of injuries for workers; Portland Press Herald, October 16, 2016; www.
pressherald.com/2016/10/16/back-injuries-most-common-type-of-injuries-for-workers/; accessed 1.8.2017.
52 Lawlor, Joe; 2016.
53 Lawlor, Joe; 2016.
54 Blanchette, MA., Rivard, M., Dionne, C.E. et al. J Occup Rehabil (2016). doi:10.1007/s10926-016-9667-9; link.springer.com/article/10.1007/s10926-016-9667-9.
55 Keeney BJ, et al. Early predictors of lumbar spine surgery after occupational back injury: results from a prospective study
of workers in Washington State. Spine 2013 May 15;38(11):953-64.
6 Dorr, Hannah and Townley, Charles; Chronic Pain Management Therapies in Medicaid: Policy Considerations for Non-Pharmacological
Alternatives to Opioids; National Academy for State Health Policy, September 2, 2016; nashp.org/chronic-pain-management-therapies-medicaid-policy-considerations-non-pharmacological-alternatives-opioids/
57 It is important to note that the KFF data tracks which states allow direct reimbursement to the specific provider type (e.g.,
directly reimbursing a physical therapist for physical therapy services); states that do not directly reimburse these providers
may actually cover the service if billed by another provider (e.g., an institutional setting). For more information, please
see the notes in the following references.
Kaiser Family Foundation. �Medicaid Benefits: Physical Therapy Services.� Retrieved August 24, 2016. kff.org/medicaid/state-indicator/physical-therapy-services/
Kaiser Family Foundation. �Medicaid Benefits: Psychologist Services.� Retrieved August 24, 2016. kff.org/medicaid/state-indicator/psychologist-services/
Kaiser Family Foundation. �Medicaid Benefits: Occupational Therapy Services.� Retrieved August 24, 2016.http://
kff.org/medicaid/state-indicator/occupational-therapy-services/
Kaiser Family Foundation. �Medicaid Benefits: Chiropractor Services.� Retrieved August 24, 2016. kff.org/medicaid/state-indicator/chiropractor-services/
58 Dagenais, S., Brady, O., Haldeman, S., & Manga, P. 2015, October 19. A systematic review comparing the costs of
chiropractic care to other interventions for spine pain in the United States. Retrieved February 08, 2017, from www.ncbi.nlm.nih.gov/pmc/articles/PMC4615617/
59 Neighborhood Health Plan of Rhode Island Clinical Practice Guideline, Complementary and Alternative Medicine (CAM).
December 18, 2014.
60 U.S. National Institutes of Health; Assessment of Chiropractic Treatment for Low Back Pain and Smoking Cessation in Military
Active Duty Personnel; clinicaltrials.gov/ct2/show/NCT01692275; accessed January 8, 2017.
61 U.S. National Institutes of Health
62 Goertz, Christine M. DC, PhD, et. al; Adding Chiropractic Manipulative Therapy to Standard Medical Care for Patients With
Acute Low Back Pain: Results of a Pragmatic Randomized Comparative Effectiveness Study; SPINE, Volume 38, Issue 8,
April 15, 2013; journals.lww.com/spinejournal/Abstract/2013/04150/Adding_Chiropractic_Manipulative_Therapy_to.2.aspx
63 Dowell D, Haegerich TM, Chou R. CDC Guideline for Prescribing Opioids for Chronic Pain � United States, 2016. MMWR
Recomm Rep 2016;65(No. RR-1):1�49. DOI: dx.doi.org/10.15585/mmwr.rr6501e1.
64 CBS News/AP. (2016, March 15). CDC guidelines aim to reduce epidemic of opioid painkiller abuse. Retrieved January 15,
2017, from www.cbsnews.com/news/opioid-painkiller-guidelines/.
Foundation For Chiropractic Progress�
BOARD OF DIRECTORS
Kent S. Greenawalt, CEO, Foot Levelers; Chairman of the Board of Directors, F4CP
Mickey G. Burt, DC, Executive Director of Alumni and Development, Palmer College of Chiropractic Gerard W. Clum, DC, Director, The Octagon, Life University
Kristine L. Dowell, Executive Director, Michigan Association of Chiropractors
Joe Doyle, Publisher, Chiropractic Economics
Charles C. Dubois, President/CEO, Standard Process, Inc.
J. Michael Flynn, DC
R. A. Foxworth, DC, FICC, MCS-P, President, ChiroHealthUSA
Arlan W. Fuhr, Chairman/Founder, Activator Methods International Ltd.
Greg Harris, Vice President for University Advancement, Life University
Kray Kibler, CEO, ScripHessco
Thomas M. Klapp, DC, COCSA Representative
Carol Ann Malizia, DC, CAM Integrative Consulting
Fabrizio Mancini, DC, President Emeritus, Parker University
Brian McAulay, DC, PhD
William Meeker, DC, MPH, President, Palmer College of Chiropractic � San Jose Campus
Robert Moberg, CEO, Chirotouch
Donald M. Petersen, Jr., Publisher, MPA Media
Mark Sanna, DC, FICC, ACRB, Level II, President, Breakthrough Coaching
Paul Timko, Vice President/General Manager of U.S. Clinical Business, Performance Health
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine